Embed Size (px)
Citation preview
October 12, 2016 DUR Meeting Minutes Page 1 of 26
Drug Utilization Review Board Meeting Minutes, Open Session
October 12, 2016 Drug Utilization Review Board Meeting Location: HP Enterprise Services, Building #283, Capital Room 6511 SE Forbes Ave, Topeka, KS 66619
DUR Board Members Present Lauren Morton, Pharm.D., BCPS, Chair James Backes, Pharm.D. Tim Heston, DO LaTonyua Rice, Pharm.D., CGP Roger Unruh, DO Moneeshindra Mittal, MD (phone) Judy Dowd, PA-C DUR Board Members Absent John Kollhoff, Pharm.D. DHCF Staff Present Annette Grant, RPh Carol Arace, Sr. Administrative Assistant Liane Larson, Pharm.D., Consultant to KDHE/DHCF HP Enterprise Services Staff Present Nancy Perry, R.N. Karen Kluczykowski, RPh HID Staff Present Rachel Boyer, PharmD, BCPS Ariane Casey, Pharm.D. (Phone) MCO Staff Present Jonalan Smith, Pharm.D., FASCP: Sunflower Health Plan Jennifer Murff, RPh: United Healthcare Community Plan Sosunmolu Shoyinka: Sunflower Health Plan
Representatives: Ashley Guerricagoiha; Austin Morgen, KU; Berend Koops, Merck; Brandon Shaffer, Celgene; Brent Hildebrand, Giliad; Chet Steckler, Purdue; Chris Stanfield, Supernus; Christina Yuan, KU; Danielle Harvey, Biogen; Deirdre Mourve, Allergan; Doug Wood, ViiV; Edie Dodson, Genzyme; Gay Thomas, BMS; Haley Gish, Pfizer; Hilary Gee, ACS CAN; Jeff Knappen, Allergan; Jim Baumann, Pfizer; Jody Reel, Pharm.D.; John Brokas, BMS; Julie McDavitt, B.I.; Kari Rinker, National MS Society; Laura Hill, Abbvie; Mary Jo DeFlorio, Janssen; Melissa Basil, Abbvie; Phil King, Pfizer; Roy Lindfield, Sunovion; Salen Benee; Scott Maurice, B.I.; Sue Boldra, Kansas House; Susan Zalenski, J & J; Teresa Blair, Ipsen; Terry McCurren, Otsuka; Todd Hudson, Ipsen
TOPIC DISCUSSION DECISION AND/OR ACTION I. Call to Order [13:05] Dr. Morton called the meeting to order at 10:08 am.
A. Announcements Dr. Larson provided the general parking announcement; Dr. Casey will be on the phone and Dr. Boyer is here; and introduced Annette Grant as the new Pharmacy Program Manager with KDHE. Dr. Larson noted there was a change to the original agenda and invited everyone to pick up the new one.
II. Old Business A. Review and Approval of the
Board Discussion None
Dr. Backes moved to accept the minutes as written.
October 12, 2016 DUR Meeting Minutes Page 2 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION July 13, 2016 DUR Meeting Minutes
Dr. Unruh seconded the motion.
The July 13, 2016 minutes were approved unanimously.
III. New Business A. Revised Prior Authorization
(PA) Criteria 1. Enbrel (Erelzi® [etanercept-szzs])
i. Revised PA Criteria
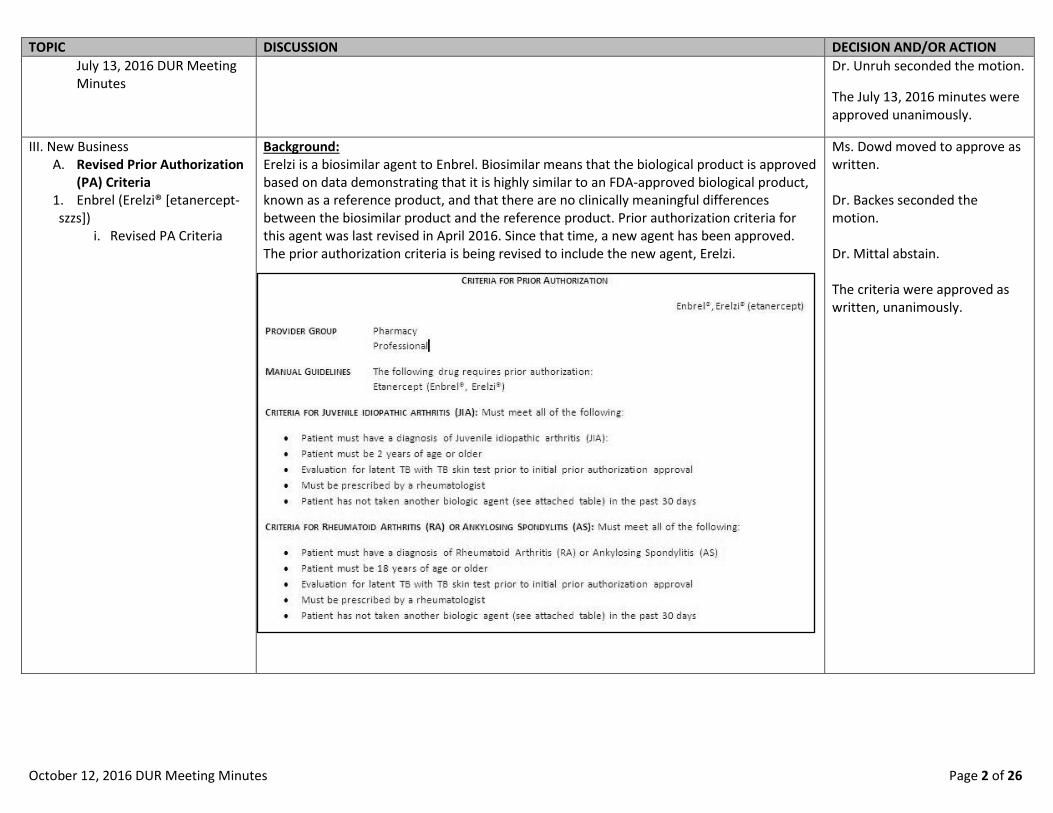
Background: Erelzi is a biosimilar agent to Enbrel. Biosimilar means that the biological product is approved based on data demonstrating that it is highly similar to an FDA-approved biological product, known as a reference product, and that there are no clinically meaningful differences between the biosimilar product and the reference product. Prior authorization criteria for this agent was last revised in April 2016. Since that time, a new agent has been approved. The prior authorization criteria is being revised to include the new agent, Erelzi.
Ms. Dowd moved to approve as written. Dr. Backes seconded the motion. Dr. Mittal abstain. The criteria were approved as written, unanimously.
