Embed Size (px)
Citation preview


I
Official Organization for Scientific Dissemination of the Escola Paulista de Enfermagem, Universidade Federal de São PauloActa Paulista de Enfermagem/ Escola Paulista de Enfermagem/ Universidade Federal de São PauloAddress: Napoleão de Barros street, 754, Vila Clementino, São Paulo, SP, Brazil. Zip Code: 04024-002Acta Paul Enferm. volume 30, issue(3), May/June 2017ISSN: 1982-0194 (electronic version)Frequency: BimonthlyPhone: +55 11 5576.4430 Extensions 2589/2590E-mail: [email protected]/ [email protected] Page: http://www.unifesp.br/acta/Facebook: https://www.facebook.com/actapaulistadeenfermagemTwitter: @ActaPaulEnfermTumblr: actapaulenferm.tumblr.com
Editorial Council
Editor-in-ChiefJanine SchirmerActa Paulista de Enfermagem - Unifesp, São Paulo-SP, Brazil
Technical EditorEdna Terezinha RotherActa Paulista de Enfermagem - Unifesp, São Paulo-SP, Brazil
Associate EditorsAriane Ferreira Machado Avelar, Escola Paulista de Enfermagem, Universidade Federal de São Paulo, São Paulo, SP, Brazil.Alexandre Pazetto Balsanelli, Escola Paulista de Enfermagem, Universidade Federal de São Paulo, São Paulo, SP, Brazil.Ana Lúcia de Moraes Horta, Escola Paulista de Enfermagem, Universidade Federal de São Paulo, São Paulo, SP, Brazil.Bartira de Aguiar Roza, Escola Paulista de Enfermagem, Universidade Federal de São Paulo, São Paulo, SP, Brazil.Dayana Souza Fram, Universidade Federal de São Paulo, Escola Paulista de Enfermagem, São Paulo, SP, BrazilEdvane Birelo Lopes De Domenico, Escola Paulista de Enfermagem, Universidade Federal de São Paulo, São Paulo, SP, Brazil.Eliana Campos Leite Saparolli, Escola Paulista de Enfermagem, Universidade Federal de São Paulo, São Paulo, SP, Brazil.Erika de Sá Vieira Abuchaim, Escola Paulista de Enfermagem, Universidade Federal de São Paulo, São Paulo, SP, Brazil.João Fernando Marcolan, Escola Paulista de Enfermagem, Universidade Federal de São Paulo, São Paulo, SP, Brazil.Manuela Frederico-Ferreira, Escola Superior de Enfermagem de Coimbra, Coimbra, PortugalMaria Magda Ferreira Balieiro, Escola Paulista de Enfermagem, Universidade Federal de São Paulo, São Paulo, SP, Brazil.Rosely Erlach Goldman, Escola Paulista de Enfermagem, Universidade Federal de São Paulo, São Paulo, SP, Brazil.Tracy Heather Herdman, University of Wisconsin, CEO & Executive Director NANDA International, Green Bay-Wisconsin, USA
Editorial BoardDonna K. Hathaway, The University of Tennessee Health Science Center College of Nursing; Memphis, Tennessee, USADorothy A. Jones, Boston College, Chestnut Hill, MA, USAEster Christine Gallegos-Cabriales, Universidad Autónomo de Nuevo León, Monterrey, MexicoGeraldyne Lyte, University of Manchester, Manchester, United Kingdom, USA Helen M. Castillo, College of Health and Human Development, California State University, Northbridge, California, USAJane Brokel, The University of Iowa, Iowa, USAJoanne McCloskey Dotcherman, The University of Iowa, Iowa, USAKay Avant, University of Texas, Austin, Texas, USALuz Angelica Muñoz Gonzales, Universidad Nacional Andrés Bello, Santiago, ChileMargaret Lunney, Staten Island University, Staten Island, New York, USAMaría Consuelo Castrillón Agudelo, Universidad de Antioquia, Medellín, ColombiaMaria Müller Staub, Institute of Nursing, ZHAW University, Winterthur, SwitzerlandMartha Curley, Children Hospital Boston, Boston, New York, USAPatricia Marck, University of Alberta Faculty of Nursing, Edmonton Alberta, CanadaShigemi Kamitsuru, Shigemi Kamitsuru, Kangolabo, Tokyo, JapanSue Ann P. Moorhead, The University of Iowa, Iowa, USA
Editorial Office Bruno Henrique Sena FerreiraMaria Aparecida Nascimento
Graphic DesignAdriano Aguina

II
Information Services
App Acta Paulista de Enfermagem
Support
Member of the Brazilian Association of Scientifi c EditorsAll content of the journal, except where identifi ed, is licensed under a Creative Commons attribution-type CC-BY.With a view tward sustainability and accessibility, Acta Paulista de Enfermagem is published exclusively in the digital format.
Completion

III
EditorialEnvironment, health & sustainability
in the context of cities
I was honored by the invitation from Acta Paulista de Enfermagem to address the theme of Environment, Health and Sustainability. The rela-tionship between this editorial and the International Nursing Day (cele-
brated in May) was also significant for me due to the comprehensive actions taken and developed by these professionals.
Both the reference global conceptual frameworks and the practical fields indicate that the current social changes are pressing researchers to consid-er other forms of conducting their investigations, including the environ-ment-health-sustainability relationship in urban contexts. Researchers need to focus on the human beings and their intrinsic relationship with environ-ment and health to better understand the new social contexts. Such focus will contribute to give effective responses to the concrete needs in the people daily life and the changing urban environment, taking into account both the sustainability principles and articulation needs, including the interdis-ciplinary concepts of knowledge production. Therefore, expanding the re-flection and discussion spaces in the academic field is necessary to deepen new analytical categories and environmental and health intervention in the urban context.
Currently, 54% of the world’s population live in big cities, where this number should reach 66% in 2050. Today, the situation is even more alarm-ing in Latin America and the Caribbean, where 80% of the population already lives in urban areas, with the perspective of increasing to 87% until 2050. This means that 650 of the 750 million people are expected to live in urban areas in this region by 2050.(1)
Furthermore, 28 megacities were formed, with more than 10 million inhabitants until today, and this number is predicted to be 41 by 2030. The metropolis of São Paulo, Mexico, and Mumbai, each one with about 21 million people, occupy the 4th place among the largest cities in the world, being exceeded only by Shanghai (23 million), Delhi (25 million), and Tokyo (38 million).(1)
In the international scenario, the decisions of the Paris Agreement (21st General Conference of the Parties, COP-21, 2015) and the Sus-tainable Development Goals (SDG) caused the urban themes to be re-assessed. An agreement has been reached with 17 SDG and 169 goals involving different issues. The discussions arising from the Millennium Development Goals (MDGs), COP-21 and SDG guidelines have already inspired a number of initiatives. They used technologies as ingredient to connect and engage both government and citizens in a common effort to rebuild, recreate, and motivate urban communities with view to the social welfare.

IV
The thematic areas of sustainability, information, vulnerability, and par-ticipatory inclusion are gaining additional relevance when contemporary urban changes are studied. This is due to factors such as the global phenom-enon of urban population growth, increasing demand for housing, mobil-ity, infrastructure, cultural and leisure equipment, environmental, health, and educational services, and new productive occupations. These factors require new responses to rethink and reorganize the urban lifestyle in the contemporary social time.
In social terms, building and developing a greater population protag-onism in decision-making processes allows to incorporate people’s knowl-edge, cultures, and longings, that open perspectives to obtain a greater con-vergence in plans, programs, projects, and activities directed to the develop-ment of cities on a sustainable basis.(2)
When dealing with the health-environment-sustainability rela-tionship in this perspective, three articles of the Constitution of the Federative Republic of Brazil (1988), concerning Urban Policy (Art. 182), Health (Art. 196), and Environment (Art. 225), are brought to consideration. Article 182 (Urban Policy) aims at “ordering the full de-velopment of the social functions in the city and ensuring the well-being of its inhabitants”. Article 196 (Health) establishes that “the universal and equal access to actions and services for health promotion, protection, and recovery is the right of all and a duty of the State”. Article 225 (Environ-ment) defines the “right to the ecologically balanced environment, which is essential to a healthy quality of life, imposing on the public power and the collectivity the duty to defend and preserve it for the present and future generations”.
In these three articles, the desire of the Brazilian constitutional legislator to leave the sustainability principles clear to the Society is perceived. The search for the well-being of its inhabitants (from the development of the social functions of the city) and consideration of their rights (universal and equal access to actions and services and the balanced environment, which are essential to the healthy quality of life of the present and future genera-tions) are emphasized in those articles.
Public policy guidelines (including environment, health, water resourc-es, conservation units, urban development, climate change, solid waste, as well as environmental crimes, education, and sanitation) were defined and established by the Brazilian Congress to move in this direction.
In view of the urban development complexity, considering the challeng-es posed by the accelerated urbanization processes (demographic growth, migration, and transition, as well as capacity for governance and governabil-ity) is necessary because they can affect improvement in the quality of life of their inhabitants. Since quality of life presupposes environmental quality, then attention should be given to the specific needs of human beings, flora, and fauna, as well as their physiological, epidemiological, and psychological mechanisms, including the general environmental needs (i.e, the necessary ecological balance). In this context, the search for quality of life (starting

V
from the virtuous relationship between environment and health) essentially requires education, work, housing, sanitation, leisure, mobility, which are considered central elements for the development with basis on sustainability.
The availability of knowledge, tools, and technologies, (such as territo-rial, environmental, and urban planning, environmental and health edu-cation, social research, environmental and health legislation, information system, monitoring, evaluation, and control) provide solid foundations for decision-making processes at all levels. They contribute to establish integrated development systems, becoming an important subsidy to meet the SDG.
While searching for economic growth with viability, eradication of pover-ty and reduction of social inequalities, and environmental and health balance concern, cities can be more and more sustainable, resilient, and adapted. “The world would not be less happy, democratic, or with less opportunities for self-realization; instead, it will be different cultivating planning, accepting the limits to human action, and seeking satisfaction in less materialistic values, so that the challenge of sustainability can be achieved”.(3) In this approach, the inherent complexity of this issue is that the development paradigm leads to a double ethical imperative: “synchronic solidarity with the present generation and diachronic solidarity with the future generations”.(4)
It should be highlighted that the social condition and human develop-ment are changed by the scientific and technological development, which reciprocally influence development. Thus, “defining the place that science and technology should occupy in a society means understanding both an important part the human condition and the development stage in which that society is”.(5) In this context, the complex and bordering nature of the theme “environment, health, and sustainability” requires interaction, interrelationship, including integration between sciences. Thus, it also re-quires competence and commitment from professionals in different fields of knowledge for a better perception of realities; consequently, greater possibil-ities for better equating problems and routing solutions will arise.
Studies conducted within this theme by Schools of Nursing have brought answers to problems and issues related to the theme of “environment, health, and sustainability”. New fields of teaching, research, and extension for health professionals were shown here, thus increasing their responsibil-ities and possibilities of contributions to the development of more fair and happy, i.e, sustainable cities and societies.
References
1. United Nations, Department of Economic and Social Affairs, Population Division (2014). World Urbanization Prospects: The 2014 Revision, Highlights (ST/ESA/SER.A/352) [Internet]. New York: United Nations; 2014. [cited 2016 Sep 7]. Available from: http://esa.un.org/Unpd/Wup/Highlights/WUP2014-Highlights.pdf.
2. Coutinho SM, Vasconcellos MP, Zancul ES, Yanase KH Lopes, RD. Contextos criativos: potencializando a institucionalização da interdisciplinaridade na graduação. In: Philippi Jr A, Fernandes V, Pacheco RC. Ensino, pesquisa e inovação: desenvolvendo a Interdisciplinaridade. Barueri (SP): Manole, 2017.

VI
3. Hogan DJ, Marandola Jr E, organizadores. População e mudança climática. Campinas, SP: NEPO/UNFP; 2010.
4. Sachs I. Caminhos para o desenvolvimento sustentável. 2a ed. Rio de Janeiro: Garamond; 2002.
5. Philippi Jr A, Fernandes V, Pacheco RC. Ensino, pesquisa e inovação: desenvolvendo a Interdisciplinaridade. Barueri (SP): Manole, 2017. Interdisciplinaridade e institucionalização: reciprocidade e alteridade.
Arlindo Philippi Jr.Civil Engineer (UFSC), Sanitary Engineer (USP), MSc in Environmen-
tal Health, PhD in Public Health (USP), Post-Doctor in Urban and Regional Studies (MIT), Livre-Docente in Environmental Policy and Management
(USP), and Full Professor (Faculdade de Saúde Pública, USP)
DOI: http://dx.doi.org/10.1590/1982-0194201700033

VII
Contents
Original ArticlesLighting impact on the emotional expression of pregnant women: a randomized clinical trialInfluência da iluminação nas expressões emocionais de parturientes: ensaio clínico randomizadoMichelle Gonçalves da Silva, Antonieta Keiko Kakuda Shimo .................................................................................................217
Validation of phone messages to promote health in people with HIVValidação de mensagens telefônicas para promoção da saúde de pessoas com HIVIvana Cristina Vieira de Lima, Marli Teresinha Gimeniz Galvão, Samyla Citó Pedrosa, Camila Aparecida Costa Silva, Maria Lúcia Duarte Pereira ......................................................................................................................................................227
Effect of Astrocaryum aculeatum (tucumã) on doxorubicin toxicity: in vivo experimental modelEfeito da Astrocaryum aculeatum (Tucumã) na toxicidade da Doxorrubicina: modelo experimental in vivoAlan Bruno Aurélio Carneiro, Eduardo Júnior Serrão Pinto, Ivagner Ferreira Ribeiro, Mayck Rian Gonçalves Magalhães, Moacir de Azevedo Bentes Monteiro Neto ..........................................................................................................................................233
Association between intensities of pain and sedation in intensive care patientsAssociação entre intensidades de dor e sedação em pacientes de terapia intensivaDaniele Cristiny da Silva, Taís Pagliuco Barbosa, Alessandra Soler de Bastos, Lúcia Marinilza Beccaria ...................................240
Nursing Education: conceptualizing a pedagogical project from the view of professorsEducação em Enfermagem: conceituando projeto pedagógico na visão de professoresSolange Maria Fustinoni Magalhães, Maria Cristina Gabrielloni, Maria Cristina Sanna, Márcia Barbieri ................................247
Hospitalizations of children for preventable conditions in the state of Parana: causes and trendsHospitalizações de crianças por condições evitáveis no Estado do Paraná: causas e tendênciaKelly Holanda Prezotto, Maicon Henrique Lentsck, Tirza Aidar, Hosanna Pattrig Fertonani, Thais Aidar de Freitas Mathias .................................................................................................................................................254
Care protocols with risk classification in pediatrics: inter-observer reliabilityProtocolo de acolhimento com classificação de risco em pediatria: confiabilidade interobservadoresFernanda Jorge Magalhães, Francisca Elisângela Teixeira Lima, Paulo César Almeida, Lorena Barbosa Ximenes, Caroline Magna Pessoa Chaves ................................................................................................................................................262
Questionnaire for assessment of HIV/AIDS control actions in the primary careQuestionário para avaliação das ações de controle do HIV/Aids na Atenção BásicaRichardson Augusto Rosendo da Silva, Révia Ribeiro Castro, Illiana Rose Benvinda de Oliveira Pereira, Sylvia Silva de Oliveira ............................................................................................................................................................271
Epidemiological profile of patients on the waiting list for renal transplantationPerfil epidemiológico dos pacientes em lista de espera para o transplante renalCamilla Maria Mesquita Batista, Rita Simone Lopes Moreira, João Luís Erbs Pessoa, Agenor Spallini Ferraz, Bartira de Aguiar Roza ............................................................................................................................................................280

VIII
Profile of accidents in children and adolescents receiving care at a public hospitalPerfil dos acidentes na infância e adolescência atendidos em um hospital públicoFernanda Rocha Fodor Filócomo, Maria de Jesus Castro Sousa Harada, Renata Mantovani, Conceição Vieira da Silva Ohara............................................................................................................................................. 287
Care planning for patients receiving palliative care in an oncology intensive care unitPlanejamento da assistência ao paciente em cuidados paliativos na terapia intensiva oncológicaDébora Cristina Leitão dos Santos, Marcelle Miranda da Silva, Marléa Chagas Moreira, Karen Gisela Moraes Zepeda, Rafael Barroso Gaspar ............................................................................................................................................................ 295
Difficulties of living with HIV/Aids: Obstacles to quality of lifeDificuldades do viver com HIV/Aids: Entraves na qualidade de vidaGiselle Juliana de Jesus, Layze Braz de Oliveira, Juliano de Souza Caliari, Artur Acelino Francisco Luz Queiroz, Elucir Gir, Renata Karina Reis ............................................................................................................................................... 301
Factors related to leisure-time physical inactivity in obese womenFatores relacionados à inatividade física no lazer em mulheres obesasTaise Santos do Nascimento, Fernanda Carneiro Mussi, Cátia Suely Palmeira, Carlos Antônio Teles Santos, Melissa Almeida Santos .......................................................................................................................................................... 308
Laryngotracheal mucosa injury and associated factors after endotracheal extubation: a pilot studyLesão de mucosa laringotraqueal e fatores associados após extubação endotraqueal: estudo pilotoAldenora Laísa Paiva de Carvalho Cordeiro, Renata Silva, Carolina Beatriz da Cunha Prado, Karoline Faria de Oliveira, Maria Helena Barbosa ............................................................................................................................................................ 316
Integrative review article
Concept analysis of nursing care management in the hospital contextAnálise conceitual da gestão do cuidado em enfermagem no âmbito hospitalarDeborah Dinorah de Sá Mororó, Bertha Cruz Enders, Ana Luisa Brandão de Carvalho Lira, Cícera Maria Braz da Silva, Rejane Maria Paiva de Menezes .............................................................................................................................................. 323

217Acta Paul Enferm. 2017; 30(3):217-26.
Original Article
Lighting impact on the emotional expression of pregnant women: a randomized clinical trial
Influência da iluminação nas expressões emocionais de parturientes: ensaio clínico randomizado
Michelle Gonçalves da Silva1
Antonieta Keiko Kakuda Shimo2
Corresponding authorMichelle Gonçalves da SilvaRua Tessália Vieira de Camargo, 126, 13083-887, Campinas, SP, [email protected]
DOIhttp://dx.doi.org/10.1590/1982-0194201700034
1Universidade Estadual de Campinas, Campinas, SP, Brazil.Conflicts of interest: there are no conflicts of interest to declare.
AbstractObjective: To identify and compare the emotional expression of pregnant women during the stage of expulsion under common and regular lighting and low lighting.Methods: Pragmatic, randomized controlled clinical trial. Ninety-five pregnant women were selected, and divided into two groups: common and regular lighting and low lighting in the delivery room.Results: The most evident emotion during the stage of expulsion is anger (33.9%). The differences between the study groups regarding the presence of emotions are significant: fear (p< 0.0001), disgust (p = 0.0091), and sadness (p = 0.0060) were more evident for the group under common and regular lighting. The group under low lighting expressed more joy (p< 0.0001) and anger (p< 0.0001). All pregnant women finished their deliveries feeling joy.Conclusion: Low lighting provides a series of emotions that respect and help women’s physiology during the stage of expulsion in labor.
ResumoObjetivo: Identificar e comparar as expressões emocionais das parturientes no período expulsivo sob iluminação comum e usual e com baixa luminosidade.Métodos: Ensaio clínico, controlado e randomizado de abordagem pragmática. Selecionado 95 parturientes, divididas em dois grupos: iluminação comum e usual e baixa luminosidade da sala de parto.Resultados: A emoção mais presente no período expulsivo é a raiva (33,9%). As diferenças entre os grupos do estudo quanto à presença de emoções são significativas: medo (p< 0,0001), nojo (p = 0,0091) e tristeza (p = 0,0060) estiveram mais presentes no grupo de iluminação comum e usual. Já o grupo de baixa luminosidade apresentou mais alegria (p< 0,0001) e raiva (p< 0,0001). Todas as parturientes terminaram seus partos com a emoção alegria.Conclusão: O ambiente com baixa luminosidade promove uma sequência de emoções que respeita e auxilia a fisiologia do período expulsivo do trabalho de parto.Universal Trial Number: U1111-1148-4976
KeywordsExpressed emotion; Lighting; Delivery
rooms; Natural childbirth; Obstetric nursing
DescritoresEmoções manifestas; Iluminação; Sala
de parto; Parto normal; Enfermagem obstétrica
Submitted November 30, 2016
Accepted May 29, 2017

218 Acta Paul Enferm. 2017; 30(3):217-26.
Lighting impact on the emotional expression of pregnant women: a randomized clinical trial
Introduction
Childbirth represents a milestone in the life of wom-en, since it has a profound effect on physical, men-tal, emotional, and social aspects. No other event in the life of a human being involving pain, emotional overload, vulnerability, possible physical damages, and even death is so complex, besides amounting to a definitive role shift, including the responsibility of taking care and promoting the development of other totally dependent human being.(1)
Environmental factors and the emotional state of pregnant women can have an impact on labor, especially during the stage of expulsion in the de-livery room. Among these factors are respect re-garding individuality/privacy, presence of a com-panion, supportive environment, presence of noise, multi-professional team care, and low lighting.(1)
The presence of steady lighting in hospitals stimulates the cerebral cortex of women in labor. According to the environmental theory of Florence Nightingale, it is not the intensity of light that is important for the binomial care, but its quality. She believed that sunlight probably did not interfere with the cortex of mothers, and that women felt comfortable with this kind of contact. Converse-ly, she claimed that artificial lights inhibit the pri-mal cortex, whereas low light stimulates it. Thus, keeping the environment as natural as possible is a care technology, taking into account that, during the stage of expulsion, women must deactivate their neocortex and activate the primitive brain in order to guarantee the hormonal balance necessary for an adequate parturition physiology.(2)
Scientific studies have been discussing the need to have a deeper understanding on the natural con-texts, based on individual emotional expressions, and challenging the old paradigm that emotion and reason are two distinct mechanisms. It can be noted that these two processes are interconnected along with the prefrontal cortex functions and the lim-bic system. Consequently, emotion has the power to influence rationality, personal relationships, mo-tor skills, and decision-making processes, which are expressed in traits, gestures and facial motricity, physiognomic and mimic aspects, speech intona-
tion, quality or intonation of gestures, and posture variations.(3)
This concern regarding how the ambiance is structured at the moment of labor is perceived by the authors by indicating that low lighting stim-ulates emotional expressions of pregnant women during the expulsive stage. Thus, women feel less observed and have their privacy preserved, with more focus and respect from the multi-professional team assisting them, which in turn facilitates the parturition process.
It was believing in this supportive parturition setting that is opposed to the childbirth institution-alization model, practiced in a technocratic man-ner, commonly applied after the second half of the 20th century by most of Brazilian maternities, and also given the lack of studies on the benefits of an environment with low lighting in the delivery room, that the researchers developed this study based on the following question: Does a delivery room set-ting with low lighting stimulate different emotion-al expressions in pregnant women compared to a common and regular lighted environment?
The objectives of the study were to identify and compare emotional expressions of pregnant women during the stage of expulsion under common and regular lighting and with low lighting.
Methods
Type of studyThis is a pragmatic, controlled, randomized, and clinical experimental trial (protocol # ReBEC: U1111-1148-4976) with the aim of conducting a clinical practice study to test the influence of light-ing in the delivery room on emotional manifesta-tions of pregnant women, applying the Facial Ac-tion Coding System (FACS).(4,5) It was carried out from February to April 2015 in the Obstetric Cen-ter of Municipal Hospital Prof. Dr. Alípio Correa Netto, located in the eastern zone of São Paulo city, state of São Paulo.
This study was preceded by the approval of the Research Ethics Committee of the State University

219Acta Paul Enferm. 2017; 30(3):217-26.
Silva MG, Shimo AK
of Campinas, with co-partnership of the Research Ethics Committee of the Municipal Health Of-fice of São Paulo (Approval no. 654.694) in accor-dance with resolution no. 466/2012 of the Nation-al Health Council, authorized by the participating healthcare institution and as per an informed con-sent form signed by the pregnant women.
Population and sampleThe study population consisted of women un-dergoing vaginal delivery and assisted, during the stage of expulsion, by 10 nurse-midwives of the Obstetrician Center at the participating in-stitution, who previously received the study ba-sic guidelines and were on duty at the moment of data collection.
This population was divided into two groups: Control Group (CG), consisting of pregnant wom-en that had vaginal delivery in a common and reg-ular setting (all lights on in the delivery room); and Intervention Group (IG), consisting of pregnant women that had vaginal delivery in a setting with low light (only surgical lights on and positioned in the lower part of the table with light beam focused on where the perineal region of pregnant women is routinely accommodated).
The study included pregnant women that met the following criteria: being over 18 years of age; having a full-term pregnancy and fetus in cephalic presentation; with no clinical and/or obstetric complications; cervical dilatation equal or lower than six centimeters at the time of hos-pital admission, presence of a companion of her choice during labor, and understanding Portu-guese language.
The study excluded women previously diag-nosed with mental illnesses, and women that expe-rienced clinical or obstetric complications during the stage of expulsion. The sample was composed after a pilot trial, initially consisting of 30 pregnant
women, and divided as follows: 15 in the CG and 15 in the IG. Three pregnant women were excluded from the study due to clinical complications during labor, totaling 27 pregnant women in the pilot trial.
In addition, a power of 80% and a significance level of 5% in the sample estimates were assumed. Taking into account the objective of comparing the control and the intervention groups in relation to the occurrence rate of “fear”, “joy”, and “anger” emotions, the remaining emotions were not in-cluded in the sample calculation because of lack of statistically significant differences. The sample size obtained by the unpaired t-student test was 14 in-dividuals per group (Table 1).
Randomization was carried out through random selection with sequentially numbered opaque envelopes containing the information on which group the pregnant women were par-ticipating. These envelopes were developed and sealed by the Statistical Office of the Unicamp Nursing School, and their content was unknown by the researcher and the patients. The infor-mation on which group they belonged was only revealed after the pregnant women had signed the informed consent form to participate in the study, and with the researcher opening the enve-lope during labor.
InterventionIn the first contact with the pregnant women (time of admission or during stay in the prenatal, respect-ing the cervical dilatation equal or lower than 6 cm criterion), the purpose of the study was explained, including the shooting of their face during child-birth, as well as the request to sign the consent form and the opening of the randomization envelope, considering the delivery room lighting as the in-tervention proposed and applied, and the facial ex-pressions coded according to the results found from this intervention.
Table 1. Mean, standard deviation, alpha, and power values and number of pregnant women suggested for composing the sample according to fear, joy, and angerVariable Contr Mean Contr Standard Deviation Exp Mean Exp Standard Deviation Alpha Power n/group
Fear 30.17 11.53 2.80 2.70 0.05 0.80 4
Joy 21.58 5.14 29.20 8.19 0.05 0.80 14
Anger 24.58 11.77 50.73 12.76 0.05 0.80 5

220 Acta Paul Enferm. 2017; 30(3):217-26.
Lighting impact on the emotional expression of pregnant women: a randomized clinical trial
Facial image capture: regardless of the light-ing chosen for the delivery room after random-ization (CG or IG), an Aiptek Go HD Blue with 720pTM camcorder was used, duly approved by Inmetro, and specific for capturing precise im-ages in a poorly lit setting. The camcorder was held by the researcher, who was positioned next to the gynecological table for adequate shoot-ing and visualization of the facial image of the pregnant women during the stage of expulsion in both study situations, assuming the possibility of causing some embarrassment to the pregnant women. However, during data collection, this possibility of embarrassment was not an issue as expressed verbally by all the pregnant women immediately after giving birth, who denied hav-ing had such a feeling, since they were aware of the study and, during childbirth, they did not even notice the shooting because of the particu-lar intense moment they were experiencing.
The camcorder was turned on at the moment the nurse-midwife entered the delivery room, and it was turned off after placenta abruption, varying the intervention exposure time since each woman had a different time of expulsion.
The nurse-midwives on duty at the time of data collection received basic instructions on the pur-pose of the study and previous training regarding the institutional protocol for conducting the preg-nant women to the delivery room during the stage of expulsion only (full dilatation, fetal presentation higher than +1 of De Lee plan, and presence of in-voluntary bearing-down efforts).
Variables• Independent: delivery room lighting;• Dependent: facial expressions of pregnant
women, classified according to the FACS, such as: fear, joy, anger, sadness, surprise, and dis-gust;
• Characterization: age, school level, parity, preparation for childbirth, marital status, eth-nicity, use of oxytocin during labor and child-birth, duration of expulsion, acceptance of pregnancy, skin-to-skin contact, and Apgar score.
Data analysisFor ensuring proper reading of the facial expres-sion coding and the recognition of real emo-tions, one of the researchers decided to study the FACS, obtaining the entire system from its creators. This in-depth study on facial coding re-quired intense dedication that took more than one year of study. After all the knowledge ac-quired, the researcher took an International Paul Ekman Group test on the skills of facial move-ment coding and emotions in December, 2014. After passing the test, she became the first Bra-zilian official FACS facial encoder, making vi-able this research and, thus, guaranteeing data analysis accuracy.
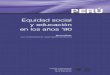
The FACS breaks down facial actions into small units called “action units”, in which each unit rep-resents an individual muscle action or an action of a small group of muscles in a recognizable facial expres-sion (Figure 1). In total, the classification of 66 action units, combined after comparisons and corrections of specific scores by FACS Score Checker software, can generate six well-defined expressions of facial emo-tions: fear, joy, disgust, sadness, and surprise, regard-less of cultural differences (Charts 1 and 2).(4,6)
Figure 1. Schematic representation of the FACS measurement units

221Acta Paul Enferm. 2017; 30(3):217-26.
Silva MG, Shimo AK
Data were analyzed and coded in a two-step procedure:
Step A: evaluation and coding of images cap-tured from emotion manifestations of pregnant women (mean of four codes per image second), based on the Facial Action Coding System.
Step B: coding comparison and correction car-ried out by the researcher using a comparative anal-ysis of the facial images watching the videos and assuring the proper interpretation of the emotions through the FACS Score Checker software,(4) which allowed the researcher to refer to the final coding of the image under evaluation and compare this coding with an image provided by the software database.
Results
The Control Group was comprised of 46 pregnant women, and the Intervention Group of 54 pregnant
Chart 1. Action units (AUs) according to facial muscle actions, based on the FACSAU Facial muscle action
Upper face
1 Inner brow raising
2 Outer brow raising
4 Brow lowering
5 Upper eyelid raising
6 Cheek raising
7 Eyelid tightening
43 Eyes closed
45 Blinking both eyes
46 Winking one eye
Lower face
9 Nose wrinkling
10 Upper lip raising
11 Nasolabial deepening
12 Lip corner pulling
13 Intense lip corner pulling
14 Dimple
15 Lip corner depressing
16 Lower lip depressing
17 Chin raising
18 Lip puckering
20 Lip stretching
22 Lip funneling
23 Lip tightening
24 Lip pressing
28 Lip sucking
Head movements
51 Head turn left
52 Head turn right
53 Head up
54 Head down
55 Head tilt left
56 Head tilt right
57 Head forward
58 Head back
Eye movements
61 Eyes turn left
62 Eyes turn right
63 Eyes up
64 Eyes down
65 Each eye looking to an outer side
66 Eyes looking in
Lip parting and jaw opening
25 Lip parting
26 Jaw dropping
27 Mouth stretching
Other AUs
8 Lips toward each other
19 Tongue showing
21 Neck tightening
29 Jaw thrusting
30 Jaw sideways
31 Jaw clenching
32 [Lip] biting
33 [Cheek] blowing
34 [Cheek] puffing
35 [Cheek] sucking
36 [Tongue] bulging
37 Lip wiping
38 Nostril dilation
39 Nostril compression
Source: Ekman et al., 2002 and Ekman&Friesen, 1978
Chart 2. Emotions according to key combinations of Action Units (AUs) and their main variations, based on the FACSEmotion AU combination Main variations
Surprise 1+2+5B+26 1+2+5B
1+2+5B+27 1+2+26
1+2+27
5B+26
5B+27
Fear 1+2+4+5*+20+25,26 or 27 1+2+4+5*+L or R20*+25,26 or 27
1+2+4+5*+25,26 or 27 1+2+4+5*
1+2+5Z, with or without 25,26,27
5*+20* with or without 25,26,27
Joy 6+12*
12C/D
Sadness 1+4+11+15B with or without 54+64 1+4+11 with or without 54+64
1+4+15* with or without 54+64 1+4+15B with or without 54+64
6+15* with or without 54+64 1+4+15B+17 with or without 54+64
11+17
25 or 26 can occur with all AU combinations or with main variations.
Disgust 9
9+16+15,26
9+17
10*
10*+16+25,26
10+17
Anger 4+5*+7+10*+22+23+25,26 Any combination of AUs without any of the following AUs: 4,5,7 or 10
4+5*+7+10*+23+25,26
4+5*+7+23+25,26
4+5*+7+17+23
4+5*+7+17+24
4+5*+7+23
4+5*+7+24
Source: Ekman et al., 2002 and Ekman&Friesen, 1978

222 Acta Paul Enferm. 2017; 30(3):217-26.
Lighting impact on the emotional expression of pregnant women: a randomized clinical trial
Analyzing the results of all pregnant women, none received orientation for childbirth and all verbally expressed accepting the pregnancy. Most of the participants (43 = 45.2%) had brown skin and 65 (68.4%) had a partner. Regarding child-birth with use of synthetic oxytocin, most did not use this medication (59 = 62.1%) and 81 (85.2%) of the births benefited from skin-to-skin contact. The differences between the study groups related to presence of emotions are shown in table 3.
During the coding process, it was noted that, in both groups, emotions followed a line of ap-pearance and concentration. For better assessing this distribution, the coding and results were di-vided into six alternating sequences of emotions. However, some of the pregnant women showed five periods of emotion. Evaluating the sequen-tial order of appearance and predominance of emotions during the evolution of the stage of
expulsion and comparing CG with IG, it was possible to analyze the p-value through the chi-squared test and Fisher’s exact test, as presented in table 4.
women, totaling n = 95, higher than the requested for the sample calculation (14 pregnant women per group), however of great value in terms of statisti-cal calculations and accuracy of the results. Table 2 shows the overall characteristics of the participants and the main quantitative evaluations of the study, according to the variables age, school level, parity, cervical dilation at admission, first- and fifth-min-ute Apgar, and prevalence of six emotions.
Table 3. Frequency of emotions between control and intervention groupsEmotion Group n Mean Standard deviation p-value*
Fear Control 46 34.33 10.63 < 0.0001
Intervention 49 7.33 10.43
Joy Control 46 21.70 5.36 < 0.0001
Intervention 49 27.73 8.63
Anger Control 46 21.50 10.38 < 0.0001
Intervention 49 45.71 16.26
Disgust Control 46 4.13 4.36 0.0091
Intervention 49 1.88 2.66
Sadness Control 46 2.57 2.81 0.0060
Intervention 49 1.29 3.04
Surprise Control 46 15.13 7.18 0.4814
Intervention 49 16.08 7.16
*p-value obtained through Mann-Whitney testTable 2. Distribution of study variables and presence of emotions in the total amount of deliveries, according to quantitative analysisVariables n Mean Standard deviation
Age 95 26.52 7.48
School level 95 8.82 2.51
Previous pregnancies 95 2.95 2.22
Previous vaginal deliveries 95 1.42 1.88
Previous abortions 95 0.34 0.74
Cervical dilation at admission 95 4.82 1.02
Time of expulsion 95 16.92 10.58
1st min Apgar 95 8.55 0.71
5th min Apgar 95 9.65 0.50
Fear 95 20.40 17.13
Joy 95 24.81 7.81
Anger 95 33.99 18.29
Disgust 95 2.97 3.74
Sadness 95 1.91 2.99
Surprise 95 15.62 7.14
n=95
Table 4. Comparison of the sequence of emotions related to the progression of the stage of expulsion, according to the control and intervention groups
Time/Emotion
Group
p-valueControl Intervention
n(%) n(%)
Emotion 1 0.1010**
Fear 35(76.09) 30(61.22)
Disgust 5(10.87) 7(14.29)
Surprise 1(2.17) 8(16.33)
Sadness 5(10.87) 4(8.16)
Emotion 2 0.0277*
Fear 8(17.39) 9(18.37)
Disgust 11(23.91) 6(12.24)
Anger 3(6.52) 9(18.37)
Surprise 12(26.09) 21(42.86)
Sadness 12(26.09) 4(8.16)
Emotion 3 0.0022**
Joy 1(2.17) 8(16.33)
Fear 2(4.35) 0(0.00)
Disgust 14(30.43) 5(10.20)
Anger 13(28.26) 20(40.82)
Surprise 10(21.74) 15(30.61)
Sadness 6(13.04) 1(2.04)
Emotion 4 0.0016**
Joy 14(31.11) 20(48.78)
Disgust 1(2.22) 0(0.00)
Anger 12(26.67) 17(41.46)
Surprise 18(40.00) 3(7.32)
Sadness 0(0.00) 1(2.44)
Emotion 5 0.0009**
Joy 8(25.81) 16(76.19)
Anger 18(58.06) 3(14.29)
Surprise 5(16.13) 2(9.52)
Emotion 6
Joy 23(100.00) 5(100.00)
*p-value obtained through the chi-squared test; **p-value obtained through Fisher’s exact test

223Acta Paul Enferm. 2017; 30(3):217-26.
Silva MG, Shimo AK
Analyzing the emotional manifestations of the studied groups in relation to the marital sta-tus of the pregnant women, statistically signifi-cant differences were noticed, whereas 65 preg-nant women reported having partners. When ad-dressing the conduction of the delivery, it always comes to mind the common and regular issue raised by professionals in the field of obstetrics: that the infusion of synthetic oxytocin speeds up labor. However, the data assessed through the Mann-Whitney test showed a contradiction of this routine practice carried out at maternities, and that its use during the stage of expulsion pro-longs birth in almost six minutes, with a statisti-cal relevance of p = 0.0210.
Discussion
This research sought to study the impact of lighting in the delivery room on the emotional expressions of pregnant women. Since similar studies were not found, data discussion was carried out considering major international studies as reference for emotion coding and how the six analyzed emotions are orga-nized in our body. Furthermore, studies conducted by physiologists dealing with the impact of lighting on human beings were also sought.
The difficulty found was that all studies related to the assessment of women’s emotions during the pregnant-puerperal cycle are qualitative in nature, guided by verbalizations of women, thus hampering the comparison with this study.
Analyzing the results on the school level of the pregnant women, there was an attempt to establish the differences in the type of emotion showed along with educational training throughout their lives, considering previously the assumption that the higher the school level, the tougher would be the labor, due to the activation of maternal neocortex of intellectual activity when compared to a higher lev-el of education. However, the findings of the study did not show statistically significant differences be-tween these relationships, because the low school-ing level of the pregnant women in the study (mean of 8.8 years) made this comparison difficult.(1)
The mean time of 16.9 minutes in the stage of expulsion was not considered relevant, since labors were carried out by different professionals, each one having a particular way of referring the prena-tal pregnant women to the delivery room, despite pre-established training and institutional protocols. There are professionals that only refer pregnant women with total dilation, fetal presentation high-er than +1 of DeLee plan, and involuntary bear-ing-down efforts, whereas others refer them at the earliest possible stage.
Among the six analyzed emotions, “fear” is the most scientifically well-established emotion due to several studies conducted on this topic, probably because it is easy to arouse it with threats of physical or psychological damages, and because it is possible to learn to feel fear of almost anything. Thus, there are qualitative studies in which women strongly verbalize their fear of transition that this moment offers, of the new social role they will assume as mothers, that things might go wrong, fear of death, fear of their child not being totally healthy, fear of not being capable to give birth, fear of not being well-treated and respected and, finally, fear of the greatest worry cast by our Brazilian “Cesareanistic” culture: fear of pain.(7-11)
Fear was present on an average of 20.4% of pregnant women, whereas 100% of women ex-pressed not having received previous orientation or preparation for the labor and childbirth, which un-fortunately could be characterized as an inadequate prenatal care(12), thus favoring the exacerbation of this emotion during childbirth.
In contrast to “fear”, “joy” is the least studied emotion, probably because almost all studies are ded-icated to disturbing emotions that concentrate their worries on the problems, and also probably because the healthcare field puts more value towards the cura-tive aspects, that is, solving problems and forgetting to put an emphasis on what is pleasant.(11)
Among qualitative studies, women that became mothers expressed intense joy for conceiving a child and saw, despite the pain, how childbirth brings a pleasant reward, which is the fulfillment of a dream come true of “becoming a mother”, especially with the arrival of a healthy child, the support received

224 Acta Paul Enferm. 2017; 30(3):217-26.
Lighting impact on the emotional expression of pregnant women: a randomized clinical trial
from her partner and, finally, the formation or ex-pansion of the social unit called family.(8,13-15)
The “anger” emotion, by its turn, is widely stud-ied in studies addressing mental disorders and any type of violence. On the other hand, when analyz-ing studies in the field of obstetrics, this emotion is only described in qualitative studies on obstet-ric violence, reaching the conclusion that pregnant women were unsatisfied with the care they received during childbirth.(7,16-18)
Ekman & Rosenberg(11) claim that “anger” con-trols, punishes, and retaliates. Thus, how can we imagine “anger” as the most present emotion in all childbirths in this study? How can childbirth be so-cially exclamatory for being rewarding and joyful, but generate an emotion of dissatisfaction?
This triad of anger that controls, punishes, and retaliates(11) may be better understood through stud-ies on primal health, which evidenced this emotion as the most primitive of human beings, from the beginning of time of the cavemen era.(1,18,19)
Considering that humanity is only possible thanks to the primal and physiological event of childbirth, since nobody is born otherwise, the as-sociation that childbirth involves “anger” can be made. For a woman to physiologically consent her child to be born, she needs to rescue her animal side, the mammalian that exists within her body, regard-less of her intellectual evolution. Namely, “anger”, as a primal emotion, controls the childbirth phys-iology, to the extent that, due to its intensity, “an-ger” filters and even prevents the suffering caused by neocortical interferences.(1)
As punishment, “anger” causes pain, the pain that uterine contractions generate by releasing oxy-tocin and, in its turn, “anger” retaliates making the women expel the child out of themselves. Accord-ing to these studies on emotions and primal health, it is possible to understand “anger” as the key trig-ger for the labor stage of expulsion.(1,11)
When analyzing the most frequent emotions in each study group, data revealed that, in the CG, the most predominant emotions were “fear” (p < 0.0001), “sadness” (p = 0.0060), and “disgust” (p = 0.0091). As for the IG, the most predominant were “joy” (p < 0.0001) and “anger” (p < 0.0001). How-
ever, the “surprise” emotion was equally presented in both groups, with averages of 15.13% in the CG and 16.08% in the IG.
These results show that lighting in the delivery room stimulates the emergence of different types of emotions according to its intensity, although the six emotions assessed were present in almost all deliveries.
Within a psychoanalytic approach, a literature review on the impact sadness has on adults revealed and concluded that sadness is passive and the indi-vidual involved in this emotion is actually asking mentally and involuntarily to be helped and com-forted. Therefore, bringing this information to the obstetric practice under study, the association of sadness being more present in the CG may have been caused by higher exposure of the pregnant women to intense lighting in the delivery room, which physiologists claim to be a source for better evaluation, and which most part of human beings, when feeling monitored and evaluated, tend to act differently.(1,2,7,19-21)
In its turn, “disgust” is the only emotion on which all specialists in the cognitive field have reached a consensus. It is a learned emotion, not inherent to the primal cortex, possibly developed from four years of age on, and influenced by the culture to which each person belongs.(11,19,22)
It is not just about taste, smell and touch, or an idea, a vision or a sound that could cause “disgust”, but actions and physical appearances as well. Roz-in et al.(23) found that the most powerful universal triggers for the “disgust” emotion are bodily waste products: feces, vomit, urine, mucous, and blood, plus morally pervert social situations, such as por-nography and sexual activity.
When evaluating this emotion more present in the CG, lighting can be associated with mind acti-vation and, consequently, the awareness of the preg-nant women regarding their own blood, feces, urine, and vomit. These excretions are socially learned as disgusting and the pregnant women may awaken to the scene in which they have been submitted: naked from the waist down, in gynecological position, one or more observers in front of them (professional as-sisting the childbirth), watching the gloved hands

225Acta Paul Enferm. 2017; 30(3):217-26.
Silva MG, Shimo AK
covered with blood from nurse-midwives, feeling the smell of their own excretions. In addition, they be-come aware that their companion, who is generally the partner, and all of those present might be watch-ing and experiencing that situation as well.
Qualitative studies also evidenced pregnant women talking about frequent obstetric-gyneco-logical examinations that are still very present in this institution during the stage of expulsion. Dis-gust can also be unleashed through the perception of the pregnant women, facing the intensity of light in the delivery room, in which digital pelvic examination may lead to the sensation that she has been degraded, especially in this singular moment that is childbirth.(7,17,24,25)
Against the most prevalent emotions in the CG, and also despite the presence of “fear”, “sadness”, and “disgust”, the IG was characterized by higher exacerbation of “joy” and “anger” emotions. The main determinant may be the fact that the low light setting promoted privacy with the activation of the primal cortex, releasing endorphins and oxytocin and, as a result, inhibiting the synapses in the neo-cortex and the release of adrenaline.(1,21,26)
These facts demonstrate that the presence of “anger” and its essence throughout labor and during the stage of expulsion has been characterized as the key trigger for the stage of expulsion, due to the pri-mal strength nature of this emotion.(11) “Joy” can be associated with the pleasant emotion driven by the arrival of the baby, a dream come true, the patient feeling respected, and having the benefit of privacy provided by the low light setting, which promotes better physiology of the childbirth.(1,2)
It is a consensus among specialists that “sur-prise” is the briefest of all emotions. It lasts only a few seconds. Therefore, “surprise” lasts while there is an understanding of what is going on and, after that, it gets mixed with other emotions.(3,11)
The striking point in our results was the statis-tical consistency related to the appearance of “sur-prise” in both groups, as a very singular characteris-tic: it serves as a trigger to unchain “anger” in both groups. There is only a time gap from its appearance in the stage of expulsion, as in CG it is present in emotion time 4 and in IG in emotion time 2.
Regarding the six times that emotions appeared, the study assessed that CG was characterized for showing a higher concentration of emotions in the following order: “fear”, “surprise/fear”, “disgust”, “surprise”, “anger”, and “joy”; whereas IG evidenced the following order: “fear”, “surprise”, “anger”, “joy”, “joy”. “Joy” obtained statistical significance for time 2 (p = 0.0277), time 3 (p = 0.0022), time 4 (p = 0.0016), and time 5 (p = 0.0009).
With these findings, low light settings may be linked to the promotion of a more physiological se-quence of emotions, since there is the initial appear-ance of “fear”, which is common to someone who is about to experience an intense moment, such as a childbirth, and because of all the characteristics already mentioned about this emotion, followed by “surprise”, which is a transition emotion for the third emotion, “anger”. This is the one in this study regarded as the trigger for expelling out the baby. Next, “joy” is more concentrated as an emotion in stage time 4, 5, and 6.
The environment with common and regular lighting, widely practiced, promotes the appear-ance of a more disturbed sequence of emotions. “Fear” comes first, although without statistical sig-nificance when compared to IG, it lingers more than expected, reaching time 2 of emotions, next to “surprise”, which is the transition to “anger”. Yet, this transition is blocked by the appearance of “disgust”, probably due to mind activation and what is socially accepted and pleasant. Nev-ertheless, as labor evolves, the “surprise” emotion appears again, making the transition to “anger”, which accomplishes its role as the trigger for expel-ling out the baby, and “joy” settles in closing the emotion times.(3)
In this study, it was possible to show that 100% of the deliveries finished expressing the emotion of “joy”. Despite its quantitative na-ture, the results of this study corroborated the qualitative studies in the scientific scenario, which showed phrases expressing satisfaction when the pregnant women see their babies for the first time, in skin-to-skin contact, being able to breastfeed, and acknowledging that all the ef-fort and intensity of pain were worthwhile.(27)

226 Acta Paul Enferm. 2017; 30(3):217-26.
Lighting impact on the emotional expression of pregnant women: a randomized clinical trial
Conclusion
All six emotions (fear, joy, anger, disgust, sadness, and surprise), intentionally put into evaluation, were identified during the stage of expulsion in the delivery room. It has been shown that a low light setting promotes a sequence of emotions that re-spect and help the physiology of the labor expulsion (fear, surprise, anger, and joy). An environment with common and regular lighting suffers interfer-ence in the sequential appearance of emotions, dis-rupting the physiological process during expulsion (fear, fear/surprise, disgust, anger, and joy).
CollaboratorsSilva MG and Shimo AKK contributed to the proj-ect conception, data analysis and interpretation, manuscript writing, relevant critical review of its intellectual content, and final approval of the ver-sion to be published.
References
1. Odent M. A cientificação do amor. 2a ed. Florianópolis: Saint Germain; 2002.
2. Macedo PO, Quitete JB, Lima EC, Santos I, Vargens OM. As tecnologias de cuidado em enfermagem obstétrica fundamentadas pela teoria ambientalista de Florence Nightingale. Esc Anna Nery Rev Enferm. 2008; 12(2):341-7.
3. Ekman P. A linguagem das emoções. São Paulo: Lua de Papel; 2011.
4. Ekman P, Friesen WV, Hager JC. Facial Action Coding System [CD-ROM]. Arizona: Published by A Human Face; 2002.
5. Schulz KF, Altman DG, Moher D and the CONSORT Group. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. Trials. 2010;11:32.
6. Ekman P, Friesen WV. The facial action coding system: A technique for the measurement of facial movement. Consulting Psychologists Press Inc. Sao Francisco, CA, 1978.
7. Hodnett ED, Gates S, Hofmeyr GJ, Sakala C. Continuous support for women during childbirth. Cochrane Review The Cochrane Library, Issue 10. Update Software, Oxford; 2012.
8. Tostes NA, Seidl EM. Expectativas de gestantes sobre o parto e suas percepções acerca da preparação para o parto. Temas Psicol. 2016; 24(2):681-93.
9. Antunes JT, Pereira LB, Vieira MA, Lima AL. Presença paterna na sala de parto: expectativas, sentimentos e significados durante o nascimento. Rev Enferm UFSM. 2014; 4(3):536-45.
10. Larsson BW, Bojo AKS, Starrin B, Larsson G. Birthgiving women’s feelings and perceptions of quality of intrapartal care: anationwide Swedish cross-sectional study. J Clin Nurs. 2011; 20(7-8):1168-77.
11. Ekman P, Rosenberg EL. What the face reveals: basic and applied studies of spontaneous expression using the facial action coding system (FACS). 2ª ed. New York: Oxford University Press; 2005.
12. Brasil. Ministério da Saúde. Agência Nacional de Saúde Suplementar. O modelo de atenção obstétrica no setor suplementar de saúde no Brasil: cenários e perspectivas. Brasília (DF): Ministério da Saúde; 2008.
13. Guittier MJ, Cedraschi C, Jamei N, Boulvain M, Guillemin F. Impact of mode of delivery on the birth experience in first-time mothers: a qualitative study. BMC Pregnancy Childbirth. 2014 Aug 1; 14:254.
14. Velho MB, Santos EK, Collaço VS. Parto normal e cesárea: representações sociais de mulheres que os vivenciaram. Rev Bras Enferm. 2014; 67(2):282-9.
15. Ekman P, Friesen WV. Pictures of facial affect. Palo Alto, CA: Consulting Psychologists Press; 1976.
16. Maia MB. Humanização do parto: política pública, comportamento organizacional e ethos profissional. Rio de Janeiro: Fiocruz; 2010.
17. Dip A. Na hora de fazer não gritou. Agência de Reportagem e Jornalismo Investigativo [Internet]. 2012 [citado 2013 mar 25]. Disponível em: http:// www.apublica.org/2013/03/na-hora-de-fazer-nao-gritou.
18. Spiteri MC, Jomeen J, Martin CR. Reimagining the General Health Questionnaire as a measure of emotional wellbeing: A study of postpartum women in Malta. Women Birth 2013 Dec; 26(4):e105-11.
19. Vingersgoets AJ, Cornelius RR, Heck VG, Becht MC. Adult crying: a model and review of the literature. Rev Gen Psychol. 2000; 4(4):354-70.
20. Logomarsino BS, van der Sand IC, Perlini NM, Linck CL, Ressel LB. A cultura mediando preferências pelo tipo de parto: entrelaçamento de fios pessoais, familiares e sociais. Rev Min Enferm. 2013; 17(3):680-7.
21. Leboyer F. Nascer sorrindo. 14a ed. São Paulo: Editora Brasiliense; 1992.
22. Nussbaum M, Secret sewers of vice: disgust, bodies, and the law,. In: Bandes AS. editor. The passions of law. New York: University Press; 1999.
23. Rosin P, Haidt J, McCauley CR. Disgust: the body and soul emotion. Cognit Emotion. 1999; 22: 435-8.
24. Venturi W, Bokany V, Dias G, Alba D, Rosas W, Figueiredo N. Mulheres brasileiras e gênero nos espaços públicos e privado. Fundação Perseu Abramo e SESC [Internet]. 2010 [citado 2013 Mar 21]. Disponível em: http://novo.fpabramo.org.br/ sites/default/files/pesquisaintegra_0.pdf.
25. World Health Organization (WHO). Care in normal birth: a practical guide [Internet]. Bull Word Health Organ; 2012 [cited 2013 Sept 8] Available from: http://www.who.int/maternal_child_adolescent/documents/who_frh_msm_9624/en.
26. Lelis AL, Cardoso MU, Farias LM, Lelis AL, Farias LM, Cipriano MA, Cardoso UM, Galvão MT, Caetano JÁ. Cuidado humanístico e percepções de enfermagem diante da dor do recém-nascido. Esc Anna Nery. 2011; 15(4):694-700.
27. Brasil. Ministério da Saúde. Manual prático para implementação da rede cegonha. Brasília (DF): Ministério da Saúde; 2011.

