Embed Size (px)
Citation preview
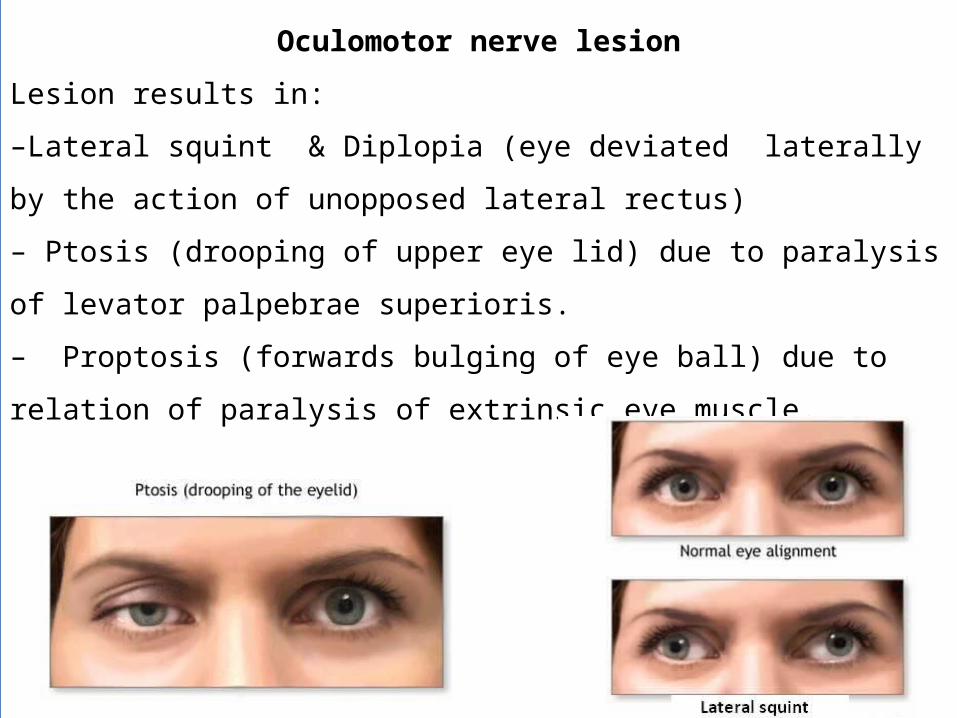
Oculomotor nerve lesion
Lesion results in:
–Lateral squint & Diplopia (eye deviated laterally by the action of unopposed
lateral rectus)
– Ptosis (drooping of upper eye lid) due to paralysis of levator palpebrae
superioris.
– Proptosis (forwards bulging of eye ball) due to relation of paralysis of
extrinsic eye muscle.
-Pupil dilatation & loss of light reflex due to paralysis of constrictor pupillae.
-Loss of accommodation (& convergence) reflex due to paralysis of ciliary
muscle.
- Impaired downward & outward movement of the eye ball on the damaged
side. The preganglionic parasympathetic fibers run superficially in the nerve
and are therefore the first axons to suffer when a nerve is affected by external
pressure. Consequently, the first sign of compression of the occulomotor nerve
is ipsilateral slowness of the pupillary response to light.
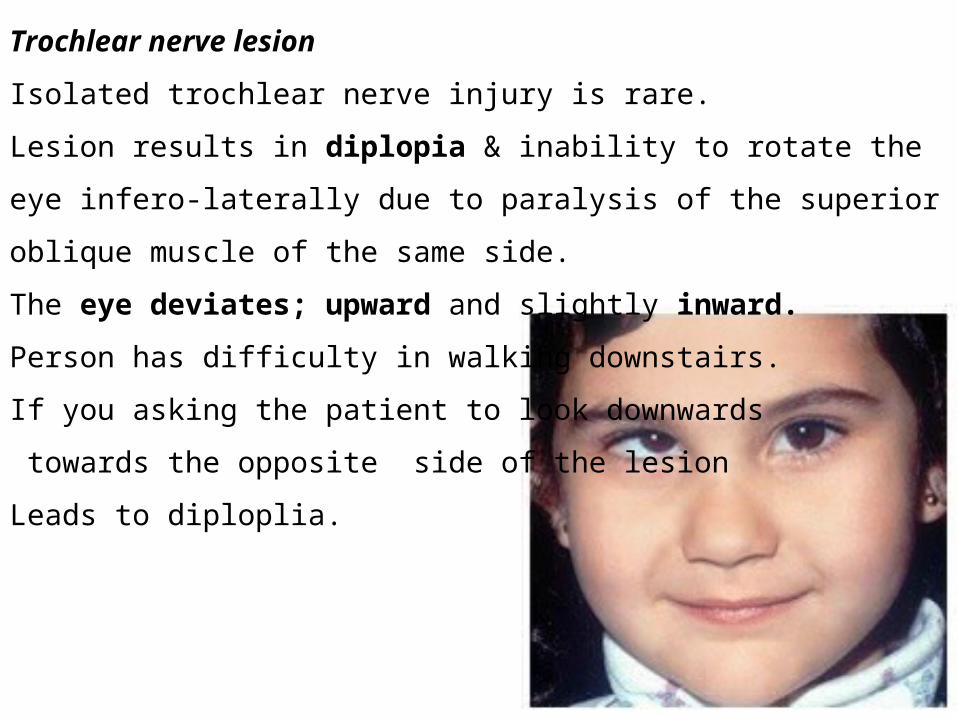
Trochlear nerve lesion
Isolated trochlear nerve injury is rare.
