Embed Size (px)
Citation preview

HSEHealth & Safety
Executive
Proceedings at the OccupationalHealth Offshore Conference
Aberdeen 27-29 March 2001
Prepared by AEA Technology Environmentfor the Health and Safety Executive
OFFSHORE TECHNOLOGY REPORT
2001/041

HSEHealth & Safety
Executive
Proceedings at the OccupationalHealth Offshore Conference
Aberdeen 27-29 March 2001
Angela Crosbie & Fiona DaviesAEA Technology Environment
HarwellDidcot
OxfordshireOX11 0QJ
United Kingdom
HSE BOOKS

ii
© Crown copyright 2002Applications for reproduction should be made in writing to:Copyright Unit, Her Majesty’s Stationery Office,St Clements House, 2-16 Colegate, Norwich NR3 1BQ
First published 2002
ISBN 0 7176 2260 6
All rights reserved. No part of this publication may bereproduced, stored in a retrieval system, or transmittedin any form or by any means (electronic, mechanical,photocopying, recording or otherwise) without the priorwritten permission of the copyright owner.
This report is made available by the Health and SafetyExecutive as part of a series of reports of work which hasbeen supported by funds provided by the Executive.Neither the Executive, nor the contractors concernedassume any liability for the reports nor do theynecessarily reflect the views or policy of the Executive.

iii
SUMMARY
The papers and presentations in this volume constitute the proceedings of an HSE sponsored conferenceon Occupational Health Offshore. The conference was held at the Aberdeen Exhibition and ConferenceCentre from 27 to 29 March 2001 and was supported by UKOOA, TUC, IADC, OCA, IMCA, BROAand WSCA. This event followed the successful Occupational Health Offshore conference held in 1996.Twenty-nine papers were presented and over 160 delegates attended. The range of papers reflectsdiverse areas of interest:
• scene setting - policy, strategy and leadership• the management and implementation of occupational health (including use of data, performance
measures, cost effectiveness, health promotion etc)• occupational health in the offshore design process• practical control of health risks (e.g. noise, radiation, chemicals)• the occupational health and human factors interface (e.g. how attention to human factors can
address health issues such as those related to stress and shift work)• well being and fitness for duty
The range of speakers was also wide, including representation from offshore operators and contractors,occupational health practitioners, trades unions, academics, consultants and regulators from Britain andNorway.
The aim of the conference was to raise the profile of all aspects of occupational health offshore. Itprovided an opportunity for everyone - including managers, supervisors, occupational health managersand practitioners and workforce representatives - to share views, challenges, successes, case studies andresearch findings.
The conference was not designed to develop solutions to specific problems or find ways forward oncontentious topics. However, some of the presentations and audience comments do offer suchopportunities. These will be addressed by the HSE and carried forward by various routes (e.g. OIACand Step Change).
The proceedings are a mixture of formal papers and presentations; the decision on which format wasused for the individual papers was the author’s. The papers published here have not been subject topeer review - although some have the support of various committees. They have been subjected tosome editorial work, mainly to ensure consistency of textual presentation. The question and answersessions, which were transcribed from audio tapes, have been edited to convert, so far as is possible, thespoken word into a readable text.
Ron Gardner

iv

v
CONTENTS
SUMMARY……………………………………………………………………………………………….. iii
DAY 1 – TUESDAY 27 MARCH 2001Session Theme – Scene Setting – Policy, Strategy and Leadership
Opening Address …………………………………………………………………………………………3Mr Bill Callaghan, Chair of The Health and Safety Commission
Securing Health Together – An Occupational Health Strategy For Great Britain...............................9Mrs Sandra Caldwell, Director of Health, HSE
Keynote Speech - Delivering on Health ................................................................................................15Mr Malcolm Brinded, Managing Director, Shell U.K. Exploration and Production
Offshore Industry Advisory Committee Perspective .............................................................................31Mr Roger Spiller, MSF Offshore Team Leader
The Medical Manager’s Perspective .....................................................................................................35Dr Jim Keech, BP, Manager Health BP Upstream UK, Chairman UKOOA HAC
The Challenge Of Setting Occupational Health Targets......................................................................41Mr Stephen Williams, Step Change Support Team
Offshore Safety Division National Inspection Projects: Findings And Lessons On OccupationalHealth Management In The Offshore Sector .......................................................................................47Dr Ron Gardner, Offshore Safety Division, HSE
Health Planning Tool For Occupational Health Assurance................................................................61Mr Lindsay Ross, Occupational Hygiene Co-Ordinator, BP Exploration
Feedback And Discussion “Determining And Using Occupational Health Performance Indicators”................................................................................................................................................................65
DAY 2 – WEDNESDAY 28 MARCH 2001 (Morning Session)Session Theme – Occupational Health in the Offshore Design Process
Occupational Health in the Engineering Phase of Offshore Development Projects – LegislativeBasis and Experience from Project Auditing in Norway……………………………………………73Mr Sigvart Zachariassen and Mrs Anne Myhrvold, Norwegian Petroleum Directorate, Stavanger,Norway
Systematic Follow-up of Working Environment Activities During Design of OffshoreInstallations…………………………………………………………………………………….………77Mrs Claudia C. González Hague and Wenche Solberg, Scandpower AS, Norway
Design of Offshore Installations – Don’t Forget Occupational Health…………………………..…..83Mr Kevin O’Donnell, OSD, HSE
Designed-in Occupational Health Risk Management…………………………………………...……89Geoff Simpson, Amey Vectra, Melanie Clark, Amey Vectra and Mr Kevin O’Donnell, HSE
The Development of a Human Factors Engineering Strategy in Petrochemical Engineering andProjects - Part 1……………………………………………………………………………………….105Mr Harrie J T Rensink, Group Advisor Human Factors Engineering, Shell International HealthServices, The Hague, The Netherlands and Martin E J van Uden, Co-ordinating Process Engineer, ShellInternational Chemicals, Amsterdam, The Netherlands.

vi
The Development of a Human Factors Engineering Strategy in Petrochemical Engineering andProjects - Part 2…………………………………………………………………………….…………115Martin E J van Uden, Co-ordinating Process Engineer, Shell International Chemicals, Amsterdam, TheNetherlands and Mr Harrie J T Rensink, Group Advisor Human Factors Engineering, ShellInternational Health Services, The Hague, The Netherlands
Health and Safety by Design - Integrating Human Factors into the Offshore Design Process…....131Dr Ian Randle, Hu-Tech Associates Ltd, 81 Addison Road, Guildford, Surrey, GU1 3QE and Mr EdTerry, Sauf Consulting Ltd, 30 Observatory Road, London, SW14 7QD
DAY 2 – WEDNESDAY 28 MARCH 2001 (Afternoon Session)Session Theme – Physical, Chemical and Biological Agents – Case Studies
Experience from Supervision of Operator Companies' Assessment of Chemical Risk…….………147Mrs Anne Myhrvold, Mr Sigvart Zachariassen and Mr J A Ask, Norwegian Petroleum Directorate,Stavanger, Norway
Measuring Occupational Exposure to Hazardous Chemicals in the Offshore Industry……….…..151Mr Lindsay Ross, BP, Dr Ahsan Saleem, Offshore Safety Division, HSE and Mr Stuart Whiteley, ShellUK Exploration and Production
Legionella and Other Issues within Potable Water Maintenance. A Consultant’s Perspective…..153Dr Mark Brown, Commercial Microbiology Ltd, Aberdeen
Implementation of the Noise at Work Regulations, Offshore………………………………….……157Mr Curt Robinson, Acoustic Technology Ltd
The LSA Focused Results Delivery Project on NORM………………………………………………163Mr Brian McKendrick, Shell Expro
Tackling Bad Vibes in the Oil and Gas Industry – A Case Study on Hand Arm Vibration Syndrome(HAVS)………………………………………………………………………………………………...169Mr Stuart McIlroy, Senior HSE Advisor, Halliburton Brown and Root
Report on Hand Arm Vibration Syndrome…………………………………………………………...173Ian Campbell, BP, HSE Advisor Health
DAY 3 – THURSDAY 29 MARCH 2001 (Morning Session)Session Theme – Human Factors and Psychological Health
Circadian Adaptation to Shift Change in Offshore Shift Workers………………………………….187Michelle Gibbs, S. Hampton, L. Morgan and Professor Josephine Arendt, Centre for Chronobiology,University of Surrey, Guildford, Surrey, GU2 7XH
Managing Stress in the Offshore Working Environment…………………………………………....195Dr Valerie J Sutherland, Chartered Psychologist, Sutherland-Bradley Associates, 5 Minorca Avenue,Deepcut, Camberley, Surrey GU16 6TT
What’s New in Stress Management?………………………………………………………………....205Ronny Lardner, Chartered Occupational Psychologist, The Keil Centre Ltd and Bob Miles, HumanFactors Team Leader, HSE
The Role of Employee Assistance Programmes in Organisational Stress Management……...……209Dr Stephen Galliano, ICAS Group
Feedback and Discussion – Human Factors and Psychological Health – Where Next?……….….215

vii
DAY 3 – THURSDAY 29 MARCH 2001 (Afternoon Session)Session Theme – Wellbeing and Fitness for Duty
Health Care and First Aid on Offshore Installations - The Revised ACOP……………………..….225Alan Morley, Safety Policy Directorate, HSE
Wellbeing at Work……………………………………………………………………………….……227Fiona Farmer, Regional Officer, MSF
The Medical and Physical Fitness of Offshore Emergency Response Rescue Team Members…....229Dr Allan C Prentice, Aon Occupational Health
Ageing of the Offshore Workforce in the Norwegian Offshore Industry: Implications for Safety andHealth…………………………………………………………………………………………….……255Dr Eirik Bjerkeboek, Dr Helge Wiig and Dr Hilde Heber, Norwegian Petroleum Directorate, Pb 600,Ullandhaug, N-4003 Stavanger, Norway
Impact of Health Surveillance and Promotion on Offshore Accident Rates……………………..…263Dr Kathryn Mearns, Industrial Psychology Group, William Guild Building, University of Aberdeen,Aberdeen, AB24 2UB

viii

1
DAY 1
SESSION 1
SESSION THEME – SCENE SETTING – POLICY, STRATEGY ANDLEADERSHIP

2

3
OPENING ADDRESS
Mr Bill Callaghan, Chair of the Health and Safety Commission
I would like to add my welcome to that of PaulDavies and say how pleased I am to be heretoday. I endorse his view that this is an idealopportunity to reflect on what has happened inthe last five years and to refocus your attentionon the important issues today.
I was in Edinburgh two weeks ago hearingfrom a range of Scottish organisations abouthow they are putting into action SecuringHealth Together, the occupational healthstrategy for Great Britain.
I was impressed by the partnership activity inScotland, for example, through organisationssuch as Scotland’s Health at Work. Partnershipis central to our strategy. So far as SecuringHealth Together is concerned, to borrow thephrase from the (Ronseal) advert, ‘it does whatit says on the tin’. Securing Health Together.The watchword is together.
You may be interested that one of the delegatesin Edinburgh, from Strathclyde Fire Brigade,said they had trialed providing injured firemenwith physiotherapy. They found a payback oftwo pounds for every pound spent. We will befollowing up for more details. But it is aninteresting indication of how investment inoccupational health can pay.
This conference gives you the opportunity toconsider how we can Secure Health Togetheron the UK sector of the Continental Shelf.
I’m going to consider:- Revitalising and Securing Health Together- occupational health in Great Britain and
offshore- how the industry has moved on in the last
five years- how legislation relating to health has changed- ill-health issues offshore- baseline data and targets- the way forward and the key challenges
Revitalising and Securing Health Together
The Commission and the Government stronglysupport work to address ill-health in theworkplace. Last year the Deputy PrimeMinister and I launched the Revitalising Heathand Safety initiative.
It injects new impetus into the health and safetyagenda and identifies new approaches toreduce further rates of accidents and ill-healthcaused by work. Especially approachesrelevant to small firms - although there arerelatively few of these offshore.
Revitalising aims to ensure that our approachto health and safety regulation remains relevantfor the changing world of work over the next25 years. It also aims to gain maximum benefitfrom links between occupational health andsafety and other Government programmes.
Securing Health Together is an essential part ofRevitalising. Work that contributes to it willensure that we meet targets to reduce the casesof work-related ill-health and absence. Youwill hear more about Securing Health Togetherfrom Sandra Caldwell later today.
Occupational health in Great Britain
Let me ask you to consider why occupationalhealth is important. Around two million peoplein Great Britain suffer from some form ofwork-related ill-health. These two millionpeople are not on their own. At home their ill-health will affect their families. At work itmeans their skills and experience are likely tobe wasted. Can your company afford this loss?Can we as a nation afford it?
Occupational health Offshore
Occupational health is vitally important for theoffshore industry. Unless you see it as such,progress will be limited.
If this conference is the success that itdeserves, and which I’m sure you all want, itwill raise the profile of ill-health offshore. Ifthis increased awareness prompts everyoneinvolved with occupational health to do

4
something, there will be fewer cases ofoccupational ill-health among the offshoreworkforce. The offshore industry, industryassociations, trade unions and HSE, over thelast five years, have all done an excellent job ofraising awareness and developing action plans.But there is no room for complacency. There ismuch more to be done. Later I will challengeyou to move occupational health offshoreforward. If the number of cases of ill-health isto be reduced, everyone’s recent efforts need tobe maintained or increased.
Ill-health is as likely to occur from workoffshore as it is onshore. The reasons fortackling it are no different. It is in everyone’sinterest to do this for sound moral, legal andeconomic reasons.
Improvements can only be achieved if theoffshore industry and everyone involved in ittakes occupational health seriously. People’shealth at work must be properly managed. Thisdoes not mean it is the sole responsibility ofoffshore managers and the medical profession.Everyone has a role to play, by which I meaneveryone in the industry, industry associations,trade unions as well as HSE. Partnership is atthe heart of Revitalising and Securing HealthTogether. You must look for opportunities toimprove existing partnerships or forge newones and decide what you are going to do tohelp reduce the incidence of ill-health offshore.
The last conference, in 1996, raised the profileof occupational health offshore. It gave allthose with an interest a chance to be heard.
At that time, many delegates felt thatoccupational health was a "Cinderella" subjectoffshore. But this was not surprising in view ofthe industry’s need to focus on controllingmajor hazards. The conference was a goodstarting point for the offshore industry. Itencouraged discussion of occupational healthoffshore. But progress has been slow. It isessential that this conference stimulates actionby those who can influence occupational healthoffshore. There is no quick fix for occupationalhealth - securing improvement takes much timeand effort.
But there have been some significantdevelopments. Today health certainly has ahigher profile offshore. The industry has donemuch good work in raising awareness ofhealth. Some offshore companies have takenup the challenge of Scotland’s Health at Workscheme, which focuses on health promotion.
As a result some platforms belonging to BP,Conoco, Marathon and Shell have progressed,through bronze and silver, to reach the goldaward. This is exactly what Securing HealthTogether is all about.
Also, Step Change has been working on theVantage card system - the Offshore Passport.The information this will carry means it has thepotential to become a very valuable tool. Allthese developments indicate that companiesrecognise that a healthy workforce is good forbusiness.
Step Change provides valuable support. It is anindustry initiative, funded and voluntarilystaffed by the trade unions and the industry toimprove offshore health and safetyperformance. It has taken on responsibility forcatalysing and monitoring progress with theindustry’s contribution to Revitalising, and forkeeping HSC’s Offshore Industry AdvisoryCommittee (OIAC) abreast of developments. Ithas also worked jointly with OIAC to developand run a workshop to set offshore Revitalisingtargets, which are an important part ofdeveloping a way forward for occupationalhealth offshore. I hope Malcolm Brinded willsay more about Step Change.
How the industry has moved on in the lastfive years
The offshore industry has changed in the lastfive years. Much more use is made of new anddeveloping technology. Oil and gas are alsonow being sought in new locations - forexample west of Shetland where the weatherconditions are more extreme and travel timescan be lengthy. Today much greater use ismade of contractors. The number of peopleworking offshore has come down from around27,000 in 1996 to 19,000 today. The demandson these people have for the most partincreased, for example by multi-skilling, teamworking and through more campaign basedmaintenance. The effect of one person’sinability to perform their duties is likely to bemore noticeable today, than five years ago. Asthere are fewer people offshore, absencescreate extra pressure and increased stresslevels, and the length of tours may increase.
How legislation relating to health haschanged
On the legislative side there have been changestoo. New and revised legislation applying bothon and offshore has come into force, such as

5
the revised Control of Substances Hazardous toHealth Regulations and the regulations aimedat controlling the health risks of asbestos andlead. The Noise at Work Regulations nowapply offshore and the Approved Code ofPractice on offshore health care and first aidhas been revised. All these require people tofocus on health.
The results from HSE’s inspections indicatethat there are still areas where improvementsare needed - especially in terms of assessingand controlling risk. This is true of even wellknown hazards such as noise, vibration andhazardous substances. Last year about 25% ofthe improvement notices issued by HSE’soffshore inspectors were related to health orwelfare. Effort needs to be concentrated on allhealth and welfare issues and not just thosecovered by specific legislation.
HSE is playing its part in other ways too. Notjust through Revitalising, Step Change and theother initiatives I have already mentioned. Butalso through routine work on inspections andseminars to launch case study guidance - forexample, “Sound solutions offshore” (noisecontrol case studies) and “Well Handled”(manual handling control case studies).
HSE is working in partnership with theindustry on a number of joint research projectsto examine aspects of health. A number ofthese will be covered later in the conference,for example, on the health effects of exposureto toxic substances in drilling muds, and onadaptation to shift work. HSE and someindividual companies are also developingpartnerships, as part of the philosophy ofSecuring Health Together. For instance, theguidance on health in design will be piloted bytwo companies. You will hear more about thistomorrow.
Let’s now look at one area of occupationalhealth in the offshore industry. I’ve beenoffshore several times, and know something ofthe realities of working offshore. I’ve seen howin many ways offshore working conditionshave no onshore parallels. Consider cateringstaff, a perhaps less obvious group of people,who perform a key role offshore. Many of therisks they face will be found onshore, forexample, slips, trips, cuts and burns.
But offshore catering staff also face additionalstressors like vulnerability to complaints oftheir colleagues, absence from their familiesfor weeks at a time, low manning levels, and,
as a result, fatigue and stress. Difficulties withmanual handling arise for catering staffbecause of the lack of space. This is asignificant list of problems for a group ofpeople who do one of the jobs that istraditionally seen as less demanding!
Ill-health issues offshore
Currently our main source of information onill-health and injury is the reports legallyrequired under the RIDDOR. Each year HSEpublishes a summary of these as offshorestatistics on reported injuries, ill-health andincidents. The latest report indicates that lastyear the main reported cause of ill-health waschicken pox. Whilst the cause is beyond ourcontrol, it highlights the problem oftransmission of diseases in the unique offshoreenvironment.
HSE was surprised at the low level of thenumber of cases of work related dermatitisbeing reported. Dermatitis is a disease thatoccurs at a significant level in other relatedindustries and other countries’ offshoreindustries. From the reports that are beingmade, or rather not being made, it seems verylikely that some work-related illness is notbeing reported. Some of this may be partlyrelated to legal requirements. For example, fora disease to be reported the regulations say thatit must have been diagnosed by a doctor. Asyou know there are no doctors offshore, and inmany cases people will have recovered beforethey go onshore.
Companies tell us they see stress andmusculoskeletal diseases as important. Workrelated stress is not reportable, but we areaware of individuals with stress beingmedivaced from offshore. We know thatmusculoskeletal disorders and stress cause thegreatest number of cases of work-related ill-health across all industries.
We know too that noise and vibration areimportant offshore hazards. They can lead tohearing loss and hand-arm vibration syndrome.
Reports of injuries indicate that manualhandling is a major source of accidents andconsequently ill-health.
Manual handling represented 28% of allinjuries reported last year and in many caseswill lead to long term absence from continuingback pain. HSE is dedicating a seminar to thevery important topic of offshore manual

6
handling later this year, where it can beexplored further.
Baseline data and targets
Targets are powerful tools. If they are palpablethey can bring people into partnership,allowing them to consider radical changes,helping to avoid the temptation to blame othersand enabling people to share and be involvedin meeting those targets. Once set, targets arean incentive and allow people to measure theirprogress. Later this afternoon you will hearabout the “Challenge of setting OccupationalHealth Targets”.
The Revitalising workshop identified the lackof baseline data on work-related ill-health as amajor hindrance to setting offshore targets. Itconcluded that a cross-industry database wouldenable the industry to establish a baselineagainst which it could measure its progress.
Such a database would capture all the data atpresent recorded by offshore medics in theirlogbooks or other ways, and data arising fromsickness absence. The workshop agreed itwould be a good idea to develop a scheme forclassifying, coding and collating reports. It alsoagreed that the proposed database should bemanaged by an independent academic body, toensure both confidentiality and quality.
This work will be taken forward by a workinggroup under the auspices of Step Change. Apilot study will be carried out and evaluated inthe next year. Then the database will belaunched in spring 2002.
Industry is of course also free, if it wishes, todevelop other more stretching targets thanthose under Revitalising. What is vital is not tolose the momentum.
The way forward
So how can we deal with the significant issuesoffshore? I believe it comes down tomanagement of the issues. There are three maingroups of people who can provide leadershipto achieve this: employers, trade unions and theregulator - HSC and HSE. Providing effectivemanagement and leadership not only requiresthe three groups to work independently, butalso to do so in co-operation with one another,for example through OIAC and Step Change.
I believe it is right that the offshore industryand trade unions should be driving forward
ideas and approaches aimed at improvingoffshore health and safety. Our experience isthat all involved in Step Change are committedto making real improvements.
To achieve these improvements requires thecommitment of the most senior people in theindustry. I therefore welcome the attendancetoday of Malcolm Brinded and Roger Spiller. Ifind when people at the top are involved andprepared to commit resources in order tochange attitudes and culture, then things beginto happen.
I’m sure everyone here is committed toreducing ill-health amongst the offshoreworkforce. We all need to spread this message,not just to our immediate colleagues, butthroughout the industry. I hope what you hearin the next three days will help you do this.
Key challenges
To summarise:In the next three days I would ask you toconsider occupational health in the context ofworking offshore on the UK sector of theContinental Shelf, in order to identify ways toreduce occupational ill-health there.
I challenge you to move the topic ofoccupational health offshore forward.
To measure your success in dealing withoccupational health offshore, you will firstneed to establish a baseline and I support yourplans to do this. Once you have determined thebaseline, I challenge you to improve on it.
Improvements can only be achieved ifeveryone involved in the offshore industrytakes occupational health seriously. People’shealth at work must be properly managed. Ichallenge you to decide what are you going todo to help manage ill-health offshore and thendo it.
Finally, I challenge everyone involved inoccupational health offshore, to make sure thatthe next five years are marked by a significantreduction in the number of people who becomeill as a result of working offshore.
Thank you for your attention.

7
QUESTIONS AND ANSWERS SESSION
Question - Chris Hopson, UpstreamNewspaperBill, you've talked about these five-year targetsjust now. Could you elaborate a bit more onthe kind of measures that the Commission andGovernment are looking at, to enforce thosetargets in the longer term.
Answer – Mr Bill Callaghan, HSCWell the Commission has recently discussed itsstrategic plan and we discussed this at an openmeeting with our stakeholders – Paul (Davies),you were part of the panel on that day. Interms of the commitment of HSE resources, weare clear that we need to prioritise ouractivities in three key sectors and on five majorhazards. I can perhaps go through what thoseare at a later stage. I think the important pointto stress to this conference is that achieving ouroutcome targets is not just a matter for HSEand its enforcement effort. This is why I'mdelighted to accept invitations to speak toaudiences such as this.
Achieving the targets is going to be broughtabout by our stakeholders, industry, employersand trade unions representative of employees,improving their health and safety. I stronglybelieve that's the main way we are going tomeet those targets. It is not for us from theCommission to come and say your target forthe next five years is 'n' percent. What we wantto happen is our stakeholders to be workingtogether to develop and own their own targetsfor their particular sector. Then drive throughthose management and culture changes whichare needed to achieve the targets. So yes, we'regoing to prioritise our efforts, but we see a keyrole for our stakeholders.
Comment – Dr Paul Davies, HSEIf I could just add, I think also the governmentis committed to making a major contributionitself. The government is a big employer bothdirectly and through contracts. It will seek toensure that it is an exemplary employer byexceeding the target that is set for the countryas a whole and ensuring that its contractors doas well.
Question - Mark Gibb, Blowout MagazineFive years between conferences doesn't seemto impart a sense of urgency to findingsolutions?
Answer – Mr Bill Callaghan, HSCSome people say there are too manyconferences. I think the important point is notthe frequency of conferences, but the point Iwas trying to emphasise in my talk about whataction happens in between. I think we do needconferences every now and again to raise theprofile and raise the awareness. But I hope youwill have taken from my talk that it's not justenough to have conferences. The importantthing is what action flows from conferences.Today and the next couple of days need toestablish a sense of common purpose. WhatI'm looking for is not more conferencesnecessarily, I'm looking for more action.
Question - Mark Gibb, Blowout MagazineSo what can be done about keeping informedabout what is actually happening?
Answer – Mr Bill Callaghan, HSCLater this afternoon you'll hear from Roger(Spiller) and some others about the StepChange initiative and the monitoring andarrangements that are going to be put in placeto provide feedback and to keep informationcoming, so we can track performance againstour aspirations.
Question - Mr Graham Cowling, AcousticTechnology LtdOn your last slide you specifically referred to amanaged approach to reducing health risksoffshore. Is your request to see that approach,based on any concern about the way things arebeing handled at the moment?
Answer – Mr Bill Callaghan, HSCThe key point here is that occupational healthis not just a medical issue. The danger is thatpeople see occupational health as a question ofdoctors and nurses and of course yes, that'simportant. The key point I want to emphasiseis that if occupational health is going to beimproved it needs a concerted managementeffort. That means finding out where you areat the moment. That's the importance of baseline data, setting what I hope are stretchingtargets to then improve from. It's having aproper approach to do this, so that's theimportance of managing this process. Afundamental part of health and safetymanagement is continuous improvement. So Ido hope that we can engender that spiritthrough this conference and encourage allthose offshore to see occupational health andsafety as a key performance indicator formanagers offshore.

8

9
SECURING HEALTH TOGETHER – AN OCCUPATIONALHEALTH STRATEGY FOR GREAT BRITAIN
Mrs Sandra Caldwell, Director of Health, HSE
I am going to give a brief overview of theSecuring Health Together Strategy – as, thoughI know many of you will already be familiarwith it, there are some of you who may not be.I will outline some of the key aspects of HSE’scontribution. Work has already begun toimplement the Strategy and so I can share withyou some of the early actions and finally Iwould like you to be considering how thisapplies to your work as I will conclude byasking you what you can contribute.
Costs of occupational ill health
We know that despite good progress inreducing the numbers of accidents at work, westill need to strive to achieve a similar successin tackling the high level of work-related illhealth we face today.From the self reported work related illnesssurvey of 1995 we estimate that over twomillion people in Great Britain suffer from anillness they believe is caused by or made worseby the work they do. A study carried out bythe water industry found that on average a caseof work-related ill health cost a company atleast two and a half times that caused by anindustrial injury. Behind these figures is agreat deal of personal suffering and familyhardship, and cost to the individualsthemselves, their employers and society atlarge.
Musculoskeletal disorders were by far the mostcommon self-reported illness, affecting anestimated 1.2 million individuals. The secondmost commonly reported condition affectingjust over ½ a million was stress, depression andanxiety and those who reported that stressarising from work made existing conditionsworse, such as hypertension, heart disease orstroke.We have not yet solved the problems ofoccupational diseases that arise from exposureto hazardous substances. We can estimate withsome certainty that we have upwards of athousand new cases a year of work-relatedasthma and some 3000 cases of occupationalcontact dermatitis are seen by dermatologistsor occupational physicians each year. This islikely for both these diseases to be anunderestimate.
Unfortunately we can be certain that the trendin the rate of deaths from mesotheliomacontinues to rise steeply (as it has since 1968).In 1998, 1527 people died from mesothelioma– a legacy from their exposure to asbestos inthe period from the 1930s to the early 1980s.Though we are hopeful that the falling numberof under-50s affected may reflect better controlof more recent exposure to asbestos this is anarea in which we will continue to be vigilant.
Nationally, if we are going to make adifference to the overall levels of work-relatedill health we must tackle the causes of the bigtwo – Musculoskeletal disorders and ill healtharising from stress at work. I will tell youmore about HSE’s plans – but you will alsowant to consider if the national picture isreflected in the offshore industry and whetheryou are currently looking at the right priorities.
You may be interested to know about a majorchemical company that improved their ownsystem of using the data they collected onsickness absence to identify the causes of illhealth in their workforce. Though they foundthat the work they had done to controlexposure to sensitisers very effectively kept thenumbers of asthma and dermatitis cases low -they actually had large numbers of people withmusculoskeletal disorders. This informationprompted a change of approach and theyintroduced an early intervention programmethat helped prevent ill health and got peopleback to work faster. The better targeting oftheir resources meant they found they gotreturn for the money they spent.
This type of approach is welcomed and wehope will be taken up by more organisations inorder to contribute to Securing HealthTogether.
I have heard a little about OIAC’s plans tointroduce a new system of recording the healthissues that cause workers to visit medics whilstoffshore – this should lead to better data –making it easier to make decisions about whatyour priorities must be. I look forward to
10
hearing more about how the OIAC projectdevelops.
Securing Health Together
Securing Health Together was developedthrough an open public discussion process towhich I know some of you contributed. Weheard and understood that what we needed todo to make a difference to this heavy toll of illhealth was to think innovatively, be flexibleand respond to both the complexity ofoccupational health problems and changes thatarise from modern work patterns and workingconditions.
In light of this, Securing Health Together takesa broad understanding of occupational healthembracing both the effects of work on healthand health on work. Its overall aims are:• A reduction in work-related ill health to
workers and to the public• A reduction in sickness absence• A culture where people are:
o rehabilitated back to work followingillness, or
o provided with opportunities to workdespite health conditions or disability.
The offshore sector has of course always had arather broader view of occupational health thanmany sectors onshore. As the offshoreinstallation is the workers’ home as well astheir workplace the employer has to partlyreplace the usual health support functions ofthe NHS on a day-to-day basis. Also thecaptive audience has already led to a traditionof good health promotion initiatives. Thatsaid, the setting of targets should stimulate youto review your approach to ensure you do havethe right priorities.
Targets
We are clear about what needs to be achieved.Challenging national targets have been set andare supported by nine Government Ministers.By 2010 we want to• cut by 20% work-related ill health for
workers;• and the public;• cut the number of working days lost due to
work-related ill health by 30%; and• create a culture of rehabilitation, by
ensuring that opportunities forrehabilitation or access to work areextended to everyone who has been ill orwho has a disability – where it is necessaryand appropriate.
Of course these targets will only be achieved atthe national level if action is taken at theworkplace level.
I would like to clarify that the second targetconcerning ill health to the public caused bywork relates mainly to illness arising fromhospital-acquired infection and therefore isunlikely to be a priority for the offshoreindustry.
I hope that you will sign up to meeting theother targets.
Targets are important because:• they act as motivators for action,• they make us focus on what we know about
the current situation and whether we canaffect the causes of the big problems; and
• we must evaluate what we do againstoutcomes: we ask “does what I am doingreally stop people being made ill, or helpthem to return to or take up work?”
Partnership
Securing Health Together is based on apartnership approach and will only succeed ifthe existing successful partnerships flourishand we take up the opportunities that newpartnerships have to offer.At the national level there have been someevents at which we have seen Partnershipbeginning to take the Strategy forward. I won’tdwell on these, but in brief:
The Partnership Board, of which I am amember, has the role of producing strategicideas; championing the cause; providingoversight on the progress that is being madeand having a challenge function. We meetagain next week and I look forward to havingsome feed back from today that I can add to theother conferences I have attended recently –we are keen to hear feedback on SecuringHealth Together and what you can do or arealready doing to play your part.
In December we held a workshop at which awide range of stakeholders met who have aninterest in how we can measure progressagainst Securing Health Together’s targets.We’ve not solved all the difficulties yet, but welearnt a lot and will soon be publishing atechnical note that will set out what HSE in co-operation with other organisations andgovernment departments will be doing. But

11
after all the best source of data is often theindustry itself.
Conferences to discuss Securing HealthTogether in action have been held• in Cardiff in October, hosted by HSE in
partnership with the National Assembly forWales;
• and at Murrayfield just a fortnight ago,hosted by HSE with the Scottish Executive.
Both events were well attended. At the latter Iwas pleased to hear from a selection of Scottishorganisations about the actions they havealready been taking to really reduce the numberof people made ill by work or help them getback to work when they have been ill. I’ll saya little more about this later.
The five programmes of work
To explain how each of these bits of the puzzlefit together to contribute to Securing HealthTogether’s overall targets. We have set outfive programmes of work. Over the next fewweeks the Programme Action Groups will eachmeet for the first time. The membership ofeach is made up from leading players in therespective fields and they will oversee andfacilitate the delivery of the Strategy's fiveprogrammes of work by identifying andoutlining what actions must be taken. The fiveprogrammes of work each deal with aspects ofwhat we need to do.
First we must improve the law on occupationalhealth and the level of compliance with it. Weare considering here not just the Health andSafety at Work Act and related Regulations,but also provisions under the DisabilityDiscrimination Act.
Second we want to move to a culture ofcontinuous improvement where peoplecollaborate, form partnerships and share bestpractice – often taking action above the legalminimum.
Third we must share our knowledge and collectthe data and other information that will help usreach the targets and evaluate how we aredoing. The examples I’ve referred to on cost-benefit analysis would contribute here.
Fourth we need to achieve a better spread ofcompetence and skills – we want to have theright person for the right task.
Finally we want to improve the delivery andtargeting of advice and support. No single
method will suit everyone, it will requireflexibility and a multidisciplinary approach.Meeting the needs of small firms will becentral.
HSE’s contribution
I think it’s helpful to understand how the fiveprogrammes are going to be followed throughto give you some examples of what HSE isplanning to contribute to reducing theincidence of ill health arising from work-related stress.• For Compliance we are working to develop
standards of good management practice fora range of stressors.
• For Continuous Improvement we will pilotlocal benchmarking groups to share goodpractice and knowledge about work-relatedstress in small and medium enterprises andbetween trade union safety representatives.
• For Knowledge we are starting aprogramme of research to pin down someof the remaining questions about stress andits relationship to ill health.
• For Skills we are developing trainingmaterials for managers and safetyrepresentatives on how to carry out a stressrisk assessment.
• For Support we will publish guidance toassist employers to manage stress that willkeep up to date with the developments thatarise from our other work. This approachis important because it helps to demystifyhealth issues. We will concentrate onpractical solutions where we have them asthis helps managers and others to see howthey can contribute.
We have already begun to plan our other keywork along these lines, for example ourstrategies for tackling musculoskeletaldisorders and asthma.
Examples of others’ contributions
But I have focussed on what HSE has beendoing. As I have already stressed the targetsare only going to be achieved if others work inpartnership to deliver them.
I said I’d heard some interesting examples ofeffective work to improve occupational healthat the recent Scottish conference and I’d like to

12
tell you a little about those and some others ofwhich I’m aware.
The Scotland Back in Work campaign, run bythe Health Education Boards on the basis ofresearch by the Faculty of OccupationalMedicine, was able to show that their simplemessage – that the best action to take if youhave back pain is to get mobile and takenormal pain killers – delivered through theright campaign – using local radio – had raisedawareness and that resulted in changedbehaviours.
Lothian Occupational Health Forum, a jointtrade union and local health authority initiative,explained how their advisors had approachedthe issue by contacting the worker at their GPs’and helping them explore the causes of their illhealth and the ways of overcoming it. This didhelp individuals to return to work and in somecases the advisors were invited into theworkplace to help advise on changes that couldbe made there to prevent further ill health.
I was particularly interested that speakers fromthe floor took up the need to look at cost-benefit analyses for occupational healthinterventions. We heard the concerns aboutthe costs of interventions. What we need tohear about are the costs of ill health – and thesavings to be made if we prevent that. Oneconsultant occupational physician referred tosome work he’d done to establish aphysiotherapy service that was so successfulhe’d lost the contract to in-house providers!
It may not be possible to do cost-benefitanalysis alone – a group of major UKcompanies are in the process of establishing acommon set of data on their staff’s ill healthand absence. They are intending to use this asthe basis of research into the effectiveness ofoccupational health and health promotioninterventions. So far they are in thedevelopment stage, but we will be keeping intouch with them and they have agreed to sharetheir results with us all.
On a bigger scale again the companies in thewater industry have signed up to Clearwater2010 – a campaign to reduce the ill healthcaused by work in workers in the waterindustry and allied construction workers. Theyhave set targets and are concentrating ontackling priority ill health issues by settingspecific goals across the industry.
What the offshore industry can do
So there are many contributions at many levels.I would like you to consider how you, yourorganisation or the offshore industry as a wholecan contribute. I know that over the next fewdays you are going to hear more about workthat has already begun.
I recognise the achievements that many of youhave made by taking part in Scotland’s Healthat Work awards scheme and progressedthrough from bronze to gold. I am sure thatyou already value the benefits to the generalhealth and fitness of your workforce. I thinkthe message we can take from this is thatefforts to manage risks can make a realdifference – even in areas where the managerdoes not have direct control of the cause of therisk. If the same approach is applied to risksarising from the work processes the returnscould potentially be even greater.
For example, you can look for ways ofimproving your compliance with existinghealth and safety law:• A major current programme of work for my
colleagues in the Offshore Inspectorateincludes investigation of manual handlingaccidents and their prevention. You cantake up this and the existing case studiesguidance and apply it to your ownworkplace – don’t wait to be inspected!
You may need to consider if you have set upthe arrangements you need to comply with theDisability Discrimination Act.
You may be able to participate in initiativesthat contribute to continuous improvement inthe standards of occupational health practice• I know the industry and HSE’s Offshore
Shore Directorate has already run someseminars for companies that manufactureequipment that is associated with hand-armvibration on the best ways to assess andcontrol exposure.
• I also know that Offshore Directorate hasprojects with various offshore companiesand industry associations developingstandards and guidance on a range oftopics, including stress management,manual handling aspects of scaffoldingwork, assessment and control of exposureto mud chemicals and design. Indeed youwill hear more about some of these later inthe conference.
I am sure you can think of more examples.

13
As I mentioned earlier I am very pleased tohear about OIAC’s cross-industry initiative toimprove our knowledge about the sorts of illhealth that occur offshore, by recording thereasons for visits to medics. Data collection isnot straightforward. We need it to measuretrends so we can show what we do is working –or learn if it is not. We also use it to chooseour priorities and you’re probably already in aposition to do this – if you reflect the nationalsituation those will be stress related ill healthand musculoskeletal disorders.
On the last two programmes of work I amgoing to suggest areas that I would like you toconsider:
There are a wide range of skills that arerequired if we are going to have the rightpeople to do the work that is needed to reducethe toll of work-related ill health and getpeople back to work who have been ill.However, at the centre of any action is themanager at the workplace and all our effortshinge on his or her understanding of the causesof ill health absence (whether that is work orhome related) and whether the right techniquesare being used to encourage people to return towork when they have been sick withoutincreasing risks to themselves or others. Doyou have access to the sorts of management ofattendance courses that you or your managersneed? Do you support managers to attendsuch courses? Can you provide this sort oftraining?
I would like you to consider whether or not youhave the support that you need to improve youroccupational health record. By support I meanaccess to information, advice, skills orresources. I would like you to consider how
you can overcome any difficulties. Oftenoccupational health problems need solutionsfrom multi-disciplinary teams. Do youunderstand the services that your partnersprovide and how to access them? Are you onepart of the solution and can you improve howyou work with others?
I suspect the answer will often come in theform of partnership. In particular, partnershipis likely to be the answer to how we get themessage across to all parts of the offshoreindustry – the smaller enterprises as well as thebig players. This is one of our biggestchallenges to which I know we do not yet havethe right solutions.
Concluding remarks
I have run briefly through the key aspects ofthe Strategy at a national level, some of thefirst actions taken in partnership and what HSEis planning to contribute.
The five programmes of work are the key tothe way that we will begin to make progress.
When I began I asked you to consider how thisapplies to your work and what you couldcontribute … I would be delighted to hearfrom you as individuals if you can catch me inthe margins here. Or our Securing HealthTogether Team at HSE, London are collectingexamples of work that people are contributing– you can find out more and submit an exampleby visiting our website at www.ohstrategy.net.
QUESTIONS AND ANSWERS SESSION
Delegates were asked to save their questionsfor later.

14

15
KEYNOTE SPEECH
Mr Malcolm Brinded, Managing Director, Shell U.K. Explorationand Production

• T
hank
you
Pau
l (D
avie
s)•
I am
ver
y pl
ease
d to
be
spea
king
at a
cru
cial
con
fere
nce
on a
topi
c w
hich
is s
o ve
rype
rson
ally
impo
rtan
t to
us a
ll•
In th
e co
min
g th
irty
min
utes
, I h
ope
to p
rese
nt h
ow S
hell
Exp
ro•
is ta
cklin
g th
e ch
alle
nges
of
occu
patio
nal h
ealth
ons
hore
and
off
shor
e,•
how
man
agin
g he
alth
pla
ys a
key
rol
e in
our
com
pani
es v
alue
s,•
and
espe
cial
ly
the
key
role
of
le
ader
ship
in
he
lpin
g pr
ogre
ss
the
agen
da
onoc
cupa
tiona
l hea
lth.
• T
his
last
iss
ue i
s of
cru
cial
im
port
ance
sin
ce i
t is
so
easy
for
com
pany
man
ager
s to
assu
me
that
bec
ause
the
y ar
e no
t th
emse
lves
exp
erts
in
the
fiel
d of
hea
lth,
that
ther
efor
e H
ealth
Man
agem
ent
is n
ot s
omet
hing
the
y ne
ed t
o be
inv
olve
d in
. Thi
s is
quite
sim
ply
wro
ng.
• I
wou
ld l
ike
to s
tart
by
rem
indi
ng o
urse
lves
why
it
is t
hat
we
belie
ve o
ccup
atio
nal
heal
th i
s so
im
port
ant
- in
deed
why
the
con
fere
nce
here
the
se t
hree
day
s is
so
impo
rtan
t to
us a
s an
indu
stry
• co
mpl
ian
ce w
ith le
gisl
atio
n is
the
begi
nnin
g an
d a
key
driv
er f
or u
s -
but w
e w
ill n
otlim
it ou
r am
bitio
n to
com
plia
nce.
Lat
er I
will
dis
cuss
the
nee
ds f
or a
mor
e ri
goro
ussy
stem
to e
nsur
e im
prov
emen
t in
our
heal
th m
anag
emen
t•
we
mus
t co
ntro
l ou
r lo
sses
thr
ough
dir
ect
and
indi
rect
abs
ence
cos
t an
d lo
stbu
sine
ss o
ppor
tuni
ties
- se
vera
l mill
ions
of
poun
ds p
er a
nnum
• W
e ar
e co
mm
itted
to
prot
ecti
ng a
ll th
e pe
ople
inv
olve
d w
ith o
ur o
pera
tions
- a
mor
al im
pera
tive
of le
ader
ship
at t
he c
ore
of S
hell’
s B
usin
ess
Prin
cipl
es•
Hea
lth m
anag
emen
t is
not
jus
t ab
out
bein
g re
activ
e -
it is
a k
ey f
acto
r in
unl
ocki
ngpo
tent
ial -
hel
ping
our
peo
ple
in g
ivin
g th
eir
best
• So
whe
re d
oes
heal
th m
anag
emen
t fit
in o
ur a
gend
a?...
Del
iver
ing
on
Hea
lth
Mal
colm
Bri
nded
Man
agin
g D
irec
tor
She
ll U
.K.
Exp
lora
tio
n a
ndP
rod
uct
ion
Occ
up
atio
nal
Hea
lth
Off
sho
re
27
Mar
ch 2
00
1
Wh
y m
an
age
hea
lth
?
Tac
kli
ng
th
e ne
ed…
sei
zin
g t
he
oppo
rtu
nit
y
•co
mp
lian
ce
•lo
ss c
on
tro
l
•p
rote
ctin
g p
eopl
e
•u
nlo
ckin
g p
ote
ntia
l
16

• Sh
own
here
are
wha
t the
peo
ple
who
mak
e up
She
ll E
xpro
det
erm
ined
to b
e ou
rke
y va
lues
.•
Tho
usan
ds w
ere
invo
lved
- e
valu
atin
g be
havi
ours
of
staf
f ag
ains
t the
se v
alue
s is
part
of
thei
r an
nual
app
rais
al•
One
of
the
abso
lute
val
ues
we
hold
is o
ur r
espe
ct f
or p
eopl
e•
Thi
s m
eans
that
in a
ll ou
r op
erat
ions
, we
mus
t ens
ure
the
safe
ty, a
nd th
e he
alth
,of
all
our
staf
f, a
nd a
ll th
ose
who
are
aff
ecte
d by
our
bus
ines
s, i
nclu
ding
our
cont
ract
ors
and
our
com
mun
ities
clo
se to
our
pla
nts
and
faci
litie
s
• T
he k
ey v
alue
s an
d be
havi
ours
I h
ave
show
n ar
e an
inte
gral
par
t of
that
we
call
our
Em
ploy
ee V
alue
pro
posi
tion
- w
hat
is t
he d
eal
betw
een
our
com
pany
and
the
peop
le w
ho w
ork
for
us:
• A
ttitu
des
and
beha
viou
rs h
as p
artic
ular
rel
evan
ce f
or p
erso
nal
heal
th a
nd l
evel
sof
psy
chol
ogic
al il
lnes
s in
the
wor
kpla
ce.
• W
e ca
nnot
be
seri
ous
abou
t th
is s
trat
egy
unle
ss w
e pr
otec
t an
d en
hanc
e ou
rpe
ople
’s h
ealth
.•
Wha
t is
the
purp
ose
of o
ur f
ocus
on
our
Em
ploy
ees
- it
is th
e ab
ililit
y to
unl
ock
pote
ntia
l an
d ac
hiev
e an
im
prov
ed
Staf
f co
mm
itmen
t, m
otiv
atio
n an
dpe
rfor
man
ce•
Thi
s ha
s be
en i
nstr
umen
tal
in S
hell
Exp
ro’s
suc
cess
ful
tran
sfor
mat
ion
over
the
last
dec
ade,
and
will
be
vita
l in
mee
ting
the
chal
leng
es a
head
of
us•
Oth
er e
lem
ents
of
the
Jigs
aw a
re a
lso
rele
vant
to h
ealth
:•
A s
timul
atin
g w
ork
envi
ronm
ent,
with
a h
ealth
y w
ork-
life
bala
nce,
tho
ught
ful
ergo
nom
ics,
enc
oura
gem
ent f
or h
ealth
and
per
sona
l fitn
ess
• im
prov
ing
heal
th i
s a
natu
ral
fit
to t
his
who
le a
gend
a an
d w
e se
e it
as a
prer
equi
site
for
the
suc
cess
of
our
othe
r ke
y st
rate
gies
, suc
h as
Ste
p C
hang
e in
Safe
ty
• In
sho
rt, n
ot o
nly
will
we
com
ply
with
the
law
but
will
see
k al
l op
port
uniti
es t
oad
d va
lue
to o
ur b
usin
ess
thro
ugh
our
peop
le.
•O
uts
tand
ing
Bu
sin
ess
Per
form
ance
•R
espe
ct f
or
Peo
ple
•F
air
Lea
ders
hip
•H
on
esty
and
Ope
nnes
s
•In
tegr
ity
•P
rid
e
•C
lari
ty o
f P
urp
ose
•S
usta
inab
le D
eve
lop
me
nt
•T
eam
wo
rk a
nd P
rofe
ssio
nal
ism
•T
rust
EX
PR
O V
AL
UE
SD
RIV
E L
OC
AL
BE
HA
VIO
UR
S
T
eam
Ex
pro
Va
lues
Em
plo
yee
Va
lue
Pro
po
siti
on
(E
VP
)
“Tea
m E
xpro
” V
alu
es&
Beh
avio
urs
Imp
rove
dP
erso
nal
Dev
elo
pm
ent
Re
cog
nit
ion
&R
ewa
rd
Mo
reS
tim
ula
tin
g W
ork
En
viro
nm
en
t
Imp
rove
d S
taff
C
om
mit
me
nt,
Mo
tiv
atio
n&
Per
form
ance
Imp
rove
d B
usi
nes
s P
erfo
rma
nce
17

• H
,S, a
nd E
is o
ften
man
aged
as
a co
mbi
ned
unit
• Sa
fety
has
typi
cally
bee
n be
en r
ecei
ving
top
billi
ng•
The
Hea
lth e
lem
ent,
on th
e ot
her
hand
, is
ofte
n he
ld in
the
back
grou
nd a
s a
supp
ortin
g ca
st•
Man
agin
g O
ccup
atio
nal H
ealth
has
som
e pa
rtic
ular
cha
lleng
es, h
owev
er•
It i
s th
e m
ost
pers
onal
of
the
thre
e -
this
can
be
seen
on
the
one
hand
in
are
luct
ance
to s
peak
up,
but
als
o in
a r
esis
tanc
e to
inte
rven
tion
• T
he i
mpa
ct o
f po
or m
anag
emen
t is
not
im
med
iate
ly s
een,
but
can
be
wid
era
ngin
g an
d da
mag
ing
to t
he i
ndiv
idua
l an
d th
e bu
sine
ss p
erfo
rman
ce.
Ear
lier
this
yea
r ou
r Sh
ell T
anke
rs a
nd T
radi
ng lo
st a
cou
rt c
ase
conc
erni
ngm
esot
helio
ma
- m
ore
than
45
year
s af
ter
the
peri
od o
f em
ploy
men
t. T
hecr
ux o
f th
e ca
se c
once
rned
whe
ther
the
com
pany
sho
uld
have
kno
wn
the
link
betw
een
expo
sure
to
asbe
stos
and
mes
othe
liom
a in
the
mid
50’
s. T
his
is n
ot a
com
plai
nt,
but
a co
mm
ent
on t
he n
eed
to r
ecog
nise
the
ton
g te
rmim
plic
atio
ns o
f ge
tting
hea
lth m
anag
emen
t wro
ng•
We
see
Man
agin
g O
ccup
atio
nal
Hea
lth
as
an
abso
lute
ne
cess
ity,
and
incr
easi
ngly
pro
min
ent o
n ou
r ag
enda
.•
So w
hat
do w
e in
She
ll E
xpro
bel
ieve
fal
ls u
nder
the
man
agem
ent
ofO
ccup
atio
nal H
ealth
...
• Fi
rst
of a
ll ou
r vi
sion
: "p
eopl
e gi
ving
the
ir b
est"
thr
ough
im
prov
ed h
ealt
h an
dpe
rfor
man
ce.
• A
n am
bitio
us ta
rget
not
res
tric
ted
to lo
ss c
ontr
ol.
• ad
opt
an
incl
usiv
e,
acce
ssib
le
and
far
reac
hing
ag
enda
, w
e m
ust
incl
ude
cont
ract
ors
and
busi
ness
par
tner
s in
our
ide
as,
incl
udin
g th
em i
n ou
r ke
y ac
tivity
prog
ram
mes
- w
e ar
e ex
tend
ing
the
role
of
our
off
shor
e m
edic
s to
inc
lude
hea
lthpr
omot
ion
and
safe
ty a
t w
ork.
O
ur p
hilo
soph
y is
to
take
the
mes
sage
to
the
wor
kpla
ce.
• W
ork
on h
ealth
in th
ree
key
area
s•
prev
enti
ng w
ork
rela
ted
illn
ess
• li
mit
ing
impa
ct o
f il
lnes
s th
ough
ear
ly in
terv
enti
on•
prom
otin
g he
alth
and
hea
lthy
beh
avio
urs
• F
irst
I s
hall
desc
ribe
She
ll E
xpro
’s a
ppro
ach
to th
ese
thre
e ar
eas
• I
shal
l th
en g
o in
to t
he r
ole
of l
eade
rshi
p, a
nd s
ome
of t
he f
ive
key
area
shi
ghlig
hted
in
the
HSE
’s s
trat
egy
as o
utlin
ed i
n th
e Se
curi
ng H
ealth
Tog
ethe
rdo
cum
ent
Occ
up
ati
on
al H
ea
lth
•In
tegr
ated
Hea
lth
and
Saf
ety
man
agem
ent
•S
afet
y g
ets
“to
p b
illi
ng
”
•H
ealt
h i
s in
“su
pp
ort
ing
cas
t”
•K
ey C
hall
enge
s
–he
alth
is
ver
y p
erso
nal
–im
pac
t o
f p
oo
r m
anag
emen
t is
no
t im
med
iate
ly v
isib
le
•R
enew
ed f
ocu
s on
hea
lth
A s
trat
egic
ap
pro
ach
to
hea
lth
Peo
ple
givi
ng t
heir
bes
t th
roug
h im
prov
edhe
alth
and
per
form
ance
Pre
vent
ing
wor
kre
late
d il
l he
alth
Red
ucin
g th
eim
pact
of
illn
ess
or i
njur
y
Pro
mot
ing
heal
than
d he
alth
ybe
havi
ours
Lea
der
ship
Co
mp
lian
ceC
on
tin
uo
us
imp
rov
emen
tK
no
wle
dg
eS
kill
sS
up
po
rt
18

prev
enti
ng w
ork
rela
ted
illn
ess
• W
e ar
e co
ntin
uous
ly
prog
ress
ing
the
boun
dari
es
and
beco
min
g m
ore
soph
isiti
cate
d in
our
und
erst
andi
ng a
nd a
ppro
ach
to w
ork
rela
ted
illne
ss•
nois
e, v
ibra
tion,
CO
SHH
hav
e be
en m
anag
ed f
or a
long
er p
erio
d•
espe
cial
ly w
e re
cogn
ise
we
mus
t stil
l tac
kle
mus
culo
-ske
leta
l illn
ess
• A
Man
ual h
andl
ing
initi
ativ
e in
bei
ng p
rogr
esse
d in
the
Nor
ther
n Se
ctor
• Pr
ogra
mm
es a
re i
n pl
ace
for
Dis
play
Scr
een
Equ
ipm
ent
Ris
k A
sses
smen
t an
dtr
aini
ng•
a ke
y ro
le i
n th
is i
s er
gono
mic
s -
getti
ng i
t ri
ght
from
the
out
set
in t
he d
esig
nst
age
- fo
r ex
ampl
e on
She
arw
ater
, we
inve
sted
hea
vily
in a
n er
gono
mic
s st
udy.
Key
out
com
es w
ere
a m
aint
enan
ce p
hilo
soph
y of
shi
p-to
-sho
re f
or e
quip
men
tre
pair
, m
inim
isin
g m
anua
l w
ork
in
sub-
optim
al
conf
ined
sp
aces
, an
dco
nsid
erat
ion
for
the
loca
tion
of v
alve
han
dles
. A
gre
at h
elp
in d
efin
ing
the
ergo
nom
ics
was
the
sign
ific
ant i
nvol
vem
ent o
f of
fhor
e op
erat
ors
in th
e de
sign
• O
ur l
ates
t w
ork
is a
lso
focu
ssin
g on
Men
tal
heal
th i
ssue
s -
and
I w
ill r
etur
n to
this
late
r•
An
impo
rtan
t ste
p in
all
thes
e pr
ogra
mm
es is
ful
l inv
olve
men
t and
par
ticip
atio
nin
the
offs
hore
env
iron
men
t.•
We
are
utili
sing
our
off
shor
e m
edic
s as
an
inva
luab
le r
esou
rce
in t
his
resp
ect
with
the
ir r
ole
bein
g en
hanc
ed a
nd d
evel
oped
to
incl
ude
heal
th p
rom
otio
n an
dtr
aini
ng s
kills
• T
hese
are
som
e re
sults
fro
m o
ur 2
000
Shel
l Peo
ple
Surv
ey, w
hich
is v
ital i
n sh
owin
gth
e ex
peri
ence
and
fee
lings
of
our
staf
f an
d co
ntra
ctor
s vs
two
year
s ag
o•
Show
n he
re t
he r
elat
ive
mov
emen
t on
key
que
stio
ns f
rom
the
sur
vey
rela
ting
to o
urco
mm
itmen
t to
the
saf
ety,
and
to
the
heal
th,
of o
ur s
taff
, tw
o ke
y m
easu
res
onw
heth
er w
e ar
e m
eetin
g ou
r ob
ject
ives
of
dem
onst
ratin
g ou
r re
spec
t for
peo
ple
• T
here
are
two
poin
ts I
wou
ld li
ke to
hig
hlig
ht:
• fi
rstly
, w
e ca
n be
qui
te p
roud
of
the
sign
ific
ant
impr
ovem
ent
in S
taff
bel
ief
in o
urco
mm
itmen
t to
saf
ety,
rel
ativ
e to
ear
ly 1
998
- w
ith o
ur a
ttent
ion
mov
ing
to l
eadi
ngvs
lagg
ing
indi
cato
rs•
seco
ndly
, th
ere
is c
lear
ly a
lot
of
wor
k to
be
done
bef
ore
we
are
at t
he s
ame
leve
lw
ith h
ealth
• 19
98: 4
7% f
eel e
xces
sive
pre
ssur
e, in
200
0: 5
3%
Pre
ven
tin
g w
ork
rel
ate
d i
ll h
ea
lth
No
ise
CO
SH
H
Vib
rati
onE
rgo
no
mic
sMen
tal h
ealt
h
Mus
culo
-sk
elet
al
Incr
easi
ng S
ophi
stic
atio
n
Sh
ell
Su
rvey
Res
ult
s -
Ex
pro
02
04
06
08
01
00
Go
od
Wo
rk/
life
ba
lan
ce
No
t E
xc
es
siv
e W
ork
Pre
ssu
re
Ne
ve
r ig
no
re s
afe
ty r
ule
s
Sa
fety
Ta
ke
s P
rio
rity
fav
ou
rab
le r
es
po
ns
es
(%
)
19
98
20
00
19

lim
itin
g im
pact
of
illn
ess
thou
gh e
arly
inte
rven
tion
• ex
celle
nce
in f
irst
aid
and
em
erge
ncy
resp
onse
• E
xpro
wel
com
es t
he n
ew a
ppro
ved
code
of
prac
tice
in o
ffsh
ore
firs
t ai
d -
effe
ctiv
e A
pril
2001
, in
par
ticul
ar r
isk
base
d ap
proa
ch.
Thi
s su
ppor
ts o
urvi
ew
and
prac
tice
that
ef
fect
ive
casu
alty
m
anag
emen
t st
arts
w
ith
the
imm
edia
te a
id o
f a
colle
ague
, and
pro
gres
ses
thro
ugh
to t
he o
ffsh
ore
med
ical
supp
ort
and
evac
uatio
n fr
om t
he i
nsta
llatio
n as
nec
essa
ry.
UK
OO
A a
re a
lso
wor
king
on
med
ic tr
aini
ng a
nd c
ompe
tenc
ies
and
we
wel
com
e th
is•
expe
rtis
e in
off
shor
e em
erge
ncy
med
icin
e•
Key
to
of
fsho
re
med
icin
e is
co
mm
unic
atio
n an
d ef
fect
ive
links
w
ithse
cond
ary
and
tert
iary
car
e ce
nter
s on
the
bea
ch.
We
like
the
look
of
BP'
s"W
ay 2
Go"
pro
ject
loo
king
at
the
incr
ease
d us
e of
tel
emed
icin
e in
the
offs
hore
env
iron
men
t an
d w
e lo
ok f
orw
ard
to s
eein
g an
d un
ders
tand
ing
the
oppo
rtun
ities
this
will
giv
e us
.•
earl
y an
d ac
tive
reha
bilit
atio
n of
the
ill/in
jure
d•
We
have
ver
y fe
w i
njur
ies
/abs
ence
s th
roug
h ill
hea
lth -
abo
ut 1
% o
f th
ew
orkf
orce
at
any
one
time.
H
owev
er t
he c
osts
of
an a
bsen
ce i
n th
e of
fsho
rein
dust
ry
are
very
hi
gh
-
abou
t £7
00
per
day.
So
earl
y an
d ac
tive
reha
bilit
atio
n is
vita
l. W
e ut
ilise
fle
xibl
e w
orki
ng p
ract
ice
(par
t tim
e, w
ork
from
hom
e )
for
our
on s
hore
sta
ff a
nd o
ffsh
ore
are
usin
g de
taile
d ca
se r
isk
asse
ssm
ent
to d
ecid
e w
hen
we
can
safe
ly r
etur
n em
ploy
ees
to t
he o
ffsh
ore
envi
ronm
ent.
We
are
chal
leng
ing
prev
ious
ly h
eld
belie
fs t
hat
som
e ill
ness
espr
even
t of
fsho
re w
orki
ng -
e.g
. on
diab
etes
. Of
prim
e im
port
ance
is
wha
t th
ein
divi
dual
wan
ts.
We
shou
ld r
emem
ber
that
it is
the
"saf
e fu
nctio
nal c
apac
ityth
at c
ount
s an
d no
t the
illn
ess
labe
l"
prom
otin
g he
alth
and
hea
lthy
beh
avio
urs
• ch
alle
ngin
g he
alth
beh
avio
urs
• ob
esity
, ina
ctiv
ity, s
mok
ing,
alc
ohol
and
sub
stan
ce a
buse
• A
war
enes
s pr
ogra
mm
es•
Hea
lth p
rom
otio
n pr
ogra
mm
es -
in
the
curr
ent
year
we
are
runn
ing
prog
ram
mes
on h
ealth
y ea
ting,
exe
rcis
e, tr
avel
hea
lth, i
nfec
tious
dis
ease
s an
d dr
ug a
nd a
lcoh
olaw
aren
ess
• A
key
are
a to
foc
us i
s on
our
wor
k/lif
e ba
lanc
e -
and
ther
e is
a k
ey r
ole
here
for
lead
ersh
ip b
y ex
ampl
e -
I kn
ow h
ow I
str
uggl
e•
The
pro
visi
on o
f sp
orts
fac
ilitie
s on
and
off
shor
e, a
nd t
he e
ncou
rage
men
t fo
rSp
orts
is k
ey, i
n A
berd
een
thro
ugh
the
Pect
en C
lub
and
the
Woo
dban
k fa
cilit
ies
• I
know
that
I s
houl
d do
mor
e he
re m
ysel
f!•
you
may
fin
d it
hard
to
belie
ve t
hat
I us
ed t
o ru
n m
arat
hon’
s -
15 y
ears
and
3st
one
ago!
• th
at m
ay n
ot e
asily
ret
urn,
but
per
sona
lly I
am
com
mitt
ed t
o m
y st
ep c
hang
epe
rson
al c
ontr
act
- in
clud
ing
regu
lar
exer
cise
, an
d I
am v
ery
luck
y to
hav
ere
ceiv
ed th
e co
mm
itmen
t of
my
colle
ague
s to
hel
p su
ppor
t me
achi
eve
thos
e go
als
Lim
itin
g i
mp
act
of
illn
ess
thro
ug
h e
arly
in
terv
enti
on
•E
xcel
lenc
e in
fir
st a
id a
nd e
mer
genc
y re
spon
se
–ne
w a
ppro
ved
code
of
pra
ctic
e
•ex
per
tise
in
off
shor
e em
erge
ncy
med
icin
e
–co
mm
un
icat
ion
and
sec
onda
ry/t
erti
ary
care
cen
tres
•ea
rly
and
act
ive
reha
bili
tatio
n o
f th
e il
l/in
jure
d
–“s
afe
fun
ctio
nal
cap
acit
y”
cou
nts
, n
ot “
illn
ess
labe
l”
Pro
mo
tin
g h
ea
lth
an
d h
ea
lth
y b
ehav
iou
rs
•C
hal
leng
ing
hea
lth
beh
avio
urs
–ob
esit
y
–in
acti
vity
–sm
oki
ng
–al
coho
l
–su
bsta
nce
abus
e
•A
war
enes
s pr
ogra
mm
es
•W
ork
/lif
e ba
lanc
e
•S
port
s fa
cili
ties
20

Hea
lth
man
agem
ent
thro
ug
h t
he
sup
ply
ch
ain
She
ll s
taff
off
shor
e
Co
re o
ffsh
ore
con
tract
ors
Itin
eran
to
ffsh
ore
con
tract
ors
Co
ntr
acto
rso
n t
hei
rin
stal
lati
ons
Dec
reas
ing
influ
ence
• It
is
vita
l to
rec
ogni
se t
hat
the
thre
e ar
eas
of f
ocus
I h
ave
just
des
crib
ed a
pply
to
all
peop
le in
volv
ed in
our
ope
ratio
ns o
ffsh
ore
– w
e ha
ve t
radi
tiona
lly f
ocus
sed
on o
ur S
hell
staf
f, b
ut h
ave
reco
gnis
ed t
hat
we
have
lif
e of
fie
ld a
llian
ces
with
our
int
egra
ted
serv
ice
cont
ract
ors,
and
we
are
wel
l ad
vanc
ed
in
ensu
ring
lik
e-fo
r lik
e tr
eatm
ent,
enco
urag
ing
our
core
cont
ract
ors
to a
dopt
pol
icie
s an
d pr
actic
e to
at l
east
our
sta
ndar
d–
our
infl
uenc
e on
itin
eran
t off
shor
e co
ntra
ctor
s is
sm
alle
r•
as a
min
imum
, w
e pr
ovid
e id
entic
al o
ffsh
ore
med
ical
fac
ilitie
s an
dca
re
- bu
t w
e ar
e in
crea
sing
ly
chec
king
on
th
e w
ider
he
alth
man
agem
ent p
ract
ices
of
such
em
ploy
ers
– th
e ha
rdes
t gro
up to
infl
uenc
e ar
e th
e co
ntra
ctor
s on
the
ship
s, r
igs
and
barg
esin
volv
ed in
our
ope
ratio
ns•
we
will
en
cour
age
our
regu
lar
cont
ract
ors
to
deve
lop
heal
thm
anag
emen
t sy
stem
s co
mpa
rabl
e w
ith
our
own
to
ensu
re
the
prot
ectio
n of
thei
r st
aff
Ma
na
gin
g O
cc
up
ati
on
al
He
alt
h
•L
eade
rshi
p
•C
om
pli
ance
•C
on
tinu
ou
s im
pro
vem
ent
•K
no
wle
dge
•S
kill
s
•S
uppo
rt
• C
omm
on to
man
agin
g th
e th
ree
area
s:–
prev
entin
g w
ork
rela
ted
heal
th–
redu
cing
the
impa
ct o
f illn
ess
– pr
omot
ing
heal
th a
nd h
ealt
hy b
ehav
iour
s•
firs
t of
all l
eade
rshi
p, a
nd th
e fi
ve k
ey p
rogr
amm
e to
pics
fro
m th
e H
SE s
trat
egy
• I
shal
l fir
st o
f al
l foc
us o
n th
e ro
le o
f le
ader
ship
,•
then
I s
hall
disc
uss
man
agin
g co
ntin
uous
im
prov
emen
t an
d co
mpe
tenc
e an
d sk
ills
deve
lopm
ent,
pres
entin
g so
me
key
data
fro
m E
xpro
21

Lea
der
ship
Vis
ible
an
d c
lear
lea
ders
hip
•li
ne m
anag
emen
t
•su
pe
rvis
ors
•sa
fety
rep
rese
nta
tiv
es a
nd
HS
E f
oca
l po
ints
•In
du
stry
-wid
e S
up
po
rt
–In
du
stry
Lea
ders
hip
Tea
m
–H
SE
- r
evit
alis
ing
Hea
lth
and
Saf
ety
–U
KO
OA
–S
tep
Cha
nge
in S
afet
y
• V
ital t
hat a
ll co
mpa
nies
hav
e cl
ear
lead
ersh
ip o
n H
SE a
nd e
spec
ially
hea
lth,
whi
ch c
an b
e ne
glec
ted
part
.•
Lin
e m
anag
emen
t -
visi
ble
com
mitm
ent
& k
now
ledg
e, a
nd c
reat
ing
anen
viro
nmen
t w
here
su
perv
isor
s ar
e co
mm
itted
to
ke
y ro
le
in
taki
ngac
coun
tabi
lity
for
thei
r st
aff’
s he
alth
, eng
agin
g a
netw
ork
of s
taff
, inc
ludi
ngof
fsho
re s
afet
y re
ps a
nd o
nsho
re H
SE f
ocal
poi
nts
• L
eade
rshi
p on
Hea
lth is
an
indu
stry
, not
a c
ompa
ny is
sue
• ke
y ro
les
here
are
with
the
indu
stry
lead
ersh
ip te
am, w
ith r
epre
sent
atio
n no
ton
ly f
rom
the
ope
rato
rs b
ut a
lso
from
sup
plie
rs,
cont
ract
ors,
SM
E’s
and
Tra
de U
nion
s•
the
regu
lato
r pl
ays
a ke
y ro
le -
and
we
wel
com
e th
e fo
cus
give
n in
the
HSE
stra
tegy
on
Rev
italis
ing
Hea
lth a
nd S
afet
y•
Supp
ort
also
fro
m t
he t
rade
ass
ocia
tions
, in
clud
e U
KO
OA
, O
CA
, IA
DC
,IM
CA
, BR
OA
etc
.•
Key
rol
e fo
r O
IAC
, wor
king
with
Ste
p C
hang
e
Ma
na
gin
g c
on
tin
uo
us
imp
rove
me
nt
•M
anag
emen
t sy
stem
s
•M
easu
rin
g p
erfo
rman
ce
–G
HQ
–T
RO
IF
–A
nxi
ety
•S
hari
ng
lea
rnin
g a
nd b
est p
ract
ice
• O
ne o
f th
e ke
y co
mm
itmen
ts w
e ar
e m
akin
g as
an
indu
stry
is
to m
anag
eco
ntin
uous
impr
ovem
ent
• A
lthou
gh
we
have
de
velo
ped
form
al
man
agem
ent
syst
ems
for
HSE
, he
alth
man
agem
ent
has
som
ehow
not
bee
n tr
eate
d as
rig
orou
sly
as o
ur s
afet
y or
envi
ronm
ent p
erfo
rman
ce•
I w
ould
lik
e to
rem
ind
ours
elve
s of
the
key
ele
men
ts r
equi
red
to m
anag
eco
ntin
uous
impr
ovem
ent
– fi
rst t
he r
ole
of m
anag
emen
t sys
tem
s–
seco
ndly
th
e ke
y ne
ed
to
mea
sure
ou
r pe
rfor
man
ce
- w
ith
som
ein
tere
stin
g ex
ampl
es–
and
thir
dly,
how
to
acce
lera
te t
he i
mpr
ovem
ents
acr
oss
our
indu
stry
by
shar
ing
lear
ning
and
bes
t pra
ctic
e
22

Ide
nti
fy &
Ass
ess
Ris
ks
Op
era
tion
al
con
tro
l
Mo
nit
ori
ng
lega
lco
mp
lian
ce
Pol
icy
Leg
al
Ro
les
&re
sour
ces
Do
cum
en
t-a
tion
Re
cord
s
Co
rre
ctiv
ea
ctio
n
Re
vie
w
Au
dit
Gen
eric
Ma
na
gem
en
t S
yst
em
Ob
ject
ives
& T
arg
ets
Man
agem
ent
Pro
gra
mm
e
• T
his
diag
ram
is
ta
ken
from
ou
r w
ork
on
ISO
14
001
for
our
Env
iron
men
tal
Man
agem
ent
Syst
ems
- it
look
s in
cred
ibly
du
ll bu
t I
com
men
d it
to
you
for
exam
inin
g yo
ur H
ealth
Man
agem
ent S
yste
m•
it is
rea
lly v
alid
for
any
man
agem
ent
syst
em,
cont
aini
ng t
he t
hree
key
ele
men
ts o
fpl
an, d
o, r
evie
w:
– pl
an -
the
fiv
e ite
ms
show
n in
gre
en,
incl
udin
g ke
y in
puts
suc
h as
our
com
pany
pol
icy,
leg
al a
nd o
ther
req
uire
men
ts,
a m
echa
nism
to
iden
tify
and
asse
ss th
e ke
y ri
sks
or a
spec
ts to
man
age,
set
ting
clea
r ob
ject
ives
and
targ
ets
for
thes
e as
pect
s (a
nd t
hese
mus
t be
mea
sura
ble
- I
will
com
e ba
ck t
o th
is i
na
mom
ent)
, and
dev
elop
ing
a m
anag
emen
t pro
gram
me
to d
eliv
er th
e ta
rget
s–
do -
sho
wn
in y
ello
w a
re t
he o
pera
tiona
l el
emen
ts o
f ac
tual
ly d
eliv
erin
g th
epl
an
- w
ith
key
assi
gned
ro
les
and
reso
urce
(a
nd
rela
ted
to
this
th
eco
mpe
tenc
es
and
skill
s w
hich
I
shal
l co
ver
mor
e sp
ecif
ical
ly),
th
eop
erat
iona
l le
vel
cont
rols
suc
h as
man
ual
hand
ling
proc
edur
es o
r pr
oced
ures
for
nois
e m
appi
ng, a
nd th
e ba
sic
docu
men
t cen
tre
proc
esse
s–
and
in b
lue
the
revi
ew a
nd a
udit
proc
ess
- of
ten
lack
ing,
but
vita
l fo
ren
suri
ng
we
mon
itor
lega
l co
mpl
ianc
e,
iden
tify
corr
ectiv
e ac
tion,
an
dpr
ovid
e ke
y le
arni
ng f
or th
e ne
xt p
lan
cycl
e
Gen
eric
Ma
na
gem
en
t S
yst
em
Ide
nti
fy &
Ass
ess
Ris
ks
Op
era
tion
al
con
tro
l
Mo
nit
ori
ng
lega
lco
mp
lian
ce
Pol
icy
Leg
al
Ro
les
&re
sour
ces
Do
cum
en
t-at
ion
Re
cord
s
Co
rre
ctiv
ea
ctio
n
Re
vie
w
Au
dit
Ob
ject
ives
& T
arg
ets
Man
agem
ent
Pro
gra
mm
e
need
to im
pro
ve
sati
sfa
cto
ry
go
ing
wel
l
• M
any
part
s of
the
man
agem
ent
syst
em a
re f
irm
ly i
n pl
ace
- sh
own
in g
reen
, e.
g.ou
r po
licy,
und
erst
andi
ng o
f le
gal r
equi
rem
ents
• T
hose
in a
mbe
r ar
e O
.K.,
but w
e co
uld
still
do
bette
r•
We
have
iden
tifie
d ke
y is
sues
, and
are
mea
suri
ng o
ur p
erfo
rman
ce•
A k
ey a
rea
to im
prov
e is
in th
e se
tting
of
targ
ets
and
obje
ctiv
es–
cros
s-in
dust
ry d
atab
ase
for
base
line
data
– co
mm
on m
easu
rem
ent m
etho
ds•
I sh
all
show
som
e of
the
key
mea
sure
s th
at w
e ha
ve b
een
mea
suri
ng i
n E
xpro
,w
hich
we
expe
ct to
pro
vide
a g
ood
basi
s fo
r th
e di
scus
sion
on
setti
ng o
bjec
tives
23

Mea
suri
ng
an
d i
mp
rovi
ng
in
he
alt
h
Tot
al r
ecor
dabl
e oc
cupa
tiona
l illn
ess
freq
uenc
y(S
hell
and
cont
ract
ors)
012345678case rate
19
95
19
96
19
97
19
98
19
99
20
00
• O
ur m
ain
mea
sure
of
heal
th p
erfo
rman
ce is
our
TR
OIF
dat
a•
tota
l re
cord
able
occ
upat
iona
l ill
ness
fre
quen
cy r
ate,
exp
ress
ed a
s th
e nu
mbe
r of
los
tw
orkt
ime
case
s pe
r m
illio
n ho
urs
wor
ked
• It
ha
s sh
own
a st
eady
im
prov
emen
t ov
er
the
past
fi
ve
year
s w
ith
part
icul
arim
prov
emen
t in
a r
educ
ed n
umbe
r of
str
ess
rela
ted
case
s an
d de
rmat
itis
due
tosi
gnif
ican
t im
prov
emen
ts in
the
man
agem
ent o
f ha
zard
ous
chem
ical
s in
our
off
shor
een
viro
nmen
ts•
2000
She
ll G
loba
l ave
rage
is 1
.5 -
we
perf
orm
bet
ter
• In
200
0 th
ere
wer
e 17
cas
es o
f oc
cupa
tiona
l illn
ess
resu
lting
in a
loss
of
570
wor
king
days
.•
TR
OIF
dat
a is
a v
ery
usef
ul m
easu
re b
ut w
e ha
ve to
be
vigi
lant
to e
nsur
e w
e ca
ptur
eal
l ne
w c
ases
as
they
occ
ur.
As
with
all
such
mon
itori
ng s
chem
es t
here
is
a da
nger
of
unde
rrep
ortin
g,
with
su
bseq
uent
di
stor
tion
of
the
true
pi
ctur
e -
so
mor
eco
nsite
men
t mea
sure
men
t is
need
ed
Mea
suri
ng
an
d i
mp
rovi
ng
in
he
alt
h
01
02
03
04
05
06
0
Ex
pro
95
Ex
pro
98
Ex
pro
99
Ex
pro
20
00
Civ
al
Se
rva
nts
Me
dic
al
Stu
de
nts
NH
S 9
5
Ho
me
les
s m
oth
ers
%
Case rate
GHQ
>3
Men
tal
Hea
lth
- D
istr
ess
Be
nch
ma
rks
• G
ener
al H
ealth
Quo
tient
is a
wid
ely
reco
gnis
ed m
easu
re o
f un
derl
ying
ove
rall
psyc
holo
gica
l hea
lth.
• T
his
is a
mea
sure
of
psyc
holo
gica
l he
alth
and
sho
ws
a st
able
tre
nd o
ver
five
year
s w
ith th
e E
xpro
pop
ulat
ion
com
pari
ng w
ell t
o th
e ge
nera
l pop
ulat
ion.
• T
here
are
how
ever
sig
nifi
cant
num
bers
of
peop
le i
n th
e co
mpa
ny w
ho a
reop
erat
ing
with
sig
nifi
cant
leve
ls o
f di
stre
ss a
nd th
is is
was
tefu
l.•
Not
onl
y is
the
re a
hum
an c
ost
but
a lo
st b
usin
ess
oppo
rtun
ity a
s 15
% o
f ou
rhu
man
res
ourc
e w
ill b
e pe
rfor
min
g at
les
s th
an o
ptim
al l
evel
s.
We
cons
ider
that
Exp
ro i
s a
lead
er i
n th
is a
rea.
V
ery
few
oth
er o
rgan
isat
ions
hav
e a
data
base
of
know
ledg
e, w
hich
allo
ws
inte
rpre
tatio
n an
d tr
acki
ng o
f th
e st
ress
issu
e in
this
way
.
24