227Acta Paul Enferm. 2017; 30(3):227-32.
Original Article
Validation of phone messages to promote health in people with HIV
Validação de mensagens telefônicas para promoção da saúde de pessoas com HIV
Ivana Cristina Vieira de Lima1
Marli Teresinha Gimeniz Galvão1
Samyla Citó Pedrosa1
Camila Aparecida Costa Silva1
Maria Lúcia Duarte Pereira2
Corresponding authorIvana Cristina Vieira de LimaAlexandre Baraúna street, 1115, 60430-160, Fortaleza, CE, [email protected]
DOIhttp://dx.doi.org/10.1590/1982-0194201700035
1Universidade Federal do Ceará, Fortaleza, Ceará, Brazil.2Universidade Estadual do Ceará, Fortaleza, Ceará, Brazil.Conflicts of interest: there are no conflicts of interest to declare.
AbstractObjective: To evaluate the opinion of experts about the content of phone messages to promote health in people with HIV.Methods: Methodological development study to validate 10 phone messages, with participation of 11 experts that assessed their clarity and relevance. The content validity index of each phone message was calculated and a minimum concordance of 75% was established.Results: The messages were considered clear (79.1%) and very relevant (98.2%). The general content validity index was 0.98. Main suggested alterations: inclusion of a series of short questions about the subject at the beginning of every message; adjustment to a simpler and more interactive language; replacement of specific terms and exclusion of words or expressions related to HIV.Conclusion: The experts considered the messages clear and relevant to promote health in people with HIV.
ResumoObjetivo: Avaliar a opinião de experts sobre o conteúdo de mensagens telefônicas para a promoção da saúde de pessoas vivendo com HIV.Métodos: Estudo de desenvolvimento metodológico direcionado à validação de dez mensagens telefônicas, com participação de 11 experts que avaliaram sua clareza e grau de relevância. O índice de validade de conteúdo relativo a cada mensagem foi calculado e estabeleceu-se uma concordância mínima de 75%.Resultados: Foram consideradas mensagens claras (79,1%) e muito relevantes (98,2%). O índice de validade de conteúdo geral foi 0,98. Principais alterações sugeridas: inclusão de um questionamento sobre o tema no início de cada mensagem; adequação para uma linguagem mais simples e interativa; substituição de termos específicos e exclusão de palavras ou expressões relacionadas ao HIV.Conclusão: Os experts consideraram as mensagens claras e relevantes para a promoção da saúde das pessoas vivendo com HIV.
KeywordsHIV; Text messaging; Communication;
Health promotion; Validation studies
DescritoresHIV; Mensagem de texto; Comunicação;
Promoção da saúde; Estudos de validação
Submitted December 16, 2016
Accepted June 5, 2017

228 Acta Paul Enferm. 2017; 30(3):227-32.
Validation of phone messages to promote health in people with HIV
Introduction
Considering the stigma associated with the in-fection, the emotional repercussions of living with the virus, and the incipient social support received after the diagnosis,(1) it is a challenge to promote health in people living with HIV/AIDS (PLWHA). To reach effective results in clinical practice, the healthcare team needs tools that strengthen ties and potentialize health educa-tion, with the aim of maintaining the client’s au-tonomy and offering resources to appropriately manage the health condition.(2)
The use of information and communica-tion technologies focused on promoting health in PLWHA is considered promising for allowing support to self-care, incentives to the adoption of healthy habits, sharing of information, and emo-tional support. The telephone stands out as one of the most prominent technologies; it can be used to make phone calls and send messages with proven efficacy regarding adhesion to the treatment and a good cost-benefit ratio.(3)
Text messages with an emphasis on health education have advantages over phone calls, be-cause the former can be read quickly, at any time and anywhere, and do not require much effort by the clients or the professionals sending the message.(4) Evidence points to the positive use of Short Message Service (SMS) to send text mes-sages to boost health habits among clients with chronic conditions.(5-8)
With the expanded use of the Internet, smart-phone apps such as WhatsApp Messenger have po-tentialized instant communication between client and professional regarding health communication, with a variety of resources of interaction,(9) increas-ing the possibilities of the use of text messages in health care.
The use of technologies to promote health in PLWHA is fundamental to improve the immune system, prevent comorbidities, boost quality of life, and stimulate adhesion to the treatment. However, these tools must be properly developed and validated to assure their efficacy and accep-tance by the target audience.(10) Studies with
this focus may offer professionals and research resources to increase access to healthcare educa-tional actions in the context of this important chronic condition.
Taking this into account, the objective of the present study was to evaluate the opinion of experts about the content of phone messages to promote health in PLWHA.
Methods
The present study was methodological and de-velopmental in nature, and carried out in August 2016 with the participation of 11 experts. “Ex-pert” is defined as a professional that has great knowledge and skills in clinical practice, teach-ing, or research, with recognition in their field.(11) The present study was the initial step in an experimental research project to assess the effects of phone calls sent by WhatsApp to promote health in PLWHA.
The phone messages were designed according to the guidelines described in national manuals about assistance to PLWHA(12-15) and addressed the following subjects: adhesion to antiretroviral therapy; physical activity; social support; self-es-teem; anxiety and depression; dietary habits; pre-ventive behavior; and sexuality. Two additional messages were also evaluated, one concerning the presentation of the phone monitoring and another one about its ending.
The experts were selected through intentional and convenience sampling. The participants had to meet at least two of the following inclusion criteria: to have a master’s or PhD in the health area; to have published papers about care to PLWHA; to be part of research groups or projects about this subject; to be a professor in a health school and teach about as-sistance to PLWHA; and to have professional expe-rience in HIV/AIDS reference hospitals or clinics.
Selection of potential participants was per-formed with the information available at Lattes Platform, from the National Council for Scientific and Technological Development. Thirteen profes-sionals were chosen. After an invitation by phone

229Acta Paul Enferm. 2017; 30(3):227-32.
Lima IC, Galvão MT, Pedrosa SC, Silva CA, Pereira ML
call and/or e-mail, 11 experts expressed their in-terest in contributing to the validation. Thereafter, they received the free and informed consent form, the expert characterization form, and the phone messages and validation instrument by e-mail, and were informed that they had 15 days to send the evaluation back.
The evaluation instrument was used to investi-gate the perception of the expert regarding the clar-ity and relevance of the messages. The former was assessed through dichotomous items, such as yes or no, and the latter was analyzed through a Likert scale with the options: irrelevant; slightly relevant; and very relevant. The instrument had a field for inclusion of considerations and suggestions.
The information gathered through the ap-plication of the evaluation instrument was or-ganized by the software Excel for Windows and analyzed with the Content Validity Index (CVI), which consists in the measure of the proportion of experts that agree on the evaluation of the messages.(16) The CVI value was calculated using three equations: S-CVI/Ave (mean of the content validity indexes for all the messages); S-CVI/UA (proportion of evaluated items that reach a score of 3-very relevant-unanimously); and I-CVI (content validity index for individual items).(17) It was established that a CVI of at least 0.90 was necessary for the messages to achieve excellence in their validity.(18)
In addition, the percentage of general agree-ment regarding the clarity of the messages was assessed through the application of the formula: number of items with the answer yes shared by the total number of evaluated items and multi-plied by 100. The minimum agreement rate was set as 75%.(16)
The research project was approved by the Re-search Ethics Committee from the Federal Univer-sity of Ceará (report 1.482.508).
Results
All of the experts were females, with ages be-tween 26 and 57 years (38.1 years old, on av-
erage); there were 10 nurses and one medical doctor. Their graduate time varied from 4 to 32 years (14.8 years, on average). Four participants had a master’s degree, six had a PhD, and one had a post-doctoral degree. All of them had been members of research groups, seven had around 10 years of experience as professors and eight had on average 11.6 years of clinical experience in as-sisting PLWHA.
Table 1 shows the phone messages and the ex-perts’ opinions on their clarity. Half of the texts had an agreement percentage higher than 75%, but the message about anxiety and depression reached the lowest value (63.6%). All of the messages with an agreement percentage lower than 75% were changed according to the experts’ suggestions. It is important to stress that every message started with the greeting “Hello/Good morning/Good after-noon/Good evening!” The average number of char-acters in each message was 298.
Table 1. Experts’ evaluation regarding the clarity of the phone messages
Subject
Clarity evaluation
Yes No
n(%) n(%)
Presentation of the monitoring 10(90.9) 1(9.1)
Adhesion to antiretroviral therapy 8(72.7) 3(27.3)
Physical activity 8(72.7) 3(27.3)
Social support 10(90.9) 1(9.1)
Self-esteem 9(81.8) 2(18.2)
Anxiety and depression 7(63.6) 4(36.4)
Dietary habits 10(90.9) 1(9.1)
Preventive behavior 9(81.8) 2(18.2)
Sexuality 8(72.7) 3(27.3)
Ending of the monitoring 8(72.7) 3(27.3)
The general agreement percentage of the ex-perts regarding the clarity of the messages revealed that 79.1% of the participants considered the texts clear. As for the relevance, most experts (98.2%) judged the chosen subjects to be very relevant to promote health in PLWHA. The assessment of CVI applied to the relevance of the messages that showed an I-CVI higher than 0.90 for most texts, an S-CVI/Ave of 0.98 and an S-CVI/UA of 0.80 (Table 2).

230 Acta Paul Enferm. 2017; 30(3):227-32.
Validation of phone messages to promote health in people with HIV
The main changes were the inclusion of a series of short questions about the subject at the begin-ning of some messages and the adjustment of the texts to a simpler and more interactive language, with replacement of specific terms from the health-care area-for instance, “medicine” as an alternative to “medication.” In addition, the experts recom-mended the exclusion of words or expressions that could refer to the infection by HIV, such as “num-ber of virus particles”, “immunity,” and “immune cells” (Chart 1).
Discussion
Phone messages are a way to encourage the adher-ence to and consolidation of a healthy lifestyle in people with chronic conditions(7) such as infection by HIV, because they allow clients to widen their knowledge about health.(19,20) Their use can help cli-ents to make choices about their mental and physi-cal health, have a positive view of life, and avoid risk behaviors.(8)
According to the experts’ evaluations, the top-ics of the messages were considered very relevant to promote health in PLWHA, corroborating na-tional guidelines focused on that audience.(15) In alignment with the present study, an investigation carried out with recently diagnosed patients showed that most participants considered it important to maintain a physical, mental, and behavioral equilib-rium to have a healthy life. They expressed concern about health habits after the diagnosis, with a de-crease in the consumption of alcohol and cigarettes, use of condoms, and an attempt to adopt a healthy diet and practice physical activities.(16)
An important issue in the design of the messag-es was to emphasize the benefits of healthy behav-iors instead of focusing on the risks of not adopting
Table 2. Experts’ evaluation regarding the relevance of the phone messages
Subject
Relevance evaluation
I-CVIIrrelevantSlightly relevant
Very relevant
n(%) n(%) n(%)
Presentation of the monitoring 0 0 11(100) 1.00
Adhesion to antiretroviral therapy 0 1(9.1) 10(90.9) 0.90
Physical activity 0 0 11(100) 1.00
Social support 0 1(9.1) 10(90.9) 0.90
Self-esteem 0 0 11(100) 1.00
Anxiety and depression 0 0 11(100) 1.00
Dietary habits 0 0 11(100) 1.00
Preventive behavior 0 0 11(100) 1.00
Sexuality 0 0 11(100) 1.00
Ending of the monitoring 0 0 11(100) 1.00
S-CVI/Ave 0.98
I-CVI - Content Validity Index for individual items; S-CVI/Ave - Mean of the content validity indexes for all the messages
Chart 1. Description of the phone messages after validation by the expertsSubject Message
Presentation of the phone monitoring My name is (professional’s name); I am the nurse responsible for sending you messages about health instructions every 15 days. I would like you to confirm that you received my messages by replying with a smiley emoticon. If you have questions about the subject, you can contact me by WhatsApp every day, at any time.
Adhesion to antiretroviral therapy Did you know that taking your medicines every day, at the same time, according to your doctor’s instructions, helps improve your health and your quality of life? Not missing appointments and having your medical examinations are important. Talk to your doctor about any difficulty with the medicine. Do not give up on your treatment!
Physical activity Have you exercised today? Practicing exercises every day or at least three times a week for 30 minutes makes your body’s defenses stronger, helps you to lose weight, and decreases the content of fat in your blood. You will feel well and your mind will get calm. You can choose a physical activity that you like, always under the supervision of your doctor.
Social support Did you know that it is important to take some time to be with your family and friends? Talking to someone you trust about the difficulties helps in your treatment. You can ask questions and look for help from the healthcare team at your clinic whenever you need. Keep in mind that there are people and professionals that can help you overcome the challenges.
Self-esteem Be aware that liking yourself helps in daily activities and improves your health. Think of today and value your achievements. Do something that makes you happy every day. It can be something simple, such as dancing, reading, taking some time off, listening to music, walking, or whatever you like. Keep in mind that you are unique, special, and valuable.
Anxiety and depression Anxiety and depression may occur sometimes in our lives. Exercising, sleeping well, having a healthy diet, and keeping good relationships with family and friends help to prevent anxiety and depression. In some situations, medicines are necessary. Seek help from the healthcare team at your clinic.
Dietary habits How is your diet? Did you know that a healthy diet gives you energy for daily activities and helps avoiding undesirable effects from the drugs? Also, an appropriate diet prevents diabetes, heart diseases, increases in bad cholesterol levels in your blood, and lipodystrophy (change in the distribution of body fat). You can make an appointment with a nutritionist to improve your dietary habits. Do not forget to drink at least two liters of water a day!
Preventive behavior Use of alcohol, cigarettes, and illicit drugs may impair the action of the medicines and intensify their undesirable effects. It is important to avoid or decrease the consumption of these substances so as not to hinder your treatment. Anyway, be sure to take your medicine.
Sexuality Sex is important in people’s lives and helps them to feel well. During intercourse, it is important to use condoms to protect yourself and your partner from sexually transmitted diseases. Kisses, hugs, and caresses are ways to give and receive sexual pleasure without the risk of contracting these diseases.
Ending of the phone monitoring Thank you for answering the messages. We are finished with the phone monitoring by WhatsApp now. However, you will continue to be assisted in the health service and may ask for help from the healthcare team if you need it. Our last meeting will be on the day of your follow-up (date of the appointment). I would like to count on your presence to perform the last evaluation of your health. We will ask your opinion about this experience and finish the survey.

231Acta Paul Enferm. 2017; 30(3):227-32.
Lima IC, Galvão MT, Pedrosa SC, Silva CA, Pereira ML
the target behavior (gain-framed appeal), a guideline considered efficient to stimulate physical activity in a study with clients that developed coronary artery disease.(5)
Another point was the use of a language that motivated empowerment and freedom of choice and was not authoritarian. Preserving autonomy is crucial in the process of health education and evi-dence showed that recommendations for a healthy lifestyle are more effective when they stimulate de-cision-making using arguments that preserve the freedom of the clients.(21)
The experts did not mention the number of characters in the phone messages. The advocated number for messages sent through SMS is 160.(22) For messages sent through WhatsApp, there is no evidence suggesting the ideal number of characters. Future investigations may tackle this issue.
The participants also suggested adjustments in the language used in the messages to make them more direct and accessible and favor understand-ing, mainly by replacing technical terms. A research study carried out with hypertensive elderly people revealed an interest in receiving objective and sim-ple phone messages that stimulated adhesion to the treatment.(6)
Regarding this fact, it is important to empha-size that effective communication between client and professional is fundamental in health care. To achieve this, it is necessary to provide information in a language suitable for the educational and cultural level of the client.(10) Substitution of plain language for technical terms may favor the understanding of the messages and make information more attractive.
The experts’ suggestion to exclude words or expressions that refer to the infection by HIV was considered fundamental to assure the confidential-ity of the diagnosis of future participants in the re-search.(23) This measure is related to the principle of nonmaleficence, that is, the intention of not caus-ing harm and/or damage to the participants in the research.(24)
In addition, clients’ fear of revelation of their serological status is an aspect that affects the quality of life of PLWHA;(1) this is a reason why the confi-dentiality of the diagnosis must be considered as a
priority in phone interventions directed to promote health in this target audience.(3)
Conclusion
Overall, the experts judged the phone messages to be clear and relevant to promote health in PLWHA. The messages reached a CVI of 0.98. Some participants suggested alterations in the language of the messages to make the information more clear and objective. The present study offers a set of messages validated by experts that can be applied to other investigations and in the assistance to PLWHA in the services of specialized care. A limitation of the study design was the lack of experts from other professional categories and the absence of validation by the target public. Future research that uses the messages may raise the need to adapt them to new circumstances.
AcknowledgementsTo the National Council for Scientific and Techno-logical Development for a PhD grant.
CollaborationsLima ICV, Galvão MTG, and Pedrosa SC contrib-uted to the project design and execution, manu-script writing, and approval of its final version. Silva CAC and Cunha GH contributed to project execu-tion and manuscript writing.
References
1. Galvão MT, Soares LL, Pedrosa SC, Fiuza ML, Lemos LA. Qualidade de vida e adesão à medicação antirretroviral em pessoas com HIV. Acta Paul Enferm. 2015; 28(1):48-53.
2. Deeks SG, Lewin SR, Havlir DV. The end of aids: HIV infection as a chronic disease. Lancet. 2013; 382 (9903):1525-32.
3. Lima IC, Galvão MT, Alexandre HO, Lima FE, Araujo TL. Information and communication technologies for adherence to antiretroviral treatment in adults with HIV/AIDS. Int J Med Inform. 2016; 92:54-61.
4. Thomas K, Linderoth C, Bendtsen M, Bendtsen P, Müssener U. Text message-based intervention targeting alcohol consumption among university students: findings from a formative development study. JMIR Mhealth Uhealth. 2016;4(4):e119.
5. Mendez RD, Rodrigues RC, Spana TM, Cornélio ME, Gallani MC, Pérez-Nebra AR. Validation of persuasive messages for the promotion of

232 Acta Paul Enferm. 2017; 30(3):227-32.
Validation of phone messages to promote health in people with HIV
physical activity among people with coronary heart disease. Rev Lat Am Enfermagem. 2012; 20(6):1015-23.
6. Yazdanshenas H, Bazargan M, Jones L, Vawer M, Seto TB, Farooq S, et al. Engaging gatekeeper-stakeholders in development of a mobile health intervention to improve medication adherence among african american and pacific islander elderly patients with hypertension. JMIR mHealth uHealth. 2016; 4(4):e116.
7. Chow CK, Islam SM, Farmer A, Bobrow K, Maddision R, Whittaker R, et al. Text2PreventCVD: protocol for a systematic review and individual participant data meta-analysis of text message-based interventions for the prevention of cardiovascular diseases. BMJ Open. 2016; 6:e012723.
8. Quintiliani LM, Mann DM, Puputti M, Quinn E, Bowen DJ. Pilot and feasibility test of a mobile health-supported behavioral counseling intervention for weight management among breast cancer survivors. JMIR Cancer. 2016; 2(1):e4.
9. Veneroni L, Ferrari A, Acerra S, Massimino M, Clerici CA. Considerations on the use of WhatsApp in physician-patient communication and relationship. Recenti Prog Med. 2015; 106(7): 331-6.
10. Benevides JL, Coutinho JFV, Pascoal LC, Joventino ES, Martins MC, Gubert FA, et al. Development and validation of educational technology for venous ulcer care. Rev Esc Enferm USP. 2016;50(2):306-12.
11. Jasper MA. Expert: a discussion of the implications of the concept as used in nursing. J Adv Nurs. 1994; 20(4):769-76.
12. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Programa Nacional de DST/Aids. Alimentação e nutrição para pessoas que vivem com HIV e Aids. Brasília (DF): Ministério da Saúde; 2006.
13. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de DST, Aids e Hepatites Virais. Guia para o cuidador domiciliar de pessoas que vivem com HIV/Aids. Brasília (DF): Ministério da Saúde; 2010.
14. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de DST, Aids e Hepatites Virais. Recomendações para a prática de atividades físicas para pessoas vivendo com HIV e aids. Brasília (DF): Ministério da Saúde; 2012.
15. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de DST, Aids e Hepatites virais. Protocolo clínico e diretrizes terapêuticas para manejo da infecção pelo HIV em adultos. Brasília (DF): Ministério da Saúde; 2015.
16. Alexandre NM, Coluci MZ. Content validity in the development and adaptation processes of measurement instruments. Ciênc Saude Coletiva. 2011;16(7):3061-8.
17. Polit D, Beck CT. The Content Validity Index: are you sure you know what’s being reported? Critique and recommendations. Res Nurs Health. 2006;29(5):489-97.
18. Polit DF, Beck CT. Fundamentos de pesquisa em enfermagem: avaliação de evidências para a prática de enfermagem. Porto Alegre: Artmed; 2011.
19. Flickinger TE, DeBolt C, Waldman AL, Reynolds G, Cohn WF, Beach MC, Ingersoll K, Dillingham R. Social support in a virtual community: analysis of a clinic-affiliated online support group for persons living with HIV/AIDS. AIDS Behav. 2016. [Epub ahead of print].
20. Alexandre HO, Galvão MT, Lima IC, Guedes DS, Pedrosa SC, Cunha GH, Cavalcante EF. Perceptions that people newly diagnosed with hiv have on health. Int Arch Med. 2016; 9(130):1-6.
21. Bigi S. Communication skills for patient engagement: argumentation competencies as means to prevent or limit reactance arousal, with an example from the italian healthcare system. Front Psychol. 2016; 7 (1472):1-7.
22. Zurovac D, Sudoi RK, Akhwale WS, Ndiritu M, Hamer DH, Rowe AK, et al. The effect of mobile phone text-message reminders on Kenyan health workers’ adherence to malaria treatment guidelines: a cluster randomised trial. Lancet. 2011;378(9793):795-803.
23. Paula CC, Clarissa B, Zanon BP, Brum CN, Padoin SM. Ética na pesquisa com adolescentes que vivem com HIV/Aids. Rev Bioét. 2015; 23(1):161-8.
24. Brasil. Ministério da Saúde. Resolução N° 510/2016 do Conselho Nacional de Saúde. Brasília (DF): Conselho Nacional de Saúde; 2016.

233Acta Paul Enferm. 2017; 30(3):233-9.
Original Article
Effect of Astrocaryum aculeatum (tucumã) on doxorubicin toxicity: in vivo experimental model
Efeito da Astrocaryum aculeatum (Tucumã) na toxicidade da Doxorrubicina: modelo experimental in vivo
Alan Bruno Aurélio Carneiro1
Eduardo Júnior Serrão Pinto1
Ivagner Ferreira Ribeiro1
Mayck Rian Gonçalves Magalhães2
Moacir de Azevedo Bentes Monteiro Neto1
Corresponding authorAlan Bruno Aurélio CarneiroRodovia Juscelino Kubitscheck,68903-419, Macapá, AP, [email protected]
DOIhttp://dx.doi.org/10.1590/1982-0194201700036
1Universidade Federal do Amapá, Macapá, AP, Brazil.2Faculdade Estácio de Macapá, Macapá, AP, Brazil.Conflicts of interest: there are no conflicts of interest to declare.
AbstractObjective: To obtain the oil of Astrocaryum aculeatum (A.a), and evaluate its genotoxicity/antigenotoxicity activities using the micronucleus test in peripheral blood cells.Methods: The oil of Astrocaryum aculeatum was obtained by hydraulic pressing. The animals used were healthy Swiss male mice, at 6-7 weeks of age; there were six per group. The genotoxic and antigenotoxic activity of concentrations were 500, 1,000 and 2,000 mg/kg per 0.5 mL (oral), followed or not followed by intraperitoneal injection of doxorubicin (0.3 mL-15 mg/kg by body weight), in addition to a negative group (water) and dimethyl sulfoxide (600 μL). Peripheral blood samples were collected 24h and 48h after treatment.Results: A statistically significant reduction was identified in the frequency of micronuclei in polychromatic cells ranging from 34.72% to 38.19% for 24-hour treatments, and from 63.70% to 66.12% for 48 hour.Conclusion: The fixed oil of tucumã presented antigenotoxic potential for the concentrations used in acute treatments.
ResumoObjetivo: Obter o óleo do Astrocaryum aculeatum (A.a) e avaliar a genotoxidade/antigenotoxidade pelo teste do micronúcleo em células do sangue periférico.Métodos: O óleo da A.a foi obtido por prensagem hidráulica. Os animais foram camundongos Swiss, machos e saudáveis com 6-7 semanas de idade, 6 por grupo. Teste genotóxico e antigenotóxico as concentrações foram de 500, 1.000 e 2.000 mg/kg por 0,5 mL (via oral), seguidas ou não de injeção intraperitoneal de doxorrubicina (0,3mL - 15 mg/kg por peso corporal), além do grupo negativo (água) e dimetilsufóxido (600 µL). As amostras de sangue periférico foram coletadas 24h e 48h após o tratamento.Resultados: Houve redução estatisticamente significativa na frequência de micronúcleos em células policromáticas que variou de 34,72% à 38,19% para os tratamentos de 24h, e de 63,70 à 66,12% para os de 48h.Conclusão: O óleo fixo do tucumã apresentou potencial antigenotóxico para as concentrações em tratamentos agudos.
KeywordsDoxorubicin/toxicity; Plant extracts/
analysis; Micronucleus tests
DescritoresDoxorrubicina/toxicidade; Extrato
de plantas/análise; Testes para micronúcleos
Submitted February 15, 2017
Accepted May 29, 2017

234 Acta Paul Enferm. 2017; 30(3):233-9.
Effect of Astrocaryum aculeatum (tucumã) on doxorubicin toxicity: in vivo experimental model
Introduction
The Astrocaryum aculeatum (tucumã) is a fruit of yellow color with reddish tones, which is from a palm tree of the Arecaceae Family that reaches 10 to 25 meters high, 15 to 30cm in diameter,(1) usual-ly solitary, stem with dark thorns, ascending leaves, erect flowers and broadly distributed in Amazon, which presents great biodiversity of the genus Astro-caryum.(1,2) This is an exceptionally tolerant species to acidic and nutrient poor soils, which is character-istic of the Amazonian region.(3)
The fruit has an ovoid shape, whose fibrous mesocarp provides a high nutritional content. The pulp is well appreciated, and consumed in natura by the population, or as a filling in sandwiches, tap-iocas, custard, ice cream, and flour.(4)
de Rosso & Mercadante(5) described 24 carot-enoids; 21 were chemically identified in the tucumã. Tucumã analysis show one of the highest concentra-tions of pro-vitamin A, representing 52 mg/100 g of pulp, with a potential antioxidant that block the harmful effects caused by free radicals. Carotenoids are essential for cell differentiation, embryonic de-velopment, vision, as well as many other functions, including potential therapeutic benefits (5,6)
According to Ambrósio et al., (2006),(7) β-caro-tene is a powerful antioxidant that protects against cardiovascular diseases by inhibiting the oxidative process of low-density lipoprotein (LDL). Import-ant polyphenols, such as quercetin, are also present in tucumã, which is one of the main flavonoids pres-ent in the human diet. Flavonoids are compounds found in plants, which also have antioxidant prop-erties.(7,8)
Chemotherapeutic doxorubicin (DXR) is an an-thracyclic antibiotic and a potent, broad spectrum, antitumor medicine, frequently used in combina-tion with different medicines in the treatment of acute leukemia, lymphomas and solid tumors, such as breast, ovarian, and endometrial. Its toxicity can be caused in different ways: its planar agglutinated portion can be inserted between adjacent base pairs in the DNA, modifying the ability of nuclear heli-cases to dissociate the DNA double-strand and the topoisomerase II enzyme. Acting as an aggressor for
this enzyme, it modifies its normal purpose to in-duce DNA damage, which occurs by loss of one or two electrons, generating reactive compounds with the potential to damage macromolecules and lipid membranes.(9)
Chemotherapy is a method that uses chemical compounds for treatment of diseases by biological agents, called chemotherapeutic. When used for cancer, it is called antineoplastic chemotherapy, and according to the Federal Nursing Council, the nurse is the one who can administer these medications. The nurse must know that there are natural ways to assist with this treatment,(10) in which the oil of tucumã presents with considerable potential for the support of chemotherapy, as vitamin A produces less side effects, and prevents a break in the conti-nuity of treatment. The present study may provide a theoretical basis to support advanced nursing prac-tice in cancer patients.(11)
The consumption of fruits rich in antioxidants prevents excessive oxidation by the body itself, or in actions of medications such as doxorubicin, which promotes the production of free radicals that, if not controlled, can cause cellular damage which may lead to the development of several chronic and de-generative diseases.(9) As the search for natural anti-oxidants has increased greatly in recent years, main-ly for applications in the pharmaceutical, cosmetic and nutritional sectors, the hypothesis for this study is that the consumption of tucumã should be en-couraged.
The objective of this study is to obtain the oil of Astrocaryum aculeatum (A.a) (tucumã) and to evaluate the genotoxicity/antigenotoxicity using the micronucleus test in peripheral blood cells.
Methods
Obtaining the fixed oil from Astrocaryum aculeatumThe oil was supplied by the Institute of Scientific and Technological Research of the State of Amapá (IEPA). The fruit was washed dry and the seed was removed to obtain the mesocarp, which was distrib-

235Acta Paul Enferm. 2017; 30(3):233-9.
Carneiro AB, Pinto EJ, Ribeiro IF, Magalhães MR, Monteiro Neto MA
uted onto trays for dehydration in a greenhouse, with air recirculation at 50°C for 24 hours, and then was cooled to room temperature.
The resulting mass was quantified at 28.21% of the total initial mass. The dry material was sub-jected to hydraulic pressing, with 15 tons capacity (SIWA model FM3), obtaining 22.21% of fixed oil.
Chemical agent inducing DNA damageThe chemotherapeutic agent, doxorubicin (DXR, Rubidox®), was used as a micronucleus inducer in peripheral blood cells, as a positive control. The chemical inducer was dissolved in distilled water and intraperitoneally administered (0.3 mL/ani-mal) at the concentration of 15 mg/kg body weight, established according to studies of Franke et al.,(12)
and Venkatesh et al.(13)
Animals and TreatmentsSwiss male mice were used for the experiments; they were 6-7 weeks of life, with a body weight of approximately 30g; they were obtained from the Biothermium of the Multidisciplinary Center for Biological Research in the Laboratory Animal Sci-ence Area (CEMIB) of the University of Campi-nas (UNICAMP). The research was conducted in accordance with international protocols, regarding the use and care of laboratory animals. The animals were kept in grid boxes with dimensions of 30x19x-12cm in a experimental room, under the following controlled conditions: temperature (22±2°C), hu-midity (50±10%), 12 hours of light-dark cycle, with ad libitum access to feed and water. The treatment protocols performed in this study were approved by the Committee of Ethics in the Use of Animals of UNIFAP, protocol 0012/2015.
Experimental designThe animals were divided into different groups, with six mice in each treatment group. The con-centrations of the fixed oil of Astrocaryum aculea-tum (A.a) were 500, 1,000 and 2,000 mg/kg of body weight, administered by gavage (0.5 ml) for observation of the genotoxic processes. The oil di-lutions were made, respectively, in 0.5 ml of dis-tilled water, with the solvent dimethylsulfoxide
(DMSO) in the concentrations 150μl, 300μl and 600μl, respectively.
For antigenotoxic evaluation, immediately after administration of the A. a, the animals were treated with an intraperitoneal injection of DXR (0.3 ml), at a dose of 15 mg/kg of corporal weight. The sol-vent group is represented by treatment with DMSO at the concentration of 600 μl, because it was the dosage used in animals receiving 2,000 mg/kg of body weight of A.a. Peripheral blood samples from the acute treatment groups were collected after 24 and 48 hours (Table 1).
Table 1. Experimental groups and acute treatment protocols for the micronucleus testTreatment Group Dosage (mg/kg)
Negative control 1a,b -
DMSO 2a -
A. a I 3a 500
A. a II 4a 1,000
A. a III 5a 2,000
DXR 6a,b 15
DMSO + DXR 7b As in (2) and (6)
A. a. I + DXR 8b As in (3) and (6)
A. a II + DXR 9b As in (4) and (6)
A. a III + DXR 10b As in (5) and (6)
DMSO - Dimethyl sulfoxide; A. a. - Astrocaryum aculeatum; DXR - Doxorubicin; a protocols for genotoxicity; b protocols for antigenotoxicity
Micronucleus testThe levels of micronucleated polychromatic eryth-rocytes (MNPCEs) in the peripheral blood were sampled based on the technique of MacGregor et al.,(14) and adapted, consisting of the following pro-cedures:• The tip of the animals’ tails were cut and blood
was dripped directly onto the dry slides;• The material was smeared with a cover slip;• The material was fixed in methanol for five
minutes, after drying;• The material was stained with Giemsa in the
next day, according to the Manual for the Lab-oratory Diagnostic of Malaria (2005). Giemsa powder 0.75g was used for each 100 ml of the solution - 35 ml Glycerol and 65 ml Methanol, in a ratio of 1:10 (Giemsa/buffered water), for 20 minutes.

236 Acta Paul Enferm. 2017; 30(3):233-9.
Effect of Astrocaryum aculeatum (tucumã) on doxorubicin toxicity: in vivo experimental model
• Less mature micronuclei in polychromatic erythrocytes (PCEs) that were stained in blue were analyzed. More mature Nitrous Eryth-rocytes (NCEs) showed little or no influence from the stain, and were not analyzed.
Analysis of the glass slidesThe glass slides of each animal were coded and an-alyzed within a short time in a blind test, in order to eliminate analysis errors. The analysis was per-formed by three observers, using a balanced system; that is, an equal number of cells were analyzed on different glass slides, for each animal of the study, by each observer.
The glass slides were first analyzed under a 40x mean magnification optical microscope to find fields of good technical quality, where the cells were well spread, undamaged and properly stained. After these fields were located, the observers followed the cell analysis process to identify the presence of the micronucleus, using a 100x magnification (immer-sion lens).
The micronucleus distribution among the cells may have value in identification of the mechanism, so, for its determination, 2,000 PCEs per animal were analyzed in the peripheral blood samples (24h and 48h), and a total of 400 erythrocytes per ani-mal were analyzed to calculate the Nuclear Division Index (IDN)(15-17) using the formula:
IDN = ___PCE___PCE + NCE
The percentage of frequency reduction of PCEMNs was calculated according to Waters et al. (1990),(18) to determine the effectiveness of treat-ments for antigenotoxic effect, using the following formula:
% of reduction = A – BA – C
A corresponds to the DXR group (positive con-trol), B corresponds to the groups treated with A. a. + DXR (antigenotoxic groups), and C corresponds to the group treated with water (negative control).
Statistical analysisThe data were analyzed statistically using the anal-ysis of variance (ANOVA) for completely random-
ized experiments, with the calculation of the F statistic and respective “p-values”. In cases where p <0.05, the treatment means were compared using the Tukey method, with the calculation of the min-imum significant difference for α = 0.05, using the Graph Pad Prism 6 program.
Results
The results obtained for the treatments in Swiss mice with different doses of the fixed oil of Astro-caryum aculeatum, and/or these combined with the intraperitoneal administration of DXR in the dos-age of 15 mg/kg of body weight, and their respec-tive controls are shown in table 2.
Simultaneous administration of a single oral dose of each fixed oil concentration of Astrocaryum aculeatum per gavage and intraperitoneal injec-tion of DXR, resulted in a significant reduction in the frequency of PCEMNs. Values ranging from 34.72% to 38.19% for the 24-hour treatments (Figure 1), and from 63.70 to 66.12% for the 48-hour treatments where found (Figure 2), when compared to the group treated with DXR alone. The gradual increase of the fixed oil concentration of Astrocaryum aculeatum resulted in a proportion-al increase in the reduction of genotoxicity in 24 hours; however the evaluation of the treatments at
Table 2. Frequencies of micronucleated polychromatic erythrocytes (PCEMNs) from the peripheral blood cells of animals submitted to treatment of different doses of A.a., and their respective controls
Treatment(mg/kg of body weight)
PCEMNs total PCEMNs (mean ± SD)
24 h 48 h 24 h 48 h
Control 27 26 4.50 ± 0.55 4.33 ± 0.52
DMSO 31 34 5.16 ± 0.63 5.66 ± 0.82
A. a. I (500 mg) 29 29 5.16 ± 0.98 4.83 ± 0.41
A. a. II (1000 mg) 29 29 4.83 ± 0.75 4.83 ± 0.75
A. a. III (2000 mg) 28 28 4.66 ± 0.52 4.66 ± 0.52
DXR mg 171ª 274ª 28.50 ± 1.38 45.66 ± 1.63
DMSO + DXR 167ª 267ª 27.83 ± 0.75 44.66 ± 1.05
A. a. I + DXR 121ª,b 116ª,b 20.16 ± 1.16 19.33 ± 0.52
A. a. II + DXR 118ª,b 111ª,b 19.66 ± 1.03 18.50 ± 0.55
A. a. III + DXR 116ª,b 110ª,b 19.33 ± 1.37 18.33 ± 0.52
A total of 2,000 PCEs were analyzed per animal, for a total of 12,000 cells per treatment; DXR: doxorubicin (15mg/kg body weight); ªsignificant difference for control group (p<0.05); b Significant difference for the DXR group (p < 0.05).

237Acta Paul Enferm. 2017; 30(3):233-9.
Carneiro AB, Pinto EJ, Ribeiro IF, Magalhães MR, Monteiro Neto MA
48 hours indicated no dose-response relationship (Table 2). The frequency of PCEMNs was lower in animals treated with DMSO + DXR than in those treated with DXR alone, but these differences were not statistically significant, and the IDN did not show any indication of cytotoxic potential in all groups evaluated (Table 3).
Figure 1. Frequencies of PCEMNs after 24 hours of treatment, with different doses of A.a. and DXR, and their respective controls
Figure 2. Frequencies of PCEMNs after 48 hours of treatment, with different doses of A.a. and DXR, and their respective controls
Table 3. Results of A.a. and DXR treatments and their respective controls (at 24 and 48 hours)
Treatment(mg/kg body weight)
IDNPCEMNs/1,000
PCEsREDUCTION
(%)
24 h 48 h 24 h 48 h 24 h 48 h
Control 0.011 ± 0.51 0.010 ± 0.51 2.25 2.16 - -
DMSO 0.013 ± 0.54 0.011 ± 0.54 2.58 2.83 - -
A. a. I 0.013 ± 0.54 0.011 ± 0.83 2.42 2.42 - -
A. a. II 0.014 ± 0.75 0.013 ± 0.75 2.42 2.42 - -
A. a. III 0.013 ± 0.83 0.013 ± 0.75 2.33 2.33 - -
DXR 0.013 ± 1.03 0.012 ± 0.89 14.25 22.83 - -
DMSO+DXR 0.013 ± 0.75 0.010 ± 0.51 14.08 22.25 - -
A. a. I + DXR 0.012 ± 1.16 0.011 ± 0.81 11.33 9.66 34.72 63.70
A. a. II + DXR 0.013 ± 0.75 0.011 ± 0.83 10.08 9.25 36.80 65.72
A. a. III + DXR 0.012 ± 0.75 0.010 ± 0.51 9.66 9.16 38.19 66.12
Discussion
The present study investigated the genotoxic and antigenotoxic effect of tucumã oil, an Amazonian fruit rich in carotenoids and other bioactive com-pounds, such as polyphenols.(5,12-19) The findings of this study demonstrated that A.a. presents char-acteristics similar to previously reported results on studies of tucumã, even in its various derivative forms in which it was examined.(7,8,19,20)
Substances, such as carotenoids and polyphe-nols found in the oil of tucumã, were previous-ly evaluated by de Rosso and Mercadante,(5) and Gonçalves et al.,(8) who associated these compounds with the elimination of free radicals. These affirma-tions are corroborated with this study, because A.a. is described as rich in carotenoids and flavonoids; both compounds are known as antioxidants in the literature.
Several therapeutic properties of bioactive com-pounds, such as flavonoids, especially quercetin which is abundant in tucumã, have been extensively studied in the last decade, due to their antioxidant effects, anticancer potential, and protective effects on renal, cardiovascular and hepatic systems.(19-21, 23)
The antimicrobial properties of the tucumã are reported by Jobim et al.(21) These antimicrobial ef-fects of the fruit are associated with its chemical composition, which includes several types of poly-phenols. According to Daglia,(22) polyphenols are secondary metabolites produced by superior plants that have antibacterial, antiviral and antifungal properties.
Mic
ronu
cleo
us/P
CEs
24h
0
Nega
tive
Cont
rol
DMSO
A.a.
(500
mg)
A.a.
(100
0 m
g)
A.a.
(200
0 m
g)
DXR
DMSO
+ D
XR
A.a.
(500
mg
+ D
XR)
A.a.
(100
0 m
g +
DXR
)
A.a.
(200
0 m
g +
DXR
)
10
20
30
40
Mic
ronu
cleo
us/P
CEs
48h
0
Nega
tive
Cont
rol
DMSO
A.a.
(500
mg)
A.a.
(100
0 m
g)
A.a.
(200
0 m
g)
DXR
DMSO
+ D
XR
A.a.
(500
mg
+ D
XR)
A.a.
(100
0 m
g +
DXR
)
A.a.
(200
0 m
g +
DXR
)
10
20
30
40
50

238 Acta Paul Enferm. 2017; 30(3):233-9.
Effect of Astrocaryum aculeatum (tucumã) on doxorubicin toxicity: in vivo experimental model
However, in addition of the variability in bioac-tive compounds of different natures present in the fruit, the benefits derived from tucumã can be at-tributed to the antioxidant properties distinct from its several carotenoids. de Rosso and Mercadante(5) list 60 species of carotenoids present in different fruits, including 24 in the tucumã.
The bioactive molecules found in the tucumã present great antioxidant capacity.(24-26) However, the rich concentration of these molecules in the fixed oil of the fruit is not a guarantee that it will be able to completely reverse the free radicals (19) of a living organism exposed to molecules that can dam-age the genetic content of the cells.
Chemotherapeutic DXR, used in this study, is an anthracyclic antibiotic and a potent broad spec-trum antitumor medicine, often used in the treat-ment of acute leukemia, lymphomas and tumors.(9) Doxorubicin is a micronucleus inducer, and is fre-quently used in mutagenicity tests as a positive con-trol. It is reported as a metabolically active molecule for a free radical state that interacts with molecular oxygen to generate superoxide radicals.(27)
The results of the present study demonstrated a significant decrease in the frequency of micronuclei in polychromatic erythrocytes, which corroborates the studies of Sagrillo et al.,(19) and de Souza Fil-ho,(20) which recognized the protective potential of tucumã in cells submitted to oxidative stress, which is a producer of free radicals. The results obtained in the evaluations of the treatment groups of this study that used A. a. associated with DXR, to test the an-tigenotoxic effect, indicated a significant reduction of 36.57 ± 1.74% for treatments of 24 hours and 65.18 ± 1, 29% for those of 48 hours.
The results of the genotoxic effect for the three concentrations tested (A. a. I 500 mg, A. a. II 1,000 mg and A. a. III 2,000 mg) as well as the DMSO group, when compared with the negative control group, demonstrated the absence of a tox-ic effect on DNA. These results corroborate(19,20) that different concentrations of tucumã provided a protective effect for the cell to oxidative stress, indicating some carotenoids, such as β-carotene, as an inducer of increased resistance to oxidative DNA damage.(20)
de Souza Filho et al.,(20) in their findings, suggested a relative genotoxic effect of tucumã on human peripheral blood mononuclear cells (PBMC), at concentrations higher than 500 μg/mg, when tested in vitro by the comet assay; how-ever they recognized the methodological limita-tions related to their study, and emphasized that the results from studies that use only in vitro pro-tocols to analyze the potential genotoxic effect of tucumã cannot be directly transferred to in vivo models.
Sagrillo et al.,(19) extracted the pulp and peel of tucumã in six different concentrations (100, 300, 600, 900, 1,200, and 1,500 ug/ml) to test its ability to treat oxidative stress induced in hu-man lymphocyte cell cultures, and obtained best results with antioxidants effects at the lowest con-centrations tested.
It was verified that there was a significant differ-ence in the reduced rates of micronuclei when com-paring treatment times (24 and 48 hours; a 32% difference was found with the 48-hour treatment. Studies that evaluate the genotoxic/antigenotoxic effect of tucumã in vivo were not found to compare results to this research, which makes it the reference for future investigations.
Conclusion
The results of this research demonstrate an evident protective potential for cellular DNA, at all the concentrations used, proving its antigenotoxic po-tential; however the genotoxic possibility was not demonstrated to be produced by the fixed oil of tucumã in every concentration studied. Therefore, the fixed oil of tucumã is an efficient antigenotoxic agent, producing satisfactory effects as a protector of cellular DNA damage, both at 24 and 48 hours after administration, achieving better results after 48 hours.
AcknowldgementsTo the Institute of Scientific and Technological Re-search (Instituto de Pesquisas Científicas e Tecnológi-cas) in the State of Amapá, Brazil - IEPA.

239Acta Paul Enferm. 2017; 30(3):233-9.
Carneiro AB, Pinto EJ, Ribeiro IF, Magalhães MR, Monteiro Neto MA
CollaborationsCarneiro ABA, Pinto EJS, Ribeiro IF, Magalhães MRG and Monteiro Neto MAB contributed to the study design, analysis and data interpretation, rele-vant critical review of the intellectual content, and final approval of the version to be published.
References
1. Bacelar-Lima CG, Mendonça M, Barbosa T. Morfologia floral de uma população de tucumã Astrocaryum aculeatum G. Mey (Arecaceae) na Amazônia central. Acta Amaz. 2006; 36(4):407-12.
2. Gentil DF, Ferreira SA. Morfologia da plântula em desenvolvimento de Astrocaryum aculeatum Meyer (Arecaceae). Acta Amaz. 2005; 35(3):337-41.
3. Ferreira SA, Castro AF, Gentil DF. Emergência de plântulas de tucumã (Astrocaryum aculeatum) em função do prétratamento das sementes e da condição de semeadura. Rev Bras Frutic. 2010; 32(4):1189-95.
4. Yuyama LK, Maeda RN, Pantoja L, Aguiar JP, Marinho HÁ. Processamento e avaliação da vida-de-prateleira do tucumã (Astrocaryum aculeatum Meyer) desidratado e pulverizado. Ciênc E Tecnol Aliment. 2008; 28(2):408-12.
5. de Rosso VV, Mercadante AZ. Identification and quantification of carotenoids, by HPLC-PDA-MS/MS, from Amazonian fruits. J Agric Food Chem. 2007; 55(13):5062-72.
6. Gross MD, Bishop TD, Belcher JD, Jacobs Jr DR. Induction of HL-60 cell diferentiation by carotenoids. Nutr Cancer. 1997; 27(2):169-73.
7. Ambrósio CL, Campos FA, Faro ZP. Carotenóides como alternativa contra a hipovitaminose A. Rev Nutr. 2006; 19(2):233-43.
8. Gonçalves AE. Avaliação da capacidade antioxidante de frutas e polpas de frutas nativas e determinação dos teores de flavonóides e vitamina C [dissertação]. São Paulo: Universidade de São Paulo; 2008.
9. Injac R, Strukelj B. Recent advances in protection against doxorubicin-induced toxicity. Technol Cancer Res Treat. 2008; 7(6):497-516.
10. dos Santos HS, Cruz WM. A terapia nutricional com vitaminas antioxidantes e o tratamento quimioterápico oncológico. Rev Bras Cancerol. 2001; 47(3):303-8.
11. de Souza RS, Carvalho SS, Matos DO, Da Silva MH. Novas tecnologias no tratamento quimioterápico por enfermeiros em um hospital. Rev Cient Enferm. 2016; 17(1):24-35.
12. Franke SI, Prá D, da Silva J, Erdtmann B, Henriques JA. Possible repair action of Vitamin C on DNA damage induced by methyl methanesulfonate, cyclophosphamide, FeSO 4 and CuSO 4 in mouse blood cells in vivo. Mutat Res Toxicol Environ Mutagen. 2005; 583(1):75-84.
13. Venkatesh P, Shantala B, Jagetia GC, Rao KK, Baliga MS. Modulation of doxorubicin-induced genotoxicity by Aegle marmelos in mouse bone marrow: a micronucleus study. Integr Cancer Ther. 2007; 6(1):42-53.
14. MacGregor, James T., et al. The in vivo erythrocyte micronucleus test: measurement at steady state increases assay efficiency and permits integration with toxicity studies. Fundam Appl Toxicol. 1990; 14(3):513-22.
15. Brasil. Ministério da Saúde. Manual de diagnóstico laboratorial da malária. Brasília (DF); Ministério da Saúde; 2005.
17. Ribeiro LR, Salvadori DM, Marques EK. Mutagênese ambiental. Canoas: Ed ULBRA; 2003.
18. Waters MD, Brady AL, Stack HF, Brockman HE. Antimutagenicity profiles for some model compounds. Mutat Res Genet Toxicol. 1990; 238(1):57-85.
19. Sagrillo MR, Garcia LF, de Souza Filho OC, Duarte MM, Ribeiro EE, Cadoná FC, et al. Tucuma fruit extracts (Astrocaryum aculeatum Meyer) decrease cytotoxic effects of hydrogen peroxide on human lymphocytes. Food Chem. 2015; 173:741-8.
20. de Souza Filho OC, Sagrillo MR, Garcia LF, Machado AK, Cadoná F, Ribeiro EE, et al. The in vitro genotoxic effect of Tucuma (Astrocaryum aculeatum), an Amazonian fruit rich in carotenoids. J Med Food. 2013; 16(11):1013-21.
21. Jobim ML, Santos RC, dos Santos Alves CF, Oliveira RM, Mostardeiro CP, Sagrillo MR, et al. Antimicrobial activity of Amazon Astrocaryum aculeatum extracts and its association to oxidative metabolism. Microbiol Res. 2014; 169(4):314-23.
22. Daglia M. Polyphenols as antimicrobial agents. Curr Opin Biotechnol. 2012; 23(2):174-181.
23. Böhm F, Edge R, George Truscott T. Interactions of dietary carotenoids with singlet oxygen (1O2) and free radicals: potential effects for human health. Acta Biochim Pol. 2012; 59(1):27-30.
24. Stephensen CB. Provitamin A carotenoids and immune function. In: Sanumihardjo AS. editor. Carotenoids and Human Health. New York: Springer; 2013. Cap. 16. p. 261-70.
25. Skibsted LH. Carotenoids in antioxidant networks. Colorants or radical scavengers. J Agric Food Chem. 2012; 60(10):2409-17.
26. Bianchi ML, Antunes LM. Radicais livres e os principais antioxidantes da dieta. Rev Nutr. 1999; 12(2):123-30.
27. Tavares DC, Cecchi AO, Antunes LM, Takahashi CS. Protective effects of the amino acid glutamine and of ascorbic acid against chromosomal damage induced by doxorubicin in mammalian cells. Teratog Carcinog Mutagen. 1998; 18(4):153-61.

