Embed Size (px)
Citation preview

Ola Didrik SaugstadOla Didrik Saugstad
Department of Pediatric ResearchDepartment of Pediatric ResearchRikshospitalet, University of OsloRikshospitalet, University of Oslo NORWAYNORWAY
Resucitation of newborn infants
•6-10 out of 130 mill newborns need intervention at birth
FactsFacts
•Most newborn infantsare born outsidehospitals withouthealth personelattending
•1 mill die and a similar numberdevelop sequels due to birthasphyxia (CP, Epilepsia)
•4 mill birth asphyxia
Newborn Resuscitation
Guidelines
Is newborn resuscitation Is newborn resuscitation evidence based?evidence based?
AHA and AAP in their last guidelines (2000) AHA and AAP in their last guidelines (2000) summarised the literature and tried to determine summarised the literature and tried to determine what is and what is not evidence basedwhat is and what is not evidence based
If a procedure is not evidence based If a procedure is not evidence based evidenced based information should be collected evidenced based information should be collected before the procedure in case is changedbefore the procedure in case is changed
Resuscitation of Newborn Infants
WHO: Basic Newborn Resuscitation (WHO, Geneva 1998)
ILCOR: An Advisory Statement From the Pediatric Working Group of the International Liason Committee on Resuscitation.
(Pediatrics, April 1999)
AHA/AAP: International Guidelines for Neonatal Resuscitation. (Pediatrics September 2000)
WHO guidelines
