Embed Size (px)
Citation preview

October 7, 2013
Overview of Evidence-BasedSelf-Management Programs

Outline
• Overview of Partners in Care• Chronic Disease Self-Management Programs• Los Angeles Caregiver Resource Centerd• HomeMeds Program• Home Support Program

Mission
To serve as a catalyst for shaping a new vision of health care by partnering with organizations, families and community leaders
in the work of changing health care systems, changing communities and changing lives

Partners in CareWho We Are
Partners in Care is a transforming presence, an innovator and an advocate to shape the future of health care
We address social and environmental determinants of health to broaden the impact of medicine
We have a two-fold approach, creating and using evidence-based models for: provider/system practice change and enhanced patient self-management
Changing the shape of health care through new community partnerships and innovations


Building the New HCBS Services Model: Focus Areas
Evidence-Based Self Management
Assessments & Care Coordination
Collaboratives/Networks/TA
Chronic Disease Care Transitions Intervention Evidence-Based Leadership Council
Chronic Pain CBAS Eligibility Determination Care Coordination Network
Diabetes (billable) Home Safety Evaluation Care Transitions Intervention Network
Matter of Balance HomeMeds
Savvy Caregiver Care Coordination
Powerful Tools for Caregivers
Arthritis Foundation Exercise
Arthritis Foundation Walk with Ease
UCLA Early Memory Loss
What is Self-Management?The actions that individuals living with chronic
conditions must do in order to live a healthy life.
Better Breathing
Problem-Solving
Planning
Physical Activity
Manage Fatigue
Medications
Working with Health Professionals
Using Your MindManaging Pain
Communication
Healthy Eating
Understanding Emotions

Chronic Disease Self-Management Education (CDSME)
Program Overview
Evidence based programs developed & licensed by Stanford University
Patient Education Research Center

Self-Management Programs
• Chronic Disease Self-Management*
• Diabetes (Eng/Spanish)
• Chronic Pain
• Tomando Control de su Salud (Spanish)
*Leader manual available in Arabic, Bengali, Chinese, Dutch, French, German, Greek, Hindi, Italian, Japanese, Korean, Khmer, Norwegian, Punjabi, Russian, Somali, Swedish, Tagalog, Tamil, Turkish, Vietnamese
Diabetes Self-Management Program
• Developed at Stanford University by Kate Lorig, RN, Dr.PH
• Patients with Type 2 diabetes learn to take charge and control of their diabetes.
• Develop tools to understand and deal with:– Emotions– Manage medications– Worth with health care providers– Make weekly action plans for
exercise and healthy eating
Designed to empower participants through a mutually
supportive and interactive education process
Added benefit – socialize with new people!
Chronic Pain Self-Management Program
• Developed at Stanford University by Kate Lorig, RN, Dr.PH
• Patients with Primary or Secondary Diagnosis of chronic pain learn to manage & lower their chronic pain. Participants Report:– Less Pain – Lower Dependency on Others– More Energy– Improved Mental Health– Increased satisfaction with life– More involvement in every day
activities
Designed to empower participants through a mutually
supportive and interactive education process
Added benefit – develop relationships with others
suffering from chronic pain!

CDSME Program Goals
To build self-confidence & provide:
Social InteractionShared Experiences & Support
Identification of ProblemsReinterpretation of Symptoms
Skill Development to Control Symptoms

Program Design
• 12 -16 participants
– Two Trained Leaders
– People with different conditions
Six-week Program 2 ½ hours, one day a week Includes:
Group discussions Activities Short lectures
Book: Living a Healthy Life with Chronic Conditions
Target Population
People with at least one chronic condition – OR –
A family member, friend or caregiver of someone with a chronic conditionStamina to attend 2 ½ hour session
Cognitive function to participate

