Embed Size (px)
Citation preview

British Journal ofOphthalmology, 1983, 67, 493-503
Ocular manifestations of Alport's syndrome:a hereditary disorder of basement membranes?*J. A. A. GOVAN
From the Department of Ophthalmology, Guy's Hospital, London SE]
SUMMARY The ocular manifestations in 16 patients with Alport's syndrome were lenticonus andretinal flecks in the macula and mid periphery. These 3 features appear to be specific for thissyndrome and are a considerable aid to diagnosis. Lens opacities are common, and other ocularabnormalities occur sporadically. The present evidence indicates that this is a hereditary,widespread disorder of basement membrane, and it is suggested that ophthalmologists maycontribute to the further understanding of it by directing attention towards analysis of the lenscapsule after cataract extraction. The similarity of the retinopathy to that of fundus albipunctatus isnoted, and it is suggested that the latter condition should not be diagnosed in the absence of renalinvestigation and audiometry.
Alport's syndrome"3 is clinically characterised by thefamilial occurrence of progressive, haematuricnephritis and sensorineural deafness in which therenal prognosis is better in female patients. Ocularfeatures most frequently described include lensabnormalities4 characterised by lenticonus37 andcataract, central and midperipheral retinal flecks,8'7and comeal arcus.67 'F18 Most previous ophthalmicreports have tended to concentrate on an isolatedocular manifestation of this syndrome.
This paper describes the detailed ocular findings in16 patients who have been treated in the RenalDepartments at Guy's Hospital and attempts todifferentiate the nonspecific from the specific ocularfeatures that occur in this syndrome.
Patients and methods (Table 1)
The diagnosis of Alport's syndrome was based on thepresence of chronic renal failure and the presence ofbilateral sensorineural deafness which in most caseswas confirmed by audiometry. Twelve patients had apositive family history of renal disease, and all casesexcept 2 (patients 5 and 11) had suffered from hyper-tension in the past, which was controlled at the time ofexamination. The average age at examination was 24years (range 16-39 years), and the average age at*Presented in part at the 24th International Congress of Ophthal-mology, 1982, San Francisco. Correspondence to Mr J. A. A. Govan.
which renal failure necessitated maintenance dialysisor renal transplantation supervened (13/16 patients)was 21 years (range 13-35 years). Nine of thesepatients at the time of examination had a renal trans-plant which had been successfully functioning for anaverage 4 years (range 6/12-7 years), whereas theremaining 4 were on maintenance dialysis. All exceptone of the latter group had renal transplants whichwere either successful or had subsequently rejected,and consequently 12 of the whole group had been onimmunosuppressives and systemic steroids in the past.One patient had associated macrothrombocytopenia.19
Ocular examination included subjective andobjective refraction with best visual acuity and bio-microscopy of the anterior segment. The posteriorsegment was studied by both indirect ophthalmoscopyand by biomicroscopy with a fundus contact lens.Fundus photography was undertaken in 12 patientsand fluorescein angiography in 7 selected cases. Anelectroretinogram (ERG) was recorded in both lightand dark adapted states using skin electrodes in 5patients with a flash intensity of 0-2 Joules and arecording band width of 1 to 100 Hz. An electro-oculogram (EOG) was recorded in 4 patients afterdark adaptation and during light adaptation to obtainmaximum light: minimum dark ratios. Serum tri-glycerides, cholesterol, vitamin A and plasma aminoacid levels were measured after an overnightfast.
493
on July 17, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.67.8.493 on 1 August 1983. D
ownloaded from

Table I Ocularfeatures and serum vitamin A levels
Patient Age (yr) Sex Renal status Familt' Corrected visual Corneal arcus Lenticonushistory acuitv + = Microscopic + + = Definite
at at renal + + = Macroscopic + = Probableexamination failure OD OS
1 221 21 M Dialysis + 6/9 6/12 -2 30 22 M Failed + 6/5 6/5 + + +
transplant- Dialysis
3 33 22 M Functioning + 6/9 6/9 + + +transplant
4 28 22 M Functioning + 6/9 6/9 + + +transplant
5 16 - M - + 6/9 6/9 +6 33 29 M Functioning + 6/6 6/6 + + + +
transplant7 18 - M - + 6/12 6/9 -
8 20 13 M Functioning - 6/9 6/9 + + + +transplant
9 19 - F - + 6/9 6/9 - ++10 14 14 M Functioning - 6/9 6/6
Transplant11 39 35 M Functioning ? 6/24 6/9 +
transplant
12 16 14 M Functioning + 6/9 6/9transplant
13 19 14 M Failed + 6/9 6/18 - ++transplant- Dialysis
14 34 32 M Failed + 6/6 6/6 + +transplant- Dialysis
15 24 20 M Functioning + 6/12 6/9transplant
16 20 13 M Functioning - 6/6 6/9 + + +
transplant
*Upper limit of normal=0-7 mg/I.Results (Table 1)
VISUAL ACUITYThe visual acuities were generally compatible withthe degree of lens opacity present, though 5 of the 6patients with clear ocular media had slightly reducedcorrected vision (6/9-6/12). Although 3 of thesepatients had lenticonus, in none of the 5 patients didthe acuity improve with a pinhole. Five patients hadmyopia (>2 00 D), and 3 of these and 5 other patientshad myopic astigmatism (>2O00 D). One patient hadhypermetropic astigmatism (>2.00 D). Theserefractions were bilateral and tended to besymmetrical. One patient had a strabismic amblyopiceye. No history of definite night blindness waselicited, though every patient was specificallyquestioned.
