Embed Size (px)
Citation preview
POINTS OF INTEREST . . . . . . . . . . . . . . . . . . . . . .
New coding changes on page 2.
Key changes to RVU
of codes prompts new Medicare fee schedule on page 3.
Virtual AuthTech®
program enhance-ments. See page 4.
Assistant surgery
claims need documen-tation to show medical necessity. See page 4.
OIG focusing on
potential fraud for eye care services on page 5.
Concurrent care
billing may not be recognized by adjudication system. Details on page 6.
VE RSN code reviews
IMRT planning and simulation being billed together or separate on page 7.
Quest Diagnostics
settles False Claims Act on page-8.
NY physician to serve 2
years for unsupervised PA, See page 9.
VOLUME 7, ISSUE 4 October 2015
OCTOBER 1, 2015 ICD-10-CM IMPLEMENTATION ICD-10-CM is now a coding reality and we hope that the transition is going smoothly for your organization. Virtual Examiner® has been updated and the update has been applied to your VE modules by the PCG staff As members of the PCG team were completing the AAPC ICD-10-CM training, one of the most important coding recommendations was to read the information and guidance in the ICD-10-CM manual. While many of the coding concepts are brought forward from ICD-9-CM, each chapter has new information and the guidance within the manual is critical to meet the 7th digit and other coding criteria. A complete list of the 2016 ICD-10-CM valid codes and code titles is posted on the CMS website at http://www.cms.gov/Medicare/Coding/ICD10/2016-ICD-10-CM-and-GEMs.html. The codes are listed in tabular order which corresponds with the manual. Mental Health providers will be basing their diagnoses on DSM-5 after October 1, 2015. DSM-5 contains all the standard criteria for the identification of psychiatric disorders along with both ICD-9-CM and ICD-10-CM. The previously used DSM-IV only has the ICD-9-CM and will not be used after September 30, 2015. The American Psychiatric Association (APA) maintains the DSM-5 criteria and the related ICD-10-CM codes. The DSM-5 can be found online at: www.dsm5.org The website is a valuable resource on both the coding and criteria for psychiatric conditions. On September 22, 2015, CMS updated the Clarifying Questions and Answers Related to the July 6, 2015 CMS/AMA Joint Announcement and Guidance Regarding ICD-10 Flexibilities and included information about Medicare Advantage plans.
proceedings, and Medicare coverage guidance documents. The website is accessible via Virtual AuthTech® main menu or it can be reviewed with Internet Explorer at: https://www.cms.gov/medicare-coverage-database/
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2015 AND 2016 CODING CHANGES AMA CPT®
As we start preparing for 2016, the AMA announced that there are 140 additional new codes, 134 code revisions and 92 deleted CPT® codes. PCG staff will be attending the AMA 2016 Symposium in Chicago in November and we will begin updating the Virtual Examiner® suite. Other code sets that are released by CMS, including the HCPCs, will not be released until December. PLACE OF SERVICE CODES
A new Place of Service (POS) Code 19 has been added to the data set with an effective date of January 1, 2016. The new POS, named Off Campus—Outpatient Hospital, was added to meet the needs of current practice and is described as: “A portion of an off-campus hospital provider based department which provides diagnostic, therapeutic (both surgical and nonsurgical), and rehabilitation services to sick or injured persons who do not require hospitalization or institutionalization. (Effective January 1, 2016)”
Page 2
Question 14: (new 09/22/2015) Do the Medicare fee-for-service audit and quality program flexibilities apply to Medicare Advantage? Answer 14: No, the Guidance applies only to Medicare fee-for-service claims from physicians or other practitioners billed under the Medicare Fee-for-Service Part B physician fee schedule. Medicare Advantage risk adjustment payment and audit criteria remain unchanged.