Mea
suri
ng
an
d i
mp
rov
ing
in
he
alt
h
HA
DS
An
xie
ty c
ase
ra
tes
(>1
0)
Sh
ell
Sta
ff
02468
10
Percentage of
survey
19
95
19
98
19
99
20
00
On
sh
ore
Off
sh
or
e
• (H
ospi
tal
Anx
iety
Dep
ress
ion
Scal
e) H
AD
S an
xiet
y is
a m
arke
r fo
r le
vels
of
psyc
holo
gica
l dis
tres
s in
the
orga
nisa
tion.
• Is
a u
sefu
l rea
l tim
e m
easu
re o
f th
e le
vels
of
anxi
ety
with
in th
e co
mpa
ny a
nd h
asde
mon
stra
ted
that
whi
lst
ther
e is
no
epid
emic
of
stre
ss w
e do
see
poc
kets
and
vari
atio
n be
twee
n di
rect
orat
es a
nd w
ith ti
me
• th
e ov
eral
l tr
end
over
the
pas
t th
ree
year
s is
con
stan
t on
shor
e, b
ut e
spec
ially
dow
nwar
ds o
ffsh
ore
• us
ing
this
tec
hniq
ue w
e ar
e ab
le t
o fo
cus
activ
ity t
o as
sist
our
em
ploy
ees
and
mon
itor
thei
r pr
ogre
ss•
inte
rven
tions
in
stre
ss h
ave
utili
sed
both
ind
ivid
ual
trai
ning
and
org
anis
atio
nal
appr
oach
es–
orga
nisa
tiona
l ap
proa
ches
ar
e ba
sed
on
dire
ctiv
es
unde
rsta
ndin
gw
orkp
lace
issu
es c
ontr
ibut
ing
to h
igh
leve
ls o
f st
ress
in th
e w
orkp
lace
-es
peci
ally
dep
artm
ents
with
hig
h le
vels
of
chan
ge–
Man
ager
s sp
ottin
g th
e sy
mpt
oms
of s
tres
s an
d im
prov
ing
thei
r ab
ility
to m
anag
e–
Indi
vidu
al
prog
ram
mes
ha
ve
incl
uded
In
ner
Qua
lity
Man
agem
ent
whi
ch
aim
s to
te
ach
staf
f
pers
onal
sk
ills
to
assi
st
with
st
ress
man
agem
ent
– th
e co
mpa
ny E
VP
and
valu
es a
nd b
ehav
iour
s pr
ogra
mm
es a
re k
ey n
ext
step
s in
thi
s re
spec
t an
d w
e w
ill c
lose
ly m
onito
r th
e im
pact
of
thes
ein
itiat
ives
on
the
heal
th o
f ou
r w
orkf
orce
.
Sh
arin
g o
f le
arn
ing
an
d b
est
pra
ctic
e
•U
KO
OA
Hea
lth
Ad
viso
ry C
om
mit
tee
•O
ccu
pat
ion
al H
ealt
h w
ork
ing
gro
up
re
po
rtin
gth
rou
gh
th
e S
tep
Cha
nge
Ste
erin
g C
om
mit
tee
•L
earn
ing
fro
m S
tep
Cha
nge
–le
ader
ship
co
mm
itm
ent
–su
perv
isor
ski
lls a
nd a
war
enes
s
–at
titu
des
an
d b
ehav
iou
rs
–w
ork
forc
e in
volv
emen
t
• w
e w
elco
me
the
focu
s gi
ven
to H
SE b
y “R
evita
lisin
g H
ealth
and
Saf
ety”
• w
e w
ill p
artic
ipat
e ac
tivel
y in
the
Occ
upat
iona
l H
ealth
Wor
king
Gro
up -
with
Rob
inD
onel
ly, o
ur n
ew s
enio
r m
edic
al a
dvis
or•
lead
ing
and
cont
ribu
ting
to th
e de
bate
in o
ffsh
ore
heal
th c
are
in a
ll its
for
ms
• w
e ho
pe t
o bu
ild o
n th
e ex
celle
nt r
elat
ions
hips
we
have
bui
lt up
thr
ough
the
ste
pch
ange
in s
afet
y w
ork
• th
ere
will
be
key
less
ons
we
can
adop
t fro
m th
e st
ep c
hang
e pr
ogra
mm
e–
focu
s on
lead
ersh
ip–
Supe
rvis
or s
kills
and
aw
aren
ess
– fo
cus
on a
ttitu
des
and
beha
viou
rs -
look
ing
afte
r yo
ur c
olle
ague
s–
vita
l rol
e of
wor
kfor
ce in
volv
emen
t
25

Co
mp
eten
ce a
nd
sk
ills
dev
elo
pm
ent
•O
ccu
pat
ion
al h
ea
lth is
no
t ju
st f
or
med
ical
adv
isor
s
•D
eve
lop
men
t of
skil
ls a
nd
un
der
stan
din
g a
t all
lev
els
in t
he
org
anis
atio
n
•C
om
pet
ence
is
mo
re t
ha
n k
no
wle
dg
e
• K
ey t
o an
im
prov
ed p
erfo
rman
ce i
n oc
cupa
tiona
l he
alth
is
deve
lopi
ng s
kill
s an
daw
aren
ess
at a
ll le
vels
- h
ealth
is n
ot a
pur
ely
func
tiona
l act
ivity
of
the
occu
patio
nal
heal
th d
epar
tmen
t.•
IN E
xpro
- a
num
ber
of p
rogr
amm
es w
ill c
ome
toge
ther
to
achi
eve
the
desi
red
outc
ome
of b
ette
r he
alth
..•
Wor
k pl
ace
exam
ples
inc
lude
Dis
play
Scr
een
Equ
ipm
ent
prog
ram
me
utili
sing
aco
mpu
ter
base
d tr
aini
ng p
acka
ge w
hich
is
sim
ple,
eff
ectiv
e an
d hi
ghly
acc
essi
ble
toal
l of
the
wor
kfor
ce v
ia o
ur in
tran
et p
age.
• A
rev
iew
of
man
ual
hand
ing
in t
he o
ffsh
ore
envi
ronm
ent
is u
nder
way
to
atte
mpt
to
redu
ce i
njur
ies
and
abse
nce
from
thi
s ac
tivity
. I
t w
ill l
ook
at b
oth
orga
nisa
tiona
lis
sues
- t
he w
orkp
lace
, the
way
we
do t
he j
ob b
ut a
lso
pers
onal
ski
lls i
nclu
ding
ris
kas
sess
men
t and
saf
e lif
ting.
• M
anag
ers
have
rec
eive
d sp
ecif
ic t
rain
ing
on s
tres
s du
ring
cha
nge
man
agem
ent,
for
exam
ple
for
the
mov
e of
our
sta
ff f
rom
Lon
don
to A
bder
deen
fol
low
ing
the
sale
of
our
Lon
don
Hea
d O
ffic
e in
199
9•
com
pete
nce
is m
ore
than
kno
wle
dge
- it
invo
lves
beh
avio
ur m
odif
icat
ion
• to
ach
ieve
thi
s w
e ne
ed
buy
in a
nd a
ctiv
e pa
rtic
ipat
ion.
E
asy
to s
witc
h pe
ople
off
-pa
rtic
ular
ly f
or a
spec
ts o
f th
eir
heal
th w
hich
the
y m
ay r
egar
d as
per
sona
l an
dno
thin
g to
do
with
wor
k
Co
ncl
usi
on
s
•S
hell
Exp
ro h
as a
str
on
g t
rack
rec
ord
of c
om
mit
men
t to
heal
th i
ssue
s w
ith
co
nsi
der
able
suc
cess
•tr
adit
iona
l haz
ard
s ar
e co
ntro
lled
, but
we
mus
t not
be
com
pla
cent
•ne
wer
ch
alle
nges
in s
ocie
ty,
as w
ell
as t
he
wo
rkp
lace
,
dem
and
that
we
lead
and
del
iver
on
hea
lth
•it
’s a
win
fo
r o
ur
peo
ple,
it’
s a
win
fo
r S
hell
Exp
ro
• In
con
clus
ion:
• Sh
ell E
xpro
will
rem
ain
com
mitt
ed to
hea
lth is
sues
• W
e ha
ve id
entif
ied
key
area
s fo
r im
prov
emen
t, an
d w
e lo
ok f
orw
ard
to w
orki
ng w
ithin
dust
ry to
mee
t the
cha
lleng
es f
acin
g us
• O
ccup
atio
nal H
ealth
is a
ver
y re
war
ding
are
a:–
it’s
a w
in f
or o
ur p
eopl
e, a
nd a
win
for
our
bus
ines
s–
a ch
alle
nge
to o
ur in
dust
ry to
rai
se o
ur g
ame
26

Nex
t S
tep
s fo
r In
du
stry
•M
ajo
r ch
alle
nge
stil
l ah
ead
•In
tegr
ate
focu
s on
Hea
lth
Im
pro
vem
ent i
n o
ur
ind
ust
ry in
Ste
p C
hang
e in
Saf
ety
–T
arg
ets
and
obje
ctiv
es
–S
hari
ng
of
bes
t p
ract
ise
–L
eade
rshi
p
–W
ides
prea
d In
volv
emen
t
• T
here
is s
till a
maj
or c
halle
nge
ahea
d fo
r in
dust
ry•
Inte
grat
e fo
cus
on H
ealth
Im
prov
emen
t in
our
indu
stry
in S
tep
Cha
nge
in S
afet
y–
Setti
ng b
asel
ine
Tar
gets
and
obj
ectiv
es–
Shar
ing
of b
est p
ract
ise
– L
eade
rshi
p–
Wid
espr
ead
Invo
lvem
ent -
ope
rato
rs, a
ll co
ntra
ctor
s, s
uper
viso
rs, w
orkf
orce
27

28
QUESTIONS AND ANSWERS SESSION
Question - Gareth Powell, BPOne of the things you mentioned was makinggreater use of your offshore medics andincreasing their skill base. I just wondered ifyou would like to comment on two aspects ofthat. One is when multi-tasking of medics isrequired and whether being asked to do non-medical functions might detract from theirmedic functions. There is also the question ofoutsourcing as against direct employment ofmedics.
Answer – Mr Malcolm Brinded, ShellYes I think they are both important. I'll takethe second one first. I think in the end, the keyis getting the right skills. Wherever you obtainthat from, you want to have the right skills, theright levels of performance and the rightcommitment. If you outsource because youregard it as more likely that you'll get long termthe quality of people that you want, it's no goodsaying it's no longer my problem. It mayactually give you more issues to focus on thanif you had traditional in-house capability.
I think multi-tasking is an important issue. It isa reality that we have reduced numbersoffshore. On some installations, where 10 or20 years ago there were 200 on the installationand a high degree of activity - andunfortunately of safety incidents and injuries,the medic was 100% occupied as a medic.
Where I think we have gone wrong, is to misswhere the workload on those individualsbecomes unmanageable and their core role as amedic is in some way diluted by the other tasksthey're asked to take on. That can happenparticularly during periods of upmanning to,say, do a summer shutdown. We've got thesame medic that we've always had, then comesthe summer shutdown, two or three times themanning on the installation, and you've notactually changed and supported the medic totake on that additional burden. That's the way Isee it.
Question - Dr Eirik Bjerkeboek, TheNorwegian Petroleum DirectorateYou showed us that you have quite a clear-cutdecrease in the case rate of work-related illnessduring recent years. You also touched on theissue of under reporting, and that you don'treckon that has increased, but do you see acomparable drop in sickness absence?
Answer – Mr Malcolm Brinded, ShellWe've done quite well on sickness absenceonshore but I'm not sure whether it's wholly asgood as the TROIF (Total RecordableOccupational Illness Frequency) data that I'veshown there. I don't know whether there'sanyone who can give me a supplementarycomment on that? Una?
Comment - Una Corpe, Senior OccupationalHealth Nurse, Shell ExproThe sickness absence rate for Shell Expro in2000 was just about 1%, which has droppedfrom previous years. The sickness absence rateis very low by comparison to national figures.As regards occupational health reporting, we'vegot a system in place where all cases that arereported through the offshore medics andthrough the onshore occupational health focalpoints are screened thoroughly andinvestigated to identify the causation for thereported cases. All cases that are reportedthrough the occupational health system areactually then recorded. There isn’t underreporting unless they haven't been brought toour attention.
Comment - Malcolm Brinded, ShellI suppose my only comment would be I suspectthere still is under reporting. I don't think it'sany worse, so I think that trend is fair. But Isuspect all of us have an intrinsic underreporting in some ways, particularly because ofthis lag effect that I referred to earlier in termsof time delay. I feel good that the trend is rightbut I'm sure that there are more cases thanthose statistics pick up in one way or another.
Question - Jake Molloy - OILC OffshoreUnionMalcolm, I was wondering if there is anysignificant difference between the statistics forShell staff and those of contractor staff onsickness absence etc. If so, would you holdwith the view that perhaps this is as a directresult of the significantly less hours exposurefor Shell staff compared with their contractorcompatriots.
Answer - Malcolm Brinded, ShellMy understanding is that where we've got gooddata, which is around offshore staff of our corecontractors, then we don't see such adifference. To go on to your second part, Idon't think there is a factor there in terms ofdifference in the hours worked. I think it is a

29
concern that we've not done as well in reallycapturing what is happening on the contractormanaged installations and perhaps to a certainextent the itinerant work force that comes andgoes around the patch. So in terms of 80% ofstaff offshore, typically 20-25% are Shell staffand of the remaining 75–80%, the majority,80%, of those are core staff who are long term
on our installations. We've got good data forthose, with no obvious difference in statisticsbut we haven't got data that extends properlyinto further up the staircase that I referred toearlier. It took us a long time to get there onsafety, but I think we have to get there onhealth as an industry.

30
31
OFFSHORE INDUSTRY ADVISORY COMMITTEEPERSPECTIVE
Mr Roger Spiller, MSF Offshore Team Leader
The role of OIAC
The Offshore IAC is part of an extensivenetwork of Advisory Committees which theHealth and Safety Commission, theExecutive’s governing body, set up to provideadvice to the Commission, issue industryguidance and to promulgate best practice notgood practice. An important point – As low asis reasonably practicable.
All ACs are tripartite bodies with employers,government and the trade unions represented.Additional members representing the widerpublic interest are now being introduced alongwith greater transparency.
Post Piper Alpha the emphasis was on newregulations and guidance promoting safetyresource shortage inevitably meant too littleregard for Health.
Revitalising Health and Safety and SecuringHealth Together – Cross departmentalcommitment from Government. Ministers areinvolved and remarkably well briefed - notleaving it to others and they expect action.Keeping an eye on what we do.
Review of IACs. Are we effective; arerelationships too cosy; is our work relevant tothe needs of the industry? If not, then they willeither act without us, in spite of us or find amore effective mechanism for action. Gone arethe days when if we couldn’t agree or reachconsensus nothing happened. Government nowwant the range of options not the conventionalwisdom a la MAFF.
OIAC therefore has to prove itself dealing withHealth
First is Problem identification – what problem?RIDDOR; cause and effect; short working lifeoffshore; often long development time fordisease; presentation of disease when theworker is out of the industry or retired.
Costs to industry – skill shortage; training andassimilation; loss of knowledge; higher
insurance premiums; reducedproductivity/efficiency; higher safety risks.
Health not occupational health – cause isirrelevant if the worker is unable to work or isineffective – cost/inconvenience to employerare the same.
Integral to success is rehabilitation which is notgood due in large part to perhaps to the historicorganisation of the industry where operatorsgave responsibility but often little authority toContractors who simply recruited areplacement. Not any more.
Last year change in name from “Oil” to“Offshore” to focus more clearly.
Unique series of problems for OIAC – workersspend half their life offshore including leisuretime.
Health (physiological and psychological) offamilies also relevant
Globally mobile workforce – increasingproportion due to more overseas work withAberdeen and elsewhere as source of expertise.
Revolution in working methods – maintenance,vendor, campaign and less planned; floatingsystems, sub sea; reliability.
But we have older platforms and smallernumbers with ageing plant tied in to a -
Changed workforce – higher proportion ofcontractors; ageing workforce; long serviceworkforce.
Reduced numbers (35,000 to <20,000);reduced transport; greater responsibility;reduced flexibility
Perception of Stress; insecurity; uncertainty;unreliability

32
The aim of this Conference is to raise profileand create an awareness of health as an
issue as well as looking at the problems andsome solutions
Problem solving – OIAC unique ability –Operators-various varieties of Contractor-unions and various regulators (policy andoperations). (HSE; CAA; MCA; DTI) All addscredibility to the total package thus betterreceived by the workforce, not just furtherexhortation from employer.
OIAC in conjunction with Step Change – SCneeds to focus on the practical avenues forimprovement uniting the whole industry and allstakeholders about the issues and solutions.OIAC to take the political and morecontentious issues forward.
Workforce and management networks – bestpractice and informality
Target setting criteria in hand – realistic yetstretching
A great asset is the existing high standards ofOccupational Health provision by someoperators. Even greater is the availability ofmedics on each installation for recording;health promotion; consistent interpretation anda humanitarian approach to health issues.
Vantage Card both for storage of informationand access to it
Conclusion
Industry is beginning to recognise the costs ofill health
A partnership beginning to develop born out ofOIAC and nurtured by Step Change
Only way of tackling the problems broughtabout by – declining fields; reduced numbers;multi-tasking; additional pressures- stress;remote fields; incorporation of Working TimeRegulations.
Big challenges will be how to deal withproducing an integrated rehabilitation policyand programme and preventing psycho-socialproblems, some of which seem inherent in theindustry, as required under “Securing HealthTogether”, securing the Offshore Industry’scontribution to Revitalising Health and Safety
Conference will have succeeded if we are ableto identify issues and develop ways of workingtogether without fear of the consequences, butconfidence in the outcome.

33
DAY 1
SESSION 2
SESSION THEME – OCCUPATIONAL HEALTH MANAGEMENT ANDIMPLEMENTATION

34

35
THE MEDICAL MANAGER’S PERSPECTIVE
Dr Jim Keech, BP, Manager Health BP Upstream UK, Chairman ofUKOOA HAC
The management of occupational health is anaspect of my task which I take most seriously.We hear - and it has become somewhat cliched- that 'good health is good business'.Unfortunately at times that seems to have beenthe business of cost accounting rather thanwhat I think the authors of the statement reallymeant.
Proactive versus reactiveThe value of a medical has often been simplyparaphrased to its price. That clearly isn't right.We have to change, to be proactive and notreactive. 'Medical' has been long associatedwith the oil industry but not necessarily 'health'and this is where we need to change. 'Health' isno longer something indistinct from safety. Toperform, we need to ensure that health is seenas distinct from safety, no longer that silent 'h'in HSE. But health should not be separatedfrom safety - it should learn and move forwardtogether with safety.
Managing risk - understanding thecomplexitiesHealth is a complex issue but it's not helped bybeing seen as only the preserve of doctors andnurses. Many doctors and nurses are poor atexplaining the complexities to their partnersand to other managers. We can use the samebusiness principles in health as are usedelsewhere in our industry. But it is necessaryfor us as health managers to learn thosebusiness principles and apply them. Health andsafety is very much about caring for people.'Caring' is an awkward word for many. Peoplefeel uncomfortable and think it means'motherhood and apple pie'. But it is aboutcaring for people getting sick, it's about caringfor people getting injured. Do you care enoughto prevent them getting sick and injured? Ithink, as you'll see later, that there is a link intosome processes which I hope you will takeforward in your respective companies.
Value demonstrationWe have had difficulty in health withdemonstrating value. When the oil price is up,we can talk about 'value'. When it's down, weonly hear about 'cost'. The concepts of 'good
cost' and 'bad cost' are often lost. We need toimprove our financial management. As healthmanagers, we need to understand aboutfinancial management, we need to talk to theaccountants. They have, after all, beenmanaging to convince the industry over theyears to move forward, to invest in projects.Project Way to Go was mentioned earlier. Forthat project to move forward I have tocomplete financial memorandums, I have tolearn the techniques, I have to find the'switches and buttons' that make mymanagement move. Unless I can learn thatlanguage, and unless I can find those switchesand buttons I am not going to succeed. Andhealth will not succeed - for us in BP at least.We had to get to materiality and to explain thatwe often work with very small budgetscompared with the enormous prizes that thereare in our industry - the millions and billionsthat we hear quoted. Very often our healthbudgets - and I control a budget of about £1million - are small beer. Because it's smallbeer, and because it doesn't add in the extendedhealth team, the medics offshore, the healthspending (where the total health spend issomewhere in the region of £5-6 million), itdoesn't reach materiality. It's too smalltherefore we can ignore it, therefore we canoutsource it, therefore we don't need to worry.In business, if you cost a lot, somebody takessome notice. Maybe I don't cost enough!
Meaningful metricsHow excited are you by the term 'occupationalillness frequency rate'? It doesn't excite memuch. This isn't the end of the truce betweenBP and Shell by the way. It's simply that, as ametric, this doesn't excite. It may bemeaningful because this is what we have to beabsolutely intolerant of. We cannot haveoccupational illness. Occupational hazards arenot acceptable. They show that we are notcaring enough. Occupational illness is what wecaused, it's what we did, it was the work thatmade them ill. People shouldn't come to workto get ill, to get sick, to get injured. After allthere is a healthy worker effect. Those inemployment are healthier than those who arenot, so let's build on that. Why not have those

36
people who come to work going homehealthier? What is wrong with that? Maybe wecan make those kinds of differences.
I think meaningful metrics will be a key.Sometimes we are very good at presentingmetrics which we like and which we know wecan manage. Sometimes we are going to haveto get into the meaning. 'Sickness absence' is apreferred metric of mine, simply because itmeans a lot. If somebody is not at work a lot ofmoney and a lot of pain are involved. We needto use that sort of meaningful metric - which issimple to understand and use and doesn'tinvolve deciding what's an occupational illnessand what isn't. After all, unless you can haveclear definitions of occupational illness thenyour occupational illness frequency rate is notgoing to change and may be subject tomanipulation.
Managing to performWe have to manage to perform. We have tolearn to start setting targets in health. Previousspeakers have mentioned this. We areencouraged to do this by government. I'm notparticularly happy with 'wet finger' estimatesand Labour Force Surveys being used as thedrivers but we have to start somewhere. We'veheard the excuses and we can work with it. Weare trying to do better in the industry. The workwe are trying to do with Step Change andformation of a Step Change OccupationalHealth Steering Group is a way forward. I hopethat we will be setting targets. But, each of usin our individual companies, and certainly inmy own case in BP, needs to think aboutsetting targets for ourselves. In BP, we havebeen working to a performance contract. Ithasn't been easy. Three years ago when the firstperformance contract was demanded by mythen line manager I thought 'Oh dear, nowwhat'. It had to go on one side of A4.Everything goes on one side of A4 these days -and no more than 4 bullets on a slide. Myperformance contract in Year 1 was nodifferent. But over the years I have becomeused to it, and those on my team will knowhow much value we have got out of theperformance contract. We have linkedperformance contract to terms, and to our ownpay at times - and that focusses the mindsomewhat!
Non-holistic is not an optionAlong with previous speakers, I do not see thatthe classification 'occupational' is particularlyuseful in our environment. In fact, there is aprofessor in Singapore who runs the Faculty of
Occupational Health. His faculty is shared withthe Faculty of Family Medicine andCommunity Medicine. So, within the samefaculty, general practice and public health areall included. That is the place we are at in anoffshore setting, where non-holistic is not anoption. You do have to cover health - as healthdefined by the World Health Organisation, as astate of total physical, psychological and socialwell being. There is nothing wrong with that asa definition of health. Those of you who workin health offshore know you cannot get awaywith just focussing on one aspect of thatdefinition.
We need to provide a breadth of service. Weare there 24 hours a day for a couple of weeksa month. There isn’t access to the generalpractitioner, to the counsellor, to all theservices that are commonplace in an onshoresetting. It's the whole person who comes towork, it's the whole person who gets sick, it'sthe whole person that needs to be dealt with.So 'holistic' could have a 'w' at the front of it -we need to look at that totality of care. Thisbrings us to the fact that we hear a lot aboutpsychological health. It is said thatpsychological health is important. Many of ourcompanies lack psychological health plans,because we have been dominated by physicalhealth in the past. We need to work on this. I'mglad to say the HSE is stimulating us. Theytried to stimulate us with an ACOP butfortunately other methods are now to the fore. Ihave worked hard with psychological healthplans myself. I don't know if it's been making adifference yet but certainly we are tracking thedata in the same way as Shell and others are, tosee whether the plans are working.
Inclusion of all stakeholdersSo, the services need to be holistic, broad andto include all the stakeholders. In the past theterm 'medical' was used. What was 'medical'? Itwas some medics and the UKOOA MAC as itwas called then. Health clearly has to include alot more than that. Everyone is a stakeholder intheir own health. There are many groups -professional groups, employment groups - whohave something very positive to add. I ampleased to say that the Step Change Initiativeand the work group we are trying to pulltogether is going to be a broad church. It willinclude stakeholders who have traditionally notbeen included. This encompasses the NHS - abody that has picked up our problems year onyear and dealt with them, with very littlesupport from ourselves. We need to recognisetheir input in terms of a stakeholder.

37
Demographic challengesWe have some interesting demographicchallenges. The ageing workforce is mentionedfrequently. In BP the average age of anoffshore worker is about 46 now. We havesmall specialist teams formed from the moreexperienced older men. The so-called SWATteams, that go fixing problems, tend to be olderpeople. Thus right sizing and specialist teamsbring with them their own health problems.
Contractorisation has been mentioned at lengthand does give us issues around control. But I'dlike to mention another challenge - the war fortalent - getting the right people to come intothe industry. Many of us, and BP is certainlyno exception, are after increased production.We can't grow production as a global companyunless we maintain the base of production wepresently get out of the North Sea. We have tomaintain that base and grow from it. To do so,we need people, and there is a war for talent.That is an area where health can positivelycontribute. It can be seen as a benefit. Thehealth benefits you can provide for youremployees can help win that war for talent.
Performance beyond complianceLooking at performance, we have heard thatthe industry under-reports. I would challengethat. But part of the problem has to be ourregulatory systems. If we only use a regulatorysystem to manage performance perhaps that isnot the right tool. Perhaps we need to look atother tools. We need to set up to managebeyond the compliance. Health is somewhatdifferent in that, unlike safety, it goes beyond'No (ill health)', it goes beyond zero. You canenhance health, which can be difficult in thesafety arena and certainly in environment. Oneperson's environmental enhancement isanother's environmental destruction. We needto be more imaginative in our goal setting forcontinuous improvement. There are some signsthat we are willing to do so. I recently took partin a workshop within BP where safety andhealth professionals worked together and, tomy surprise, decided that we would work on'wellness'. These were some serious hard-edgedsafety guys who I didn't think knew whatwellness meant. But we are looking at a newparadigm to try to improve performancebeyond the regulation, beyond compliance.
I titled the final slide 'Plan, Do, Measure,Learn, Improve' - a simple mantra that we oftenquote as the way to fix things. Hopefully, Ihave included in my list some of the positive
areas that we are moving into. Evidence-basedpractice and evidence-based medicine are the'in terms', the buzz words in the learnedjournals. The offshore industry needs evidence-based practice, and we have heard about ourlack of baselines. We are getting together thecross-industry health database and I appeal forvolunteers. Those who want to work in aworking group who are in this audience, pleaselet me know because I need people to help usin that endeavour.
Sharing best practiceThis conference is going to be about sharingbest practice. There is much that you are goingto hear over the next two days which is allabout sharing best practice. Hand armvibration, Noise, Health planning - all of thesethings we share. As an industry the last fiveyears has seen big changes. It has certainlyseen some changes on OIAC (the OffshoreIndustry Advisory Committee). Echoing thewords of previous speakers, we have movedmuch better together, we have had the publicagreement of Shell and BP, we have had thepublic agreement of Roger (Spiller) and myselfon matters during consultation on the ACOP. Ithink we all agree that the Regulations still gotthe wrong name being called 'First Aid', but theACOP actually says 'health care', which is avery big move forward.
Some of the work that was done during theconsultation on medic training will be takenforward by the UKOOA Health AdvisoryCommittee. We hope that will bring in a newera in medic training - more appropriate, moreembracing, more about multi-skilling ratherthan multi-tasking, and recognising theimportance of health promotion and matterssuch as hygiene. In my own company, we useour medic staff a great deal to deliver hygieneperformance on our offshore installations.
Managing challengesWe have some real challenges to manage.Managing the fitness to work - especially atpresent, firefighter fitness - raises issues, e.g. ifputting people into firefighting trainingexposes them to the risk of having a heartattack as a result of the exertion of the training.The date of knowledge has passed, we are notarguing whether it is bad for you or not. Thisisn't the same as mesothelioma and asbestosexposure - we know that if you push someoneto climb up and down a ladder while carrying ahose etc they may well have a heart attack.This may not occur while they are doing thetraining but afterwards. If we know that this is

38
a possibility, we have a duty of care to protectthe individuals from it. That means needing tofind a way of determining the underlying levelof fitness. This is not easy, it can mean havingto discriminate, but we have to do that againstthe background of the DisabilityDiscrimination Act. We have been done nofavours as an industry by not having theDisability Discrimination Act enacted offshore.Many of us in health management in theoffshore industry have taken it on in broadprinciple. We are moving now to a positionwhere, for example, we will look at stablediabetics being able to work offshore, we willlook at not excluding epileptics who have beenfit-free for many years, we will look at takingpeople who are on anti-depressant medicationand where is no safety contra-indication forthem being offshore. An SAS-type selectionshould not be applied before you are able to gooffshore. There is an ageing workforce so besensible. We have to deal with rehabilitation.Many of the companies are doing so as part oftheir case management.
Sustainable developmentFor those of you who follow things likesustainable development, I have included thisas I think it may be one of the keys to thefuture. Triple bottom line economics -Economic prosperity, Environmental qualityand Social justice - are known to our industry.We have a Sustainable Development Group inBP who talk about this topic all the time,maintain websites, and run conferences.Despite the taxation, and despite the oil price'scyclical nature, I think we have been prettygood at economic prosperity. In relation toenvironmental quality, we have learnt how toplay the green card. But what about socialjustice? I see social justice as the key. It's aboutwhat I said earlier, about being intolerant tooccupational hazards, being intolerant ofhurting people and of making them sick. It'sabout giving them justice.

39
T he Business of Health
♥ Good Health is Good Business♥ Proactive versus Reactive
♥Prof i le putting the H in HSE♥ M anaging risk, understanding the complexities, clarity of
processes♥ V alue demonstration
♥Good cost bad cost: getting to materiality♥M eaningful metrics
♥ M anaging to perform♥Setting targets♥The Performance Contract
Offshore Occupational H ealth
♥ Non holistic not an option♥Definition of Health♥Breadth of service provision
♥ All Stakeholders♥ Demographic challenges
♥Ageing workforce♥Right sizing♥Contractorization♥War for Talent
♥ Performance beyond regulation, beyond compliance,setting the right goals for continuous improvement
Plan, Do, M easure, L earn, Improve
♥ Evidence based practice♥Cross industry health database: Step Change
♥ Sharing best practice♥HAVS, Noise (NEM S), Health Planning
♥ M anaging challenges♥Fitness to Work, Disabil i ty, Rehabil i tation
♥ New ACoP: Health care and f irst aid …♥ Sustainable development
♥Triple bottom l ine♥Economic Prosperity, Environmental Quali ty and
Social Justice

40

41
THE CHALLENGE OF SETTING OCCUPATIONAL HEALTHTARGETS
Mr Stephen Williams, Step Change Support Team
[Paper given on behalf of Paul Blakeley, Talisman (UK) Ltd.]
The subject I have been asked to talk about isthe challenge of setting occupational healthtargets. I think that I should first dispel someexpectations that you may have. My paper isabout the challenge of setting the targets - Idon't have the answer. I'm not going to be ableto tell you what the targets are. Also, in thelight of the comments from previous speakers,it is perhaps also appropriate for me to dispelsome other expectations you might have aboutStep Change; about who or what Step Changeis.
Step Change is not an organisation that is setup to solve the industry’s problems. StepChange was a commitment by the wholeindustry to improve safety so it basicallyincludes all of you and all other people in theindustry. It's all of us who are going to have towork the issues and develop the solutions. Thesmall support team that I am part of will helpto facilitate that process. Some of the things Iwill talk about this afternoon will be about theways in which the support team can try tofacilitate the process of setting of the targetsand then the delivery against them. But,unfortunately, we are not going to be able to doit for you.
What's the challenge?Why is there a challenge for settingoccupational health targets? They have beenset for us, haven't they? 'Revitalising Healthand Safety' (RHS) and 'Securing HealthTogether' (SHT) contain the targets - what elseis there left to do apart from deliver againstthem?
Well, I'd like to share with you a little of theexperience of the Step Change in Safetyinitiative. This was started in 1997 with thetarget of improving safety by 50% over 3years. Clear enough? It sounds clear enoughuntil you get down to the detail of thinkingthrough:ð What does it actually mean?ð 50% of what?
ð How are you going to measure it?ð Where is the data going to come from?ð What baseline should you be using?
The same issues now apply for occupationalhealth. The targets may have been set for usbut what else do we need to do? Theexperience we had with Step Change suggeststhat the simple target is not sufficient. Thechallenge is to interpret the target and make itmeaningful and something that we can workwith.
The current reporting requirements areinadequate. We have heard how, according tothe RIDDOR statistics, chickenpox is the issuefor the offshore industry. Fortunately, I thinknone of us believe that is the real challenge.But then, what is the challenge? There are lotsof data within companies but there is a lack ofconsolidated data for the industry. The figuresthat were mentioned by speakers earlier thisafternoon - on musculoskeletal issues andothers - are based on estimates of what wethink are the main problems. But we lack thedata.
There is another problem with the targetswhich are set in 'RHS', and that is that they aremeasuring outcomes. These are occasionswhen things have gone wrong and we haveobserved a consequence. Yet we know that formany occupational illnesses there can be manyyears between the observable effects and theexposure that gave rise to them. If we wait untilwe have observable outcomes, we may buildup another 10 or 15 years of unavoidableconsequences that we don't want. Relying onthe outcomes, therefore, is not sufficient. Weneed a mixture of both proactive and reactivemeasures. By proactive measures, I mean thetype of measures that are sometimes referred toas leading indicators. These are things that wecan monitor now to give advanced warning offuture potential problems and allow corrective

42
actions to be taken before the unwantedoutcomes occur.
PartnershipThe need for partnerships has been referred toseveral times this afternoon. Building effectivepartnerships will be a major part of thechallenge.
There have been major changes in the industryover the past five years or so. The demarcationlines between different parts of the industry arenow very different from what they were. Thesources of expertise and the people who cancontribute to the debate and the solutions arenow very varied. We need to engage all partiesto participate in the discussion, to share theirinformation, share their learning and insights todevelop an effective way forward.
The need to work together and shareinformation brings up the point ofconfidentiality, particularly with the medicalissues, where there are obligations ofconfidentiality to the individuals. It's difficultto share the information and yet, if we are tounderstand what are the proactive things weshould look for, we need to understand notonly the outcomes to be avoided but also thecausation that leads to them. This will needanalysis of information about the circumstancethat may have contributed to the outcome, notjust the outcome itself. So there areconfidentiality issues to be overcome to enableinformation to be shared whilst still protectingthe confidentiality of personal information.
First stepsWhat has the industry done to tackle theseissues? There was a workshop on 11 January2001. Fifty people from across the industrycame together to talk about the challengesfacing the industry and the processes fordelivering on the targets that are contained inthe RHS and SHT documents and the othertargets from the HSE's Offshore Division.
There were three groups at the workshop:ð One considering the major hazards and
what needs to be done to improve integrity;ð Another dealing with occupational safety;ð And, the third one on occupational health.
It is this last one that we are really addressingtoday and in the subsequent days of thisconference. One of the main outcomes fromthat workgroup was the recognition that weneed to have a broad-based working group toaddress the occupational health challenge. This
group would need to understand the issues andfind ways of sharing data. It would need verybroad participation, not only from thepartnering groups that are active within theindustry, but also other ones, such as theNational Health Service, that are outside theindustry but who have a very real role to play.The Step Change support team has been askedto help co-ordinate the process. As I mentionedearlier, the support team can’t solve thechallenges for the industry but it can helpfacilitate the process through the mechanismsthat have been developed for engagingdifferent participants and through the networksthat enable greater workforce participation inthe debate.
What is the scope of work that theOccupational Health working group has setitself to do?The first activity is to develop commonclassification codes for occupational health.Many companies are already gatheringoccupational health data but do it in differentways. We need to agree a common way inwhich we can classify the information so that itcan be shared and we can try to understand thecausation as well as the outcomes.
There is also a debate on what kind ofindicators can be used. What is the right mix ofreactive and proactive indicators that can bothinform our actions and engage people'sinterests? Which indicators will help to makethe issues real and motivate effort to deliver thetargets? How are we actually going to measurethe data? What baselines are we going to use? Idon't have the answers to these questions butthey are part of the scope of work that theworking group will be addressing over theforthcoming months.
A database will probably be required to collectand handle the data. The issue ofconfidentiality of personal information willneed to be considered. It is likely that thedatabase will need to be held by a respectedand trusted third party that can be independentand can address the confidentiality issues.
I've got no answers to the OH challenges thathave been identified, but I do have a timelinefor how we are going to move forward.
The first part of the work will be a pilot study.A pilot is needed because we are not going toget it right first time. We are not going to get itright in all the details of the information thatneeds to be gathered. As we collect data we are

43
also going to develop additional insights intowhat the data means for the offshore industryand the actions that will be necessary toimprove occupational health in the industry.The proposal is to gather data for 6 to 9 monthsthrough to the early part of 2002. Followinganalysis of the pilot study, the industry willthen be in a position to:§ evaluate the information,§ finalise what the indicators should be,§ confirm the way data will be collected,§ confirm the ways of interpreting the data,§ initiate full implementation during Q2 of
2002.
We have undertaken to develop this planfurther and to report on progress to theOffshore Industry Advisory Committee(OIAC) in time for their July meeting. Thismilestone will help to maintain a sense ofurgency and ensure that, although it's a 10-yearprogramme for RHS, we start to take actionsnow.
Communication of progress.There is a recognised lack of reliableoccupational health data. Without data it isdifficult to know what the problem is and whatcan be done to improve performance. Thisleads to the ‘chicken and egg’ situationreferred to earlier by Sandra (Caldwell); Whatdo you do first, gather the information toestablish a baseline or set the targets?
The way the UK offshore industry proposes tomove forward is to accept the nationalimprovement target and then collect data toestablish the baseline and identify actions todeliver the required improvement. Once thedatabase and data collection process have beenput in place, further time will be required tobuild up the level and quality of the reporting.As a consequence, it will probably be 2003before a reliable baseline will be established.
It is not suggested that the industry waits untilthe baseline is available before developing animprovement programme. Preliminary actionsto improve occupational health can be initiatedin parallel with the pilot phase of the datacollection activities. However, the delay inknowing what the baseline will be does have animportant consequence for the industry.
One of the RHS targets is for 50% of theimprovement to be achieved halfway throughthe period, that is by 2004. With no existingbaseline, it will be difficult to demonstrate
much measurable progress by 2004. Indeed, itis likely that, during the first couple of years ofgathering data, there will be an increase in theamount of reported occupational health data.This is the final challenge that I want tohighlight for setting the occupational healthtargets; the challenge of communicating whatis being done.
It will be a challenge to communicate theactions being planned by the industry in a waythat makes it clear that real progress is beingachieved despite numbers that may appear tosay the opposite. It may be difficult to explainthat an increase in the reported occupationalhealth data is actually a positive sign of theincreased reporting rather than an indication ofan increasing problem in occupational health.
I think the plans being developed by theoffshore industry provide a sound way forwardto address the RHS challenges but - because ofthe time required to compensate for the initiallack of data and to get a good understanding ofwhat are the real issues and challenges - we aregoing to have to take care to communicate veryclearly: what it is that we are doing; why weare doing it; and why, initially, there may be anincrease in the incidence of occupational healthissues which are reported.
Thank you for your attention.

44
What Challenge?
Targets are set in ‘Revitalising Health andSafety’ and ‘Securing Health Together’e.g. by 2010:
• 30% reduction in the number of working days lost
• 20% reduction in incidence of work related ill-health
The Challenge
• Current reporting requirements inadequate• Lack of data• What indicators to use?
– Observable effects may be years after exposure– Proactive and reactive
• Partnerships to agree and achieve targets• Confidentiality
The Challenge
• Chicken Pox?
The Challenge
• Current reporting requirements inadequate• Lack of data• What indicators to use?
– Observable effects may be years after exposure– Proactive and reactive
• Partnerships to agree and achieve targets• Confidentiality
Industry Response
• OIAC- Step Change workshop 11thJanuary
• OH working group– broad participation
– include NHS and academia
• Step Change to help co-ordinate
Next Steps
• OH working Group– classification codes
– what to use as indicators
– how to measure
– what baseline to use
– what targets to set: proactive and reactive
• Third party administration (?)

45
Timeline
• 5/01 -4/02 Pilot study– classification code– indicators– database and hosting arrangements– communication
• Q1 2002 Evaluate pilot
• Q2 2002 Full implementation– data collection and improvement activities
• 2003 Baseline data
Likely consequences:
• Expect to see increasing numbersduring first year or two– indication of improving data collection
• Unlikely to be able to demonstrate50% of improvement by 2004
Performance Indicators
Characteristics of required indicators:
• Simplicity and clarity
• Relevance
• Amenable to intervention
• Ownership
• Rigour but engage interest
• Proactive as well as reactive

46

47
OFFSHORE SAFETY DIVISION NATIONAL INSPECTIONPROJECTS: FINDINGS AND LESSONS ON OCCUPATIONAL
HEALTH MANAGEMENT IN THE OFFSHORE SECTOR
Dr Ron Gardner, Offshore Safety Division, HSE
Abstract
This paper describes the general reasons for,and aims of the “National Inspection Projects”(NIPs) run by OSD over the past few years.The findings and conclusions are summarisedfrom NIPs on the management and control of:noise, hazardous substances, asbestos,dermatitis, vibration and food hygiene. Thefindings were useful for considering bestpractices and in providing lessons for feedbackto duty holders. The latter can include bothstrengths and weaknesses, so that the formercan be built on and the latter corrected. TheNIPs reveal where the Regulator may need toput more effort, whether by inspection,enforcement, or guidance.
Introduction
HSE’s early experience (Gardner, 1997) of theway occupational health was handled byoffshore duty holders suggested that the sectorwere good at the person orientated aspects ofoccupational health such as fitness for work,provision of first-aid and medic support, andemergency response. However, the assessmentand control of recognised and potential healthrisks in the workplace was less well developedand managed. There are various reasons forthis. For instance, there was a view amongmany managers that “health” was a difficulttopic that should be left to the healthprofessionals. Line managers are also lesslikely to be involved in the investigation ofcases of work-related ill health than they are inworkplace accidents. The fact that work-relatedill health may only appear years after theindividual’s exposure to the causative agent(s),also means that managers are less likely to befaced with the results and costs of ill healtharising from causes in the workplaces theycurrently manage. This latter effect may beexacerbated in the offshore sector by the self-selecting nature of the work and the potential“healthy worker” effect generated by thefitness for offshore work medical requirements(UKOOA, 2000). This latter effect may
account for the low level of failure at returnmedicals (HSE, 1998).
As well as ensuring compliance with healthrelated legislation, the key aims of the HSE inthe North Sea have therefore been to raise theprofile of occupational health in the sector andto improve the assessment and control of healthrisks by line management. NIPs have been oneelement in achieving these aims.
The nature of NIPs
NIPs are focused inspections designed toexamine a specific risk area in some depth.Various types of NIP can be devised, but thosethat have provided the information for thispaper were targeted inspections examining themanagement and control of specific healthrisks using a structured questionnaire. Some ofthese NIPs had two parts: part for applicationat the duty holder’s onshore offices and partfor application on one of their offshoreinstallations. This allowed the application ofcompany wide policies to be tested on selectedinstallations. The questionnaires, whilefocusing inspection effort, were not intended toconstrain the inspector, but provided a probe toopen up the topic as necessary. Because noduty holder preparation was required, specialvisits were not necessary. Hence the NIPs wereapplied during normal preventive inspectionsover a period of one work-planning year.
Since raising the profile of the topic was animportant aim NIPs have rarely been stand-alone initiatives. For instance seminars, orother meetings, on the topic of interest wereheld during the periods over which NIPS ondermatitis, noise and HAV were run, andinitiatives were supported by publications suchas “Sound Solutions Offshore” (HSE, 1998a).
Aims of the NIPs
The principal aims of inspection are toinfluence duty holders to comply with legalprovisions for the health safety and welfare of

48
the workforce, and to encourage them toimprove performance. The aims of individualNIPs varied within this envelope, but the basicaims of all of them were to raise the profile ofthe topic considered and to test compliancewith the appropriate Regulations. In somecases (e.g. the asbestos NIP) an additional aimwas to assist in assessing the potential impactof possible changes to Regulations.
Testing compliance was mainly done byexamining the adequacy of duty holders riskassessments and the controls put in place as aresult of these. In most cases the NIP wasconstructed around the elements of a healthand safety management system using the modelof policy, organising, planning, measuringperformance, and auditing and reviewingperformance as described in HSE’s“Successful Health and Safety Management”(HSE, 1997) and the Oil Industry AdvisoryCommittee publication “Management ofoccupational health risks in the offshore oil andgas industry” (OIAC, 1996).
Topics included in NIPS
The topics covered by the 6 NIPS consideredhere were: noise (1994 - 1995 and again in1999 - 2000), dermatitis (1996 - 1997)asbestos (1996 - 1997), COSHH (1997 -1998), Hand Arm Vibration (HAV) risks (1998- 1999) and food hygiene (1998 - 1999).
Prioritising target topics for NIPs
Various factors were taken into account whendeciding on the target topic for individualNIPs. These included: the nature and extent ofthe hazard; HSE wide campaigns; the need tofollow up compliance with new, or newlyapplied legislation; and general offshoreintelligence from other sources. For a NIP tobe worthwhile several of these factors usuallyneeded to be significant.
Hazard basis for NIPs
There has been a range of reports on thegeneral health of offshore workers (see forinstance HSE 1994; Hahn 1987; HSE 1998;Wiige 1996; Horsley and MacKenzie 1997)and psychological and psychosocial aspects ofoffshore work (Lauridsen et al, 1991; Parkes1998). However, published data on chronicwork-related ill health in offshore workers isscarce. Thus we are not aware of anyepidemiologicaI studies of themortality/morbidity of offshore workers,
though a limited number of upstream workershave been included in some epidemiologicalstudies of refinery workers (Divine and Barron1987; Schnatter et al. 1992; Divine andHartman 2000 and references therein). ANorwegian prospective study of cancer amongoffshore workers has begun, and data from theNorwegian Petroleum Directorate (NPD)(Wiige 1996; NPD 2000) does include someinformation on chronic work-relatedconditions. The findings from the latter arebroadly in-line with onshore findings in the UK(HSC, 2000); thus the main concerns relate tomusculoskeletal diseases and stress.
Most of the available published offshore data(HSE 2000; NPD 2000) relates to acuteaccident events collected through statutoryreporting schemes. Some of theseaccidents/incidents may be the result of, orresult in, chronic conditions, but it is notusually possible to judge this from theavailable reports. Studies of medicalevacuation from offshore installations (Normanet al, 1988; HSE 1999) include diseases aswell as accidents, but it is not necessarily clearwhether or not they are work-related.
In the absence of good risk data the HSE hasapproached the management of health risksoffshore by “reading across” from knownonshore risks (such as those from noise,vibrating tools, asbestos, etc.) and monitoringthe assessment and management of these byoffshore duty holders. This approach ties inwell with the aim of improving occupationalhealth management, but means that the NIPsdiscussed here have been designed to examinequite well established hazards. However, thesecould be regarded as a good test of how wellhealth issues are managed at installation levelon the basis that if well-known hazards are notwell managed then newly emerging issues(such as stress) may be even further behind.
Campaign basis for NIPs
Over the past few years the HSE has run amajor campaign to improve health riskmanagement in the workplace under the banner“Good Health is Good Business” (GHGB).While the general aim of the campaign was toraise the profile of occupational health andimprove its management, specific health riskswere targeted each year. Many of the riskstargeted were important offshore (e.g. noise,HAV, dermatitis, asbestos). The campaigngenerated publicity and guidance that wasgenerally applicable to the offshore situation.

49
Hence it made sense to take the campaignplans into account when planning NIPs.
Compliance basis for NIPs
Although no new health related legislation hasbeen applied offshore for some years, certainexisting onshore Regulations have beenextended to the sector; notably The Control ofSubstances Hazardous to Health Regulationsand The Noise at Work Regulations (NAWR).The need to check how well these wereunderstood and being complied with was afactor in deciding to have NIPs on COSHHand noise. Also, HSE is committed to checkingthe impact of new, or newly applied,legislation, including post-implementationassessment of the costs and benefits. COSHHNIP was thus also designed to collect someinformation on implementation costs.
Intelligence needs
A secondary, but sometimes important, reasonfor choosing a topic for a NIP was the need togather intelligence in that area. An examplewas the NIP on noise where the informationobtained was useful as part of the HSEregulatory impact study before extending thelegislation offshore.
Other intelligence as a basis for NIPs
Intelligence from a range of sources alsosuggested that some topics justified closerinspection. An example was feedback frominspections which suggested that the riskassessment and control of vibration from handtools needed improving Another example wasour understanding of the views of offshoreoccupational health professionals in relation tonoise on offshore installations.
Findings
Tables 1 (Annex 1) summarises the findingsfrom the dermatitis, asbestos, COSHH andfood hygiene NIPs, while Table 2 (Annex1)summarises those from the noise and HAVNIPs.
Findings and conclusions from individualNIPs
The findings from the NIPs were very detailed,so only selected points and the mainconclusions are given below.
Dermatitis
Relatively few companies had specific policieson dermatitis, but over 70% of respondentscarried out assessments that included dermatitisrisk. However, these were often hazardassessments using the Material Safety DataSheets (MSDSs) as a prompt for the use ofPPE. In fact all the companies questioned usedPPE as the main, or only method of controllingskin exposures. There were few examples ofother methods such as substitution and betterhousekeeping.
Risks to the skin from hazardous substanceswere generally included in COSHHassessments, however, this meant that the issuewas rarely addressed in detail.
Barrier creams were in widespread use andaround 50% of the companies had unwrittenobjectives concerning them. No otherobjectives or targets relating to dermatitis werenoted. In some cases barrier creams appearedto be regarded as PPE.
About half the companies said that they usedsolvents or abrasives for hand cleaning. Thisappears to have been a misunderstanding, butsome companies were using theseinappropriate methods
Employees were comfortable to go to medicsfor advice and treatment of skin problems, butthe level of formal reporting to the regulatordid not reflect the number of visits to themedics. (Note: this was before the applicationof RIDDOR offshore).
Training and awareness of employees to skindisorders was on an ad-hoc basis.
Conclusionsa) Companies that had carried out specific
skin related risk assessments had benefitedby developing more effective methods toprevent and control the risk.
b) Duty holders needed to consider riskreduction methods other than PPE such assubstitution, closed systems, mechanicalaids and better housekeeping).
c) The use of barrier creams required carefulmonitoring since, in some cases, they wereregarded as a form of PPE hence giving afalse sense of security.
d) Work-related dermatitis seems to occurmore often than it is reported to theRegulator.

50
Asbestos
Findings
82% of companies questioned said that theystill have asbestos on one or more of theirinstallations. This was most commonlyChrysotile (white asbestos) but Amosite(brown asbestos) and Crocidolite (blueasbestos) were also widespread. Uses current atthe time of the NIP included lagging (35%),ceiling tiles (35%), insulation boards ( 41%)and in items such as compressed asbestos fibre(CAF) gaskets, acoustic hoods, and brake andclutch linings.
All but one of the companies had some sort ofpolicy on asbestos and 82% had policies onasbestos substitution or were in the process ofproducing them. Only 18% of the companieshad set specific objectives in relation toasbestos, but this lack of objectives had to beset against the fact that all the companieshaving asbestos on an their installationsreported some action. 41% had programmesfor removal of all asbestos on theirInstallations or selective removal where thiswas considered necessary.
External consultants had been, or were being,used to carry out full or part surveys on 71% ofthe Installations. In only 36% of the reportswas the condition of the asbestos noted andmost of the reports lacked recommendations.Most survey work seems to be triggered byfinding suspect areas or word of mouth reportsabout asbestos.
Just over half (55%) of the installations hadlabeled asbestos containing materials.
Most installations had no one trained in what todo if asbestos was damaged. However,awareness of asbestos hazards amongemployees offshore was quite high and concernlow. But they were often not aware of itspresence except when planned work onasbestos was going on.
Conclusions
a) It was likely that even if they are not awareof it most offshore companies will haveasbestos on some of their installations,albeit in low hazard forms (e.g. brake andclutch linings).
b) Asbestos was still present in structuralfeatures (e.g. ceiling tiles and wall boards)on some mobile installations were there
was a belief that the installation had beenstripped some years before Management ofasbestos seemed to be largely a reactiveprocess.
c) Few companies (24%) had ongoingprogrammes to survey and maintainasbestos on their installations. It is vitalwhen surveys are done that the condition ofany asbestos found is noted and acted on.
d) The number of companies saying that theyhave made use of their Own expertise(71%) for information on measures tocontrol asbestos was high compared withthe number saying that say they had madeasbestos assessments (47%). It is likely thatthis reflected expertise being used only onan ad hoc basis (e.g. when asbestos isfound or suspected during ongoing work).
Control of Hazardous substances
Findings
All companies had a system in place toimplement COSHH requirements, includingsome form of audit and review, or (in one case)were in the process of planning a system ofaudit and review. The majority (52%) ofcompanies used COSHH re-assessments, orgeneral HS&E audits, to trigger the reviewprocedure All the companies had also carriedout COSHH assessments, but, the quality ofassessments was patchy with some beinghazard assessments based on information in theMSDSs rather than risk assessment of theprocess using or producing the hazardoussubstance.
It was common for companies to appointsomeone to “be responsible for” COSHH.However, they often had a range of otherresponsibilities to handle as well.
The most common activities assessed wererelated to drilling (e.g. mixing mud chemicalsand related activities, work on the drill floor orin shaker houses and cleaning mud pits) andgeneral workplace maintenance processes (e.g.painting; welding and cleaning.
A range of controls were reported as havingbeen introduced post COSHH, suggesting thatthe Regulations had considerable impact.Outside consultants were widely used andgenerally thought to provide value for money.However, the information provided on costswas surprisingly sparse and were obviouslyloose estimates. For instance, the provision ofLEV was generally considered to be expensive,

51
but quoted costs ranged from £50,000 per rigto £500,000 on one installation, though thelatter included some improvements to thegeneral ventilation.
Eight companies had introduced newmaintenance records as a result of the COSHHassessments, but some others had not addednew LEV to their maintenance regimes.
Some reported benefits of introducing COSHHincluded more efficient use of chemicals andreduction in stocks (up to 30% in one case).Also, 19% of the companies reported a reducednumber of chemical incidents.
Some companies had introduced new healthsurveillance, because of COSHH This rangedfrom simply monitoring the medic's log toperiodic skin checks and 6 monthly lungfunction tests. However, there was muchconfusion in this area with many companiesinterpreting periodic offshore medicals asbeing appropriate health surveillance.
Conclusions
a) There have been significant improvementsas a result of COSHH being appliedoffshore but this is patchy. Overall thepicture presented by the survey may be bestsummarised by inspectors’ opinions. Nocompany presented an 'exemplary'assessment, six were considered'satisfactory' and all the others requiredsome rectification.
b) The responsibility for implementingCOSHH onshore and offshore is one of anumber of responsibilities within staffportfolios, and this dilutes the effort givento COSHH.
c) There were areas where improvement wasrequired, particularly related to the standardof assessments (which were occasionallyonly hazard based) and the quality andunderstanding of health surveillance.
Food Hygiene
Findings
All but one of the catering companies had welldeveloped food safety management systems(FSMSs) covering policy, aims and objectives,risk assessment - in this case HACCP (hazardand critical control point) assessments,organisation, performance measures and auditsystems. The only exception was a non-UK
based company which was the subject ofenforcement.
The problems noted were at thecontractor/client interface. Examples included:a lack of clarity over who had whatresponsibilities in emergencies such as anoutbreak of food poisoning; maintenance ofgalley equipment not being seen as a priorityby clients; and lack of client facilitation ingetting catering company managers offshore tocarry out audits, even when the clients requiredthese.Economic pressures could also lead to areduction in manning levels in hotel/cateringstaff on some installations. This was a cause ofpotential stress and a reduction in foodhygiene. Another effect of this was a growinguse of stewards as food handlers. While theirtraining was good, this was not ideal because itpotentially introduced a new risk of crosscontamination.
Since temperature control regimens are vitallyimportant to good food hygiene this wasspecifically targeted in the NIP as a “marker”.In general temperature controls were goodthough, though a range of relatively minorfaults were noted on different installations.Examples included questions in individualcases on: the effectiveness of the methods usedto clean thermometer probes between uses; thecalibration of temperature probes and theprovision of a back-up; and the effectiveness ofchecking the acceptability of incoming food.
Conclusions
a) The FSMSs and HACCPs put in place bythe catering companies were, with a singlenon-UK exception, very good.
b) There were some problems of under-staffing (often cost based) that couldpotentially result in stress among cateringstaff and a reduction in food hygiene.
c) Most problems arose at the interfacebetween contractor and client SafetyManagement Systems (e.g. difficulties inmaintaining galley equipment and in gettingSenior managers from catering offshore tocarry out necessary audits).
d) Temperature control (a critical element offood hygiene) was generally well addressedwith only relatively minor and scatteredfaults being found.

52
Noise
Findings
Perhaps the most interesting findings relate tothe two noise NIPs.
The first NIP (1994 – 1995) was carried outbefore the NAWR were applied offshore andmost of the organisation on noise mattersrelated to the requirements of the thenCertifying Authorities (CAs). So at that timeonly about a third of the installations coveredby the NIP had a policy specificallymentioning noise, but virtually all of them hadregular surveys of area noise levels by the CAs.Also, half of them had other area surveysbeyond the CAs requirements. The CAsgenerally used the area noise level standardsgiven in Den/HSE guidance on design,construction and certification of offshoreinstallations (DEN/HSE, 1990), but CArecommendations often seem to have beenrepeated over several years with little apparentaction. Most companies were also using theaction levels of the then onshore NAWR withthe area noise surveys to identify areas wherehearing protection had to be worn.
As might have been predicted, there were somemarked differences between these pre- NAWRfindings and the post-application of the NAWRoffshore.
Given that the NIP was carried out only 2 yearafter the NAWR was applied offshore therewere some very positive findings. Theseincluded: the percentage of duty holders withpolicies and procedures on noise had doubledand others were developing; all but one hadcompleted noise assessments and includedexposure assessments; around 20% hadidentified further potential noise controlmeasures; and some had targets for assessmentand training. It was also evident that workforceawareness was higher than before.
Some 65 % had appointed a “Responsibleperson” for noise matters, but this person wasnot necessarily a “Competent person” andoften had limited authority.
Rather disappointing was the fact that the basiccontrol measure was still delineation of hazardareas based on the action levels in the NAWRand the provision of PPE and a lack ofrecognition of the need under NAWR to reducenoise exposure as low as reasonablypracticable. There was also much dependence
on the periodic UKOOA medicals for fitness towork offshore to provide audiometry. Thiscould be building problems for the future sincehearing damage by noise is usually most at anearly age i.e. at the time when the periodicmedicals are furthest apart.
Conclusions
The general conclusion to the 1994- 1995Noise NIP was that: “Three quarters of thereports indicated a need for the operator to takefurther action. A wide range of topics wasnoted, of which dose assessment and control ofnoise at source were prominent.”
The overall conclusions from the 1999 – 20001NIP on noise were:
a) Compliance with the Noise at WorkRegulations can be improved
b) Duty holders should improve theirmanagement of noise risks
c) Better ALARP demonstrations should bedemanded by inspectors
d) Duty holder s should have better systemsfor providing education and information totheir employees
HAV
Findings and conclusions
Early in the NIP it became apparent thatalthough c 30% of the companies had somepolicy/assessment on HAV, little exposureassessment had been done, few controls put inplace and little training given. Interestingly,c25% of the companies had some healthsurveillance in place, suggesting that healthprofessionals were aware of the problem butthat it had not become a matter for linemanagement.
Only 15% of respondents said they had seen atleast one of HSE’s publications.
The situation was such that of the 19companies investigated inspectors judged that15 had made little or no attempt to comply withthe applicable legislation. Over the course ofthe NIP a meeting was held with industryrepresentatives and the situation improvedmarkedly. By the end of the year systems to

53
assess the risks (including measuring orotherwise assessing the vibration levels ofequipment), purchasing new lower vibrationtools and controls (e.g. limiting and recordingthe time spent using vibrating tools) werebecoming widespread. The effects of theseinitiatives are the subjects of other papers forthis conference.
A somewhat unexpected conclusion was thatthe use of hand held vibrating tools was muchmore widespread than had been thought beforethe survey. Among the companies surveyed,which included contractors, about 1800workers were reported as using hand heldvibrating equipment. Scaling this up across thesector would suggest 2000-3000 workers areregularly exposed to the risk of HAV. Themost frequently used equipment known to havehigh vibration levels were grinders, needleguns, impact wrenches, air drills and chippinghammers. Also reported in use less were,nibblers, scrabblers, air drills, jigsaws, a floorpolishing machine and an engraving pen.
Discussion
In considering the findings from NIPs we needto bear in mind the nature of the exercise.
1 The NIPs described were not statisticallybased surveys designed to provide scientificdata. The cover achieved was, however,reasonable, with returns in the range of c 28- 40% of duty holders and c 10 - 19% ofmanned installations. (In the case of thefood hygiene NIP all the then extantcatering companies were included and thenumber of occasions when the NIP wasapplied to each of them was proportionateto the scale of their presence in the NorthSea.)
2 The NIPs are a snapshot of an ongoingprocess - stills from a moving picture.Hence some of the findings were alreadybecoming out of date by the end of the yearthe individual NIPs were applied in - thiswas particularly the case with HAV. Indeedthe NIPs, with other activities, contributedto the process of change, for example theyoften led to companies re-examining theway they approached the topic beingexamined and on several occasions toformal enforcement activity on the part ofinspectors.
3 Except in the case of the two NIPs on noisethere was nothing to compare the findings
with - they are simply stand-alone results.The findings do, however, provide abenchmark for future follow up.
Even with these provisos some general trendscan be discerned.
1 A number of the findings would suggestthat the more specific (if not prescriptive)the legislation the better the assessment andcontrol. This is best illustrated bycomparing the extreme cases of foodhygiene and HAV. In the former thedetailed onshore legislation does not applyoffshore, but is used as the standard forenforcing offshore provisions; in the caseof HAV only the general provisions of theHealth and Safety at Work Act 1974 andthe Management of Health and Safety atWork Regulations 1999 apply andassessment and control regimes were notwell developed. Comparison of thesituation before and after the application ofthe Noise at Work Regulations offshorehighlights the same point.
2 There were few targets or objectives set onhealth matters at the installation level andfew specific performance measures inrelation to the topics covered.
3 There was considerable confusion abouthealth surveillance with many duty holdersquoting the annual offshore medicals astheir health surveillance. This is unlikely tobe satisfactory for conditions such asdermatitis that can develop rapidly or forthe early detection of hearing loss inyounger workers.
4 It was evident that there was still someconfusion between hazard and risk as abasis for COSHH assessments. Exampleswere the existence of some substance basedCOSHH assessments (essentially using theMSDS without reference to the way thematerial was used) and the fact that mostinspectors thought that one of the strongestelements of the way duty holders handledCOSHH was in the computerisation of data.
5 The NIPs suggest a quite heavy reliance onPPE for control - particularly with respectto hazardous substances (including skinprotection) and noise. General inspectionexperience supports this. Many exposuresoffshore are of short duration and PPE maybe a quite satisfactory method of control.However, PPE use can lead to a false sense

54
of security - after all the cause of the risk isstill there. An extreme example, notedduring the NIP on dermatitis, was the use ofbarrier creams as if they were PPE.
6 Some of HSE guidance had not reallypenetrated – for instance there seemed to belittle awareness of HSE guidance on HAV.
Conclusion
The NIPs have provided good intelligence forinspection purposes in highlightingdeficiencies in the management of varioushealth issues and provide a benchmark forfuture comparisons.
At the 1996 Offshore Occupational HealthConference a number of speakers commentedon the “Cinderella status” of the topiccompared with safety (HSE 1997a). With otherinformation (e.g. from general inspection) thefindings from the NIPs suggest that this ischanging and that the management ofoccupational health matters at installation levelhas improved in the last five years. The targetsgiven in the recently published long-termoccupational health strategy for England,Scotland and Wales (HSC 2000a) shouldprovide further impetus for improvement.
References
Den/HSE 1990 “Offshore Installations:Guidance on design, construction andcertification” Fourth Edition, HMSO.
Divine, B.J., and Barron, V. 1987 "Texacomortality study III. A cohort study ofproducing and pipeline workers",Am.J.Ind.Med. 10, 371-381.
Divine, B.J., and Hartman, C. M. 2000"”Update of a study of crude oilWorkers 1946 - 1994", Occup. Environ. Med.57, 411- 417.
Gardner, R. J., 1997 “ Occupational Health:OSD’s Inspection Experience”, Proceedings ofthe Occupational Health Offshore Conference:Aberdeen 26 - 28 March 1996, HSE OffshoreTechnology Report OTH 531 pp 35 – 40 HSEBooks, 35 (ISBN 0-7176-1423-9).
Hahn, M., J., 1987 The dental status ofworkers on offshore installations in the UK oiland gas industry”, Br. Dental. J., 163 262.
Horsley, H., and MacKenzie, I. G., 1997“Lifestyle Survey Amongst North Sea OilWorkers”, Proceedings of the OccupationalHealth Offshore Conference: Aberdeen 26 - 28March 1996, HSE Offshore TechnologyReport, HSE Books, p161 (ISBN 0 - 7176 -1423 - 9).
HSC 2000 “Health and Safety Statistics1999/2000” HSE Books (ISBN 0 – 7176 –1867 – 6).
HSC 2000a “Securing Health Together. Along-term occupational health strategy forEngland, Scotland and Wales. HSE BooksMISC 225.
HSE 1994 “Diet, Health and the OffshoreWorker”, HSE Offshore Technology ReportOTH 93 399.
HSE 1997 “Successful Health and SafetyManagement” HSG65, HSE Books (ISBN 0 -7176 - 1276 - 7).
HSE 1997a “Proceedings of the OccupationalHealth Offshore Conference: Aberdeen 26 - 28March 1996”, HSE Offshore TechnologyReport OTH 531 (ISBN 0 - 7 176 - 1423 - 9).
HSE 1998 “Medical Status of the OffshorePopulation” Offshore Technology Report OTO97 057.
HSE 1998a “Sound Solutions Offshore:practical examples of noise reduction”,HSG182, HSE Books, (1998) (ISBN 0 - 7176 -1581 - 2).
HSE 1999 “Study of medical evacuations fromoffshore installations Five year report 1987 -1992” HSE Offshore Technology Report OTO098 171.
HSE 2000 “Offshore Injury, Ill health andIncident Statistics Report 1999/2000” HSEOffshore Technology Report OTO 2000 111.
HSC 2000 “Health and Safety Statistics1999/2000” HSE Books (ISBN 0 - 7176 -1867 - 6).
Lauridsen, O., et al, 1991 “Shift-work andhealth: Shift-work, sleeping difficulties,psychosocial work environment andpsychosomatic complaints”, Report RF 127/91,Phillips Petroleum Company, Norway and theRogaland Research Institute, Norway (1991).

55
Norman, J. N., et al, 1988 “Medicalevacuations from offshore structures”, Br. J.Ind. Med., 45, 619-623.
NPD 2000 “Norwegian Petroleum DirectorateAnnual Report”, NPD.
OIAC, 1996 “Management of occupationalhealth risks in the offshore oil and gasindustry”, Oil Industry Advisory Committee,HSE Books (ISBN 0 - 7176 - 0886 -7).
Parkes, K.R., 1998 “Psychosocial aspects ofstress, health and safety in North Seainstallations”, Scand. J Work Environ Health,24(5) 321.
Schnatter, A.R., Thériault, G., Katz, A.M.,Thompson, F.S., Donaleski, D and Murray,(1992) "A Retrospective Mortality Studywithin Operating Segments of a PetroleumCompany". Amer.Jnl. Ind.Med., 22, 209-229.
Wiige, H., 1996 “Frequency of work-relateddiseases - an indictor of working environmentstandard”, Proceedings of the thirdinternational conference on Health, Safety andthe Environment in oil and gas Production,New Orleans, 303.
UKOOA 2000 “Guidelines for MedicalAspects of Fitness for Offshore Work” IssueNo. 4, January 2000, United KingdomOffshore Operators Association.