CORNEANine out of 16 patients, who were on average 9 4years older than the remaining patients, had a
bilateral symmetrical corneal arcus tending to sparethe interpalpebral region. This was well defined in 7patients but visible only microscopically in 2 patients.One patient (patient 11) had a definite bilateralincrease of the normal comeal stromal granularappearance.
LENSAnterior lenticonus was diagnosed by the character-istic anterior axial projection of the central 3-4mm ofthe lens seen on biomicroscopy and the 'oil droplet'appearance of the red reflex. Two patients (patients 8and 13) satisfied both these criteria, one ofwhom hadan abnormal shagreen of the central anterior lenscapsule bilaterally. Four patients (patients 2, 3, 4, and16) displayed only the oil droplet appearance, whichwas in one patient (patient 2) apparent only onoblique viewing, and 2 patients (patients 6 and 9) haddefinite biomicroscopic evidence of anteriorlenticonus with the oil droplet appearance evidentonly on oblique viewing. In each case the appearance
J. A. A. Govan494
on July 17, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.67.8.493 on 1 August 1983. D
ownloaded from

Ocular manifestations ofAlport's syndrome: a hereditary disorder ofbasementmembranes?
Cataract Macular Mid peripheral ERG EOG Fundus Vitamin A Commentflecks flecks photography levels
(mg/l)*
-- - - 1-1 Preretinal membranePost. + - Colours 1-0polar only >:~BrothersCortical - + + Colours 0-8
only++ + + Colours + -
fluoresceinLamellar + - - 09Ant. subcaps. + + + + Normal Normal Colours + 0 9 Preretinal membranecortical fluorescein
+ - Colours + -
fluoresceinPost. ++ + Colours 1-3subcapsular - - only
+ + Colours 1.0only
Post. + ant. - + + Nornal Colours + 1-1 AmblyopicODsubcapsular fluoresceinDotPost. + - Normal Normal Colours + - )subcapsular fluoresceinCorticalPost. + ant. Colours + 0-8 Half-brothers, anisocoriasubcapsular fluoresceinDotJ
Post. + - Normal Normal Colours + 0 9 Macrothrombocytopeniasubcapsular fluoresceinPost. + + ++ Normal Normal Colours 1-1subcapsular only
was identical on both sides, and no case of trueposterior lenticonus was seen. Four of this group(patients 2, 3, 4, and 13) had noticed that their visionwas blurred in bright sunlight, whereas one patient(patient 8) complained that his vision was blurred forabout 10 minutes after awakening each morning.Four patients had symptoms of myopia, which hadgradually progressed in one patient over 16 years, andone patient (patient 6) had bilateral unioculardiplopia which was correctable with lenses.Ten patients displayed lens opacities. Six patients,
all ofwhom had been on systemic steroids in the past,had posterior subcapsular lens opacities. Other lensopacities included anterior axial subcapsular,posterior polar, and anterior and posterior axialcortical opacities, and one patient had bilaterallamellar lens opacities of 6-2 mm diameter in whichthe posterior lamellar opacity bowed posteriorlyaxially in what has been called an internallenticonus.20 Also seen were anterior and posteriorsubcapsular vacuolation and blue dot opacities.
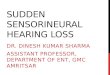
FUNDIFlecks were seen in 14 patients. Macular flecks wereseen in 10 cases, of which 6 cases on clinical exam-ination showed only sparse flecks lying mainly in thetemporal region (Fig. 1). These appeared morewidespread, however, when the fundus photographswere examined, and in one case this was the onlymeans of seeing the flecks. The remaining 4 patientsshowed more profuse macular flecks which werefound in an oval distribution, the widest radius beinghorizontal and beginning 0 5-0*6mm from the fovealpit, tending to spare the foveolar and central para-foveal region. These flecks were a pale yellow colour,round, 20-5 um diameter, and on biomicroscopicexamination appeared in the innermost layer of theretina. The flecks in patient 10 extended 1'2 mmhorizontally find 1-0mm vertically from the foveal pit,whereas tho;e in patients 6, 8, and 16 extended 2'0mm from the foveal pit and further in the temporalregion. The latter 3 patients had more profuse flecks.
Patient 4 had the most florid picture (Fig. 2A), in
495
on July 17, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.67.8.493 on 1 August 1983. D
ownloaded from

J. A. A. Govan
Fig. 1 Patient 10. Sparse macularflecks were seen in 6 Fig. 2B Patient 4. Fluorescein angiogram. The retinalpatients. vessels appearfocally attenuated in places and there is an
irregularfine spotty hyperfluorescence in the nasalwhich the flecks had a less regular outline, were up to100gm diameter and became confluent in parts. Theywere more extensive, appearing within the centralparafoveal area, and extending much furtherperipherally. Occasionally flecks in cases 4 and 6formed horizontal linear streaks in the nasal maculaand almost vertical linear streaks in the temporalmacula, both showing conformation to the nerve fibrelayer distribution (Fig. 2A). In general the flecks
Fig. ZA ratient 4. More profusepecks were present inmpatients. Only occasionalflecks lie anterior to the retinalvessels and in places theflecks form linear streaksconforming to the nervefibre pattern (arrows).
parajoveal area.
tended to spare the retinal vessels, but in case 6 andparticularly in case 4 some flecks were seen lyinganterior to the vessels (Figs. 2A, 3). In each case theappearance of the flecks was symmetrical, althoughsome cases showed a slightly denser distribution onone side.The macular flecks in general appeared to transmit
fluorescence from both the choroidal and retinalvasculature, though in some places the angiographicappearance of the retinal vessels appeared focallyattenuated by the flecks (Fig. 2B). In addition therewere a few areas of masking of background choroidal
Fig. 3 Patient6. Simple preretinalmembraneshowing welldefined lacuna (arrow).