240 Acta Paul Enferm. 2017; 30(3):240-6.
Original Article
Association between intensities of pain and sedation in intensive care patientsAssociação entre intensidades de dor e sedação em pacientes de terapia intensivaDaniele Cristiny da Silva1
Taís Pagliuco Barbosa1
Alessandra Soler de Bastos1
Lúcia Marinilza Beccaria1
Corresponding authorDaniele Cristiny da SilvaAv. Brigadeiro Faria Lima, 5416, 15090-000, São José do Rio Preto, SP, [email protected]
DOIhttp://dx.doi.org/10.1590/1982-0194201700037
1Faculdade de Medicina de São José do Rio Preto, São Paulo, SP, Brasil.Conflicts of interest: no conflicts of interest to declare.
AbstractObjective: To identify the clinical profile, intensities of pain and sedation in patients in the intensive care unit, and associate the data.Methods: Quantitative and cross-sectional study performed in an intensive care unit of a teaching hospital. Sample of 240 patients. Clinical data were obtained from the electronic medical record. The following scales filled out by nurses were used: Richmond Agitation-Sedation Scale (RASS), visual numeric pain scale and Behavioral Pain Scale (BPS).Results: Prevalence of non-elderly, male, neurological and surgical patients in deep sedation. There was higher mortality in patients in deep sedation, and longer hospitalization time in patients in moderate sedation. Sedation was not effective in suppressing pain, but it served to control its intensity.Conclusion: The identification of intensity of pain and sedation performed by nurses helps decision making and provides adequate management of sedoanalgesia in patients of intensive care.
ResumoObjetivos: Identificar o perfil clínico, intensidades de dor e sedação em pacientes na unidade de terapia intensiva e associar os dados.Métodos: Estudo quantitativo e transversal, realizado em unidade de terapia intensiva de um hospital de ensino. Amostra de 240 pacientes. Os dados clínicos foram obtidos do prontuário eletrônico. Foram utilizadas escalas de sedação e agitação de Richmond, dor visual numérica e Behavioral pain scale, preenchidas por enfermeiros.Resultados: Prevaleceram pacientes não idosos, masculinos, neurológicos, cirúrgicos, com sedação profunda. Houve maior mortalidade em pacientes com sedação profunda e maior tempo de internação naqueles com sedação moderada. A sedação não se mostrou efetiva para suprimir a dor, mas serviu para controlar sua intensidade.Conclusão: A identificação da intensidade de dor e sedação realizada por enfermeiros auxilia na tomada de decisão e propicia adequado manejo da sedoanalgesia de pacientes em terapia intensiva.
KeywordsPain; Pain measurement; Sedation; Patients; Intensive care units
DescritoresDor; Medição da dor; Sedação; Pacientes; Unidade de terapia intensiva
Submitted February 14, 2017
Accepted June 19, 2017

241Acta Paul Enferm. 2017; 30(3):240-6.
Silva DC, Barbosa TP, Bastos AS, Beccaria LM
Introduction
International multi-center studies indicate the majority of patients in intensive care units (ICU) presents pain, and its systematic evaluation is fundamental to provide adequate analgesia.(1) The self-report is considered ‘gold standard’ in pain assessment. For awake patients with ade-quate cognitive and auditory abilities, assessment scores can be used. One of them is the visual nu-meric scale (VNS), in which patients are asked to rate their pain between zero and ten, that is, ‘no pain’ and ‘worst possible pain’, respectively.(2) However, as many patients in ICUs are in critical state, intubated, in mechanical ventilation and/or sedated, and with suppressed level of con-sciousness, their adequate expression of duration of pain can be impossible.
Scales are used to assess patients’ behavior-al pain in the context of intensive care, and are an important tool for nurses’ clinical practice. The Behavioral Pain Scale (BPS) was translated and adapted to Portuguese in 2014, and assess-es three aspects, namely: facial expression, body movements and adaptation to mechanical ven-tilation.(3) Once identified, pain needs adequate management through analgesic and/or sedative drugs with the aim to control stressors, patient’s adaptation to mechanical ventilation in severe respiratory diseases, control of intracranial pres-sure, epileptic disease and to facilitate the care provided by health professionals, offering com-fort during the performance of invasive proce-dures at the bedside.(4)
In patients’ sedation process, their level of con-sciousness is depressed mainly with use of benzo-diazepines drugs, which exert profound effects on the central nervous system. These drugs also act on other organs and systems, which can often be underestimated, highlighting the influence on the immune system. This system is involved with pa-thologies that prolong the length of stay in ICUs, such as nosocomial infections.(5-7)
The excessive use of sedatives makes it difficult and delays the withdrawal of mechanical ventila-tion. Depending on the chosen drugs, in some cases
it may exacerbate the effects of sepsis, increase hos-pitalization time, incidence of delirium, and mor-bidity and mortality in ICU.(8) Studies have demon-strated lower hospitalization time with consequent reduction in mortality in patients using lower level of sedation.(9)
Some sedation guidelines recommend its start to provide adequate analgesia. However, a study of patients on mechanical ventilation has shown that administering analgesia to the patient with morphine first, instead of sedating, may lead to a shorter length of stay in ICUs and the hospital because it provides early weaning from mechanical ventilation.(10)
Scales have been developed when researching the need for adequate titration and control of use of sedation. The Richmond Agitation-Seda-tion Scale (RASS), for example, is used to clas-sify sedation intensities in light, moderate, or deep. It is important to control the use of seda-tion through protocols based on the use of anal-gesics prior to administration of sedation. This helps to reduce the use of hypnotics and improve the practice of sedation in patients in need of mechanical ventilation. Opioids offer lighter sedation, thus facilitate assessment of patients, and provide faster awakening with consequent reduction in length of hospital stay and institu-tional expenditures.(11)
National and international studies emphasize the importance of using scales to assess the levels of sedation in ICUs in order to establish protocols guiding the sedation practice by goals, and patients benefit from shorter hospitalization time, lower in-cidence of nosocomial pneumonias and mortality.(12) However, in the literature and clinical practice, there is little involvement of nurses in relation to established guidelines for the use of sedation and analgesics.(13)
With the use of pain and sedation assessment scales by intensive care unit nurses, the following questions emerge: What is the importance of these sedation and analgesia protocols for the manage-ment of patients’ pain? How does the nurse use these data for decision making on pain and sedoan-algesia? Therefore, the objective of this study was to

242 Acta Paul Enferm. 2017; 30(3):240-6.
Association between intensities of pain and sedation in intensive care patients
identify the clinical profile, intensities of pain and sedation in patients in the intensive care unit, and associate the data.
Methods
A cross-sectional study was conducted at an ICU (clinical, surgical and neurological) divided into 27 beds (17 for clinical and surgical patients, and 10 for neurological patients) of a teaching hospital that is part of the Sentinel Network of the Nation-al Sanitary Surveillance Agency of the northwest-ern region of São Paulo. Data collection was per-formed through the Richmond Agitation-Sedation Scale (RASS) for assessment of the level of sedation; the Visual Numeric Pain Scale (VNS) was used for self-reported pain; and the Behavioral Pain Scale (BPS) for behavioral pain. Clinical data were ob-tained from electronic medical records (gender, age, diagnosis, discharge or death in the hospital and ICU, and length of stay in the ICU).
The sample included 240 patients, considering the inherent rotation of the sector. All hospitalized patients during the data collection period were in-cluded, and those hospitalized for less than 24 hours were excluded. The scales were filled out by nurses from the unit, from Monday to Friday, in alternat-ing periods (morning, afternoon and night), once every 24 hours, next to the patient by the bedside.
From the total sample of 240 patients, 161 could be evaluated for behavioral pain and 140 for self-reported pain. With patients’ clinical evolution throughout the data collection period, 61 patients could be evaluated for behavioral pain at a certain time, and in relation to self-reported pain at anoth-er time, or vice versa. As during hospitalization pa-tients presented changes in levels of consciousness resulting from withdrawal, employment or changes in sedation doses, it was possible to assess the same patient with different scales at different times.
The RASS scores range between -5 and 4; the lower the score the deeper the sedation, and the higher the score the more agitated the pa-tient.(14) In this study, was considered the mean RASS score of each patient that was established
through the applications of the scale. The score classification for the levels of sedation was con-sidered as follows: light sedation (-2 to 4), mod-erate sedation (-2.1 to -3.9), and deep sedation (-4 to -5).
The BPS version translated and validated for the Brazilian reality and used in patients under mechanical ventilation and/or sedated was used for assessment of behavioral pain. Its scores range between 3 and 12; 3 means the patient is without pain and 12 means maximum pain, and the following items are evaluated: facial ex-pression, limbs and compliance with mechanical ventilation.(15) For this study, was considered the mean pain score of each patient that was estab-lished from all applications. Afterwards, the pain intensity was classified into: no pain (3.00 to 3.09), mild pain (3.10 to 4.09), moderate (4.10 to 6.09), severe (6.10 to 11.99), and maximum (12.00). The VNS was used for identification of self-reported pain, when patients with appropri-ate level of consciousness could report the inten-sity of their pain, ranging from 0 (no pain) to 10 (worst possible pain).(16) For this study, the intensity of pain was classified according to the mean scores of each patient obtained from all applications, being 0 to 0.9 (no pain); 1.0 to 3.0 (mild pain); 3.1 to 6.0 (moderate); and 6.1 to 10.0 (severe).
The study complied with resolution 244/12 that involves human beings, and opinion num-ber 984.505. Data were grouped into a database in Excel® 2010 (Microsoft Inc.), submitted to descriptive analysis of the variables of sample characterization, application of analysis of vari-ance (ANOVA) with multiple comparison test of Tukey averages or chi-square test. All statistical analyzes were applied with a significance level of 5% or (P<0.05). The Minitab® 17 software (Minitab Inc.) was used.
Results
Overall, 240 patients were evaluated regarding age, length of stay in the ICU, presence of behavioral

243Acta Paul Enferm. 2017; 30(3):240-6.
Silva DC, Barbosa TP, Bastos AS, Beccaria LM
pain and/or self-reported pain and RASS score. The 161 assessments of behavioral pain and the 140 of pain by self report were evaluated separately, as shown in table 1.
In relation to the total sample (58.7%), patients older than 60 years of age had death as a prevalent clinical outcome, and 65% of those younger than 60 years were discharged. The male gender pre-vailed in 64.5% of discharges, 64.1% of deaths in the ICU, and 70.4% of deaths in the hospital.
Regarding the intensity of behavioral pain, of the 161 patients evaluated, 93 (57.8%) present-ed no pain, 59 (36.6%) had mild pain, and nine (5.6%) had moderate pain. No patient had severe behavioral pain. Male patients presented a mean score of 3.23, and female patients’ mean score was 3.20 hence, both had mild pain.
Regarding self-reported pain, of the 140 patients as-sessed, 106 (75.7%) presented no pain, 28 (20%) had mild pain, four (2.9%) had moderate pain, and two (1.4%) had severe pain. Male patients had a mean score of 0.63 and the female mean score was 0.85, which means both were considered as having no pain. The percentiles for qualitative variables are shown in table 2.
The results related to the use of sedation during hospitalization were grouped according to their inten-sities (light, moderate, deep) and non-sedated patients. For each of these levels, was made an association with quantitative and qualitative variables (Table 3).
Table 1. Quantitative variables of the general profile by behavioral pain and by self-report in intensive care unit patients
Quantitative variables MeanStandard deviation
Median Minimum Maximum
Total patients (240)
Age 55.9 20.7 58.0 15.0 97.0
Length of hospital stay 10.7 9.0 7.5 1.0 47.0
Behavioral pain 3.2 0.5 3.0 2.0 5.8
Self-reported pain 0.7 1.4 0.0 0.0 8.0
RASS -2.9 2.0 -2.6 -5.0 -1.2
Behavioral pain (161)
Age 57.4 20.5 61.0 16.0 97.0
Length of hospital stay 13.2 9.6 10.0 1.0 47.0
RASS -3.5 1.4 -3.8 -5.0 1.0
Self-reported pain (140)
Age 52.1 21.7 53.0 15.0 97.0
Length of hospital stay 9.3 8.9 6.0 1.0 46.0
RASS -1.1 1.6 -0.3 -5.0 1.2
RASS - Richmond Agitation-Sedation Scale
Table 2. Qualitative variables of patients in relation to the total sample regarding the assessment of behavioral pain and self-reported pain in the intensive care unit
Qualitative variablesTotal Behavioral pain Self-reported painn(%) n(%) n(%)
Gender
Male 155(64.6) 108(67.0) 91(65.0)
Female 85(35.4) 53(33.0) 49(35.0)
Type of hospitalization
Clinical 67(27.9) 45(28.0) 41(29.3)
Surgical 173(72.1) 116(72.0) 99(70.7)
Clinical outcome
Discharge 121(50.4) 52(32.3) 101(72.1)
Death in ICU 92(38.3) 93(57.8) 28(20.0)
Death in the hospital 27(11.3) 16(9.0) 11(7.9)
Specialties
Neurology 112(46.7) 75(46.6) 61(43.6)
Others 128(53.3) 86(53.4) 79(56.4)
Level of sedation
Light 66(27.5) 26(16.1) 62(44.3)
Moderate 54(22.5) 54(33.5) 25(17.9)
Deep 78(32.5) 78(48.4) 11(7.9)
Not sedated 42(17.5) 03(1.9) 42(30.0)
ICU - Intensive Care Unit
Table 3. Quantitative variables of patients in relation to sedation levels in intensive care unit
Qualitative variablesLight Moderate Deep
Not sedated p-value
n(%) n(%) n(%) n(%)Gender
Male 42(63.6) 34(63.0) 52(66.7) 27(64.3) 0.864
Female 24(36.4) 20(37.0) 26(33.3) 15(35.7)
Classification of hospitalization
Clinical 14(21.2) 15(27.8) 25(32.0) 13(31.0) 0.428
Surgical 52(78.8) 39(72.2) 53(68.0) 29(69.0)
Clinical outcome
Discharge 53(80.3) 22(40.7) 08(10.3) 38(90.5) <0.001
Death in ICU 08(12.1) 23(42.6) 59(84.3) 02(4.8)
Death in the hospital 05(7.6) 09(16.7) 11(15.7) 02(4.8)
Specialty
Neurology 34(51.5) 23(42.6) 41(52.6) 14(33.3) 0.203
Others 32(48.5) 31(57.4) 37(47.4) 28(66.7)
Quantitative variablesAge
Mean±SD 48.9±21.7 56.1±20.5 62.9±16.6 53.8±22.6 0.001
Median 51.5 57.5 66.5 53.0
Minimum 15 18 20 17
Maximum 90 96 97 91
Length of hospital stay
Mean±SD 12.2±7.1 16.2±9.6 8.4±9.2 4.5±4.8 <0.001
Median 6.0 16 9.5 3.0
Minimum 2 1 1 1
Maximum 46 42 47 27
Behavioral pain
Mean±SD 3.5±0.8 3.3±0.5 3.1±0.3 2.0 -
Median 3.3 3.2 3.0 2.0
Minimum 2.2 2.0 2.2 2.0
Maximum 5.9 5.0 5.0 2.0
Self-reported pain
Mean±SD 0.9±1.6 0.9±1.6 0.5±1.1 0.4±0.7 0.195
Median 0.1 0.0 0.0 0.0
Minimum 0.0 0.0 0.0 0.0
Maximum 8.0 7.5 3.0 2.7
Qualitative variables: p-value for the chi-square test; Quantitative variables: p-value for the ANOVA test - Analysis of variance and Tukey test; ICU - Intensive Care Unit

244 Acta Paul Enferm. 2017; 30(3):240-6.
Association between intensities of pain and sedation in intensive care patients
Discussion
The male gender, age under 60 years old, and mean time of 10.7 days of hospitalization of pa-tients in this study corroborate with recent studies.(12,17,18) The prevalent specialty (neurology) can be justified according to the profile of the studied hos-pital that is a reference in the care of polytrauma patients, and traumatic brain injury (TBI) is the predominant diagnosis in these hospitalizations, which also justifies the higher incidence of surgical hospitalizations (72.1%).
Regarding the clinical outcome, there was prev-alence of discharges compared to deaths in the ICU, differing from the literature findings that show death as the predominant outcome.(12) However, comparing deaths in the ICU and the hospital, the difference was relatively small. Male patients pre-sented higher mortality both in the ICU and after discharge in other hospital admission units.
A study indicates prevalence of deaths in the el-derly, with increased mortality throughout hospital-ization time, and a higher number of discharges for patients younger than 60 years.(17) These data cor-roborate with the present study findings, in which most deaths occurred in individuals aged over 60 years and those younger than 60 years old were dis-charged from the ICU.
In relation to behavioral pain, the majority pre-sented mild pain, and self-reported pain was ab-sence of pain. An international study found 40% of the assessed patients had pain with prevalence of mild to moderate intensity.(12) In another study, mild pain was observed in 65% of patients.(3)
Deep sedation was predominant, but the mean RASS score was equivalent to moderate sedation. For patients assessed for behavioral pain, the RASS score was equivalent to moderate sedation and the length of hospital stay was 2.5 days longer com-pared to the total sample. In patients assessed by self-report, the RASS score was light sedation, as ex-pected. As the effective application of the visual nu-meric pain scale requires that patients are conscious and oriented to report the intensity of pain, the lev-els of sedation must be superficial. The hospitaliza-tion time for this group was reduced by 1.4 days,
compared to the total sample. It was also observed that the higher the intensity of pain the higher the incidence of death.
Regardless of the intensity of sedation (light, moderate and deep), patients presented behavior-al pain varying from mild to moderate intensity. Patients in light and moderate sedation showed self-reported pain ranging from mild to severe in-tensity. Therefore, the use of sedation was effec-tive in pain control, but not sufficient to suppress patients’ pain.
Elderly patients presented lower pain intensi-ty when compared to younger patients. Probably given the weakness of advanced age, lower doses of analgesic-sedative drugs are sufficient for pain relief and their adaptation to invasive conditions inher-ent to hospitalization itself and their clinical status. However, in this study there was no significant as-sociation between pain and age, which is equiva-lent to the recent study in which elderly patients also demonstrated greater tolerance to discomforts resulting from hospitalization, including pain.(18) There was no statistical relevance between inten-sity of behavioral pain and gender, type of hospi-talization (clinical/surgical) and clinical outcome (p>0.05).
Pain is the most found stressor in intensive care units. When untreated, it can lead individuals to present other stressors such as anxiety and agitation.(18) One of the challenges for the treatment of pain is the deficiency of its perception by analyzing body and facial expressions, and identifying its intensi-ty and nature of origin. Even with the initiative to make pain the fifth vital sign, professionals are often passive in relation to this theme, and less than 50% of health professionals perform pain assessment.(3)
In relation to use of sedation, the present study showed a significant association between the lev-els of sedation used and the length of hospital stay (p<0.001). Patients in moderate sedation had lon-ger length of hospital stay, followed by those in deep sedation. On the other hand, patients who were not sedated or in light sedation presented shorter length of hospital stay.
There was a statistical relationship between the intensity of sedation and ICU mortality; the deep-

245Acta Paul Enferm. 2017; 30(3):240-6.
Silva DC, Barbosa TP, Bastos AS, Beccaria LM
er the sedation the greater the number of deaths, and the more superficial (or absent) the sedation the higher the number of discharges (p <0.001). A research on this subject found that patients submit-ted to deep sedation tend to present agitation after the weaning of sedation and psychological changes, even after hospital discharge.(12)
The use of more superficial levels of sedation was observed mainly in younger patients and deep-er levels are used with older patients. Younger pa-tients tend to remain with more superficial sedation and older patients with deeper sedation. Moderate sedation and absence of sedation are commonly ob-served in patients of intermediate ages (less than 60 years). There was no significant association between levels of sedation and gender, type of hospitalization (clinical/surgical), specialty and intensity of pain by self-report (p> 0.05).
Analgesic-sedative drugs are used in intensive care units to reduce stress response and provide com-fort and safety to patients. However, sedoanalgesia must be kept at safe levels, preferably at more superfi-cial levels, so patients are monitored for pain control appropriately without completely suppressing their level of consciousness in a way that they can interact and express their physical and emotional needs
Conclusion
Regarding the clinical profile, most patients were older than 60 years old, male, neurology specialty, surgical, deep sedation level, and the clinical out-come showed higher number of ICU discharges than deaths. Patients in moderate sedation had lon-ger length of stay in the ICU, while young adults (younger than 60 years old) in light sedation had more discharges from ICU and later from oth-er hospitalization units of the hospital. There was pain of mild intensity in sedated patients, therefore, sedation was not effective in suppressing pain, but it provided control of its intensity. In conclusion, nurses’ identification of the intensity of pain and sedation performed with use of scales helps decision making and provides adequate management of se-doanalgesia in the ICU.
CollaborationsSilva DC, Barbosa TP, Bastos AS and Beccaria LM declare they have contributed to project design, analysis and interpretation of data, article writing, critical review of intellectual content and final ap-proval of the version to be published.
References
1. Stein-Parbury J, McKinley S. Patients’experiences of being in an intensive care unit: a select literature review. Am J Crit Care. 2000; 9(1):20-7.
2. Fortunado JGS, Furtado MS, Hirabae LFA, Oliveira JA. Escalas de dor no paciente crítico: uma revisão integrativa. Rev HUPE. 2013; 12(3):110-7.
3. Moreti MC, Mofatto SC, Pereira CA, Silva AP, Odierna MT. Tradução e adaptação cultural da versão portuguesa (Brasil) da escala de dor Behavioural Pain Scale. Rev Bras Ter Intensiva. 2014; 26(4):373-8.
4. Shinotsuka CR, Salluh JI. Percepções e práticas sobre delirium, sedação e analgesia em pacientes críticos: uma revisão narrativa. Rev Bras Ter Intensiva. 2013; 25(2):155-61.
5. Bugedo G, Tobar E, Aguirre M, Gonzalez H, Godoy J, Lira MT, et al. Implantação de protocolo de redução de sedação profunda baseado em analgesia comprovadamente seguro e factível em pacientes submetidos à ventilação mecânica. Rev Bras Ter Intensiva. 2013; 25(3):188-96.
6. Tanios MA, Wit M, Epstein SK, Devlin JW. Perceived barriers to the use of sedation protocols and daily sedation interruption: a multidisciplinary survey. J Crit Care. 2009; 24(1):66-73.
7. O’Connor M, Bucknall T, Manias E. Sedation management in Australian and New Zealand intensive care units: doctors’ and nurses’ practices and opinions. Am J Crit Care. 2010; 19(3):285-95.
8. Basto PA, Soares YO, Oliveira HS, Gonçalves WS, Balestra LF, Gardenchi G. Repercussões da sedação em pacientes internados em unidades de terapia intensiva: uma revisão sistemática. ASSOBRAFIR Ciênc. 2014; 5(2):59-72.
9. Reade MC, Finfer S. Sedation and delirium in the intensive care unit. N Engl J Med. 2014; 370(5):444-54.
10. Puntillo KA, Arai S, Cohen NH, Gropper MA, Neuhaus J, Paul SM, et al. Symptoms experienced by intensive care unit patients at high risk of dying. Crit Care Med. 2010; 38(11):2155-60.
11. Dias DS, Resende MV, Diniz GC. Estresse do paciente em terapia intensiva: comparação entre unidade coronariana e pós-operatória geral. Rev Bras Ter Intensiva. 2015; 27(1):18-25.
12. Costa JB, Marcon SS, Macedo CR, Jorge AC, Duarte PA. Sedação e memórias de pacientes submetidos à ventilação mecânica em unidade de terapia intensiva. Rev Bras Ter Intensiva. 2014; 26(2):122-9.
13. Barbosa TP, Beccaria LM, Pereira AM. Avaliação da experiência de dor pós-operatória em pacientes de unidade de terapia intensiva. Rev Bras Ter Intensiva. 2011; 23(4):470-7.
14. O’Connor M, Bucknall T, Manias E. Sedation management in Australian and New Zealand intensive care units: doctors’ and nurses’ practices and opinions. Am J Crit Care. 2010; 19(3):285-95.
15. Berbigier EJ. Estudo comparativo da clonidina com a dexmedetomidina para a sedação do paciente crítico sob ventilação mecânica

246 Acta Paul Enferm. 2017; 30(3):240-6.
Association between intensities of pain and sedation in intensive care patients
[dissertação]. Florianópolis: Universidade Federal de Santa Catarina; 2012.
16. Shehabi Y, Bellomo R, Reade MC, Bailey M, Bass F, Howe B, et al. Early intensive care sedation predicts longterm mortality in ventilated critically ill patients. Am J Respir Crit Care Med. 2012; 186(8):724-31.
17. Freitas ER. Perfil e gravidade dos pacientes das unidades de terapia intensiva: aplicação prospectiva do escore APACHE II. Rev Lat Am Enfermagem. 2010; 18(3):20-6.
18. Rosa BA, Rodrigues RC, Galani MC, Spana TM, Pereira CG. Estressores em unidade de terapia intensiva: versão brasileira do The Environmental Stressor Questionnaire. Rev Esc Enferm USP. 2010; 44(3):627-35.

247Acta Paul Enferm. 2017; 30(3):247-53.
Original Article
Nursing Education: conceptualizing a pedagogical project from the view of professors
Educação em Enfermagem: conceituando projeto pedagógico na visão de professores
Solange Maria Fustinoni Magalhães1
Maria Cristina Gabrielloni2
Maria Cristina Sanna2
Márcia Barbieri2
Corresponding authorSolange Maria Fustinoni MagalhãesAfonso Celso street, 711, 04119-060, São Paulo, SP, [email protected]
DOIhttp://dx.doi.org/10.1590/1982-0194201700038
1Centro Universitário Assunção, São Paulo, SP Brazil.2Escola Paulista de Enfermagem, Universidade Federal de São Paulo, SP Brazil.Conflicts of interest: there are no conflicts of interest to declare
AbstractObjective: To understand the pedagogical project concept of the professors of the Paulista School of Nursing, and to identify the challenges and the limits faced by them during its development.Methods: Qualitative study, in the oral history thematic modality. Using semi-structured interviews, the narratives of six professors who participated in, at least, half of the meetings for the pedagogical development were obtained. The statements were recorded, interpreted text transcribed, recreated and analyzed, respecting the methodological steps and ethical precepts. The Social World Theory of Pierre Bourdieu was used as a reference for analysis.Results: The concept of the pedagogical project was limited to the curriculum frameworks; training of the professors is the main difficulty for the planning phase of the paradigmatic change.Conclusion: Professors value the pedagogical project development, but do not advance the proposition because they are steeped in previous models that support workload and organization according to specialty.
ResumoObjetivo: Apreender o conceito de Projeto Pedagógico dos professores da Escola Paulista de Enfermagem e identificar os desafios e os limites enfrentados por eles durante sua elaboração.Métodos: Estudo qualitativo, na modalidade História Oral Temática. Por meio de entrevistas semiestruturadas obtiveram-se as narrativas de seis professores que participaram de, no mínimo, metade dos encontros para essa construção. Os depoimentos foram gravados, transcritos, transcriados e analisados, respeitando-se as etapas do método e os preceitos éticos. Foi utilizada a Teoria de Mundo Social de Pierre Bourdieu como referencial de análise.Resultados: O conceito de Projeto Pedagógico ficou circunscrito à grade curricular e a formação docente é a principal dificuldade para a mudança de paradigma na ação do planejamento.Conclusão: Os docentes valorizam a elaboração do Projeto Pedagógico, mas não avançam na proposição porque estão fixados em modelos anteriores que privilegiam a carga horária e a organização por disciplinas.
KeywordsEducation, nursing; Education higher;
Curriculum
DescritoresEducação em enfermagem, Ensino
superior, Curso de enfermagem, Currículo
Submitted February 22, 2017
Accepted June 5, 2017

248 Acta Paul Enferm. 2017; 30(3):247-53.
Nursing Education: conceptualizing a pedagogical project from the view of professors
Introduction
The process of the Pedagogical Project of the Cur-riculum (PPC) development of the undergraduate nursing program of Paulista School of Nursing (Es-cola Paulista de Enfermagem -EPE) of the Federal University of São Paulo (Universidade Federal de São Paulo- UNIFESP) during the period of 2010-2012, was a remarkable experience that should be stud-ied, due to the reference-model role played by this institution.
Currently, much has been discussed about the importance of the pedagogical project (PPC) devel-opment. A collective development is proposed, in a conscious movement of cooperation and solidarity. Based on this premise, it is opportune to understand the perception of the professors who participated in the aforementioned development process. The perception here is understood as the dimension of knowledge, and not just as learning by the senses.(1)
According to the National Education Guide-lines and Bases law (Lei de Diretrizes e Bases da Educação Nacional - LDB 9394/96),(2) educational institutions are responsible for organizing pedagog-ical proposals and reflecting on their education-al intention, an action which must be collectively conducted, with the participation of the different individuals involved in the school.
The PPC consists of a set of collective actions that aimed to create structural changes in the orga-nization of the pedagogical work. It is a fact that its development occurs within a dynamic, continuous, flexible and unfinished process; it requires a perma-nent commitment from its participants, which is necessary for its transformation.(3)
This project requires deep reflection on the in-stitution’s purposes, its social role, and a clear defi-nition of the path to be followed and the operation-alization of the actions that will be undertaken.(4-6)
The priorities of citizen development, pedagogical and didactic activities that led the institution to reach its goals are expressed in the PPC.(7-9)
Teaching in the health care is a challenge for higher education institutions (Instituições de ensino superior-IES) to think the PPC as a training model capable of transforming practices, seeking to over-
come the health problems and improving the in-dividual and collective health care.(10,11) The EPE, founded in 1939, sought to adapt the course to the determinations of the regulatory teaching agencies and the nursing profession. This behavior was fixed in its teachers, who show difficulty in breaking with this model.
Changing in education implies disrupt with crystallized practices and confronting challeng-es in search of a formation that contemplates the needs pointed out in the policies established by the Ministry of Education and Health, as well as the priorities and principles of the Unified Health System (Sistema Único de Saúde-SUS), as well the needs of changes indicated by the professionals of the health area.(10,12)
Given this background, it is imperative to cap-ture the concept of the Pedagogical Project (PPC) from the EPE- UNIFESP professors, and to identify the challenges and limits faced by them during its development, as the school should be seen as a producer of knowledge - not merely as reproducers of knowledge - and the professors must discuss the factors that enable its selection and organization.(13,14)
Methods
The method used in the study was that of an oral history (OH), which provides qualitative interpre-tations of historical-social processes and, by means of precise methods and techniques in which the constitution of sources and oral files plays an im-portant role, which aims to highlight and focus analysis according to the experience of social indi-viduals. Oral history means to produce historical and scientific knowledge, not simply to provide an organized report of the life and/or experiences of individuals.(15)
Listening to the narratives of the EPE professors who participated in the development of the PPC, in the period between 2010-2012, enabled us to ob-tain a volume of original and relevant data. Among the types of OH, thematic oral history was the one that best met the purposes of the study.(16)

249Acta Paul Enferm. 2017; 30(3):247-53.
Magalhães SM, Gabrielloni MC, Sanna MC, Barbieri M
The study scenario was the Paulista School of Nursing (EPE - UNIFESP), a septuagenarian insti-tution that has been continuously educating nurses, and has become a reference for this practice in the country. It was decided to listen to the statements of the EPE professors who contributed to the develop-ment of the PPC, with eligibility criteria including: participation in at least 50% of the meetings con-ducted for this purpose, names identified by means of attendance lists and meeting minutes compris-ing six subjects. These subjects agreed to partici-pate, after being contacted, and were presented the study objectives and signed the Terms of Free and Informed Consent form (TFIC). It also contains the cession statement for research purposes, which eliminates the requirement for a copyright assign-ment letter. These subjects were identified by letters of the alphabet, according to the order of the inter-views. The project was previously submitted to the Research Ethics Committee of the Federal Universi-ty of São Paulo (Universidade Federal de São Paulo), and was approved on September 24, 2014, under protocol No. 804,651.
Interviews were scheduled, and the participant was aware that electronic recording would used to support data collection. The interview was conduct-ed by a researcher who had no ties with the par-ticipants. The meetings were scheduled according to the availability of each interviewee and, when necessary, repeated until the subject matter was ex-hausted; in some cases, two to three meetings were necessary to clarify and deepen the information provided in previous interviews.
A semi-structured interview script was used to obtain the statements, and the guiding question was: “How did you, [name of the participant], per-ceive the collective development of the PPC at the Paulista School of Nursing, during the 2010-2012 period?” According to the narrative evolution, the need for resumption of focus and deepening of some aspects, other questions were added, based on the script.
Following the steps of the method, the recorded interview was transcribed in full and sent to the par-ticipant for knowledge and validation. At that mo-ment, he/she was able to review the text and make
changes, if necessary. Once the participant was sat-isfied with the text, each page was printed with the transcribed text of his/her interview, initialed by the interviewee, and then archived.
Subsequently, a copy of these validated tran-scripts was subjected to repeated readings by the principal investigator, coding of the texts with let-ters and numbers in the excerpts that dealt with the same subject. The related themes were grouped after coding, from which the transcribed text was developed, receiving a treatment that ordered the text in a linear and non-recurrent narrative, as occurs with speech, approaching the reader and better communicating the meaning, but keeping the original intention of what was recorded.(16,17)
A doctorally prepared nurse, who was expert in the HO method, but not linked to the research in focus, compared this transcript with the text of the transcript initialed by the interviewee, to verify if the intentionality contained in the reports was not modified in that process and if all the information, impressions and opinions on the object of study enunciated by the interviewee were included, vali-dating the interpreted text.
After this validation of the interpreted text, the previously assigned codes that were grouped by sim-ilarity and thematic pertinence, three categories of analysis emerged, which were again validated by a doctorally prepared nurse and then analyzed and discussed following the literature on the object of study, and the concepts of Pierre Bourdieu.(18) This paper will present the results corresponding to the Vision category about the pedagogical project.
Bourdieu considered the school to be a space for the reproduction of social structures, capital transfers, and of legitimating positions in the field, defined as a system or a structured space of positions.(18)
The EPE-UNIFESP is a social space of profes-sorial action, of those who participate in educating nurses. This institution is a scientific field, endowed with a force, which confers on its social members a certain cultural, social and economic capital.
So, if the school is a field, that is, a space in which cultural capital is transferred and that con-tributes to the formation of habitus, the develop-

250 Acta Paul Enferm. 2017; 30(3):247-53.
Nursing Education: conceptualizing a pedagogical project from the view of professors
ment of a PPC and a curricular matrix is not isolat-ed from the internal dynamics of a field, its agents, their positions, and the relationships resulting from this process.(19,20)
One of these positions is that of pedagogical ac-tion, because it selects and legitimizes the culture through imposition and inculcation, seeking to form the individual’s habitus according to the dom-inant culture. The greater the prestige and recogni-tion of the institution, the greater its pedagogical authority and its cultural capital.
Results and Discussion
As a result, the transcription of the interviews gen-erates the statements for analysis. Analyzing the statements, the professor point of view about the pedagogical project emerged, as presented below.
The need for schools to adapt their pedagogical projects and their curricular organization to meet the demand of students has been indicated within the scientific literature, to guarantee quality edu-cation and to seek critical and reflexive autonomy.(10,21) Therefore, it is necessary to break with the certainties of what is already established. The state-ment of Subject B, denotes that EPE professors are concerned about undertaking changes that meet the demands for nurses’ education:
Everyone knows about the importance of a PPC in any institution that has, as an objective, the matter of education, and here, in the nursing school, it would not be different. (...) Society is changing as well as technologies and, at some point, we have to sit down and discuss what happened to evaluate and propose changes. (Subject B)
The statement of the subject above, reinforc-es the need for the HEI to assume the political pedagogical commitment and aware that it must be realized and collectively accepted, with the in-volvement of each one in the process. However, the statement of subject B showed that not everyone participated, which impacted on the process of the proposal adherence.
I mean the absence, even in the discussion, in the debate. Let’s talk about the frequency: we can even
compare, in an objective way, with the presence list ... how many professors have established the plan of the institution and how many were actually pres-ent and participated in this discussion, this develop-ment, 90%? I do not think so. It was 50%? 40%? (Subject B)
The LDB 9394/96 requirements, the Law of the Professional Exercise of Nursing and the National Curriculum Guidelines for Health and Nursing were met during the development of the PPC at EPE, in addition to the discussions conducted by the Brazil-ian Association of Nursing (Associação Brasileira de Enfermagem - ABEn) in the National Seminar on Guidelines for Nursing Education (Seminário Na-cional de Diretrizes para o Ensino de Enfermagem - SENADEns), and health-inducing policies, which are indicated as guiding elements,(22,23) as perceived in the statement of Subject C.
One of the challenges was to try to deconstruct what we already had in the PPC, and that was not responding to the organizations, to the MEC, LDB, MEC Curriculum Guidelines, and the market needs. (Subject C)
It can be verified that only those internal to the school are able to attribute identity to the PPC. This identity of nurses to be educated means, above all, the result of collective reflections, considering the organization of the pedagogical work, and the reality in which the EPE is integrated.
During the restructuring process of the PPC-EPE, an understanding was identified about the concept and importance of the project to the con-struction of the institution’s identity, because the school is organized to transmit culture, procedures and reflective programs, and acts as a habit-forming force that facilitates this transmission, based on the Bordieu statements,(20,23) as reported by Subject F:
The construction of this pedagogical project is not just to do it. It is dynamic and continuous. If we lose the comprehensive picture, if we do not have moments to look, discuss and think about what is working, what has already been integrated and what has not, where are the edges, what remains detached. It is in that sense. (Subject F)
This action was permeated by limits that brought difficulties. Every debate and decision making pro-

251Acta Paul Enferm. 2017; 30(3):247-53.
Magalhães SM, Gabrielloni MC, Sanna MC, Barbieri M
cess in the collective sphere presented difficulties, and the same thing happened in the development of PPC. Changes imply giving up the safety of what is already done and, often, this makes the position taken difficult, generating conflicts.(5,7,24)
The statements of the interviewed subjects, some limits were indicated, such as the length of the process, absence of and lack of commitment of professors in the discussion, which made the pro-cess tiring, often leading to the closure of the dis-cussions to be performed by small groups, as stated by Subject C.
“Wow! What a lack of vision!” A boycott of igno-rance and aiming to maintain power. Because there was no opportunity for deeper discussion. People from the UEL (University of Londrina), University of São Paulo (USP) also presented changes made in their cur-ricula. It was interesting, but there was no quorum. Always the same people take part, watch and discuss (...) But, between quotation marks: “whoever needs it most, does not come, stays out of this activity.” There were many unpleasant things. The way people acted, derived the most profound strength of the pedagogical discussion, the way you want to get with the student, the profile. (Subject F)
For Bourdieu,(19) this power mentioned by Subject F is represented by symbolic capital. This capital gives a certain power, and it is valued by a certain social group.(19,24) This force may lead some people to conformity, leading them to uncritical positions, because for these subjects, the context is seen from the perspective of no change, as reported by Subject D.
“I found it tiring. In the end, sometimes we were exhausting these discussions and had no more idea of how to discuss, to put together, being democratic. I felt that sometimes ideas were accepted, because it was that, there was no more, and if something were main-tained according to the group perceptions, we had great changes.” (Subject D)
For the subjects to consider the changes to be necessary, they must perceive it, participate in the decisions and be willing to undertake them. As stated by subject E, this effective participa-tion also needs to be deepened with regard to the pedagogical issues.
Most of us, professors and administrative techni-cians, stop being a nurse one day to become a teach-er in the other; that is, we do not have didactic and pedagogical training, and that is where the limitation begins. The limit is that, to change and broaden my view, I also need to learn. We had to provide this for yesterday, for teachers and, in a general way, to be able to improve this pedagogical didactic part. We always talk, here at school, about providing this to teachers, so they can be qualified, improve, but I don’t see any progress.” (Subject E)
Bourdieu’s(19) approach leads us to consider that pedagogical practice without knowledge and reflec-tion plays the sole function of inculcating habitus, which tends to reproduce social inequalities, which seem to be incapable of transforming themselves in the light of new educational paradigms.
As seen, the PPC-EPE development process presented limits and, ahead of these, a series of challenges to be overcome were identified, such as: greater integration among professors and under-standing of the concept of interdisciplinarity and its implications in the teaching-learning process.
Interdisciplinarity appeared in the discourse of several subjects, but was presented in a simplistic view of the concept, as can be seen in the statement of Subject B, for whom the proposal is only a result of integration, in the sense of joining content and not the relationship between disciplines:
To optimize this design, in order to reduce the workload, the idea was that content would not be re-peated. (...) The interdisciplinary question is discussed. In my view, we did not progress on this because we did not make this communication between disciplines. The discourse of every one is that their specialty is more im-portant, because only it will give this knowledge; thus, it cannot be cut.” (Subject B)
It should be emphasized that the concept of in-terdisciplinarity goes beyond the content/specialty relationship; is based on the interaction between two or more specialties on the scope of knowledge, methods and learning, breaking with the paradigm of isolated specialties, as it involves questions about the meaning and relevance of the collaboration of the specialties, searching for knowledge, according to the degree of integration between them.(25)

252 Acta Paul Enferm. 2017; 30(3):247-53.
Nursing Education: conceptualizing a pedagogical project from the view of professors
The statements showed the need for professors to acquire pedagogical knowledge that guides the elaboration of a PPC, conferring on it its own iden-tity and not only constituting itself in a list of spe-cialties and isolated content that present specialties hierarchically.
The symbolic power was exercised in the discus-sions of the PPC of EPE, according to the interview-ees, because not all participated effectively, allowing decisions to be made by a small group. This result was also attributed to the fact that some individuals did not feel they were active subjects in the process, and considered themselves devalued by their posi-tion in the field, and as coping strategies these in-dividuals delegated to others this decision-making role in the definition of PPC.
It can be seen that the school must break with fragmentation and hierarchical control, and devel-op conditions to generate other forms of pedagogi-cal work. Applying the Bourdieu concept, it can be said that it is in the relationship between the agents and the structure that transformations in the hab-itus are possible. The teaching process requires the development of necessary skills so that, in a con-crete situation, the acquired theoretical resources are mobilized, allowing the transformation of in-culcated habitus.(19,20)
This reorganization must begin from the in-side out, with a collective commitment, in order to break with what exists and no longer simply meet current needs, but rather move forward. Thus, the PPC will be a reflection of daily life and not just a document to be followed, as it re-quires continuity of actions, decentralization of power, democratization in decision making, and a process of continuous assessment of an eman-cipatory nature.
Conclusion
It is possible to identify that professors understood the significance of the PPC, recognized the meaning and importance of its development to be conduct-ed collectively, as well as perceived the role played as a guiding instrument of the HEI. However, it
is concluded that, in this process of development, the inflexibility of some social individuals led to the difficulty of reaching a common denominator, con-stantly causing the emptying of decisions.
The process of the PPC - EPE development was not freed from the condition of symbolic power, and its development ended up an arena of conflicts in the face of the difficulty of letting go of the education references, elements that com-prise the habitus of the group, which are inculcat-ed and, therefore reproduced without reflection. The discussions were marked by moral values in-culcated in the professorial educational process, that tend to prioritize the amount of content, valuing the curricular matrix much more than other elements that compound the project, such as: curriculum typology, teaching-learning strat-egies, and forms and instruments of evaluation. It is pertinent to emphasize that these consid-erations were due to the analysis of the percep-tions revealed by the interviewed professors of this teaching institution during this process of development of the PPC, and indicate that there is still a long way to go in the direction of the ap-propriation of the pedagogical concepts, as well as how to deal with the resistances and obstacles in the teaching practice.
AcknowledgementsTo the Paulista Nursing School of UNIFESP for the support received, to the Committee of Studies of the Nursing Curriculum (Comissão de Estudos do Currículo de Enfermagem - CECE) that allowed the participation in the meetings for development of the Pedagogical Project, and to the research groups in Obstetric Nursing Research Center (Centro de Estudos em Enfermagem Obstétrica - CENFOBS), and Group of Studies and Research in Administra-tion of Health Services and Nursing Management (Grupo de Estudos e Pesquisa em Administração dos Serviços de Saúde e Gerenciamento de Enfermagem- GEPAG).
CollaborationsMagalhães SMF, Gabrielloni MC, Sanna MC, and Barbieri M contributed to the study design, analy-

253Acta Paul Enferm. 2017; 30(3):247-53.
Magalhães SM, Gabrielloni MC, Sanna MC, Barbieri M
sis and data interpretation, revision of the article, relevant critical review of the intellectual content, and final approval of the version to be published. It should be noted that there are no conflicts of in-terest for the authors, all of whom contributed in a fundamental way to the conduct of this study.
References
1. Nóbrega TP. Corpo, percepção e conhecimento em Merleau-Ponty. Estudo Psicol. 2008; 13(2):141-8.
2. Brasil. Leis, Decretos. Lei 9394, de 20 de dezembro de 1996. Estabelece as diretrizes e bases da educação nacional [online]. [citado em 2013 Jan 20] Disponível em: http://www.planalto.gov.br/ccivil_03/leis/l9394.htm.
3. Ito EE, Peres AM, Takahashi T, Leite MM. O ensino de enfermagem e as diretrizes curriculares: utopia x realidade. Rev Esc Enferm USP. 2006; 40(4):570-5.
4. Batista NA. Planejamento na prática docente em saúde. In: Batista NA, Batista SH, organizadores. Docência em saúde. São Paulo: SENAC; 2004. p.35-56.
5. Abdalla IG, Stella RC , Perim GL, Silva RH , Lampert JB, Costa NM Projeto pedagógico e as mudanças na educação médica. Rev Bras Educ Med. 2009; 33(1Supl.1):44-52.
6. Silva VG. Projeto pedagógico e a qualidade do ensino público: algumas categorias de análise. Cad Pesq. 2012; 42(145):204-55.
7. Nobrega-Therrien SM, Guerreiro MG, Moreira TM, Almeida MI. Projeto Político Pedagógico: concepção, construção e avaliação na enfermagem. Rev Esc Enferm USP. 2010; 44(3):678-86.
8. Venâncio L, Darido SC. A educação física e o projeto político pedagógico: um processo de construção coletiva a partir da pesquisa ação. Rev Bras Educ Fis Esporte. 2012; 26(1):97-109.
9. Lima JO, Esperidião E, Munari DB, Brasil VV. A formação ético-humanista do enfermeiro: um olhar para os projetos pedagógicos dos cursos de graduação em enfermagem de Goiânia, Brasil. Interface Comun Saúde Educ. 2011; 15(39):111-25.
10. Souza MC de, Otoni A, Santos LL dos, Campos LG, Oliveira V J de. Oficina sobre projeto pedagógico de curso de enfermagem: refletindo sobre inovações, desafios e potencialidades. Rev Enf Ref. 2012; serIII( 8 ): 67-73.
11. Brasil. Ministério da Educação. Conselho Nacional de Educação. Câmara de Educação Superior. Parecer CNE/ CES n. 1133, de 7 agosto de 2001. Institui as diretrizes curriculares nacionais dos cursos de graduação em Enfermagem, Medicina e Nutrição. Diário Oficial da República Federativa do Brasil [Internet]. Brasília (DF), 03 out. 2001. [citado 2014 Abr 14]. Disponível em: http://portal.mec.gov.br/dmdocuments/ces1133.pdf.
12. Backes A, Silva RP. Rodrigues RM. Reformas curriculares no ensino de graduação em Enfermagem: processos, tendências e desafios. Ciênc Cuid Saúde. 2007; 6(2):223-30.
13. Andrade MR, Bagnato MH. Políticas de formação para os profissionais da área da saúde ou políticas de mudanças na formação na área da saúde. In: Silva NM, Rausch RB, organizadores. Formação de professores: políticas, gestão e práticas. Blumenau: Edifurb; 2010.
14. Corbucci PR. Desafios da educação superior e desenvolvimento no Brasil. Brasília(DF): IPEA; 2007.
15. Ferreira MM, Amado J. Usos e abusos da história oral. 8ª ed. Rio de Janeiro: Fundação Getúlio Vargas; 2008.
16. Meihy JC, Holanda F. História oral: como fazer, como pensar. 2ª ed. São Paulo: Contexto; 2013.
17. Padilha MI, Borestein MS, Bastiani J, Zytkuewisz GV, Lessmann JC. As fontes históricas em pauta: a história oral e a pesquisa documental. In: Borestein MS, Padilha MI. Enfermagem em Santa Catarina: recortes de uma história (1900-2011). Florianópolis (SC): Secco; 2011. p. 37-55.
18. Ortiz RA sociologia de Pierre Bourdieu. São Paulo: Olho D’Água, 2013.
19. Bourdieu P. A economia das trocas simbólicas. São Paulo: Perspectiva; 2005.
20. Pinto L. Pierre Bourdieu e a teoria do mundo social. Rio de Janeiro: FGV; 2000.
21. Silva KL, Sena RR, Silveira MR, Tavares TS, Silva PM. Desafios na formação do enfermeiro no contexto da expansão do ensino superior. Rev Esc Anna Nery. 2012; 16(2):380-7.
22. Rodrigues AM, Freitas CH, Jorge MS, Guerreiro MG, Santos DC. Projetos políticos pedagógicos e sua interface com as Diretrizes Curriculares Nacionais da Enfermagem. Rev Eletr Enf. 2013; 15(1):182-90.
23. Mafra IF, Souza NV, Fernandes MC, Correia LM, Penna LG. Projeto político pedagógico: fragilidades e potencialidades vividas por docentes universitários de enfermagem. Rev Enferm UERJ. 2013; 21(3):361-5.
24. Ferrari GV. A importância do coletivo na construção do projeto político pedagógico na instituição escolar. Perspectiva. 2011; 35(132):159-70.
25. Penteado CL, Silva JS, Fonseca KC. Humanidades na UFABC: produção do conhecimento interdisciplinar na pós-graduação. Rev Bras Pós-graduação. 2015; 12(28):475-500.

254 Acta Paul Enferm. 2017; 30(3):254-61.
Original Article
Hospitalizations of children for preventable conditions in the state of Parana: causes and trendsHospitalizações de crianças por condições evitáveis no Estado do Paraná: causas e tendênciaKelly Holanda Prezotto1
Maicon Henrique Lentsck2
Tirza Aidar3
Hosanna Pattrig Fertonani4
Thais Aidar de Freitas Mathias4
Corresponding authorKelly Holanda PrezottoHighway BR 369, km 51,86360-000, Bandeirantes, PR, [email protected]
DOIhttp://dx.doi.org/10.1590/1982-0194201700039
1Universidade Estadual do Norte do Paraná, Jacarezinho, PR, Brazil.2Universidade Estadual do Centro Oeste, Guarapuava, PR, Brazil.3Universidade Estadual de Campinas, Campinas, SP, Brazil.4Universidade Estadual de Maringá, Maringá, PR, Brazil.Conflicts of interest: no conflicts of interest to declare.
AbstractObjective: To analyze the trends of hospitalizations for ambulatory care-sensitive conditions, according to the main causes among children under five years old.Method: Ecological time-series study carried out with data from the Hospital Information System of the State of Parana. The analysis was based on hospitalization rates and polynomial regression models according to age and cause.Results: The most frequent causes were pneumonia, gastroenteritis, asthma, kidney and urinary tract infection and nutritional disorders. Hospitalizations for pneumonia, asthma and nutritional deficiencies decreased among children under five and hospitalizations rates for gastroenteritis remained stable. There was an increase in hospitalization rates for kidney and urinary tract infection in all ages.Conclusion: Hospitalization for care-sensitive conditions among children under five years presented an increasing trend only for children under one year old. Hospitalizations for pneumonia, gastroenteritis, asthma and nutritional deficiencies showed a decreasing trend.
ResumoObjetivo: Analisar a tendência das hospitalizações por condições sensíveis à atenção primária, segundo principais causas em menores de cinco anos.Métodos: Estudo de séries temporais do tipo ecológico realizado com dados do Sistema de Informação Hospitalar do Estado do Paraná. A análise ocorreu a partir das taxas de hospitalização e de modelos de regressão polinomial segundo idade e causa.Resultados: As causas mais frequentes foram pneumonias, gastrenterites, asma, infeção no rim e trato urinário e deficiências nutricionais. As hospitalizações por pneumonia, asma e deficiências nutricionais em menores de cinco anos reduziram e por gastroenterites mantiveram-se estáveis. Houve aumento nas taxas de hospitalização por infecção no rim e trato urinário em todas as idades.Conclusão: A tendência de hospitalização por condições sensíveis em menores de cinco anos foi crescente apenas para as crianças menores de um ano. As hospitalizações por pneumonias, gastroenterites, asma e deficiências nutricionais apresentaram tendência decrescente.
KeywordsHospitalization; Primary health care; Health profile; Pediatric nursing; Child
DescritoresHospitalização; Atenção primária à saúde; Perfil de saúde; Enfermagem pediátrica; Criança
Submitted February 23, 2017
Accepted June 5, 2017

255Acta Paul Enferm. 2017; 30(3):254-61.
Prezotto KH, Lentsck MH, Aidar T, Fertonani HP, Mathias TA
Introduction
Ambulatory Care-Sensitive Conditions - ACSC are conditions that can be managed through an adequate assistance in the Primary Health Care – PHC.(1) Hospitalizations for these con-ditions are understood as preventable, since the causes should be handled at a primary level of care. Therefore, these hospitalizations have been widely used as indicators of the impact of public policies and the accessibility and quality of basic health services.(1-3)
In the field of child health, hospitalizations for ACSC indicate poor attention in primary care, especially since children are considered a priority due to their susceptibility to illness.(4) The importance of primary care for the preven-tion of hospitalizations is emphasized in sever-al studies, such as one conducted in the United States, which concluded that children who were attended by ambulatory care teams with preven-tive actions and early detection of health prob-lems had a significant reduction in hospitaliza-tion.(5) In Brazil, hospitalizations of children for ACSC still have a high incidence.(6)
Data on the main causes and the trends of hos-pitalizations for ACSC contribute to support man-agers and health professionals, especially nurses, in planning and implementing actions to combat the most frequent diseases that affect this population and that can be treated in PHC, thus preventing unnecessary hospitalizations.(3)
An important Brazilian tool that profession-als can use to find data on these hospitalizations is the Hospital Information System (SIH-SUS). The SIH-SUS provides reliable data for epidemi-ological analysis, mainly due to the advantage of covering the entire national territory and all hos-pitalizations funded by the public health sector.(7) This source is useful for health professionals and managers and includes data on the impact of hospitalizations for ACSC in the country. A survey conducted in the western region of the State of Paraná using data from the SIH-SUS identified that 55.6% of hospitalizations were for respiratory problems, 14.8% for infectious
and parasitic diseases and 12.9% for diseases in the perinatal period, all ambulatory care-sensi-tive conditions.(7)
This study was proposed considering the prior-ity of child health and the need to indirectly assess the quality of primary care and the availability of a safe data source, so that actions can be better tar-geted. Up to the present no other research was con-ducted on the causes, behavior and trends of hospi-talizations of children for ACSC over the last years in the State of Paraná.
Thus, this study aimed to analyze the main causes and the trends of hospitalizations for ACSC among children under five years of age living in the State of Paraná - Brazil from 2000 to 2015.
Methods
This is an ecological time-series study based on all hospitalizations of children under five years of age residing in the State of Paraná - Brazil, occurred between 2000 and 2015 and funded by the Unified Health System - SUS. The data used are available in the SIH-SUS, a tool that system-atizes information from the Authorization for Hospital Admission (AHA), a document based on the medical report and filled at the time of hospitalization. The data were arranged using the official software of the Ministry of Health - Tabwin and are available according to the month and the year. Therefore, twelve files were ob-tained for each year of the study.
After the selection of all hospitalizations in the State of Paraná, hospitalizations of children under 5 years of age were identified, extension AHAs were excluded (type 5 AHA), residence addresses were confirmed and the hospitalization diagnoses were classified (Figure 1).
The Brazilian National List of Ambulatory Care-Sensitive Conditions - LCSAP, composed of 19 diagnosis-related groups based on the 10th revi-sion of the International Classification of Diseases - ICD 10, was used to select the diagnoses of interest: vaccine-preventable diseases and avoidable condi-

256 Acta Paul Enferm. 2017; 30(3):254-61.
Hospitalizations of children for preventable conditions in the state of Parana: causes and trends
tions (A33-A37, A95, B16, B05-B06, B26, G00.0, A17.0, A19, A15-A16, A18, A17.1-A17.9, I00-I02, A51-A53, B50-B54, B77), infectious gastroenteri-tis and its complications (E86, A00-A09), anemia (D50), nutritional deficiencies (E40-E46, E50-E64), infections of the ear, nose and throat (H66, J00-J03, J06, J31), bacterial pneumonia (J13-J14, J15.3-J15.4, J15.8-J15.9, J18.1), asthma (J45-J46), lower respira-tory diseases (J20, J21, J40-J44, J47), hypertension (I10-I11), angina pectoris (I20), cardiac insufficien-cy (I50, J81), cerebrovascular conditions (I63-I67, I69, G45-G46), diabetes mellitus (E10-E14), epi-lepsies (G40-G41), kidney and urinary tract infec-tions (N10-N12, N30, N34, N39.0), skin and sub-cutaneous tissue infections (A46, L01-L04, L08), pelvic inflammatory disease in females (N70-N73, N75-N76), gastrointestinal ulcer (K25-K28, K92.0, K92.1, K92.2) and conditions related to prenatal care and childbirth (O23, A50, P35.0).
Hospital morbidity was analyzed by absolute and relative frequencies, for three years. Trends were calculated based on hospitalization rates (per 10,000 inhabitants of each age group). The censuses and
estimates of the Brazilian Institute of Geography and Statistics (IBGE) were used as data source of the resident population between the years of 2000 and 2012. For the years of 2013 to 2015 statistical projections were calculated. Polynomial regression models were constructed according to age and cause of hospitalization.
The hospitalization rate was considered as de-pendent variable (Y) and the calendar years as in-dependent variable (X). The variable year was trans-formed into the variable year-centered, that is, X= Year - 2007, the midpoint of the time-series, and the simple linear regression models (Y=β0+β1X), the second-degree models (Y=β0+β1X+β2X
2) and the third degree models (Y=β0+ β1X + β2X
2 + β3X3)
were tested. Scatter diagrams were constructed con-sidering rates and calendar years to identify the most appropriate function. A trend in which the estimat-ed model presented p<0.05 was considered signif-icant and the parsimony principle was taken into account when two models were statistically similar. The Excel® software was used for organization of the data and calculation of hospitalization rates and the
Figure 1. Process of identification of hospitalizations of children under five years of age
Hospitalizations in the State of Paraná, from January 1st, 2000 to December 31st, 2015.
12,449,577
Hospitalizations of children under five years of age1,031,991
Hospitalizations of residents under five years of age1,024,951
Hospitalizations of patients over five years of age excluded
11,417,586
Type 5 AHA excluded97
Hospitalizations for other conditions922,935
Hospitalizations for ambulatory care-sensitive conditions
102,016
Hospitalization of non-residents excluded
6,943Excluded from analysis

257Acta Paul Enferm. 2017; 30(3):254-61.
Prezotto KH, Lentsck MH, Aidar T, Fertonani HP, Mathias TA
Statistical Package for the Social Sciences® - SPSS 18.0 software was used for statistical analysis.
The study did not name the hospitalized children; therefore, exemption from the consent form was requested. The research project was submitted to the Research Ethics Committee of the Universidade Estadual de Maringá-UEM and exempted from analysis under the number 038/2012, due to the nature of the research and the design using exclusively secondary and pub-lic access data.
Results
From 2000 to 2015, 1,024,951 hospitalizations of children under five years of age occurred in Paraná. 9.9% (102,016) of them were for ACSC, of which 1.1% (1,160) were of patients under one year of age, 66.1% (67,444) of patients one and two years old and 32.8% (33,412) of pa-tients three and four years old. The five main di-agnoses of hospitalization for ACSC among chil-dren under five in the four trienniums assessed were bacterial pneumonia (38.4%), gastroenteri-tis (35.8%), asthma (8.8%), kidney and uri-nary tract infection (7.4%) and nutritional de-ficiencies (3.8%). Considering the first and last trienniums, the number of hospitalizations for kidney infection increased (8.3%), whereas for
pneumonia, the number decreased (-6.9%). The hospitalization rates for pneumonia presented oscillations, with an increase in the second trien-nium (8.6%) and a subsequent decrease (9.0%), and after 2007 it became the second leading cause of hospitalization in children from Paraná, only behind gastroenteritis. Asthma remained as the third leading cause until 2007, and then it became the fourth after kidney and urinary tract infection. There was a 4.1% reduction in the percentage of hospitalizations due to nutritional deficiencies and a 7.8% increase in the propor-tion of pulmonary diseases (Table 1).
Rates of hospitalizations for all care-sensitive conditions decreased (r2 = 0.39; p=0.016). The anal-ysis by age group showed differentiated patterns, with increase for children under one year old (r2 = 0.38; p=0.017), decrease for children aged one to two years old (r2 = 0.58; p=0.001) and stability for children aged three to four years (r2 = 0.01; p=0.713). The trends of hospitalization for pneumonia, gas-troenteritis and nutritional deficiencies were differ-ent according to the age groups investigated. The rates of hospitalization for pneumonia decreased for children aged one to four years and remained stable for children younger than one year old (r2 = 0.20, p= 0.633). Rates of hospitalization for gastroenteri-tis decreased for children aged one to two years and remained stable in the other age groups. In all age groups asthma presented a decrease and kidney and
Table 1. Hospitalizations of children under five years of age (no. and %) for care-sensitive conditions, according to main diagnosis, per trienniumCare-sensitive conditions groups n(%) n(%) n(%) n(%)
Bacterial pneumonia 10721(37.2) 13726(45.8) 8788(36.8) 5890(30.4)
Gastroenteritis and complications 10595(36.8) 10100(33.7) 8848(37.1) 6989(36.1)
Asthma 3299(11.5) 2803(9.4) 1565(6.6) 1280(6.6)
Kidney and urinary tract infections 1348(4.7) 1642(5.5) 2013(8.4) 2518(13.0)
Nutritional deficiencies 1875(6.5) 980(3.3) 587(2.5) 462(2.4)
Respiratory diseases 198(0.7) 48(0.2) 1132(4.7) 1642(8.5)
Diabetes mellitus 202(0.7) 206(0.7) 313(1.3) 254(1.3)
Skin and subcutaneous tissue infections 268(0.9) 172(0.6) 210(0.9) 117(0.6)
Vaccine-preventable diseases and preventable conditions 52(0.2) 105(0.4) 180(0.8) 19(0.1)
Gastrointestinal ulcer 106(0.4) 58(0.2) 51(0.2) 74(0.4)
Hypertension 16(0.1) 28(0.1) 83(0.4) 52(0.3)
Conditions related to prenatal care and childbirth 74(0.3) 47(0.2) 46(0.2) 9(0.1)
Cerebrovascular conditions 21(0.1) 54(0.2) 36(0.2) 56(0.3)
Cardiad insufficiency 9(0.0) 5(0.0) 15(0.1) 10(0.1)
infections of the ear, nose and throat 2(0.0) 1(0.0) 8(0.0) 8(0.0)
Total 28786(100.0) 29975(100.0) 23875(100.0) 19380(100.0)