56

Tab
le 1
: S
um
mary
of
fin
din
gs
fro
m c
hem
ical
an
d f
oo
d r
ela
ted
NIP
SIt
emD
erm
atiti
s(1
996
- 19
97)
Asb
esto
s(1
996
– 19
97)
CO
SHH
(199
7 –
1998
)Fo
od H
ygie
ne(1
998
- 19
99)
Num
ber
of r
epor
ts r
ecei
ved.
33 (
22 d
rilli
ng r
igs;
11 p
rodu
ctio
n pl
atfo
rms)
21 (
17 d
iffe
rent
dut
y ho
lder
s)19
(17
dif
fere
nt d
uty
hold
ers)
31 (
7 ca
teri
ng c
ompa
nies
and
24 c
lient
s)Po
licy
and
orga
nisa
tion
(ons
hore
)O
nly
1 ha
d a
spec
ific
wri
tten
polic
y.15
% b
elie
ved
skin
issu
es w
ere
cove
red
by th
eir
gene
ral p
olic
y
18%
had
a p
olic
y of
som
e so
rt
53%
had
pol
icie
s on
subs
titut
ion.
86%
had
a C
OSH
H p
olic
y A
llha
d an
im
plem
enta
tion
syst
emin
pla
ce.
Onl
y on
e no
n-U
K b
ased
com
pany
did
n’t h
ave
a w
ell-
deve
lope
d fo
od s
afet
ym
anag
emen
t sys
tem
cov
erin
gpo
licy,
aim
s, o
bjec
tives
etc
. and
syst
ems
to im
plem
ent i
t.R
isk
asse
ssm
ent
-
gene
ral
(ins
talla
tion
basi
s)G
ener
ally
incl
uded
in C
OSH
Has
sess
men
t - to
a g
reat
er o
rle
sser
leve
l of
effe
ctiv
enes
s
57%
had
sur
veye
d fo
r as
best
osbu
t on
ly 3
6% r
epor
ted
on t
heco
nditi
on
All
had
som
e fo
rm
ofas
sess
men
t; th
e qu
ality
va
ried
and
som
e w
ere
haza
rd b
ased
All
exce
pt th
e no
n-U
Kco
mpa
ny h
ad p
erfo
rmed
HA
CC
Ps a
s re
quir
ed.
Ass
essm
ent o
f ex
posu
re(i
nsta
llatio
n ba
sis)
If a
t al
l it
was
in
the
CO
SHH
asse
ssm
ent.
A f
ew a
tmos
pher
icm
onito
ring
sur
veys
had
been
don
e.
75%
had
per
form
ed s
ome
atm
osph
eric
mon
itori
ng(b
enze
ne, o
il m
ists
, wel
ding
,dr
illin
g ch
emic
als
(dus
t))
Not
app
licab
le
Ass
esso
rs u
sed
(ins
talla
tion
basi
s)In
hou
se o
r co
nsul
tant
s fo
rC
OSH
HM
ainl
y co
nsul
tant
sIn
hou
se o
r co
nsul
tant
sIn
hou
se
Con
trol
s(i
nsta
llatio
n ba
sis)
All
relie
d on
PPE
as
the
only
or
maj
or c
ontr
ol m
etho
d fo
r sk
inex
posu
re
with
ba
rrie
r cr
eam
san
d pr
e-po
st
wor
k cr
eam
s as
adju
ncts
. So
me
subs
titut
ion
and
use
of m
echa
nica
l sy
stem
s w
asno
ted
50%
had
pro
gram
mes
for
asbe
stos
rem
oval
;53
% h
ad p
olic
ies
onsu
bstit
utio
n50
% h
ad la
bele
d kn
own
site
s of
asbe
stos
.54
% h
ad s
eale
d so
me
asbe
stos
Men
tione
d as
a r
esul
t of
CO
SHH
wer
e Su
bstit
utio
n (1
3),
elim
inat
ion
(11)
, mod
ifie
dpr
oced
ures
(11
), L
EV
(10
),im
prov
ed g
ener
al v
entil
atio
n(8
) im
prov
ed P
PE (
10)
othe
rPP
E (
8)
Tem
pera
ture
con
trol
reg
imes
wer
e sp
ecif
ical
ly e
xplo
red.
The
se w
ere
wel
l dev
elop
ed a
ndm
onito
red
by a
ll th
e ca
tere
rs.
Mon
itori
ng,
audi
t an
d re
view
(ins
talla
tion
basi
s)N
ot e
xam
ined
Not
exa
min
edV
irtu
ally
al
l ha
d au
dit
and
revi
ew s
yste
ms
of s
ome
sort
.A
ll ha
d pe
riod
ic a
uditi
ng b
ysh
ore-
base
d m
anag
emen
t and
mos
t had
per
iodi
c O
IM m
edic
wal
k-th
roug
h in
spec
tions
. Som
eal
so h
ad c
lient
or
cons
ulta
ntau
dits
.
57
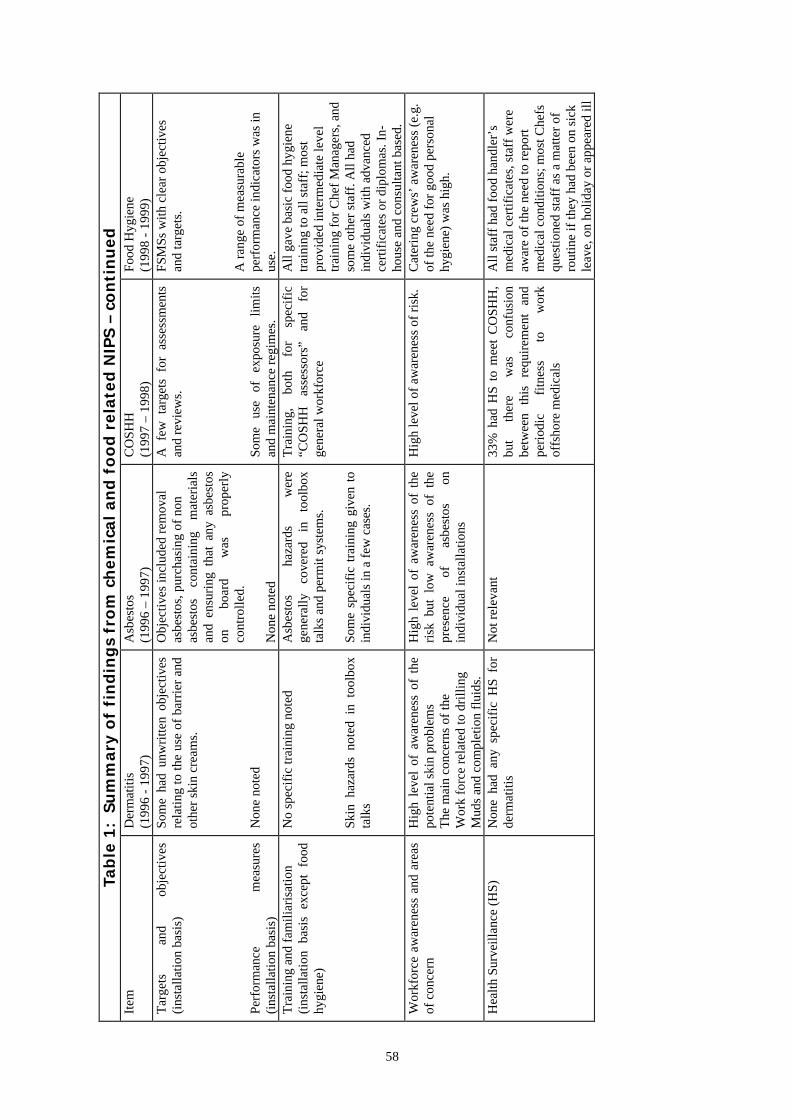
Tab
le 1
: S
um
mary
of
fin
din
gs
fro
m c
hem
ical
an
d f
oo
d r
ela
ted
NIP
S –
co
nti
nu
ed
Item
Der
mat
itis
(199
6 -
1997
)A
sbes
tos
(199
6 –
1997
)C
OSH
H(1
997
– 19
98)
Food
Hyg
iene
(199
8 -
1999
)T
arge
ts
and
obje
ctiv
es(i
nsta
llatio
n ba
sis)
Perf
orm
ance
m
easu
res
(ins
talla
tion
basi
s)
Som
e ha
d un
wri
tten
obje
ctiv
esre
latin
g to
the
use
of b
arri
er a
ndot
her
skin
cre
ams.
Non
e no
ted
Obj
ectiv
es in
clud
ed r
emov
alas
best
os, p
urch
asin
g of
non
asbe
stos
co
ntai
ning
m
ater
ials
and
ensu
ring
tha
t an
y as
best
oson
bo
ard
was
pr
oper
lyco
ntro
lled.
Non
e no
ted
A f
ew t
arge
ts f
or a
sses
smen
tsan
d re
view
s.
Som
e us
e of
ex
posu
re
limits
and
mai
nten
ance
reg
imes
.
FSM
Ss w
ith c
lear
obj
ectiv
esan
d ta
rget
s.
A r
ange
of
mea
sura
ble
perf
orm
ance
indi
cato
rs w
as in
use.
Tra
inin
g an
d fa
mili
aris
atio
n(i
nsta
llatio
n ba
sis
exce
pt f
ood
hygi
ene)
No
spec
ific
trai
ning
not
ed
Skin
haz
ards
not
ed i
n to
olbo
xta
lks
Asb
esto
s ha
zard
s w
ere
gene
rally
co
vere
d in
to
olbo
xta
lks
and
perm
it sy
stem
s.
Som
e sp
ecif
ic t
rain
ing
give
n to
indi
vidu
als
in a
few
cas
es.
Tra
inin
g,
both
fo
r sp
ecif
ic“C
OSH
H
asse
ssor
s”
and
for
gene
ral w
orkf
orce
All
gave
bas
ic f
ood
hygi
ene
trai
ning
to a
ll st
aff;
mos
tpr
ovid
ed in
term
edia
te le
vel
trai
ning
for
Che
f M
anag
ers,
and
som
e ot
her
staf
f. A
ll ha
din
divi
dual
s w
ith a
dvan
ced
cert
ific
ates
or
dipl
omas
. In-
hous
e an
d co
nsul
tant
bas
ed.
Wor
kfor
ce a
war
enes
s an
d ar
eas
of c
once
rnH
igh
leve
l of
aw
aren
ess
of t
hepo
tent
ial s
kin
prob
lem
sT
he m
ain
conc
erns
of
the
Wor
k fo
rce
rela
ted
to d
rilli
ngM
uds
and
com
plet
ion
flui
ds.
Hig
h le
vel
of a
war
enes
s of
the
risk
but
low
aw
aren
ess
of t
hepr
esen
ce
of
asbe
stos
on
indi
vidu
al in
stal
latio
ns
Hig
h le
vel o
f aw
aren
ess
of r
isk.
Cat
erin
g cr
ews’
aw
aren
ess
(e.g
.of
the
need
for
goo
d pe
rson
alhy
gien
e) w
as h
igh.
Hea
lth S
urve
illan
ce (
HS)
Non
e ha
d an
y sp
ecif
ic H
S fo
rde
rmat
itis
Not
rel
evan
t33
% h
ad H
S to
mee
t C
OSH
H,
but
ther
e w
as
conf
usio
nbe
twee
n th
is
requ
irem
ent
and
peri
odic
fi
tnes
s to
w
ork
offs
hore
med
ical
s
All
staf
f ha
d fo
od h
andl
er’s
med
ical
cer
tific
ates
, sta
ff w
ere
awar
e of
the
need
to r
epor
tm
edic
al c
ondi
tions
; mos
t Che
fsqu
estio
ned
staf
f as
a m
atte
r of
rout
ine
if th
ey h
ad b
een
on s
ick
leav
e, o
n ho
liday
or
appe
ared
ill
58

Tab
le 2
: S
um
mary
of
fin
din
gs
fro
m N
IPs
on
No
ise a
nd
HA
VIt
emN
oise
(19
94-1
995)
Noi
se (
1999
-200
0)H
AV
(19
98-1
999)
Num
ber
of r
epor
ts16
2019
(25
com
pani
es)
Polic
y an
d O
rgan
isat
ion
c33%
had
pol
icy
spec
ific
ally
men
tioni
ngno
ise
Som
e ha
d al
loca
ted
PPE
res
pons
ibili
ties.
c65%
had
a p
olic
yc6
5% h
ad a
ppoi
nted
som
eone
to “
deal
with
noi
se”
(the
trai
ning
and
exp
erie
nce
of th
is in
divi
dual
was
oft
en n
otsu
ffic
ient
)
c30%
had
a f
orm
al p
olic
y or
pro
cedu
refo
r as
sess
ing
risk
.c6
6% h
ad a
lloca
ted
resp
onsi
bilit
y fo
rH
AV
ris
k to
som
eone
Ris
k as
sess
men
t – g
ener
alN
earl
y al
l had
CA
are
a su
rvey
s ; c
50%
had
othe
r ar
ea s
urve
ysA
ll bu
t one
had
com
plet
ed a
noi
seas
sess
men
t as
requ
ired
by
the
Noi
se a
tw
ork
Reg
ulat
ions
c30%
had
a f
orm
al p
olic
y or
pro
cedu
refo
r as
sess
ing
risk
.
Ass
essm
ent o
f ex
posu
rec3
3% c
onsi
dere
d no
ise
dose
All
but o
ne h
ad in
clud
ed e
xpos
ure
asse
ssm
ents
;15
% h
ad s
ome
dosi
met
ry
Vir
tual
ly n
o as
sess
men
t at t
he ti
me
the
NIP
beg
an (
see
text
)1
resp
onde
nt h
ad c
arri
ed o
ut v
ibra
tion
mea
sure
men
tsA
sses
sors
CA
s an
d ot
her
cons
ulta
nts
Con
sulta
nts
-C
rite
ria
for
appl
ying
con
trol
sT
he a
ctio
n le
vels
in th
e (o
nsho
re)
Noi
seat
Wor
k R
egul
atio
ns a
nd th
e ar
ea li
mits
reco
mm
ende
d in
the
Den
/HSE
4th
editi
on
Act
ion
leve
ls f
rom
the
Noi
se a
t Wor
kR
egul
atio
ns.
EE
C D
irec
tive
and
HSE
gui
danc
e.
Con
trol
mea
sure
sH
azar
d ar
ea id
entif
icat
ion
(bas
ed o
nac
tion
leve
ls)
and
PPE
Enc
losu
re o
f so
me
equi
pmen
t (e.
g. w
ater
pum
ps)
was
com
mon
but
sim
ilar
cont
rols
wer
e no
t com
mon
ly u
sed
else
whe
re
Con
trol
s w
ere
still
set
in te
rms
of th
eac
tion
leve
ls w
ith h
azar
d ar
eas
and
use
of P
PE r
athe
r th
an r
educ
ing
nois
eA
LA
RP.
c20%
iden
tifie
d po
tent
ial n
oise
con
trol
mea
sure
s.
Ess
entia
lly n
one
had
addr
esse
d co
ntro
lto
mee
t the
rec
omm
ende
d le
vels
.
59

Tab
le 2
(C
on
tin
ued
) :
Su
mm
ary
of
fin
din
gs
fro
m N
IPs
on
No
ise a
nd
HA
VIt
emN
oise
(19
94-1
995)
Noi
se (
1999
-200
0)H
AV
(19
98-1
999)
Obj
ectiv
es a
nd ta
rget
s1
had
risk
-rel
ated
targ
ets
and
obje
ctiv
esSo
me
had
targ
ets
for
asse
ssm
ent a
ndtr
aini
ngM
any
(esp
ecia
lly c
ontr
acto
rs)
had
plan
sto
ass
ess
vibr
atio
n ou
tput
s by
mea
sure
men
t or
com
para
tive
tech
niqu
es.
Mon
itori
ng a
udit
and
revi
ew75
% h
ad s
ome
syst
ems
in p
lace
but
thes
e m
ainl
y re
late
d to
CA
rev
iew
and
PP
E
Not
cov
ered
in th
e N
IPN
one
Tra
inin
gc7
5% h
ad tr
aini
ng o
f so
me
sort
c50%
com
plie
d w
ith th
e re
quir
emen
ts o
fth
e N
oise
at w
ork
regu
latio
ns; o
ther
s ha
dpr
ogra
mm
es in
dev
elop
men
t.
Ver
y lit
tle s
peci
fic
trai
ning
- a
t the
tim
eof
the
surv
ey o
nly
one
com
pany
had
any
sort
of
cam
paig
n (p
oste
r an
d vi
deo)
.W
orkf
orce
aw
aren
ess
and
invo
lvem
ent
The
re w
as a
rea
sona
ble
leve
l of
awar
enes
s of
noi
se h
azar
ds a
nd th
e ne
edfo
r PP
Ec4
0%of
the
repo
rts
sugg
este
d so
me
wor
kfor
ce c
once
rn a
bout
noi
se (
PPE
,he
li-de
ck n
oise
and
nui
sanc
e)
Aw
aren
ess
was
hig
h, b
utm
ost c
once
rns
rela
ted
to n
uisa
nce
nois
e(e
.g. n
oise
in c
abin
s ga
lley,
sic
kbay
)
Not
exa
min
ed
Hea
lth S
urve
illan
cec3
3% o
ffer
ed a
udio
met
ry b
eyon
d th
at in
the
fitn
ess
for
wor
k of
fsho
re m
edic
als.
Situ
atio
n re
mai
ned
muc
h th
e sa
me;
som
eri
sk b
ased
vie
w, s
o if
a m
edic
al s
how
edev
iden
ce o
f an
y si
gnif
ican
t or
unus
ual
hear
ing
loss
the
mon
itori
ng f
requ
ency
was
incr
ease
d.
25%
had
som
e su
rvei
llanc
e fo
r H
AV
sym
ptom
sO
ther
s w
ere
putti
ng s
yste
ms
in p
lace
.
60

61
HEALTH PLANNING TOOL FOR OCCUPATIONAL HEALTHASSURANCE
Mr Lindsay Ross, Occupational Hygiene Co-ordinator, BPExploration
Abstract
BP commitment to Health, Safety andEnvironment (HSE) performance is simplystated:
No accidents;No harm to people;No damage to the environment.
Everyone who works for BP anywhere isresponsible for getting HSE right and BP’sbusiness plans include measurable HSE targets.Therefore where ever BP operates or wheneverit enters into new and different ventures andcountries; management systems forimplementing the relevant HSE programmes,procedures and legislative requirements shouldbe either already in place or being initiated.
Normally, of the three HSE elements, ‘Health’is the least well understood and resourced, andis therefore given the least attention. To helpensure that health aspects in BP Exploration(BPX) are initially identified, easilyunderstood and then addressed in an ongoingand suitable, sufficient and timely manner, aHealth Planning process has been developed.
The concept of health planning is important forthree reasons:
• It is based on examined practice;• It is an effective way of managing the
business issues of health;• It shares a common language with that of
safety.
The Health Planning Resource Pack (BP) wasdeveloped as a practical tool for implementinghealth planning. It also works well as amarketing vehicle or device to raise the profileof health as a business performance issue.Each pack contains an overview of the healthplanning process and offers a number of toolsto assist Business Units (BU’s) in constructingtheir own specific health plan. The principalplanning tool is a Generic Planning Matrix or
table designed to capture the main elements ofan occupational health managementprogramme, to set out clear expectations andoutcomes to improve health auditing and assistin identifying key performance measures. Thegeneric table is modified to reflect the needs ofeach business unit and it then becomes the BUSpecific Planning Matrix, which is used by thesite health planning team to develop theirneeds on a three year rolling timeline.
In addition, seven specialist appendicesranging from Occupational Hygiene to StressManagement have also been prepared asfurther guidance. The pack also contains anintroductory brochure, several health planninggraphics, an outline of a health planningseminar or workshop and reference materials.
Introduction
Safe and efficient operations depend on peopleand BP attempts to operate its facilities in away that minimises health risks to employees,contractors and the community, andencourages people to adopt a healthy lifestyle.Thus enhancing operations integrity, BP’sreputation and productivity, and establishing afirm foundation for growth. Healthencompasses a spectrum of states ranging fromextremes of premature death to optimumhealth. Preventing work related ill health is arecognised management responsibility and isspecifically stated in the Company HSECommitment of “No Harm to People....”.There is also potential to achieve distinctiveperformance by addressing positive preventionand health enhancement. Good health benefitsthe individual and plays an integral part indelivering successful business performance byminimising loss and maximising gain.
The full BP management HSE expectations aregiven in the internal guidelines ‘getting HSEright’ (BP, 1999a) and the management healthstrategy in ‘getting Health right’ (BP, 1999b).The three elements of health managementbeing designated as:

62
• Prevention;
• Management;
• Promotion.
The ‘Health Planning Resource Pack’, ifutilised fully and correctly, will ensure that allthree are carried out correctly and effectively.
Health Planning Resource Pack
The Resource Pack contains planning sectionsset out as generic templates, which consist oftables with columns, entitled;
Expectations - Set objectives.
Activities - Task(s) required to achieve theobjective
Outcome - Goal or deliverable.
Responsible Persons - Who is accountable fordelivery.
Both the core elements and the specialistAppendices use the same format.
Prevention of Injury and Ill Health
This forms the first core element of the healthplanning process. It utilises an established riskmanagement approach; risk assessment,planned intervention and evaluation by audit.The plan includes contingencies for thefollowing:
1. Evaluation & Control - The identification,measurement and appraisal of risk. Anability to control the physical, chemical andbiological factors arising in or from theworkplace which may effect the health orwell -being of those at work, or those in thecommunity.
2. Assessment of Fitness to Work -Recognition and diagnosis of occupationalmedical conditions and the early stages ofoccupational disease.
3. Projects - Minimise health risks by theapplication of sound standard, proceduresand management systems for the design,procurement, construction and start up ofBPX facilities.
4. Audit & Monitoring - Regular review, auditand surveillance programmes to verify andprovide assurance of performance againstexpectations.
5. Data Management - Methods adoptedshould be simple but provide for accurateand efficient recording and speedy retrievalof information.
6. Accident Investigation - Health input aspart of an interdisciplinary team approachto accident awareness and prevention.
7. Compliance - Familiarisation with all newand current health and safety legislation.
8. External Communication & Networking -Liaison with regulatory bodies, industryassociations, health professionals etc.
The pack also contains specialist appendicesprepared to assist in planning key health riskareas:
• Occupational Hygiene• Ergonomics• Environmental Health• Stress• Projects• Normally Unmanned Installations (NUI’s)• Indoor Working Environments
Developments for further specialist planningappendices are dealt with on request.
Management of Injury and Illness
The second core element ensures that sick orinjured personnel are managed to ensure cost-effective utilisation of health services and aprompt and safe return to work. First aid andemergency care are included in this element,which is sub-divided into:
1. Primary Care - Provision of treatmentfacilities for immediate care andarrangements for first aid and resuscitationwhere medical facilities are remote.
2. Oil Industry Specific - Development ofspecialist expertise to cope withemergencies unique to the industry.Participation in developing contingencyplans for major disasters in collaborationwith external emergency services.
3. Management & Administration of Ill Health- Provision of information, advice or

63
counselling and referrals of illness.Assessment of employees’ health followingabsence from work and re-settlement ofsick or injured worker in collaboration withother health professionals and management.
4. Rehabilitation - Manage return to work.Medical pension and medical earlyretirement, and consultation withspecialists.
Health Promotion
Health promotion focuses on significantmodifiable health factors and aims to helpemployees help themselves. Quality assuredhealth promotion is one of the few tools formanaging the health of the ageing workforcewhere the diseases of lifestyle are increasinglyimportant.
1. Marketing Health - Promote a healthylifestyle at work and at home. Deliver astrategic quality assured risk basedprogramme with the emphasis on a holisticapproach to wellness including physical,psychological and social well-being.
2. Health Screening - Programmes include avariety of screening interventions rangingfrom questionnaires to consultations withhealth professionals. Focus is on the majorhealth risks: coronary heart disease, stroke,stress and cancers. These risks areassociated with modifiable lifestyle factors:smoking, alcohol, diet and exercise.
3. Needs Based Campaigns - Reinforcing themaxim that ‘Good Health is GoodBusiness’ through the use of healthpromotion campaigns based on identifiableneeds. Links maintained with occupationalhealth hazards where relevant, such asnoise, stress and musculoskeletal disorders.Cost effective campaigns to be deliveredthrough the range of resources available viathe ‘Alive and Kicking’ project (additionalmaterial is contained within the pack).
4. Raising Local Health Profile - Engaging inhealth award campaigns e.g. Health atWork Award Schemes. Utilising campaignsto maintain a longer term focus on healthawareness. Participation in local charitableevents.
Health planning is a process by which the BPXHealth Team along with key HSE andmanagement BU personnel can work togetherto achieve the timely production of a businessspecific health plan. The objective being todeliver a draft plan with clear deliverables andperformance measures. Resource management,budget and time can be included if required.Plans should then be reviewed regularly i.e. ona quarterly basis.
Health Management
Management of health risk is a continuousprocess, and it is hoped that line managers andHSE personnel will use the BPX HealthPlanning Resource Pack to identify relevanthealth protection operating procedures,assessment forms and BP best practicedocuments. In addition, occupational medicineand hygiene expertise will be harnessed asnecessary to help ensure not only legislativecompliance and with the full requirements ofBP “getting HSE right” (BP, 1999a) and‘getting Health right’ expectations (BP,1999b), but most importantly, active protectionof the health of the workforce and localcommunity will be achieved.
Health Performance Improvement
In the BP HSE expectations (BP, 1999a) itstates that the Company will periodically assessthe implementation of and compliance with theexpectations to assure employees andstakeholders that management processes are inplace and working effectively. It will then usesuch information to improve its performanceand processes. Furthermore, in the firstelement of the HSE Management SystemFramework it specifically states that leadersshould continuously strive to improve HSEperformance.
Businesses are therefore recommended toprepare a one-page summary of their healthplan these to focus on the key health risks,opportunities and resulting performancemeasures can then form part of their HSEperformance contracts.
BP now requires all business units to developand have a Health Plan in place. The nextstage, already in progress, is to develop anelectronic version of the process.
Health Planning Workshops

64
Conclusion
The Health and Safety Executive in the UnitedKingdom use the slogan “Good Health is GoodBusiness”. BP states that “Health is an IntegralPart of Business Activity” and we hope thatwith the correct use of the planning tooldescribed within, that this will be true for allBP Exploration activities.
Acknowledgments
Dr Jim Keech and Martin Delaney of the BPExploration Health Team.
References
BP; ‘Health Planning Resource Pack’produced by the BP Health Team, Dyce.
BP 1999a; BP Amoco “getting HSEright....”the HSE Expectation assessment tool”,a guide for BP Amoco Managers. GlobalHealth Assurance Team, April 1999.
BP 1999b; BP Amoco “getting Healthright...the basics for health management”.Global Health assurance Team, April 1999.

65
FEEDBACK AND DISCUSSION “DETERMINING AND USINGOCCUPATIONAL HEALTH PERFORMANCE INDICATORS”
Question - Chris Hopson, UpstreamNewspaperI wonder if I could ask Steve Williams just tocomment a little bit about worker involvementin offshore safety, in particular where theChanging Minds initiative has got to. I thoughtthat leaflet was due to be produced beforeChristmas. Perhaps you could just comment abit on that?
Answer – Mr Stephen Williams, Step ChangeSupport TeamThe Changing Minds document has beenreleased. Copies are available for people whowant them and it's publicised via the flyer andthe website, so if you want a copy let me knowand you can have a copy. It was published atthe end of last year, about November I think.
About workforce involvement in it. Stickingwith the occupational health side because that'swhat we're debating today, there is definitely aneed to get workforce involvement in agreeingthe targets that we should be setting. The waythat we're proposing to do this is through threework groups that are being established. Thereis one for each of the three major target areasfor the industry; one being occupational health,another occupational safety and the third themajor hazards. Those work groups willinvolve a broad spread of stakeholders to puttogether a proposal for both the indicators andthe targets. That will be consolidated into aconsultation document which will then be sentout to trade associations, the various networksand other stakeholders to get feedback. Thiswill allow consolidation into an overallposition which we hope will reflect all parts ofthe industry and which can be taken to OIACin July.
Question - Kevin O'Donnell, Offshore SafetyDivision HSEA question possibly for Stephen but certainlyfor Lindsay. There's obviously quite a lot ofdetail behind the occupational health plan thatyou explained, but is there anything in it thatmight work towards performance standards?Some things I've got in my mind are noise andvibration. Noise - for example, the number ofpeople, or the decrease in exposure in peopleoffshore to first and second action levels orspecific noise levels. Or, for example, hand
arm vibration - the progress with decreasingexposure. Again, people and time abovecertain vibration levels. To me those are thesorts of ways we need to be thinking forperformance standards. They are someexamples of the way we can think ofperformance standards that we could measureand hopefully see an improvement as time goesby, making due allowances for decreases innumbers of people. Is there anything in thework that either of you two have come acrossthat involves something like that?
Answer - Lindsay Ross, BPYes, well certainly in the area of noise Kevin.We have developed systems that have helpedproduce those performance standards now.There's the Noise Exposure Managementsystem which can deliver quite a lot of data onpeople’s exposure levels above first andsecond action levels etc, the amount of trainingthat's on the go and all the rest of it. We havebuilt them into some of our business plansalready. On the hand arm vibration side we'rejust on the verge of launching a managementsystem for that, so as a follow on to that wewould obviously look at putting in someperformance levels there as well. The hygienelends itself to developing these keyperformance indicators and we have got anumber of them spread through our businessplans.
Answer – Mr Stephen Williams, Step ChangeSupport TeamI can't really add to that in that the performancestandards will tend to be issues for individualcompanies and, whereas within the networkingand the working together as an industry we'resharing that information, ultimately thedecisions of what individual companiesimplement will be a decision for thosecompanies.
Answer - Dr Jim Keech, BP, Chairman ofUKOOA HACAs one of the architects I suppose of the ideaof a coherent cross industry database - as it wasmyself that facilitated the workshop thatdecided that that was a way forward - we arevery clear that, with a lack of baseline and alack of clear sharing of the data that is outthere already, it is very difficult to set realistictargets. I think we were surprised at the way

66
that that particular working group at theworkshop on 11 January actually cametogether. Despite being from across theindustry and with many different stakeholdergroups represented, there was good agreementas to what the way forward was.
The specifics of the performance indicatorswill have to wait until we have actually gotsome baseline data to work with. Meanwhile,certainly individual companies I know arealready working these issues. If I take our ownexample we have focused, for instance ondealing with a particular problem - low backpain. By having a classification system inplace, we were able to see what our low backpain figures actually were. In that performancecontract I mentioned, we looked to how couldwe contribute, what could we do, and the targetwe set was to reduce the severity index, toreduce the days lost per case of low back pain.Last year we paid out on the gain share on thebasis that we had managed our stretch target ofreducing that not just by the 25% that we setout in the beginning of the year, but by 30%.My team benefited around this time of the yearwhen our bonus gets paid. I'm sure mine is notthe only company that is able to set specifictargets and I think when we get the databasetogether, then we as an industry can start tolook at what those targets might be.
Comment - Jake Molloy - OILC OffshoreUnionFirstly I'd just like to say I support everythingthat you're saying here today - commendable,very laudable sentiments. However I think youwill continue to struggle significantly in certainareas, unless something tangible, demonstrableis done for the offshore workforce as a whole.You talked about under reporting. I haveabsolutely no doubt in my own mind that thereis significant under reporting, wholly andsimply because of the financial penalties whichindividuals incur simply by going sick. Theywill harbour and hide illnesses and conditionsin order to avoid loss of income. That's asimple plain fact. Care is significantly lacking,significantly lacking. People, members of thisorganisation and others in this room, have beensitting effectively disabled for year upon yearwith no contact from their employers, nosupport, no backup, no rehabilitation. Thatbrings me to my final point, Jim. If you wantevidence-based practice put my name on yourlist. I will provide you with more evidencethan you could ever imagine because we don'thave a problem with confidentiality, simplybecause the membership trust us to use that
material to their own benefit and adevelopment of trust is absolutely essential.
Answer - Dr Jim Keech, BP, Chairman ofUKOOA HACYes I'd like to respond on the confidentialityissue. Although I appreciate the sentiment andcertainly it is the intent to use the database in aproper and appropriate manner, it is a sensitiveissue. If we are to use that database in a waythat is going to allow us to track back - maybeif in years to come we find that there was someparticular exposure, some particular event thatmay not even come under the general hygiene-like exposure classification - then we have gotto solve the problem around names, aroundbeing able to link back. As a country we've gotsome good stuff to go on. There are somecross-industry databases already out there interms of reporting occupational disease.Occupational physicians reporting activity(OPERA) has just produced a report that's beenpublished and there's some interesting stuff inthere. We hope, with the guidance of the verypeople that have produced those databases, totry and do something equivalent for theoffshore industry.
To take the point about contractors, I wouldhope - well I can hand on heart say as far asBP’s concerned - you don't sit for 12 monthswithout any contact. However, I appreciatethat for many of the contractor organisationsthey frankly don't have that level of follow-up.I think as we move together and as we sharewith our contractor colleagues then standards,new standards in case management, are beingintroduced into many of the contractororganisations. It's not going to happenovernight and I'm sure you can give meevidence and examples of horror stories. But Ithink it is moving and there is a great dealmore social justice being introduced into theindustry than clearly ever was before.
Comment - Jake Molloy, OILC OffshoreUnionCould I just say one thing there. We aremoving in actual fact. Sick pay has gone upfrom £50 to £60 per week, so thank you.
Comments – Dr Ron Gardner, HSECould I make a couple of comments there.First of all, on confidentiality in this context.The sort of database that's being developed.Confidentiality is important to individualcompanies, but what I would hope to see,whether the data is confidential or not, is thatit’s accurate, that it's presented and that in

67
particular it gives trends once we get oversome period of time. It's not just for seeinghow well you do against your baseline but itcan give you early warning of problems thatmay be developing. I think that's absolutelykey to that sort of database.
The other point is on the reporting or underreporting. Jim and I had various discussionsabout this. We have some disagreement aboutthis. In some areas I think there is underreporting and I'm pretty certain RIDDOR isunder reported, but that's not just offshore butonshore as well. There are all sorts of reasonsfor that. In some cases it's misunderstanding,in some cases it may be purposeful, I don'tknow. In other cases it's the regulation itself,it’s not particularly useful for the offshoreworld. I think that's something that asregulators we need to look at and think about,just whether RIDDOR is really fit for purpose.I think that comes very squarely under theCompliance programme of Securing HealthTogether.
Question – Mr Graham Cowling, AcousticTechnology LtdA question for Dr. Gardner. Your presentationindicated that if we're talking about a target,that the real target actually is the condition ofALARP (as low as reasonably practicable).How does that sit with the fact that perhaps theALARP situation may mean that differentcompanies set different targets? How wouldyou resolve them having different targets?
Answer – Dr Ron Gardner, HSEI have no great difficulty with different targets.I'd be happy if there were the targets! I'mstarting from that sort of baseline. Graduallyover a period of time with sharing of practice,with sharing of best practice, with sharing ofsuch targets, I think those targets wouldequalise. It's getting those targets and theindicators there in the first place and sharingthem. To be fair a lot of companies do have allsorts of targets on health and some haveperformance measures, but often they're notshared and I think that's something that thisconference could be very useful for andsomething certainly the Step Change initiativewould be very useful for.
People sometimes lack a bit of imagination Ithink in setting targets or indeed performancemeasures. I was very startled at a differentexample to noise, but with COSHH. A largenumber of companies have done some goodwork since COSHH was applied. Very few
have any performance indicators in there andyet some are very obvious. Have we actuallyreduced exposure? Many companies have putLEV in (Local Exhaust Ventilation) and yetthey didn't check how effective it was and that'snecessary under the regulations. Is it every 14months? In fact they've not put any system inplace to do that, yet it was a very obviousmeasure of performance. So perhaps I startfrom a slightly lower baseline than you arethinking of. Does that answer your question?
Question - Dr Ron Gardner, HSEA question for Lindsay and Jim really.When/how long's this programme been inplace? What I didn't pick up (maybe trying toread at an angle doesn't help), is how do youaudit it? How do you check with the businessunits how well they're doing or do they do thatthemselves? Is there any central view of this?
Answer – Dr Jim Keech, BP, Chairman ofUKOOA HACThe Health summary sheet went into all theexploration business units globally, who wererequired to submit a summary of their healthplan. We managed to get all the business unitsin our area to submit. It was remarkable whenwe examined the health risk matrices that werebehind those, how right across the globe wehad the same issues; psychological health,stress, musculoskeletal injury and disease weretop right hand issues. That was commonwhether it was Venezuela, Angola or Bruce,Brae or Miller. It was that summary that wasin there. Different business units have chosendifferent routes to get to the summary. Wehave taken exception when we have found thatall they've got is a summary because franklythat's not good enough.
Comment – Lindsay Ross, BPWe do actually internally audit as well. Wehave an audit group within BP in HSE, gettingHSE right. The group go round and obviouslythey look for the detail behind the summaryhealth plans, making sure that they're meetingthe company expectations.
Question – Dr Ron Gardner, HSEAre lessons from those passed back generallyacross the other units as well? Again comingback to best practice.
Answer – Lindsay Ross, BPI think we'll be able to facilitate that muchbetter once we get it onto a shared electronicbasis. At the moment it's hard copy and eachkeep their own systems so that limits the

68
amount of sharing that goes on. As anOccupational Health team we can obviouslyhelp facilitate that sharing as well. Where wesee a good performance measure somewherewe can maybe suggest that to another businessunit that has similar risk scenarios, so there is adegree of sharing that goes on.
Question - Dennis Krahn, InternationalAssociation of Drilling ContractorsA question for Jim Keech. I'm sorry I didn'tthink of the question after Malcolm Brinded'spresentation, but it was during the coffee breakthat I was having a discussion with some of mymembers. There was the implication inMalcolm's presentation that their systems weresuperior to those that hadn't heard the gospelyet. So those that had installations that weren'tcompany installations were perhaps inferior,implied maybe but you could draw thatconclusion. Now some of my members tell methat they have very good systems and so myquestion is this. Do you think that you areconcentrating on your own systems and maynot be able to recognise those of thecontractors who have very good systems? Andif they have very good systems, could youleave them functioning like they are or maybeeven in an ideal world learn from them bysharing best practice?
Answer - Dr Jim Keech, BP, Chairman ofUKOOA HACI assure you we do, and I would take theexample of the drilling contractor on theFaeroes operation, who demonstrated anexcellent health surveillance scheme. This is agreat model and a model that certainly I will beadopting in BP where it makes sense. I think ithas been alluded to already, the confusion thatthere has been in an industry that has had afitness-to-work medical which has nothing todo with health surveillance. What we saw withthat particular drilling contractor was anexcellent attempt at managing the whole issueof health surveillance. I don't think thatnecessarily we are superior because we've gotbetter resources, because we're big operators.We're learning all the time and I'm sureMalcolm was not suggesting that we havenothing to learn from your members. That'scertainly not the case.
Comment - Dennis Krahn, InternationalAssociation of Drilling ContractorsThank you for that. It just came to my mindthat for safety management systems we have aninterfacing document. That was what was atthe back of my mind. If we find something that
works very well, we just take the one we have,interface it with the one that the client has, andlet them both perhaps exhibit their best pointsor work together effectively. So thank you foranswering the question.
Comment - Dr Ron Gardner, HSEDennis, it is interesting that you mentionedinterface documents. I had experience oflooking at safety management systems, when Ifirst joined OSD, before getting into the healthbit. It was very interesting that the healthtopics were often the ones that didn't getcovered particularly well in the interfacedocument. If there is going to be a holeanywhere it's often related to something to dowith health. The sort of message you're givingme now is quite encouraging. If either side canprovide the management system to cover someof these topics, that’s excellent. But it was anarea, certainly historically, where there wasoften a hole in the interface.
Comment – Mr Taf Powell, HSEI've been away from Offshore Division for awhile. I came back last summer and have justa couple of observations that I'll share withyou. First of all I've not seen Step Change. Itwas invented, or discovered while I was away,but it certainly has impressed me in a sense thatit has joined up a lot of people under acommon enterprise. It started with seniorleadership and that was very good. However,one thing I thought about Step Change was thatperhaps some of the leading indicators tendedto be on a softer side, things that we weredoing well as a good leading indicator perhapsrather than measuring some of the precursorfailures, where you get a lot of data abouttrends and where that might be taking you. Ifthere was one extrapolation into the health areawhere you need to develop leading indicatorsclearly to make a difference in the future, isthat some of those leading indicators probablydo need to be the harder side, where things aregoing wrong, of no consequence maybe, butnevertheless not just where we're showingsigns of doing things well like training, workerinvolvement and so on.
Comment – Mr Stephen Williams, StepChange Support TeamLeading indicators are something which haveincredible power and benefit to help us moveforward, providing they're used correctly.There are a lot of ways, a lot of pitfalls in theiruse, one of which is measuring somethingwhich we're already doing well in that the mainvalue for leading performance indicators to me

69
is to actually drive the improvement processand therefore they need to be measuringsomething which you feel is relevant forimproving performance and something whichyou could do better.
Additional guidance is being developed onleading performance indicators, both for safetyand for health. The draft consultationdocument for that is being prepared at themoment. If there are people who would like toobtain copies of that, during April we'rebasically trying to seek input on the guidancewe're giving for the more effective use ofLeading Performance Indicators, to try andcounter the shortcomings and potential pitfallsand get more effective use. I think they arepotentially very powerful vehicles for bothengagement and workforce participation inidentifying what the important issues are andthen having identified them, are givingrecognition for where there is improvement inperformance on those.
Comment - Dennis Krahn, InternationalAssociation of Drilling ContractorsIADC was pretty instrumental in leadingindicators. Charlie Mearns was the one that ledintellectually on that. The inspiration was thatin the beginning of a contract process wewould often be asked by the clients about ourlost time injury frequency and of course theyhave a right to know that and you gatherstatistics and do an excellent job. But it wasnot what they were doing offshore with theirworkforce to inspire better performance, so itdidn't feel right. It was backward looking andmeasured failure etc so we wanted to get awayfrom that. Now you're quite right in that theyare imprecise and that they tend to measurewhat you're already doing well. However, Ithink Stephen is right in the inspirational bitthat they have for your company and for yourworkforce - you know the positive feeling andthe desire to excel and perform well instead ofthe kind of negative feeling that comes withthings that happen so that's how we use andhow we think of those.
For lots of Leading Performance Indicators wedon’t have the right metrics yet. We knowwhat we want to talk about but we don’t yetknow how to measure progress quite so well.
Comment – Dr Jim Keech, BP, Chairman ofUKOOA HACI would just like to share some thoughts on theleading indicator argument because it'ssomething that I've been contributing some
stinging papers to people who then don'tpublish them so I'll have to take myopportunity. First off yes, we are very good asan industry at measuring what we didn't wantto have happened and this gives us a verynegative view of safety which is very oftenunhelpful when it comes to improvingperformance. The same can be said of healthas well.
Two things - one is that many of us, as healthprofessionals, safety professionals etc., seem tohave forgotten all that statistics andepidemiology as too difficult. It was in a bookthat we probably didn't read and how often dowe actually use the techniques of the analysisof variance, of determining whether asignificant change has actually happened? It isin all the scientific literature, it's there but do Iever see it in health and safety data in theindustry? No, so a lot of the time we chase ourtails on things that have happened by chance.We've ignored those techniques in our pursuitof the Holy Grail. We could learn somethingfrom the marketers. We could learn somethingfrom the social scientists. We could learn fromthose people that sell us things we never knewwe wanted by analysing their questionnaires ina very clever way. I mean, I would love toknow how they keep selling new boxes of soappowder with no real significant difference andit still just cleans your kit, but they do. So whycan't we learn from those folks as to how toproduce leading indicators, how to interpretdata to make some meaningful change?
Comment – Dr Kathryn Mearns, University ofAberdeenCan I say something as a social scientist whohas been working with the industry. We've justcompleted a benchmarking study where we'velooked at a number of different leadingindicators and we've been using some of thestatistical techniques you've just mentioned interms of regressions and analysis of variance.There is a lot of value in that, in understandingactual relationships between variables andwhat has the impact, which variables have animpact on another. So I would very muchsupport your comments.
Comment - Dennis Krahn, InternationalAssociation of Drilling ContractorsIt's visible when I go round to my members'offices. Now I see fruit out. It brightens upthe place and is an indication of healthy eating.I see people having competitions at lunchtime,riding stationary bicycles for charity. In termsof leading indicators for health performance,

70
hopefully that will feed into our ideas abouthow to do what Jim said, market safety. Safetyfor some people I've heard say, offshore atleast for the workers, it's kind of a burden now.We need to take some of these ideas whichhealth seems to have and capture those for howto make safety fun and interesting and getpeople to contribute with the same kind ofenthusiasm.
Comment - Dr Ron Gardner, HSECan I slightly play devil's advocate with a wordof caution here. I agree with Jim in the sensethat you need a very scientific approach to this.But I spent a fair part of my life using thingslike regression, analysis of variance and I see alot of work now which worries me. There islots of data. The world is awash with data andpeople mine that data rather unthinkingly andthey come up with associations like ‘theanalysis of variance supports an associationbetween X and Y’ and you look at it and youthink how on earth can they be associated? A
statistical association on its own meansnothing, unless you've actually got somemechanism that makes the association sensible.But to be honest I see far too much scientificwork that doesn't have that. It just has thestatistics. This is just a health warning. If youare going to use it, make sure you understand.Have your hypothesis first and test it. Don'tcome up with lots of associations. It justconfuses everybody.
Comment – Dr Jim Keech, BP, Chairman ofUKOOA HACMy appeal was not for associations necessarily,but understanding the difference betweenassociation, correlation and causation. Assome of my poor health and safety colleaguesknow I am likely to send out, I think it’s theBradford Hill Postulates (I see Nerys nodding).I send those around the globe every now andagain just to keep them on the right tracks.

71
DAY 2
MORNING SESSION
SESSION THEME – OCCUPATIONAL HEALTH IN THE OFFSHOREDESIGN PROCESS

72

73
OCCUPATIONAL HEALTH IN THE ENGINEERING PHASE OFOFFSHORE DEVELOPMENT PROJECTS – LEGISLATIVE BASISAND EXPERIENCE FROM PROJECT AUDITING IN NORWAY
Mr Sigvart Zachariassen, Mrs Anne Myhrvold, NorwegianPetroleum Directorate, Stavanger, Norway
Abstract
Many employees on offshore oil and gasinstallations have to rely on personal protectiveequipment to avoid work related diseases. Thisis not recognised as a proper preventionstrategy. High noise levels and bad ergonomicsolutions are often deeply grounded in thedesign of the installation and type andarrangement of machinery. Technicalmodifications in order to achieve significantreduction of exposure and risk levels aredifficult to achieve and expensive to perform.Occupational health achievements seem not tofit well into traditional cost benefit baseddecision-making.
The Norwegian Petroleum Directorate (NPD)has since 1995 enforced an occupational healthlegislation that focus in particular on asystematic approach to the design andengineering phase in offshore developmentprojects. The NPD has followed most of therecent offshore projects closely by audits andverifications.
The industry has followed up the legislativeinitiative by developing a specific standard forhow to deal with occupational health aspects inthe engineering phase.
Over the last few years there has been observedsubstantial improvements of the engineeringpractice. A common understanding andstructured co-operation between projectmanagement, experienced workers, designengineers and occupational health experts seemto be important pre-requisites for success.
This paper will describe and discuss keyelements of the Norwegian legislative basis anddiscuss the Norwegian approach forimplementation of occupational healthrequirements in the planning phase of offshoreinstallations and modifications.
Why focusing the engineeringphase?
Based on audits and follow up activity mainlydirected at occupational health conditions inthe operating phase of offshore installationsthrough the eighties and beginning of thenineties, we realised several characteristics ofthe existing occupational health conditions:
• Occupational overexposure and workrelated illnesses/injuries due to poorarrangements in areas and poor design ofmachines and equipment
• Occupational health requirements notregarded as hardcore technicalrequirement and consequently notidentified and followed up throughformalised management systems
• Modification work to rectify badoccupational health conditions in theoperating phase is expensive andtroublesome
• Weaknesses are copied to newinstallations
These observations gradually led to a change infocus from the operating phase to theengineering phase. The last years the NPDhave closely followed most of the mainoffshore development projects from anoccupational health point of view. Lack oflegislative framework and requirements wasone of the problems we faced in the first phaseof applying the new strategic approach.
Legislative framework Regulation relating to systematic follow-up ofthe working environment in the petroleumactivity (SAM-regulation) was issued by theNPD and entered into force August 1st 1995. One important aspect of the regulation was toapply the quality assurance and internal controlprinciples and terminology on the occupationalhealth area. Specifically the regulationaddresses requirements on occupational health

74
in connection with planning of newinstallations and main modifications: • Systematically transfer of experience• Occupational health programme
describing goals, requirements,responsibility and list of planned activities
• Requirement to define specificrequirements
• Occupational health related analysis andassessments applied as decision support
• Active involvement of personnel withoperational experience and workersrepresentatives
The climate in the industry was at this point oftime positive; - several of the main oilcompanies had competent and experiencedprofessionals with quite a good influence ondecision makers. They contributed veryactively to the implementation of the newregulation, but the most important thing theydid was probably to develop occupationalhealth design standards and requirements. Standards – recognised practice It is not possible to discuss design standardswithout mentioning NORSOK – the parallel tothe UK Crane initiative. The NORSOK processhad several elements, some of them with acontradictory relationship. One part of it wasthe new cheaper/faster/simpler – philosophythat indeed had implications for design; -mostly negative. Another part was thedevelopment of industry standards (NORSOK-standards), which in many cases resulted inimprovements. The Norsok Standard S-002 –Working Environment was issued in 1996 andrepresented a specification of the functionalrequirements in the new regulation (above).The standard is split into two parts: 1) Requirements related to management ofoccupational health in the engineering andconstruction phase• Procedures and work instructions for
studies and analyses including scope,timing, resources etc.
• List of studies and analyses to beperformed
• Verification activities, design reviews etc.• Working environment area charts for
documentation and follow up 2) Specific requirements on factor level• Arrangement, layout, ergonomics• Noise and vibration• Chemical hazards
• Illumination• Indoor climate and outdoor operations• Radiation The Norsok S-002 is the main design standardwith regard to occupational health, but thereare several other standards that give relevantsupport: • Norsok S-005 Machinery – working
environment analyses and documentation• Norsok C-002 Architectural components
and equipment• Norsok C-001 Living quarters area The Norsok standards are available in Englishon http://www.nts.no/norsok The NPD was involved in the development ofthe standards and the SAM-regulation nowrefers to the relevant Norsok standards asrecognised practise. This means that theNorsok standards reflect the level ofoccupational health conditions. If the level isreached by other means, it is accepted, butshould be documented. On the other hand, ifthe level is not achieved, the oil company hasto apply for deviation from the relevant sectionin the regulation.
Resources One important criteria for success is a propercombination of and co-operation betweendifferent kinds of personnel that haveknowledge and common understanding of therelevant legal and contractual requirements• The discipline design engineers• The experienced operator/workers
representative• The safety/occupational health specialist Most commonly an HSE/occupational healthco-ordinator in the oil company and a similarposition with the main contractor organises thedifferent activities and order resources. Onechallenge is to secure that operational staff areavailable on short notice to take part in designreviews etc far from where they normally work.Availability of personnel at the right time iscritical for proper timing and quality of thedesign input. It is our experience that a clean-cut consultantbased approach is not the best way to achievegood results. Consultants are often workingwith a too long geographically and mentaldistance to the project and are not in a position

75
which allows him to follow up on a continualbasis and actively influence the decisions. Fullor part-wise integration of occupational healthspecialists and operating personnel within theproject team is a key aspect, but it ischallenging and requires well defined rules forco-operation.
Management tools Systematic follow up of observations andrecommendations from studies, analyses,reviews etc are essential in order to prioritise,decide and implement the best solutions. Inmost project organisations there are establishedcomputer based follow up systems that make itsimple to follow status, responsibility,deadlines etc. If this system is actively used asa management tool, it can be an effectivedriving force for solving outstanding issues andhit the imaginary point between too early andtoo late. It is a general experience that existing andcommon project management systems shouldbe utilised for occupational health matters.Specialised systems will very often loseattention from the engineers and the linemanagement. Contractual power and professional
deficiency? The Norsok standards are laid down ascontractual requirements in most offshoredevelopment and modification projects.Depending on specific needs, the operator alsodefines addendums to the Norsok standards. Inprinciple violations of the standard are treatedas violation on the contractual requirements.This is a very strong enforcement tool, in somecases we have experienced that it is misused. In an offshore project the contractual structureis very complex, normally with an EPCI-contract between the oil company and the maincontractor as the top level. The main contractorplaces contracts with a lot of sub-contractorsand suppliers. The “back to back” contractualprinciple is most often applied. This means thatevery small sub-contractor and supplier has theresponsibility to fulfil the full scope ofrequirements in the original contract. If the understanding of requirements is not thesame through the contractual hierarchy, theresults might well become insufficient. Thereare several barriers for a mutual understandingand implementation of requirements:
• Cultural differences between countries and
continents and between industry traditions• Different approaches and methodology• Lack of occupational health expertise The NPD has experienced that contractors andsuppliers have been claimed for contractualviolations in a way that obviously is unfair. Ithas been necessary to focus the role of the oilcompany as facilitator in order to improve thework processes and the purpose of the pro-active approach necessary to achieve the bestoccupational health solutions. The oil companyshould together with the main contractorcommunicate the requirements andexpectations and give relevant and specificadvice to sub-contractors. Although significant improvements have beenachieved by implementing new regulations,new standards and systematic methodology inoffshore development and modificationprojects, this strategy is still challenged by anarrow-minded cost-benefit attitude. It isimportant to remind us on the probably bestarguments to resist the everlasting doubtwhether or not occupational health conditionscontribute to increased economical values: • Good occupational health conditions are a
pre-requisite for productivity and safeoperation
• Due to best technical/economical practisethe proper way of achieving best solutionsis to implement sound requirements in thedesign basis
QUESTIONS AND ANSWERS SESSION Question – Dr Ron Gardner, HSE That was a very interesting presentation. Idon’t want to pre-empt Kevin but you’ll find alot of parallels with our experience. I have aquestion for you. Have you any thoughts onhow experience from one design situation canbe passed onto the next, because what we comeacross is that teams come together, do a designjob then break up so there’s no memory ofwhat they did carried forward into other jobs.So in effect you have to repeat the wholeprocess or they take things off the shelf. Answer – Mr Sigvart Zachariassen, NPD We experience that bad solution, transferred tonew projects over and over again. That’s whywe have focused in our regulations, and alsothe Norsok standard has focused, on asystematical experience transfer.

76
Comment - Dr Ron Gardner, HSE Could I just say, that transfers the standardsand knowledge. It doesn’t transfer experience. Answer - Mr Sigvart Zachariassen, NPD Well maybe I did not get your question right,but from our point of view it is important tocollect experience data from a former projectactively and document it and take it on boardin new projects. Question – Mr Ed Terry, Sauf Consulting Ltd You mentioned one phrase about manyoccupational health issues weren’t recognisedas formal analyses. I think we’ve seen thatmaybe the Norsok standard is trying to drive
some formal analyses into the design basis. Iwas wondering how much success you’ve seenof that being adopted within the designprocess? Answer – Mr Sigvart Zachariassen, NPD I think it differs a lot. With regard to noise, wehave a very well established methodology forestimating noise levels and also for estimatingnoise dose, but with regard to other factors thisis not simple. We are not satisfied with thesituation for chemical exposure for instance.We think that there are tools available formodelling exposure that are not as fullyutilised.

77
SYSTEMATIC FOLLOW-UP OF WORKING ENVIRONMENTACTIVITIES DURING DESIGN OF OFFSHORE INSTALLATIONS
Mrs Claudia C. González Hague and Wenche Solberg, ScandpowerAS, Norway
Introduction
In Norway, working environment has hadspecial focus during design and construction ofoffshore installations during the last five years.Poor design solutions with respect to workingenvironment represents a risk for occupationalaccidents and diseases. In the engineeringphase, decisions are made that affect theoccupational health standard on theinstallation, both during operation andconstruction. Implementing a highoccupational health standard during theengineering phase avoids expensivemodifications in the operation phase andreduces the risk for occupational accidents anddiseases, which are economically beneficial forthe operating company. Occupational Health Requirements
Authority regulations together with the Norsokstandard for working environment, S-002,apply to design of new offshore installationsand modifications of existing installations. Thisstandard is referred to as recognised practise inthe NPD regulations. The standard addresses design principlesrelated to occupational health and workingenvironment. The standard also coversrequirements to the procedures for control andverification of design in order to ensure that theprinciples are implemented. The purpose ofthe standard is to ensure the quality of theworking environment during the operationalphase and that this complies with theapplicable regulations.
Occupational Competence in theEngineering Phases
Working environment analyses in theengineering phases may be performed by anoccupational health specialist as an integratedpart of the project organisation or performedon consultancy basis. Our experience as consultants is that the bestresult is achieved when the occupational health
specialist is integrated in the project teamduring the entire project. We have also experienced that it is goodpractise for the occupational health specialistto give training courses to the disciplineengineers in the beginning of the project tomake sure that all members of the project teamhave necessary basic understanding of theworking environment requirements in theproject.
Roles and Responsibilities in theDesign Process
The Operator has the overall responsibility forimplementing authority requirements withrespect to occupational health. The Operatorspecifies working environment requirements tothe new installation in the contract with thecontractor. During the engineering andconstruction periods, inspections and audits areperformed to verify that requirements areimplemented in the design. The operator shallalso provide experience data from installationsin operation to the project. The engineering company shall identify alloccupational health requirements to theinstallation and perform the required activitiesto make sure that the requirements areimplemented in the design. During the designphase, the engineering company shall alsomake sure that working environmentrequirements are understood and implementedby their vendors. The engineering companyshall also conduct audits and inspections intheir own organisation and towards theirvendors to verify the level of implementationof working environment requirements.
Working Environment Activitiesduring the Engineering Phases
When designing new offshore installations, aseries of analyses and studies are to beperformed and documented in order to controland verify that the design principles are met.Responsibility and schedule for analyses,control and verification activities shall be
78
defined in a Working EnvironmentProgramme. Systematic activities within workingenvironment to be performed include: Concept Phase: - Concept working environment analysis –
to identify and evaluate potential problemareas as input to concept selection andverification of design. Main focus in thisphase should be: location of noisyequipment, living quarter and CentralControl Room; distribution within LQ;transport and transportation ways;permanent work places in respect to windand weather.
Basic Engineering Phase: - Specify working environment area limits –
to establish specific limits for workingenvironment factors such as illumination,temperature, concentration of chemicalsubstances in the working atmosphere,ventilation, noise and vibration for eachroom/area on the installation as input toengineering.
- Noise and Vibration control – coarse noise
prediction including identify noise andvibration sources and evaluate principalacoustic, vibration and noise controlsolutions; prepare specific packagerequirements for noise emitting items forinclusion in inquiry documentation (NoiseData Sheet).
− Coarse working environment evaluation –
systematic evaluation of the selectedconcept design with respect to workingenvironment factors in order to identifypossible problem areas for further analysesor report recommendations to the design.
Detailed Engineering Phase: - Detailed job safety analysis – systematic
analysis of selected areas or equipmentpackages to ensure that risks foroccupational injuries are eliminated orreduced to a minimum.
- Ergonomic analysis – to identify potential
problem areas in design of workplaceswith respect to ergonomic factors,including evaluation of layout, clearancesfor performance of tasks, location of work
functions, needs of stairs and accessplatforms, lifting and transportation aids.
- Human-machine interface analysis for
control rooms – to ensure that the workingenvironment in the control room(s) are inaccordance with requirements from theauthorities, and to evaluate the controlrooms’ ability to handle abnormalsituations.
- Analysis of handling hazardous
substances/chemicals – to ensure that therisk of exposure from use, storage,handling and disposal of chemicals andother hazardous substances are eliminatedor reduced to a minimum.
- Outdoor operations analysis – to evaluate
weather exposure at outdoor workplaces inorder to identify and remedy potentialproblem areas related to wind chill andhypothermia.
- Noise and vibration control – to identify
potential sources of noise and vibrationand recommend remedial measures.
The work includes:« preparation of preliminary
predictions of personnel noise exposure;« specification of requirements to
sound insulation, sound absorption andvibration isolation;
« follow-up of procurement anddesign of equipment packages to ensurethat noise and vibration limits areadhered to as closely as possible bysuppliers;
« using all available data, calculatepredicted area noise levels for all mainareas/rooms on the platform; advise theproject on noise and vibration controlrelated matters and
« witnessing equipment noise tests aspart of the projects QS activities.
- Material handling study - detailed
evaluation of transport routes, transportmethods and equipment forhandling/transport of heavy items above25 kg during operation and maintenancework onboard the installation in order toensure safe and efficient operation as wellas obtaining an acceptable workingenvironment.
- Updating of working environment area
limits with predicted values and resultsfrom performed audits.
79
Scandpower has developed and documentedmethods and guidance (internal) withinworking environment activities in design. Thisdocumentation includes: working environmentprograms, checklists, specific workingenvironment requirements (for rooms/areas onthe installation(s)), working environmentanalyses and evaluations, working environmentaudits, working environment courses andelectronic follow-up systems. These methodsand guidance have been used in a series ofprojects and have proved efficient.
Performing Working EnvironmentAnalyses
A high level of co-operation between personsfrom different disciplines in the engineeringteam, operation representatives andoccupational health specialist is an importantcriterion for success in performing workingenvironment evaluations. Therefore most evaluations are conducted inform of review meetings with participants fromthe different disciplines in the project team andfrom operations representatives. A workingenvironment specialist will plan, conduct andreport the meeting. HSE is a line responsibilityin projects so implementation of actions fromreviews is the responsibility of the engineeringdisciplines. Special checklists are prepared and used to beable to carryout the evaluations in a systematicway. In most projects, an electronic follow-upsystem is required to have an overview thestatus of implementation of the actions fromreviews.
Follow-up activities Working environment follow up activities:
- Inspections at the construction site(s) andat vendors to ensure, that workingenvironment requirements are implementedin design.
- Verifications and audits towards the
engineering team and towards vendors - Design reviews, e.g. 3D-model reviews to
verify implementation of actions fromperformed analyses and other workingenvironment requirements.
- Working environment status reporting, e.g.on implementation of actions.
Experience from previous projects
Experience from previous projects show:
- Fewer changes needed to be made during
fabrication if follow up for access andergonomics is conducted during detailengineering.
- Experience and input from operators and
maintenance personnel during theengineering period is important.
- Difficult to follow-up space requirements
of the single components/equipmentpackages due to total space allowed by theproject.
- Requirements to vendors should be
followed up closely even if the vendorsactually have the responsibility to complywith the EU Safety of Machinery Directive.
- Material handling and transportation of all
heavy equipment needs to be consideredthroughout the engineering phases.
- Competitive requirements between
technical requirements and workingenvironment requirements, e.g. location ofsafety relief valves.
- Useful to have an electronic follow-up
system for actions.
Conclusion Working environment analyses/evaluations aidin improving working environment and helpimprove the quality of design. By improvingworking environment during the design phase,occupational health problems duringinstallation’s operation are prevented. Working environment analyses/evaluationsalso: - Allow experience transfer through:« participation from operation« survey (mapping) reports from
existing installations« HSE data from operations
- Stimulates multi-discipline co-operationwith occupational health/workingenvironment in focus

80
- Is a systematic approach to occupationalhealth in the design process
Performing these working environmentanalyses during engineering phases is costbeneficial due to reduced need for changesduring fabrication, installation and operation.It ensures improved compliance withapplicable standards and regulations and alsoensures that client’s requirements are alsoincluded as part of design. QUESTIONS AND ANSWERS SESSION Question - Dave Freeman, Norwich HSE Can you comment on the Norwegian state onthe company losses for occupational healthfigures? Do you get data banks of why youhave the different accidents? Can you say youprioritise them? Then can you comment on theproject costs, the percentage that’s put forwardfor occupational health compared to the rest ofthe project costs please? Also can youcomment finally on wind chill? Why is this socritical in the Norwegian waters? Answer - Mr Sigvart Zachariassen, NPD Well that was about the data collected fromoccupational diseases and injuries. Did I getyou right? What is the basis? (Dave Freeman -That’s correct). Well we have for many yearscollected information about both occupationaldiseases and injuries and we analysed theresults and in both the databases we find thatthe design aspect is a main cause for a lot ofthe injuries and diseases and that is our basis. Idon’t think that we have any specific figuresrelated to cost for those. Question - David Freeman, HSE: The fourth question was wind chill. Why is itso critical on the Norwegian shelf? Answer - Mrs Claudia C. Gonzalez Hague,Scandpower AS, Norway Well it’s very important because of thetemperature. We are located quite far northand the wind is very strong. We have veryhigh levels of high velocity winds in the NorthSea. It is important to ensure that you protectthe workers when they are performing theirmaintenance activities and their operations. Question - Kevin O’Donnell, HSE The systems you have described - could I askhow long have they been in existence and whatis the general experience with running them sofar? Are they reasonably successful or is it tooearly to tell?
Answer - Mrs Claudia C. Gonzalez Hague,Scandpower AS, Norway Norsok came in in ‘96 and I think it’s taken aperiod of time to ensure that you have the rightmethodology, that you have the rightcompetence in the project. I think fromexperience, the more active the differentdisciplines are, the more education and trainingthey get in the early phase, the more effectivethe design reviews can be. From myexperience I think they’re quite effective butyou don’t get everything. There are alwaysissues that you need to follow up in thefabrication phase and during the operationalphase. Question – Michelle Gibbs, University ofSurrey In the design of an offshore installation, whatconsideration is given to the illumination indifferent areas – are the levels of lighting basedon research of appropriate light levels fordifferent work? Answer - Mrs Claudia C. Gonzalez Hague,Scandpower AS, Norway Norsok has highlighted for the various roomsand areas in the installation, there’s a differentrequirement with respect to lux values. Foroffices, let’s say, you have much higherrequirements in respect to illumination thanyou have in access ways for example. But interms of how they’re based on scientificresearch, I’m sure they’re based partly onscientific research and on experience I wouldassume. Question - Tony Garner, Conoco Do you have any input into the psychosocialwell-being of the people before the engineeringstandards are made, such as gymnasiums orliving quarters accommodation, space - bedspace, personal space. Does this matter toyou? Answer - Mrs Claudia C. Gonzalez Hague,Scandpower AS, Norway There are requirements in the living quarterNorsok standard. There are requirementsrelated to square metres per person and alsorequirements for size of cabins. There’sdescription of activity rooms, what kinds ofactivity rooms are on the installations? Withrespect also to psychosocial, the operatingcompany has responsibility for carrying out apsychosocial evaluation to look at manning onthe installation and the type of work that theycarry out.

81
Comment -: Dr Eirik Bjerkeboek, NPD Maybe I could comment on the psychosocialaspect. The Norsok S002 standard requires asClaudia mentioned that kind of analysis to becarried out. This is of course referring toseveral of the speakers yesterday. The focuson mental health should have a large focus alsoon the side effects. But it is extremely difficultto forecast what kind of stress level or whatkind of health output you will have from thepsychosocial working environment. One of thecompanies that has at least tried to develop amethodology here is Norsk Hydro, where theyuse a kind of comparing analysis with workingand psychosocial environment on existinginstallations, and try to adapt stress levels andwork load levels there into the new design. Question - Mr Curt Robinson, AcousticTechnology Ltd Does the NPD have any input during thedesign stage, or is it similar to the HSE where Iguess the first time they get to see whether thedesign’s been successful is when the platformis first operating? Answer - Mr Sigvart Zachariassen, NPD Well it’s when the installation is operating thatit is finally possible to verify. However, in ourfollow up activity we look very closely at howthe work is being performed and if there are setrequirements, for instance, for equipmentdepending on the layout and several things. Sowe pick up things in the engineering andconstruction phase but at the end of the day itis the level that is verified at the end when theinstallation comes into operation that is final.If there is some exceedance from the limitvalues, the operator has to apply for non-conformance and normally we do not give thatin the case of a new installation. Question - Mr Curt Robinson, AcousticTechnology Ltd That strikes me as almost too late, especially Iguess for some instances, mainly noise. It isvery difficult to then actually apply litigationmeasures after the platform has beencommissioned. So the designers don’t have tosubmit anything to you during the actual initialdesign stage and say this is how we’d like toset out our platform, so that they can perhapsuse the experience from the NPD? Answer - Mr Sigvart Zachariassen, NPD No they do not have to submit as a normalroutine. But when we have an audit at thatspecific project, we normally ask for a noise
report and go through the systems, themethodology, the competence etc. Answer - Mrs Claudia C. Gonzalez Hague,Scandpower AS, Norway I’d like to answer that. During the engineeringphase, for me sitting in the project, what isrequired from the engineering company is tosubmit non-conformance requests. Sothroughout the design the different disciplines,when they cannot comply with the regulations,they submit a non-conformance request to theoperating company for approval. It’s a systemthat is going throughout the entire projectduring the design and fabrication phase soyou’re always aware of where you are actuallynot complying with the regulations. Question – unknown speaker Obviously the Norsok standard is in Norway.There are also other standards around in theNorth Sea. Can you tell us a little bit abouthow your efforts are to harmonise all theseregulations instead of changing rules everytime you cross the border. Answer - Mr Sigvart Zachariassen, NPD I don’t think I’m the right person to explainthat, but that is a matter that is discussedalmost continuously and we are being told thatit’s very expensive to come from UK watersinto Norwegian waters. A study has beenperformed, I think about one year ago and itshows that the difference is not as big as it’sclaimed, so I don’t think it’s a very greatproblem at all. Question – unknown speaker But you have a lot of rules up in Norway withNorsok but the results in health and safety arenot different. I mean the rules that youimplement are not proving that it makes betterhealth and safety. Answer - Mr Sigvart Zachariassen, NPD Well the Norsok standard which we havetalked about today is a design standard and itdoesn’t apply for existing mobile units forinstance so maybe that is sorting out some ofthe problems. The requirements in theNorwegian regulations are not very muchstricter than the UK regulations but maybethere’s a difference in the practice of theregulations, the enforcement of the regulations. Comment - Kevin O’Donnell, HSE I just want to make a comment in relation tothe point the gentleman has just raised. I don’twant to pre-empt what I am going to say but

82
having heard the last two speakers, there’s a lotof common elements in what they’ve said andwhat we’re looking at. In seeking to followconsistency we will look very closely at whathas been done in the Norwegian sector to seewhere we can learn and what things we can doin conjunction with the industry to try andmaximise the consistency between the regimes.We’ll have to look at it very carefully.
Comment – unknown speaker It’s a comment actually on the documentationof the effect of the Norwegian regulations andwhether we have actually improved our healthoutcome from these regulations. I think you’reright in that this has not been documented on abroad basis. However, we’ve had one study onautomatic pipe handling systems whichdemonstrates very clearly that there has been areduced rate of injuries and accidents when thistype of equipment was introduced. The resultsof this study are very well agreed upon by allparties.

83
DESIGN OF OFFSHORE INSTALLATIONS – DON’T FORGETOCCUPATIONAL HEALTH
Mr Kevin O’Donnell, OSD, HSE
Abstract
This paper outlines the background to theconsideration of Occupational Health issues inthe design of Offshore Installations, and raisessome of the problems and difficulties with thisprocess. The provision of Occupational Healthdesign guidance for Offshore Installations isoutlined. HSE’s Offshore Safety Division’sKey Programme of work includes thisobjective and offshore design safety cases willbe reviewed using these guidelines.
Introduction Since the review of the safety regime of the UKoffshore industry about ten years ago, atremendous amount of work has been done toaddress the numerous hazards to safety thatexist. Most safety hazards are well recognisedand the industry has done a great deal in recentyears to reduce the risks from these hazards. During this time Occupational Health hastended to be overlooked, particularly in theearly 1990’s, largely because of the drive toaddress safety issues. Within Offshore SafetyDivision a small team has worked to raise theprofile of offshore Occupational Health issues,so that they receive proper consideration bothas part of routine operational work, and duringthe offshore installation design process. Wehave initiated a project to bring together gooddesign procedures and practice forOccupational Health issues as well asaddressing regulatory requirements. Thispaper describes the reasons for this work andintroduces the next stage, the production ofOccupational Health guidelines for offshoreinstallation designers. Review of Oil Industry Guidance and
Approach to OH and Design Recently OSD conducted a detailed review(HMSO, 1998) of how Occupational Health isconsidered during the design of offshoreinstallations. The aim of the review was toidentify opportunities and problems withcurrent design methods and to recommendways to improve consideration of occupational
health risks during design. A number ofOccupational Health specialists, engineers andproject staff from offshore design contractorsand operators were interviewed and theyexplained their experiences concerningOccupational Health requirements and theoffshore design process. Occupational Health risks associated with, forexample, noise, manual handling, hazardoussubstances, food contamination, radiation,general welfare should all be addressed duringthe design stage, well before any metal cuttingbegins. Basic guidance on some OccupationalHealth issues is provided in the 4th EditionGuidance on design, construction andcertification (HMSO, 1990) but the designguidance given for Occupational Health issuesis not comprehensive, and in some cases isoutdated. In some areas it has been supersededby Regulatory changes or more modern waysof thinking. The application of the Design andConstruction Regulations (1996) offshoreoffered a new opportunity to raiseOccupational Health on the agenda, but theRegulations and Guidance only address someof these issues in limited detail. The review concludes that the biggest singlefactor influencing the overall risk ofoccupational illness is the original design of aninstallation, rather than the procedures andhealth management systems implementedduring its life. Assessment, removal andcontrol of Occupational Health risks on the jobare important, but by then installationoperational staff are usually presented with a‘fait accompli’ and must make the best theycan out of the situation they face. Fundamentalchanges to a task may not be feasible orreasonably practicable at this stage of theoperational phase. Factors affecting occupational healthconsiderations in design: There are a number of factors that can affecthow well Occupational Health is considered inthe design of offshore installations. Theseinclude:

84
• Occupational Health is not seen as a coredesign topic and there is a general lack ofawareness of a problem by designers;
• Occupational Health requirements can bepoorly specified by the operator;
• There can be insufficient feedback fromprevious installations regardingoccupational health problems and theircauses on existing installations;
• Communication and co-operation withinoperating companies can be poor,contributing to lack of feedback;
• Budgetary constraints and conflicts (egCAPEX vs OPEX conflicts) maycompromise Occupational Healthconsideration during design;
• Poor communication between the operator,design contractor and other partiesinvolved in the design;
• Design reviews may not be conducted in away which focuses on OccupationalHealth risks;
• Delaying action on Occupational Healthdesign problems can leave themunresolved until too late in the designprocess;
• Conflict between design requirements cancompromise consideration of OccupationalHealth;
• Contractors, subcontractors and suppliersmay not provide adequate OccupationalHealth consideration;
• Design conservatism may hinderdevelopment of innovative solutions;
• Occupational Health specialists may notbe consulted, or not consulted earlyenough in the design process;
• Occupational Health controls may not beinstalled correctly during the fabricationand construction stage.
There are other issues that will influence thesepoints, one of the most important being thecontractual agreement between the operatorand design contractor, and the workingrelationship that develops during the contract.These issues are directly dependent on thefinancial and resource constraints imposed bythe contract and project.
‘Off the shelf’ solutions When new projects or redevelopment work arebeing considered in some situations there isunderstandably is a tendency to go for ‘off theshelf’ solutions whether for completeinstallations (drilling rigs) or for specificequipment such as pumps or compressors.
This has been illustrated by cases whereOccupational Health provisions, particularly inaccommodation areas, do not seem to haveprogressed much in some cases since earlydesigns. One recent example of anaccommodation re-design was almost a perfectcarbon copy of earlier sister installations. Thiscan lead to mistakes being repeated, and takeslittle or no account of previous problems andexperience. Many equipment suppliers have ‘off the shelf’design of equipment such as valves, pumps andcompressors and these may cost considerablyless than, for example, a ‘noise reduced’bespoke version, and have a much quickeravailability. The review indicated that thiswould more often be the automatic way ahead,rather than considering an alternative thatmight cost more in the short term, and initiallytake longer and more effort to procure, butwould be likely to bring long term benefits interms of reduced health risks.
Fast-tracking and CRINE These concepts for projects have among theirobjectives those of achieving fixed, often tighttimescales, and of removing any unnecessaryexpenditure. This may mean that tasks ofperceived lesser importance may be put back,or worst still, left to look after themselves, andwill tend to drive designers in the ‘off-the-shelf’ direction. This can easily result inOccupational Health topics getting pushed tothe back of the queue. Design contractors willbe constrained by what is in their contract, andthey will not get paid for what isn’t included.
The financing of developmentprojects
Exploration and development offshore ishugely expensive. The costs involved inexploration, production development andassociated infrastructure can be enormous. Butthe potential rewards are enormous and returnscan be expected for a considerable period frommost developments. Initial financial capitalrequired for a development is often huge, andall attempts are usually made to minimise this.When production is underway money may beavailable to spend to address issues that werenot properly considered at the design stage.This background encourages the tendency todelay the consideration of perceived non-essential items during initial planning anddesign until production has started and theremay be more time and money available to

85
address them. Occupational Health issuesoften fall into this cul-de-sac, in that they areparked until it is more convenient to deal withthem. This can be false economy becausesubsequently much time and effort can beconsumed dealing retrospectively withproblems at the operational stage that have notbeen properly addressed at the design stage. Alot of these issues clearly fall into theRegulatory framework and enforcement actionby HSE inspectors can occur. Another relevant factor is the way the industryhas been influenced by dramatic fluctuations inthe oil price, and has had to address ways ofworking to ensure that oil and gas can continueto be delivered to markets from marginalfields. This has not surprisingly led to costcontrols and manning reductions, which mustbe acknowledged. But the old proverb ‘a stitchin time saves nine’ is relevant here, andspending time and effort at the design stagewill pay dividends in the long term. So itshould be recognised that making economies inthe design phase will create problems in thefuture, and time and effort spent at the designstage will produce benefits in the longer term.Short term views over a 3-4 year period, reflectshort-term economics and will often lead togreater costs in the long term.
Why bother about OccupationalHealth at the design stage?
Legal requirements In the UK there is a legal framework thatrequires the risks to workers’ health and safetyto be reduced to as low as reasonablypracticable. A company must have a writtenHealth and Safety Policy outlining thecompany aims and objectives with respect tothe health and safety at work of employees andthe organisation and arrangements in place forimplementing that policy. It is essential thatHealth and Safety issues be addressed at thedesign stage of a project if they are to beproperly controlled during the life of theinstallation, and it is important to look at theHealth and Safety Policy to see how itaddresses design activities. The Securing Health Together (SHT) initiativeis very important here. The ComplianceProgramme (number 1) is important but in thecontext of issues we are discussing here theother Programmes are more directly relevant. Programme 2 of SHT aims to promote aculture of continuous improvement achieved
through collaboration, partnerships andinnovation. Promoting good physical andmental health at work is central to thisprogramme. There is a lot being done in theindustry through collaboration andpartnerships, not necessarily on OccupationalHealth though, but the basis is there to workon. Programme 3 of SHT aims to increaseknowledge of Occupational Health byimproving data processing methods, but thisassumes the data is there in the first place.This is an area we have been working on inOSD. Purchase and supply of equipment that ispotentially harmful to health is controlled bythe Supply of Machinery (Safety) Regulations1992. These Regulations require that relevantmachinery meets essential health and safetyrequirements. For example the supplier ofnoisy machinery must be able to show that it isdesigned and constructed so that risks fromnoise are reduced to the lowest level takingaccount of technical progress and the availablemeans of reducing noise. Health related civil compensation claims forOccupational Health issues such as Noise,HAVs, back injuries and stress are rising allthe time. All of these are real issues and theircauses can be found on most offshoreinstallations. Taking proper account of Occupational Healthissues at the design stage is the most effectiveway of dealing with them. The problem is thattime and resources are often limited. But it ismuch more cost effective to plan and integratemeasures at this stage than later in the life of aninstallation. But perhaps the most important reason forproperly addressing Occupational Health issuesis the well being of the workforce. Who arethe key people that any organisation dependson to get things done, keep production going,to deliver the goods? Investment in them,keeping them healthy (and happy) and in place,doing their job has got to be worth a lot to anycompany. In the short-term corner cutting mayapparently pay, but in the long term it is a falseeconomy. By reducing exposure to healthrisks, wear and tear on workers is reduced,their well-being is raised, and the likelihood ofan employee feeling valued will rise.

86
It may be a cliché to state that the workforce isthe most important asset of any company.However, an office or item of equipment canbe replaced relatively quickly, but if anemployee is lost either due to ill-health effects,or due to a move (particularly to a competitor),then finding a replacement and then bringingthem up to speed in the job is an expensive andtime consuming process. Investment in humanresources will bring benefits in these areas.
Recommendations to improveOccupational Health control during
design The Occupational Health design review made aseries of recommendations to improve theconsideration of Occupational Health duringoffshore installation design, and if these are putinto practice they will help to address the mainproblem areas that have been identified, whichare: • Lack of awareness by designers and
project managers of Occupational Healthissues and lack of effective controlsystems;
• Addressing Occupational Health too latein the design process;
• Lack of feedback on Occupational Healthaspects of previous installations;
• Poor communication between operationaland project teams.
To ensure adequate attention to OccupationalHealth an offshore installation designprogramme should include the following keyfeatures: • Commitment of design contractor and
operator senior management to improvedOccupational Health;
• Awareness of Occupational Health issueswithin the design team, and education ofengineers at the start of the project;
• Easy access to information onOccupational Health specifications, designguidelines and examples of successfulapplication;
• Use of structured design reviewprocedures and tools to capture potentialOccupational Health related designdefects;
• Early and active involvement ofoperational personnel in the designprocess;
• An expert in Occupational Health as a coremember of the design team;
• Active efforts to gather feedback fromprevious and similar installation designprojects.
To address these recommendations HSE havecommissioned production of design guidancefor Occupational Health issues and the firststage of this work has produced guidance fornoise, manual handling, and hazardousmaterials. This guidance will be tested on atleast one development in the UK sector of theNorth Sea, and will be reviewed using thefeedback. Next other Occupational Healthissues will be dealt with, and the guidelineswill then be published.
SUMMARY This paper outlines the background to theconsideration of Occupational Health issues inthe design of Offshore Installations, and raisessome of the problems and difficulties with thisprocess. The methodology being used byOffshore Safety Division to approach theseissues is outlined. The detail will be given inthe following presentation. On a wider front HSE and HSC are leading theSecuring Health Together initiatives and inScotland this is being jointly promoted with theScottish Executive. This is a governmentinitiative to reduce costs to the nation of peoplehaving time off work, or being unable to workdue to health problems. Programme 1 of Securing Health Togetheraims to improve laws concerning occupationalhealth compliance, including developing bestpractice, legislation support and lawenforcement. Priorities include revisingexisting or introducing new health relatedlegislation or guidance. Offshore Safety Divisions intervention strategyfor the next three years includes activities tosupport these aims.
References HMSO 1998 “Occupational Healthconsiderations in the design and constructionof Offshore Installations”, OffshoreTechnology Report – OTO 98 157,. HMSO 1990 Offshore installations: Guidanceon Design, Construction and Certification. (4th
Edition Guidance.) Dept of Energy.

87
The offshore installations and Wells (Designand Construction, etc) Regulations 1996. SI913.

88

89
DESIGNED-IN OCCUPATIONAL HEALTH RISKMANAGEMENT
Geoff Simpson, Amey Vectra, Melanie Clark, Amey Vectra and MrKevin O’Donnell, HSE
Introduction The process of design, build and operate foroffshore operations is extremely complex,extremely costly (with considerable financialpenalties for failure to meet contractualobligations) and involves a considerable time-frame. In addition, given the enormous capitalinvestment required in what is always, to adegree at least, a potentially risky exercise, it isnot surprising that major capital investmentand major builds are becoming morecommonly based on consortia than individualcompanies acting within their own resource. The extremely complex engineeringconsiderations involved have also created asituation where much of the design and buildoperations are contracted out to specialistorganisations. Moreover it is not uncommonfor the operation to be manned (wholly, or inpart) by contract staff. The net result is an extremely complex projectmanagement operation involving numerousorganisations many of which are involved foronly a limited period and, often, only within asingle phase of the Concept Design – FEED –Fabrication – Commissioning – Operation lifecycle. Keeping track of the engineering and the costis, in itself a major task and it is hardlysurprising if “peripheral” issues such asoccupational health risk management are“sidelined” either within the whole process orat one or other of the various interfacesbetween the stages. Although there can be considerable costimplications (arising from lost time,compensation etc.) from inadequateconsideration of occupational health riskmanagement even these, hard, businessconsiderations can become “lost” in the cleardemarcation maintained between CAPEX and
OPEX. Relatively small sums spent duringdesign and build (for example a slightly highercost for lower noise plant) are known tosignificantly reduce or even remove the longerterm costs arising from inadequateoccupational health risk management. Howeverthe position often arises where there theorganisation liable to the long-term costs hasno link with the organisation benefiting fromthe short-term savings or indeed may not evenbe involved at the point where the decision ismade to go for short-term savings even thoughthey are likely to predispose long-term cost. Introducing a systematic structured and rationalapproach to improving occupational health riskmanagement in this context is, therefore, notmerely about the provision of information butalso about the inclusion of the consideration ofoccupational health risk management as anintegral part of the design to operate life cycle. Unless this is achieved, the risk remains thateven ideal guidance incorporated at one pointwill be “lost” in the transition from phase tophase or will be “sacrificed” for (apparentlylegitimate) budgetary reasons at one phasewithout due consideration of the longer-termcost. It is essential therefore that any occupationalhealth risk management guidance providedmust come “ready packed” in a process whichwill allow/encourage its incorporation withinthe overall project management process toensure that the provision made at one stage willbe carried through to implementation at thenext. Even if such a process/procedure is provided,improvements in occupational health provisioncannot be guaranteed unless the contract brieffor each stage specifically includes the need todeliver best practice standards in occupationalhealth. No matter how good the information, howuseful and practical the process, there is a need

90
for overt corporate commitment to improvedoccupational health. An acceptance and sharedownership of the fact that detailedconsideration of and expenditure onoccupational health assurance in the early,design stages, is essential to deliver not only ahealthy workforce but also the significantoperating cost reductions that arise therefrom. This project was developed to provide bothguidance on three occupational health issues(i.e. manual handling, noise and COSHH) anda framework by which the guidance could besystematically considered as an integral part ofthe overall project management process.
Project Approach The brief given was to develop a new approachto the provision of occupational healthguidance to the off-shore oil and gas industrywhich would take cognisance of the differingneeds at the various stages in the life-cyclefrom Concept Design to Operation. Three topics were to act as case studies for thedevelopment of the approach:
• Manual handling• Noise• COSHH The study consisted of a series of discussionswith representatives of major oil and gascompanies, the Regulators and a number of oiland gas industry support companies to identify: • Current practice in integrating
occupational health risk management intothe Design-Operate life-cycle
• Perceived limitations on the introductionof improved occupational health riskmanagement
• Perceived motivators for the improvementof occupational health provision
• Examples of successful risk controlmeasures and procedures in relation to thethree case-study topics
The results of the discussions can besummarized under three headings as follows:
The cost of inadequate occupational healthassurance • increasing willingness for civil litigation• increasing value of compensation claims
• increasing frequency of ill-healthretirement
• extended periods of sickness absence The problems in providing occupational healthassurance • latency period for occupational ill-health• increasing frequency of consortia based
projects / contracting out• sidelining of occupational health• clear demarcation between CAPEX and
OPEX
Needs in moving toward a solution • generic action-based approach• based on existing good practice• compatible with familiar processes and
procedures• capable of integrating into standard
project management techniques This information was collated and used todevelop a Framework for the incorporation ofoccupational health risk management into thedesign-operation life cycle. A number ofconditions were established for the Frameworkas follows: • It must be a process rather than a
procedure. It must be a generic approachwhich can be tailored to any designprogramme (e.g. platform, rig, FPSU etc.)and any occupational health issue.
• It must be sufficiently structured to allowspecific activities and specificdecisions/actions at each of the stages inthe life cycle (e.g. Concept Design –FEED – Fabrication – Commissioning –Operation).
• It should be linked into an accepted modelof occupational health and safetymanagement (e.g. HS(G)65).
• It should be built around standard healthand safety practice compliant with currentregulations (e.g. risk assessmenttechniques).
• It should, ideally, not use processes andprocedures unfamiliar to the industry.
• It should be compatible with standardproject management techniques.
An example of the generic framework (in itsnoise application) is shown in Figure 1.