Lesion results in diplopia & inability to rotate the eye infero-laterally due to
paralysis of the superior oblique muscle of the same side.
The eye deviates; upward and slightly inward.
Person has difficulty in walking downstairs.
If you asking the patient to look downwards
towards the opposite side of the lesion
Leads to diploplia.
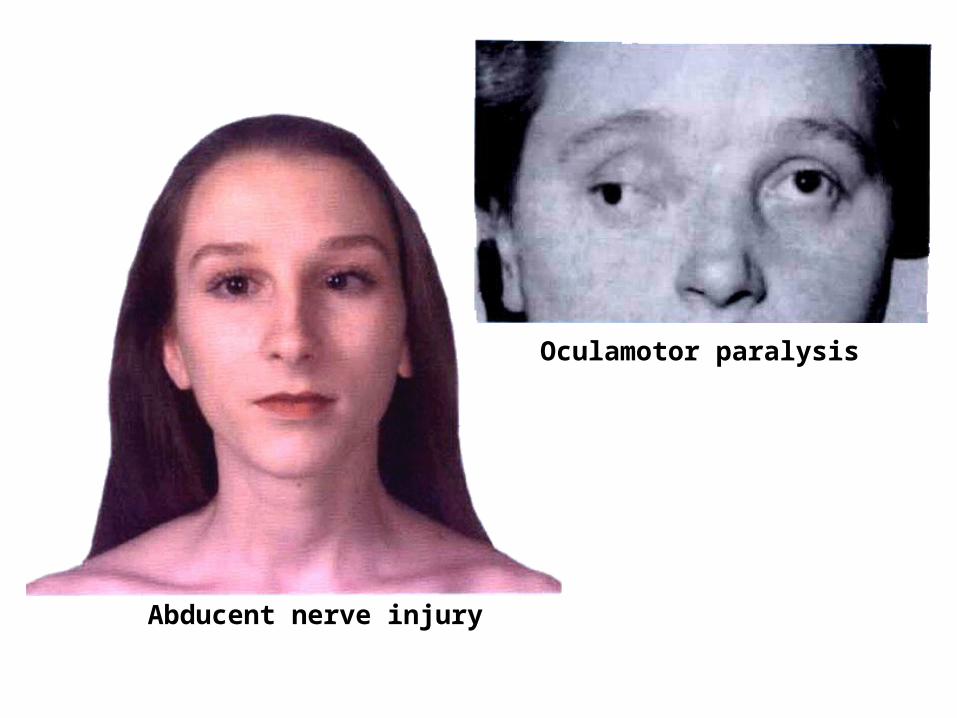
Oculamotor paralysis
Abducent nerve injury
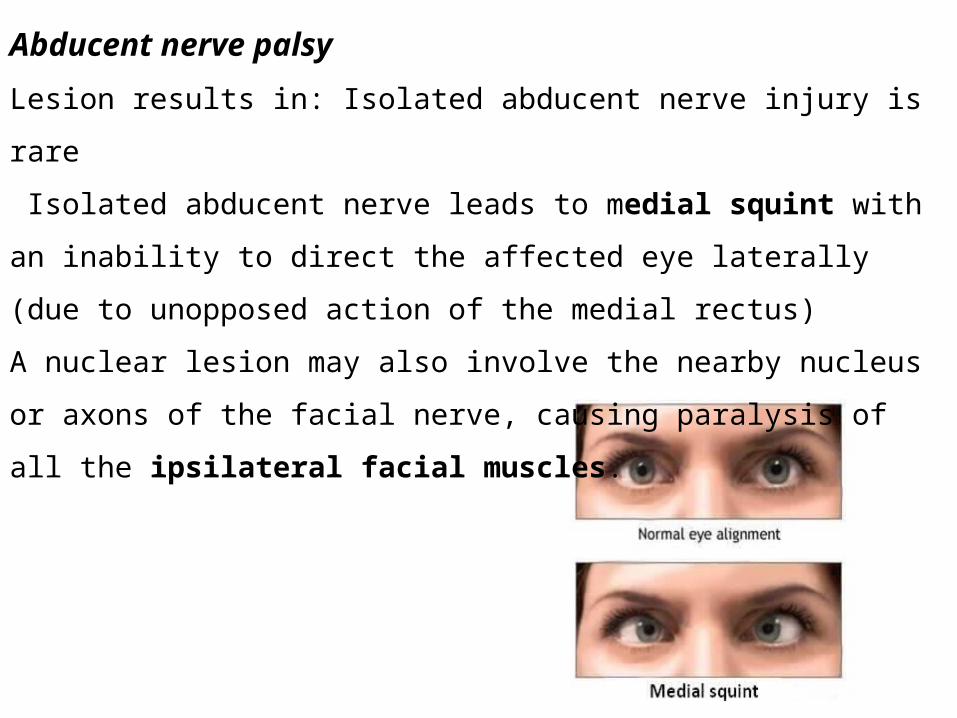
Abducent nerve palsy
Lesion results in: Isolated abducent nerve injury is rare
Isolated abducent nerve leads to medial squint with an inability to direct the
affected eye laterally (due to unopposed action of the medial rectus)
A nuclear lesion may also involve the nearby nucleus or axons of the facial
nerve, causing paralysis of all the ipsilateral facial muscles.