October 12, 2016 DUR Meeting Minutes Page 3 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
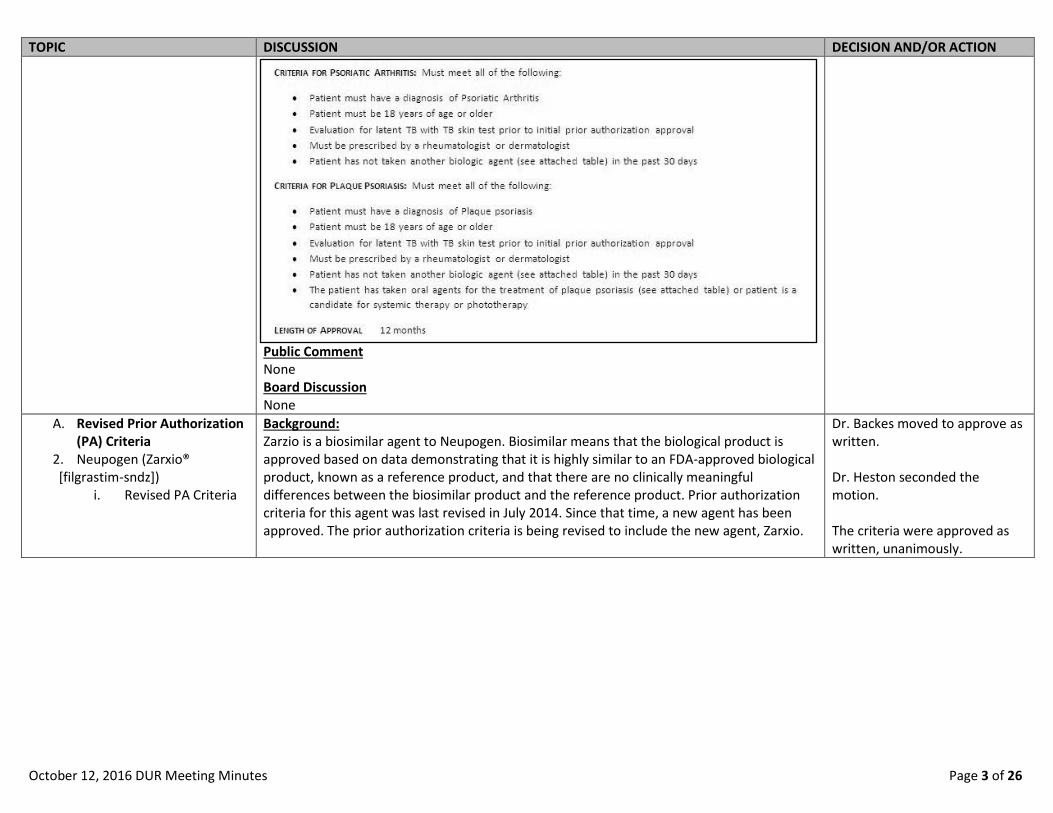
Public Comment None Board Discussion None
A. Revised Prior Authorization (PA) Criteria
2. Neupogen (Zarxio® [filgrastim-sndz])
i. Revised PA Criteria
Background: Zarzio is a biosimilar agent to Neupogen. Biosimilar means that the biological product is approved based on data demonstrating that it is highly similar to an FDA-approved biological product, known as a reference product, and that there are no clinically meaningful differences between the biosimilar product and the reference product. Prior authorization criteria for this agent was last revised in July 2014. Since that time, a new agent has been approved. The prior authorization criteria is being revised to include the new agent, Zarxio.
Dr. Backes moved to approve as written. Dr. Heston seconded the motion. The criteria were approved as written, unanimously.
October 12, 2016 DUR Meeting Minutes Page 4 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
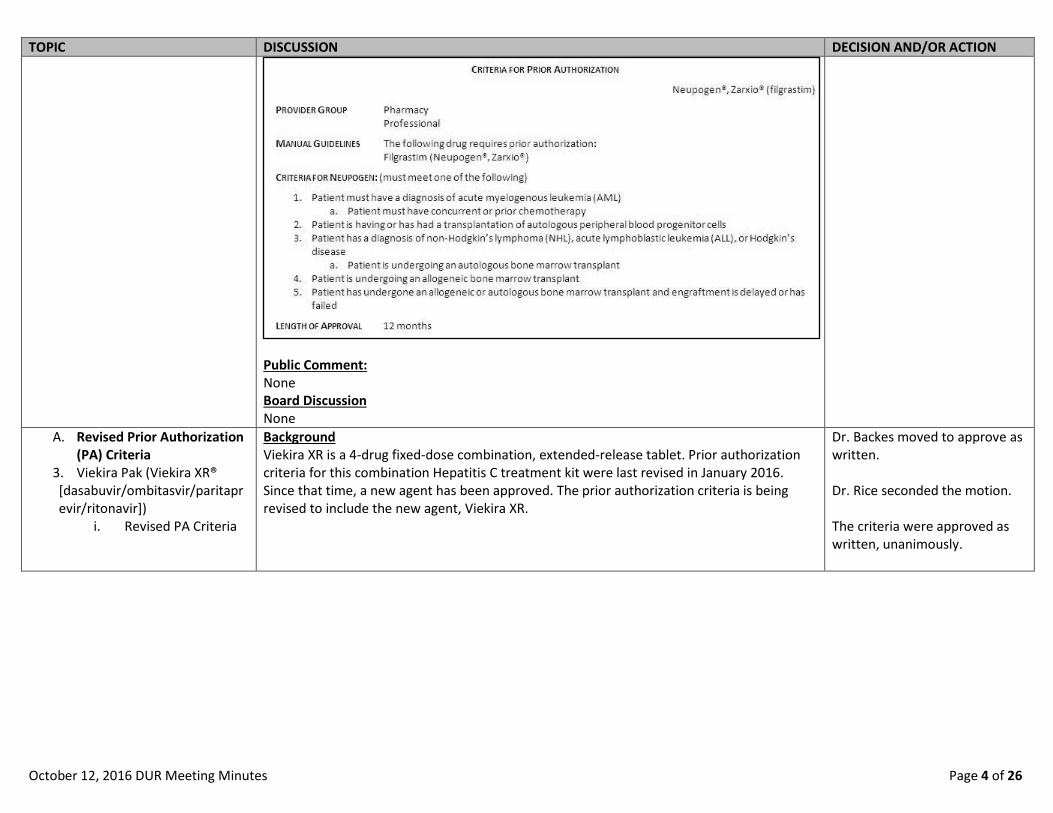
Public Comment: None Board Discussion None
A. Revised Prior Authorization (PA) Criteria
3. Viekira Pak (Viekira XR® [dasabuvir/ombitasvir/paritaprevir/ritonavir])
i. Revised PA Criteria
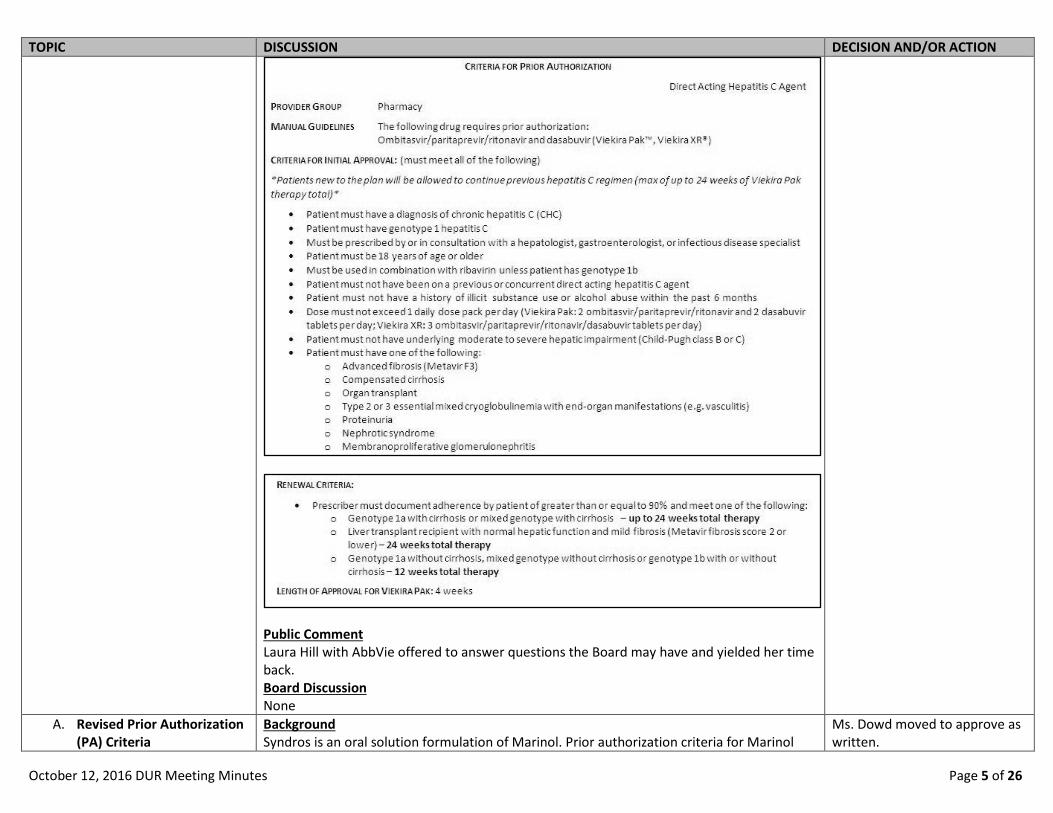
Background Viekira XR is a 4-drug fixed-dose combination, extended-release tablet. Prior authorization criteria for this combination Hepatitis C treatment kit were last revised in January 2016. Since that time, a new agent has been approved. The prior authorization criteria is being revised to include the new agent, Viekira XR.
