Embed Size (px)
Citation preview

401
Ann. N.Y. Acad. Sci. 956: 401–404 (2002). © 2002 New York Academy of Sciences.
Ocular Motor Myotonic Phenomenon in Myotonic Dystrophy
MAURIZIO VERSINO,a,b SILVIA COLNAGHI,b GIORGIO SANDRINI,a,b AND VITTORIO COSIa,b aFondazione Istituto Neurologico C. Mondino, IRCCS, Pavia, ItalybDipartimento di Scienze Neurologiche Università di Pavia, Pavia, Italy
Keywords: myotonic dystrophy; extraocular myotonia; warming-up phenomenon; ocular motor myotonic phenomenon
INTRODUCTION
Myotonic dystrophy (MyD) is an autosomal dominant multisystem disorder inwhich skeletal muscles may present dystrophic changes and a delay in muscle relax-ation after contraction. This delay is the defining feature of the myotonic phenome-non, or myotonia.1,2 Several and repetitive muscle contractions may momentarilyreduce myotonia in the given muscle, and this has been called the warm-up phenom-enon.3 Although myotonic discharges are electromyographically detectable in ex-traocular muscles,4 to our knowledge only one case report has addressed thequestion of the possible occurrence of extraocular myotonia.5 The aim of the presentreport is to demonstrate that saccadic abnormalities may be related both to the ex-traocular myotonia and to the warming-up phenomenon.
MATERIALS AND METHODS
The study enlisted twenty MyD patients, 10 patients suffering from multiple scle-rosis (MS) and 10 controls (Ctrl). All subjects showed visual acuity above 7/10 inboth eyes, and none of them presented with clinically evident ocular motor signs. Weincluded the MS group because their ocular motor abnormalities are attributable toa CNS rather than to an extraocular muscle dysfunction. Using scleral search coiltechnique (Skalar 3010 system), we recorded monocularly visually guided saccadiceye movements simultaneously from both eyes in binocular vision after the signalhad been calibrated monocularly in monocular vision.
We used two different target displacements, that is, small (± 25 degrees to prima-ry position) and large (50 degrees, back and forth from +25 to −25 degrees), and twodifferent interstimulus intervals (ISIs), that is, short (1 second) and long (5 seconds).
Address for correspondence: Maurizio Versino, M.D., Dipartimento Scienze NeurologicheUniversità di Pavia, Fondazione Istituto Neurologico C. Mondino, IRCCS, Via Palestro 3, 27100Pavia, Italy. Voice: +39 0382 380340; fax: +39 0382 380286.

402 ANNALS NEW YORK ACADEMY OF SCIENCES
For each subject, for each eye, for each paradigm, and for each saccade direction,we computed the mean value, the duration, the peak velocity and skewness of the ve-locity profile, namely, the ratio of the duration of the acceleration period to the du-ration of the deceleration period. All the parameters were divided by the actual eyedisplacement (amplitude) values.
We hypothesized that short but not long ISIs would promote the warming-up phe-nomenon. Accordingly, for each subject and for each eye parameter, we computedthe difference between short and long ISIs for corresponding parameters divided bythe average of the two values. Finally, since the myotonic phenomenon is likely toinvolve the extraocular muscles on an individual basis, for each subject we consid-ered the largest (as an absolute value) ISI difference with its sign among the fouravailable (two eyes and two saccade directions) for each small- and large-amplitudeparadigm.
RESULTS
The maximal short–long ISI difference mean values for saccade duration were in-variably negative, that is, durations were greater for long than for short ISIs. The meanvalues for the three groups were significantly different both for small (F2,37 = 3.33, p= 0.047) and for large (F2,37 = 7.32, p = 0.002) amplitudes, and contrast analysisshowed that MyD mean value was larger than those of the MS (contrast 1: t37 = 2.13and p = 0.04 for small saccades; t37 = 2.21 and p = 0.034 for large saccades) and ofthe Ctrl (contrast 2: t37 = 2.1 and p = 0.045 for small saccades; t37 = 3.68 and p =0.001 for large saccades) groups for both target displacements.
The maximal short–long ISI difference mean values for saccade skewness werenegative. In other words, acceleration duration was greater than the deceleration du-ration for long ISIs than it was for short ISIs: in the MyD group, this was the caseboth for small and for large target displacements, while in the MS group, it was thecase for large but not for small saccades; moreover the skewness maximal differenc-es were positive in the control group. The mean values for the three groups differedsignificantly for small (F2,37 = 6.94, p = 0.003) but not for large (F2,37 = 2.59, p =0.089) amplitudes. For small target displacements, contrast analysis showed that theMyD mean value was higher than those of the MS (contrast 1: t37 = 3.19 and p =0.03) and of the Ctrl groups (contrast 2: t37 = 2.88 and p = 0.007).
The maximal short–long ISI difference mean values for saccade peak velocitywere invariably positive, that is, peak velocities were usually higher for short thanfor long ISIs. The mean values for the three groups did not differ significantly eitherfor small (F2,37 = 0.68, p = 0.513) or for large (F2,37 = 2.45, p = 0.1) amplitudes.
We compared the MyD and the MS groups for differences in abnormal individualmaximal short–long ISIs. Any individual value was considered to be abnormal if itexceeded the mean ±2 standard deviations of the control groups. MyD patientsshowed a greater occurrence of abnormal duration (for small amplitudes only: 60%vs. 20%, p = 0.045) and of abnormal skewness (for small amplitudes only: 55% vs.0%, p = 0.003), but not of abnormal peak velocity.