Trigeminal nerve lesion
Complete injury of the trigeminal nerve
1- Paralysis of the ipsilateral muscles of mastication & other muscles supplied
by mandibular nerve.
2- Loss of sensation on the ipsilateral ½ of the face except the area over lateral
½ of the mandible . There is also unilateral loss of sensation of the anterior ½ of
the scalp. Cornea, conjunctiva, mucosa of themouth & anterior 2/3 of the
tongue.
TRIGEMINAL NEURALGIA
Inflammatory condition affecting one or more of the three divisions of
trigeminal nerve. It is characterized by recurring of episodes of intense stabbing
pain, radiating from angle of jaw along a branch of trigeminal nerve. Usually
involves maxillary & mandibular nerves, sparing the ophthalmic division.
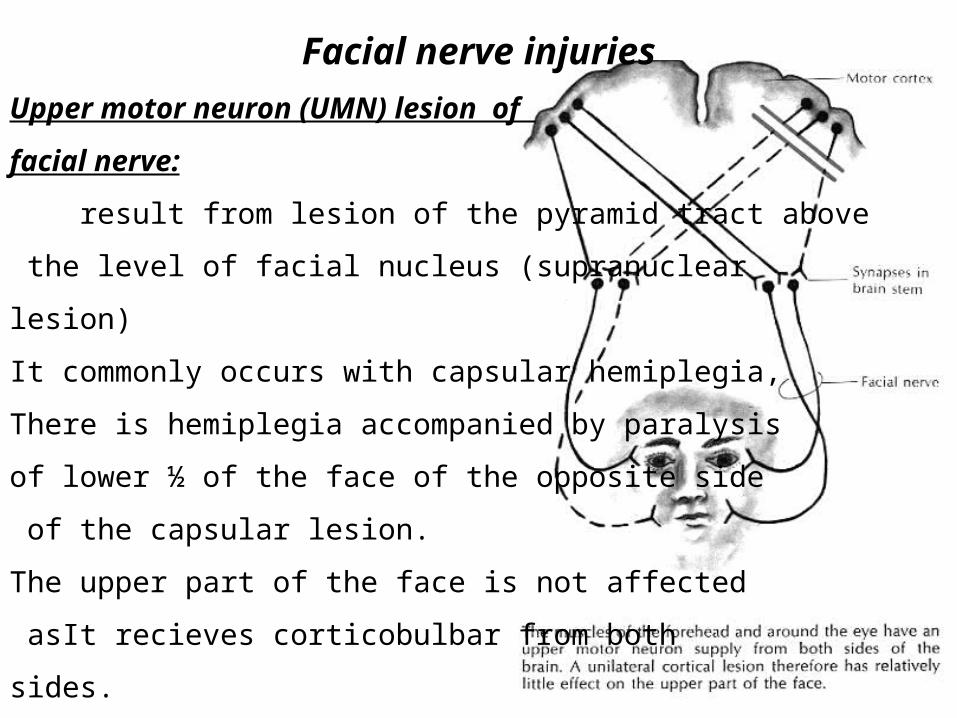
Facial nerve injuries
Upper motor neuron (UMN) lesion of
facial nerve:
result from lesion of the pyramid tract above
the level of facial nucleus (supranuclear
lesion)
It commonly occurs with capsular hemiplegia,
There is hemiplegia accompanied by paralysis
of lower ½ of the face of the opposite side
of the capsular lesion.
The upper part of the face is not affected
asIt recieves corticobulbar from both
sides.
