Embed Size (px)
Citation preview
October 2009
Medical Equipment GuidelinesClaim Attachments andDenial Resolution
Presented by EDS Provider Field Consultants
MEDICAL EQUIPMENT UPDATES2 / OCTOBER 2009
Agenda
• Date of Service
• Provider Code Sets
• Capped Rental
• Repair and Replacement
• Billing the Member
• Rolling 12 Month Period
• Mail Order Incontinence, Ostomy, and Colostomy Supplies
• Claim Attachments
• Denials and Resolutions
• Helpful Tools
• Questions
Welcome and Announcements
MEDICAL EQUIPMENT UPDATES3 / OCTOBER 2009
Session Objectives
• Following this session, providers will be able to understand:
– Medical Equipment Guidelines
– Claim Attachment Process
– Top Denials and Resolutions
MEDICAL EQUIPMENT UPDATES4 / OCTOBER 2009
Medical Equipment Guidelines
MEDICAL EQUIPMENT UPDATES5 / OCTOBER 2009
Date of Service
•The date of service is the date the equipment is delivered, not ordered
•For the IHCP to reimburse for medical equipment, the member must be eligible on the date of service (date of delivery)
MEDICAL EQUIPMENT UPDATES6 / OCTOBER 2009
Provider Code Sets
•The IHCP established code sets to ensure appropriate reimbursement for medical equipment codes
•Providers must ensure that they are enrolled as the correct provider type and specialty
– Type and specialty can be verified using the Provider Profile option on the Web interChange
MEDICAL EQUIPMENT UPDATES7 / OCTOBER 2009
Provider Code Sets
•The durable medical equipment (DME) provider type is 25 and the following are provider specialties:– 251 – Home medical equipment provider
– 250 – DME/Medical supply dealer
– Enrolling in the 251 specialty does not cover services in the 250 specialty, and enrolling in the 250 specialty does not cover services in the 251 specialty
Page 5 of the paper Provider Enrollment form lists the primary specialty in box 39, the additional specialty can be hand written in the unassigned box to the right
MEDICAL EQUIPMENT UPDATES8 / OCTOBER 2009
Capped Rental
• Certain procedure codes are limited to 15 months of continuous rental
• The IHCP evaluates requests from providers for approval of capped rental items
– In long-term need situations, a decision may be made to classify the item as “purchase” instead of “rental”
• Continuous rental is defined as rental without interruption for a period of more than 60 days
– A change in provider does not cause an interruption in the rental period
• A complete list of procedure codes for capped rental can be found in the Indiana Health Coverage Programs Provider Manual, Chapter 8, Section 4
• The provider must service the item at no cost to the IHCP
MEDICAL EQUIPMENT UPDATES9 / OCTOBER 2009
Capped Rental
•Centers for Medicare and Medicaid Services (CMS) changed the capped rental policy for DME
•The new policy states that the capped rental period is 13 months
– After 13 months, the member owns the DME
•Medicare will pay for reasonable and necessary maintenance and service of the DME item