496
on July 17, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.67.8.493 on 1 August 1983. D
ownloaded from

Ocular manifestations ofAlport's syndrome: a hereditary disorder ofbasement membranes?
kk..az.;a.....I
Fig. 4A
Fig. 4B
497
h.
-sT
,f
N
I,L.
on July 17, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.67.8.493 on 1 August 1983. D
ownloaded from

J. A. A. Govan
Fig. 4C Fig. 5A Patient 11. Peripheral coalescedflecks.Fig. 4A,B Patient 11. Montages to show distribution ofmid peripheral coalescences offlecks, which are irregularly (Fig. 3) and 3 lacunae centred about the rightcircular and in parts elongated radially. C: Peripheralflecks In no patient was a posterior vitreous detachm4ofpatient 1I with presumed choroidal infarct ofsimilar Patient 15, who had associated macrot]dimensions. _ -1_ --1 6 -
fluorescence corresponding to the flecks, though thiswas usually difficult to identify amid the normalmottled appearance of the choroidal vasculature.One case displayed a bilateral irregular fine spottyhyperfluorescence particularly in the nasal parafovealarea (Fig. 2B).
Flecks in the midperipheral fundus were seen in 9patients. These were profuse small round lesions in 4cases, and in 5 cases they were prominent and tendedto form irregular circular coalescences of250-500 ,umdiameter which showed a tendency to be elongatedradially (Figs. 4A, B). In the five patients whodisplayed both macular and coalesced midperipheralflecks there was an intervening ring area in whichflecks were both less dense in distribution and lessvisible. No flecks were seen anterior to the equator.The peripheral flecks tended to spare the retinalvessels and could rarely be seen overlying them, butowing to the thinness of the retina in this region it wasimpossible to determine in which layer they lay.Fluorescein angiography of the midperipheral areashowed in some photographs a widespread spottyhyperfluorescence which did not appear to corres-pond with the flecks (Figs. 5A, B).
Several patients had no discernible macular reflex,and there were 2 cases of bilateral macular preretinalmembrane formation which appeared as a subtlewrinkling of the internal limiting membrane (case 1)and as a well defined simple preretinal membraneshowing one lacuna superonasal to the left foveola
:foveola.rent seen.birombo-__v:4-. 1: -cytopenia, lisplayeo multiple tocal pigment epitneiiai
lesions lying predominantly temporal to the maculararea. These were depigmented lesions 300-500 Amdiameter with hyperpigmented centres and werethought to -be choroidal infarcts probably sustainedduring a period of severe hypertension. Four furtherpatients displayed isolated similar lesions (Fig. 4C).
Fig. 58 Patient 11. Correspondingfluorescein angiogramshowing no correlation ofthe peripheral coalescedflecks tothe choroidal lobular vasculature.
498
on July 17, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.67.8.493 on 1 August 1983. D
ownloaded from

Ocular manifestations ofAlport's syndrome: a hereditary disorder ofbasement membranes?
Table 2 Serum lipid and lipoprotein levels (mmol/l) in patients 3, 4, 7, 9, 11, 13
Alport's±SD, Normal range Successfully transplantedall patients patients only
(4, 7, 9, 13)±SD
Triglycerides Total 2-68±159 1 -38±0-85 2-45±1-68VLDL 1-59±0-99 0-80±0-76 1-69±1-30LDL 0-42±0-17 0-31±0-13 0-42±0-17HDL 0-19±0-04 0-15±0-06 0-18±0-03
Cholesterol Total 4-92±1-21 5-72±1-15 5-69±0 67VLDL 1-10±0-69 0-44±0-38 0-93±0-66LDL 2-83±0-68 3-50±1-02 3-22±0-64HDL 1-12±0-30 1-23±0-29 1-17±0-33
VLDL=very low density lipoproteins. LDL=low density lipoproteins. HDL=high density lipoproteins.
Both the ERGs and EOGs were normal in all patientstested.
BIOCHEMICAL DATA (Tables 1, 2, 3)Both total serum triglycerides and very low densitylipoproteins were slightly elevated (Table 2).However, abnormal levels, when repeated, wereinconsistently found, and multiple factors includingimmunosuppressive agents, systemic steroids andrenal failure made correlation with the ocularfeatures impracticable. Serum vitamin A levels(Table 1) were raised in 11 patients tested inagreement with previous reports of patients inchronic renal failure and following successful renaltransplantation.2"-23 Plasma amino acids wereestimated in 9 patients. The means of the levels in 5
Table 3 Plasma amino acids (lumolll) in S successfullytransplanted patients
Normal-SD Alport's, Maximummean-SD normal(n=5) concentration
Taurine 59±12 80±25 256Aspartic acid 25±6 14±9 100Threonine 138±31 100±8 336Serine 99±19 86±19 324Asparagine 56±15 28±23 52Glutamic acid 34±15 87±42 142Glutamine 640±58 272±113 960Proline 183±39 140±67 435Glycine 234±44 233±45 515Alanine 320±71 243±76 675Citralline 35±8 32±6 63Aminobutyric acid 20±6 9±4 40Valine 225±40 177±32 370Cysteine 49±9 28±13 92Methionine 21±4 19±1 96Isoleucine 60±12 55± 12 105Leucine 115±23 117±20 230Tyrosine 54±11 39±5 196Phenylalanine 48±7 27±7 182Ornithine 58±14 123±45 214Lysine 186±36 156±42 316Histidine 88±16 61±13 195Arginine 82±17 30±9 155
successfully transplanted patients (Table 2) show nosignificant deviation from their normal values, and inno patient was any single amino acid level greaterthan the normal maximum concentration.