91
Concept Design FEED Fabrication C o m m issioning Operation
O u tput requirements for each part of the Design to Operat ion Life-Cycle
* Noise Pol icy - consider audi tory / non- auditory effects of noise - Regulatory - al locat ion of responsibi l i t ies
* CAPEX/procurement po l icy
* In i t ia te the development of an inventory of known/potent ia l no ise sources
* Inventory of previously successfu l noise contro l measures
* Source in format ion on noise e m ission levels for identi f ied equipment f rom di f ferent suppl iers
Act ions above to be formal lys igned-of f , documented as
transferred to FEED
* Review inventory o f known/potent ia l noise sources
* Speci fy a l l noise sources > 1st Act ion Level
* Opt imise locat ion to m inim ise exposure of personne l
* Deve lop no ise zone maps
* Assess pract ical i ty of prev iously successfu l contro l measures in current context
* Col la te comprehensive speci f icat ion of noise cont ro l measures
Act ions above to be formal lys igned-of f , documented astransferred to Fabr icat ion
* Moni tor and rev iew (us ing R isk Act ion Checkl ist f rom FEED outpu t ) purchase o f equ ipment aga inst speci f icat ion on noise levels etc.
* Moni tor and rev iew (us ing R isk Act ion Checkl ist f rom FEED output ) locat ion of no ise sources re zone mapping/emiss ion paths etc.
* Moni tor and rev iew (us ing R isk Act ion Checkl ist f rom FEED output) a l l addi t ional no ise cont ro l measures
Act ions above to be formal lys igned-of f , documented ast ransferred to Commiss ioning
* Review Risk Act ion Checkl is t
* Complete al l noise r isk assessments
* Conf i rm compl iance wi th Regulat ions
* Establ ish detai led Train ing Needs Analys is
* Select appropr ia te PPE
* Ensure demarcat ion o f no ise zones/hazard warn ings
Act ions to be formal ly s igned-off ,documented and t ransferred toOpera t ions
* Establ ish responsibi l i t ies
* Im p lem e n t training
* Issue PPE as requ i red
* Review/Audi t operat ional ef fect iveness of controls
* Estab l ish and implement Act ion Plan
Ident i fy potent ial noisesource(s) & in tegrate past
exper ience
Agreement o f Noise Pol icy &CAPEX / p rocurment
constraintsMon itorimplementat ion of
Conduct zone-based r isk assessments -no ise mapp ing
Identify al lno isezones -
markclear ly
Identi fycorrectP P Eaccord ingto
zones /exposu re
Identi fytrainingneeds -designcourse
s
A udit /
Speci fy where equ ipment is tobe posi t ioned on insta l lat ion
Create no ise zones /m a p s
Spec i fy zones a t 1s t and 2ndact ion leve l (dBA dependent on area)
Design / p rocure reduced
no ise emiss ion equ ipment
( remove / reduce)
Design/procure acoust ic
screening, hoods,barr iers,
PPE etc. ( reduce/protect )
Figure 1: An example of the generic framework (in this case applied to Noise Risk Management)
92
The basic principles of risk management wereapplied, i.e. remove, reduce, protect with theassumption that the earlier in the Design-Operate life-cycle that risk management isapplied the more likely that opportunities toremove or reduce risks will be viable. Theexamples below indicate the type of questionasked in relation to remove, reduce, protect: Remove• Is the operation / process essential?• Will other aspects of the process train, for
example, need to be adapted if selecteditem is removed?
• Does the benefit of reduced exposuremerit the potential costs?
Reduce
• Can the exposure level be reduced?• Are identified control measures
appropriate / effective?• Are there any risk management lessons
arising from past experience?• Are there any costs implications? Protect
• PPE, for example, should only beconsidered after all other alternatives havebeen exhausted and higher level protectionis in place
The Guidelines
Each of the three sets of model guidelinesproduced (noise, manual handling andCOSHH) begins with a listing of the relevantRegulations and an outline of the general stepsnecessary to achieve compliance with theRegulations. This is then followed by a sectioncovering the general issues to be considered.For example, in relation to noise there are moreconsiderations than the potential for hearingloss and, ideally, the influence of high noiselevel on communications, nuisance noise andenvironmental noise, should also beconsidered. Each of these is dealt with briefly,at a level which, hopefully, will ensure thatthey are considered, as shown below: • Communications – high noise levels can
detrimentally affect both verbal and non-verbal (e.g. warning signals)communication. Such disruption can havesafety implications or, potentially, increasestress levels through frustration andincreased error probability. Allowanceshould also be made for the fact that theuse of personal protection (e.g. hearing
defenders/inserts etc.) to protect againstpotential hearing loss can exacerbatecommunications difficulties.
• Nuisance Noise – high noise levels
impinging on, for example,accommodation areas can interrupt sleeppatterns, disrupt leisure activities etc. andthereby increase fatigue and stress. Thelong-term implications of such problemsare known to include increased accidentpotential and reduced general well being(potentially increasing sickness absence).
• Environmental Noise – offshore
operations by their nature can be subjectto very high levels of wind noise whichwill exacerbate each of the above,although little can be done to remove suchproblems they need consideration indesign, layout etc. to do whatever ispossible to reduce the effect.
This is followed by a section dealing with thecosts, the problem and the approach tosolution. This section is largely generic to allthree sets of guidelines as the problems and, indeed, the solutions to occupational healthproblems are, generally, common (almost)regardless of the particular hazard. Following these orientation sections, the actualguidelines begin with the emphasis placed onthe description of a design based riskmanagement process which can be tailored toany particular facility. The Guidance begins with a diagram whichsummaries the process as a whole. An exampleof this diagram, taken from the ManualHandling Guidelines is shown in Figure 2. Each major element in the design-to-operatelife cycle is then presented as individualsections covering: Concept Design FEED Fabrication Commissioning Operation Each section is divided into three sub-sections. The first deals with the Risk ManagementObjectives for that stage in the design-to-operate life cycle.

93
The second deals with the Risk ManagementProcess (the issues to be addressed to meet theabove objectives) for that stage in the design-to-operate life cycle. The third deals with the required RiskManagement Outcomes for that stage in thedesign-to-operate life cycle.
The outcomes from each stage become theinputs to the next. In this way it is possible toincorporate the noise risk management intostandard project management techniques.

94
Examine total supplies &equipment movement requirements
- create inventory
Specify mechanical handling needs
Design / procure mechanical handlingand/or transport equipment / systems
Specify non-mechanicalhandling operations
Specify those items which on firstprinciples (e.g. size, shape, weight)
need mechanical handling
Concept Design
Commissioning
Fabrication
FEED
Operation Audit / Review
Conduct task based risk assessments
Identify retrofitimprovements to design,
workplace orenvironment
Identify trainingneeds - design
courses
Idenitfymechanical
handling
Monitor implementation of action fromouptut of FEED
Agreement of Manual HandlingPolicy & CAPEX / procurment
constraints
Figure 2. Example of the Risk Management Process (in this case, Manual Handling)

95
The guidelines are deliberately designed to beconcise, providing a top-level route map whichcan be used to check-off what needs to be donewhen, and to confirm completion. Clearly, onsome designs, the work required at any onestage may be considerably greater than onother configurations however if each of theissues raised in the process is completed, andfollowed throughout the design process then itis likely that all the necessary steps to minimisenoise risk will have been accommodated withina few weeks of the start of operations thusensuring a high level of compliance. Additional information to expand on the pointsprovided in the guidance and some examples ofsuccessful noise risk management controlinitiatives are provided in the Appendices tothe Guidance. The COSHH guidelines have been used belowto provide an example of an Objectives section.The COSHH objectives at Concept Design aredivided into two steps: COSHH Objectives (Concept Design) STEP 1: The four primary considerations for STEP 1are shown in the box below: • Agreement on initial COSHH policy • Creation of an initial inventory of
hazardous substances across all aspects ofwork on the facility covering operation,maintenance and services
• Collation of existing and potentially
relevant COSHH assessments from allparticipating organisations
• Agreement on purchasing policy (e.g.
agreement not to enter any supplycontracts without receipt of relevantHazard or COSHH data sheets)
COSHH Objectives (Concept Design) STEP 2: The principle aim of STEP 2 is to start theprocess of converting the initial policy intopractice and aims to address the question ofwhether to:• Eliminate
• Substitute
• Engineering Control
The main questions that should be addressed atthis stage are: • Is the proposed installation likely to
present any potential risk to health fromthe use / storage / transportation and/ordisposal of controlled substances?
• Is any health problem in the industry
traceable to the use / storage /transportation and/or disposal ofcontrolled substances likely to be used?
• Can past experiences from participating
companies / organisations / industry beutilised to eliminate / substitute or controlthe identified risk?
• Does the proposed installation present any
new risks arising from theuse / storage / transportation and/ordisposal of controlled substances?
• How can the workforce be ‘best
protected’ from potential exposure(eliminate / substitute/control)?
An example of the Process description, in theform of a flowchart, which links in with Step 2above (from the COSHH guidelines dealingwith Concept Design), is shown in Figure 3. The final section within each of the Design-Operate phases is that detailing the expectedoutcomes from that phase. It is important tonote that, although presented in a general form,these outcomes are crucial in that they providethe input to the next phase. As such theybecome the critical information in the transitionfrom design phase to design phase, which is, asdescribed in the Introduction, the most likelyfailure point in developing a seamlessprogramme of effective occupational healthassurance which capitalises on all theopportunities available. On this basis the importance of building theoccupational health riskassessment/management assurance into theproject design process becomes critical,without such inclusion (and the associateddiscipline of signing-off and transferring-on),the probability of control action failing to findits way through into operation increasesconsiderably.

96
Cantask / operationbe eliminated?
Are controlmeasuresrequired?
Areavailable engineeringcontrols adequate/
effective?
Yes
No
Yes
Arealternate
engineering controlsavailable?
Monitoring / training/ PPE essential
No
Source newalternatives
Yes
Outcome of STEP 2 - Action forFEED
No
Outcome from STEP1
Cantask / operation besubstituted bylesslessLess
hazardoussubstance?
Canhazardoussubstancebe substituted?
Yes
Yes
Yes
No
No
No
If TLV's*available is likely exposure
acceptable?
Figure 3: An example of a Process description(taken from the Concept Design section of the COSHH guidelines)
An example of the expected outcomes from theFEED section of the Manual Handlingguidelines is presented below. Having worked through Concept Design,FEED, Fabrication, Commissioning andOperation, detailing the Objectives, Processand Outcomes of risk assessment/managementfor the particular topic, the guidelines thenprovide a series examples of how the processcould operate based on a series ofHAZOP/HAZID style exercises, again workingthrough each phase in the Design – Operate lifecycle. At the end of each of these sections aseries of examples, taken from the industry, ofgood occupational health design practice areprovided, not as a definitive listing of good
practice but simply as an indication that, goodrisk management action is feasible, phase byphase, during the design process. An example of the material presented in theapproach to implementation section of theManual Handling guidelines, dealing with theConcept Design phase is presented below.
HAZID 1 The first essential step is to establish linkswithin all collaborating parties in order tofreely share past experience on manualhandling hazards and risk control measuresused. It is also useful at this point to establishsimilar links with both cross-industry bodies

97
(such as the Step Change Programme) and theRegulators to seek information on theirexperience of best practice standards. • Assess practicality of selected mechanical
handling equipment in current context –initiate further examination whereproblems arise (where possible resolvebefore completion of FEED or documentfor future action)
• Review all operations / tasks for which
manual handling is unavoidable withregard to the possible provision ofmechanical handling aids
• Specify and review risk control measures • Optimise internal layout of storage areas /
loading bays etc. to reduce manualhandling requirements and/or to minimiserestricted movement andconstrained/awkward postures
• Specify operational and maintenance
activities that may presentmusculoskeletal risks beyond loadlifting/carriage
• Actions above to be formally signed-off,
documented and transferred toFabrication
Below are the four principal issues to beaddressed in HAZID 1: • Agreement on manual handling policy to
be used across the project up to andincluding operation
• Identification of potential manual handlingat-risk tasks/operations based on previousexperience
• Creation of an inventory of potential riskitems to be moved (supplies, replacementparts heavy/awkward manual operationsetc.)
• Agreement on the extent to whichpurchasing policy can be used toremove/reduce manual handling risk andtop-level specification of such policies.
Each of these issues is expanded briefly below:
Establishing Project Policy It is essential that a Manual Handling RiskManagement Policy is established at the onsetof the project to fully capitalise on the remove-
reduce-control hierarchy of best practice in riskmanagement. The Policy should include, as well as standardrequirements such as high level corporatecommitment to reducing manual handlinginjury etc., the establishment of a ManualHandling process/programme and themechanisms for signing-off actions andtransferring actions from one stage to the next.This is essential to ensure that the developmentof a comprehensive risk managementprogramme is maintained regardless of theprincipals involved at each stage. Identification of Potentially at-risk
operations/tasks The past experience of collaborating parties interms of previous manual handling risks onsimilar operations should be collated as a startpoint to identify an initial suite of potential riskmanagement requirements. For example,information can be obtained from: • Previous risk assessments conducted for
similar operations/tasks• Past sickness absence information relating
to musculoskeletal problems• Past injury/accident data involving manual
handling activities Where possible similar information should besought from cross-industry bodies and fromHSE. The latter should not only include cross-industry accident data but also informationfrom specific projects commissioned by them(for example HSE research project:‘Ergonomic Issues in the Design andOperation of FPSOs’ includes consideration ofpotential manual handling problems onFPSOs).
Creation of an inventory ofpotentially risky items to be moved HAZID 1 should initiate the process of creatinga complete schedule of items of equipment,supplies etc. (for both operational andmaintenance requirements) which will need tobe moved on the facility. The list should, initially, make no distinctionbetween items which could be moved manually(if necessary) and those which will clearlyrequire mechanical handling (e.g. major itemsof replacement plant). The reason that allshould be included at this stage is to ensure that

98
mechanical handling requirements are alsoconsidered systematically through the process.It is not uncommon for oversights to lead to theuse of sub-optimal mechanical handling aidswhich can often introduce additional,unforeseen, manual handling risks. It is highly unlikely that any list will becomplete at this stage, it will be refined as theprocess develops, however it is essential tostart as early as possible so as many potentialproblems can be considered during the designprocess.
Purchasing Policy The potential value of a purchasing policyaimed at reducing the manual handling risk ofan operation is often under-estimated. A policywhich requires the supplier to conform (wherepossible) to maximum packaged weights cansignificantly reduce risk. Similar benefits canbe obtained from maximum packaged size andthe nature of the outer packaging (in terms ofallowing a good grip etc.). Clearly there will be items (particularlyreplacement plant) where little can be done toreduce the size or weight etc. However even insome of these apparently “impossible”circumstances improvements can be made withsome imaginative forethought – for examplefitters occasionally need to partially stripcomponents to get them in situ. Thereforethere are potential operational benefits as wellas manual handling benefits to having themdelivered appropriately “semi-stripped”. Although it will not be possible to address suchspecific issues at this stage the establishment ofa purchasing policy (whereappropriate/feasible) will help to reduce themanual handling risk. The minimum output from HAZID 1 (once allthe actions have been signed-off) should be asfollows: • A draft Manual Handling Risk
Management Policy for the Operation(and, thereby, for the Project) agreed, as aworking draft, by all parties to the project.
• An initial listing of potentially at-riskoperations/tasks (from past experience).
• An initial listing of potentially risky itemsto be moved.
• A decision on the use of purchasingpolicies as an aid to the removal orreduction of risk.
These outputs from HAZID 1 become theinputs to HAZID 2.
HAZID 2 The purpose of HAZID 2 is to startestablishing the detailed suite of issues to beexamined fully during the remaining stages.The output from HAZID 1 should be used tofurther examine the following primary issues: • Collation of detailed listing of potentially
at-risk loads/operations/tasks –identification of major manual handlingsites and major manual transhipmentroutes.
• Assessment of utility and practicality ofpreviously used control measures in thenew context.
• Comparison of the above against ManualHandling Regulatory requirements toidentify risk reduction priorities.
• Detailed listing of equipment, plant,supplies requiring mechanical handlingfacilities for design specification andpurchase during FEED/Fabrication.
• Identify requirements for additional riskassessment in relation to “new” plant,equipment, systems where there is no pastexperience within participating companies.
• Develop outline risk control specificationsfor development during FEED.
Each of the above are expanded below: Detailed listing of potentially at-risk
loads/operations/tasks HAZID 1 will have identified candidatetasks/operations from accident/sicknessabsence data, from previous risk assessmentsetc. This base needs to be developed and putinto the new context. This should include thespecification of areas which will involve majormanual handling (including, for example,loading/unloading areas on deck and helipad,stores etc.) and the definition of start and endpoints of major manual handling transhipmentroutes. Early identification of both of theseissues will enable initial specifications to bedeveloped for use during FEED. For example: • consideration should be given to overall
storage requirements in relation to thelimits on the height of racking,
• major manual handling routes may needadditional consideration in relation to

99
floor surface, protection from the worst ofthe external environment,
• load/unload areas may need to includespace for turning loads and/orconsideration of the access to the routefrom the loading area to point ofuse/storage etc.,
• consideration will also need to be given tonon-normal operations such as patientevac and the need to manhandle a stretcherfrom almost any point on the facility to thehelipad.
• consideration will need to be given tospace requirements in manualtranshipment areas where the size of theload (in particular the length) may requireextra provision in relation to turning etc.
• where possible consideration should begiven to the minimal use of stairs on majormanual handling transhipment routes(negotiating stairs while carrying a load,especially if exposed to the weather canadd a significant further risk) – althoughavoiding stairs completely will beimpossible unless the issue is raised littlethought will be given to alternatives.
Utility and practicality of previously
used control measures Previous operations will have used a widerange of manual handling risk controlmeasures, some of which may be equallyapplicable in the new context. Care should betaken however to avoid the assumption thatthey will be as effective without consideringtheir use in the new context. Where previous control measures do appearvalid then there may be requirements whichneed to be fed forward into the detailed design.For example, stair climbing stack trolleys mayneed more lateral space than is normallyallowed on walkways, stairs etc. They willcertainly need more turning space than wouldbe needed by an operator. Other mechanical aids, e.g. a scissor lift usedfor unloading from helicopters, may needconsiderable for and aft space for positioningetc. Other mechanical handling aids mayrequire minimal clearances or may needtemporary anchoring – all such considerationsare best dealt with during design rather than asretrofits.
Clearly, given the nature of off-shoreoperations involving everything from theoperation and maintenance of often heavy,bulky and awkward equipment through to the“everyday” chores of housing and feeding thecrew, a large number of potential manualhandling risks are likely to emerge. It maymake operational sense to prioritise riskmitigation action to ensure that the initial focusis on the higher risk areas and that potentialrisks do not get overlooked during theextremely complex process of moving throughthe design to operation process. The secret in adopting a practical approach tomanual handling risk assessment/prioritisationis to start with, as is emphasised in theRegulations, a systems based approach. Theimportance of this is that it ensures that the riskfactors are dealt with at an appropriate level.For example, if it has not been possible at theearly stages to reduce the weight or size of thematerial to be handled (e.g. by purchasingpolicy or by agreement with suppliers onpackaged weight of material) then there is littlewhich can be done at the task level – such riskfactors may have to be taken as a given factand other aspects of the risk equationaddressed to find practical means of riskmitigation. If nothing can be done about theweight of the load early in the risk managementprogramme, it must be considered during taskbased risk assessment. Some possibilities mayemerge – for example, in dealing with bulkmaterial only handling the amount that isrequired for the job in hand. In othercircumstances there may be nothing that can bedone as will be likely in relation to componentweights during maintenance activities In thiscase it is necessary to consider other aspects ofthe task-load-environment-personal factors forpossible avenues for mitigation. Manipulation at the task level should howeveronly be considered when all other avenues todeal with the issue have been shown to beimpractical. To establish an initial risk prioritisation it willbe necessary to undertake some early manualhandling risk assessments covering classic riskassessment issues such as the risk factors, thefrequency of exposure and the potentialseverity of injury. This may seem daunting atsuch an early stage however simple buteffective approaches are possible. An initial assessment need not cover all of thetask-load-environment-personal factors but
Identify risk reduction priorities

Primary Risk Factors
1 low
2
3
4
5
high Keeping the object close to the body Bending Twisting
Lifting above shoulders
Co-ordination
Environment Carrying, moving
One or more risk factors scoring 4 or 5 in theabove table will merit a detailed riskassessment of that task. This will involveestimation of the frequency of the operationand the severity of the likely injuries. Tocalculate where the priority focus should be, itis necessary to consider both the severity ofrisk severity (obtained, for example, fromaccident/sickness absence data) and the likelyfrequency of occurrence (using for examplewith information obtained during HAZID 1).There are a number of techniques for achievingthis, however when combining severity andfrequency (likelihood) into a subject risk“score” many approaches assign a value to
each (e.g. on a 1 – 6 scale) and then take theproduct of the two. This is potentiallymisleading, as the subjective numbers used todescribe the scale points have no mathematicalmeaning. The result is that if 1 = lowlikelihood/severity and 6 = high then 1 x 6gives the same risk “score” as 6 x 1. On thisbasis then a low likelihood of a major severityhas the same risk “value” as the high likelihoodof a minor severity. One of the best ways to avoid this is to use amatrix as shown below:
Likelihood
Severity 1 2 3 4 5 6
1 1 2 4 7 11 16
2 3 5 8 12 17 22
3 6 9 13 18 23 27
4 10 14 19 24 28 31
5 15 20 25 29 32 34
6 21 26 30 33 35 36
In this way each combination of likelihood andseverity has a unique “score” and the potentialconfusion described above is avoided. To makethe situation easier and provide an initialprioritisation the matrix can be blocked off inpriority bands ( see below). The number of scale points or actualboundaries used to describe the priority bandsis a matter of preference – there is no right orwrong, the important point is the creation of a
rational and practical system which can be usedeasily with available or, at least, accessibledata.
100
rather focus on a smaller suite of wellestablished influential factors judged against a
simple subjective scale as shown below:

101
Likelihood
Severity 1 2 3 4 5 6
1 1 2 4 7 11 16
2 3 5 8 12 17 22
3 6 9 13 18 23 27
4 10 14 19 24 28 31
5 15 20 25 29 32 34
6 21 26 30 33 35 36
High Priority
Medium Priority
Low Priority
Detailed listing of equipment, plant,
supplies requiring mechanicalhandling facilities
This action is self-explanatory however theimportance in identifying the needs early in theprocess should not be under-estimated.Without such early intervention it is likely thatthe adequacy of provision will decrease and thecost of installation and/or the need forexpensive modification will increase. Identify requirements for new risk
assessment in relation to plant,equipment, systems
If “new” plant, equipment, systems or indeedoperations or layouts are envisaged where thereis no operational experience held by any of theparticipating companies it will be necessary tocharge someone (as part of the HAZID 2actions) to undertake an initial desk-top riskassessment which can be checked, refined anddeveloped as the design hardens during theremaining stages of the process.
Develop outline risk controlspecifications for development
during FEED This step is essentially a collation of theoutputs from HAZIDs 1 and 2 and forms theoutline (or initial) risk control specification
used to develop the detailed design duringFEED.
Further Development. It is the intention of HSE to trail the threemodules during a major design process toassess the potential of the approach in practice.Should these trails suggest benefits will arisethen the likelihood is that further modules,dealing with other occupational health issueswill be developed along similar lines.
Acknowledgements. The authors would like to express their thanksto the many people in the industry, from a widerange of companies, who through theirwillingness to discuss their actions andconcerns in relation to occupational healthassurance, helped considerably in framing theapproach presented here QUESTIONS AND ANSWERS SESSION
Comment - Geoff Simpson, Amey Vectra As third author of this paper I feel obliged tosay something, it’s not a question, just acomment. In Mel’s section in particular it wasextremely difficult for us to get a real picture ofthe guidance on slides especially as someone inour parent organisation decided to use a styleguide which doesn’t allow us to use portraitslides and made it a lot more difficult.

102
We have got hard copies of the draft guidancewith us, so if anybody would like to see what itreally looks like, as opposed to how we had toshoehorn it on the slides, then please just giveeither Mel or me a shout and we’ll show youwhat it looks like. Question – Fiona Davies, AEA TechnologyEnvironment When you are actually at the stage of havingthe guidance agreed and to be made available,what form are you thinking of having itavailable in. Conventional reporting format orpotentially the software tool? We were talkingabout the problem of trying to capture it onscreen, but it does actually look like somethingI could imagine being web-based and workingthrough the stages and that would actuallyenforce the carrying through from each stage tothe next. Answer – Mr Kevin O’Donnell, HSE I think it would have to be available in allcommonly used media. Personally I would liketo see it available on a CD-ROM so that youare not carrying round a considerable amountof paper work at any one time. It would fitwith modern working practices and be veryflexible to use. It is also interesting to hear thatthe Norwegian standards are available on theinternet as well, so I think we’ve got toconsider all ways of using it. I wouldn’t saywe’d set a hard and fast way, saying thatpeople must use it this way. They can use theprinciples and adapt them to their own systems.I don’t want to impose changes on the existingcompany systems just for the sake of it. Question – Mr Graham Cowling, AcousticTechnology Ltd We’ve worked on designs both on theNorwegian method using the work areaenvironments chart and on the UK systemswhere basically we do a lot of the engineeredpost build stage. One of the elements of theNorwegian system is the systematic followingup of the gradual meeting of various noiselimits which actually have a legal significancein the Norwegian sector. Those limits are thereto be met. The requirement effectively is toapply for a deviation if you can’t meet thoselimits. In the UK system though, which isproposed to be based on a design processwhich has documentation at various stages, isthere an element where the HSE are likely tosay no, we don’t like what’s going on with thisdesign? Answer – Mr Kevin O’Donnell, HSE
There is not a specific element as suchGraham. But the way regulations are now, wecan say something equivalent to that. Theguidance is based on the regulations as they arenow. Having said that, the Securing HealthTogether compliance programme does say‘examine existing legislation to see that it’ssatisfactory’ and I’m sure that will be a by-product of this process and other processes.The messages and lessons that we may be ableto learn from other areas we’ll look at. Question - Chris Freeman, PhillipsPetroleum You were talking about the transfer ofexperience and knowledge from one project toanother. You mention the idea of usingoperational personnel who’ve worked on oneproject to review new designs but implied thatyou didn’t feel that was a particularlysatisfactory method. Are you thinking of anyother methods? Answer - Mr Kevin O’Donnell, HSE I hope I didn’t give you the wrong impression.I think it’s a very valid method but only as partof the overall process, part of looking at healthincidence data as well as using operationalexperience. I think it is a very valid methodusing operator experience, but not the onlymethod. It should be supplemented by others. Comment - Dr Ron Gardner, HSE Can I just add a comment to that since I raiseda question earlier. Trevor Kletz on the majorhazards side always used to say industrydoesn’t have a corporate memory and that’s athing that always concerned me about thedesign side. Bringing in operational people asKevin says is only part of it, because they onlyhave a partial experience of their particulararea. I think wherever feasible what I want tosomehow see is the experience of the wholedesign team being captured. We need to retaincorporate memory between design jobs anddesign teams. Comment – Geoff Simpson, Amey Vectra What we’ve tried to do in the guidelines thatwe’ve produced is that as part of the process,part of the definition of the objectives and theprocesses of each stage, there is capture ofsuccessful control measures that have beenused before, and control measures that havebeen used before which haven’t provedsuccessful. So, what we’ve created is a processthat will allow that collective memory to becaptured. Whether of course it is captureddepends upon the people that are actually

103
operating the system and there’s no way we cango much further than that. But the ‘aidememoire’ is now built into the process if youlike.

104

105
THE DEVELOPMENT OF A HUMAN FACTORS ENGINEERINGSTRATEGY IN PETROCHEMICAL ENGINEERING AND
PROJECTS
PART 1
Mr Harrie J T Rensink, Group Advisor Human Factors Engineering,Shell International Health Services, The Hague and Martin E J van
Uden, Co-ordinating Process Engineer, Shell InternationalChemicals, Amsterdam
Summary Although the human-machine interface inpetrochemical manufacturing projects hasalways been considered to be an integral partof a sound engineering design, many misfits inoperability and maintainability have beenexperienced after implementation. Based on that experience a vision and policywas developed by Technical and OccupationalHealth management at Shell NederlandRefinery Pernis and Shell NederlandChemicals Moerdijk resulting in a humanfactors engineering strategy integrated in theearly development phases of the businessprocess project preparation and execution. The benefits of this strategy are identified bothin business terms (economics) and in workingconditions; e.g. improvement of Health, Safetyand Environmental (HSE) aspects. Based onhistorical data it is now identified that for atypical $ 400 million petrochemical project thestrategy can result in a reduction of : • 0.25 - 5 % of capital expenditure
(CAPEX),• 1 - 10 % of engineering hours and• 3 - 6 % of life-cycle costs of facilities
(OPEX). This paper consists of two parts. Part 1describes the main drivers of the developmentof a human factors strategy within Shell Pernisand Moerdijk organisations. Part 2 will give a detailed view on the actualmanagement of human factors in petrochemicalprojects and will evaluate the costs and benefitsbased on the experience of implementation
human factors engineering in smaller andlarger petrochemical projects.
Introduction Although the human-machine interface in newpetrochemical manufacturing projects wasconsidered to be an integral part of soundengineering design, many misfits in operabilityand maintainability have been experiencedafter implementation. Engineers and constructors have to deal withmany (technical, legal HSE, etc.) constraintsduring their work, one of the constraints beingthe human-machine interface. Technical designers however:• are by nature more interested in the
technical performance of their products,• do not have to operate or maintain the
facility/installation after implementationand are therefore unconsciously lessmotivated to take care of the human-machine interface,
• have insufficient knowledge of people’sphysical and mental behaviour.
For these reasons, application of human factorsand ergonomic principles is 'easily forgotten'when decisions are made during design.
In 1992 the Technical management andOccupational Health management at ShellNederland Refinery and Chemical complex atPernis and Moerdijk set up an ErgonomicsSteering Committee (STER) based on adefined policy. Further a multi-disciplinaryworking group, reporting to STER, wasinstalled to improve the implementation ofergonomics in projects as well as to train andgive information about ergonomics to projectstaff and engineering contractors. At Pernis and

106
Moerdijk, the goal is to integrate humancapabilities in the design of work systems, likeproduction facilities, workshops, laboratoriesand offices. Systematically integrated in allproject and design phases, human factorsengineering principles results in an effective,safe and healthy functioning of people. Thebenefits are identified both in business terms(economics) and in working conditions (HSEaspects), resulting in a reduction of life cyclecosts of facilities.
Why Human Factors Engineering
At Pernis and Moerdijk sites the ergonomicsworking group (WEER) listed a number ofmaintenance misfits, the so-called Ergonomics"Top Ten". Inefficiencies in the field ofmaterial handling, vertical pump lay-out,hoisting equipment and valve operations wereidentified. Results of task analysis studiesrevealed problems in control room buildingswith regard to the lay-out of the panel room,noise, lighting and console lay-out. In the fieldof 'human/computer interaction',inconsistencies were found in the coding ofinformation, as well as a lack of standardisationin the design of the graphical displays.
Also pre-start-up and post implementationreviews indicated efficiency problems as theresult of sub optimal human machine interfacedesign. E.g. in the Pernis HYCON plant (Shell1986) many pre-start-up auditrecommendations focused on improvement ofoperability, accessibility and maintainability. Itwas concluded that during engineering phasesopportunities could have been taken tooptimise the design without increased capitalexpenditure in many cases. Even in recent postimplementation reviews of some internationalprojects the same conclusions were drawn.After start-up of a brand new refinery in theFar East in 1996 the following statement isillustrative: “Basic concept is not anoperationally friendly machine”.
Definition of Human FactorsEngineering
Human factors engineering is an appliedscience aiming at the integration of knowledgeof human capabilities and restraints withproduct design, workplaces and installations inorder to improve the efficient, comfortable,safe and healthy functioning of people. This is
the current definition at Shell Pernis based onthe ISO-6385 standard: ‘Ergonomic principlesin the design of worksystems’ [ISO, 1983].This ISO-standard describes the starting pointsand applications of human factors engineeringprinciples in the design of worksystems. Beforedefining the scope of human factorsengineering it is necessary to discussterminology. Human factors engineering andergonomics were originally two fields of study,which have evolved into one.
Human factors engineers and ergonomists usethe same techniques but the origin of the twofields differ:• Human factors traditionally emerged from
a military background and concentrates onhuman performance- i.e. the effect humanshave on their working environment.
• Ergonomics focuses on the safety andcomfort of workers- i.e. the effect theworking environment has on humans.
In practice these two disciplines areinseparable and they have therefore evolvedinto one single discipline. For this reason theterms ‘human factors’ and ‘ergonomics’ tend tobe used synonymously in this paper. In other businesses, for instance InformationTechnology, Human factors engineering is alsocalled ‘Usability engineering’ or ‘User centreddesign’. Human factors engineering is above all aimedat optimising the part of a work system calledHuman machine Interface (HMI). In particular,it is concerned with cognitive (information andknowledge transfer) and physical interactionsthat occur at the interface of the human withtechnical systems. Also environmental factorssuch as noise, light, climate, vibrations andorganisational aspects may play an importantrole designing an optimal human machineinterface. In the design of work systems and work places,know-how of various sources is being used,such as psychology, physiology, anatomy,labour-organisations, information-transfer andknowledge about environmental factors (seefigure 1). To effectively apply ergonomics,know-how is also necessary of designtechniques, project management and business-economics (investment decisions).

107
Figure 1: Knowledge areas of Human factors engineering Causes of Resistance Against Human
Factors Engineering There is a wealth of literature describingergonomic research dedicated to the correctionof existing problems. These problems arose asa result of lack of attention for the user in thedesign. Few literature references can be founddescribing human factors engineering as anintegral part of the total engineering process.By paying attention to the capabilities andconstraints of the user during the conceptualdesign phase, problems during life cycle of afacility have been be prevented. As will beshown later, the efforts and costs by followingthis philosophy are much smaller than in thecorrective mode. We may ask ourselves why preventive humanfactors engineering is not always selected overcurative human factors engineering. A numberof arguments for this will be given in thefollowing sections.
• Lack of competence of designtechnicians
Probably one of the most important reasons forthis is that designers of machines and toolsoften have received only technical education.By nature, technicians are more interested inthe technology involved in their design than theuser-friendliness. As the designer usually willnot work with or maintain the machines andtools designed, he will not be confronted withthe shortcomings. Therefore, a designer oftenhardly realises the consequences of certaindesign decisions have for the users. This isamplified by having insufficient knowledge ofpeople’s physical and mental behaviour. • Lack of focus of the Human factors
engineering discipline Not only technicians, but also human factorsengineers and ergonomists are to blame withrespect to the low human factors input indesign and engineering. Too much effort is putin research identifying and solving existingproblems. Ergonomists should strive toconvince ‘champions’ in the organisation of the

108
added value of an ergonomically designedwork systems or products. This may be doneby transferring knowledge about human factorsprinciples and ‘best practices’ to projectmanagers, construction managers and linemanagers of organisations. • Lack of ‘fit for purpose’ standards and
guidelines Technicians hardly have knowledge of thephysical and mental behaviour of people,necessary for designing a proper humanmachine interface. The existing ISO-standards[ISO, 1983] and technical approaches - aimedat assisting the technicians - are poor. Thereason is that the level of these ISO-standardsis rather abstract. Therefore the guidelines donot have sufficient added value to beincorporated in a list of technical designspecifications. This situation does not promotethe integration of human factors in design.Ergonomists working in the field shouldundertake action to ‘translate’ the ergonomicstandards so that they can be used bytechnicians. This “translation” should befocused at frequently occurring operational andmaintenance problems. To this extent, ananalysis of frequently occurring problems maybe useful, however existing rules andregulations of governing bodies may help to setpriorities, too. • Image problem Another reason for human factors engineeringnot being fully exploited in new designs ofproduction facilities is due to the fact that linemanagement, and people in general, do notwell understand the art of ergonomicengineering and still relating it to the design oftables and chairs. People underestimate thepower of application of human factorsprinciples in the design of production-facilities.There is a clear image-problem! • Awareness problem Another serious problem related to a successfulimplementation is that line management oftenconsiders of human factors as a kind of luxurywith little added value. It is sometimesaddressed in terms like “the ribbon on a giftparcel’ or ‘we do this only to satisfy the plantpersonnel’s wishes’. In projects which do nothave ergonomic principles integrated duringthe front end loading we often see that endusers criteria are being developed duringdetailed engineering, thereby frustrating projectmanagers and as a result unwanted scopechanges and extra investments. Theseexperiences do enforce the idea of human
factors implementation being costly and havinga negative effect on project schedule. • An overestimate of the designers own
competence Research shows [Slappendel, 1994] that amajority of the designers think that the intuitiveapplication of ergonomics is possible (thecommon sense approach). Results of pre-start-up reviews of petrochemical facilitiesdemonstrate that this is a misconception. Often,a multi-disciplinary task force performs such areview prior to the start up of a petrochemicalfacility as a final check on safety, operabilityand maintainability. In particular the lack ofstructural application of ergonomics in thedesign may be regarded as the cause of pooroperability of some new facilities [Shell,1986].
Success Factors for theDevelopment of a Human Factors
Engineering Strategy After many years of experience withimplementing human factors in design andengineering of petro chemical facilities it hasbeen identified that a number of key factorsenabling the successful and effectiveimplementation of human factors in anengineering project need to be fulfilled. • Realising management commitment One of the most important conditions is the(active) support and involvement of line andproject management. Without this support mostinitiatives are doomed to fail. Involvementshould not only come from top management,but also from middle management and projectleaders. Management support can be obtainedor increased by reports about demonstrationprojects. These demonstration projects shouldclearly show the benefits of the human factorsdesign strategy. The key-figures in anorganisation (managers of design-, productionand maintenance departments, occupationalhealth service) should be fully informed aboutthe of ergonomic integrated design andengineering. It is important that they knowwere to obtain knowledge about human factorsin order to be able to identify problems and todeal with them in an adequate manner. • Providing a clear vision statement;
priority to new plants An organisation should give priority to theintegrated implementation of human factors innew construction projects over the solution ofexisting problems [Rensink, van Eijsden,

109
1991). This is supported by economic analyses.A number of so-called post-implementationinvestigations showed that in the first few yearsafter starting up a factory often problems occurwith the lay-out and operation of equipmenthaving a negative effect on the efficiency of thecompany as well as on the health and safety ofthe employees. These problems aresubsequently cured at high cost or remain toexist throughout the entire life cycle of theplant, with all negative consequences. The plea to give priority to new constructionsis also based on the vision that specificationsfor new plants will result in simple andapplicable guidelines and tools for assessmentof existing plants. • Making available practical tools and
techniques Human factors engineering offers a number ofdesign methods taking user demands intoaccount in a structural way. An example of thisis shown in literature as the Doering approach.However, this method is rather complex andtheoretical and not designed to function inpetrochemical design and engineering.Therefore, at Shell Pernis and Moerdijk, anumber of ‘fit for purpose’ engineering andmanagement tools were developed that arespecifically aimed at the design ofpetrochemical plants. • Ensuring structural input of end users
in projects Recent publications report positively aboutprojects applying the principle of so-called ‘“participative ergonomics”. This approachvalues the structural participation of (end)usersduring all phases of improvement orconstruction projects. This multi-disciplinaryapproach uses knowledge from allorganisational layers to realise an innovation. In the international literature the participativeapproach is sometimes called ‘sharingergonomics’. Some ergonomic scientists rejectthis approach as it is considered to be ‘givingaway the art of ergonomics’. This defensiveattitude is counteracted by the statement:‘ergonomics is nothing unless it is applied’[Wilson, 1994]. This contradicting vision ofWilson supports participative ergonomics as aneffective strategy for implementation. Shell Pernis and Moerdijk vision also meansthat participative ergonomics is applied. Toexplicitly use the practical experience of theworkforce during design and engineering an
ergonomics platform was founded in whichworkfloor employees from operations,maintenance and various engineeringdisciplines work together in order to definenorms, standards and tools to help designers toapply plant user’s experience. Experience so far shows that the participativeergonomics approach has led to the necessarysupport within the Shell Pernis and Moerdijkorganisation. The understanding by bothmiddle-management as well as the end users ofthe importance of ergonomics in business hasincreased significantly. • Management of ergonomics in the
design process To manage the integration of human factors inthe design process efficiently, a number ofspecific conditions have to be met: • In the conceptual phase of a design it is
necessary to conduct an analysis of alltasks that have to be performed (operation,maintenance, inspection, transport,cleaning etc.) in the future plant. HMI'sidentified as ‘critical’ should be analysedand translated in ‘user demands’. Thesespecifications should be part of the ‘basisof design’ document of a project. The userdemands should meet equal treatment andimpact as technical and otherspecifications during the design andproject phases. This is a difficult tasksince designers and builders already meeta wide variety of conditions, such aseconomical, technical, legal, safety, healthand environmental demands. Adding enduser demands will however balance theseconditions and lead to a more effectivedesign.
• The technical disciplines, vendors andsubcontractors should all work togetherand concurrently to guarantee theincorporation of human factors in thedesign.
• Experiences of the group of end-usersshould be taken into account.
A design and project approach in which theabove conditions are taken into account andanchored in the procedures of the QualityManagement System will result in a designguaranteeing an efficient task-performance.This will be visible in improvements in allrelated areas.

110
Management of Human FactorsEngineering in Projects
It was learned that it is important to addresshuman factors engineering right from theconceptual phase of the project. In Pernis thisexperience resulted in the development of astandard procedure, the Front End ErgonomicEvaluation Matrix (FEEEM ) designanalysis. This design analysis identifiesoperational and maintenance tasks at an earlystage of a project, that is during the feasibilityand/or definition phase, and is the 'motor' for asound ergonomic design. The FEEEM isexecuted by a multi-disciplinary team and theresults, i.e. potential bottlenecks andrecommendations on human-machine
Interfaces forms part of the Basis of Design(BOD).
At this moment, based on further experiencewith several smaller and larger projects, thedevelopment of, the so-called ErgonomicsManagement and Information System SNR/C(EMIS), is ongoing. The procedures, designtools, standards and guidelines within thesystem are considered to be necessary forassuring a proper human factors design. TheEMIS scheme is shown schematically intable 1.
Table 1: Ergonomic Management & Information System (EMIS )
Guideline on the implementation of ergonomics in engineering andprojects
Informationand training
tools
Projectmanagement
& Qualitytools
Engineeringtools
Procurementmanagement
tools
Constructionmanagement
tools
Necessity of the Quantification ofthe Benefits of Human Factors
Engineering: The Development of aCost Benefit Model
In many cases, ergonomics is incorrectlyregarded as an additional cost to the design.The benefits offered by ergonomics are notalways clear to all. A complication in thisrespect is that not all benefits can be directlyexpressed as tangible financial savings. Manybenefits are intangible and not easy to use tojustify an ergonomic approach.
In the above we have seen that it is imperativeto convince ‘champions’ within theorganisation of the benefits of ergonomicallydesign. The better the arguments, the moreeffective one can carry this message. Sincemany decisions in business are based on
economical facts, we will now focus on thisquestion.
At Shell Netherlands Refinery and Chemicalcomplex in Pernis and Moerdijk the benefits ofefficient design as a result of the application ofhuman factors have been demonstrated in anumber of projects [Rensink 1992, Rensink1994, WEER 1995]. Based on many casestudies it was obvious that application ofergonomics may realise considerable savingson the cost of production and maintenance incombination with increased safety andreduction of physical strain to workers. Theadvantages for the employees are fewer healthcomplaints and workplaces which are moresafe and comfortable. For the company thebenefits will be expressed in terms of increasedefficiency and reliability leading to reduction inlife-cycle costs. [Rensink, 1996].
These case studies have led to the opinion thatthe application of ergonomics may reduce life-cycle costs of petrochemical installations asshown in figure 2.
To support this opinion Shell NetherlandsRefinery and Chemical complex Pernis and
Moerdijk, in co-operation with the NAM hasrecently developed a cost-benefit model(Rensink, van Uden, Aartsma, van Eijsden,Dekker 1996). One of the initial starting pointsof developing a cost benefit model was forawareness purposes. However it is nowexperienced that the model is of value not only

111
during project preparation, but also during theexecution of projects. The goal of the methodis to visualise the potential benefits ofergonomically design and to serve as an aid toprocess technicians, human factors engineers
and project managers who have to takedecisions about the design in new constructionor improvement projects.
Figure 2 Cash flow during the life cycle of a petrochemical installation comparing anergonomically and a non-ergonomically design. Note : for trend indications only [Shell, 1995].
Similar to the description of the case studies adistinction is made in the cost-benefit modelbetween tangible and intangible economicalbenefits of ergonomics. A number of mainareas are acknowledged in the model withpotential exploitation benefits by application ofergonomics. These main areas have been listedtogether with examples of these benefits asshown in table 2.
In most case studies, the economically tangibleexploitation benefits can be calculated easilyfrom reduction in time or material that wasspent and loss reduction. These benefits shouldfit the return-on-investment policy of thecompany. If not, the criteria may be relaxeddepending on the impact of the economicallyintangible risk or danger.
With regard to the economically intangiblebenefits - to be found mostly in the main areasof health, safety and environment - the riskmust be determined with respect to thefrequency, the number of people involved andthe consequences for individuals, environmentor hardware. In the case of non-feasibility ofthe investment, the risk should be avoidedsome other way. This may be done by non-technical means such as instructions,requirements or procedures.
In part 2 of this paper the use of the costbenefit model and the evaluation of humanfactors implementation in projects will bediscussed in more detail.

112
Table 2. Benefits resulting from the application of human factors engineering by main area
Main area Example of possible savings
1. Operations less waste
decrease in number of failures
increased productivity
2. Maintenance less labour
less waiting
less material necessary
less administration
improved quality of maintenance
3. Reliability less mistakes
less machine failures
4. Health Reduced risk of accidents
Increased motivation
less sick leave
less physical load
5. Safety better visibility
Improved safety
Reduced risk of accidents
Reduced risk of stumbling
6. Environment less waste
7. Legislation Comply to the legal rules
Comply to the legal rules
8. Labour Reduction of labour expenses
Improved functioning of personnel
Reduced sick leave fees
Conclusions and Recommendations
The profit of a production system is largelydetermined by the people working in it. Tooptimise the performance of these people,human capabilities and technical equipmentshould be fully compatible. It is thereforeimperative that in addition to financial andtechnical aspects, human factors are also takeninto account in the design of a productionsystem.
Many work situations currently considered tobe problematic were caused by insufficientattention for the design of Human machineinterfaces. Such problems can be prevented bystructurally applying ergonomics in the design.
It is essential to define and analyse the criticalhuman machine interface in the conceptualphase of the design. To assure these proceduresproperly, a quality system is needed.
The challenge for human factor engineers andergonomists within large organisations wouldbe to motivate ‘key people’ in projectmanagement to implement human factors in thebusiness process preparation and execution ofprojects. A human factors policy and qualityassurance program is needed to support this.This means that fit for purpose engineeringtools and techniques have to be developed andtraining of the various target groups plays anessential role. Self management of humanfactors issues should be one of the drivers.

113
Vendors and equipment suppliers should beinformed about the significance of taking user-demand structurally into consideration duringthe development of a product. A simple (3 DCAD) prototype or mock-up to be used in thetest phase by future users may offer aninexpensive and effective method to alleviatethe reduction of user-unfriendly designs. Inprioritising solutions to potential problems it isrecommended to focus on deleting future tasksthereby reducing capital expenditure as well aslife cycle costs. Whenever a decision oninvestment in ergonomics is to be taken, theseaspects should be considered explicitly.
Acknowledgement
The authors are indebted to the management ofShell Nederland Refinery and ChemicalsPernis B.V. to be given the opportunity to writethis paper.
References
International Standard Organisation,Ergonomic principles in the design of worksystems, ISO standard 6385, 1983.
Rensink, H.J.T., Cost/benefit study VALLAcrane, Shell Nederland Refinery, Pernis, 1994.
Rensink, H.J.T. and Van Uden, M.E.J.,Management information on theimplementation of ergonomics in SNR/Cengineering and projects, document
EMIS.MG1, Technical Projects Department(TAP) Shell Nederland Refinery, Pernis, 1996.
Rensink, H.J.T., C. van Eijsden,Implementation of ergonomics, ShellNederland Refinery, Pernis, 1991.
Rensink, H.J.T., Ergonomics at Shell Pernis,part 2, Costs and benefits of ergonomicactivities, Shell, Pernis, 1992.
Rensink, H.J.T., M.E.J. van Uden, R. Aartsma,C. van Eijsden, G.F. Dekker, Benefits ofergonomic design, part 1 Quantification model,part 2 Case studies, Shell SNR/C, Pernis, 1996.
Shell, Pre-start-up review HYCON plantPernis, MFE 95/88, SIPM, The Hague, 1986.Shell, Ergonomics, a human factorsengineering strategy for Shell, SIOP, TheHague, 1995.
Slappendel, C., Ergonomics capability inproduct design and development; anorganisational analysis, Applied Ergonomics,Vol. 25, nr. 5, 1994.
WEER (WORKING GROUP ERGONOMICS), Use ofa mobile platforms reduces maintenance costs,Intercom, Shell SNR/C, Pernis, 1995.
Wilson, J.R., Devolving ergonomics; the key toergonomics management programmes,Ergonomics, Vol. 37, nr. 4, 1994.

114

115
THE DEVELOPMENT OF A HUMAN FACTORS ENGINEERINGSTRATEGY IN PETROCHEMICAL ENGINEERING AND
PROJECTS
PART 2
Martin E J van Uden, Co-ordinating Process Engineer, ShellInternational Chemicals, Amsterdam and Mr Harrie J T Rensink,Group Advisor Human Factors Engineering, Shell International
Health Services, The Hague
Content of the Article
Although the man-machine interface inpetrochemical manufacturing projects hasalways been considered to be an integral partof a sound engineering design, manyergonomic misfits in operability andmaintainability has been experienced afterimplementation.
Based on that experience a vision and policywas formulated, which resulted in a humanfactors engineering strategy integrated in thefront end loading (the early developmentphases) of the business process of “projectpreparation and execution”.
The benefits of this strategy are identified bothin business terms (economics) and in workingconditions; like improvement in Health, Safetyand Environmental (HSE) aspects. Based onhistorical data it is now identified that for atypical $ 400 million petrochemical project thestrategy can result in a reduction of :• 0.25 - 5 % of capital expenditure
(CAPEX),• 1 – 10 % of the total engineering hours
and• 3 - 6 % of operational and maintenance
life-cycle costs of facilities (OPEX). This paper consists of two parts. Part 1describes the development of the strategystarting with creating awareness within anorganisation up to the general approach basedon a developed vision and policy. Part 2 will give the reader insight in the actualProject Management and Quality Assurance ofHuman Factors Engineering in petrochemicalprojects.
The above explained statements that humanfactors and ergonomic principles are notsufficiently anchored in the design process isnot world shocking. However, especially forprojects in the petrochemical industry, a clearrecipe cannot been found in literature. Muchwise words have been written but anincorporated control system is not found. In chapter 2 the project business process isanalysed. It will be discussed where and howergonomic principles should be integrated inthe process. Chapter 3 will further give thetotal framework in terms of a warranted qualitysystem, including management monitoringtools and system auditing. In chapter 4 the main driver for integratinghuman factors in the technical design process isdiscussed, being the benefits of integratingergonomic principles in the business process.One could discuss to deal with costs andbenefits in the first place as well, but in thisarticle we have chosen not too, as thecost/benefits are probably better understoodafter reading about the management system andunderlying tools. In chapter 5 an example of integration ofHuman Factors Engineering into newengineering developments will be given.
Introduction
The traditional ‘design process‘ After the birth of an idea to invest in apetrochemical plant, either for economic orother reasons, a conceptual design is made, onbasis of existing, improved or new technology(ies). The conceptual design is normallyfollowed by a study into the feasibility of theproject and an early (economic) evaluation willindicate whether to proceed with the basic

116
engineering study during which the project isfurther defined in terms of scope,implementation and financing. The so-calledbasic engineering and design package (BDEP)or project specification (PS) contains enough
information to make an accurate cost estimate(accuracy normally ± 10%). At this pointbusiness premises and forecasts are frozen andan economic evaluation, including technical
Scouting phase
Operation,maintenance
and improvement(change)
Commisioning andstart-up
Definition phaseBasic engineering
Feasibility phase
Detailedengineering
Procurement
Civil work
Construction
AuditingExpediting
Typical high level business process description"PROJECT PREPARATION AND EXECUTION”
NSTRUCTION"scouting report
typically a ± 30% estimateeconomic evaluation
Feasibility reporttypically a ± 20% estimate
project execution planeconomic evaluation
ITB for basic engineering
BDEP packagetypically a ± 10% estimate
project implementation planeconomic evaluation
ITB for implementation
a.o.Project deliverables(data/documents)
Construction safety reportsLife-cycle ERP system
Trained staffCommissioning & SU plan
contracting out
contracting out
Hand-over to life-cycle organisation
Post implementation review(during early exploitation)
Figure 1

117
and financial risks and sensitivities, isperformed. In most petrochemical companiesthis evaluation is the basis for approval of theproject. During this front end engineeringphase typically some 5% of the capital is spent.After approval of the project theimplementation phase is started including thedetail engineering, during which the equipmentand material specifications are completelydescribed in requisitions, being the startingpoint for the procurement. During detailed engineering drawings (or now-a-days drawings based on data) are produced toenable the constructors to build thepetrochemical facility. During the last decades(two dimensional) computer techniques havebeen increasingly used and during the lastdecade graphic oriented 3D computer imaginghas been used, while today 2D and 3D designis integrated on basis of object oriented designand engineering. Today virtual reality iscommonly used on the construction side aswell after construction the new facility is testedand started-up. The process as described above can be shownin relation with time schematically, showingthe deliverables of each process step on theright hand, as shown in figure 1. The input of engineering disciplines
in the design process During the process of design, engineering,procurement and construction manyengineering disciplines are involved, e.g.process technologists/engineers, mechanical,electrical, civil and instrumentation engineers.Cultural, strategic, and logistic considerationsgive a continuous input during the designprocess, resulting in decision mostly influencedby conflicting arguments or constraints. Oftenthe capital investment must be incorporatedinto existing infrastructure and especially inrecent years much capital investment is spent inretrofitting and de-bottlenecking existing units. Good engineering is considered when alldisciplines mentioned are working integrallyand where mutual empathetic behaviour isshown. Although it is sometimes said that thisis the project managers role, we have noticedand are of the opinion that the system(organisation and availability of the correctprocedures and behaving culture) in which theresponsible project manager has to work is ofdetermining influence to the success.
Budget constraints (foreseen or unexpected)are a danger for good integration between thedisciplines as this is often thought or at least itis easy to think that this is in conflict withproper engineering, procurement andconstruction. It should be noticed that many petrochemicalcompanies have slimmed down theirengineering strength, relying more and more onthe aid of engineering contractors. Althoughthis is attractive from a staffing point of viewsome "punishment" for this policy is receivedas well. Engineering contractors "unfortunately" do notoperate the plant and are therefore notobtaining enough feedback (as a companyengineer will) to improve the level of hisengineering skills with respect to anticipatinglife-cycle operations, maintenance and otherrisks. Therefore and further greatly dependingon the type of the contract, EC's are not alwaystoo interested in the plant life after constructionhas finished. The above constraints definitely influence thequality of the projects. Lack of user participation in design
Those who have read the previous paragraphsseriously may have noticed that someimportant participants in the project have notbeen mentioned yet. This important group of,let us say "potential" contributors to the design,are often NOT, TOO LATE or in only aCOMMENTING WAY involved during thedesign process. They are those who have tooperate and maintain the plant for many yearsto come. Of course these ‘end users’ were alwaysrecognised as participants in a project, butmore in the sense of giving comments to adesign or a document. Seldom have they beenrecognised as really contributing to the designas a demand defining participant. From interviews with designers, engineers,constructors and project managers as well asoperators and maintenance workers it can beconcluded that there is a difference in attitudebetween the two groups, in that the first groupis motivated to deliver a product that full fillsthe "basis of design" and concentratethemselves on those issues but that the end-users are motivated to operate and maintain theplant in an efficient and effective way and are

118
more concentrated towards the life-cycle.Although engineers told and apparentlythought that they had sufficient empathy for thelife-cycle, more detailed questioning broughtthem into the situation in which they concludedand confessed they were not enough taking thelife-cycle of the plant under design intoconsideration. The attitude of the engineer canbe generally explained as an attitude in thesense of : “......as long as it’s working I did afine job.....” Operators and maintenanceworkers on the other hand complain that theyneed more effort to do their job during theexploitation as a result of user unfriendlydesigns. They also claimed that this increasesexploitation costs. The fact is that if end-users, as being therepresentatives of the operator/owner, areinsufficiently involved during the design andconstruction phases, this results in a negativeinfluencing factor what is generally identifiedas limited ‘client commitment level’ (CCL). However a new dilemma exists in view ofavailability of operational and maintenancestaff during the design and methods shouldtherefore be developed to overcome thisdilemma efficient.
Problem definition Ergonomics or human factors engineering is"easily forgotten" during all phases of a project(Refer to Part 1 of this article for the argumentsleading to this statement). This leads to many disadvantages, amongstothers extra costs during the further life cycleof the plant for operations and maintenance,and additional health and safety risks. Furthermore those who might contribute toavoid ergonomic misfits are not oftenconsulted. Not enough emphasis is paid to the many taskswhich have to be done when the plant is inoperation and has to be maintained. It can beconcluded that the design process should haveincorporated more means to assure theknowledge of ergonomics, human factorsengineering, task analysis of which the resultshave influence on the design and userparticipation.
Conclusion of the above analysis Too many ergonomic misfits exist inpetrochemical plants, even those recently built
even after already making use of graphic butstatic oriented 3D computer programs. This isdue to the fact that project and designorganisations and their engineering contractorshave not the appropriate business controls inplace to make sure the defect is addressedproperly. Furthermore those who mightcontribute to avoid ergonomic misfits, the end-users of a work system, are not often consulted. This can only be best achieved by anergonomic awareness program for all thoseinvolved in projects, through organisation andmanagement procedures and last but not leastby showing the economical and non-economical benefits of human factorsengineering in projects. Furthermore theapplication of new simulation tools based ondata centric and object oriented, and thus2D/3D integrated (dynamic) engineeringsystems, with a proven history in theautomobile, aircraft and shipbuilding sectors ofthe industry, will lead to extremely simple andearly 3D simulation of the plant under design.This leads to better understanding an early“design out” of ergonomic misfits as well asoptimised life cycle oriented designs.
Management of Human FactorsEngineering in Projects; The
Procedure to Follow
Introduction In this procedure, the human factorsengineering activities, as experienced in anumber of recent projects, are described inrelation to the project phases. On the left-handside the status of the project is given, rangingfrom the feasibility phase, through thedefinition (basic engineering) phase into thedetailed design, procurement and constructionphase. It can be noticed that already early inthe design ergonomic demands have to bespecified; the main reasons being :• that it is in this phase that inside battery
limit (IBL) operational and maintenancephilosophies are being defined
• that the design is still flexible in its scopedefinition, so that ergonomic demands,especially on IBL philosophy level can beeasily and at no cost be integrated in thedesign
• demands and scope ergonomiccategorisation can be set for use in thebasic and detailed engineering phases
The business process flow diagram as given inthe centre part of figure 2 can be followed to

119
understand the scope, purpose, organisationand management of human factors engineeringin projects. Keywords in this procedure are :Plant lay-out, Human Machine Interfacedesign, Control room and Human ComputerInterface design, Ergonomics, Userparticipation, Client commitment level,Operability, Maintainability and SystemReliability. The purpose of this procedure is tointegrate the user’s requirements into thedesign of a system at the right time, well inbalance with the technical and economicalconstraints, with respect to project investmentas well as life cycle cost savings andoccupational health and safety benefits. Indoing so, the design will also reflect the waythe future operators and maintenance people ofthe system want to utilise their systemeffectively while at the same time theyunderstand and accept that impossible demandsin view of additional investment versus lowbenefits, are not implemented. The procedurein general leads to lower Capital expenditure(CAPEX) as well as lower life cycle costs ofinstallations and costs of plant change (Shell,a). Executing a Human Factors task analysis inbasic design and/or definition phase is crucialfor catching the technical/usabilityrequirements of the human machine interfacesearly. After these requirements are identifiedand recorded, there is a standard approach tofollow during the proceeding phases. This procedure is applicable for new grassroots projects as well as for brown fielders andde-bottlenecking or major retrofitting. Theprocedure demands the co-operation betweenoperations/maintenance, process engineering,project management, construction managementand the engineering contractor. Disciplineengineers normally do not participate duringthe analysis or audits, but are consulted alongthe road. The policy with respect to human factorsengineering is geared towards achieving anoptimal Human Machine Interface forinstallations, control rooms, work places,laboratories, and offices. It is essential that thepersons who are ultimately responsible forensuring a user friendly design are thedesigners, engineers and project managersexecuting the project; they need the input oflife-cycle users in time to avoid later changesduring detailed engineering or even worseduring construction, not to speak about changesduring the life cycle as such.
Below the activities found back in theprocedure are discussed; a good quality controlis guaranteed when there is proof in the form ofdeliverables, sometimes integrated in generalreports, like BDEP packages or ProjectSpecifications. The type of deliverables isindicated on the right hand side of figure 2. Identify necessary human factorsengineering input with respect to the projectscope The person responsible for putting together theBasic Process Design Package (BDP or oftencalled BOD) and/or the Basic Design andEngineering Package (BDEP), often theprocess engineer or the project co-ordinator/manager, should discuss and evaluatewith the human factors engineer, the necessaryeffort for the project. Within our Companyprotocols and checklists for facilitating thisdiscussion are available. Inform project team/manager/Kick offmeeting The process engineer informs the project teamleader or manager about the proposed strategy,including the initial costs (it is assumed that theproject team leader or manager is anexperienced professional and relates the initialcosts to the benefits to be captured later,although many times the challenge from theproject team leader indicated differently. Theagreed Human Factors Engineering plan ofaction is then part of the agenda of the projectkick-off meeting. Within larger projects (> $50 million) the human factors engineer oftenplays a co-ordinating role. Nominate the Project Ergonomics Team(PET) The person responsible for drafting the BDPand/or BDEP should nominate (in consultancywith the appropriate discipline managers) theparticipants of the PET. The ProjectErgonomic Team normally consists of a (lead)process engineer, participants experienced inoperations and maintenance, sometimesspecialists (mechanical, instrumentation)depending on the type of project and thehuman factors engineer. Decide the necessary training for the project It is necessary to decide what kind of trainingis appropriate for the project, based on theproject scope and the competence of projectparticipants. For example, before the execution

120
of the FEEEM ® design analysis, it isnecessary that the nominated participants of thePET meet several criteria: Operations/maintenance personnel should havefollowed a training module focussing on theirfunction within the PET team (Shell, b; Shell,c) Process engineer/discipline engineer andproject manager should have participated in afull scope human factors competenceimprovement training, focussing oncosts/benefits and implementation procedureswith respect to management of Human Factorsengineering during all phases of a project. Itshould be considered to have engineeringcontractor and/or vendor representativesparticipating during ergonomics workshops, ifthought relevant. The human factors engineerwill co-ordinate the execution of the trainingrequirements as specified in this step of theprocedure. Normal training is ranging from 4to 8 hours. Execute FEEEM ® design analysis This analysis should be implemented by thePET according to the procedure. The FrondEnd Ergonomic Evaluation Matrix designanalysis describes a multi-disciplinary taskanalysis method to be apply during feasibilityor definition phase to evaluate potentialergonomic bottlenecks in the design. Thisprocedure is part of the Pernis Projects Qualitysystem (Shell, d). A standard part of theFEEEM® design analysis is implementation ofthe Identification of Valves Analysis (IVA®)(Shell, e). The results of the FEEEM® designanalysis along with the IVA® are documentedin the FEEEM report. Also the strategy withrespect to implementing ergonomics in long
delivery items and (critical) Skid packagedunits should be part of the report (Shell, f). Incase of control room or re-instrumentationprojects the management of informationneeded for graphical display design is ofutmost importance to achieve an effectivehuman computer interface along with the moretraditional design tools like e.g. link analysismethods aiming at an efficient control roombuilding lay-out for human efficiencyimprovement during normal and emergencyoperations. Include the FEEEM report in the BDP orBDEP/PS document The person responsible for co-ordinating theBDP or BDEP/PS document incorporates theFEEEM® report into the BDEP document. Atthe end of the BDEP phase the FEEEM reportwill be up-dated and the resultant actionsderived by the FEEEM® report should beverified in relation to the scope of theBDEP/PS and integrated into the initial plotplan. Assure FEEEM® analysis results, forinstance identified ‘soft boxes’ of criticalmaintenance or logistic routing are integratedin the layout of plant. Determine Ergonomics Implementation Plan End of BDEP/PS phase the ErgonomicsImplementation Plan is set up to secure theergonomic requirements and demands,resulting from the FEEEM analysis, duringdetail engineering, procurement and theconstruction phase. For projects less than $ 5million CAPEX, it is in general sufficient toinclude the FEEEM® report into the ProjectExecution Plan/Project Implementation Plan.The project manager should be committed toand is responsible for the execution of theErgonomic Implementation Plan.

121
execute FEEEM
START
STOP
PIR report
BDEP/PS
Quality doc. FEEEMreport
BDP or BDEP
Q doc. ErgonomicsImplementation
Plan
Requisitions:Vendors andConstructionContractors
Q doc. ErgonomicsConstruction Plan
6
8
11
12
1
2
3
4
5
9
10
RR1464-a.af3
Projectpreparation
Feasibility phase
Basicengineering
phase
EPCphase
postimplementation
phase
dependingon
decision7
DetermineHF input
Informproject team
Nominate PET
Determinetraining program
Executetraining PET
Include FEEEMreport in BDEP
Update FEEEM report
Ergonomics imple-mentation plan
Execute modelreviews/audits
Execute ergonomicsconstruction plan
Evaluation
Figure 2

122
Execute model reviews/audits To ensure that the ergonomic requirements aremet within the project, a 3D CAD modelreview is used during 30%, 60% and 90% ofthe detailed engineering phase (see chapter 5for special integration of ergonomic analysiswith state of the art 2D/3D integrated CAEsystems). Critical operations and/ormaintenance activities should be simulated(preferably dynamically) during detailedengineering making use of new technologies inorder to check the operational and maintenanceprocedures as indicated in the FEEEM®report. Often the life-time proves thatimpressive constructed procedures do not workin the life-cycle and have to be violatedthrough safety and health risks and costs;dynamic functional simulation, now-a-daysbecoming available, will be more and moreused. Special attention should be given to Skidpackaged units. Execute the Ergonomic Construction Plan This plan’s purpose is to guide the constructioncontractor about installing “field run”equipment which is not always shown in thephysical computer models, but only in thefunctional models. This concerns mainly “fieldrun” installed items like small bore piping,lighting fixtures, secondary cable trays etc. Theplan normally includes :• inserting ergonomic requirements into
standard paragraphs of contracts withinstallation contractors, includingprocedures how to handle diagnosedmisfits
• awareness sessions with on sitecontractors.
• use physical (3D) model on site forreference
• execution of “ergonomic verificationrounds”.
Evaluate the application of human factorsengineering The human factors engineer, the projectmanager and/or client’s maintenance managernormally will decide to evaluate the successesor failures of the ergonomics program duringthe post-implementation period.
Cost and Benefits Showing costs and benefits of programsnormally motivate professionals to apply or notapply programs. To demonstrate the benefits ofthe implementation with respect to costs anextensive study was done into the cost andbenefits items by Shell Nederland Raffinaderijand Shell Nederland Chemie in Pernis andMoerdijk, in cooperation with NederlandseAardolie Maatschappy Assen some three tofour years ago (Shell, g). Generally it was found that benefit/cost ratiofor new (grass roots or brown field projects)are high, but that also in de-bottlenecking orretrofitting projects the balance between costsof analysis and their benefits for CAPEX andlife-cycle exploitation costs are still veryfavourable. More critical were small projectsor so-called plant changes, normally directlypaid out of the exploitation budget, which weremeant to abandon ergonomic misfits existing inplants in operation. Justification of suchinvestments was often done on rather softgrounds, based on a kind of common sense andunderstanding rather than backed by economicor other calculations. It was there were thestudy team concentrated themselves. It wasbelieved that a model able to discriminatebetween the justification of these type ofexploitation costs or not, could certainly alsobe used for the larger grass roots or brown fieldprojects. Benefit Areas As costs can normally be estimated up front onbasis of scope and hours, the team firstconcentrated on the benefit areas; three levelsof benefit areas were established. The highlevel of benefit areas were defined atstakeholder level, where a rough definition of astakeholder is that this is anyone or any groupsharing the costs and other disadvantagesand/or the benefits and other advantages of thebusiness. In figure 3 below a graphic representation isgiven of the high level benefit area’s in relationto the main stakeholders.