Anticipate• Be prepared for every birth by having skill to
resuscitate and by knowing the institutions policy on resuscitation
• Review the risk factors for birth asphyxia
• Clearly decide on the responsibilities of each health care provider during resuscitation
• Remember that the mother is also at risk of complications
WHO Guidelines
Risk factors for birth asphyxiamaternal illness traumatic delivery
sexually transmitted diseases prolapsed cord
malaria mec stained amniot fluid
eclampsia congenital anomaly
maternal bleeding prolonged labour
maternal sedation breech/other abn presnt
fever during labour PROM
WHO Guidelines 1998Prepare for birth• two clean towels for thermal protection and small)• a suction device ( mucus extractor)• a radiant heater (if available• a draught-free delivery room > 25oC • clean delivery kit for cord care, gloves• two infant masks (normal)• a blanket• a clock• an additional set of equipment in reserve for multiple births or in case of failure of the first
set• inform mother• open the airway - clear the airway by suctioning first the mouth and then the nose• ventilate with appropriate mask (size 1 for a normal weight and 0 for a small newborn)• observe the rise of the chest• ventilate 40 (30-60) breaths/min• stop an look for spontaneous breathing after about 1 min
Recommendations resulting from collaboration among
–AHA Pediatric Subcommittee–ILCOR Pediatric Working Group
–AAP Neonatal Resuscitation Program
AHA/AAP 2000