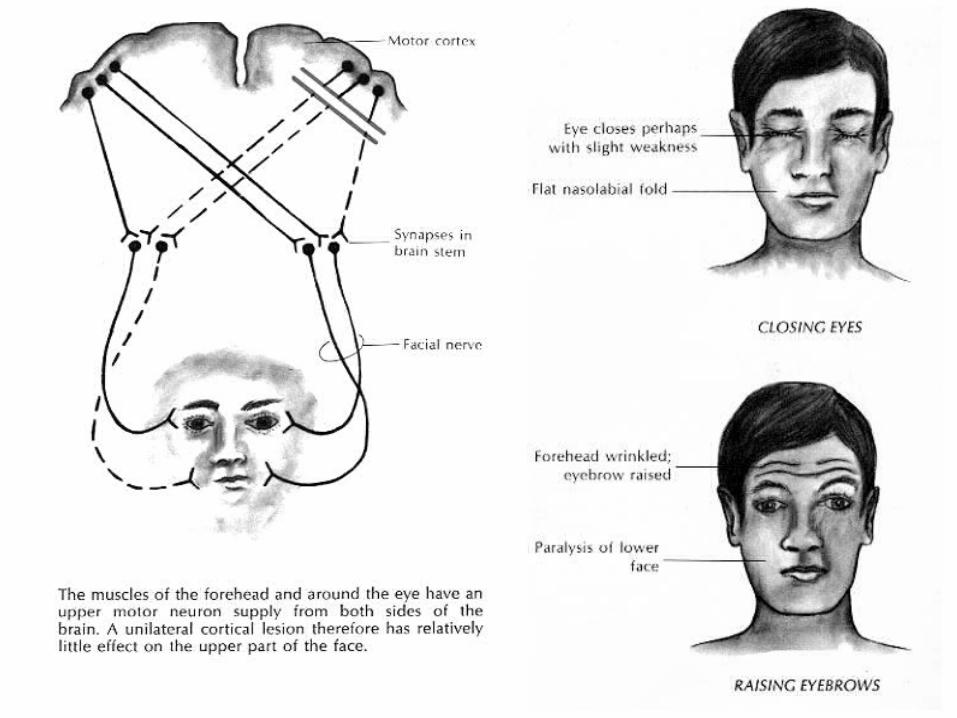
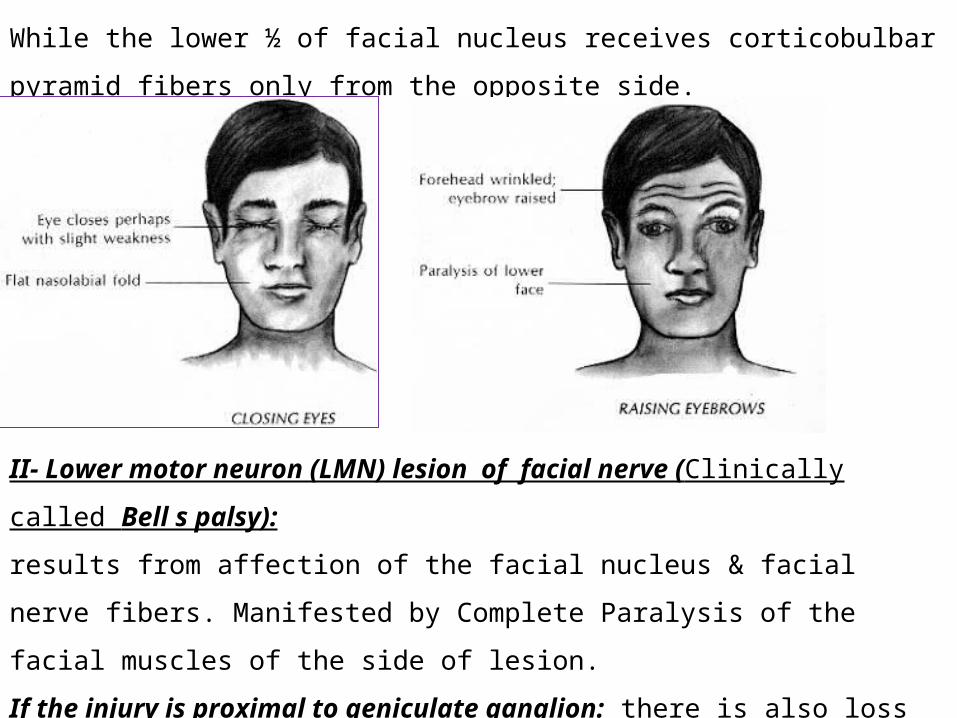
While the lower ½ of facial nucleus receives corticobulbar pyramid fibers only from
the opposite side.
II- Lower motor neuron (LMN) lesion of facial nerve (Clinically called Bell s
palsy):
results from affection of the facial nucleus & facial nerve fibers. Manifested by
Complete Paralysis of the facial muscles of the side of lesion.
If the injury is proximal to geniculate ganglion: there is also loss of secrtion from
lacrimal, nasal, buccal, sunmandibular & sublingual glands in addition to loss of taste
sensation from the anterior 2/3 of the tongue on the affected side.