MANAGEMENTLenticonus resulted in myopia in photopic conditionsin patient 13, who despite previous attemptedspectacle correction was unable to pass the sight testof his driving examination. He achieved OD 6/9, OS6/12 uncorrected in mesopic conditions but requiredOD -2-00 D/-0-75 Dx180 and OS -3-5 D toachieve similar acuities under photopic conditions.Spectacles were preferred to mydriatics, although inthose patients with marked lens opacities confined tothe axial region dilute topical phenylephrineimproved the vision both subjectively and objectively.One patient (patient 15), with profound deafness,was dependent upon lip reading to communicate andunderwent unilateral cataract extraction.
Discussion
The incidence of comeal arcus if found to be slightlyhigher than that in normal persons24 (Table 4),though the samples were too small to be of statisticalsignificance. Of the 8 previously reported cases ofarcus in association with lenticonus, 2 (ages 17 and 19years) 6 2S were aged less than 20 years. Other isolatedcomeal anomalies have been variously described assuperficial white deposits,'0 bilateral fine punctatechanges,26 thickening of the anterior layers of thecornea,27 and lattice type dystrophy.28 Interstitial
Table 4 Incidence ofcorneal arcus in Alport's syndromecompared with that in normalpersons
Age (years) Alport's-present Forsius24series
0-19 17% (1/6) 5% (2/37)20-39 60% (3/5) 38% (40/106)30-39 100% (5/5) 66% (57/86)
499
on July 17, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.67.8.493 on 1 August 1983. D
ownloaded from

J. A. A. Govan
lipid laden foam cells in renal biopsy specimens are aprominent, although not exclusive, histologicalfeature in Alport's syndrome. This has been proposedas evidence of an abnormality of lipid metabolism.28However, the abundance of foam cells is roughlycorrelated with the extent of alteration of theglomerular basement membrane,29 and it is thoughtthat they may result from abnormal glomerularfiltration and subsequent tubular reabsorption of lipidmaterial.30 Most authors agree on the existence of acorrelation between an arcus and hypercholestero-laemia in the general population in these agegroups,24 3' but a comparison of the incidence of arcusin Alport's syndrome with the incidence in otherpatients in chronic renal failure is required before anyfurther inferences are made.True anterior lenticonus has been confused with
anterior pyramidal opacities, which may be associatedwith microcomea and anterior chamber cleavageanomalies.3233 The literature on lenticonus inAlport's syndrome has been reviewed by Amott etal.6 and more recently by Nielsen.' The latter authorstated that during the previous 13 years all reportedcases of lenticonus which had been investigated werefound to have evidence of nephritis and concludedthat anterior lenticonus was seen only as a part ofAlport's syndrome. A defect of embryogenesis hasbeen proposed as the aetiology of lenticonus, thoughthe usual presence of a clear lens capsule and anteriorlens epithelium and the absence of other anteriorchamber defects militate against this theory.32 Thethickness of the lens capsule varies according to theage of the eye and site of the capsule. The thinnestpart of the anterior capsule is at the anterior pole andit becomes thickest in a circular area 3mm from this.34Several patients in this study could date the onset oftheir myopia and often stated that it was progressive.However, a well documented increase in the lenti-conus has been rarely reported. 12 3SSpontaneous change of anterior lenticonus to
anterior capsular cataract has been welldescribed,5 25 36 and this has been observed to followspontaneous rupture of the capsule overlying thecone. 3738 It would seem likely therefore that there isan inherent weakness of the anterior lens capsule inlenticonus.39 Lenticonus posterior has beensporadically reported in Alport's syndrome.727404'Spherophakia has been reported in medical surveys
426thof Alport's syndrome, in which the coronaldiameters of the lens are not commented upon, and itis possible that these patients had a marked anteriorlenticonus.Many lens opacities have been described in associa-
tion with Alport's syndrome, including anterior andposterior polar,42 anterior subcapsular,'o3842posterior subcapsular,27 cortical and coronary,47384546
and lamellar.27 Up to 75% of patients under 40 yearsdevelop posterior subcapsular lens opacities afterrenal transplantation, and there are only isolatedreports of lens opacities developing in patients onhaemodialysis not receiving steroids.47 No lensopacity appears to be specific for Alport's syndrome.
Macular flecks in Alport's syndrome were firstrecorded by Castleman and Kibbee48 and later char-acterised by Peterson and Albert'0 as a few flecks inthe perifoveal region and by Polak and Hogewind" ina much more profuse distribution around the foveawhich they considered to lie at the level of the internallimiting membrane. Fluorescein angiography of themacular region has been reported as alwaysnormal." 3 Reports of flecks in the mid periphery areless frequent.8'0 14 'S Peterson and Albert'0 describedmultiple small peripheral flecks which they consideredto he in the pigment epithelium, and on fluoresceinangiography they found tiny hyperfluorescentwindowdefects. This angiographic appearance was confirmedby others,'5 and the authors of both studies suggestedthat there was a widespread disturbance of the retinalpigment epithelium. These findings are in accord withthis study but were not seen by others. '4 The com-bination of both macular and peripheral flecks hasonly been described in 3 patients. '0 '4The distribution of the macular flecks appears to
conform with the thickness of the internal limitingmembrane (ILM). Foos49 found that both thethickness and the variation in thickness of the ILMincreased progressively from the basal zone towardsthe posterior zone. At the origin of the foveal clivus inan area 1 5 mm in diameter the ILM gradually thins to0-2 ,um or less at the fovea.50 Furthermore the ILM isreduced to as little as 0 5 um over retinal vessels.5'The flecks may also be related to the different under-lying glial cells, Muller cells producing thick basementmembrane and other astrocytes producing thinbasement membrane.52 The distribution of thecoalescences of the peripheral flecks is difficult toexplain. However, the only anatomical correlate isthe choroidal lobular vasculature,53 and in Fig. 4B canbe seen a presumed choroidal infarct of similardimensions to the coalescences. Fluorescein angio-graphic studies in the mid peripheral region in an areaof relative choroidal hypoperfusion show thechoroidal lobular filling pattern well (Figs. 5A, B).However, the coalescing flecks do riot appear to bearany relationship to these. The lack of correlationbetween the presence of the macular and peripheralflecks suggests that they might have a separatepathogenesis.