Textbook and video is availablewww.aap.org
Newborn ResuscitationAHA/AAP Guidelines
• Meconium -stained amniotic fluid: endotracheal suctioning of the depressed - not the vigorous child
• Hyperthermia should be avoided
• 100% oxygen is still recommended, however if supplemental oxygen is unavailable room air should be used
• Chest compression: Initiated if heart rate is absent or remains < 60 bpm despite adequate ventilation for 30 sec
• Medications: Epinephrine 0.01-0.03 mg/kg if heart rate < 60 bpm in spite of 30 seconds adequate ventilation and chest compression
• Volume: Isotonic crystalloid solution or 0-neg blood
Summary of changes from 1992
Newborn Resuscitation
Physiology
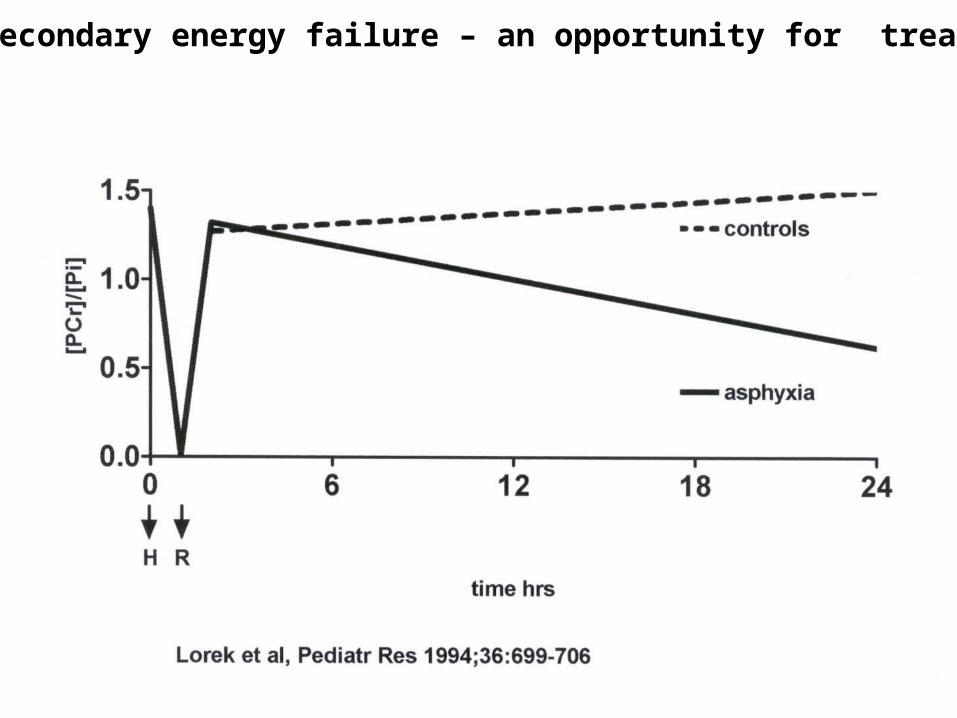
Secondary energy failure – an opportunity for treatment
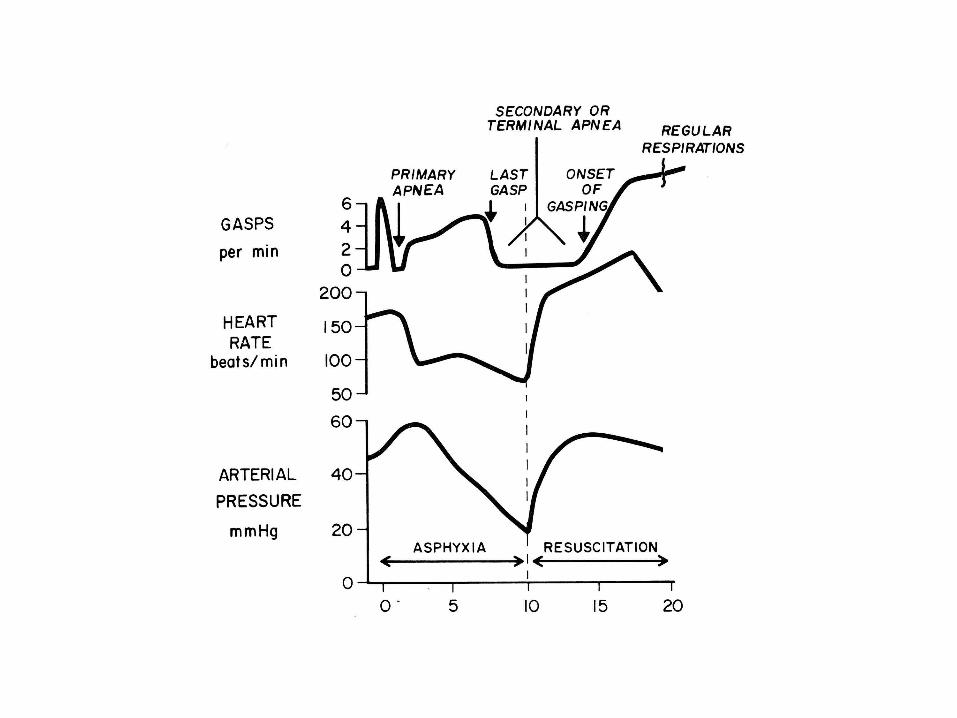
Perinatal asphyxia – some basic facts
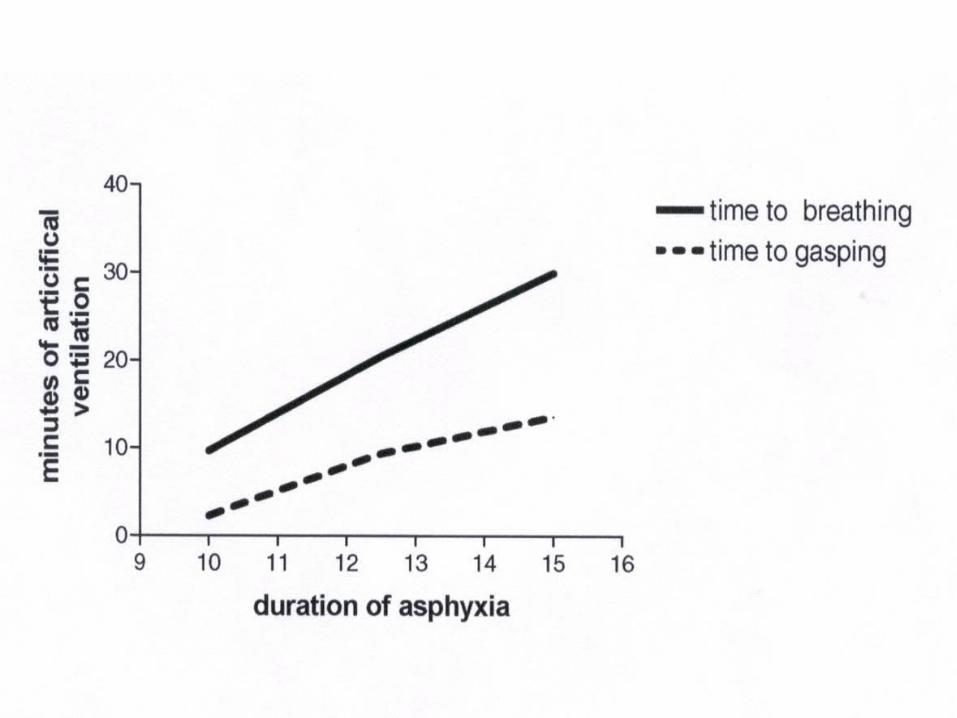
•Primary to 2nd apnea lasts 8-10 min. Auto resuscitation possible
•Secondary apnea about 10 min asphyxia. Auto resuscitation not possible
•pCO2 10 mm Hg (1.3 kPa) /min
•Serum potassium 15 mmol/L after 10 min
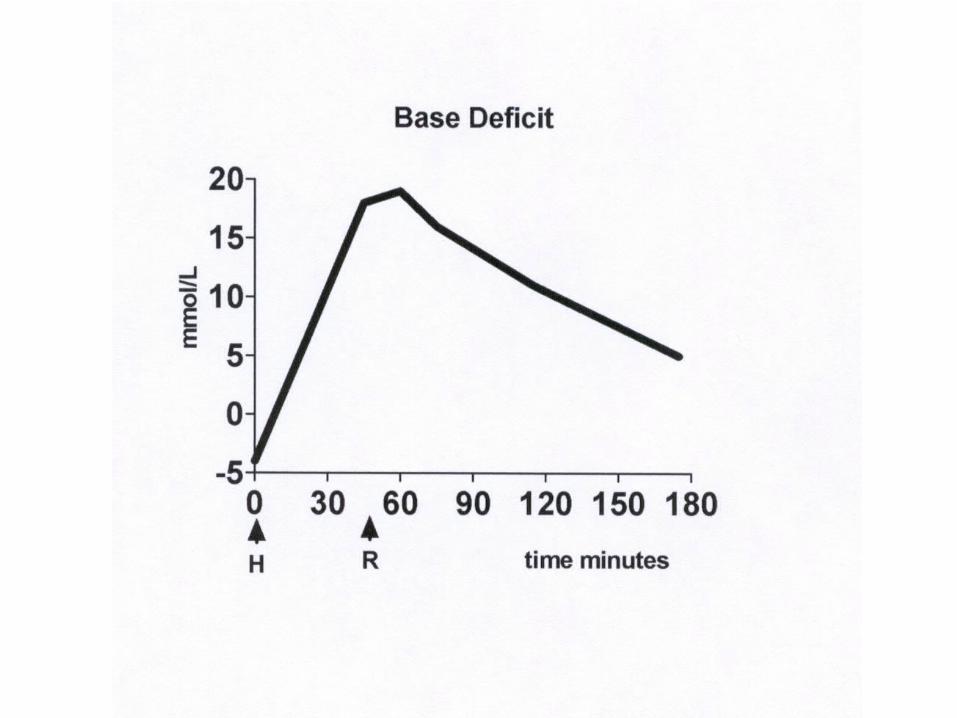
•Base deficit 2/5 mmol/L/min in 8% O2
2/3 mmol/L/min in 6% O2
Newborn Resuscitation
Clinical sequences
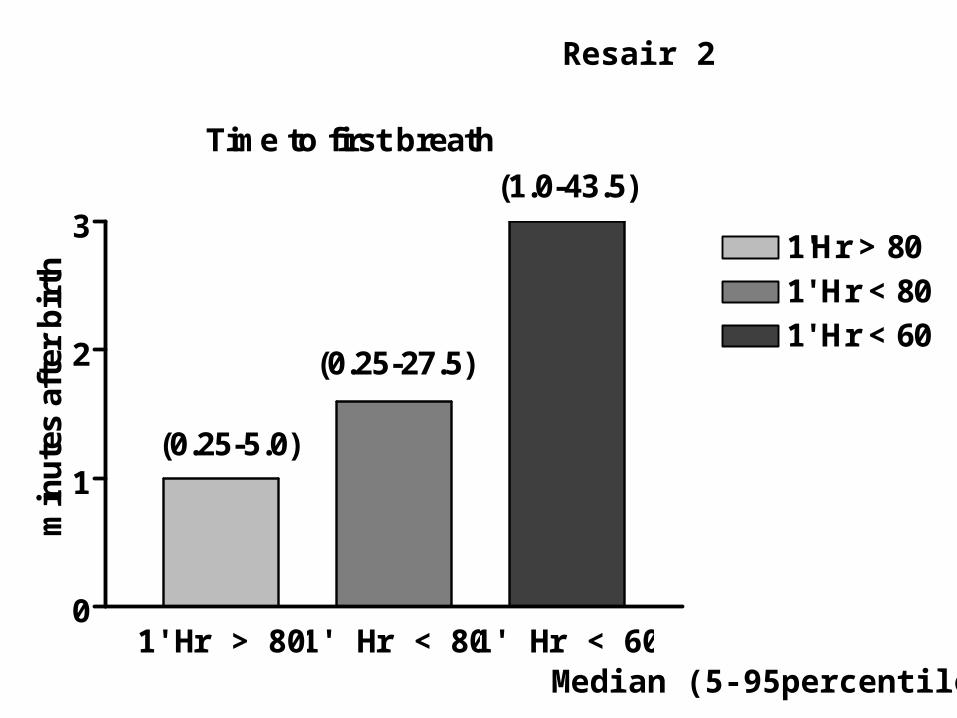
1'Hr > 80 1' Hr < 80 1' Hr < 600
1
2
31'Hr > 801' Hr < 801' Hr < 60
Time to first breath
min
ute
s af
ter
bir
th
(0.25-5.0)
(0.25-27.5)
(1.0-43.5)
Resair 2
Median (5-95percentile)