– This policy change applies to DME items in which the first month of rental is on or after January 1, 2006
•At this time, Medical Policy has not been directed to make changes to the IHCP’s capped rental policy
MEDICAL EQUIPMENT UPDATES10 / OCTOBER 2009
Capped RentalClaims Submitted for Capped Rental Items
The allowed charge is the lower of the 1993 Medicare rental fee schedule amount or the actual submitted charge
•The IHCP pays claims until the number of rental payments made reaches the capped rental number of 15 months
•When the 15 month rental period has been exhausted, the DME/HME equipment is considered purchased and becomes the property of OMPP
•Providers should base their decisions to rent or purchase DME or HME on the least expensive option available for the anticipated period of need
MEDICAL EQUIPMENT UPDATES11 / OCTOBER 2009
Repair and Replacement
•Repair of purchased equipment may require prior authorization based on the Healthcare Common Procedure Coding System (HCPCS) codes
•The IHCP does not pay for repair of equipment still under warranty
•The IHCP does not authorize payment for repair necessitated by member misuse or abuse, whether intentional or unintentional
•The rental provider is responsible for repairs to rental equipment
MEDICAL EQUIPMENT UPDATES12 / OCTOBER 2009
Repair and Replacement
•The IHCP does not cover payment for maintenance charges of properly functioning equipment
•The IHCP does not authorize replacement of medical equipment more than once every five years per member
– More frequent replacement is allowed only if there is a change in the member’s medical needs that is documented in writing and significant enough to warrant a different type of equipment. Such requests require PA
•A long-term care (LTC) facility’s per diem rate includes repair costs for equipment
MEDICAL EQUIPMENT UPDATES13 / OCTOBER 2009
Billing the Member•The following circumstances are the only situations in
which an IHCP provider may bill a member:
– The service rendered is non-covered by the IHCP
– The member has exceeded the program limitations for a particular service; for example, the services were denied prior authorization (PA)
– Before receiving the service, the member must understand that the service is not covered under the IHCP, and the member is responsible for the charges associated with the service
– A signed waiver must be maintained in the member’s record that the member voluntarily chose to receive a service that was not covered by IHCP
MEDICAL EQUIPMENT UPDATES14 / OCTOBER 2009
Billing the Member• “Medicaid-pending” individuals are responsible to pay the
provider
• It is the patient’s responsibility to notify the provider of Medicaid approved status within 12 months of the date of service
• Providers may bill the patient if there is no notification of Medicaid eligibility within this time period
• Providers may also bill the member when the spend-down or a copay applies to the claim