123
Operability
Maintenance
Reliability
Safety
Health
Environment
Legislation
Labour turnover
Relation to stakeholders
personnel
society
government
share-holders
&clients
Quantify or rank
Figure 3 The next level was determined by investigatingthe benefits, tangible or intangible, within themain (high level) benefit areas. It appeared thatmany second level benefits were found tobenefit more than one of the main benefitareas. A cross reference graph was constructed,which became the foundation on which thebenefit identification process was built.
This cross-reference benefit table, given belowin figure 4, is an example how benefits areranked. A third level of benefits are longchecklist, belonging to each of the second levelbenefits on the left hand side of figure 4. Thisthird level of benefits are of great help toidentify benefits, which are then classified inthe matrix shown below.

no
.D
escr
ipti
on
of
ben
efit
op
erat
ion
sm
ain
ten
ance
relia
bili
tysa
fety
hea
lth
envi
ron
men
t leg
isla
tio
nla
bo
ur
turn
ove
r1
Sav
ing
time/
hum
an r
esou
rces
2
Sav
ing
prod
uct
3 W
aste
red
uctio
n 4
Red
ucin
g/pr
even
ting
erro
rs
5 R
educ
ing/
elim
inat
ing
phys
ical
/men
tal s
tres
s 6
Red
ucin
g tr
aini
ng c
osts
(re
quire
men
ts/ti
me)
7 Im
prov
ing
the
qual
ity o
f the
end
-pro
duct
8 P
reve
ntin
g da
mag
e/ris
k to
pla
nt
9 M
akin
g op
erat
ors’
insp
ectio
n ro
unds
mor
e ef
fect
ive
10 Im
prov
ing
mai
nten
ance
qua
lity/
life-
cycl
e ex
tens
ion
11 P
arts
sav
ings
12 S
avin
g on
hoi
stin
g/tr
ansp
ort c
osts
13 S
avin
g on
tool
s14
Sav
ing
on d
irty
wor
k/cl
eani
ng/P
PE
cos
ts15
Sav
ing
on w
orks
hop
cost
s16
Sav
ing
on s
caffo
ldin
g co
sts
17 R
educ
ing
the
risk
of t
rips
18 P
reve
ntin
g/sh
orte
ning
pla
nt s
hut-
dow
ns
19 P
reve
ntin
g te
mpo
rary
cap
acity
red
uctio
ns20
Sav
ings
on
mon
itorin
g on
job-
rela
ted
risks
21 R
educ
ing
unau
thor
ised
ove
rrid
es o
f pr
otec
tive
syst
ems
22 I
ncre
asin
g pr
oces
s sa
fety
23 In
crea
sing
ope
ratio
nal s
afet
y24
Few
er c
ontr
ol m
easu
res
requ
ired
25 R
educ
ing
the
risk
of a
ccid
ents
26 P
reve
ntin
g he
alth
-rel
ated
abs
ente
eism
27 R
educ
ing
occu
patio
nal d
isea
ses
28 P
reve
ntin
g co
mpe
nsat
ion
clai
ms
and
rela
ted
inte
rnal
dis
cuss
ions
29 R
educ
ing
the
num
ber
of e
mpl
oyee
s w
ho b
ecom
e un
fit for
wor
k30
Red
ucin
g th
e nu
mbe
r of
day
s of
ada
pted
wor
k31
Pre
vent
ing
impa
ired
perf
orm
ance
32 Im
prov
ed o
ccup
atio
nal h
ygie
ne (
toxi
city
, noi
se, e
tc.)
33 R
educ
ed p
ollu
tion
of t
he s
oil/w
ater
/atm
osph
ere
34 R
educ
ing
the
prob
abili
ty o
f env
ironm
enta
l inc
iden
ts
35 R
educ
ing
the
num
ber
of e
nviro
nmen
tal c
ompl
aint
s 36
Impr
ovin
g th
e co
mpa
ny’s
imag
e/re
puta
tion
37 P
reve
ntin
g/re
duci
ng n
otic
es/s
anct
ions
from
the
HS
E a
utho
ritie
s38
Impr
ovin
g th
e st
aff m
otiv
atio
n39
Red
ucin
g th
e nu
mbe
r of
vac
anci
es w
hich
are
har
d to
fill
40 Im
pro
ving th
e p
erf
orm
ance
of o
lder/
sick
pers
onnel
41 R
educ
ing
dem
urra
ge
124
Figure 4

125
After the identification of the benefits, thebenefits need to be quantified. If the identifiedbenefits are to a great extent feasible to beestimated, the benefits are outweighed againstthe estimated costs. In many cases however thebenefits are rather intangible, e.g. “What is the$ value of safety ? “. In cases where no tangible figures can bederived from the benefits, the benefits aresimply ranked according according to a systemvaluating :• the exposure class, showing the risk of
exposure. This exposure class isdetermined taking the frequency of thetask to be judged and the number ofexposed people into account.
• the effect level, showing the effect onpeople, environment, etc. should the taskfail.
• the total risk factor, being a ranking onbasis of the exposure class and effectlevel.
Costs and ranked or quantified
benefits As mentioned above benefits with a tangiblecontent may already simply justify the cost ofergonomic improvement in existing plant or indesign. When a ranking exercise is needed onlythe highest risk factor is used to determine thepayout criteria, which have been agreed beforewith management. So for intangible benefits,only the benefit with the highest classificationcounts, while for tangible benefits benefits ($)can be added. The payout criteria justmentioned are also dependent of the height ofthe costs. If payout criteria are reduced to zeroa full intangible benefit has justified the coststo be made. In most cases there is acombination of intangible and tangiblebenefits, which justify or not justify necessarycosts. The total procedure takes approximately5 to 10 minutes. The tables and matrixes as discussed in 4.2 and4.3 have not been further shown as theapplication and threshold levels are fullydependent on Company policy. Identified benefits for a large grass
root project, implemented in anexisting site.
After having completed an ergonomicsprogram as mentioned above on an $ 400billion investment, the costs and benefits havebeen analysed together with the future
operations and maintenance organisation, ownproject management and the engineeringcontractor involved in basic engineering,detailed engineering, procurement andconstruction. Although in such an exercisecosts and benefits are sometimes partlyintangible, many tangible costs and benefitshave been identified. Although the contents ofthe complete report can not be disclosed in thisarticle, it can be mentioned that duringengineering approximately 150 man days wereused for analysis and engineering follow-upand approximately one man year for follow-upduring construction. Minor costs, e.g. formaking CD-ROM with animated trainingmaterial for construction firms, are notincluded. The “LOOK BACK” exercise/analysis showed(ABB LUMMUS): • Identified CAPEX saving were in the
order of $ 2 million or 0,25 % of capital(it is believed that this figure is higher dueto material wastes resulting fromconstruction REDO.
• Additional CAPEX was estimated to be $60,000.- to improve operations andmaintenance
• Identified savings during the first ten yearsof operation amounted to $ 0.9 million
• Identified cost savings during two fourannual major shutdowns were estimated tobe $ 460.000,-
• A large list of intangible benefits, relatedto safety, health and environment.
Integration of Human Factors
Engineering into New EngineringDevelopments
In figure 5 the procedure is shown in moredetail how ergonomics has been integrated in asingle object oriented database driven CAEsystem with integrated and thus consistentfunctional and physical design and engineeringcapabilities. The CAE system, CC Plant basedon the CATIA kernel of object oriented designand engineering, has the availability to capturedesign intent and apply Knowledge BasedEngineering (KBE). During a recent projectusing these advanced, fully Product DataModel based, techniques a plant was designedand engineered and the Human FactorsEngineering Discipline was participating in atrue concurrent mode with other disciplines asexplained below.
126
The participation of ergonomics all started withthe given area for the plant to be built, becausethis will put the spatial constraints on the table.It can be mentioned at this stage that giventypical areas for known plants and technologies
normally used are not at stake, becauseexperience with the ergonomic analysis showsthat this will certainly not lead to the need formore area.
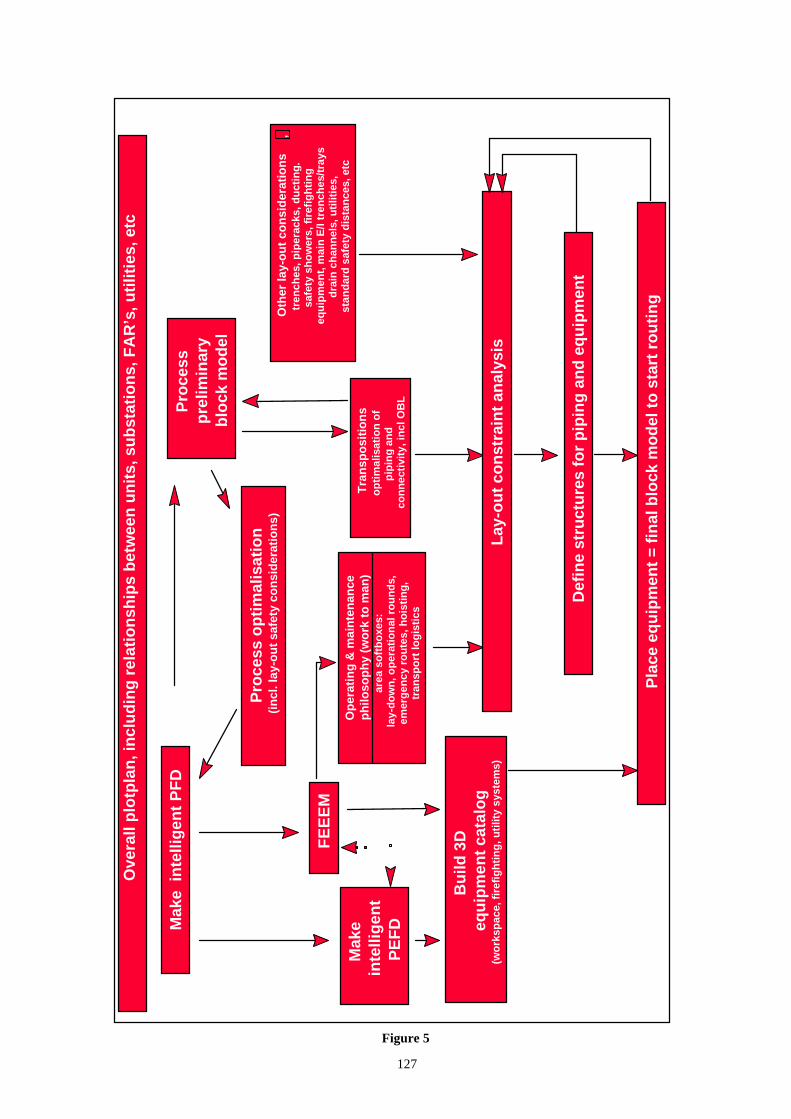
Mak
e in
telli
gen
t P
FD
Pro
cess
pre
limin
ary
blo
ck m
od
el
Pro
cess
op
tim
alis
atio
n(i
ncl
. lay
-ou
t sa
fety
co
nsi
der
atio
ns)
Op
erat
ing
& m
ain
ten
ance
ph
iloso
ph
y (w
ork
to
man
)ar
ea s
oft
bo
xes:
lay-
do
wn
, op
erat
ion
al r
ou
nd
s,
emer
gen
cy r
ou
tes,
ho
isti
ng
, tr
ansp
ort
log
isti
cs
FE
EE
M
Mak
e in
telli
gen
tP
EF
D
Bu
ild 3
Deq
uip
men
t ca
talo
g(w
ork
spac
e, f
iref
igh
tin
g, u
tilit
y sy
stem
s)
Def
ine
stru
ctu
res
for
pip
ing
an
d e
qu
ipm
ent
P
lace
eq
uip
men
t =
fin
al b
lock
mo
del
to
sta
rt r
ou
tin
g
Ove
rall
plo
tpla
n, i
ncl
ud
ing
rel
atio
nsh
ips
bet
wee
n u
nit
s, s
ub
stat
ion
s, F
AR
’s, u
tilit
ies,
etc
Tra
nsp
osi
tio
ns
op
tim
alis
atio
n o
fp
ipin
g a
nd
con
nec
tivi
ty, i
ncl
OB
L
Oth
er la
y-o
ut
con
sid
erat
ion
s,
tren
ches
, pip
erac
ks, d
uct
ing
.sa
fety
sh
ow
ers,
fir
efig
hti
ng
eq
uip
men
t, m
ain
E/I
tren
ches
/tra
ysd
rain
ch
ann
els,
uti
litie
s,st
and
ard
saf
ety
dis
tan
ces,
etc
Lay
-ou
t co
nst
rain
t an
alys
is
Figure 5
127

128
In the case of the particular project to be builtat an existing plot after demolishment of aformer plant, the existing residual existingbuildings, etc had to be taken into account andto be used if needed and attractive (e.g.substations, field auxiliary rooms, analyserhouses, etc.). In figure 5 it can be seen that onbasis of the PFD an initial 3D block model wasmade very early during the feasibility phase asdiscussed before. With fully integratedintelligent 2D/3D engineering (one singledatabase) this effort is negligible. The procedure shows how this preliminaryblock model, after it had served to save some 2to 3 % on capital investment during the processoptimalisation, is used to define furtherrefinements. On basis of the analysis based onthe FEEEM matrix, demands are being definedto equipment on the one hand and detailedoperating and maintenance (life-cycle)philosophies on the other hand. It can benoticed from the figure that the FEEEM ®design analysis is done in a concurrent modewith the development of the PEFD’s and thatsome constraint handling between ergonomic,operational, maintenance and engineeringdemands is already taking place at thatmoment. In fact at the right moment, therebyexcluding a number of engineering recycles oreven worse.ending with a less optimal design. With respect to spatial equipment design,which at the same time (concurrently) isdeveloped as well, the ergonomic analysisleads to demands on free areas needed aroundequipment and these design intents are definedas part of the equipment in the equipmentcatalogue. With respect to the operating andmaintenance philosophies the ergonomicanalysis yield spatial demands in terms of softboxes (a technique also used in conventional3D systems, however at a much later stage inthis project), based on identified needs for laydown areas for inspection and maintenance,operator rounds, emergency routes, logicalsafety shower positions, hoisting and transportneeds. Looking at the initial preliminary and verysimple block model, one can see that this atleast served the design team a second time byusing it for piping transpositions and lay-outoptimalisation studies. The operating and maintenance demands, theoptimal piping lay-out and other mostlycommon engineering or statutory lay-outdemands are all combined and used to arrive at
the “final constraint analysis” necessary todefine the plant’s civil “building”, includingthe often COMBINED soft boxes necessary foroptimal piping, ergonomics or statutorydemands. Only when the “building” with all itssoft boxes is defined it is time to place theequipment finalised in the equipmentcatalogue. It is obvious of course that thisexercise, as simply explained above, is not astraight or “from start to finish” exercise, butthat a number of recycles, as a result of work inprogress, exist to make further optimalisations. Although the suspicious reader may doubt theefficiency of the procedure it can be said that,due to the fact that the approach is verystructural and professional, considerable timeis saved, not only during the procedure itself,by avoiding many conventional and ‘out ofsync’ recycles, but especially by avoiding a lotof recycles during the later detailedengineering. It should be mentioned that apartfrom the defined ergonomic demands onequipment and general lay-out as used in theabove procedure, the FEEEM analysis alsogenerated many detailed demands for thedetailed engineering phase on piping,instrumentation and so-called ‘ field run’ (e.g.small bore, secondary cable tray, lightingfixtures, etc.) items. Ergonomic analysis (as well as other types ofanalysis) and the use of a data centric objectoriented single database can be consideredsynergetic.
References SHELLa “Managing human factorsengineering in projects procedure”, doc IDEMIS.PMQ.01, Shell International, HumanFactors Engineering, The Hague. SHELLb “Workshop ergonomics in processinstallations”, doc.ID EMIS.IT.03, ShellInternational, Human Factors Engineering,The Hague. SHELLc “Ergonomic Training module foroperators and maintenance worker”, doc IDEMIS.IT.05, Shell International, HumanFactors engineering, The Hague. SHELLd “FEEEM ® design analysis”, doc IDEMIS.PMQ.02, Shell International, HumanFactors Engineering, The Hague. SHELLe “Identification of valve analysis(IVA® )”, doc ID EMISPMQ2A, ShellInternational Human Factors Engineering, TheHague

129
SHELLf “Best practice ergonomic guidelinesfor skid package units design”, doc IDEMIS.VM.01, Shell International, HumanFactors Engineering, The Hague. SHELLg “Benefits of ergonomic design, Part 1Quantification model, part 2 Case studies”, doc
ID EMIS.PMQ.07, Shell International HumanFactors engineering, The Hague. FEEEM analysis report MSPO/2 project, docID. LGVSFOR 02-7000-02.021, ABBLUMMUS, Voorburg, The Netherlands

130

131
HEALTH AND SAFETY BY DESIGN - INTEGRATING HUMANFACTORS INTO THE OFFSHORE DESIGN PROCESS.
Dr Ian Randle, Hu-Tech Associates Ltd and Mr Ed Terry, SaufConsulting Ltd
Introduction
Human Factors (HF) input is now realised tobe the common factor, in its broadest sense, ofthe remaining barriers to excellent safety andenvironmental performance. Many issues arise from an individual’sperformance in certain contexts, but thereremains the opportunity to include HF in thedesign of systems, what is sometimes termedthe Man-Machine Interface (MMI). Theseissues have been dealt with in engineering ofnew plant and equipment but much of the focushas been on direct interfaces, notably controlsystems. There remains an alternative approach; typicaldesign deliverables and activities prepared orundertaken during the design of an offshore oiland gas platform are the mechanisms by whichdesign decisions are generated, reviewed andimplemented. Individual technical andmanagerial discipline specialists canthemselves consider and incorporate (or not)solutions for areas where HF issues should bekey. The project team considering these issuescan then note the solution of the issue and themanner in which the solution can beincorporated. Using this approach, whereby the disciplinespecialists implement HF themselves into theirtraditional discipline deliverables, allows thetechnical and management teams to identifywhere HF will benefit their particular areas ofresponsibility and also allows HFconsiderations to benefit from their expertiseand their specialist activities. Implementingthis process will, in addition, spread theawareness and understanding to other technicaland management disciplines.
The regulators have an interest in this area as ameans to foster improved safety andenvironmental performance, this approachbrings 2 current strands of thinking together; • Raising the understanding of the
importance of design, and
• Facilitating the incorporation of HF intoall project system characteristics.
This paper presents the outline of the methodcurrently under development and which is thesubject of an industry proposal. The paperdescribes the steps to be taken to facilitate orsupport individual engineering disciplinecontribution to include Human Factors in thetraditional deliverables of the design processfor oil and gas installations. The method will look to define categories ofdesign deliverables and will also look at theimportance of CAD deliverables. The methodintends to outline some basic requirements thatdiscipline engineers can then incorporatewithout recourse to specialist HF advice. The method will allow the HF consultant toconsolidate the inputs and inclusions, confirmthat they are appropriate and to deal with noveland innovative issues. This process therefore reflects a “bottom-up”approach for incorporating Human Factor’sconsiderations into the design.
Fitting into the design process The HF considerations must meet the needs ofthe stage in the design lifecycle, so it ispertinent to reiterate what the demands of eachdesign are, these are described below.
4 D e s i g n P r o c e s s
F e a s i b i l i t y èè C o n c e p t u a l D e s i g n èè F E E D èè D e t a i l D e s i g n
W h a t c o u l d W h a t w i l l H o w w i l l i t M a k e i t
w o r k w o r k w o r k w o r k !

132
Understanding the key objectives of eachdesign stage is paramount. The inclusion of HFmust be targeted precisely to meet the overallobjective of the design stage being undertaken.This paper has proceeded on the basis that theabove objectives hold true. The potential HF inclusions are detailed furtherin the tables later in this paper. The key to the successful implementation ofthis approach is to have a clear definition of thedesign phases, the related deliverables andtheir dependence upon the CAD model.
It is a base assumption of this method that theCAD model can function as the main vehiclefor collating and consolidating HF inputs. Therelationship to the information held in the CADmodel to each of the above design stages mustalso be understood carefully. The informationrequired and available at each stage containsvarying detail and is based on varyinguncertainty. The HF issues must recognise thisevolution of data. Further detail on the objectives of each of thedesign stages is contained in the figureoverleaf.

Wha
t is
th
e d
esi
gn
pro
cess
?
Fe
asi
bil
ity
èèC
on
ce
ptu
al
De
sig
nèè
FE
ED
èèD
eta
il D
esi
gn
De
ve
lop
a r
an
ge
of
stu
die
sD
ev
elo
p a
nd
ju
stif
yse
lec
ted
co
nc
ep
tC
on
firm
de
sig
n o
fc
ho
sen
co
nc
ep
tS
pe
cif
y&
pu
rch
ase
•De
ve
lop
me
nt
op
tio
ns
ide
nti
fie
d
•Co
ars
e r
isk
ra
nk
ing
of
op
tio
ns
•Co
st
•We
igh
t
•Sch
ed
ule
•Id
en
tify
de
sig
no
pti
on
s
• S
ele
ct
co
nc
ep
t(u
sin
g i
nh
ere
nt
safe
ty p
rin
cip
les)
• D
em
on
stra
tese
lec
ted
co
nc
ep
t is
AL
AR
P
•Id
en
tify
/ a
sse
ssh
aza
rds
• E
lim
ina
te a
nd
pre
ve
nt
ha
zard
s
• S
et P
erf
orm
an
ceS
tan
da
rds
•AL
AR
P p
roc
ess
• C
on
firm
ha
zard
sa
sse
ssm
en
t
• R
ed
uc
e a
nd
mit
iga
te h
aza
rds
• C
on
firm
ati
on
of
Pe
rfo
rma
nc
eS
tan
da
rds
• C
on
firm
ris
ks
are
AL
AR
P
4
133

134
It should be noted at this time that this paperdoes not address project stages beyond design.
The issues defined in the figure above alsoserve to reiterate that much more influence isavailable early in the design phase.
I terates towardsdesign goals
4How is safety incorporated into thedesign process?
T he design process
T he safety process Iterates towards safety goals
Design activit ies
Safety activit ies
A distinctive attribute of the method proposedis the manner in which the inclusion of HFissues is undertaken. To illustrate thisapproach, a traditional view of implementingsafety has been set out above. It can be seenthat traditionally, the safety process tends torun in parallel with the design process wherethe activities within the design and safetyprocesses inform each other. Each parallelprocess encompasses iterations that progresstowards the defined goals being achieved. It is our suggestion that there is an opportunityfor HF studies to develop an integrated processat this point in the evolution of HF in design.The potential for merging HF directly into theactivities of other disciplines within the designprocess is in our view even greater and mayeven precede the incorporation of the safetyprocess. This approach could then build on theexperience of the safety teams where some
aspects of safety can be successfully integratedinto the design process but some aspectsactually benefit from remaining independent.As education and awareness of safety hasimproved, the ownership of aspects of theprocess has and should be taken over by otherswith a direct impact on the outcome. The skillis to balance which tasks fall into whichcategory. The figure above reinforces the concept thatdesign and safety are rolling iterations. It mustbe realised that not all information will beavailable early in a project or will be availablewith acceptable levels of certainty. It is ourcontention that the engineers responsible forthat information may be the best ones to makethe judgement of what they can demand anduse by way of HF information.

135
4 The D esign Pr o cess is St aged
3 In the ear ly st ages, Feasibilit y and C o nceptual, it is
open to inf luence and change
3 This is w her e H F input w ill be m o st cost -effect ive, but
w here least ef fort is undertaken
The figure above summarises and emphasises the points discussed in the previous section.
A review of past practice
4 G aps in Integr at ing H F int o D esign
3 Past p r act ices:
– Less emphasis on “ m ino r ” hazards
– Less emphasis on U sability / w o r kp lace t asks
– Insufficient feedback fr o m past successes and
failur es
– Insufficient input fr o m End U ser s
The incorporation of HF has had a particularfocus in its past application. The incorporationof HF has often been through the safetydiscipline and has focussed on major hazards(as required by the Safety Case). There hasbeen more emphasis on high profile HFusability issues such as control room layout,access to large valves and handling access forequipment replacement. The remaining 2 points in the figure above areself evident and reflects the often inadequatefeedback mechanisms between operations anddesign. The paper discussed earlier the reasonsfor deliverables. For many years the industryhas produced deliverables for reporting,contractual fulfilment and passing oninformation, with fabrication, construction,installation, hook-up & commissioning andoperations being the real customers. It has beena trend of recent designs to reduce unnecessarywork and a success has been to simplify
reporting requirements. Thus it should be notedthat the key customers for reporting only arethe regulators.
Linking HF to deliverables In order to execute their projects effectively,engineering contractors have planning systemsthat have been built from lists of typical projectdeliverables and activities, these listings formthe basis of a planning network that governsthe smooth running of the project. A typicalnetwork will show the activities listed bydiscipline and it will identify the inputs andoutputs for these activities. This informationwill be compiled into a detailed planningnetwork. The planning networks have changed incharacter over the last few years and now tendto deal in a more focussed fashion with

136
activities rather than individual projectdeliverables. For example the main deliverableis the 3 dimensional model produced by theCAD system. In many design contractors thepiping and layout discipline holds ownershipover this model with other specialistscontributing as their skills and knowledgedemand. So in this case, the planning networkdefines the contributing activities but wouldregister only one deliverable. The proposed method will need to ensure thatproject personnel work to the guidance orprotocol developed. This means that themethod must be demonstrably easy for them toimplement. The method must therefore identify the benefitsarising from the inclusion of HF during eachactivity and where in the project lifecycle thatbenefit will be felt. This will entail identifyingthe differences that HF will make in contentand form to the outputs of each activity andthen assessing the benefit that has accrued. Itmay be that the benefit is not felt in theimmediate output of each activity but needs tobe consolidated with other activities andoutputs before some benefit can be identified,this “roll-up” effect will also be reviewed aspart of the exercise.
It is therefore key to; • Collect existing and typical planning
schedules and other supportinginformation
• Identify the areas where HF should and
could be considered in the activities onthose schedules
• Identify the benefits that may accrue, using
a wider and critical forum to review thosebenefits
• A more tentative step will be to
benchmark the value added from HF sothat the worth of the activity can bedemonstrated
This information will enable appropriate areasto be listed where HF analysis can contribute(given the quality of information on the projectat that time) and will facilitate the generation ofa checklist in matrix form to show where HFcontributions can take place and what theywould contribute. In addition, the activities will need to beclassified by their position in the projectlifecycle, the figures below and the tablesoverleaf identify some considerations.
4Feasibility D esign and H F input
F e a sibilit y Gener ic H F Tasks
• System Requir ement s Analysis• Funct ional Analysis• U ser Requirements Analysis• Ident ify all U ser s and Stakeho lder s• Ident ify T asks and H uman Interventions

137
4Conceptual Design and HF input
Conceptual D esign Gener ic HF Tasks
• Allocat ion of Funct ion• Manpower Planning• Task Descr ipt ion and Synthesis• Human Factors Specificat ion
4 FEED and D e t ail D esign a n d H F in p u t
F E E D &D e t a i l D e sig n
G ener ic H F T ask s -
• W o r k st at io n d esign• Equ ipm e n t d esign• H u m an Er r o r A nalysis
(fo r Q RA )
• U ser M anuals & T r ain ing

138
Engineering Design Stage
Key Tasks Human Factors Tasks
Feasibility • Define basic process from reservoirfluids
• Confirm location & orientation• Estimate basic size (footprint)• Estimate basic weight and organise
lift vessels• Determine suitable structure for
support (or mooring if a vessel)• Identify coarse import & export
requirements• Use benchmark accommodation
sizing (i.e. comparative platformtypes)
• System Requirements Analysis• Function analysis• User Requirements Analysis• Identify Users and Stakeholders• Identify tasks and human
interventions
Conceptual Design • Confirm process requirements andspecification
• Fix orientation, footprint andlocation
• Reduce uncertainty on weight &therefore on structural requirements
• Confirm accommodation andsurvival craft sizes
• Identify long lead purchase timeequipment and determinepreliminary specifications for them
• Confirm capacity and type ofimport/export arrangements
• Human Factors specification• Allocation of function• Manpower planning – numbers,
job functions• Task description / synthesis
Detailed Design • Translate process requirements intodetailed specifications and purchaseorders for equipment
• Confirm and freeze weight ifnecessary, buy steel and confirmfabrication arrangements
• Place sub-contract foraccommodation unit and placepurchase orders for any relatedsafety equipment
• Set in motion, complete purchaseand QA programmes and arrangesystems for material delivery to sitefor building.
• Equipment / Interface design• Task design• Workplace / workspace design• Human error and reliability
analysis• Manpower planning - job
definitions, teams, organisationalstructure, skills and training needs
• Design of user manuals / trainingprogramme

139
Construction /Fabrication
• Allocate contract & set in placeprogress monitoring arrangements
• Build main steelwork in-situ, addlarger modules and equipmentpackages (having arranged delivery).This is the area where the largestnumbers of personnel are employed.
• Develop integrity testingrequirements e.g. steel, piping,welds, material checks.
• Mock-up / prototyping• User trials / fitting trials
Testing &Commissioning
• Arrange testing & commissioningprogrammes
• Organise all sub-contractors arrivingon site with test equipment whilefinishing touches to construction arebeing carried out
• Arrange all appropriate testing /commissioning agreements so thatthey either interface or arecompletely separated as required.
• Ergonomic design evaluation• Risk assessment / compliance
certification• User training
Operation /Maintenance
• Run steady state operations• Train for emergency situations and
process upsets• Run regular training for maintenance
teams as well as safety teams• Organise interfaces for sub-
contractors to come on board fortheir regular input to platform well-being
• Plan shutdowns• Organise updates for personnel on
board• Monitoring & supervision of key
items on board
• Post-design evaluation• Feedback to designers (These
generally do not happen)
Linkage to the CAD model
The CAD model is the most powerful vehiclefor illustrating the final product. It provides a(relatively) realistic facsimile of the plant.Other information can be attached to items onthe model, so that other engineers can retrieveinformation based on layout and equipmentlocation.
The model can be constructed in stages orlayers to illustrate the construction, modelshave been used to track material on its way tothe fabrication site, e.g. structure that was inplace and built showed as one colour, materialthat was ordered and on its way was anothercolour, and material yet to be bought (i.e.where most flexibility still existed) would be athird colour.
The models can be viewed by disciplineresponsibility, so that all safety equipment andareas under control of the safety discipline canbe coded to be a particular colour.
It is our proposal that added into thesedemarcations, each individual discipline attachthe HF information relating to issues under itscontrol.

140
Reference information
The inclusion of HF has some precedents fromother industries. The references below show
example standards from the military, nuclearand aerospace industries.
4 HF D esign Specificat ions, Standards & Guidance
4Military - eg D EF STAN 0025
4N uclear - eg N U REG
4Aerospace - CAA & FAA HF design guides
Goals for the guidance
The guidance should provide a toolkit fordiscipline engineers to use. The toolkit shouldbe designed to be readily used by manydiscipline engineers with a low startingawareness of HF.
This approach would have the added benefit ofdemonstrating the benefits of early inclusion ofHF into design. The discipline engineers willhave the advantage of seeing benefits derivingfrom their own actions in a specialist area withwhich they were not initially familiar. This inturn will build their understanding andawareness of HF issues.
4 W hat is the gu idance pr o p o sin g t o d o ?
3 Pr o vid e a t o o lk i t fo r designe r s t o apply H F
c o n sider at io n s t o t he ir o w n d e l iver ables & act iv i t ies
3 I l lu st r at e t h e b e n e fit s ar ising fr o m an ear ly co n sid e r at io n
o f H F
3 Im p r o ve educat io n and aw ar e n e ss o f H F am o ngst o t he r
d isc ip l ine special ist s
Benefits of the guidance
It is our contention that the benefits of theproposed bottom-up approach will be
significant and will follow the points in thefigure below.
4 B e n e f i t s3 I m p r o v e s s a f e t y p e r f o r m a n c e ( m i n o r & m a j o r h a z a r d s )
3 R e d u c e s o p e r a t i o n a l u p s e t s
3 I m p r o v e s p r o d u c t i v i t y a n d u s a b i l i t y
3 I n c r e a s e s c o m f o r t a n d m o r a l e a m o n g w o r k f o r c e
3 I m p r o v e s e f f i c i e n c y o f o p e r a t i o n s t e a m s
Conclusions
We have identified a bottom-up approach toHuman Factors that will involve the
engineering disciplines themselvesincorporating HF issues under guidance.

141
The method should make maximum use ofexisting deliverables and most notably theCAD model.
The model should be integrated into the projectlife cycle, and the HF issues contained in theguidance should be appropriate to the stage inthe life cycle.
By adopting the bottom-up approach weconsider that the disciplines will deal withmany lower hazard issues as well as thoseassociated with major accident hazards.
Our conclusions are summarised in the figurebelow.
4C o nclusions3 M o del addr esses gaps in H F input into design
3 Individual engineer ing disciplines can take con t ro l of
H F in their o w n pat ch
3 The form of deliverables facilit ates the inclusion of H F
as never before
3 The focus is on making it easier for discipline engineer s
to integr ate H F int o t he pr o ject
3 There ar e benefit s fo r t he user , the operat o r , the
const r uct o r and the r egulato r
QUESTIONS AND ANSWERS SESSION
Question – Dr Ron Gardner, HSEA question probably to both speakers really,but especially Ian working a sort of bottom-upapproach. I just wonder about the languageyou use when you talk about human factors orhealth to engineers because I've found that onoccasion a problem. I come in to this as anoccupational hygienist and I find we talkdifferent languages, sometimes even using thesame word to mean entirely different things. Ijust wondered if you've come across that, whatsort of views you have and how you mighttackle it.
Answer - Dr Ian Randle, Hu Tech AssociatesLtdIt's a point very well made. It's got to beframed in terms that are understandable. Ithink that's very much the focus of the project -using terminology, their terminology and notour terminology, making it user friendly for thediscipline engineers. It’s kind of practisingwhat we preach as human factors professionals.It’s about the user-centred design for theinformation we're providing for that set ofusers. The secret, the solution? Well you'vegot to get in amongst them. You’ve got to learntheir terminology and you've got to getintegrated and trusted and get critical feedbackfrom what you are presenting to them andensure that it does meet their needs.
Question - Ian Loughran, Phillips PetroleumIn a previous life I had experience of the use of3D CAD modelling on a project that I workedon as a project engineer. However, myrecollection when we used the CAD model,from the point of view of human factors Ithink, is that we didn't really know what wewere looking for when we were going throughit, because we're all engineers basically.What's your experience in trying to educate,and perhaps providing check sheets etc., so thatpeople can make the most of the toolsavailable?
Answer - Ed Terry, Sauf Consulting LtdPerhaps I can answer that. I think one of thethings we don't use with the CAD model is thevisual aspect and I was interested youimmediately said ‘should we use some sort ofchecklist’? An example I'd seen my old teamuse was on aligning gas detectors. As you areprobably aware, you fit gas detectors overoffshore platforms and they don't always lookat the piece of kit that you are supposed to beprotecting. What they ended up doing waspublishing a pamphlet of views that the gasdetectors should see, straight out of the 3Dmodel. So, when it went to the fabricationyard, the guy who was fitting the detectors justhad to line up his eye along the axis and if hesaw exactly the same picture that he had in hispamphlet, it was looking at exactly the right

142
piece of equipment. Now that's an obviousexample. I'm sure there are many more wherewe could actually make use of the visual aspectof the model. As you know models areextraordinary these days, the detail isphenomenal.
I think the trick is to try and pick somethingthat's visual to help the guy who is actuallyfitting it together and then help the guy who isdoing the job. That's why we think that's goingto be such a good vehicle. It has been used andthe move is there but I think with recent turndown in activity it might just need an extralittle push back again to get back on track.
Comments - Mr Harrie Rensink, ShellInternationalMay I add some remarks. First, the model is asbad as its input. In the old days we had aplastic model, now we have a 3D model. Fine.Something more flexible but it's as bad as itsinputs. Now I'll ask the second question to youand that is, you didn't know where to checkagainst. Now I'll ask you if you are a processengineer or instrument engineer? (IanLoughran - process engineer) That's good. Sowhere do you check your design against then?Against your process engineering spec’s Iassume. So the answer to what would you beusing during model reviews is the spec’s thatshould have been developed/implemented in anearlier phase. That's the way to do a properdesign.
It's interesting that, now we are talking aboutergonomics or health or whatever, you thinkyou can do this with a check list instead offollowing your own discipline engineeringprocess? Being at least one of the steps -produce specs. And in another remark becauseI like process engineers very much, you willsee that one is one of the co authors of mypaper. I even think that's its very important tohave these types of activities integrated in theprocess engineering process because it's thesame type of analysis and it should have beenthe same type of deliverables. It also makesuse of the same type of input being a processflow scheme, at least in our approach. Soplease address this type of activity the same asyou would do with any other engineeringdiscipline would be my final statement.
Comment – Dr Ian Randall, Hu TechAssociates LtdJust one tiny bit to add to that building on whatEd has said. The complexity of the CADmodels now could mimic the posture of the
chap operating the valve manually. There isthat level of capability and so that will help toguide us. We wouldn't have to wait until he'sactually doing it, to see the posture and thehazards. We could do that at the CAD stage.
Comment – Mr Harrie Rensink, ShellInternationalThere is also the economic rule - don’t thinkthat with the pace that we are having to dotoday in project management that during areview you can change valve layouts. So,before detailed design starts you must havemade clear to the layout designers which ofyour valve layouts should be a hundred percentaccording to the rules and which of them wecan more or less forget. In the old days wewere told we will design all valves according tothe rules. That is an unrealistic statementbecause then our plants would be fromAberdeen to Edinburgh. A typical ergonomicactivity would be to identify real critical humanmachine interfaces and one of them should leadto identification of what we call category 1valve layout. That information should bepassed over to the layout guy so that he canreally work with it before the layout is frozen.The layout is frozen at the end of projectspecification. Keep in mind that everythingchanged after freezing of your project spec willresult in extra rework and we can't afford it.So, everything you think is relevant for thedesign should be brought up before that’sfinished.
Question - Mr Colin Burgess, Shell ExproOne for Harrie really. How do you sell thebenefits of human factors engineering to a maincontractor who's responsible for engineering,procurement, installation, commissioning andfit for purpose?
Answer - Mr Harrie Rensink, ShellInternationalThat's indeed a problem. If you really want tohave the proper answer you should have beenable to identify all the goals of the variousstakeholders. I touched on the fact thatsometimes an engineering contractor’s goal isquite different from an operator’s goal. It maylook a little bit basic too. I'm not askingengineering contractors to do more than theyshould do, but there are differences in goals.What we have learnt is that, if there is acontract type that enhances ‘right first time’,then a contractor will be willing to getoperators, maintenance and human factorsengineering activity up in the process (80% ofmisfits during detailed engineering are related

143
to operability and maintainability). In otherwords, look into the contract - the type ofcontract - and that will guide you at least tocheck the willingness of the contractor. At theend of the day if you look at our figures relatedto Capex and related to total cost of ownershipreduction, the plant owner should be the driverof all this type of activity. But, the type ofcontract is important for how the contractorwill act and react on proposals. Does that helpyou a little bit?
Answer – Mr Colin Burgess, Shell ExproYes, thanks.
Comment – Dr Ian Randall, Hu TechAssociates LtdCan I just add something very quickly to that.I've been involved over the years in producingresponses to human factor specifications fromoperators on behalf of design houses. Quiteoften those specifications can require a lot ofdetail but are not very specific in what theyrequire and obviously one does one's best.What strikes me is that there is then a gap interms of the enforcement of that, theverification of that, later on. I don't know if itis just that I've not won that sort of work. ButI've not really been involved in verifying thatwhat was asked for was actually beingdelivered from the human factors perspective.

144

145
DAY 2
AFTERNOON SESSION
SESSION THEME – PHYSICAL, CHEMICAL AND BIOLOGICAL AGENTS –CASE STUDIES

146

147
EXPERIENCE FROM SUPERVISION OF OPERATORCOMPANIES' ASSESSMENT OF CHEMICAL RISK.
Mrs Anne Myhrvold, Mr Sigvart Zachariassen And Mr J A Ask,Norwegian Petroleum Directorate, Stavanger
Abstract
Norwegian regulations relevant for petroleumactivities do not have specific requirements torisk assessments of chemical agents, like theCOSHH-regulations in the UK. The EUcouncil directive, ”Chemical agents at work”,includes requirements to risk assessments andthis will be implemented in Norwegianlegislation later this year.
In 1999 the Norwegian Petroleum Directorate(NPD) performed a supervisory activity ofchemical risk assessment towards the main oilcompanies operating on the Norwegiancontinental shelf.
The joint approach for the activity was to letthe companies perform specific riskassessments, while NPD followed the processfrom the identification of assessment objectsuntil final reporting, communicating andimplementing of measures. Each company wasevaluated towards their ability to performchemical risk assessment, within a holisticchemical management strategy.
NPD’s supervisory activity showed variationbetween the oil companies in all of the aspectsthat were evaluated. We observed weaknessesin identification and ability to give prioritybetween critical items, insufficient specialistcompetence, weakness in methodology andstrategy, and lack of management commitmentand employee involvement. This paperpresents NPD’s experience from thesupervisory activity and discusses genericrequirements to chemical risk assessmentmethodology.
Introduction
In 1999 the Norwegian Petroleum Directorateperformed a supervisory activity on chemicalrisk assessment towards the main oilcompanies operating on the Norwegiancontinental shelf. The background for the NPDactivity was experience from performed auditsand verifications within working environmentwhere we observed several activities just on
sampling data, but very few qualifiedassessments.
Additional motivation for starting thissupervisory activity was the data on accidents,incidents and work related diseases NPD getfrom the oil companies. These data showed asignificant number and a variety of differentdiseases related to chemical exposure.
The requirements for chemical riskassessments are found in the “Regulationrelating to systematic follow-up of the workingenvironment in the petroleum activities”. TheEU council directive, ”Chemical agents atwork”, includes requirements for riskassessments and this directive will beimplemented in Norwegian legislation laterthis year.
The goals and the approach
The goals for the supervisory activity were tocontribute to improve the companies’ ability toperform and follow up chemical riskassessment for the working environment and togenerate knowledge related to chemicalexposure relevant for the petroleum activity.NPD also wanted to contribute to experienceand knowledge exchange between parties inthe petroleum sector.
Each company performed one or a few riskassessments relevant for their installations andongoing activity. The supervisory activitystarted with a process in the companies to findout for what area and activity they needed toperform a risk assessment. NPD followed theassessment process starting with theidentification of areas and tasks, the planningphase, and continued with the performing andreporting phase. At the end of 1999 thecompanies presented the results from theperformed risk assessments to NDP. We gavefeedback to each company.

148
Areas and operations covered bythe oil companies’ risk assessments
Norsk Hydro:• Re-injection and other treatment of
cuttings (Oseberg)• Hydrocarbons relevant for operation
of offshore process plant• Chemical treatment in offshore
process plant (Saga)BP-Amoco:
• Oil based mud in shaker and mud-pitareas (Valhall)
• Relevant NDT-activitiesNorske Shell:
• Various cleaning operationsStatoil:
• Mud mixing and mud treatment(Statfjord C)
• Operation and maintenance of amine-plant for CO2 removal
• Thermal breakdown of polyurethane-coatings
Exxon:• Mud and cement mixing (Jotun B)
Phillips Petroleum Company Norway:• Use of biocides in drilling and
production• Thermal breakdown of polyurethane-
coatings
NPD’s experiences with thesupervisory activity
The experiences from the supervisory activityshowed variation in ability and qualitybetween the oil companies’ in all of the aspectsthat were evaluated. Many of the companieshad problems with performing a chemical riskassessment.
The supervisory activity started with a processin each company where they identified tasksand operations suitable for performing a riskassessment. We found that there was not asystematic approach to identify and prioritisebetween the critical items. This, together withthe fact that many of the companies did nothave a methodology established for performingrisk assessments of chemical exposure,resulted in serious starting problems for someof the companies. Some companies used riskmatrixes alone as the “method” for riskassessments, while others had good developedmethods in use. The uncritical use of riskmatrixes demonstrated the need for somecompanies to gain knowledge of riskassessment methodology.
Another connected aspect to the problems withperforming risk assessments was related toinsufficient resources and specialistcompetence. The specialists needed inchemical risk assessments are occupationalhygiene professionals and occupationalmedicine specialists together with personnelwith relevant technical and operationalbackground.
We noticed lack of management commitmentand employee involvement during theseprocesses in most of the companies. Thisaspect we specifically looked for in thissupervisory activity, since both involvementand commitment are success factors forachieving improvements.
Positive experience was also observed, forinstance the good processes in and between thecompanies, where monitored data was shared,similar problems were discussed etc. This isappropriate to one of the goals of thissupervisory activity: to contribute exchange ofexperience and knowledge between thecompanies.
Generic requirements forperforming risk assessments
The experience from this supervisory activityindicated a need for practical guidelines onhow to perform chemical risk assessments.NPD is about to finish a report summarisingour requirements and expectations to riskassessment and risk management relating tochemical agents. The report will coverprinciples and practises of the complete qualityloop (control-loop) for each step in theassessment process, from identification ofpotential hazard, monitoring and modelling ofexposure, risk assessment and evaluation anddecisions of preventive measures.
The coming report can be used as a guidelinefor the different companies to ensure a goodway of performing risk assessments. Thereport tries to give a holistic view of therequirements, the needs for resources andcompetence and the criteria for managementcommitment and employee involvement.
A successful risk assessment and riskmanagement does also depend on co-operationbetween competent participants. To make thisco-operation possible it is important to knoweach other’s competence. Further on it issubstantial to know one’s own limitation andto have competence to order additionalresources.

149
Another aspect that is essential for performinggood risk assessments is to pay attention to thequality control in the assessment process, forinstance to verify the data and to qualify thelaboratory used.
Of other generic requirements we mention theneed for transparent methodology and thenecessity for documentation of the riskassessment and the whole process. The comingreport also states the hierarchy of preventivemeasures to reduce the chemical risk.
QUESTIONS AND ANSWERS SESSION
Question – Tony Parkinson Noble Drilling,for TexacoI’m surprised that you say they’re using oil-based muds again. We thought we’d reducedthat and cut it down. Is that correct?
Answer - Mrs Anne Myhrvold, NPDYes. There was reduction in use of oil-basedmuds because of both working environment oroccupational health and the environmentoutside. But with this new technology, re-injection, we have seen oil-based mud iscoming back again.
Question - Mr Graham Cowling, AcousticTechnology LtdYou mentioned that the risk assessmentsseemed to require a specialist to carry out theassessments. Was there any evidence of anyattempt to transfer competency in doing thoseassessments to the offshore workforce and doyou think there would be any benefit in raisingthe awareness of risk assessment issues if thathappened?
Answer - Mrs Anne Myhrvold, NPDWell I think it’s important to have differentpeople in the process but of course thespecialist has to have a central role in this riskassessment. Dealing with the aspects ofworker involvement, employees do not havethe competence to perform risk assessments
like a specialist does. I don’t think it ispossible to transfer this kind of competencythroughout the company. It is important tostress the need for specialist competence. Butthe worker involvement plays an importantrole to ensure a “realistic” risk assessment.We saw that some of the companies had goodworker involvement in the risk assessment.The activity was used to visualise the risks andneed for preventive measures, and in this way“educating the company” and I think this willraise awareness of risk assessments. It isimportant to have both specialists and workerinvolvement in the risk assessment activity.
Question - Dr Ron Gardner, HSEAnne, we’ve spoken before about our parallelexperiences with hazardous substances. Inmuch of what you say I can see parallels withwhat we’ve found offshore. Right at the endthough you mentioned preventive measures,something close to every occupationalhygienist’s heart. Just what did you find inpractice because one of the things we noticedvery much was there was a great tendency tolook at something, say yes there’s a risk, here’syour personal protective equipment. What’syour experience?
Answer - Mrs Anne Myhrvold, NPDVery much the same unfortunately but stillthey are paying more attention to it. I think weare moving upwards to try other things toavoid personal equipment.
Question – Edmund Brookes, BROAI noticed in your presentation you indicatedyou were going about the process in anunusual way and following on from that youwere having your own conference or seminar,presumably in Stavanger fairly soon. Open toall? Does that include people from this side ofthe Norwegian/ UK divide?
Answer - Mrs Anne Myhrvold, NPDIf you speak Norwegian - just come. You willhave to understand Norwegian.

150

151
MEASURING OCCUPATIONAL EXPOSURE TO HAZARDOUSCHEMICALS IN THE OFFSHORE INDUSTRY
Mr Lindsay Ross, BP, Dr Ahsan Saleem, Offshore Safety Division,HSE and Mr Stuart Whiteley, Shell UK Exploration and Production
Occupational exposure to hazardous chemicalsis a daily occurrence for many workers in theoffshore industry. To manage this risk, it isimportant to have a good understanding of thenature of chemical usage offshore in terms ofthe substances used, the potential for exposureand the resulting health risks. Following theextension of COSHH to apply offshore in1995, UKOOA’s Occupational HygieneWorking Group commissioned a review ofchemical exposure data collected by itsmembers. The objectives of the review were toidentify deficiencies in the available database,provide information to support industry-widestandards and help to prioritise furtherexposure monitoring work. The reviewidentified a number of deficiencies in theavailable exposure data and recommendedfurther work to develop the offshoreoccupational exposure database. As a result aworking group was set up between HSE andIndustry to develop and carry out exposuresurveys on an industry-wide basis. The firsttwo areas identified by the working group forfurther work were the measurement ofoccupational exposure to Benzene and Drillingfluids.
Benzene is a natural component of crude oiland unrefined natural gas (0.1-3%).Epidemiological studies have demonstrated anassociation between benzene exposure and thedevelopment of leukaemia and benzene is aregarded as a human carcinogen. However, nothreshold for carcinogenicity has beendemonstrated and it is not possible to establisha level below which risks to health cease toexist. This led to the introduction of aMaximum Exposure Limit (MEL, 8-hourTWA) in the UK of 5 ppm in 1991. The firstamendment to the Carcinogens Directive,which was adopted by the EuropeanCommission in June 1997, called for revisionof the MEL for benzene over a 3 year period.The UK implemented the directive, inDecember 1998, with a phased reduction ofthe MEL for benzene from 5 ppm to 3 ppm inJune 2000, and from 3 ppm to 1 ppm in June2003. Although, the available exposure datadid not indicate a significant problem offshorethe proposed reduction in the occupationalexposure limit for benzene and somelimitations in the existing exposure data
necessitated the need for further investigation.As a result, an exposure survey was carried outjointly by HSE and UKOOA to assess theimpact that the lowering of the MEL forbenzene would have on the offshore industry(HSE, 1999a).
Over 90% of chemicals supplied offshore areused in drilling operations. Drilling fluids arecomplex chemical mixtures designed to havespecific properties under very specific drillingconditions (HSE, 1999b). Aerosols andvapours generated from the use of drillingfluids are associated with a number of ill-health effects including eye and respiratorytract irritation. Also, skin contact with wholemuds and some individual components hasbeen associated with dermatitis. Previousexposure assessments have used a variety ofsampling methodologies and various exposurestandards. There was a lack of personalexposure data but the range of available staticsampling results indicated the potential forsignificant personal exposure. In view of thepotential for exposure and the limitations in theavailable exposure data, it was decided tostandardise the sampling methods and to carryout a survey of occupational exposure todrilling fluid vapours and mist.
References
HSE 1999a “Occupational exposure tobenzene, toluene, xylene and ethylbenzeneduring routine offshore oil and gas productionoperations”, HSE Offshore Technology Report- OTO 1999 088
HSE 1999b “Drilling fluids composition anduse within the UK Offshore drilling industry”,HSE Offshore Technology Report - OTO 1999089
QUESTIONS AND ANSWERS SESSION
Question - Andy Curran, HSEYou referred to a lot of environmentalsampling. Has any thought been given tobiological sampling because obviously forcontamination of the skin, your environmentalsampling is not going to reveal that. Nor willenvironmental sampling say what they wereexposed to.

152
Answer – Stuart Whiteley, Shell ExproIn terms of the dermatitis hazard, I think that’swell understood and the control methods areactually in place for that. Simple things likepeople having good personal hygiene,changing their overalls, not allowing their
welly boots to be filled with mud, things likethat and a general awareness. In terms ofbiological sampling, perhaps Dr John Cockerat the back there can bring us up to date withbiological sampling for these sorts of issues?

153
LEGIONELLA AND OTHER ISSUES WITHIN POTABLE WATERMAINTENANCE. A CONSULTANT’S PERSPECTIVE
Dr Mark Brown, Commercial Microbiology Ltd, Aberdeen
Dr Mark BrownMicrobiologist
Microbiology at work™
Legionella and Potable Waterin the Offshore Industry -
A Consultants Perspective
®
®
Microbiology at work™
iHistory of Legionella
iBacterial cell growth
iBiofilm formation
iInspection
iCurrent legislation (L8)
Introduction
®
History of Legionella
• Outbreak of pneumonia at US Legion Convention in 1976
• Isolated organism from lung tissue - Legionella pneumophilia
• 90% of cases in UK caused by Legionella pneumophila
• Typical number in potable water may be < 1cell per litre
• Carried in aerosolised droplets (cooling towers, showers, etc.)
• Risk Groups include middle aged smokers (offshore workforce)
• Current Legislation L8 Approved Code of Practice and Guidance (January 2001)
Microbiology at work™
®
Microbiology at work™
Essentials Required For Bacterial Growth
For growth bacteria require:
• Carbon source• Nitrogen Source• Trace metals (Mg, Ca, Fe etc)
Legionella has a specific requirement for:
• Iron• Sulphur (cysteine)
®
Bacterial growth
• Growth kinetics - binary fission
• Lag phase
• Exponential growth phase
• Stationary phase
• Death phase
®
Single cell
Two cells
Microbiology at work™
Doubling time - 20 minutes
®
0 - 1
1 - 2
2 - 4
3 - 8
4 - 16
5 - 32
6 - 64
7 - 128
8 - 256
9 - 512
10 - 1,024
3.5 hr
Microbiology at work™
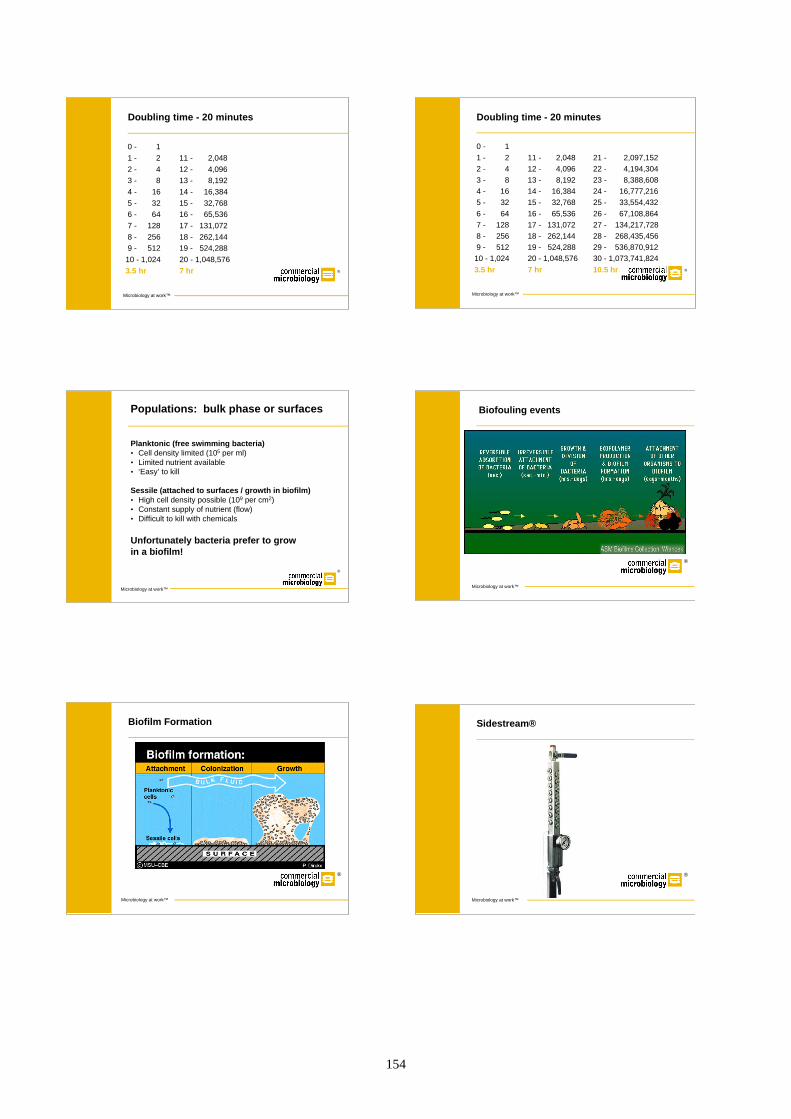
154
Doubling time - 20 minutes
®
0 - 1
1 - 2
2 - 4
3 - 8
4 - 16
5 - 32
6 - 64
7 - 128
8 - 256
9 - 512
10 - 1,024
3.5 hr
11 - 2,048
12 - 4,096
13 - 8,192
14 - 16,384
15 - 32,768
16 - 65,536
17 - 131,072
18 - 262,144
19 - 524,288
20 - 1,048,576
7 hr
Microbiology at work™
Doubling time - 20 minutes
®
0 - 1
1 - 2
2 - 4
3 - 8
4 - 16
5 - 32
6 - 64
7 - 128
8 - 256
9 - 512
10 - 1,024
3.5 hr
11 - 2,048
12 - 4,096
13 - 8,192
14 - 16,384
15 - 32,768
16 - 65,536
17 - 131,072
18 - 262,144
19 - 524,288
20 - 1,048,576
7 hr
21 - 2,097,152
22 - 4,194,304
23 - 8,388,608
24 - 16,777,216
25 - 33,554,432
26 - 67,108,864
27 - 134,217,728
28 - 268,435,456
29 - 536,870,912
30 - 1,073,741,824
10.5 hr
Microbiology at work™
Microbiology at work™
Populations: bulk phase or surfaces
Planktonic (free swimming bacteria)• Cell density limited (105 per ml)• Limited nutrient available• ‘Easy’ to kill
Sessile (attached to surfaces / growth in biofilm)• High cell density possible (109 per cm2)• Constant supply of nutrient (flow) • Difficult to kill with chemicals
Unfortunately bacteria prefer to grow in a biofilm!
®
Biofouling events
®
Microbiology at work™
Biofilm Formation
®
Microbiology at work™
Sidestream®
®
Microbiology at work™

155
Microbiology at work™
Factors affecting bacterial attachment
Materials
• Metals: Iron, Steel, Copper, etc.
• Non-metal: Plastic, Rubber, Ceramic, etc.
System Conditions
• Temperature (avoid > 20°C - < 50°C)
• Flow Rate (avoid stagnation/dead legs)
®
Microbiology at work™
Areas of interest
Areas prone to biofilm formation:
• Dead Legs• Unused cabins• Unused tanks• Drinking fountains
• Temperature abuse• Calorifier• Humidifiers
• Scale• Corroding pipe• Calorifier
®
Microbiology at work™
Offshore Monitoring (Bacterial Parameters)
• Total Viable Counts @ 22ºC and 37ºC Indicators of bacterial loading & trend analysis
• Legionella spp.
• Hot and cold systems
• ‘Complex’ equipment (e.g. TMV’s)
• UKAS accredited laboratory
According to L8 monthly monitoring should be considered®
Microbiology at work™
Offshore Monitoring (chemical parameters)
• pH
• Residual Chlorine, Chlorine Dioxide or other
• Alkalinity
• Hardness
• Metal Content • Inorganic anions
®
System Inspection
Microbiology at work™
Inspection of Physical Parameters
• Water temperature (weekly)
• Tank conditions (annual Risk Assessment (RA))
• Water appearance (weekly)
• Chemical dosing (weekly/evaluate in RA)
• Pipework condition (annual RA)
®
Summary
Microbiology at work™
• Legionella spp. Have been detected offshore
• The workforce can meet the criteria for ‘at risk’
• L8 allows a best practice approach
• Applying L8 will allow demonstration of due diligence
®

156
QUESTIONS AND ANSWERS SESSION
Question - Tony Parkinson, Noble Drilling,for TexacoIs legionella caused by inhalation or bydrinking contaminated water?
Answer - Mark Brown, CommercialMicrobiology LtdInhalation primarily, leading to colonisation inlung tissue.
Question - Tony Parkinson, Noble Drilling,for TexacoWhy does it affect smokers?
Answer - Mark Brown, CommercialMicrobiology LtdPrimarily I presume because of the state oftheir lungs; a weakened immune response I’dimagine.
Question - Bill Morgan, Shell ExproYou mentioned this at-risk. Usually in an at-risk group there’s usually some prevalencewithin an at-risk group. I’ve worked for ShellExpro for 22 years. We’ve not had a case oflegionella in 22 years. The Public HealthLaboratory system has no data whatsoever onany offshore oil worker suffering fromlegionella. Would you like to respond?
Answer - Mark Brown, CommercialMicrobiology LtdI think you’re right. There have been rumoursand speculation that it does occur offshore, butas you say there have been no documentedcases of Legionnaires disease offshore. But, Ithink we should just be aware that it’s gotpotential to occur and cause disease if we don’tcontrol it. Think of the recent BBC case withcooling towers. I think with cooling towerssome of the main problems are due to the factthat we’re dispensing perhaps a large numberof organisms into the atmosphere. With theBBC case it was found that for individuals thatwere actually walking past the BBC, perhaps athousand of those individuals wouldn’t beaffected but one would. They traced all thecases of Legionnaires disease back to peoplethat had walked past the BBC, purely becausethey were being exposed to aerosolation fromcooling towers.
Comment – Bill Morgan, Shell ExproI accept what you’re saying, but I think wereally need to try and keep the problem inperspective.
Comment – Dr Ron Gardner, HSEI can add to that. I think a better phrase wouldbe ‘people at higher risk’ rather than ‘at-riskgrouping’ but that’s a semantic point maybe. Iwant to emphasise something though. Markhas talked very specifically about legionella.Offshore you take on the water supplier’sresponsibility so don’t take the comment in L8(Legionnaires’ disease. The control oflegionella bacteria in water systems.Approved Code of Practice and Guidance) tomean that you can’t stop sampling for otherbacteria including coliforms or that you can’tstop doing chemical analysis. You have thatresponsibility under the Management andAdministration Regulations.
Could I also add that if you take those samples,(it’s a plea really), often people look at thesample results and say ‘we’re within spec’ andthey get put in a file. Look at the trends. Ironin particular Mark has mentioned – don’t lookat a one-off value. Look at the trend, becausethat will tell you a great deal, that onemeasurement, about the condition of yoursystem and the chances of you developingbacterial growth, not just legionella but otherthings as well. It’s a plea on my part really.
Question - Mark Gibb, Blowout MagazineIs the necessary equipment available and arethe necessarily qualified personnel available tocarry out the tests that are required on allinstallations?
Answer – Mark Brown, CommercialMicrobiology LtdI think it’s a difficult one but the operator has aresponsibility to be performing these riskassessments but not necessarily a responsibilityto actually be doing the sampling itself. Thiscould be given out to third party individuals.Qualified legionella risk assessors can come inand do audits for you. So it’s not necessarilypersonnel on board that need to be doing thesampling.

157
IMPLEMENTATION OF THE NOISE AT WORK REGULATIONS,OFFSHORE
Mr Curt Robinson, Acoustic Technology Ltd
Introduction
After the implementation of the Noise at WorkRegulations (NWR) offshore through SI1997/1993 “The Electricity and Noise at WorkRegulations” in January 1998, the initialemphasis was to ensure that assets had carriedout a noise exposure assessment and had beguna hearing conservation programme. In the past18 months most of these assets have reachedthe limit of the bi-annual assessment periodand a further survey has been completed.During this latest survey more emphasis wasplaced on an audit of the managementprocedures in place and the general “health” ofthe hearing conservation programme. Thispaper summarises the findings found duringthese latest assessments and highlights thegeneral strength and weaknesses of mosthearing conservation programmes.
Policy
The cornerstone for ensuring that a hearingconservation programme is likely to besuccessful is a management policy andprocedures that outlines lines of responsibilityand actions to be undertaken by identifiedpersonnel. Most assets, in the main, have anacceptable policy and procedures in place.Two common weaknesses are that it is notalways to hand and that it does not identifypersons within the lines of responsibility.Most notably, the “competent” person is alsoconsidered to be the “responsible” person forthe implementation of the regulations.
Competency vs. Responsibility
It is common to find that the medic or safetyofficer has been assigned the task of managinghearing the conservation programme. Thesepersons have often completed an approvedtraining course to demonstrate their“competency” and, therefore, they largely havesufficient knowledge to carry out anassessment, advise on hearing protection andzones, provide training and information on theeffects of noise and keep an up-to-date recordof the programme.
Competency, however, does not inferresponsibility. A “responsible person” has theresponsibility to ensure that the programme is
implemented; this requires an authority andaccess to a budget that the medic/safety officeroften does not have. If the responsible personis not identified within the managementprocedures then it will default to the OIM asopposed to the competent person. If theexposure assessment identifies a particular areathat gives rise to a significant proportion of therisk to the asset, then it is the responsibleperson who is required to ensure that that riskis minimised to as low as reasonablypracticable. This is not an impediment toassigning the responsible task to the competentperson, however, they must be authorised withthe necessary authority, support and funds toinitiate improvements/actions where necessary.
Assessment (Regulation 4)
ATL’s noise exposure management systemassessment programme (NEMS) has beeninstalled on the majority of assets within theUK sector. The programme, which is intendedfor risk assessment, assesses the long termexposure of personnel (work patterns areassessed typically over a two week shift – withthe sanction of the HSE) whereas theregulations set their criteria based on dailyexposure, for highly variable tasks theexposure may also be averaged over a week.
For example:
A Mechanical Technician is required to run thefire water pumps (2 off) once a week. Eachpump is run for 15 minutes, only 5 minutes ofthat time is spent within the pump enclosurewith the engine running (room noise level –108 dB(A)):
• The fractional exposure for this activity is91 LEP,d.
• The weekly fractional exposure for thetechnician will be 83 dB(A);
• If there are 4 mechanical technicians withinthe team and each is equally likely to carryout the task then the group fractionalexposure reduces to 77 dB(A).
Over the long term, therefore, ensuring anequal rotation through the task, reduces therisk to a minimum level. It is still important toremember that for the day the task is carried

out, the technician will have a second actionlevel exposure.
The benefit of the NEMS system is that itprovides an overall risk assessment of theasset, it identifies personnel most at risk fromnoise exposure and areas within the asset thatgive rise to that risk. This is useful whenconsidering the practicability of noise control.
In addition, NEMS normally does not includecontributions from hand tools unless they arepart of the job function (e.g. needle guns forthe paint crew). Therefore, personnel that use“high noise” tools such as impact wrencheswill significantly increase their daily exposurelevel.
For an asset using NEMS, ATL recommends adosimetry programme (also an HSErecommendation). The purpose of this is toverify and trend the noise exposure of specifictrades, using a meter worn throughout anumber of shifts. The benefits of dosimetrystudies include:
• Verification – particularly appropriate toborderline first and second action levelcases, individuals with high second actionlevel exposures and trades with highlyvariable work patterns.
• Information from dosimetry can be used toadjust and fine tune the NEMS model.
• Undertaking dosimetry allows contact timeto discuss noise issues with persons most atrisk and maintain awareness of noise.
• Providing data on peak levels and whetherthe action level has been exceeded.
Surprisingly the dosimetry data does show thatthe 200 Pa level can apparently be exceededregularly. Analysis has shown that thiscommonly occurs around traditional “break”periods. Possibly due to a heavy karaokesession in the ‘coffee’ areas, more likelythough to be due to an impact on themicrophone as the overalls are removed andstored in lockers. Another likely cause is theinterference from radios located in the samearea as the dosimeter microphone.
Most modern assets (built within the previous10 years) still have healthy reservoirs and,therefore, have larger budgets to work withand are open to implement noise controlmeasures. Often these assets are looking at de-bottlenecking or other projects to improve theefficiency/output of the asset and it is possibleto incorporate noise control improvements intothese projects, thereby demonstratingcontinuous improvement.
For older assets where the production ratemight not be so healthy, budgets are muchtighter, equipment older and noise controlimprovements do not appear as desirable.
We believe that there are still some measuresthat can be implemented that can reduce thenoise exposure risk and effective noise controlmeasures need not always be expensive. Forexample, high noise levels within a waterinjection module were traced to a control valveon the discharge line of a non operating waterinjection pump that had not properly seated;water was flowing back through the valve.Repairs to that valve would improved thewater injection system and reduce the noiselevels within the module by 3 dB(A) (or interms of fractional exposure, by 50 %).
Another method is to implement a noisecontrol register of all measures implementedon-board. The register can then be auditedannually and used to demonstrate that themeasures already incorporated are maintainedand kept in good condition.
Two case studies given below illustrate thatnoise control measures can be cost effectivealthough they may not always achieve thedesired goal!
CASE STUDY 1 An acoustic enclosure wasfitted over a water injection pump. Measurednoise levels increased by 4 dB(A) after theenclosure was fitted. Preliminaryinvestigations suggest that the enclosure hasbeen rigidly fixed to the skid, thereby allowingthe large enclosure panels to become aneffective radiating surface for energytransmitted through the package structure.Noise levels were not improved be leavinglarge apertures open on the enclosure.Isolating the enclosure from the skid with aresilient strip and sealing the apertures shouldimprove the effectiveness of the enclosure.
Noise Exposure Reduction (Regulations 6and 7)
158

159
CASE STUDY 2 A JT gas exchanger locatedwithin the process module generated surfacenoise levels to 118 dB(A) from pipeworkleading from the dry gas scrubber to theexchanger. Applying acoustic insulation to
this pipework, less than 30 m in length woulddecrease deck noise levels by upwards of 5dB(A) and the overall asset risk byapproximately 40 %.
Hearing Protection/Zones (Regulations 8and 9)
This is considered to be the facet of theregulations that is most closely followed, mostassets maintain a minimum number ofprotection devices and these normally provideadequate coverage. Areas for improvementthat have been noted are:
• It is considered good practice to havemarked up plot plans in the coffee areasand at exit points from accommodationmodule, highlighting areas of risk;
• The issue of ear muffs or moulded plugsshould be recorded to illustrate that thedevices are replaced at the correct intervals;
• It is important to ensure that hearingprotection devices provided to contractorsby their employers are in good conditionand are acceptable for use on the asset.
One major inconsistency found across assets isthe policy of mandatory use of hearingprotection outside accommodation modules.The major arguments for this policy presentedby the assets are:

160
• Hearing protectors should become acceptedas part of PPE similar to the use of eyeprotection;
• The policy is easier to enforce;• It minimises the risk of hearing decay.
We believe that the arguments against are:
• Compulsory use of hearing protection isnot enforced by the HSE in areas below 85dB(A);
• Wearing of personal hearing protection inlower noise areas could impedecommunication including the hearing ofPA announcements that may contain safetymessages;
• Wearing of hearing protection can beuncomfortable over a long period of time(especially ear muffs worn in conjunctionwith spectacles);
• Complacency in removing hearingprotection in obvious quiet zones and notreplacing them for high noise level areas.
Most importantly it was understood that theHSE was against this policy because the goalof the regulations was to minimise the risk toas low as reasonably practicable without theuse of hearing protection.
We believe that the implementation of thispolicy has become confused with the HSEendorsing the mandatory use policy on someassets whilst requesting other assets to desist;this has made the arguments against the policydifficult to defend and is an area that requiresclarification.
Records (Regulation 5)
This is an important area, particularly for theemployer, as it is through record keeping thatholds the evidence demonstrating theimplementation of the regulations. Most assetsare good at storing copies of reports ofexposure assessments and noise controlstudies. The main weakness is in keepingrecords of services provided to employees.This includes hearing protection, training andinformation provided.
Health Surveillance
Although health surveillance is not mentionedwithin the regulations it is covered within theManagement of Health and Safety at WorkRegulations and is specifically mentionedwithin the HSE guidance notes of the NWR“Reducing Noise at Work”.
“The appropriate technique for noise healthsurveillance is audiometry”.
The important facet about audiometry is that itis the feedback loop that demonstrates that theobjective of the regulations “to preventdamage to the hearing of workers fromexcessive noise at work” has been met.Unfortunately most audiometry is carried outby third parties, records of previousassessments are not always kept in a centraldatabase and the data is rarely audited to assessthe effectiveness of the programme. It isunlikely, therefore, that any feedback occurs toenable the responsible/competent person to usethe data to improve the programme.
Some assets carry out audiometry onboard,which gives the competent person morefeedback on the success of the programme.ATL is in the process, with a major UKoperator, of maximising the information thatcan be obtained with audiometric screening atthe work site. Audiometry is now carried outannually and instead of trying to minimise thepossibility of personnel suffering fromTemporary Threshold Shift (TTS) by carryingout the tests in the morning, etc., the tests arecarried out at the end of each shift in order tolook for TTS. If a person is displaying TTS, itis evidence that the hearing conservationprogramme has failed in some way for thatperson, because if hearing protection had beenworn correctly then the exposure should beless than that required to give TTS. The testsmay not be as accurate as those carried outonshore but if a person is demonstratingworrying signs of hearing threshold decay thenthey should be referred to a practitioner as amatter of course where a more accurateassessment can be carried out.

161
Category 1 to 3: “Referral Category 4: “Warning” Category 5: “Acceptable”
Example of Audiometric Data for a UK Field Assessed against HSE Criteria in 1999
In this way the competent/responsible personscan be satisfied that they have implemented asuccessful hearing conservation programme.
Summary
In summary, it is believed that most assetshave implemented the regulations in goodfaith, keep up to date with the assessments andensure that the hearing protection provided isadequate and is used by personnel.Weaknesses include not differentiatingbetween competent and responsible persons,not keeping records on training andinformation provided or operating an adequatehealth surveillance programme.
QUESTIONS AND ANSWERS SESSION
Comment – Mr Kevin O’Donnell, OffshoreSafety Division, HSEA bit of feedback on your view, or the viewexpressed about HSE’s view of total hearingprotection zones outside the accommodation. Ihave come across them but to say that HSE‘thinks it’s good’ - I’m sure you have quotedother people who say that’s not true. Our viewis that, at best, it’s a rather crude way to dealwith the problem. It may be appropriate on
smaller platforms, perhaps where it’sparticularly noisy. But it is open to abuse ifyou do find quiet areas because people willtake their hearing protection off. I would saygenerally it’s the lazy way out, so I would saygenerally we are not keen on it. It’s notsomething that we can prohibit as such though,but to say we think it’s a good idea, I hope thatmy comment reflects that we don’t think it’s agood idea per se.
Answer - Mr Curt Robinson, AcousticTechnologyI agree. All I think is that perhaps it is the wayit’s communicated to the people because it’sthen been disseminated through the otherassets and so forth so as soon as I say I don’tthink it’s a good idea I get this feedbackcoming through.
Question – Unknown speaker, offshore medicwith ShellI recently attended a noise awareness courseand want to know if it is true that levels are todrop by 5dBs.
Answer - Mr Curt Robinson, AcousticTechnology Ltd
2215 13
19
68
0
10
20
30
40
50
60
70
80
1 2 3 4 5
HSE Category
% P
op
ula
tio
n

162
There was a European Directive a while backwhere it was proposed that the levels bedropped by about 5dBs. Basically, it is not somuch that the first action level becomes 80 butit’s really having the actions commensuratewith the second action level applying after85dBs. Then nothing really happened fromthat and it met with some resistance. But it’sinteresting that the European Presidency hasjust changed over to Sweden and there is aVibration Physical Agents Directive that’sbeen on the cards for a while now looking atHand Arm Vibration. It’s been a bit of afootball. The Swedish Presidency suddenlyalso reintroduced the Physical AgentsDirective on noise. At the moment it’s up as aproposal and up for discussions.
Question - Bob Hanson, BG GroupThe data that you presented is from onecompany and it refers to fixed installations. Isthat correct?
Answer - Mr Curt Robinson, AcousticTechnology LtdIt’s mainly fixed installations. There are acouple of FPSOs in there as well.
Question - Bob Hanson, BG GroupHave you done any work and have you anydata on drilling rigs and how did the twocompare?
Answer - Mr Curt Robinson, AcousticTechnology LtdThat’s something we’re hoping to look at inthe next six months. We had a federal contractwith BP to oversee noise management issues,so that’s where I got my data from. But ATLhas done a number of measurements on allsorts of installations and it’s something thatwe’ll be looking at producing in the future, thatis the comparisons between different types ofvessels.
Question - Bob Hanson, BG GroupThe reason I ask the question is from my ownexperience it would seem that when you arriveon a drilling rig that they do tend to be noisier.I know it’s anecdotal but I’d be interested ifany of the drilling organisations have done anywork in assessing noise exposure on drillingrigs specifically.
Answer - Mr Curt Robinson, AcousticTechnology LtdIt is part of the legislation, that they need to Ithink that the effort put in by some of thedrilling companies is equal to the oilinstallations. Because of the fact that they aresmall and live then yes, there are noise issues.But I’d like to think that the drilling companiesare taking measures to put precautions through.

163
THE LSA FOCUSED RESULTS DELIVERY PROJECT ON NORM
Mr Brian McKendrick, Shell Expro
The FRD Team and Why it WasFormed
Focussed Results Delivery (FRD) projects areused by Shell Expro to bring a high-poweredteam to focus on a problem which has becomeintractable, proven “too difficult” or needsmultiple skills. The team has a sponsor,usually an Asset Manager, a budget and a tighttimescale. Team dynamics training is used tomaximise team effectiveness. It is, in effect, a“tough nut cracker”.
Shell Expro has had Naturally OccurringRadioactive Material (NORM), in the form ofLow Specific Activity (LSA) scale, within itswells, plant and pipelines for many years. Ithas developed working procedures (LocalRules) and recording systems to manage theproblem over the years. These have beendeveloped in a “top down” way - companyexperts writing procedures for the workforce toapply.
However a number of issues had recently madeus uncomfortable about our NORMmanagement systems. These included -
1 A growing NORM contamination of theprocess plant on our platforms, both interms of extent and activity. In effect, allof our oil producing wells and processesare NORM contaminated. NORM is alsobeing found in service water systems.The NORM in some wells, coolers andother equipment is also growing steadilymore active.
This in turn means that many more staffare potentially exposed to NORM.Virtually every maintenance job now hasa NORM dimension. It also means anincreasing burden to the business in termsof planning, preparation, delays, costs,training and record keeping.
2 An increasing number of incidents whereNORM contaminated equipment has notbeen identified or has been wronglyassigned. The installation of a gatedetector at our Torry base now identifiesevery mistake. Each of these incidentshas potential legal exposure andreputational damage if the contaminated
item is not caught before it leaves ourcontrol.
3 The Scottish Environment ProtectionAgency (SEPA) has adopted a muchmore stringent inspection approach,particularly on record keeping, and hasidentified certain shortcomings.
4 ISO 14001, the environmentalmanagement standard, requires rigorousdocumentation systems, and while theNORM systems passed the inspection,the piecemeal nature was noted.
In response to these concerns, an FRDapproach was used to improve the NORMmanagement system. The logic was that thework was urgent and important, so neededconcentrated and dedicated effort. It was amulti-stakeholder issue, so needed input from arange of angles, and in particular fromoperators who had not really been involved inthe decision making in the previous “topdown” process.
A team of eleven people was set up, consistingof radiation specialists (RPA, corporate andBusiness Unit), plus representatives fromoperations, logistics, procurement, productionchemistry and a decontamination contractor.All the key stakeholders were represented.
The FRD Process
The FRD project was sponsored by ShellExpro’s Tern/Eider/North Cormorant (TENC)asset.
The team spent three days together off-site tobuild, exchange positions and analyse the jobin hand. Team building exercises helped tobuild inter-personal understanding and trust.Rules of engagement were agreed.Brainstorming of the key NORM issues foreach individual, and thus each sector, wascarried out, and this was used to identify theperfect situation and the gaps to be filled. Acomplete general process map of NORMmanagement from identification to disposalwas developed, and possible improvementactions locked into each stage of the processmap. These were then assessed, prioritised andlocked into an improvement plan.

164
Each person on the team then worked theiractions from the plan, meeting at monthlyintervals to report progress and agree nextsteps as required. The Team Leadermaintained rigorous control on progress.
Concrete Deliverables
The concrete deliverables developed by theFRD team fall into five groups -
• Working Procedures• Identification and Marking of
Contaminated Equipment• Record Keeping• Disposal• Information, Instruction and Training.
WORKING PROCEDURES
Analysis of the NORM Processes andFlow Diagrams
The overall NORM process and each sub-process was mapped. Decision points wereidentified, and bottlenecks, duplications andunclear areas considered and resolved. Theinformation flows supporting each processwere also mapped and streamlined. This wasused as the basis of Local Rules review.
Improved Definitive Local Rules
The Local Rules (radiation protectionprocedures) were reviewed by the team in acollaborative way. Two workshops were heldwith the Radiation Protection Supervisors fromthe offshore installations, at which further lineby line reviews were carried out. This meantthat all players had their concerns addressed,that good ideas from the users wereincorporated, and that a much greaterownership and understanding of the procedureswas obtained.
A pocket (A5) version was also produced foroperator use on the plant.
Rationalisation of Permit Checklistsand Local Rules
Some contradictions between Permit to Workchecklists and Local Rules were identified. Anew system was set up where the Permitsignposts directly to the Local Rules onradiation matters, rather than to checklists.
IDENTIFICATION AND MARKING OF
CONTAMINATED EQUIPMENT
Process Map for each Installationwith NORM Areas Highlighted
At the request of the FRD team, eachinstallation developed a process plan, markedup with areas known to be NORMcontaminated and a feel for the extent of thecontamination. This will be used in workplanning to predict NORM problems at theplanning stage.
The Aberdeen University NORMProject
Shell Expro has sponsored a project atAberdeen University, part of which is toidentify better meters for identification ofNORM contamination. The researcher waspart of the FRD team, which allowed betterunderstanding of the operator requirementsfrom such meters. It also allowed the FRDteam to understand the restrictions andtradeoffs on such meters.
Use of EP15 Meter to ConfirmExternal Tubular Contamination
A particular problem addressed was theidentification of external contamination oninternally contaminated tubulars, where theinternal NORM affects the external reading. Asolution using an alpha sensing meter wasdeveloped.
Better SAP Descriptions of Meters
The SAP ordering system was revised to give abetter description of the NORM meters andthus make new meter ordering easier.
Improved Meter RecalibrationProcess
The meter repair and recalibration process waschanged from each installation having its ownmeters and organising their own repair andcalibration, to a pool of meters being held byAberdeen University and receipt of a brokenmeter stimulating immediate return of a newmeter. True NORM calibration standards willalso be used. This will give better turnroundtimes, better use of the meter pool and bettercalibration.

Improved StandardTaping/Tagging/Labelling
Conventions
Marking of contaminated items was reviewed,and new improved tape, tags and labelsdesigned. Green tape and labels for tested -externally clean items were introduced.
RECORD KEEPING
Improved Source Register Layout
The Source Register, which is the on-siterecord of audit and use of radioactive sources,was reviewed and improved in a collaborativeway. Several new fields were introduced toallow better traceability across the total life ofthe source.
Electronic Source Register
The FRD team has initiated work on anelectronic source register to replace thepaper version. This will give betteraccess and search features.
Improved LSA Work Record Form
The LSA Work Record Form, which is theoverview of each NORM job, was reviewedand improved in the same way. A jobnumbering system was developed, and severalnew fields were introduced to give a completerecord of the job.
New Sampling/Testing/RecordingSystem for Offshore Discharges
A better sampling, testing and recordingsystem for offshore discharge data wasdeveloped and installed. New features includethe use of Production Chemistry ascoordinator, sample tracking through theintranet and result calculation and recordingthrough a shared data system accessibledirectly from offshore.
New Recording System for OnshoreNORM Arisings
A shared data system capable of assigningShell NORM arisings at AEAT Dounreay backto the source platform was developed andinstalled. This is also accessible directly fromonshore.
The annual Radiation Protection Adviser audithas been enlarged to include a detailedinspection of records.
DISPOSAL
Improved Information Flow andTransaction Efficiency between
Shell and AEAT
The relationship and interface between ShellExpro and its onshore decontaminationcontractor, AEAT Dounreay, was discussedfully. Inefficiencies and “niggles” wereidentified and corrected, particularly aroundjob accounting and information flow.
Sponsor, Plan and Test Platform forNORM Reinjection
Shell Expro considers reinjection as the bestpracticable environmental option for NORMdisposal. Regulators are presently consideringthis option, and, if so minded, will permit itthrough review of Authorisations. The FRDteam reviewed the technical and radiologicalprotection issues around reinjection, andidentified the Tern as first candidate platform.
Consideration of NewDecontamination Options
The FRD team investigated a series of ideasfor more efficient decontamination ofhardware, such as chemical dissolving (in situor in baths), ultrasonic cleaning, and differenttypes of jet hosing, such as in situ retrojetting.While these are all longer term projects, theteam intends to keep a watching eye on them.
INFORMATION, INSTRUCTION AND
TRAINING
Policy on NORM versus LSA NamingConvention
There are two distinct names in Shell Exprofor the radioactive material produced with wellfluids - Naturally Occurring RadioactiveMaterial (NORM) and Low Specific Activity(LSA) scale. Both names have their strengths,but two names for the same thing can beconfusing. The FRD team consideredstandardising on one name, but settled on acompromise position.
Improved Record Auditing
165

The FRD team has developed its own brandstyle, with a definitive logo. The newsletter,overhead pack etc are in this style. This willgive an identity to NORM informationalmaterial.
Training Matrix
A matrix of NORM competence, on a scale 1(aware) to 5 (expert) was produced. Thisshows the level of competence that eachposition with NORM responsibility requires.It also gives guidance on training methods toreach each competence level.
New Training Package
A new overhead training package wasproduced. This is a resource pack, allowingthe presenter to select material from the packappropriate to the knowledge and needs of theaudience. It also includes a matrix which tiesinto the competence matrix above to guide thepresenter on the material to use with eachaudience.
Computer based training (CBT) for delivery oflower level training was investigated, but theFRD team felt that for such a complex andemotive subject, person to person training wasbest.
Onshore Awareness and Training onNORM
It was recognised at an early stage thatplanning of the NORM elements of workshould start in the onshore planning of the jobrather than when NORM is encounteredoffshore. This requires a greater awareness ofNORM management among onshoresupervisory, support and planning staff. Aseries of onshore workshops (about 2 hours)were run to raise onshore awareness.
Setup of RPS Network and RPSWorkshops
The was a recognition that the RadiationProtection Supervisor (RPS) - the on-sitesupervisor responsible for NORMmanagement at each location, is critical to thesuccess of the system. An RPS network wasestablished and two large one day RPSworkshops run to get a common understandingand discussion of issues, and particularly adetailed review of the Local Rules.
The FRD team produced two NORMnewsletters aimed at the general workforce.Feedback on these was good.
SOFT DELIVERABLES
In addition to these concrete deliverables, theuse of the FRD process in this way sent severalimportant messages around the organisation.The following were important.
Demonstration of Seriousness andCommitment to Solving NORM
Problems
While the management has repeatedlyemphasised the importance of proper NORMmanagement, this amount of concentratedeffort gives tangible evidence of thatcommitment.
Better Onshore/Offshore Liaison onNORM Issues - Openness and Trust
The involvement of operations anddecontamination contractor personnel in thedecision making around NORM gave a betteropenness and trust across the onshore/offshoredivide. By co-creating the solutions, a betterunderstanding of where they came from andwhy they are the way they are, and thus abetter ownership and buy-in, was obtained.
Emphasis on Onshore planning ofNORM Work
The Local Rules and onshore training nowemphasise the need for NORM management tobe built into workplans right at the onshoreplanning stage.
Knowledge Improvement of FRDTeam - Ambassadors
Participation in the FRD project created agroup of eleven people with a much greaterappreciation of NORM issues, who will act asadvisers and ambassadors for the issue in theirbusiness sectors.
Focusing and Communicating theRange of NORM Work Ongoing
The FRD team found that a number of smallprojects and initiatives on NORMimprovement were going on in isolation. Alsoa lot of good ideas had been implemented on
FRD Brand Style (Logo, Look) NORM/LSA NEWSLETTERS
166

167
specific locations. The FRD team focussed,collated and communicated these.
Understanding of Pros and Cons ofOffshore versus Onshore
Decontamination
There has been a growing demand for offshoreNORM decontamination. The FRD team,during the mapping phase, reviewed whenoffshore decontamination is appropriate, underwhat circumstances, and what arrangementsmust be put in place. This has been formalisedinto the Local Rules.
Contact with SEPA
SEPA is the regulator of NORM disposal.They were kept appraised of the work beingdone by the FRD team, and invited to presenttheir position at the RPS workshops. Thisallowed us to give SEPA a favourableimpression of our commitment to improvementof our NORM management, and allowed us abetter understanding of the drivers on them asregulator.
Contact with AEAT
AEAT is Shell Expro’s onshoredecontamination contractor. They wereinvited to present details of their business atthe RPS workshops. This gave a betterunderstanding of what they do.
Ideas Exchange with BP
BP has been appraised of the work of the FRDproject, and is impressed with what has beendone. Joint opportunities have been identified.
Setup of Radiation CoordinationGroup
FRD teams, by definition, do the workrequired, then disband. It was felt that, toembed the lessons of the FRD project and tomaintain the new systems, a RadiationCoordination Group be set up to maintain themomentum. The membership will be the sameas the FRD team, and a Terms of Referencehas been drawn up.
Conclusion
The use of an FRD approach has resulted in amuch more robust NORM managementsystem, with the requirements of allstakeholders recognised and accommodated,and understanding and buy-in from around the
business. This would not have been achievedby conventional review systems.
Team and Authors
Paul Abernethy DecontaminationContractor Representative
Fred Beadling OperationsJim Beresford-Lambert Procurement AdviserDouglas Clark Corporate HS&E Adviser
Contact AuthorMuriel Dorthe Research StudentErica Edwards Logistics AdviserTerry Harvey OperationsBrian Heaton Radiation Protection
AdviserBrian McKendrick Operations LeaderIan Reynolds Northern Business Unit
HS&E AdviserStuart McGregor Production Chemist
Dave Windle TENC Asset ManagerSponsor
QUESTIONS AND ANSWERS SESSION
Question - Ed Brookes, BROACould I kick off Brian. That’s a veryinteresting video. Is that just for Shell or areyou going to be making a profit and selling it?
Answer – Mr Brian McKendrick, Shell ExproLet’s face it, with health and safety andenvironmental matters in Shell Expro we don’tmake profits! But we’re happy to share ourexperiences with other operators.
Question - Dr Ahsan Saleem, HSEI was interested in the training matrix, whereyou had level 1 to 5, and particularly with thefact that you said there is some offshoredecontamination work that goes on. Do youhave any classified workers and how do youmonitor their doses?
Answer – Mr Brian McKendrick, Shell ExproBasically our classified workers are from ourISE contractor, Rigblast, and they areclassified workers and they do havecertification for offshore decontamination.
Question - Alan Wilson, PGSNot just the video for across industry trainingbut it looks as though the entire job has beenwell thought out and I’m also impressed. Withthe rest of the training, is that possible forsomething like a cross industry initiative?
Answer – Mr Brian McKendrick, Shell Expro

168
The actual training consists of, from level 1 tolevel 5, about 65 viewgraphs. Obviously forlevel 1 only about 10 or so viewgraphs will beused and then up to level 5 (the expert level),the 65. I’m sure that they can also be madeavailable. Is that okay Stuart?
Answer – Mr Stuart Whitely, Shell ExproYes, Brian. The main forum for sharingknowledge that we’ve got at the moment is aUKOOA Radiation Working Group which sitsunder the Environmental Committee. I thinkin time it will be forming links with BROAand IADC and people like that, again to sharethe knowledge as wide as possible.
Question – Mr Lindsay Ross, BPI just wonder if you use this FRD focusedresults delivery nutcracker that you have hereto tackle any other kind of occupational healthhygiene-related issues?
Answer - Brian McKendrick, Shell ExproI’m actually sure we do. People in the ShellExpro safety department, have you got anyhistory of this? [to colleagues in audience – noimmediate response] For instance, with theenvironment, we had to go back to flared gason one platform. It was so huge we knew therewas a problem but the difficulty was againthere were quite a few potential solutions. Wehave a big FRD team at the moment looking atthat as well, but it’s not a very goodreputational thing for our platforms.
Comment – Mr Lindsay Ross, BPFor a similar size organisation (BP) it seemslike a good way of approaching these type ofissues.