The entire Question and Answers related to the CMS/AMA Joint Announcement can be reviewed at: https://www.cms.gov/Medicare/Coding/ICD10/Clarifying-Questions-and-Answers-Related-to-the-July-6-2015-CMS-AMA-Joint-Announcement.pdf Along with the challenges of implementing payment policies and making the correct determinations using ICD-10-CM, National and Local Coverage Determinations have been issued with the new diagnosis codes. The website is user friendly and worth using to assist your staff. The Medicare Coverage Database (MCD) contains all National Coverage Deter-minations (NCDs) and Local Coverage Determinations (LCDs), local articles, and proposed NCD decisions. The database also includes several other types of National Coverage policy related documents, including National Coverage Analyses (NCAs), Coding Analyses for Labs (CALs), Medicare Evidence Development & Coverage Advisory Committee (MEDCAC)
adjudication system as in most instances, the RVUs changed. The MPFSDB was revised September 30, 2015 to reflect the revised CR9266 issued on September 29. Additional codes (G0105 and G0121) are added in the “What You Need to Know” section listing RVU changes. Also, a number of codes with a revised bilateral surgery indicator are listed in that same section. The CR release date, transmittal number, and the Web address for CR9266 are also revised. Changes included in the October update to the 2015 MPFSDB are effective for dates of service on and after January 1 (unless otherwise stated). The key change is to the Malpractice Relative Value Units (RVU) of the following CPT/HCPCS codes: 33471, 33606, 33611, 33619, 33676, 33677, 33692, 33737, 33755, 33762, 33764, 33768, 33770, 33771, 33775, 33776, 33777, 33778, 33779, 33780, 33781, 33783, 33786, 33803, 33813, 33822, 33840, and 33851; and the Work RVUs for G0105 and G0121. The RVU changes for these codes are retroactive to January 1, 2015. In addition, effective January 1, 2015, codes 76641, 76641-TC, 76641-26, 76642, 76642-TC, 76642-26, 95866, 95866-TC, and 95866-26 have a revised bilateral surgery indicator = 3. Also, effective October 1, 2015, CPT/HCPCS code Q9979 is assigned a procedure status indicator of E (Excluded from the PFS by regulation. These codes are for items and services that CMS has excluded from the PFS by regulation. No payment may be made under the PFS for
Page 3
With the addition of the POS 19, the current outpatient POS 22 was revised with a change to the POS name and description. The new name is On Campus—Outpatient Hospital with the following description: “A portion of a hospital’s main campus which provides diagnostic, therapeutic (both surgical and nonsurgical), and rehabilitation services to sick or injured persons who do not require hospitalization or institutionalization. (Description change effective January 1, 2016)”
With the number of Evaluation and Management services for POS 11 decreasing, and a greatly increasing number of E/M services in POS 22, CMS is correct in addressing this financial issue. Facility based services are more costly than office (non-facility) services The new POS data set was updated on August 6, 2015, and can be downloaded at:
https://www.cms.gov/Medicare/Coding/place-of-service-codes/
Place_of_Service_Code_Set.html
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CMS 4TH QUARTER 2015 (21.3) RELEASE NOTES MPFSDB—What You Need to Know
There were some last minute changes to the Medicare Physician Fee Schedule Data Base (MPFSDB) that became effective on October 5, 2015. Please evaluate whether these changes were added to your
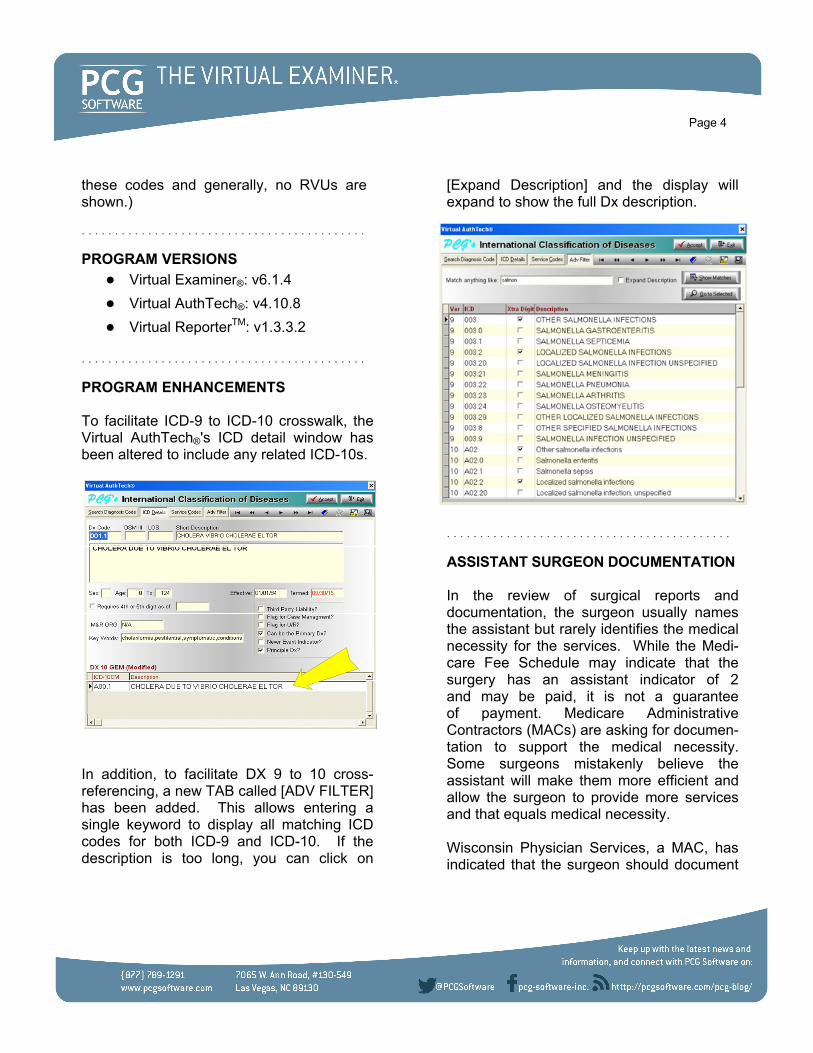
[Expand Description] and the display will expand to show the full Dx description.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