• Spend-down – Look for ARC Code 178 on the remittance advice
• Copay – Look for ARC Code 3 on the remittance advice
MEDICAL EQUIPMENT UPDATES15 / OCTOBER 2009
Rolling 12 Month Period
• Is not:– Based on a 12-month calendar year
– Based on a fiscal year
– Renewable on January 1 of each year
• Is:– Based on the first date that services are
rendered by a particular provider
– Renewable one unit at a time beginning 365 days after the date that services are rendered by a particular provider
MEDICAL EQUIPMENT UPDATES16 / OCTOBER 2009
Mail Order Incontinence, Ostomy, and Colostomy SuppliesContracted Vendors
•Effective February 1, 2008, the OMPP contracted with three vendors to provide incontinence, ostomy, and urological supplies to fee-for-service members
•The three contracted vendors are:– Binson’s Home Health Care Center
1-888-217-9610www.binsons.com
– Healthcare Products Delivery, Inc (HPD)1-800-291-8011www.hpdinc.net
– J & B Medical1-866-674-5850www.jandbmedical.com
MEDICAL EQUIPMENT UPDATES17 / OCTOBER 2009
•Members must obtain supplies via mail order – The contracted vendor may make other
arrangements in emergency situations
•The contracted vendors began providing services February 1, 2008, with full implementation completed on June 1, 2008
•A full listing of codes affected by this change is available in BT200823
•The annual maximum allowable reimbursement is $1,950 per member per rolling calendar year.
Mail Order Incontinence, Ostomy, and Colostomy Supplies
MEDICAL EQUIPMENT UPDATES18 / OCTOBER 2009
Mail Order Incontinence, Ostomy, and Colostomy Supplies
•The contracted vendor service applies to the Fee for Service and Care Select Programs
•Only paid Crossovers and TPL claims are excluded from the program– If Medicare or the TPL denies the claim, the services are
limited to the 3 contracted vendors
•The following programs and claim types are not affected by the contract:– 590 Program– Medical Review Team (MRT)– Pre-Admission Screening and Resident Review (PASRR)– Long Term Care (LTC)– Waiver
•Risk-based managed care (RBMC) members are excluded– Supplies for these members are billed to the appropriate
managed care organization (MCO)
Program Guidelines
MEDICAL EQUIPMENT UPDATES19 / OCTOBER 2009
Nursing Assessment
•A needs assessment is part of the initial enrollment process
•Members receive a telephone call from a staff nurse or a questionnaire by mail
•The questionnaire gives the vendor additional information regarding the member’s supply needs
Mail Order Incontinence, Ostomy and Colostomy Supplies

MEDICAL EQUIPMENT UPDATES20 / OCTOBER 2009
Claim Attachments

MEDICAL EQUIPMENT UPDATES21 / OCTOBER 2009
Claim Attachments
MEDICAL EQUIPMENT UPDATES22 / OCTOBER 2009
Claim Attachments
MEDICAL EQUIPMENT UPDATES23 / OCTOBER 2009
Claim Attachments
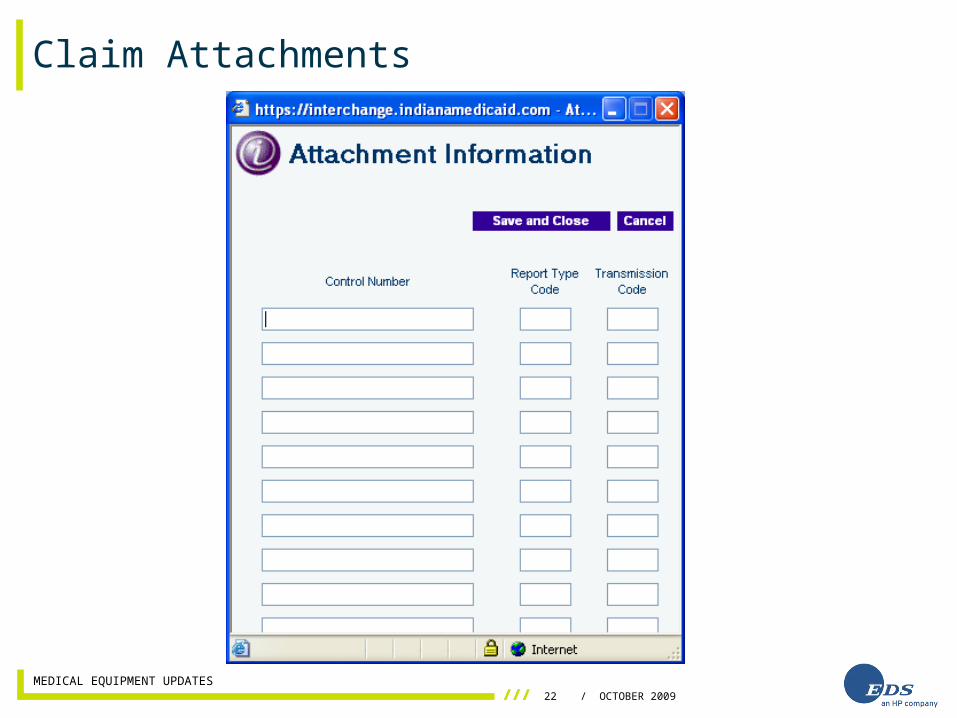
•Unique number assigned by provider
•Claim and document specific
•Each ACN may only be used one time
•Write “ACN #” and the assigned ACN on each page of documentation corresponding to that number
