Embed Size (px)
Citation preview

1
October 2013
Purpose This analysis resource provides the Department of Energy’s (DOE) electrical safety community with a compilation of, and informal observations on, electrical safety occurrences reported through the Occurrence Reporting and Processing System (ORPS). The topics addressed in this analysis resource are responsive to requests for this information by the electrical safety community, who utilizes this information through monthly conference calls to foster information exchange and continual learning regarding electrical safety occurrences and their prevention across the DOE complex.
Key Observations The number of electrical safety occurrences for October was 15, which is an increase from 11 in September. There were four reported electrical shocks, two electrical intrusion occurrences, and five lockout/tagout occurrences. In October, workers identified electrical hazards 53 percent of the time, which is a decrease in hazards identification from 73 percent in September.
Electrical Safety Occurrences The following sections provide a summary of selected occurrences based upon specific areas of concern regarding electrical safety (e.g., bad outcomes or prevention/barrier failures). The complete list and full report of the occurrence reports is provided in Attachment 2. Electrical Shock There were four reported electrical shocks in the month of October which is an increase from the two occurrences reported in September. These occurrences are summarized below. 1. A protective force officer received a minor electrical shock while unplugging an extension
cord from a 110-volt duplex wall outlet. The other end of the extension cord is hard wired to a charging unit for an indoor plant vehicle (scooter). The officer reported to their manager describing the shock as a "tingle". No defects were found with the electrical outlet; however, the plug on cord had a gap in the insulation and it was repaired on the spot.
2. An electrician received a minor shock to his right ring finger while performing circuit breaker maintenance on a motor control center (MCC). Analysis indicated the shock was from a
Office of Health, Safety and Security
Monthly Analysis of Electrical Safety Occurrences
2
single phase 120-volt circuit. The 480-volt power supply to the MCC had been locked and tagged out before the start of work. In most MCCs, the control power is stepped down from the primary power supply; specifically from 480 volts to 120 volts. There was no indication before the incident that there was a second source of power to the control terminal. After the incident, it was determined that the control terminal had a second source of power consisting of 120 volts, single phase.
3. Two administrative assistants noted electrical sparking while plugging an EPSON LCD Projector (Model: EMP-1715) into a power strip. The assistant holding the plug felt an electrical shock. There was no injury and an investigation was initiated.
4. An employee was troubleshooting an instrumentation problem when he received an electrical shock. Simultaneously, the accelerator high voltage bus tripped on a ground fault indication, shutting down power to the bus. While reading a monitor, he rested his left hand on a vertical section of one side of a relay rack while at the same time he rested his right hand on the vertical section of the other side of the relay rack. There were two heliax cables, terminated with connectors but not grounded or connected to a device, tied together with a cable tie running along the right side of the relay rack. As the employee grasped the relay rack with his right hand, his hand also came in contact with the connectors on the ends of these cables and received the shock.
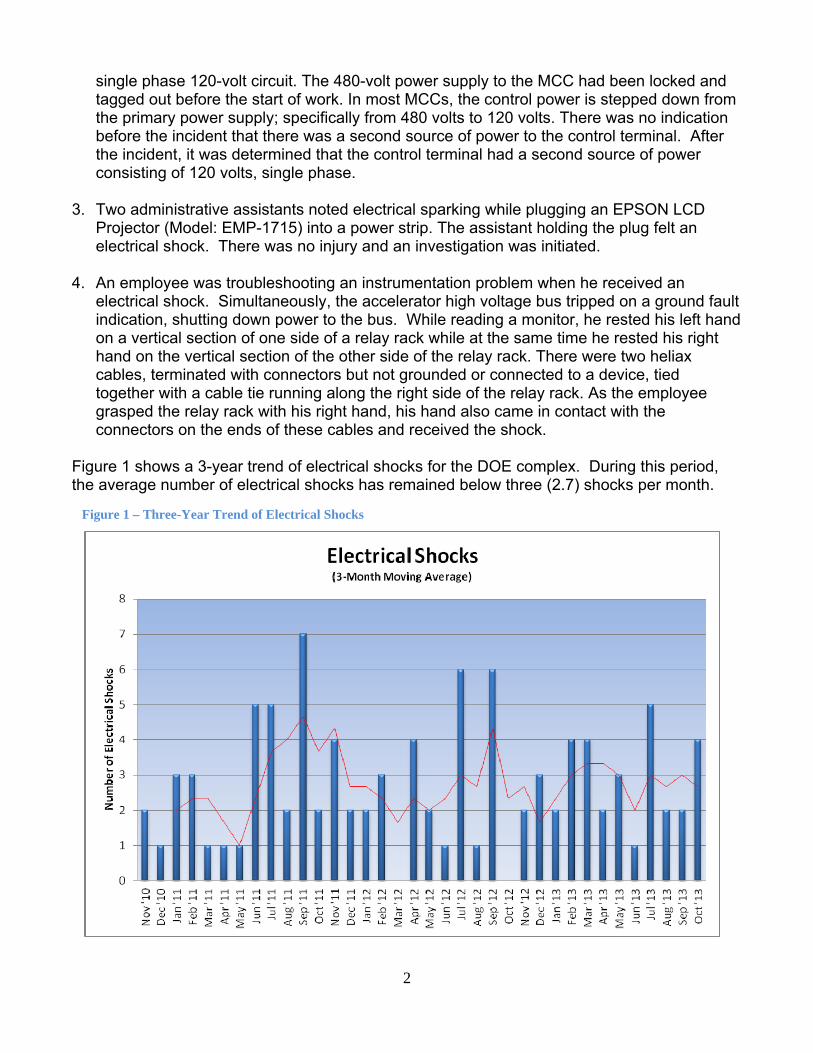
Figure 1 shows a 3-year trend of electrical shocks for the DOE complex. During this period, the average number of electrical shocks has remained below three (2.7) shocks per month.
Figure 1 – Three-Year Trend of Electrical Shocks
3
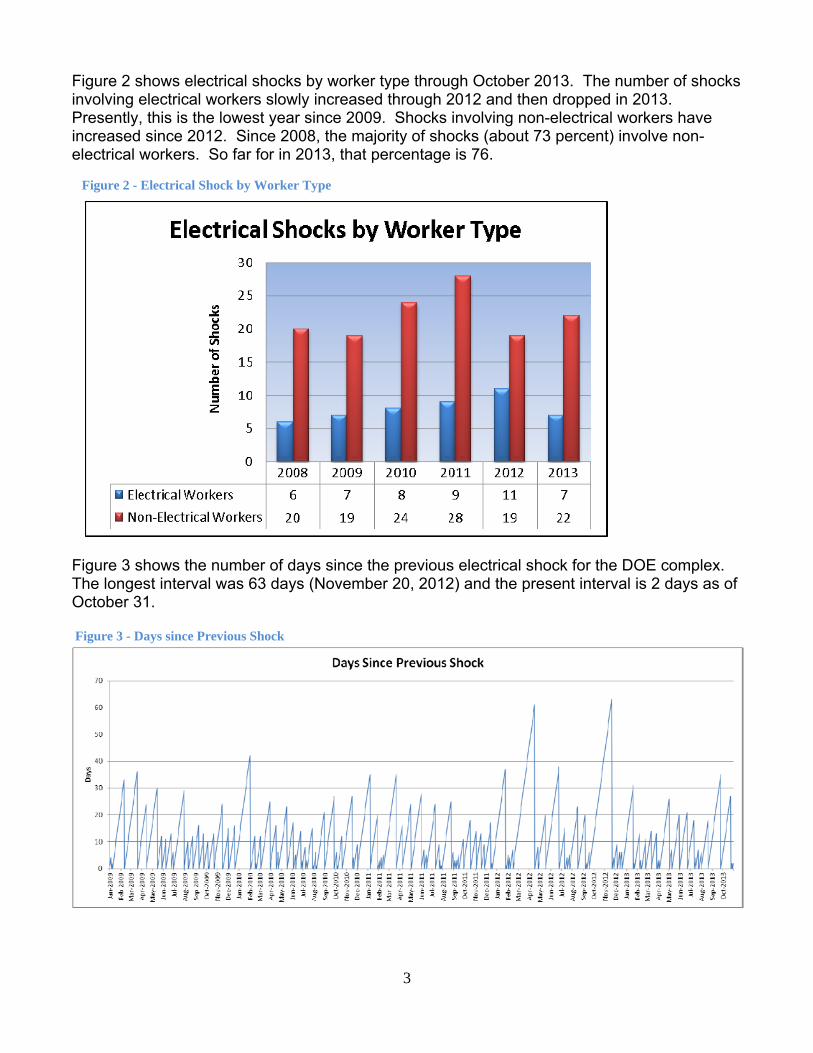
Figure 2 shows electrical shocks by worker type through October 2013. The number of shocks involving electrical workers slowly increased through 2012 and then dropped in 2013. Presently, this is the lowest year since 2009. Shocks involving non-electrical workers have increased since 2012. Since 2008, the majority of shocks (about 73 percent) involve non-electrical workers. So far for in 2013, that percentage is 76.
Figure 3 shows the number of days since the previous electrical shock for the DOE complex. The longest interval was 63 days (November 20, 2012) and the present interval is 2 days as of October 31.
Figure 3 - Days since Previous Shock
Figure 2 - Electrical Shock by Worker Type

4
Electrical Intrusion There were two electrical intrusion occurrences (i.e., cutting/penetrating, excavating, or vehicle/equipment contact of overhead electrical hazards) for October, which is the same as September. These occurrences are summarized below. 1. A roofing contractor inadvertently breached an electrical conduit containing 480-volt power to
an exhaust fan with a gas-powered roof cutter while removing old roofing material in preparation for a new roof on a building. It was unknown at the time that an electrical conduit was underneath the roofing material. The roof cutter had a depth gauge and a 7-inch blade. The depth gauge on the blade was the only barrier to prevent exposure to a hazardous energy source. Although an approved integrated work document had been issued for the roofing work, an approved penetration permit was not acquired to perform the penetration work.
2. A mechanical contractor cut into an energized 277-volt circuit with a Sawzall while cutting a 2-inch copper pipe. The contractor did not see conduit because it was obscured by the pipe. There was no shock and no injury to the worker. Lighting to two offices was impacted. A hazard analysis had been conducted for the operation. The contractor was wearing gloves and used a GFCI with the double insulated saw.
Figure 4 shows a 3-year trend of electrical intrusion occurrences for the DOE complex. During this period we have seen an average of just under 3 occurrences per month (2.2).
Figure 4 – Three-Year Trend of Electrical Intrusion Occurrences
5
Hazardous Energy Control In October there were five reported occurrences involving lockout/tagout (LOTO), which is a decrease from the six reported in September. These occurrences are summarized below. Occurrences Involving Lockout/Tagout 1. A facility operations manager, a supervisor, and electricians went to verify the isolation
point for a Controlling Organization LOTO on a tank heater control panel and discovered that the locking T bar was not installed in the locking device, which was found in the bottom of the panel. The use of the locking device was suspended pending an investigation.
2. Pipefitters determined that a LOTO for the replacement of solenoid drain valves had only locked out the heat trace circuit and not the solenoid valves when they heard the solenoid valve activate while removing tank insulation. An Instrument Shop supervisor traced out the source of power and found that the solenoid valves were powered from a circuit breaker panel and not the disconnect switch that served only the heat trace.
3. A shift supervisor and a DOE facility representative were reviewing active LOTO record sheets in preparation to start the replacement of relief valves when the shift supervisor discovered that pressurizer heaters were not part of that LOTO as required to enter the area. Crafts personnel had signed into the LOTO and had entered the area for a job walk-down. There was no electrical hazard present during the walk-down. A critique was held.
4. A subcontractor connected motor wires to a vacuum pump without proper implementation of a LOTO permit. The subcontractor believed that they could proceed because the circuit was protected by an administrative LOTO lock. The work resulted in the violation of the 'one worker, one lock' requirement.
5. Two employees violated the site LOTO process when they opened a panel on a recently installed instrument without applying personal locks. Although the instrument was not in service, a 120-volt circuit had been installed between the breaker and the instrument. The circuit had been locked out by an electrician and was verified to be in a safe condition.
Occurrences Involving Discovery of Uncontrolled Hazardous Energy
1. A safety employee noticed that the enclosure door of an electric controller box was left open, with wires hanging out of the box, without warning signs or barriers. An electrical safety engineer confirmed the box contained several energized 120-volt exposed contacts.
2. An electrical worker replaced a 120-volt circuit relay after performing a LOTO at the breakers indicated on drawings. A zero energy check indicating zero voltage. The electrician discovered an unexpected 120-volt energized source during a post-maintenance continuity check. An equipment labeling error was the problem.
Figure 5 shows a 3-year trend of LOTO occurrences for the DOE complex. The monthly average is 4.1 occurrences.

6
Figure 6 shows LOTO occurrences by worker type. The distribution by percentage is 44% for electrical workers, 31% for electrical subcontractors, 19% for non-electrical workers, and 6% for non-electrical subcontractors.
Figure 6 – LOTO Occurrences by Worker Type
Figure 5 – Three-Year Trend of Lockout/Tagout Occurrences
7
Electrical Near Miss There were three electrical near miss occurrences reported in October, which is the same number reported in September. 1. A roofing contractor inadvertently breached an electrical conduit containing 480-volt power
to an exhaust fan with a gas-powered roof cutter while removing old roofing material in preparation for a new roof on a building. (See Electrical Intrusion Section – #1)
2. A mechanical contractor cut into an energized 277-volt circuit with a power saw while cutting a 2-inch copper pipe. (See Electrical Intrusion Section – Occurrence #2)
3. An electrical arc occurred while an employee attempted to unplug a 110-volt space heater cord from a power strip. Since the cord was difficult to remove, the employee pulled hard and their hand slid off the plug and the cord separated from the plug resulting in a popping sound from the exposed arcing, which left black residue on the employee's right fingers.
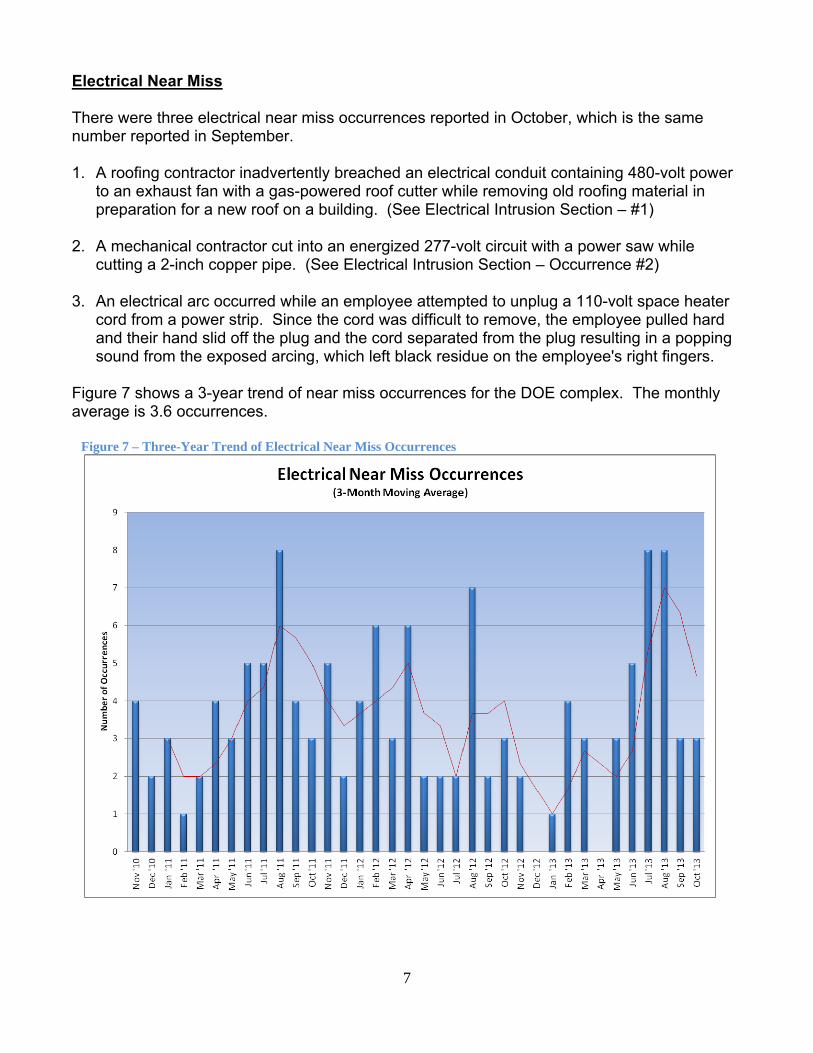
Figure 7 shows a 3-year trend of near miss occurrences for the DOE complex. The monthly average is 3.6 occurrences.
Figure 7 – Three-Year Trend of Electrical Near Miss Occurrences