ASSISTANT SURGEON DOCUMENTATION In the review of surgical reports and documentation, the surgeon usually names the assistant but rarely identifies the medical necessity for the services. While the Medi-care Fee Schedule may indicate that the surgery has an assistant indicator of 2 and may be paid, it is not a guarantee of payment. Medicare Administrative Contractors (MACs) are asking for documen-tation to support the medical necessity. Some surgeons mistakenly believe the assistant will make them more efficient and allow the surgeon to provide more services and that equals medical necessity. Wisconsin Physician Services, a MAC, has indicated that the surgeon should document
Page 4
these codes and generally, no RVUs are shown.)
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
PROGRAM VERSIONS
Virtual Examiner®: v6.1.4
Virtual AuthTech®: v4.10.8
Virtual ReporterTM: v1.3.3.2
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
PROGRAM ENHANCEMENTS To facilitate ICD-9 to ICD-10 crosswalk, the Virtual AuthTech®'s ICD detail window has been altered to include any related ICD-10s.
In addition, to facilitate DX 9 to 10 cross-referencing, a new TAB called [ADV FILTER] has been added. This allows entering a single keyword to display all matching ICD codes for both ICD-9 and ICD-10. If the description is too long, you can click on

degeneration diagnoses. The first question in the summary of the OIG report is – Why We Did This Study. “In 2012, Medicare paid $6.7 billion to 44,960 providers for ophthal-mology services that screen for, diagnose, evaluate, or treat two prominent eye conditions: wet age related macular degeneration (wet AMD) and cataracts.” Since 2010, OIG has investigated over 100 providers of ophthalmology services for fraud. What is not surprising is that the OIG found that “4 percent of providers billing Medicare for ophthalmology services demonstrated at least one of our nine measures of questionable billing. Overall, Medicare paid these 1,726 providers $768 million for ophthalmology services in 2012, of which $171 million was for services associated with the measures on which these providers demonstrated questionable billing.” In addition, there were trends of bad billing centered around specific metropolitan areas and provider issues. “Medicare also paid $2 million for ophthalmology services to 821 providers that were not listed as eye care specialists in CMS databases.” What is particularly helpful is that this study lists in Table 3 the categories and measures of questionable billing for AMD and Cataracts. This is a valuable resource for initiating a study to evaluate any current ophthalmology trends in abusive billing within your provider network. The full OIG Report is available at: http://oig.hhs.gov/oei/reports/oei-04-12-00281.pdf.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Page 5
the medical necessity of the assistant surgeon and what part of the surgery the assistant supported. The WPS documenta-tion guideline states: “A frequent question Medicare receives is whether or not an assistant surgeon must sign the operative report. The answer is no. The primary surgeon must document, with specificity, the activities the assistant surgeon performed and that the additional 'skilled' operative assistance was needed to perform a medically necessary and other-wise covered Medicare service. The primary surgeon must authenticate his/her entry in the medical record, but the assistant surgeon need not sign the operative report. Providers need to be cognizant that a non-restrictive assistant surgery payment indicator on the Medicare Physician Fee Schedule Database does not alone determine that Medicare will approve payment for an assistant at surgery service.”