403VERSINO et al.: MYOTONIC DYSTROPHY
DISCUSSION
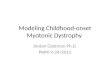
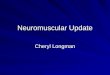
Our findings showed that saccade duration and skewness were influenced by thethe inter-stimulus interval. In the MyD patients, prolongation of the stimulus inter-val led to an increase in saccade duration, without significant modification in sac-cade peak velocity, and to a reduction in saccade skewness; this latter derived froman increase in the acceleration duration with respect to the deceleration duration(FIG. 1)6. These modifications were more significant for small than for large targetdisplacements, and were larger, and occurred more frequently, in the MyD than in
FIGURE 1. A and B show the velocity (thinner lines) and the position profile (thickerlines) of a leftward centripetal saccade to primary position after the 25 degrees position hasbeen kept for 1 sec (short ISI: dotted lines) or for 5 sec (long ISI: continuous lines). A showsa control subject, whereas B shows a patient suffering from myotonic dystrophy. The patientmakes a saccade which is slower than that of the control subject with both ISIs. In the con-trol subject, both the saccadic duration and the velocity profile are not significantly modi-fied by the difference in ISI, although the peak velocity is slightly lower for long than forshort ISIs. In contrast, the patient’s saccade reaches the same peak velocity with both ISIs,but with the long ISI the saccade lasts longer; this effect is due to a prolongation of accel-eration period, which increases the skewness of the velocity profile. These same points areshown in C and D, where saccade velocity is plotted against eye position, starting from 25degrees to primary position (0 degrees) during the same respective saccades shown in A andB. The control subject (C) shows the same profile for both ISIs. In contrast, the patient (D)shows a longer acceleration period for long (continuous line) than for short (dotted line) ISI.Note that this does not hold true for corrective saccades. (From Versino et al.6 Reprintedwith permission from the Journal of Neurology, Neurosurgery & Psychiatry.)

404 ANNALS NEW YORK ACADEMY OF SCIENCES
the control or the MS groups. Taken together, these findings may be presumed toderive from a delay in de-contracting an extraocular muscle after fixation, in orderto make a saccade in the off-direction for that muscle (for instance: a delay in de-contracting the right lateral rectus to make a leftward saccade starting from a right-ward orbital position).
Moreover, the fact that the delay described here occurs more frequently the MyDthan in the MS group suggests that this phenomenon likely derives from ocular mus-cle rather than from CNS dysfunction; we hypothesize that the delay may be consid-ered an ocular motor myotonic phenomenon, although we cannot exclude amyopathic origin.
REFERENCES
1. MORGENLANDER, J.C & J.M. MASSEY. 1991. Myotonic dystrophy. Semin. Neurol. 11:236–243.
2. THORNTON, C. 1999. The myotonic dystrophies. Semin. Neurol. 19: 25–33.3. COOPER, R.G. et al. 1988. Physiological characterisation of the “warm up” effect of
activity in patients with myotonic dystrophy. J. Neurol. Neurosurg. Psychiatry51:1134–1141.
4. DAVIDSON, S.I. 1961. The eye in dystrophia myotonica with a report on electromyo-graphy of the extra-ocular muscles. Br. J. Ophthalmol. 45:183–196.
5. HANSEN, H.C. et al. 1993. Evidence for the occurrence of myotonia in the extraocularmusculature in patients with dystrophia myotonica. Neuro-ophthalmology 13:17–24.
6. VERSINO, M., B. ROSSI, G. BELTRAMI, et al. 2002. Ocular motor myotonic phenome-non in myotonic dystrophy. J. Neurol. Neurosurg. Psychiatry 72: 236–240.