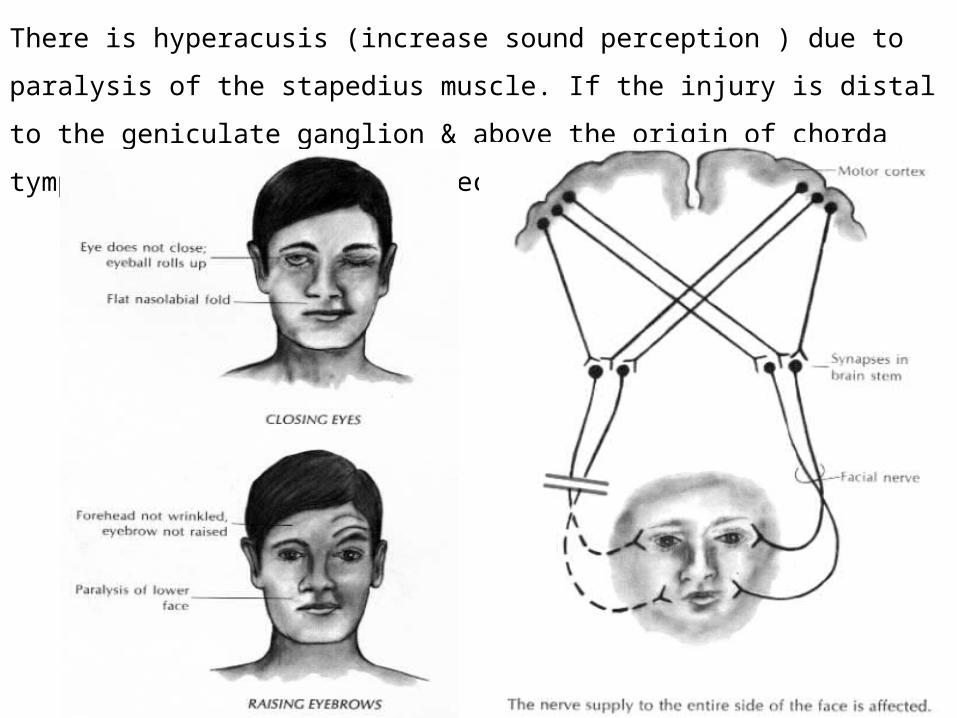
There is hyperacusis (increase sound perception ) due to paralysis of the stapedius
muscle. If the injury is distal to the geniculate ganglion & above the origin of chorda
tympani, glands will not affected.
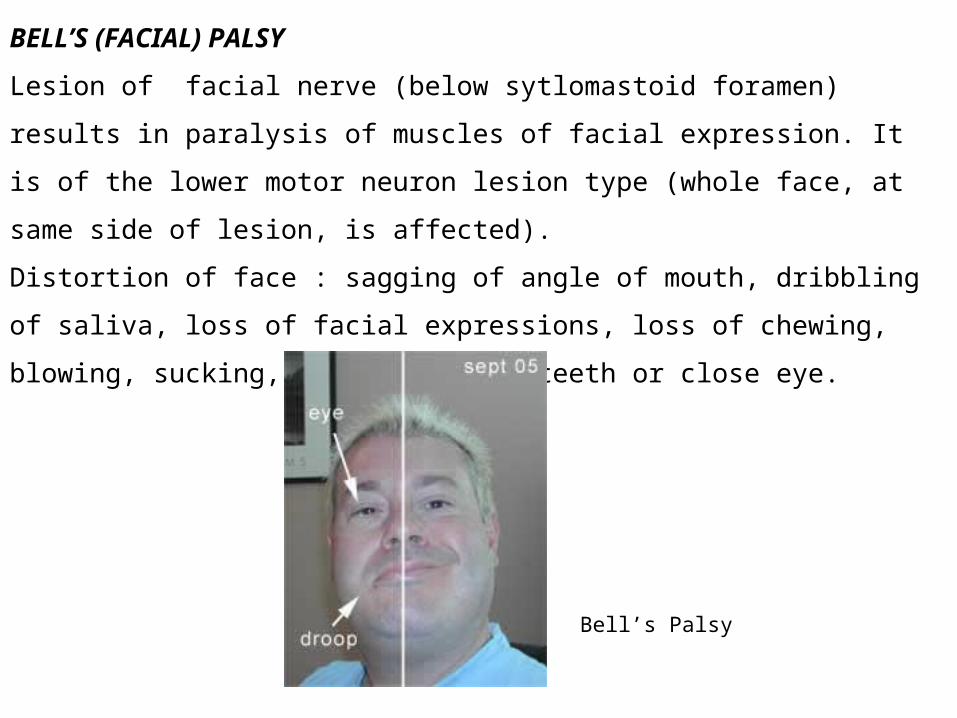
Bell’s Palsy
BELL’S (FACIAL) PALSY
Lesion of facial nerve (below sytlomastoid foramen) results in paralysis of muscles of
facial expression. It is of the lower motor neuron lesion type (whole face, at same side
of lesion, is affected).
Distortion of face : sagging of angle of mouth, dribbling of saliva, loss of facial
expressions, loss of chewing, blowing, sucking, unable to show teeth or close eye.
Vestibular nerve lesion: leads to:
1- Vertigo: in the form of subjective feeling of rotaion of the individual or his
surroundings.
2- Nystagmus: in the form of oscillating jerk movements of the eyes.
3- Nausea & vomiting.
Cochlear nerve lesion:
1- complete loss of hearing of the same side of the lesion.
Lesion of glossopharyngeal nerve Isolated injury of the glossopharyngeal is rare.
But its lesion result in loss of taste & general sensations from the posterior 1/3 of
the tongue (corresponding side), anaesthesia of the pharynx , partial dryness of the
mouth & loss of carotid sinus reflex.
Vagus Nerve Lesion
Unilateral Injury of the vagus nerve at the base of the skull result in paralysis of
the muscles of the pharynx, palate & larynx on the same side, this leads to:
1- Dysphagis 2- Hoarseness of the voice
3- Loss of pharyngeal reflexes on the affected side & uvula deviation to the healthy
side (palatal paralysis).