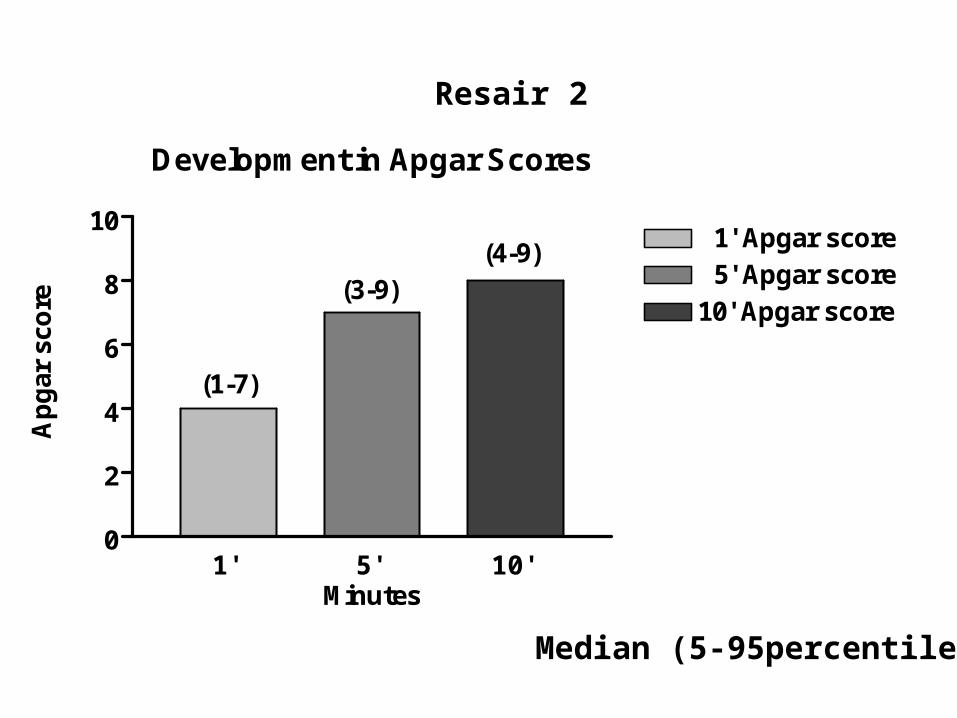
Development in Apgar Scores
1' 5' 10'0
2
4
6
8
10 1' Apgar score 5' Apgar score10' Apgar score
(1-7)
(3-9)(4-9)
Minutes
Ap
gar
sco
re
Resair 2
Median (5-95percentile)
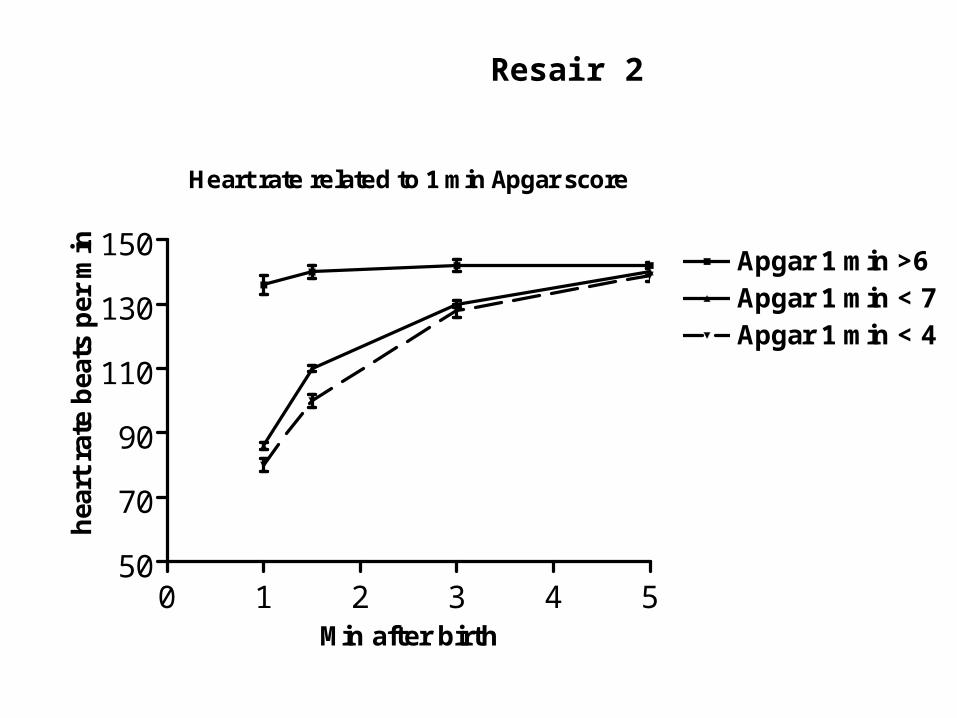
Heart rate related to 1 min Apgar score
0 1 2 3 4 550
70
90
110
130
150Apgar 1 min >6Apgar 1 min < 7Apgar 1 min < 4
Min after birth
hea
rt r
ate
bea
ts p
er m
inResair 2
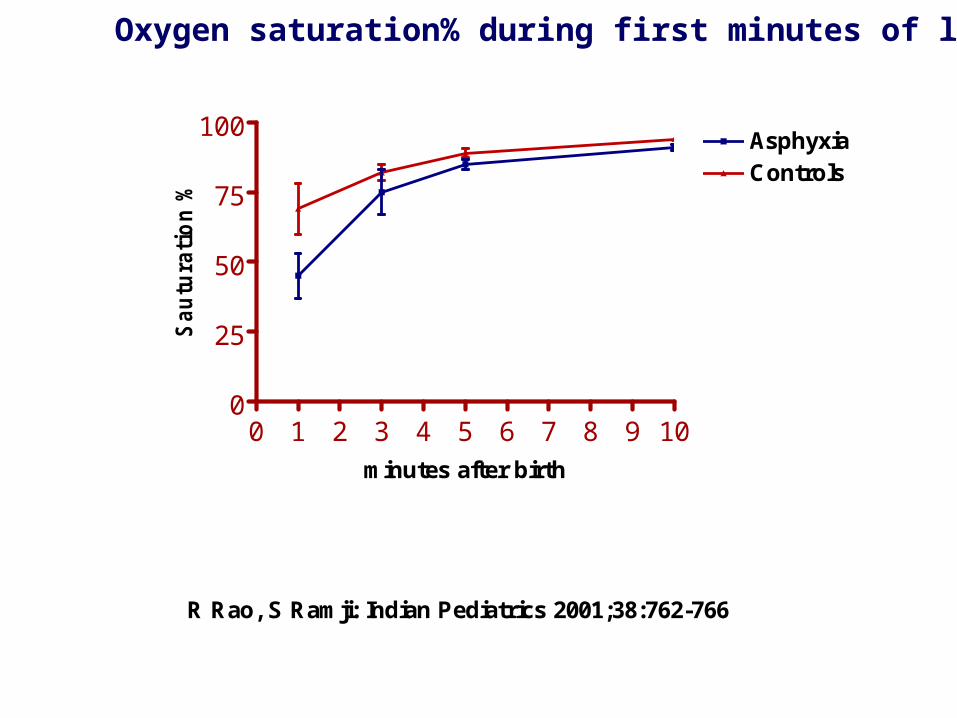
0 1 2 3 4 5 6 7 8 9 100
25
50
75
100AsphyxiaControls
R Rao, S Ramji: Indian Pediatrics 2001;38:762-766
minutes after birth
Sau
tura
tio
n %
Oxygen saturation% during first minutes of life
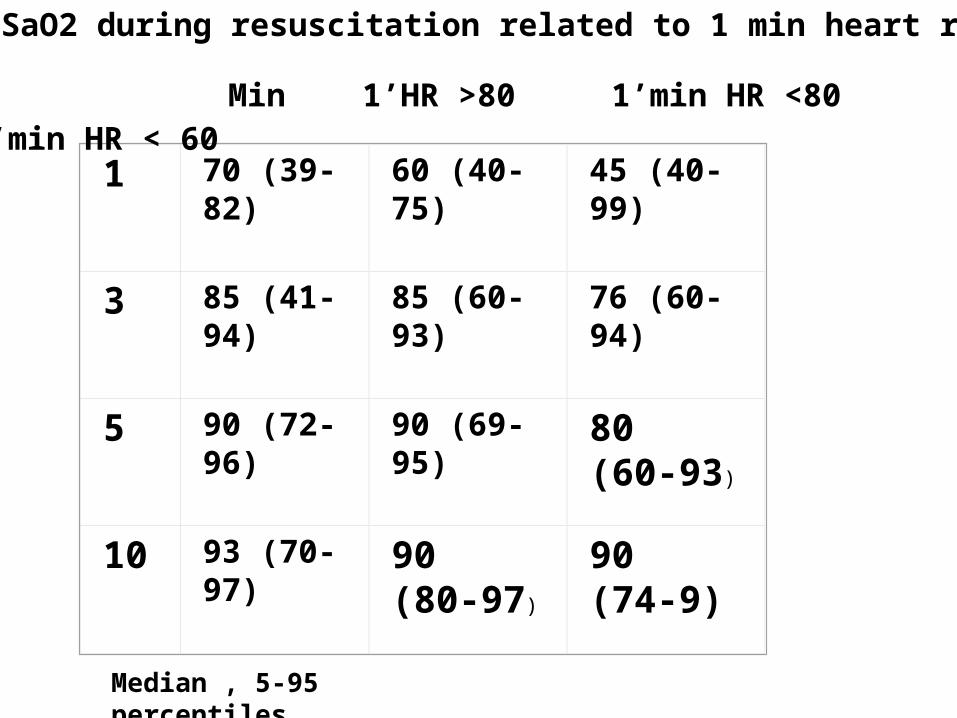
1 70 (39-82) 60 (40-75) 45 (40-99)
3 85 (41-94) 85 (60-93) 76 (60-94)
5 90 (72-96) 90 (69-95) 80 (60-93)
10 93 (70-97) 90 (80-97) 90 (74-9)
Min 1’HR >80 1’min HR <80 1’min HR < 60
SaO2 during resuscitation related to 1 min heart rate
Median , 5-95 percentiles
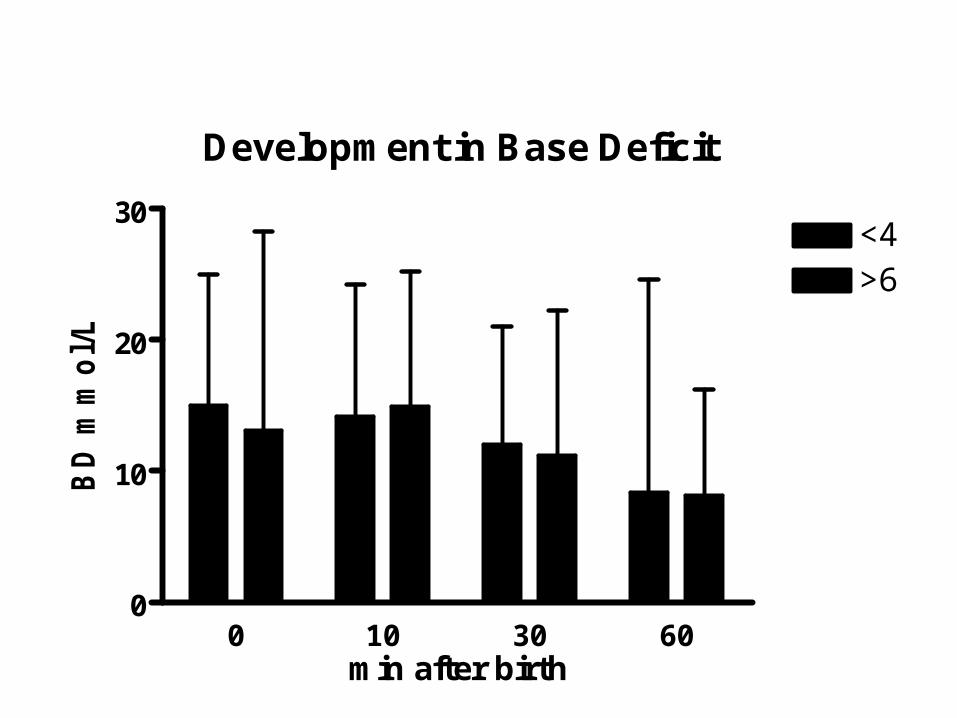
Development in Base Deficit
0 10 30 600
10
20
30<4>6
min after birth
BD
mm
ol/
L
Newborn Resuscitation
How to carry out?
Neonatal Resuscitation
• Is the amniotic fluid clear of meconium?
• Is the baby breathing or crying?
• Is there a good muscle tone?
• Is the color pink?
• Was the baby born at term?If the answer is no to any of these consider resuscitation
The following questions should be answered after
every birth:
Be prepared: every newborn baby might need resuscitation!