258 Acta Paul Enferm. 2017; 30(3):254-61.
Hospitalizations of children for preventable conditions in the state of Parana: causes and trends
under one year old. This was the only age group that presented an increase in hospitalizations for nutritional deficiencies and stability in hospital-izations for pneumonia. Considering the sub-stantial number of health programs and policies for infants, especially those under one year of age, the results showed that the actions did not have an impact on the reduction of ambulatory care-sensitive conditions.Discontinuation of breastfeeding, introduction of the child in group settings, such as schools and day care centers, and their immunological system which is still in development, may be rea-sons that increase the exposure of infants to risk factors for illnesses such as respiratory diseases, infectious diseases and nutritional deficiencies, which are included in the ACSC group. Howev-er, all these aspects can be worked out in primary health care.
The childcare consultation is one of the pos-sible vigilance actions; it is instituted in sever-al health policies and it is critical to the child’s healthy growth and development, especially for children under one year of age. It is a systematic follow-up in which the physician or nurse con-ducts detailed clinical examination, guides the family about the proper care for each age and teaches how to identify signs and symptoms of the most common childhood illnesses. Childcare facilitates the contact of the child’s family with the primary care team and, if done properly, should result in the reduction of hospitalizations for care-sensitive conditions.
The trend analysis revealed a decrease in hospitalizations for all care-sensitive conditions among children under five and children aged one to two years, and stability in hospitalizations among children aged three to four years. This stable trends is considered a negative result of public health policies, since primary health care is regarded as essential to prevent and treat these health problems, especially in the most vulnera-ble populations, such as children under five years of age.(8)
It is important to note that several factors may have influenced this result. Health practices are not
Table 2. Trends in hospitalizations for ambulatory care-sensitive conditions, according to main diagnosis and ageAge Model* r2** p-value Trend
All ambulatory care-sensitive conditions
< 1 year y= 4.85 + 0.24 x 0.38 0.017 Increasing
1-2 years y= 141.17 – 2.65 x 0.58 0.001 Decreasing
3-4 years y= 63.48 – 0.11 x 0.01 0.713 Stable
< 5 years y= 79.10 – 1.09x 0.39 0.016 Decreasing
Bacterial pneumonia
<1 year y= 1.488 + 0.012x 0.20 0.633 Stable
1-2 years y= 54.20 – 2.06x 0.41 0.013 Decreasing
3-4 years y= 22.99 – 0.71x 0.38 0.019 Decreasing
< 5 years y= 31.01 – 1.11x 0.40 0.014 Decresasing
Gastroenteritis
< 1 year y= 0.57+ 0.01 x 0.07 0.334 Stable
1-2 years y= 47.38- 0.84 x 0.45 0.009 Decreasing
3-4 years y= 22.61+ 0.27 x 0.25 0.066 Stable
< 5 years y= 27.97 – 0.02x 0.15 0.160 Stable
Asthma
< 1 year y= 0.193- 0.01 x 0.45 0.007 Decreasing
1-2 years y=10.56 – 0.71x 0.85 <0.001 Decreasing
3-4 years y= 6.34 – 0.39 x 0.75 <0.001 Decreasing
< 5 years y= 6.79 – 0.44 x 0.82 <0.001 Decreasing
Kidney and urinary tract infections
<1 year y=0.63 + 0.08x 0.84 <0.001 Crescente
1-2 years y=8.12 + 0.64x 0.94 <0.001 Crescente
3-4 years y=5.74 + 0.44x 0.92 <0.001 Crescente
< 5 years y=5.66+0.44x 0.95 <0.001 Crescente
Nutritional deficiencies
<1 year y=0.25 + 0.03x 0.84 <0.001 Crescente
1-2 years y=5.46 – 0.56x 0.86 <0.001 Decrescente
3-4 years y=1.63 – 0.13x 0.72 <0.001 Decrescente
< 5 years y=2.86 – 0.27x 0.83 <0.001 Decrescente
*Model y= hospitalization rate (per 10.000); x= estimate year - 2007; **r²= coefficient of determination
urinary tract infection an increase. The percentage variation of kidney and urinary tract infection was higher for children aged three to four years, going from 2.97 in 2000 to 9.18 in 2015, an increase of 208.47%. On the other hand, the rate with the greatest decrease was nutritional deficiencies, which went from 4.18 to 0.75, a reduction of 81.89%. (Table 2).
Discussion
The main causes of hospitalization for ACSC among children under five were pneumonia, gastroenteri-tis, asthma, kidney and urinary tract infection, and nutritional deficiencies.Considering the age group, the results showed that hospitalizations for care-sensitive condi-tions had an increasing trend among children

259Acta Paul Enferm. 2017; 30(3):254-61.
Prezotto KH, Lentsck MH, Aidar T, Fertonani HP, Mathias TA
tation, which contributed to the reduction of cases, as demonstrated by a study carried out in a large urban center in Brazil.(13) A study conducted in the state of Bahia found a reduction in hospitalization for gastroenteritis among children, and the expan-sion of health and basic sanitation services was asso-ciated with the decrease.(14)
Asthma appears as the third leading cause of hospitalizations for care-sensitive conditions among children under five years of age. Several studies show the impact of asthma on children’s health and the importance of nurses providing health education to control the disease.(15,16) A study conducted in China showed an increase in the prevalence of childhood asthma, which indi-cates the need to control the disease and reduce hospitalizations.(17)
A decrease in hospitalizations for asthma was found among all age groups of the study. Asthma is relevant because it is one of the main childhood dis-eases, demanding special attention from the health-care team for its control. A study conducted in the United States demonstrated the importance of the nurses’ work in asthma programs, in which these professionals follow the evolution of the acute con-dition and assist in deciding the most appropriate treatment for each child.(18)
Rates of hospitalizations for nutritional defi-ciencies, as well as asthma, presented a reduction among children aged one to four years. This is a positive aspect identified in the study. Nutritional deficiencies were a cause of infant morbidity and mortality for many years. However, the reorgani-zation of the health system in Brazil, the increased level of education of mothers and socioeconomic improvements are aspects that may have influenced this result.(19) However, despite the good results, children under one year old still remain vulnerable to this condition.
Another factor worth mentioning is the in-crease in hospitalizations for kidney and urinary tract infections, observed in all age groups. A study carried out with the population of Brazil identified an increase in admissions for kidney and urinary tract infection between 1998 and 2009.(20) In the State of São Paulo, kidney and
totally dependent on primary care services. Other factors such as family experiences and habits are determining factors in the process. However, it is essential to stress the importance of the healthcare team’s efforts to maintain relationships with the families they attend and, based on that, provide guidance on the early signs and correct treatment of childhood illnesses.
There was a decrease in hospitalizations for pneumonia among children aged one to four years. Respiratory diseases are some of the main causes of hospitalization of children, which was also identi-fied in this study. A recent study comparing rates of hospitalization for pneumonia among children under 4 years of age before and after the adoption of pneumococcal vaccination in Brazil identified a 12.65% decrease and a decreasing trend, demon-strating the efficacy of the vaccine on Brazilian public health.(9)
The main respiratory diseases that affect chil-dren’s health have known risk factors, such as expo-sure to smoking and household overcrowding.(10,11) In the presence of factors that contribute to the on-set of respiratory diseases, the healthcare team can plan measures for prevention and control of these diseases. These measures must be continuously im-plemented and evaluated, since table 1 showed an increase in the number of hospitalizations for pul-monary diseases, which includes bronchitis, bron-chiectasis and other chronic obstructive pulmonary diseases. However, this increase may also be related to the already mentioned negative aspects of the in-formation system.
Hospitalizations for gastroenteritis remained stable among children under one year of age and for children aged three to four years, and presented a decrease among children aged one to two years. Gastroenteritis is another important ACSC and a cause of morbidity in the world. However, most cases are of mild intensity and would mostly not lead to hospitalization if there was a proper resolu-tion in primary care.(12)
In addition, several actions were implemented to help reduce the incidence of this condition, such as the rotavirus vaccination, implemented in Brazil in the mid-2000s, and the expansion of basic sani-

260 Acta Paul Enferm. 2017; 30(3):254-61.
Hospitalizations of children for preventable conditions in the state of Parana: causes and trends
urinary tract infections were more frequent in children under one year old. These conditions were the third leading cause of hospitalizations in 2006 and 2007 (6.86% and 9.33%, respec-tively) and the second leading cause in 2008 (14.63%) among that age group.(21)
Kidney and urinary tract problems are common in childhood, and the main factors that contribute to their occurrence are hygiene habits and the anat-omy of the genitalia.(22) However, signs that show early manifestation of urinary diseases may be easily identified and managed by the family and health care team through proper inspection and hygiene of the genitals, adequate nutrition and hydration, and in case of illness, hospitalizations can be prevented through proper early treatment in primary care.
Nurses play a key role in the context of hospi-talizations for care-sensitive conditions. The per-formance of these professionals as health care pro-viders is demonstrated in studies that point to the importance of nurses in the management of care. Nurses are responsible for monitoring the child’s health, which allows the detection of the diseases and a proper and early assistance, thus avoiding hospitalization. In addition, as a primary care pro-fessional, the nurse must train team members to identify risk factors and cases of respiratory and infectious diseases.
Regarding the team, the work of the primary care professionals and the bond that they develop with the population have an impact on the reduc-tion of hospitalizations for care-sensitive condi-tions, since they provide health surveillance, early detection of major diseases and treatment and con-trol of their causes.(23)
The assessment of ambulatory care-sensitive hospitalization rates may provide an understanding of the effectiveness and the quality of the care pro-vided in this area. The use of information systems in Brazil, especially the SIH-SUS, has an important impact in the area of epidemiology, since they en-able this monitoring, which represents the work of the health services and morbidity trends. Therefore, the results of the present study demonstrated the real evolution of hospitalizations of children under five years. In addition, the results can guide actions
of the healthcare professionals and public policies for the treatment of children in primary care, main-ly targeting the main illnesses.
The limitations of the surveys that use the SIH-SUS are related to the reliability of the information obtained. The system is filled in a decentralized way, and each hospital unit enters the records of hospital-izations. In addition, the SIH-SUS data determines the funding given to hospitals and, for this reason, mistaken system insertions may occur.
However, the results of epidemiological studies that use the SIH-SUS represents publicly funded hospitalizations, and the large number of regis-tered hospitalizations contributes to minimize the possible errors. In several localities, secondary data sources have been used to study hospitalizations in large populations,(24,25) including children.(2,4)
Conclusion
Trend analysis showed that hospitalizations for pneumonia, asthma, and nutritional deficiencies presented a decrease and hospitalizations for gastro-enteritis remained stable among children under five years of age. There was an increase in hospitalization rates for kidney and urinary tract infection among all age groups assessed.
CollaborationsPrezotto KH, Lentsck MH, Aidar T, Fertonani HP and Mathias TAF declare that they contributed to the conception of the project, the analysis and in-terpretation of data, the writing of the article, the critical review of intellectual content and the final approval of the version to be published.
References
1. Gray BM, Vandergrift JL, Johnston MM, Reschovsky JD, Lynn LA, Holmboe ES et al. Association between imposition of a maintenance of certification requirement and ambulatory care-sensitive hospitalizations and health care costs. JAMA. 2014; 31(22):2348-57.
2. Agha MM, Glazier RH, Guttmann A. Relationship between social inequalities and ambulatory care-sensitive hospitalizations persists for up to 9 years among children born a major Canadian urban center. Ambul Pediatr. 2007; 7(3):258-62.

261Acta Paul Enferm. 2017; 30(3):254-61.
Prezotto KH, Lentsck MH, Aidar T, Fertonani HP, Mathias TA
3. Tom JO, Tseng CW, Davis J, Solomon C, Zhou C, Mangione-Smith R. Missed well-child care visits, low continuity of care, and risk of ambulatory care-sensitive hospitalizations in young children. Arch Pediatr Adolesc Med. 2010; 164(11):1052-8.
4. Oliveira BR, Viera CS, Furtado MC, Mello DF, Lima RA. Perfil de morbidade de crianças hospitalizadas em um hospital público: implicações para a Enfermagem. Rev Bras Enferm. 2012; 65(4):586-93.
5. Pittard WB. Well-child care in infancy and emergency department use by south Carolina Medicaid Children birth to 6 years old. South Med J. 2011; 104(8):604-8.
6. Pedraza DF, Araujo EM. Internações das crianças brasileiras menores de cinco anos: revisão sistemática da literatura. Epidemiol Serv Saúde. 2017; 26(1):169-82.
7. Oliveira RR, Costa JR, Mathias TA. Hospitalizações de menores de cinco anos por causas evitáveis. Rev Lat Am Enfermagem. 2012; 20(1):135-42.
8. Zhao Y, Wright J, Steven Guthridge S, Lawton P. The relationship between number of primary health care visits and hospitalisations: evidence from linked clinic and hospital data for remote Indigenous Australians. BMC Health Serv Res. 2013; 13:466-74.
9. Scotta MC, Veras TN, Kleina PC, Troncoa V, Polack FP, Mattiello R, et al. Impact of 10-valent pneumococcal non-typeable Haemophilus influenzae protein D conjugate vaccine (PHiD-CV) on childhood pneumonia hospitalizations in Brazil two years after introduction. Vaccine. 2014; 32(5):4495-9.
10. Trenholme A, Vogel A, Lennon D, McBride C, Stewart J, Best E, Mason H, Percival T. Household characteristics of children under 2 years admitted with lower respiratory tract infection in Counties Manukau, South Auckland. N Z Med J. 2012; 125(1367):15-23.
11. Jin Y, Seiber EE, Ferketich AK. Secondhand smoke and asthma: what are the effects on healthcare utilization among children? Prevet Med. 2013; 57(2):125-8.
12. Lamberti LM, Fischer W, Christa L, Black RE. Systematic review of diarrhea duration and severity in children and adults in low- and middle-income countries. BMC Public Health. 2012; 12:276.
13. Genser B, Strina A, Santos LA, Teles CA, Prado MS, Cairncross S, Barreto ML. Impact of a city-wide sanitation intervention in a large urban centre on social, environmental and behavioural determinants of childhood diarrhoea: analysis of two cohort studies Int J Epidemiol. 2008; 37(4):831-40.
14. Monahan LJ, Calip GS, Novo PM, Sherstinsky M, Casiano M, Mota E, Dourado I. Impact of the Family Health Program on gastroenteritis in children in Bahia, Northeast Brazil: an analysis of primary care-sensitive conditions. J Epidemiol Glob Health. 2013; 3(3):175-85.
15. Auger KA, Kahn RS, Davis MM, Beck AF, Simmons JM. Medical home quality and readmission risk for children hospitalized with asthma exacerbations. Pediatrics. 2013; 131(1):64-70.
16. Liberatos P, Leone J, Craig AM, Frei EM, Fuentes N, Harris IM. Challenges of asthma management for school nurses in districts with high asthma hospitalization rates. J School Health. 2013; 83(12):867-75.
17. Yangzong Y, Shi Z, Nafstad P, Haheim LL, Luobu O, Bjertness E. The prevalence of childhood asthma in China: a systematic review. BMC Public Health. 2012; 12: 860.
18. Garwick, AW, Seppelt A, Riesgraf M. Addressing asthma management challenges in a multisite, Urban Head Start Program. Public Health Nurs. 2010; 27(4):329-36.
19. Victora CG, Aquino EM, Leal MC, Monteiro CA, Barros FC, Szwarcwald CL. Maternal and child health in Brazil: progress and challenges. Lancet. 2011; 377(9780):1863-76.
20. Boing AF, Vicenzi RB, Magajewski F, Boing AC, Moretti-Pires RO, Peres KG, et al. [Reduction of ambulatory care sensitive conditions in Brazil between 1998 and 2009]. Rev Saúde Pública. 2012; 46(2): 359-66. Portuguese.
21. Rehem TC, Ciosak SI, Egry EY. Internações por condições sensíveis à atenção primária no hospital geral de uma microrregião de saúde do município de São Paulo, Brasil. Texto Contexto Enferm. 2012; 21(3):535-42.
22. Averbuch D, Nir-Paz R, Tenenbaum A, Stepensky P, Brooks R, Koplewitz B et al. Factors associated with bacteremia in young infants with urinary tract infection. Pediatr Infect Dis J. 2014; 33(6):571-5.
23. Macinko J, Oliveira VB, Turci MA, Guanais FC, Bonolo PF, Lima-Costa MF. The influence of primary care and hospital supply on ambulatory care-sensitive hospitalizations among adults in Brazil, 1999-2007. Am J Public Health. 2011; 101(10):1963-70.
24. Craig E, Anderson P, Jackson G, Jackson C. Measuring potentially avoidable and ambulatory care sensitive hospitalisations in New Zealand children using a newly developed tool. N Z Med J. 2012; 125(1366):38-50.
25. Gill PJ, Goldacre MJ, Mant D, Heneghan C, Thomson A, Seagroatt V, Harnden, A. Increase in emergency admissions to hospital for children aged under 15 in England, 1999-2010: national database analysis. Arch Dis Child. 2013; 98(5):328-34.

262 Acta Paul Enferm. 2017; 30(3):262-70.
Original Article
Care protocols with risk classification in pediatrics: inter-observer reliabilityProtocolo de acolhimento com classificação de risco em pediatria: confiabilidade interobservadoresFernanda Jorge Magalhães1,2
Francisca Elisângela Teixeira Lima2
Paulo César Almeida2
Lorena Barbosa Ximenes2
Caroline Magna Pessoa Chaves3
Corresponding authorFernanda Jorge MagalhãesWashington Soares Avenue, 1321,60811-905, Fortaleza, CE, [email protected]
DOIhttp://dx.doi.org/10.1590/1982-0194201700040 1Universidade de Fortaleza, Fortaleza, CE, Brazil.
2Universidade Federal do Ceará, Fortaleza, CE, Brazil.3Universidade Estadual do Ceará, Fortaleza, CE, Brazil.Conflicts of interest: no conflicts of interest to declare.
AbstractObjective: To analyze the inter-observer reliability of the second edition of the Care protocols with risk classification in pediatrics, in the clinical practice of urgent/emergency care.Method: Methodological study, developed through assessment of the inter-observer reliability of two Trained Inter-observers Triage Nurses (TITN) and two Untrained ITNs (UITN) with the researcher, with a total of 400 classifications. Data was analyzed using the Kappa Coefficient, with a 95% Confidence Interval (CI).Results: A total of 80.0% of patients were classified as standard(green-50.7%) and non-urgent (blue-29.3%); substantial and “almost perfect” agreement between the nurses and the researcher (Kappa between 0.62 and 1.0) was found. “Almost perfect” agreement was found between TITN-2 and the researcher (Kappa 1.0), UITN-2 and the researcher (Kappa 0.877) and TITN-1 and the researcher (Kappa 0.725). Substantial agreement was found between UITN-1 and the researcher (Kappa 0.619).Conclusion: Care protocols with risk classification in pediatrics is a reliable technology to guide nurses in the triage of patients in pediatric emergency/urgent care situations.
ResumoObjetivo: Analisar a confiabilidade interobservadores da segunda edição do protocolo de Acolhimento com Classificação de Risco em Pediatria, na prática clínica de urgência/emergência.Métodos: Estudo metodológico, desenvolvido por meio da confiabilidade interobservadores de dois Enfermeiros Classificadores Interobservadores Treinados (ECIT) e de dois ECI Não Treinados (ECINT) com a pesquisadora, totalizando 400 classificações. Dados analisados utilizando-se do Coeficiente Kappa, com Intervalo de Confiança (IC) de 95%.Resultados: Predomínio de 80,0% de pacientes classificados como menor urgência (verde-50,7%) e não urgente (azul-29,3%); revelou-se substancial “quase perfeita” concordância entre os enfermeiros e a pesquisadora (Kappa entre 0,62 e 1,0). Houve “quase perfeita” concordância entre ECIT-2 e pesquisadora (Kappa 1,0), ECINT-2 e pesquisadora (Kappa 0,887) e ECIT-1 e pesquisadora (Kappa 0,725). Houve substancial concordância entre ECINT-1 e pesquisadora (Kappa 0,619).Conclusão: O Protocolo de ACCR em Pediatria é uma tecnologia confiável para direcionar enfermeiros à classificação de risco em situações de urgência/emergência pediátrica.
KeywordsReception; Pediatric; Risk assesment/classification; Validation studies; Child
DescritoresAcolhimento; Pediatria; Avaliação de risco/classificação; Estudos de validação; Criança
Submitted March 7 2017
Accepted June 5 2017

263Acta Paul Enferm. 2017; 30(3):262-70.
Magalhães FJ, Lima FE, Almeida PC, Ximenes LB, Chaves CM
Introduction
Clinical judgment and decision-making are con-sidered broad and significant challenges involved in the different situations in the healthcare prac-tice. Among these, urgent/emergency situations stand out. In these situations, it is necessary to prioritize the information received and facilitating conditions in order to determine the severity of the conditions and the risk of death of patients visiting healthcare institutions.
In these situations, the healthcare profession-als working in urgent/emergency units, especially the nurses, need knowledge, ability and attitude to properly care, listen and guide the healthcare users in these units(1) and to triage patients arriving at the hospital.
Experts in the field(2) clarify that the term risk classification indicates the act of identifying the main issue manifested or reported by patients and/or their companions, in order to establish a waiting list based not on order of arrival, but on clinical risk. Therefore, the triage process consists in con-ducting the collection of anamnesis and the physi-cal examination of the signs and symptoms, aiming at determining the priority of care related to the conditions expressed, the possible complications and the risk of death.
To perform the risk classification, health insti-tutions suggest and use health technologies, such as admission protocols to guide the Care with Risk Classification.
A review carried out to identify the health technology instruments used in the triage/risk classification of children or adolescents indicat-ed nine instruments for this purpose: Pediatric Assessment Triangle, Canadian Pediatric Triage and Acuity Scale and its computerized version - Staturg, Emergency Triage Assessment and Treat-ment, Emergency severity index for pediatric triage, Pediatric Taiwan Triage System, Pediatric Triage and Acuity System, Manchester Triage System for pediatric emergency care and Pediat-ric Triage Tape.(3)
In addition to the findings of this review, the Care protocols with risk classification in pediat-
rics stands out as another triage instrument. This protocol assists in the characterization, evalua-tion and classification of the risk presented by the child and/or adolescent, to determine the priority of treatment in the emergency/urgent care service. This instrument, developed by the Health Department of Fortaleza-Ceará-Brazil, uses five colors to classify the risk and deter-mine the expected waiting time for medical care: red (priority I), immediate medical attention; orange (medical care in up to 15 minutes; can be reassessed by the nurse every 15 minutes); yellow (medical care in up to 30 minutes; can be reassessed by the nurse every 30 minutes); green (medical care in up to 60 minutes, can be reassessed by the nurse every 60 minutes); and blue (patient will receive medical care in order of arrival or will be directed to the primary care unit). This instrument was evaluated by experts specialized in pediatrics and triage, and its con-tent and its appearance were considered valid.(4)
Based on the study mentioned, the need to assess the inter-observer reliability and the va-lidity of the protocol in the clinical practice was evidenced. An instrument is considered reliable when it is able to accurately measure a phenome-non and to produce results that are consistent in time, space and with different observers, if prop-erly used.(5)
This study is justified and relevant since it pre-sented the evaluation of the reliability of this instru-ment in the clinical practice, assessing its adequacy for the decision-making process and for adequate and safe determination of the priority of care of children and/or adolescents in emergency/urgent care services. The study also made it possible to use the instrument to provide a quality care and im-prove the risk classification process in the admission of the targeted population in a timely and effective manner, in order to prevent and minimize compli-cations and risk of death at the emergency/urgent health service.
Therefore, the objective of this study was to as-sess the inter-observer reliability of the second edi-tion of the Pediatric Risk Classification in clinical practice for emergency/urgent care.

264 Acta Paul Enferm. 2017; 30(3):262-70.
Care protocols with risk classification in pediatrics: inter-observer reliability
Methods
Methodological study, with a quantitative approach, aimed at evaluating the Care protocols with risk classification in pediatrics as a reliable instrument that can be used by health professionals in pediatric emergency/urgent care units.
The study was conducted in the emergency unit of a municipal hospital reference in pediat-ric care in the city of Fortaleza-CE-Brazil, where there are children and adolescents in high risk for complications.
For the selection of the children and/or adoles-cents, the inclusion criteria were: being from zero to 16 years old, seeking care in the emergency/urgent care unit of the institution assessed and being with a companion. The exclusion criterion was: people who were seeking elective care with a physician or nurse (pediatrics).
For sample size calculation, the recommen-dations of the Kendall’s coefficient of concor-dance, used in attribute agreement analysis, were followed. This coefficient also indicated the de-gree of correlation of ordinal rankings carried out by different evaluators when analyzing the same samples.
The Kendall’s coefficient determined a num-ber of at least 96 children and/or adolescents as sample size for each inter-observer nurse. How-ever, a total sample of 100 children and/or ad-olescents for each Trained Inter-observer Triage Nurse (TITN-1 and 2) and Untrained Inter-ob-server Triage Nurse (UITN-1 and 2), that means, each nurse, along with the researcher, evaluated and classified 100 children and/or adolescents in-dependently. Therefore, the final sample consist-ed of 400 children and/or adolescents in the risk classification in pediatrics.
Data collection was conducted with the in-ter-observer nurses and the researcher. The reli-ability and degree of correlation of the risk classi-fication were determined by TITN-1 and TITN-2 and the researcher, and UITN-1 and UITN-2 and the researcher.
The inclusion criteria for the UITN were: not having participated in the training course on the
Pediatric Risk Classification Protocol, having at least two years of experience and to be working in the institution’s risk classification during the period of data collection. The exclusion criteria were: being on vacation, maternity leave or sick leave during the period of data collection. Af-ter the selection, four untrained nurses willing to contribute were selected; however, during the collection, there was one withdrawal and one sick leave. Thus, only two UITN were assessed, and it was agreed with each of them that the researcher would collect the data according to the schedule pre-established by the Institution’s nursing coordination.
For the TITNs, inclusion criteria were: partic-ipating and having more than 80% frequency in the 40-hour training course on the Pediatric Risk Classification Protocol and in the discussion group about improving the applicability of the protocol. The exclusion criteria were: being on vacation, ma-ternity leave or sick leave in the period of data col-lection and being a temporary professional in the period of data collection.
The data collection began with the UITN-1 evaluating the children and/or adolescents and determining the priority of care of each one. The researcher observed, captured the information de-scribed by the nurse and followed the priority of care recommended by the second edition of the Pediatric Risk Classification Protocol according to the clinical situation of each patient. This process was repeated with the 100 children evaluated by the researcher and by each of the evaluator nurses, following the se-quence: UITN-1, UITN-2, TITN-1 and TITN-2.
A total of 400 classifications were attained for the assessment of the inter-observer reliability. The data collection lasted about eight months and the approximate time took by the triage nurse with each patient was five minutes, varying depending on the complexity and severity of the main complaint re-ported by the child, adolescent or companion. The data was collected in day and night shifts, according to the schedule and availability of the triage nurs-es. The period of data collection was extended due to the seasonality of common diseases in pediatric emergency/urgent care units.

265Acta Paul Enferm. 2017; 30(3):262-70.
Magalhães FJ, Lima FE, Almeida PC, Ximenes LB, Chaves CM
The data collection instruments were: 1) Characterization of the triage nurses on age, lev-el of education, time of experience in pediatrics, mean time of experience in triage, participation in the Training Course on the Pediatric Risk Classification Protocol, use of the Pediatric Risk Classification Protocol and difficulty in using the Pediatric Risk Classification Protocol; 2) Triage instrument containing data regarding identifica-tion and classification of the children and/or ad-olescents, such as age (in months), gender, level of education, vital signs, anthropometric data, main complaint, time spent in the evaluation, waiting time for medical care, clinical discrim-inators (main clinical conditions related to the main complaint), pain scale and determination of risk classification based on the five colors of the protocol.
In addition, the researcher obtained individ-ualized data by approaching the guardians of the children and/or adolescents who sought care. The objectives of the study were presented and the sign-ing of the consent form was requested for these par-ticipants, respecting ethical and legal aspects.
To analyze the reliability of the second edition of the Pediatric Risk Classification Protocol, the kappa coefficient was used. This coefficient mea-sures the level of agreement, the consistency of the evaluations or the relative position of the evalua-tions of the data by the evaluators/judges. This in-dex assesses the capacity that an instrument has to reach the same results when applied by two or more observers, giving the magnitude of the inter-observ-er reliability as result.
According to scholars, there are six classifica-tions for the interpretation of the Kappa test, with the following agreement values: No agreement (0); Slight agreement (> 0 to 0.19); Fair agreement(0.20 to 0.39); Moderate agreement (0.40 to 0.59); Sub-stantial agreement (0.60 to 0.79); and “Almost per-fect” agreement or Excellent (0.80 to 1).
Kappa values greater than 0.60 - substantial agreement - are recommended to obtain reliable re-sults. If the values are lower than 0.60, the level of agreement between the judges or the adequacy of the instrument should be questioned.
The study complied with the principles of Res-olution 466/12 of the National Health Council/Ministry of Health, and was approved for develop-ment under the number 1.282.924 and CAAE nº 49076915.7.0000.5054.
Results
Regarding the characterization of the participants, four were nurses, three were female and one male. The mean age of the nurses was 26 years and five months. All of them had graduate certification de-gree and two participated in research groups and had scientific publications related to the subject Child Health. All had professional experience in this area and also in emergency/urgent care, with a mean experience of four years.
The comparison between the groups showed that the TITNs had less time of clinical experience in pediatrics (at least one year of professional ex-perience), whereas the UITNs had a mean of five years of experience. Participating nurses reported that they rarely used the Protocol studied and that they had no difficulty using the second edition of the Pediatric Risk Classification Protocol, classify-ing it as excellent.
Among the children and/or adolescents evaluat-ed, 51.2% (205) were male; the mean age was 50.2 months (approximately four years) with a median of 26.5 months (two years) and standard deviation of 40.3 months (three years).
Regarding the risk classification determined by the inter-observer nurses and by the researcher, equivalence between these was evidenced by the agreement between the priorities of care established by the nurses in the pediatric emergency/urgent care practice, as shown in table 1.
The data in table 1 shows a 50.7% (203) pre-dominance of patients classified as green - priority IV (standard) and a 29.3 % (117) predominance of blue - priority V (non-urgent) given by the TITNs, totaling a sample of 80%. These results were similar to the classification given by the re-searcher, who classified 77.7% of the children as green and blue.

266 Acta Paul Enferm. 2017; 30(3):262-70.
Care protocols with risk classification in pediatrics: inter-observer reliability
Considering the comparison of the classifica-tion given by the TITNs and the UITNs with the researcher classification, the importance of evaluat-ing the degree of correlation of the Pediatric Risk Classification Protocol regarding its legitimacy in contrasting groups in the Pediatric emergency/ur-gent care practice is evident.
It should be noted that there were no children or adolescents in this study who were considered immediate, that is, none of the participating nurses nor the researcher attributed the red classification (priority I), which means the patient is at immedi-ate risk of complications or death.
Regarding the orange risk classification (priori-ty II), none of the patients evaluated by the UITN group and only one patient evaluated by the TITN group was classified as requiring medical attention within 15 minutes. The researcher, however, iden-tified 4.5% (9) of the children and/or adolescents who sought very urgent care as orange priority.
Regarding the other classification colors, most of, many of the patients (41%) were classified as green (priority IV) and 39% were classified as blue (priority V) by the TITNs. The same was predom-inant in the UITN group, which attributed green priority to 49.5% and blue priority to 29.5% of the evaluated patients. For the researcher, there were 93% standard care patients (green) and 61% (122) non-urgent patients (blue).
The data determine the patient profile in the institution studied, which were mostly classified with standard care (green) and non-urgent (blue). Regarding the comparison between the risk classifi-cation attributed by the group of trained inter-ob-server nurses (T1 and T2) and by the researcher in the inter-observer reliability phase, the data found is described in table 2.
An “almost-perfect” agreement was found be-tween UITN-2 and the researcher (Kappa = 1; p < 0.0001). Between UITN-1 and the researcher, sub-stantial agreement was obtained (Kappa = 0.726; p = 0.060). Table 3 displays the data regarding the agreement of the risk classifications attributed by the group of non-trained inter-observer nurses (U1 and U2) and by the researcher in the inter-observer reliability phase.
Table 3 shows results that demonstrate a substan-tial agreement (Kappa = 0.619; p = 0.067) between the UITN-1 and the researcher. The UITN-2 had an “almost perfect” agreement with the researcher (Kappa = 0.887; p = 0.410). However, this index was not sta-tistically significant when compared to trained nurses.
It is possible to perceive that the data present-ed higher percentages in the diagonals of table 3. Considering that the agreement between the ob-servers, higher agreement was found for standard classification (green), with very few differences in agreement for non-urgent classifications (blue). In other words, it was verified that there was no sig-nificant difference between the means of the total scores given by the trained nurses and the untrained nurses and the scores given by the researcher. There-fore, “almost perfect” agreement was found with the TITNs (Kappa = 0.863 e p = 0.030), whereas substantial agreement was found with the UITNs (Kappa = 0.753 and p = 0.355).
The results can indicate that the protocol is re-liable, simple and self-explanatory to determine the risk classification of children and/or adolescents in emergency/urgent care situation. This means that the protocol, whether used by a trained or un-trained nurse, is reliable in producing the same re-sults on repeated evaluations, being a consistent and predictable tool for determining priority of care.
However, it is important to note that differenc-es of agreement were found between the inter-ob-server nurses and the researcher, but this was not statistically significant. However, this finding in the risk classification may demonstrate a need for greater sensitivity for the clinical complaint in order to determine the discriminators and the respective clinical indicators in the situation of the child and/or adolescent.
Table 1. Distribution of the children according to the risk classification assessed through the Pediatric Risk Classification Protocol, conducted by Inter-observer Triage Nurses and by the researcher
Triage classificationInter-observer triage nurse Researcher
n(%) n(%)
Orange - Priority II 1(0.3) 9(2.3)
Yellow - Priority III 79(19.8) 80(20.0)
Green - Priority IV 203(50.7) 205(51.2)
Blue - Priority V 117(29.3) 106(26.5)
Total 400(100.0) 400(100.0)

267Acta Paul Enferm. 2017; 30(3):262-70.
Magalhães FJ, Lima FE, Almeida PC, Ximenes LB, Chaves CM
In this aspect, data showed that some patients were classified by the researcher with a higher prior-ity of care, while the nurses indicated a lower level of care priority compared to the protocol. This may be due to the direction of the main clinical complaint and can indicate a situation of underestimation of the priority of care. This demonstrates the impor-tance of using the protocol as a health technolo-gy for determining the priority of care in a reliable and safe manner for children and/or adolescents in emergency/urgent care situation.
Discussion
For the legal practice of the profession, the nurse who performs the triage must have in-depth knowl-edge about what is an urgent/emergency care situa-tion and an elective situation, in order to assess the clinical signs with skill and direction and make the decision about which service should be indicated to provide adequate care, thus reducing the subjectivi-ty bias on the emergency/urgent service.
Age was identified as an important socio-de-mographic characteristic, since the prevalence of infants and preschool children was verified. This data can be compared to a pediatric emergency study in a teaching hospital in Mato Grosso do Sul, Brazil, in which out of the 1236 patients attended, 988 (79.9%) were infants and preschool children. Therefore, it is known that this age group may be more predisposed to diseases and can require more attention from the health team.(6)
However, another study assessed 2,153 med-ical records of children and adolescents attending an emergency unit in Alagoas and found patients between 10 and 18 years as the most representative age group, with 931 (43.2%) patients.(7)
The most urgent situations (red or orange) pres-ent in pediatric urgent/emergency units include cardiorespiratory arrest, severe sepsis, convulsions, among others, which require immediate attention, indicated with the activation of a sound alarm. The results are in agreement with other studies, which also indicated that these occurrences were not very frequent in the pediatric services.(6,8)
Table 2. Risk classification attributed by the TITN and by the researcher in the inter-observer reliability phase
Classification by the researcher
Classification by the TITN
Total Kappa p-valueOrange Yellow Green Blue
T1 T2 T1 T2 T1 T2 T1 T2Orange T1 1 - 1 - 1 - 0 - 3
T2 - 0 - 0 - 0 - 0 0 T1 0.726 T1 0.060Yellow T1 0 - 12 - 6 - 2 - 20
T2 - 0 - 22 - 0 - 0 22 T2 1.000 T2 0.0001Green T1 0 - 3 - 45 - 3 - 51
T2 - - - 0 - 34 - 0 34Blue T1 0 - 0 - 1 - 25 - 26
T2 - - - 0 - 0 - 44 44Total T1 1 - 16 - 53 - 30 - 100
T2 - - - 22 - 34 - 44 100
Table 3. Risk classification attributed by the UITN and the researcher in the inter-observer reliability phase
Classification by the Researcher
Classification by the UITN
Total Kappa p-valueYellow Green Blue
U1 U2 U1 U2 U1 U2
Orange NT1 1 - 1 - 0 - 2
NT2 - 1 - 1 - 0 2 NT1 0.619 NT1 0.067
Yellow NT1 15 - 4 - 3 - 22 NT2 0.887 NT2 0.410
NT2 - 18 - 1 - 0 19
Green NT1 5 - 40 - 7 - 52
NT2 - 2 - 48 - 1 51
Blue NT1 0 - 3 - 21 - 24
NT2 - 0 - 1 - 27 28
Total NT1 21 - 48 - 31 - 100
NT2 - 21 - 51 - 28 100

268 Acta Paul Enferm. 2017; 30(3):262-70.
Care protocols with risk classification in pediatrics: inter-observer reliability
The present study identified that more than half of the children and adolescents analyzed were classified as standard (green), indicating that many of the hospital emergency units remain as a gateway for the Unified Health System. This re-sult also shows that parents or guardians of chil-dren and/or adolescents often go to these units instead of going to primary health care units.(6)
The additional number of patients in emergencies also occurs because users consider these sectors as more accessible, since they offer greater resources, such as consultations, laboratory exams, medica-tions, image exams, among others. The search for these services in an erroneous way compromises the functioning of the emergency units and this is mainly due to lack of orientation of the pop-ulation and insufficient structuring in the basic health care networks.(9)
Regarding the inter-observer reliability, the results agree with international studies that dis-cuss the degree of agreement between nurses us-ing Triage Protocols to determine the priority of care in emergency/urgent situations. These stud-ies also include the validity and the reliability of the protocols in Pediatrics, and present instru-ments that contain reliable information to de-fine care protocols that improve and broaden the practice of nurses.(10-14)
The data are similar to another study(15) which found “almost perfect” agreement (Kappa = 0.884) between the complaint given at admission and the discharge medical diagnosis, indicating that the Canadian scale evaluated in this study represented a new instrument to be used in emer-gency services.
Another study(16) also obtained similar re-sults, finding substantial or “almost perfect” degrees of agreement between the four observer nurses, with Kappa values ranging from 0.68 to 0.90. This demonstrated that the classification instrument presents reliability to be used in the nurse’s managerial practice as a diagnostic tool to determine the category of care to which the patient belongs.
However, it is important to emphasize the importance of continued formal education for
professionals and undergraduate students, aim-ing to learn and practice the use of this technol-ogy in order to improve performance and reli-ability in the pediatric triage, a need that has also been highlighted by national and international authors.(15-17)
This also shows the importance of the triage for the care implementation, since it provides greater accessibility to emergency services, priori-tizes the most serious cases, and is operative when the situation demands. It promotes a lower injury to users’ health, since it facilitates the classifica-tion and orientation of the flow of patients, pri-oritizing the most serious patients in relation to the least severe ones. Therefore, the triage proto-cols promote a better organization of emergency services, which have as main objective guarantee-ing the Unified Health System (SUS) principles: universality, resoluteness and humanization of the care provided.(8,18,19)
As limitation of the study, the nurses demon-strated difficulty in valuing and adhering to the training course on the use of the Pediatric Risk Classification Protocol as a health technology. Regarding the clinical profile of the children and adolescents attended at the studied institution, there was no case of an emergency with red clas-sification, needing immediate medical care and requiring the activation of the alarm, on days and times of data collection. The difficulty of involv-ing health managers in the implementation of the Pediatric Risk Classification Protocol in the pe-diatric emergency was also a limitation, since a reduction of human resources was often found, with only one nurse on the 12-hour scale and lack of adequate material to carry out the physical ex-amination of children and/or adolescents in emer-gency situation.
The present research brought as contribution to the clinical practice the Pediatric Risk Classi-fication Protocol as a reliable health technology, since its use can configure an appropriate and safe strategy, providing the triage nurse with ad-equate direction to determine the priority of care of children and adolescents in pediatric emer-gency situations.

269Acta Paul Enferm. 2017; 30(3):262-70.
Magalhães FJ, Lima FE, Almeida PC, Ximenes LB, Chaves CM
Conclusion
The Pediatric Risk Classification Protocol for care, developed in Fortaleza-Ceará-Brazil, was identified as reliable to classify the priority of care of children and adolescents in an emergency/ur-gent situation, based on the degree of suffering and risk of complications and death. The use of this instrument in the waiting lines in pediatric emergencies contributed for quick and effective decision making in the care of these health users. Regarding the inter-observer reliability of the Pe-diatric Risk Classification Protocol, equivalence was evidenced through the degree of agreement of trained nurses and the researcher, as well as untrained nurses and the researcher, during the evaluation of children and/or adolescents in situ-ation of emergency.
Therefore, the protocol studied was established as reliable tool for the triage of children and adoles-cents. It can be used by any nurse, whether trained on not on its use, to determine the priority of care. Therefore, it is possible to infer that the Protocol is a reliable technology to determine the priority of care of children and/or adolescents in an emergency situation, regardless of training.
AcknowledgmentsTo the funding granted by the National Council for Scientific and Technological Development (CNPq) and the Coordination for the Improvement of Higher Education Personnel (CAPES).
CollaborationsMagalhães FJ, Lima FET, Almeida PC, Ximenes LB and Chaves CMP declare that they contributed with the conception of the project, analysis and in-terpretation of the data, writing of the article, criti-cal review of intellectual content and final approval of the version to be published.
References
1. Weykamp JM, Pickersgill CS, Cecagno D, Vieira FP, Siqueira HC. Welcom in gwith risk classification in urgent and emergency services: applicability in nursing. Rev Rene. 2015; 16(3):327-36.
2. Magalhães-Barbosa MC, Prata-Barbosa A, Cunha AJ, Lopes CS. CLARIPED: a new tool for risk classification in pediatric emergencies. Rev Paul Pediatr (English Edition). 2016; 34(3):254-62.
3. Felipe GF, Silva VM, Cardoso MV, Lima FE, Magalhães FJ. Produção científica sobre triagem e acolhimento com classificação de risco em pediatria. In: Seminário Nacional de Pesquisa em Enfermagem, 18o., 2015, Fortaleza. Anais. Fortaleza: ABEn; 2015.
4. Magalhães FJ. Validação do protocolo de acolhimento com classificação de risco em pediatria [dissertação]. Fortaleza (CE): Universidade Federal do Ceará, Faculdade de Farmácia, Odontologia e Enfermagem; 2012.
5. Silveira MF, Almeida JC, Freire RS, Haikal DA, Martins AE. Propriedades psicrométricas do instrumento de avaliação da qualidade de vida: 12-item health survey (SF-12). Ciênc Saúde Coletiva. 2013; 18(7):1923-31.
6. Salgado RM, Aguero FC. Perfil dos pacientes pediátricos atendidos na emergência de um hospital universitário. Pediatria (São Paulo). 2010; 32(2):90-7.
7. Simons DA, Monlleó IL, Simons AS, Araújo Junior JL. Adequação da demanda de crianças e adolescentes atendidos na unidade de emergência em Maceió, Alagoas, Brasil. Rev Bras Saúde Mater Infant. 2010; 10(1):59-67.
8. Veras JE, Rodrigues AP, Silva MJ, Aquino PS, Ximenes LB. Competências de enfermeiras para a promoção da saúde durante atendimentos pediátricos em unidade de emergência. Acta Paul Enferm. 2015; 28(5):467-74.
9. Oliveira DA, Guimarães JP. A importância do acolhimento com classificação de risco nos serviços de emergência. Cad Saúde Desenvol. 2013; 2(2):25-44.
10. Jafari-Rouh AH, Sardashti S, Taghizadieh A, Soleimanpour H, Barzegar M. The Emergency Severity Index, version 4, for pediatric triage: a reliability study in Tabriz Children’s Hospital, Tabriz, Iran. Int J Emerg Med. 2013; 6(36):1-5.
11. Zachariasse JM, Seiger N, Rood PP, Alves CF, Freitas P, Smit FJ, Roukema GR, Moll HA. Validity of the Manchester Triage System in emergency care: A prospective observational study. PlosOne. 2017; 2:1-14.
12. Azeredo TR, Guedes HM, Almeida RA, Chianca TC, Martins JC. Efficacy of the Manchester Triage System: a systematic review. Int Emerg Nurs. 2015; 23(2):47-52.
13. Parenti N, Reggiani ML, Iannone P, Percudani D, Dowding D. A systematic review on the validity and reliability of na emergency department triage scale, the Manchester Triage System. Int J Nurs Studies. 2014; 51(7):1062-9.
14. Santos MA. Acolhimento com classificação de risco: um fio guia da administração em emergência. Rev Saúde Desenvol. 2014; 6(3):56-69.
15. Pires PS. Tradução para o português e validação de instrumento para triagem de pacientes em serviço de emergência: “Canadian Triage and Acuity Scale” (CTAS) [tese]. São Paulo: Universidade de São Paulo, Escola de Enfermagem da USP; 2003.
16. Perroca MG, Gaidzinski RR. Avaliando a confiabilidade intervaliadores de um instrumento para classificação de pacientes - coeficiente Kappa. Rev Esc Enferm USP. 2003; 37(1): 72-80.
17. Sieger N, Van Veen M, Almeida H, Steyerberg EW, Van Meurs AH, Carneiro R, et al. Improving the Manchester Triage System for Pediatric Emergency Care: An International Multicenter Study. PlosOne. 2014; 9(1):83267.

270 Acta Paul Enferm. 2017; 30(3):262-70.
Care protocols with risk classification in pediatrics: inter-observer reliability
18. Inoue KC, Bellucci JJ, Papa MA, Vidor RC, Matsuda LM. Evaluation of quality of Risk Classification in Emergency Services. Acta Paul Enferm. 2015; 28(5):420-5.
19. Souza CC, Araújo FA, Chianca TC. Produção científica sobre a validade e confiabilidade do Protocolo de Manchester: revisão integrativa da literatura. Rev Esc Enferm USP. 2015; 49(1):144-51.

271Acta Paul Enferm. 2017; 30(3):271-9.
Original Article
Questionnaire for assessment of HIV/AIDS control actions in the primary care
Questionário para avaliação das ações de controle do HIV/Aids na Atenção Básica
Richardson Augusto Rosendo da Silva1
Révia Ribeiro Castro2
Illiana Rose Benvinda de Oliveira Pereira1
Sylvia Silva de Oliveira1
Corresponding authorRévia Ribeiro CastroAlberto Maranhão Avenue, 2244, 59600-195, Mossoró, RN, [email protected]
DOIhttp://dx.doi.org/10.1590/1982-0194201700041
1Universidade Federal do Rio Grande do Norte, Natal, RN, Brazil.2Universidade Estadual do Rio Grande do Norte, Mossoró, RN, Brazil.Conflicts of interest: there are no conflicts of interest to declare.
AbstractObjective: To validate the content of a questionnaire to assess the care provided by healthcare professionals to control the HIV/AIDS epidemic in primary care.Methods: A methodological study was conducted, based on the development of a questionnaire using an integrative review, and subsequent validation by experts, using a two-round Delphi technique. Data were analyzed by considering the level of consensus responses, associated with the Kappa index. The criteria for retaining the questions were: ≤ 75% agreement, and Kappa ≤ 0.41.Results: The first round eliminated 16 questions, five questions were revised according to vocabulary changes requested by experts, and criteria for topic coverage and clarity. In the second round, 31 questions were considered appropriate.Conclusion: This questionnaire, unpublished nationally or internationally, achieved acceptable content validity after a careful review of its questions.
ResumoObjetivo: Validar o conteúdo de um questionário para a avaliação da atenção ofertada pelos profissionais de saúde para o controle da epidemia do HIV/Aids na atenção básica.Métodos: Estudo metodológico realizado a partir da construção de questionário por meio de uma revisão integrativa, com posterior validação por juízes, utilizando-se a técnica Delphi em duas rodadas. Os dados foram analisados tomando o nível de consenso das respostas, associado ao índice Kappa. Os critérios para a permanência das questões foram: porcentagem de concordância ≤ 75% e Kappa ≤ 0,41.Resultados: Na primeira rodada, 16 questões foram eliminadas, 05 questões sofreram mudanças para atender à solicitação dos especialistas quanto aos critérios de vocabulário, abrangência ao tema e clareza e Na segunda rodada, as 31 questões foram consideradas adequadas.Conclusão: O questionário, inédito tanto no âmbito nacional quanto no internacional, encontra-se validado em relação ao seu conteúdo, após cuidadosa revisão de suas questões.
KeywordsAcquired immunodeficiency syndrome;
HIV; Primary health care; Validation studies
DescritoresSíndrome da imunodeficiência
adquirida; HIV; Atenção primária à saúde; Estudos de validação
Submitted March 9, 2017
Accepted May 29, 2017

272 Acta Paul Enferm. 2017; 30(3):271-9.
Questionnaire for assessment of HIV/AIDS control actions in the primary care
Introduction
Acquired Immune Deficiency Syndrome (AIDS) corresponds to the most advanced stage of the human immunodeficiency virus (HIV) infec-tion.(1) A global challenge presented with its dis-covery, related to epidemiological, socio-cultur-al, economic and clinical aspects, characterizing the need to implement policies to address social and structural barriers to diagnosis and care, as well as discrimination and stigma associated with HIV.(2)
Around 1.6 million people live with HIV in Latin America, and data accumulated from 2007 to 2016, demonstrate 136,946 cases of infection in Brazil.(3,4) The AIDS epidemic showed in-creased bias in the number of cases in the poorest population strata, and a general reduction in the male/female ratio in the Brazilian population. Given such a context, combating HIV/AIDS re-quires commitment and effort on the part of the entire society, as it involves not only behavioral aspects, but issues that contribute to increased vulnerability.(5)
Public policies have been implemented to fight and control HIV/AIDS that culminated in health care focused on: improving the quality of life of people living with HIV,(1) highlighting the availability of antiretroviral treatment in the Unified Health System (UHS-SUS) network, the creation of a Specialized Assistance Service (SAS) for people with HIV/AIDS, biosecurity actions of health workers in order to minimize the risk of HIV infection due to occupational accidents, as well as expanding the availability of diagnostic tests and prevention.(6)
In view of this epidemic, the 90-90-90 targets were established, which refer to: 90% of people living with HIV/AIDS (HIV-positive people) must be diagnosed, 90% of HIV-positive peo-ple should be receiving treatment with antiret-roviral therapy, and 90% of HIV-positive people should be receiving viral suppression treatment.(7) In order to meet these goals, it is necessary to rethink the construction and operationalization of responses in the health care network, with em-
phasis on primary care, which presents itself as a privileged locus of control to act in the fight against HIV/AIDS, because is one of the main gateways to the system’s health care network, as well as being committed to allocating actions for HIV/AIDS control, such as: health education, HIV prevention, early diagnosis, and access to appropriate treatment.(8)
The relevance of the study is related to the need to measure the attention offered to the control of HIV/AIDS by health professionals in primary care, in order to develop a situational diagnosis that supports the development of knowledge and practices aimed at prevention and management of the disease.
In this sense, a validated questionnaire will promote the development of theoretical and op-erational knowledge aimed at understanding and evaluating the performance of HIV/AIDS preven-tion and control actions, in the context of prima-ry health care, especially in view of the different organizational models adopted in Brazil. In har-mony with the diversity of the local and regional contexts, configuring pluralistic care (within tra-ditional Basic Health Units, Community Health Agent Program, and the Family Health Strategy). Thus, the availability of tools allowing evaluation of the performance of these services is fundamen-tal for qualification of health practices, especially in the control of HIV/AIDS. In addition, it is pos-sible to collaborate on public policies at this level of health care, helping to plan interventions aimed at the 90-90-90 targets of the Brazilian Ministry of Health.
The objective was to complete the content val-idation of a questionnaire to evaluate HIV/AIDS control in the primary health care network, based on the care provided by health professionals.
Methods
This was methodological research with a quantita-tive approach, for face and sampling validation of questionnaire content,(9,10) performed by a group of experts using the Delphi technique.(11) The study

273Acta Paul Enferm. 2017; 30(3):271-9.
Silva RA, Castro RR, Pereira IR, Oliveira SS
was developed in two sequential phases. In the first, an integrative review was completed to con-struct the instrument; in the second, the content validation was completed.
Development of the instrumentThe questionnaire was developed after an inte-grative review of the literature was completed on HIV/AIDS control in periodicals that were: published in the last ten years, available in the Virtual Health Library (VHL- BVS), Latin American and Caribbean Literature (LILACS), International Literature in Health and Biomed-ical Sciences (MEDLINE), SCOPUS, and Cu-mulative Index to Nursing and Allied Health Literature (CINAHL). The following Health Sciences Descriptors (HSD-DeCS) were used: primary health care; acquired immunodeficiency syndrome and HIV. In a complementary way, ma-terials available from the Ministry of Health that were associated with the researchers’ experiences were used.
The questionnaire was composed of two sec-tions: socio-demographic and economic char-acteristics of the participants (containing seven questions regarding: sex, age, family income, reli-gion, marital status, profession and time working in the primary health network); characteristics of the care provided (containing 47 questions relat-ed to the assessment of HIV/AIDS control, based on the following pillars: knowledge of profession-als about control of the epidemic at the primary health care level, health education, diagnosis, con-tinuity of care, availability of material resources and physical space in the health unit, and access to healthcare services and supplies for prevention of HIV infection).
Content validation of the instrumentPreceding the content validation, a peer review was developed with a committee of experts, select-ed by convenience, composed of three academic professors with experience in public policies to cope with HIV/AIDS, who performed an evalua-tion on the conceptual and semantic equivalence of the questionnaire.
In order to verify the content validity, the questionnaire was submitted to expert evalua-tion by professionals considered qualified to as-sess clarity, content, disposition and comprehen-sion of a questionnaire,(12) to analyze the repre-sentativeness of the questions, and to constitute a representative sample of what it is proposed to measure.(13)
Because no consensus was found in the litera-ture to define the number of subjects that should participate in content validation, the establishment of the sample was at the criterion and accessibility of the researcher. However, in order to minimize bias, the delimitation of the inclusion criteria of the par-ticipants must be in consonance with the object of the study.(14)
The specialists were selected through the review of their curriculum vitaes, based on the following inclusion criteria: undergraduate professors and/or healthcare professionals working in primary care; graduation lato sensu or stricto sensu in the area of public health, community health, health sciences and/or health management, research re-lated to HIV/AIDS control in the last five years; professional experience equal to or greater than two years; the exclusion criterion was the return of incomplete instruments by a primary health care professional or professor.
The sample consisted of 20 participants: ten health professionals and ten undergraduate profes-sors that met the criteria for inclusion. The study was conducted by electronic mail in the period from February of 2014 to April of 2014. The initial contact was made by means of an invitation letter, specifying the assessment criteria and the request for consideration and, after acceptance, the instru-ment and the Terms of Free and Informed Consent (TFIC), was sent to the participants.
The data collected from the specialists in the sample validation were obtained by means of a two-point scale for individual evaluation of the ques-tions, regarding agreement (A) and disagreement (D) with the retention of the question in the ques-tionnaire. In the face validation, the experts provid-ed their judgments, which were captured in spaces destined for comments/suggestions.