Several authors have previously commented upona weakened macular reflex,' 13 26 54 and Zylberman etal. 14 reported a Cellophane light reflex. Theoccurrence of a well defined bilateral simple pre-
500
on July 17, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.67.8.493 on 1 August 1983. D
ownloaded from

Ocular manifestations ofAlport's syndrome: a hereditary disorder of basement membranes?
retinal macular membrane in a 33-year-old patient ishighly suggestive of a defect of the ILM. Idiopathicpreretinal macular gliosis (IPMG), which has not beenreported in patients under 30 years of age,55 isassociated with a break in the ILM through whichglial cells penetrate and proliferate.5657 Manypatients with IPMG are hypertensive," and glial pro-liferation has been described both clinically followingsevere hypertensive retinopathy associated withexudative retinal detachment58 and also patho-logically following severe hypertension.57 Although ithas been stated that epiretinal membranes arerelatively common over cotton-wool spots,59 sub-sequent histological studies of ischaemic retinalinfarcts have not revealed any evidence of preretinalmembrane.60 This has been attributed to glial celldeath.6' Hypertension may be the aetiology of IPMGin this patient. However, although a weakenedmacular reflex has been commented upon in patientswith chronic renal failure associated with thenephrotic syndrome, further studies in other patientswith chronic renal failure are required to determinethe significance of IPMG in patients with Alport'ssyndrome.
Polak and Hogewind" described a photopic ERGat the lower limit of normal in one patient withAlport's syndrome and both low scotopic andphotopic ERGs in relatives. Other authors havedescribed similar changes,'31462 and there is onereport of abnormalities of the EOG. ,5 However, theamplitude of the b wave of the ERG is often reducedin patients with chronic renal failure63 4 and in thoseon dialysis63 65 67 and following renal trans-plantations.68 Both hypertension69 and steroidadministration70 have been reported to alter the bwave amplitude, and low EOGs have been describedin patients on haemodialysis.7' Therefore no con-clusions concerning the electrodiagnostic changes inAlport's syndrome can be made until normal values inthis group of patients have been determined.Macular flecks have been detected in patients
whose renal function at the time of examination wasnormal but who many years later developed renalfailure. 13 The appearance of the flecks bears aremarkable resemblance to many earlier reports offundus albipunctatus,72 which may be stationarywithout any symptoms, or with stationary nightblindness, and in which abnormalities of the ERGand EOG are inconstant. In this disorder the visualacuity is normal or near normal, and the flecks lie inthe macular region, generally sparing the fovea andextending towards the equatorial region. They mayoccur in either region alone and sometimes form aradial distribution, though this is very variable.73Both poor73 and irregular74 macular reflexes havebeen described, and the flecks are reported to lie at all
neuroretinal levels. Fundus photography confirmsthat they do not as a rule overlie the retinal vessels.Fluorescein angiography shows a variable picture ofoccasional masking by the individual flecks andmottled choroidal transmission which does notcorrelate with the flecks. Most case reports do notcontain general medical details, but in 4 casesreported by Nettleship75 nearly 100 years ago 2 sisterswere noted to be deaf.The incidence of optic disc drusen in the general
population is 0.34%,76 and the much quoted singlecase described'6 in association with Alport'ssyndrome is likely to be coincidental. An increase ordisturbance of the macular pigmentation has beennoted754 but not detailed further. Anisocoria,'° irisheterochromia,754 and iris atrophy7" have been noted,and it is of interest that the sister of patient 5, who alsohas Alport's syndrome, displayed a unilateral con-genital Horner's syndrome, and one patient hadanisocoria.
Although an autosomal dominant inheritance ismost commonly described (for discussion andreferences see Gubler et al.,78) some family studiesshow a sex-linked dominant inheritance79 and othersare compatible with an autosomal recessive in-heritance.78 Genetic heterogeneity has beenproposed as an explanation of the presence orabsence of ocular features among families and also ofthe varying severity of renal disease. 78The characteristic ultrastructural alterations of the
glomerular basal lamina in hereditary nephritis areirregular thickening of the basal lamina and replica-tion of the lamina densa with a 'basket weave' patternin which fibrils of lamina densa interconnect with oneanother and enclose electron-lucent lacunae whichfrequently contain small dense particles.29 A wide-spread basket weave pattern appears to be specific forhereditary nephritis.80 These appearances are notconstant, and it is interesting that the renal biopsies of2 patients (patients 4 and 6) who displayed floridretinal flecks and lenticonus showed no electronmicroscopy evidence of Alport's syndrome. Thecochlear abnormalities characterised by atrophy ofthe stria vascularis and electron microscopy studieshave shown a multilayered basement membrane ofthe vas spirale.81 It has been suggested that there maybe a metabolic defect in the biosynthesis ormetabolism of collagen with changes in theglomerular basement membrane, cochlea, andcapsule of the lens, with the possibility that thecollagen may be specific in these 3 places.82 Tina etal.83 have shown an increased excretion of urinaryhydroxylysine glycosides (collagen metabolites) inchildren with Alport's syndrome, suggesting thatthere is an alteration of collagen metabolism. It seemslikely that the retinal internal membrane may be
501
on July 17, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.67.8.493 on 1 August 1983. D
ownloaded from

J. A. A. Govan
additionally primarily involved in this syndrome. Onemight also make the conjecture that an abnormalbasement membrane of the retinal pigment epi-thelium could result in the pigment epithelialabnormality.