169
TACKLING BAD VIBES IN THE OIL AND GAS INDUSTRY – ACASE STUDY ON HAND ARM VIBRATION SYNDROME
(HAVS)
Mr Stuart McIlroy, Senior HSE Advisor, Halliburton Brown andRoot
Introduction
According to HSE funded research more than amillion workers are exposed to potentiallyharmful levels of vibration. Around 300,000have symptoms of vibration white finger. Theproposals for a Directive on vibration areprogressing through the E.U System and arelikely to effect all activities that cause handarm vibration. If as seems likely the directiveis adopted this will lead to the introduction ofexposure limit values and with it a change inU.K law, this in turn will have a significantimpact on how organisations manage the risksassociated with Physical agents such asvibration.
It would be reasonable to say that If employersare to work within the law they have to ensurethey have effective means of controlling therisk associated with using hand held powertools.
This was highlighted in the1996 test case whena group of miners took out a civil actionagainst their employer and successfully wontheir case. The employer - British Coal werewell aware of the dangers of using percussiontools as far back as 1973, they had carried outa study, the results of which were largelysuppressed or ignored. The judge ruled thatthey should have taken steps to prevent injuryby warning those working with percussiontools of the possible dangers.
Workers whose hands are regularly exposed tohigh vibration may suffer from several kinds ofinjury to the hands and arms - collectivelyknown as Hand Arm Vibration Syndrome(HAVS) common names for such injuries are• Dead Finger• Dead Hand• White finger
The injuries may be due to impaired bloodcirculation, neurological and muscular damageor damage to joints.
Damage is progressive and may not beapparent initially; gradual numbness andpaleness increase with cold conditions
followed by pain and loss of grip duringmanual tasks. HAVS is a prescribed industrialdisease and is reportable under the Reportingof injuries, diseases and dangerous occurrenceregulations (RIDDOR).
It can be seen as a ‘people problem’ – it hurtspeople in the workplace and continuedexposure to high levels of vibration can makethe health effects irreversible. The results ofthis type of exposure are graphically shown inthe HSE health promotion video “Hard toHandle”
The Case Study
The case study looks at vibration issuesidentified during work carried out by membersof the integrated HSE team on Shell CentralBusiness unit.The focus is on the way in which informationand ideas were shared with others within theindustry and how that communication processensured that the tools were available foreffective management of the issue within theOil and Gas Industry.
At the start of 1998 there was a nervousnesssurrounding the possibility that the Physicalagents directive would be introduced – thiswas the directive aimed at controlling vibrationexposure to individuals who regularly usedpercussion/power tools.
The HSE were raising the awareness of theHAVS problem and were also taking a keeninterest in how companies were managing theissue – from a business unit perspective wewere conscious that existing controls formanaging vibration exposure was based oncustom and practice rather than scientificmeasurement.
In conjunction with the Tool Manufacturersand fabric maintenance contractors a powertool trial was set up the main deliverablesbeing to:-
• Measuring the vibration exposure levelsgenerated by using hand held power tools

170
• Benchmarking against current exposurestandards
• Identify areas of weakness in achievingcompliance with future legislation
Occupational hygienists were contracted in totake measurements to a recognised industrystandard; all power tools were tested undernormal operating conditions. By being proactive in addressing the issue this provided agood opportunity to apply best practice withinthe business unit.
During the course of 1998 the team gatheredinformation internal and external to theindustry on how best to tackle the issues –Shell occupational health departmentintroduced Design Engineers from AtlasCopco who manufactured low vibrationtooling. – They had vast experience indesigning high performance tooling forindustry and had worked extensively in thisarea with British Aerospace.
British aerospace were happy to share theirexperiences with us and this gave us somedirection on how to formulate a workablepolicy for controlling HAVS,
This led to the introduction of a Business unitHAV policy developed as an operational guideto managers and supervisors to assist them inapplying appropriate controls for the healthand safety of exposed employees. The keyelements of the policy were as follows
• To provide management awareness ofwhere there might be a risk of HAVS andthe type of control measures to reduceexposure
• To enable those employees likely to beexposed to recognise and understand thenature of the problem and the precautionsto be observed
• To ensure the above employees recogniseearly onset of symptoms and how to obtainexpert advice.
During the first quarter of 1999 a series ofmeetings were held involving Atlas Copco aswell as operating and service companies fromthe industry.
It was clear from the large number of attendeesat these meetings that many companies hadbeen working in isolation on the issue, manycompanies were already implementingworkable solutions to reduce vibrationexposure for example: -
• Introduction of engineering controls suchas ultra high pressure water jetting as amethod of removing weld metal around ascrap compressor housing. Conventionalremoval would mean hours of exposureusing a caulking gun
Such controls were identified and implementedas part of the activity risk assessment process,care being taken not to eliminate one problemand introduce another!
A consensus was reached that a co-operativeapproach was the way forward to facilitateunderstanding and common ground tomanaging the issues.
There was recognition that HAVS was a liveissue and not all companies would face thesame problems in addressing the issue. Oneexample being the Fabrication Facility wheredue to the nature of the business workforceexposure to vibration may be high. Comparethis against a small offshore installation wherethe use of power tools is infrequent – in bothcases there would be a need to balance the costof proposed controls against the perceived riskof exposure.
Lack of available HSE resource would alsopresent problems to small service companies –how many could call on a residentOccupational health expert to give them soundadvice, the more likely scenario being one oftaking HSE advice from ‘another hat’
HSE specialist inspectors attended thesemeetings, they acknowledged that the groupwas moving along the right lines in terms ofidentifying where likely exposure would arise.The question was raised as to who ‘owned ‘theproblem was it the oil companies or thecontracting companies themselves
Although operating companies haveresponsibility to satisfy themselves thatactivities are being carried out on theirinstallations and Facilities in a safe mannerultimately it’s the contracting companiesresponsibility for managing the risk and for thehealth of their employees in the workplace.
Given that ownership of the problem lay withthe contracting companies it was decided thatthe best way to raise the profile would bethrough the Offshore Contractors Association.
A case was put before the OCA Technicalcommittee who noted that although there wassome excellent guidance already published

171
including the HSE publication VibrationSolutions it was agreed that there was a needfor some specific industry guidance -consequently a working group was set up witha remit to: -
• Develop a guidance document that wouldbenefit and recognise the broad needs ofthe oil and gas industry i.e. fabricationfacility V small manned platform,occupational hygienist V “another hat”.
Practice Sharing Opportunities
The OCA document entitled Guidance notesof Good Contracting Practice within the Oiland Gas Industry –Hand Arm VibrationSyndrome was published in January 2000.
Prior to issue of the document practice sharinghad been carried out in an ad hoc manner –within my own organisation this was achievedby carrying out presentations at safetymeetings and forums and through articlespublished in company bulletins
After publication of the OCA guidance wewere able to promote the document in a moreformal manner. Forums such as the Industryled Step Change in safety presented anopportunity to promote the work carried out todate -the shopping Mall workshops werespecifically set up to enable anyone to cherrypick good ideas and best practice for usewithin their own organisation.
To date a total of 200 copies of the documenthave been taken up by member companies ofthe OCA and operating companies ofUKOOA.
An OCA data bank was set up to encouragefurther sharing of knowledge and experienceson the subject, reference and how to access theOCA data bank are made in the document.The OCA working group acknowledged this asa further opportunity to cascade and shareknowledge and experience – so far there hasbeen poor response to this offer
In November 2000 the case study was used asan example of how the practice sharing processpresently works in the Oil and Gas Industry,there were seen to be many plus pointsincluding: -
• Exchange of information and vibration casestudies within the industry
• Buying in of experience external to ourIndustry – British Aerospace study
• Agreed common approach for managingthe issue
• Tangible benefits to the workforce
With the imminent introduction of the PhysicalAgents Directive comes new challenges, dailyexposure action values and daily exposurelimit values will be introduced to protectpersonnel exposed to vibration on a regularbasis. The Directive will have an impact onmeasurement methodology and with it a needto develop standard methodology for taking ofmeasurements.
The OCA Health Committee met in November2000 to follow up on identified issues and willcontinue to work towards industry widestandards for management of HAVS.
Conclusions
One of the key areas in achieving a “stepChange” is the sharing of HS&E informationand best practice to satisfy project needs andguide industry in general. The approach topractice sharing initially was adhoc, howeversafety professionals played a large part indriving the issue and developing industryguidance on the subject.
Practice sharing provided some practicalexamples of elimination and reductionmeasurers, this showed excellent lateralthinking when looking for solutions to reduceHAVS exposure in the workplace, theseexamples were drawn from all areas of ourindustry.
Due to the different working environmentswithin the industry there will be a need forindividual companies to take a risk basedapproach when adopting management controlsto meet their given situation.
As a direct result of trading ideas manycompanies have now introduced tangiblebenefits to the workforce – brought about byintroducing improved tooling andunderstanding of the problem. This in itselfcan be seen as a motivator for improved HSEperformance amongst the workforce.
Overall we set out to benchmark against futurelegislation and I think that from the efforts todate the different sectors of our industry candraw on the lessons learnt along the way andare in a position to comply with futurelegislation

172

173
REPORT ON HAND ARM VIBRATION SYNDROME
Ian Campbell, BP, HSE Advisor Health
A major focus for the HSE this year is in thearea of occupational health. Noise and otherallied health issues has been, and will continueto be scrutinised by the HSE Inspectorslooking at how individual assets comply withlegislation, regulations and guidance. TheHarding platform has a HAVS workingpractice document, first issued in May 1999.Since then the document has been updatedtwice to incorporate comments as a result oftwo external audits.
BP Amoco Harding has a recognised duty ofcare to ensure that the local workforce areprotected against the effects of Hand-ArmVibration Syndrome (HAVS), under thefollowing legislation;
• Section 2 of the Health and Safety at WorkAct 1974
• Management of Health and Safety at WorkRegulations 1992
• Supply of Machinery ( Safety) Regulation1992
• The Provision and Use of Work EquipmentRegulations 1992 (PUWER)
• Reporting of Injuries, Disease andDangerous Occurrences Regulation 1995(RIDDOR)
• HSE Guidance on Hand -Arm VibrationHS (G) 88.
Current legislation in the UK, recommendshealth surveillance for workers who’s exposureregularly exceeds a guidance level formaximum hand - arm vibration exposure of 2.8ms² over 8 hours. Harding prior to May 1999, had made attemptsto control HAVS exposure to personnel by theissue of HAVS timesheets whenever avibrating tool was in use. However this wasnot uniformly used across the platform, norwas the actual level of vibration generatedfrom a tool known. The HAVS workingpractice document sets out the standard bywhich all tools sent to the Harding platformand tools already on the platform arecontrolled. The principle methods of control areRegistration, Specification, Risk Assessment,Reporting, Awareness and Analysis & Audit,for example;
Specification:- Responsible person: PlatformOIM/OOE Ensuring that the power tools used onHarding create the lowest HAVS risk whilstbeing suitable for the intended workscope• Both BP Amoco and contractor-owned
tools used on the platform shall bespecified as having the lowest HAVS riskbut still be able to be used for a practicableworking period
• All Harding contracts will include theHarding Tool Specification as a contractrequirement, and that data sheets areprovided for all equipment.
Registration:- Responsible person: PlatformHSEA [ HEALTH ] Ensuring that all HAVS risk equipment isuniquely registered on a central platformregister that records all tool detailsincluding HAVS risk level All powered tools on Harding will:-• be registered in an index bearing unique
identification numbers and HAVS detailsas provided by the supplier / manufacturer
• be issued with a HAVS Risk AssessmentSheet recording vibration level andrecommended daily use
• be supplied with a coloured label showingthe maximum permissible use per day
Awareness:- Responsible person: HSEA [HEALTH ] Ensuring that all Harding personnel areaware of hand arm vibration syndrome andthe control measures to be taken to reducerisk• All new personnel to the Harding platform
will be made aware of the Harding HAVSpolicy
• All personnel using powered tools and willbe trained in the requirements of theHarding HAVS Policy before being issuedwith the tools. This will include watchingthe HAVS video / Interactive CD - ROM
Risk Assessment:- Responsible person:HSEA [ HEALTH ] Ensuring that the HAVS risk is assessed andminimised• Where possible, alternative methods shall
be used to remove the risk of hand armvibration syndrome

174
• Risk Assessments will be carried out toidentify the minimisation of HAVSexposure prior to each task
Reporting:- Responsible person: HSEA [HEALTH ] Ensuring that all platform personnel recordtheir use of power tools in a controllableand auditable manner• Each registered HAVS tool user on
Harding will be issued with a HAVS LogSheet
• HAVS tool users will be responsible forcompleting HAVS Log Sheets with actualexposure time
• Supervisors and users will ensure that boththe maximum permitted time and the dailycumulative time for the tool(s) is notexceeded
Analysis & Audit:- Responsible person:HSEA [ HEALTH ] The Harding HAVS Policy will use a processof data analysis and audit to drive a continuousHAVS risk improvement process. The initial approach utilised on the HardingPlatform, was to register the tools with aunique HAVS number, then to request thecompanies who supplied the tools ( Deutag,Cape, KOGL and AMEC ) for the tool productdata sheet. Tool product sheets usually accompany a toolwhich is purchased from a DIY outlet etc,however it was not usual practice for thecomplete data sheet to travel offshore.Normally electrical and air tools arrivedoffshore with a letter of conformity issued bythe contracting company, which cover topicsas; Safety and Operating Instructions, Use ofthe Machine, Maintenance and Repair,Lubrication, Air Supply, Electrical supply etc.,but rarely included information on Vibrationor noise generated by the tool. Thus it has beena major achievement that information for everytool has eventually been received on theplatform, with details of Vibration and noise.This contained the vital information thatallowed the risk assessment process to begin. Hand-arm vibration is measured in terms ofacceleration (in ms²). Therefore measurementsare made with an accelerometer attached toeither the tool or the workpiece. However,because the risk depends on the frequencycontent of the vibration, the signal from theaccelerometer is passed through an electricalfilter. This filter gives greater weighting to
frequencies between 5 and 20 Hz and lessoutside these frequencies. Two methods of measuring vibration arewidely used. Tri - axial accelerometermeasures and sums the three directions x, yand z simultaneously, however, measuringseparately in each direction x, y and z givesadditional information on the direction withthe highest vibration, the individual results arethen summed to give a total vibration level. Itis widely accepted that measuring individuallyin the three directions gives the most accuratevibration level. The HSE recommends a programme ofpreventative measures and health surveillancewhere workers exposure regularly exceeds2.8ms² for a period of 8hours, which isachieved using the following mathematicalcalculation A(8) =ah.w.x√(t/8). The value A(8)is equivalent to an average vibration level of2.8ms² for a period of 8hours. This gives thefollowing exposure / level relationship; Exposure time ( hours ) 16 8
4 2 1 ½ Vibration ah.w ms² 22.8 4 5.68 11.2 Thus a tool that vibrates at 11.2 ms² can onlysafely be used for 30 minutes, however a toolsthat vibrates at 2ms² can safely be used for upto 16 hours. One of the key components to the HardingHAVS practice was the label to be attached tothe Hand tools. Most tools already have somedistinguishing mark or test certificate attached,Harding wanted a system that was easilyidentifiable to all workers, thus Harding optedfor a visual risk system, utilising the concept ofthe traffic lights ; ( See appendix 1 )
• Red : Potentially Hazardous, canbe used up to 2 hours
• Yellow : Medium risk, can be usedfor between 2 - 4 hours
• Green : Slight risk, can be usedbetween 4 - 8 hours
• Black : Low risk, can be usedbetween 8 - 12 hours
The system above was well received by theworkforce, it allowed them to easily identifyand differentiate between high risk and lowrisk tools and offered a degree ofempowerment to the workforce in choosing thetool for the task. With the arrival of the tooldata sheets, all tools were risked assessed and

175
labelled according to the above classification,(see appendix 2) and a tool registerestablished, ( see appendix 3 ). There are various tools which are known tocause high vibration in particular, Needle guns,impact wrenches and air saws. Thereforewithin the Harding working practice wespecified that power tools should create thelowest HAVS risk commensurate with beingsuitable for the task proposed. All companiessupplying personnel and power tools werefurther advised that the platform expected highvibration red labelled tools to be graduallyphased out and replaced with HAVS friendlytools. Through continuous onboard audits themain contracting companies have beenchallenged, and responded positively inreplacing high vibration tools with tools thatthey believed to be low vibration. During May 2000, the Harding platform wasaudited, by an Engineer from AcousticTechnology Limited ( ATL ). Part of the ATLaudit was to conduct the final Noise survey onthe ‘Green Compressor’, but the visit wasmainly to obtain vibration data readings fromall the hand - held vibrating tools in operationon the Harding Platform and compare themwith previously obtained data. The Engineerused a Bruel and Kjaer Type 2537 Hand ArmVibration Kit, fitted with a Bruel and KlaerType 4505 accelerometer. This equipment wascalibrated prior to and after the measurementusing a Bruel and Kjaer Type 4294 VibrationExciter. ATL’s calibration procedures aretraceable to NPL standards. For each type of tool the hand - arm vibrationmeasurements were taken over a representativeperiod, by an operator carrying out a simulatedtask. The measurement period includedvariations in vibration levels due to pressure,lifting or movement of the tool. The meteraveraged the vibration level over the measuredperiod. Measurements were made using theintegral hand - arm weighting filter built intothis unit. All measurements were in terms ofaverage hand - arm weighted acceleration (ah.w
ms²). All results obtained were then enteredinto a data base and are presented in ( appendix4 ).
Conclusion It is clear that there is a significant level ofdisparity between the information suppliedwith the tools and the actual results obtainedby the ATL Engineer whilst testing on theinstallation, (appendix 3 & 4 ).
All risk assessment sheets on the installationhad been formed on the information supplied,which we now know to be inaccurate at thetime of testing. Thus personnel were exposedto vibration levels higher than thoserecommended by the HSE. The large disparity between the measuredvibration levels and data supplied with thetools may be due to several factors, includingwear of the tool during normal use, thecondition of the blade or disc fitted to the tooland the test conditions. It is not known theexact methods that tool manufactures use toobtain their vibration and noise levels. The vast majority of tools used and testedduring this audit on BP Harding were underone year old. Through discussions with various BPA sitesthere appears to be a requirement for coachingof the workforce into the mechanics of Hand -Arm Vibration syndrome and the provisions tomitigate against its effects, in the majority ofBPA sites in the UK.
Recommendations There are several measures which can beimplement which will reduce the potentialeffect of vibration to the hand, these include • Factors influencing grip• Posture• Tool Choice• Vibration Isolation• Work Rotation and Planning• Tool Maintenance• Training and Information• Health Surveillance• Purchasing Policy• Contracts There will be continuous maintenance andconstruction activities both offshore andonshore within BPA. It is recommended thateach unit should address the Hand - Armvibration issue., by the implementation ofrecognised tools and best practice. The HSE recently conducted an audit of themanagement of HAVS on Harding and regardthe Harding model as best practice. The HSE has released several aids which canassist business units in meeting the requiredstandards, these include ;

176
• ‘The Successful Management of Hand -Arm vibration’ ; CD - ROM,
• ‘ Hard To Handle’, video, Hand -Armvibration - manage the risk,
• ‘Vibration Solutions’, HSE publication,
References
A guide to the Health and Safety at Work etc.Act 1974 ( 5th ed ) HSE Books 1992
Management of Health and Safety at WorksRegulations 1992 Approved Code of PracticeL21 HSE Books
The Supply of Machinery ( Safety )Regulations 1992, as amended by the Supplyof Machinery ( Safety ) ( Amendment )Regulations 1994 SI 1992/3073 HMSO 1992
Hand -arm vibration HS(G) 88 HSE Books1994
BS 6842:1987 Guide to measurement andevaluation of human exposure to vibrationtransmitted to the hand
Whole- body vibration; Occupational exposureand their health effects in Great Britain.Contract research report 233 / 1999. Instituteof Sound and Vibration Research, Universityof Southampton
Hand-transmitted vibration; Occupationalexposure and their health effects in GreatBritain. Contract research report 232 / 1999.Institute of Sound and Vibration Research,University of Southampton
Hand - Arm Vibration Assessment, Technicalreport No: AT 4794/1 REV 0 AcousticTechnology Ltd

177
Appendix 1
Serial No.
Vib. Level
Noise Level
Max Daily Use
Serial No.
Vib. Level
Noise Level
Max Daily Use
Serial No.
Vib. Level
Noise Level
Max Daily Use
Serial No.
Vib. Level
Noise Level
Max Daily Use

178
Appendix 2
HAVS Tool Risk Assessment
BPA Harding Tool No.BPA Harding Tool No. HARptID 1654HARptID 1654 UserUser AMECAMECTool Tool DescriptionDescription :
Atlas Copco 5" Electric Angle GrinderSupplier AMEC Serial NumberSerial Number JSMP 95718Technical Technical Details :Details :
Vibration LevelVibration Level Noise LevelNoise LevelTested ByTested By: ATL10/06/00
10.13 m/s² 105.00 dB(A) Status:Status:
Recommended Maximum Daily Use 0.61
Hearing ProtectionHearing Protection: Wear Hearing Protection
CommentsComments James Scott Test 15/10/99 Vibration 2.2m/s², 87dB(A), Re-tested by ATL 10/06/00
Personnel involved in the use of this tool whilst onboard BPAHarding must be aware of the BPA Harding HAVS Policy
Date Used:........................
Start:........................ Stop:...................... Start:.........................
Start:........................ Stop:...................... Start:.........................
Start:........................ Stop:...................... Start:.........................
Start:........................ Stop:...................... Start:.........................
TOOL User Name Job Title Signature
Supervisor Approved Signed Date

App
endi
x 3
Ass
essm
ent #
Typ
e of
Too
lSe
rial
#H
ardi
ng #
Noi
se le
vel
dB(A
)M
ax U
sage
Tim
e (h
rs)
Vib
ratio
nm
s²B
PA 0
1C
P 78
5 3/
8” d
rill
KA
T 6
1H
arPT
166
690
91.
1ms²
BPA
02
CP
785H
½”
drill
KA
T 6
2H
arPT
166
590
90.
55 m
s²B
PA03
Cen
gar
Air
Saw
KA
T 5
7H
arPT
165
595
102.
5 m
s²B
PA04
Cen
gar
Air
Saw
KA
T 5
8H
arPT
166
395
102.
5 m
s²B
PA05
Spitz
ner
Air
Saw
KA
T 5
9H
arPT
165
310
010
2.5
ms²
Dri
lling
01
Inge
rsol
- R
and
1” im
pact
wre
nch
SWJ0
6002
95
Har
PT19
7510
4.6
30 M
inut
es9.
4 m
s²D
rilli
ng 0
2H
itach
i 13m
m c
huck
rot
ary
drill
D80
059
Har
PT 1
973
100
92.
5 m
s²D
rilli
ng 0
3M
AK
ITA
6.5
mm
chu
ck r
otar
y dr
ill37
7309
EH
arPT
195
481
92.
5 m
s²D
rilli
ng 0
4M
AK
ITA
rot
ary
drill
5002
155
Har
PT 1
955
891.
43.
6 m
s²D
rilli
ng 0
5In
gers
ol -
Ran
d ½
“ im
pact
wre
nch
231
- E
UH
arPT
1667
102
25.
2 m
s²D
rilli
ng 0
6A
ngle
gri
nder
AG
130
0 -
125
EX
Har
PT16
6987
1.2
7 m
s²D
rilli
ng 0
7IN
GE
RSO
L-R
AN
D d
rill
1978
Har
PT 1
959
92.9
120.
4 m
s²D
rilli
ng 0
8IN
GE
RSO
L-R
AN
D 3
/8”
drill
7502
Har
PT 1
951
92.9
121.
8 m
s²D
rilli
ng 0
9C
P857
Ang
le G
rind
erH
arPT
167
193
3.6
4.2
ms²
Dri
lling
10
CP8
75 M
ini -
Ang
le D
ie G
rind
erC
A15
6680
Har
PT16
7510
112
2.5
ms²
Dri
lling
11
Atla
s C
opco
Ele
ctri
c G
rind
erH
arPT
1673
8712
2.5
ms²
Dri
lling
12
Air
Wre
nch
292
9700
1AH
arPT
1662
110
4.5
AM
EC
01
Air
pen
cil g
rind
erJS
MP9
4249
H
arPT
1693
907
3 m
s²A
ME
C03
Air
pis
tol d
rill
JSM
P242
5H
arPT
1682
9010
2.5
ms²
AM
EC
04C
enge
r R
S ai
r sa
w (
Cla
mp
mou
nted
)JS
MP9
0648
Har
PT16
8395
102.
5 m
s²
179

App
endi
x 3
Con
tinu
edA
sses
smen
t #T
ype
of T
ool
Seri
al #
Har
ding
#N
oise
leve
ldB
(A)
Max
Usa
geT
ime
(hrs
)V
ibra
tion
ms²
AM
EC
05C
enge
r R
S ai
r sa
w (
Cla
mp
mou
nted
)JS
MP9
4231
Har
PT16
8495
102.
5 m
s²A
ME
C06
Spitz
nas
RS2
1 ai
r sa
w (
Cla
mp
mou
nted
)JS
MP9
0627
Har
PT16
8510
010
2.5
ms²
AM
EC
071”
Air
Im
pact
wre
nch
JSM
P958
61H
arPT
1686
110
3.4
4.3m
s²A
ME
C09
7” A
ir a
ngle
gri
nder
JSM
P952
85H
arPT
1688
9012
1.3
ms²
AM
EC
12
Air
Nee
dle
gun
JSM
P941
83H
arPT
1652
97.6
6.5
3.1
ms²
AM
EC
134”
Ele
ctri
c an
gle
grin
der
JSM
P957
18H
arPT
1654
100
132.
2 m
s²
Cap
e01
Vib
ro -
Lo
200
need
le g
unR
2344
Har
PT 1
699
98.6
43.
7 m
s²C
ape0
2V
ibro
- L
o 20
0 ne
edle
gun
-H
arPT
168
098
.64
3.7
ms²
Cap
e03
Vib
ro -
Lo
200
need
le g
un-
Har
PT16
7998
.64
3.7
ms²
Cap
e04
Vib
ro -
Lo
200
need
le g
unR
2345
Har
PT 1
700
98.6
43.
7 m
s²C
ape
053/
8 ca
paci
ty p
isto
l gri
p dr
illR
2367
Har
PT 1
953
103.
49
2.5
ms²
Cap
e 06
Air
Nib
bler
R23
66H
arPT
169
882
.26
3.0
ms²
180

App
endi
x 4
HA
VA
sse
ssm
en
tN
o.
To
ol T
ype
Ta
g N
o.
Vib
ratio
n (
ms ²
)M
axi
mum
Re
com
me
nd
ed
Co
ntin
uo
us
Use
(ho
urs
)
Nois
e d
B(A
)
BP
A 0
1C
P 7
85
3/8
" d
rill
Ha
rPT
16
66
1.1
50.6
92.7
BP
A 0
2C
P 7
85
1/2
" d
rill
Ha
rPT
16
65
0.6
20
5.6
90.6
BP
A 0
3C
en
ga
r A
ir S
aw
Ha
rPT
16
55
0.0
90.0
BP
A 0
4C
en
ga
r A
ir S
aw
Ha
rPT
16
63
8.8
0.8
87.8
BP
A 0
5S
pitz
ne
r A
ir S
aw
Ha
rPT
16
53
10.2
0.6
83.8
Dri
llin
g 0
1In
ge
rso
l - R
an
d 1
" im
pa
ct w
ren
chH
arP
T 1
97
59.4
0.7
10
9.5
Dri
llin
g 0
2H
itach
i 13
mm
ch
uck
ro
tary
dri
llH
arP
T 1
97
33.4
5.4
93.1
Dri
llin
g 0
3M
AK
ITA
6.5
mm
ch
ck r
ota
ry d
rill
Ha
rPT
19
54
3.7
4.6
85.3
Dri
llin
g 0
4M
AT
IKA
ro
tary
dri
llH
arP
T 1
95
50.0
90.0
Dri
llin
g 0
5In
ge
rso
l - R
an
d 1
/2"
imp
act
wre
nch
Ha
rPT
16
67
1.9
16.6
99.4
Dri
llin
g 0
6A
ngle
grin
der
Ha
rPT
16
69
0.0
90.0
Dri
llin
g 0
7IN
GE
RS
OL
- R
AN
D d
rill
Ha
rPT
19
59
0.7
11
9.2
91.8
Dri
llin
g 0
8IN
GE
RS
OL
- R
AN
D 3
/8"
dri
llH
arP
T 1
95
11.8
19.4
90.9
Dri
llin
g 0
9C
P8
57
An
gle
Grin
de
rH
arP
T 1
67
12.2
12.5
10
3.2
Dri
llin
g 1
0C
P8
75
Min
i - A
ng
le D
ie G
rin
de
rH
arP
T 1
67
55.5
2.0
99.2
Dri
llin
g 1
1A
tlas
Co
pco
Ele
ctri
c G
rin
de
rH
arP
T 1
67
34.0
3.8
10
1.3
Dri
llin
g 1
2A
ir W
ren
ch 2
92
Ha
rPT
16
62
3.6
4.9
11
1.6
AM
EC
01
Air
pe
nci
l gri
nd
er
Ha
rPT
16
93
5.9
1.8
98.0
AM
EC
03
Air
pis
tol d
rill
Ha
rPT
16
82
1.8
19.6
95.7
AM
EC
04
Ce
ng
er
RS
air
sa
w (
Cla
mp
mo
un
ted
)H
arP
T 1
68
30.0
90.0
AM
EC
05
Ce
ng
er
RS
air
sa
w (
Cla
mp
mo
un
ted
)H
arP
T 1
68
46.7
1.4
91.0
181

App
endi
x 4
cont
inue
d
HA
VA
sse
ssm
en
tN
o.
To
ol T
ype
Ta
g N
o.
Vib
ratio
n (
m/s
2)
Maxi
mum
Re
com
me
nd
ed
Co
ntin
uo
us
Use
(ho
urs
)
Nois
e d
B(A
)
AM
EC
06
Sp
itzn
er
RS
21
air
sa
w (
Cla
mp
mo
un
ted
)H
arP
T 1
68
513
.60.3
92.8
AM
EC
07
1"
Air
Im
pa
ct W
ren
chH
arP
T 1
68
68.1
0.9
10
6.5
AM
EC
09
7"
Air a
ngle
grinder
Ha
rPT
16
88
2.5
10.0
CA
PE
01
Vib
ro -
Lo
20
0 n
ee
dle
gu
nH
arP
T 1
69
90.0
10
5.2
CA
PE
02
Vib
ro -
Lo
20
0 n
ee
dle
gu
nH
arP
T 1
68
011
.80.4
10
4.7
CA
PE
03
Vib
ro -
Lo
20
0 n
ee
dle
gu
nH
arP
T 1
67
98.9
0.8
10
5.2
CA
PE
04
Vib
ro -
Lo
20
0 n
ee
dle
gu
nH
arP
T 1
70
00.0
90.0
CA
PE
05
3/8
ca
pa
city
pis
tol g
rip
dri
llH
arP
T 1
95
32.8
7.7
92.9
CA
PE
06
Air
Nib
ble
rH
arP
T 1
69
82.9
7.3
91.1
CA
PE
08
Ha
nd
he
ld g
rin
de
rH
arP
T 1
65
82.6
9.4
93.7
CA
PE
07
Ha
nd
he
ld c
om
pre
sse
d a
ir p
ain
t m
ixe
rH
arP
T 1
65
74.4
3.2
93.7
BP
A 0
9H
an
d h
eld
grin
de
rH
arP
T 1
66
43.5
5.0
97.2
N/A
Co
mp
Air
imp
act
wre
nch
BW
10
19
A33
.20.0
10
7.3
AM
EC
04
Ce
ng
er
air
sa
wH
arP
T 1
68
37.8
1.0
90.3
BP
A 0
6C
en
ge
r a
ir s
aw
Ha
rPT
16
74
8.3
0.9
87.6
BP
A 0
7S
BA
55
K B
att
ery
po
we
red
dri
llH
arP
T 1
67
21.9
17.5
87.1
BP
A 0
8H
itach
i CJ6
5V
2 J
igsa
wH
arP
T 1
66
03.6
5.0
92.7
182

183
Following Ian Campbell’s presentation,Richard McLellan gave a presentationexplaining the use of the database.
QUESTIONS AND ANSWERS SESSION
Question - Dave Freeman, HSE NorwichThe rest period, you say for using the tools‘per day’. Is that a per 12 hour day or 24 hourday and are rest periods between a week or afortnight? Do you have weekends off? Arethe rest periods critical to your findings please?
Answer – Richard McLellan, BPI think the HSE guidance says that you canhave an exposure of 2.8 metres per second forevery 24 hour period. The long term is that ifsomeone is exposed to 2.8 metres per secondon a five day week over 8 years, 15% of themwill suffer white finger or something like that.I’m getting nodding heads from the HSE, so Ithink that’s pretty near right.
Question - Tony Parkinson, Noble Drilling,for TexacoDid you do calculations on the eight hour dayor was it 12 hours for offshore workers?
Answer – Richard McLellan, BPWe do it on eight hours, which is anotherfactor of safety.
Question - Steve Taylor, Shell ExproSouthern North SeaAgain a question for the vibration boys ontheir experience. We’ve looked at all the goodstuff for reducing the risk as such. Have welooked at the susceptibility of certain people tothis? That is, through pre-employmentmedicals or for on-going reasons, are therecertain people who just shouldn’t be doing it inthe first place?
Answer - Richard McLellan, BPThe guys get an induction. They’re registeredin the system before they go on. There’s aquestionnaire we go through, we show themthe video, discuss the system, how it works. Ican’t say we’ve ever identified anyone with aproblem yet, but we would refer that onshoreto our medical department. If we had a guywho looked as though he was at risk due toprevious exposure, or if he had blanching ortingling, we’d refer him onshore to ourmedical department for referral for furtheradvice.
Answer – Ian Campbell?That is part of our induction process, actuallyasking the guys if they have experience of it or
have they got it themselves, so we immediatelyidentify from day one, any guys going on theplatform who do have a concern with it, orhave been exposed to it previously. Of courseone of the core components of HAVsmaintenance and health surveillance is actuallyfeeding the information that we’re collectingback to the parent companies so that they canstart looking after their chaps.
Comment – Dr Jim Keech, BP, Chairman ofUKOOA HACI must sound a warning bell for any processthat would be so grossly discriminating as wasmaybe suggested from the back of the roomhere. We have to be very careful as anindustry. We have a reputation of beingsomewhat elitist in terms of selecting ourworkers. It is quite contrary to the DisabilityDiscrimination Act. As the chair of theUKOOA Health Advisory Committee I amvery sensitive about this and although it is asensible precaution to exclude those whoalready may have suffered some harm, I thinkwe must be very careful not to use that as aselection procedure. I would recommend thepreventative measures which we’ve heard fromthe speakers as against selection.
Comment - Mr Graham Cowling, AcousticTechnology LtdJust to clarify one thing. Probably one of thereasons why you are getting unsatisfactorydata from manufacturers is not because they’retrying to sell you tools but the actual standardsthat the tools are measured to, have themhanging on wires unloaded. Whereas themeasurements you take have the tools in thereal situation with people actually using themup against the wall. So there’s likely to bequite a difference. It is the fault of thestandards. This can be easily remedied. Youcredited Amec with giving you good data andthat’s because they have bothered to set up atesting booth. Also they train the people whopack up the tools in boxes and send them toyou, to a basic level in competence inmeasuring. That’s something that can beeasily achieved by contractors.
Answer – Ian Campbell?Thanks for that Graham. We are aware alsothat the HSE are setting up a working grouplooking at the measurements so that we geteffective and cross industry measurements inrelation to power tools.
Question - Tony Garner, ConocoDo you take into account any off-the-jobexposures?

184
Answer – unknown speakerNo.
Comment – Edmund Brookes, BROAI suppose that argument could well be appliedequally with sound with a chap being at a discoall night. He then goes offshore and he’s gothis ears ringing because of the noise level.We’ve got no control over that. That raises allsorts of issues.

185
DAY 3
MORNING SESSION
SESSION THEME – HUMAN FACTORS AND PSYCHOLOGICAL HEALTH

186

187
CIRCADIAN ADAPTATION TO SHIFT CHANGE IN OFFSHORESHIFT WORKERS
Michelle Gibbs, S. Hampton, L. Morgan and Professor JosephineArendt, Centre for Chronobiology, University of Surrey
Abstract
There is increasing interest in the healthproblems associated with working shifts andthe role of circadian adaptation to a night shift.Previously it has been shown thatphysiological adaptation to night shift can beachieved in offshore shift workers, but thatshift schedule and season may both beimportant influencing factors. In this study 11males were studied for a fourteen-day touroffshore on a schedule of 7 nights followed by7 days. Circadian adaptation was measured byacrophase of the urinary melatonin metabolite6-sulphatoxymelatonin (aMT6s). A significantdifference was found in the mean acrophase(peak time) of aMT6s between the start(05:34h) and end (10.95h) of the night shiftweek (p = 0.0004). There was no significantdifference in the mean acrophase between thestart (11:04h) and end (12:59h) of the day shiftweek, suggesting that as a group the subjectsdid adapt to the night shift, but did not adapt tothe change back to day shift. However theinter-subject variation was high and increasedover the day shift week. Adaptation to a nightshift occurred in 73% (n = 8) of subjects, ofthose who adapt to nights, only 37.5% (n = 3)adapted back to day shift. A further 37.5%showed no adaptation to night or day shift. Allthe adaptation to the night shift occurred bydelay, but the adaptation to day shift showedboth advance (n=1) and delay (n=2) of theinternal clock. These individual differencesclearly require further study.
Introduction
Shift work is becoming more and more anecessary part of working life as the demandfor a 24 hour society increases, yet itintroduces some concerns for the health &safety of the worker. Reported symptoms ofreduced well being amongst shift workersinclude fatigue, and reduced sleep quality(Nicholson and D’Auria, 1999). In addition tothese undesired symptoms, when the workingenvironment incorporates dangerous activityfatigue and reduced cognitive performancepresent a more immediate health and safetyrisk. Performance and safety are of concern inshift workers and circadian rhythms have been
discussed as a probable factor in decreasedwork efficiency and vulnerability to humanerror during night work (Costa, 1997).
Working shifts, especially night shift, causesthe body to attempt to make physiologicaladjustments in order to adapt to the differentworking times. These physiologicaladjustments require investigation, not only toidentify changes that may have health andsafety implications, but also to distinguish ifcertain shift patterns offer greater or lesser riskthan others, and to find solutions.
Shift schedules
Offshore oil and gas installation workers havedifferent shift patterns and environmentalfactors to onshore shiftworkers, producingdifferent physiological responses particularlywith regard to circadian adaptation to nightshifts. There is currently a number of shiftpatterns being worked offshore and it isunclear if there are benefits or increasedproblems with each schedule. The complexityof designing shift schedules requiresconsideration of factors other than simply themost appropriate for circadian adaptation.Operational constraints, such as helicopterschedules and crew change arrangements,further complicate decisions about shiftrotation schedules.
Adaptation to shift work offshore
The offshore petrochemical industry is theonly industry working 12-hour shifts for 7,14or 21 days/nights with managed meal times,segregated shifts and daytime darkness fornight workers. While it has been shown that,in some schedules they do physiologicallyadapt to a night shift (Barnes et al, 1998a), theprocess takes days, so they may be working asignificant percentage of their tour in anunadapted state on both the day and nightshifts. Barnes showed that on North Sea rigs,for a 14-day 12-hour night shift (1800-0600h),subjects are out of phase for at least the first 4-5 days of the night shift (Barnes et al, 1998a).For a 7 day sequence starting with day shift(1200-2400h) then switching to night shift(2400-1200h) the majority of crew do not

188
adapt to night shift (Barnes et al, 1998b). It islikely that for a 7 day sequence, 12 hour shift,starting with night shift (1800-0600h), subjectswill be out of phase for at least 4-5 days out of7 days on night shift followed by 4-5 days outof phase on day shift.
Here we have studied the schedule that causesthe worker to attempt adaptation to two shiftchanges over a two-week period, workingseven nights followed by seven days. Theobjective was to measure the extent anddirection of circadian adaptation in a 14 dayschedule of 7 nights and 7 days (12 hour shifts1800h to 0600h) on oil installations in theNorth Sea (61oN).
Methods
Eleven healthy male subjects aged between 25and 47 years with a mean body mass index of25.7kg/m2 (± 2.45 SD), were studied for afourteen day tour offshore. Circadianadaptation was measured by the urinarymelatonin metabolite 6-sulphatoxymelatonin(aMT6s). Sequential 3-4h urine collections (8-10h overnight) were taken throughout the 14-day study and aliquots frozen for analysis ofthe urinary melatonin metabolite aMT6s, byspecific radioimmunoassay (Aldhous andArendt, 1988). Acrophase of the aMT6srhythm was calculated by cosinor analysis.The criteria for adaptation was taken as at leasta three hour acrophase shift from baselinemaintained for three or more days, and foradaptation back to day shift was a shift inacrophase to within 3 hours of the basalacrophase time. Day two was used as basalacrophase, as this was the first full 24-hourperiod of the study. Paired t-tests were appliedto the data to identify statistically significantdata.
Results
There was a significant difference in the meanacrophase between the start (05:34h) and end(10.95h) of the night shift week (p = 0.0004)suggesting that as a group the subjects didadapt to the night shift (figure 1.). There wasno significant difference in the acrophasechange between the start (11:04h) and end(12:59h) of the day shift week suggesting thatas a group the subjects did not adapt to thechange back to day shift.
The variance between the subjects was highand increased over the day shift week,representing the subjects as a group servesonly to disguise the variation in adaptation
pattern amongst them. The subjects havetherefore been grouped into those who did notadapt at all (n = 3) figure 2, those who adaptedto the night shift but not to the day shift (n =5) figure 3, and those who adapted to both thenight and day shifts (n = 3) figure 4. Of thesubjects who adapted to both of the shiftchanges, all demonstrated adaptation to thenight shift by delay of their rhythm but furtheradaptation to the day shift was by acombination of delay and advance (figure 4).
Discussion
We conclude that on a 14 day schedule of 7nights (1800h to 0600h) followed by 7 days(0600h to 1800h) adaptation to a night shiftdid occur in 73% (n = 8) of subjects but withhigh inter-subject variation of adaptation rateand extent. Of those who adapted to nights37.5% (n = 3) adapt to the change back to dayshift. All adaptation to the night shift on thisschedule occurs by delay, but the adaptation today shift is divided in the ratio 2:1.
Previously circadian adaptation in offshoreshiftworkers has been found in a schedule of14 nights 1800h to 0600h by delay of thecircadian rhythm, and in a schedule of 7 daysand 7 nights working 00.00h to 12.00h during(Barnes et al, 1998b), where the partialadaptation was by advance of the rhythm. Thisdifference indicates that the work time withinthe schedule may be critical in the direction ofadaptation. Here, in contrast, we have found acombination of advance and delay, along withno adaptation at all within the same schedule.The schedule of 7 nights followed by 7 days isthe most complex in terms of adaptation,requiring an adjustment twice during theschedule. The subjects while all working onthe same installation had differing duties andtherefore different activity and environmentalconditions such as light exposure. There maybe endogenous differences as well as theseexogenous influences contributing to theindividual variation in adaptation found here.
Subject specific light exposure data mayprovide some explanation of the variation inadaptation patterns as the duration, timing andbrightness of light exposure are associatedwith the entrainment of circadian rhythms.Light exposure data has been collectedsubjects on a shift schedule of 14 nights andwill be recorded on the 7N/7D shift schedulein further studies to determine the mostdesirable for performance and health, alongside the patterns and physiological effects ofadaptation. If adaptation is found to be

189
desirable, then studies applying strategies forencouraging adaptation will also be proposed.
This research was undertaken with support andfunding from the Health and Safety Executive- Offshore Safety Division, to whom ourthanks are extended.
References
Aldhous ME, & Arendt J. 1988,Radioimmunoassay for 6-sulphatoxy-melatonin in urine using an iodinated tracer.Ann. Clin. Biochem, 25:298-303.
Barnes RG, Deacon SJ, Forbes MJ, Arendt J.1998a, Adaptation of the 6-sulphatoxymelatonin rhythm in shiftworkers
on offshore oil installations during a 2 week12-h night shift. Neurosci Lett, 241: 9-12.
Barnes RG, Forbes MJ, Arendt J. 1998b, Shifttype and season affect adaptation of the 6-sulphatoxy melatonin rhythm in offshore oilrig workers. Neurosci Lett, 252:179-182.
Costa G. 1997, The Problem:Shiftwork.Chronobiology International, 14(2):89-98.
Nicholson PJ, and D’Auria DAP. 1999, Shiftwork, health, the working time regulations andhealth assessments. Occupational Medicine :49(3):127-137.

190
Figure 1. Mean acrophase time at start and end of each week of the tour.
Figure 2. Subjects showing no adaptation to either night or day shift (mean ±± sem).
nightsdays
start
end
0
2
4
6
8
10
12
14m
ean
acr
op
ha
se
tim
e
week of nights/days
difference in mean acrophase time between the start and end of each week
Circadian Clock Timing(evaluated by urinary melatonin metabolite aMT6s) Subjects Not Adapting to Nights or Days (mean).
NIGHTS DAYS
1
5
9
13
17
1 8
day of tour
ac
rop
ha
se t
ime
(ho
urs
)

191
Figure 3. Subjects who adapt to night shift but not back to day shift (mean ±± sem).
Figure 4. Subjects showing adaptation to nights and back to days.
Acrophase shift of subjects (s3,s7,s8) who adapt to night shift and day shift
0
5
10
15
20
25
30
1 2 3 4 5 6 7 8 9 10 11 12 13 14
day of tour
acro
ph
ase
tim
e (h
ou
rs)
Circadian Clock Timing(evaluated by urinary melatonin metabolite aMT6s)
Subjects Adapting to Nights But Not Back to Days.
NIGHTS DAYS
4
8
12
16
20
1 8
day of tour
ac
rop
ha
se
tim
e (
ho
urs
)
192
QUESTIONS AND ANSWERS SESSION
Question - Melanie Clark, Amey VectraAre you intending or hoping to use those Actiwrist watches which we’ve used, I’ve certainlyused in the past, to get them to observe theeffect when they go home? So, not just whenthey’re on the rig or platform but when they’reat home as well?
Answer – Professor Josephine Arendt,University of SurreyYes absolutely.
Question - Tony Garner, ConocoHave you done any crossover trials from the7/7 and 14/14 people and seen if the responseis the same?
Answer – Professor Josephine Arendt,University of SurreyYou mean, have we done 14 days day shift aswell as 14 days night shift?
Question - Tony Garner, ConocoYes, do they respond in the same way?
Answer – Professor Josephine Arendt,University of SurreyThese are people who alternate on the Ternstudy that we did. They did 2 weeks of nights,2 weeks off and then 2 weeks of days, so wehave the day shift to compare with the nightshift.
Question - Tony Garner, ConocoSorry, I was meaning have they done a 7 dayday shift, then a night shift and then maybe a14 day day shift?
Answer – Professor Josephine Arendt,University of SurreyNo we haven’t got that comparative data. Thatwould be very interesting.
Question - Jake Molloy, OILC OffshoreUnionTheoretically, I suppose hypothetically, do youbelieve, or do you consider, that a reduction inshift work, that is to say extended leaveperiods, may reduce the health risks to workerscarrying out these sorts of shift patterns?
Answer – Professor Josephine Arendt,University of SurreyWell quite honestly I think that question isenormously important, but it’s beyond myexpertise. I don’t know whether Andy Smithwould like to reply?
Answer - Andy Smith, Cardiff UniversityI agree, I think that’s a very important point. Idon’t really think we know enough about themedium-term effects, let alone the long-termeffects. Clearly as Jo said, one of the ways ofextending this is to focus not just on what’sgoing on on the installations. I’d like to see itextended over a much longer time period, toreally assess the impact of leave and work incombination. I think this is a weakness ofshiftwork research in general, not just thestudies that we’re doing offshore.
Question - Gareth Powell, BPDid you notice any difference at all in theresults from installations at different latitudes?I notice you had the latitudes on some of themand some of them are quite far north. I wonderif you’ve got any of the southern sector onesand was there any difference there?
Answer – Professor Josephine Arendt,University of SurreyThat was why it was interesting to do fourteennights at 53°N and fourteen nights at 61°N,because the daylight changes are very muchgreater at 61°N. In the winter there is muchless likelihood of exposure to natural light at61°N than there is at 53°N. Natural light at thewrong time will counter adaptation to nightshift. This is if you like a classical situation.You come off night shift at 6 o’clock in themorning onshore and you go home in lightfrequently and that light is at exactly the wrongtime if you wanted to adapt. It counters theshift of your clock, that morning light. Weactually believe that the different results we getfrom the drilling rig, for example, the 7 days/7nights compared to the 14 nights, is related tothe light exposure that these guys have becauseof the different hours of work that they did.This is why we are currently recording lightexposure. But in fact, when we looked at53°N and at 61°N on the 14 nights, they alladapted on both of those latitudes so that’scomforting from the point of view of peoplewho favour 14 nights on the trot.
Question - Alan Atkinson, Total Fina Elf,NorwayDid you take into consideration the ages of theparticipants? It’s just that during unscientificdiscussions with our own people, when theyhit the 45-50 bracket they have a tremendousproblem with shift work and coming back ontonormal living when they go home.

193
Question - Rab Wilson, AEEUCould I just attach to that question there. Whatpercentage of male and female were in thestudy as well?
Answer – Professor Josephine Arendt,University of SurreyI regret to say they were all male. We’d loveto have a mix of course and look at themseparately. This intolerance is a well-knownphenomenon as you get older. It’s also true ofadapting to time zone change. It becomesmuch harder as you get older. We have arange of ages. I think the average age is about40. We’re grateful for anybody whovolunteers so we’re not going turn anybodydown on the grounds of age but we haven’t gotenough to look at age differences.
Question - Tony Parkinson, Noble Drilling,for TexacoOur platform does 2 weeks off, 2 weeks on.Have you thought about the rigs that do 3/3?
Answer – Professor Josephine Arendt,University of SurreyWe’d like to get at them. Please.
Question - Ian Campbell, BP AmocoYou mentioned at the start there that one of thethings you were looking at were the markersfor CHD. Have you got any information onresults so far?
Answer – Professor Josephine Arendt,University of SurreyWe have a trend which is not significant yet toan increase of triacylglycerol during the nightshift but it is not significant yet.
Question - Ian Campbell, BP AmocoMay it possibly be due to the fact that for thenight shift workers, the only meal they haveavailable prior going to bed is a nice big fattybreakfast?
Answer – Professor Josephine Arendt,University of SurreyThis is where I think I ought to introduceMichelle because Michelle has expertise in thedietary area. We do get significant increases intriacylglycerol in simulation experiments thatwe do in the lab very clearly, no doubt about it,and incidentally evidence that light treatmentreduces that blood lipid. I think the reasonwe’re not getting significance is because thediet is uncontrolled out there as you quiterightly point out. This is going to make a hugedifference to the results. We are keepingnutrition diaries so that we can look back atwhat they’ve eaten but frankly I don’t thinkthey’re terribly reliable.

194

195
MANAGING STRESS IN THE OFFSHORE WORKINGENVIRONMENT
Dr Valerie J Sutherland, Chartered Psychologist, Sutherland-Bradley Associates
The topic of stress has featured on offshore oiland gas industry agendas for nearly twodecades. However, as an academic andconsultant, observing from the outside, Ibelieve that unease about ‘stress’ and stressmanagement still exists in the Industry. Someforward thinking companies have gainedbenefits from including stress management intheir business plan. However, others havesimply paid lip service to ‘stress’ because itwas fashionable, flavour of the month, orbecause of pressures from a parentorganisation.
Much of this resistance seems to have beencreated because the word, ‘stress’ evokesnegative reaction and emotion – it has becomea four-letter word! Problems seem to arise,because, like love and electricity, we cannotsee ‘stress’. Media hype and constant attentionhave not helped. It has become a whippingboy, blamed for all our ills and problems. Tooften, stress is now used as an excuse, andstress-related illness is in danger of becomingthe ‘back-pain’ of the new millennium.
Today I wish to help set this record straight. Iwant to propose that it will be much moreuseful and productive for the industry, andbeneficial for the men and women workingoffshore, if we stop using this word ‘stress’. Iwould like to suggest that instead of using theterm ‘stress management’, we begin to thinkabout the ways we can optimise theperformance effectiveness, health, satisfactionand happiness of the workforce. In otherwords, we need to find out what barriers existto adversely impact upon the productivity andwell-being of the offshore employee. This doesnot mean that we wallow in a negative anddamaging, ‘isn’t it awful’ climate because partof the process of identifying barriers toeffectiveness is the need to acknowledge thefactors that facilitate optimal performance andhealth offshore.
The Triple ‘A’ Stress Management Model
The ‘Triple A’ approach is recommended as astress management model: This stands for:
AWARENESS
ANALYSISACTION
‘AWARENESS’ – What is stress?
This means defining what we mean by the‘stress’ word, and understanding why and howstress is damaging in its consequences. Theproblem here is one of definition since there islack of agreement about the meaning of thisword stress, and if, in fact, it exists. Stress,pressure and strain are used interchangeably tomean the same thing. Incorrect use of theword stress is common since it is used to referto a state, a condition, or a symptom. Also,people tend to perceive stress in negativeterms. Prevalence of this view is likely to bedetrimental to the effective management ofstress in the work environment because it isregarded as synonymous with not coping. Theoutcome is that staff will hide their problemsand health condition until they become victimsof exposure to stress, rather than actively andpositively managing the strains and pressurethat are an inevitable part of modern-day livingand working offshore.
Furthermore, it is important that weacknowledge that NOT ALL STRESS ISBAD. Hans Selye, the acknowledged "father"of stress research said that the only personwithout stress was a dead person. By this hemeant that stress is an inevitable part of beingalive, and should be viewed as, 'stimulation togrowth and development, challenge andvariety – stress is the spice of life'. In Selye'sterms stress is simply 'arousal' and so it is anystimulus, event or demand impacting on thesensory nervous system. When an imbalanceexists between a perceived demand (thestimulus) and our perceived ability to meet thatdemand, we will experience a state of stress(i.e. distress). Stress, therefore, is unwantedpressure and is manifest when we feel that asituation is out of our control or when we feelunable to cope. It is a subjective experience, -"in the eye of the beholder", and this explainswhy in a given situation one person might behighly distressed, yet another seems to prosperand thrive. In organisational life it is likely thatwe are now denied natural outlet of the stressresponse since we cannot "fight" nor "flee".

196
We are physiologically primed to take actionsthat are inappropriate and the sedentary natureof the job further exacerbates this problem.Each of us, at various times during our life,will be vulnerable and will need to know howto actively and positively manage a stressfulsituation without resorting to maladaptiveways of coping (e.g. excessive alcohol andnicotine; drug dependence; lack of exercise;and comfort eating), which render us less fit tocope with a demand. Thus, it is mismanagedstress that is damaging in its consequences.
ANALYSIS – Identifying Stress
The identification and measurement of stress atwork has been described as the ‘stress audit’.The objective of this type of psychological riskassessment is to identify the negative factors orbarriers to performance effectiveness and well-being at work, and either eliminating orminimising these harmful sources of stress.Thus, we acknowledge the maxim, ‘healthywork force - healthy organisation’. The word‘health’ is used in its’ widest sense, to meannot just the absence of physical andpsychological diseases, but to describe feelingsof well-being, happiness, and satisfaction. Toidentify the action to be taken is it vital toaccurately diagnose the problem(s) (i.e. what,who, how?). Stress audit benefits include:1. It is a proactive rather than a reactiveapproach to managing stress at work2. It can identify organisational and individualstrengths and weaknesses and so is similar toan appraisal or training and development needsanalysis. Thus it helps us to target scarceresources.3. Identify the level of stress managementrequired (primary, secondary, tertiary – seebelow); thus this includes guidance in theplanning of organisational developmentstrategies.4. Provides a baseline measure from which toevaluate subsequent interventions5. It makes stress a respectable topic fordiscussion in the workplace.By considering some of the most commonlycited sources of stress it is possible to see thatthere is not one problem, neither is there onecure.
Stress in the Offshore Environment• Stress in the job.Level of demand and workload is a potentialproblem for many people working offshore.This includes having too much to do, workinglong hours and shift working (perhapsexacerbated by ‘below strength’ manpowerlevels) can create overload conditions, leading
to ‘burnout’. Having too little to do or a jobthat does not offer stimulation, variety orchallenge are also a sources of stress, knownas, ‘rust-out’, leading to boredom and de-motivation. Responsibility withoutcommensurate power, a fast pace of work, lackof job control, and uneven distribution ofresources are also sources of pressure.Fluctuations (peaks and troughs) in workdemand create uncertainty that can be stressful.The introduction of new technology, originallythought to be stressful because it wasassociated with de-skilling of jobs, is often apotent source of pressure because of themanner in which it is introduced. That is,without consultation, unfit for the purpose or alack of training etc. A scaled-down workforceis often required to become multi-skilled sothat maximum use is made of the costlyinvestment in new technology. Whilst this canoffer variety and challenge, it can create stressif the changes are introduced withoutconsultation or reward for extra effort. For theoffshore worker, safety concerns, the need totravel by helicopter, and the environmental andphysical conditions of the work and livingenvironment have been described as sources ofstrain intrinsic to the job offshore.
Job role stressFor many employees changes to job rolestructure are common as companiescontinually re-invent themselves. Oftenchange is stressful because we tend to resist it,but the impact of change might also result inrole ambiguity (lack of clarity about the task)and/or role conflict (for example, coping withthe conflicting demands of quantity versusquality, or safety versus quantity). Roleambiguity has been associated with tensionand fatigue, resulting in leaving the job andhigh levels of anxiety, physical andpsychological strain and sickness absence.Role conflict has been associated with sicknessabsence, job dissatisfaction, abnormal bloodchemistry and elevated blood pressure.• Relationships with other peopleHaving to live and work with other people,lack of privacy, constant company - 24-hours aday, for seven or 14 days at a time can bestressful. Perceived inequity between the oilcompany and contractor status personnel cancreate a strain in working relationships. A lackof supportive relationships or poorrelationships with one’s crew, colleagues orthe boss are stress agents, leading to a lowlevel of trust, low supportiveness and lowinterest in problem solving. Some personnel,by virtue of their job role are exposed tobullying and violence at work. Reports of this

197
seem to be increasing and it is likely that theextent of the problem is not well understood.• Career stress.Expectations not met, feeling undervalued andfrustration in attaining a sense of achievementare common 'career'' stressors. Ultimately,restricted opportunities for promotion and jobinsecurity resulting from down-sizing and theincreased use of contract labour are potentsources of stress. The ‘slimmed-down’ UKworkforce is also an ageing population and theindustry faces the issue of coping with this andattracting a new breed of youngsters who enterthe world of work with very differentexpectations than they did 25-30 years ago.Although the stress of unemployment is moredamaging than the stress of work, threat of jobloss is a potent source of stress linked toseveral serious health problems, includingulcers, colitis, alopecia and increased muscularand emotional complaints. Also, as thepyramid shape of organisations becomesflatter, and many job levels are removed, thereare fewer opportunities for career progression.Finally, in a recessionary climate, training anddevelopment opportunities may be restricted.The 'leaner' work-force experience pressuresassociated with trying to release colleagues fortraining, in addition to the time off necessaryfor cover for holidays and sickness absence,while trying to maintain performance, safetyand production demands. This creates ademoralised workforce and quite clearly, anunder-trained workforce will perceive the workenvironment to be more stressful and less safe.• Stress in the organisational structure
and climate. Simply 'being in the organisation', can bringconcerns about the sense of belonging, officepolitics, social support from the managementstructure in terms of resources, communicationand consultation. It is associated with thethreat to freedom, autonomy and decision-making imposed by the organisationalstructure and climate. There is some evidenceto suggest that lack of participation indecision-making processes, lack of effectiveconsultation and communication andunjustified restrictions on behaviour areassociated with negative psychological mood,escapist drinking and heavy smoking. Aculture and climate of threat and/or fear tospeak out, simply creates a climate of mistrust,resistance to change, an unwillingness to beinnovative or commitment to the vision andgoals of the organisation.• Home-work interface stress.Included in this category are the personal lifeevents that might have an effect uponperformance, efficiency, well-being and
adjustment at work. Concerns within thefamily, life crises, financial difficulties,conflicting personal and company beliefs, andthe conflict between organisational andfamily/social demands are examples ofpotential stressors which might spill over intothe individual's work domain, in the same wayin which stress at work might spill over andhave a negative impact on one's family andpersonal life. Working and living away fromhome can be an added source of stress for theoffshore worker. Leaving a partner to cope;difficulties with the children; problemsunwinding on return home; feeling unable tobecome involved in community and socialactivities because of the demands of offshorework, are all problems associated withoffshore working that must be activelymanaged.
‘ACTION’ – Options for the managementof stress
The processes of awareness raising andanalysis are necessary steps to guide andinform action. However, too often, stressmanagement courses are introduced as areaction, in response to a perceived problemwithin the organization. Other stressmanagement initiatives, such as the use of acounselling service or an employee assistanceprogramme seek to ‘cure’ the symptoms ofexposure to stress. This type of stress controlprogrammes focuses solely on the individualand places the onus and burden for change onthe employee. The message is loud and clear.It says ‘You do not seem to be able to handlethe stress and pressure of your job, so we willhelp you to cope more effectively’. Whilstthese aims are well intentioned, the underlyingmessage to the employee also implies that, ‘we(the organization) are not going to change theway we do things around here. You must learnto cope with the situation!’ Although theseapproaches to stress control have a certainappeal and can be very effective, stress controlcan only be really successful if it is tackled at thelevel of the individual, the team and theorganisation – that is, eliminate the source ofstress. The strategy of waiting for an employeeto become a victim of stress, before takingaction, is risky and costly for the organisationfrom both legal and insurance perspectives. Itcan also be damaging because it supposes thatdistressed victims of exposure to stress areeither at work and probably behaving inineffective, non-productive ways, or they areabsent from their job, thereby causing extrastrains and pressures on the remaining work

198
colleagues or team. Both situations areundesirable and costly.
A Tripartite Model For Stress Management
It is recommended that stress in the workplaceshould be addressed by adopting a tripartiteapproach consisting of:1. Primary level stress managementThis type of strategy or intervention is‘stressor directed’ in that they eliminate,reduce or control a source of stress. The aim isto prevent stress at work.2. Secondary level stress
managementThese interventions are ‘response directed’ inthat they help individual employees or groupsof workers to recognise a potentially negativeresponse to stress, and change it before itbecomes harmful Thus, the aim is to developstress resistance and adaptive coping strategiesthrough education and training.3. Tertiary level stress managementThese forms of intervention are ‘symptomdirected’. The objective is to assist in the cureand rehabilitation of stressed employees.
Using an, ‘onion’ as our metaphor, we woulddescribe stress management in the workplace,as ‘peeling an onion’. The organisation existswithin its universe and is thereby exposed tomany different factors. Peel off this layer andyou find the organisation, exposed to changeand pressures imposed by the global economy,financial constraints, international politics, andlegal requirements, etc. All of these, andmore, influence the fortunes of the businessand the decisions made. A description of each‘level’ with examples of strategies andinterventions, are provided below.
Primary level stress managementinterventions
A more commonly used term for this type ofstress management strategy is ‘organizational-level interventions’. Essentially, these‘stressor’ directed strategies for the reductionor elimination of stress in the workplace arecategorised in three ways, namely:1. Change the macro environment; that is,organisational culture and leadership, physicalwork conditions and work load, safety climate,career development programmes and bullyingat work.2. Change the micro-environment; that issystems and task redesign, alternative workarrangements, shift working, and
communication exercises such as rolenegotiation.3. Improving perceptions of worker control;this includes increasing opportunities fordecision-making.
Change the Macro-environmentThis includes attention to issues such as• Organisational cultureBuilding a supportive and open climate andculture, and ensuring that the style ofmanagement is compatible with the goals andaims of the organisation, are important inreducing stress at work. It also meansdeveloping a culture that encourages staff bemore supportive of each other. This willfacilitate team working and good interpersonalrelationships in the workplace. The benefit ofsocial support as a stress reduction strategy iswell documented. It is likely to be an importantstress reduction prevention mechanism sinceexternal forces prevents us from eliminatingcertain sources of pressure and strain in theworkplace. For example, this would include theneed to work shifts, especially night-shift work.An assessment of organisation culture guides theprocess of culture change. Likewise, the use ofpsychometric measures to understand theappropriateness of ‘management style’ and itsrole as a source of stress in the workplace mightbe necessary• Work overload conditions and long-hours
of workingIt is acknowledged that both work over-load(burnout) and under-load (rust-out – see nextsection) are potent sources of stress incontemporary organisations. A high workloadleads to long hours of working, extra duty shifts,or reduced time-off periods. A re-analysis ofstaffing levels and an improved (real) costingof the impact of de-manning, or job and taskre-design are also recommended to help reducework overload stress and shift work. Someorganisations have found that their enthusiasmfor down-sizing has been too zealous, and asubsequent cost benefit analysis has proven thereinstatement of certain jobs to be the mosteffective management strategy.• The physical work environmentIn a work overload situation it is important toensure that employees are not also stressed bythe physical conditions of the work environment.In addition to being a source of stress in theirown right, they also take-up the attentionalcapacity of the individual, and the employee ismore vulnerable to workplace stress. Researchevidence indicates that unpleasant workingconditions, the necessity to work fast, to expenda lot of effort, and working excessive andinconvenient hours were related to poor mental

199
health. Therefore, the work environment shouldprovide satisfying physical conditions. Also aclean and orderly place of work is important forboth safety and hygiene reasons. This hasimplications for the morale of the work force,especially in an environment where the worksituation is acknowledged as hazardous. Clearly,many of the opportunities for the prevention ofstress associated with the physical demands ofworking exist at the design stage, and of course,in the provision of adequate personal protectionequipment. Complaints about the lack ofventilation, or conditions that are too hot, toocold or too stuffy, are common, and in theoffshore environment this is exacerbated by theperceived lack of personal control over physicalwork conditions. Whenever possible, thepractice of more open discussion and debateabout the issues that directly affect workingconditions should be encouraged. This includesthe arrangements for rest and lunch breaks. Thework environment should be perceived ascomfortable and safe and a high standard ofhygiene and cleanliness is desirable.• Safety climateMany individuals offshore are exposed to certaindangers and hazardous conditions at work.While a risk assessment allows us to control andminimise these dangers, some jobs still haveinherent or perceived dangers. For example, thesafety of helicopter travel was identified as oneof the top ten sources of stress by offshore oiland gas workers (Sutherland and Cooper, 1991).Also, among Norwegian offshore workers, morethan one third reported that they felt unsafeabout the transportation of people by helicopter(Hellesøy, 1985). The perceived risk associatedwith helicopter travel was the most commonreason cited for resignation from offshoreemployment in Norway. This action is costly tothe industry and helicopter travel remains areality that must be faced by these workers sincewe do not yet have any means of ‘beamingpeople through space’. However, educationabout the nature of the risk and safetyperformance might help to overcome theirrational fears that are held.• Career development.Fear of job loss and threat of redundancy arecommon features of contemporary working life.Perceived or real, pay and job status inequity,lack of job security or limited potential for futurecareer development are sources of stress. Intimes of instability, poor work conditions aretolerated and employees endure long hours andarduous conditions. This does not happenwithout personal and organisational costs. Akeen, competitive jobs market can threaten thequality of co-worker relationships at a time whensocial support is of particular importance.
Indeed, the stress of insecurity that can bealleviated by supportive working relationshipsmay be broken down if the work force perceivesthat competition is necessary to retain a job.Personnel may also stay in a job that isunsuitable or disliked because no suitablealternative for change exists. This results in coststo the organisation due to poor productivity orperformance• Bullying at workRecent reports suggest that the incidents ofbullying in the workplace may be increasing.However, we can not be sure if this now thereality of work life in the 1990s, or due to thefact that people are more willing to report thatthey are being bullied. Nevertheless, there is anacknowledgement that oppressive behaviour hasa negative effect in terms of reduced well being,morale, motivation and contribution to the job. Itis suggested that bullies are ‘stress carriers’within the organisation. Usually these people donot personally suffer from the effects of stress,but their behaviour causes a great deal of stressfor subordinates and colleagues alike. Whilstthere is no specific health and safety legislationthat deals with bullying at work, employers havea general duty to protect employees’ health andsafety. In law, it is possible to seek redress forbullying behaviours that generate sufficientemotional distress and unhealthy physical stress.Thus an employer must ensure that the dignity ofthe employee is upheld, and acknowledge that heor she has a right to be treated with respect. Anauthoritarian culture, poor work relationships, alack of clear codes of acceptable behaviours, areall conditions that foster a climate in whichbullying is likely to occur. Bullying is oftenconfused with strong management and sobecomes condoned and part of the culture of theorganisation. It can often be insidious and subtleand so the victim has no witnesses and if thereare witnesses they are often afraid of supportinga victim. In some organisations, help-line, help-desk, employee assistance programmes, face-to-face counselling, and the occupational healthservice, all play some role in dealing withbullying in the workplace.
• Change the Micro-environmentRather than put the responsibility for stressmanagement on the individual employee,exposure to stressful work conditions might bereduced by the redesign of work systems andpractices. It is suggested that work redesigncan improve worker morale, motivation andperformance. Although many workerscomplain about having too much to do, orhaving to work at a pace that is too fast, theyalso complain that the job does not provideenough variety or challenge. This can lead to

200
boredom, apathy and low motivation to work.Thus, job redesign interventions can be used toalleviate the problem of ‘rust-out’ in theworkplace.• Work under-load: Under-stimulation
and boredomPrevention of stress associated with ‘rust-out’,due to boredom, and lack of stimulation in theworkplace can be achieved by changing the‘micro’ work environment. This includesincreasing workers' skills, autonomy in the joband providing more opportunities for decision-making. By re-designing or enriching the job, toimprove the amount of skill variety, taskidentity, task significance, autonomy andfeedback, it is possible to improve bothmotivation and job performance and reducelevels of stress. Decisions to make this type ofchange are usually made on the basis of a jobanalysis, in conjunction with work force andjobholder discussions. Job enrichmentintervention strategies can increase jobsatisfaction, improve production, and reduce jobabsence and turnover.• Reducing the stress of shift-workThe need to engage in shift work and work longhours is the reality of work offshore, and thespill-over impact can cause negativeconsequences and costs for the family andsociety itself. Thus it becomes a prudent part ofa stress management strategy to minimise theimpact of these potential sources of strain anddistress that cannot be eliminated from the worldof work. These options include the design of theshift system, flexitime, selection and recruitmentfor shift working, stress management education,and physical interventions such as the use oflight therapy and the drug, melatonin. Clearly,the need to work shifts represents a major sourceof stress among offshore workers but it is likelythat individuals do habituate to shift work and itbecomes physically less stressful with time.However, some work patterns might preventhabituation occurring. Thus, there is a need tofollow guidelines provided for minimising thenegative impact of shift-work and long hours ofworking.• Reduce role stressThe constructs of role ambiguity and roleconflict are acknowledged as potent sources ofstress in the work environment that areassociated with a variety of negative attitudinalhealth and behavioural outcomes. Thus roleclarification interventions can be used as stresscontrol strategies. For example, a roleclarification intervention was used in anengineering company to improve employeecommunication and manage stressful workdemands. Role negotiation is a useful way ofovercoming the problems that lead to
ineffectiveness caused by behaviour that anindividual is unwilling to change, because itwould mean a loss of power or influence. Thismethod works because most people prefer afair negotiated settlement to a state ofunresolved conflict. Thus, they will bemotivated to engage in some action themselvesand make concessions in order to achieve thisaim.• Improve perceptions of worker controlLack of job control is acknowledged as apotent source of stress and perception ofcontrol seems to be important for jobsatisfaction, health and well-being. A varietyof strategies exist to improve perceptions ofworker control and increase the opportunitiesfor decision making at work. These includebuilding and developing semi-autonomouswork groups, quality circles, safetyimprovement groups and health circles.Ultimately the aim is to for the work force tobe empowered and involved in changes to anysystem or practice that induces stress at work.This is to create a better balance between theperceived level of demand and worker control.• Increase worker participation in decision
makingLack of participation in decision-making is aprimary cause of role conflict and roleambiguity, mediated by one's perceivedinfluence over the situation and the efficacy ofcommunication in the organisation. Feelingcontrolled rather than 'in-control' is associatedwith a state of stress; individuals who feelcontrolled are likely to perceive their job as a'strain' rather than a challenge and source ofmotivation.
Secondary level interventions
Although a growing body of evidence supportsthe view that organisational-level stress controland stress prevention interventions are moreeffective than individual-level coping strategies,because they have a more lasting effect, it isclear that the prevention of all sources ofnegative stress is not possible. Thus, the effectsof exposure to stress can be minimised by theuse of techniques to improve the stress copingprocess. They are classified as ‘skills trainingoptions’ and ‘healthy-lifestyle education andmanagement’.
Skills Training to Cope with StressThe objective of skills training is to improve ormodify the individual's response to perceivedstrain to avoid a negative outcome. Thisincludes:

201
• Interpersonal and social skills; leadership skills• Assertiveness• Cognitive coping techniques, e.g. avoiding faulty thinking• Time management• Relaxation training, meditation, yoga, and biofeedback• Type A behaviour management• Anger management
• Interpersonal and social skills trainingEveryone has a vast capacity to being moreunderstanding, respectful, genuine, open,direct, and concrete in his/her humanrelationships. With a sound body oftheoretical knowledge, appropriate models,and numerous opportunities for personalexperiencing, the process of becoming morefully human can be greatly accelerated. This isthe essence of interpersonal skills training. Itincludes a range of communication skills andthe need to understand the barriers to goodcommunication. Interpersonal skills trainingare usually key components of leadershiptraining.• AssertivenessHaving to deal with other people as part ofone’s job can be one of the most stressfulaspect of working life. For example, having toconvey a decision that you know your staffwill not like; having to handle an iratecustomer without losing valuable business ormaking promises that are difficult to keep; or,being faced with unreasonable work demandsor time deadlines. Assertiveness training helpsus to deal with such demands withoutbecoming angry or upset. Assertivenesstraining teaches us to be able to speak-up andbe taken seriously without damaging the rightsof other people• Cognitive copingOccupational stress is now viewed as atransactional process whereby employeesappraise and react to a potential source ofstress. Cognitive style influences our appraisalof a potentially stressful situation and the copingstrategy subsequently used. The use of certaincoping strategies, such as ‘avoidance coping’ ordenial is associated with poor psychological wellbeing, whilst the use of problem-oriented copingis linked to positive mental health. The use ofcognitive restructuring as a stress managementtechnique aims to examine dysfunctionalattitudes and irrational thoughts. The processaims to improve the balance betweenperceptions of a demand and our ability tocope.
• Time managementAs we have acknowledged, an ever-increasingvolume of demand and pressure to do moreand more, in less time, and with fewerresources, are ‘hot-spot’ sources of stress incontemporary organisations. However, ademand situation is only defined as stressfulwhen the perception of that level of demandexceeds the perception of one’s ability to meetthe demand. Thus, the goal of timemanagement is, to ‘work smarter not harder’.• RelaxationThe purpose of relaxation training is to reducethe individual's arousal level when exposed to asource of stress. This technique is used to bringabout a calmer state of affairs, bothphysiologically and psychologically.Psychological benefits include a sense ofpersonal control and mastery, a reduction in felttension and anxiety, and an enhanced feeling ofwell-being; physiological benefits include adecrease in blood pressure, slower respirationand heart rate, reduced muscle tension, lessstomach acid, lower cholesterol in the blood andincreased alpha and theta brain waves toenhance creative and cognitive processes.• Type ‘A’ behaviour managementIn the late 1950s, a pattern of behaviour amongheart attack survivors, called 'Type Abehaviour' was observed. It is nowacknowledged that the Type A Style ofBehaviour, referred to as 'TAB', is a risk factorfor heart disease, independent of heredityfactors (i.e. high blood pressure andcholesterol levels), cigarette smoking, alcoholconsumption and obesity. Recent researchsuggests that it is the hostility component ofTAB that is the factor that increases the risk ofheart disease. TAB appears to be a response toa challenge in the environment and is a way ofcoping which the individual finds rewarding.Although the long-term impact is likely to becostly to the individual and the organisation,the immediate outcome is one of gain fromthese workaholic individuals.• Anger managementThe inability to manage recurrent anger-provoking situations is associated withimpulsive behaviours, aggression and

202
cardiovascular disease. Suppressed anger isviewed as maladaptive and also associatedwith cardiovascular problems. Whilst stressinoculation interventions may help to reducethe stress response when the individual isexposed to difficult conditions, angermanagement courses may also help to avoidundesirable behavioural outcomes.
Also at the ‘secondary level’, options areavailable that aim to keep the individual fit tocope with the pressures of work and living.These include stress education and awarenessprogrammes, and on-site ‘healthy-lifestyleoptions.• Stress education and awareness raisingThese programmes are designed to increaseknowledge about stress, to increase awarenessof links between stress, illness and personalbehaviour, and improve personal stress copingskills. Promoting self-awareness helps theindividual to take actions to reduce their ownstress levels. This is usually offered withfollow-up programmes such as, skills training,relaxation, assertiveness and keep-fitprogrammes.• Healthy lifestyle options for the
management of stressIn addition to stress management training,many companies have adopted healthpromotion as an attempt to keep employeeshealthy. These include weight control anddietary advice, smoking and alcohol cessation,hypertension reduction, substance abuseclinics and fitness programmes.• Exercise and fitness programmesEmployee exercise programmes are probablythe most popular forms of stress managementactivities offered to employees in theworkplace. They are usually offered to as away of reducing sickness absence andimproving work performance. As ourunderstanding of the effects of work-relatedstress increased, it is accepted that ourincreasing sedentary lifestyle is a contributoryfactor to ill-health and a sedentary lifestyle isassociated with increased risk for coronaryheart disease. Benefits of exercise and fitnessprogrammes are in terms of a decrease inabsenteeism, staff turnover, and improved staffmorale and productivity. Reductions in levelsof anxiety and depression, improved moodstates are reported and employees say that theyfeel ‘better’. They also report fewer symptomsof stress and perceive the organisation morefavourably.
This type of intervention is directed atsymptoms of exposure to stress. It is concernedwith the rehabilitation and recovery process ofthose individuals who have suffered or aresuffering from ill health as a result of stress• Counselling servicesCounselling services typically help theindividual employees deal with a particularpersonal or work-related problem. Thereby, theyattempt to increase the employee's capacity towithstand the perceived stressor. Counselling isdescribed by the British Association ofCounselling as the task of giving a client anopportunity to explore, discover, and clarifyways of living more resourcefully and toward agreater well-being.• Employee assistance programmesAn organisation contracts an EmployeeAssistance Programme (EAP) provider to giveemployees (and sometimes their immediatefamilies) access to an external, independent,confidential advice and s short-counsellingservice. EAP counselling is for individualswith work related problems, relationshipdifficulties, illness worries, redundancy orretirement concerns, substance abuse, orfinancial worries, etc. Typically the function ofan EAP is to assist in the identification ofproblems that lead to impaired jobperformance and constructive confrontation ofthe issue. Ultimately the objective is toimprove job performance• Training supervisors and managers in
basic counselling skillsKnowledge that a spouse or partner is unhappymay affect one’s performance, safety or well-being. Management sometimes prefers toregard these issues as ‘none of our business’.However, an important part of themanagement process is ensuring that there iscollaboration with employees in order toremove any barriers that exist to adverselyimpact upon performance and productivity.Distressed employees who are anxious anddepressed because of worries about home arelikely to be ineffective, potentially unsafe, andoften disruptive when they are at work. Byhelping the individual to resolve a home-related stress problem quickly and efficiently,the manager regains an effective worker.Making stress a respectable topic fordiscussion in the workplace is the first step inthis process, because a climate of trust andopenness is necessary for the exchange ofpotentially sensitive information. Therefore,supervisors and managers need training inbasic counselling skills.
Tertiary level interventions

203
• Social support as a stress reducerThe value of emotional support in one's socialnetwork as a protection against adverseenvironmental forces or negative life events iswell documented. Social support from one’sfellow workers and supervisor appears tomoderate the effects of job stress moreeffectively than support from one’s family andfriends and there is much evidence to suggestthat social support can play a significant role inenhancing the level of employee well being. It isnecessary to emphasise the importance ofsupportive relationships and networks during theselection process in order to promote a desirableclimate and culture, since this affects the qualityof working relationships. Thu, a supportiveimage should be encouraged, reinforced andacknowledged as criteria for recruitment into thejob. Managers and supervisors should beselected and trained for their ability tounderstand the need for social support andreflect it in their style of supervision. Structuresto provide support include access to anoccupational health and counselling services andsocial networks and self-help groups need to beencouraged.• Career sabbaticalsThe opportunity to take a career sabbatical canhelp an individual to recover from the effectsof stress. With so many people today workingto the point of exhaustion, organisationsshould encourage staff to take sabbaticals torecharge themselves, ideally, before theindividual becomes a victim of stress.
An integrated model of stress management
It is desirable that organisations will useproactive, preventive AND curativeapproaches to the management of stress, and atthe same time operating at more than onelevel.
Successful Stress Management1. Have a clear idea about why you are
becoming involved in a stressmanagement programme. Identify clearobjectives and goals. For example, is yourobjective to reduce sickness absence oraccident levels?
2. Decide how you are going evaluatemeasure the benefits. Share rewards withemployees to sustain a culture and climatethat acknowledges the link betweenemployee well being and businesseffectiveness.
3. Take the time to understand staff attitudesto the stress management policy andstrategy. Ask employees for heir opinions
and what they need to be more effective,productive and healthy as employees.
4. Define who is to be involved in theinitiative, the project champion, how itwill be staffed, who will be involved, andwhat will you need from each employee.The project must be endorsed at thehighest level to gain commitment to theinitiative and subsequent change.
5. Communicate your intentions in a clearmanner – verbally, visually andpreferably, more than once!
6. Provide guarantees of confidentiality.7. Define and communicate how the
feedback of results of a stress audit or riskassessment will be used.
Conclusion
It is worth remembering that pressure is aninevitable part of living and working, butdistress is not! Whilst our lives will continue tobecome more complex and change willcontinue to be a feature of life in the 21stCentury, we must remember that not all stressis bad. It is a vital part of being alive.
Ultimately, we might need to concede that isno longer useful to use this word ‘stress’ andthe term stress management, because ‘stress’has a negative image. Employees do not likebeing labelled, ‘stressed’, or ‘non-copers’.Organisations do not like causing ‘stress’ totheir staff. In reality, stress managementsimply means identifying all those barriers thatexist to adversely impact upon theperformance effectiveness at work, and thesatisfaction, health, well-being and happinessof personnel offshore - IT IS ABOUTMANAGING ONE’S BUSINESSEFFECTIVELY. Nevertheless, as a genericway of discussing how we can optimiseperformance effectiveness at work, and thesatisfaction, health, well-being and happinessof personnel offshore, it is a useful shorthandphrase to use until we can find another lessemotive label.
Both preventive and curative stressmanagement strategies are essential in anorganisational approach to stress control in thework place. Increasingly, evaluation studiesindicate that prevention is more effective ANDcheaper than trying to cure problems andvictims of exposure to stress.
Undoubtedly, stress management in theworkplace must be the joint responsibility ofboth the organisation and the individual. Bothparties have a duty of care and need to exercise

204
this obligation in order to remain healthy andfree from harm. Ultimately, the effectivemanagement of potential sources of stress isabout being in control of the pressures in one’slife.
Whilst change will continue to exert aconsiderable force on our working lives, itmust be acknowledged that some degree ofpressure is inevitable and can be spur toimproved performance and motivation. Stressis a dynamic process and this means that stressmanagement is not a one-off project. It mustbecome an on-going process within theorganisation. To be successful it must becomepart of day-to-day management and practice,and embedded within the culture of theorganisation. Ultimately this is the onlyeffective and cost efficient strategy to avoidthe unacceptable costs of distress in theworkplace.
We need to understand the nature of stress atwork before we can eliminate or moderate it. Astress control programme can be effective ifresources are targeted to specific problems andaimed at the elimination of the source of stress.Organisations who recognise the high costs ofmismanaged stress in the workplace and seek toachieve enhanced levels of effectiveness and thewell being of their work force, will adopt thisintegrated approach to stress management. Itembraces both individual coping andorganisational change to combat the problemsassociated with stress at work.
References
Hellesoy, O H, (Editor) 1985 “Workenvironment: Statfjord field” Bergen(Norway): Universitetsforlaget.
Sutherland, V J, and Cooper, C L. 1991,“Personality, stress and accident involvementin the offshore oil and gas industry.” Pers.Indiv. Diff., 12:195-204”
QUESTIONS AND ANSWERS SESSION
Question – Dr Ron Gardner, HSEActually it’s more of a point I’d like a view on.Very interesting when you said you felt astress policy should be integrated with thegeneral policy. We’ve found with traditionalhazards it’s more effective to have a set policyon that topic as it focuses the mind. I think thebig difference is that the management isusually the stress problem so I think you’reright in this particular case but I’d just like aview. The second thing is, I think you are alsoright to put health as the tertiary end of this. Itend, (although we’ve got the topic covered atthis conference), to think of stress as amanagement issue rather than a health issue.
Answer – Dr Valerie Sutherland, Sutherland-Bradley AssociatesAs I said, I do get asked for help in how towrite a stress management policy and I don’treally think that’s the way to go. I think if youhave a good health and safety in the workplacepolicy and policies for the way you manageyour business, that actually should cover whatyou need to have in place. My only concern isthat this stress activity just then becomes anisolated issue which is given to some poorproject manager who is targeted as the stressmanagement manager. They are foreveralmost like a leper pushed into the cupboardbecause everybody else would rather get onwith what they see as the more importantbusiness of the day. So that’s my onlywarning on that and what I see going on in lotsof other businesses, certainly not just in theoffshore industry. It’s the same onshore aswell.

205
WHAT’S NEW IN STRESS MANAGEMENT?
Ronny Lardner, Chartered Occupational Psychologist, The KeilCentre Ltd and Mr Bob Miles, HSE
PRESENTATION OVERVIEW• HSE view• Current offshore stress trends• HSE’s strategy• Joint industry project
OCCUPATIONAL STRESS IS A PROBLEM• HSE receives regular complaints from members of the working public• HSE is under pressure from Government, the Trades Unions and a number of single issue groups
to “do something”• Successful civil compensation cases indicate that harm to workers can be demonstrated in court
STRESS OFFSHORE• Until recently, HSE research had not given reason to believe there is a particular problem offshore• The presence of rig medics and offshore medicals has tended to ensure a healthier than average
workforce.
RECENT STRESS OFFSHORE TRENDS• Emerging data from Kathy Parkes’ research indicates GHQ “caseness” up from 15.8% in 1995 to
19.9% in 2000• e.g. six “extra” cases on 150 POB platform• Aggressive down-manning and cost cutting has increased workloads• Rise in complaints about long working hours• Indications of a “two tier” workforce with those in low status contract jobs worse off
HEALTH OR SAFETY?• Debate within HSE, is work-related stress primarily a health issue, or a safety issue?• Civil compensation, stress practitioner industry and stress audits have concentrated on health at the
expense of safety• This bias may be quite inappropriate for high hazard industries, such as offshore
TIME TO ALIGN OCCUPATIONAL STRESS AND SAFETY• Offshore workers’ complaints regarding stress or fatigue usually focus on the increased probability
of human error leading to personal injury or a major incident• The threshold stress or fatigue level, and duration necessary for a significant increase in error
probability, is almost certainly lower than that required to cause a permanent decrement in longterm health
A HIERARCHY• Workers in high hazard industries tend to rank the possible stress outcomes in order of immediacy
and severity:• increased accident risk• reduced physical health• reduced mental health• Why do we tend to address these in the reverse order?• What does this mean?• Probable that stress reduction and human error reduction strategies overlap to a very significant
extent

206
• Emerging evidence from JIP on HF incident investigation (Rachel Gordon at Aberdeen Univ.)that HF error reduction strategies and good management (safety and business) are closely related
PSYCHOLOGICAL HEALTH AND SAFETY HAZARDS? - WHERE TO NOW?• We should be able to integrate HF root cause analyses into business improvement / knowledge
management programmes, most of the issues addressed are turning out to be the same• It is only a small step to include occupational stress into the same programmes as it is all about
“good management”
THE OFFSHORE STRESS JIP• The current work by The Keil Centre / Birkbeck College is challenging HSE’s approach• Explicit links to HF root cause and risk assessment methodologies• Response in terms of the hazard control hierarchy, as first suggested by Tom Cox, and
management standards• Prevention at source
HSE’S STRESS STRATEGY• Public consultation• Work with industry partners• Develop “management standards” on how to deal with a range of work-related stressors
JOINT INDUSTRY PROJECT• HSE / BP / East of Scotland Water / The Keil Centre / Birkbeck College• Initiated by BP’s Occupational Health Department• Risk management framework• Develop simple risk assessment methodology
- stress & human factors• Identify “top three” stressors• Develop, apply and evaluate internal management standards
MANAGEMENT STANDARDS• internally vs externally-developed• specific, locally-relevant stressors• how to prevent / manage• gap analysis• HSE interested in process & outcomes
DEBATE• In your organisation:
- do you have any work-related stress cases?- are these treated as LTIs?- if not, why not?- would doing so help address root causes?
DEBATE• Do you think the video promotes the right message about work-related stress?• Do you think it would help remove stigma?• Would your organisation endorse this type of message?
QUESTIONS AND ANSWERS SESSION
Question - Jake Molloy, OILC OffshoreUnionYou say that Kathy Parkes’ research suggesteda 4% increase in stress cases. Could it be thatin actual fact there is significantly more and adegree of under reporting? The reason I put
that to you is that certainly in the last sixmonths I’ve dealt with two individuals whohave reported stress, who subsequently weresacked in actual fact because the medicalaspects for offshore working deemed them tobe unsuitable for offshore working. So do youthink that could be a deterrent for reportingstress?

207
Answer – Ronny Lardner, Keil CentreI guess that’s possible. I guess the other thingthat we need to remember is that in anyorganisation no matter how well run it is, youwill get incidences of mental health problemsat any point in time. I think the important
point with this research was that it tended topoint towards an increase, without explainingat the present time why that increase hasoccurred.

208

209
THE ROLE OF EMPLOYEE ASSISTANCE PROGRAMMES INORGANISATIONAL STRESS MANAGEMENT
Dr Stephen Galliano, ICAS Group
Occupational Health Offshore
The role of EAP in OrganisationalStress Management
29 March 2001
Work Stress
Body of evidence work can cause stress
working environmentworking conditionsnew technologywork overload/underloadjob design
work pacerole in organisationrelationshipspoor communicationsdecision-makingorganisational style
Work/Personal Stress
Many personal sources of stress butwork/non work issues will often beclosely inter-related and thereforedifficult to disentangle
Health & Safety at Work (1974)
If work stress and
stress ill health then it
becomes a health and safety issue
Employee Assistance Programmes
Worksite focused service to assist in theidentification and resolution of employee concernswhich affect, or may affect, performance
work matters ………. work demands, relationships,work-life balance, stress
personal matters ….. relationships, health,emotional, family, alcohol,drugs, financial, etc.
Employee Assistance ProgrammesCore elements
For employees & managers
• Confidential/timely problem assessment
• Provision of short-term psychological helpand other specialist support services
• Referral on for longer term help
• Manager/OH/HR referral
• Manager consultation

210
Employee Assistance ProgrammesCore elements
For the employer
• Assessment of need/design
• Communication of EAP policy
• Partnership philosophy
• Effective implementation/promotion
• Training for managers
• Feedback to organisations of themes and trend
EAPs & Organisational Stress Management
EAPs are not intended (primarily)to prevent work-related stress norto reduce the likelihood that it willever occur ……...
Employee Assistance Programme
A strategic intervention designed to
produce organisational benefit
Matrix ofOrganisational Stress Management
Primary Secondary Tertiary
Prevention Resilience/coping resources
Remedial
• Change management andPolicy implementation
• Stress auditing• Risk Assessment
• Training and education• Health & fitness• Manager Training
• Medical treatment• Psychological treatment
and counselling• Grievance Procedures
Accurate and timelyorganisational feedback
Early identification ofindividual problems
Counselling (self-referral)
Consulting Manager training in identifying atrisk employees
Crisis support
Crisis Management Policy work-life balance services Manager referrals
Manager consultation
Employee Assistance Programmes
Usage of EAP Services
Work Life
Services
65%
Counsel l ing
Services
30%
Managerial
Consul tancy
5 %
Counselling Clients
Supervisory 35%
Non-Supervisory 65%
Usage of EAP Services (by problems)
Oil Industry
General
Stress
25%
Other
(contractual)
etc
35%
Change
Issue
40%Work-related
25%
Personal
Problem
75%

211
EAP & Organisational Stress Management
Case Study 1
Large insurance company, sites throughout the UK.
8 calls received at our 24-hour centre regarding alleged ‘bullying’in one large site (call centre) involving 2 different call centresupervisors.
Feedback process agreed
Outcome relaunch of corporate harassment policy
training of internal harassment “counsellors”
EAP and Organisational Stress Management
Case Study 2
Multinational telecoms company
4 Middle managers in 2 different business units understress long hours expected (12+) and overseastravel v. poor work-life balance and consequent familyimpact.
Outcome Work-life balance/travel policy
Time in lieu procedures

212
QUESTIONS AND ANSWERS SESSIONS
Question - Tony Garner, ConocoYou say you’re a good provider and seem todifferentiate between good and bad EAPproviders. How do you know you’re goodbecause it’s so difficult to audit EAP becauseof the confidentiality issue? By definition,occupational health/human resources don’treally know what you are doing.
Answer - Dr Stephen Galliano, ICAS GroupDid you say Conoco? I just wanted to checkwhere you came from because we’ve justmanaged to survive a major audit by DuPontand they sent in their heavy troops from theUS and we’re expecting companies likeConoco and our oil customers to do exactly thesame. We’ve had probably about four or fiveaudits every year. The auditors up till now,most of them have been Americans coming inworking with occupational health in the UK.So we’ve had occupational health doctorsviewing our cases, viewing our workflow,studying our procedures, looking to seewhether we implement the procedures that wehave written down, interviewing our affiliates,checking out their credentials, checking outwhat they think about us as an EAP provider.We’ve also had one audit, which has involvedUK-based auditors. That has also gone well.An audit is possible, and audits are done. AllEAPs should be audited at least every twoyears. You can find out a great deal about itthrough an auditor, if you know what you arelooking for, and I take your point.
Question - Jim Johnson, Shell UKJust on the point of confidentiality. When wehave a problem with an employee we tend tohave a sort of mini case conference where wetypically bring in OH, HR and the line. Itwould be useful and perhaps reduce a sense ofstandaloneness of the EAP if they could join inthese things. Would you have to have theclient’s express permission before you takepart in such a mini case conference?
Answer - Dr Stephen Galliano, ICAS GroupThat is if we are already consulting the clientand helping that client?
Answer - Jim Johnson, Shell UKYes.
Answer - Dr Stephen Galliano, ICAS GroupThere has to be consent for any one of us todisclose any information about the client soyes, you need the client’s support for us to dothat. It would be totally unethical for us to
turn up and disclose issues that hadn’t beenconsented to with the client beforehand.However, I have to say that in that sort of case,it would probably have been referred to ussome months before. We would prefer that amanager or an occupational health doctoractually made a referral and in the process ofreferral engaged the employee’s consent forICAS to disclose to that one person forexample on a need-to-know basis. I think tobe able to have a clinical discussion about theclient’s issues in front of a whole panel ofpeople would also be somewhat questionable.
I often leave it to occupational health doctorsto say what they want to say to HR and linemanagers. We will disclose everything withoccupational health and I know that they willgive as little information as they can, butenough to make the determination aboutfitness for duty etc, work safety etc. So theanswer is ‘yes’, you could have somebody at acase conference, but you would need somekind of consent from the client to be able todisclose any clinical personal data.
Question - Bob Hanson, BG GroupYou made reference to the fact you traincounsellors? Are these lay counsellors, peoplein the workforce?
Answer - Dr Stephen Galliano, ICAS GroupWithin the context of the harassment exercise?
Answer - Bob Hanson, BG Group?Yes.
Answer - Dr Stephen Galliano, ICAS GroupWe didn’t call them counsellors. They werecalled listening posts but nobody wanted todescribe them as listening posts, so theorganisation was quite keen to call themharassment counsellors but with a very clearbrief, supervised on a regular basis by the way.We did train them. We did a whole series offour-day counselling skills programmes andwe did a top-up every year for them.
Question - Bob Hanson, BG GroupAnd did their colleagues feel happy aboutusing them?
Answer - Dr Stephen Galliano, ICAS GroupThe policy was quite well written up really andit allowed for people in certain business unitsto contact a harassment counsellor in anotherunit so they were not expected to be talking totheir own colleagues. They’d set it up in asindependent and safe a way as possible really.There was a published list in the organisation

213
with the locations of all of those people, so theidea was they would ring somebody who wasthree hundred miles away in another site ratherthan in their own location.

214

215
FEEDBACK AND DISCUSSION – HUMAN FACTORS ANDPSYCHOLOGICAL HEALTH – WHERE NEXT?
Introduction to Video Session – Ronny Lardner
Just a little bit of introduction to this video.It’s intended really as a concrete example ofhow an organisation can perhaps bringtogether many of the things we’ve discussedthis morning in relation to stress. This isparticularly relevant to the awareness part ofdealing with stress. The history of this is thatit is something that occurred in your ownindustry where back in 1998 BP atGrangemouth had some issues about stress.There was an analysis, an action exercisecarried out there to identify what were themain work-related causes of stress and thosewere addressed. At the same time it wasrealised that there was a need to raiseawareness amongst the whole workforce aboutthe site’s position on the topic of stress andwhat was available locally to deal with it.
I was a member, along with many other BPemployees of a working party, a vertical slicethroughout the organisation including safetyreps and process operators who had the task ofputting together an educational programme forthe site about stress. The final product of thiswas a video, an intranet website, booklets forevery employee and also a poster campaign.That was followed up by seminars formanagers, team leaders and safety reps, inshort everybody who had responsibility forother people.
What we are going to do is look at the video.Bear in mind that it was produced three yearsago and maybe thinking has moved forward abit since then but at the time it was believed tobe the right message to put forward. I wouldbe interested in getting your views after we’veseen it about whether you agree with that.
- Video shown to delegates.
Question - Ronny Lardner, Keil CentreOn the basis of what we’ve listened to todayand your own personal experience do youthink that video promotes the right sort ofmessage from an organisation about workrelated stress? Does anybody have a view onthat?
Answer - Tony Garner, ConocoI thought it was a bit on the negative sidewhereas Dr Sutherland was very much on thepositive side of stress. Stress is veryimportant, a very good tool, it’s a verymotivating subject and that was a negativeimpression of stress. Stress isn’t negative.
Question - Ronny Lardner, Keil CentreAny other views on that, on the overallmessage that came over?
Answer – Dr Ron Gardner, HSEIt’s a little focused on the individual. It wasnice to hear you say there had also beenseminars and materials for managers, but whatmanagers could actually do towards theprocess didn’t really come out of that at all. Itwas very person orientated.
Answer - Ronny Lardner, Keil CentreIt’s interesting you should say that. At thetime our intention was to try and get themessage over about the importance ofpreventing things rather than it being anindividual – a subject that was purely aboutindividual coping. We thought we made greatstrides in doing that by getting the seniormanagement to endorse it and allow inclusionof that sort of message. I think perhaps thingshave moved forward a bit since then and nowpeople would be looking for a much strongerpreventative message.
Question - Dennis Krahn, InternationalAssociation of Drilling ContractorsIn that situation you had the ability to gooffsite. In an offshore location you don’t.Could you talk about the difference in thesituations and what we might do about that?
Answer - Ronny Lardner, Keil CentreIs that in a sense Dennis that employees havethe ability to seek support offsite?
Question - Dennis Krahn, InternationalAssociation of Drilling ContractorsThat’s correct, implying perhaps that initiallythere may be some shyness to be seen to betaking advantage of these resources. If so,then your only recourse is to go where yourshyness doesn’t matter, where nobody but

216
yourself can see. Is that a factor in getting tothe state of play offshore that we would like tobe at?
Answer - Ronny Lardner, Keil CentreYes, I’m sure the fact that it’s a lot moredifficult to access resources confidentially ifyou’re working offshore for a fortnight at atime is very relevant. I guess perhaps peoplestore that up until they come back onshore.One of the intentions of the video was to tryand help remove some of the stigma that’sassociated with stress, so it’s a legitimatesubject for conversation. Personally I used tobe in the police service. I was in the policeservice for twelve years and at that time thenotion of mentioning or discussing that youmight be experiencing stress would becompletely out of the question. It would justnot be a subject that you could have raised anddiscussed because it would have been viewedvery much as though it was about yourindividual ability to cope. It wouldn’t reallybe a legitimate subject. So, one of the things Iwondered of the audience was, do you thinksomething along those lines actually helps toremove the stigma that is attached to the topicof stress and legitimise it as something you candiscuss?
Comment – Mr Kevin O’Donnell, HSEI tend to agree with you there. If you see thevideo as part of a package, some of the aspectsdescribing the symptoms of stress are useful.People here are probably reasonably welleducated as to what these are. A lot of peoplein the workplace may not realise very simplywhat the symptoms are that they areexperiencing and having it explained at a verybasic level, as Ian and Tony did, is a very goodstarting point as an overall package, not just onits own. It’s got to be remembered that thevideo isn’t standalone, it’s got to be part of apackage for a whole set of issues.
Question - Ronny Lardner, Keil CentreI guess the final question I wanted to ask theaudience is do they feel that their ownorganisation would endorse that general sort ofmessage about the subject of stress? Wouldthat be the sort of message you would endorseputting over to your own employees, or wouldthere be a different type of message you wouldwant to put over?
Chairman – Rab Wilson, AEEUIn essence, what the video was for me, wasgiving the opportunity to show you what BP isdoing. Now whether we like it or not, BP isidentifying that there are problems with stress.
Dennis has raised an important question, butwe’re here today for one particular thing.We’re talking about offshore and there aredifferences. I think really we want to open upthe debate. We’ve got a panel of speakers hereand really what we should be doing is sharingthe views because I think there’s a silence instress that is ready to explode in this industry.I think the one area that certain people havegot to deal with, particularly in dealing withoccupational health, is stress.
As Ronny says, it’s three years ago. BP hasdone this on their refinery at Grangemouth.Dennis has raised an important question thatwill be in everybody’s mind. There was alsothe question from Conoco which I thoughtStephen in a sense had answered - how do youthink you’re doing well? Well it’s up to theorganisations that take you on to audit.
In general let’s open up for the panel and ifanybody wants to, throw in questions aboutstress. How we would handle it? How wewould tackle it? Bear in mind that our aim isto share views, challenges and successes andlook at research studies.
Comment – Una Corpe, Shell ExproI’ve been involved in stress management atShell for about 10–12 years and this iscomment rather than a question. We’ve donelarge-scale research in the past. It’s takenmaybe 12–18 months to do some research andthen to get our final figures. To carry on fromthat, we looked at EAP programmes, many ofthem in the UK and we looked at someexperience in one of our own Shell operatingcompanies further south. We really didn’t findit beneficial. Going back to the speaker’scomments of good and bad EAPs, we didn’tfind EAPs particularly helpful at that time.Because there were particularly maybe good tothe individuals, but not particularly good to theorganisation for the management of stress,whatever the causation was.
We haven’t seen much development from thatas such. What we’ve done within theorganisation is we’ve used the ‘Triple A’management approach that Dr. ValerieSutherland has described. We’ve more or lesshad that system in force for probably aboutfive years. Now what we do; we do real timemeasurement; we do the ‘Triple A’ approachas regards the education and awareness; we dothe stress research in real time where weinclude GHQ and the HADs mental healthquestionnaires in all of our health screening.In addition to that, we do surveys for any areas

217
that consider they’ve got hot spots onshore oroffshore throughout our organisation. Thefigures that we’ve got on this real time stressanalysis are about 14-15% which comparewith Kathy Parkes’ figures from about four tofive years ago which we were part of her studyand which haven’t increased since then.
We look closely at our stress measurementwithin the organisation and integrate it into themanagement. There are one or two of ourareas where we’ve got hot spots. We’ve hadhot spots on offshore installations and one ofthem in particular that had fairly high casesrates was actually one of the areas that had anEAP type programme in place. So, using our‘Triple A’ approach for reinforcement in thatparticular area, the levels have come rightdown to the 14-15% for the company as awhole.
Going back to the EAP programme again. Inour experience that system wasn’t integrated.We weren’t able to integrate that system intothe company because of the confidentialityelement. Not to do away with theconfidentiality to employees, but to releaseinformation to management as a whole, youneed to be able to have more real timeintervention so as to do something about it.Because, if the individuals go off sick withstress that may be the first time that you findout about it, if it’s just an EAP programmethat’s in place.
We measure sickness absence within ourcompany. I said at the beginning of thisconference that our sickness absence rate forShell Expro is one percent. We look at thecausation of absence and looking at thecausation of absences of 28 days or over, stressand backs are the main problems. They are avery small proportion of the total, but in sayingthat, if somebody actually goes off sick withstress, they’re off for at least six months.What we need to do is have an earlyintervention programme which is a total‘Triple A’ management approach, which iswhat we’ve got in operation and which works.
Comment – Dr Stephen Galliano, ICASGroupI think one of the challenges when you’relooking for an EAP, (well an external EAPbecause a lot of organisations have internalprogrammes equally but not more effectiveand powerful than external ones) is trying todecide what you want the EAP to do, and howyou want to position the EAP. I think if thereis a very up front substantial stress
management initiative and you’ve got prettyfirm views of how you want to roll thatinitiative out, then it would be pointless to getan off-the-shelf programme coming into yourorganisation because it wouldn’t integrate thatwell with your requirements.
If you want GHQs and HADs and whateverelse done for all those employees presenting toan EAP for example then I think you can, ifyou specify that, and if it fits in. It has to beupfront but I have to say you need to positionit very carefully. One of the problems thatexists in the market is that you get customerorganisations saying okay, we want an EAP.Let’s invite proposals and let these people sendus one of their proposals and it’s often not easyto try and understand the real motivationbehind the EAP. It may not be that easy tounderstand why the organisation wants an EAPand in fact how far the organisation is going toroll out an effective stress managementprogramme. But it’s sad that you had thatexperience I’ve got to say, and it’s regrettable.
Comment - Dr Valerie Sutherland,Sutherland-Bradley AssociatesI have been in the fortunate position to be ableto speak to a lot of the guys and fewer of thewomen who work offshore and certainly not toadmit to being under stress is something thatcomes over quite clearly. What they also tellme is that they don’t have anybody to talk towhen they’ve got problems. When you teasethat out a bit further they probably will go andtalk to somebody like the radio operator or themedic. So I think that’s a resource andStephen’s going to hate me for this, but weshould consider training somebody like that insome basic skills. We need to acknowledgethat they can’t provide the full gamut of acounselling service offered by an EAP, butthey can provide help.
If you’re on a rig for fourteen days and youhave a problem, and you’ve got to sit there foranother thirteen and stew about it, well that’sprobably a person who is an accident lookingfor a place to happen, so I do think you doneed this. You can’t go (as they do in BPGrangemouth) to another building tuckedaway in a corner of a site somewhere. It’s gotto be something that people can do. There isaccess to telephone services with EAPs.Maybe that could be used more, but then thereis still this issue of confidentiality. That’s mypoint on EAPs.
I do want to say something about getting topeople quicker before they become sick which

218
I agree is absolutely crucial. We are inprevention here and being proactive. Part ofmy notion of integrating something into day-to-day systems and practices is that there’s gotto be some mechanism where people either asindividuals, or in a group, can just simplyreflect without even using the word stress.How am I doing? Am I effective? If I’m noteffective, why not? If I don’t feel job satisfiedwhy not? Then you’re going to tease out thereasons for this.
If that’s done, I guess I’m saying a bottom-updriven model, they can then go to a supervisor,or crew manager, or whatever you like to callthem, and then sit down as a group and say canwe do something about this? Can we take theheat out of this situation? I don’t think wereally tap in enough to people out there andask their opinions of what they want done andhow they would better manage their stress. Ifeel, because we’re all so busy all the timewe’re rather like hamsters aren’t we running inthis wretched wheel and hamsters just seem todo it for hours and hours and hours and hours.It’s not just offshore this is a criticism of, it’sall the other places I go onshore. We justdon’t seem to be able to get out of that wheeland think about what it is we’re doing. A lotof the time we look around and think if I couldjust stop for a few minutes and reorganisemyself, things would just be so much betterand less stressful. But we seem to be on thismadcap go go go all the time and that’s what Ithink is creating a lot of stress.
Chairman – Rab Wilson, AEEUWe are here today, in particular to listen to youand you’ve been very patient out there. Just acouple of thoughts for debate here. I’ve beengiven something here. In your organisation doyou have any work-related stress cases? Arethese treated as LTIs? If not, why not andwould doing so help address the root causes?It’s something to think about but becausewe’re here to listen to you and the speakershave had a fair bit today, maybe if we take oneor two questions and open it up.
Question - Ian Loughran, Phillips PetroleumWithin our organisation, people who work forPhillips have got access to an EAP throughtheir health care if I remember rightly. Whatare the panel’s thoughts about the fact thatwith multi-skilling, that it uses contractorworkforces etc. which means you’ve gotpeople who’ve got different terms andconditions and may not have access to EAPs?How can the duty holder try and deal with thisissue to try and bring stress out into the open
for those who haven’t got the ability to fallback on an EAP programme themselves? Youtalked about basic training for the medics. Itseemed to me that the medic or the OIM,should surely have some sort of responsibilityhere – probably the OIM - because he isresponsible for everybody’s health and welfareon the platform. I can understand there aresome pitfalls involved, but how would we goabout trying to ensure that all the people thatyou have working on your platform can getsome stress counselling?
Chairman – Rab Wilson, AEEUThere’s somebody else who has got a questionand we’ll ask it because you’ve asked thepanel on their views on the multi-skilling onewith stress. There’s another question as welland we could take two questions so that thepanel get the opportunity.
Question - Gareth Powell, BPI’m in design but I’m an offshore medic, so it’srelevant to both the last points in a way.Certainly within BP we do have training inbasic counselling and stress managementskills, but you need to remember the situationoffshore, that we’re offshore for fourteen dayswith these people as well. Whereas somepeople are quite comfortable to come and talkto us about problems in their personal life ortheir work life, there are others for whomwe’re just a bit too close. They’d much ratherspeak to someone they don’t know, a bit moredistant on the end of the telephone. I certainlythink that’s where EAPs are invaluable. I’vehad experience over the last couple of years ofpeople that have used both those routes withequally good outcomes.
Answer – Dr Stephen Galliano, ICAS GroupI wanted to make a comment in fact, initiallyin response to this gentleman’s question aboutoffshore workers and how do they get to seesomebody offsite and partly to this lastquestion. I think that all of our oil customersallow access to the EAP to the contractors aswell. I can’t think of any of our customers thatdon’t to be honest with you. It would seemthat they also pay for that, i.e. it’s not thecontracting companies that are paying for theservice, but that the oil producers have takenthe view that the contractors are working onproducers’ installations, producers’ platforms.It’s the producers’ responsibility and thereforeit is important that contractors also have accessto certainly at least the telephone serviceswhen they’re offshore and all the rest of itwhen they’re onshore and that their familiesalso have access to it.

219
I know that these people use our services.There are telephones on platforms, thoughconditions are better in some than others interms of how much privacy you get, how manylines there are and how many telephone pointsthere are. I have to say that we do get regularcalls from the platforms. The only problem weexperience is that the contracting companiestend not to join in in the promotion andimplementation of those services to theircontractors. Therefore, what we do now is gooffshore on a fairly regular basis and dopresentations offshore to the managers,supervisors and to all staff, whether they arecontractors or employed staff.
Comment - Dr Valerie Sutherland,Sutherland-Bradley AssociatesMy comment is to the gentleman from Phillips.I agree with Stephen on that. I presume,unless you specify that all your contractorsprovide a service for their employees, thenprobably you are going to be it.
Question - Dennis Krahn, InternationalAssociation of Drilling ContractorsI would like to ask a question relating stress tosafety performance. In the drilling industrywe’ve had, I can recall, three very seriousincidents where it seemed like the team knewwhat to do, but they didn’t do it. One of theteam didn’t do something right and nobodyelse called that out. Training seems to havebeen okay, management tells them to take timeout for safety and not to hurry, so my questionis this. Is there some amount of stress that wehaven’t identified that causes them to losesituation awareness such that they almost don’tsee that it’s wrong; or like it’s disembodied -they see it’s wrong but it’s not going to happento them, or they’re for the moment immortal orsomething. Can you help us to understand thisperhaps, this relationship?
Comment – Dr Jim Keech, BP, Chairman ofUKOOA HACMy first comment is that the approach has tobe an integrated approach. We’ve heardaspects of bits and pieces. If the EAP is towork, and I believe EAPs can work, they haveto be integrated within the whole of thepsychological health plan. I would say tooperators and contractors alike that they needto consider planning for psychological healthjust as much as physical health. Your EAP, ifproperly utilised, can be very much part ofthat. Certainly we’ve been working toimprove access to EAP. We do have accessvia telephone and yes we do pay for all our
contractors to access. But we’ve found thatthere is a barrier, there is a psychologicalbarrier. It’s very difficult sometimes to pickup that telephone and there is clear evidencethat many people pick up the telephone and putit down again before it actually gets answered.What we are trying to do there is look at, incooperation with our EAP provider, alternativeportals. We’re looking at the use of the web,we’re looking at the use of chatrooms andusing any technique that people will feelcomfortable with to get this help that we’repaying for.
The other issue is using your EAP. Not everyoffshore worker lives in Aberdeen. Myworkforce is spread throughout the UK andnear Europe and I have a great benefit in usingthe EAP. Our EAP has a very good networkof psychiatrists, psychologists, specialistcounsellors. We have been using those fortherapeutic reasons to provide us with thepsychological support network where we canrefer where necessary. This is a service I canoffer to general practitioners when managingour cases as well. I suppose the end of it isthat you have to integrate the whole lot.Include the medic training - we certainly havedone that. Include the management training aswell. Keep it in the public domain. Keep it inmanagement’s view. Finally, try and stopmanagement taking unthought out initiatives,because there’s one sure thing, there is nomagic bullet, but that doesn’t necessarily stopmany of our managers going in search of it,somewhat like the holy grail I suppose.
Comment - Ronny LardnerI’m just going to comment on I think it wasDennis’ point about incidents where youwonder whether stress played a part in it. Iguess the only thing you can say about that isit’s very difficult to determine after the eventwhether that’s actually the case and it wouldsimply be speculation on my part to commentfurther on that. I think it’s very difficult afteran incident has taken place to determine withany certainty whether, for the individualsinvolved, being under stress was relevant inindividual cases.
Comment – Professor Josephine Arendt,University of SurreyI was just going to add to that question aboutlack of decision making ability cognitiveimpairment over here. Without wanting tolabour the point, there has been the recentpublication that jet-lag crossing time zonesrapidly induces deficits in cognitive reasoningand ability to perform, and long term

220
moreover. Now you may think that’sirrelevant but it’s not because it’s precisely thesame situation for an unadapted night shiftworker.
Comment - Dr Valerie Sutherland,Sutherland-Bradley AssociatesCould I just say that I think if people weretrained and educated to understand the stressprocess, not just to be told it’s going to makethem feel irritable or have a dry mouth, butwhy they feel like that. As Jo says, we knowthat if you are under stress you do havecognitive impairment that will affect yourreaction times. If they can know that they aregoing to be impaired in these ways and theyare going to have the physiological andemotional reactions, then they are a little bitmore prepared for it, without blaming them forsomething that they can’t cope with, that it is anormal response and if they can recognise it.It’s the sort of training you would expect bombdisposal experts to have. If they’re crouchedover the bomb I should imagine their stresslevels are very high but they are just trained tooverride those because they know that’s what’sgoing to happen to their body. They arehuman beings. They’re not robots.
Comment - Jake Molloy, OILC OffshoreUnionAll the speakers have touched on, and indeedthe video touched on, the issue of self-confidence, which in itself brings about thisfeeling of empowerment. I think anobservation sitting on the workforce side of thefence is that that is severely lacking. If youcan address the self confidence andempowerment issue, then it may assist inreducing stress, incidents, accidents etc. Onetypical example:- if the workforce wereempowered I’m quite sure that we would seean immediate reduction in working hoursoffshore and address a lot of the problems thatwe were talking about here this morning.
Question - Steve Taylor, Shell ExproYour comments, Mr Chairman, on the questionthat’s not been answered at the moment. Yousaid about the opinion of people actuallyclassifying stress or people off with stress asan LTI. Well I guess there are the regulatorsin the room secreted amongst us at themoment. I’d like to hear what their view is onthat because to my knowledge everything thatwe have is either medical, the guy’s injured,he’s off as an LTI, or he’s off for medicalreasons which doesn’t appear. An opinionplease.
Answer - Dr Ron Gardner, HSEThere are various aspects to that. I might wantto pull in Shirley and Alan as well because oftheir background to make sure I get this right.Stress per se is not reportable. There is nomechanism for reporting it except as I recall inparts of RIDDOR there’s some generality tocover things you need to report, but stress as acondition isn’t reportable. It’s not included. Idon’t see any simple mechanism for sayingyes, you report it. Accidents are the only oneswhere you need to have a three-day limit. Allthe other illnesses and diseases if you’ve gotthem, if they are reportable, they are reported.It doesn’t depend on the amount of time youhave off. It just happens that stress per se isnot defined.
Comment - Steve Taylor, Shell ExproThe very point of this conference is getting offthe back foot, which is lagging indicators ifyou like, such as accidents, and getting on thefront foot - occupational health - stoppingaccidents before we have them. My pointwould be perhaps we need to look at this againbecause, as the lady said up there, stress is anaccident waiting to happen.
Comment – Dr Ron Gardner, HSEI couldn’t agree more but your originalquestion was about what the regulationscurrently say. One of the points that was madeearly on in the conference was that underSecuring Health Together one of theprogrammes is entitled ‘Compliance’ and partof that is looking at whether our regulationsare fit for purpose, whether they needchanging. Maybe this is one area where we doneed some changes. The other point I wouldmake, Jim Keech spoke earlier as well aboutthe work that Step Change is setting up interms of collecting medic consultation data,time off data, things like that and maybe againthis is a mechanism for picking up this sort ofincident.
Answer – Dr Jim Keech, BP, Chairman ofUKOOA HACJust to answer some of the points. Theregulator doesn’t help. RIDDOR certainlydoesn’t help. It’s not their fault. Most of theoperators here are already recording theseevents and certainly I can speak very definitelyfor BP that we do record psychological illnessas an occupational illness. It is reported as a‘day away from work case’ and we are awareof it and do report it and try and manage it. Togo on on Ron’s point, we intend certainly inStep Change as we find this way forward withthe health database, to look at psychological

221
health issues. I’ve recently had a report.We’ve got nine thousand encounters nowclassified in the last two years in BP. We haveincluded psychological health classification inthere and this is very much the sort of thing wewould want to do with a cross industrydatabase. I think what it has shown me, andwhat I’ve been able to use when presenting tomanagement, is the psychological ill-healthload as represented by the work that theoffshore medics are doing. It doesn’tnecessarily cause an accident, it doesn’tnecessarily cause anybody to go off sick but itis captured there in the encounter. Certainlyon some installations we have classified a thirdof the workload on encounters as being due topsychosocial encounters.
Question - James Johnson, ShellWe, like BP, record sickness absence frompsychological problems as well, and we alsoinclude contractor staff as well as operatorstaff. We’re faced always with the problemmentioned earlier of trying to tease out thepersonal or domestic component from thepurely occupational one and we really have toget around and decide which is the more
predominant factor there. I wonder if thepsychologists have got any comment to makeabout the use of the word ‘pressure’ as being agood thing in the individual? I think that tomost people pressure has got a bit of aprejorative spin to it.
Answer – Ronny Lardner, Keil CentreMy comment would be that I think there is alot of confusion about these terms and you’vegot to come to a decision about the best ones touse and use them consistently. I notice that theHSE’s definition of stress in their publicity isthat there is no such thing as good stress. Youoften hear people say well a bit of stress isgood for you. I don’t think that’s a helpfulmessage to use because people can use that illadvisedly. I certainly feel that the messagethat there is no such thing as good stress, butpressure is a positive thing is a consistentmessage. I think perhaps what you’re referringto is that many people would say whenpressure becomes excessive it is a problem.That’s when it becomes stress.

222

223
DAY 3
AFTERNOON SESSION
SESSION THEME – WELLBEING AND FITNESS FOR DUTY

224

225
HEALTH CARE AND FIRST AID ON OFFSHOREINSTALLATIONS
- THE REVISED ACOP
Alan Morley, Safety Policy Directorate, HSE
I worked on production of the revisedApproved Code of Practice on the OffshoreFirst Aid Regulations. I shall outline for yousome of the main changes that were made andexplain why we made them.
The revised ACoP comes into force on 2 April2001. And on that day the old one ceases tohave effect. You can buy copies of the revisedACoP from HSE Books and other good booksellers. The price is £6.00.
Revision of the ACoP followed the Health andSafety Commission’s review of all health andsafety regulations and ACoPs. TheCommission found the offshore first aidregulations were properly goal setting, but thatthe ACoP was too prescriptive. As a result, in1998, it published a Consultative Documentproposing changes to the ACoP (but not theregulations) and inviting comments. I’d like tothank everyone who responded. We tookcareful note of all of the comments wereceived, where possible making alterations towhat had been proposed. It became a lengthyprocess. Health care and first aid is a subjectabout which people have strong views. It led toa further round of informal consultation beforethe revised ACoP could be finalised.
There were a number of reasons that wecouldn’t take everything into account. Theseinclude:- legal reasons,- the extent of HSE’s remit,- some respondents gave opposing views or
their suggestions were not workable.
There are five main changes.
The first is about assessing needs. The revisedACoP brings the provision of offshore healthcare and first aid into line with modernlegislation. For health care and first aid, dutyholders will now determine what people,equipment and facilities are required throughan assessment of needs. So that, in future, dutyholders will establish the requirements for theirown particular installation, rather than mostlyrelying on lists in the old ACoP.
Continuing to specify minimum provisionlevels for people, equipment and facilities doesnot fit in with making an individual assessmentof needs. So these lists were dropped in favourof a new appendix, which sets out factors thatduty holders need to consider when makingtheir assessments. Factors like:- how many people are normally on board,- the types of activity taking place,- likely weather conditions,- and proper storage, supervision and security
for prescription only drugs.
Lets now look at the medical equipment list. Anumber of respondents asked for the lists ofequipment and facilities in the old ACoP to beretained. Their continued publication by HSCwould have been against the Commission’spolicy of moving to a goal based regime. Butthey still have value, for example, as a meansof reference. UKOOA have therefore takenthem over and published updated lists. Theyare called Guidelines for First aid on MedicalEquipment on Offshore Installations andcopies are available from UKOOA.
So far as the role and responsibilities of anoffshore medic are concerned, we have addedguidance as an Appendix. It includes advice onwhat are and are not suitable secondary rolesfor offshore medics. Suitable ones may wellinclude:- helping prepare the assessment of needs for
an installation,- making health-based risk assessments,- and basic first-aid training.But not roles that could be conflicting, forexample, helicopter landing officer - youshould not plan to have one person in twoplaces at once during an emergency.
More prominence has been given to healthcare. As already indicated, the name of theACoP has changed to ‘Health care and first aidon offshore installations and pipeline works’.Thus adding ‘health care’. This followsconcerns raised by a number of people, thathealth care should clearly be a part of theACoP, and not take second place to first aid. Inspite of their titles, the regulations and ACoPhave always dealt with both health care and

226
first aid. But in re-writing the ACoP we havetried to make the place of health care clearer.So, as well as the title, for example, theAppendix on the roles and responsibilities ofoffshore medics clearly includes health care.
Finally, we have revised some of the trainingarrangements. In particular trainers no longerhave to have experience of working offshore.This will only directly affect the trainingorganisations. The old ACoP gave noindication about what the experience shouldbe. We concluded an understanding could - forthe purposes of first aid and health care - beobtained in other ways. The most importantfactor is for people to be used who are goodtrainers. This should ultimately be of benefit toeveryone.
And secondly, for training, especially first aidtraining, the ACoP has been revised to bring itmore into line with what is said in theONSHORE first aid ACoP. For example, thelist of training subjects for offshore first-aiders, has been re-written as a list ofcompetencies.
In revising the ACoP, we realised that theoffshore emergency first aid advice leaflet isvery similar to the onshore one - ‘Basic Adviceon first aid at work’. After consideration byour doctors, we decided that there is no need tohave a separate offshore leaflet. So this hasbeen replaced by the onshore one - which isnow approved for use offshore, as well as
onshore. Copies are available from HSEBooks.
To sum up, we believe that this revised ACoPwill allow duty holders much greater flexibilityto assess their own health care and first aidneeds. In future, you will tailor what isprovided to suit your individual offshorelocation, instead of a standard package whichis less fitted to the needs of that place. In otherwords - as a duty holder, you decide what youneed and you provide it. This revised ACoP isrelevant to everyone in promoting health careand well being offshore.
QUESTIONS AND ANSWERS SESSION
(NB – The following question and answer wastaken from FD’s notes as this session was notrecorded on tape.)
Question – Jake Malloy, OILC OffshoreUnionIs the ACOP enforceable? Particularly inrelation to medics’ alternative roles, such ascleaning duties.
Answer – Alan Morley, HSEThe guidance suggests that medics should notbe undertaking cleaning duties. It would bedifficult for an OIM to show that a medic whowas doing cleaning was immediately availablefor emergencies. Inspectors may challengesuch a situation.

227
WELLBEING AT WORK
Fiona Farmer, Regional Officer, MSF
The World Health Organisation defineshealth as “a state of complete physical,mental and social well-being and does notmerely consist of an absence of disease orinfirmity.”
MSF is running a campaign to demonstrate theimportance of well-being to the employee andthe employer.
Occupational health has improved in the pasttwo decades but still concentrates on thephysical issues where cause and effect areclearly demonstrated. The tackling of stress isstill seen by too many as a “difficult” area, letalone some of the “softer” areas such a well-being which incorporate social and familyfactors into the equation.
Workers well-being will be high if employersprovide a good response to the issues of:
Workplace hazardsDignity at workEqual opportunities
Family responsibilitiesWorking hoursEmployment securityMusculoskeletal DisordersControl of workOccupational health scheme
Really good occupational health as expressedby well-being, can only be effective if alldecisions in the organisation are subject to anOH audit. All decisions need to take accountof the potential impact on well-being. Well-being should be seen as an holistic approach tothe broadest interpretation of OccupationalHealth.
To be effective these issues have to beaddressed by a partnership between employersand employees, which has to be reflected at alllevels in the organisation. Thus occupationalhealth should not be seen as something whichis “done” to or for employees but something ofwhich they take joint control.

228

229
THE MEDICAL AND PHYSICAL FITNESS OF OFFSHOREEMERGENCY RESPONSE RESCUE TEAM MEMBERS
Dr Allan C Prentice, Aon Occupational Health
Abstract
Objective – To determine whether the selectionprocess for fire-team duties in the offshore oilindustry takes sufficient account of the medicaland physical status of the personnel selected.
Methods – The medical selection criteria forfire-fighters onshore were identified, with aliterature review to determine their basis, andthe relevance of the physiological performancetests to fire-fighting. These were contrastedwith the guidelines for offshore work. Aphysical fitness assessment, comparable to thatused for fire-fighters, was performed onoffshore fire-team members following thecompletion of a fitness questionnaire. Theiroccupational health records were thenreviewed to determine whether there were anyissues relevant to fire-fighting.
Main findings - 73 per cent of subjects in thestudy group (n = 48) had a satisfactory cardio-respiratory fitness for effective fire-fighting(VO2 max ≥ 45 ml/kg/min). A further 23 percent had an equivocal aerobic fitness (VO2
max ≥ 40 ml/kg/min, < 45 ml/kg/min). Only 4per cent found with poor cardio-respiratoryfitness for fire-fighting (VO2 max <40ml/kg/min).
75 per cent had sufficient lower body strength,when compared to the desired level (leg/backpull ≥ 139 kg). All but one had a leg/backpull score within the current guidelines forfire-fighting (≥ 117kg). All subjects hadsatisfactory upper body strength (grip strength≥ 35 kg) when compared to the fire-fightingstandard. All grip strengths were also abovethe desired level (≥ 40 kg). Two subjects fellout with the visual acuity standards for fire-fighting (6/60, N48 (uncorrected), 6/9-4, N12(corrected).
Conclusion – An additional assessment to thatrequired for offshore work is needed for fire-team members. This should include a detailedevaluation of musculo-skeletal and cardio-respiratory fitness. Recommendations for thisassessment have been made, which includesphysiological testing.
Introduction
My interest in the issue of medical andphysical fitness for fire-team duties in theoffshore environment commenced many yearsago following an enquiry from an employerwhen an employee had been refused entry ontoa fire-team course. The employee had assumedthat since the employee had already passed amedical assessment for offshore work that hewould be fit for this additional role. Further tothis I identified more cases where fitness forfire-team duties was an issue. These weremostly problems with the loco-motor system,respiratory problems, visual defects andcardio-respiratory fitness problems.
Fitness for fire-team duties can be regarded asa health and safety issue where it would beappropriate to assess an individual’s suitabilityrather than leaving the identification of anypotential problems to chance.
Fitness for fire-fighting onshore is governed bylegislative standards. The Fire Service(Appointments and Provisions) AmendmentRegulations 1988 and The Fire Service(Appointments and Provisions) Regulations1978. What are these standards and wouldthey be appropriate? The amendments werebased on the work of Scott (Scott, 1987) andare essentially physical fitness standards.
This research identified that a low physicalfitness capability existed in serving fire-fighters. Only 14 per cent were of normalweight, with 27 per cent mildly overweightand the remaining 59 per cent either obese orexcessively obese. In addition the fire-fightersas a group possessed only average aerobicfitness, with nearly 25 per cent having amaximum aerobic capacity (VO2 max) wherethey would be unduly fatigued whenundertaking some drills and calls (Brown etal, 1982; Lemon and Hermiston, 1977;Horowitz and Montgomery, 1993; Saupe et al,1991). Also reported was an increasingpercentage of low physiological test scores inolder groups indicating that fire-fighters werenot able to maintain their fitness as they aged.

230
Other studies in the UK and abroad haveidentified similar findings. This decline hasbeen reported, in part to be caused by theincreasing prevalence of medical conditionswith ageing. Lifestyle factors may alsocontribute to this change (Freil et al, 1988) andspecific fitness training programmes have beenrecommended together with health educationto mitigate against this effect. (Shephard,1991; Posner et al, 1986).
Fitness for fire-fighting
Cardiovascular FitnessSeveral studies have demonstrated thecardiovascular strain imposed by fire-fightingin the emergency situation (Barnard andDuncan, 1975; Sothman et al, 1992; Douglaset al, 1988). It is also recognised that thosefire-fighters, with lower cardiovascular fitness,performing at lower work rates, will takelonger to complete any physically strenuouswork tasks (Manning and Griggs, 1983;Sothman et al, 1990; Sothman et al, 1991).This can have serious implications to theindividual fire-fighter, his colleagues andothers, where the success of an operation canbe defined in terms of lives saved and in theminimisation of structural or property damage.
Emergency fire fighting is a strenuous physicalactivity where any cardiovascular strain causedby the tasks is compounded by the conditionsencountered. The effect of an increasedworkload caused by the weight of protectiveequipment and the use of positive pressuredemand self contained breathing apparatus(SCBA) is well documented (Lusa et al, 1993;Sköldström, 1987; Louhevarara et al,1995). Fire fighters have reported that workinvolving the use of SCBA and underconditions of extreme heat is particularlyfatiguing (Lusa et al, 1994) with up to a 25 percent increase in fatigue reported (Davis, 1982).When SCBA respiratory effort is increased dueto exhalation resistance from the valve,designed to maintain positive pressure withinthe facemask. The respiratory dead space isalso increased which has the effect ofincreasing alveolar carbon dioxide tensionthereby increasing ventilation rate at rest and atwork. However, in those with adequaterespiratory function this will not have anysignificant implications. Pulmonary factorswill not limit cardio-respiratory performanceunless there is significant pulmonary disease orthe exercise is being performed at altitude.
The high ambient temperature and humiditythat may be encountered on the fire-ground
will also affect the cardiovascular response toexercise. The normal thermo-regulatoryresponse is compromised, as sweat will not beable to evaporate. The increase in core bodytemperature, which cannot be dissipated, leadsto a further reduction in peripheral resistanceand to an increase in peripheral circulation.Venous return is reduced and with thisventricular filling. The reduced stroke volumeleads to a compensatory increase in heart rateto maintain cardiac output, thereby creatingmore cardiac strain. In extreme situationswhere cardiac output cannot be maintainedcollapse will occur.
In order to avoid fatigue in an individual,aerobic work lasting longer than one hourshould only be sustained at a level, which isapproximately equal to 50 per cent of theirVO2 max. A more intense work rate can besustained for a shorter period and work at 85per cent VO2 max can be performed forperiods of up to 10 minutes.
Employment discrimination law in NorthAmerica has focused attention on job specificfunctional fitness requirements, and with fire-fighting this has been determined followinganalysis of the energy costs of key tasks. Thishas then been used to determine a level ofaerobic capacity considered appropriate.Gledhill and Jamnik (1992) studied the mostdemanding fire-fighting operations. Ninetyper cent of these required a mean oxygenconsumption (VO2) of 23 ml/kg/min, but themost demanding tasks require a mean VO2 of41.5 ml/kg/min. Based on this a minimumstandard for fire-fighter applicants of 45ml/kg/min was recommended. Sothman et al(1991) measured oxygen consumption duringsimulated fire-fighting tasks and concludedthat a minimum VO2 max of 33.5 ml/kg/minwould be necessary. However, the tasksinvolved were representative of a walk up orlow rise fire and they then questioned whetherthis limit would provide sufficient reserve foreffective performance under situationsdemanding more strenuous physical work. AVO2 of 41 ml/kg/min was the level at which alltasks were completed correctly and in a laterstudy, it was concluded that aerobic capacityshould be maintained at a level of 42ml/kg/min or above (Douglas et al, 1988).This is the same figure that was recommendedby Davis et al in 1982 as the minimum, with49 ml/kg/min recommended to meet therequirements of the job, and to provide asufficient margin of safety.

231
In the UK the recommended minimum aerobiccapacity for fire-fighter recruits is 45ml/kg/min (Home Office, 1988). Thisrecommendation is based on Scott’s findingswhere the top 75 per cent of his subjects werefound to have an aerobic capacity equal to orabove this level. Guidance producedsubsequently recommended that for in servicefire-fighters age related criteria should be
applied, with the minimum acceptable aerobiccapacity reducing, as shown in Table 1, fromthe recruitment level to 37 ml/kg/min at age 65(Home Office, 1991). This position issomewhat controversial, since it is not possibleto match the demands of any particularemergency task to the age of the fire-fighter(Haisman, 1996).
Table 1 : Suggested minimum VO2 max values for serving fire-fighters
Nearest Age (years)
VO2 max.(ml/kg/min)
25 4530 4435 4340 4245 4150 4055 3960 3865 37
Muscular FitnessGood cardio-respiratory function is not theonly physiological parameter necessary foreffective fire-fighting. Reports from both fire-fighters and from job analysis studies haveidentified that certain key emergency tasksrequire a satisfactory level of muscular fitness(Lusa, 1993; Davis et al, 1982; Gledhill andJamnik, 1992). The relevance of muscularfitness and endurance has been recognised formany years and testing was prescribed underthe 1978 Fire Services’ (Appointments andPromotions) Regulations. However, thestrength test prescribed was somewhatempirical. A fire-fighter was expected to beable to carry a person weighing between 63.5 -76.2 kg (10 - 12 St) a distance of 91.4 km (100yd) in a time not exceeding 60 seconds. Thistest was recognised as being neither sensitivenor specific and did not test upper-bodystrength. The 1988 Regulations introduced theconcept of strength tests for different musclegroups with measurements of upper-body andlower-body strength, although it was noted thatseveral brigades had already introduced similartesting procedures prior to this. Theregulations specify that isometric strengthtesting should be performed. Handgrip shouldbe tested as a measure for upper-body strength(≥ 35 kg dominant hand, ≥ 33 kg subordinatehand) with leg/back strength as the measurefor the lower-body (≥ 117 kg).
The justification for such tests, is also based onthe work of Scott. He showed that muscularstrength, in contrast to the findingssurrounding aerobic capacity, was effectivelymaintained at a suitable level by the dailyduties required of a fire-fighter. Less than oneper cent assessed were found with insufficientstrength for the job. The JWPAP in its reportused these findings to recommend minimumstrength standards for fire-fighters (mean valueminus two standard deviations). Using thiscriterion, the standards for handgrip were ≥ 40kg dominant hand and ≥ 38 kg subordinatehand, with a leg/back pull strength of ≥ 139 kg.However, these figures were not included inthe regulations as concerns were raised thatthey may discriminate against women fire-fighters and applicants indirectly, due tonatural differences in physique. Toaccommodate for this, and to ensure that thereis reasonable account taken to avoid the chargeof sex discrimination, the standards were set atthe 50th centile of strength for women.
Respiratory FitnessThe current regulations specify that lungfunction should be tested using standardspirometric techniques with measures of theForced Expiratory Volume at one second(FEV1) and the Forced Vital Capacity (FVC)being prescribed. No specific limits are set,candidates being assessed on clinical grounds.Exposure to smoke and the products ofpyrolysis is a recognised occupational hazard

232
to fire-fighters and was particularly commonprior to the introduction of self-containedBreathing Apparatus (SCBA) as a routinemeasure. Acute reduction in respiratoryfunction is well documented (Musk et al, 1979;Sheppard et al, 1986; Brandt-Rauf et al, 1989;Sherman et al, 1989; Chia et al, 1990). Thechronic effect of smoke inhalation is less clear.Some have suggested an adverse effect(Guidotti and Clough, 1992; Moisan, 1991)whereas others have not (Douglas et al, 1985;Horsfield et al, 1988). Thus, the JWPAPrecommendation for respiratory function wasincluded as a specific health surveillancemeasure.
Anthropometric StandardsThe 1988 Regulations continued with therecommendation for a minimum height of 1.68m and introduced a maximum height limit of1.93 m. The minimum height requirement canbe traced back to the 1950 Fire Services’(Appointments and Promotions) Regulations,when a minimum height of 170 cm (5 ft 7 in)was stipulated. This was reduced to thecurrent limit in 1967 to enable fire authoritiesto recruit from a larger proportion of thepopulation than previously (David andHoffman, 1996). The recommendation for aminimum height requirement was initiallybased on the assumption of a good correlationbetween height and strength. Since fire-fighting is regarded as a team based activity, itwas argued that maximum efficiency could beachieved if all team members were of nearequal height. The need for a maximum heightlimit (1.93 m) followed, giving what wasconsidered to be a reasonable and workablespan (25 cm). It was also argued that for FireServices to accommodate for those who wereout with the specified range was impractical asthe redesign of any necessary equipment wasconsidered to be difficult due to technicalconstraints and, if possible, likely to beprohibitively expensive.
David and Hoffman did not consider thesearguments to be valid. Height was notconsidered to be a useful selection tool, asheight does not correlate well with strength.Also, any difficulties in team handling of loadscan usually be accommodated for with theappropriate positioning of those individuals ofunequal heights. It has also been possible todesign improved equipment storage systemson Fire Service vehicles. Therefore, theyconcluded that the retention of the heightlimits could not be justified.
Vision Standards
Visual AcuityThe visual requirements were recentlyreviewed by the Fireground Vision ResearchUnit (City University, 1995). Stringent visualacuity standards are specified on entry to full-time work 6/6, 6/6 (Scottish Office, 1996).This reflects an intention to ensure that a fire-fighter’s vision will remain satisfactorythroughout an operational career, anticipatingthe possibility of presbyopic or other changes.Subsequently, the in service standard is 6/9-4,N12 (corrected if necessary). Fromassessment many of the distance tasks a fire-fighter must perform equate to 6/9-4 and neartasks to N12. Notwithstanding this, theuncorrected visual acuity standards 6/60, N48must be met, the minimum identified foreffective safety performance should spectaclesbe lost. The in service standards also apply toretained fire-fighters, although the entrystandard is less strict (6/9, 6/9) and can berelaxed, where recruitment difficulties exist, tothe previous limit for serving fire-fighters(6/18, 6/24). Where visual correction isneeded the spectacles must be compatible withthe SCBA mask, as when ordinary spectacleshave been used a significant reduction incylinder discharge has been noted, implyingthat leakage must have occurred.
Colour VisionThe Fireground Vision Research Unit alsoreviewed the colour vision requirements.Failure to identify colour codes quickly andaccurately may be extremely hazardous duringa fire emergency. Commonly encounteredtasks include the recognition of safety signs,pipelines, gas cylinders (medical andindustrial), portable fire extinguishers and lineswhich may be used to power various pieces offire-fighting equipment. Historically, onlyindividuals with perfect colour vision wererecruited to the Fire Service, but the standardsnow permit those with a slight impairment ofgreen perception (deuteranomaloustrichromatism) to be considered fit for fire-fighting. It was shown that those with this as amild impairment do not compromise safety. Incontrast, those with defective reddiscrimination (protanomalous trichromatism)are a safety hazard. They are also unable todifferentiate numerous industrial gas cylinderssuch as propane and methyl chloride, argonand oxygen, and acetylene and oxygen. Theyare unable to distinguish colours used to codethe contents of pipelines, as are severedeuteranomalopes. Protanomalopes may also

233
confuse oxygen (black) and acetylene(maroon) cylinders.
Medical StandardsNo national medical standards for fire-fightingexist at present. A medical examination isrequired on entry and recommended three-yearly thereafter, but the Fire ServiceRegulations only state that the medicalexaminer must be satisfied that a candidate isable to perform fire-fighting duties. In itsreport, the JWPAP did comment on certainspecific medical conditions and made arecommendation that Fire Service MedicalAdvisers should establish a forum to meet andformulate common medical standards, policiesand practice. Comprehensive medicalguidelines are currently being prepared by theAssociation of Local Authority MedicalAdvisors (ALAMA), which should form thebasis of nationally recognised minimumstandards (Davies, 1997).
In making their recommendations for specificmedical conditions, the JWPAP obtainedguidance from the Faculty of OccupationalMedicine. Conditions such as insulin-dependant diabetes and epilepsy, where suddencollapse is a possibility, were considered to bea bar to fire-fighting. Other conditions notedby the JWPAP to require special considerationinclude disorders of the skin, musculo-skeletalsystem, cardiovascular disease and hearing.Back and knee conditions are a leading causeof disability reported in fire-fighters (Lusa etal, 1993). The cardiovascular strain imposedby fire-fighting has been discussed above. Nocomment was made specifically aboutrespiratory disease, although as mentionedabove lung function tests are recommended asa health surveillance measure.
Contrast Between the Offshore MedicalGuidelines and Standards for Fire-fighting
Fire-fighting offshore is performed as anadditional function to the employee’s maintask and the examination to determine fitnessfor offshore work does not assess fitness forfire-fighting specifically. The UKOOAmedical guidelines include comprehensiveguidance about the history and examinationfindings for each body system, indicatingwhich conditions would not be acceptable forwork in this environment. For the most partthe guidance is generic and not specific to anygroup or occupation, although appendices tothe document offer additional guidance whereparticular issues have been identified e.g.catering crew and crane operators. There is no
such additional guidance for fire-fighting atpresent. However, the guidelines do includegeneral guidance that a medical examiner, inthe assessment, needs to take account of thework environment, and that individuals arerequired to be physically fit for theiremployment. This includes the ability to reacteffectively to an emergency situation.Although individuals are required to bephysically fit no physical performance tests orstandards are recommended, except for lungfunction. A peak flow measurement isrecommended to be part of each initialassessment. Further spirometry is not essentialalthough the guidelines stipulate that, whereFVC is below 70 percent or FEV1 below 65per cent of predicted values, this wouldindicate a significant disability.
In contrast to the offshore guidelines the fire-fighting standards provide general guidanceabout the medical history and examinationfindings, The current standards are essentiallybased on the results from the physiologicaltests, with additional account being taken ofany medical conditions. This situation istherefore, almost the reverse to that requiredfor offshore work.
The UKOOA medical guidelines and theMedical Standards for fire-fighters arecontrasted in Table 2.

234
Table 2 : Contrast between Fire-fighting Standards and UKOOA Guidelines
Fire-fighting Standard UKOOA GuidelinesSystems Review General guidance only
(specific guidance beingdeveloped)
Specific guidance for each systemindicating what is acceptable /unacceptable
Height 1.68m to 1.93m None specified
Weight None specified None specified
BMI None specified > 35 kg/m2
generally unacceptable
Visual Acuity (distance) 6/9-4 (corrected),6/60 (uncorrected) when in service with higherstandards at recruitment
6/12 (corrected) in better eye.No uncorrected standardspecified currently
Visual Acuity (near) N12 (corrected),N48 (uncorrected)when in service with higherstandards at recruitment
None specified
Colour Vision Normal and mild greenimpairment acceptable
Should be adequate for particulartype of employment to beundertaken
Lung Function Spirometry required as a healthsurveillance measure.No set limits
Peak Flow recommended atinitial assessment. FVC < 70 %and FEV1 < 65% stated to beindicative of significant disabilitybut no requirement for testing
Aerobic Capacity Age related standard45 ml/kg/min specified forrecruits reducing to 37 ml/kg/min at age 65
No requirement to test
Grip Strength ≥ 35 kg (dominant),≥ 33 kg (subordinate)
No requirement to test
Leg/Back Strength ≥ 117 kg No requirement to test
The differences highlight the need to ensurethat a reasonable assessment is made todetermine the suitability of an offshore workerto undertake fire-fighting duties, withparticular reference to their vision and physicalfitness. However, whether this means thatthey need to meet the onshore fire-fightingstandard could be questioned, as this is asecondary function to their main occupation.This argument has also been used with part-time retained fire-fighters onshore, but hasbeen discounted. When in the fire-fightingsituation they face the same hazards and mustperform the same tasks as full-time fire-fighters, possibly at the same fire scene. Such
tasks are assessed as critical to safety andeffective performance, so the same medicaland fitness standards should apply. Thesituation offshore is comparable, where inaddition, the fire-team member may beexposed to some of the most extremeconditions that could be encountered in fire-fighting. These include high ambienttemperatures in humid conditions, fightingindustrial type fires in confined spaces, andwhere withdrawal from the fire scene may berestricted (Bennet et al, 1995). The structure ofan offshore installation also means that accessto the fire scene may involve a significant levelof exertion (O’Connell et al, 1986). Therefore,

235
it is entirely appropriate that such fitnessstandards or a similar equivalent should beapplied.
Offshore Emergency Response RescueTeam Medical And Physical Fitness Study
Objective and SettingThe objective of the study was to determinewhether the current selection process foroffshore emergency response rescue team(fire-team) duties takes sufficient account ofthe medical and physical status of thepersonnel selected. The study was based onthe workforce from an Operator with platformsin the North Sea. The fire-teams consist ofboth operator and contractor personnel.
MethodsFire-team members were identified fromcompany records and sent letters inviting themto participate in the study; there were 48positive replies from 115. Individuals wereasked to assess their own capability andproficiency using a modified Fitness ofFiremen questionnaire. The Fitness of Firemenquestionnaire had been developed to gaininformation from full time fire-fightersregarding their own perception of fitness(Goldsmith, 1995). The questions specific tofull-time fire-fighting and training activitieswere omitted and the lengthy section on sportand leisure activities condensed. Thequestionnaire was then slightly alteredfollowing a test with onshore safety personnelresponsible for emergency response.
After completing the questionnaire,physiological parameters were assessed. Thiswas done at work, in the installation healthcentres, by one of the offshore medics ormyself. Height and weight were measured andBody Mass Index (BMI) was calculated(weight/height2). Visual acuity was measuredusing Snellen Charts at 6 m for distance andreading cards at 30 cm. Colour vision wasassessed using the Ishihara method. Lungfunction was measured using standardspirometry measurements, FVC, FEV1 andFEV1%. The spirometry measurements weretaken using a Micro Medical microspirometercalibrated to read at body temperature andpressure saturated with water vapour (BTPS).
Volunteers then underwent tests of aerobiccapacity and isometric muscle strength.Maximum aerobic capacity (VO2 max) wasmeasured indirectly from a sub-maximalexercise step following the Chester Step Testprotocol at the 30 cm (12 inch) stepping
height. This height is recommended for thoseused to a moderate degree of vigorous exertionto ensure that the heart rate is elevated to 80percent of the age related maximum (Sykes,1995). The stepping rate was controlled from atape recorded metronome. Heart rate wasmonitored throughout the test using a Polarheart rate monitor. The Chester Step Test is amultistaged procedure, where the stagedincrease in work-rate is controlled through anincrementally increasing step rate. Each stagelasts for two minutes and heart rate ismeasured at the end. This is to ensure that asteady heart rate has been reached therebyincreasing prediction accuracy. The subject’sresults were plotted on the set chart fromwhich the predicted maximum aerobic capacity(VO2 max) was then read.
Isometric muscle strength was assessed usingmeasurements of grip and leg/back strengthtaken with digital dynamometers (TakeiScientific Instruments). Grip strength wasmeasured after adjusting the grip for thesubject’s size. The average of 4 measurementswas taken from alternating tests on left andright hands. The manufacturer’s guidelineswere followed with subjects standing uprightwith arms extending downwards. Then, whileholding the dynamometer, they were requestedto exert full force without touching their body.A modified procedure was used for assessingleg/back strength because of the potential forinducing injury when following themanufacturer’s guidelines. The handleattachment was adjusted for the patient’sheight and with the knees bent at 130°-140°and back straight the subject was requested topull upwards using maximum force whilebreathing out.
Occupational health records were reviewed,where these were obtainable, to determinewhether there was any significant conditiondocumented liable to affect fitness for fire-fighting. Particular emphasis was placed onany cardio-respiratory or musculo-skeletalproblems because of the perceived increaseddemands on such systems, which would beemployed in fire-fighting duties in contrast togeneral offshore work.
Statistical AnalysisThe records were collated on computer usingthe Microsoft Access database and analysedusing the Excel spreadsheet and AnalysisToolpak. Where relevant, parameters werecompared to the statutory fire-fightingstandard. This included the visualrequirements, aerobic capacity and musculo-

236
skeletal measurements. Correlation analysiswas then performed on the anthropometricdata, lung function and physical fitness tests.Aerobic capacity and musculo-skeletalstrength were grouped according to the fire-fighting standard, and in the case of theleg/back strength, also to the standardsoriginally recommended by the JWPAP.
Before analysis the ordered data obtained fromthe Fitness for Firemen questionnaire was
allocated a numerical equivalent, as outlinedbelow in Table 3.
Smoking was categorised dependant uponwhether the subject was a cigarette smoker (4),pipe/cigar smoker (3), ex-smoker (2), or non-smoker (1). Alcohol intake was converted intoequivalent dosage in units/week using thestandard conversion formula (glasswine/measure of spirit/half-pint beer = 1 unit).
Table 3: Numerical allocation of data from activity assessment
Numerical EquivalentFitness Rating None 0 Extremely Low 1 Much Below Average 2 Slightly Below Average 3 Average 4 Slightly Above Average 5 Much Above Average 6 Extremely High 7
Frequency of Physical Activity None 0 Monthly 1 Weekly 2 Daily 3
Description of Activity None 0 Primarily Anaerobic 1 Mixed 2 Primarily Aerobic 3
Level of Physical Exertion Very Light 1 Light 2 Fairly Light 3 Moderate 4 Fairly Hard 5 Hard 6 Very Hard 7
The data was analysed by non-parametric techniques using Spearman’s coefficient for correlation andthe Mann Whitney test for inter-group analysis.