8
Monthly Occurrences Tables Table 1 shows a breakdown of the outcomes, performance issues, and worker types associated with the electrical safety occurrences for October 2013.
Table 1 - Breakdown of Electrical Occurrences
Number of Occurrences
(October)
Involving: Last Month
(September) 4 Electrical Shocks 2 0 Electrical Burns 0 5 Hazardous Energy Control (LOTO) 6 4 Inadequate Job Planning 2 2 Inadvertent Drilling/Cutting of
Electrical Conductors 1
0 Excavation of Electrical Conductors 1 0 Vehicle Intrusion of Electrical
Conductors or Equipment 0
3 Electrical Near Misses 3 6 Electrical Workers 5 9 Non-Electrical Workers 5 4 Subcontractors 5
NOTE: The numbers in the left-hand column are not intended to total the number of occurrences for the month and are only associated with the items in the center column.
In compiling the monthly totals, the search looked for occurrence discovery dates in this month [excluding Significance Category R (Recurring) reports] and for the following ORPS HQ keywords:
01K – Lockout/Tagout Electrical, 01M – Inadequate Job Planning (Electrical), 08A – Electrical Shock, 08J – Near Miss (Electrical), 12C – Electrical Safety
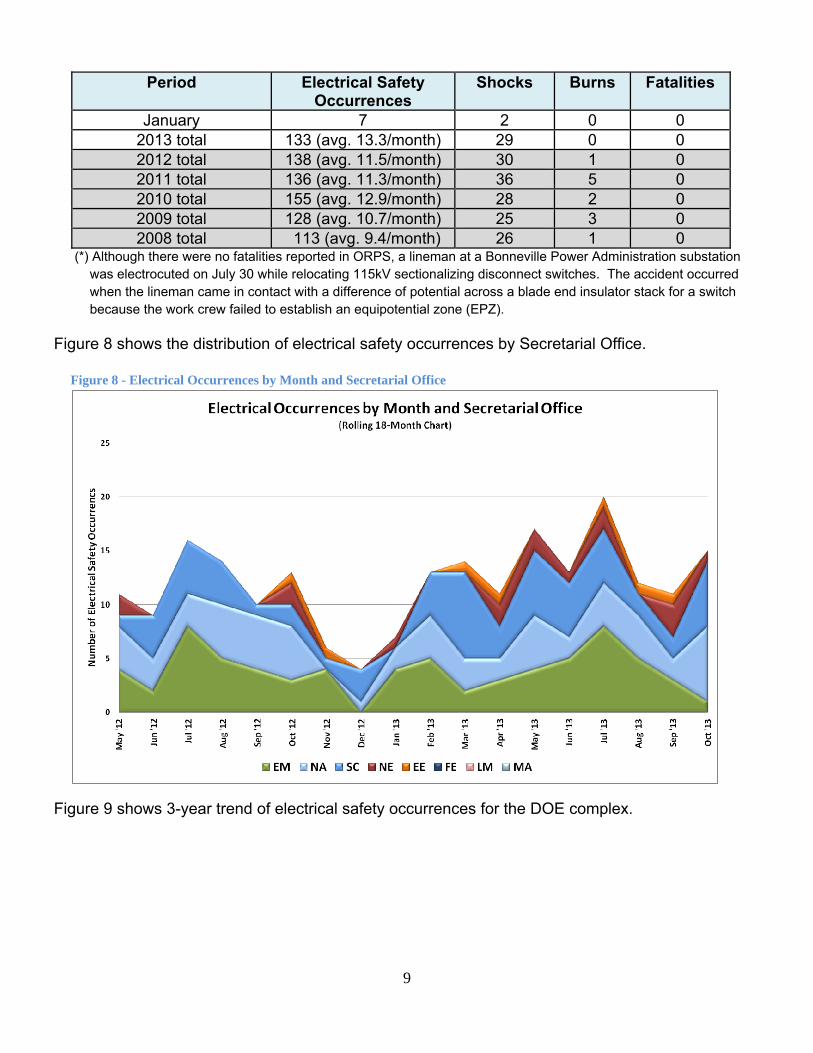
Table 2 provides a summary of the electrical safety occurrences for the previous 5 years and CY 2013. The average number of occurrences a year ago (October 2012) was 12.8 per month and the number of shocks were 25.
Table 2 - Summary of Electrical Occurrences
Period Electrical Safety Occurrences
Shocks Burns Fatalities
October 15 4 0 0 September 11 2 0 0
August 12 2 0 0 July 20 5 0 0* June 13 1 0 0 May 17 3 0 0 April 11 2 0 0
March 14 4 0 0 February 13 4 0 0
9
Period Electrical Safety Occurrences
Shocks Burns Fatalities
January 7 2 0 0 2013 total 133 (avg. 13.3/month) 29 0 0 2012 total 138 (avg. 11.5/month) 30 1 0 2011 total 136 (avg. 11.3/month) 36 5 0 2010 total 155 (avg. 12.9/month) 28 2 0 2009 total 128 (avg. 10.7/month) 25 3 0 2008 total 113 (avg. 9.4/month) 26 1 0
(*) Although there were no fatalities reported in ORPS, a lineman at a Bonneville Power Administration substation was electrocuted on July 30 while relocating 115kV sectionalizing disconnect switches. The accident occurred when the lineman came in contact with a difference of potential across a blade end insulator stack for a switch because the work crew failed to establish an equipotential zone (EPZ).
Figure 8 shows the distribution of electrical safety occurrences by Secretarial Office.
Figure 9 shows 3-year trend of electrical safety occurrences for the DOE complex.
Figure 8 - Electrical Occurrences by Month and Secretarial Office

10
Figure 9 – Three-Year Trend of Electrical Safety Occurrences
Electrical Severity The electrical severity of an electrical occurrence is based on an evaluation of electrical factors that include: electrical hazard, environment, shock proximity, arc flash proximity, thermal proximity and any resulting injury(s) to affected personnel. Calculating an electrical severity for an occurrence provides a metric that can be consistently applied to evaluate electrical occurrences across the DOE complex. Electrical Severity Scores The electrical severity scores (ES) are calculated using the Electrical Severity Measurement Tool (http://www.efcog.org/bp/p/doc/bp48-Electrical_Severity_Measurement_Tool%20R3.pdf). The seventeen occurrences are classified as shown in Table 3. Actual scores are provided in Attachment 1.
Table 3 – Classification of Electrical Safety Occurrences by ES Score Occurrence Classification
Electrical Severity Score
Number of Occurrences
HIGH ≥ 1750 0 MEDIUM 31-1749 5 LOW 0-30 10
11
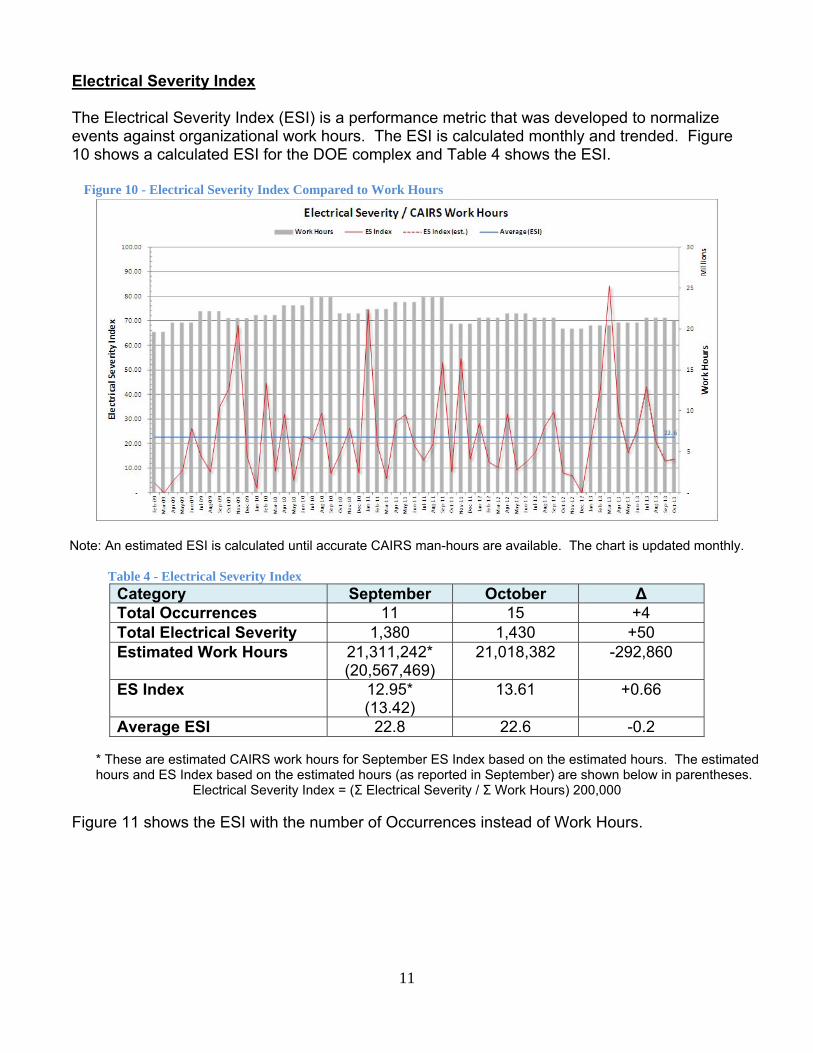
Electrical Severity Index
The Electrical Severity Index (ESI) is a performance metric that was developed to normalize events against organizational work hours. The ESI is calculated monthly and trended. Figure 10 shows a calculated ESI for the DOE complex and Table 4 shows the ESI.
Figure 10 - Electrical Severity Index Compared to Work Hours
Note: An estimated ESI is calculated until accurate CAIRS man-hours are available. The chart is updated monthly.
Table 4 - Electrical Severity Index Category September October Δ Total Occurrences 11 15 +4 Total Electrical Severity 1,380 1,430 +50 Estimated Work Hours 21,311,242*
(20,567,469) 21,018,382 -292,860
ES Index 12.95* (13.42)
13.61 +0.66
Average ESI 22.8 22.6 -0.2
* These are estimated CAIRS work hours for September ES Index based on the estimated hours. The estimated hours and ES Index based on the estimated hours (as reported in September) are shown below in parentheses.
Electrical Severity Index = (Σ Electrical Severity / Σ Work Hours) 200,000
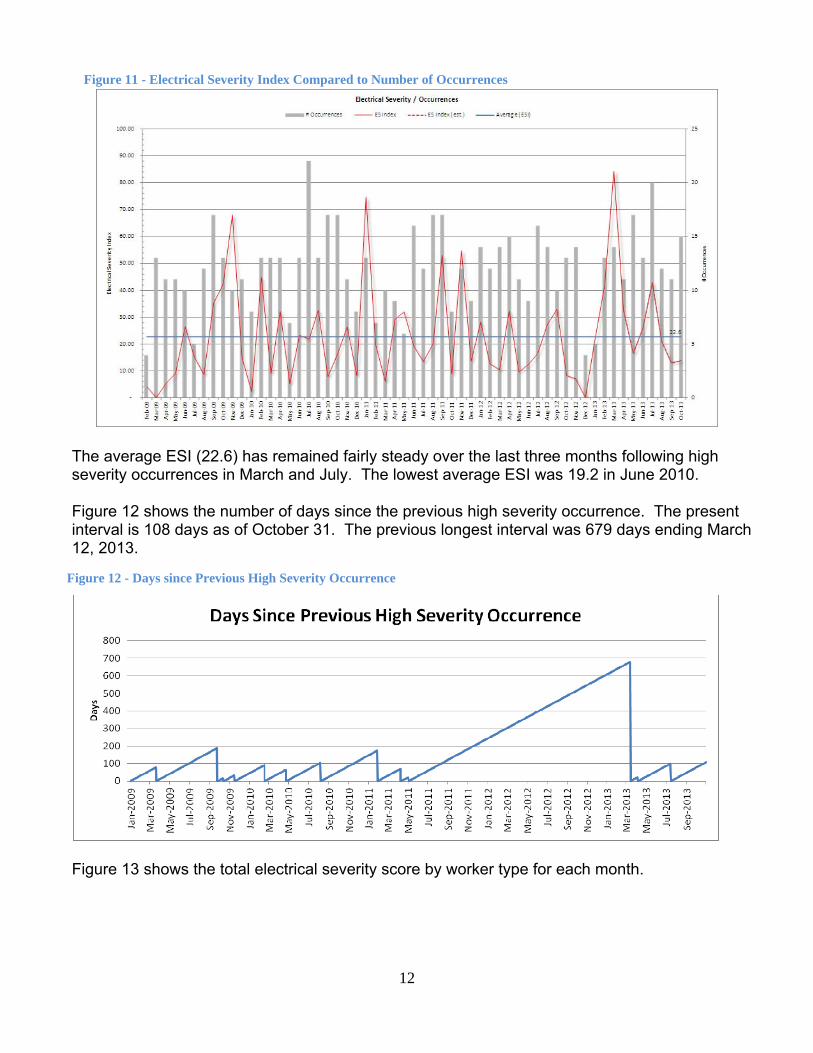
Figure 11 shows the ESI with the number of Occurrences instead of Work Hours.
12
Figure 11 - Electrical Severity Index Compared to Number of Occurrences
The average ESI (22.6) has remained fairly steady over the last three months following high severity occurrences in March and July. The lowest average ESI was 19.2 in June 2010. Figure 12 shows the number of days since the previous high severity occurrence. The present interval is 108 days as of October 31. The previous longest interval was 679 days ending March 12, 2013.
Figure 13 shows the total electrical severity score by worker type for each month.
Figure 12 - Days since Previous High Severity Occurrence

13
Figure 13 – Electrical Severity by Worker Type
The present ES score for electrical workers is 670 and 760 for non-electrical workers. Summary of Occurrences by Severity Band
For the interval October 2012 through October 2013 (current month and the past 12), Figures 14 and 15 summarize occurrences by severity band and month of discovery date by percentage of total occurrences in month and number of occurrences in month. Figure 14 - Occurrences by Electrical Severity Band (Percentage)

14
Figure 15 - Occurrences by Electrical Severity Band (Number)
The previous two charts show that a high electrical severity event occurred in March, April and July ending a 679-day period since the last occurrence in May 2011. The number of occurrences with Medium severity scores decreased slightly while the Low severity scores jumped in October. Medium and Low Severity with Trend
Figure 16 focuses on the Medium and Low severity data series for October 2012 through October 2013. Trend lines are included for each, using a 3-month moving average. Figure 16 - Trend of Medium and Low Electrical Severity Occurrences
The 3-month moving average shows a slightly decreasing trend for Low and Medium severity occurrences following an increase since the beginning of the year.