It is concluded therefore that the diagnosis offundus albipunctatus should not be made in theabsence of a full renal investigation and audiometry.The diagnosis of Alport's syndrome can be made onthe presence of one of 3 characteristic features. Theseare anterior lenticonus, macular flecks at the level ofthe ILM, and peripheral coalescing flecks conformingto Fig. 4. However, the absence of these features doesnot exclude the diagnosis. Other ocular features occurless regularly and are not specific. It seems likely thatAlport's syndrome is due to a widespread defect ofcertain basement membranes which is irregularlyclinically manifest. Further studies into the morpho-logical, biochemical, and biophysical properties ofthese important extracellular matrices are required.The lens capsule is not only the thickest basementmembrane in the body but also the one most easilyisolated (for review of this subject see Heathcote andGrant84). Cataract extraction is not infrequentlyrequired following steroid therapy for renal trans-plantation, when this basement membrane becomesavailable for analysis.
I thank the consultant staff of both the adult and paediatric renalunits forallowing this study of their patients and particularly ProfessorS. Cameron for helpful direction to the literature. I am also gratefulto Mr D. Watson and Mr R. Daniel for making available the facilitiesof the Department of Ophthalmology, to Mr N. Dalton, MrM Mattock, and Dr P. Toseland for the biochemical assays, to MrC. Clements and the Department of Medical Photography for photo-graphic assistance, Dr P. Mayles for the electrodiagnostic studies,and to Miss Louise Barker for typing the manuscript.
This study was supported in part by a grant from the RoyalNational Institute for the Blind.
References
I Guthrie LG. Idiopathic or congenital hereditary and familialnephritis. Lancet 1902; i: 1243-6.
2 Hurst AF. Hereditary familial congenital haemorrhagic nephritisoccurring in sixteen individuals in three generations. Guy's HospRep 1923; 73: 368-70.
3 Alport AC. Hereditary familial congenital haemorrhagicnephritis. Br Med J 1927; i: 504-6.
4 Sohar E. Renal disease, inner ear deafness and ocular changes.Arch Intern Med 1956; 97: 627-30.
5 Jaworski A. Ein Fall von Lenticonus Anterior und uber dessenEntstehen. 1910; 65: 313-7. Summarised in Rones B.32
6 Arnott EJ, Crawford MD'A, Toghill PJ. Anterior lenticonus andAlport's syndrome. Br J Ophthalmol 1966; 50: 390-403.
7 Nielsen CE. Lenticonus anterior and Alport's syndrome. ActaOphthalmol (Kbh) 1978; 56: 518-30.
8 Unger H-H, Rother K. Netzhautreranderungen beim Alport-syndrom (erbliche Nephropathie mit Innenohrschwerhorigkeit).Ber Dtsch Ophthalmol Ges 1964; 65: 293-8.
9 Bunge H. Mitteilungen aus der Praxis-Fur die praxis (Fundusalbipunctatus beim Alport-Syndrom). Klin MonatsblAuenheilkd 1965; 147: 751-3.
10 Peterson WS, Albert DM. Fundus changes in the hereditarynephropathies. Trans Am Acad Ophthalmol Otolaryngol 1974;78: OP 762-71.
11 Polak BCP, Hogewind BL. Macular lesions in Alport's disease.Am J Ophthalmol 1977; 84: 532-5.
12 Ursui J, Kogo S, Kitahara H. Alport's syndrome. FoliaOphthalmolJpn 1978; 29: 1012-8.
13 Perrin D, Jungers P, Grunfeld JP, Delous S, Noel L-H, ZenattiC. Perimacular changes in Alport's syndrome. Clin Nephrol 1980;13:163-7.
14 Zylberman R, Silverstone B-Z, Brandes E, Drukker A. Retinallesions in Alport's syndrome. J Pediatr Ophthalmol 1980; 17:255-60.
15 Hochesand P, Steinbach PD, Straub E. Augenveranderungen beiAlport-Syndrom. Klin Monatsbl Augenheilkd 1974; 165: 447-52.
16 Friedberg D. Pseudoneuritis und Drusenpapille beimAlport-Syndrom. Klin Monatsbl Augenheilkd 1968; 152: 379-83.
17 Chavis RM, Groshong T. Corneal arcus in Alport's syndrome.Am J Ophthalmol 1973; 75: 793-4.
18 Stevens PR. Anterior lenticonus and the Wardenburg syndrome.BrJ Ophthalmol 1970; 54: 621-3.
19 Epstein CJ, Sahud MA, Piel CF, et al. Hereditary macro-thrombocytopenia, nephritis and deafness. Am J Med 1972; 52:299-310.
20 Duke-Elder S. System of ophthalmology. London: Kimpton,1977:11:159.
21 Smith FR, Goodman DS. The effects of diseases of the liver,thyroid and kidneys on the transplant of vitamin A in humanplasma. J Clin Invest 1971; 50: 2426-36.
22 Yatzidis H, Digenis P, Fountas P. Hypervitaminosis Aaccompanying advanced chronic renal failure. Br MedJ 1975; iii:352-3.