Dr. Backes moved to approve as written. Dr. Rice seconded the motion. The criteria were approved as written, unanimously.
October 12, 2016 DUR Meeting Minutes Page 5 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
Public Comment Laura Hill with AbbVie offered to answer questions the Board may have and yielded her time back. Board Discussion None
A. Revised Prior Authorization (PA) Criteria
Background Syndros is an oral solution formulation of Marinol. Prior authorization criteria for Marinol
Ms. Dowd moved to approve as written.

October 12, 2016 DUR Meeting Minutes Page 6 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION 4. Marinol (Syndros® [dronabinol])
i. Revised PA Criteria
were last revised in July 2013. Since that time, a new agent has been approved. The prior authorization criteria is being revised to include the new agent, Syndros.
Public Comment None Board Discussion The Board discussion involved other indications for this agent and individuals over 65 years of age. Ms. Grant noted that if the State is the secondary payer, it goes through per the primary, i.e.: Medicare, and whatever criteria they may have.
Dr. Backes seconded the motion. The criteria were approved as written, unanimously.
A. Revised Prior Authorization (PA) Criteria
5. Long-Acting Opioid Dose Optimization (Troxyca ER® [oxycodone ER])
i. Revised PA Criteria
Background Troxyca ER is an opioid agonist indicated for the management of pain severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate. Prior authorization quantity criteria for these opiate agents were last revised in October 2015. Since that time, a new agent have been approved. The prior authorization criteria is being revised to include the new agent, Troxyca ER and change quantity limits before a PA is required.
Dr. Heston moved to approve as written. Dr. Backes seconded the motion. The criteria were approved as written, unanimously.

October 12, 2016 DUR Meeting Minutes Page 7 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
Public Comment Jim Bauman with Pfizer spoke on behalf of Troxyca. Board Discussion The FDA black box warning concerning the concurrent use of Benzodiazepines and Opioids was discussed. The State noted to the board that the Mental Health Medication Advisory Committee is revising the criteria and will be sending it to the DUR board for review. Ms. Grant clarified that the dose limits are for all drugs listed on the chart and not just this added new drug.
A. Revised Prior Authorization (PA) Criteria
6. Berinert® (C1 esterase
Background Berinert is a protein C1 inhibitor indicated for the acute treatment of hereditary angioedema (HAE) attacks. Prior authorization criteria were last revised in January 2016. Since that time,
Dr. Mittal moved to approve as written.

October 12, 2016 DUR Meeting Minutes Page 8 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION inhibitor, human)
i. Revised PA Criteria it has become approved in pediatrics at least 6 years of age. The prior authorization criteria is being revised to include ages 6-12 years.
Public Comment None Board Discussion None
Ms. Dowd seconded the motion. The criteria were approved as written, unanimously.
A. Revised Prior Authorization (PA) Criteria
7. Xolair® (omalizumab) i. Revised PA Criteria
Background Xolair is a monoclonal antibody indicated for the treatment of persistent asthma and chronic idiopathic urticaria. Prior authorization criteria were last revised in October 2014. Since that time, it has become approved in pediatrics at least 6 years of age for the maintenance treatment of asthma. The prior authorization criteria is being revised to include ages 6-12 years for this indication.
Ms. Dowd moved to approve as written. Dr. Unruh seconded the motion. The criteria were approved as written, unanimously.

October 12, 2016 DUR Meeting Minutes Page 9 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
Public Comment None Board Discussion The Board received verification that the age change was only for Asthma.
A. Revised Prior Authorization (PA) Criteria
8. Tecfidera® (dimethyl fumarate)
i. Revised PA Criteria
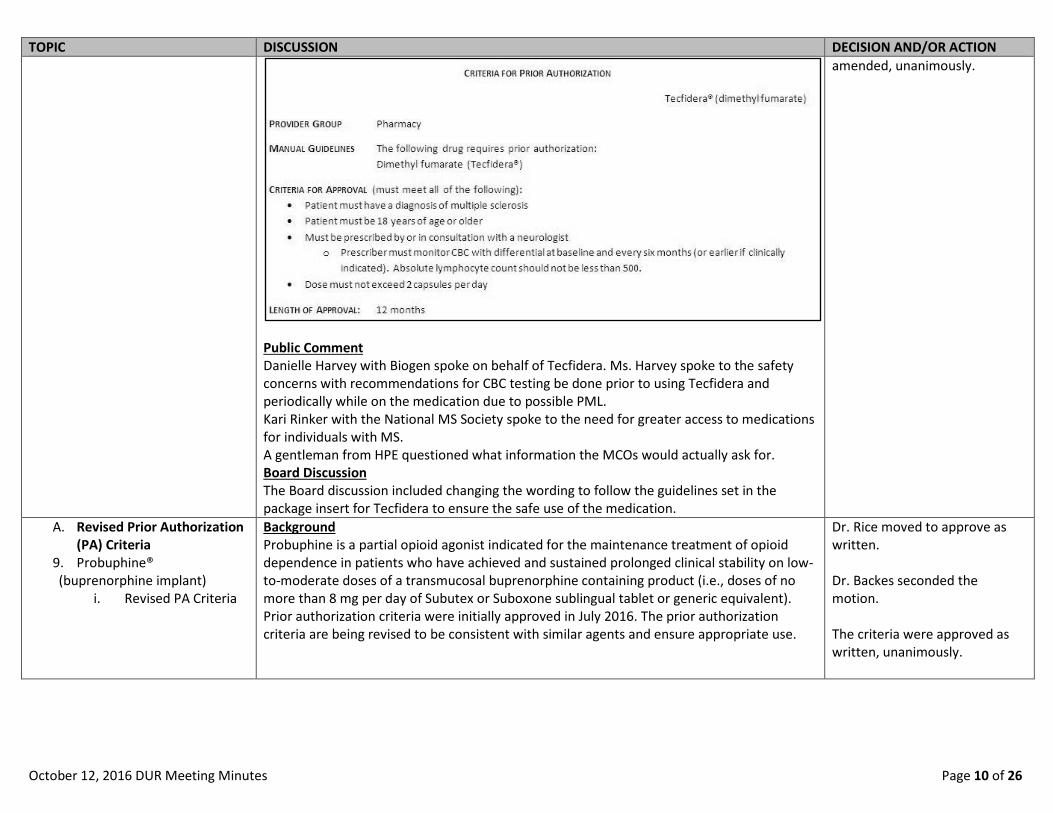
Background Tecfidera is an immunomodulator indicated for the treatment of relapsing forms of multiple sclerosis (MS). The prior authorization criteria is being revised to correct the dosing regimen.