274 Acta Paul Enferm. 2017; 30(3):271-9.
Questionnaire for assessment of HIV/AIDS control actions in the primary care
The methodological process occurred in two rounds because the first, conducted with 20 participants, did not reach the consensus level adopted for this research. Data collection pro-ceeded with eight experts, because the others did not present suggestions or comments in the first round.(14)
Data were analyzed using the Statistical Pack-age for the Social Sciences (SPSS) software, ver-sion 20.0. The data analysis for content validity was performed using the level of consensus of the answers,(14) associated with the Kappa index to measure the level of agreement and consisten-cy of the experts, regarding whether or not the questions should be retained in the instrument. These values ranged from +1 to -1; values be-tween 0.41 and 0.60 were classified as moderate, 0.61 to 0.80 as substantial, and 0.81 to 1.0 as excellent.(14)
The Kappa coefficient value was consid-ered as a criterion for retaining the questions, ranging between moderate, substantial and ex-cellent, associated with an agreement of ≥75%. Questions with a Kappa coefficient and/or per-centages of agreement less than the referred val-ues were automatically excluded from the ques-tionnaire, and the other questions were revised, using the suggestions and comments presented during the face validation, and submitted to a re-evaluation.(15)
The development of the study met standards of ethics in research involving human subjects (Certifi-cado de Apresentação para Apreciação Ética - CAAE: 23067613.0.0000.5537).
Results
In the first round, experts agreed 100% on the socio-demographic and economic characteris-tics sections, obtaining Kappa values of +1. Of the 47 questions that comprised the question-naire in the initial version, 13 obtained 100% concordance level and Kappa +1; any suggestion for revision was presented, as demonstrated in table 1.
Sixteen questions were automatically eliminated because they did not have the index of agreement established in the survey: K≥0.41 and/or level of agreement ≥75%. The other questions were evalu-ated with Kappa values, varying between substan-tial, moderate and excellent, with 75% to 100% approval regarding retaining questions in the ques-tionnaire; however after analysis, modifications in the face validation were necessary (Chart 1).
Following the revision of the questions, as de-scribed in chart 1, and exclusion of questions that presented poor Kappa values, the questionnaire was submitted to a second round of review. Thir-ty-one questions composed the questionnaire in the second version and, among them, 15 present-ed an excellent level of agreement in the initial version and, subsequently, continued to show this result. A total of five questions were revised to meet the suggestions of the experts. Eleven questions of the instrument obtained Kappa val-ues varying between moderate, substantial and excellent, and a consensus level of 75% to 100% in the sample validation, without suggestions/comments by the experts.
All issues analyzed in the second round were ap-proved in relation to the criteria of relevance, clar-ity, objectivity, accuracy, vocabulary and compre-hensiveness. The questionnaire, in its final version (Chart 2), is composed of two sections, containing seven questions aimed at the sociodemographic and economic characteristics of health professionals, and thirty-one questions to evaluate the control of HIV/AIDS in primary care.
Discussion
The introduction of Highly Active Antiretroviral Therapy (HAART), in 1996, resulted in a signifi-cant reduction in the incidence of AIDS, due to the reduction in the viral load of HIV-positive patients, contributing to a decrease in transmission of the vi-rus.(16) Despite the relative control, some challenges to coping with HIV/AIDS persist, and among these is the expansion of prevention and early diagnosis actions within the healthcare services.(17)

275Acta Paul Enferm. 2017; 30(3):271-9.
Silva RA, Castro RR, Pereira IR, Oliveira SS
Table 1. Expert judgment on issues
QuestionsAppropriate Appropriate
with changesInappropriate
K**
n(%)* n(%)* n(%)*
1 Do you have access to Ministry of Health handbooks regarding the management of STIs (sexually transmitted infections)? 19(95) 0(0) 1(5) 0.459
2 Is an active search conducted to identify the groups most vulnerable to HIV/AIDS infection? 17(85) 0(0) 3(15) 0.34
3 Have you participated in training/qualification on issues related to HIV/AIDS control in the last five years? 19(95) 0(0) 1(5) 0.943
4 Is the availability of time per week for Pap smears sufficient to meet the demand? 13(65) 0(0) 7(35) 0.501
5 Is an information and awareness campaign about risk behaviors for HIV infection conducted in the coverage area of the healthcare unit? 19(95) 0(0) 1(5) 0.459
6 Is the rapid or serological test offered to every person with symptoms suggestive of HIV/AIDS? 16(80) 0(0) 4(20) 0.138
7 Is the prenatal visit performed as soon as possible, after confirmation of pregnancy, in women who have sought health services? 16(80) 1(5) 3(15) 0.852
8 Does the unit have adequate physical space for educational activities? 15(75) 2(10) 3(15) 0.608
9 Is the rapid test offered to partners of people diagnosed with HIV/AIDS? 18(90) 1(5) 1(5) 0.459
10 Is welcoming accomplished along with an initial evaluation of people diagnosed with HIV, in the area covered by the health unit? 18(90) 0(0) 2(10) 0.318
11 Do injecting drug users have access to new/sterile syringes provided by the health unit? 14(70) 0(0) 6(30) 0.306
12 Does the delivery of condoms occur outside the physical space of the health unit? 16(80) 0(0) 4(20) 0.483
13 Are people who are diagnosed with HIV/AIDS monitored by the health unit? 18(90) 0(0) 2(10) 0.773
14 In the initial assessment, are HIV users that can be followed at the unit identified, along with those who should be referred for follow-up in the Specialized Care Services?
17(85) 0(0) 3(15) 0.216
15 Is the management of HIV infection conducted in this unit? 18(90) 0(0) 2(10) 0.318
16 Are you aware of the contents of the manuals provided by the Ministry of Health regarding the measures used to control HIV/AIDS in primary care? 19(95) 0(0) 1(5) 0.459
17 Are information and awareness campaigns conducted for HIV/AIDS prevention in social facilities in the area covered by the health unit? 18(90) 1(5) 1(5) 1
18 Are the laboratory tests recommended by the Ministry of Health requested at the first visit, when a pregnancy result is positive? 20(100) 0(0) 0(0) 1
19 Does the health unit provide educative materials for educational actions? 19(95) 0(0) 1(5) 0.459
20 Is early detection for failure of antiretroviral therapy, and referral to the specialized service performed? 18(90) 0(0) 2(10) 0.318
21 Is the health unit supplied with medications for treatment of STIs (sexually transmitted infections)? 18(90) 0(0) 2(10) 0.318
22 Is the HIV serological test required for all pregnant women? 18(90) 0(0) 2(10) 0.318
23 Are people diagnosed with HIV/AIDS referred by the unit? 20(100) 0(0) 0(0) 1
24 Is an active search conducted for partners when the HIV/AIDS diagnosis is positive? 20(100) 0(0) 0(0) 1
25 Are pregnant women identified with HIV/AIDS referred for medium and high complexity services monitored by the health unit? 19(95) 0(0) 1(5) 1
26 Are condoms not only provided at specific times? 18(90) 0(0) 2(10) 0.139
27 Is HIV serological testing requested for women with complaints suggestive of gynecological infection? 19(95) 1(5) 1(5) 1
28 In the first contact with people suspected of HIV/AIDS has the diagnostic opportunity? 19(95) 1(5) 1(5) 1
29 Does the health facility provide material for rapid HIV/AIDS testing? 20(100) 0(0) 0(0) 1
30 Did you receive training to perform rapid HIV/AIDS testing? 20(100) 0(0) 0(0) 1
31 Is health education on healthy living habits conducted in social facilities in the area covered by the unit? 19(95) 0(0) 1(5) 0.459
32 With the distribution of condoms, is guidance provided on male use? 20(100) 0(0) 0(0) 1
33 Are the results of the 1st and 2nd HIV serology tests requested during prenatal care given to pregnant women during their pregnancy? 17(85) 0(0) 3(15) 0.608
34 Are collective educational actions addressed to the population, related to the prevention of STI (sexually transmitted infections)/AIDS, conducted? 20(100) 0(0) 0(0) 1
35 Is the HIV rapid test provided to all users of the health care facility? 18(90) 0(0) 2(10) 0.318
36 Are educational actions for information and prevention of STIs (sexually transmitted infections) offered in the health unit? 20(100) 0(0) 0(0) 1
37 Are health facility patients educated for healthy sexual habits? 18(90) 0(0) 2(10) 0.31
38 Is notification made within the SINAN (Notifiable Diseases Information System) of STIs (sexually transmitted infection) and injuries? 19(95) 0(0) 1(5) 0.459
39 Is adequate space available for the pharmacy service? 14(70) 0(0) 6(30) 0.306
40 Is an active search performed for pregnant women who began prenatal care, but did not follow through with care? 18(90) 0(0) 2(10) 0.318
41 Is the amount of condoms the unit receives per month enough to meet the demand? 20(100) 0(0) 0(0) 1
42 Is an active search conducted for people whose HIV diagnosis was positive but who did not return to receive the result? 20(100) 0(0) 0(0) 1
43 Are sex workers, homosexuals and drug users identified as vulnerable to HIV/AIDS? 13(65) 0(0) 7(35) 0.136
44 Is HIV/AIDS testing requested at the first prenatal visit? 20(100) 0(0) 0(0) 1
45 Are educational actions about HIV/AIDS provided without difficulties? 20(100) 0(0) 0(0) 1
46 Is the HIV serological test offered to patients of this unit? 19(90) 1(5) 0(0) 1
47 Do you conduct rapid HIV/AIDS pre-test and post-test counseling? 20(100) 0(0) 0(0) 1
* Number of respondents / percentage of agreement; ** Kappa test

276 Acta Paul Enferm. 2017; 30(3):271-9.
Questionnaire for assessment of HIV/AIDS control actions in the primary care
Chart 1. Suggestions from experts on issues considered appropriate with changes neededQuestion Issues evaluated Suggestions/ Expert comments (n*) Acceptance Reformulated question
Is the prenatal visit performed as soon as possible, after confirmation of pregnancy, in women who have sought health services?
Scope Focus not only on the prenatal visit, but also on screening for STIs in pregnant women, such as anti-HIV, VDRL, Hepatitis B and Hepatitis C. (1)
No-
Does the unit have available physical space for educational activities
Vocabulary Replace available physical space with adequate physical space. (2)
Yes Does the unit have adequate physical space for educational activities?
Is the rapid test offered to partners of people diagnosed with HIV/AIDS?
ScopeAdd to the question: is the serological test also offered? (1)
Yes Is the rapid test or serological test offered to partners of people diagnosed with HIV/AIDS?
Are information and awareness campaigns conducted for HIV/AIDS prevention in social facilities in the area covered by the health unit?
VocabularyChange the term social facilities to one that facilitates understanding, for example, social spaces. (1)
No-
Is HIV serological testing requested for women with complaints suggestive of gynecological infection?
Scope Add to the question: if the rapid HIV test is also requested in women who have complaints suggestive of gynecological infection? (1)
Yes Is the rapid test or HIV serological testing requested for women with complaints suggestive of gynecological infection?
In the first contact with people suspected of HIV/AIDS has the diagnostic opportunity?
ClarityRephrase the question in a manner that facilitates understanding. (1)
Yes Do people suspected of HIV infection seeking the health basic unit have the opportunity to perform the diagnostic test in the health care network
Is the HIV serological test offered to patients of this unit?
ScopeAdd the question: is the rapid test also offered? (1)
Yes Is the rapid test and HIV serological test offered to patients of this unit
*Number of experts who commented on the question
Chart 2. Final version of the questionnaire for assessment of HIV/AIDS control in basic care, from the perspective of health professionalsSOCIODEMOGRAPHIC AND ECONOMIC CHARACTERISTICSSex: ( ) Male ( ) Female
Age: _________
Family income: ( ) One minimal wage ( ) Two minimal wage ( ) Three or more
Religion: __________________________________;
Marital status: ( ) Single ( ) Married ( ) Other
Occupation:____________________________________________________;
Time working in the primary health network: ______________________;
SPECIFIC QUESTIONS1 Do you have access to Ministry of Health handbooks regarding the management of STIs (sexually transmitted infections)?
2 Have you participated in training/qualification on issues related to HIV/AIDS control in the last five years?
3 Are information and awareness campaign about risk behavior for HIV infection conducted in the coverage area of the healthcare unit?
4 Is the prenatal visit performed as soon as possible, after confirmation of pregnancy by women who have sought the health services
5 Does the unit have adequate physical space for educational activities?
6 Is the rapid test or serological test offered to partners of people diagnosed with HIV/AIDS?
7 Does the delivery of condoms occur outside the physical space of the health unit?
8 Are people who are diagnosed with HIV/AIDS monitored by the health unit?
9 Are you aware of the contents of the manuals provided by the Ministry of Health regarding the measures used to control HIV/AIDS in primary care?
10 Are information and awareness campaigns conducted for HIV/AIDS prevention in social facilities in the area covered by the health unit?
11 Are the laboratory tests recommended by the Ministry of Health requested at the first visit, when the pregnancy result is positive?
12 Does the health unit provide educative materials for educational actions?
13 Are people diagnosed with HIV/AIDS referred by the unit?
14 Is an active search conducted for partners when the HIV/AIDS diagnosis is positive?
15 Are pregnant women identified with HIV/AIDS referred for medium and high complexity services monitored by the health unit?
16 Is the rapid test or HIV serological testing requested for women with complaints suggestive of gynecological infection?
17 Do people suspected of HIV infection at the primary health unit have an opportunity to perform the diagnostic test in the health care network?
18 Does the health facility provide material for rapid HIV/AIDS testing?
19 Did you receive training to perform rapid HIV/AIDS tests?
20 Is health education on healthy living habits conducted in social facilities in the area covered by the unit?
21 With the distribution of condoms, is guidance provided on male use?
22 Are the results of the 1st and 2nd HIV serology tests requested during prenatal care given to pregnant women during their pregnancy?
23 Are collective educational actions addressed to the population, related to the prevention of STI(sexually transmitted infections)/AIDS conducted?
24 Are educational actions for information and prevention of STIs (sexually transmitted infections) offered in the health unit?
25 Is notification made within the SINAN (Notifiable Diseases Information System) of STI (sexually transmitted infection) and injuries?
26 Is the amount of condoms the unit receives per month enough to meet the demand?
27 Is an active search conducted for people whose HIV diagnosis was positive but did not return to receive the result?
28 Is HIV/AIDS testing requested at the first prenatal visit?
29 Are educational actions about HIV/AIDS provided without difficulties?
30 Is the rapid test and HIV serological test offered to patients of this unit?
31 Do you conduct HIV/AIDS pre-test and post-test counseling?

277Acta Paul Enferm. 2017; 30(3):271-9.
Silva RA, Castro RR, Pereira IR, Oliveira SS
izes the actions for the diagnosis of HIV in a broader way, thus supporting achievement of the target of 90% of people diagnosed with HIV. Brazil has until 2020 to reach the 90-90-90 tar-get established by the country within the United Nations Organization, which was also assumed by the BRICS bloc (comprising Brazil, Russia, India, China and South Africa). The global tar-get foresees a limitation of new infections to 500,000 a year, and zero discrimination.(7)
The expansion of diagnostic testing centers and the inclusion of the rapid tests in the primary health network, in addition to enabling early diag-nosis, provide opportunities for individualized in-terventions across a large number of people.(19,20) Al-though there is increased testing in the country, the absence of counseling is a concerning reality that remains, without attention to the autonomous de-cision-making of the individual, and with inequal-ities inherent in the individual’s level of education, region and race.(21,22)
For proper implementation of the rapid HIV test, four dimensions need to be developed: team awareness and dissemination of rapid test-ing procedures for target audiences; adequate physical space and equipment; availability of in-puts and material and organizational workflow, with a definition of the roles. Based on this, the question, “Does the unit have adequate physi-cal space for educational activities?”, the experts have suggested changes in terms of vocabulary and clarity, because the retention of terms or ex-pressions which are difficult to understand can lead to uncertainty, and elicit responses that do not fit the reality.
The suggestion presented for the question: “In the first contact with people suspected of HIV/AIDS has the diagnostic opportunity?” regarding the aspects of vocabulary and clarity was accepted by facilitating the understanding of the question, and giving objectivity and clarity for the content of the questionnaire.(12)
In the question: Is the prenatal visit performed as soon as possible, after confirmation of pregnan-cy, in women who have sought health services?” the suggestion was pertinent, understanding that ear-
At the national level, preventive actions that were restricted to referral services have been decen-tralized, and are present in primary care, which has developed actions directed at coping with HIV/AIDS at different degrees of complexity and quali-ty. Despite the advances, there are major challenges for improvement.(17)
Because of the responsibility of the primary net-work to control HIV/AIDS, it becomes relevant to investigate diagnoses that have been made opera-tional in this service. However, as seen in the lack of observed questionnaires proposed for this purpose, the importance of a questionnaire and its evaluation by means of a committee of experts is emphasized, since organized collective judgment is more pro-ductive than that of an individual or a group devoid of specific knowledge.(16)
A validated questionnaire can lead to a more precise diagnosis development, as it supports deci-sion-making, insofar as it systematically allows col-lection of data, which are translated into pertinent information about a certain reality, seeking an iden-tification of the needs within each context.(13) The data presented in this study reaffirm the importance of the operationalization of rigorous methodological techniques, and responsibility for the data collected for the development of a validated questionnaire.(12)
The opinion of the experts allowed the de-velopment of a more precise questionnaire.(18) After the first round, a significant portion of the suggestions concerning requirements related to vocabulary, clarity, and comprehensiveness were adopted. Of the seven questions considered ap-propriate, but with needed revision, five were modified for relevance and correspondence with the literature.
Three of the above five questions related to the HIV test were modified according to expert recommendation: “Is the rapid test or HIV sero-logical testing requested for women with com-plaints suggestive of gynecological infection?” and “Is the rapid test and HIV serological test offered to patients of this unit”. These modifi-cations allowed the inclusion of the rapid test along with the serological test, allowing the in-vestigation of how the health team operational-

278 Acta Paul Enferm. 2017; 30(3):271-9.
Questionnaire for assessment of HIV/AIDS control actions in the primary care
which different units of primary health care partic-ipate in the provision of care for those with HIV/AIDS, composing an integrated and articulated network.(23)
In this new model, the design of the care network recognizes primary health care as the entrance into and coordinator of care. Strate-gies such as the support of specialized services for primary care, and the shared care between these services, guarantee greater access for the users into the health system. The decision to im-plement this new model is local, and one of the fundamental points is that health professionals are integrated into the processes of continuous education, thus guaranteeing adequate qualifica-tion for these new demands.(23)
Conclusion
The content validation by expert evaluation proved useful for development and improvement, resulting in the provision of a valid questionnaire, composed of 31 questions focused on evaluating actions for the control of HIV/AIDS in primary health care. The lack of national or international published questionnaires presents this as a possi-ble instrument to be considered by managers and health professionals, to develop a situational diag-nosis of the possibilities and fragilities of primary care in the face of HIV/AIDS control, and may support them in defining a strategic plan. This may therefore contribute to changes in the epi-demiological framework, resulting in benefits for the family, community and users of the primary health network.
CollaborationsSilva RAR and Castro RR contributed to the study design, analysis and data interpretation, article writing, relevant critical review of the intellectu-al content, and final approval of the version to be published. Pereira IRBO and Oliveira SS declare that they contributed to the article writing, relevant critical review of the intellectual content, and final approval of the version to be published.
ly detection of STIs and reduction of vertical HIV transmission can be achieved if these diseases are prevented and/or diagnosed during prenatal care. Thus, the sooner there is adherence to quality pre-natal care, the more effective it may be in reducing transmission, according to the National STD/AIDS policy emphasizing the strategies of the Stork Network, which has primary health care as one of the pillars.(19) However, revision was not performed, because another question in the questionnaire already en-compassed this proposal: “Is HIV/AIDS testing re-quested at the first prenatal visit? “
As recommended by the Ministry of Health, prenatal care should begin in the first trimes-ter and should include the complementary tests, such as the rapid screening test for syphilis and/or VDRL/RPR, rapid HIV test; IgM and IgG toxo-plasmosis, and hepatitis B (HbsAg) testing. Thus, the suggestion to not focus solely on the prenatal visit was not accepted.(18)
The limitations of this study are related to the absence of some issues in the validated ver-sion, associated to the management of HIV in-fection in primary care. The first instrument in-cluded questions that contained this aspect, such as: welcoming and initial evaluation of people diagnosed with HIV, management of HIV infec-tions, identification of users who could be treat-ed at the unit and those who should be referred to a specialized service, and the early detection of antiretroviral therapy failure. The experts jus-tified the removal of these issues based on the lack of permanent education of health profes-sionals to act in the face of this new demand, inadequate physical structure of the units, and the lack of an integrated and articulated network of support in the case of therapeutic failures in primary health care.
However, given the change in the management of HIV infection in Brazil, in which the manage-ment of stable patients using simplified treatment regimens is identified, which is similar to the care of patients with chronic diseases, a new model of care has been established in Brazilian municipali-ties. This model presents an evolution of the mod-els focused on specialized and dynamic services, in

279Acta Paul Enferm. 2017; 30(3):271-9.
Silva RA, Castro RR, Pereira IR, Oliveira SS
12. Silva MB, Argenta C, Saurin G, Crossett MG, Almeida MA. Utilização da técnica delphi na validação de diagnósticos de enfermagem. Rev Enferm UFPE. 2013; 7(1):262-8.
13. Miranda AR, Araújo CS, Castro FS. Instrumento para coleta de dados de pacientes com artrite reumatoide. Rev Enferm Cent O Min. 2012; 2(2):228-42.
14. Scarparo AF, Laus AM, Azevedo AL, Freitas MR, Gabriel CS, Chaves LD. Reflexões sobre o uso da técnica delphi em pesquisas na enfermagem. Rev Rene. 2012; 13(1):242-51.
15. Melo RP, Moreira RP, Fontenele FC, Aguiar AS, Joventino ES, Carvalho EC. Critérios de seleção de experts para estudos de avaliação de fenômenos de enfermagem. Rev Rene. 2011; 12(2):424-31.
16. Boletim Epidemiológico de AIDS, HIV/DST e Hepatites B e C do Município de São Paulo. São Paulo: Secretaria Municipal da Saúde, Coordenação de Vigilância em Saúde. Bol Epidemiol AIDS, HIV/DST. 2011; 14(13):12-91.
17. Paula IA, Guibu IA. DST/aids e rede básica: uma integração necessária. São Paulo: Secretária de Estado da Saúde; 2007.
18. Brêtas AC, Pereira AL. Gestão em unidades básicas de saúde. In: Harada MJ, organizador. Gestão em enfermagem: ferramenta para prática segura. São Caetano do Sul (SP): Yendis; 2011. p. 377-83.
19. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de DST, Aids e Hepatites Virais. Protocolo clínico e diretrizes terapêuticas para prevenção da transmissão vertical de HIV, sífilis e hepatites virais. Brasília (DF): Ministério da Saúde; 2015.
20. Soares PS, Brandão ER. O aconselhamento e a testagem anti-HIV como estratégia preventiva: uma revisão da literatura internacional. Saúde Soc. 2012; 21(4):940-53.
21. Paiva V, Pupo LR, Barbosa R. O direito à prevenção e os desafios da redução da vulnerabilidade ao HIV no Brasil. Rev Saúde Pública. 2006; 40 Supl:109-19.
22. Araújo MA, Farias FL, Rodrigues AV. Aconselhamento pós-teste anti-HIV: análise a luz de uma teoria humanística de Enfermagem. Esc Anna Nery Rev Enferm. 2006; 10(3):425-31.
23. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de DST, Aids e Hepatites Virais. O Manejo da Infecção pelo HIV na Atenção Básica - Manual para Profissionais Médicos. Brasília (DF): Ministério da Saúde; 2015.
References
1. Pereira BS, Costa MC, Amaral MT, Costa HS, Silva CA, Sampaio VS. Fatores associados à infecção pelo HIV/AIDS entre adolescentes e adultos jovens matriculados em Centro de Testagem e Aconselhamento no Estado da Bahia, Brasil. Ciênc Saúde Coletiva. 2014; 19(3):747-58.
2. Dantas MS, Abrão FM, Freitas CM, Oliveira DC. Representações sociais do HIV/AIDS por profissionais de saúde em serviços de referência. Rev Gaúcha Enferm. 2014; 35(4):94-100.
3. Joint United Nations Programme on HIV/AIDS (UNAIDS). Global Report: UNAIDS report on the global AIDS epidemic/2012. [Internet]. [cited 2017 May 28]. Available from: http://www.unaids.org/sites/default/files/media_asset/20121120_UNAIDS_Global_Report_2012_with_annexes_en_1.pdf.
4. Brasil. Ministério da Saúde. Programa Nacional de DST e AIDS. Boletim epidemiológico AIDS - DST. Brasília(DF): Ministério da Saúde; 2016.
5. Taquette SR, Matos HJ, Rodrigues Ade O, Bortolotti LR, Amorim E. The AIDS epidemic in adolescents between the ages of 13 and 19 in the City of Rio de Janeiro, Brazil: space-time description. Rev Soc Bras Med Trop. 2011; 44(4):467-70.
6. Mora Cárdenas CM, Monteiro S, Moreira CO. Ampliación de las estratégias de conserjería y prueba del VIH: desafios técnicos y tensiones ético-políticas. Salud Colectiva. 2014; 10(2):253-64.
7. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Manual técnico de elaboração da cascata de cuidado contínuo do HIV. Secretaria de Atenção à Saúde. Departamento de Vigilância, Prevenção, Controle das Infecções Sexualmente Transmissíveis, do HIV/Aids e das Hepatites Virais. Brasília (DF): Ministério da Saúde; 2017.
8. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Política Nacional de Atenção Básica. Secretaria de Atenção à Saúde. Brasília (DF): Ministério da Saúde; 2012.
9. Stein LM, Falcke D, Predebon JC, Rocha KB, Ávila LM, Azambuja MP. A construção de um instrumento de avaliação discente de um programa de pós-graduação. Psico-USF. 2005; 10(2):141-7.
10. Hulley SB, Cummings SR, Browner WS, Grady D, Hearst N, Newman TB. Delineando a pesquisa clínica: uma abordagem epidemiológica. 3a ed. Porto Alegre: Editora Artmed; 2008.
11. Akins RB, Tolson H, Cole BR. Stability of response characteristics of a Delphi panel: application of bootstrap data expansion. BMC Med Res Method. 2005; 5:37.

280 Acta Paul Enferm. 2017; 30(3):280-6.
Original Article
Epidemiological profile of patients on the waiting list for renal transplantationPerfil epidemiológico dos pacientes em lista de espera para o transplante renalCamilla Maria Mesquita Batista1
Rita Simone Lopes Moreira1
João Luís Erbs Pessoa2
Agenor Spallini Ferraz3
Bartira de Aguiar Roza1
Corresponding authorCamilla Maria Mesquita BatistaRua Napoleão de Barros, 754,04024-002, São Paulo, SP, [email protected]
DOIhttp://dx.doi.org/10.1590/1982-0194201700042
1Escola Paulista de Enfermagem, Universidade Federal de São Paulo, São Paulo, SP, Brazil.2Central Estadual de Transplantes, Secretaria de Saúde do Estado de São Paulo, São Paulo, SP, Brazil.3Sistema Estadual de Transplantes, Secretaria de Saúde do Estado de São Paulo, São Paulo, SP, Brazil.Conflicts of interest: Although Roza BA is an Associate Editor of the Acta Paulista de Enfermagem, the manuscript of her co-authorship has been evaluated by experts not linked to her team. This measure ensures and guarantees scientific and ethics confidentiality explicit in the guidelines of this journal.
AbstractObjective: To identify and describe the profile of patients placed on a single waiting list for renal transplantation in the state of São Paulo.Methods: Cross-sectional epidemiological study of quantitative approach to identify and describe the profile of patients placed on a single waiting list for renal transplantation. In the period from 2009 to 2015, a survey was conducted in the databases of the Notification, Collection and Distribution Center of Organs of the Single Technical Registry, and the following characteristics were established as variables: clinical, demographic and information related to the convocation result. The sample included 12,415 patients undergoing hemodialysis who were simultaneously registered for renal transplantation. The Chi-Square and Student’s t-test were used for descriptive statistical analysis and the Kaplan-Meier estimate was used for significance.Results: A total of 12,415 patients were included, mean age was 50 years, male gender (59.6%), white color (63.1%), blood type O (48.9%), metropolitan region of São Paulo (73.82%), unspecified diagnosis (34.5%), did not undergo transplantation (77.2%), and without clinical conditions to perform the transplant (99.8%).Conclusion: Knowing the profile of patients with chronic kidney disease on the single waiting list allows the development of new health care strategies for reducing mainly morbidity and mortality rates. There is lack in meeting the care demands and high rates of refusal.
ResumoObjetivo: Identificar e descrever o perfil dos pacientes inscritos em lista única de espera para a realização do transplante renal no estado de São Paulo.Métodos: Estudo epidemiológico transversal com abordagem quantitativa para identificar e descrever o perfil dos pacientes inscritos em fila única de espera para o transplante renal. Realizou-se levantamento nas bases de dados da Central de Notificação, Captação e Distribuição de Órgãos do Cadastro Técnico Único, estabelecendo-se como variáveis as características clínicas, demográficas e relativas ao desfecho de convocação no período de período de 2009 a 2015. A amostra foi composta por 12.415 pacientes que realizavam hemodiálise e paralelo ao tratamento encontravam-se inscritos para a realização do transplante renal. Para análise estatística descritiva, utilizou-se os testes Qui-Quadrado, t de Student e para significância Kaplan Meier.Resultados: Foram incluídos 12.415 pacientes, identificou-se média de idade de 50 anos, sexo masculino (59,6%), cor branca (63,1%), tipo sanguíneo O (48,9%), região metropolitana de São Paulo (73,82%), diagnóstico não especificado (34,5%), não realizaram transplante (77,2%) e sem condições clínicas de realizar o transplante (99,8%).Conclusão: Conhecer o perfil dos pacientes com doença renal crônica que aguardam em lista única nos permite traçar novas estratégias de cuidados em saúde para redução principalmente das taxas de morbidade e mortalidade. Nota-se carência de atendimento da demanda e altos índices de recusa.
KeywordsKidney transplantation; Kidney diseases; Health profile; Waiting lists
DescritoresTransplante renal; Nefropatias; Perfil de saúde; Listas de espera
Submitted March 15, 2017
Accepted June 26, 2017

281Acta Paul Enferm. 2017; 30(3):280-6.
Batista CM, Moreira RS, Pessoa JL, Ferraz AS, Roza BA
Introduction
Chronic kidney disease (CKD) has become in-creasingly important in Brazil. It is an increas-ingly common disease associated with high mortality and morbidity, and costs that impact negatively on health-related quality of life. The annual increase in number of new patients with end-stage renal disease requiring renal transplan-tation, and the growing gap between demand and supply of kidneys has led to the progres-sive expansion of the renal transplant waiting list globally. This has become a major problem, since many patients die while waiting to receive a kidney.(1-3)
In Brazil, the number of kidney transplants performed per year covers only an average of 30% of the total of people on the waiting list for this organ. Transplants are part of the budget of finan-cial resources destined to the health sector, and Brazil has the largest public system of transplants in the world, financing more than 90% of surgeries performed by the Unified Health System (SUS - Sistema Único de Saúde). In the state of São Pau-lo, control of the convocation of registered candi-dates is performed by the Single Technical Regis-try (CTU), a computerized database of the State System of Transplants of São Paulo (SIGSET). This database stores receptors’ information (ac-tive potentials, semi-active, removed, transplanted patients and deceased), notifications of donors in brain death and heart failure, effective organ and tissue donors, transplant medical staff, notification and transplant hospitals in the state, Organ Pro-curement Organizations (OPOs), and Intra Hos-pital Commissions of Organ and Tissue Donation for Transplantation (CIHT).(4-7)
The waiting list is the only option for kidney patients without contraindications and who cannot find a donor among their relatives up to the fourth degree of kinship, donation of spouses or anyone else. In all states of the federation, there is a single waiting list, organ allocation is regulated by specific legislation, controlled by the National Transplant System, and distribution is based on the HLA (Hu-man Leucocyte Antigen) compatibility test.(1,2,7)
In the first half of 2016, the 120 kidney transplant centers recorded 2,651 transplants. In the whole year of 2015, were performed 5,556 kidney transplants, of which 1,172 were from a living donor, 4,384 from a deceased donor, 951 from relatives, 165 from non-relative/spouse, and 56 from non-relative/others. The southeast and south regions had the highest number of transplants performed, highlighting the state of São Paulo with a total of 1,983 procedures, lead-er in the number of renal transplant teams, with 33 active teams.(2)
The state of São Paulo is the largest in absolute number of transplants given the size of its popula-tion and the migration of patients from other states. Over the past three years, the numbers of effective donors and about 2,000 kidney transplants per year have remained stable, with 75% of deceased donors.(1,2) In São Paulo, it is possible to perform all types of transplants in numbers above the average of the region and the country. The objective of this study was to identify and describe the epidemiological profile of patients registered in the Single Registry of Renal Transplantation of the state of São Paulo from 2009 to 2015.
Methods
Cross-sectional epidemiological study with quantitative approach to identify and describe the profile of patients placed on a single wait-ing list for renal transplantation in the state of São Paulo. Data were collected from the Noti-fication, Collection and Distribution of Organs Central (CNCDO 1) of the Single Technical Registry (CTU) between years 2009 and 2015. The following characteristics were established as variables: clinical (diagnosis and blood group), demographic (sex, age in years, race and origin) and related to the convocation result (perfor-mance of renal transplantation or not, and rea-sons for refusal).
The sample included 12,415 patients un-dergoing hemodialysis and simultaneously reg-istered for renal transplantation. The collect-

282 Acta Paul Enferm. 2017; 30(3):280-6.
Epidemiological profile of patients on the waiting list for renal transplantation
ed data were extracted into a Microsoft Excel spreadsheet. Subsequently, was performed an analysis using the IBM® Statistical Package for social Science SPSS® 20.0 and the Data Analysis and Statistical Software STATA®, version 12.0. The loss of incomplete bank data and the elim-ination of duplicate information were not con-sidered significant or a posing risk in the reflec-tion of results obtained.
The associations between categorical vari-ables were verified using the Chi-Square test. The comparison of two means was performed using the Student’s t-test for independent sam-ples. The Kruskal-Wallis nonparametric test, necessary for the analysis of variance - ANOVA, was used for the comparison of more than two means.
The survival functions were analyzed sep-arately for each predictor variable (univariate analysis) by patient’s characteristics. The Ka-plan-Meier survival test was used for categorical variables. Subsequently, the Cox model (multi-variate) was applied for the simultaneous evalu-ation of effects of all predictor variables on sur-vival time. All predictor variables selected (race, ABO, diagnosis, sex, age and region) were in-cluded in the model.
The significance level was set at 5% for all sta-tistical tests.
The study met the ethical standards for research involving human beings - Presentation Certificate for Ethical Appreciation (CAAE - Certificado de Apresentação para Apreciação Ética) Registration number 16300113.6.0000.5505.
Results
The sample consisted of 12,415 patients registered in the CTU in São Paulo to undergo renal trans-plantation. The mean age at the time of registration was 50.2 years (SD=15.3 years), with a minimum age of 2 years and maximum age of 98 years. The median of ages was 52 years.
The Chi-square test and the Student’s t-test were used, and predominance of male patients
was found with 59.6% of the sample (p <0.001). In addition, 63.1% of the patients were white, 48.9% had blood type O, and 26.2% were from the city of São Paulo. Regarding disease diag-nosis, 34.5% had umspecified etiology (Other), 28.2% presented Systemic Arterial Hypertension (SAH), and 20.8% had diabetes mellitus (DM), as shown in table 1.
Table 1. Analysis of patients by predictive characteristicsVariables n(%)
Sex 12415(100.0)
Female 5016(40.4)
Male 7399(59.6)
Race 12415(100.0)
Asian 234(1.9)
White 7840(63.1)
Black 1528(12.3)
Mixed 2813(22.7)
Blood type 12415(100.0)
A 4393(35.4)
AB 419(3.4)
B 1528(12.3)
O 6075(48.9)
Diagnosis 12397(100.0)
Diabetes 2576(20.8)
Hypertensive arterial disease 3499(28.2)
Glomerulonephritis 1777(14.3)
Interstitial nephritis (pyelonephritis) 266(2.1)
Other 4279(34.5)
No information 18(0.1)
County 12415(100.0)
SP 3257(26.2)
Other 9158(73.8)
The discriminant analysis of variables demonstrates patients’ distribution by refusals and transplant situation. In 6.9% of patients, there was at least one refusal before receiving the transplant. The percentage of transplants per-formed in the first offer was 15.9%, and regis-tered candidates who did not receive nor under-go renal transplantation correspond to 77.2% (Figure 1).
A profile of the patients placed on the waiting list in the CTU of São Paulo can be traced based on the results found. The predominant clinical and demographic characteristics, and those related to the convocation result (if renal transplantation was performed or not) were evaluated and are presented below (Figure 2).

283Acta Paul Enferm. 2017; 30(3):280-6.
Batista CM, Moreira RS, Pessoa JL, Ferraz AS, Roza BA
Discussion
Some limitations of the study are related to the fact that it is a cross-sectional epidemiological analysis with limited execution time that excluded patients registered outside the established period. In the present study, issues on patients’ awareness
and adherence to treatment during their time on the waiting list were not controlled. In addition, the findings only cover the profile characteriza-tion of renal transplant candidates in the state of São Paulo.
Tracing the epidemiological profile of pa-tients undergoing hemodialysis treatment in the
Figure 1. Patients’ distribution by refusals and transplant situation
Transplantation in thefirst offerN=1,975(15.9%)
With refusals beforetransplantation
N=861(6.9%)
No offer and notransplantN=9,579(77.2%)
Figure 2. Profile of patients registered in the renal single technical registry of São Paulo
Male59.6%
White race63.1%
Blood type O48.9%
Did not undergotransplantation
77.2%
Receptor withoutclinical conditions
99.8%
Metropolitanregion of SP
73.8%
Unspecified diagnosis“Other”34.5%

284 Acta Paul Enferm. 2017; 30(3):280-6.
Epidemiological profile of patients on the waiting list for renal transplantation
state of São Paulo allows a better understand-ing of the population on the waiting list for re-nal transplantation, the achievement of greater chances of success in the care provided, adequate follow up of treatment, and fewer occurrences in the period of adaptation to the new organ. In addition, it provides subsidies for health profes-sionals’ clinical practice in the improvement of services provided.
The results showed that most individuals reg-istered on the CTU list were male (59.6%), aged between 51 and 60 years (mean age 50.2 years), minimum age of two years and maximum age of 98 years. Similar studies conducted in the south, southeast and northeast regions corroborate with these findings, in which it was observed that most patients registered with hemodialysis programs awaiting kidney transplant are over 50 years of age and predominantly male.(8)
Results of the Brazilian Society of Nephrolo-gy’s 2015 Census also confirm that, out of a total of 111,303 patients in renal replacement therapy (RRT) in Brazil, the majority is aged between 45 and 62 years, and about 58% is male. Likewise, the survey of the Brazilian Chronic Dialysis Survey of 2014 found that 58% of patients with chronic kid-ney disease on the waiting list for renal transplanta-tion are males with an age percentage correspond-ing to the present study.(9,10)
According to the Ministry of Health, men are more vulnerable to chronic diseases, particularly systemic arterial hypertension (SAH) and diabetes mellitus (DM), the main risk factors for CKD. In the daily routine of health services, it is observed empirically that men of working age seek less care than women, as women seek health services more often because of gynecological care. This fact may be related to male vulnerability and with propensity to suggest superiority on the waiting list for renal transplantation.(4,11-13)
In the present study, the underlying diagnosis ‘Other’ (unspecified) was the most frequent cause of chronic renal failure with 34.5%, followed by hypertension with 28.2%, DM with 20.8%, glo-merulonephritis with 14.3%, and interstitial ne-phritis (pyelonephritis) with 2.1%. Similar epide-
miological studies have shown that HAS and DM underlying diseases are commonly identified as the main primary diagnoses and responsible for about half of pathologies of patients undergoing dialysis treatment in Brazil. Causes of unknown etiology for CKD also appear constantly in the registries. Sim-ilar studies indicate DM is consistently the main cause in some northeastern states.(13-15)
In the evaluation of survival functions by pa-tients’ characteristics, was found the mean time of 63.4 months until the transplant using the Ka-plan-Meier model, and the probability estimate of not undergoing transplantation in up to five years was 87.8%. In a detailed analysis of the relation-ship between underlying diagnoses by patients’ sex, was found male prevalence in hypertensive arterial disease with 29.1%, and diabetes mellitus with 23.2%. The diagnosis of glomerulonephritis is predominantly observed in females with 16%, the same way as the diagnosis ‘Other’ that corre-sponds to 37.4% of the total. Among patients of both sexes who did not undergo transplantation, more than half presented DM as the underlying disease. Another study conducted by Malta et al.(17) confirms these results. A higher prevalence of hypertension and DM was found in male patients with CKD.(16,17)
In the ethnic group, there was predominance of the white race with 63.1% of the total, followed by mixed race with 22.7%, black race with 12.3% and Asians with 1.9%. However, data analysis demonstrates this feature is not necessarily relat-ed to transplantation because the assessment of clinical conditions of patients on the waiting list and their selection occur regardless of race thus, non-ethnic differences. Similar studies performed in the southeast and south regions presented sim-ilar results with predominance of white race by self-report.(18)
Blood type O patients had fewer transplants compared to patients from other blood type groups, which may be explained by the presence of anti-A and anti-B agglutinins in plasma. Re-garding the ABO system, there is greater per-centage of blood type O individuals on the sin-gle waiting list. This information is in line with

285Acta Paul Enferm. 2017; 30(3):280-6.
Batista CM, Moreira RS, Pessoa JL, Ferraz AS, Roza BA
studies of Machado et al.,(5)and associated to the fact that blood type O individuals are compatible only with those of the same blood type group.(19)
Regarding the origin, most patients registered in the CTU came from the metropolitan region of São Paulo (78.3% of the total), while 26.2% were from the city of São Paulo. This is explained by the provision of services by the public health net-work through an agreement with SUS, with offer of ambulatory care before and after transplantation (mainly with supply of immunosuppressive drugs after renal transplantation), a specialized unit for hospitalization, surgical procedures, and high com-plexity diagnoses for treated patients.(3,11,17)
In view of these findings, it is important that patients entering RRT for renal transplantation are referred early (while they are on the single waiting list), because dialysis time may negatively influence the identification of a compatible donor and the time of survival of the transplanted organ. Health professionals should be attentive to improvements in the health care of renal patients in dialysis ther-apy. The clinical condition and development of co-morbidities may inactivate the patient on the list or even definitively prevent him/her from undergoing renal transplantation.
Conclusion
By knowing the profile of the population on the single waiting list for kidney transplantation, new health care strategies can be developed to reduce mainly morbidity and mortality rates. There is lack in meeting the care demands and high rates of re-fusal. The conclusion is that the identification and analysis of patients’ profile can support health pro-fessionals working in the clinical area by facilitat-ing the management of activities developed in the field. The characterization of patients placed on the waiting list for renal transplantation is necessary in all transplant centers and renal replacement ther-apy treatment centers, because socio-populational aspects can determine the type of commitment re-sulting from chronic kidney disease, as well as their evolution in the period after renal transplantation.
AcknowledgementsThanks to the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) for granting a postgraduate program scholarship, master’s level, to Batista CMM.
CollaborationsBatista CMM, Moreira RSL, Roza BA, Pessoa JLE and Ferraz AS contributed to the project de-sign, data collection, analysis and interpretation, article writing, critical review of the intellectual content and final approval of the version to be published.
References
1. Brasil. Ministério da Saúde. Governo Federal. DATASUS. Indicadores de Morbidade. Prevalência de pacientes em diálise SUS - Brasil. Brasília (DF): Ministério da Saúde; 2015.
2. Associação Brasileira de Transplante de Órgãos - ABTO. Registro Brasileiro de Transplantes - RBT. Dados numéricos da doação de órgãos e transplantes realizados por estado e instituição no período: Janeiro / Junho. 2015. RBT. 2015; 21(1):1-29.
3. Shrestha BM. Strategies for reducing the renal transplant waiting list: a review. Exp Clin Transplant. 2009; 7(3):173-9.
4. Torres GV, de Mendonça AE, Amorim IG, de Oliveira IC, Dantas RA, Freire IL. Profile of patientes on the waiting list for kidney transplantation. Rev Enferm UFSM. 2013; 3(Esp):700-8.
5. Machado EL, Cherchiglia ML, Acúrcio FD. Profile and clinical outcome of patients in waiting list for kidney transplantation, Belo Horizonte (MG, Brasil), 2000-2005. Ciênc Saúde Coletiva. 2011; 16(3):1981-92.
6. São Paulo (Estado) Governo do Estado. Gabinete do Secretário. Resolução SS nº 114, de 29 de Setembro de 2014. Dispõe sobre a estrutura organizacional e operacional do Sistema Estadual de Transplantes de São Paulo. Diário Oficial do Estado (São Paulo). 2014; 30 de Setembro de 2014; Seção 1. p. 34.
7. Brasil. Ministério da Saúde. Gabinete do Ministro. Portaria nº 2.600, de 21 de Outubro de 2009. Aprova o Regulamento Técnico do Sistema Nacional de Transplantes. Diário Oficial da União: República Federativa do Brasil [Internet]. [citado 2017 Ju 24]. Disponível em: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2009/prt2600_21_10_2009.html.
8. de Oliveira HM Jr, Formiga FF, Alexandre CS. Clinical and epidemiological profile of chronic hemodialysis patients in João Pessoa. J Bras Nefrol. 2014; 36(3):367-74.
9. Sesso RC, Lopes AA, Thomé FS, Lugon JR, Martins CT. Brazilian Chronic Dialysis Census 2014. J Bras Nefrol. 2016; 38(1):54-61.
10. Sociedade Brasileira de Nefrologia. Censo de Diálise 2015 [Internet]. [citado 2017 Jun 24]. Disponível em: http://censo-sbn.org.br/inicio.
11. Oliveira CS, da Silva EC, Ferreira LW, Skalinski LM. [Profile of chronic renal patients on renal dialysis treatment]. Rev Baiana Enf. 2015; 29(1):42-9. Portuguese.

286 Acta Paul Enferm. 2017; 30(3):280-6.
Epidemiological profile of patients on the waiting list for renal transplantation
12. Teixeira FI, Lopes ML, Silva GA, Santos RF. Survival of hemodialysis patients at a university hospital. J Bras Nefrol. 2015; 37(1):64-71.
13. Negretti CD, Mesquita PG, Baracho NC. Epidemiological profile of chronic renal failure on conservative treatment in a hospital in southern school of Minas. Rev Ciênc Saúde. 2014; 4(4):1-12.
14. Soares GL, Oliveira EA, Lima LH, Formiga LM, de Brito BB. Epidemiological profile of chronic renal failure patients on hemodialysis: a descriptive study. Rev Mult em Saude do Hosp São Marcos. 2013; 1(1).
15. Carmona CF, Couto VV, Scorsolini-Comin F. A experiência de solidão e a rede de apoio social de idosas. Psicol Estudo (Maringá). 2014; 19(4):681-91.
16. Almeida MC, Cardoso MS, Garcia CP, de Oliveira JR, Gomes MF. Profile of chronic kidney patients at a public hospital of Bahia. Rev Enf Contemp. 2013; 2(1):157-68.
17. Malta DC, Stopa SR, Szwarcwald CL, Gomes NL, Silva Junior JB, dos Reis AA. Surveillance and monitoring of major chronic diseases in Brazil - National Health Survey, 2013. Rev Bras Epidemiol. 2015; 18 Suppl 2:3-16.
18. Coutinho NP, Tavares MC. Care for chronic renal patients undergoing hemodialysis, from the perspective of the user. Cad Saúde Colet. 2011; 19(2):232-9.
19. Mendes KD, Lopes NL, Fabbris MA, de Castro-e-Silva JO, Galvão CM. Sociodemographic and clinical characteristics of candidates for liver transplantation. Acta Paul Enferm. 2016; 29(2):128-35.