23 Kellaher J, Humphrey CS, Horner D, Losowsky MS. Vitamin Aand retinal binding protein following renal transplantation inman. Presented at 5th Fat soluble vitamin meeting March 1981,Leeds, UK.
24 Forsius H. Arcus senilis corneae. Acta Ophthalmol (Kbh) 1954;42 (suppl): 1-78.
25 Tsukahara Y. Zwei Falle von Lentiglobus anterior. Anhang:Resultate der Untersuchung der Tatigkeit des vegetativenNervensystems. Zentralbl Ophthalmol 1931; 24: 171-2.
26 Purriel PD, Diets M, Pascale E, Cestan RS, Borras A, FerreiraWA, De Lucca A, Ferrnndez L. Familial hereditary nephropathy(Alport's syndrome). Am J Med 1970; 49: 753-73.
27 Perrin D. Le Syndrome d'Alport. Nephropathies hereditariesavec surdite et atteinte oculaire. Ann Oculist (Paris) 1964; 197:329-46.
28 Kaufmann DB, McIntosh RM, Smith FG, Verrier RL. Diffusefamilial nephropathy: a clinicopathological study. J Pediatr 1970;37:37-47.
29 Hinglais N, Grunfeld J-P, Bois E. Characteristic ultrastructurallesion of the glomerular basement membrane in progressivehereditary nephritis (Alport's syndrome). Lab Invest 1972; 27:473-87.
30 Rosen S, Pirani CL, Muchrcke RC. Renal interstitial foam cells: alight and electron microscopic study. Am J Clin Pathol 1966; 45:32-41.
31 Varnek L, Schnohr P, Jensen G. Presenile corneal arcus inhealthy persons: a possible cardiovascular risk indicator inyounger adults. Acta Ophthalmol (Kbh) 1979; 57: 755-65.
32 Rones B. Anterior lenticonus. JAMA 1934; 103: 327-30.33 Sand BJ, Abraham SV. Anterior lenticonus. Am J Ophthalmol
1962; 53: 636-9.34 Hogan MJ, Alvarado JA, Weddell JE. Histology of the human
eye. Philadelphia: Saunders, 1971; 12: 652-3.35 Van der Laan. Nagel's Jahresbericht 1880; 2: 369. Summarised in
Rones B.3236 Feigenbaum A. The origin of lenticonus. Folia Ophthalmol
Orient 1932; 1: 103-10. Summarised in Rones B.32
502
on July 17, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.67.8.493 on 1 August 1983. D
ownloaded from

Ocular manifestations ofAlport's syndrome: a hereditary disorder of basement membranes?
37 Ehrlich LH. Spontaneous rupture of the lens capsule in anteriorlenticonus. Am J Ophthalmol 1946; 29: 1274-81.
38 Gregg JB, Becker SF. Concomitant progressive deafness, chronicnephritis and ocular lens disease. Arch Ophthalmol 1963: 69:293-9.
39 Duke-Elder S. System of ophthalmology London: Kimpton.1977; 11:59-61.
40 Asperti G. Lenticono anteriore hilaterale con lenticonoposteriore monolaterale in nephritic iperazotemico. AnnOttalmol 1964; 90: 107-1 1.
41 Vancea P, Lazarescu D. Contributions a l'6tude du lenticone.Ophthalmologica 1958; 135: 67-8.
42 Faggioni R, Scouras J, Streiff EB. Alport's svndrome. Clinico-pathological considerations. Ophthalmologica 1972' 165: 1-14.
43 Goldbloom RB. Fraser FC. Waugh D. Aronovitch M.Wigglesworth FW. Hereditary renal disease associated with nervedeafness and ocular lesions. Pediatrics 1957: 20: 241-52.
44 Brownell RD, Walter JR. Anterior lenticonus in familialhaemorrhagic nephritis. Arch Ophthalmol 1964; 71: 481-3.
45 Hauser J. Nephropathie chronique her6ditaire avec surdite etatteinte oculaire. Schweiz Med Wochenschr 1974; 104: 724-8.
46 Rome L, Cuppage FE, Vertes V. Familial haematuric nephritis.Pediatrics 1966; 38: 808-18.
47 Polak BCP. Ophthalmological complications of haemodialvsisand kidney transplant. Doc Ophthalmol 1980:49: 1-96.
48 Castleman B, Kibbee BU. Case records of the Massachusettsgeneral hospital. N Engl J Med 1957; 257: 1231-7.
49 Foos RY. Vitreoretinal juncture: topographical variations. InvestOphthalmol Visual Sci 1972; 11: 801-8.
50 Yamada E. Some structural features of the fovea centralis in thehuman retina. Arch Ophthalmol 1969; 82: 151-9.
51 Foos RJ. Vitreoretinal juncture over retinal vessels. Albrecht vonGraefes Arch Klin Ophthalmol 1977: 204: 223-34.
52 Fine BS, Yanoff M. Ocular histology. New York: Harper andRow, 1972; 11:235.
53 Torczynski E, Tso MOM. The architecture of the choriocapillarisat the posterior pole. Am J Ophthalmol 1976; 81: 428-4(1.
54 Singh DS, Bisht DB, Kapoor S. Sharma RN. Samkaran K.Majumdar NK. Lenticonus in Alport's syndrome: a familv studv.Acta Ophthalmol (Kbh) 1977; 55: 164-70.
55 Sidd RJ, Fine SL, Owen SL. Patz A. Idiopathic preretinal gliosis.Am J Ophthalmol 1982; 94: 44-8.
56 Bellhorn MB, Friedman AH, Wise GN. Henkind P. Ultra-structure and clinicopathological correlation of idiopathicpreretinal macular fibrosis. Am J Ophthalmol 1975: 79: 366-73.