Dr. Heston moved to approve as amended. Dr. Unruh seconded the motion. The criteria were approved as
October 12, 2016 DUR Meeting Minutes Page 10 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
Public Comment Danielle Harvey with Biogen spoke on behalf of Tecfidera. Ms. Harvey spoke to the safety concerns with recommendations for CBC testing be done prior to using Tecfidera and periodically while on the medication due to possible PML. Kari Rinker with the National MS Society spoke to the need for greater access to medications for individuals with MS. A gentleman from HPE questioned what information the MCOs would actually ask for. Board Discussion The Board discussion included changing the wording to follow the guidelines set in the package insert for Tecfidera to ensure the safe use of the medication.
amended, unanimously.
A. Revised Prior Authorization (PA) Criteria
9. Probuphine® (buprenorphine implant)
i. Revised PA Criteria
Background Probuphine is a partial opioid agonist indicated for the maintenance treatment of opioid dependence in patients who have achieved and sustained prolonged clinical stability on low-to-moderate doses of a transmucosal buprenorphine containing product (i.e., doses of no more than 8 mg per day of Subutex or Suboxone sublingual tablet or generic equivalent). Prior authorization criteria were initially approved in July 2016. The prior authorization criteria are being revised to be consistent with similar agents and ensure appropriate use.
Dr. Rice moved to approve as written. Dr. Backes seconded the motion. The criteria were approved as written, unanimously.

October 12, 2016 DUR Meeting Minutes Page 11 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
Public Comment None Board Discussion None
A. Revised Prior Authorization (PA) Criteria
10. Humira® (adalimumab) [Amjevita (adalimumab-atto)]
i. Revised PA Criteria
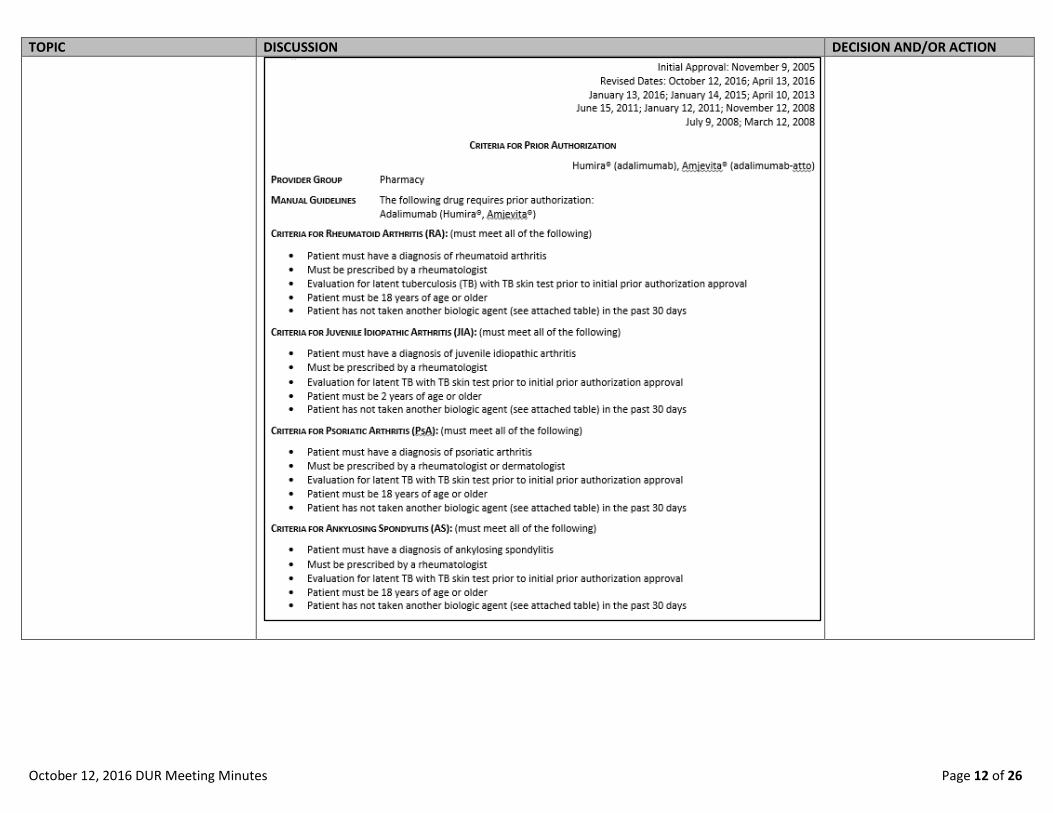
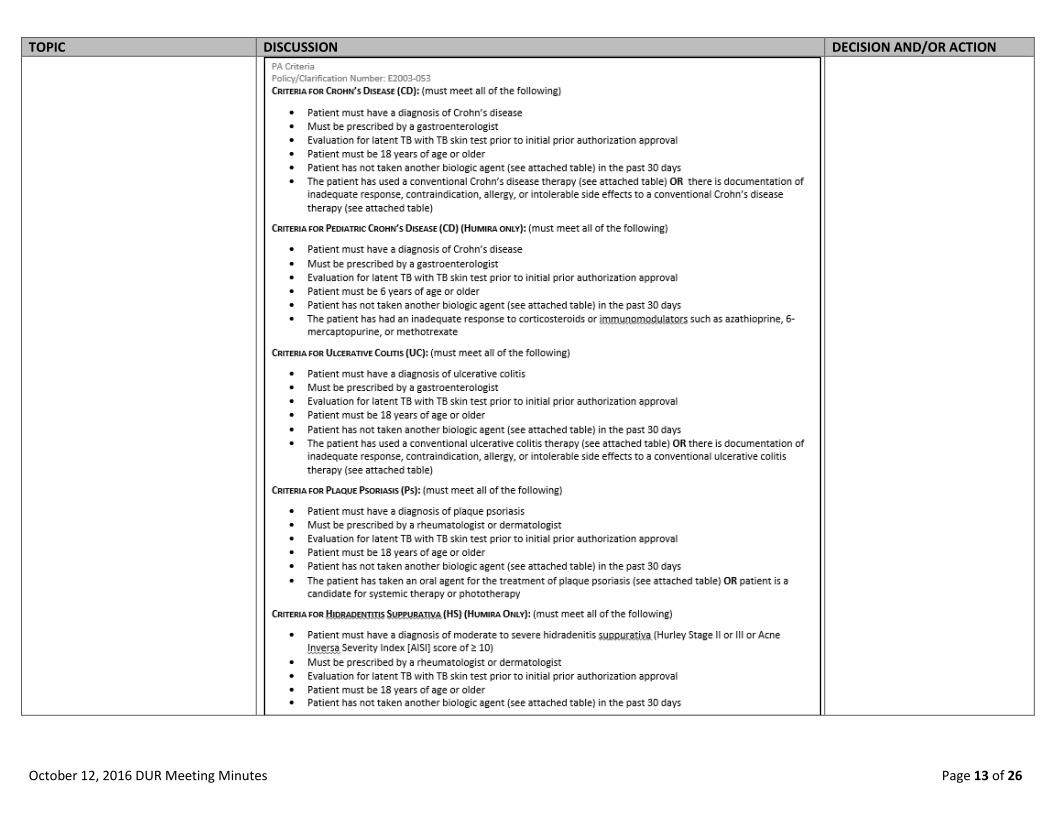
Background Humira is a biologic agent. Prior authorization criteria were last revised in April 2016. Since that time, Humira has become indicated for the treatment of non-infectious intermediate, posterior and panuveitis. The prior authorization criteria are being revised to be consistent with similar agents and ensure appropriate use. Since that time, a new agent has been approved. The prior authorization criteria is also being revised to include the new agent, Amjevita.