AAP/AHA
Neonatal Resuscitation
AHA/AAP (2000)Four Categories• Basic steps including rapid assessments
and initial steps of stabilisation• Ventilation, including bag-mask or bag -
tube ventilation• Chest compression• Administration of medications or fluids

Facts About Newborn ResuscitationThe most important is to get air into the lungs
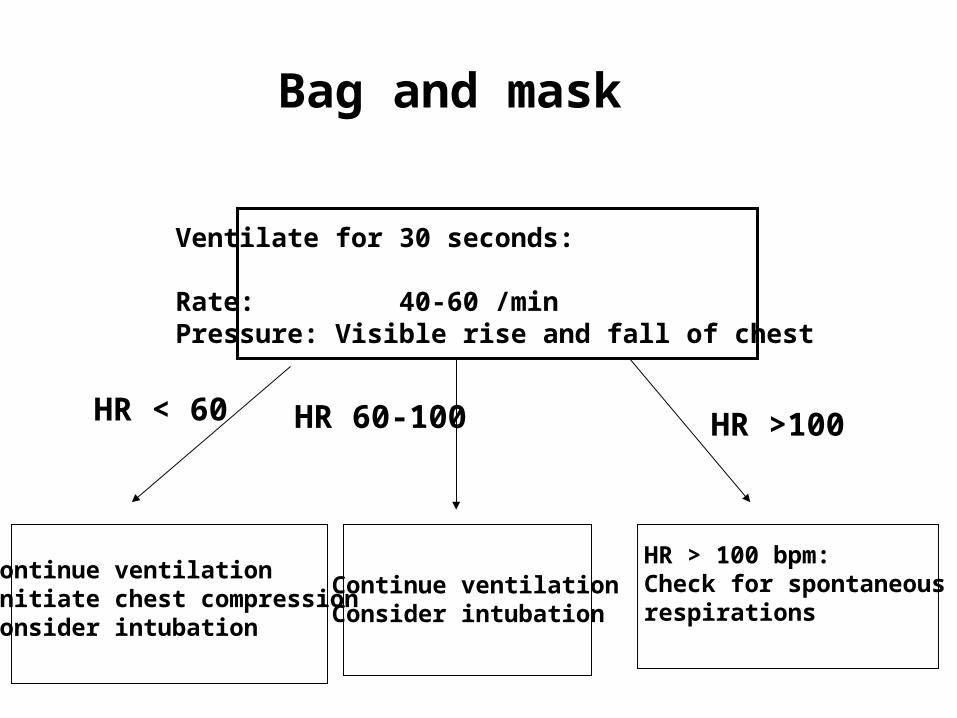
Bag and mask
Ventilate for 30 seconds:
Rate: 40-60 /minPressure: Visible rise and fall of chest
Continue ventilationInitiate chest compressionConsider intubation
Continue ventilationConsider intubation
HR > 100 bpm:Check for spontaneousrespirations
HR < 60 HR 60-100 HR >100

Bag and mask the most important tool in newborn resuscitation
0
2
4
6
8
10
12
14
16
18
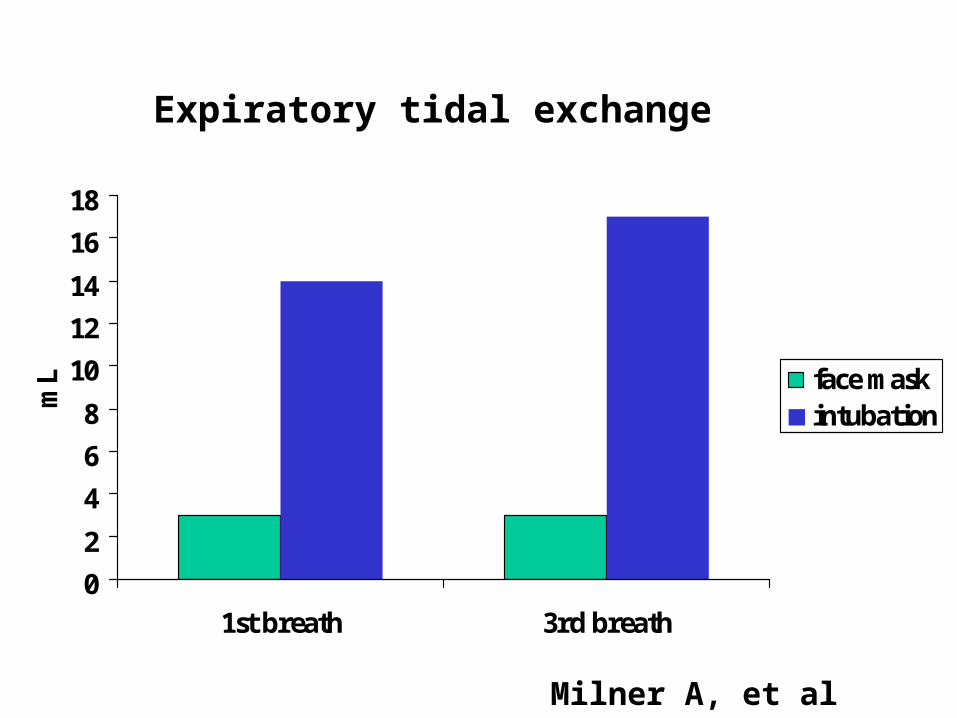
1st breath 3rd breath
mL face mask
intubation
Expiratory tidal exchange
Milner A, et al
Ventilation
Even a few (6) blows with a too high tidal volume (35-40 mL/kg) before surfactant destroys the lungs of premature lambs
A too high or a too low tidal volume triggers inflammatory changes in the lungs leading to influx of phagocytes, proinflammatory cytokines increase
Neonatal ResuscitationChest compressions - indication
Chest compressions should be performed if the heart rate is < 60 beats/minute, despite adequate ventilation with 100% oxygen for 30 seconds. [ILCOR 1999 Advisory Statement],AHA- AAP 2000
Chest compression
If: HR < 60 after 30 seconds ventilation and stimulation
• Thumb technique: Place your thumbs side by side or, on a small baby, one over the other, immediately above xyphoid. The other fingers provide support needed for the back
• Pressure so that you depress the sternum to a depth of approximately1/3 of the anterior/posterior diameter of the chest. Then release.
• The downward stroke should be somewhat shorter than duration of the release.