15
Additional Resources
Electrical Safety Blog http://hsselectricalsafety.wordpress.com/
Electrical Safety Wiki http://electricalsafety.doe-hss.wikispaces.net/home
EFCOG Electrical Safety Subgroup http://www.efcog.org/wg/esh_es/index.htm
Center of Excellence for Electrical Safety http://www.lanl.gov/safety/electrical/
Contact
Glenn S. Searfoss Office of Analysis, HS-24 Phone: 301-903-8085 Email: [email protected]

Attachment 1
1
Electrical Safety Occurrences – October 2013
No
Report Number
Event Summary SHOCK BURN ARCF(1) LOTO(2) PLAN(3) EXCAV(4) CUT/D(5) VEH(6) SC(7) RC(8)
ES(9)
1
EM-RL--CPRC-GPP-2013-0006
A locking T bar was not installed in the locking device and was found in the bottom of the panel.
X 4 2E(3) 0
2
NA--KCSO-AS-KCP-2013-0008
A protective force officer received a minor electrical shock while unplugging a defective extension cord from a 110-volt outlet.
X 2 2E(1) 330
3
NA--LASO-LANL-ACCCOMPLEX-2013-0012
A breaker for a heater (208V) was locked and tagged out but later removed without coordinating the removal of the LOTO.
X 4 10(2) 0
4
NA--LASO-LANL-FIRNGHELAB-2013-0004
A roofing contractor inadvertently breached an electrical conduit containing 480V power with a gas-powered roof cutter.
X 3 10(3) 0
5
NA--LASO-LANL-TA55-2013-0031
An electrician received a minor 120V shock to his right ring finger while performing breaker maintenance on a MCC.
X X 2 2E(1) 330
6
NA--PS-BWP-PANTEX-2013-0065
It was discovered that electrical power to solenoid valves had not be locked out as required when the valves operated.
X X 3 2E(2) 10
7
NA--SS-SNL-NMFAC-2013-0006
A mechanical contractor cut into an energized 277V circuit with a Sawzall while cutting a pipe.
X 3 2E(2) 50
8
NA--YSO-BWXT-Y12SITE-2013-0025
A worker attempted to unplug a 110V space heater cord from a power strip when the plug separated from the cord and arced.
3 10(3) 20
9
NE-ID--BEA-ATR-2013-0036
The circuit for 480V pressurizer heaters was not locked out as required for entry into the area.
X 4 2E(3) 0
10
SC--BHSO-BNL-BNL-2013-0009
Worker receives electrical shock while plugging in a laptop video projector to a power strip.
X 2 2E(1) 330

Attachment 1
2
No
Report Number
Event Summary SHOCK BURN ARCF(1) LOTO(2) PLAN(3) EXCAV(4) CUT/D(5) VEH(6) SC(7) RC(8)
ES(9)
11
SC--BSO-LBL-EHS-2013-0003
A safety employee noticed the enclosure door of an electric controller box was left open with exposed energized 120V circuits.
3 2E(2) 20
12
SC--BSO-LBL-OPERATIONS-2013-0019
A subcontractor, worked on a vacuum pump without implementing a LOTO permit.
X 4 2E(3) 0
13
SC--FSO-FNAL-FERMILAB-2013-0008
An employee was troubleshooting an instrumentation problem when he received an electrical shock.
X 2 2E(1) 330
14
SC-ORO--ORNL-X10EAST-2013-0010
An electrician replaced a 120V circuit relay under a LOTO and an unexpected energized source was later discovered.
X 3 2E(2) 0
15
SC-ORO--ORNL-X10WEST-2013-0002
Two employees violated the LOTO process when they opened an instrument panel without applying personal locks.
X 4 2E(3) 10
TOTAL 4 0 0 5 4 0 2 0
Key (1) ARCF = significant arc flash, (2) LOTO = lockout/tagout, (3) PLAN = job planning, (4) EXCAV = excavation/penetration, (5) CUT/D = cutting or drilling, (6) VEH = vehicle or equipment intrusion, (7) SC = ORPS significance category, (8) RC = ORPS reporting criteria, (9) ES = electrical severity ES Scores: High is > 1750, Medium is 31-1749, and Low is 1-30

Attachment 1
3
Electrical Safety Occurrences – October 2013
No
Report Number
Event Summary EW(1) N-EW(2) SUB(3) HFW(4)
WFH(5) PPE(6) 70E(7)
VOLT(8)
H L C/I(9) NEUT(10) NM(11)
1 EM-RL--CPRC-GPP-2013-0006
A locking T bar was not installed in the locking device and was found in the bottom of the panel.
X X X
2
NA--KCSO-AS-KCP-2013-0008
A protective force officer received a minor electrical shock while unplugging a defective extension cord from a 110-volt outlet.
X X X
3
NA--LASO-LANL-ACCCOMPLEX-2013-0012
A breaker for a heater (208V) waslocked and tagged out but later removed without coordinating the removal of the LOTO.
X X X
4
NA--LASO-LANL-FIRNGHELAB-2013-0004
A roofing contractor inadvertently breached an electrical conduit containing 480V power with a gas-powered roof cutter.
X X X X X
5
NA--LASO-LANL-TA55-2013-0031
An electrician received a minor 120V shock to his right ring finger while performing breaker maintenance on a MCC.
X X X
6
NA--PS-BWP-PANTEX-2013-0065
It was discovered that electrical power to solenoid valves had not be locked out as required when the valves operated.
X X X
7
NA--SS-SNL-NMFAC-2013-0006
A mechanical contractor cut into an energized 277V circuit with a Sawzall while cutting a pipe.
X X X X X
8
NA--YSO-BWXT-Y12SITE-2013-0025
A worker attempted to unplug a 110V space heater cord from a power strip when the plug separated from the cord and arced.
X X X X
9
NE-ID--BEA-ATR-2013-0036
The circuit for 480V pressurizer heaters was not locked out as required for entry into the area.
X X X
10
SC--BHSO-BNL-BNL-2013-0009
Worker receives electrical shock while plugging in a laptop video projector to a power strip.
X X X

Attachment 1
4
No
Report Number
Event Summary EW(1) N-EW(2) SUB(3) HFW(4)
WFH(5) PPE(6) 70E(7)
VOLT(8)
H L C/I(9) NEUT(10) NM(11)
11 SC--BSO-LBL-EHS-2013-0003
A safety employee noticed the enclosure door of an electric controller box was left open with exposed energized 120V circuits.
X X X X
12
SC--BSO-LBL-OPERATIONS-2013-0019
A subcontractor, worked on a vacuum pump without implementing a LOTO permit.
X X X X
13
SC--FSO-FNAL-FERMILAB-2013-0008
An employee was troubleshooting an instrumentation problem when he received an electrical shock.
X X X
14
SC-ORO--ORNL-X10EAST-2013-0010
An electrician replaced a 120V circuit relay under a LOTO and an unexpected energized source was later discovered.
X X X
15
SC-ORO--ORNL-X10WEST-2013-0002
Two employees violated the LOTO process when they opened an instrument panel without applying personal locks.
X X X X
TOTAL 6 9 4 7 8 0 1 0 15 0 0 3
Key (1) EW = electrical worker, (2) N-EW = non-electrical worker, (3) SUB = subcontractor, (4) HFW = hazard found the worker, (5) WFH = worker found the hazard, (6) PPE = inadequate or no PPE used, (7) 70E = NFPA 70E issues, (8) VOLT = H (>600) L(≤600), (9) C/I = Capacitance/Inductance, (10) NEUT = neutral circuit, (11) NM = near miss
Attachment 2
1
ORPS Operating Experience Report
ORPS contains 56423 OR(s) with 59733 occurrences(s) as of 12/9/2013 12:40:20 PM
Query selected 15 OR(s) with 15 occurrences(s) as of 12/9/2013 12:41:19 PM
Download this report in Microsoft Word format.
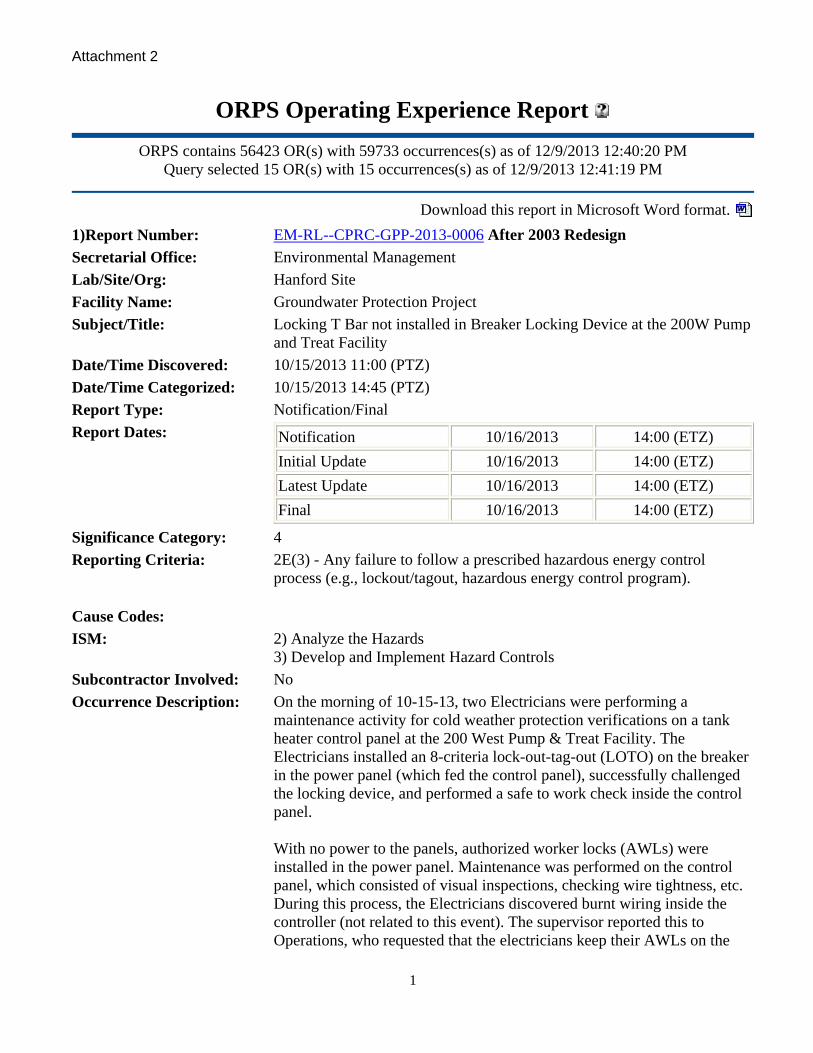
1)Report Number: EM-RL--CPRC-GPP-2013-0006 After 2003 Redesign
Secretarial Office: Environmental Management
Lab/Site/Org: Hanford Site
Facility Name: Groundwater Protection Project
Subject/Title: Locking T Bar not installed in Breaker Locking Device at the 200W Pump and Treat Facility
Date/Time Discovered: 10/15/2013 11:00 (PTZ)
Date/Time Categorized: 10/15/2013 14:45 (PTZ)
Report Type: Notification/Final
Report Dates: Notification 10/16/2013 14:00 (ETZ)
Initial Update 10/16/2013 14:00 (ETZ)
Latest Update 10/16/2013 14:00 (ETZ)
Final 10/16/2013 14:00 (ETZ)
Significance Category: 4
Reporting Criteria: 2E(3) - Any failure to follow a prescribed hazardous energy control process (e.g., lockout/tagout, hazardous energy control program).
Cause Codes:
ISM: 2) Analyze the Hazards 3) Develop and Implement Hazard Controls
Subcontractor Involved: No
Occurrence Description: On the morning of 10-15-13, two Electricians were performing a maintenance activity for cold weather protection verifications on a tank heater control panel at the 200 West Pump & Treat Facility. The Electricians installed an 8-criteria lock-out-tag-out (LOTO) on the breaker in the power panel (which fed the control panel), successfully challenged the locking device, and performed a safe to work check inside the control panel. With no power to the panels, authorized worker locks (AWLs) were installed in the power panel. Maintenance was performed on the control panel, which consisted of visual inspections, checking wire tightness, etc. During this process, the Electricians discovered burnt wiring inside the controller (not related to this event). The supervisor reported this to Operations, who requested that the electricians keep their AWLs on the
Attachment 2
2
circuit until a controlling organization (CO) LOTO could be prepared and installed. At approximately 1055 hours, the facility operations manager went with the supervisor and electricians to verify the isolation point for the CO LOTO. At that time, it was observed that the locking T bar was not installed in the locking device, and that a locking T-bar was present at the bottom of the panel. No personnel came in contact with the electrical energy, and no material damage was discovered as a result of this event. Work was stopped. An ORPS occurrence was declared - Group 2, Subgroup E, Hazardous Electrical Energy Control, (3) SC-4. Notifications were made and a field investigation was initiated.
Cause Description:
Operating Conditions: Operating Conditions were normal at the time of the occurrence
Activity Category: Normal Operations (other than Activities specifically listed in this Category)
Immediate Action(s): -Work activity was stopped. -Area was cleared of personnel. -Suspended further use of the locking device pending completion of an investigation. -Event scene was preserved. -Notifications of the event were made. -Initial investigation was conducted. -Critique is being scheduled.
FM Evaluation:
DOE Facility Representative Input:
DOE Program Manager Input:
Further Evaluation is Required:
No
Division or Project: CHPRC Soil and Groundwater Remediation Project
Plant Area: 200 West Area
System/Building/Equipment: 200W Pump and Treat Facility
Facility Function: Environmental Restoration Operations
Corrective Action:
Lessons(s) Learned:
HQ Keywords: 01K--Inadequate Conduct of Operations - Lockout/Tagout Noncompliance (Electrical) 08H--OSHA Reportable/Industrial Hygiene - Safety Noncompliance 12I--EH Categories - Lockout/Tagout (Electrical or Mechanical) 14E--Quality Assurance - Work Process Deficiency
HQ Summary: On October 15, 2013, a facility operations manager, a supervisor, and

Attachment 2
3
electricians went to verify the isolation point for a Controlling Organization lockout/tagout on a tank heater control panel at the 200 West Pump & Treat Facility and discovered that the locking T bar was not installed in the locking device, which was found in the bottom of the panel. No personnel came in contact with the electrical energy, and no material damage was discovered as a result of this event. The use of the locking device has been suspended pending completion of an investigation.
Similar OR Report Number:
Facility Manager: Name BARMETTLOR, ROBERT B
Phone (509) 373-9501
Title MANAGER OF OPERATIONS ASSURANCE
Originator: Name NELSON, ROBERT J.
Phone (509) 373-6657
Title OPERATIONS SPECIALIST
HQ OC Notification: Date Time Person Notified Organization
NA NA NA NA
Other Notifications: Date Time Person Notified Organization
10/15/2013 14:45 (PTZ) Bill Barrett CHPRC
10/15/2013 15:30 (PTZ) Brian Biro DOE-RL
10/15/2013 15:31 (PTZ) Bob Popielarczyk CHPRC
10/15/2013 16:05 (PTZ) Hanford ONC DOE
Authorized Classifier(AC):
2)Report Number: NA--KCSO-AS-KCP-2013-0008 After 2003 Redesign
Secretarial Office: National Nuclear Security Administration
Lab/Site/Org: Kansas City Plant
Facility Name: Kansas City Plant
Subject/Title: Employee Receives Minor Electrical Shock Unplugging a Cord for Electric Scooter Charging Unit
Date/Time Discovered: 10/23/2013 10:15 (CTZ)
Date/Time Categorized: 10/23/2013 12:00 (CTZ)
Report Type: Update
Report Dates: Notification 10/24/2013 17:24 (ETZ)
Initial Update 10/25/2013 08:31 (ETZ)
Latest Update 10/28/2013 08:59 (ETZ)
Final
Attachment 2
4
Significance Category: 2
Reporting Criteria: 2E(1) - Any unexpected or unintended personal contact (burn, injury, etc.) with an electrical hazardous energy source (e.g., live electrical power circuit, etc.).
Cause Codes:
ISM: 2) Analyze the Hazards 4) Perform Work Within Controls
Subcontractor Involved: No
Occurrence Description: On October 23, 2013, at approximately 1015 hours a Honeywell Federal Manufacturing & Technologies Kansas City (FM&T/KC) Protective Force Officer (PFO) received a minor electrical shock while unplugging an extension cord from a 110 volt duplex wall outlet. The other end of the extension cord is hard wired to the charging unit for an indoor plant vehicle (scooter) at the National Security Campus (NSC). The PFO reported to their manager describing the shock as a "tingle". The employee reported to FM&T/KC Medical Care Services for evaluation, and was subsequently released back to full duty.
Cause Description:
Operating Conditions: Does not apply.
Activity Category: Normal Operations (other than Activities specifically listed in this Category)
Immediate Action(s): An electrician was requested to check out the electrical outlet and the electric vehicle (scooter). No defects were found with the electrical outlet. The plug on the scooter charging cord was found to have a gap in the insulation, and was subsequently repaired on the spot. A FM&T/KC Health Safety & Environment (HS&E) Engineer was notified and briefed. The remaining electric scooters used by the Protective Force Officers at the National Security Campus were evaluated for electrical issues. No issues were identified. This report has been reviewed and determined to be unclassified by: Derivative Classifier: Clyde E. Hicks Title: HS&E Administrator II Date: October 28, 2013
FM Evaluation: The incident investigator confirmed on October 28, 2013 the cord was repaired, not replaced.
DOE Facility Representative Input:
DOE Program Manager Input:
Further Evaluation is Required:
No

Attachment 2
5
Division or Project: Honeywell Federal MFG. & Technologies Kansas City
Plant Area: NSC Bldg. 2
System/Building/Equipment: Electric scooter (leased)
Facility Function: Balance of Plant - Infrastructure (Other Functions not specifically listed in this Category)
Corrective Action 01: Target Completion Date:10/23/2013
Actual Completion Date:10/23/2013
Evaluate the electrical outlet and electric scooter for corrective actions.
Corrective Action 02: Target Completion Date:10/23/2013
Actual Completion Date:10/23/2013
Repair the plug on the electric scooter charging cord.
Corrective Action 03: Target Completion Date:10/23/2013
Actual Completion Date:10/23/2013
Evaluate remaining National Security Campus Protective Force electric vehicles for issues - none identified.
Lessons(s) Learned:
HQ Keywords: 07D--Electrical Systems - Electrical Wiring 08A--OSHA Reportable/Industrial Hygiene - Electrical Shock 12C--EH Categories - Electrical Safety 14L--Quality Assurance - No QA Deficiency
HQ Summary: On October 23, 2013, a Honeywell Federal Manufacturing & Technologies Kansas City (FM&T/KC) Protective Force officer received a minor electrical shock while unplugging an extension cord from a 110-volt duplex wall outlet. The other end of the extension cord is hard wired to the charging unit for an indoor plant vehicle (scooter) at the National Security Campus. The officer reported to their manager describing the shock as a "tingle". The employee reported to FM&T/KC Medical Care Services for evaluation, and was subsequently released back to full duty. No defects were found with the electrical outlet; however, the plug on cord had a gap in the insulation and it was repaired on the spot.
Similar OR Report Number:
Facility Manager: Name Kevin Allgeyer
Phone (816) 488-5107
Title Sr. Health, Safety & Environment (HS&E) Manager
Originator: Name HICKS, CLYDE E
Phone (816) 997-2262
Title EMERGENCY MGT SPECIALIST
HQ OC Notification: Date Time Person Notified Organization