Ms. Dowd moved to approve as written. Dr. Unruh seconded the motion. The criteria were approved as written, unanimously.
October 12, 2016 DUR Meeting Minutes Page 12 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
October 12, 2016 DUR Meeting Minutes Page 13 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
October 12, 2016 DUR Meeting Minutes Page 14 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
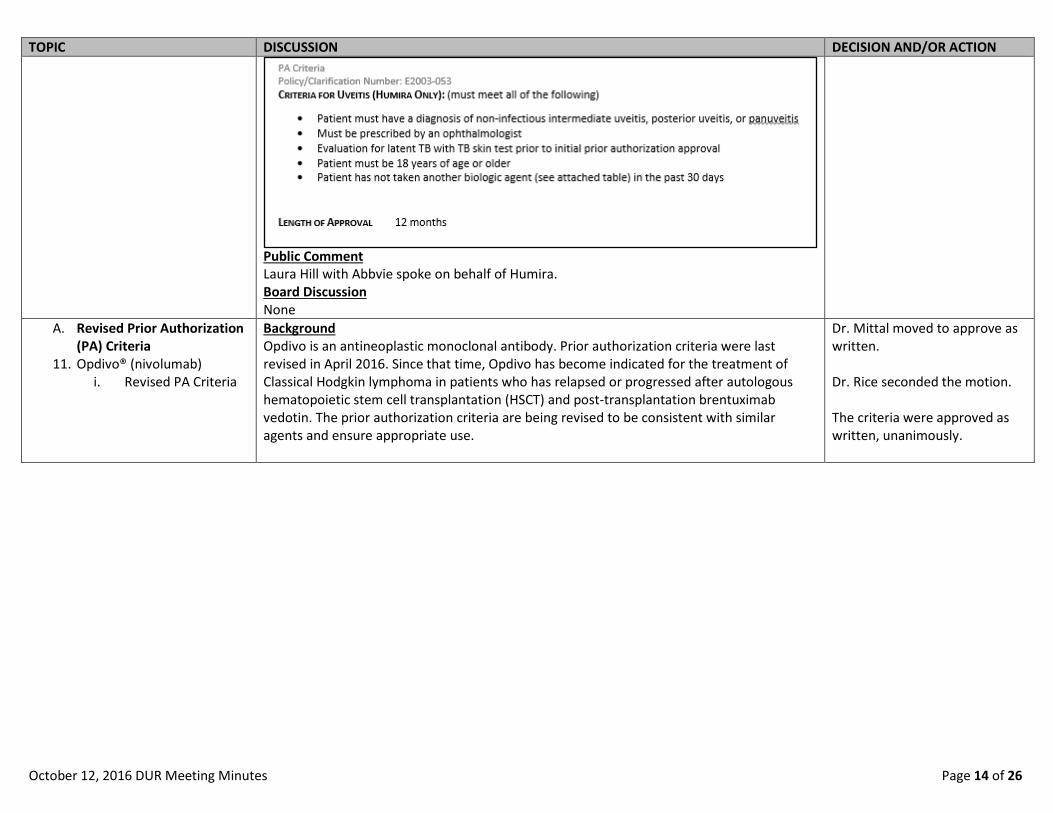
Public Comment Laura Hill with Abbvie spoke on behalf of Humira. Board Discussion None
A. Revised Prior Authorization (PA) Criteria
11. Opdivo® (nivolumab) i. Revised PA Criteria
Background Opdivo is an antineoplastic monoclonal antibody. Prior authorization criteria were last revised in April 2016. Since that time, Opdivo has become indicated for the treatment of Classical Hodgkin lymphoma in patients who has relapsed or progressed after autologous hematopoietic stem cell transplantation (HSCT) and post-transplantation brentuximab vedotin. The prior authorization criteria are being revised to be consistent with similar agents and ensure appropriate use.
Dr. Mittal moved to approve as written. Dr. Rice seconded the motion. The criteria were approved as written, unanimously.

October 12, 2016 DUR Meeting Minutes Page 15 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
Public Comment John Brokas with BMS spoke on behalf of Opdivo. Board Discussion None
A. Revised Prior Authorization (PA) Criteria
12. Botulinum Toxins (Dysport® [abobotulinumtoxinA], Botox® [onabotulinumtoxinA])
i. Revised PA Criteria
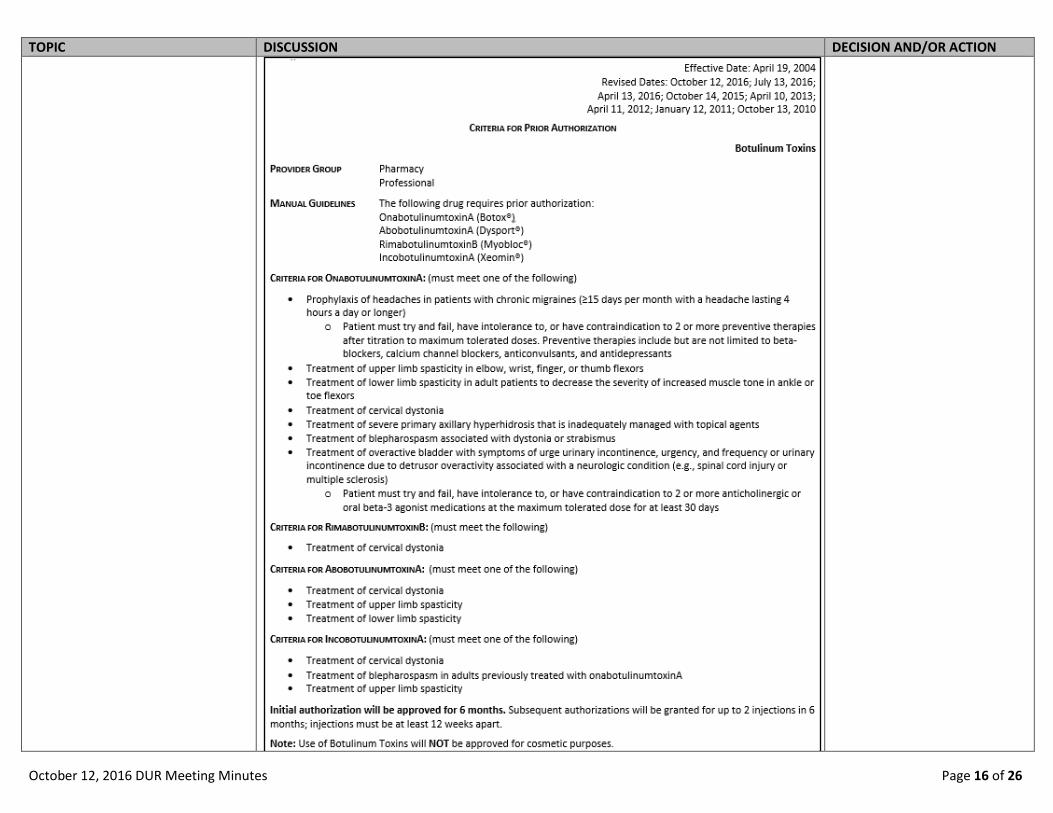
Background Dysport and Botox are botulinum toxins. Prior authorization criteria were last revised in July 2016. Since that time, Dysport has become indicated for the treatment of lower limb spasticity. Step therapy for Botox is being proposed for the indications of migraines and overactive bladder. The prior authorization criteria are being revised to be consistent with similar agents and ensure appropriate and cost-effective use.