Bilateral vagus injury at the base of the skull may be fatal as they lead to bilateral
paralysis of the all laryngeal muscles lead to asphyxia unless emergency
tracheostomy is done. Loss of vagal tone lead to tachycardia, dyspnea & loss of
respiratory reflexes .
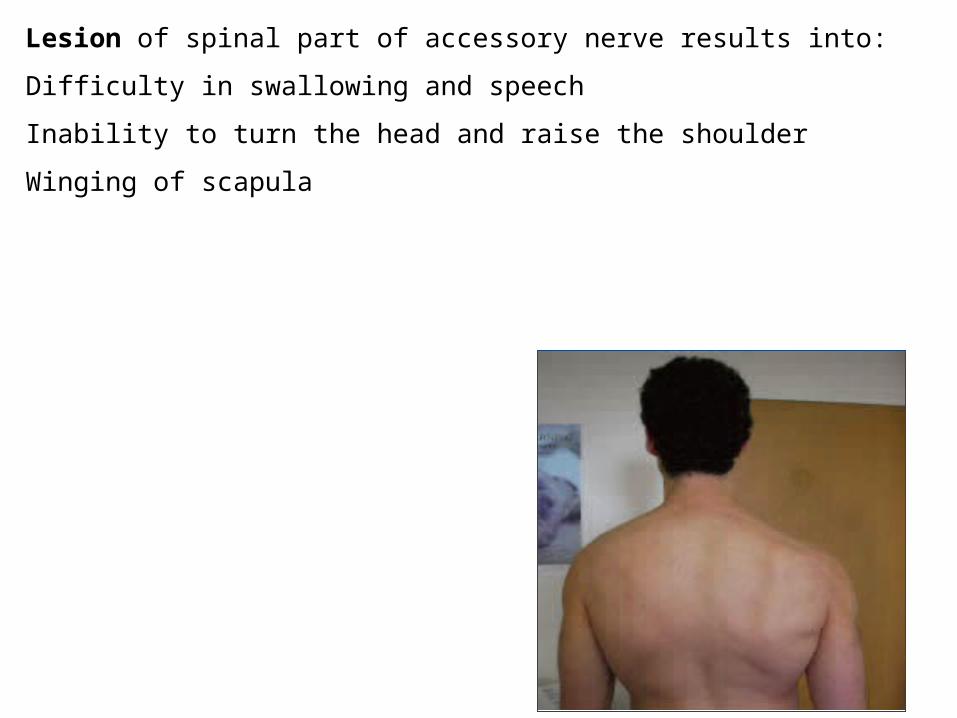
Lesion of spinal part of accessory nerve results into:
Difficulty in swallowing and speech
Inability to turn the head and raise the shoulder
Winging of scapula
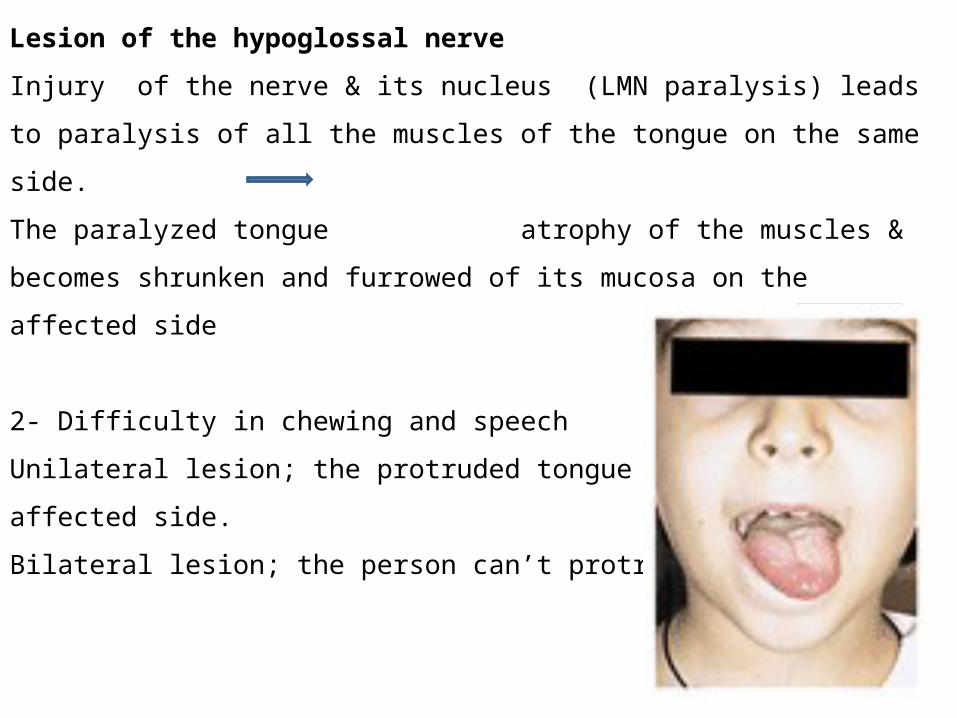
Lesion of the hypoglossal nerve
Injury of the nerve & its nucleus (LMN paralysis) leads to paralysis of all the muscles
of the tongue on the same side.