Attachment 2
6
NA NA NA NA
Other Notifications: Date Time Person Notified Organization
10/23/2013 13:40 (CTZ) M. Roberts KCFO
Authorized Classifier(AC): Clyde E. Hicks Date: 10/28/2013
3)Report Number: NA--LASO-LANL-ACCCOMPLEX-2013-0012 After 2003 Redesign
Secretarial Office: National Nuclear Security Administration
Lab/Site/Org: Los Alamos National Laboratory
Facility Name: Accelerator Complex
Subject/Title: Management Concern: Potential Impacts from Energized Heater in Substation Identified during Maintenance
Date/Time Discovered: 10/16/2013 13:04 (MTZ)
Date/Time Categorized: 10/25/2013 10:46 (MTZ)
Report Type: Notification/Final
Report Dates: Notification 10/29/2013 20:06 (ETZ)
Initial Update 10/29/2013 20:06 (ETZ)
Latest Update 10/29/2013 20:06 (ETZ)
Final 10/29/2013 20:06 (ETZ)
Revision 1 10/31/2013 13:19 (ETZ)
Significance Category: 4
Reporting Criteria: 10(2) - An event, condition, or series of events that does not meet any of the other reporting criteria, but is determined by the Facility Manager or line management to be of safety significance or of concern for that facility or other facilities or activities in the DOE complex. The significance category assigned to the management concern should be based on an evaluation of the potential risks and impact on safe operations. (1 of 4 criteria - This is a SC 4 occurrence)
Cause Codes:
ISM: 2) Analyze the Hazards 4) Perform Work Within Controls
Subcontractor Involved: No
Occurrence Description: MANAGEMENT SYNOPSIS: At 1304 on October 16, 2013, after opening the door to Cubicle HV of a substation at Technical Area 53, Sector B, the Utilities and Infrastructure (UI) linemen smelled a burning odor. Further inspection found the source of the odor was an energized heater inside Cubicle HV on the north side of the substation. Following identification of the source, the AOT-RFE personnel shut off the heater breaker. Using a ten-foot insulated stick and wearing 15 kV personal protective equipment (PPE) including Class 2 di-electric gloves, the
Attachment 2
7
lineman removed the grounding cluster from Cubicle HV. At the time, the linemen were supporting the Accelerator Operations and Technology Radio Frequency Engineering Group (AOT-RFE) maintenance activities on the transformer rectifier unit. The AOT-RFE work documentation specified that during transformer rectifier maintenance the heater breaker (208V) is to be locked and tagged out. The AOT-RFE management stated that the heater breaker had been locked and tagged out (LOTO) for their portion of the work on the south cubicle, but they removed the LOTO after they completed their portion of the maintenance. The linemen’s portion of the work was performed in the north cubicle. Prior to removing the grounding cluster, the linemen discussed the status of the heater with the AOT-RFE engineer that led the engineer to have the circuit de-energized. Based on their PPE, not conducting work on the heater circuit or within the subject cubicle, and the use of the insulated stick, the linemen determined that their work documentation and controls were appropriate to proceed safely with the task. Therefore, the linemen and the AOT-RFE personnel did not perceive an actual event occurred; thus, did not report the event on October 16, 2013. This event did not result in any impact to the safety and health of the workers, operations, equipment, or the facility. On October 24, 2013, the AOT-RFE engineer discussed the event with the AOT RFE Group Leader. At 0956 and following the discussion, event notification was made to the Utilities and Infrastructure Facility Operations Director Designee. At 1046 on October 25, 2013, because of the potential that workers may have been exposed to hazardous electrical energy, the UI FOD Designee conservatively categorized the event as reportable under the Hazardous Electrical Energy criteria pending a critique. On October 28, 2013, the UI FOD Designee convened a critique. Because the linemen wore the 15 kV PPE, used the ten-foot insulated stick to perform the work and the heater breaker was isolated prior to removing the grounding cluster, the Chief Electrical Safety Officer determined that the workers were not exposed to hazardous electrical energy. Further the institutional LOTO program manager deemed that there was no LOTO violation because the LOTO was identified in the work documentation and had been utilized; the LOTO was removed out-of-sequence and before all activities were completed. However, there were concerns that the linkage between the AOT-RFE and UI linemen activities was inadequate. The AOT-RFE personnel removed the LOTO before all activities were completed which was not the preferred scenario. Because they received verbal notification that the heater breaker was isolated and based on their assessment that the work controls and prescribed PPE were appropriate, the linemen felt that no LOTO was required and proceeded with the task. At 1115, because of the communication and linkage concerns, the UI FOD Designee re-categorized the event as Management Concern, Significance

Attachment 2
8
Category 4 event. BACKGROUND: According to the UI linemen management, the linemen were supporting the AOT-RFE maintenance activities that required the linemen to add the grounding cluster following de-energizing the substation, then removing the grounding cluster prior to re-energizing the substation. The linemen performed this work in accordance with a switching procedure for Transformer TA-53-0074. The AOT-RFE maintenance activities were authorized via Integrated Work Document IWD-OPS-1012 Procedure, "Electrically Securing the LANSCE Accelerator Sectors A-H and ETL 805 High-Voltage Pads Equipment." Prior to the start of work on October 15, 2013, the AOT-RFE management conducted an informal pre-job briefing where the AOT-RFE and linemen work activities were discussed. The linemen also held a pre-job briefing to review their switching procedure. At 0800, the AOT-RFE deputy group leader locked and tagged out the heater breaker in the south cubicle. At 0833, the linemen began the switching procedure for Transformer TA-53-0074. The linemen verified the specified circuit breakers were opened. Next, the linemen tested and verified the circuit was de-energized and applied the grounds in the north cubicle. The AOT-RFE personnel then performed their maintenance activities on the south cubicle. On October 16, 2013, the AOT-RFE asked the linemen to re-energize the substation. Prior to the start of work, the AOT-RFE deputy group leader reviewed the work activities and the linemen reviewed their switching procedure. Prior to 1304, the AOT-RFE deputy group leader removed the LOTO from the heater breaker. At 1304, the AOT-RFE group leader opened the door to the north cubicle so that the linemen could remove the grounding cluster. After the door was opened, the linemen smelled the burning odor. Further inspection found that the energized heater was the source of the odor. The workers subsequently indicated that they were unaware of the heater’s location in the north cubicle and that it was fed by the heater breaker in the south cubicle.
Cause Description:
Operating Conditions: Transformer Rectifier Maintenance
Activity Category: Maintenance
Immediate Action(s): 1. The AOT-RFE management will revise the IWD to add a step stating that the heater LOTO will remain in place until the linemen complete their work. After the IWD has been revised and approved, the appropriate AOT-RFE personnel will be briefed to the revised IWD. 2. The AOT-RFE management will task personnel to identify and post the hazards on the substation.

Attachment 2
9
3. The AOT-RFE management will perform an engineering assessment of seven (7) substations to determine if the heater is required or not. Based on the assessment results, the AOT-RFE management will take action as warranted. 4. The UI work control personnel will revise the linemen work document to add a step to verify that the substation heater or any low voltage circuit hazards have been assessed and appropriate controls implemented prior to the start of work.
FM Evaluation:
DOE Facility Representative Input:
DOE Program Manager Input:
Further Evaluation is Required:
No
Division or Project: Accelerator Operations & Technology Division
Plant Area: TA-53-Sector B
System/Building/Equipment: Substation Heater, 208V
Facility Function: Balance-of-Plant - Site/outside utilities
Corrective Action:
Lessons(s) Learned:
HQ Keywords: 01A--Inadequate Conduct of Operations - Inadequate Conduct of Operations (miscellaneous) 01E--Inadequate Conduct of Operations - Operations Procedure Noncompliance 01M--Inadequate Conduct of Operations - Inadequate Job Planning (Electrical) 01P--Inadequate Conduct of Operations - Inadequate Oral Communication12B--EH Categories - Conduct of Operations 14D--Quality Assurance - Documents and Records Deficiency 14E--Quality Assurance - Work Process Deficiency
HQ Summary: On October 16, 2013, after opening the door to Cubicle HV of a substation at Technical Area 53, Sector B, the Utilities and Infrastructure linemen smelled a burning odor. Further inspection found the source of the odor was an energized heater inside Cubicle HV. Following identification of the source, the Accelerator Operations and Technology Radio Frequency Engineering (AOT-RFE) personnel shut off the heater breaker. Using a ten-foot insulated stick and wearing 15 kV personal protective equipment the lineman removed the grounding cluster from Cubicle HV. At the time, the linemen were supporting the AOT-RFE maintenance activities on the transformer rectifier unit. The AOT-RFE work documentation specified that during transformer rectifier maintenance the heater breaker (208V) is

Attachment 2
10
to be locked and tagged out. The AOT-RFE management stated that the heater breaker had been locked and tagged out (LOTO) for their portion of the work on the south cubicle, but they removed the LOTO after they completed their portion of the maintenance. The linemen’s portion of the work was performed in the north cubicle.
Similar OR Report Number:
Facility Manager: Name Lawrence Chavez
Phone (505) 699-7606
Title UI Facility Operations Manager Designee
Originator: Name YAZZIE, ALVA M
Phone (505) 664-0666
Title OCCURRENCE INVESTIGATOR
HQ OC Notification: Date Time Person Notified Organization
NA NA NA NA
Other Notifications: Date Time Person Notified Organization
10/28/2013 06:45 (MTZ) Dave George NNSA
10/28/2013 11:15 (MTZ) Curtis McHaley NNSA
10/28/2013 11:15 (MTZ) Dave George NNSA
Authorized Classifier(AC): Linda Collier Date: 10/31/2013
4)Report Number: NA--LASO-LANL-FIRNGHELAB-2013-0004 After 2003 Redesign
Secretarial Office: National Nuclear Security Administration
Lab/Site/Org: Los Alamos National Laboratory
Facility Name: Firing Sites and HE Lab.
Subject/Title: Near Miss to Personnel Exposure to Hazardous Energy Source: Electrical Conduit Damaged During Roofing Demolition Operations
Date/Time Discovered: 10/11/2013 09:30 (MTZ)
Date/Time Categorized: 10/11/2013 10:30 (MTZ)
Report Type: Final
Report Dates: Notification 10/17/2013 17:25 (ETZ)
Initial Update 11/27/2013 13:50 (ETZ)
Latest Update 11/27/2013 13:50 (ETZ)
Final 11/27/2013 13:50 (ETZ)
Significance Category: 3
Reporting Criteria: 10(3) - A near miss to an otherwise ORPS reportable event, where something physically happened that was unexpected or unintended, or where no or only one barrier prevented an event from having a reportable

Attachment 2
11
consequence. The significance category assigned to the near miss must be based on an evaluation of the potential risks and extent of personnel exposure to the hazard. (1 of 3 criteria - This is a SC 3 occurrence)
Cause Codes: A1B3C02 - Design/Engineering Problem; Design / documentation LTA; Design/documentation not up-to-date A4B1C01 - Management Problem; Management Methods Less Than Adequate (LTA); Management policy guidance / expectations not well-defined, understood or enforced
ISM: 2) Analyze the Hazards 5) Provide Feedback and Continuous Improvement
Subcontractor Involved: Yes Schreiber Roofing Contractor
Occurrence Description: MANAGEMENT SYNOPSIS On October 11, 2013, at 0930, at Los Alamos National Laboratory (LANL), Technical Area 9, Building 0021 (TA9-21), while conducting roofing demolition activities, a Schreiber Roofing worker (W1) inadvertently damaged an electrical conduit with a gas powered roof cutter during the removal of the first layer or roofing material of a multi-layered roof. The scope of work was to remove the old roofing material layers in preparation for a new roof. The process for removal of the old roofing layers consisted of cutting out each 5-6 inch deep layer in sections prior to manually removing with hand tools. It was unknown at the time that an electrical conduit existed under the roofing layer being removed. The roof cutter was equipped with a depth gauge and a 7 inch blade. The depth gauge was set at 1.5 inches which required the worker to take more than one cut to reach the final depth of the roofing material. The electrical conduit was damaged during the workers first cut. The work activity was performed in accordance with an approved Integrated Work Document (IWD). When the roofing crew lifted the section of roof, they discovered an electrical conduit line had been installed on the surface of the original roofing layer beneath the layer being removed. The work was immediately paused and notifications were made to the Weapons Facilities Operations (WFO) Manager. The Weapons Facilities Operations Director (WFO FOD), WFO Electrical Safety Officer, and the High Explosives Science and Technology (WX-7) Group Leader were also notified of the event. At 1030, the WFO FOD initially categorized the event as sub-ORPS. On October 15, 2013, at 1530, a critique was convened. Information obtained at the critique caused the WFO Deputy FOD to be concerned about the work planning process for the project. In particular, the applicability of penetration permits and the adequacy of information
Attachment 2
12
regarding potential hazards and subsequent controls prior to commencing work. The event was subsequently re-categorized to a Management Concern Near Miss, 10(3c), due to the potential for unexpected or unintended personal contact with an electrical hazardous energy source. The results of the electrical severity significance evaluation by the Chair of the Laboratory's Electrical Safety Committee was that since the insulation was not compromised and no breaker tripped, there was no exposure to a hazardous energy source, and the Electrical Severity Measurement Tool gave a score of zero. There were no personnel injuries, no impact to the environment, and minor impact to the program as a result of this event. BACKGROUND The roofing work is part of the Department of Energy (DOE) Roof Asset Management Program (RAMP). The DOE has contracted the RAMP work to Building Technology Associates (BTA) who in turn subcontracted the LANL roofing project to Schreiber Roofing. The Facility and Infrastructure Recapitalization Project Group (FIRP) manages the LANL roofing project under a DOE agreement. According to the DOE Los Alamos Field Office RAMP Project Director and the BTA RAMP Complex-wide Representative, the RAMP project has not been required to obtain a penetration permit at any DOE site for roofing demolition activities. Project planning for the TA9-21 roof replacement was conducted normally. This included characterization and walkdowns for developing the required project documents. During the walkdowns it was determined that the rooftop equipment at TA9-21 could remain in place and would not need to be de-energized in order to perform the roofing demolition and re-roofing activities. EVENT SEQUENCE At 0730, on October 11, 2013, Schreiber held their daily safety meeting prior to beginning work. The workers then proceeded to check their equipment. The power to the rooftop exhaust fans was turned off, but not de-energized using a lock out tag out (LO/TO) process. This was according to procedure. At 0900 roof cutting operations commenced using a power cutter machine with the cutting blade locked at a 1.5 inch setting. The marked section being cut was approximately six (6) inches from the roof crown. The roofer was not wearing dielectric gloves while performing cutting work as they were not required for the cutting work.