Dr. Heston moved to approve as written. Dr. Unruh seconded the motion. The criteria were approved as written, unanimously.
October 12, 2016 DUR Meeting Minutes Page 16 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
October 12, 2016 DUR Meeting Minutes Page 17 of 26
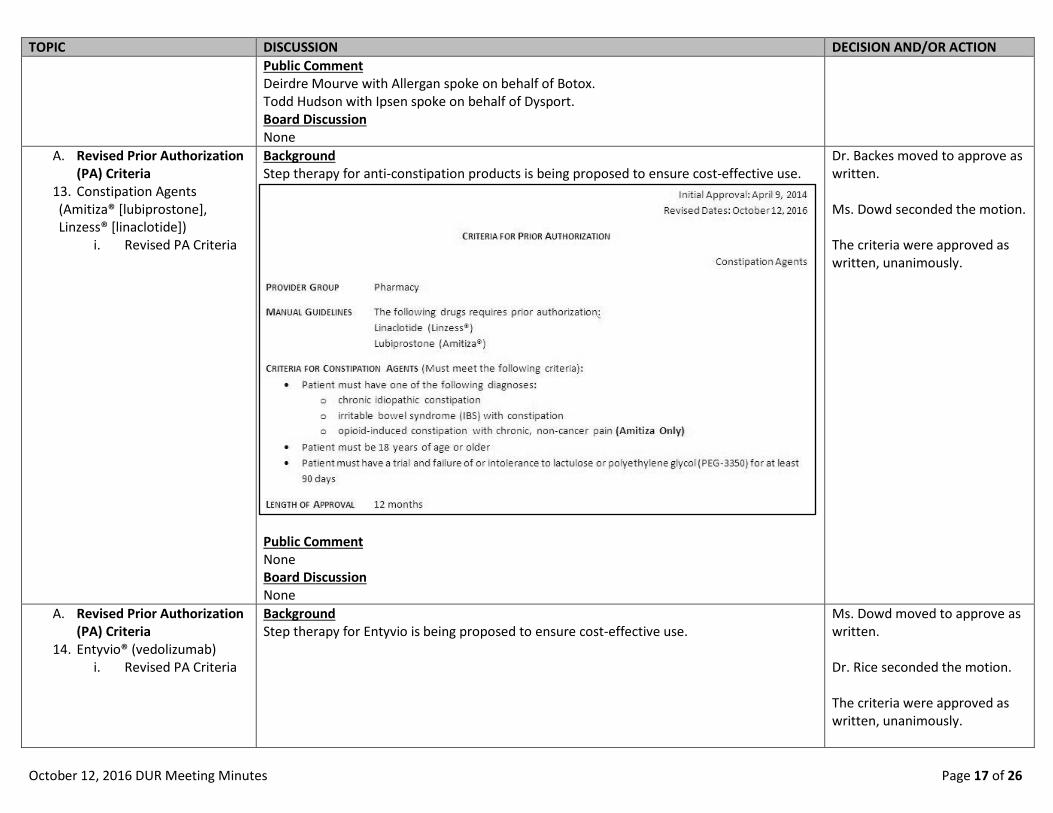
TOPIC DISCUSSION DECISION AND/OR ACTION Public Comment Deirdre Mourve with Allergan spoke on behalf of Botox. Todd Hudson with Ipsen spoke on behalf of Dysport. Board Discussion None
A. Revised Prior Authorization (PA) Criteria
13. Constipation Agents (Amitiza® [lubiprostone], Linzess® [linaclotide])
i. Revised PA Criteria
Background Step therapy for anti-constipation products is being proposed to ensure cost-effective use.
Public Comment None Board Discussion None
Dr. Backes moved to approve as written. Ms. Dowd seconded the motion. The criteria were approved as written, unanimously.
A. Revised Prior Authorization (PA) Criteria
14. Entyvio® (vedolizumab) i. Revised PA Criteria
Background Step therapy for Entyvio is being proposed to ensure cost-effective use.
Ms. Dowd moved to approve as written. Dr. Rice seconded the motion. The criteria were approved as written, unanimously.

October 12, 2016 DUR Meeting Minutes Page 18 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
Public Comment None Board Discussion None

October 12, 2016 DUR Meeting Minutes Page 19 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION A. Revised Prior Authorization
(PA) Criteria 15. Sodium-Glucose Co-Transporter 2 (SGLT2) Inhibitor Combinations (Invokamet® [Canagliflozin/metformin], Xigduo XR® [dapagliflozin/metformin], Glyxambi® [empagliflozin/linagliptin], Synjardy® [empagliflozin/ metformin])
i. Revised PA Criteria
Background Step therapy for Sodium-Glucose Co-Transporter 2 (SGLT2) Inhibitor combinations is being proposed to ensure cost-effective use.
Public Comment Julie McDavitt with Boehringer Ingelheim spoke on behalf of Glyxambi and Synjardy. Board Discussion None
Dr. Backes moved to approve as written. Dr. Mittal seconded the motion. The criteria were approved as written, unanimously.
B. New Prior Authorization (PA) Criteria
1. Beta-Blocker/Angiotensin II Receptor Blockers Combinations (Byvalson® [nebivolol/valsartan])
i. Prior Authorization Criteria
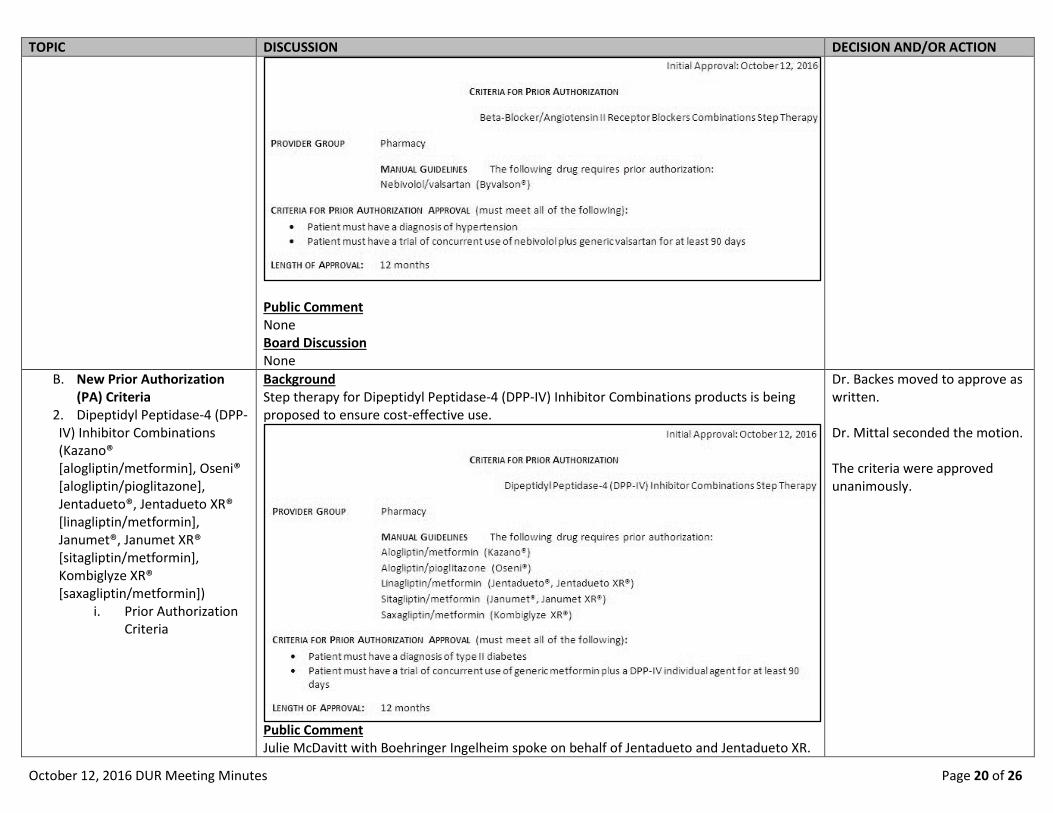
Background Step therapy for Beta-Blocker/Angiotensin II Receptor combination products is being proposed to ensure cost-effective use.