287Acta Paul Enferm. 2017; 30(3):287-94.
Original Article
Profile of accidents in children and adolescents receiving care at a public hospital
Perfil dos acidentes na infância e adolescência atendidos em um hospital público
Fernanda Rocha Fodor Filócomo1
Maria de Jesus Castro Sousa Harada2
Renata Mantovani3
Conceição Vieira da Silva Ohara1
Corresponding authorFernanda Rocha Fodor FilócomoShishima Hifumi Avenue, 2911,12244-000, São José dos Campos, SP, [email protected]
DOIhttp://dx.doi.org/10.1590/1982-0194201700044
1Universidade do Vale do Paraíba, São José dos Campos, SP, Brazil.2Escola Paulista de Enfermagem, Universidade Federal de São Paulo, São Paulo, SP, Brazil.3Hospital Municipal José de Carvalho Florence, São José dos Campos, SP, Brazil.Conflicts of interest: authors declare that they do not have any political, personal, finance, or institutional current or potential conflict of interest. This paper was adapted from the Master degree thesis “Accidents in childhood and adolescence: frequency, characteristics, and related factors”, presented at Escola Paulista de Enfermagem, Universidade Federal de São Paulo, SP, Brazil.
AbstractObjective: To analyze the occurrence of accidents in a pediatric emergency room at a public hospital.Methods: This was a cross-sectional, descriptive, and correlational study on the occurrence of accidents among children and adolescents identified during care delivery in a pediatric emergency room in the municipality of São José dos Campos. The initial sample included 2440 recorded cases, but the sample sized was reduced to 2,421 because 16 cases were suspected of a violent cause and 3 cases were missing data. The data collection instrument was completed by data registration in the unit using a care form. Data were collected from September 01 to December 31, 2013. Inclusion criteria were children and adolescents aged 0 to 13 years with an accident-related admission to the emergency room at the hospital where the study was carried out. We excluded those who were assisted in the emergency room for any other reason during the study period.Results: Accidents corresponded to 12.1% of instances of care delivered. A majority occurred in boys (62.5%); participants’ ages ranged from 0 to 13 years (33.6%). Falls were the most frequent type of accident (48.7%). The body part most affected in children up to 1 year of age was cephalic/neck (75.0%); among adolescents, the most affected body parts were the upper limbs and lower limbs (approximately 30% occurrence). Main in-hospital procedures were radiography (67.6%), evaluation by a specialist (52.7%), and orthopedic splinting (25.9%). Discharge was the most common endpoint (84.0%), followed by observation (10.5%), hospitalization (4.2%), and death (one patient). Conclusion: Accidents had a higher incidence and had an impact on the population and health sector of the municipality, including an increase in the number of instances of care and, consequently, in cost, in addition to the incalculable emotional impact.
ResumoObjetivo: Analisar as ocorrências de acidentes atendidos no pronto-socorro pediátrico de um hospital público.Métodos: Trata-se de uma pesquisa transversal, descritiva e correlacional sobre a ocorrência de acidentes em crianças e adolescentes, identificados no momento do atendimento em um pronto-socorro pediátrico no Município de São José dos Campos. A amostra inicial foi de 2.440 registros de atendimentos, mas foi reduzida para 2.421, porque em 16 casos houve a suspeita de violência e em três não foi possível localizar os dados. O preenchimento do instrumento de coleta de dados foi realizado por meio de dados registrados na ficha de atendimento da unidade. O período de coleta foi de 01 de setembro a 31 de dezembro de 2013. Os critérios de inclusão foram: ser criança ou adolescente de 0 a 13 anos de idade; ser atendidos por acidentes, no pronto-atendimento do referido hospital no período do estudo. O critério de exclusão foi ter sido atendido no referido pronto-atendimento devido a outras causas no período do estudo.Resultados: Os acidentes corresponderam a 12,1% do atendimento; predominância do sexo masculino (62,5%); faixa etária mais acometida foi a de 10 a 13 (33,6%). O tipo de acidente mais frequente foi queda (48,7%). A parte do corpo acometida, em crianças de até um ano, foi o segmento cefálico/pescoço (75,0%), nos adolescentes, foram membros superiores (MMSS) e inferiores (MMII) com aproximadamente 30,0%. Os principais procedimentos intra-hospitalares foram: Raio-X (67,6%), avaliação de especialista (52,7%); imobilização ortopédica (25,9%). Alta foi o desfecho mais ocorrido (84,0%), seguido por observação (10,5%), internação (4,2%) e um óbito. Conclusão: Acidentes tiveram alta incidência, acarretando impacto para a população e setor saúde, incluindo elevação do número de atendimentos e, por consequência, do custo, além de incalculáveis reflexos emocionais.
KeywordsChild; Adolescent; Accident prevention;
External cause
DescritoresCriança; Adolescente; Prevenção de
acidentes; Causas externas
Submitted April 5, 2017
Accepted June 26, 2017

288 Acta Paul Enferm. 2017; 30(3):287-94.
Profile of accidents in children and adolescents receiving care at a public hospital
Introduction
Accidents in childhood and adolescence have been implicated as responsible for an increase in morbidity and mortality rates in this population worldwide. In 2007, the U.S. nongovernmental organization Safe Kids stated that a mean of 12 children are harmed per minute. Every 101 min-utes, a child dies from these injuries; for this rea-son, such accidents are considered the main cause of death and disability in individuals aged 1 to 14 years.(1)
In Brazil, the rate of accidents has increased, and accidents have become a serious public health problem. In 2013, according to prelimi-nary data from the Information System on Mor-tality (SIM), 75,685 deaths occurred among population aged 0 to 19 years. Of these, 21,859 deaths (28.88%) were related to external causes, and among them 7,520 (34.4%) were caused by accidents.(2) Concerning morbidity, from January to September 2015, accidents were responsible to 170,066 hospitalizations of individuals aged 0 to 19 years.(3)
In 2001, the Brazilian Ministry of Health created a national policy for reduction of acci-dents and violence. One of the main goals is to reduce morbidity and mortality rates by using ar-ticulated and systematized actions related to the promotion and prevention of such events.(4) After 16 years of implementation of this policy(4), the impact of this disease has improved and the visi-bility of strategies for prevention and control has been amplified.
Another important measure was to diffuse the concept, adopted by the scientific community, that accidents are predictable and can be prevented and thereby to strengthen the knowledge of researchers on factors associated with risk for and protection against accidents.
An accident is defined as a series of uninten-tional events in a short period of time in which an external agent causes an imbalance, leading to the transfer of energy of the environment to the individual and physical, material and/or physical damages. This energy can be mechanical (falls,
collisions), thermic (burns), electric (shocks) or chemical (poisoning).(5)
Understanding how the context of accidents allows the opportunity to analyze how accidents present in specific population and how they are di-mensioned would help in the allocation of funding for direct specific actions to prevent or reduce this disease damage.
This study analyzed the occurrence of accidents in children and adolescents assisted at the pediatric emergency room at a public hospital in the munici-pality of São José dos Campos, São Paulo.
Methods
This cross-sectional, descriptive, correlational study evaluated the occurrence of accidents in children and adolescents at a pediatric emergency room in the municipality of São José dos Campos.
The initial sample consisted of medical records from 2440 instances of care, but it was reduced to 2421 because 16 cases were suspected of being caused by violence and three were missing data. The data collection instrument was completed by with registered records using an assistance form from the unit.
Data were collected from September 1 to De-cember 21, 2013. Inclusion criteria were children and adolescents aged 0 to 13 years who were ad-mitted because of an accidents and assisted at the emergency room of the specific hospital during the study period. Patients were excluded if they were assisted in the emergency room because of other causes during the study period.
This study followed ethical principles of reso-lution no. 466/12 from the National Council of Health.(6) The ethical and research committee of Universidade Federal de São Paulo approved the study under no. 319.241 in July/2013.
Results
A majority of patients seen were male (1512 cas-es [62.5%]); 909 females were seen (37.5%). Falls

289Acta Paul Enferm. 2017; 30(3):287-94.
Filócomo FR, Harada MJ, Mantovani R, Ohara CV
were the most frequent accident (48.7%), fol-lowed by accidents caused by contact with objects (16.5%) and unidentified accidents with unde-fined injuries (10.6%).
Accidents seen more frequently in males were animal bites (77.7%), being run over by moving vehicle (75.0%), environmental poi-soning (72.7%), physical shocks (72.2%), stings (66.7%), unidentified accident with undefined injury (65.4%), contact with objects (65.0%), falls (60.9%), foreign body ingestion (56.1%), collision (54.3%), and unidentified accident with sprain injury (53.3%).
Table 1 shows that burns (50.0%), poisoning (66.7%), swallowing or introduction of a foreign body (55.3%), and other accidents (62.9%) oc-curred mainly in individuals aged 1 to 4 years. In contrast, falls (27.4%), physical shock (44.4%),
animal bites (38.4%), and stings (50.0%) were more common among children aged 5 to 9 years.
Among children younger than 1 year and those aged 1 to 4 years (Table 2), the majority had affect-ed cephalic segment, corresponding to 75.0% and 34.0%, respectively. Upper and lower limbs were more affected in children aged 5 to 9 years (28.2% and 23.6%) and adolescents aged 10 to 13 years (35.7% and 30.8%), respectively.
Total number of procedure done in the hospi-tal because of accidents was 4,230, correspond-ing to 1.75 procedures per child. Most proce-dures consisted of radiographic examinations (n=1527) and specialist evaluation (n=1191), followed by orthopedic splinting (n=584), com-puted tomography (n=237), dressing or sutur-ing (n=193), symptomatic prescription (n=104), administration of saline solution and/or vaccine
Table 1. Children and adolescents who sustained accidents and received care at H.M.J.C.F by age range and type of accident
Type of accidentAge range n (%)
Total0 to 1 year 1 to 5 years 5 to 10 years 10 to 14 years
Contact with object 5(1.3) 95(23.8) 140(35.0) 160(40.0) 400(100.0)
Burns - 11(50.0) 5(22.7) 6(27.3) 22(100.0)
Poisoning 1(3.0) 22(66.7) 4(12.1) 6(18.2) 33(100.0)
Fall 119(10.1) 323(27.4) 387(32.9) 349(29.6) 1178(100.0)
Physical shock - 5(27.8) 8(44.4) 5(27.8) 18(100.0)
Animal bites 2(1.9) 35(34.0) 40(38.8) 26(25.2) 103(100.0)
Stings - 4(33.3) 6(50.0) 2(16.7) 12(100.0)
Swallowing or introduction of foreign body 2(1.8) 63(55.3) 38(33.3) 11(9.6) 114(100.0)
Collision 5(10.9) 9(19.6) 15(32.6) 17(37.0) 46(100.0)
Being run over - 12(25.0) 13(27.1) 23(47.9) 48(100.0)
Unidentified accident/ sprain injury - 20(16.7) 32(26.7) 68(56.7) 120(100.0)
Unidentified accident / undefined injury† 4(1.6) 40(15.6) 82(31.9) 131(51.0) 257(100.0)
Other accidents‡ 10(14.3) 44(62.9) 7(10.0) 9(12.9) 70(100.0)
Total 148(6.1) 683(28.2) 777(32.1) 813(33.6) 2421(100.0)
†Case with trauma diagnosis without defined injury because of unidentified accident; ‡33 cases in which an object fell on the child and 37 cases of painful pronation
Table 2. Children and adolescents who sustained accidents and were assisted at Hospital MJCF by age range, according to affected part of body
Affected part of the bodyAge range – n(%)
Total (n=2,421) p-value*
0 t 1 year (n= 148) 1 to 5 years (n=683) 5 to 10 years (n=777) 10 to 14 years (n=813)
Cephalic segment and neck 111(75.0) 232(34.0) 166(21.4) 72(8.9) 581(24) < 0.001
Upper limbs 18(12.2) 140(20.5) 219(28.2) 290(35.7) 667(27.6) < 0.001
Lower limbs 4(2.7) 91(13.3) 183(23.6) 250(30.8) 528(21.8) < 0.001
Hip 2(1.4) 6(0.9) 14(1.8) 14(1.7) 36(1.5) 0.461
Thorax 2(1.4) 4(0.6) 14(1.8) 11(1.4) 31(1.3) 0.229
Multiple regions of the body 1(0.7) 11(1.6) 20(2.6) 17(2.1) 49(2) 0.369
No information 9(6.1) 124(18.2) 147(18.9) 161(19.8) 441(18.2) 0.001
*Descriptive level of chi-squared test

290 Acta Paul Enferm. 2017; 30(3):287-94.
Profile of accidents in children and adolescents receiving care at a public hospital
Table 3. Children and adolescents who sustained accidents and received care at Hospital MJCF according to assistance progress and type of accident
Type of accident
Progress n(%)
TotalHigh
Pediatric observation
Hospitalized at ICU
Hospitalized in pediatric nurse ward
Death Evasion Transferred
Contact with object 383(95.8) 9(2.3) - 7(1.8) - 1(0.3) - 400(100.0)
Burns 20(90.9) - - 2(9.1) - - - 22(100.0)
Environmental poisoning 18(54.5) 12(36.4) 2(6.1) 1(3.0) - - - 33(100.0)
Fall 936(79.5) 167(14.2) 4(0.3) 61(5.2) - 9(0.8) 1(0.1) 1178(100.0)
Physical shock 15(83.3) 2(11.1) - 1(5.6) - - - 18(100.0)
Animal bites 100(91.1) 2(1.9) - 1(1.0) - - - 103(100.0)
Stings 8(66.7) 4(33.3) - - - - - 12(100.0)
Foreign body† 87(76.3) 10(8.8) - 16(14.0) - 1(0.9) - 114(100.0)
Collision 14(30.4) 28(60.9) - 3(6.5) 1(2.2) - - 46(100.0)
Being run over 22(45.8) 16(33.3) 3(6.3) 7(14.6) - - - 48(100.0)
Unidentified accident‡ 118(98.3) - - - - 2(1.7) - 120(100.0)
Unidentified accident § 252(98.1) 1(0.4) - 1(0.4) - 3(1.2) - 257(100.0)
Other accidents‡‡ 60(85.7) 4(5.7) 2(2.9) 2(2.9) - 2(2.9) - -
Total 2.033(84.00) 255(10.5) 11(0.5) 102(4.2) 1(0.0) 18(0.7) 1(0.0) 2421(100.0)
†swallow or introduction of foreign body; ‡sprain injury; §with non-defined injury; ‡‡33 cases of object fall over the child and 37 cases of painful pronation
nel resources and considerable funding away from other causes.
In the analysis according to sex, a predominance of males was seen, with a ratio of 1.66 boys for each girl. This result agrees with the report from VIVA/MS concerning the emergency assistance because of accidents with children younger than 10 years, and this predominance of males totaled 59.4%.(8)
The higher number of males can be explained by the types of activities boys may engage in more frequently, including those involving speed, strength, and body impact. For this reason, boys traditionally may be exposed to situations that can lead to accidents. Another possibility is that girls traditionally may be more likely to partici-pate more introspective activities and games that require less energy and exposed them to closer vig-ilance, thereby reducing the risks of accidents.(8) Despite these possible explanations, it is import-ant to emphasize that no rules exist to determine which games each sex participates in; play involves fantasy, and this is the way in which children in-teract with each other and is essential for healthy development.
The mean age of patients experiencing an acci-dents was 7.2 years, with a standard deviation of 4.2 years, and median of 7.5 years In this study, the age range most affected was 10 to 13 years (33.6%), fol-
(n=110), surgical intervention (n=91) and ad-vises (n=21).
Table 3 shows that the following cases were under surveillance: 36.4% of environmental poi-soning, 60.9% of collision occurrences, 33.3% of runover cases, and 14.2% of falls. We also observed that only 4.2% of children remained hospitalized (in a nurse ward) and 0.5% were referred to inten-sive care therapy. One 6-year-old child who was a traffic accident victim died.
Discussion
In the past few decades, achievements related to health promotion to children have been reported, and these improvements are reflected in the reduc-tion of child mortality. In relation to accidents, part of these occurrences, is considered integrating fact of life and concerning development in all spheres of the society.(7)
The results of this study revealed that seeking emergency care because of an accidents during childhood and adolescence is significant, account-ing for 12.1% of all instances of care provided in a reference hospital of the region. This value is im-portant mainly because most accidents are avoid-able and force institutions to divert time, person-

291Acta Paul Enferm. 2017; 30(3):287-94.
Filócomo FR, Harada MJ, Mantovani R, Ohara CV
lowed by 5 to 9 years (32.1%), 1 to 4 years (28.2%), and younger than 1 year (6.1%).
In a retrospective study carried out in the mu-nicipality of Ribeirão Preto (2008) among children and adolescents, the group aged 15 to 19 years (37.1%) had the most accidents, followed by the groups aged 5 to 9 years (24.4%), 10 to 14 years (23%), 1 to 4 years (13.9%), and younger than 1 year (1.6%). Thus, we observed a concordance of results only in the less affected age range.(9)
In our study, falls were the most frequent type of accident (48.7%). Falls are the main mechanisms of trauma and are important because of variety of inju-ries that can cause small traumas and even death.(10)
Data from the VIVA/MS report in the region of Campinas in 2009 stated that most instances of care provided by an emergency service are falls, rep-resenting 35.8%.(11)
In relation to accidents caused by contact with an objects, the most affected age range was 10 to 13 years (40.0%), followed by 5 to 9 years (35.0%), from 1 to 5 years (23.8%), and younger than 1 year (1.3%). The predominance of adolescence affected by this type of accident can be related to adolescents’ desire for autonomy yet lack of dexterity, such as an inability to properly handle sharp objects, and their difficulty ascertaining risk.
The severity of accidents caused by swallowing a foreign body is related to the type of object, the location of the object in the body, and age of the child. When the object is located in the respiratory tract, such accidents are potentially severe, because of the risk of asphyxia. The younger the child, the lower the caliber of the airways, which increases the chance of total obstruction.
Accidents caused swallowing a foreign body oc-cur mainly in individuals aged 1 to 4 years (55.3%), followed by 5 to 9 years (33.3%), 10 to 13 years (9.6%), and younger than 1 year (1.8%). These data are similar to those found in a study in the municipality of São Luís (MA); predominance is 81.9% in the age range of 1 to 3 years.(12)
Animal bites occurred mainly among males (77.7%) and in the age range of 5 to 9 years (38.8%). This occurrence can be explained by the fact that boys may more frequently be permitted
greater liberty and often engage in more hostile games with animals, in addition to a lack of percep-tion of risk and lack of knowledge of aggressiveness of the animal.
Because of younger children’s small stature and less intense physical contact of child with an ani-mal, animal bites are more likely to affect the face and neck, thereby increasing the severity of this ac-cident. Results found in this study differ from data on admission for bites from dogs/other mammals in 2013 from DataSUS, in which the most affected age range was 1 to 4 years.(2)
Traffic accidents (being run over by a car) oc-cur with higher frequency in the population aged 10 to 13 years (47.9%), followed by 5 to 9 years (27.1%) and 1 to 4 years (25.0%). These data agree with research done in 2011, revealing that 28.6% of admissions for traffic accidents occurred in the age range of 15 to 19 years, 27.38% for 10 to 14 years, and 27.84% for 5 to 9 years.(13)
The fact that the most affected age range was 10 to 14 years can be related to the desire for au-tonomy, whereby children/adolescents will tend to walk alone on the street. It is important to high-light that presence of such factors as difficulty cal-culating time/velocity of a car and participating in race games with friends along busy avenues favor these accidents.
However, children younger than 10 years are vulnerable to being run over because of their own characteristics, such as difficulty precisely locating sounds and speed of vehicles, partial peripheral vi-sion, short stature, and distractible behavior. These characteristics, along with curiosity and difficulty making rapid decisions, make these children more vulnerable to this type of accident.(7,14)
We observed that poisoning occurred predom-inantly in the age range of 1 to 4 years (667.7%), agreeing with a retrospective study done in a Hos-pital in Maringá (PR) in 2008 among children and adolescents, which found that 78.5% of these events occurred in this age range.(15)
In 2007, another study carried out in the munic-ipality of São Paulo (SP) found that in this munic-ipality there was easy access to different substances, such as medications (79.8%) and cleaning materi-

292 Acta Paul Enferm. 2017; 30(3):287-94.
Profile of accidents in children and adolescents receiving care at a public hospital
als (86.1%). Storage was also seen as inadequate in 80% of cases.(16)
Culturally, society has been suffering a medical-ization process; consumption of medicine is expand-ing and medications are easily stored at home. For this reason, they present great risk. Another factor is that some adults, when administering medications to a child, erroneously tell the child the medicine “is yummy” to encourage the child’s acceptance ; this may lead a child to make this association upon see-ing a medication and therefore improperly ingest it.
Male sex was also more prominent in terms of environmental poisoning (72.7%). These data agree with those found in the literature, although the dif-ferences are lower. In 2011, the National System of Toxic-Pharmacological Information in Brazil re-corded 105,875 cases of environmental poisoning in the general population; 50.53% of cases were in men and 48.91% were in women.(17)
According to the report of the American Asso-ciation of Poisoning Control Center in 2012, a pre-dominance of boys younger than 13 years was ob-served, but in adolescents and adults, the majority were women.(18) Analysis of this statistic suggests in-tentionality of this poisoning. In a study published in 2005 that included adolescents who received care in the emergency unit with a diagnosis of suicide in Ribeirao Preto (SP), 77.8% of patients were wom-en; of these, 75% had swallowed medicines.(19)
Burns are other type of accident and are respon-sible for 0.9% of cases. In this study the occurrence of burns was low, and we believe this because burn patients are referred to another center for treatment.
Burns in our study affected those aged 1 to 4 years (50.05), followed by 10 to 14 years (27.3%) and 5 to 9 years (22.7%). This predominance is almost entirely related to free access to the home kitchen. Accidents occurred both for boiling liquids and contact with hot surfaces.
It is important to highlight in relation to burns that the younger the child, the greater the severi-ty, because burns can affect a large body surface in relation to weight; it may result in loss of liquid of intravascular tissue. In addition, because skin layers are thinner, it might worsen the clinical picture and can compromise prognosis.(7)
In children younger than 1 year, a number of ac-cidents occurred in the segment skull/neck (75.0%) (p<0.001). In this age range, the head dimensions are disproportionate to the other parts of the body, thereby facilitating injuries in this body segment.
However, for accidents that affect MMSS and MMII (above 30%), we observed a higher percent-age in this age range of 10 to 13 years. This result can also be seen in a study with children and ad-olescents aged 0 to 19 years who were assisted at emergency and urgent services, affecting MMSS (34.4%) followed by MMII (30.2%0 and lastly the face/head (17.9%).(20)
Procedures done in this study revealed that less than half of patients (52.7%) had to be assessed by a specialist; 67.6% and 10.5% underwent radiography and computed tomography, respectively. Almost one fourth of children who participated in the study had orthopedic splinting as the prescribed treatment.
A 2000 study on expenses of the Brazilian Pub-lic Health System with hospitalizations due to ex-ternal causes showed that most of expenses were due to natural causes. Although such patients stay for a shorter time in the hospital, costs rise, espe-cially because of the need for diagnostic procedures, such as imaging, and/or surgery.(21)
In our study, we observed that 10.5% of cases had as an endpoint hospitalization in the pediatric observation unit, 4.2% of patients were hospital-ized in a nurse ward, and 0.5% were hospitalized in the intensive care unit. Therefore, the analysis of procedures adopted and results suggests that ac-cidents have a high impact in terms of direct cost for medical/hospital care in Brazil; our study, how-ever, did not directly measure costs. Therefore, we observed that costs increase and overloading of the public sector with expenses should be avoided.
Of 11 children (0.5%) who needed intensive treatment and care, 36.3% had sustained a fall, 27.2% were run over, 18.1% had environmental poisoning, and 18.1% had experienced other acci-dents. However, more children who had swallow-ing or introduced a foreign body and were run over were hospitalized in the nurse ward or intensive care unit (over 14%), compared with those who experi-enced other accidents.

293Acta Paul Enferm. 2017; 30(3):287-94.
Filócomo FR, Harada MJ, Mantovani R, Ohara CV
Children younger than 1 year of age had lon-ger lengths of stay in the pediatric observation unit (38.6%) whereas more of those aged 10 to 13 years were discharged (90.2%).
Discharge was the most frequent outcome (84.0%), showing that accidents in childhood and adolescence were less complex and less severe in the study population, considering the solubility in medical consultation or receiving continuity of treatment in domestic environment. This fact can reduce the importance of sequelae possibility, there-fore compromising the phase of plan development.
Based on results found, we confirm that acci-dents are complex phenomena and must be ana-lyzed both individually by a search for occurrenc-es and facts related to each case and collectively in existing risk situations of each age range or even in specific groups.
Conclusion
Accidents had a high incidence in the studied mu-nicipality. Data enabled a greater understanding of risk factors, causes and consequences of accidents in children and adolescents contributing to imple-ment future actions and strategies to prevent these events. In addition, accidents had a great impact in the studied population and in the municipality health sector, including an increase in the number of instances of care, and consequently, costs, in ad-dition to incalculable emotional effects. It is import-ant to highlight that during the care of children and adolescents who have sustained an accidents, the professional should be attentive to the possibility of determining whether the injury was intentional or due to negligence. The nurse and other health pro-fessionals who work with children and adolescents should participate actively in accident preventions and also assign this problem the same priority level as other issues that involve the healthy development of this population.
CollaborationsFilócomo FRF, Harada MJCS, Mantovani R, Oha-ra CVS declare to contribute to elaboration of the
Project, data collection, analysis and interpretation of data, drafting the manuscript, they also contrib-uted to the content of the articles after its critical review, and approved the final version of the paper to be published.
References
1. Safe Kids (USA). [internet]. Raising safe kids: one stage at a time 2009; [cited 2014 Nov 20]. Available from: http://www.safekids.org/research-report/raising-safe-kids-one-stage-time-march-2009.
2. Brasil. Ministério da Saúde, Secretaria Executiva, Datasus. Mortalidade - óbitos por ocorrência segundo causa CID 10. Tabela. Brasília (DF): Ministério da Saúde; s.d. [citado 29 Nov 29]. Disponível em: http://www.tabnet.datasus.gov.br.
3. Brasil. Ministério da Saúde, Secretaria Executiva, Datasus. Morbidade hospitalar - Internações por ocorrência segundo causas externas. Tabela [Internet]. Brasília (DF): Ministério da Saúde; [citado 2015 Nov 29]. Disponível em: http://tabnet.datasus.gov.br/cgi/sih/eidescr.htm.
4. Brasil. Ministério da Saúde, Gabinete do Ministro. Portaria nº 737, de 16 de maio de 2001. Dispõe sobre a Política Nacional de Redução de Morbimortalidade por Acidentes e Violências. Diário Oficial da União: República Federativa do Brasil. 2001 Maio 18; Seção 1e: 2-28.
5. Blank D. Por que as crianças sofrem acidentes? In: Waksman RD, Gikas RM, Maciel W, organizadores. Crianças e adolescentes seguros. São Paulo: Sociedade Brasileira de Pediatria; 2005. p.24-30.
6. Brasil. Ministério da Saúde, Conselho Nacional de Saúde. Resolução nº466 de 12 de dezembro de 2012. Dispõe sobre as Diretrizes e Normas Regulamentadoras de Pesquisas envolvendo Seres Humanos. Diário Oficial da União: República Federativa do Brasil. 2013 Junho 13; Seção 1: 59-62.
7. Harada M de J, Pedreira MG, Viana DL. Injúrias físicas não intencionais na infância e adolescência. In: Promoção da Saúde: fundamentos e práticas. São Paulo: Yendis; 2012. p. 237-61.
8. Malta DC, Mascarenhas MD, Bernal RT, Viegas AP, Sá NN, Silva Junior JB. Acidentes e violência na infância: evidências do inquérito sobre atendimentos de emergência por causas externas - Brasil, 2009. Ciênc Saúde Coletiva. 2012; 17(9):2247-58.
9. Silva MA, Pan R, Melo L. Perfil dos atendimentos a crianças e adolescentes vítimas de causas externas de morbimortalidade. Rev Gaúcha Enferm. 2010 ; 31(2):351-8.
10. Carrera RM. Quedas. In: Waksman RD, Gikas RM, Blank D, organizadores. Crianças e adolescentes em segurança. Barueri (SP): Manole; 2014. p. 357-60.
11. Belon AP, Silveira NY, Barros MB, Baldo C, Silva MM. Atendimentos de emergência a vítimas de violências e acidentes: diferenças no perfil epidemiológico entre o setor público e o privado VIVA - Campinas/SP, 2009. Ciênc Saúde Coletiva. 2012; 17(9):2279-90.
12. Sousa ST, Ribeiro VS, Menezes Filho JM, Santos AM, Barbieri MA, Figueiredo Neto JA. Aspiração de corpo estranho por menores de 15 anos: experiência de um centro de referência do Brasil. J Bras Pneumol. 2009; 35(7):653-59.

294 Acta Paul Enferm. 2017; 30(3):287-94.
Profile of accidents in children and adolescents receiving care at a public hospital
13. Jorge MH, Martins, CB. A criança, o adolescente e o trânsito: algumas reflexões importantes. Rev Assoc Med Bras. 2013; 59(3):199-208.
14. Mascarenhas MD, Silva MM, Malta DC, Moura L, Gawryszewski UP, Costa VC, et al. Atendimentos de emergência por acidentes na Rede de Vigilância de Violência e Acidentes. Ciênc Saúde Coletiva. 2009; 14(5):1657-68.
15. Tavares EO, Buriola AA, Santos JA, Ballani TS, Oliveira ML. Fatores associados à intoxicação infantil. Esc Anna Nery. 2013; 17(1):31-7.
16. Waksman RD, Carrera RM, Santos E, Abramovici S, Schvartsman C. Morbidade por trauma em crianças moradoras da comunidade de Paraisópolis, São Paulo, Brasil. einstein (São Paulo). 2014; 12(1):1-5.
17. Brasil. Ministério da Saúde. Instituto de Comunicação e Informação Científica e Tecnológica em Saúde, Sistema Nacional de Informações Tóxico Farmacológicas. Casos registrados de intoxicação humana por agente tóxico e sexo. Tabela 8 [Internet]. Brasília (DF): Ministério da Saúde; 2003 [citado 2014 Nov 5]. Disponível em: http://www.fiocruz.br/sinitox/2003/tabela08.pdf.
18. Mowry JB, Spyker DA, Cantilena Jr LR, Bailey E, Ford M. 2012 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 30th Annual Report. Clin Toxicol (Phila). 2013; 51(10):949-1229.
19. Avanci RC, Pedrão LJ, Costa Junior ML. Perfil do adolescente que tenta suicídio em uma unidade de emergência. Rev Bras Enferm. 2005; 58(5):535-9.
20. Rocha MC. Características clínicas e epidemiológicas dos agravos por causas externas entre menores de 19 anos em serviço de atendimento de urgência de Barbacena [dissertação]. Belo Horizonte (MG): Universidade Federal de Minas Gerais; 2008.
21. Jorge MH, Koizumi MS. Gastos governamentais do SUS com internações hospitalares por causas externas. Rev Bras Epidemiol. 2004; 7(2):228-38.

295Acta Paul Enferm. 2017; 30(3):295-300.
Original Article
Care planning for patients receiving palliative care in an oncology intensive care unit
Planejamento da assistência ao paciente em cuidados paliativos na terapia intensiva oncológica
Débora Cristina Leitão dos Santos1
Marcelle Miranda da Silva2
Marléa Chagas Moreira2
Karen Gisela Moraes Zepeda3
Rafael Barroso Gaspar4
Corresponding authorMarcelle Miranda da SilvaAfonso Cavalcanti street, 275,20211-110, Rio de Janeiro, RJ, [email protected]
DOIhttp://dx.doi.org/10.1590/1982-0194201700045
1Instituto Nacional de Câncer José Alencar Gomes da Silva, Rio de Janeiro, RJ, Brazil.2Escola de Enfermagem Anna Nery, Universidade Federal do Rio de Janeiro, Rio de Janeiro, RJ, Brazil.3Instituto de Puericultura e Pediatria Martagão Gesteira, Universidade Federal do Rio de Janeiro, Rio de Janeiro, RJ, Brazil.4Hospital Universitário Clementino Fraga Filho, Universidade Federal do Rio de Janeiro, Rio de Janeiro, RJ, Brazil.Conflicts of interest: there are no conflicts of interest to declare.
AbstractObjective: To study the understanding of health professionals in relation to end-of-life patient care in an oncology intensive care unit, and discuss the objectives they seek to achieve when planning care from a palliative point of view.Methods: Descriptive study, with a qualitative approach, conducted in the adult ICU of a cancer hospital. Twenty-five professionals participated in the study: 12 nurses, eight physicians, two nutritionists and three physiotherapists. The inclusion criterion was: working in the sector for one year or more. Professionals on vacation or medical leave during the data collection, which took place between December 2015 and May 2016, were excluded. The data collection technique used was the semi-structured interview. Thematic content analysis was employed to analyze the data, in the following stages: preanalysis; exploration of the material or codification; treatment of the results, inference and interpretation.Results: The three categories encompass contextual particularities according to the severity of the cases, disease stages and treatments, end-of-life condition, medication and management difficulties. However, a need was noted to promote comfort, attend to families and invest in the integration of palliative and critical care.Conclusion: Care planning from a palliative perspective in this context is in the initial stages; challenges for putting it into practice are listed, with a concern to humanize care. It is suggested to use an interconsultive model for integration of specialties, through institutional characteristics.
ResumoObjetivo: Analisar o entendimento dos profissionais de saúde acerca da assistência ao paciente em cuidados ao fim da vida na unidade de terapia intensiva (UTI) oncológica, e discutir os objetivos que buscam alcançar ao planejar a assistência na perspectiva dos cuidados paliativos.Métodos: Estudo descritivo, com abordagem qualitativa, realizado na UTI adulto de um Hospital do Câncer. Participaram do estudo 25 profissionais: 12 enfermeiros, oito médicos, dois nutricionistas e três fisioterapeutas. Respeitou-se o critério de inclusão: estar atuando no setor por tempo maior ou igual a um ano. Foram excluídos profissionais de férias e de licença médica durante o período de coleta de dados, que transcorreu entre dezembro de 2015 a maio de 2016. A técnica de coleta de dados foi a entrevista semiestruturada. Para análise dos dados utilizou-se a análise de conteúdo temática, seguindo as etapas: pré-análise; exploração do material ou codificação; tratamento dos resultados, inferência e interpretação.Resultados: As três categorias abrangem particularidades contextuais pela gravidade dos casos, fases da doença e tratamentos, terminalidade da vida, medicalização e dificuldades gerenciais. Entretanto, evidenciou-se a necessidade de promover conforto, atender a família, e investir na integração dos cuidados paliativos e críticos.Conclusão: O planejamento assistencial na perspectiva dos cuidados paliativos no contexto é incipiente; elencam-se desafios para a prática e preocupa-se em humanizar a assistência. Sugere-se o modelo interconsultivo para integração das especialidades, mediante características institucionais.
KeywordsPalliative care; Intensive care units;
Patient care; Oncology
DescritoresCuidados paliativos; Unidades de terapia intensiva; Assistência ao
paciente; Oncologia
Submitted April 11, 2017
Accepted June 26, 2017

296 Acta Paul Enferm. 2017; 30(3):295-300.
Care planning for patients receiving palliative care in an oncology intensive care unit
Introduction
Technological and scientific advances, as well as public policies, have contributed to the early diag-nosis and treatment of cancer, but they are unable to reduce its incidence and, consequently, its im-pact on the health conditions of the Brazilian and world population. Given this reality, cancer mor-tality rates are high and death largely takes place in hospitals, particularly intensive care units.(1,2)
Although health professionals undergo situa-tions permeated with risk and uncertainty, tied to the dialogue of life and death, palliative measures in this regard are essential. This is especially the case in ICUs where death assumes its pathological nature, to the detriment of the natural inclination of the unit in favor of life, in that the evolution of science and the collective and political consciousness have been focused on fighting against death.(2)
The conflict between critical care and pallia-tive care occurs against the backdrop of this para-digm, especially when dealing with death processes in end-of-life care that require decisions regarding therapeutic limits. Although the characteristics of cancer can facilitate its prognosis based on the pro-gressive decline in the patient’s clinical conditions during this final stage of life, insistence on thera-peutic intervention is not uncommon in ICUs.
Therefore, planning end-of-life care for ICU patients can be complex, conflictive and challeng-ing, presenting ethical dilemmas that initially raise questions regarding the definition of reversibility or not, followed by various decisions, such as whether to invest in treatment or not, feed or not, or even, indicate or not ICU admission.(2-7)
Consequently, this study sought to explore the understanding of health professionals in relation to end-of-life care for patients in an oncology ICU, as well as discuss the objectives to be achieved in planning care from a palliative point of view.
Methods
This descriptive qualitative study was conducted in the adult ICU of Cancer Hospital 1 of the José
Alencar Gomes da Silva National Cancer Institute (INCA), located in the city of Rio de Janeiro, Bra-zil. This sector has 19 beds: ten for clinical oncology and nine for surgical oncology.
Twenty-five professionals participated in the study: 12 nurses, eight physicians, two nutritionists and three physiotherapists. The inclusion criterion was: having worked in the sector for one year or more. Professionals on vacation or medical leave during the data collection period, which took place between De-cember 2015 and May 2016, were excluded.
The data collection technique employed was the semi-structured interview, based on the following script: What is your understanding of end-of-life care for patients in the oncology ICU? Have you ever provided this type of care in this unit? If so, what was it like? If not, what do you think it would be like? How did (would) you plan your actions? Did (would) you have difficulties? What objective did (would) you seek to achieve when planning the care for this type of patient? How did the care team participate in this situation? In your work, do you adopt palliative care concepts? How was your rela-tionship with the family members? Do you feel you could provide better care for these patients? In what way? What would you need?
The interviews were conducted individually, at a prescheduled location, date and time, according to the participants’ preferences. Each interview lasted an average of 30 minutes. All the testimonies were recorded in audio and fully transcribed, identified by alphanumeric codes. After this stage, the partici-pants were revisited on the field in order to validate their testimonies.
Thematic content analysis was used to analyze the data, in the following stages: preanalysis; explo-ration of the material or codification; treatment of the results, inference and interpretation.(8) The last stage was based on national and international con-ceptual frameworks related to palliative care, ICUs and the best scientific evidence.
The study obtained approval from the Re-search Ethics Committee of the Anna Nery School of Nursing, as the applicant institution (Opinion No.1.275.38), and INCA, as a coparticipant insti-tution (Opinion No. 1.324.491).

297Acta Paul Enferm. 2017; 30(3):295-300.
Santos DC, Silva MM, Moreira MC, Zepeda KG, Gaspar RB
Results
Three categories emerged, as presented in chart 1.
Discussion
Discussing palliative care in ICUs can be paradoxical, in that the practices seem incompatible, since end-of-life patients may not benefit from the technologies available in this unit, due to the irreversibility of the disease, which is manifested in multiple spheres of the human being and presages death. Nevertheless, end-of-life patients are often in ICUs, receiving care intended to reverse the clinical situation and that seeks to harness technological advances to relieve suffering and provide comfort, which distinguishes therapeutic (dis)proportionality.
The process of caring for ICU patients from a palliative point of view is multifaceted, wrought with contradictions, negative feelings and little hu-manized care. Coping with death is also challeng-ing, since there are ethical and paradigmatic dilem-mas, in that health professionals are educated and trained based on a model that prioritizes disease and cure.(4)
Furthermore, death awakens in profession-als an awareness of their own finiteness, creat-ing internal conflicts and doubts about the ef-fectiveness, objectives and relevance of the care provided. Decision-making processes, primarily focused on a single person, especially generate questions regarding the ability to reverse the situation, resulting in insistence on therapeutic measures.(9)
Chart 1. Inferences, empirical categories and the testimonies of the professionalsCategory 1. Particularities of the adult oncology ICU and its relationship with palliative care and medication
Witness Inferences
“I’ve worked in other ICUs and there is a comparison of end-of-life expectancy in each one. In oncology, it is clear because the patient is admitted and palliative care starts immediately” (Nursing P24).“This is not an ICU whose mortality rate is due to inadequate care, but because patients arrive here already in a critical state, making us an ICU that provides end-of-life care [...]” (Physiotherapy P6).
High complexity of the profile of patients, related to rapid evolution of the disease, aggressive treatment and high mortality.
“It is difficult to define patients where there is no hope of recovery. I imagine due to lack of knowledge and difficulty in assuming risk [...]” (Physiotherapy P12).
Lack of knowledge on the subject. Delay in establishing the prognosis. Concerns about ethical and legal repercussions.
“I think we have more end-of-life than intensive care patients in our sector, two for every one, so either we need to rethink which patients come here or receive more information about palliative care” (Nursing P25).
Predominance of patients receiving end-of-life in the oncology ICU. Need to screen each case to facilitate appropriate indication of critical care, as well as for ongoing education.
“We are highly limited to few types of care; the truth is we do the basics, which is to alleviate pain. We could provide more comprehensive support or perhaps offer palliative care much earlier. After the person is intubated, then sedated, I think morphine and palliative care could be started [...]” (Medicine P18).
Medication as the main approach for relieving symptoms. Insistence on therapeutic intervention and undermining the patient’s autonomy. Need for early integration of critical and palliative care.
Category 2. Promoting the patient’s comfort in end-of-life care in the oncology ICU
Witness Inferences
“The dedication of professionals must remain the same; what changes is the care focus, which shifts more to treating symptoms [...]” (Medicine P8).
Promotion of comfort as a care planning goal. Focus on physical symptoms.
“[...] maintain physical integrity, respect for the body, for the life therein, for the family coming to see the patient, who wants, as much as possible, to see the patient, as being presentable and looking cared for [...]” (Nursing P10).
Respect for the body. Sensitivity in caring for the family’s needs, ensuring the person’s dignity, seeking to provide care based on a clean and comfortable appearance.
“Do not perform any procedure, any invasive testing, nothing that requires transportation, nor create any type of discomfort such as glycemic monitoring or finger insertion, try to leave the patient properly hooked up, which is what you have here, mechanical ventilation, do not treat hypotension, let things flow according to the natural course of the disease” (Medicine P22).
Minimize futile therapy to promote comfort, while at the same time employing technological resources to prolong life, which is contradictory.
Category 3. Limits and challenges in planning end-of-life care for patients in the oncology ICU
Witness Inferences
“Palliative care does not go with intensive care. Patients are cared for because they occupy a bed, but there is no direct relationship with the activities of this unit [...]” (Medicine P20).“[...] A patient with no hope of recovery occupies a place that could be for a patient that has possibilities. I think that such palliative care patients could have better quality of life staying with their family rather than coming to the ICU, being subjected to invasive and unnecessary procedures [...]” (Nursing P1).
Incompatibility between critical and palliative care. Inappropriate indication of intensive care. Patients with no reasonable expectation of recovery should not be admitted to the ICU, since they will not benefit from it.
“The objective is usually determined by the person who will provide the treatment, i.e., the physician. So, if the situation is defined by the physician as without hope, or if he or she is unable to establish this... we get mixed up in our objectives as well [...]” (Physiotherapy P12).
Decision-making limited to the physician. Difficulty working as a team and communicating.
“It’s tiring to look after a patient where nothing has been established, since one day you have to do everything and then the next day you undo it all. This is not good from a technical perspective and even worse emotionally [...]” (Nursing P25).
Professionals are not prepared to deal with patients in the process of dying or with death. Shortcomings in professional training. Indicates the needs for emotional support.
“If a critical patient is always ill in the ICU, regardless of what led to the deterioration, it represents an undue occupation of beds. We act according to the need; this results in pressure, even if disguised; there is no specific place for patients without hope of recovery [...]” (Medicine P20).
Need to establish palliative care nursing. Complex ethical questions that may involve legal decisions and institutional policy.

298 Acta Paul Enferm. 2017; 30(3):295-300.
Care planning for patients receiving palliative care in an oncology intensive care unit
This study examined end-of-life care in an ICU, from the perspective of the specialty of oncology. Despite the evolutive characteristics of cancer, they facilitate to a certain extent the survival prognosis and forecast compared to other chronic diseases that develop slowly. The difficulties expressed through-out the testimonies were similar to the context of a general ICU.
When dealing with cancer patients, it is un-derstood that their clinical condition is affected by variables related to the disease itself and the treat-ments, which has a negative impact on quality of life, particularly if they are manifesting physical symptoms and undergoing anticancer treatments, even for palliative purposes.(9) Such manifestations, when acutely exacerbated, can require ICU admis-sion. Care planning, from that point on, should fo-cus on stabilizing and improving such causes that, on the other hand, may be resistant to treatment, in addition to treating new infections that often arise from being hospitalized. Ultimately, there may be no therapeutic possibilities of recovery.
The transition from curative to palliative care in oncology ICUs is a frequent occurrence and does not mean, in some cases, that the indication of in-tensive care was incorrect. When this happens, it is important to recognize therapeutic limits and manage the situation based on principles that gov-ern human care, bioethics and palliation. Howev-er, since during the first hours of hospitalization, expectations of good results may run high among professionals and family members, it is difficult to accept the situation and make this transition.(10)
Ethical dilemmas and conflicts mainly stem from lack of alignment with palliative care principles, as per the recommendations of the World Health Organization, when dealing with life-threatening chronic diseases and the need to implement palliative measures from the time of di-agnosis, although the usefulness of these is much clearer and more evident as the disease progresses and reaches high levels of suffering, where medi-cine can no longer work against the disease, but in favor of the person.(11-14)
The need for early integration of curative and palliative care in ICUs has been addressed in the
literature. Among the various strategies to promote this practice, there is unanimous agreement about ongoing investment in health professionals, since, regardless of the model to be followed, they will have the means to recognize patients in need of pal-liative care, make a better diagnosis and even screen those eligible or not for intensive care.(15-17)
In light of these difficulties, it should be em-phasized that, according to the recommendations of the Federal Council of Medicine, contained in Resolution No. 2156/2016, which establishes ICU admission and discharge criteria, this service is in-tended for patients with critical clinical and risk conditions, but who are likely to survive and recov-er. This Resolution also stipulates that physicians, in cases of incurable and terminal diseases, provide palliative care rather than insist on useless diagnos-tic or therapeutic actions. Therefore, in Article 6, ICU admission must comply with specific criteria, ordered in priority from one to five. The last prior-ity, i.e., the fifth, applies to patients with character-istics where there are no therapeutic possibilities of recovery.
Different care options must be considered for end-of-life patients in the hospital context. Howev-er, over the course of this process, the current view does not exclude this profile of patient from the ICU, where it is urgent to provide palliative care whenever necessary.
Based on the scientific evidence and the study of the reality investigated, the consultive model is suggested as the most appropriate for implementing palliative care in the ICU, in view of the fact the institution has a specialized unit in palliative care, as well as specialized human capital. With this mod-el, a specialized team can be mobilized through an agreement among professionals from different cat-egories, and when working jointly with emergency teams, it can play an essential role in the process for screening patients, as well as promptly assist with possible indications for ICU admission and end-of-life decision-making.(10,17) However, medium and long-term strategies can be considered and imple-mented concomitantly, in order to invest continual-ly in the integration between curative and palliative care in the ICU. This integration is associated with

299Acta Paul Enferm. 2017; 30(3):295-300.
Santos DC, Silva MM, Moreira MC, Zepeda KG, Gaspar RB
better flow in clinical management and hospital discharge processes, with a significant reduction in readmissions, fewer referrals to the ICU, lower costs and greater quality of care.
Among the contradictions and problems in implementing an integration model based on con-sulting with a palliative care specialist, many health professionals may consider this type of intervention unnecessary, since they consider comfort measures to be common in their area of work and, for this reason, palliative care ends up not being recognized as a specialty.
Another measure that could facilitate care planning in this context is shared decision mak-ing, based on open and honest discussions regard-ing reasonable treatment options. This implies clear and constant communication, aimed at es-tablishing a relationship of trust, especially with family members. Faulty communication raises false hopes of recovery, resulting in the refusal to accept therapeutic limits and triggering processes of pathological grief.(18)
Prognostication is a challenge, accompanied by dilemmas in various domains, such as technical, eth-ical and legal. Insufficient knowledge and/or lack of interest in palliative care, reluctance to accept that it is no longer possible to keep seeking for a cure and the feeling of impotence in the face of inevitable death are issues that influence decision making, re-sulting in undue occupation of beds, overcrowding, futile or useless treatment and misuse of financial resources in the ICU.(6)
Concerns about ethical and legal repercussions related to decision making, especially medical, in-terfere with the implementation of palliative care. Care planning and decision making are complex stages in this process, given the difficulty of reach-ing a consensus and defining which types of care should be continued and which ones suspended, or even, not implemented, which leads to the need for specific protocols.(19-21)
A limitation of this study was the time restraints of professionals for the interviews, which in some cases were interrupted, interfering with the flow and development of ideas. Also, since this research was conducted in one single location, future studies in
regard to other specialties, other integration models between critical and palliative care, or that enable care protocols are essential for delving deeper into issues related to end-of-life in intensive care units.
Conclusion
Although professionals recognized the importance of palliative care, their understanding of it was weak, associating such care only with patients clearly in the final stages of life. There was no apparent con-cern to provide palliative care in the continuation of care after discharge from the ICU, for example. The emphasis was on physical care. In addition, difficul-ties related to screening, prognosticating and recog-nizing patients in need of palliative care, sharing de-cision making among team members and planning comprehensive care, combined with fears of ethical and legal repercussions, especially for physicians, were negative intervening factors for providing pal-liative care in the oncology ICU. Also worth not-ing was the lack of training of professionals on the subject, insufficient communication between teams and with family members, and divergent opinions in relation to therapeutic approaches.
CollaborationsSantos DCL, Silva MM, Moreira MC, Zepeda KGM and Gaspar RB contributed toward concep-tion and design, data analysis and interpretation, writing of the article, relevant critical review of its intellectual content and final approval of the ver-sion for publication.
References
1. Burlá C, Py L. [Palliative care: science and protection at the end of life]. Cad Saúde Pública. 2014; 30(6):1139-41. Portuguese.
2. Pessini L. [Life and death in the ICU: ethics on the razor’s edge]. Rev Bioét. 2016;24 (1):54-63. Portuguese.
3. Silva RS, Pereira A, Mussi FC. [Comfort for a good death: perspective nursing staff’s of intensive care]. Esc Anna Nery. 2015; 19(1):40-6. Portuguese.
4. Alcantara LS, Sant’Anna JL, Souza MG. [Illness and finitude: considerations about the interdisciplinary approach in the oncological Intensive Care Unit]. Ciênc Saúde Coletiva. 2013; 18(9):2507-14. Portuguese.

300 Acta Paul Enferm. 2017; 30(3):295-300.
Care planning for patients receiving palliative care in an oncology intensive care unit
5. Silva CF, Souza DM, Pedreira LC, Santos MR, Faustino TN. [Perceptions of the multi-professional team on the implementation of palliative care in intensive care units]. Ciênc Saúde Coletiva. 2013; 18(9):2597-604. Portuguese.
6. Baruzzi AC, Ikeoka DT. [End of life and palliative care in intensive care]. Rev Assoc Med Bras. 2013; 59(6):528-30. Portuguese.
7. Morin E. O homem e a morte. 3a ed. Rio de Janeiro:Imago; 1997.
8. Bardin L. Análise de conteúdo. Lisboa, Portugal: LTDA; 2011.
9. Picanço CM, Sadigursky D. [Nurses’ view on artificial extension of life]. Rev Enferm UERJ. 2014; 22(5):668-73. Portuguese.
10. Coombs MA, Addington-Hall J, Long-Sutehall T. Challenges in transition from intervention to end of life care in intensive care: a qualitative study. Int J Nurs Stud. 2012; 49(5):519-27.
11. Sawada NO, Nicolussi AC, Paula JM, Garcia-Caro MP, Marti-Garcia C, Cruz-Quintana F. [Quality of life of Brazilian and Spanish cancer patients undergoing chemotherapy: an integrative literature review]. Rev Lat Am Enfermagem. 2016; 24:e2688. Portuguese.
12. Kostakou E, Rovina N, Kyriakopoulou M, Koulouris NG, Koutsoukou A. Critically ill cancer patient in intensive care unit: Issues that arise. J Crit Care. 2014; 29(5):817-22.
13. Torres VB, Soares M. [Patients with hematological malignancies admitted to intensive care units: new challenges for the intensivist]. Rev Bras Ter Intensiva. 2015; 27(3):193-5. Portuguese.
14. Arantes AC. A morte é um dia que vale a pena viver. Rio de Janeiro: Casa da Palavra; 2016.
15. Baker M, Luce J, Bosslet GT. Integration of palliative care services in the Intensive Care Unit: a roadmap for overcoming barriers. Clin Chest Med. 2015; 36(3):441-8.
16. Aslakson RA, Curtis JR, Nelson JE. The changing role of palliative care in the ICU. Crit Care Med. 2014; 42(11):2418-28.
17. Walker KA, Mayo RL, Camire LM, Kearney CD. Effectiveness of integration of palliative medicine specialist services into the intensive care unit of a community teaching hospital. J Palliat Med. 2013; 16(10):1237-41.
18. Pattison N, O’Gara G, Wigmore T. Negotiating transitions: involvement of critical care outreach teams in end-of-life decision making. Am J Crit Care. 2015; 24(3):232-40.
19. Mendonça AC, Moreira MC, Carvalho V. [Cancer palliative care in an intensive care unit: a scientific production study of nursing]. Esc Anna Nery. 2012; 16(4):817-23. Portuguese.
20. Vicensi MC. Reflection on death and dying in the ICU from a professional perspective in intensive care. Rev Bioet. 2016; 24(1):64-72. Portuguese.
21. Santos EC, Oliveira IC, Feijão AR. [Validation of a Nursing care protocol for patients undergoing Palliative care. Acta Paul Enferm. 2016; 29(4):363-73. Portuguese.

301Acta Paul Enferm. 2017; 30(3):301-7.
Original Article
Difficulties of living with HIV/Aids: Obstacles to quality of life
Dificuldades do viver com HIV/Aids: Entraves na qualidade de vidaGiselle Juliana de Jesus1
Layze Braz de Oliveira1
Juliano de Souza Caliari1
Artur Acelino Francisco Luz Queiroz1
Elucir Gir1
Renata Karina Reis1
Corresponding authorGiselle Juliana de JesusBandeirantes Avenue, 3900,14040-902, Campus Universitário, Ribeirão Preto, SP, [email protected]
DOIhttp://dx.doi.org/10.1590/1982-0194201700046
1Escola de Enfermagem de Ribeirão Preto, Universidade de São Paulo, Ribeirão Preto, SP, Brazil.Conflicts of interest: there are no conflicts of interest.
AbstractObjective: To identify and explore the dimensions of the difficulties faced by people living with HIV/Aids in the disease management.Methods: A qualitative, descriptive, exploratory study was developed in Specialized Care Services, with 26 patients. The recorded interviews were transcribed, and then processed and analyzed by means of descending hierarchical classification. Findings were based on the collective subject discourse.Results: Five classes were obtained: “Intrafamilial prejudice and its impact on coping with the disease”; “Social prejudice: macro environment impacts”; “Difficulties in managing the risk of HIV/Aids transmission and its implications on partnerships”, “Maintenance of high rates of HIV/Aids treatment adherence: qualifying the service” and “Quality of life promotion for people living with HIV/Aids”.Conclusion: The difficulties experienced go far beyond the disease, with central, intimate aspects, and are linked to prejudice, which hinders their personal, professional and affective development, expanding into abstract macro-concepts such as quality of life.
ResumoObjetivo: Identificar e explorar as dimensões das dificuldades enfrentadas por Pessoas Vivendo com HIV/Aids no manejo da doença.Métodos: Estudo descritivo, exploratório, de abordagem qualitativa desenvolvido em Serviços de Atendimento Especializado, com 26 pacientes. As entrevistas gravadas foram transcritas e posteriormente, processadas analisadas pela Classificação Hierárquica Descendente. Os achados foram fundamentados no Discurso do Sujeito Coletivo.Resultados: Obteve-se cinco classes: “O preconceito intrafamiliar e seu impacto no enfrentamento da doença”; “Preconceito social: os impactos do macroambiente”; “As dificuldades em gerenciar o risco de transmissão do HIV/Aids e as implicações em parcerias”, “A manutenção de altas taxas de adesão ao tratamento do HIV/Aids: qualificando o serviço” e “ Promovendo a qualidade de vida em pessoas vivendo com HIV/Aids”.Conclusão: As dificuldades experienciadas vão muito além da doença, tomando aspectos íntimos, centrais ligadas ao preconceito, que impede seu desenvolvimento pessoal, profissional e afetivo expandindo-se a macro-conceitos abstratos como qualidade de vida.
KeywordsHIV; Acquired immunodeficiency
syndrome; Quality of life; Patient care; Adaptation, psychological
DescritoresHIV; Síndrome de imunodeficiência
adquirida; Qualidade de vida; Assistência ao paciente; Enfrentamento
Submitted April 12, 2017
Accepted June 19, 2017

302 Acta Paul Enferm. 2017; 30(3):301-7.
Difficulties of living with HIV/Aids: Obstacles to quality of life
Introduction
In Brazil, up to 2015, 830,000 cases of people liv-ing with HIV infection (PLWHA) were recorded, a finding that places the country in a prominent position for the pandemic in Latin America, be-ing the only one that still showed an increase in the number of new infections in the last decade, of about 11%.(1)
With the therapeutic advances and the intro-duction of new classes of antiretrovirals in the last decades, the context of this infection pro-gresses from fatal disease to a chronic condition. However, this improvement in treatment is pre-sented as a challenge for patients and healthcare professionals who, in this new context of chro-nicity, should face HIV infection not as a death sentence, but as a potential obstacle to their quality of life. The measurement of this con-struct in PLWHA provides information on the aspects that permeate this problem, and reveal the interfaces of living with HIV/AIDS in the current context.(2)
People living with HIV face several difficul-ties when they try to achieve a satisfactory quali-ty of life, from interruptions of their life history; disruption of interpersonal and occupational re-lationships, which can lead to social isolation; to problems with sexuality and social relationships, which can compromise their mental and physi-cal health. Adapting to these changes can some-times be challenging, requiring an approach that reconciles the particularities related to HIV, and the subject’s perception in his/her biopsychoso-cial context.(3)
Currently, living with HIV requires more than only treating the disease, because PLWHA daily have to deal with transdisciplinary prob-lems involving depression symptoms, stigma, discrimination, and adverse effects related to the therapy regimen.(4)
Based on these problems, the objective of this study was to identify and explore the dimensions of the difficulties faced by people living with HIV/Aids in the management of the disease.
Methods
This was a descriptive, exploratory study with a qualitative approach based on the collective subject discourse method, in which the speeches (empirical data of a verbal nature) are organized and tabulated though key expressions that allow the identification of the central ideas, so that collective thinking can be apprehended and grouped into categories.(5)
The subjects participating in the study were PLWHA, followed in two HIV/Aids Specialized Care Services (SAE, as per its acronym in Portu-guese) of a large city in the Northwest region of the state of São Paulo, Brazil. The participants were cho-sen through convenience sampling, provided that they met the pre-defined criteria: awareness of the HIV seropositivity, age greater than or equal to 18 years, and to be clinically followed as an outpatient in the services chosen. Institutionalized patients or those living in support houses were excluded.
The convenience sample consisted of 26 PLWHA. Data were collected from May to August 2015, using data saturation as the criterion for com-pleting the collection. To begin the collection, there was a previous contact with the institution, and the participants were invited to integrate the research while they were in the waiting room, waiting for consultations with healthcare professionals.
Data were collected through semi-structured in-terviews, in a reserved room of the institution. The interviews were guided by a script, previously vali-dated by experts, with two guiding questions about the difficulties of living with HIV/Aids and their relation with quality of life, with an average dura-tion of 40 minutes. The statements were recorded and fully transcribed for analysis.
For data processing, the lexical type analysis technique was used, with the help of the software IRaMuTeQ (Interface de R pour les Analyses Multi-dimensionnelles de Textes et de Questionnaires).(6) A p value of 0.05 was adopted; thus, for every p ≤ 0.05, the test is considered significant, and the word is considered pertaining to the class determined in the software. The same has been emphasized in studies using a qualitative approach, by the use of

303Acta Paul Enferm. 2017; 30(3):301-7.
Jesus GJ, Oliveira LB, Caliari JS, Queiroz AA, Gir E, Reis RK
statistical techniques to help researchers grasp the social construct, and create classes of analysis based on the apprehension and identification of units of meaning.(7,8) It is noteworthy that the use of the software is not an absolute data analysis method, but a procedural tool that facilitates and helps in-terpret the findings.(9)
For the textual analysis, the descending hi-erarchical classification (DHC) method was de-fined, in which the texts are classified according to their respective words and their set is divided by the frequency of the reduced forms.(10) Thus, classes of text segments were obtained, which were called “pre-class”. Later, the organization of key expressions from the interviewed speeches, and the identification of central ideas comple-menting the DHC findings were performed, and allowed the delimitation of statements in definite classes.(8)
The recommendations for the development of studies with human beings were followed, with the project being approved by the Ethics Committee of the Ribeirão Preto College of Nursing (protocol no. 16740).
Results
The mean age of the 26 people living with HIV/Aids who participated in this study was 50 years, with 13 being male and 13 female. The mean time since diagnosis was 10 years, and 22 of them had a monthly income of one to two minimum wages, and education level of less than 8 years.
Regarding the statements, the software rec-ognized the corpus separation in 449 elementary context units (ECU), from 26 initial context units (ICU) with utilization of 85.75% of the initial cor-pus. Based on the DHC, the more relevant words present in the statements and their relationship with the research object were analyzed, to form the “pre-classes”. Then, based on the collective subject discourse method, the identification of “key expres-sions” was performed, and they were quantified to facilitate the identification of central ideas, which
allowed the creation of definite classes, as shown on the following dendrogram (Figure 1).
The arrangement of classes reveals that the ma-terial has been consecutively divided into three axes: the first one related to quality of life (class 5), the second linked to the importance of health services to the PLWHA’s quality of life (class 4), and the third encompassing the other classes (classes 1, 2 and 3), related to the various confrontations that these individuals experience on a daily basis. Each class was named according to the content it pres-ents, represented by the words, interpretation of its thematic convergence, and identification of the central idea associated with it as it appears in the dendrogram (Figure 1).
Class 1. Intrafamilial prejudice and its im-pact on coping with the diseaseThis class includes a large number of words, sug-gesting that the subjects know about the theme or, at least, have experience with it. The greatest diffi-culties faced by these subjects are in the intra-fam-ily environment, experiencing prejudice from close family members. In the statements, the key expressions, as well as the words, were condensed in the nucleus “family, children and friends”. This triad is considered by the participants as an im-portant support base, and when it is not present, it has greater negative repercussions that directly affect the process of living with the disease, mak-ing it more tiring.
Failure to recognize the importance of family members in the care for the member living with HIV suggests the lack of promising perspectives in living with HIV, because family support is essential for these patients, especially at early diagnosis, when they need support in recognizing the disease, and in the search for specialized care, encouragement for self-care, and emotional support.
Class 2. Social prejudice: macro environ-ment impactsThis class complements the previous one, because its contents transcend the difficulties and prejudices experienced in the family environment, extending them to the civil society. The lower concentration