Attachment 2
13
At 0930, while the roofer was making a cut, he felt and heard a connection with metal. The roofer believed he had contacted the metal decking structure of the roof. The roofer did not observe arcing, nor did he experience an electrical shock upon contact. The roofer immediately discontinued the cutting work and stepped back from the area. He notified the Schreiber foreman of the event and the Schreiber foreman continued to make the required notifications and reported to the work site. At 0931 the area of the roof where the metal connection was made was exposed to identify the damage. It was confirmed that there was damage to a hard electrical conduit located one (1) to two and a half (2.5) inches below the top layer of the roof that contained energized, 480V current. The electrical conduit powered the exhaust fans mounted on the roof. The affected area of the roof was flagged off and secured from access. Between 0930 and 1100, associated project and FOD management reported to the site to make further assessments of the event. At 1050 the exhaust fan units were LO/TO. At 1115 a penetration permit for roof cutting activities was obtained at the request of the FOD, the IWD was revised to reflect that dielectric gloves would be work during roof cutting activities, and the work was resumed. A temporary cover was placed over the exposed area of the roof until repairs to the damaged electrical conduit could be made. On October 15, 2013, repairs were made to the electrical conduit by a local subcontractor to Schreiber, Pueblo Electric. The electrician who made the repairs provided the following information regarding the damage to the electrical conduit: the conduit was True Rigid one (1) inch conduit with a conduit wall of approximately .126 inches (3.20mm); the cut was more than halfway through the wall of the conduit; the conduit wall was not cut through to the interior; the wiring was not damaged or compromised in any way as a result of the damage to the conduit. The electrical conduit was repaired and installed to meet current code requirements. At 1530 the WFO FOD held a critique of the event.
Cause Description: ISM SUMMARY The first ISM weakness in this event was a lack of clarity in the Institutional expectations regarding the requirement of a penetration permit for all roofing demolition activities at LANL in the LANL procedure “Penetration Operations” (P101-22). Step 3 Develop and Implement Hazard Controls. A second ISM weakness was the lack of building schematics that

Attachment 2
14
accurately reflected the rooftop equipment configuration. Step 5 Provide Feedback and Continuous Improvement. A third ISM weakness in this event was the missed opportunity by the project management to incorporate previous operational experience into the project planning. LANL has experienced two (2) ORPS-reportable events in recent years concerning damage to electrical conduit during RAMP roofing projects. Additionally, it is not uncommon for roofing activities at LANL to experience atypical configuration while performing roofing demolition activities. However, the RAMP project did not consider these previous operational experiences when planning the FY13 RAMP project. Step 2 Analyze the Hazards, Step 5 Provide Feedback and Continuous Improvement. EXTENT OF CONDITION The FOD assessed the need for an Extent of Condition (EOC), in accordance with DOE Order 232.2, Occurrence Reporting and Processing of Operations Information, and determined one was not warranted for this event because there were no other roofing replacement projects ongoing or scheduled. CAUSAL ANALYSIS METHODOLOGY Apparent Cause Analysis and the Causal Analysis Tree, as described in the DOE Occurrence Reporting Causal Analysis standard (DOE-STD-1197-2011), were used to identify the causes for this event. Apparent causes are identified as the most probable causes of an event or condition that management has the control to fix and for which effective recommendations for corrective actions can be generated (in accordance with DOE O 232.2, Attachments 4 and 6). CAUSAL ANALYSIS APPARENT CAUSE The apparent cause in this event was the lack of clarity in the LANL Procedure “Penetration Operations” (P101-22) regarding the Institutional expectation that a penetration permit was required for all roofing demolition activities. P101-22 states in Section 3.1 “Penetration Implementation Procedure” that “Class 1 penetrations are penetrations into hollow walls, ceilings, floors, or 1.5 inch or less into solid material”. In Section 9.1 “Definitions”, the procedure defines a solid material as “A … roof … consisting of: cast-in-place or pre-cast concrete, brick, … masonry block materials”. Historically, RAMP project activities will obtain a penetration permit for roofing demolition activities at LANL that meet the solid material

Attachment 2
15
definition in P101-22 (see previous paragraph). However, roofing material that is not of the nature specifically iterated in the P101-22 definition of ‘solid material’ have been considered soft material. Soft roofing material is not specifically addressed in P101-22 and therefore has been considered as not applicable to the Penetration Operations requirements and penetration permits have not been obtained for these types of roofs (as was the case at TA9-21). It warrants re-stating that the RAMP project adheres to the P101-22 requirements as they are written. For example, they have obtained penetration permits for roofing demolition activities on concrete roofs and have always obtained a penetration permit for keying to vertical surfaces of the exterior walls (as included in the TA9-21 IWD). The cause code that best describes this apparent cause is A4B1C01 “Management policy guidance/expectations not well-defined, understood or enforced” because P101-22 does not clearly communicate the Institutional expectation that all roofing demolition activities at LANL require a penetration permit. Corrective actions 1, 2, and 3 address this cause code. CONTRIBUTING CAUSE A contributing cause in this event was the lack of schematic drawings that reflected accurate rooftop equipment configuration. In approximately 1995 a new Overlay Roofing System was put on TA9-21. The new roof was placed on top of the old roof. The electrical conduit supplying power to the exhaust fans was not moved from its location on top of the old roof to be placed either in the ceiling space or on top of the new roof. Instead, it was buried between the old and new roofs. At the time, schematics were not updated or created to reflect this configuration. Therefore, the RAMP project team was unaware of this atypical condition and was unable to determine controls for the hazard. The cause code that best describes this contributing cause is A1B3C02 “Design/documentation not up-to-date” because the schematics did not provide accurate rooftop equipment configuration information. Corrective actions 2 and 3 address this cause code.
Operating Conditions: Normal
Activity Category: Construction
Immediate Action(s): 1) Notifications made to RAMP STR, WFO FOD, D FOD, WFO ESO, and WX-7 Group Leader. 2) Work was immediately paused upon discovery of the damaged electrical conduit. 3) The circuit was locked and tagged out. 4) On October 11, 2013, a penetration permit was acquired at the request

Attachment 2
16
of the FOD and the work was resumed.
FM Evaluation: Facility damages were minor and were repaired promptly. No additional actions are required.
DOE Facility Representative Input:
DOE Program Manager Input:
Further Evaluation is Required:
No
Division or Project: DOE RAMP Project
Plant Area: TA-9-0021
System/Building/Equipment: TA-9-0021 Roof
Facility Function: Explosive
Corrective Action 01: Target Completion Date:11/27/2013
Actual Completion Date:11/27/2013
REVISION OR EXTENSION OF THIS ACTION REQUIRES FACILITY OPERATIONS DIRECTOR APPROVAL. Title: Obtain Penetration Permit for roof investigation work. Action: Obtain Penetration Permit for roof investigation work at TA 09-0021 A&C to reflect use of di-electric gloves as standard PPE during cutting activities. Deliverable: Penetration Permit Responsible Organization: PM6 See PFITS 2013-3576, action 5 for action closure and objective evidence. Target Due Date: 12/24/2013 This action addresses cause code A4B1C01, which is identified in the causal analysis. NOTE: This action has been closed in ORPS based on the documented completion of the Performance Feedback Improvement Tracking System entry.
Corrective Action 02: Target Completion Date:11/27/2013
Actual Completion Date:11/27/2013
REVISION OR EXTENSION OF THIS ACTION REQUIRES FACILITY OPERATIONS DIRECTOR APPROVAL.

Attachment 2
17
Title: Interim Instruction for roof investigation work. Action: An Interim Instruction for the pending P101-22, Penetration Operations, revision reflecting immediate instructions to the Laboratory regarding the requirement of a penetration permit for all roof demolition work will be issued. Deliverable: Interim Instruction Responsible Organization: DSESH See PFITS 2013-3576, action 6 for action closure and objective evidence. Target Due Date: 12/18/2013. This action addresses cause code A4B1C01, which is identified in the causal analysis. NOTE: This action has been closed in ORPS based on the documented completion of the Performance Feedback Improvement Tracking System entry.
Corrective Action 03: Target Completion Date:11/27/2013
Actual Completion Date:11/27/2013
REVISION OR EXTENSION OF THIS ACTION REQUIRES FACILITY OPERATIONS DIRECTOR APPROVAL. Title: Revise P 101-22, Penetration Operations, regarding roof demolition activities. Action: Revise P 101-22, Penetration Operations, to include specific language that ensures all roof demolition activities at LANL are performed using a penetration permit. Deliverable: Revised P 101-22, Penetration Operations Responsible Organization: OSH-ISH See PFITS 2013-3576, action 4 for action closure and objective evidence. Target Due Date: 4/30/2014 This action addresses cause codes A4B1C01 and A1B3C02, which are identified in the causal analysis.

Attachment 2
18
NOTE: This action has been closed in ORPS based on the documented completion of the Performance Feedback Improvement Tracking System entry.
Lessons(s) Learned:
HQ Keywords: 01A--Inadequate Conduct of Operations - Inadequate Conduct of Operations (miscellaneous) 01B--Inadequate Conduct of Operations - Loss of Configuration Management/Control 01G--Inadequate Conduct of Operations - Inadequate Procedure 01N--Inadequate Conduct of Operations - Inadequate Job Planning (Other)01R--Inadequate Conduct of Operations - Management issues 07D--Electrical Systems - Electrical Wiring 08J--OSHA Reportable/Industrial Hygiene - Near Miss (Electrical) 11G--Other - Subcontractor 12K--EH Categories - Near Miss (Could have been a serious injury or fatality) 14D--Quality Assurance - Documents and Records Deficiency 14E--Quality Assurance - Work Process Deficiency 14G--Quality Assurance - Procurement Deficiency
HQ Summary: On October 11, 2013, a roofing contractor inadvertently breached an electrical conduit containing 480-volt power to an exhaust fan with a gas-powered roof cutter while removing old roofing material in preparation for a new roof on Building 0021. It was unknown at the time that an electrical conduit was underneath the roofing material. The roof cutter had a depth gauge and a 7-inch blade. The depth gauge was set at 1½ inches which required the contractor to take more than one cut to reach the final depth of the roofing material. The conduit was breached during the second cut which would have been at 3 inches. The depth gauge on the blade was the only barrier to prevent exposure to a hazardous energy source. Although an approved integrated work document had been issued for the roofing work, an approved penetration permit was not acquired to perform the penetration work.
Similar OR Report Number: 1. NA--LASO-LANL-FIRNGHELAB-2005-0009
2. NA--LASO-LANL-PHYSTECH-2008-0009
Facility Manager: Name Brian Watkins
Phone (505) 667-0562
Title WFO Deputy Facility Operations Director
Originator: Name TANNER, KIMBERLI K
Phone (505) 665-8197
Title OCCURRENCE INVESTIGATOR
HQ OC Notification: Date Time Person Notified Organization

Attachment 2
19
NA NA NA NA
Other Notifications: Date Time Person Notified Organization
10/11/2013 13:48 (MTZ) Steven Frye NNSA
Authorized Classifier(AC): Kimberli Tanner Date: 11/27/2013
5)Report Number: NA--LASO-LANL-TA55-2013-0031 After 2003 Redesign
Secretarial Office: National Nuclear Security Administration
Lab/Site/Org: Los Alamos National Laboratory
Facility Name: Plutonium Proc & Handling Fac
Subject/Title: Electrician Receives Minor Electric Shock While Performing Breaker Maintenance
Date/Time Discovered: 10/26/2013 10:15 (MTZ)
Date/Time Categorized: 10/26/2013 10:40 (MTZ)
Report Type: Notification
Report Dates: Notification 10/29/2013 17:23 (ETZ)
Initial Update
Latest Update
Final
Significance Category: 2
Reporting Criteria: 2E(1) - Any unexpected or unintended personal contact (burn, injury, etc.) with an electrical hazardous energy source (e.g., live electrical power circuit, etc.).
Cause Codes:
ISM:
Subcontractor Involved: No
Occurrence Description: MANAGEMENT SYNOPSIS: On Saturday, October 26, 2013, at approximately 1015, at Technical Area 50, Building 2 (TA-50-2), a Logistics Central Shops (LOG-CS) electrician (E1) received a minor shock to his right ring finger while performing breaker maintenance on Motor Control Center A (MCC-A). The work was paused and E1 was transported to occupational medicine where he was evaluated and release to return to work without restrictions. Analysis indicated the shock was from a single phase 120volt circuit BACKGROUND: Five year breaker maintenance was scheduled for MCC-A. This was the first time that the breaker maintenance was not part of a complete shut down of power to the building. The 480 volt power supply to MCC-A had been locked and tagged out prior to the start of work. It was stated in the critique that in most MCCs the control power is

Attachment 2
20
stepped down from the primary power supply; specifically from 480 volts to 120 volts. There was no indication prior to the incident that there was a second source of power to the control terminal. After the incident it was determined that the control terminal had a second source of power consisting of 120 volts, single phase. A pre-job briefing was held prior to the start of work. A zero energy check was performed on the 480 volt circuit; however, not all the terminals were checked. E1 was torqueing the control panel terminal strip when he felt what he described as a pin prick on his right ring finger. E1 assumed he had contacted a sharp edge on the control box, stopped torqueing, and ran his thumb over the area. When he found no sharp edge he thought he might have been shocked and checked the terminals with his voltage meter. E1 got a reading of 120 volts on one of the terminals.
Cause Description:
Operating Conditions: Breaker maintenance
Activity Category: Normal Operations (other than Activities specifically listed in this Category)
Immediate Action(s): E1 reported the incident to his foreman and the Person in Charge (PIC). Work was paused and the facility was placed in a safe configuration. E1 was transported to occupational medicine where he was evaluated and release to return to work without restrictions. A visual inspection was performed of the other breakers undergoing maintenance for similar situations. Because of freeze protection issues and other considerations it was decided to restore power to the equipment with oversight by of the Facility Electrical Safety Officer. A critique was scheduled for Monday, October 29, 2013.
FM Evaluation:
DOE Facility Representative Input:
DOE Program Manager Input:
Further Evaluation is Required:
Yes. Before Further Operation? No By Whom: TA-55-RLW, TA55-DO By When: 12/10/2013
Division or Project: TA-55-RLW
Plant Area: TA-50
Attachment 2
21
System/Building/Equipment: TA-50, Building 2, MCC-A
Facility Function: Plutonium Processing and Handling
Corrective Action:
Lessons(s) Learned:
HQ Keywords: 01M--Inadequate Conduct of Operations - Inadequate Job Planning (Electrical) 08A--OSHA Reportable/Industrial Hygiene - Electrical Shock 12C--EH Categories - Electrical Safety 14E--Quality Assurance - Work Process Deficiency
HQ Summary: On October 26, 2013, at Technical Area 50, Building 2, a Logistics Central Shops electrician received a minor shock to his right ring finger while performing breaker maintenance on Motor Control Center A (MCC-A). The work was paused and the electrician was transported to occupational medicine where he was evaluated and released without restrictions. Analysis indicated the shock was from a single phase 120-volt circuit. The 480-volt power supply to MCC-A had been locked and tagged out prior to the start of work. In most MCCs, the control power is stepped down from the primary power supply; specifically from 480 volts to 120 volts. There was no indication prior to the incident that there was a second source of power to the control terminal. After the incident it was determined that the control terminal had a second source of power consisting of 120 volts, single phase. A critique was held.
Similar OR Report Number:
Facility Manager: Name Stu McKernan
Phone (505) 667-3030
Title Deputy Facility Operations Manager
Originator: Name HUNSINGER, MARK W
Phone (505) 665-1496
Title OCCURRENCE INVESTIGATOR
HQ OC Notification: Date Time Person Notified Organization
NA NA NA NA
Other Notifications: Date Time Person Notified Organization
10/26/2013 10:40 (MTZ) Dave Stewart NNSA/FR
Authorized Classifier(AC): Mark Hunsinger Date: 10/29/2013
6)Report Number: NA--PS-BWP-PANTEX-2013-0065 After 2003 Redesign
Secretarial Office: National Nuclear Security Administration
Lab/Site/Org: Pantex Plant
Facility Name: Pantex Plant

Attachment 2
22
Subject/Title: Lockout/Tagout (LO/TO) Hazardous Energy Control Issue
Date/Time Discovered: 10/10/2013 14:00 (CTZ)
Date/Time Categorized: 10/10/2013 15:32 (CTZ)
Report Type: Update
Report Dates: Notification 10/15/2013 16:54 (ETZ)
Initial Update 12/03/2013 12:36 (ETZ)
Latest Update 12/03/2013 12:36 (ETZ)
Final
Significance Category: 3
Reporting Criteria: 2E(2) - Any unexpected discovery of an uncontrolled electrical hazardous energy source (e.g., live electrical power circuit, etc.). This criterion does not include discoveries made by zero-energy checks and other precautionary investigations made before work is authorized to begin.
Cause Codes:
ISM: 4) Perform Work Within Controls
Subcontractor Involved: No
Occurrence Description: On Wednesday, 10/09/13, at approximately 10:30, when the pipefitters returned to complete work they determined that a lockout/tagout (LO/TO) executed earlier for work on a solenoid and heat trace circuit only locked out the heat trace circuit. The Pipe Shop and Instrument Shop were working on the Air Receiver tanks outside on the Northwest corner of a Zone 11 facility (there are two receiver tanks, a north tank and a south tank). The pipefitters were to remove the insulation cover ring at the bottom of the receiver tanks so the solenoid drain valves could be replaced. The instrument technicians were to execute a LO/TO on the solenoid valves, and would also isolate the heat trace circuit, which was in the same ground level junction box as the solenoids. Once the circuit was locked out, the instrument technicians were to unwire the solenoid valve, and the pipefitters would replace the valve with a new valve and solenoid. The instrument technicians would then wire in the new valve and return the receivers back to normal operations. Utilities operators were present to align the tanks receiving and discharge valves, and isolate the energy source. There is a uni-strut rack 3’ east of the receiver tanks, mounted on the same pad as the receiver tanks. At the base of this rack in a 6” X 6” junction box (JB), with 2 - ½“ plasti-bond rigid metal conduits entering the JB from the ground. The junction box has the solenoid circuits entering (just looping through the JB) in one of the plasti-bond conduits and exiting the JB in a ½ “ non-coated rigid metal conduit, feeding the solenoids on the North and South receiver tanks.