For most payers the assistant surgeon is paid at least 16% of the primary surgeon’s fee. All assistant services provided to members should be medically necessary. http://www.wpsmedicare.com/j5macpartb/departments/cert/documentation-assistant-surgery-services.shtml
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
MEDICARE PAID $6.7 BILLION FOR SERVICES TO SCREEN AND TREAT—CATARACTS AND AMD A new OIG report focuses on areas of potential fraud for eye care services to treat cataract and age-related macular
The billing of concurrent care is an area of financial concern as multiple billings within the same vendor grouping may not be recognized by the adjudication system. VE's RSN code 250 will identify multiple E&Ms on the same day for a group. Concurrent care is fully discussed in both the CMS Medicare Policy and Claims Processing Manuals as noted below: https://www.cms.gov/Regulations-and-guidance/Guidance/Manuals/downloads/bp102c15.pdf https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
INTENSITY MODULATED RADIATION THERAPY—IMRT Intensity-modulated radiation therapy (IMRT) is an advanced mode of high-precision radio-therapy that uses computer-controlled linear accelerators to deliver precise radiation doses to a malignant tumor or specific areas within the tumor. The precise delivery of the radiation spares the normal tissue and focuses the treatment on the tumor. IMRT planning is a computer-based method-ology for developing the treatment program. Before planning treatment, a physical examination and medical history review are conducted. Next, there is a treatment simulation session, which includes CT scanning, from which the radiation oncologist specifies the three-dimensional shape of the tumor and normal tissues. In most cases, a
Page 6
MULTIPLE EVALUATION AND MANAGEMENT CHARGES ON THE SAME DATE OF SERVICE “Concurrent care” exists when services are performed by more than one physician or nonphysician practitioner (NPP) during a period of time for the same patient. Most commonly, concurrent care occurs when the same patient is seen by multiple providers of the same or similar specialties for the same diagnosis. The reasonable and necessary services of each physician/NPP rendering concurrent care may be covered if the medical record substantiates the necessity for that provider to provide care. Each provider must supply knowledge or services that are not able to be provided by the attending physician. Of important consideration is the coding guidelines from both CMS and the AMA that physician assistants and advance practice nurses working with physicians are considered to be of the same specialty as the physician.
When more than one E/M service is provided to the same patient on the same date by more than one physician/NPP in the same specialty in the same group, only one E/M service may be reported unless the E/M services are for unrelated problems.
Physicians/NPPs in the same group practice who are in the same specialty must bill and be paid as though the services were provided by a single physician.
development of the IMRT plan. See reported code."