57 Roth AM, Foos RY. Surface wrinkling retinopathv in evesenucleated at autopsy. Trans Am Acad Ophthalmol Otolarvngol1971;75: 1047-58.
58 Buchanan WS, Ellis PP. Retinal separation in chronic glomerulo-nephritis. Report of a patient cured bv bilateral nephrectomiesand subsequent successful kidney transplant. Arch Ophthalmol1964; 71: 182-6.
59 Foos RY. Surface wrinkling retinopathv. In Freeman HM.Hirose T, Schepens CL, eds. Vitreous suirgerv and advances infundus diagnosis and treatment. New York: Appleton-Centurv-Crofts, 1977: 23-38.
60 Foos RY. Regional ischaemic infarcts of the retina. Albrecht von
Graefes Arch Klin Ophthalmol 1976: 200: 183-94.61 Yanoff N, Fine BS. Ocular pathology. Hagerstown: Harper and
Row, 1975; 11: 397-8.62 Huch D, Meythaler H, Rix R. Alport-Syndrom' mit Horn-
hautbeteiligung und Veranderungen des ERG. Klin MonatsblAugenheilkd 1976; 168: 553-6.
63 Perossini M, Tota G. Electroretinographic findings in chronicuraemics treated with periodic haemodialysis. Doc Ophthalmol
Proceedings Series 15. 15th ISCEV Symposium. The Hague:Junk. 1978: 257-63.
64 Farkas A. ERG on patients with chronic nephropathy. DocOphthalmol Proceedings Series 23. 17th ISCEV Symposium. TheHague: Junk, 5-110 June 1979: 149-52.
65 Mikara A. The studies on the eyes of the subjects of renal diseasewith the treatment bv the haemodialysis and the peritonealdialvsis. Report 11. The correlation between the EOG and ERG.Nippon Ganka Gakkai Zasshi 1973; 77: 1116-23.
66 Sverak J, Peregrin J, Hejcmanova D, Erben J, Groh J. Logisticfunction in the analysis of the ERG in dialysed patients. DocOphthalmol Proceedings Series 23. 17th ISCEV Symposium. TheHague: Junk, 5-10 June 1979: 153-7.
67 Muller W. Haase E, Niedlich R, Gauss J. Jung N. Chronichaemodialvsis and ERG. Doc Ophthalmol Proceedings Series 23.17th ISCEV Symposium. The Hague: Junk, 5-10 June 1979:159-66.
68 Dr6becka-Brvdak E, Moszcynsha-Kowahka A. Electroretino-graphic studies in patients after renal transplantation. DocOphthalmol Proceedings Series 23. 17th ISCEV Symposium. TheHague: Junk. 5-10 June 1979: 167-70.
69 Henkes HE, Van de Kam JP, WesthoffAJS. Electroretinographicstudies in arterial hypertension. Effect of reduction in bloodpressure on electrical responses of human retina. ArchOphthalmol 1954; 52: 221-33.
70 Zimmerman TJ, Dawson WW, Fitzgerald CR. Electroretino-graphic changes in normal eyes during administration ofprednisolone. Ann Ophthalmol 1973: 5: 757-65.
71 Muller W. Thieler H. Electrooculographic findings in cases ofregular haemodialysis. Doc Ophthalmol Proceedings Series 23.17th ISCEV Symposium. The Hague: Junk, 5-10 June 1979:143-7.
72 Krill AE. Hereditars retinal and choroidal diseases. Hagerstown:Harper and Row. 1977: 2: 739-824.
73 Marmor MF. Fundus albipunctatus: a clinical study of the funduslesions, the physiological deficit, and vitamin A metabolism. DocOphthalmol 1977; 43: 277-302.
74 Krill AE, Klein BA. Flecked retina syndrome. Arch Ophthalmol1965; 74: 496-508.
75 Nettleship E. Cases of permanent partial night-blindness withunusual ophthalmoscopic changes. Trans Ophthalmol Soc UK1887:7:301-5.
76 Lorentzen SE. Drusen of the optic disc. A clincial and geneticstudy. Acta Ophthalmol (Kbh) 1966; 90 (suppl): 1-180.
77 Davies PD. Pigment dispersion in a case of Alport's syndrome. BrJ Ophthalmol 1970; 54: 557-61.
78 Gubler M, Levy M, Broyer M, etal. Alport's Syndrome: a reportof 58 cases and a review of the literature. Am J Med 1981; 70:493-505.
79 O'Neill VN, Atkin CL. Bloomer HA. Hereditary nephritis: are-examination of its clinical and genetic features. Ann InternMed 1978; 88: 176-82.
80 Yoshikawa N, Cameron AH, White RHR. The glomerular basallamina in hereditary nephritis. J Pathol 1981; 135: 199-209.
81 Weidauer H, Arnold W. Consideration to the aetiology ofAlport's syndrome. Arch Otorhinolarvngol 1975; 210: 361.
82 McCrory WW, Shibuya M, Worthen HG. Hereditary renalglomerular disease in infancy and childhood. Adv Pediatr 1966;14: 253-80.
83 Tina LU, Lou MF, Dizio D, Calcagio PL. Alteration of collagenmetabolism in hereditary nephritis. PaediatrRes 1979; 13: 774-6.
84 Heathcote JG, Grant ME. The molecular organisation ofbasement membranes. Int Rev Connect Tissue Res 1981; 9:191-264.
503
on July 17, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.67.8.493 on 1 August 1983. D
ownloaded from