Ms. Dowd moved to approve as written. Dr. Unruh seconded the motion. The criteria were approved as written, unanimously.
October 12, 2016 DUR Meeting Minutes Page 20 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
Public Comment None Board Discussion None
B. New Prior Authorization (PA) Criteria
2. Dipeptidyl Peptidase-4 (DPP-IV) Inhibitor Combinations (Kazano® [alogliptin/metformin], Oseni® [alogliptin/pioglitazone], Jentadueto®, Jentadueto XR® [linagliptin/metformin], Janumet®, Janumet XR® [sitagliptin/metformin], Kombiglyze XR® [saxagliptin/metformin])
i. Prior Authorization Criteria
Background Step therapy for Dipeptidyl Peptidase-4 (DPP-IV) Inhibitor Combinations products is being proposed to ensure cost-effective use.
Public Comment Julie McDavitt with Boehringer Ingelheim spoke on behalf of Jentadueto and Jentadueto XR.
Dr. Backes moved to approve as written. Dr. Mittal seconded the motion. The criteria were approved unanimously.

October 12, 2016 DUR Meeting Minutes Page 21 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION Board Discussion None
B. New Prior Authorization (PA) Criteria
3. Intranasal Antihistamine/Corticosteroid Agents (Dymista® [Azelastine/fluticasone])
i. Prior Authorization Criteria
Background Step therapy for intranasal antihistamine/corticosteroid products is being proposed to ensure cost-effective use.
Public Comment None Board Discussion None
Dr. Mittal moved to approve as written. Dr. Backes seconded the motion. The criteria were approved as written, unanimously.
B. New Prior Authorization (PA) Criteria
4. NSAID plus PPI/H2 Blocking Agents (Duexis® [ibuprofen/famotidine], Vimovo® [naproxen/esomeprazole])
i. Prior Authorization Criteria
Background Step therapy for NSAID plus PPI/H2 blocking agents is being proposed to ensure cost-effective use.
Dr. Mittal moved to approve as written. Dr. Unruh seconded the motion. The criteria were approved as written, unanimously.

October 12, 2016 DUR Meeting Minutes Page 22 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
Public Comment None Board Discussion None
B. New Prior Authorization (PA) Criteria
5. Adlyxin® (lixisenatide) i. Prior Authorization
Criteria
Background Adlyxin is a Glucagon-Like Peptide 1 (GLP-1) Receptor Agonist indicated for the treatment of type 2 diabetes mellitus (noninsulin dependent, NIDDM) to improve glycemic control in adult patients as an adjunct to diet and exercise. Prior authorization criteria is being proposed to ensure appropriate use based upon the FDA-approved labeling information and to remain consistent with other agents used for the approved indication.
Ms. Dowd moved to approve as written. Dr. Mittal seconded the motion. The criteria were approved as written, unanimously.

October 12, 2016 DUR Meeting Minutes Page 23 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
Public Comment None Board Discussion None
B. New Prior Authorization (PA) Criteria
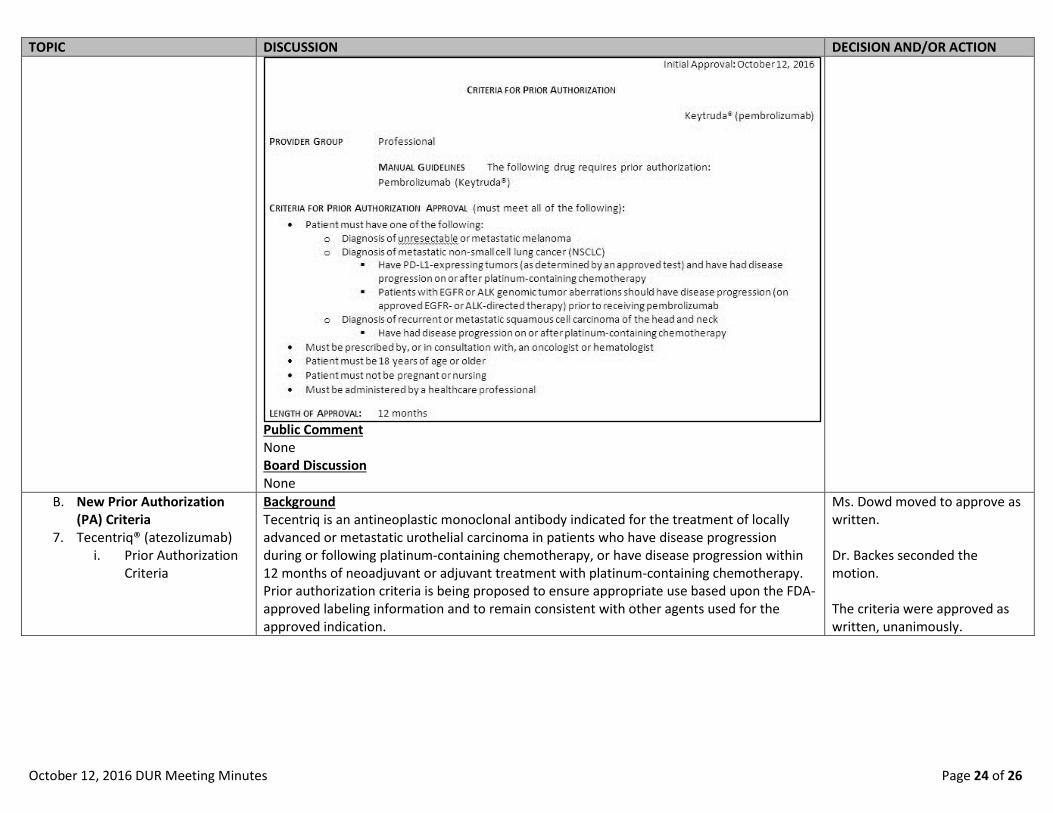
6. Keytruda® (pembrolizumab) i. Prior Authorization
Criteria
Background Keytruda is an immunomodulator indicated for the treatment of unresectable or metastatic melanoma, metastatic non-small cell lung cancer (NSCLC), and recurrent or metastatic squamous cell carcinoma of the head and neck. Prior authorization criteria is being proposed to ensure appropriate use based upon the FDA-approved labeling information and to remain consistent with other agents used for the approved indication.
Dr. Mittal moved to approve as written. Dr. Heston seconded the motion. The criteria were approved as written, unanimously.