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
DRUG OVERPAYMENTS A recent OIG Report – “Medicare Part B Overpaid Millions on Selected Outpatient Drugs” is a testament to either the incompe-tence or the greed of many providers. Medicare incorrectly paid $36 million out of a total net payment of $131 million between 2009 and 2012. The errors are primarily caused by either reporting the incorrect number of units or selection of the wrong J code. CMS will be reviewing claims for the follow-ing drugs back to 2009 with recoveries as a focus:
J0150 Adenosine for therapeutic use, 6 mg (deleted 2014)
J0151 Adenosine for diagnostic use, 1mg (deleted 2014)
J0152 Adenosine, 30 mg (deleted 2014)
J1745 Injection infliximab, 10 mg
J9310 Injection rituximab, 100 mg
J9041 Injection bortezomib, 0.1 mg
J9217 Leuprolide acetate (for depot suspension), 7.5 mg
Evaluation of the correct billing and payment for these high dollar drug therapies will be enhanced with the soon to be developed Medically Unlikely Edits for the drugs. The MUEs will be for date of service instead of line item level as providers have been billing
Page 7
treatment preparation session may be necessary to mold a special device that will help the patient maintain an exact position. The Medicare Administrative Contractors and the HHS Inspector General have been reviewing records and claims data to deter-mine whether the IMRT and simulations have been billed separately, whether it is a single day, week or month prior to the treat-ment. In previous years, simulations were separately billable, but the AMA changed the planning codes to include the simulations. The NCCI edits introduced in January 2014, ended the billing of simulations when there is IMRT planning. The NCCI edit does not allow the IMRT planning code (77301) to be billed with 77280-77295. In all the column 1 and column 2 codes edits, we are usually reviewing the claim data for the procedure performed on the same date of service. Since the IMRT planning and simulation, along with the other edits, are not usually performed on the same date of service, this scenario has proven to be an operational nightmare for provider and hospital billers. If all the planning and simulation codes were billed on the same date of service, the APC calculation would include all the services and the simulations would not be reimbursed. Within Virtual Examiner®, RSN Code 12 has been revised to review for the Column 2 codes for simulation services whether they were billed on the same date as the IMRT planning or on another date of service. The new CCI RSN Code 12 message will read: "Standards of medical/surgical practice: Comprehensive procedure includes all simulation services performed in the

physician and or therapists, and treatment plans associated with the necessary 30 day certifications. While most Medical Management depart-ments have moved away from the prior authorization of the therapies, a review of the treatment plans and adherence to the plan and the associated claims is a worthwhile endeavor. The AgeWell practice was over-paid $1.4 million. There are multiple releases from the OIG on this case: http://oig.hhs.gov/oas/reports/region2/21301031.asp http://oig.hhs.gov/oas/reports/region2/21301031.pdf
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
QUEST DIAGNOSTICS TO PAY $1.79 MILLION TO SETTLE FRAUD CLAIMS ACT LAWSUIT The US Attorney’s Office for the Eastern District of California has reached a settle-ment in the latest suit against Quest Diagnostics. According to the details of the settlement, Quest Diagnostics is alleged to have ordered and performed duplicative services including venipunctures, upcoded certain tests, unbundled panel tests and some components of the panels, and over-billed the government for its services. The alleged misconduct spanned a period of at least ten years, ranging from 2004 through 2014. During the investigation, Quest was accused of trying to cover up the duplicate
Page 8
the drugs with the incorrect units over multiple lines to increase revenue. In the meantime, all contracts should require the billing of the J code with a corresponding NDC code. Examiners can consult the NDC to J code crosswalk to validate that the J code billed is for the correct drug and dosage. The crosswalk is resident in Virtual AuthTech® under the Codes menu. As of May 4, 2015, Medicare contractors had recovered 63 percent of the $35.8 million in overpayments, and 10 of the 13 Medicare contractors had used the results of the OIG audits in ongoing provider education activities. The full OIG report “Medicare Part B Over-paid Millions on Selected Outpatient Drugs” is interesting reading and provides the basis for an internal audit: http://oig.hhs.gov/oas/reports/region9/91402024.asp. RadiologyInfo.org has a valuable layperson description of the IMRT services at: http://www.radiologyinfo.org/en/info.cfm?pg=imrt.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
