Embed Size (px)
DESCRIPTION
Ocular Manifestations of Systemic Diseases. Dalman. Dysthyroid Orbitopathy. autoimmune disorder usually associated with Graves' disease 10-25% euthyroid extra-ocular muscles are the target of the autoimmune attack restrictive ophthalmoplegia and proptosis Cardinal Signs - PowerPoint PPT Presentation
Citation preview

Ocular Manifestations of Systemic Diseases
Dalman

Dysthyroid Orbitopathy
• autoimmune disorder usually associated with Graves' disease
• 10-25% euthyroid• extra-ocular muscles are the target of the
autoimmune attack restrictive ophthalmoplegia and proptosis
• Cardinal Signs– upper eyelid retraction and lag, conjunctival injection
and chemosis, and periorbital edema.

Dysthyroid Orbitopathy
• Pathophysiology– antibody-mediated reaction against the TSH
receptor with orbital fibroblast modulation of T-cell lymphocytes

Dysthyroid Orbitopathy
• Pathophysiology
T- cells Thyroid cells inflammation
cytokines mucopolysaccharides
Orbital fibroblast
EOM edema
Hyperosmotic shift

Dysthyroid Orbitopathy
• Pathophysiology
Preadipocyte fibroblasts adipocytes
Inc. orbital volume Inc. fat proptosis
edema Tissue damage and fibrosis
lagophthalmos
EO motility restriction


Dysthyroid Orbitopathy

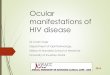
Dysthyroid Orbitopathy


Dysthyroid Orbitopathy

Dysthyroid Orbitopathy
• Management– self-limited (over 1 year)– No immediate cure available

Dysthyroid Orbitopathy
• Management– Orbital radiation
• moderate-to-severe inflammatory symptoms, diplopia, and visual loss in patients with TAO
– Optic nerve compression• High-dose steroids (proceed to surgery if unresponsive)
– Surgical• Orbital decompression• Strabismus surgery• Lid lengthening • Blepharoplasty

Occular Changes in Hypertension
• Damage to the retina caused by high blood pressure
• 3 manifestations– Hypertensive retinopathy– Hypertensive optic neuropathy– Hypertensive choroidopathy

Occular Changes in Hypertension
• Pathophysiology– Retinal microvasculature
Inc BPHyperoxic &
hypercapneic stress
Bifurcation angles and retinal arteriolar diameters show Dec
vascular reactivity
Disadvantageous branching geometry in retinal vasculature

Occular Changes in Hypertension
• Pathophysiology– Dynamics of ocular blood flow
Inc BP
Hypertensive arterial changes
Breakdown of autoregulation
Inc resistance to optic nerve head
blood flow

Occular Changes in Hypertension
• Pathophysiology– Different manifestations because• Acute HTN disrupts blood-retinal barriers• Retinal and optic nerve head vascular beds have
autoregulation (choroidal has none)• Choroidal vessels has no blood-ocular barrier• Retinal vessels (no autonomic nerve supply)• Choroidal vessels (richly supplied by both sympathetic
and parasympathetic nerves)

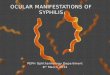
Hypertensive Retinopathy
• Represents target-organ damage

Grade II

Grade III

Grade IV

Hypertensive Retinopathy
• Clinical features– Vasoconstriction – Fundus
• focal and generalised arteriolar narrowing, microaneurysms, intraretinal hemorrhages, cotton-wool spots, hard exudates, optic disc swelling• 2o to arteriolosclerosis arteriovenous nipping• Flame-shaped hemorrhages (abnormal vascular
permeability)• Macular star (lipid deposition around the fovea)• Disc swelling (minimal microvascular change)



• Cotton-wool spots


Hypertensive Retinopathy
• Clinical features– Vasoconstriction – Fundus• Untreated hypertension hemorrhagic detachment of
retina and vitreous hemorrhage


Hypertensive Retinopathy
• Clinical features– Vasoconstriction – Fundus– Secondary arteriosclerosis• Bonnet’s sign - banking of the venule distal to the
crossing• Gunn’s sign - nipping of the blood column• Salus’ sign - displacement of the venule at right angles
to the arteriole

Hypertensive Retinopathy
• Gunn’s sign and Bonnet’s sign

Hypertensive Retinopathy
• Focal arterial narrowing of the retina

Hypertensive Optic Neuropathy
• Papilloedema or bilateral disc swelling– Grade IV hypertensive retinopathy– Poor prognostic sign– Other causes like space-occupying lesions and
benign intracranial HTN should be excluded– Theories on the pathophysiology• Ischemia and raised ICP as a part of hypertensive
retinopathy/enchephalopathy

Hypertensive Optic Neuropathy
• Usually resolve following control of BP, but some might develop disc pallor
• Longstanding uncontrolled HTN retinal nerve fiber loss

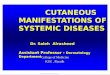
Hypertensive Choroidopathy
• Less well recognized than retinopathy• Commonly described features:– Choroidal vascular sclerosis– Elschnig spots – focal areas of degenerative retinal
pigment epithelium– Siegrist’s streaks – linear pigment epithelial
changes• poor prognosis

Hypertensive Choroidopathy
• Elschnig spots

Management
• Control hypertension• Grade I and II– Non-urgent referral
• Grade III– More urgent referral to the GP
• Grade IV– Patient is in medical crisis. Patient needs immediate
referral to a hospital eye casualty department