Attachment Control Number (ACN)
MEDICAL EQUIPMENT UPDATES24 / OCTOBER 2009
Claim Attachments
•Select the appropriate Report Type
– Report Type describes the document being sent
•Transmission Code defaults to “BM” – by mail
– Electronic and e-mailed attachments are not accepted
Report Type and Transmission Code
MEDICAL EQUIPMENT UPDATES25 / OCTOBER 2009
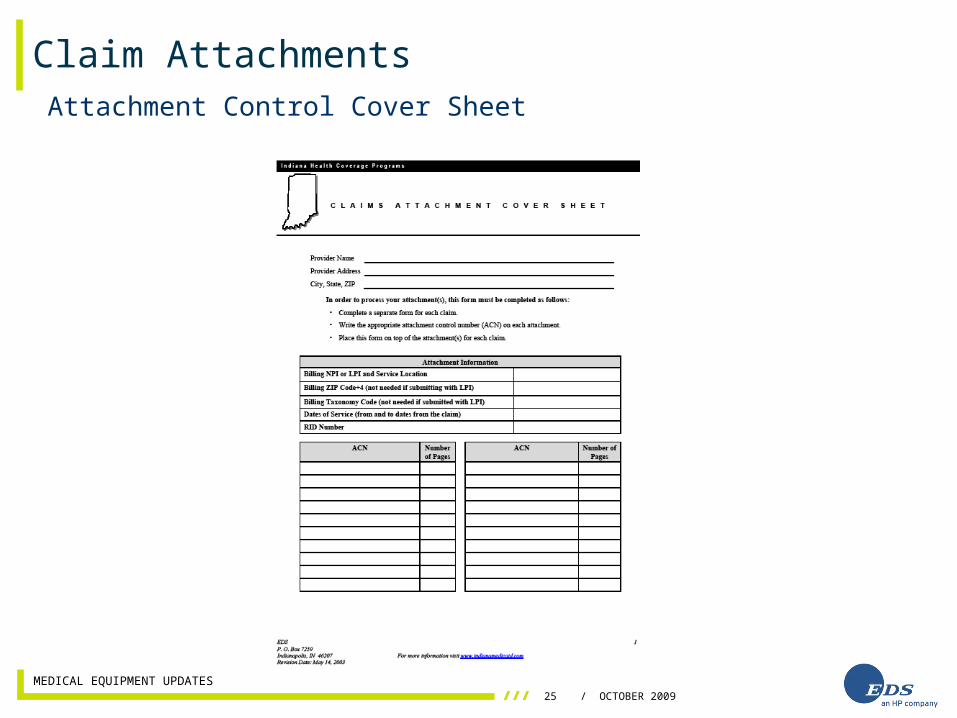
Claim AttachmentsAttachment Control Cover Sheet
MEDICAL EQUIPMENT UPDATES26 / OCTOBER 2009
Claim Attachments
•Available on IHCP home page, under Forms
•Complete cover sheet for each claim
• Include provider information
•Provide member ID
•List each ACN pertaining to specific attachment
• Indicate the number of pages of documentation submitted per attachment (not including the cover sheet)
•Mail cover sheet and supporting documentation to the appropriate P.O. Box (P.O. Box 7259)
Attachment Control Cover Sheet

MEDICAL EQUIPMENT UPDATES27 / OCTOBER 2009
Denials and Resolutions
MEDICAL EQUIPMENT UPDATES28 / OCTOBER 2009
Denials and Resolution
Denial: Edit 0593 – Medicare Denied Detail
Cause:
At least one detail submitted contains Medicare COB data resulting in a review of all detail COB data
Resolution:
• Review to ensure COB data for detail in question does not contain all zeros or is missing
• Crossover claim that has Medicare denied detail along with covered detail should be adjusted to only include the covered detail.
• Submit non-covered detail on separate claim with Medicare EOB – this is not a crossover claim
MEDICAL EQUIPMENT UPDATES29 / OCTOBER 2009
Denials and ResolutionDenial: Edit 0558 – Co-Insurance and Deductible Missing
Cause:
Claim submitted has no coinsurance and deductible amount indicating that this is not a crossover claim.
Resolution:• Compare the detail line(s) to the Medicare EOB and complete crossover
information• Medicare crossover claims can be submitted electronically using Web
interChange
The following header information is required for the claim to process:– Payer ID and Payer Name– TPL/Medicare Paid Amount – Subscriber Name, Primary ID, Relationship Code, Gender, DOB, and Claim
Filing Code – If the Payer ID is a Medicare payer and the Claim Filing Code is MA or MB, the
claim is considered to have crossover information
Note: Obtain COB information, including Payer IDs from the HELP tab, Reference Materials on Web interChange
MEDICAL EQUIPMENT UPDATES30 / OCTOBER 2009
Denials and Resolution
Denial: Edit 4209 – Procedure Code/Modifier Combination
Cause:
No matching pricing segment for the procedure/modifier combination billed on the HCFA 1500 Claim form
Resolution:
• Refer to the Provider Procedures Manual for the appropriate use of the modifiers TC, 26, RR, and NU.
- Effective December 31, 2008, the Centers for Medicare & Medicaid Services (CMS) end-dated modifier RP – replacement and repair, as announced in provider bulletin BT200843, dated December 30, 2008.