The paralyzed tongue atrophy of the muscles & becomes shrunken and furrowed
of its mucosa on the affected side
2- Difficulty in chewing and speech
Unilateral lesion; the protruded tongue deviates to the
affected side.
Bilateral lesion; the person can’t protrude the tongue.
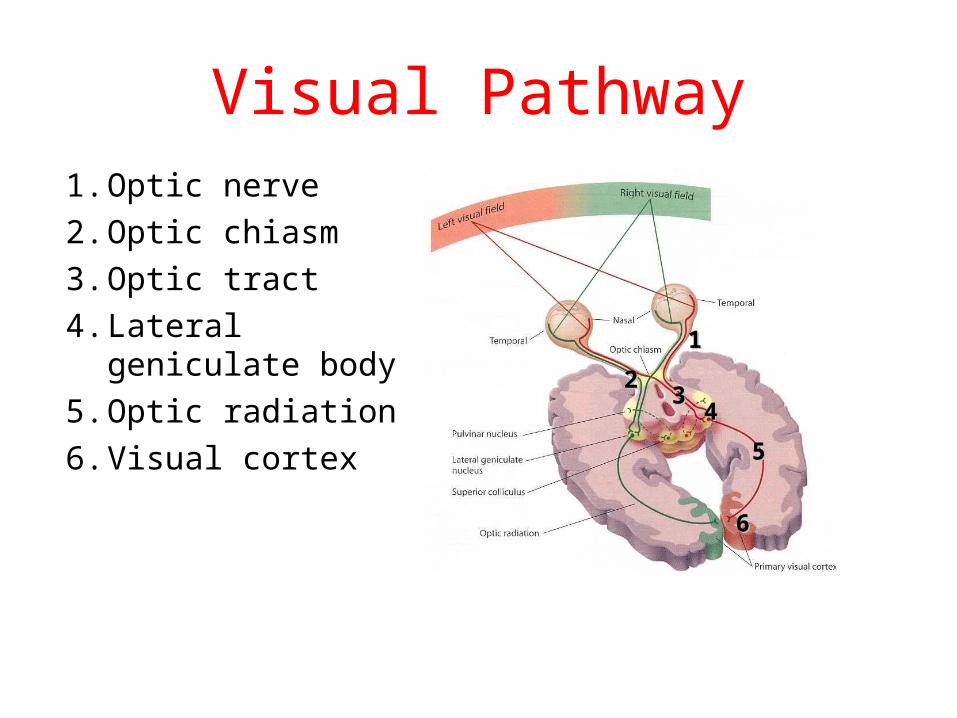
Visual Pathway1. Optic nerve
2. Optic chiasm
3. Optic tract
4. Lateral geniculate body
5. Optic radiation
6. Visual cortex
11
2233
44
55
66
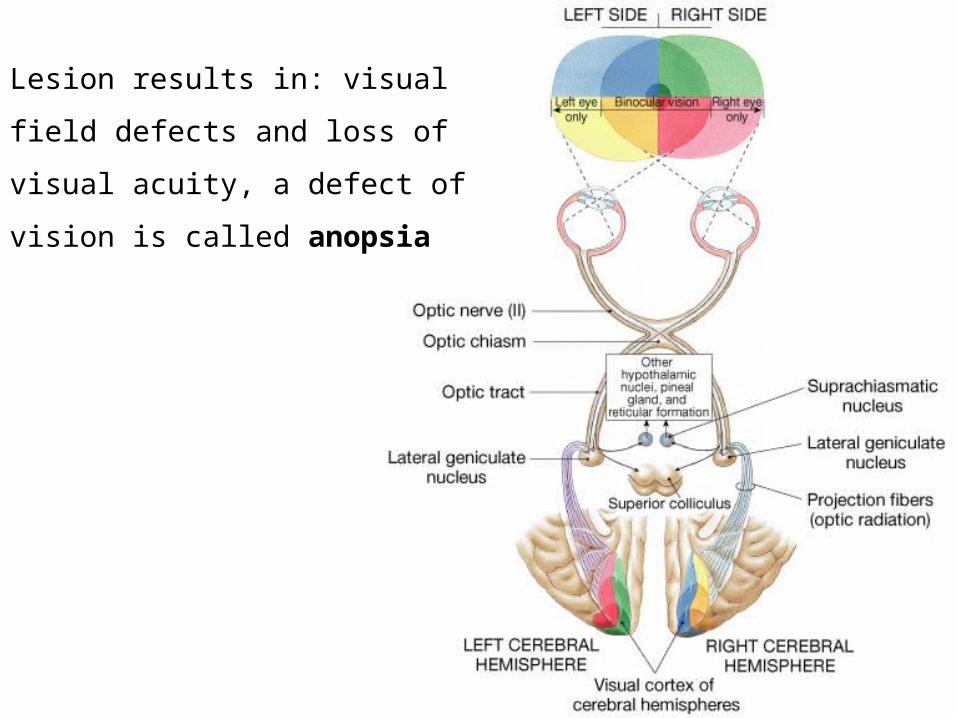
Lesion results in: visual field defects
and loss of visual acuity, a defect of
vision is called anopsia
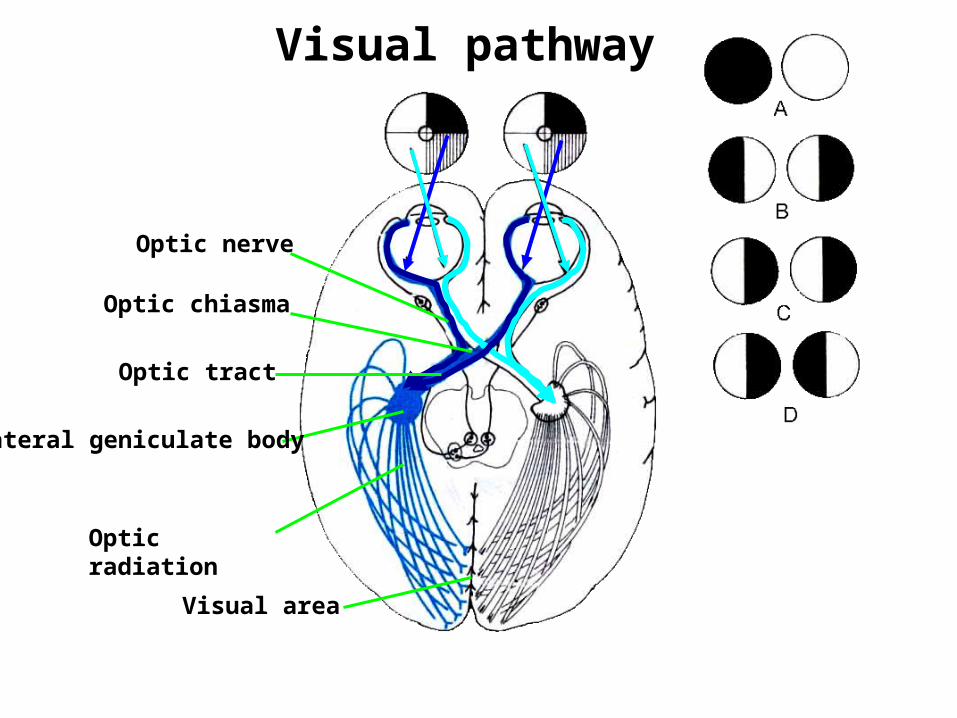
Visual pathway