• Your thumbs should remain in contact with the chest at all times
• 90 compressions + 30 breaths per min
”One and two and three and breath, and one and two and three and breath …”
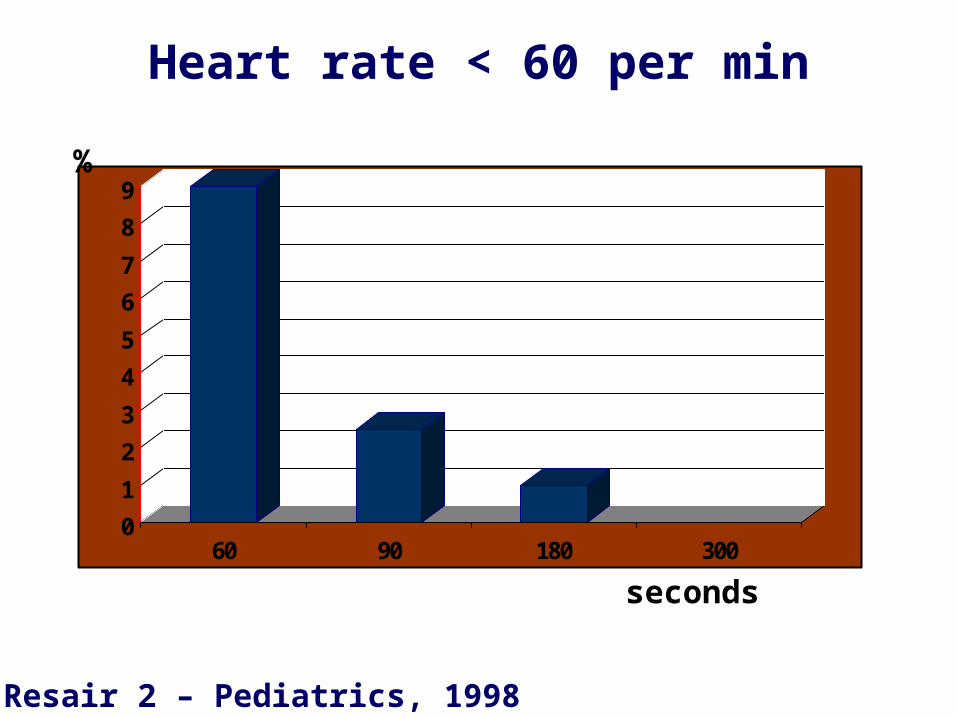
Heart rate < 60 per min
0
1
2
3
4
5
6
7
8
9
60 90 180 300
seconds
%
Resair 2 – Pediatrics, 1998

Chest compression 19%
But needed in only 1-2% …
RESAIR 2
Neonatal Resuscitation Room air vs. 100% Oxygen
If assisted ventilation is required, 100% oxygen should be delivered by positive pressure ventilation … If supplemental oxygen is not available, resuscitation of the newly born infant should be initiated with positive pressure ventilation and room air. AAP/AHA 2000:Not sufficient data to change present guidelines (grandfather principle)
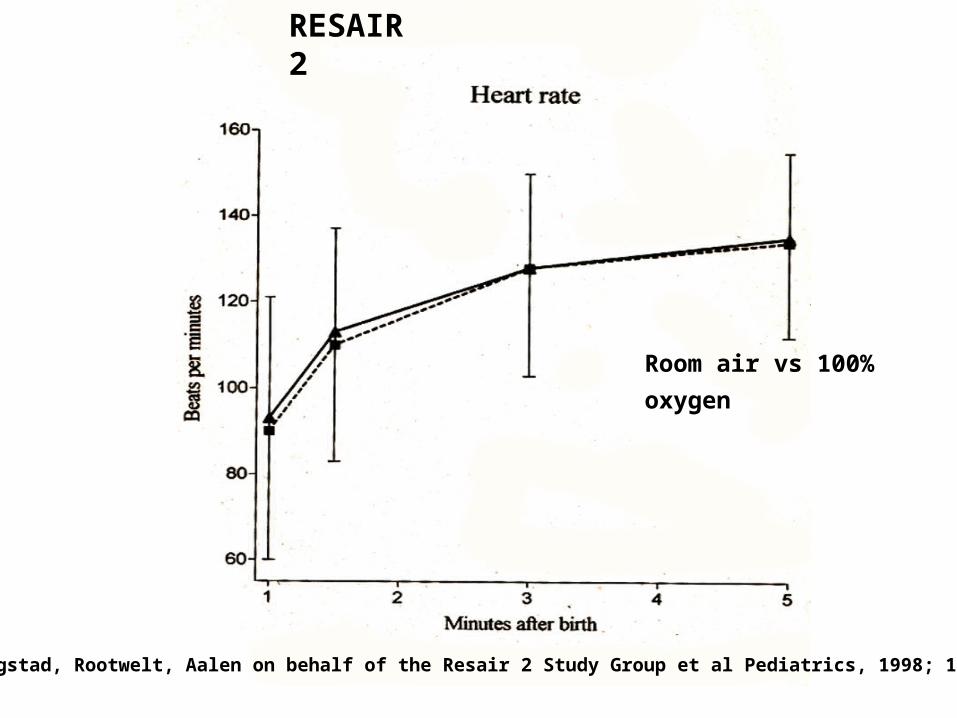
Saugstad, Rootwelt, Aalen on behalf of the Resair 2 Study Group et al Pediatrics, 1998; 102:e1
RESAIR 2
Room air vs 100% oxygen
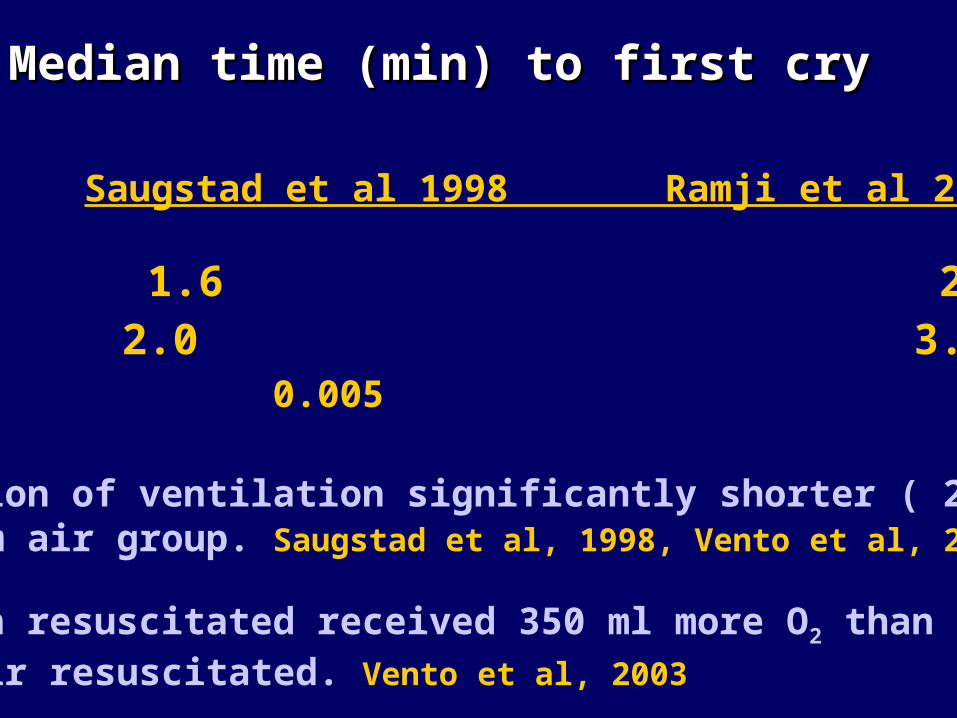
Saugstad et al 1998 Ramji et al 2003
21% O2 1.6 2.0100% O2 2.0 3.0 p 0.005 0.008
•Duration of ventilation significantly shorter ( 2 min) in room air group. Saugstad et al, 1998, Vento et al, 2001
•Oxygen resuscitated received 350 ml more O2 than room air resuscitated. Vento et al, 2003
Median time (min) to first cryMedian time (min) to first cry