CDSME Workshop
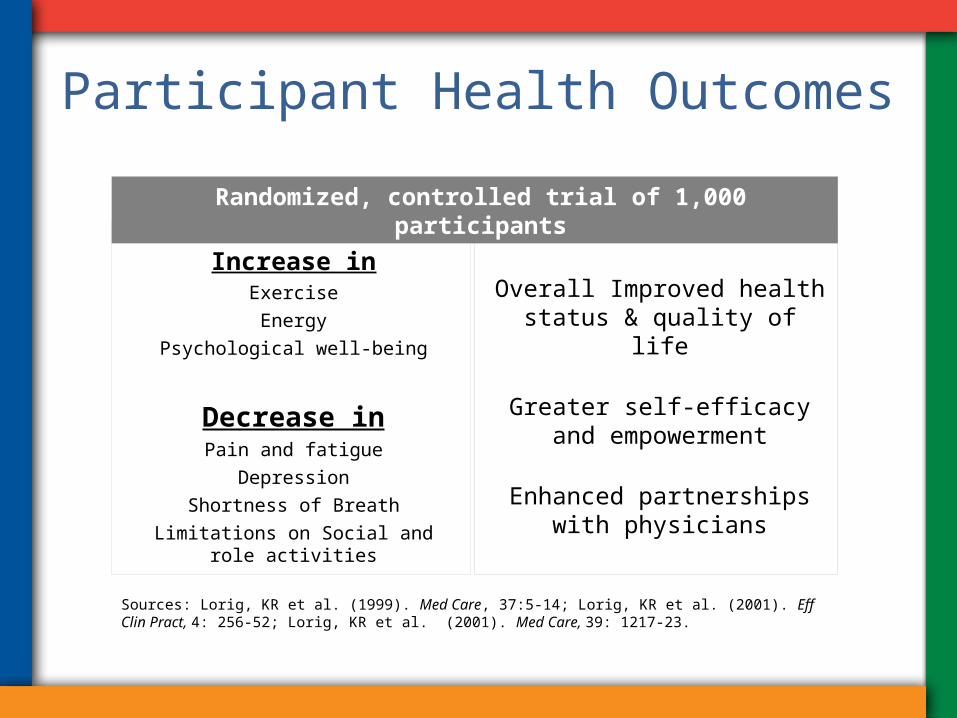
Participant Health Outcomes
Increase inExerciseEnergy
Psychological well-being
Decrease inPain and fatigue
DepressionShortness of Breath
Limitations on Social and role activities
Overall Improved health status & quality of life
Greater self-efficacy and empowerment
Enhanced partnerships with physicians
Sources: Lorig, KR et al. (1999). Med Care, 37:5-14; Lorig, KR et al. (2001). Eff Clin Pract, 4: 256-52; Lorig, KR et al. (2001). Med Care, 39: 1217-23.
Randomized, controlled trial of 1,000 participants

Health Care Utilization Effects
• Results showed more appropriate utilization of health care resources through decreased:
• Outpatient visits• Emergency room visits• Hospitalizations• Days in hospital
Ultimate Result: Reduction in health care expenditures

Testimonials• “Because I have been afflicted with Parkinson’s for over 20 years, I have suffered a
great deal of depression. The skills you've taught me in maintaining positive thinking and combating depression have really helped to improve my condition.” - John, age 69
• “I found the interaction with the other students in the class to be most enlightening. I realized that although I have a chronic illness I am not alone. Thank you for all the lessons in helping me to deal with this.” - Suzanne, age 57
• “The workshop put me back in charge of my life, and I feel great. I only wish I had done this sooner.” - Robert, age 68
Los Angeles Caregiver Resource Center (LACRC)
Established in 1989, the LACRC provides information, support, training and respite assistance to families caregiving for a person with a brain impairment or chronic condition residing in Los Angeles county.
This program is one of a network of 11 similar CRCs across California.
As a program of Partners in Care Foundation, the LACRC helps identify caregiving individuals and links them with culturally and linguistically appropriate programs in their communities.
LACRC Programs and Services:• Information and Referral• Support Groups (face to face and via the telephone)• Community Education (weekly or monthly events held in
partnership with senior centers and other community-based organizations)
• Caregiver Education: Evidence-based programs including Savvy Caregiver and Powerful Tools for Caregivers workshops.
• Respite Assistance: Limited short –term grants to allow caregiving individuals to get relief from the many stressors related to providing care for their loved one.
• Family Consultations: Assistance to caregivers in resolving and planning for immediate and long term care-related issues.