•Verify the procedure code/modifier combination on the Fee Schedule on the IHCP home page
MEDICAL EQUIPMENT UPDATES31 / OCTOBER 2009
Denial Edit 4021 – Procedure Code Vs Program Indicator
Cause:Procedure code is not covered for the dates of service for the
program billed
Resolution:Verify the procedure code and program coverage on the Fee
Schedule on the IHCP home page
Denials and Resolution
MEDICAL EQUIPMENT UPDATES32 / OCTOBER 2009
Denial: Edit 4033 - Invalid Procedure Code Modifier Combination
Cause:
The modifier used is not compatible with the procedure
code billed Resolution:
•Verify procedure code and modifier combination on the Fee Schedule on the IHCP home page
•Consult the IHCP Provider Manual
Denials and Resolution
MEDICAL EQUIPMENT UPDATES33 / OCTOBER 2009
Denial: Edit 6000 – Manual Pricing Required
Resolution: Submit Manual Pricing– Invoice requirements
• Date• Billed amount per unit (for example, box, case,
and so forth)• Calories (enteral feeding)• Procedure code• Member name• Member ID number• Itemization of repairs
– Bulk Invoices – illustrate calculations specific to the member
Denials and Resolution
MEDICAL EQUIPMENT UPDATES34 / OCTOBER 2009
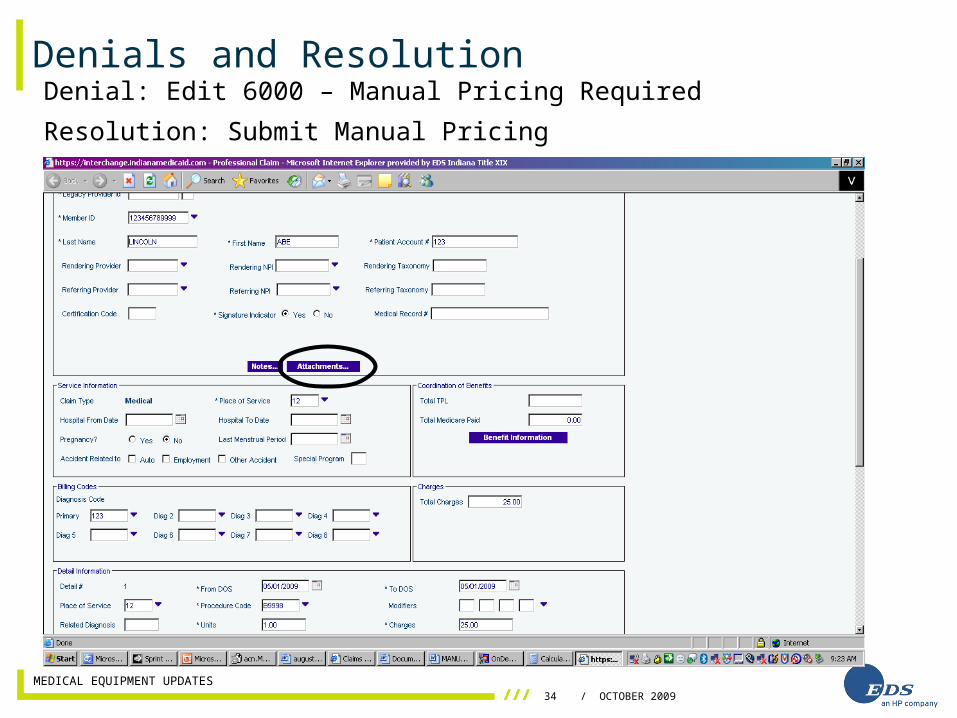
Denial: Edit 6000 – Manual Pricing Required
Resolution: Submit Manual Pricing
Denials and Resolution
MEDICAL EQUIPMENT UPDATES35 / OCTOBER 2009
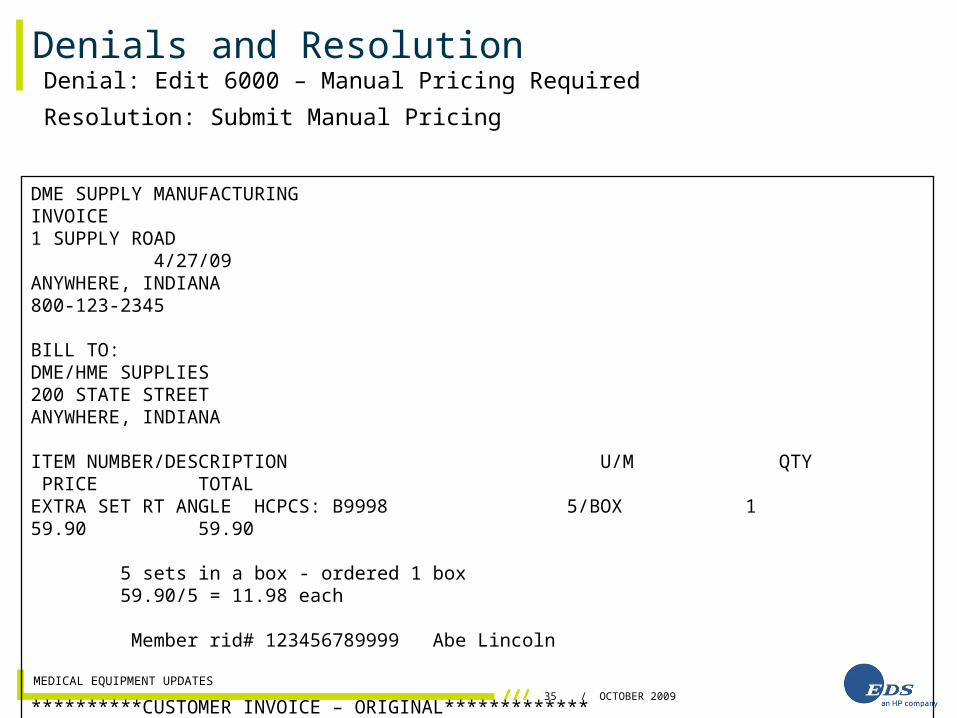
Denial: Edit 6000 – Manual Pricing Required
Resolution: Submit Manual Pricing
Denials and Resolution
DME SUPPLY MANUFACTURING INVOICE1 SUPPLY ROAD 4/27/09ANYWHERE, INDIANA800-123-2345
BILL TO:DME/HME SUPPLIES200 STATE STREETANYWHERE, INDIANA
ITEM NUMBER/DESCRIPTION U/M QTY PRICE TOTALEXTRA SET RT ANGLE HCPCS: B9998 5/BOX 1 59.90 59.90 5 sets in a box - ordered 1 box 59.90/5 = 11.98 each
Member rid# 123456789999 Abe Lincoln
**********CUSTOMER INVOICE – ORIGINAL*************
MEDICAL EQUIPMENT UPDATES36 / OCTOBER 2009