Attachment 2
23
The other ½ “ plasti-bond conduit has a 120 volt circuit that enters the JB and leaves the JB in a ½” non-coated rigid metal conduit on the north side of the JB. This conduit goes to a 30 amp, 3 pole non-fusible disconnect, which feeds the heat trace circuit. They are only using 1 phase of the disconnect, and then it feeds back to the JB and out to the same ½ “non-coated rigid metal conduit that feeds the solenoid valves. It was assumed that the disconnect fed the solenoid valves and the heat trace circuit. The craftsmen performed the job on the South receiver tank on Tuesday, 10/08/13, afternoon without any problems and everything worked perfectly. The pipefitters returned to the job site on Wednesday, 10/09/13, and met Utilities personnel who opened the disconnect and aligned valves in preparation for the lockout on the north receiver. While the pipefitters were removing the insulated skirting on the bottom of the receiver, they were startled when they heard the solenoid valve activate on the south receiver. They looked and saw the disconnect was open and knew power should not be available to operate the valve. The pipefitters stopped work and notified their supervisor. The supervisor notified the Instrument Shop supervisor of his concern. A meeting was arranged for the next morning to investigate. On Thursday, 10/10/13, the Pipe Shop supervisor and pipefitters met with the Instrument Shop supervisor and technicians at the job site to investigate. The Instrument Shop supervisor notified the system owner and with his help, traced out the source of power for the solenoid valves and found the power is supplied from Panel LA, breaker 8, and not the disconnect as believed. The disconnect only served power to the heat trace. No craftsmen were in imminent danger, as they were wearing their personal protective equipment (PPE) during the absence of energy check and were wearing their gloves during the unwiring and wiring of the solenoid valves. There were no injuries to personnel or electrical shocks in this event.
Cause Description:
Operating Conditions: Normal
Activity Category: Maintenance
Immediate Action(s): Pipefitters stopped work and reported event to their supervisor. Pipe Shop and Instrument Shop employees met on Thursday, 10/10/13, to determine how the valve actuated with the disconnect in the "OFF" position.

Attachment 2
24
Critique was conducted on 10/10/13 and the event was categorized as 2E(2)SC3, Hazardous Electrical Energy Control, any unexpected discovery of an uncontrolled hazardous energy source.
FM Evaluation: Due date extended to 12/05/13 to match NTS reporting due date.
DOE Facility Representative Input:
DOE Program Manager Input:
Further Evaluation is Required:
No
Division or Project: Maintenance
Plant Area: Zone 11
System/Building/Equipment: Zone 11 Facility
Facility Function: Balance-of-Plant - Site/outside utilities
Corrective Action:
Lessons(s) Learned:
HQ Keywords: 01K--Inadequate Conduct of Operations - Lockout/Tagout Noncompliance (Electrical) 01L--Inadequate Conduct of Operations - Lockout/Tagout Noncompliance (Other) 01M--Inadequate Conduct of Operations - Inadequate Job Planning (Electrical) 01N--Inadequate Conduct of Operations - Inadequate Job Planning (Other)08H--OSHA Reportable/Industrial Hygiene - Safety Noncompliance 12I--EH Categories - Lockout/Tagout (Electrical or Mechanical) 14E--Quality Assurance - Work Process Deficiency
HQ Summary: On October 9, 2013, pipefitters determined that a lockout/tagout, which had been prepared for the replacement of solenoid drain valves, had only locked out the heat trace circuit and not the solenoid valves. While the pipefitters were removing the insulated skirting on the bottom of a receiver tank, they were startled when they heard the solenoid valve activate on the south receiver. They saw that a disconnect switch was open and knew power should not be available to operate the valve. On October 10, the Pipe Shop supervisor and pipefitters met with the Instrument Shop supervisor and technicians at the job site to investigate. The Instrument Shop supervisor notified the system owner and with his help, traced out the source of power for the solenoid valves and found the power is supplied from Panel LA, Breaker 8, and not the disconnect as believed. The disconnect switch only served power to the heat trace.
Similar OR Report Number:
Facility Manager: Name Ronnie Payne
Phone (806) 477-6364

Attachment 2
25
Title Plant Maintenance Department Manager
Originator: Name HALL, BEVERLY J
Phone (806) 477-3222
Title
HQ OC Notification: Date Time Person Notified Organization
NA NA NA NA
Other Notifications: Date Time Person Notified Organization
10/10/2013 15:32 (CTZ) Richard Clampitt B&W
10/10/2013 15:32 (CTZ) Mike Childers NPO
Authorized Classifier(AC): Stan Stambaugh Date: 12/02/2013
7)Report Number: NA--SS-SNL-NMFAC-2013-0006 After 2003 Redesign
Secretarial Office: National Nuclear Security Administration
Lab/Site/Org: Sandia National Laboratories - SS
Facility Name: SNL NM Site-wide F & M
Subject/Title: Subcontract Worker Cuts Into a Conduit and Nicks Conductor, No Shock or Injury at Building 956
Date/Time Discovered: 10/15/2013 08:40 (MTZ)
Date/Time Categorized: 10/15/2013 10:10 (MTZ)
Report Type: Final
Report Dates: Notification 10/17/2013 15:58 (ETZ)
Initial Update 11/20/2013 16:38 (ETZ)
Latest Update 11/20/2013 16:38 (ETZ)
Final 11/20/2013 16:38 (ETZ)
Significance Category: 3
Reporting Criteria: 2E(2) - Any unexpected discovery of an uncontrolled electrical hazardous energy source (e.g., live electrical power circuit, etc.). This criterion does not include discoveries made by zero-energy checks and other precautionary investigations made before work is authorized to begin.
Cause Codes: A3B3C06 - Human Performance Less Than Adequate (LTA); Knowledge Based Error; Individual underestimated the problem by using past events as basis -->couplet - A4B3C08 - Management Problem; Work Organization & Planning LTA; Job scoping did not identify special circumstances and/or conditions A5B4C01 - Communications Less Than Adequate (LTA); Verbal Communications LTA; Communication between work groups LTA
Attachment 2
26
ISM: 3) Develop and Implement Hazard Controls 4) Perform Work Within Controls
Subcontractor Involved: Yes Cross Connection Inc.
Occurrence Description: At approximately 0840 a mechanical contractor cut into an energized circuit while using a Sawzall at Building 956. The contractor was cutting a 2-inch copper pipe and did not identify the conduit/circuit prior to the operation because the conduit was obscured by the copper pipe. The circuit that was impacted was 277 volts and was inside of a standard one inch conduit. The task was conducted from an 8-foot stepladder at approximately 12 feet in height and the impact to the conduit was approximately one eighth of an inch. There was no shock and no injury to the worker. The lighting to two offices was impacted for forty-five minutes. A hazard analysis (daily pre-task plan) was conducted for the operation. The Sawzall was double insulated and the contract worker was utilizing gloves and a GFCI was utilized during the operation. The task was paused and notifications were conducted. Accident scene preservation was maintained and an investigation was initiated. The Electrical Severity for this event is 50 (medium severity event), as follows: Electrical hazard factor = 50 (277 VAC / single phase); Environment Factor = 0 (dry); Shock Proximity Factor = 0 (outside the limited approach boundary-exposure contained in pipe, breaker tripped immediately, double insulated tools); Arc Flash Proximity Factor = 0 (no arc flash hazard on single phase); thermal proximity factor = NA (no thermal hazard); No PPE Mitigations in place; Injury Factor = 1 (no injury). A critique meeting was held at 1400 to review the event. A review of the extent of condition revealed that the task is a standard operation and it is regularly conducted in a safe manner by the contractors. The extent of condition review also found only one previous event that was similar in the previous five years, and this occurred in a different organization. Considering the frequency with which this task is performed, the problem does not appear to be prevalent.
Cause Description: Critique/Fact Finding Performed: 10/15/2013 A3-B3-C06: The worker underestimated the problem by using past events as basis. The team determined that the worker had conducted this work successfully prior to the event and did not use the best available tools (longer ladder, shorter Sawzall blade) due to previous success with these specific tools. However, there was no electrical conduit in close proximity
Attachment 2
27
to the water line on the previous work. A4-B3-C08: Job scoping did not identify special circumstances and/or conditions. The team determined that contractor did not have a policy or guidance for working in a ceiling area. The congested nature of the elevated work needs some work direction. A5-B4-C01: Communications between work groups less than adequate. During the investigation it was discovered that a worker was below the work are and was in plain sight of the electrical conduit and did not speak about the hazard. Communication between the two workers on this hazard could have prevented the event.
Operating Conditions: Normal
Activity Category: Construction
Immediate Action(s): The work area was placed in a safe condition. Notifications were conducted. Investigation was initiated.
FM Evaluation: A less-than-adequate walk-down of the work area was conducted due to previous success with simple water piping removal. While the contract worker physically checked behind the pipe with his hand for other utilities, a visual from other angles would have easily discovered the electrical conduit. The 8-inch Sawzall blade could have been reduced to a 6-inch, and the event thereby could have been prevented. Ceiling areas are commonly congested and a thorough investigation of the work area for hazards is needed. The ladder that was utilized was also an 8 foot ladder and a 10-12 foot ladder would have given the contract work greater ability to see over the water pipe and identify the electrical conduit. During the causal analysis, the causal analysis team discovered that a laborer was underneath the cutting operation with a bucket to control a potential water release. The contractor utilizes a behavior-based safety (BBS) program; however, BBS failed to assist in the prevention of this event because the belief was that extra input was not needed. Better communication in the contractor's BBS program could have prevented the event. While the contractor incorporated a new policy for working in the ceiling area that addresses walk-downs, lighting, and ladder selection, the contractor also disciplined the employee. FMOC will share this policy with all contractors. EOC #31178
DOE Facility Representative Input:

Attachment 2
28
DOE Program Manager Input:
Further Evaluation is Required:
No
Division or Project: 4820/Construction
Plant Area: Tech Area II
System/Building/Equipment: Cooling tower electrical conductor/Building 956/Inside
Facility Function: Balance of Plant - Infrastructure (Other Functions not specifically listed in this Category)
Corrective Action 01: Target Completion Date:01/10/2014 Actual Completion Date:
A3B3C06 - The Lessons Learned will be shared in the Construction News Sense and the Quarterly Construction Seminar. (Dept. 4878, Anthony Chavez)
Corrective Action 02: Target Completion Date:01/10/2014 Actual Completion Date:
A4B3C08 - The contractor will develop a new procedure for work in the ceiling area. (Dept. 4822, Darell Rogers)
Corrective Action 03: Target Completion Date:01/10/2014 Actual Completion Date:
A5B4C01- The contractor will document communication with their employees on behavior-based safety to ensure that all employees are actively looking for and communicating hazards to fellow workers. (Dept. 4878, Anthony Chavez)
Lessons(s) Learned:
HQ Keywords: 01A--Inadequate Conduct of Operations - Inadequate Conduct of Operations (miscellaneous) 01G--Inadequate Conduct of Operations - Inadequate Procedure 01N--Inadequate Conduct of Operations - Inadequate Job Planning (Other)01P--Inadequate Conduct of Operations - Inadequate Oral Communication07C--Electrical Systems - Power Outage 07D--Electrical Systems - Electrical Wiring 08J--OSHA Reportable/Industrial Hygiene - Near Miss (Electrical) 11G--Other - Subcontractor 12B--EH Categories - Conduct of Operations 14D--Quality Assurance - Documents and Records Deficiency 14E--Quality Assurance - Work Process Deficiency 14G--Quality Assurance - Procurement Deficiency
HQ Summary: On October 15, 2013, a mechanical contractor cut into an energized 277-volt circuit with a Sawzall while cutting a 2-inch copper pipe at Building 956. The contractor did not see conduit because the pipe obscured it. There was no shock and no injury to the worker. Lighting to two offices was impacted for 45 minutes. A hazard analysis had been conducted for the operation. The contract worker was wearing gloves and used a GFCI with the double insulated saw.

Attachment 2
29
Similar OR Report Number: 1. NA--LASO-LANL-FIRNGHELAB-2013-0004
Facility Manager: Name Greg Kirsch
Phone (505) 845-9497
Title FESH Lead
Originator: Name Goetsch, Robert S.
Phone (505) 284-4647
Title POLICIES AND PROCEDURES ANALYST
HQ OC Notification: Date Time Person Notified Organization
NA NA NA NA
Other Notifications: Date Time Person Notified Organization
10/15/2013 09:10 (MTZ) Lynne Schluter 4840
10/15/2013 09:10 (MTZ) Art Ratzel 4800
10/15/2013 09:10 (MTZ) Stan Harrison 4870
10/15/2013 09:10 (MTZ) Anthony Chavez 4878
10/15/2013 10:10 (MTZ) Veronica Martinez DOE/SFO
10/15/2013 10:15 (MTZ) EOC 4236
Authorized Classifier(AC): John Zavadil Date: 11/14/2013
8)Report Number: NA--YSO-BWXT-Y12SITE-2013-0025 After 2003 Redesign
Secretarial Office: National Nuclear Security Administration
Lab/Site/Org: Y12 National Security Complex
Facility Name: Y-12 Site
Subject/Title: Electrical Arc Due to Separated Cord - Space Heater (Near Miss)
Date/Time Discovered: 10/14/2013 10:40 (ETZ)
Date/Time Categorized: 10/14/2013 12:23 (ETZ)
Report Type: Final
Report Dates: Notification 10/16/2013 16:37 (ETZ)
Initial Update 11/21/2013 13:57 (ETZ)
Latest Update 11/21/2013 13:57 (ETZ)
Final 11/21/2013 13:57 (ETZ)
Significance Category: 3
Reporting Criteria: 10(3) - A near miss to an otherwise ORPS reportable event, where something physically happened that was unexpected or unintended, or where no or only one barrier prevented an event from having a reportable consequence. The significance category assigned to the near miss must be based on an

Attachment 2
30
evaluation of the potential risks and extent of personnel exposure to the hazard. (1 of 3 criteria - This is a SC 3 occurrence)
Cause Codes: A2B6C01 - Equipment/ material problem; Defective, Failed or Contaminated; Defective or failed part
ISM: 4) Perform Work Within Controls
Subcontractor Involved: No
Occurrence Description: On October 14, 2013 at 10:40 a.m., an electrical arc occurred while an employee attempted to unplug a 110 volt space heater cord from a power strip. Since the cord was difficult to remove, the employee pulled hard and their hand slid off the plug. The cord had become separated from the plug resulting in a popping sound from the exposed arcing which left black residue on the employee's right fingers. The employee was evaluated at Occupational Health Services and initially diagnosed with electrical shock to the right hand with no injury. After further review, it was determined the employee had not received an electrical shock.
Cause Description: A causal analysis was performed using the Events and Causal Factors Analysis methodology. Following the requirements for use of an electrical space heater, the employee was unplugging the heater prior to departing the work area. Because the plug was difficult to remove, the employee's hand slipped from the plug to the cord. The cord was pulled and partially separated from the plug. The wires were still connected to the plug. This resulted in an arc between the bare wires when the employee pulled the cord. Causal Factor: The employee was focusing on unplugging the electrical heater to ensure compliance with requirements associated with electrical equipment. The employee did not realize that the cord had partially separated from the plug, which resulted in the arc which occurred. Extent of Condition Review: Portable electric heaters are used in multiple work areas across the Y-12 Site. A similar situation could occur when one is used in these work area. Actions have been defined in the Corrective Action Plan to communicate to personnel within the Development organization (Action #3) and across the Y-12 Site (Action #5) the importance of periodically verifying the integrity of electrical cords for portable electric heaters.
Operating Conditions: Normal office environment
Activity Category: Normal Operations (other than Activities specifically listed in this Category)
Immediate Action(s): 1.Employee was taken to Medical for evaluation. 2.Initially categorized as a 2E-1, Cat. 2 occurrence. 3.The power strip was placed in safe configuration and the breaker was reset. 4.After consultation with the appropriate subject matter experts it was determined the employee did not receive an electrical shock. At this time, the significant category was changed to 10-3, Cat. 3.