304 Acta Paul Enferm. 2017; 30(3):301-7.
Difficulties of living with HIV/Aids: Obstacles to quality of life
of words in this class suggests that this object, al-though close to the participants, does not impact as much as the prejudice, or the intrafamilial stigma. Thus, the score given to prejudice and/or stigma against the disease in family life seems to be higher than in social life.
In the civil society, their experiences include stigmas and lack of information about the infec-tion, treatment and perspectives of care. Among these, lack of information directly affects the search by PLWHA for a better quality of life, because the HIV prognosis is not known before the beginning of the treatment, and indirectly, because its relations become permeated by prej-udice of people who see them as “contaminated” or “condemned”, limiting their social support. This isolation can be observed in the key expres-sions contained in this class, in which the partici-pants emphasize: “at work I do not tell anyone that I have HIV”.
Class 3. Difficulties in managing the risk of HIV transmission and its implications in partnershipsIn spite of complementing the previous class, the words belonging to these classes stood out for their more personal and intimate character, be-cause their contents address sexual partnerships and love relationships. This class highlights the fragility that permeates the affective and sexual in-timacy of people living with HIV/AIDS. The key expressions identified “I am alone; always alone; without anyone,” point towards feelings of isola-tion and loneliness.
Those experiencing a relationship report dif-ficulties in negotiating the use of condoms with the partner, with a resistance to its use by men and women being mentioned, which can indi-cate unprotected and high-risk sexual practices. The most mentioned words highlight problems in the affective-sexual life that can lead individ-
Note: ECU – Elementary Context Unit
Figure 1. Thematic structure about difficulties of living with HIV/Aids
Difficulties of living with HIV/Aids: Obstacles to quality of life
Class 1129 ECU* (33.51%)Intrafamilial prejudice and its impact on coping with the disease
Class 260 ECU* (15.58%)Social prejudice: macro environment impacts
Class 354 ECU* (14.03%)Difficulties in managing the risk of HIV/Aids transmission and its implications on partnerships
Class 484 ECU* (21.82%)Maintenance of high rates of HIV/Aids treatment adherence: qualifying the service
Class 558 ECU* (15.06%)Quality of life promotion for people living with HIV/Aids
Word X2 Word X2 Word X2 Word X2 Word X2
HIVFamilyPrejudicePersonPeople Difficulty Friend Right Same DiseaseGreater GroupSon DiscriminationWorse Place Income Former husbandProblem
24.323.921.221.017.316.614.713.211.710.99.38.78.28.06.36.06.06.05.3
Thing Life TelevisionSocietyGod Psychological NormalPreventionCauseAlone AidsSexBetter Husband InformationWorld TermPointLive
57.228.021.821.216.915.915.014.911.110.89.39.38.87.66.46.06.06.05.8
PartnerCondom Woman HourRiskUse_of_condomRelationshipMarried Bedroom Man Boyfriend Young Street NightBrother Fear Equal Sex
75.964.561.944.131.031.031.031.024.724.724.724.212.410.98.87.06.95.0
ExamBeginning MedicationDayMonthMedicationBlood TreatmentPhysician Tablet CD4Center OrganismResultAdverse effectHead Beginning Healthcare center PneumoniaIll person VirusHouse Low Calm
52.940.530.829.429.226.725.523.018.918.118.114.414.414.413.913.513.510.810.810.810.07.16.76.1
Food Adhesion groupPsychologist Health Booklet Quality of lifeImportancePhysical_exercisesHealthy foodPossible Orientation Help Meeting Good CareDepressionProcessImportantHealthcare_professionalsQualityHIV_carrierHealth_teamSubject
63.862.557.851.946.545.041.140.228.522.722.217.816.614.212.69.77.97.97.96.26.26.26.2

305Acta Paul Enferm. 2017; 30(3):301-7.
Jesus GJ, Oliveira LB, Caliari JS, Queiroz AA, Gir E, Reis RK
uals and their partners to physical, psychic and social damages.
Class 4. Maintenance of high rates of HIV/Aids treatment adherence: qualifying the serviceCategorized by the physical, social and psycho-logical changes and difficulties experienced by the interviewees during the stages of diagnosis and treatment of HIV infection, the most evoked words reveal the positive and negative influences coming mainly from drug treatment, interfering with their self-care and quality of life. This axis moves away from subjective and emotional con-tents, and is anchored in real objects about the therapeutic treatment of HIV.
The central ideas about adherence to treatment take over, in a symbolic and concrete way, as well as the difficulty in clinical follow-up, participation in the adherence group, number of tablets, and their adverse effects.
The success of highly active antiretroviral therapy for AIDS (HAART) depends on the maintenance of high rates of patient adherence to drug treatment. Analyzing how the factors associated with this adherence are perceived by PLWHA is crucial for the improvement of health policies and practices aimed at improving the treatment effectiveness.
Class 5. Quality of life promotion in peo-ple living with HIV/AidsThis class, as well as the contents that it entails, involves all the others and points out that despite advances in the treatment of HIV and the increase in life expectancy, the implementation of actions promoting quality of life still presents gaps. In the statements, the most evoked words refer to the need to build comprehensive care that meets the needs of people living with HIV/AIDS.
Quality of life is the central axis of this class, and its elements are varied and show a plurality of sub-items that can make up this construct, varying from concrete (food, physical exercises, and ad-herence group) to abstract representations (health, company, guidance and help).
Understanding this complexity is an increasing need of healthcare professionals, especially the nurs-ing team, due to their functions as caregivers and health educators; and also as creators and users of light technologies for interventions on PLWHA’s quality of life.
Discussion
The impact of living with a chronic disease that still carries a lot of stigma and prejudice is the greatest obstacle between these individuals and their quality of life, impacting their micro and macro environment, and directly interfering in their coping capacity. In an attempt to manage their quality of life, it was observed that PLWHA have different strategies to manage and confront the disease, depending on the environment, the degree of intimacy, or the importance of their rela-tionships, and their own capacity in this manage-ment, which make them assign different scores to different situations.
In the family environment, hiding the sero-logical status as a primary coping strategy was common. This is due to the search for social support in an attempt to keep family harmony, because families are afraid of acquiring the in-fection and losing their social prestige in their communities.(11)
Living with this stigma in such an intimate envi-ronment as the family impairs PLWHA social sup-port, reducing their emotional coping, and forcing them to search for coping strategies in extra-family environments. Family support is one of the most important forms of social support for people in situations of vulnerability, being an important pro-tective factor for the development of psychosocial disorders such as depressive symptoms and suicidal thoughts.(7,12)
When the family environment is insufficient, or unable to meet their demands, PLWHA sought support in society in general, represented here as a network of individuals and institutions that had no family relationship with the participants. The participants’ statements, and the way the words be-

306 Acta Paul Enferm. 2017; 30(3):301-7.
Difficulties of living with HIV/Aids: Obstacles to quality of life
haved in the classes, point to a situation of help-lessness, in which individuals do not have social or emotional support. This lack of support is associat-ed with more severe symptoms resulting from HIV infection, such as fatigue, malaise, numbness, and body changes (e.g. weight gain).(13)
This constant reassertion of placing them as sick and marginalized individuals, by their own families and/or society, affects self-esteem. This effect, asso-ciated with the internalization of stigma and preju-dice, can trigger a progressive isolation reaction, as a way to protect against future prejudice, culminating in negative psychological conditions such as anxiety and depression. Another characteristic of the study participants was being older (<50), which makes them more likely to have less social support and de-velop mental health problems.(12,14)
The perception by PLWHA of health services as an obstacle to their quality of life is an alarming finding. The constant procedures, considered rou-tine for professionals, become symbolic and repre-sentative images of the disease. It is not always that these professionals pay attention to the comorbid-ities accompanying the process of disease chronifi-cation and population aging, which leads PLWHA to take several medications and require various care specialties. The understanding by the professionals that these therapeutic and technical actions can re-inforce negative feelings in their patients corrobo-rates the importance of a humanized care, which is not impositive, but rather empowering.(15,16)
The configuration of health services and policies in Brazil focused on PLWHA allows for few changes that fit the specific needs of this population, and this involves changes in the therapy regimen, service time options, influence of socio-cultural factors that take the patient away from the service (in the case of the LGBT population), and bring losses in various aspects of their quality of life. European countries that have invested in this flexibility already show better rates of life expectancy and quality of life in PLWHA.(17-19)
Quality of life is a multidimensional variable, and can be affected by several aspects. In the present study, the several difficulties of coping are directly related to this variable. Thus, in addition to identi-
fying the main difficulties of living with HIV, it is necessary to implement interventions that support the development of coping strategies.(20)
The great focus of the health team on bio-medical processes and hard technologies is a problem that affects not only PLWHA but vir-tually all health settings today. The requirement for diagnosis, effectiveness of interventions and treatment through increasingly sophisticated techniques, and with more noticeable evidence (CD4 count, viral load or body mass index) be-come a demand of professionals and patients, who use the technological advances as the only therapeutic option, neglecting psychosocial problems. Therefore, more abstract constructs are underestimated, and become an even more difficult goal to achieve.(21)
The use of light technologies provides support for the development of educational processes in different population segments. These tools aim to increase the efficiency of information acquisi-tion in educational contexts; and the integration of this technology in teaching and learning has showed a positive impact on the affective and cog-nitive domains.(22)
Faced with the challenge and importance of the generation of technological innovations developed specifically for PLWHA, it is opportune to imple-ment actions that are based on such technologies for interventions in gaps related to coping.(22)
The limitations of this study are related to its cross-sectional design, which limits the comprehen-siveness of the results to the universe of the par-ticipants and their sample, consisting of only two health institutions. The expansion of research fields and participants could broaden the findings, deep-ening the issues addressed, and allowing the strati-fication by gender, age group or sexual orientation.
Conclusion
The difficulties faced by people living with HIV in-fection are presented throughout their statements as obstacles to a final objective: quality of life. The main difficulties cited are the prejudice experienced in the

307Acta Paul Enferm. 2017; 30(3):301-7.
Jesus GJ, Oliveira LB, Caliari JS, Queiroz AA, Gir E, Reis RK
family and in the social context; managing affective and sexual partnerships; managing treatment and quality of life achievement. The statements, their central nuclei, and key expressions point out that the experience of HIV/AIDS behaves as a spiral of barriers between people living with HIV infection and their quality of life. These barriers have personi-fications and concrete elements, which are based on prejudice and stigma as a common branch. These barriers are anchored in a network of “intimate and essential contacts”, among which family members seem to have a more negative impact, and cover other forms of social, intimate and affective-sexual support.
CollaborationsJesus GJ, Oliveira LB, Caliari JS, Queiroz AAFL, Gir E and Reis RK declare that they contributed to the project design, data analysis and interpretation, article writing, relevant critical review of its intel-lectual content, and final approval of the version to be published.
References
1. UNAIDS, Joint United Nations Program HIV/Aids. Global Report. UNAIDS The Gap Report. Geneva: Joint United Nations Program HIV/AIDS; 2016.
2. Syed IA, Sulaiman SA, Hassali MA, Lee CK. Adverse drug reactions and quality of life in HIV/AIDS patients: Advocacy on valuation and role of pharmacovigilance in developing countries. HIV & AIDS Rev. 2015; 14(1):28-30.
3. Macapagal KR, Ringer JM, Woller SE, Lysaker PH. Personal narratives, coping, and quality of life in persons living with HIV. JANAC. 2012; 23(4):361-8.
4. Oliveira FB, Queiroz AA, Sousa AL, Moura ME, Reis RK. Orientação sexual e qualidade de vida de pessoas vivendo com HIV/AIDS. Rev Bras Enferm. 2017; (70)3.
5. Lefèvre F, Lefèvre AM. O discurso do sujeito coletivo: um novo enfoque em pesquisa qualitativa; desdobramentos. São Paulo: EDUCS; 2005.
6. Ratinaud P, Marchand P. Application of the ALCESTE method to the large corpus and stabilised lexical worlds or ‘cablegate’, using IRAMUTEQ. Actes des 11eme JADT.2012;2012:835-44.Available from: http://lexicometrica.univ-paris3.fr/jadt/jadt2012/Communications/Ratinaud,%20Pierre%20et%20al.%20-%20Application%20de%20la%20methode%20Alceste.pdf.
7. Sousa AF, Queiroz AA, Oliveira LB, Moura ME, Batista OM, Andrade D. Social representations of biosecurity in nursing: occupational health and preventive care. Rev Bras Enferm. 2016; 69(5):864-71.
8. Sousa AF, Queiroz AA, Oliveira LB, Valle AR, Moura ME. Social representations of community-acquired infection by primary care professionals. Acta Paul Enferm. 2015; 28(5):454-9.
9. Rodrigues PS, Sousa AF, Magro MS, Andrade D, Hermann PR. Occupational acidentes among nursing professionals working in critical units of an emergency service. Esc Anna Nery. 2017; 21(2):e20170005.
10. Reinert M. Une methode de classification descendante hierarchique: application a l’analyse lexicale par contexte. Cahiers l’Analyse Donnees. 1983; 8(2):187-98.
11. Shrestha S., Poudel KC, Poudel-Tandukar K, Kobayashi J, Pandey BD, Yasuoka J, et al. Perceived Family Support and Depression among People Living with HIV/AIDS in the Kathmandu Valley, Nepal. J Int Assoc Provid AIDS Care. 2014; 13(3):214-22.
12. Amiya RM, Poudel KC, Poudel-Tandukar K, Pandey BD, Jimba M. Perceived family support, depression, and suicidal ideation among people living with HIV/AIDS: a cross-sectional study in the Kathmandu Valley, Nepal. PLOS One. 2014; 9:e90959.
13. Earnshaw VA, Lang SM, Lippitt M, Jin H, Chaudoir SR. HIV Stigma and physical health symptoms: do social support, adaptive coping, and/or identity centrality act as resilience resources? AIDS Behav. 2015; 19(1):41-9.
14. Oppong Asante K. Social support and the psychological wellbeing of people living with HIV/AIDS in Ghana. Afr J Psychiatry. Afr J Psychiatry. 2012; 15(5):340-5.
15. Paschoal EP, Espírito Santo CC, Gomes AM, Santos EI, Oliveira DC, Pontes AP. Adherence to antiretroviral therapy and its representations for people living with HIV/AIDS. Esc Anna Nery. 2014; 18(1):32-40.
16. Macêdo SM, Miranda KC, Silveira LC, Gomes AM. Nursing care in specialized HIV/Aids outpatient services. Rev Bras Enf. 2016; 69(3):515-2.
17. Seang S, Thibault V, Valantin MA, Katlama C. Adjustment of antiretroviral regimen may lead to HBV reactivation even in patients with past HBV infection serological profile. J Infect Chemother. 2013; 19(5):987-9.
18. Alencar GA, Lima CG, Quirino GS, Alves MJ, Belém JM, Figueiredo FW, et al. Access to health services by lesbian, gay, bisexual, and transgender persons: systematic literature review. BMC Int Health Hum Rights. 2016; 16:2.
19. Queiroz AA, Sousa AF, Araújo TM, Oliveira FB, Moura ME, Reis RK. a review of risk behaviors for hiv infection by men who have sex with men through geosocial networking phone Apps. J Assoc Nurses AIDS Care. 2017; S1055-3290.
20. Ferreira DC, Silva GA. Routes to care: the itineraries of people living with HIV. Ciênc Saúde Coletiva. 2012; 17(11): 3087-98.
21. Schwonke CR, Lunardi Filho WD, Lunardi VL, Santos SS, Barlem EL. Phylosophical perspectives about the use of tecnology in critical care nursing Rev Bras Enferm. 2011; 64(1):189-92.
22. Keser H, Özcan D. Current trends in educational technologies studies presented in World Conferences on Educational Sciences. Soc Behav Sci. 2011; 15:3989-98.

308 Acta Paul Enferm. 2017; 30(3):308-15.
Original Article
Factors related to leisure-time physical inactivity in obese womenFatores relacionados à inatividade física no lazer em mulheres obesasTaise Santos do Nascimento1
Fernanda Carneiro Mussi1
Cátia Suely Palmeira1
Carlos Antônio Teles Santos2
Melissa Almeida Santos1
Corresponding authorFernanda Carneiro Mussi.Dr. Augusto Viana Filho Avenue, SN, 40110-16, Campus Canela, Canela, BA, [email protected]
DOIhttp://dx.doi.org/10.1590/1982-0194201700047 1Escola de Enfermagem, Universidade Federal da Bahia, Salvador, Bahia, Brazil.
2Laboratório de Epidemiologia Molecular e Bioestatística no Centro de Pesquisas Gonçalo Moniz-FIOCRUZ/SSA, Salvador, Bahia, Brazil.Conflicts of interest: there are no conflicts of interest to declare.
AbstractObjective: To verify the factors related to leisure-time physical inactivity (PI) in overweight women.Methods: A cross-sectional study, part of a matrix project entitled, “Remote nurse monitoring of overweight women”, conducted in an outpatient reference clinic for obesity in Salvador, Bahia, Brazil, in which a multidisciplinary team and 300 patients, 91% women, of the Unified Health System, were selected for the study. A total of 174 women were recruited, according to inclusion criteria for the matrix project: overweight (BMI ≥ 25 kg/m²), more than 18 years of age, attended a medical visit in the last 12 months, and had a landline telephone and/or cell phone. Exclusion criteria were: lack of physical conditions for anthropometric measures, lack of cognitive ability to respond to research instruments, psychiatric disorders, use of medications for weight loss, and bariatric surgery. The International Physical Activity Questionnaire guidelines for data processing and analysis were followed.Results: A high prevalence of PI (85.2%) was identified, as well as a significant association between PI and body mass index, self-efficacy for physical activity, environment perception, dependents at home, perceived health status, and number of comorbidities. Regression analysis showed that PI was associated with the number of comorbidities RP:1.31; IC 95% 1.06; 1.64); poor self-perception of health (RP: 1.28, 1.01, 1.61); low self-efficacy (RP: 1.27, 1.06, 1.51); and poor environmental perception (RP: 1.27, 95% CI 1.01, 1.60).Conclusion: Leisure-time physical inactivity was associated with individual and environmental variables.
ResumoObjetivo: Verificar os fatores relacionados à inatividade física (IF) no lazer em mulheres com excesso de peso.Métodos: Estudo transversal, recorte de um projeto matriz denominado “Monitoramento remoto de enfermagem de mulheres com excesso de peso”, desenvolvido em ambulatório de referência para obesidade, em Salvador, Bahia, Brasil, no qual uma equipe multidisciplinar cerca de 300 usuários do Sistema Único de Saúde, sendo 91% mulheres, razão pela qual foram selecionadas para o estudo. Mediante consulta aos prontuários 174 mulheres foram recrutadas atendendo aos critérios de inclusão para o projeto matriz: ter excesso de peso (IMC ≥25 Kg/m²), idade superior a 18 anos, comparecido a consulta médica nos últimos doze meses e telefone fixo e/ou celular. Foram critérios de exclusão: ausência de condições físicas para medidas antropométricas e cognitivas para responder aos instrumentos da pesquisa, distúrbios psiquiátricos, uso de drogas para perda de peso e realização de cirurgia bariátrica. Obedeceu-se as orientações do processamento e de análise dos dados do IPAQ.Resultados: Houve alta prevalência de IF (85,2%) e associação significante entre IF e índice de massa corporal, autoeficácia para atividade física, percepção do ambiente, dependentes no domicílio, estado de saúde percebido e número de comorbidades. Na regressão, a IF associou-se ao número de comorbidades (RP:1,31; IC 95% 1,06;1,64); a autopercepção de saúde ruim (RP: 1,28; 1,01;1,61); a baixa autoeficácia (RP:1,27; 1,06; 1,51) e a percepção do ambiente ruim (RP:1,27; IC 95% 1,01;1,60).Conclusão: A IF no lazer associou-se a variáveis individuais e ambientais.
KeywordsExercise; Women; Sedentary lifestyle; Obesity
DescritoresExercício; Mulheres; Estilo de vida sedentário; Obesidade
Submitted April 21, 2017
Accepted June 30, 2017

309Acta Paul Enferm. 2017; 30(3):308-15.
Nascimento TS, Mussi FC, Palmeira CS, Santos CA, Santos MA
Introduction
Non-communicable and chronic diseases, such as obesity, are increasing significantly in developed and developing countries. The prevalence of over-weight in the Brazilian adult population, in 2015, was 53.9.5% (57.6% men and 50.8% women). This panorama is associated with the way of life of a modern society, which determines a food pattern that, associated with the sedentary lifestyle, is not favorable to the health of the population.(1)
Excess weight is a risk factor for cardiovascular diseases, endocrine and respiratory disorders, and some types of neoplasms, and is one of the risk factors for illness and death.(2) The increase in the prevalence of overweight is a public health problem, considering the impact of this condition on health and quality of life. Preventing and controlling this risk factor is a challenge, and calls for reflection on the causal factors.
The etiology of obesity is complex and multi-factorial, resulting from the interaction between genes, environment, lifestyle, physical activity prac-tices, and dietary pattern.(3) The more active one’s lifestyle, the lower the likelihood of that person be-coming obese.(4)
Although the benefits of physical activity in pro-moting and preventing health problems are known, more than two million annual deaths are attribut-ed to PI, due to its repercussion in the increase of non-communicable chronic diseases that, if current trends are maintained, will be related to 73% of the world’s deaths by 2020.(2) The last survey of the Bra-zilian Ministry of Health, in 2015, showed that the prevalence of PI remains high, reaching 47.5% of the population in 2015.(5)
Several researchers have sought to understand how physical activity can be influenced and how to motivate the population. Sociodemographic char-acteristics, such as sex, age, education, occupation and marital status, appear to be determining factors for a sedentary lifestyle. In addition, other variables, such as self-efficacy and environmental factors, ap-pear to be associated.(6,7)
However, despite the advances in the state of the art on factors involved in PI, gaps in the literature
regarding individual and environmental factors that affect women remain, particularly overweight and obesity. Most studies available were conducted in developed countries.(8,9)
Considering the importance of regular physical activity in the collective, and a healthy lifestyle for controlling body weight and prevention of chron-ic non-communicable diseases, the knowledge about the epidemiological pattern of this practice must be mastered, and sub-groups of individuals monitored. This knowledge can guide health and nursing care practices, as well as public policies to support the practice of physical activity and con-trolling of body weight through integrated and in-terrelated actions of health professionals and the community at large.
On the basis of the above, the objective of this study was to verify the factors associated with lei-sure-time PI in obese women.
Methods
This was a cross-sectional study, which was one portion of a matrix project entitled, “Remote nurse monitoring of overweight women”, con-ducted in a outpatient reference clinic for obesity in Salvador, Bahia, Brazil, in which a multidisci-plinary team and about 300 patients of the Unified Health System, 91% of whom were women, were se-lected for the study.
A total of 174 women were recruited, accord-ing to the inclusion criteria for the matrix project: overweight (BMI ≥ 25 kg/m²), more than 18 years of age, attended a medical visit in the last twelve months, and who had a landline telephone and/or cell phone. The exclusion criteria were: absence of physical conditions for anthropometric measures, cognitive inability to respond the research instru-ments, psychiatric disorders, use of medications for weight loss, and bariatric surgery.
Eligible women were consulted by telephone about their interest in participating in the survey, and were invited to the office on a scheduled date. At that occasion, the objectives and procedures of the research were clarified, and the Terms of Free

310 Acta Paul Enferm. 2017; 30(3):308-15.
Factors related to leisure-time physical inactivity in obese women
and Informed Consent Form was signed. After re-ceiving consent, the interview and anthropometric evaluation began in a private room.
Body weight was verified using a digital scale, TEC 30-Techline® model, with a variation of 0.1 kg; stature was measured using a portable stadiometer, according to the procedures specified in the litera-ture.(10) The body mass index was obtained by tak-ing the weight, in kilograms, divided by the square of the height, in meters. The following classification was adopted: overweight (25 to 29.9kg/m²); Class I obesity (30 to 34.9kg/m²); Class II obesity (35 to 39.9kg/m²), and Class III obesity (≥40kg/m²).
Closed questions were used for sociodemo-graphic characteristics, involving: age, self-declared race/skin color, marital status, education, work situation, monthly family income, and number of household dependents.
The International Physical Activity Question-naire (IPAQ-L) was used to evaluate the physical ac-tivity pattern, with questions related to the frequen-cy, duration and intensity of the physical activities performed for more than ten continuous minutes during the past week, including four physical ac-tivities (work, commuting, domestic activities, and leisure). Its validity and reliability are described in the literature.(12) The IPAQ guidelines for data pro-cessing and analysis were followed.
Health self-perception was assessed by the ques-tion: “how do you consider your health today?”.(13) The answers were categorized as very good/good, normal, and bad/very bad.
The Perception of the environment for physi-cal activity practice scale was used, validated by Florindo et al. (2009), with 38 questions, and scores varying from 0 to 58 points. The higher the score obtained, the better the perception of the environment. The scale assesses different as-pects of the physical environment that can favor walking and the practice of physical activity in leisure and movement.(14) The first part contains 18 questions about availability and proximity of leisure structures, services and convenienc-es in the neighborhood, which are less than a ten-minute walk from home. The second part contains 20 questions related to the availability
and quality of environmental structures (green areas, sidewalks, garbage accumulation) close to the patient’s home, perceived safety in traffic and environment, social support, climate, and the presence of pets at home. The validation study on the scale does not suggest cutoff points, but indicates that the higher the score, the better the perception of the environment. Thus, the scores obtained by the quartiles enabled the classifica-tion of the environmental perception by individ-uals as: good (36 to 51 points), satisfactory (31 to 35 points), normal (27 to 30 points), and bad (13-26 points).
The self-efficacy for physical activity practice was evaluated by the Brazilian-validated scale, by Rech et al. (2011), with ten items distribut-ed in two groups, with scores ranging from zero to ten: 1) walks in free time (five items) and 2) participates in moderate and/or vigorous phys-ical activity (five items). The scale scores were computed with the sum of the responses of each group considering the answer “yes” as value one, and “no” as zero. The higher the value obtained, the higher the self-efficacy. Thus, using the quartiles, the scores allowed the classification of self-efficacy as: good (7 to 10 points); normal (5 to 6 points); satisfactory (3 to 4 points); and poor (0 to 2 points).
The research was approved by the Ethics Com-mittee, protocol nº 1,152,259 and met the national and international norms of ethics in research in-volving human beings.
Data analyzed are presented in absolute and relative frequencies, means and standard devia-tions. The prevalence ratio was used, with a 95% confidence interval (CI) to analyze the associa-tion between the variables of interest and physical inactivity in leisure-time. In the bivariate analy-sis, the Pearson’s Chi-square test was used, and the variables with a value of p≤0.20 was included in the logistic regression model: dependent per-son at home; body mass index; number of co-morbidities; health self-perception; self-efficacy; and perception of the environment. The regres-sion modeling was performed using the backward algorithm. To choose the model, the Akaike in-

311Acta Paul Enferm. 2017; 30(3):308-15.
Nascimento TS, Mussi FC, Palmeira CS, Santos CA, Santos MA
formation criterion (AIC) and the lowest values were chosen. The Hosmer-Lemeshow test and the ROC curve area were used to assess the accuracy and quality of fit for the logistic model. Due to the fact that PI was common in the sample, the Robust Poisson Regression Model was applied to correct risks. The STATA Statistical software, ver-sion 12, was used.
Results
One hundred and forty-two women met the in-clusion criteria and agreed to participate in the study. The mean age was 50.66 years (SD=11.59), minimum age was 21 and maximum was 81 years. Black women (93.7%) and those who were married/in a stable union (55.6%) predominat-ed, with a medium educational level; 66.4% had complete or incomplete high school/higher edu-cation. The majority was self-employed at a paid occupation (51.4%), retired but participated in some work activity, or were employed. The prev-alent monthly family income was one to three times the minimum wage (39.2%), with a mean of three people living at home (SD= 0.328), and 31.0% had dependents for whom they provided care at home.
The mean BMI was 36.29 kg/m2 (SD=6.23), with a higher proportion of obese women (83.1%), 31.7% had class III obesity, 29.5% had class I, and 21.8% had class II. Of the total, 16.9% were over-weight. Most patients had one or more comorbid-ities, such as hypertension, diabetes mellitus, or arthrosis, and considered their health status to be normal (54.9%).
The analysis of global PI, as evaluated by the IPAQ, considering the domains of work, commut-ing, domestic activities, and leisure, showed that 65.5% of the women were active/very active, as they achieved the recommendation for participating in physical activity ≥150minutes/week. A lower pro-portion (34.5%) was irregularly active/sedentary. Regarding the level of PI per IPAQ domain, 54.2% were inactive at home; 64.4% at work; 78.1% when commuting, and 85.2% during leisure. The self-ef-
ficacy for participating in physical activity was nor-mal/bad for 53.5% of the participants.
A higher prevalence of leisure-time PI was identified in women who were: aged 40-59 years (87.8%); white skin color/race (88.9%); without a stable union (88.9%); elementary level of education (89.6%); unemployed (88.4%); living with people dependent on care (93.2%); income one to three times the minimum wage (89.3%); obesity class III (95.6%); two associated comorbidities (90.6%); very poor/poor self-perception of health (96.3%); poor self-efficacy for participating in physical ac-tivity (97.6%); and who had a normal/satisfactory perception of the environment (89.7%) (Table 1).
In the bivariate analysis, an association of PI in leisure-time was found in those with home care de-pendents (PR: 1.14, 95% CI 1.01, 1.29), patients with class III obesity (PR: 1.27, 95 % 1.00, 1.62); two associated comorbidities (PR: 1.23, 95% CI 0.98, 1.56); normal health self-perception (PR: 1.33, 95% CI 1.05, 1.68); poor/very poor health self-perception (PR: 1.43, 95% CI 1.13, 1.80); poor self-efficacy (PR: 1.25, 95% CI 1.03, 1.51); and poor/satisfactory perception of the environ-ment (PR: 1.26, 95% CI 0.97, 1.63) (Table 1).
The best logistic model was chosen according to the lowest Akaike information criterion; the accuracy of the model was evaluated by the ROC curve, whose area was 0.88; and the quality of the model obtained by the Hosmer-Lemeshow test was p=0.83. In the multivariate model, women with one and two comorbidities had a respective increase of 27% (PR 1.27; 95% CI:1.02;1.58) and 31% (PR: 1.31, 95% CI:1,06;1.64) in PI during leisure-time. Those with poor (PR: 1.28, 95% CI:1.01;1.61) and normal (PR: 1.25, 95% CI:1.00;1.56) self-percep-tion were 28% and 25% less active, respectively. Women with poor self-efficacy for participating in physical activity were 27% less active (PR: 1.27, 95% CI:1.06;1.51), as well as those with a satis-factory perception of the environment (PR : 1.27, 95% CI: 1.01;1.60). Although there was no statis-tically significant association between PI and envi-ronmental perception, it was noticed that women with a worse perception presented as being prone to increasing their PI during leisure-time. Similarly,

312 Acta Paul Enferm. 2017; 30(3):308-15.
Factors related to leisure-time physical inactivity in obese women
this likelihood for increase was noted in those with home care of dependents, and obesity class I and III (Table 2).
Discussion
Physical activity during leisure-time is one of the di-mensions of physical activity which is recommend-ed worldwide;(15) however, in this study, the preva-lence of PI was high, and it was in fact higher than that of other investigations.(16-18)
The socio-demographic profile of the sample was corroborated with other studies, with a high-er proportion of PI in those who were: aged 40-59 years,(19) educated at a lower level,(20) married,(21) and had home care dependents.(21) Physical inactivity in leisure-time is also associated with family income, because, women with lower incomes tend to have less knowledge about healthy habits, time to spend on healthy levels of physical activity, and opportu-nities for recreational activities, which is one of the main barriers to participation in physical activity in developing countries.(22)
Table 1. Prevalence and prevalence ratio of inactivity in leisure-time according to sociodemographic and clinical characteristics, self-perception of health, and perception of the environment of overweight womenSociodemographic characteristics
n(%)Prevalence
(%)p-value PR 95% CI
Age 0.520
18 -39 years old 25(17.6) 80.0
≥40 to 59 years old 90(63.4) 87.8 1.10 (0.89; 1.36)
≥60 years old 27(19.0) 81.8 1.02 (0.78; 1.33)
Race/Skin color 0.748
White 9(6.3) 88.9
Mixed color (brown and black)
133(93.7) 85.0 0.96 (0.75; 1.22)
Marital status 0.270
Without partner 63(44.4) 88.9
With partner 79(55.6) 82.3 0.93 (0.81; 1.06)
Education 0.294
Up to elementary education 48(33.8) 89.6
High school/incomplete or complete Higher education
94(66.2) 83.0 0.57 (0.19; 1.65)
Occupation 0.297
Unemployed 69(48.6) 88.4
Employed 73(51.4) 82.2 0.93 (0.81; 1.07)
Home care dependents 0.073*
No 98(69.0) 81.6
Yes 44(31.0) 93.2 1.14 (1.01; 1.29)
Family monthly income 0.310
≥ 3 MW 36(25.4) 77.8
> 1 to <3 MW12 56(39.4) 89.3 1.15 (0.94; 1.40)
≤ 1 MW (2) 50(35.2) 86.0 1.11 (0.90; 1.36)
BMI 0.063*
Overweight 24(16.9) 75.0
Class I obesity 42(29.6) 85.7 1.14 (0.88; 1.48)
Class II obesity 31(21.8) 77.4 1.03 (0.77; 1.40)
Class III obesity 45(31.7) 95.6 1.27 (1.00; 1.62)
Number of comorbidities 0.200*
None (0) 30(21.1) 73.3
One (1) 45(31.7) 86.7 1.18 (0.92; 1.51)
Two (2) 53(37.3) 90.6 1.23 (0.98; 1.56)
Three (3) 14(9.9) 85.7 1.17 (0.86; 1.59)
Health self perception* 0.001*
Good/ very good 37(26.1) 67.6
Normal 78(54.9) 89.7 1.33 (1.05; 1.68)
Very poor/poor (2) 27(19.0) 96.3 1.43 (1.13; 1.80)
Self-efficacy for physical activity (n=140)
0.059*
Good 32(22.9) 78.1
Satisfactory 33(23.6) 78.8 1.00 (0.78; 1.30)
Normal 34(24.2) 82.3 1.05 (0.83; 1.34)
Bad 41(29.3) 97.6 1.25 (1.03; 1.51)
Perception of the environment (n=140)
0.143*
Good 28(20.0) 71.4
Satisfactory 39(27.9) 89.7 1.26 (0.97;1.63)
Normal 34(24.2) 85.3 1.19 (0.91;1.57)
Bad 39(27.9) 89.7 1.26 (0.97;1.63)
* Pearson Chi-square test p-value; † Fisher’s exact test p-value; MW - Minimum Wage; PR - Prevalence ratio; CI - Confidence interval; * Standardized by Z Score
Table 2. Factors related to physical inactivity during leisure-time in overweight womenVariables PR CI(95%)
Home care dependents
No 1 1.00
Yes 1.14 (0.99; 1.32)
BMI
Overweight 1 1.00
Class I obesity 1.14 (0.90; 1.46)
Class II obesity 0.95 (0.73; 1.23)
Class III obesity 1.21 (0.97; 1.51)
Number of comorbidities*
None 1 1.00
One 1.27 (1.02; 1.58)
Two 1.31 (1.06; 1.64)
Three 1.29 (0.98; 1.70)
Health self-perception*
Good 1 1.00
Normal 1.25 (1.00; 1.56)
Poor 1.28 (1.01; 1.61)
Self-efficacy (n=140)
Good 1
Satisfactory 1.09 (0.86; 1.37)
Normal 1.15 (0.92; 1.43)
Bad 1.27 (1.06; 1.51)
Perception of the environment *(n=140)
Good 1 1.00
Satisfactory 1.27 (1.01; 1.60)
Normal 1.15 (0.90; 1.46)
Bad 1.21 (0.96; 1.53)
AIC = 299,0284
Logistic regression model - p-value <0.05; RP - Prevalence ratio

313Acta Paul Enferm. 2017; 30(3):308-15.
Nascimento TS, Mussi FC, Palmeira CS, Santos CA, Santos MA
The prevalence of PI was higher in women with home care dependents (children and/or sick people), relating to the historical roles played by women as wives, mothers and caregivers, corrob-orating the findings of another study in which the presence of a great number of children at home made it difficult to participate in physi-cal activity during leisure-time, when they had no one to take care of their children.(21) Oth-er research showed that family obligations and family income were associated with PI during leisure-time within the population (45.4%) and, for women, these obligations were statistically significant.(23)
Another relevant fact was that the higher the body mass index, the greater the prevalence of PI in leisure-time, demonstrating that excess of weight is a factor negatively associated with participation in physical activity, as previously evidenced.(24)
Health self-perception, although rarely used in the clinic, has a strong association with mor-tality, morbidity and quality of life,(13,19,25) and was a predictor for inactive behavior during leisure-time in this study. Thus, nurses need to know the health self-perception of overweight women in their daily care, as well as illness and self-care, and be able to establish and propose health care actions guided by their characteris-tics and needs.(13) The nurse can identify with the women in how they can help them to im-prove their health condition, and support them with shared care actions.
This study showed self-efficacy was predictive of PI, that is, the belief of the individual’s success in the result of physical activity is fundamental to her practice. Meurer et al. (2015), identified that elderly individual participants of physical activity programs presented greater self-efficacy for walking compared to non-participants, emphasizing the im-portance of self-efficacy in planning and systematiz-ing actions to increase physical activity.(26) Thus, in-creasing the levels of self-efficacy may be an import-ant component in health promotion strategies.(6,27)
Activities in which women express their beliefs can provide a better understanding of the actual per-spectives for results. In addition, visualizing other
people adopting the behavior can increase the belief in the accomplishment of the activity. Techniques involving group discussion, private conversations, telephone conversations, e-mail messages, and read-ing behavioral texts may be strategies used by nurses to increase the women’s confidence in their ability to perform and maintain the behavior.(27)
The lowest perception of the environment was also associated with PI during leisure-time. In the American study conducted with 3,434 women, those living in areas with greater number of fa-cilities and shopping centers were more likely to meet walking recommendations, and those living near food places were almost twice as likely to be overweight (OR=1.77, 95% CI: 1.33; 2.20).(28) Similar data were found in the study that iden-tified that people who participated in physical activity during leisure-time had greater means in the scores of facilities/conveniences, perception of general safety, and social support for partici-pating in physical activity.(29) In this sense, vari-ables related to environment can improve the un-derstanding of individual behaviors and barriers to maintaining inactive behavior. Public policies and actions should focus on improving environ-mental conditions to enhance participation in physical activity.
Given these findings, it is a challenge for the multidisciplinary health team to stimulate the ac-quisition and maintenance of regular participation in physical activity during leisure-time, beginning at the youngest ages. Multiprofessional teams in the follow-up of overweight women should develop health education programs that stimulate recovery and clarify the recommendations for participation in physical activity. The stimulation for participa-tion in physical activity can be provided by differ-ent integrated actions of nurses and physical educa-tors, along with overweight women, even using the public space as a way to stimulate healthier living habits in an interactive and fun way. In addition, the provision of public spaces for participation in physical activities during leisure-time, individually or in groups, is a fundamental governmental strat-egy for health improvement, especially for the less favored subgroups.

314 Acta Paul Enferm. 2017; 30(3):308-15.
Factors related to leisure-time physical inactivity in obese women
The results support the development of inter-vention programs that emphasize individual and environmental characteristics for a good level of physical activity.
One of the limitations refers to a cross-sectional study, that does not allow for inferring the causality of the results (reverse causality), as the exposure and outcome are collected simultaneously.
Conclusion
A high prevalence of PI during leisure-time was iden-tified. The multivariate model showed that PI was significantly associated with: the number of comor-bidities; poor self-perception of health; low self-effi-cacy; and the perception of a bad environment.
AcknowledgementsTo the National Council for Scientific and Technolog-ical Development (Conselho Nacional de Desenvolvi-mento de Pesquisa e Tecnologia - CNPQ), for funding the research project, “Remote nurse monitoring of overweight women”, of which this article is a part.
CollaborationsNascimento TS, Mussi FC and Palmeira CS con-tributed to the study design, analysis and data inter-pretation, article writing, adaptation to the norms of the journal, and final approval of the version to be published. Santos CAT contributed to the an-alytical planning, analysis and data interpretation, and final approval of the version to be published. Santos MA contributed to the data collection, data treatment, and final approval of the version to be published.
References
1. Brasil. Ministério da Saúde. VIGITEL BRASIL 2015: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico [Internet]. Brasília (DF): Ministério da Saúde; 2016. [citado 2017 Jul 4]. Disponível em: http://portalsaude.saude.gov.br/images/pdf/2016/outubro/16/vigitel_brasil_2015.pdf.
2. World Healht Organization (WHO). Global status report on noncommunicable diseases. Geneva: WHO; 2010.
3. Knuth AG, Malta DC, Dumith SC, Pereira CA, Morais Neto OL, Temporão JG, et al. Prática de atividade física e sedentarismo em brasileiros: resultados da Pesquisa Nacional por Amostra de Domicílios (PNAD) 2008. Cien Saúde Colet. 2011; 16(9):3697-705.
4. Barbieri AF, Mello RA. As causas da obesidade: uma análise sob a perspectiva materialista histórica. Conex Rev Fac Educ Física da UNICAMP. 2012; 10(1):133-53.
5. Brasil. Ministério da Saúde. VIGITEL BRASIL 2014. vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico. Brasília (DF): Ministério da Saúde; 2014. [citado 2017 Jul 4]. Disponível em: bvsms.saude.gov.br/bvs/publicacoes/vigitel_brasil_2014.pdf.
6. Barros MB, Iaochite RT. Autoeficácia para a prática de atividade física por indivíduos adultos. Motricidade. 2012; 8(2):32-41.
7. Velásquez-Meléndez G, Mendes LL, Maria C, Padez P. Ambiente construído e ambiente social : associações com o excesso de peso em adultos. Cad Saúde Publica. 2012; 29(10):1988-96.
8. Mansfield ED, Ducharme N, Koski KG. Individual, social and environmental factors influencing physical activity levels and behaviours of multiethnic socio-economically disadvantaged urban mothers in Canada: A mixed methods approach. Int J Behav Nutr Phys Act. 2012; 9(1):42.
9. Rhodes RE, Mark RS, Temmel CP. Adult sedentary behavior: A systematic review. Am J Prev Med. 2012; 42(3):e3-28.
10. Brasil. Ministério de Planejamento Orçamento e Gestão. Pesquisa Nacional de Saúde 2013. Manual de antropometria. Rio de Janeiro; 2013.[citado 2017 Jul 4]. Disponível em: http://www.pns.icict.fiocruz.br/arquivos/Portaria.pdf.
11. World Healht Organization (WHO). Process for a global strategy on diet, physical activity and health. [Internet]. Geneva: WHO; 2003. [cited 2017 Jul 4]. Available from: http://apps.who.int/iris/bitstream/10665/67433/1/WHO_NMH_EXR.02.2_Rev.1.pdf.
12. Pardini R, Matsudo S, Matsudo V, Andrade E, Braggion G, Andrade D. Validação do questionário internacional de nível de atividade física ( IPAQ - versão 6 ): estudo piloto em adultos jovens brasileiros. Rev Bras Ciênc Mov. 2001; 9(3):45-51.
13. Arruda GO, Santos AL, Teston EF, Cecilio HP, Radovanovic CA, Marcon SS. Associação entre autopercepção de saúde e características sociodemográficas com doenças cardiovasculares em indivíduos adultos. Rev Esc Enferm USP. 2015; 49(1):60-7.
14. Florindo AA, Péricles E, Ii S, Siqueira R, Iv R. Percepção do ambiente e prática de atividade física em adultos residentes em região de baixo nível socioeconômico. Rev Saúde Pública. 2011; 45(2):302-10.
15. World Health Orgonization (WHO). Global action plan for the prevention and control of noncommunicable diseases 2013-2020. Geneva: WHO; 2013.
16. Del Duca GF, Nahas MV, Garcia LMT, Mota J, Hallal PC, Peres MA. Prevalence and sociodemographic correlates of all domains of physical activity in Brazilian adults. Prev Med (Baltim) 2013; 56(2):99-102.
17. World Health Organization (WHO). Global recommendations on physical activity for health. Geneva: WHO; 2010.
18. Jonck VT, Soares A, Araújo CC, Machado Z, Reis NM, Guimarães AC de A. Prevalencia de atividade física em mulheres. Rev Bras Promoção Saúde. 2014; 27(4):533-40.
19. Suzuki CS, Moraes SA, Freitas IC. Atividade física e fatores associados em adultos residentes em Ribeirão Preto, SP. Rev Saúde Publica. 2011; 45(2):311-20.

315Acta Paul Enferm. 2017; 30(3):308-15.
Nascimento TS, Mussi FC, Palmeira CS, Santos CA, Santos MA
20. Pitanga Godim F, Beck CC, Penas Seara Pitanga C, Mota Freitas M, Bastos Almeida LA. Prevalência e fatores sociodemograficos e ambientais associados atividade física no tempo livre e no deslocamento em adultos. Motricidade. 2014; 10(1):3-13.
21. De Sá-Silva SP, Yokoo EM, Salles-Costa R. Fatores demográficos e hábitos de vida relacionados com a inatividade física de lazer entre gêneros. Rev Nutr. 2013; 26(6):633-45.
22. Ward J, Friche AA, Caiaffa WT, Proietti FA, Xavier CC, Roux AV. Association of socioeconomic factors with body mass index, obesity, physical activity, and dietary factors in Belo Horizonte, Minas Gerais State, Brazil: The BH Health Study. Cad Saude Publica. 2015; 31:182-94.
23. Silva SG, Silva MC, Nahas MV, Viana SL. Fatores associados à inatividade física no lazer e principais barreiras na percepção de trabalhadores da indústria do Sul do Brasil. Cad Saúde Publica. 2011; 27(2):249-59.
24. Tucker JM, Tucker LA, Lecheminant J, Bailey B. Obesity increases risk of declining physical activity over time in women: A prospective cohort study. Obesity. 2013; 21(12):715-20.
25. Poubel PB, Lamar E, Araújo FC, Leite GG, Freitas S, Moisés R, et al. Autopercepção de saúde e aspectos clínico-funcionais dos idosos atendidos em uma unidade básica de saúde no norte do Brasil. J Health Biol Sci. 2017; 5(979):71-8.
26. Meurer S, Borges L, Graup S, Benedetti T. Autoeficácia de Idosos iniciantes em um Programa de Exercícios Físicos: comparação entre Permanecentes e Não Permanecentes. Rev Bras Ativ Física Saúde. 2015; 20(1):57-64.
27. Souza CA, Rech CR, Sarabia TT, Añez CRR, Reis RS. Autoeficácia e atividade física em adolescentes de Curitiba, Paraná, Brasil. Cad Saúde Publica. 2013; 29(10):2039-48.
28. Prince SA, Kristjansson EA, Russell K, Billette J, Sawada M, Ali A, et al. A multilevel analysis of neighbourhood built and social environments and adult self-reported physical activity and body mass index in Ottawa, Canada. Int J Environ Res Public Health. 2011; 7600:3953-78.
29. Florindo AA, Guimarães VV, de Farias Júnior JC, Salvador EP, de Sá TH, Reis RS, et al. Validação de uma escala de percepção do ambiente para a prática de atividade física em adultos de uma região de baixo nível socioeconômico. Rev Bras Cineantrop Desemp Hum. 2012; 14(6):647-59.

316 Acta Paul Enferm. 2017; 30(3):316-22.
Original Article
Laryngotracheal mucosa injury and associated factors after endotracheal extubation: a pilot studyLesão de mucosa laringotraqueal e fatores associados após extubação endotraqueal: estudo pilotoAldenora Laísa Paiva de Carvalho Cordeiro1
Renata Silva2
Carolina Beatriz da Cunha Prado3
Karoline Faria de Oliveira1
Maria Helena Barbosa1
Corresponding authorAldenora Laísa Paiva de Carvalho CordeiroRua Aluizio de Melo Teixeira, 480/301, 38065-290, Uberaba, MG, [email protected]
DOIhttp://dx.doi.org/10.1590/1982-0194201700048 1Universidade Federal do Triângulo Mineiro, Uberaba, MG, Brazil.
2Hospital e Maternidade São Domingos, Lar São Francisco de Assis na Providência de Deus, Uberaba, MG Brazil.3Universidade de Uberaba, Uberaba, MG, Brazil.Conflicts of interest: no conflicts of interest to declare.
AbstractObjective: To describe the clinical signs of laryngotracheal mucosal injuries and associated factors.Methods: This was an observational longitudinal study conducted with patients intubated due to general anesthesia. Assessment was carried out in the preoperative period, intraoperative period and at 24, 48, and 72 hours after extubation. Descriptive and exploratory statistics were used for analysis, in addition to odds ratio.Results: 53.3% of the sample presented at least one clinical sign of laryngotracheal mucosal injury, mainly: hoarseness (43.3%), dysphagia (40%), and odynophagia (33.3%). The following factors were associated: intracuff pressure above 25 cmH
2O, intubation longer than 120
minutes, and the use of tubes larger than 7.5mm.Conclusion: The most common clinical signs of laryngotracheal mucosal injury among the studied population were hoarseness, dysphagia, and odynophagia, associated with cuff pressure above 25 cmH
2O, followed by duration of intubation and inadequate endotracheal tube size.
ResumoObjetivo: Descrever os sinais clínicos de lesão de mucosa laringotraqueal e seus fatores associados.Métodos: Estudo observacional, longitudinal, em pacientes intubados por ocasião da anestesia geral. Foram realizadas avaliações no pré-operatório, transoperatório, e nas 24, 48 e 72 horas após extubação. Para análise, utilizaram-se estatísticas descritiva e exploratória, e também foi verificada a razão de chances.Resultados: Dentre os pacientes, 53,3% apresentaram pelo menos um sinal clínico de lesão de mucosa laringotraqueal, sendo predominantes: rouquidão (43,3%), disfagia (40%) e odinofagia (33,3%). Estiveram associados aos seguintes fatores: pressão intra-cuff acima de 25cmH
2O,
intubação por mais de 120 minutos e uso de tubos maiores que 7,5mm.Conclusão: Os sinais clínicos de lesão de mucosa laringotraqueal mais frequentes na população deste estudo foram rouquidão, disfagia e odinofagia, associados à pressão do cuff acima de 25 cmH
2O, seguido do tempo de intubação e tamanho inadequado de tubos endotraqueais.
KeywordsRisk factors; Intubation, intratracheal; Wounds and injuries; Laryngeal mucosa; Trachea
DescritoresFatores de risco; Intubação endotraqueal; Ferimentos e lesões, Mucosa da laringe; Traqueia
Submitted April 29, 2017
Accepted June 26, 2017

317Acta Paul Enferm. 2017; 30(3):316-22.
Cordeiro AL, Silva R, Prado CB, Oliveira KF, Barbosa MH
Introduction
Laryngotracheal mucosa can be damaged by vari-ous factors. The endotracheal intubation process, for example, is one of the main responsible factors for lesions; however, such lesions can be prevented based on knowledge about the pathophysiology of injuries and the adoption of prophylactic measures by multiprofessional teams involved in the care of intubated patients.(1)
Intubation-related injury in airway mucosa is difficult to diagnose, and can be severe and difficult to treat. They are common among patients with en-dotracheal tubes or tracheostomies, with the latter considered less harmful.(1-4)
The pathophysiology of injuries due to intuba-tion is mainly associated with the pressure exerted by the tube and/or cuff on the laryngotracheal mucosa. It is diagnosed through tests, such as fibrobronchos-copy, CT scans, laryngoscopy, and thoracic X-ray.(2,3) Interventions can be either surgical or conservative, with the use of appropriate drugs. However, in some cases, the effects of these injuries are irreversible.(4)
Choosing adequate tube diameter, in addition to monitoring and controlling cuff pressure are im-portant factors associated with the emergence of la-ryngotracheal injury. Other risk factors include the need for emergency intubation and prolonged in-tubation. However, some patients develop injuries even when intubation time is short.(1-5)
Adequate aspiration technique, balloon pressure monitoring, and adequate mobilization of intubat-ed patients, for example, are important activities that fall under the responsibility of the nursing staff. Handling accidental extubation or self-extubation, and all other actions that result from nursing care of patients with artificial airways must be conducted so as to mitigate any injury due to mechanical ven-tilation and the maintenance of artificial airways.(6-8)
The knowledge of clinical signs that suggest la-ryngotracheal injury, in addition to factors associ-ated by the nursing team, is of crucial importance when planning safe intubated patient care. Thus, the objective of the present study was to describe the clinical signs of laryngotracheal mucosa injury and associated factors.
Methods
This was an observational longitudinal study con-ducted in a large-scale public teaching hospital in the Southeast region of Brazil between March and June 2014.
The population consisted of patients submitted to anesthetic-surgical procedures, under general an-esthesia. Nonsystematic sampling was used due to the preliminary nature of the study.
Inclusion criteria were: hospitalized patients, in preoperative care, submitted to elective sur-gery; intubated because of anesthetic-surgical procedures (general anesthesia) and physical sta-tus classification I and II as per the American Society of Anesthesiologists (ASA).(9) Patients who presented clinical signs of laryngeal and tra-cheal alterations before the anesthetic-surgical procedure; who were submitted to surgical pro-cedures in the orotracheal cavity; whose type of anesthesia was changed immediately before the start of the surgery; referred to an intensive care unit in the immediate postoperative period; who presented hemodynamic complications in the in-traoperative period; who were discharged before 24 hours post extubation; and who dropped out of the study after extubation were excluded from the sample.
The population consisted of 72 patients who met the inclusion criteria, between May and June 2014. Of these, 42 (58%) were excluded, accord-ing to the following criteria: suspension of anes-thetic-surgical procedure (n=14); alteration of type of anesthesia (n=5); referral to intensive care unit (n=9); intraoperative hemodynamic complication (n=3); hospital discharge less than 24 hours after extubation (n=4); and participant dropout after ex-tubation (n=7). There were 30 eligible patients ac-cording to the inclusion criteria.
Data collection was conducted by four research-ers, who received specific training for two weeks by the research coordinator. The data collection in-strument was created by the authors exclusively for this study, based on the scientific literature,(1-5) and submitted to face validation by three expert judg-es. The instrument is divided into five parts: pre-

318 Acta Paul Enferm. 2017; 30(3):316-22.
Laryngotracheal mucosa injury and associated factors after endotracheal extubation: a pilot study
operative assessment; intraoperative monitoring; assessment 24 hours after extubation; assessment 48 hours after extubation; and assessment 72 hours after extubation.
The clinical variables obtained in the preoper-ative period were: ASA classification;(9) body mass index, according to World Health Organization (WHO) recommendations;(10) type of surgery; and anesthesia. The following variables were col-lected pre- and postoperatively: dysphagia verified through patient anamnesis and saliva swallowing test; odynophagia, verified through anamnesis; dysphonia or hoarseness, verified through a sim-ple voice test in which patients were asked to make long “a” and “e” sounds and through anamnesis; laryngeal stridor, verified through auscultation of tracheal region, pain on palpation, verified by pal-pating the tracheal region, in addition to observing patient expression and self-referred pain; presence of bleeding, verified by direct observation and self-referred by patients.
Predictor variables observed in the intraopera-tive period in the operating room were: surgical po-sitioning; size of endotracheal tube; number of in-tubation attempts; use of muscle relaxants; intracuff pressure of the endotracheal tube, measured with a cuff pressure gauge (analog gauge of endotracheal tube, with pressure range of zero to 120 cmH2O, color-coded for ideal pressure, with a bulb for in-flation and pressure control, with a pressure relief valve); angle of endotracheal tube to labial commis-sure; number of airway aspirations; and size of air-way aspiration probes.
The outcome variable was laryngotracheal mucosa injury, observed according to the occur-rence of the following clinical signs following extubation: dysphagia, odynophagia, dysphonia/hoarseness, dysarthria, presence of stridor, pain to touch in tracheal region and bleeding. All were verified through physical exam and anam-nesis after extubation.
The data were inserted into an electronic spreadsheet in Excel® for Windows XP®, using dou-ble entry validation (typing) and transferred to the Statistical Package for the Social Sciences (SPSS), version 18.0, for processing and analysis. Univari-
ate, descriptive and exploratory analyses were con-ducted to describe the investigated variables and subjects. Next, the odds ratio of predictor variables was verified.
This study was conducted according to reso-lution 466/12 of the Brazilian National Health Council. The protocol was submitted for appraisal and was approved by a research ethics committee, resolution no. 2.617.
Results
Mean patient age was 43.8 years, with a standard deviation of 20.6 years. Most patients were women, with 16 (53.3%) participants.
Of the 27 assessed patients, three (10%) pre-sented BMI lower than 18.5, nine (33.3%) were within the normal range, eight (26.7%) were overweight, and seven (23.3%) presented a BMI greater than 30. Three patients included in the study could not be mobilized to measure height and weight, and therefore, BMI could not be obtained.
Regarding type of surgery, of the 30 patients who participated in the study, 20 (66.7%) were submitted to surgery of the digestive system, three (10%) were submitted to plastic surgery, two (6.7%) to neurosurgery, two (6.7%) under-went urological surgery, two (6.7%), proctologi-cal surgery, and one (3.3%), ear, nose and mouth surgery.
Twenty-four (80%) patients were placed in su-pine position during the surgical procedure. Tubes smaller than 7.5 mm were the most used among the studied population. Number of intubation attempts varied from one to three attempts, and most of the sample was intubated on the first try, as shown in table 1.
Twenty-seven (90%) patients maintained mean intracuff pressure above 25 cmH2O. The angle of the endotracheal tube remained at 90° in five (16.7%) patients. Most (86.7 %) were in-tubated for over 120 minutes and, in this time, all patients underwent endotracheal aspiration procedures.