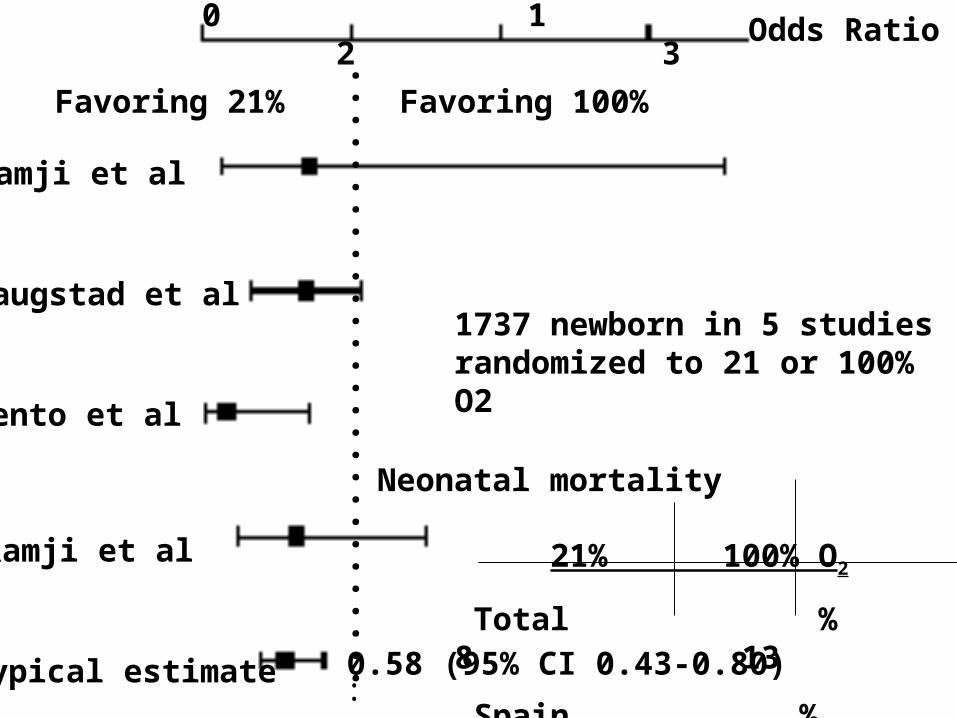
0 1 2 3
Ramji et al
Saugstad et al
Vento et al
Ramji et al
Typical estimate
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.:
Odds Ratio
0.58 (95% CI 0.43-0.80)
Neonatal mortality
Favoring 21% Favoring 100%
1737 newborn in 5 studies randomized to 21 or 100% O2
21% 100% O2
Total % 8 13
Spain % 0.5 3.5
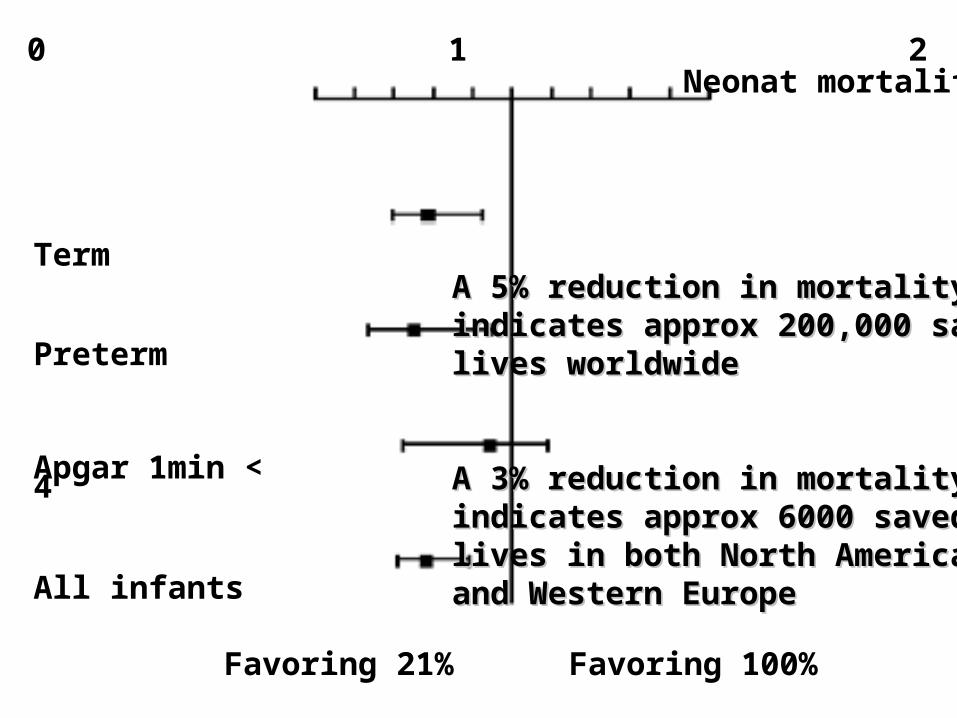
0 1 2 odds ratio
Term
Preterm
Apgar 1min < 4
All infants
Favoring 21% Favoring 100%
Neonat mortality
A 5% reduction in mortality A 5% reduction in mortality indicates approx 200,000 saved indicates approx 200,000 saved lives worldwidelives worldwide
A 3% reduction in mortalityA 3% reduction in mortalityindicates approx 6000 saved indicates approx 6000 saved lives in both North Americalives in both North Americaand Western Europeand Western Europe
Adverse effects of resuscitation with 100% O2
•Prolonges time to first breath
•Prolonges duration of positive pressure ventilation
•Increases neonatal mortality 3% in industrialised, 5% in developing countries
\
•Elevates oxidative stress (at least 4 weeks)
• Associated with acute lymphatic leukemia
Clinical data
Experimental data
• Inflammation in brain, myocardium and lungs•Increases neuronal damage?•Poorer neurological outcome
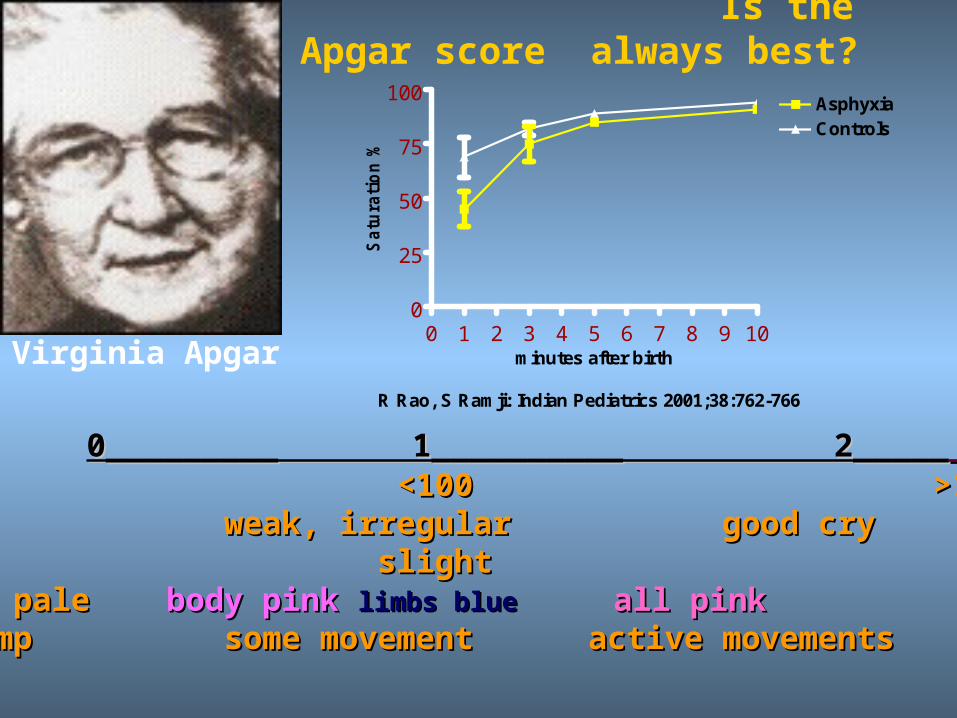
Is the highest Apgar score always best?
