Embed Size (px)
Citation preview

NOTES, CASES AND INSTRUMENTS OCULAR SYMPTOMS ARISING FROM INTRACRANIAL ANEU-RYSM OF BOTH VERTEBRAL
ARTERIES* CHARLES NELSON SPRATT, M.D., F.A.C.S.
MINNEAPOLIS
The following case of an aneurysm involving the intracranial portions of both vertebral arteries at the junction with the basilar artery is reported because: first ; the patient's symptoms of double vision caused him first to consult an ophthalmologist, second; from the symptoms, a mistaken diagnosis of brain tumor was made, third; the condition is extremely rare. I have been able to find only one other case in which both
* Read before the Minnesota Academy of Medicine, October 12, 1932.
arteries were involved; reported by Rawes1. Perrig2 has given a complete review of the subject.
In December, 1909, Fred N. aged 47 years, consulted me on account of double vision. He was a strong well-nourished man; reflexes were normal and the general physical condition was negative. He had been well and strong all his life until ten years previous, when he began to have frontal headaches. About a year ago, this pain became localized more in the left occiput. It was constant and dull in character. He had taken headache powders practically every morning for the past ten years. Three months ago, he first had double vision, originally transitory but now constant. It was more marked when looking down. Venereal infection was denied.
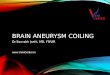
Hocutamotorka
N.triqemirxQ
A.cenb*Ui infjerier anterior
A.carotLs Interna
A.basilari5
Aneurysm of
aa.vertebraks
A.vertebralu
Fig. 1 (Spratt). Intracranial aneurysm arising from both vertebral arteries. 620
NOTES, CASES AND INSTRUMENTS 621
The vision in each eye equalled 6/6 minus. There was diplopia on looking down and to the left. (Patient became dizzy on making a sudden movement.) The left pupil was slightly dilated. Both pupils reacted to light and accommodation, the left being somewhat sluggish. The left optic disc was slightly pale. The retinal veins in each eye were dilated and tortuous. No blurring of the discs or hemorrhages were present.
In April 1910, the headaches had become more severe and constant, especially in the left occiput and parietal region. Vision was normal in each eye, diplopia was more marked. In July 19, 1910, besides the headaches, he had pain in the left eye, in the upper and lower teeth, the tongue and the left side of the head. This was a dull and constant pain and extended to the left occiput. The left external rectus muscle was completely paralyzed. The memory was now failing. He had been nauseated several times and vomited. The left side of the face was anesthetic ; there was partial paralysis of the left side of the face and slight muscle pain. He was unable to detect odors and his sense of taste had diminished. The tongue deviated to the right side. The hearing was equal in both ears, a watch being heard at four inches ; Weber located on the left side ; in walking he tended to fall toward the left. The fields of vision showed concentric contraction. The veins in the left
AN IMPROVED HΦLZER PRIESTLY-SMITH TAPE FOR RAPID AND ACCURATE MEASURE
MENTS OF STRABISMUS M. E. SMUKLER, M.D.
PHILADELPHIA
The Hölzer Priestly-Smith tape is modified as follows : Two silk cords 3/16 inch thick are used instead of tape. One cord is permanently tied on the revolving metal rings fastened to a strabis-mometer and a concave retinoscope.
optic disc were considerably enlarged. There was horizontal nystagmus, especially on looking to the left. The knee jerks were more active on the right side than on the left. Pain was so severe that the patient threatened suicide.
On July 19, 1910, I did a palliative sub-temporal decompression after the method of Cushing. An opening 4 x 6 cm. was made in the bone, and on opening the dura, there was an excess of spinal fluid and bulging of the brain. The veins of the arachnoid were much enlarged. The wound healed per primum and the patient had considerable relief from the pain. This was only temporary and on August 12, 1910, I made a cross bow incision after the method of Cushing so as to expose the cerebellum. There was much bulging of the dura and the vessels were much injected. On incising the dura, a large quantity of fluid spurted out. The arachnoid was edema-tous. The patient died suddenly on the table. An autopsy was performed, and on lifting the brain from its bed, it was found that the vertebral arteries, at the junction of the baselar were much enlarged on each side, the width of the aneurysm being 3.5 cm. by 5 cm. The appearance of the sac resembled much the hind quarters of a fat pig. The baselar internal carotids communicating, were enlarged and convulated, but not a part of the aneurysm.
1231 Medical Arts building.
The other cord has one end attached to the revolving ring on the strabismom-eter and the other end attached to a finger ring, through which passes the. measuring tape that is fastened to the ring on the retinoscope. Each cord is long enough to make the distance between the strabismometer and the retinoscope 60 cm., and between the strabismometer and the finger ring 60 cm.
The weight of the metal box containing the measuring tape is just sufficient to hold the tape taut and easy to ma-
References ' Rawes. Double aneurysm of the vertebral arteries. Trans. Hunterian Society, 1899-1900,
p. 77. "Perrig, Hans. Zur Anatomie Klinik und Therapie der Verletzungen und Aneurysmen
der Arterie Vertebralis. Bruns Beiträge zur klin. Chirurgie. 1931, Dec, v. 1S4, pt. 2, p. 262.












![DISSECTING ANEURYSM OF THE INTRACRANIAL VERTEBRAL …neurosurgery.dergisi.org/pdf/pdf_JTN_159.pdf · vertebral artery dissection. J Neurosurg 72:964-967. 1990 16. Sato O. Bascom]F,](https://img.pdfslide.us/doc/110x75/5f8d3e5128453d7acf5ec547/dissecting-aneurysm-of-the-intracranial-vertebral-vertebral-artery-dissection-j.jpg)