PHYSICAL THERAPY CLAIMS STILL AN OIG CONCERN Medicare, Medicaid and most commercial plans have physical therapy benefits. The OIG recently audited a physical therapy practice, AgeWell Physical Therapy and Wellness, PC. Out of the 100 claims selected for the audit, only 38 were correctly billed. The error rate was 62%. The audit was a medical record based review for compliance with the requirement of treatment plan matching the provided services, signatures by the attending

press release outlined the case against NewYork physician, Dr. Okon Umana. Okon Umana, 68, of West Haven, Connecticut, pleaded guilty on Dec. 1, 2014, to conspiracy to commit health care fraud. In addition to imposing the prison term, U.S. District Judge John Gleeson of the Eastern District of New York ordered Umana to pay $6,429,330 in restitution and to forfeit $6,550,036. Eight other individuals charged in connection with the scheme previously pleaded guilty. To date, one other individual has been sentenced. From 2009 to 2012, Umana was the medical director of Cropsey Medical Care PLLC (Cropsey), a health care clinic. In connection with his guilty plea, Umana admitted that many of Cropsey’s medical services were provided by a physician’s assistant who was acting without supervision by a medical doctor, and that Cropsey nevertheless billed Medicare and Medicaid for the services using Umana’s provider number. In addition, Umana admitted that in seeking reimburse-ment for costs purportedly incurred transporting certain beneficiaries to and from Cropsey by ambulette , he falsely certified that transportation by ambulette was medically necessary. The full press release can be downloaded at: http://www.justice.gov/opa/pr/doctor-brooklyn-new-york-clinic-sentenced-two-years-prison-engaging-13-million-health-care
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Page 9
claims and reported that the problem was due to a technology glitch. A former Quest Diagnostics employee, Elisa Martinez, who worked as a phlebotomist, first brought the case to light. She will receive $358,000 as her qui tam reward. Compared to what Quest Diagnostics receives in payments from commercial, federal and state payers, the settlement is a drop in the bucket and perhaps the cost of doing business. The settlement between Quest and the government in 2009 was not so paltry. In that case, Quest agreed to pay $302 million to settle claims it knowingly used defective diagnostic equipment to report patient blood draws and diagnostic tests. When performing compliance audits, review-ing which of your contracted providers are accused and settling with the Attorney General offices, is an appropriate method of selecting an audit focus. If your organization would like to profile specific providers or specialties please call our offices for additional information and assistance.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
NY PHYSICIAN TO SERVE 2 YEARS FOR UNSUPERVISED PHYSICIAN ASSISTANT PCG staff previously reviewed a series of medical records for a Physician Assistant providing oncology and chemotherapy services to patients. The problem identified was that the supervising physician was only available by phone and he was halfway around the world. In an unrelated case, the DOJ Office of Public Affairs, August 15, 2014

the Medicaid program through its managed care organizations. Following his prison term, Badawy will serve 3 years of super-vised release, will pay a fine of $5,000, and will pay restitution of nearly $200,000.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
NEW PCG POLICIES AND PROCEDURES
Policy 278-Medicaid Correct Payment Guidelines (released August 2015)
Policy 281—Executive Summary of an Audit Report
Policy VE 0250—Provider Qualifiers—Ordering, Referring and Supervising
Policy VE 0251—2% Payment Reduction Under Sequestration
HUDSON COUNTY, N.J. PEDIATRICIAN CHARGED WITH FRAUDULENTLY BILLING MEDICAID FOR NEARLY $1 MILLION Badawy M. Badawy, M.D., 50, of Bayonne, N.J., a licensed pediatrician who owns and operates Sinai Medical Center of Jersey City LLC, a medical practice focusing primarily on pediatrics and family medicine, billed Medi-caid thousands of times for nearly $900,000 worth of wound repairs on children and adolescents. Dr. Badawy pleaded guilty to health care fraud. The Department of Justice press release outlined Dr. Badawy’s fraud. “His claims for these supposed treatments represented a strong majority of all such claims submitted to Medicaid by all New Jersey medical providers during this time period, including 99.4 percent of all claims for the suturing or stapling of facial wounds larger than 30 centimeters. Virtually all of these claims, which were submitted for supposed wound repairs on children, were fraudulent. Badawy’s patient charts for a large sample of these children who supposedly received treatment revealed no entry, notation, or other evidence, such as suturing or other closing methods, to support his claims that these procedures were actually performed.” Dr. Badawy was recently sentenced to 21 months in prison for fraudulently billing
Page 10