Attachment 2
31
5.The Plant Shift Superintendent (PSS) made initial notification of the re-categorization at 1604 on 10/14/13.
FM Evaluation: Corrective Actions have been included to "dispose of the heater," to "remind group personnel of the plant requirements regarding use of electrical space heaters," to "perform an Extent of Conditions review of cord integrity for similar heaters in Development," to "determine if a recall exists on this particular model of heater," and to "issue a Plant-wide notification to reinforce the requirements for use of portable electrical heaters." An Electrical Severity Calculation was performed by the Electrical Authority Having Jurisdiction. The electrical severity (ES) rating for this event was "20." An ES of 1-30 means no hazard energy is present and therefore would not be reportable due to a shock or flash hazard.
DOE Facility Representative Input:
DOE Program Manager Input:
Further Evaluation is Required:
No
Division or Project: Development
Plant Area: Limited
System/Building/Equipment: 9202
Facility Function: Balance of Plant - Infrastructure (Other Functions not specifically listed in this Category)
Corrective Action 01: Target Completion Date:11/21/2013 Tracking ID:1
Near/MidTerm #1 - Dispose of Heater. This action was completed on 10/31/2013.
Corrective Action 02: Target Completion Date:12/09/2013 Tracking ID:2
Near/MidTerm #2 - Remind Development personnel of the plant requirements regarding use of electrical space heaters.
Corrective Action 03: Target Completion Date:12/09/2013 Tracking ID:3
Near/MidTerm #3 - Perform extent of conditions review of cord integrity for similar heaters in Development.
Corrective Action 04: Target Completion Date:11/21/2013 Tracking ID:4
Near/MidTerm #4 - Determine if recall exists on this particular model of heater. This action was completed on 10/16/2013.
Corrective Action 05: Target Completion Date:12/09/2013 Tracking ID:5
Near/MidTerm #5 - Issue a Plant-wide notification to reinforce the

Attachment 2
32
requirements for use of portable electrical heaters.
Corrective Action 06: Target Completion Date:03/10/2014 Tracking ID:90
Effectiveness Review - Perform an Effectiveness Review to determine if the actions taken will help prevent recurrence of the event.
Lessons(s) Learned: Portable electrical equipment should be regularly checked for wear and/or deterioration, especially cords and plugs. If the equipment is worn or deteriorated, it should be replaced with UL-rated equipment.
HQ Keywords: 01A--Inadequate Conduct of Operations - Inadequate Conduct of Operations (miscellaneous) 01Q--Inadequate Conduct of Operations - Personnel error 07D--Electrical Systems - Electrical Wiring 08J--OSHA Reportable/Industrial Hygiene - Near Miss (Electrical) 12K--EH Categories - Near Miss (Could have been a serious injury or fatality) 14E--Quality Assurance - Work Process Deficiency
HQ Summary: On October 14, 2013, an employee attempted to unplug a 110-volt space heater cord from a power strip when the cord separated from the plug resulting in an electrical arc. The employee pulled hard on the plug because it was difficult to remove and their hand slid off the plug causing the cord to separate from the plug, causing a popping sound and leaving black residue on the employee's right fingers. The employee did not receive an electrical shock. The power strip was placed in safe configuration and the breaker was reset.
Similar OR Report Number: 1. None identified.
Facility Manager: Name Ken N. Vara
Phone (865) 574-5124
Title Acting Director of Operations - Development
Originator: Name BRYNESTAD, ASTRID
Phone (865) 574-1566
Title OCCURRENCE REPORTING ADMINISTRATOR
HQ OC Notification: Date Time Person Notified Organization
NA NA NA NA
Other Notifications: Date Time Person Notified Organization
10/14/2013 12:25 (ETZ) PSS PSS
10/14/2013 12:36 (ETZ) Duty Fac Rep NPO
10/14/2013 12:36 (ETZ) K.D. Keith Ops Egr
Authorized Classifier(AC): Wendell Jones Date: 11/19/2013
9)Report Number: NE-ID--BEA-ATR-2013-0036 After 2003 Redesign
Attachment 2
33
Secretarial Office: Nuclear Energy, Science and Technology
Lab/Site/Org: Idaho National Laboratory
Facility Name: Advanced Test Reactor
Subject/Title: Inadequate Lockout/Tagout (LO/TO) in 2B-SE Primary Cubicle at the ATR
Date/Time Discovered: 10/23/2013 08:45 (MTZ)
Date/Time Categorized: 10/23/2013 08:45 (MTZ)
Report Type: Notification/Final
Report Dates: Notification 10/24/2013 16:46 (ETZ)
Initial Update 10/24/2013 16:46 (ETZ)
Latest Update 10/24/2013 16:46 (ETZ)
Final 10/24/2013 16:46 (ETZ)
Significance Category: 4
Reporting Criteria: 2E(3) - Any failure to follow a prescribed hazardous energy control process (e.g., lockout/tagout, hazardous energy control program).
Cause Codes:
ISM: 4) Perform Work Within Controls
Subcontractor Involved: No
Occurrence Description: On 21 October 2013, at ~0400, Operations added a work control document line item to LO/TO ATR-LOCS-2437 on experiment loop 2B-SE for Work Order (WO) 111980, Loop In-pile Tube (IPT) Relief Valve 4-year Replacement. At ~1400 on 22 October 2013, Crafts personnel signed into the ATR-LOCS-2437 LO/TO and entered the 2B-SE primary cubicle for a job walk-down in preparation to start the replacement of the 2B-SE IPT relief valves. Upon completion of the walk-down, Craft personnel exited the 2B-SE primary cubicle. Work was scheduled to start 23 October 2013. At ~0830, on 23 October 2013, the ATR DOE Facility Representative (FR) was reviewing the active LO/TO record sheets. During FR review of ATR-LOCS-2437 LO/TO, assisted by the ATR Shift Supervisor (SS), the SS discovered that the 2B-SE pressurizer heaters were not part of that LO/TO, but are required for work in the 2B-SE cubicle. It is noted that the pressurizer heaters are LO/TO de-energized for cubicle entry in LO/TO ATR-LOCS-2428. No electrical hazard was present during job walk-down.
Cause Description:
Operating Conditions: The ATR was shut down for the scheduled Cycle 155A-1 outage
Activity Category: Maintenance
Immediate Action(s): Appropriate levels of BEA management and DOE-ID were notified of this event. An extent of conditions was performed on all active Loop Operating

Attachment 2
34
Controls System (LOCS) LO/TOs and it was determined that the boundary conditions are correct. A critique was held on 23 October 2013 at 2030.
FM Evaluation:
DOE Facility Representative Input:
DOE Program Manager Input:
Further Evaluation is Required:
No
Division or Project: ATR Programs
Plant Area: 2B-SE
System/Building/Equipment: Advanced Test Reactor - 2B-SE Cubicle
Facility Function: Category "A" Reactors
Corrective Action:
Lessons(s) Learned:
HQ Keywords: 01K--Inadequate Conduct of Operations - Lockout/Tagout Noncompliance (Electrical) 01L--Inadequate Conduct of Operations - Lockout/Tagout Noncompliance (Other) 01N--Inadequate Conduct of Operations - Inadequate Job Planning (Other)08H--OSHA Reportable/Industrial Hygiene - Safety Noncompliance 12I--EH Categories - Lockout/Tagout (Electrical or Mechanical) 14E--Quality Assurance - Work Process Deficiency
HQ Summary: On October 23, 2013, the ATR shift supervisor and the DOE facility representative were reviewing active lockout/tagout (LO/TO) record sheets in preparation to start the replacement of the 2B-SE In-pile Tube relief valves when the shift supervisor discovered that the 2B-SE pressurizer heaters were not part of that LO/TO, but are required for work in the 2B-SE cubicle. Crafts personnel had signed into the LO/TO and had entered the 2B-SE primary cubicle for a job walk-down. There was no electrical hazard present during the walk-down. An extent of conditions was performed on all active Loop Operating Controls System LO/TOs and it was determined that the boundary conditions are correct. A critique was held.
Similar OR Report Number:
Facility Manager: Name Hill, Shawn Ashley
Phone (208) 533-4128
Title ADVANCED TEST REACTOR OP. FACILITY M
Attachment 2
35
Originator: Name OWENS, MARJORIE A
Phone (208) 533-4563
Title ATR OPERATIONS FACILITY ADMINISTRATI
HQ OC Notification: Date Time Person Notified Organization
NA NA NA NA
Other Notifications: Date Time Person Notified Organization
10/23/2013 09:33 (MTZ) S. Ferrara DOE-ID
Authorized Classifier(AC): Jeffrey L. Garner Date: 10/23/2013
10)Report Number: SC--BHSO-BNL-BNL-2013-0009 After 2003 Redesign
Secretarial Office: Science
Lab/Site/Org: Brookhaven National Laboratory
Facility Name: Brookhaven National Laboratory (BOP)
Subject/Title: Worker Receives Electrical Shock while Plugging in a Laptop Video Projector
Date/Time Discovered: 10/29/2013 09:50 (ETZ)
Date/Time Categorized: 11/01/2013 14:15 (ETZ)
Report Type: Notification
Report Dates: Notification 11/04/2013 15:50 (ETZ)
Initial Update
Latest Update
Final
Significance Category: 2
Reporting Criteria: 2E(1) - Any unexpected or unintended personal contact (burn, injury, etc.) with an electrical hazardous energy source (e.g., live electrical power circuit, etc.).
Cause Codes:
ISM:
Subcontractor Involved: No
Occurrence Description: At Brookhaven National Laboratory (BNL), on October 29, 2013, at approximately 9:50 AM, two administrative assistants in Building 130 noted electrical sparking while one plugged a EPSON LCD Projector (Model: EMP-1715) into a power strip. The employee holding the plug felt an electrical shock. At approximately 10:00 AM, the employee and the Environment, Safety, and Health (ESH) Coordinator reported to the BNL Occupational Medicine Clinic (OMC), where the assistant was evaluated and released for work. There was no injury. An investigation was initiated.

Attachment 2
36
Cause Description: The initial investigation, which included reconstruction of the scene, coupled with sequence of events, could not determine the cause(s) of this event. It should be noted that the scene of the event was not secured. The investigation is ongoing.
Operating Conditions: Normal Operations
Activity Category: Normal Operations (other than Activities specifically listed in this Category)
Immediate Action(s): At approximately 10:00 AM, the employee and the Coordinator reported to the BNL OMC, where the assistant was evaluated and released for work. There was no injury.
FM Evaluation: Note: This event was initially determined to be non-reportable to DOE on October 29, 2013, at 11:40 AM. On November 1, 2013, after further evaluation, the event was re-categorized to a Significance Category 2 level event.
DOE Facility Representative Input:
DOE Program Manager Input:
Further Evaluation is Required:
Yes. Before Further Operation? No By Whom: By When:
Division or Project: Nuclear Science and Technology Department
Plant Area: Building 130
System/Building/Equipment: Laptop Video Projector
Facility Function: Balance-of-Plant - Offices
Corrective Action:
Lessons(s) Learned:
HQ Keywords: 07D--Electrical Systems - Electrical Wiring 08A--OSHA Reportable/Industrial Hygiene - Electrical Shock 12C--EH Categories - Electrical Safety 14L--Quality Assurance - No QA Deficiency
HQ Summary: On October 29, 2013, two administrative assistants in Building 130, Brookhaven National Laboratory (BNL), noted electrical sparking while an EPSON LCD Projector (Model: EMP-1715) was plugged into a power strip. The employee holding the plug felt an electrical shock. The employee and the Environment, Safety, and Health Coordinator reported to the BNL Occupational Medicine Clinic, where the assistant was evaluated and released for work. There was no injury and an investigation was initiated.
Similar OR Report Number:
Facility Manager: Name HORAK, WILLIAM

Attachment 2
37
Phone (631) 344-2627
Title DEPARTMENT CHAIRMAN
Originator: Name SIERRA, EDWARD A
Phone (631) 344-4080
Title ORPS COORDINATOR
HQ OC Notification: Date Time Person Notified Organization
NA NA NA NA
Other Notifications: Date Time Person Notified Organization
11/01/2013 14:00 (ETZ) W. Horak BNL
11/01/2013 14:05 (ETZ) A. Janczewski DOE/BNL
Authorized Classifier(AC):
11)Report Number: SC--BSO-LBL-OPERATIONS-2013-0019 After 2003 Redesign
Secretarial Office: Science
Lab/Site/Org: Lawrence Berkeley National Laboratory
Facility Name: Operations Division
Subject/Title: B33 LOTO Violation - No Injury, No Exposure
Date/Time Discovered: 10/16/2013 10:00 (PTZ)
Date/Time Categorized: 10/16/2013 12:48 (PTZ)
Report Type: Notification/Final
Report Dates: Notification 10/18/2013 19:13 (ETZ)
Initial Update 10/18/2013 19:13 (ETZ)
Latest Update 10/18/2013 19:13 (ETZ)
Final 10/18/2013 19:13 (ETZ)
Significance Category: 4
Reporting Criteria: 2E(3) - Any failure to follow a prescribed hazardous energy control process (e.g., lockout/tagout, hazardous energy control program).
Cause Codes:
ISM: 4) Perform Work Within Controls
Subcontractor Involved: Yes Kinetic Mechanical Systems/Webcor
Occurrence Description: At about 1300 hours on 10/15/2013, LBNL Facilities Chief Construction Manager (CCM) noticed that workers from Kinetic Mechanical Systems (KMS), a subcontractor to Webcor Builders on the GPL (General Purpose Laboratory) project (Building 33) had not connected motor wires for a vacuum pump. The Chief Construction Manager told the KMS Project

Attachment 2
38
Manager and Project Engineer that he would obtain a Lockout/Tagout Permit (LOTO) so they could work under the LOTO and connect the wires. The Chief Construction Manager obtained LOTO Permit #939 and at the 'Plan of the Day' meeting in the morning of 10/16/2013, he notified KMS that the Permit was ready and directed KMS to contact him when work under that LOTO Permit was ready to start. At 1000 hours that day, KMS informed the CCM that the pump had already been connected. KMS workers believed that they could proceed with the connection because the circuit was protected by an administrative LOTO lock. The work was performed without proper implementation of the LOTO Permit and was in violation of the LBNL 'one worker, one lock' requirement. The CCM order a stand-down at the B33 job site. All project energization activities were suspended until further notice.
Cause Description:
Operating Conditions: indoors, lighted, dry
Activity Category: Construction
Immediate Action(s): - The Chief Construction Manager ordered a stand-down. - All energization activities on the GPL project was suspended until further notice.
FM Evaluation: - Subcontractor KMS must submit a written procedure describing how they intend to implement LBNL electrical procedures before allowed to return to work.
DOE Facility Representative Input:
DOE Program Manager Input:
Further Evaluation is Required:
No
Division or Project: Facilities Division
Plant Area: B33
System/Building/Equipment: B33 General Purpose Laboratory (GPL) vacuum pump
Facility Function: Balance of Plant - Infrastructure (Other Functions not specifically listed in this Category)
Corrective Action:
Lessons(s) Learned:
HQ Keywords: 01A--Inadequate Conduct of Operations - Inadequate Conduct of Operations (miscellaneous) 01K--Inadequate Conduct of Operations - Lockout/Tagout Noncompliance (Electrical)

Attachment 2
39
01R--Inadequate Conduct of Operations - Management issues 11G--Other - Subcontractor 12I--EH Categories - Lockout/Tagout (Electrical or Mechanical) 14E--Quality Assurance - Work Process Deficiency 14G--Quality Assurance - Procurement Deficiency
HQ Summary: On October 15, 2013, a subcontractor, Kinetic Mechanical Systems (KMS), performed work on a vacuum pump without proper implementation of a lockout/tagout (LOTO) permit. The Lawrence Berkeley National Laboratory (LBNL) Facilities Chief Construction Manager had noticed that the subcontractors had not connected motor wires for the vacuum pump and obtained a permit for KMS on October 16. However, KMS informed the Chief Construction Manager that the pump had already been connected since the subcontractor believed that they could proceed with the connection because the circuit was protected by an administrative LOTO lock. The work resulted in the violation of the LBNL 'one worker, one lock' requirement. All project activities involving energizing equipment were suspended.
Similar OR Report Number:
Facility Manager: Name Jennifer Ridgeway
Phone (510) 486-6339
Title Division Director
Originator: Name MOU, FLORENCE P.
Phone (510) 486-7872
Title SENIOR ADMINISTRATOR
HQ OC Notification: Date Time Person Notified Organization
NA NA NA NA
Other Notifications: Date Time Person Notified Organization
10/16/2013 20:32 (PTZ) Duty Officer BSO
10/16/2013 20:32 (PTZ) Mary Gross BSO
Authorized Classifier(AC):
12)Report Number: SC--BSO-LBL-OPERATIONS-2013-0021 After 2003 Redesign
Secretarial Office: Science
Lab/Site/Org: Lawrence Berkeley National Laboratory
Facility Name: Operations Division
Subject/Title: B70A Energized Electric Controller Box Door Found Open - No Exposure, No Injuries
Date/Time Discovered: 10/14/2013 13:00 (PTZ)
Date/Time Categorized: 10/18/2013 10:30 (PTZ)

Attachment 2
40
Report Type: Update
Report Dates: Notification 10/22/2013 22:34 (ETZ)
Initial Update 12/02/2013 16:34 (ETZ)
Latest Update 12/02/2013 16:34 (ETZ)
Final
Significance Category: 3
Reporting Criteria: 2E(2) - Any unexpected discovery of an uncontrolled electrical hazardous energy source (e.g., live electrical power circuit, etc.). This criterion does not include discoveries made by zero-energy checks and other precautionary investigations made before work is authorized to begin.
Cause Codes:
ISM: 3) Develop and Implement Hazard Controls 5) Provide Feedback and Continuous Improvement
Subcontractor Involved: Yes Cal Neva
Occurrence Description: At approximately 1300 hours on 10/14/2013, an EHS construction safety employee in Building 70A room 1109 noticed that the enclosure door of an electric controller box was left open, with wires hanging out of the box, without warning signs or barriers. Workers from Facilities subcontractor Cal Neva were working in room 1105 which is undergoing renovation for a research laboratory under the BARDA Project. The box was relocated to its current location in room 1109 to control ultraviolet lighting in the adjacent room through an interlock system. Cal Neva electricians installed the interlock system and determined it failed to function properly. The project construction manager requested assistance from Engineering Division's (ENG) electronics technician group leader whose technician had originally fabricated the electric controller in-house. On 10/08/2013, after surveying the box, the Engineering electronics group lead and the interlock engineer believed that some of the timing relay components might be incorrect for the installation and would require a new schematic drawing and components modification for the subcontractor workers to perform the rewiring. After surveying the box, the Engineering electronics group leader closed the hinged door and latched the door to the box. Upon noticing the open box door on 10/14/2013, the construction safety employee used a proximity tester and noted that the wires were live. He immediately notified EHS Electric Safety Program Manager who in turn requested Facilities electrical safety engineer (ESE) to assess the situation. The ESE arrived at the scene shortly thereafter and confirmed that the controller box contained several energized 120 V exposed contacts. He