237
Results
Descriptive StatisticsTable 4 summarises the descriptive statistics for the study group.
Table 4: Summary of study group
Mean (SD) Median
(Inter-quartileRange)
Minimum Maximum
Age (years) 41.7 (7.46) 41 (33.5 to 50) 24 53Height (cm) 177.5 (5.78) 176.5 (173 to 182.5) 168 188Weight (kg) 81.5 (11.26) 80.5 (73 to 89.5) 60 108BMI (kg/m2) 25.7 (2.60) 25.9 (23.6 to 27.2) 21 33
Lung Function FEV1 (litres) 4.0 (0.54) 3.9 (3.6 to 4.2) 3.1 5.3 FVC (litres) 4.7 (0.65) 4.6 (4.3 to 5.2) 3.7 6.3 FEV1 % 84.7 (4.74) 84.9 (82.2 to 87) 71.9 93.8
VO2 max(ml/kg/min)
49.3 (7.25) 49 (44 to 52) 39 69
Leg/Back Strength(kg)
163.8 (37.53) 155 (139.5 to 171.5) 110 301
Grip Strength (kg) 50.6 (5.87) 48.9 (46.2 to 55.2) 42 68.7
Three individuals had FVC values below thenormal reference range when adjusted for ageand height (European Respiratory Journal,1993. One of these included an FEV1 out withthe equivalent reference range. All FEV1 %values were normal. Sykes has produced age
related reference scores for predicted aerobiccapacity values when using the Chester StepTest. Thirty-eight percent had a good agerelated fitness rating with the remaining 63percent being in the excellent range.

238
Questionnaire Returns
Tables 5 to 9 summarise the results from the questionnaire survey.
Table 5: Fitness self assessment
Muscular Strength Stamina General FitnessFitness Rating N % n % n %
Extremely Low 0 0 0 0 0 0Much Below Average 0 0 1 2 1 2Slightly BelowAverage
3 6 4 8 4 8
Average 25 52 19 40 21 44Slightly AboveAverage
12 25 11 22 7 15
Much Above Average 7 15 13 27 15 31Extremely High 1 2 0 0 0 0
Regular Duties Fire-team Dutiesn % n %
Not fit Enough 0 0 0 0Fit Enough 32 67 31 65Fitter than Necessary 16 32 17 35
Table 6: Weight and diet
Predicted Measuredn % n %
BMI (kg/m2) < 19 0 0 0 0 19-24.9 14 29 19 40 25-29.9 30 63 26 54 30-39.9 3 6 3 6 ≥ 40 1 2 0 0
Self Assessment of weight Underweight 1 2 Normal 27 56 Slightly Overweight 7 15 Overweight 13 27
Special Effort to Diet Whole Group 12 25 Assessed Wt Normal(n=27)
5 19
Assessed Overweight(n=20)
7 35
Improvement with weightloss Overweight group (n=20) 7 35

239
Table 7: Physical activity
n %ExerciseFrequency None 7 15 Monthly 8 17 Weekly 30 63 Daily 3 6
Exercise Type None 7 15 Anaerobic 0 0 Mixed 16 33 Aerobic 25 52
Exercise Intensity None 7 15 Very Light 0 0 Light 1 2 Fairly Light 2 4 Moderate 14 29 Fairly Hard 14 29 Hard 9 19 Very Hard 1 2
Table 8: Smoking and alcohol
n %Smoking Habits Never smoked 27 56 Ex-smoker 12 25 Pipe/cigar smoker 2 4 Cigarette smoker 7 15
Alcohol(units/week) 0-21 25 52 22-34 12 25 >34 11 13
Table 9: Injuries and illnesses
N %Days Off in Past Year None 36 75 1-14 days 10 21 >14days 2 4
Injury Restricting Activity 3 6
Injury Due to Lack offitness
0 0
240
Fitness Self AssessmentIn general, most subjects believed that theywere of average or above average physicalfitness levels. All felt that they were fitenough to perform both their regular work andfire team duties.
Weight and DietFifty-six per cent thought they were in thenormal weight range with 42 per centbelieving they were either slightly overweightor overweight. However, when asked toestimate their height and weight, 29 per centwere in the desired range for weight, 63 percent were overweight and 6 per cent obese.One individual’s estimate gave him a bodymass index ≥ 40. This individual was notoverweight and there may have been someconfusion between imperial and metric values.The measured BMI showed slightly morewithin the normal range (40 per cent) andcorrespondingly less in the overweight range(54 per cent).
Twenty-five per cent of the study group as awhole claimed that they made a special effortto diet, split fairly evenly between those whoconsidered that their weight was normal andthe overweight group. Although they all feltthat they were fit enough to do the job, 35 percent in the overweight group felt that theycould do the job better if they weighed less.This compares with 19 per cent in the normalweight group a difference which is notstatistically significant (P > 0.05, Chi squaredtest).
Physical ActivityThe majority undertook some form of physicalactivity during their leisure time, more thantwo-thirds doing this on a weekly basis, ormore frequently. This was usually at amoderate, hard or fairly hard intensity. Themost popular forms of exercise mentionedwere cycling, golf, walking or hill-walking,swimming and gym workouts (cardiovascular
or circuit training). Jogging or running, weighttraining, racquet and winter sports werementioned less frequently. Those who did notexercise reported that this was either becausethey were not interested or due to lack of time.
Smoking and AlcoholSmoking was not a common activity with lessthan 20 per cent of the study group beingcurrent smokers and with over 50 percentnever having smoked. Estimated alcoholconsumption showed that over half drankwithin the recommended safe limit (≤21units/week) but 23 per cent had an estimatedalcohol consumption in the hazardous range (≥35 units/week).
Injuries and IllnessesMost reported no time off through injury orillness. One subject reported 35 days offfollowing a knee arthroscopy, and one 40 daysoff with septicaemia. One had undergonecataract surgery and required 10 days off. Therest with less than 14 days absence declaredcold or flu symptoms, or musculoskeletalcomplaints. Two of those withmusculoskeletal complaints stated that itrestricted their activities. One had a backstrain requiring 10 days off and the other 4days absence due to a neck complaint.Another subject declared a shoulder muscleinjury restricting his activities but had notrequired any time off. No one reported aninjury due to lack of fitness
Correlation AnalysisTables 10, 11 and 12 show the Spearman’sranked correlation coefficients (rs) for age andanthropometry measurements, lung functiontests and the physical fitness tests against othervariables. For sample size n = 48, if rs ≥ 0.285then P < 0.05).

241
Table 10: Correlation matrix for age and anthropometry
Age MeasuredHeight Weight BMI
Age 0.137 0.128 0.084
Self Assessed Height 0.09 0.823 0.742 0.482 Weight 0.095 0.507 0.775 0.725 BMI 0.067 0.189 0.619 0.73
Fitness Rating Stamina -0.006 -0.064 -0.174 -0.19 MuscularStrength
0.266 -0.03 0.135 0.197
General Fitness 0.085 -0.145 -0.25 -0.235
Alcohol Intake 0.013 -0.015 -0.012 -0.007
Smoking Score -0.179 -0.347 -0.193 -0.01
Exercise Type 0.206 0.1 0.025 -0.007 Amount 0.228 0.314 0.279 0.192 Level 0.144 0.121 0.017 -0.043
Table 11 : Correlation matrix for lung function
FEV1 FVC FEV1%
Age -0.22 -0.133 -0.213Measured Height 0.596 0.702 -0.268 Weight 0.394 0.451 -0.095 BMI 0.122 0.139 0.036
Alcohol Intake -0.11 -0.076 -0.123
Smoking Score -0.08 -0.152 0.217
Fitness Rating Stamina 0.117 0.063 0.154 MuscularStrength
0.006 0.041 -0.073
General Fitness 0.042 0.075 -0.071
Exercise Type 0.091 0.102 -0.078 Amount 0.288 0.268 0.112 Level 0.11 0.165 -0.149

242
Table 12: Correlation matrix for physical fitness
AerobicCapacity
Leg/backStrength
GripStrength
Age -0.348 0.101 0.041Measured Height 0.057 0.318 0.225 Weight -0.158 0.428 0.425 BMI -0.243 0.39 0.401
Lung Function FEV1 0.385 0.249 0.355 FVC 0.343 0.266 0.346 FEV1% 0.05 0.002 0.006
Alcohol Intake -0.224 -0.385 -0.068
Smoking Status 0.067 0.041 0.146
Leg/Back Strength 0.064
Grip Strength 0.027 0.26
Fitness Rating Muscular Strength -0.119 0.308 0.174 Stamina 0.301 0.238 -0.086 General Fitness 0.269 0.114 -0.084
Exercise Amount -0.061 0.269 0.025 Type -0.032 0.103 0.064 Level 0.061 0.093 -0.001
Spearman’s correlation coefficientLevels of significance (α2) (n=48)
rs ≥ 0.285, P < 0.05rs ≥ 0.336, P < 0.02rs ≥ 0.370, P < 0.01rs ≥ 0.401, P < 0.005rs ≥ 0.439, P < 0.002rs ≥ 0.465, P < 0.001
AnthropometryA good correlation was noted betweenpredicted and measured values for height andweight and consequently BMI. A significantpositive correlation was also noted betweenheight and exercise amount and a significantnegative correlation between height andsmoking score. There was also a significantnegative correlation between height andsmoking score.
Lung FunctionAs would have been expected, a significantcorrelation was noted between height and bothFEV1 and FVC. Weight, which is related toheight also, showed a significant correlation.Another finding of note was the correlationbetween exercise amount and FEV1. Thecorrelation between exercise amount and FVCdid not reach significance, although exerciseamount and height did.
Physical Fitness TestsAerobic capacity showed a significant positivecorrelation with FEV1, FVC and stamina withstamina, from the questionnaire survey. Anegative correlation was noted betweenaerobic capacity and age. A negativecorrelation was also noted between aerobiccapacity and both alcohol intake and BMI,although these did not reach significance.Similarly, a negative correlation was noted

243
between leg/back strength and alcohol intake,which was significant. A significant positivecorrelation was found between leg/backstrength and BMI and between leg/backstrength and muscular strength, from thequestionnaire survey. This is in contrast to thefindings when grip strength was compared to
muscular strength. Grip strength did correlatewith BMI and FEV1 and FVC. There was nosignificant correlation between leg/backstrength or grip strength and age.
Comparison with Onshore Fire-fighting Standards
Table 13 lists the number of subjects who did not meet the equivalent onshore fire-fighting standard forvision and fitness tests.
Table 13: Subjects who fell below the onshore fire-fighting standards
n %Vision Acuity < 6/60, or < N48 2 4 Colour defect 1 2
Aerobic Capacity < 45 ml/kg/min 13 27 < Age Allowance 4 8
Back Strength < 117 kg 1 2 < 139 kg 12 25
Grip Strength < 35 kg 0 0
VisionThe visual standards for acuity refer to the inservice requirements for part-time fire-fighters.Two subjects were found to be out with thestandards. One fell below the uncorrectedstandard, although his corrected visual acuitywas satisfactory. The second subject presentedwearing contact lenses. His corrected visualacuity was normal, but the prescriptionstrength, which he quoted, was out with thestandard.
If the recruitment visual acuity standard (6/9,6/9) were applied, a further 10 would be outwith the requirements, although one of thesewould pass the relaxed standard (6/18, 6/24).
Only one subject was found to be colour blindon Ishihara plate testing, a deuteranomalousdefect. The severity of the defect was notknown, although the subject had volunteeredthat it was severe.
Physical FitnessThe majority met the aerobic capacityguidelines, although a substantial minority (27per cent) fell below 45 ml/kg/min. Thenumber below the standard was reduced to 8
per cent when the age related adjustment wasapplied. The error of the test method (10 percent) means that those between 40 and 44ml/kg/min from this indirect test method maywell have an aerobic capacity of 45 ml/kg/minor greater were direct testing to be employed.25 per cent did not meet the originallyrecommended leg/back strength limit (≥ 139kg), but only one candidate failed to reach thecurrent standard (≥ 117 kg). All grip strengthsmeasured were satisfactory (≥ 35 kg) indeedall met the originally recommended standard(≥ 40kg).
AnthropometryNo one in the study group fell out with theheight limits for fire-fighting.
Inter-Group AnalysisTable 14 compares those who met therecommended aerobic capacity standard (≥ 45ml/kg/min) with those who did not. For samplesizes n1 = 13 and n2 = 35 using the two tailedtest, a U value of 313 or greater is consideredsignificant (P < 0.05).
Table 15 compares those who met theoriginally recommended leg/back strength

244
standard ( ≥ 139 kg) with those who did not.Where n1 = 12 and n2 = 36, a U value of 299 or
greater is considered significant (P < 0.05).
Table 14: Comparison between subjects with a VO2 max << 45 ml/kg/min to those with a VO2 max ≥≥ 45 ml/kg/min
Group A (n =13) Group B (n = 35)Aerobic Capacity < 45 ml/kg/min Aerobic Capacity ≥≥ 45 ml/kg/min
Median (Inter-quartileRange)
U value Median (Inter-quartileRange)
Uvalue
Age 46.5 (40 to 49) 309.5 40 (35 to 47) 145.5Height 178.1 (175.2 to 183) 264.5 176 (173 to 182) 190.5Weight 87 (80 to 94) 320.5 79 (71.3 to 85) 134.5BMI 26.7 (26.1 to 28.5) 328.5 25.4 (23.3 to 27.2) 126.5
Alcohol Intake 30 (10 to 43) 260.5 20 (14 to 31.5) 194.5
Leg/BackStrength
153.5 (135 to 170.5) 198 156 (143.5 to170.4)
257
Grip Strength 52.2 (46.6 to 56.5) 271 48.7 (46 to 52.4) 184Lung Function FEV1 3.8 (3.6 to 4) 193.5 4 (3.7 to 4.3 ) 261.5 FVC 4.6 (4.3 to 4.8) 204 4.7 (4.1 to 5.2) 251 FEV1% 84.8 (82.9 to 86.5 233 85.2 (82.1 to 86.9) 222
Smoking Status 1 (1 to 2) 214.5 1 (1 to 2) 240.5
Fitness Rating Muscular 5 (4 to 5) 261 4 (4 to 5) 194 Stamina 4.5 (4 to 5) 181 5 (4 to 6) 274 GeneralFitness
4 (4 to 5) 181.5 4.5 (4 to 6) 273.5
Exercise Type 3 (2 to 3) 242.5 3 (2 to 3) 212.5 Amount 2 (2 to 2) 299.5 2 (1 to 2) 155.5 Level 5 (4 to 5) 252.5 4.5 (4 to 5) 202.5
U ≥ 313, P < 0.05U ≥ 328, P < 0.02

245
Table 15: Comparison between subjects with a leg/back strength < 139 kg to those with a leg/back strength ≥≥ 139kg
Group C (n =12) Group D (n =36)Leg/Back Strength < 139 kg Leg/Back Strength ≥≥ 139 kg
Median (Inter-quartileRange)
U value Median (Inter-quartileRange)
Uvalue
Age 39.5 (32.5 to 45.5) 170 42 (39 to 48.5) 262Height 173 (172.7 to
178.1)142.5 178 (173 to 183.5) 289.5
Weight 80 (69.5 to 82.3) 142 82.8 (75 to 92) 290BMI 25 (23.1 to 26.7) 167.5 26.3 (24.2 to 27.5) 264.5
Alcohol Intake 36 (22.5 to 47) 302 19 (11.5 to 26) 130
AerobicCapacity
44.5 (42 to 51.5) 156.5 50 (45 to 52) 275
Grip Strength 48.2 (45.9 to 49.1) 145.5 50.5 (46.2 to 56.3) 286.5
Lung Function FEV1 3.8 (3.5 to 3.9) 140.5 4.0 (3.7 to 4.5) 291.5 FVC 4.4 (4.1 to 4.7) 149.5 4.7 (4.4 to 5.1) 282.5 FEV1% 84.7 (82.5 to 86.7) 206 85.1 (82.1 to 87.6) 226
SmokingStatus
1 (1 to 2) 213.5 1 (1 to 2) 218.3
Fitness Rating Muscular 4 (4 to 4) 140 5 (4 to 5) 292 Stamina 4 (3.5 to 5) 154.5 5 (4 to 6) 277.5 GeneralFitness
4 (4 to 5) 181 4 (4 to 6) 251
Exercise Type 2 (0 to 3) 144 3 (2 to 3) 288 Amount 1.5 (0 to 2) 137 2 (2 to 2) 295 Level 4 (0 to 5.5) 186.5 5 (4 to 5) 245.5
U ≥ 299, P < 0.05
Aerobic CapacityThose who did not meet the standard,≥ 45 ml/kg/min, were significantlyheavier than those who did. They alsotended to be older, although thisdifference did not reach significance.
Leg/Back StrengthA significant difference was noted in alcoholintake between the two groups. Those who didnot meet the recommended level (≥ 139 kg)drank more than those who did. Otherdifferences were noted, those with a leg/back
strength ≥ 139 kg were taller and heavier, hada stronger grip strength and larger FEV1. Theyalso undertook more exercise and from thequestionnaire had declared greater muscularstrength. These differences did not reachsignificance, which may be due to the smallsample size, as the U values for weight, FEV1,muscular strength and exercise amount fell justbelow the level of significance.
Review of Occupational Health Records
The review of medical records was restrictedto those members of the study team who were

246
employees of the Operator. Their occupationalhealth records are held at Liberty OccupationalHealth and consist principally of pre-employment and periodic medicalexaminations. This accounted for 28 (58 percent) of the total study group. The reviewconcentrated on current or recent problems(those within the previous 5 years).
Ten subjects were found who had recognisedmusculoskeletal disorders, 5 back problems, 3knee problems, one ankle injury and a shouldercondition. Two of those declaring kneeproblems had undergone arthroscopy in thepast 2 years. No respiratory disorders orcardiovascular disorders were noted, althoughone individual had undergone investigation foran ECG abnormality, finally identified as afalse positive test for ischaemia. One case ofvestibular disorder was reported and onesubject had recently undergone cataractsurgery.
Discussion
Certain limitations to the study should berecognised. The sample size was relativelysmall with recruitment being voluntary. Also,those who volunteered may have beeninfluenced through knowledge of theparameters being tested, with those who didnot consider themselves fit declining tovolunteer. However, the median age of thestudy group, 41 (33.5 to 50) comparesfavourably with the median age of the fire-team as a whole, 42 (37 to 47) and can beconsidered representative from this aspect. Italso compares favourably with the platforms’offshore workforce, 40 (33 to 46).
Limitations in the study method, in particular,the predicted accuracy of the indirectassessment of aerobic capacity and theaccuracy of the dynamometry measurements,as mentioned above, also have to berecognised. However, despite its limitations,there are several points worthy of note fromthe study, which are discussed below.
Aerobic FitnessThe aerobic fitness and muscular fitnessmeasured of the fire-team members wasgenerally satisfactory. Even those who did notmeet the equivalent onshore fire-fighteraerobic fitness standard were generally above40 ml/kg/min, equivalent to 10 per cent belowthe standard. This figure cannot be consideredto be significantly different from 45 ml/kg/minwhen the error in the test method isconsidered. Only 2 results were below 40
ml/kg/min. Likewise, only 4 subjects fellbelow the aerobic capacity standard when theage related allowance was applied. None ofthese were out with 10 per cent of thatstandard. However, the application of the age-related standard is controversial, as thephysical demands of fire-fighting cannot betailored to suit the age of fire-fightersattending an incident Gledhill and Jamnik,1992; de Vries, 1982.
AgeIn general, aerobic capacity is recognised todecrease with age (Freil, 1988; Ilmarinen,1991) and demonstrated in this study with thenegative correlation. This reduction isprimarily thought to be due to the diminishedefficiency of both the circulatory system todeliver oxygen to the tissues and for thisoxygen to be utilised by the tissues (de Vries,1982). There is considerable inter-individualvariation in this effect as well trained oldermen have been shown to be able to maintaintheir aerobic fitness at high levels. Thenegative correlation noted between aerobiccapacity and age did not reach significance.This may, of course, have been due to thesmall sample size as an age related decrease inaerobic fitness has been a concern expressedby a number of previous studies involving fire-fighters (Scott, 1987; Saupe et al, 1991;Kilbom, 1980; Freil et al, 1988). It could alsobe that the physical characteristics of offshoreinstallations impose certain physical attributeswithin the workforce. The structure of anoffshore installation means that any workerinvolved in plant maintenance or productioncan spend a considerable time ascending thenumerous stairs on the installation. Suchincidental work effort may go some way toexplaining the findings from this study.Thirdly, the voluntary nature of participationin the study may have encouraged only fit fire-team members to present themselves.
Age limits for operational fire-fighting dutiesare applied in the UK and other countries. TheUK limit is 55 years, although this does notextend to retained fire-fighters. In NorthAmerica employment discrimination lawagainst ageing provoked a lot of interest anddebate on the subject, and whether fire-fighting could be a bona fide occupationalqualification necessitating exception from thisruling. It was considered that it could not,hence the rationale behind the currentoccupational related standards, which havebeen recommended.
247
Fitness for employment and age is importantgenerally due to the changing demographiccharacteristics of the workforce (Posner et al,1986; Lancet, 1993). Advancing age is not amatter, which can be dismissed, and this isparticularly relevant to the offshore oilindustry as it matures along with theworkforce. The economics of the business andadvances in technology means that theproduction plant and support functions operatewith fewer personnel than that which wascommonly found during the industry’sinception in this country 15 - 20 years ago.The surviving workforce has been bolstered bynew, younger recruits, where necessary, butoverall the workforce is ageing and with thisgeneral medical and physical fitness willreduce. There is no longer a large additionalpool of personnel which can be drawn from sowhere there are employment fitness concernsfor additional duties such as fire-fighting thesolution to such problems has to be obtainedfrom the resources available. This mayinclude additional incentives for fire-teammembers to maintain fitness throughadvancing age, with a greater emphasis inselecting those with the appropriate physicalattributes for such duties, and traininginitiatives to ensure that those selected for suchduties do retain sufficient capacity (Brown etal, 1982). Increasing age and decreasing fitnessneed not necessarily coincide. Chronologicalage can be a relatively poor indicator of bothmedical and physical fitness in an individual.It has been noted that the best preserved 65year old worker has a greater functionalcapacity than a poorly endowed person of 25 -30 years of age (Shephard, 1995) and beenargued that those who chose a healthy lifestyleshould not be punished for the sins of thosewho do not (Sharkey, 1986).
ObesityIn addition to age, other characteristics whichmay determine aerobic capacity includegenetic endowment and factors which may beinfluenced by lifestyle such as the degree ofphysical training and relative body weight.This study showed that those in the loweraerobic capacity group were heavier and had ahigher BMI, this difference being significant.
Obesity, with its increasing prevalence, isrecognised as a major public health issue(Ashwell, 1994; Björntorp, 1997) and in fire-fighting is noted to limit performance. It hasbeen argued that obesity has a moredeleterious effect than age when assessingaerobic capacity (Schonfeld, 1990). Thisemphasises the need for both full and part time
fire-fighters to be aware of the need tomaintain fitness including body weight. Thiswas demonstrated in the study where nocorrelation between age and BMI shown wasshown. This is in contrast to reportsconcerning onshore fire-fighters weight andBMI has been noted to increase with age(Scott, 1987; Brown et al, 1982; Lemon andHermiston, 1977). The conditions and climateon offshore production facilities are muchdifferent from those which were described byLight and Gibson when they recorded anincreasing prevalence of obesity with ageing(Light and Gibson, 1986). The environment isnow more conducive to encourage effectivemaintenance of body weight.
Muscular StrengthUnlike aerobic capacity, musculoskeletalstrength test results did not decrease with agein this study, another physiological feature thathas been demonstrated with onshore fire-fighters. The same has been noted with otheroccupations, which require physical effort(Nygård, 1991). Those who were heavier andhad a higher BMI scored better in the strengthtests. There was also a strong correlationbetween exercise amount and weight. Anincreased muscle mass, in these individuals,may account for some of this difference.
Self Assessment of FitnessThe significant positive correlation foundbetween both stamina and aerobic capacity,and muscular strength and leg/back strengthsuggests that individuals already had a goodimpression of their own level of fitness. Asimilar finding has been noted in the past withboth onshore fire-fighters (Ellam, 1994) andothers (Leon et al, 1981) where it has beenconcluded that substantial prediction ofphysical fitness and work capacity can beobtained relatively easily through suchtechniques.
Lifestyle FactorsThe low leg/back strength group hadsignificantly higher alcohol consumption. Thiscould be taken as an indicator of lifestyledifferences. Exercise profile did not show anysignificant difference, although in generalthose in the high leg/back strength group didtend to exercise more than those in the lowstrength group. This difference was just belowthe level of significance and again possibly ina larger study group with greater statisticalpower the difference may have beensignificant.

248
No difference in smoking status between thehigh and low aerobic capacity group wasnoted. This may have been due to therelatively small number of smokers in thegroup, or the effect of other variables.Tobacco smoke is known to contain up to 4per cent by volume of carbon monoxide and alevel of carboxyhaemoglobin greater than 5per cent (reached from inhalation more than 10- 12 cigarettes per day) has been noted toreduce aerobic capacity and performance(Horvath, 1975).
VisionThe revised visual standards for fire-fighterstake due account of the functional needs of thetask. The main difference from the previousstandard is that allowance for visual correctioncan now be given. Two subjects fell out withthe uncorrected standard, although both hadsatisfactory corrected vision. One worecontact lenses, not the recommended methodof choice for emergency fire-fighting.However, studies have shown that contact lenswearers can perform fire-fighting tasksadequately (City University, 1995). This isparticularly true for soft contact lens wearerswhich can be worn for prolonged periods.Such visual correction should be consideredcompatible with fire-team duties offshore. Anumber in the study group use spectacles, andfor those in this category it is essential thatthese are compatible with SCBA. This hascreated logistical difficulties and added costsas the fire-team may muster at a variety ofdifferent locations, dependant on thecircumstances. Therefore, there is a need toensure that each muster station has a sufficientstock of the appropriate respiratory protectionfor those fire-team members who require touse spectacle inserts.
The fire-fighting visual standards make nospecific reference to cataract surgery.However, the improvement in visual acuitywhich can be obtained from cataract surgerycannot be dismissed. It should be consideredbest practice offshore, where the recruitmentpool is limited, to assess each such case andcontinuing fitness on an individual basis.
Review of Occupational Health RecordsThe figures from the occupational healthreview were too small for useful comparativeanalysis, but do show the need to concentrateon medical fitness for fire-fightingindependently from fitness for any otherfunction. Even in this small sample a numberof medical conditions that may impact onsuitability were found. Although the medical
specifications for offshore work and guidelinesfor fire-fighting are similar, fire-fighting doesimpose specific demands above that requiredfor offshore work in general. Closer review ofthose required to perform such duties offshoreis therefore warranted. I have been involved inseveral such cases, mostly surroundingmusculoskeletal problems, but also othersincluding a case of respiratory airwaysdysfunction syndrome (RADS). Individualsmay present when they are experiencingdifficulties, but this would not necessarilyalways be the case. Therefore, a more formalsystem of medical assessment for fire-teamduties is required. Such a system shouldinclude a physical fitness assessment similar tothat required for onshore fire-fighters.
Other Studies Relating to Fitness OffshoreLittle work has been published on the physicalfitness of offshore personnel in general. Corpestudied oil industry workers based bothonshore and offshore. Using the Harvard StepTest she reported a mean VO2 max of 44.4ml/kg/min (Corpe, 1991). This ranged from 54ml/kg/min in the 15 - 19 age group, down to38.5 ml/kg/min in the 50 - 59 age group. In astudy of North Sea divers Thompson et al(1984) reported a maximum aerobic capacityof 46 ml/kg/min and questioned whether thiswould give them sufficient cardio-respiratoryreserve. Cotes and Reed reported comparablefindings who suggested that as diving involvedmany sedentary and static tasks, this would notpromote cardiovascular fitness. They alsosuggested that the greater experience of oldermen may offset their lower aerobic capacity(Cotes and Reed, 1984). This may well be true,but has limited relevance in emergencysituations where speed of action is necessary.Fast rescue craft crew operating within theoffshore oil industry are also required toperform tasks which impose severe physicaldemands, with the task of casualty recoverynoted to be particularly strenuous. In additionto meeting the medical standards specifiedunder the Merchant Shipping Regulationsadditional physical fitness standards have beenrecommended (David et al, 1985). Theseconcentrate on muscular strength rather thancardiovascular fitness parameters.
Conclusion and Recommendations
The current selection method for choosingemergency response rescue team (fire-team)members on an offshore installation does notspecifically take account for the medical andphysical demands, which are imposed, fromthis additional duty. However, the majority in
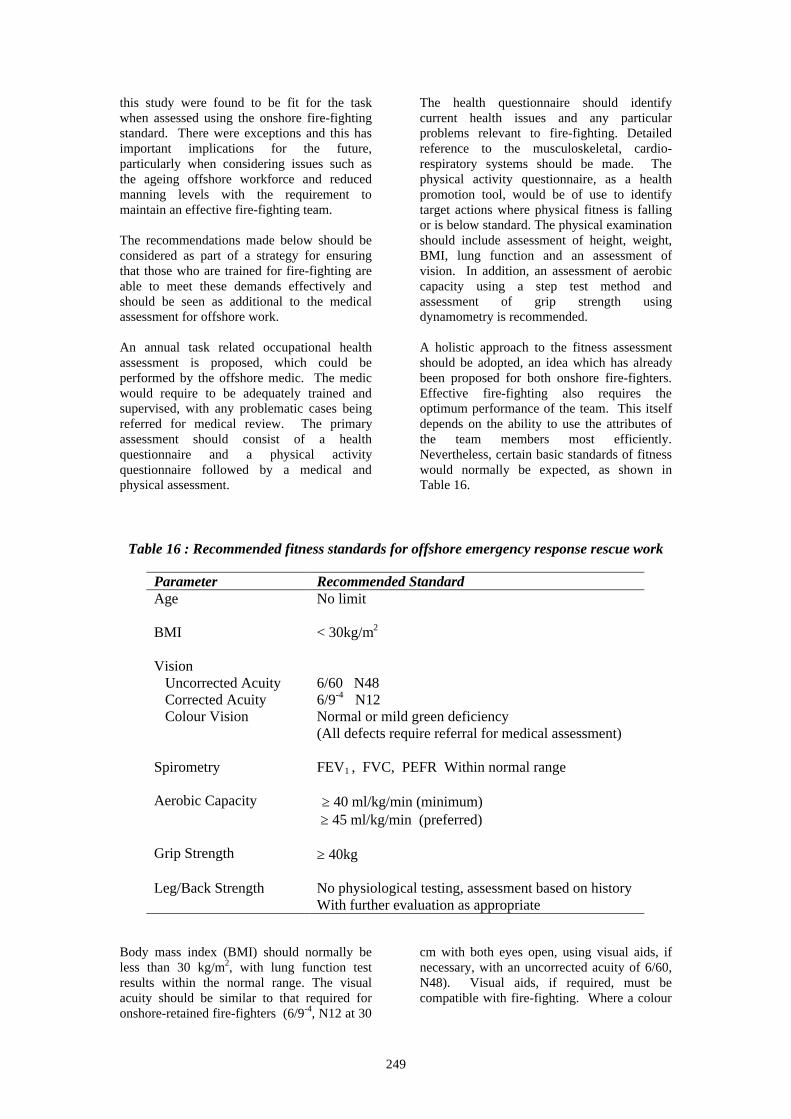
249
this study were found to be fit for the taskwhen assessed using the onshore fire-fightingstandard. There were exceptions and this hasimportant implications for the future,particularly when considering issues such asthe ageing offshore workforce and reducedmanning levels with the requirement tomaintain an effective fire-fighting team.
The recommendations made below should beconsidered as part of a strategy for ensuringthat those who are trained for fire-fighting areable to meet these demands effectively andshould be seen as additional to the medicalassessment for offshore work.
An annual task related occupational healthassessment is proposed, which could beperformed by the offshore medic. The medicwould require to be adequately trained andsupervised, with any problematic cases beingreferred for medical review. The primaryassessment should consist of a healthquestionnaire and a physical activityquestionnaire followed by a medical andphysical assessment.
The health questionnaire should identifycurrent health issues and any particularproblems relevant to fire-fighting. Detailedreference to the musculoskeletal, cardio-respiratory systems should be made. Thephysical activity questionnaire, as a healthpromotion tool, would be of use to identifytarget actions where physical fitness is fallingor is below standard. The physical examinationshould include assessment of height, weight,BMI, lung function and an assessment ofvision. In addition, an assessment of aerobiccapacity using a step test method andassessment of grip strength usingdynamometry is recommended.
A holistic approach to the fitness assessmentshould be adopted, an idea which has alreadybeen proposed for both onshore fire-fighters.Effective fire-fighting also requires theoptimum performance of the team. This itselfdepends on the ability to use the attributes ofthe team members most efficiently.Nevertheless, certain basic standards of fitnesswould normally be expected, as shown inTable 16.
Table 16 : Recommended fitness standards for offshore emergency response rescue work
Parameter Recommended StandardAge No limit
BMI < 30kg/m2
Vision Uncorrected Acuity 6/60 N48 Corrected Acuity 6/9-4 N12 Colour Vision Normal or mild green deficiency
(All defects require referral for medical assessment)
Spirometry FEV1 , FVC, PEFR Within normal range
Aerobic Capacity ≥ 40 ml/kg/min (minimum) ≥ 45 ml/kg/min (preferred)
Grip Strength ≥ 40kg
Leg/Back Strength No physiological testing, assessment based on historyWith further evaluation as appropriate
Body mass index (BMI) should normally beless than 30 kg/m2, with lung function testresults within the normal range. The visualacuity should be similar to that required foronshore-retained fire-fighters (6/9-4, N12 at 30
cm with both eyes open, using visual aids, ifnecessary, with an uncorrected acuity of 6/60,N48). Visual aids, if required, must becompatible with fire-fighting. Where a colour

250
vision defect is identified, referral should bemade for further medical evaluation.
Aerobic capacity should be ≥ 40 ml/kg/minand ideally ≥ 45 ml/kg/min. Where thisstandard is not met, other parameters need tobe assessed to determine what fire-fightingduties could be performed, and what can bedone to improve aerobic capacity. Gripstrength should be ≥ 40 kg to ensure adequateupper body strength. No assessment ofleg/back strength has been recommended dueto the concerns relating to the safety of such atest. No specific age limit for performing fire-team duties is recommended either, but whenfitness is assessed longitudinally, cases whereperformance is noted to deteriorate should beassessed on an individual basis.
The implementation of theserecommendations, by assisting with themaintenance of effective fire-teams, andimproving health and safety standards, willassist all those employed within the offshoreoil and gas industry in the United Kingdom.
References
Anonymous. Ageing at work: consequencesfor industry and individual. Lancet1993;341:87-8
Ashwell M. Obesity in men and women. Int JObesity 1994;18(Suppl 1):S1-7
Barnard RJ, Duncan HW. Heart rate and ECGresponses of fire fighters. JOM 1975;17:247-50
Bennet Bl, Hagan RD, Banta G, Williams F.Physiological responses during shipboard fire-fighting. Aviat Space Environ Med1995;65:225-31
Björntorp P. Obesity. Lancet 1997;350:423-6
Brandt-Rauf PW, Cosman B, Fallon LF,Tarantini T, Idema C. Health hazards offirefighters: acute pulmonary effects after toxicexposures. BJIM 1989;46:209-11
Brown A, Cotes JE, Mortimore IL, Reed JW.An exercise training programme for firemen.Ergonomics 1982;25:793-800
Central Fire Brigades’ Advisory Council.Report of the Joint Working Party onAppointments Provisions. London, HomeOffice, 1988
Chia KS, Jeyaratnam, Chan TB, Lim TK.Airway responsiveness of firefighters aftersmoke exposure. BJIM 1990;54:228-31
Corpe U. A Step in the Right Direction.Submitted for Certificate in OccupationalHealth Nursing, Robert Gordon’s Institute ofTechnology, Aberdeen, 1991
Cotes JE, Reed JW. North Sea divers are nofitter than sedentary men (letter). Lancet1984;2:348-9
David GC, Fernandes AF. Physical Selectionfor Rescue Craft Crew. London, HSE OffshoreTechnology Report, HMSO, 1995
David GC, Hoffman JS. Minimum andMaximum Height Requirements for fireService Recruits. Guildford, Robens Institute,University of Surrey,1996
Davies WW. Physical Fitness Standards forFirefighters. Personal communication, 1997
Davis PO, Dotson CO, Santa Maria DL.Relationship between simulated fire fightingtasks and physical performance measures. MedSci Sport Exer. 1982;14:65-71
deVries HA, Wiswell RA, Romero G,Moritani T, Bulbulian R. Comparison ofoxygen kinetics in young and old subjects. EurJ Appl Physiol 1982;49:277-86
Douglas DB, Douglas RB, Oakes D, Scott G.Pulmonary function of London firemen. BJIM1985;42:55-8
Douglas RB, Blanks R, Crowther A, Scott G.A study of stress in West Midlands firemenusing ambulatory electrocardiograms. Workand Stress 1988;2:309-18
Ellam LD, Fieldman GB, Fordham M,Goldsmith R, Barnham P. The perception ofphysical fitness as a guide to its evaluation infiremen. Ergonomics 1994;37:943-52
European Respiratory Journal, Supplement16,1993
Fireground Vision Research Unit. Aids toVision on the Fireground. London, CityUniversity, Fireground Unit Research Unit,1995
Freil JK, Gabriel A, Stones M. Nutritionalstatus of firefighters. Can J Public Health1988; 79:275-6

251
Gledhill N, Jamnik VK. Characterization ofthe physical demands of fire-fighting. Can JSpt Sci 1992;17:207-13
Goldsmith R. Fitness of Firemen. Personalcommunication. 1995
Guidotti TL, Clough VM. Occupational healthconcerns of fire-fighting. Annual Rev PublicHealth 1992;13:151-71
Haisman M. Age Limit for ServingFirefighters. London, Home Office FireResearch and Development Group, 1996
Home Office. Fire Service Circular 8/1991,Medical and Physical Standards in the FireService: The Step Test and OccupationalHealth Schemes. Home Office, 1991
Horowitz MR, Montgomery DL. Physiologicalprofile of fire fighters compared to norms forthe Canadian population. Can J Public Health1993;84:50-2
Horsfield K, Guyatt AR, Cooper FM,Buckman MP, Cumming G. Lung function inWest Sussex firemen: a four-year study. BJIM1988;45:116-21
Horvath SM, Raven PB, Dahms TE, Gray DJ.Maximal aerobic capacity at different levels ofcarboxyhaemoglobin. J Appl Physiol 1975;38:300-3
Ilmarinen J, Louhevaara V, Korhonen O,Nygård C, Hakola T, Suvanto S. Changes inmaximal cardio-respiratory capacity amongaging municipal employees. Scand J WorkEnviron Health 1991;17(suppl 1):99-109
Kilbom Å. Physical work capacity of firemen,with special reference to demands during firefighting. Scand J Work Environ Health1980;6:48-57
Lemon PWR, Hermiston RT. Physiologicalprofile of professional fire fighters. JOM 1977;19:337-40
Leon AS, Jacobs DR, DeBacker G, Taylor HL.Relationship of physical characteristics andlife habits to treadmill exercise capacity. Am JEpidemiology 1981;113:653-60
Light IM, Gibson M. Percentage body fat andprevalence of obesity in a UK offshorepopulation. B J Nutrition 1986;56:97-104
Louhevarara V, Ilmarinen R, Griefahn B,Künemund C, Mäkinen H. Maximal physicalwork performance with European based fire-protective clothing system and equipment inrelation to individual characteristics. Eur JAppl Physiol 1995;71:223-9
Lusa S, Louhevaara V, Kinnunen K. Are thejob demands on physical work capacity equalfor young and aging firefighters? JOM 1994;36:70-4
Lusa S, Louhevaara V, Smolander J, KivimäkiM, Korohonen O. Physiological responses offirefighting students during simulated smoke-diving in the heat. Am Ind Hyg Assoc J1993;54:228-31
Manning JE, Griggs TR. Heart rates in firefighters using light and heavy breathingequipment: similar near-maximal exertion inresponse to multiple work load conditions.JOM 1983;25:215-8
Moisan TC. Prolonged asthma after smokeinhalation: a report of three cases and a reviewof previous reports. JOM 1991;33:458-61
Musk AW, Smith TJ, Peters JM, McLaughlinE. Pulmonary function in firefighters: acutechanges in ventilatory capacity and theircorrelates. BJIM 1979;36:29-34
Nygård C, Luopajarvi T, Ilmarien J.Musculoskeletal capacity and its changesamong aging municipal employees in differentwork categories. Scand J Work Environ Health1991;17(suppl 1):110-7
O’Connell ER, Thomas PC, Cady LD,Karawasky RJ. Energy costs of simulated stairclimbing as a job-related task in fire fighting.JOM 1986;28:282-4
Posner JD, Gorman KM, Klein HS , WoldowA. Exercise capacity in the elderly. Am JCardiol 1986;57:52C-58C
Saupe K, Sothman M, Jasenof D. Ageing andthe fitness of fire fighters: the complex issuesin abolishing mandatory retirement ages. Am JPublic Health 1991;81:1192-94
Schonfeld BR, Doerr DF, Convertino VA. Anoccupational performance test validationprogram for firefighters at the Kennedy SpaceCenter. JOM 1990;32:638-43
Scott GE. Physical Fitness of Firefighters: ASummary Report. London, Home Office

252
Scientific Research and Development Branch,1987
Scottish Office. Fire Service Circular 6/1996,Visual Standards on the Fireground.Edinburgh, Scottish Office, 1996
Sharkey BJ. Functional vs chronological age.Med Sci Sports Exerc 1986;19:174-78
Shephard RJ. A personal perspective on agingand productivity, with particular reference tophysically demanding work. Ergonomics1995;38:617-36
Shephard RJ. Occupational demand andhuman rights, public safety officers andcardio-respiratory fitness. Sports Medicine1991;12:94-109
Sheppard D, Distefano S, Morse L, Becker C.Acute effects of routine fire-fighting on lungfunction. Am JIM 1986;9:333-40
Sherman CB, Barnhart S, Miller MF, SegalMR, Aitken M, Schoene R, Daniell W,Rosenstock L. Fire-fighting acutely increasesairway responsiveness. Am Rev Respir Dis1989;140:185-90
Sköldström B. Physiological responses of firefighters to workload and thermal stress.Ergonomics 1987;30:1589-97
Sothman M, Saupe K, Raven J, Pawelczykl J,Davis P, Dotson C, Landy F, Siliunas M.Oxygen consumption during fire suppression:error of heart rate estimation. Ergonomics1991;34:1469-74
Sothman MS, Saupe K, Jasenhof D, Blaney J.Heart rate response of firefighters to actualemergencies. JOM 1992;34:797-800
Sothman MS, Saupe KW, Jasenhof D, BlaneyJ Fuhrman SD, Woulfe T, Raven PB,Pawelczyk JP, Dotson CO, Landy FJ, SmithJJ, Davis PO. Advancing age and the cardio-respiratory stress of fire suppression:determining a minimum standard for aerobicfitness. Human Performance 1990;3:217-36
Sykes K. Chester Step Test. Chester,University College, 1995
Thompson J, Barr D, McDonald DR, RennieMJ. North Sea divers are no fitter thansedentary men (letter). Lancet 1984;2:107-8
QUESTIONS AND ANSWERS SESSION
Question - Tony Parkinson, Noble Drilling,for TexacoI think I’m one of the few people in this roomthat actually work offshore at the moment andI’ve been part of ER emergency responseteams for 20 years. So I think I know a littlebit about what I’m talking about. What theaudience will know is that all the fire fightersonshore are volunteers. Offshore they’re notand it’s the position that the company employsthem for, such as electricians, operations,safety, whatever, that drives them into beingthe ER team offshore. So, it’s a position thatthey don’t volunteer for, they’re just put into it.I’m not getting all of this in the right ordermaybe, but what does the author of thepresentation we just had suggest, if they don’tmeet the criteria? Does the company stopemploying them or at some stage in the gamesay well, you can’t be in the RT so we can nolonger employ you?
The offshore work force is getting older as weknow. I’m one of them. Also we’re gettingsmaller per platform. They’re reducing thenumber of people that they need to operate, sothat’s another factor. There are very fewpeople on my platform that can be in the team.They’re required for emergency response,they’re required for coxswains, things like that.The regulations are driving all operators tomake platforms that don’t need manualintervention. We’ve got safe havens, we’vegot fire and gas systems. Montrose teachespeople now not to be gung ho. It teaches themto think and step back and not to go in andfight it. Leave it alone. Let it burn. Let’s getoff. Let’s leave it.
Different things - the height, the weight - youcan’t control the people you employ to do anelectrician’s job. It is just a fact that he’s alsogoing to be in the emergency response team.Alcohol, that part of it; there is no alcoholoffshore so for a fortnight there’s no access tothat. We’ve mentioned about the step test.I’ve seen some results of that offshore. I gohill walking. I consider myself quite fit to goclimbing mountains but I didn’t do too well inthe step test. I know people who go to the gyma lot also failed it. It’s quite surprising, so Idon’t know how accurate that is for ajudgement.
ChairmanCan I ask you to summarise your questionplease?

253
Question - Tony Parkinson, Noble Drilling,for TexacoNot really. What are we going to do about it?When we heard about this step test, it wasmore stress - people were worried that if theyfailed it, they might be thrown out of the RT.Would they lose their job? What are wesuggesting happens from this?
Answer - Dr Allan Prentice, AonOccupational HealthWhat I was doing was suggesting a particularstandard. Obviously these sorts of questionshave to go directly to the employer in terms ofwhat they do if someone isn’t meeting thestandards. I accept the point about obviouslyvoluntary recruitment for the fire teamsoffshore. Obviously there’s a restricted choicethat is available and therefore people may notbe volunteers as such, they may be coercedinto these positions. They may be veryreluctant volunteers and that’s no motivationreally to achieve a standard. If you think youmight lose your job, well that is, but I don’t
really think that should be an issue. I certainlywouldn’t support that in terms of people losingtheir jobs.
The company has got to be aware that ifpeople are required to do these tasks then theyare possibly putting themselves at risk. Theywill get tasks done but will it be in sufficienttime? In terms of the step test, if it’s doneaccurately as I said there is a 10% error, so Iwouldn’t accept that there are these widevariations that you’re quoting. It obviouslydepends on the training of the individual that’sdone the test and if they’re done in optimalconditions even the standard is less than a 10%error.
In terms of the issue of what happens to peopleif they do not meet the standard; I would saythe same as what happens in terms of onshorefire teams, that really we have to have fitnesstraining programmes in terms of ensuring thatpeople do reach these standards.

254

255
AGEING OF THE OFFSHORE WORKFORCE IN THENORWEGIAN OFFSHORE INDUSTRY: IMPLICATIONS FOR
SAFETY AND HEALTH
Dr Eirik Bjerkeboek, Dr Helge Wiig and Dr Hilde Heber
Norwegian Petroleum Directorate
Introduction
The Norwegian offshore oil industry hasgrown through more than three decades into amature industry with well-developedinfrastructure and a fairly stable work forceemploying 15-20.000 persons depending onvariations in the activity level. Although newoil and gas fields regularly are found anddeveloped, a significant increase in the amountof labour invested. New technologies and neworganisational designs continuously reduce theamount of human energy spent on upstreamactivities.
During this period the recruitment strategy haschanged. In the early days there were good jobopportunities for low educated workers.During the last two decades mainlyexperienced and specialised workers have beenrecruited. Within the traditionally hierarchicalorganisations of the petroleum industry,offshore career opportunities have generallybeen recognised as scarce, and a pattern of lowmobility and increasing workforce age hasdeveloped.
External recruitment has been low for years.Transferring personnel from alreadyestablished offshore organisations has mostlystaffed the more recently developedorganisations on new installations. Aconsistent trend of downsizing in existingorganisations has enforced the picture of astable and steadily aging cohort.
The challenges pertaining to increasingaverage workforce age has been addressedsince the early 1990s by the different tradeunions, The Norwegian Oil IndustryOrganisation (NOIO) as well as thegovernment. During the same time period theaverage age of the Norwegian work force as awhole has increased, accompanied by largeincreases in the rate of disablementpensioning, increased health problems andlarge increases in health related costs. At thesame time predictions show that Norway will
face a shortage of labour in several sectorswithin the next decade, giving a new focus onthe positive effects of continued/increasedparticipation of senior personnel in the workforce. Challenges associated with ageing andincreased disablement of the work force istherefore currently addressed by thegovernment as an important topic.
In addition to the implications for workershealth and national economy, is has morerecently become apparent that the demographicand organisational changes seen in the offshoreindustry also may cause serious conflicts withestablished and well proven strategies foremergency preparedness and reduction of harmduring safety critical events.
Thus, the Norwegian Petroleum Directorate(NPD) as the governmental agency responsiblefor following up legislation on workingenvironment, workers health and safety on theNorwegian continental shelf, the (NPD)addresses these challenges seriously and incollaboration with trade unions and the NOIO.
Norwegian legal requirements pertaining towork environment and health for ageing
employees
As a background for a description of thechanges and challenges that increasingworkforce age raise with respect to health andsafety, a brief summary of relevant legislationand regulations is given.
The general mandatory retirement age inNorway of 67 years is established byagreement between employers and employeesorganisations. This age level is high comparedwith most other European countries. Forspecial groups of employees, such as police,firemen and seamen, the retirement age islower, set by agreement between workersunions and employers. The mandatory age of67 applies to most employees in the petroleumoffshore industry, although several companies

256
have special agreements on lower pensioningage.The Norwegian Working Environment Actstates as objectives, to secure soundemployment conditions and meaningful worksituation for the individual employee.Furthermore § 14 e states that; employer shallorganise and arrange the work giving dueconsideration to age, proficiency, workingability and other capabilities of the individualemployee. This act also requires thatemployers show attention to workers welfareand dignity, which is of relevance in handlingthe consequences of ageing.
These requirements are further elaborated inRegulations relating to systematic follow-up ofthe working environment in the petroleumactivities. Here a number of paragraphs staterequirements relevant to the topics of thispaper, such as; monitoring and follow upadverse health effects from long termexposure, as well as arrangement andorganising of work operations.
There are also mandatory health requirementsfor offshore employees in the petroleumindustry. These requirements are related tofunctional requirements in emergencypreparedness situations, and are not related toworking ability. All employees carrying outwork on offshore installations therefore needto be certified by a physician, obtaining a so-called health licence. This licence has to berenewed on a two-yearly basis and can berevoked at any time by company doctors orany other physician.
As the enforcer of these regulations, the NPDspolicy is to ensure that the industry offersworking and “off-working” conditions
offshore that allow those who wish to continueworking until mandatory retirement age.
Changes in age and health in the work forcein the Norwegian petroleum industry
In order to monitor the situation, the NPDcarried out to surveys on workers age andhealth in the offshore industry, in 1992 and1998 respectively. These surveys included themajor part of all operating companies, ship/rigowners, and entrepreneur/service companiesactive on the Norwegian continental shelf. Theinformation presented from the 1998 surveyrepresents aggregated statistics fromapproximately 11000 employees, with a fairdistribution between the different industrialcategories. This is about 2/3 of the totalpopulation carrying out regular work on thecontinental shelf. Staffing on supply andstandby vessels are not included in the survey.
Figure 1 shows the age distribution in 1992and 1998, demonstrating a clear shift towardshigher age. Mean age for the populationincreased from 38,8 to 42,9 yrs. The increaseis largest within operator company employeeson permanent installations. The increase inmean age of ca 0,7 yrs/yr. is not due tomigration effects e.g. from educationalreforms, which cause similar increases in meanwork force age in Norway as a whole. Lowrecruitment of young employees combinedwith low mobility in existing work force arethe most probable explanations. It should benoted that the increase in age probably isattenuated by a larger proportion of seniorworkers exiting from offshore employmentduring the large number of reorganisations inthe industry lately.
0
10
20
30
40
50
20-29 30-39 40-49 50-59 60 +
Age
Pro
po
rtio
n (
%)
of
emp
loye
es
1992
1997-98
Figure 1 Age distribution in the offshore industry work force

257
Health problems and thus the amount of sickleave increases markedly in the age groups of50+ yrs. We do not have data to show changesin the sick leave ratios over the last six years,but the shift in mean age probably have result
in a marked increase in yearly total number ofdays away from work. Figure 2 shows the totalnumber of sick days per employee/year.
0
5
10
15
20
25
30
35
20-29 30-39 40-49 50-59 60 +
Age
Sic
klea
ve (
day
s/em
plo
yee/
yr)
Figure 2 Sick leave in the offshore industry
The age-related increase in sick leave is notaccompanied by a similar increase in thenumber of cases of work-related sicknessreported to NPD. This may be due difficultiesdetermining work related cause-effectrelationships, especially of long-term exposureand for complaints with multi-causal origin.
A comparison of the offshore data with sickleave onshore is difficult. No similar agedistributed data for the onshore populationexist, but the national rate of long-term sickleave (more than 14 days) shows a similartrend in age development and a consistentincrease in long duration leave during the lastfive years. This supports research fromStatistics Norway (personal communication),showing that older workers stand for the majorpart of long-term sick leave. Off shore themost aggravating result is a mean value of 44days sick leave/employee/year for operatingcompany personnel over 60 years.
A mean total sick leave of ca 7 days/employeeoffshore is low, however compared to ca 17days/employee in comparable onshoreindustries. This discrepancy is probablycontributable to several factors. The healthrequirements, as well as special workingconditions offshore probably result in amarked “healthy worker” selection effect. Alsothe special shift arrangements contribute tolow reporting by the companies. With a 2week on – three/four week off schedule,sickness during off schedule is most often notregistered by the companies.
The increase in health problems and sicknesswith age is also clearly demonstrated in therate of loss of health licence, shown in figure3. The blue columns in the figure show the rateof loss of licence in 1998 relative to theproportion of employees in each age group.

258
0
2
4
6
8
10
12
20-29 30-39 40-49 50-59 60 +
Age
% o
f w
ork
fo
rce
wit
hin
ag
e g
rou
p
loss of licence disablement pensioning
Figure 3 Rate of loss of health licence in the offshore industry work force
Our data show a more than 50% rise in thefrequency of loss of licence for employees 60+ years from 1992 to 1998. For the other agegroups the frequencies are unchanged. Forcomparison, the black columns depict thefrequency of new disablement pensioners inNorway in 1999. Data presently beingcollected from the offshore industry show, thatthose who loose their health licence almostalways exit from working life altogether, mostcommonly through disablement pensioning.Licences can be revoked by any medicaldoctor in Norway. Unfortunately no register ofthe causes for loss of licence has beenestablished. Since the licence reflectsemergency preparedness requirements, and notworking ability, we must be cautious inascribing the high rate of loss to adverse healtheffects attributable to work related exposure.However, it is generally recognised thatcompany physicians revoke licences on thebasis of evaluation of working ability in an
offshore environment. The fact thatdisablement-pensioning follows most revokedlicenses, strongly indicates that doctorsjudgement is reasonable, althoughundocumented.
The rate of loss of licence within each agegroup can be used to generate a simpleprediction of “work-survival” in offshoreemployment. Such a model is shown in figure4. The remaining population progressivelydeclines as the number of “survivors” ismultiplied with the rate of license loss in eachage group.
The model clearly indicates the magnitude ofthe health problems, and implies that sicknesscontribute largely to the rate of early exit fromoffshore employment. The increased rate ofsick leave of workers age 50 + is thus clearlyin accordance with the rate of exit fromworking life due to adverse health effects.

259
20
30
40
50
60
70
80
90
100
110
20 30 40 50 60
Age
Pro
po
rtio
n r
emai
nin
g in
wo
rk
Figure 4 Modelled “survival” in an offshore workforce cohort
The challenges associated with increasinghealth problems and early exit from workinglife will most likely continue to increase in thenear future. The major proportions of theexisting work force are now between 40 and60 years. Also, a major increase in earlyretirement and increased recruitment of youngpersonnel is unlikely. Thus the old-timers willhave to carry on working with similarexposure levels as they have had up to now,with a high risk of sickness and long-term sickleave as they approach the end of their careers.
Possible causes of increased healthproblems in older offshore employees
Between the employers and employeesorganisations it is a hot topic of debate,whether offshore working conditions representespecially harmful effects, which again arereflected in more adverse health effects thanthose found in comparable industries onshore.Although we do not have statistics on thecauses for loss of licence it is generallybelieved that musculo-skeletal andcardiovascular conditions are maincontributors. These are also important causesfor the increasing rate nationally ofdisablement pensioning. On the national scale,however, mental sickness such as depressionsand neuroses is a large and the most rapidlyincreasing diagnosis group.
Pertaining to the age related increase insickness, the exposure factors that most clearly
point themselves out in the offshoreenvironment are:
• Long-term shift work. Since mobility isvery low, most employees tend to remainin a highly demanding shift schedule for amore prolonged period of time thanworkers onshore. Increased risk of sicknessfrom working shift work, especially nightshifts, is well documented in the literature.However the relationship between ageingprocesses and effects of shift work is lessstudied.
• Shift arrangements with long on-dutyperiods and even longer off-duty periods.This arrangement clearly presents manyemployees with problems handling therelatively constrained life offshore, therepeated separation from family, as well asproblems associated with fragmentedparticipation in family and social lifeduring off-duty periods.
• High physical demand/work load oftencombined with poor conditions for manualhandling of equipment. This risk factor iswell documented in the literature, resultingin both acute and chronic musculo-skeletalsickness.
• Hard surfaces, steep stairs and ladders.Several company doctors attribute the agerelated increase in prevalence of skeletalillness in the lower extremities to thesefactors.
• Motivational factors. The organisations onpermanent offshore installations have, up

260
to now, been rather bureaucratic comparedto similar industries onshore. Also, for thelarge majority of employees there arelimited opportunities for careerdevelopment. It is possible that theseconditions, combined with customisation tolong periods of leisure time, are factors thatreduce motivation for a long working life,which again may affect health and workingability.
• Uncertainty and anxiety associated with theincreases risk of travel and period of stayon the installations.
Of these factors increased individual risk ofillness is well documented for long-term shiftwork and long-term exposure to unfortunatephysical load and walking/working on hardsurfaces. For the other factors changes in riskwith age has not been systematically examinedor documented.
In addition there are a number of other factorsthat may have negative effects with increasingage, such as; rapid rate of organisational andtechnical change; increased learning demand;increased use of advanced technologies; andthe increasing use of non-hierarchicalorganisations. However, these factors are notspecific to the offshore industry.
NPD strategies on ageing and health
The NPD has during the latter years increasedits attention towards the safety and healthchallenges presented by an ageing work force.Our objective is to ensure that workers healthand well-being is appropriately attended to,allowing those who wish so to continue theircareer till retirement age. Furthermore toensure that the industries emergencypreparedness organisation and contingencyplans are adapted to the present and expectedchanges in age and health.
Search and rescue (SAR) teams are importantcomponents of most emergency preparednessorganisations on the installations in theNorwegian petroleum industry. In order tomeet the NPDs functional requirements foremergency preparedness, many companieshave established specific requirements forminimal physical capacity for participants inSAR team. Older workers do not easily meetthese limits. In some cases SAR-team agelimits well below pensioning age have beenintroduced as well. We thus see a possiblescenario where downsizing of organisationsand increasing age comes into conflict with
safety requirements, with early withdrawal as alikely result.
In our effort to ensure that early andinvoluntary exits from offshore work due tohealth complaints are minimised, we need tofocus both on measures directed towards theolder portion of the workforce. However at thesame time measures must be taken to ensurethat the younger part of the population haveworking conditions that allow long-termoccupation in the offshore business. The NPDdirects its effort to secure workers health andwelfare mainly by;
• Issuing an adequate and updated regulatoryframework that encompasses newknowledge on risk factors, identification ofrisk and risk handling measures.
• Following up of the regulatory frameworkthrough audits and quality revisions.
• Counselling, including transfer ofexperience, surveys and direct counsellingin disputes involving interpretation of theregulatory framework
In all these activities, the focus onconsequences of ageing will become moreimportant in the years to come. For instance,the major update of the regulatory framework,to be issued this year, focus on workarrangement and organisation is increased.While the main objective up to now has beenarrangement of each separate work place oroperation to obtain low-risk of injury orsickness, the new regulations require a broaderapproach where total work organisation andrestitution shall be included in risk assessment.
In our effort to ensure that long-termemployment offshore is compatible with agood health outcome, we have a main focus onpreventive strategies:
• Obviously, a good design is of essence increating work and restitution environmentsthat allow long-term employment withoutundue negative health effects. The NPDfocuses both on requirements for the designprocess and the design itself.
• Arrangement of work places andorganisation of work is followed upclosely, combined with a follow up ofgeneral screening of personnel andreporting of work related sickness. Aspecial focus is given to the follow up ofeffects of organisational restructuring in thebusiness

261
The NPD is also active in ensuring that theindustry has an adequate monitoring andfollow up of work related disease. Furthermoreto ensure that both systems and activities are inplace to follow up and support to thoseemployees who either develop, or have higherrisk of developing work related healthproblems.
Adequate measures to prevent the number ofearly exits from working life due to healthproblems are now prioritised also on a nationallevel. A governmental committee has recentlysuggested several measures that may allowolder workers to remain in active work, despiteincreasing health problems:
• Increased maximal period of self-reportedsick leave, a period where employee isallowed to stay away from work withpresumptive sickness without physician’sevaluation.
• “Active sick leave”, an arrangement wherethe employee regulates participation inwork based on a self-assessment of theability to function adequately.
• A more active collaboration between thelocal social security offices and employerin rehabilitating employee after long-termsick leave.
• Increased flexibility in disablement pensionarrangements, allowing a smaller disabilityfraction for allotment of partial pension.
Due to the special offshore shift arrangements,as well as the relatively small opportunitiesthat the petroleum industry offer for onshorerehabilitation, is questionable whether thesuggested measures will have much effect forolder workers offshore.
From the NPDs point of view it seams clearthat significant progress on improving workingconditions and health risk for older workers
can only be made if employers and employeescollaborate in defining and carrying out unifiedpreventive strategies.
The strategies of the industry and theemployers o
Recently the NOIO have initiated a project onage and health, inviting the major trade unions,the organisation for ship and rig owners, aswell as governmental agencies to participate.The aims of the project is to reduce sick leaveand disablement pensioning and developproactive measures for handling the expectedrise in mean age for offshore workers. Throughthis project the NOIO also aims to makeoffshore employment more attractive to seniorpersonnel.
Besides a closer survey and statistical analysisof relevant data from the industry, the projectaims to provide a knowledge base and apolitical platform for launching more practicalpreventive measures in the future.
Whether this strategy succeeds remains to beseen. The NOIO and the trade unions stilldisagree on major issues such as:
• Are offshore employees subject to negativehealth effects that put them significantlymore at risk than colleges onshore?
• What is a reasonable pensioning age foroffshore employees?
Hopefully the descriptive and analytical part ofthe project will give some answer to the firstquestion, while the practical part of the projectwill give results that allow older worker toremain in offshore employment withoutnegative health consequences.

262

263
IMPACT OF HEALTH SURVEILLANCE AND PROMOTION ONOFFSHORE ACCIDENT RATES
Dr Kathryn Mearns, Industrial Psychology Group, University ofAberdeen
Abstract
The Aberdeen University IndustrialPsychology Group have just completed aproject entitled ‘Benchmarking human andorganisational factors in offshore safety’involving the HSE and 13 offshore operatorand contractor companies. The exerciseinvolved using questionnaires to collect safetyinformation for the previous year for aparticular installation from three differentsources:1. The offshore workforce, in terms of how
they perceived the installation’s currentstate of safety;
2. Managers, in terms of recording healthand safety management policies andpractices;
3. Safety performance data in terms of self-reported accidents from workforcerespondents and official accident andincident rates (e.g. RIDDOR)
Nine installations were compared according totheir scores on each section of thequestionnaires, and relationships between thescores on the questionnaires and accident andincident rates were explored. A section in themanagement questionnaire requestedinformation on health surveillance andpromotion and a high significant correlationwas found between scores on this section andthe rate of LT1>3 (rho9-0.76). In addition,there was a high and significant correlation(rho9-0.81) between scores on this section andthe proportion of workforce respondentsreporting an accident in the previous year. Thispaper will present the methodology used tocollect the data and discuss the possibleimplications of this finding.
Introduction
The literature on workplace health promotionor employee ‘wellness’ programmes isextensive with the USA leading the field ininitiating, implementing and assessing theeffects of such programmes. Theseprogrammes usually focus on weightreduction, hypertension control, fitnesstraining, medical screening, stress
management, ‘stop smoking’ and advice ondiet and nutrition. In the USA their mainobjectives are to promote employee health andreduce corporate health care costs, howeverother documented spin-off effects include:• Reductions in employee absenteeism and
lateness• Fewer accidents• Less worker compensation costs and
employee turnover• Greater employee loyalty and commitment• More creativity and effectiveness in
decision-making amongst employees• Better labour relations and employee
recruitment• Improved company imageUnlike the USA and some European countries,e.g. Norway and Sweden, where legislationhas mandated health promotion, Britain haslagged behind in promoting health at theworkplace. This imbalance has been redressedto some extent in the HSE document ‘GoodHealth is Good Business (www.hse.gov.uk)which focuses employers’ attention onidentifying and mitigating against potentialoccupational health risks at the workplace.Occupational health is not a new issue for theoffshore industry and the HSE theme ‘goodhealth is good business’ underpins some of themanagement systems adopted by the industry.However, it is worthwhile noting that whereasthe issue of occupational health is receivingthe attention it merits, there is comparativelylittle research conducted on the impact ofhealth promotion programmes on the well-being of offshore workers.
A pilot study on the extent of health promotionactivities in the offshore oil industry wasconducted by Mearns and Fenn in 1993 (HSE,1994). The Medical Directors of 41 offshorecompanies operating in the UK sector and 21companies operating in the Norwegian sectorwere surveyed about the number and types ofhealth promotion programmes currently inplace on their installations and theindividuals/organisations responsible for theseprogrammes. In addition, 145 UK and 76Norwegian offshore medics were surveyedabout the need and priority for health

264
promotion offshore. The overall response ratewas 36% (53% UK rig medics: 25%Norwegian rig medics: 14% UK MedicalDirectors and 29% of Norwegian MedicalDirectors). Most respondents gave offshorehealth promotion a high priority because of theageing workforce and their relatively poorlifestyle (smoking, lack of exercise andovereating). Various health promotionactivities were in operation but were limited to47% of the Norwegian installations and 36%of the UK installations surveyed.
Method
More recently (Mearns, et al. 2000), Mearns,Whitaker, Flin, Gordon and O’Connor havecarried out a health and safety benchmarkingstudy (sponsored by 13 offshore oil and gascompanies and the HSE). This studycompared the health and safety performance of13 offshore installations (including fixedproduction platforms, well-service vessels,FPSOs and drilling rigs) on a range of leadingand lagging performance indicators. Theleading indicators included safety climatesurveys of the offshore installations in whichrespondents indicated their involvement insafety, safety behaviour, safety attitudes,satisfaction with safety measures andsatisfaction with communication about healthand safety. In addition, HSG 65 (HSE 1997)was used as a model for development of aSafety Management Questionnaire (SMQ),which recorded a range of safety performanceindicators used in other health and safetybenchmarking programmes. These covered sixmain areas: i) Health and safety policy; ii)Organising for health and safety; iii)Management Commitment; iv) WorkforceInvolvement; v) Health surveillance andpromotion; vi) Health and safety auditing.
The participating installations were alsorequired to provide details of theirmanagement structure, including the positionof safety professionals within the hierarchy,and their accident and incident statisticsincluding RIDDOR data, near-misses, visits tothe offshore medic and number of cards/reports from behavioural modificationprogrammes. Relevant documentation tosupport the questions asked in the SafetyManagement Questionnaire (SMQ) was alsorequested. All information related to theperiod June 31st 1997 to June 31st 1998 (for the1998 benchmarking survey) and June 31st 1998to June 31st 1999 (for the 1999 benchmarkingsurvey).
Results
With respect to the current paper the area ofinterest lies in the results obtained from theSafety Management Questionnaire (SMQ).Analysis of data from the nine installationswhich provided data in both 1998 and 1999(i.e. were common to both years), took theform of rank correlations between the six sub-sections of the SMQ, the total SMQ and fouroutcome measures. These outcome measureswere LTI>3 days, RIDDOR data (although it isacknowledged that this indicator is anaggregate of other lagging indicators); Nearmisses and Dangerous Occurrences. A patternof negative correlations was predicted andfound: favourable scores on the entire SMQwere associated with lower accident andincident rates. All significant negativecorrelations involving sub-scale scores wereconfined to two areas of management strategy- health promotion and surveillance and healthand safety auditing. In particular in 1998, highscores on the full sub-scale ‘Health promotionand surveillance’ (which included bothquantitative and qualitative data) weresignificantly associated with lower lost timeinjury rates (rho -0.76). Responses to anabbreviated sub-scale including justquantitative data were significantly correlatedwith lower rates of dangerous occurrence (rho–0.79), near misses (rho –0.76) and RIDDOR(rho-.78). A pattern of negative correlationswas also found in the 1999 data, however, theeffects were not as strong. From these resultsit is proposed that the benefits of healthpromotion and occupational healthprogrammes may be realised through a numberof possible processes:
1. Investment by the company in these areasfosters perceptions of companycommitment and builds worker loyalty inareas such as safety behaviour
2. Health plans and health programmesimprove worker health directly and‘immunise’ against work-related injury(although there is also a possibility thatthey mask early signs of occupational illhealth).
3. Health plans and health programmes‘weed-out’ unhealthy workers leaving a‘survivor population’ that are best suitedto the offshore environment, bothphysically and mentally. However, itshould be noted that this process is alreadyin place through the mandatory regular

265
offshore medicals that workers have topass in order to work offshore.
4. A final mechanism can also be suggestedwhereby an installation that is good atheath promotion and health surveillancemay also be good at the risk assessmentand control approaches and training.
These processes are presented speculatively.Indeed, it is important to emphasise that thedata presented here are correlational andrelatively limited. There is therefore a need toconduct further research in order tocorroborate the findings and to understand themechanism behind any effects. In other words,apart from showing associations between thesevariables it is important to model potentialcause-effect relationships.
There are three questions that can bespecifically posed with respect to the above:
1. Is enhanced health and fitness associatedwith a perceived increase in ability to copeboth physically and psychologically withthe offshore working environment? Inother words, increased feelings of physicaland mental well-being have a directimpact on physical and psycho-socialstressors leading to improved ability tocope, greater attentiveness and ability torespond to potentially hazardous situations
2. Are increased investments in healthpromotion & surveillance indicative ofhigher levels of management commitmentto safety and a culture of care andconcern? The effects of this on theworkforce could operate through twopossible mechanisms a) a higherperception of self-worth leads to personneltaking more care and experiencing feweraccidents, b) an improved perception ofcompany commitment to worker well-being builds loyalty in areas such as safetybehaviour?
These hypothesised relationships provide thebasis for a proposed new study, investigatingthe impact of health promotion andsurveillance on accident and incident ratesoffshore.
The proposed methods for collecting the dataare through questionnaires and interviewtechniques. These should be used across aslarge a sample of installations as possible(minimum 10), preferably including a sub-setof installations on which there are no healthpromotion and surveillance programmes. Thequestionnaires would be directed at the core
crew, including contractors (i.e. thosemembers of the workforce who are mostfamiliar with the installation) and wouldrequest the following information:• Demographics (age category, years
worked offshore, years worked on currentinstallation)
• Perceived management commitment tohealth and safety (both offshore andonshore),
• Perceptions of work pressure• Perceptions of social support• Perceptions of stress• Self-reported health and well being,
coping strategies, safety behaviour andaccidents/injuries/illness.
All information collected would be anonymousand confidential.
Questionnaires would also be sent to a seniormanager associated with the installationrequesting information on the following:• Type of health promotion programmes on
the installation and how long they havebeen in place.
• Details of how health issues arecommunicated to the workforce.
• Whether an occupational health plan is inplace and what percentage of the healthplan has been completed for the previousyear.
• What provision there is for routine healthsurveillance of workers. Here, there is aneed to distinguish with surveillance formedical fitness and more frequentsurveillance for auditory problems anddermatitis, for example.
• Whether there are facilities for healthreview on return to work after sickness
• Whether counselling, support andprofessional advice are made availableduring periods of ill health or stress. Forexample, uptake of Employee AssistanceProgrammes (EAPs) could be measured,as could the extent of rehabilitation afterinjury or ill health and follow-up of theindividual’s well being and progress whilestill absent.
• Whether there are mechanisms foridentifying and helping individuals withalcohol or drug related programmes. Inaddition, how the process for identifyingand helping individuals is actually carriedout may be of particular importance.
• Number of personnel visits to the sick bayin the past year. An attempt will be madeto categorise these visits according tovarious criteria, e.g. major injuries, lost

266
time injuries in excess of three days, firstaids, distribution of medication, ‘notreatment’. A mechanism will also haveto be put in place to monitor repeat visitsto sick bay. Care will be taken so as not tojeopardise patient confidentiality.
Interviews would be conducted with membersof the workforce, rig medics and seniormanagers to check the validity of the proposedquestionnaire items and also to collectqualitative data on attitudes to theorganisation, health promotion, healthsurveillance and personal health and fitnessand its perceived benefits or problems.
References
HSE (1997) Successful Health and SafetyManagement HS(G) 65. Sudbury: HSE Books.
Mearns, K. and Fenn, C. (1994) Diet, Healthand the Offshore Worker. OTH 93 339.Sudbury: HSE Books.
Mearns, K., Whitaker, S., Flin, R., Gordon, R.and O’Connor, P. (2000). Benchmarkinghuman and organisational factors in offshoresafety. Vol I of III in ‘Factoring the humaninto safety: Translating research into practice’.OTO 2000 036. Sudbury: HSE Books.

267
SUMMARY OF CONFERENCE
Ian Whewell, HSE
If I could just apologise again on behalf of TafPowell who had another pressing engagementand therefore wasn’t able to attend. My rolereally is to bring to a close what I hope andbelieve has been a very successful three dayconference. Summarising a three-dayconference, three days of quite intensepresentations, discussions and debate is not aneasy matter. I’m not sure whether it’s stress orpressure I’m under at the moment. The aim ofthe organisers was to raise the profile of whatis often a Cinderella subject. I realise thatobviously those of you who are here have aparticular interest in occupational health butthere is no doubt that there is a struggle indrawing the attention of industry and thepopulation at large to health issues becausethey tend not to be so visible as the classicaccident situations.
I hope the conference has providedopportunities to share views and challengesand successes and perhaps failures. I believethe underlying message that seems to becoming through here is one of partnership andshared responsibility. Certainly the first dayset the tone for that with Bill Callaghan fromthe Health and Safety Commission coming tothe conference and Malcolm Brinded (Shell),both emphasising aspects of sharedresponsibility and the commitment of both theregulator and the industry at large to tackleoccupational ill health. It’s certainly clear tome at any rate that all health and safetymatters.
TAPE CHANGE, therefore bit missing here
We shouldn’t forget though in looking atpartnership that it’s the employer that doeshold the key. The employer can facilitate thisand it’s encouraging to see this renewedcommitment, certainly as a result of theconference that was held under the auspices ofthe Offshore Industry Advisory Committee todevelop cooperative working. And inparticular, I think this has been emphasised atleast once today, the importance of identifyingthe statistics, of coming together, because theRIDDOR statistics, in other words thestatistics held by the regulator are pretty thinbecause of the nature of the reporting, whichhas already been criticised today.
The theme of partnership I think was extendedinto the second day where certainly the role ofgood design in occupational health, and ofcourse the ever present physical, chemical andbiological agents, emphasise how much goodwork has been done in these areas. We heardabout a number of cooperative projects andthere is clearly a considerable commitment totackle occupational health problems.
Finally, today we heard how some of thedifficult issues, and let’s be honest, these areeven more tenuous occupational health issuessuch as stress and workforce well-being issuesare being tackled. Again the partnership inparticular was emphasised by Fiona Farmerthis afternoon and I was interested to hear as Iwas writing my summary that she emphasisedthe important role of partnership in developingwell-being and good health. The other thing Ithink these sessions did do as well wasemphasise the importance of the workforceinvolvement and employee and employerawareness to jointly tackle these issues.
The conference has covered a wide range ofoccupational health issues and I think it comesas no surprise that the key topics emerging ascreating significant concern are stress andmusculoskeletal issues. HSE is alreadytackling aspects of musculoskeletal disordersas part of its current initiatives. We’ve alsorecognised stress as a problem that we have toget to grips with. Certainly we are lookingtowards next year of trying to raise the profileof our approaches to stress and see how theindustry can further deal with that.
If I could put a quick plug in here formusculoskeletal issues. There are to be twoseminars later this year and I think there’sinformation in your pack and there will beinformation on the HSE website of twoseminars, one in Aberdeen and one in GreatYarmouth, looking at musculoskeletal issues.
We must not forget in looking at emergingissues, that the traditional problems stillhaven’t gone away. We are still gettingdermatitis, we still need to tackle the problemsof noise, chemicals, other hazardous materials.

The effects of them may not be immediatelyobvious but they do need to be dealt with.
I hope you are taking away ideas from theconference. It is important that it hasstimulated your thoughts as to how you mightproceed on the issues. HSE certainly is takingaway a number of issues and certainly Ron andhis colleagues who have been here will betaking points. In particular, we have taken toheart the criticisms of ill health reporting andthat there is a review of formal accident,incident and ill health reporting whichobviously we can feed in. We have also takenaway some good examples of good practiceand best practice which as a regulator who canmove across the industry, we can provide anopportunity to deal with this.
I want to take this opportunity of remindingyou of the role that industry has got in terms ofthe Step Change initiative because there is agreat emphasis on improving the cooperativeworking as I said earlier. Certainlydistributing examples of good practice and bestpractice across the range includingoccupational ill health, dealing withoccupational ill health, is invaluable and thatshared knowledge is of great importance.
It finally remains for me to thank all thespeakers and chairmen and all the delegates foryour commitment in stimulating debate. Ioverheard a conversation at lunchtimecomplaining there wasn’t enough time fordiscussion generally over the three days. Ithink that’s always a good indicator of achallenging and interesting conference thatneeds to stimulate debate. It’s always difficultto single out individual contributors but Iwould particularly like to take the opportunityof thanking Kevin O’Donnell who has doneextensive work in organising the conferenceand Vee Gatrell and the team from DIAS, thepublications organisation for theirorganisation. Also, and it looks like he’s gone,but I was asked to thank Alistair in the booth atthe back there, who has had to tackle thevarious IT gremlins, and of course theAberdeen Conference Centre for providing thevenue.
Finally can I ask you if you could take time toprovide us with some feedback. There areforms in your pack. That would be veryuseful. Thank you very much.
Printed and published by the Health and Safety ExecutiveC0.50 1/02

OTO 2001/041
£25.00 9 780717 622603
ISBN 0-7176-2260-6