319Acta Paul Enferm. 2017; 30(3):316-22.
Cordeiro AL, Silva R, Prado CB, Oliveira KF, Barbosa MH
Regarding the emergence of clinical signs of la-ryngotracheal mucosa injury, 16 (53.3%) presented at least one sign.
Dysarthria and bleeding were not observed among the patients. The main clinical sign in the studied population after 24 hours of extubation was dysphonia/hoarseness, presented by 13 (43.3%) of patients. Clinical signs after 24, 48, and 72 hours of extubation are presented in table 2.
Men presented greater chances (odds ratio 2.31) of presenting clinical signs of laryngotracheal mu-cosa injury than women, in addition to a single in-tubation attempt.
Of the 16 (53.3%) patients who developed clinical signs of laryngotracheal mucosa injury, 14 (87.5%) presented intracuff pressure greater than 25 cmH2O; 13 (81.25%) were intubated for over 120 minutes; 12 (75%) were intubated with tubes greater than 7.5 mm and with the tube an-gle in relation to the labial commissure different than 90°.
Regarding intracuff pressure, three (18.75%) patients presented pressure ≤25 cmH2O, of which two presented clinical signs. Of the 27 (90%) pa-tients with intracuff pressure >25 cmH2O, 14 (87.5%) presented at least one clinical sign.
The odds ratio of the occurrence of clinical signs for each associated factor is displayed in table 3.
Table 1. Distribution of patients regarding variables observed in the intraoperative periodVariables n(%)
Surgical positioning
Supine 24(80.0)
Other 6(20.0)
Size of endotracheal tube, mm
Up to 7.5 23(76.7)
>7.5 7(23.3)
Intubation attempts
1 26(86.7)
>1 4(13.3)
Use of muscle relaxant
Yes 14(48.3)
No 15(51.7)
Intracuff pressure (mean of initial and final pressure), cmH2O
Up to 25 3(10.0)
> 25 27(90.0)
Angle of tube to labial commissure
90° 5(16.7)
Other 25(83.3)
Duration of intubation, minutes
Up to 120 4(13.3)
>120 26(86.7)
Number of aspirations
Up to 3 24(80.0)
> 3 6(20.0)
Table 2. Distribution of clinical signs 24, 48, and 72 hours after extubationClinical signs* n(%)
24 hours after extubation
Dysphonia/hoarseness 13(43.3)
Dysphagia 12(40.0)
Odynophagia 10(33.3)
Stridor 4(13.3)
Pain to touch in anterior cervical region 4(13.3)
48 hours after extubation
Odynophagia 6(20.0)
Dysphonia/hoarseness 4(13.3)
Dysphagia 4(13.3)
Stridor 1(3.3)
Pain to touch in anterior cervical region 1(3.3)
72 hours after extubation
Dysphagia 1(3.3)
Dysphonia/hoarseness 1(3.3)
*Categories are not mutually exclusive, i.e., more than one clinical sign could be present in the same patient
Table 3. Odds ratio of predisposing factors and clinical signs
VariablesClinical signs
OR (95%CI) p-valueYesn(%)
Non(%)
Gender 2.31(0.53-0.69) 0.26
Male 9(30.0) 5(16.7)
Female 7(23.0) 9(30)
Surgical positioning 0.0 -
Dorsal decubitus 16(53.3) 8(26.7)
Other position 0(0) 6(20)
Size of endotracheal tube, mm
0.82(0.14-4.51) 0.81
Up to 7.5 12(40.0) 11(36.7)
>7.5 4(13.3) 3(10)
Intubation attempts 4.09(0.37-44.7) 0.22
1 15(50.0) 11(36)
>1 1(3.3) 3(10)
Use of muscle relaxant 0.88(0.20-3.8) 0.85
Yes 7(24.1) 7(24.1)
No 8(26.6) 7(24.1)
Intracuff pressure, cmH2O 1.85(0.15-22.9) 0.62
Up to 25 2(6.7) 1(3.3)
>25 14(46.7) 13(43.3)
Angle of tube to labial commissure
4.33(0.42-44.4) 0.19
90° 4(13.3) 1(3.3)
Other 12(40) 13(43.3)
Duration of intubation, minutes
3.00(0.27-32.7) 0.35
Up to 120 3(10.0) 1(3.3)
>120 13(43.3) 13(43.3)
Number of aspirations 0.0 -
Up to 3 times 10(33.3) 14(46.7)
>3 times 6(20.0) 0(0)
OR - Odds ratio; 95%CI - 95% confidence interval

320 Acta Paul Enferm. 2017; 30(3):316-22.
Laryngotracheal mucosa injury and associated factors after endotracheal extubation: a pilot study
Discussion
Limitations of this study include its number of participants, not allowing for representativeness of other groups, as it is a preliminary assessment which can surely guide and foster future studies about laryngotracheal injury related to endotra-cheal intubation. However, statistical tests were conducted with methodological rigor, ensuring the reliability of the findings.
Endotracheal intubation is conducted daily in emergency rooms, pre-hospital environments and operating rooms. It is a necessary life-saving proce-dure, however, it can cause laryngotracheal injury, which can range from light to severe, temporary or permanent, and can even cause death.(11) Nurses must understand the clinical signs and associated factors of the occurrence of laryngotracheal mucosa injury to adopt due preventive measures.
The studied men developed more clinical signs of laryngotracheal mucosa injury than the women. This result was not corroborated by the results in the literature.(12) Other factors, both intrinsic and extrinsic, such as obesity and size of endotracheal tube, respectively, could have influenced results re-lated to patient gender and must be controlled in future studies.
The population of this pilot study consisted mainly by adult patients submitted to elective sur-gery of the digestive system, and the predominant clinical sign was hoarseness, a type of dysphonia and important indication of temporary or perma-nent vocal cord lesion.(3,13)
Over half of patients submitted to anesthet-ic-surgical procedures present hoarseness.(3) Howev-er, if after a week of extubation it has not subsided, professionals must suspect vocal cord paralysis.(3) A study conducted in Brazil with patients submitted to endotracheal intubation for over 24 hours and up to 14 days showed a moderate to intense level of vocal alteration in most participants, measured through patient self-perception.(13)
The occurrence of dysphagia after extubation is defined as the difficulty or inability to transfer food from the mouth to the stomach and is iden-tified through a liquid swallowing test, or with the
patient’s own saliva. This is a frequent and import-ant clinical sign in patients following endotracheal extubation.(14,15)
Odynophagia is a common postoperative clin-ical sign(1) and can predispose to temporary post-operative dysphagia. Further studies are needed to improve understanding of this clinical sign related to laryngotracheal injury after intubation.
Intracuff pressure over 25 cmH2O stood out in this study and this finding corroborates the trend found in the literature.(16) Ongoing monitoring of intracuff pressure and maintaining it at parame-ters lower than tissue perfusion pressure reduces incidence of dysphonia in patients submitted to endotracheal intubation.(3) Training health teams, especially nursing professionals, is considered a good strategy to raise awareness of the harmful ef-fects of excessive cuff pressure and contribute to safer patient care. Specific material is also neces-sary, such as cuff pressure gauges, to provide more precise readings.
In a clinical study conducted with dogs, 25 cm-H2O was established as the optimal pressure, seal-ing the tube to air leaks and preventing decreased air flow volume provided by the mechanical venti-lator, thus determining minimal injury to mucosa in contact with the cuff.(17)
Tests have been conducted with a device that au-tomatically modulates intracuff pressure, according to tidal volume, synchronized with either inspira-tion or expiration, i.e., during inspiration, intracuff pressure remains at 25 cmH2O and, during expira-tion, at 7 cmH2O. The device was tested with pigs and the automatic modulation of intracuff pressure was shown to be more efficient than maintaining constant pressure at 25 cmH2O, in terms of the oc-currence of injury.(18) This device has not yet been tested in humans.
Intubation time was also related to the emer-gence of clinical signs suggesting laryngotracheal mucosa injury. Of the 16 (53.3%) patients who developed injury, 13 (43.3%) had been intubated for over 120 minutes. The risk and incidence of lar-yngotracheal injury increase over time.(1) However, short-term intubations can also cause lesions.(5) The presence of the endotracheal tube triggers all the

321Acta Paul Enferm. 2017; 30(3):316-22.
Cordeiro AL, Silva R, Prado CB, Oliveira KF, Barbosa MH
histological phenomena of aggression and defense of the laryngotracheal mucosa, which do not de-pend on the duration of intubation. Duration of intubation seems to favor only the predominance of destructive injury.(5)
The position of the endotracheal tube in rela-tion to the labial commissure was associated with laryngotracheal injury. Of the 16 (53.3%) patients with clinical signs of laryngotracheal mucosa injury, in 12 (40%), the tube was angled different than 90° during the entire postoperative period. It is believed that the greater the inclination of the tube in rela-tion to the labial commissure, the greater the risk of developing laryngotracheal injury.
The chance of developing injury in patients who used endotracheal tubes ≤7.5 mm was lower than those who were given tubes >7.5 mm. The results described here are in accordance with the pattern described in the literature, which has indicated that larger tubes present greater risk for the development of laryngotracheal in-jury.(1,11) Choosing an adequate tube size is an import-ant factor to mitigate the risk of damaging mucosa in the laryngeal and tracheal region.
Concerning surgical positioning, it has already been shown that the position of Trendelenburg in patients undergoing laparoscopic gynecological sur-gery increases the pressure exerted by the cuff on laryngeal and tracheal mucosa, resulting in greater discomfort after extubation, and may constitute a factor associated with the occurrence of lesions La-ryngotracheals.(19)
Regarding surgical positioning, patients placed in the Trendelenburg position for laparoscopic gynecological surgery showed increased cuff pres-sure on laryngeal and tracheal mucosa, resulting in greater discomfort after extubation, considered an associated factor in the occurrence of laryngotra-cheal injury.(12,20,21)
Even though the aspiration of tracheobronchial secretions can be a necessary procedure, it can be harmful to tracheal mucosa.(7)
Studies about patient safety involving laryngo-tracheal injury are still incipient.(22) To minimize the occurrence of such lesions generated by the intubation process, healthcare teams must adopt preventive measures, such as rigorous and constant
monitoring of intracuff pressure, adequate patient position and immobilization, adequate tube size, and carrying out tracheal aspiration.
Nurses can identify risk of laryngotracheal mu-cosa injury based on the knowledge of its associ-ated factors. This type of injury can be prevented through technical and legal nursing actions. How-ever, nursing must intensify its studies about the di-agnoses, interventions, and outcomes that involve injuries to the laryngotracheal mucosa.
This pilot study can help raise awareness of nurs-es about the risks of implementing and maintaining artificial airways in patients, in addition to inciting further studies on the phenomenon of laryngotra-cheal mucosa injury.
Conclusion
The most common clinical signs of laryngotracheal mucosa were hoarseness, dysphagia, and odynopha-gia. Associated factors were cuff pressure above 25 cmH2O, duration of intubation and inadequate size of endotracheal tube.
CollaborationsCordeiro ALPC and Barbosa MH contributed to the conception of the study; data interpretation; drafting of the manuscript; and final approval of the version to be published. Silva R, Prado CBC and Oliveira KF participated in the critical review of the article for important intellectual content.
References
1. Mota LA, de Carvalho GB, Brito VA. Laryngeal complications by orotracheal intubation: Literature review. Int Arch Otorhinolaryngol. 2012; 16(2):236-45.
2. Cunningham LC, Jatana KR, Grischkan JM. Conservative management of iatrogenic membranous tracheal wall injury. JAMA Otolaryngol Head Neck Surg. 2013; 139(4):405-10.
3. Yamanaka H, Hayashi Y, Watanabe Y, Uematu H, Mashimo T. Prolonged hoarseness and arytenoid cartilage dislocation after tracheal intubation. Br J Anaesth. 2009; 103(3):452-5.
4. Esteller-Moré E, Ibañez J, Matiñó E, Ademà JM, Nolla M, Quer IM. Prognostic factors in laryngotracheal injury following intubation and/or tracheostomy in ICU patients. Eur Arch Otorhinolaryngol. 2005; 262(11):880-3.

322 Acta Paul Enferm. 2017; 30(3):316-22.
Laryngotracheal mucosa injury and associated factors after endotracheal extubation: a pilot study
5. Martins RH, Dias NH, Santos DC, Fabro AT, Braz JR. [Clinical, histological and eléctron microscopic aspects of vocal fold granulomas]. Rev Bras Otorrinolaringol. 2009; 75(1):116-22. Portuguese.
6. Rodrigues YC, Studart RM, Andrade IR, Citó CO, Melo EM, Barbosa IV. [Mechanic ventilation: evidence for nursing care]. Esc Anna Nery. 2012; 16(4):789-95. Portuguese.
7. Favretto DO, Silveira RC, Canini SR, Garbin LM, Martins FT, Dalri MC. Endotracheal suction in intubated critically ill adult patients undergoing mechanical ventilation: a systematic review. Rev Lat Am Enfermagem. 2012; 20(5):997-1007.
8. Ramalho Neto JM, Nascimento GN, Menezes MS, Nobrega MM. Extubação acidental e os cuidados de enfermagem. Rev Enferm UFPE on line. 2014; 8(11):3945-52. Portuguese.
9. Daabiss M. American Society of Anaesthesiologists physical status classification. Indian J Anaesth. 2011; 55(2): 111-5.
10. World Health Organization (WHO). Physical status: the use and interpretation of anthropometry [Internet]. Geneve: WHO; 1995 [cited 2017 Apr 21]. Available from: <http://apps.who.int/iris/handle/10665/37003.
11. Reichman EF, Lanam BJ. Tracheal rupture: a rare complication of endotracheal intubation. Pediatr Emerg Care. 2015; 31(11):774-8.
12. da Silva Costa A Jr, Juliano Perfeito JA, Succi JE, Villaça Leão LE, Rymkiewicz E, da Matta CA, et al. A video-assisted endotracheal suture technique for correction of distal tracheal laceration after intubation. Ann Thorac Surg. 2012; 93(6):2073-5.
13. Campos NF, Bougo GC, Gama AC, Vicente LC. [Effects of orotracheal intubation in voice and swallowing in adults and seniors]. Distúrb Comun. 2016; 28(4):597-608. Portuguese.
14. Macht M, Wimbish T, Clark BJ, Benson AB, Burnham EL, Williams A, et
al. Diagnosis and treatment of post-extubation dysphagia: Results from a National Survey. J Crit Care. 2012; 27(6):578-86.
15. Medeiros GC, Sassi FC, Mangilli LD, Zilberstein B, Andrade CRF. Clinical dysphagia risk predictors after prolonged orotracheal intubation. Clinics. 2014; 69(1):8-14.
16. Ryu JH, Han SS, Do SH, Lee JM, Lee SC, Choi ES. Effect of adjusted cuff pressure of endotracheal tube during thyroidectomy on postoperative airway complications: prospective, randomized, and controlled trial. World J Surg. 2013; 37(4):786-91.
17. Castilho EC, Braz JR, Catâneo AJ, Martins RH, Gregório EA, Monteiro ER. [Effects of tracheal tube cuff limit pressure (25 cmH2O) and “seal” pressure on tracheal mucosa of dog]. Rev Bras Anestesiol. 2003; 53(6):743-55. Portuguese.
18. Chadha NK, Gordin A, Luginbuehl I, Patterson G, Campisi P, Taylor G, et al. Automated cuff pressure modulation: a novel device to reduce endotracheal tube injury. Arch Otolaryngol Head Neck Surg. 2011; 137(1):30-4.
19. Geng G, Hu J, Huangs S. The effect of endotracheal tube cuff pressure change during gynecological laparoscopic surgery on postoperative sore throat: a control study. J Clin Monit Comput. 2015; 29(1):141-4.
20. Kalbhenn J, Boelke AK, Steinmann D. Prospective model-based comparison of different laryngoscope for difficult intubation in infants. Paediatr Anaesth. 2012; 22(8):776-80.
21. Yang M, Kim JA, Ahn HJ, Choi JW, Kim DK, Cho EA. Double-lumen tube tracheal intubation using a rigid video-stylet: a randomized controlled comparison with the Macintosh laryngoscope. Br J Anaesth. 2013; 111(6):990-5.
22. Pinto DM, Schons ES, Busanello J, Costa VZ. Patient safety and the prevention of skin and mucosal lesions associated with airway invasive devices. Rev Esc Enferm USP. 2015; 49(5):775-82.

323Acta Paul Enferm. 2017; 30(3):323-32.
Integrative Review
Concept analysis of nursing care management in the hospital context
Análise conceitual da gestão do cuidado em enfermagem no âmbito hospitalar
Deborah Dinorah de Sá Mororó1
Bertha Cruz Enders1
Ana Luisa Brandão de Carvalho Lira1
Cícera Maria Braz da Silva1
Rejane Maria Paiva de Menezes1
Corresponding authorDeborah Dinorah de Sá MororóRua General Gustavo Cordeiro de Faria, s/n, 59010-115, Natal, RN, [email protected]
DOIhttp://dx.doi.org/10.1590/1982-0194201700043
1Universidade Federal do Rio Grande do Norte, Natal, RN, Brazil.Conflicts of interest: there are no conflicts of interest to declare.
AbstractObjective: To analyze the concept of nursing care management in the hospital context on the basis of the theoretical-methodological framework of Walker and Avant.Methods: Elaboration of an integrative review to operationalize the analysis of the subject, extracting data from the databases Latin America and Caribbean Center on Health Sciences Information, Scientific Eletronic Library Online and the Brazilian Nursing Database, using the keywords and descriptors Care Management, Nursing and Hospital.Results: The review showed that management practice by nurses focuses on bureaucratic activities and has little relationship to care. However, coordination and integration of administration and care, leadership, communication, interaction, decision-making and cooperation were identified as essential characteristics of nursing care management.Conclusion: The application of this concept in nursing care management is an emerging need for the development of an administration model related to care.
ResumoObjetivo: Analisar o conceito gestão do cuidado em enfermagem no âmbito hospitalar, com base no referencial teórico-metodológico de Walker e Avant.Métodos: Realizou-se uma revisão integrativa, para operacionalizar a análise, nas bases de dados Literatura Latino-americana e do Caribe em Ciências da Saúde, Scientific Eletronic Library Online e a Base de dados de Enfermagem, utilizando palavra chave e descritores: Gestão do Cuidado, Enfermagem e Hospital.Resultados: Evidenciou-se uma prática gerencial do enfermeiro com enfoque para as atividades burocráticas e pouco articulada ao cuidado. Entretanto, identificaram-se a articulação e integração entre o gerenciamento e o cuidar, liderança, comunicação, interação, tomada de decisão e cooperação como atributos essenciais da gestão do cuidado em enfermagem.Conclusão: A aplicação desse conceito na prática gerencial do enfermeiro apresenta-se como uma necessidade emergente para o desenvolvimento de um modelo de gestão vinculada ao cuidar.
KeywordsHospitals; Management; Health services
administration; Health management
DescritoresHospitais; Gerência; Administração de serviços de saúde; Gestão em saúde
Submitted March 29, 2017
Accepted June 28, 2017

324 Acta Paul Enferm. 2017; 30(3):323-32.
Concept analysis of nursing care management in the hospital context
Introduction
Assuming that management and administration are synonyms and mean action, thinking and decision, they can be understood as the art of obtaining re-sults that can be defined, predicted, analyzed and evaluated. Therefore, management and administra-tion can be treated as scientific and rational fields, from which analyses and cause and effect relation-ships can be extracted. At the same time, they are exposed to unpredictability and human interac-tions, which gives them an intuitive, emotional and spontaneous dimension.(1)
Health care management is defined as the pro-vision of health technologies, taking into account the unique needs of people at different times in their lives, aiming at offering well-being, safety and autonomy. It manifests in six dimensions: in-dividual, family, professional, organizational, sys-temic and societarian.(2)
In nursing, care management is applied to the coordination of the management and service di-mensions of the nursing work process. When nurs-es act in the management dimension, they devel-op actions directed toward work organization and human resources, whose goal is to enable proper conditions for the delivery of care to patients and nursing team performance. The target of the care dimension, in its turn, is the needs of health care, which must be met fully.(3)
Therefore, two complementary dimensions can be identified in the nursing work process: the management dimension, whose subjects are work organization and nursing human resources; and the care dimension, whose focus of intervention is the care needs of patients.(4) The management function encompasses actions peculiar to nursing work that are directly associated with the nursing care process, mobilizing actions in relationships, associations and interactions among people,(3) which makes leader-ship an essential competence to accomplish this, since it facilitates personal and group interactions to meet common goals.(1,5)
However, when nurses carry out the manage-ment dimension, they often encounter dilemmas, doubts, conflicts, misunderstandings and contra-
dictions, because they have to deal with adminis-trative duties that are not well-coordinated with care actions.
This generates conflicts, frustration and dissat-isfaction about professional identity, mainly as it relates to know-how about care, given that man-agement actions usually focus on administrative and bureaucratic activities to meet institution-al demands.(6) For this reason, nurses sometimes identify their job as being of a bureaucratic-care nature and sometimes classify it as directed to care, maintaining a dichotomy between management and care.(5)
A study focused on the theoretical elaboration of nursing care management in the hospital context corroborated this, supporting the idea that nurses have conceptual difficulties with nursing care man-agement actions and revealing a dialectical rela-tionship between management and care expertise. This dialectic consists of an entanglement involving knowledge about management and care, through the existence of an interface separating these two objects in nursing practice, so that know-how has a technical and technological dimension, and in-volves personal and scientific knowledge, technical skills, and management and care competencies.(7)
Taking this into consideration, it is known that this problem is not an exclusive concern of the re-cent context of nursing practice. Other initiatives oriented to solving the conceptual and practical dichotomy of nursing care management have pre-ceded the present study. Such research has present-ed important contributions regarding reflections on nursing care management as they foster new investigations.
However, inconsistencies persists between care management concepts and their application by nurses. Thus, it is considered relevant to analyze the concept of nursing care management in the hospital context to broaden the discussion, strengthen the foundations of nursing science, and potentialize the applicability of the concept.
To achieve that, the authors proposed to ana-lyze the concept of nursing care management in the hospital context to make it clearer and contribute to this subject.

325Acta Paul Enferm. 2017; 30(3):323-32.
Mororó DD, Enders BC, Lira AL, Braz da Silva CM, Menezes RM
Methods
Concept analysis is a method that requires a careful process of examination of the basic elements of a concept, helping point out similarities and differ-ences by splitting the concept under discussion into simpler elements to make it easier to determine its internal structure.(8)
Walker and Avant(8) simplified the concept analysis procedure suggested by Wilson, which consisted of 11 steps, by reducing it to eight. The new version consisted of the following stages: 1) selection of the concept; 2) determination of the purpose of the analysis; 3) identification of the uses of the concept; 4) determination of its at-tributes; 5) identification of a model case of the concept; 6) identification of contrary cases; 7) identification of antecedents and consequences; and 8) definition of empirical references. Follow-ing the method, the authors chose to use the con-cept analysis framework by Walker and Avant,(8) by means of the stages: selection of the concept; determination of the purpose of the analysis; identification of the uses of the concept; determi-nation of its attributes; identification of a model case of the concept; identification of antecedents and consequences and definition of empirical ref-erences. Since the construction of the concept of care management in the hospital context required the clarificarion of the phenomenon in question, the authors chose not to use the identification of contrary cases, which is employed to reinforce the decision on the definition of attributes.(8)
However, the absence of this topic does not bring any loss to the concept analysis.
After the choice of the method, an integra-tive review was carried out about nursing care management in the hospital setting. The selected texts were submitted to a second screening based on the following inclusion criteria: complete pa-pers whose titles had the terms management or administration oriented to nursing care in the hospital context, available free of charge in the searched databases, in English, Portuguese or Spanish, published in the past five years. This
screening process was performed to make it eas-ier to spot the studies related to the topic in the hospital context.
The papers were selected from the data-bases Latin America and Caribbean Center on Health Sciences Information (LILACS), Scien-tific Eletronic Library Online (SciELO) and the Brazilian Nursing Database (BDENF), because these are the most important resources on Brazil-ian, South American and Caribbean literature in the health and nursing fields. Data extraction was performed by one researcher from December 27, 2015 to January 15, 2016.
Database surveys were carried out by using one keyword and two descriptors: 1: care man-agement, 2: nursing, and 3: hospital, respec-tively, in Portuguese, English and Spanish. The survey was conducted with the inclusion of the Boolean operator “and” to cross the searched items. In LILACS, 1,312 publications were se-lected by crossing the first and second items, 621 by crossing the first and third items, and 360 by crossing all the items. Inclusion criteria were subsequently applied; duplicate papers were ex-cluded. The abstracts were then read, and the re-maining material consisted of 13, 4 and 3 papers for each search combination, totaling 20 studies obtained from this database.
In BDENF, 82 papers were selected by crossing the first and second items, 265 by crossing the first and third items, and 63 from the combination of the three items. After application of the incusion criteria and exclusion of duplicates, 6 studies re-mained for analysis. After a careful reading of the full texts, 4 papers were chosen for inclusion in the final sample of the review.
The survey in SciELO provided the follow-ing results: 212 papers were obtained by crossing the first and second items, 153 by crossing the first and third items, and 66 in the search that in-cluded all the items. After exclusion of duplicate studies, application of the inclusion criteria, and meticulous reading of the manuscripts, 3 publi-cations were chosen. Figure 1 depicts the paper selection process.

326 Acta Paul Enferm. 2017; 30(3):323-32.
Concept analysis of nursing care management in the hospital context
After collection of the scientific production about the subject, exhibited in chart 1, the full pa-pers were read thoroughly to determine the defining attributes, the identification of precedents and con-sequences, and the empirical references of the con-cept of nursing care management. To identify the concept, attributes, antecedents and consequences in the studies, the following questions were created to guide the work: What is the definition of nurs-ing care management or administration in the hospi-tal context? What are the specificities that the concept under analysis presents? What events contribute to the existence of the concept under analysis? What are the results of the application of the concept under analysis?
To identify the model case and the empirical references, the guiding questions were: What model case in nursing care management demonstrates all the attributes of the concept definition? How can this concept be measured?
Careful reading of each paper allowed the iden-tification of the words related to antecedents, at-tributes, consequences and empirical references of nursing care management.
During the review process, words that referred to antecedents were highlighted in yellow, those
related to attributes in blue, and those associated with empirical references in red. Finally, the terms used more times in the papers were selected. The data are shown in a chart, and analyzed according to the literature.
Results
Identification of the use of the concept of nursing care managementMost original investigations oriented to nursing care management in the hospital context focus on the way that nurses perform management and care actions in their practice. It was noticed that care management is construed as a complementary sub-process in the nursing work process, but that it is necessary to recognize care as the target to be ad-ministered in health services.(9) Regarding the plac-es where healthcare professionals appropriated the expression, the areas that stood out were emergency and urgency units, mobile prehospital care services, general patient and obstetric units, and outpatient clinics.(9, 10, 11, 12, 13)
Figure 1. Flowchart showing the literature survey in BDENF, LILACS and SciELO
Surveyed databases
Papers published in the past five years, in English, Portuguese or Spanish,
addressing the subject of nursing care management
in the hospital context
Keyword and descriptors:#1: Care management
#2: Nursing#3: Hospital
BDENF LILACS
Papers selected for analysis
SciELO
410
4 20 3
2,293 431

327Acta Paul Enferm. 2017; 30(3):323-32.
Mororó DD, Enders BC, Lira AL, Braz da Silva CM, Menezes RM
Chart 1. Characterization of the studies about nursing care management in the hospital context; the papers are organized according to title, authors, objective and type of studyTitle/Authors Objective Type of study
Gestão contemporânea: a ciência e a arte de ser dirigente (Contemporary management: the Science and the art of being a leader). Motta PB(1)
To reconcile theory and management practice, resulting in a new and more consistent vision of the management world.
Theoretical study.
Theoretical and conceptual notes on evaluative processes taking the multiple dimensions of healthcare management into account. Cecílio LC(2)
To present a reflection on health evaluation that takes into account the multiple dimensions of health care management (individual, family, professional, organizational, systemic and societarian).
Reflection study.
Meanings of care management built throughout nurses’ professional education. Senna MH et al.(3)
To understand the meanings of care management to academics, nurses and professors built throughout professional training.
Qualitative study, guided by grounded theory.
Perception of nurses regarding management activities for user assistance. Giordani JN, Bisogno SB, Silva LA(4)
Identifiy the perception of nurses working in a general hospital about management activities in care to users.
Qualitative, exploratory and descriptive study.
Nursing and leadership: perceptions of nurse managers from a hospital in Southern Brazil. Pereira LA et al.(5)
To identify how nurse managers define and execute leadership in a philanthropic hospital in the South region of Brazil and the training methods of these nurses to develop this activity.
Quantitative study.
The affects in the managerial working process in the hospital: the Experiences of the nurse. Lima RS, Lourenço EB(6)
To understand the feelings experienced by nurses as a response to management activities in the hospital context.
Qualitative, exploratory, descriptive and cross-sectional study.
Nursing care management in hospital settings: the bulding of a construct. Christovam BP, Porto IS, Oliveira DC(7)
To create and present the theoretical definition of nursing care management in the hospital context.
Multi-referential approach to build concepts.
Strategies for theory construction in nursing. Walker LO, Avant KC(8) To describe strategies to build theories in the nursing area and the concept analysis method.
Theoretical study.
Institutional demands and care demands in the management of nurses in an emergency unit. Montezelli JH, Peres AM, Bernardino E(9)
To characterize the management activities of a nurse in an emergency room. Qualitative study.
Nursing management in the emergency unit: problems and challenges. Zambiazi BR, Costa MC(10)
To identify difficulties and challenges in the nursing management of an emergency unit and report the management activities carried out by nurses.
Qualitative and descriptive study.
Organizational context and care management by nurses at emergency care units. Santos JL et al.(11)
To understand the meanings attributed to the configurations of the organizational context and to nurses’ performance in the care management of an emergency care unit.
Qualitative study guided by grounded theory.
Emergency medical service nursing staff perceptions about nursing management. Bueno A.A, Bernardes A(12)
To characterize the management/supervision carried out by nurses in a mobile prehospital care unit according to the opinion of the nursing staff in a city in the countryside of Minas Gerais, Brazil.
Qualitative, exploratory and descriptive study.
Nurses’ care and management actions in emergency trauma cases. Azevedo AL de C.S, Scarparo AF, Chaves LDP(13)
To analyze care and management actions of the nurses in a hospital traumatic emergency unit.
Qualitative, exploratory, descriptive, multiple case study.
Nursing perceptions about abortion management and Care: a qualitative study. Strefling IS et al.(14)
To describe management and care for women admitted because of miscarriage from the perspective of nursing professionals.
Qualitative, exploratory and descriptive study.
Management of nursing care of the adolescent living with HIV/AIDS. Koerich C et al.(15)
To characterize nursing care management in a unit focused on the care of teenagers who contracted/developed HIV/AIDS through vertical transmission during the transition carried out in the reference services in the treatment of HIV/AIDS for children and adults in a state in the South region of Brazil, suggesting strategies for this adaptation period.
Qualitative, exploratory and descriptive study.
Competencies developed in a nursing management distance learning specialization course. Okagawa FS, Bohomol E, Cunha IC(16)
To identify management competencies developed during the distance education specialization in nursing management by analysing the answers of the students to a questionnaire.
Exploratory study with a qualitative and quantitative triangular approach.
Relevance level of application of management competencies in nursing. Ángel-Jiménez GM, Lopera-Arrubla CP(17)
To identify the relevance and level of application of the main competencies in nursing management.
Descriptive study with a qualitative and quantitative approach.
Management competences in the formation of nurses. Lourencao DC, Benito GA(18)
To identify the insertion of management competencies in nursing training. Qualitative study that analyzed the contents of pedagogical documents of a nursing school at a university.
Nursing care management to men with cancer. Mesquita MG(19) To discuss the interactions between gender perspective and comprehensiveness in nursing care management focused on care for men with cancer.
Qualitative study guided by grounding theory.
Management theories in health care. Paiva SM et al.(20) To review the influence of administration theories in the organization of health services, emphasizing the quality of the care and to use it as a basis for a reflection on the nursing work process.
Literature review.
Management: counterpoints perceived by nurses between training and the workplace. Montezelli JH, Peres AM(21)
To identify nurses’ perceptions about the counterpoints in training and real requirements of the work environment for the application of management practices.
Qualitative and descriptive study.
Computerization of Nursing Care System: advances in care management. Ribeiro JC, Ruoff AB, Baptista CL(22)
To discuss the facilitative and hindering aspects of the informatization of nursing care systematization in nursing care management.
Multiple case study.
La vinculación ético-jurídica entre la gestión del cuidado y la gestión de riesgos en el contexto de la seguridad del paciente. Milos P, Larraín AI(23)
To reveal the existence of an ethical-legal relationship between care management and risk management in the context of patient safety.
Reflective study about nursing care and patient safety from an ethical-legal viewpoint.
Competencias para la enfermera/o en el ámbito de gestión y administración: desafíos actuales de la profesión.. Soto-Fuentes P et al.(24)
To answer two questions: What is currently required from nurses in the management context? What are the most important nursing management competencies and how do they relate to care management?
Literature review.
Enfermería en el rol de gestora de los cuidados. Estefo Aguero S, Paravicklijn T(25)
To emphasize the importance of some aspects necessary to work as a nursing care manager
Reflective study.
The construction process of managerial profile competencies for nurse coordinators in the hospital field. Manenti AS et al.(26)
To create a profile of management competencies agreed on by nurses who act as coordinators in this area.
Action research.
Entrevista com gestores como método pedagógico para o gerenciamento na enfermagem: conhecer para ser (Interviews with managers as a pedagogical method for nursing management: learning to be). Ferreira Junior AR, Souza Vieira LJ, Barros NF(27)
To discuss active teaching-learning methodologies in nursing management. Experience report.
Care management for tuberculosis: from education to the nurse practice. Barrêto AJ(28)
To analyze the relationship between nursing training and actions oriented to tuberculosis care management.
Qualitative and descriptive study.
Analysis of the UCSF Symptom Management Theory: Implications for Pediatric Oncology Nursing. Linder L(29)
To analyze the symptom management theory developed at the University of California at San Francisco, focusing on research applications involving children with cancer.
Analysis of the theory using the process described by Walker and Avant

328 Acta Paul Enferm. 2017; 30(3):323-32.
Concept analysis of nursing care management in the hospital context
It was shown that in these places nursing man-agement practices are oriented mainly toward pro-viding material resources and determing the size of work teams, in an activity separate from care to pa-tients and the fulfillment of user needs.
Defining attributes of nursing care man-agementAlthough studies have shown that nursing manage-ment practice is focused on bureaucratic adminis-trative activities that bear little relationship to care, the analyzed papers presented coordination and integration as essential characteristics of care man-agement, as well as leadership, teamwork, commu-nication, and coordination and cooperation among nursing teams and with other healthcare profession-als and users.(3,6,12,14,15, 16,17,18)
Coordination of management actions and the care process provides nurses with possibilities to reunite with care, and consequently contrib-utes to increased satisfaction levels and decreased work stress.(6)
The literature survey allowed identification of coordination and integration of management and care, and the practices of leadership, interaction, communication, decision-making and cooperation, as fundamental attributes in nursing care manage-ment. The interactive relationship between nurses and users stands out as an important element in care management dynamics, because it allows ex-changing information and establishing trust and bonds, contributing to the realization of actions to promote and recover user health.(19)
Based on the identified attributes, it was pos-sible to create the following definition of nursing care management: “It is the coordination and inte-gration of care and management actions, through the practice of leadership and interaction, com-munication and cooperative relationships by nurs-es towards nursing teams, healthcare professionals, and users”.
Creation of a model caseThe model case is an example of use of the concept and presents all its attributes. It can be found in the literature and based on real-life events or created
by the concept analyst.(8) In the present study, the authors opted to create a model case based on the expeirences of one of the authors in a pediatric unit. The case is described below.
A nurse integrating the multi-professional team in a pediatric unit came across the case of a teen-ager with a diagnosis of chronic kidney disease; she had been submitted to a kidney transplant six months previous, having the father as the donor. Her history was marked by family conflict after her parents’ divorce and her mother’s moving abroad, which created intense conflict between her mater-nal grandmother and her father.
After the kidney transplant, the teenager was readmitted to the hospital several times because of recurrent urinary infections, a problem that was always permeated by the family issues and the precarious socioeconomic conditions she lived in. After the surgery, the father won custody of her. He was unnemployed and both were living on governament benefits.
In this scenario, chief nurses assume the posi-tion of leader of the nursing team and carry out nursing care management, emphasizing integrated and humanized care, centered on user needs. They use relational technologies and interact with pa-tients and their families by welcoming them and creating bonds, assuming that they will help estab-lish affection and trust, which are essential to care management. The nursing process systematizes this care by identifying patient needs, outlining nursing diagnoses, planning and executing nursing prescrip-tions, implementing interventions oriented to com-prehensive care, and evaluating the care provided.
From this perspective, nurses coordinate and communicate with the members of nursing teams and other health professionals (in this case, a ne-phrologist, social worker, nutritionist, psychol-ogist and pharmacist) through interprofessional discussion of the case and establishing interactive and cooperative relationships, sharing and negoti-ating responsabilities and decision-making, in the search for alternatives to improve the quality of life of patients.
Interprofessional interaction allows nurses to participate in the design of the singular thera-

329Acta Paul Enferm. 2017; 30(3):323-32.
Mororó DD, Enders BC, Lira AL, Braz da Silva CM, Menezes RM
peutic projects of patients; the goals are improve-ment of patient clinical condition, reinsertion in families, and hospital discharge. To achieve care comprehensiveness, nurses, together with inter-professional hospital teams and relatives, enables cotinuity of care at home through coordination and interaction with the Family Health Strategy or home care services.
Antecedents and consequencesIn this step, a literature survey was carried out to identify historical facts that preceded the phe-nomenon under analysis.(8) It was found that the dichotomy between management and care per-vades the nursing administration field to the pres-ent day. This understanding was influenced by sci-entific theory, which arose at the beginning of the twentieth century, during the industrial period. This approach involved application of scientific methods to administration issues; it was an ad-aptation of Taylorism or management rationality, centered on duty, productivity, division of work, specialization and standardization of activities. Subsequently, industries emerged and a need arose to organize companies more efficiently. Thus, to satisfy these demands, the bureaucratic theory was developed and quickly spread throughout business organizations, including health services. That was the consolidation of Taylorism and the bureaucratic model.(20)
This model is characterized by centralization, hierarchy, and work control through regulation, norms and standards of behavior. Therefore, the management function controlled by this concep-tion that is practiced in the hospital setting favors norms, routines and procedures to the detriment of the user needs.(20)
The management practice influenced by this model is marked mainly by fragmentation of work, with separation of the conception and steps in its execution, and management control of the production process associated with strict hier-archy and rationalization of the administration structure. As a consequence of this historical pro-cess, nursing management embarked on an area focused on human and material resources, distant
from care and oriented to institutional require-ments, whose main characteristics are fragmenta-tion and division of work, management control of the production process, impersonality in interper-sonal relationships and emphasis on procedures and routines.(3)
Nevertheless, this is a management model that does not meet the complexities of health care, which shows the need to incorporate new concepts to create a nursing professional profile based on scientific evidence and relational, ethical, political and humanistic competencies, that allows profes-sionals to practice the care management function with creativity and autonomy and move away from empiricism.(3,21)
In opposition to Taylorism, the human re-lations theory of management valued subjective aspects in management and revealed that em-ployees perform differently when their functdion are develope in groups. This theory inspired the multi-professional work model and had a positive impact in health services.(20) As a consequence of these changes in management conceptions and practices, innovative and interactive ways to man-age in the nursing area have been envisaged, to achieve shared decision-making, favor interper-sonal relationships in teams, develop systematiza-tion of nursing care (SNA), and qualify the care offered to users.(22)
Empirical referencesThis is the final step in the analysis and aims to determine the existenceof, or show the occur-rence of, the phenomenon in the real world.(8) It was observed that nursing care management qualifies care as it relates to planning, organiz-ing and controlling care delivery, which must be timely, safe, comprehensive, continuous and per-sonalized.(17,23)
When assuming positions of leadership in nursing care management through interactive and collaborative relationships with health profes-sionals and patients, nurses enable the delivery of timely, safe, continuous and individualized care. In addition, they give the profession greater visibility in the social context and increase its development.

330 Acta Paul Enferm. 2017; 30(3):323-32.
Concept analysis of nursing care management in the hospital context
Thus, the performance of nurses in care mana-gement has three dimensions: technical, unders-tood as a set of instruments, knowledge and skills necessary to meet the goals of specific projects; po-litical, characterized by coordination of manage-ment tasks and the care projects they are directed toward; and communication, which is revealed in the work relationships established by health teams, and is ideally interactive and cooperative, directed toward common care undertakings, built collecti-vely and focused on dialogue that mediates theory and practice.(26)
Leadership arises as a fundamental component of management, for which nurses must prepare by developing a crucial skill for succes: commu-nication. This is seen as the basis of leadership, an indispensable element for this process to take place. Another essential ability for the practice of leadership is decision-making, which requires the ability to spot problems, search for solutions and select alternatives that best allow for meeting the intended targets.(25)
Taking into consideration the relevance of the management function for nurses, it is necessary to emphasize the importance of investing in the management component during nurse training to provide professionals with the tools they need to develop the leadership, teamwork, communication, interpersonal relationships, decision-making, plan-ning and organization skills, among others, that are necessary in their professional profile.(17)
The crucial attributes for nursing care manage-ment must be worked on and developed during nurse training through the approximation of theo-retical knowledge and practice.(27)
However, nurs training based on the attributes of care management requires a departure from tra-ditional teaching models focused on fragmentation of information and practices, and recognition of the
(17,23) The management of nursing care processes implies minimization of risks and maximizizing of benefits for users, health teams, institutions and communities.(24)
Therefore, it is understood that the empirical references of the existence of this phenomenon may be represented by safety indicators of pa-tients, which show the quality of interprofessional interaction, effective communication, integration and coordinationn, given that care management involves essentially the promotion of safe environ-ments.(23) To achieve this, it is necessary to make efforts to implement the monitoring of safety in-dicators and of control of hospital-acquired in-fections, such as healthcare-associated infections, pressure-related injuries, and mistakes in the preparation and administration of medication, among others, that represent quality of care and can be used as empirical references for nursing care management.
Chart 2 summarizes antecedents, attributes, consequences and empirical references in nursing care management.
Discussion
Nursing care management is construed as a profes-sional practice of nurses, based on care science, and carried out through actions of planning, organiza-tion and control of timely, safe and comprehensive care delivery, to ensure continuity of care and su-pport policies and strategical orientations in heal-th institutions. From this perspective, nurses must provide an organizational culture that favors the practice of care, selecting people, developing trai-ning programs, and implementing a care model that can guide nursing practice and promote the actions of healthcare professionals.(25)
Chart 2. Antecedents, attributes, consequences and empirical references in nursing care management in the hospital contextAntecedents Attributes Consequences Empirical References
Scientific theory and bureaucratic theory, which originated in Taylorism and the bureaucratic model.
Coordination and integration of management and care; leadership, decision-making, interaction, communication and cooperative relationships between nurses, nursing teams, healthcare professionals and users.
Qualification of are for users; development of SNA; improvement of interpersonal relationships in teams; sharing of decision-making.
Indicators of the safety of the care given to patients; quality of the knowledge of teams; communication process between nursing teams, healthcare professionals and users.

331Acta Paul Enferm. 2017; 30(3):323-32.
Mororó DD, Enders BC, Lira AL, Braz da Silva CM, Menezes RM
need for transdisciplinarity and extending relation-ship networks to conform to this new professional profile. In this way, the use of pedagogical methods that allow recognition of users as singular individu-als, and that allow for experience and development of leadership skills, will provide the foundation for nurses to engage in interdisciplinarity.(18,28)
The complexity of health care refers to the need for interdisciplinary work through sharing knowl-edge, responsabilities and decisions, in order to overcome interdisciplinary barriers and achieve care comprehensiveness.(18) Nevertheless, studies have shown that in undergraduate courses, teaching spac-es are still focused mainly on clinical practice, espe-cially the healing field; the predominant approach is biological, with a significant dissociation between theory and practice.(28) It is necessary to rethink nurse training and invest in permanent education by offering varied experiences that allow profession-als to develop management skills and overcome the dichotomy between management and care. These abilities will shape professionals for collective, inter-dependent and cooperative work.(3)
From this understanding, it is possible to cre-ate other nursing care management models based on interactive and cooperative relationships with health professionals and patients to provide timely, continuous, safe and individualized care.(17,23)
In addition, it is also necessary to apply theo-ries and conceptual models to guide nursing clinical practice and conduct research in the area. However, these theories can be used only after previous anal-ysis to evaluate their applicability and identify in-consistencies and strengths. One study in the U.S. analyzed a medium-reach theory called symptom management theory, developed at the University of California at San Francisco, examining its im-plications for nursing clinical practice in pediatric oncology. The investigation showed the potential of the theory to influence guidance of nursing in-terventions and development of strategies directed to the management of symptoms in children with cancer, in addition to illustrating the applicability of the model in the research field.(29)
On the basis of the findings of the present study, it is necessary to stress the importance of investing
in the development of theoretical models that can guide clinical practice and nursing research to break the dissociation between teaching, research and care and enable continuous coordination and integra-tion of these dimensions.
The present study had some limitations. The concept analysis used secondary data, which can lead to subjectivity. In addition, the database sur-vey was conducted by only one researcher, and the selected period of five years narrowed the observa-tion to the most recent scientific production on the subject. Some positive points that deserve to be em-phasized are the relevance of concept analysis as a foundation of nursing practice and the potential of integrative reviews in the health area, considering that they provide synthesis of significant publica-tions about a specific theme, which facilitates the incorporation of results into practice.
Conclusion
The present study allowed the identification, as essen-tial attributes of the investigated phenomenon, coor-dination and integration of management and care, and interaction, communication, decision-making and cooperation, which must rule the interpersonal relashionships established by nurses with members of nursing teams, health professionals and patients. The application of this concept in nursing management practice has brought to light the need to develop a management model associated with care, sharing of duties among staff, and qualification and compre-hensiveness of the care provided to users. Its applica-bility can be assessed through quality of care indica-tors, especially those related to patient safety.
CollaborationsMororó DDS, Enders BC and Lira ALBC contrib-uted to the conception of the study, critical and rel-evant review of the manuscript, and final approval of the version to be published. Braz da Silva CM and Menezes RMP contributed to writing of the manuscript, critical and relevant review of the in-telectual content, and final approval of the version to be published.

332 Acta Paul Enferm. 2017; 30(3):323-32.
Concept analysis of nursing care management in the hospital context
15. Koerich C, Santos FC, Meirelles BH, Erdmann AL. Gestão do cuidado de enfermagem ao adolescente que vive com HIV/AIDS. Esc Anna Nery. 2015; 19(1):115-23.
16. Okagawa FS, Bohomol E, Cunha IC. Competências desenvolvidas em um curso de especialização em gestão em enfermagem à distância. Acta Paul Enferm. 2013; 26(3):238-44.
17. Ángel-Jiménez GM, Lopera-Arrubla CP. Relevance y level of application of management competencies in nursing. Invest Educ Enferm. 2013; 31(1): 8-19.
18. Lourencao DC, Benito GA. Competências gerenciais na formação do enfermeiro. Rev Bras Enferm. 2010; 63(1):91-7.
19. Mesquita MG, Paes GO, Silva MM, Duarte SC, Erdmann AL, Leite JL. Gerência do cuidado de enfermagem ao homem com câncer. Rev Pesq Cuid Fundam Online. 2015; 7(3):2949-60.
20. Paiva SM, Silveira CA, Gomes EL, Tessuto MC, Sartori NR. Teorias administrativas na saúde. Rev Enferm UERJ. 2010; 18(2):311-6.
21. Montezelli JH, Peres AM. Gerenciamento: contrapontos percebidos por enfermeiros entre a formação e o mundo do trabalho. Ciênc Cuid Saúde. 2012; 11 (Supl):138-43.
22. Ribeiro JC, Ruoff AB, Baptista CL. Informatização da sistematização da assistência de enfermagem: avanços na gestão do cuidado. J Health Inform. 2014; 6(3):75-80.
23. Milos P, Larraín AI. La vinculación ético-jurídica entre la gestión del cuidado y la gestión de riesgos en el contexto de la seguridad del paciente. Aquichan. 2015; 15(1):141-53.
24. Soto-Fuentes P, Reynaldos-Grandón K, Martínez-Santana D, Jerez-Yáñez O. Competencias para la enfermera/o en el ámbito de gestión y administración: desafíos actuales de la profesión. Aquichan. 2014; 14(1):79-99.
25. Estefo Aguero S, Paravicklijn T. Enfermeira en el rol de gestora de los cuidados. Ciênc Enferm. 2010; 16(3): 33-9.
26. Manenti AS, Ciampone MH, Mira VL, Minami LF, Soares JM. O processo de construção do perfil de competências gerenciais para enfermeiros coordenadores de área hospitalar. Rev Esc Enferm USP. 2012; 46(3):727-33.
27. Ferreira Junior AR, Souza Vieira LJ, Barros NF. Entrevista com gestores como método pedagógico para o gerenciamento na enfermagem: conhecer para ser. Enferm Glob. 2012; 11(27):106-14.
28. Barrêto AJ, Evangelista AL, Sá LD, Almeida SA, Nogueira JA, Lopes AM. Gestão do cuidado à tuberculose: da formação à prática do enfermeiro. Rev Bras Enferm. 2013; 66 (6): 847-53.
29. Linder L. Analysis of the UCSF Symptom Management Theory: Implications for Pediatric Oncology Nursing. J Pediatr Oncol Nurs. 2010; 27(6):316-24.
References
1. Motta PB. Gestão contemporânea: a ciência e a arte de ser dirigente. 15a ed. Rio de Janeiro: Record; 2004.
2. Cecílio LC. Apontamentos teórico-conceituais sobre processos avaliativos considerando as múltiplas dimensões da gestão do cuidado à saúde. Interface Comun Saúde Educ. 2011; 37(15):589-99.
3. Senna MH, Drago LC, Kirchner AR, Santos JL, Erdmann AL, Andrade SR. Meanings of care management built throughout nurses’ professional education. Rev Rene. 2014; 15(2):196-205.
4. Giordani JN, Bisogno SB, Silva LA. Percepção dos enfermeiros frente às atividades gerenciais na assistência ao usuário. Acta Paul Enferm. 2012; 25 (4):511-6.
5. Pereira LA, Primo LS, Tomaschewski-Barlem JG, Barlem EL, Ramos AM, Hirsh CD. Nursing and leadership: perceptions of nurse managers from a hospital in Southern Brazil. Rev Pesq Cuid Fundam. Online, 2015; 7(1):1875-82.
6. Lima RS, Lourenço EB. Os afetos no processo de trabalho gerencial no hospital: as vivências do enfermeiro. Rev Enferm UFSM. 2014; 4(3):478-87.
7. Christovam BP, Porto IS, Oliveira DC. Nursing care management in hospital settings: the bulding of a construct. Rev Esc Enferm USP. 2012; 46(3):734-41.
8. Walker LO, Avant KC. Strategies for theory construction in nursing. 5th ed. New Jersey: Pearson Prentice Hall; 2011.
9. Montezel JH, Peres AM, Bernadino E. Demandas institucionais e demandas do cuidado no gerenciamento de enfermeiros em um pronto socorro. Rev Bras Enferm. 2011; 64(2):348-54.
10. Zambiazi BR, Costa MC. Gerenciamento de enfermagem em unidade de emergência: dificuldades e desafios. Rev RAS. 2013; 55(61):170-6.
11. Santos JL, Pestana AL, Higashi GD, Oliveira RJ, Casstari SS, Erdmann AL. Contexto organizacional e gerência do cuidado pelos enfermeiros em unidades de pronto atendimento. Rev Gaúcha Enferm. 2014; 35(4):58-64.
12. Bueno AB, Bernandes A. Percepção da equipe de enfermagem de um serviço de atendimento pré-hospitalar móvel sobre o gerenciamento de enfermagem. Texto Contexto Enferm. 2010; 19(1):45-53.
13. Azevedo AL, Scarparo AF, Chaves LD. Nurses care and management actions in emergency trauma cases. Invest Educ Enferm. 2013; 31(1):36-43.
14. Strefling IS, Lunardi Filho WD, Kerber NP, Soares MC, Ribeiro JP. Percepções da enfermagem sobre gestão e cuidado no abortamento: estudo qualitativo. Texto Contexto Enferm. 2015; 24(3):784-91.