Optic nerve
Optic chiasma
Optic radiation
Lateral geniculate body
Visual area
Optic tract
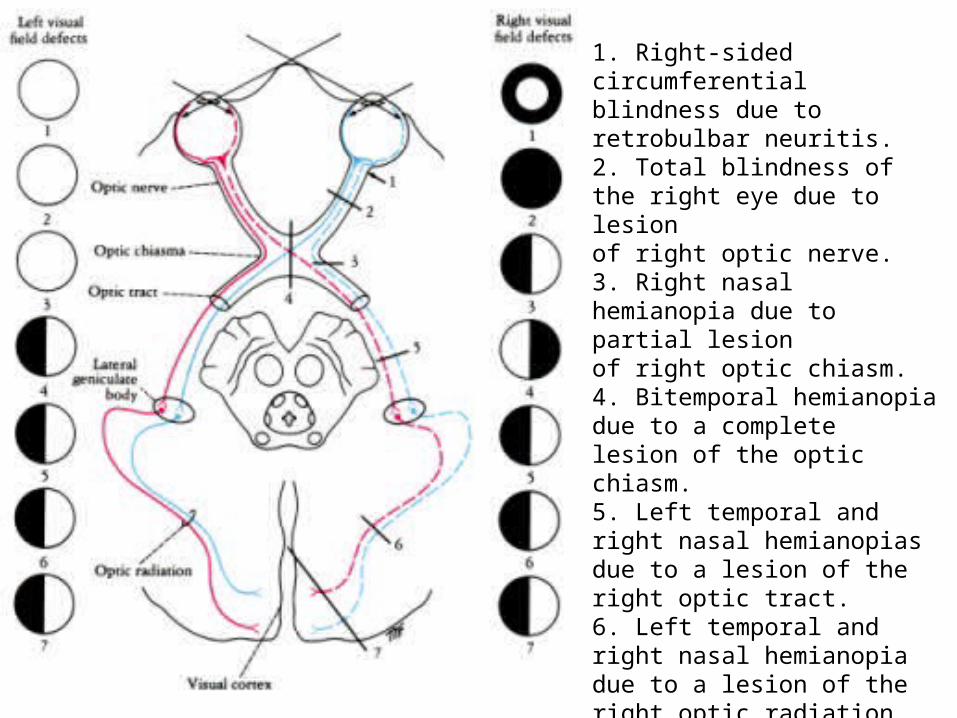
1. Right-sided circumferential blindness due to retrobulbar neuritis.2. Total blindness of the right eye due to lesionof right optic nerve.3. Right nasal hemianopia due to partial lesionof right optic chiasm.4. Bitemporal hemianopia due to a completelesion of the optic chiasm.5. Left temporal and right nasal hemianopiasdue to a lesion of the right optic tract.6. Left temporal and right nasal hemianopiadue to a lesion of the right optic radiation.7. Left temporal and right nasal hemianopia dueto a lesion of the right visual cortex.