Care Transitions
• Health reform Section 3026 addresses high Medicare readmits in 30 days after discharge
• CMS is funding tests of a new Medicare benefit – 101 nationally and 11 in California
• The hospital partnerships fund CBOs – high risk are identified and seen in hospital/home and follow up calls
• Forming a regional delivery system
What a Home Visit Looks Like • Medication Risk Assessment– Room by room “Treasure hunt”– Assessment of possible adverse effects• Recent falls, dizziness, confusion, BP, pulse
– Assessing client understanding and adherence• Environmental Assessment– Safety, cleanliness, maintenance, barriers to mobility– Evidence of problems– Fall Risks
22

The Problem- Medication Errors
• Serious: Over 700,000 people go to ED each year for adverse drug events
• Costly: Drug-related morbidity/mortality > $170 billion
• Common: Up to 48% of community-dwelling elders have medication-related problems
• Preventable: At least 25% of all harmful adverse drug events are preventable
23

Medications Related to Emergency Hospitalizations
• Frequency and rates of hospitalization after ADE-related ED visits by older adults aged 65+*
• Nearly half aged 80+• 2/3 of hospitalizations due to unintentional overdose• Four medications/classes implicated alone or in combination
in 67% of hospitalizations– Insulin and hyperglycemic medications– Anticoagulants & antiplatelets
• High-risk-designated drugs implicated in 1.2% of hospitalizations
* Emergency Hospitalizations for Adverse Drug Events in Older Americans. Daniel S. Budnitz, M.D., M.P.H., Maribeth C. Lovegrove, M.P.H., Nadine Shehab, Pharm.D., M.P.H., and Chesley L. Richards, M.D., M.P.H. N Engl J Med 2011;365:2002-12
24
The Importance a Home Visit• Uncovers many “secrets”… that prescribers may
not know about – Over-the-counter medications & supplements – Medications prescribed by other providers– Adverse effects such as falls, dizziness, confusion– Assessment information – Incorrect self-dosing – Adherence issues – “Un-manageable care” – $4 co-pays at Wal-Mart < Part D co-pay $ – Medications from other countries– Medications “borrowed” from friends and family
25

Evidence-based Protocols• Protocols identified by national expert consensus panel*• Target problems that can be identified and resolved in the
home• Likely to get a positive response by prescribers and
minimize “alert overload” • Protocols
• Unnecessary therapeutic duplication • Use of psychotropic drugs in patients with a reported recent fall and/or confusion• Use of NSAID in patients at risk of PUD/gastrointestinal bleeding.• Selected Cardiovascular medication problems
» Sub-optimal blood pressure control» Orthostatic changes/low systolic BP» Slow pulse
*"A model for improving medication use in home health care patients " Brown, N. J., Griffin, M. R., Ray, W. A., Meredith, S., Beers, M. H., Marren, J., Robles, M., Stergachis, A., Wood, A. J., & Avorn, J. (1998). Journal of the American Pharmaceutical Association, 38 (6), 696-702.
26

Further Evidence• USC Evaluation in nursing-home eligible community-
dwelling population• Population: 615 Dual Eligibles, 65+• Social workers & nurses collected data in home visit
• Results ¹ ²• 49% had potential medication problems • 29%- pharmacist recommends intervention• 61% of clients referred to MD after pharmacist review had
medication use improvement
27
[1] Prevalence of Potential Medication Problems in Dually-Eligible Older Adults in Medicaid Waiver Services. Alkema GE, Wilber KW, Enguidanos SM, Frey D. An Pharmacotherapy. 12/07[2] “The Role of Consultant Pharmacists in Reducing Medication Problems Among Older Adults Receiving Medicaid Waiver Services”. Alkema GE, Enguidanos SM, Wilber KW, Trufasiu M, Frey D. . The Consultant Pharmacist. February 2009, Volume 24, No. 2

Always looking for new partnerships
Contact:June Simmons, CEOPartners in Care [email protected]
Bertha SandovalPartners in Care Foundation818-837-3775 [email protected]