October 12, 2016 DUR Meeting Minutes Page 24 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
Public Comment None Board Discussion None
B. New Prior Authorization (PA) Criteria
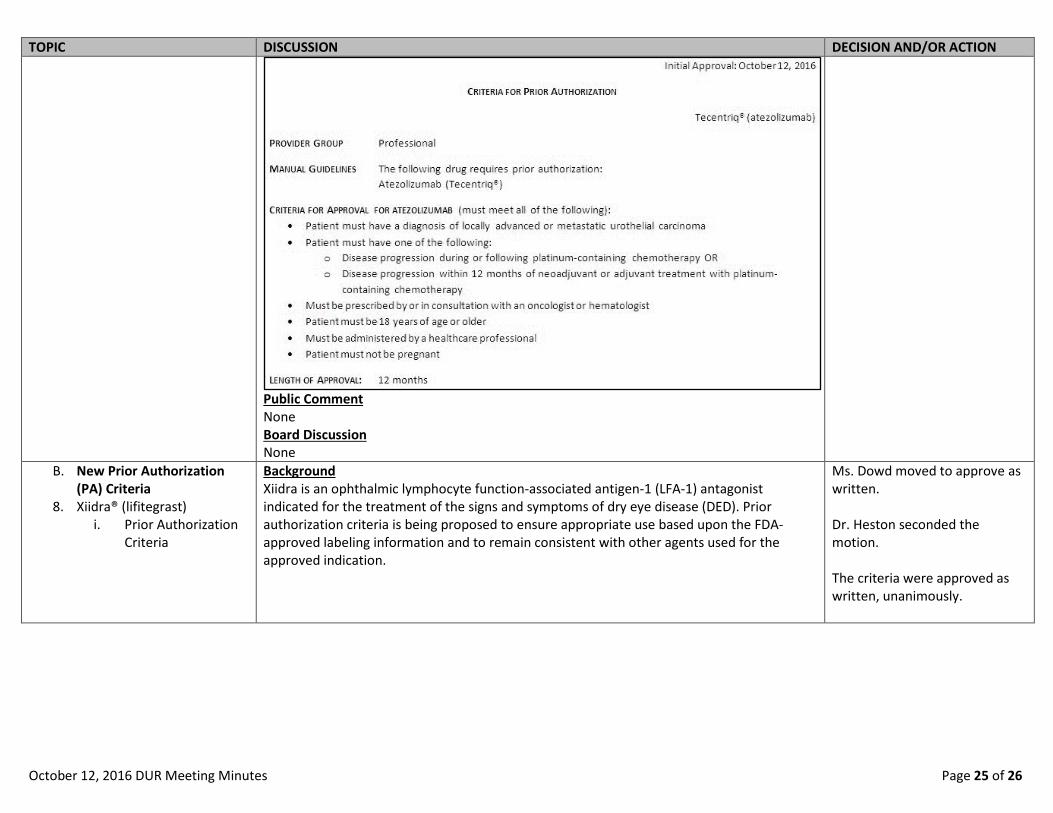
7. Tecentriq® (atezolizumab) i. Prior Authorization
Criteria
Background Tecentriq is an antineoplastic monoclonal antibody indicated for the treatment of locally advanced or metastatic urothelial carcinoma in patients who have disease progression during or following platinum-containing chemotherapy, or have disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy. Prior authorization criteria is being proposed to ensure appropriate use based upon the FDA-approved labeling information and to remain consistent with other agents used for the approved indication.
Ms. Dowd moved to approve as written. Dr. Backes seconded the motion. The criteria were approved as written, unanimously.
October 12, 2016 DUR Meeting Minutes Page 25 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
Public Comment None Board Discussion None
B. New Prior Authorization (PA) Criteria
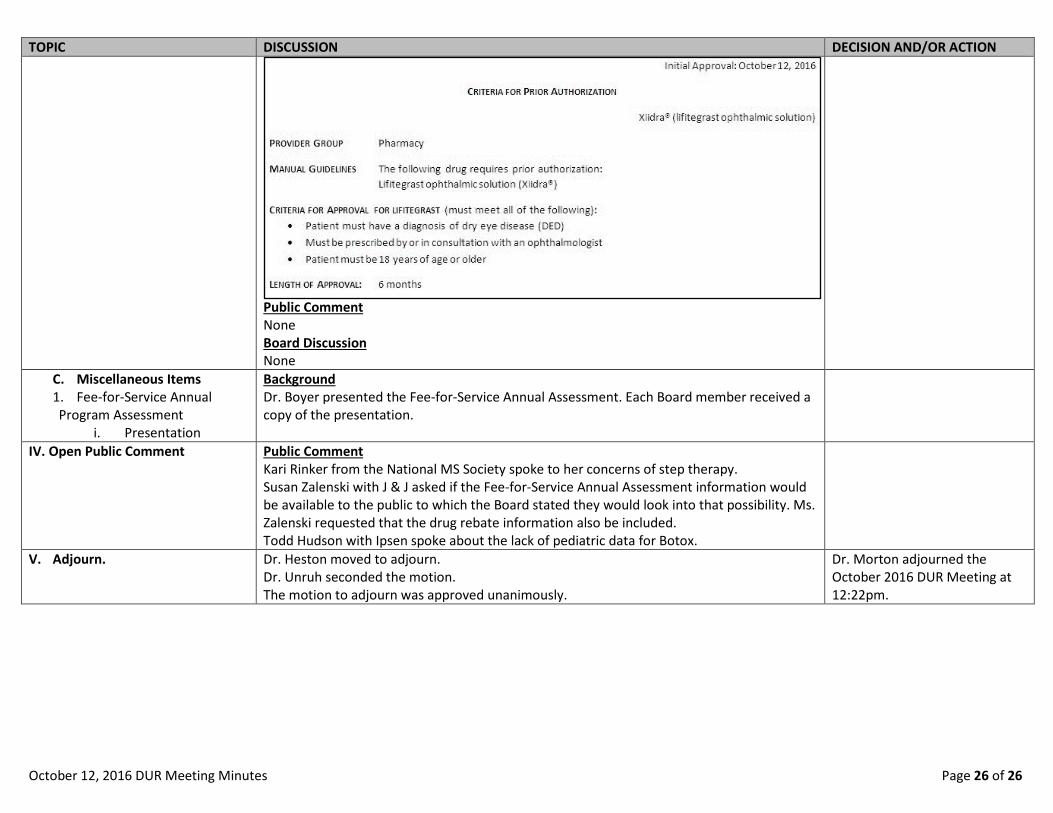
8. Xiidra® (lifitegrast) i. Prior Authorization
Criteria
Background Xiidra is an ophthalmic lymphocyte function-associated antigen-1 (LFA-1) antagonist indicated for the treatment of the signs and symptoms of dry eye disease (DED). Prior authorization criteria is being proposed to ensure appropriate use based upon the FDA-approved labeling information and to remain consistent with other agents used for the approved indication.
Ms. Dowd moved to approve as written. Dr. Heston seconded the motion. The criteria were approved as written, unanimously.
October 12, 2016 DUR Meeting Minutes Page 26 of 26
TOPIC DISCUSSION DECISION AND/OR ACTION
Public Comment None Board Discussion None
C. Miscellaneous Items 1. Fee-for-Service Annual Program Assessment
i. Presentation
Background Dr. Boyer presented the Fee-for-Service Annual Assessment. Each Board member received a copy of the presentation.
IV. Open Public Comment Public Comment Kari Rinker from the National MS Society spoke to her concerns of step therapy. Susan Zalenski with J & J asked if the Fee-for-Service Annual Assessment information would be available to the public to which the Board stated they would look into that possibility. Ms. Zalenski requested that the drug rebate information also be included. Todd Hudson with Ipsen spoke about the lack of pediatric data for Botox.
V. Adjourn. Dr. Heston moved to adjourn. Dr. Unruh seconded the motion. The motion to adjourn was approved unanimously.
Dr. Morton adjourned the October 2016 DUR Meeting at 12:22pm.







![DURONIA Observatoryroma2.rm.ingv.it/.../Bulletins/DUR/2016/November.pdf · November 2016 Edited by: Macera L., Santarelli L. 0 3 6 9 12 15 18 21 24-20 0 20 40 H[nT] Date: 01-11-2016](https://img.pdfslide.us/doc/110x75/5f1c4ef855195400e7382b9f/duronia-november-2016-edited-by-macera-l-santarelli-l-0-3-6-9-12-15-18-21-24-20.jpg)





