Attachment 2
41
requested a Facilities electrician to immediately secure the wiring, close the door, and tighten the latch screws to keep the door securely closed.
Cause Description:
Operating Conditions: Indoors, Lighted, Dry
Activity Category: Construction
Immediate Action(s): - The construction safety employee notified EHS electric safety program manager about the open box door.
FM Evaluation: - Preliminary fact finding was unable to identify definitively who had opened and left the box door open. - Activities in and personnel that accessed room 1109 between 10/08 and 10/14 are yet to be determined. - EHS will conduct an apparent cause analysis of the event. 12/02/2013 UPDATE: The reporting division for this occurrence was changed from EHS to Facilities in the beginning of November. As a result, Facilities Division chartered a new investigation and apparent cause analysis team, which is in the process of finalizing its investigation report. LBNL is requesting for a three-week extension to submit the ORPS final report on 12/20/2013.
DOE Facility Representative Input:
DOE Program Manager Input:
Further Evaluation is Required:
Yes. Before Further Operation? No By Whom: EHS, Eng, Facilities By When:
Division or Project: Facilities Division
Plant Area: B70A-1109
System/Building/Equipment: Building 70A Room 1109 Electric Controller Box
Facility Function: Balance of Plant - Infrastructure (Other Functions not specifically listed in this Category)
Corrective Action:
Lessons(s) Learned:
HQ Keywords: 01A--Inadequate Conduct of Operations - Inadequate Conduct of Operations (miscellaneous) 01Q--Inadequate Conduct of Operations - Personnel error 08H--OSHA Reportable/Industrial Hygiene - Safety Noncompliance 11G--Other - Subcontractor

Attachment 2
42
12C--EH Categories - Electrical Safety 14E--Quality Assurance - Work Process Deficiency
HQ Summary: On October 14, 2013, a construction safety employee noticed that the enclosure door of an electric controller box was left open, with wires hanging out of the box, without warning signs or barriers. The box was relocated to its current position in room 1109 to control ultraviolet lighting in the adjacent room through an interlock system. Subcontractor electricians installed the interlock system and determined it failed to function properly. The Engineering Electronics group leader surveyed the box, closed the hinged door and latched the door to the box. After discovery of the opened box, an electrical safety engineer confirmed the box contained several energized 120-volt exposed contacts. An electrician secured the wiring and tightened the latch screws to keep the door securely closed. A preliminary fact finding was unable to identify who had opened and left the box door open.
Similar OR Report Number:
Facility Manager: Name Joseph Dionne
Phone (510) 486-7586
Title Interim Division Director
Originator: Name MOU, FLORENCE P.
Phone (510) 486-7872
Title SENIOR ADMINISTRATOR
HQ OC Notification: Date Time Person Notified Organization
NA NA NA NA
Other Notifications: Date Time Person Notified Organization
10/18/2013 11:21 (PTZ) Kevin Hartnett BSO
10/18/2013 11:21 (PTZ) Mary Gross BSO
Authorized Classifier(AC):
13)Report Number: SC--FSO-FNAL-FERMILAB-2013-0008 After 2003 Redesign
Secretarial Office: Science
Lab/Site/Org: FERMI National Accelerator Laboratory
Facility Name: FERMI National Accelerator Lab.(BOP)
Subject/Title: Contact with abandoned heliax cable causes employee electrical shock
Date/Time Discovered: 10/29/2013 13:30 (CTZ)
Date/Time Categorized: 10/29/2013 15:30 (CTZ)
Report Type: Notification
Report Dates: Notification 10/30/2013 16:55 (ETZ)
Attachment 2
43
Initial Update
Latest Update
Final
Significance Category: 2
Reporting Criteria: 2E(1) - Any unexpected or unintended personal contact (burn, injury, etc.) with an electrical hazardous energy source (e.g., live electrical power circuit, etc.).
Cause Codes:
ISM:
Subcontractor Involved: No
Occurrence Description: The employee was working in the MI-30 Service Building troubleshooting an instrumentation problem when he received an electrical shock. Simultaneously, the Main Injector (MI) accelerator high voltage bus tripped on a ground fault indication, shutting down power to the bus. The employee stated that he was reading a monitor in the MI-30 Control Room. While reading the monitor, he rested his left hand on a vertical section of one side of a relay rack while at the same time he rested his right hand on the vertical section of the other side of the relay rack. There were two heliax cables, terminated with connectors but not grounded or connected to a device, tied together with a cable tie running along the right side of the relay rack. As the employee grasped the relay rack with his right hand, his hand also came in contact with the connectors on the ends of these cables. He then experienced an electric shock in his right arm. The shock caused his right hand to clench around the vertical portion of the rack and the cable connectors, bringing the connectors into contact with the grounded vertical portion of the relay rack. The employee jerked back sharply and pulled free of the rack. He experienced mild pain in his right hand due to the shock and, later, pain in his right elbow related to the force with which he pulled his hand off of the rack. He went to the onsite Medical Department where he was given an EKG which revealed no irregular conditions. The employee returned to work without restrictions. The two cables connect to larger cables before leaving the Control Room and entering the MI-30 Kicker Room. The cables then run through a penetration and down to the Main Injector Tunnel. An access was made to the Main Injector tunnel following the incident. The cables were located and one of them was found to have a damaged outer jacket. The ground shield on this cable was exposed due to the jacket damage and the ground shield had come in contact with the exposed MI bus. The bus voltage ranges up to 800 V dc. The cable was no longer in use and had been abandoned in place.
Cause Description:

Attachment 2
44
Operating Conditions: Normal
Activity Category: Normal Operations (other than Activities specifically listed in this Category)
Immediate Action(s): The Main Injector accelerator was turned off and prepared for access. An access was made by system experts; the cable with the damaged outer jacket was located and it was determined that the ground shield was contacting the MI magnet bus. The cable was moved away from the bus. The MI accelerator was kept in stand-by mode while preparations were made to do an examination of the entire MI magnet bus to look for similar conditions.
FM Evaluation: The Accelerator Division Head kept the Main Injector in stand-by mode until the evaluation of the entire MI magnet bus is completed. In addition, the Accelerator Division will conduct a thorough investigation that will include Human Performance Improvement (HPI) fundamentals and established meaningful corrective actions and lessons learned.
DOE Facility Representative Input:
DOE Program Manager Input:
Further Evaluation is Required:
Yes. Before Further Operation? Yes By Whom: Accelerator Division By When: 10/30/2013
Division or Project: Accelerator Division
Plant Area: Main Injector
System/Building/Equipment: Main Injector Service Building 30 (MI-30)
Facility Function: Accelerators
Corrective Action:
Lessons(s) Learned:
HQ Keywords: 07D--Electrical Systems - Electrical Wiring 08A--OSHA Reportable/Industrial Hygiene - Electrical Shock 12C--EH Categories - Electrical Safety 14L--Quality Assurance - No QA Deficiency
HQ Summary: On October 29, 2013, an employee was working in the Main Injector (MI)-30 Service Building troubleshooting an instrumentation problem when he received an electrical shock. Simultaneously, the MI accelerator high voltage bus tripped on a ground fault indication, shutting down power to the bus. While reading a monitor in the MI-30 Control Room, he rested his left hand on a vertical section of one side of a relay rack while at the same time he rested his right hand on the vertical section of the other side of the relay rack. There were two heliax cables, terminated with connectors but not grounded or connected to a device, tied together with a cable tie running along the right side of the relay rack. As the employee grasped the
Attachment 2
45
relay rack with his right hand, his hand also came in contact with the connectors on the ends of these cables. The employee was sent to the onsite Medical Department which revealed no irregular conditions and returned to work without restrictions.
Similar OR Report Number:
Facility Manager: Name Victoria White
Phone (630) 840-3936
Title Chief Operating Officer
Originator: Name BAIRD, DAVID I.
Phone (630) 840-3945
Title ESH SPECIALIST
HQ OC Notification: Date Time Person Notified Organization
NA NA NA NA
Other Notifications: Date Time Person Notified Organization
10/29/2013 15:00 (CTZ) Mark Bolinger DOE FSO
10/29/2013 15:00 (CTZ) Michael Herr DOE FSO
10/29/2013 15:00 (CTZ) Victoria White FNAL COO
10/29/2013 15:00 (CTZ) Paul Czarapata AD-DH
10/29/2013 15:00 (CTZ) Roger Dixon AD-Head
10/29/2013 15:00 (CTZ) Martha Michels FNAL ESH
Authorized Classifier(AC):
14)Report Number: SC-ORO--ORNL-X10EAST-2013-0010 After 2003 Redesign
Secretarial Office: Science
Lab/Site/Org: Oak Ridge National Laboratory
Facility Name: ORNL East Complex
Subject/Title: Discovery of an Unexpected Energy Source after Replacement of a Circuit Relay
Date/Time Discovered: 10/28/2013 12:40 (ETZ)
Date/Time Categorized: 10/28/2013 14:50 (ETZ)
Report Type: Notification
Report Dates: Notification 10/30/2013 18:50 (ETZ)
Initial Update
Latest Update
Final
Significance Category: 3

Attachment 2
46
Reporting Criteria: 2E(2) - Any unexpected discovery of an uncontrolled electrical hazardous energy source (e.g., live electrical power circuit, etc.). This criterion does not include discoveries made by zero-energy checks and other precautionary investigations made before work is authorized to begin.
Cause Codes:
ISM: 3) Develop and Implement Hazard Controls
Subcontractor Involved: No
Occurrence Description: On October 28, 2013, a qualified electrical worker replaced a 120 volt circuit relay after performing Lock-Out/Tag-Out (LOTO) at the breakers indicated on drawings. A zero energy check was performed at the relay's electrical contacts indicating zero voltage. The LOTO and zero energy check were performed in accordance with ORNL procedures including the appropriate PPE. After establishing electrical safe working conditions, the worker removed his voltage rated gloves. The worker installed the new relay and performed post-maintenance testing which indicated abnormal results. Investigation identified the presence of an unexpected energized source. Line Management was immediately notified. ORNL line management notified the Laboratory Shift Superintendent and the event was categorized as an SC3, 2E(2) "Unexpected Discovery of an Uncontrolled Electrical Hazardous Energy Source." There was no injury with hazardous energy or other environmental, health and safety impacts as a result of the event.
Cause Description:
Operating Conditions: Normal
Activity Category: Maintenance
Immediate Action(s): - The system was immediately placed in a safe condition. - On October 29, 2013, a critique was held.
FM Evaluation: ORNL management is evaluating the circumstances around the event, will implement actions as appropriate, and share any resulting lessons learned.
DOE Facility Representative Input:
DOE Program Manager Input:
Further Evaluation is Required:
Yes. Before Further Operation? No By Whom: Richard M. Griffey By When: 12/13/2013
Division or Project: Facilities Management Division

Attachment 2
47
Plant Area: Building 5600
System/Building/Equipment: Building 5600
Facility Function: Balance of Plant - Infrastructure (Other Functions not specifically listed in this Category)
Corrective Action:
Lessons(s) Learned:
HQ Keywords: 01M--Inadequate Conduct of Operations - Inadequate Job Planning (Electrical) 12C--EH Categories - Electrical Safety 14E--Quality Assurance - Work Process Deficiency
HQ Summary: On October 28, 2013, a qualified electrical worker replaced a 120-volt circuit relay after performing lockout/tagout at the breakers indicated on drawings. A zero energy check was performed at the relay's electrical contacts indicating zero voltage. The worker installed the new relay and performed post maintenance testing which indicated abnormal results. An investigation identified the presence of an unexpected energized source. The system was immediately placed in a safe condition and Management was notified.
Similar OR Report Number:
Facility Manager: Name Richard M. Griffey
Phone (865) 574-8907
Title Complex Facilities Manager
Originator: Name PEHRSON, PAUL B.
Phone (865) 576-7929
Title OCCURRENCE REPORTING MANAGER
HQ OC Notification: Date Time Person Notified Organization
NA NA NA NA
Other Notifications: Date Time Person Notified Organization
10/28/2013 14:50 (ETZ) Lab Shift Superintendent ORNL LSS
10/28/2013 15:38 (ETZ) Johnny Moore DOE ORNL
10/28/2013 15:38 (ETZ) Martha Kass DOE ORNL
Authorized Classifier(AC):
15)Report Number: SC-ORO--ORNL-X10WEST-2013-0002 After 2003 Redesign
Secretarial Office: Science
Lab/Site/Org: Oak Ridge National Laboratory
Facility Name: ORNL West Complex
Subject/Title: Lock Out/Tag Out Administrative Control Violation

Attachment 2
48
Date/Time Discovered: 10/14/2013 13:00 (ETZ)
Date/Time Categorized: 10/15/2013 11:30 (ETZ)
Report Type: Notification/Final
Report Dates: Notification 10/17/2013 15:14 (ETZ)
Initial Update 10/17/2013 15:14 (ETZ)
Latest Update 10/17/2013 15:14 (ETZ)
Final 10/17/2013 15:14 (ETZ)
Revision 1 10/18/2013 10:49 (ETZ)
Significance Category: 4
Reporting Criteria: 2E(3) - Any failure to follow a prescribed hazardous energy control process (e.g., lockout/tagout, hazardous energy control program).
Cause Codes:
ISM: 4) Perform Work Within Controls
Subcontractor Involved: No
Occurrence Description: On October 14, 2013, two employees opened a panel on a recently installed instrument that had not been placed in service. Although not in service, a 120 V circuit had been installed between the circuit breaker and the instrument. The circuit had been locked out by an electrician and was verified to be in a safe condition. The electrical conductors had not been attached to the instrument and were insulated and taped in an adjacent closed power supply compartment located immediately below the instrument panel accessed. The two employees did not apply personal locks prior to accessing the panel. The ORNL hazardous energy control process requires locks to be applied by all personnel involved in the work activities, which was not followed in this instance, and resulted in a violation of the ORNL lockout/tagout process. On October 15, 2013, during the critique of the event, line management determined that an administrative violation of the lockout/tagout process had occurred. Line Management notified the Laboratory Shift Superintendent and the event was categorized as a Group 2, Subgroup E(3), Significance Category 4 event, "Failure to Follow a Prescribed Hazardous Energy Control Process." There was no injury or contact with hazardous energy or other environmental, health and safety impacts as a result of the event.
Cause Description:
Operating Conditions: Normal
Activity Category: Research
Attachment 2
49
Immediate Action(s): All activities associated with the instrument were suspended and a qualified electrical worker verified that the instrument was in a safe condition.
FM Evaluation: ORNL management is evaluating the circumstances around the event, will implement actions as appropriate, and share any resulting lessons learned.
DOE Facility Representative Input:
DOE Program Manager Input:
Further Evaluation is Required:
No
Division or Project: Energy and Transportation Science Division
Plant Area: Building 3144
System/Building/Equipment: Building 3144
Facility Function: Laboratory - Research & Development
Corrective Action:
Lessons(s) Learned:
HQ Keywords: 01K--Inadequate Conduct of Operations - Lockout/Tagout Noncompliance (Electrical) 08H--OSHA Reportable/Industrial Hygiene - Safety Noncompliance 12I--EH Categories - Lockout/Tagout (Electrical or Mechanical) 14E--Quality Assurance - Work Process Deficiency
HQ Summary: On October 14, 2013, two employees violated the ORNL lockout/tagout process when they opened a panel on a recently installed instrument without applying personal locks. Although the instrument was not in service, a 120-volt circuit had been installed between the circuit breaker and the instrument. The circuit had been locked out by an electrician and was verified to be in a safe condition. The ORNL hazardous energy control process requires locks to be applied by all personnel involved in the work activities.
Similar OR Report Number:
Facility Manager: Name David E. Fowler
Phone (865) 574-7300
Title EESD Safety and Business Operations, Group Leader
Originator: Name PEHRSON, PAUL B.
Phone (865) 576-7929
Title OCCURRENCE REPORTING MANAGER
HQ OC Notification: Date Time Person Notified Organization
NA NA NA NA

Attachment 2
50
Other Notifications: Date Time Person Notified Organization
10/15/2013 11:30 (ETZ) Lab. Shift Superintendent ORNL DOE
10/15/2013 13:09 (ETZ) Johnny Moore DOE ORNL
10/15/2013 13:09 (ETZ) Martha Kass DOE ORNL
Authorized Classifier(AC):
| ORPS HOME | Data Entry | FM Functions | Search & Reports | Authorities | Help | Security/Privacy
Notice | Please send comments or questions to [email protected] or call the Helpline
at (800) 473-4375. Hours: 7:30 a.m. - 5:00 p.m., Mon - Fri (ETZ). Please include detailed information when reporting problems.





