Denial: Edit 3001 - Dates of service not on P.A. master file.
Cause:
No Prior Authorization in IndianaAim
Resolution:
•Verify the date of service and procedure code billed are correct on the requested P.A.
•Obtain amended/corrected P.A. if necessary
Denials and Resolution
MEDICAL EQUIPMENT UPDATES37 / OCTOBER 2009
Denial: Edit 0509 – Net Charge Out of Balance
Cause:
•Claim totals do not balance to the net charge entered on the claim
Resolution:
•TPL claims: the net charge on a paper claim form in field 30, should equal the total charge, field 28, less the TPL paid amount, field 29
•Medicare Crossover claims: the total charge, field 28, and the net charge, field 30, should be the same
Denials and Resolution
MEDICAL EQUIPMENT UPDATES38 / OCTOBER 2009
Denial: Edit 2003 – Recipient Ineligible on Dates of Service
Cause:
•Member is not eligible for IHCP services being billed
Resolution:
•Verify member eligibility using Web interChange, AVR or Omni
•Verify the claim was sent to the appropriate billing entity– Fee for Service and Care Select to EDS
– RBMC to the appropriate MCO
Denials and Resolution
MEDICAL EQUIPMENT UPDATES39 / OCTOBER 2009
Helpful ToolsAvenues of Resolution
• IHCP Web site at www.indianamedicaid.com
• IHCP Provider Manual (Web, CD-ROM, or paper)
• Customer Assistance
– 1-800-577-1278, or
– (317) 655-3240 in the Indianapolis local area
• Written Correspondence
– P.O. Box 7263Indianapolis, IN 46207-7263
• Provider Relations Field Consultant
– View a current territory map and contact information online at HCP Web site at www.indianamedicaid.com
MEDICAL EQUIPMENT UPDATES40 / OCTOBER 2009
Questions
MEDICAL EQUIPMENT UPDATES41 / OCTOBER 2009
EDS and the EDS logo are registered trademarks of Hewlett-Packard Development Company, LP. HP is an equal opportunity employer and values the diversity of its people. ©2008 Hewlett-Packard Development Company, LP.
EDS
950 N. Meridian St., Suite 1150
Indianapolis, IN 46204