0_________ 1__________ 2_____0_________ 1__________ 2_____ Heart rateHeart rate 0 <100 >100 0 <100 >100 RespirationRespiration 0 weak, irregular good cry 0 weak, irregular good cry ReactionReaction 0 slight good 0 slight goodColourColour blue or pale blue or pale body pink body pink limbs bluelimbs blue all pinkall pinkTone Tone limp some movement active movements limp some movement active movements limbs well flexedlimbs well flexed
Virginia Apgar0 1 2 3 4 5 6 7 8 9 10
0
25
50
75
100AsphyxiaControls
R Rao, S Ramji: Indian Pediatrics 2001;38:762-766
minutes after birthS
atu
rati
on
%
Drugs needed forNewborn Resuscitation
Neonatal ResuscitationEpinephrine dose
The recommended IV or endotracheal dose of epinephrine is 0.1 to 0.3 mL/kg of a 1:10,000 solution (0.01 to 0.03 mg/kg) repeated every 3 to 5 minutes as indicated.
Higher doses have been associated with increased risk of intracranial hemorrhage and myocardial damage.
No different dose for premature infants
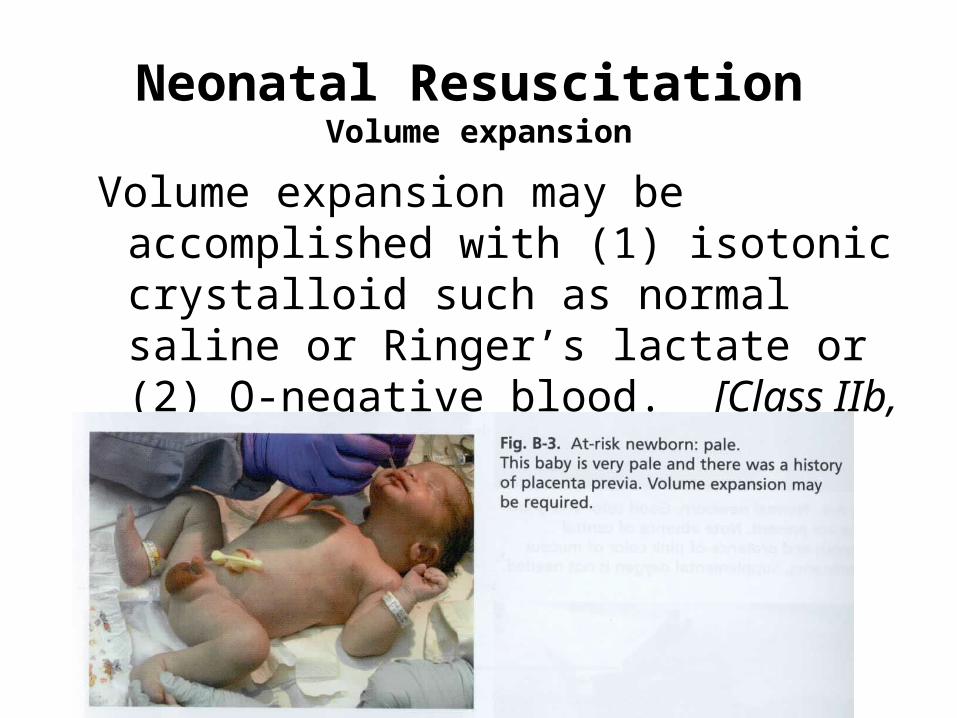
Neonatal Resuscitation Volume expansion
Volume expansion may be accomplished with (1) isotonic crystalloid such as normal saline or Ringer’s lactate or (2) O-negative blood. [Class IIb, level 7 evidence]
Neonatal Resuscitation Cerebral Hypothermia
Cerebral hypothermia cannot presently be recommended for newly born infants who have experienced severe perinatal asphyxia.
Hyperthermia appears to be injurious and should be avoided.
Neonatal Resuscitation Ethics
There are circumstances in which non-initiation or discontinuation of resuscitation in the delivery room may be appropriate…
AHA-AAP 2000
Neonatal Resuscitation Ethics
Non-initiation of resuscitation in the delivery room may be appropriate in infants with:
• confirmed gestation < 23 weeks• birthweight < 400 grams• anencephaly • confirmed trisomy 13 or 18 may be appropriate.
Current data support that resuscitation of these newborns is very unlikely to result in survival or survival without severe disability.
AHA/AAP 2000
Neonatal Resuscitation Ethics
In cases of uncertain prognosis, including uncertain gestational age, a trial of therapy, non-initiation, or discontinuation of resuscitation remain options following assessment of the baby. Ongoing evaluation and discussion with the parents and the health care team should guide continuation vs. withdrawal of support.
AHA/AAP 2000
Documentation
Written documentation of
• Personal involved
• All procedures including drugs
• Timing
Post resuscitation carePost resuscitation care infants (especially preterm) who required
resuscitation are at increased risk for all of the general post-resuscitation complications, especially:
• Heat loss• Develop RDS due to immature lungs• Intracranial hemorrhage due to a fragile
germinal matrix• Hypoglycemia• Necrotizing enterocolitis• Oxygen injury
Resuscitation of Preterm Infants
No specific guidelines. No clinical trials
WHO: principles are the same for preterm and termILCOR: No specific recommendationsAHA/AAP: ”Prematurity pointers” Avoid rapid boluses of volume expanders or
hyperosmolar solutions. Avoid heat loss. Handle with care in order to prevent ICH
Neonatal Resuscitation Meconium
• Direct endotracheal suctioning may not be necessary in the apparently vigorous infant with meconium-stained fluid.
• Direct endotracheal suctioning, using the endotracheal tube as a suction catheter, should be performed if the neonate is depressed.
AHA-AAP 2000
Newborn Resuscitation
Some conclusions• preparation and teaching in the bottom of successful
resuscitation• ventilation is the primary goal• oxygenation can in most cases be obtained by room air
- more studies are needed• Chest compression and drugs are rarely needed• ethics should carefully be considered• each step should be assessed scientifically - more
research
WHO Guidelines
Resuscitation practises not effective or even harmful
• routine aspiration of babies mouth and nose
• routine aspiration of stomach
• stimulation by slapping or flicking the soles of its feet
• postural drainage or slapping the back
• squeezing the chest to remove secretions
• routine giving sodium bicarbonate to newborns who are not breathing
WHO Guidelines
Care after successful resuscitation• do not separate mother and newborn- skin-to
skin• examine the newborn (body temp, count
breaths, observe indrawing and grunting, malformations, etc)
• record the resuscitation and the problems, if any
• clean the equipment and prepare for the next birth
Neonatal Resuscitation Confirmation of ETI
Expired CO2 detection can be useful in the secondary confirmation of endotracheal intubation in the newly born, particularly when clinical assessment is equivocal.
In newborns, data are limited and the frequent circumstances of inadequate pulmonary expansion, decreased pulmonary blood flow and small tidal volumes make extrapolation from other age groups
especially hazardous.





























