Embed Size (px)
Citation preview

Occupational and Environmental Medicine 1994;51:631-637
Occupational exposure to hydrocarbons andchronic pancreatitis: a case-referent study
R McNamee, J M Braganza, J Hogg, I Leck, P Rose, N M Cherry
AbstractObjectives-To investigate the hypothesisthat hydrocarbon exposure is a risk fac-tor for chronic pancreatitis.Methods-102 cases of chronic pancreati-tis and 204 age and sex matched referentswere interviewed about their occupa-tional histories, alcohol and cigaretteconsumption, and diet. Exposure tohydrocarbons was inferred from inter-view responses by four assessors whowere blind to disease state, and these datawere then summarised by a cumulativehydrocarbon exposure (CHE) score.Results-After adjustment for alcohol,cigarettes, dietary antioxidants, andsocial class, odds ratios for low CHEscores were 1-20 (90% CI: 0.62-2.35) and2-67 (90% CI: 1-22-5.87) for high scores. Atest for trend with level of exposureamong only those who had exposurescores >0 gave p = 0 09. Analysis by typeof hydrocarbon was limited to four expo-sures for each ofwhich there were at least20 exposed patients. The adjusted OR forpaint solvents (any level) was 0-96 (90%CI: 0-48-1-93); for diesel exhaust fumesOR = 2-66 (90% CI: 1.05-6-73); for petro-chemicals OR = 1-82 (90% CI: 0'80-4-11);and for chlorinated solvents OR = 1-49(90% CI: 0-58-3-81).Conclusions-These results support theoriginal hypothesis. Further studies areneeded to confirm or refute the findingshere and to clarify the types of hydrocar-bon involved.
(Occup Environ Med 1994;51:631-637)
Centre forOccupational HealthR McNameeJ HoggN M CherryDepartment ofMedicine(Gastroenterology),J BraganzaP RoseDepartment ofPublicHealth andEpidemiology,University ofManchesterI Leck (emeritus)Correspondence to:Dr R McNamee, School ofEpidemiological and HealthSciences, Stopford Building,Oxford Road, ManchesterM13 9PT.
Accepted 16 May 1994
Keywords: chronic pancreatitis, hydrocarbon expo-sure, epidemiology
A rising trend of idiopathic pancreatitis hasbeen noted in England,' which together withother observations, suggests that environmen-tal exposure to chemicals (xenobiotics) maybe aetiologically relevant.23 When a pharma-cokinetic study indicated induction ofcytochrome P450 in most patients, irrespec-tive of alcohol intake,4 Braganza et al under-took a preliminary occupational study.5Nineteen consecutive patients with recurrentpancreatitis were assessed, including seven ex-
alcoholics, and 12 with idiopathic disease.Regular exposure to diesel exhaust fumes or
degreasing agents and solvents was found forall patients and several of them had noted a
relation between periods away from work andabsence of symptoms.
As a consequence of these findings, the pre-sent study was set up in 1988 to test thehypothesis that exposure to occupationalhydrocarbons is a risk factor for chronic pan-creatitis. Since chronic pancreatitis is a raredisease (with an annual incidence ofbetween 1and 10/100 000 in European countries6) thecase-referent method was considered appro-priate. At that time alcohol was accepted as amajor risk factor for chronic pancreatitis,68cigarette smoking was suspected of beingindependently associated, and there was someevidence that low levels of dietary antioxi-dants may play a part.910 Information on thesepotential confounders was therefore sought aswell as occupational exposure.
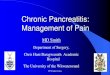
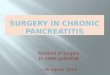
Patients and methodsIDENTIFICATION OF CASESPotential cases of chronic pancreatitis wereidentified retrospectively in three steps (fig).Firstly, the Komer episode system, whichrecords details of all hospital inpatientepisodes in England and Wales, was used toidentify all inpatients in seven health districtsin Greater Manchester (hereafter referred toas the study area), who were discharged aliveto an address in the study area during the fiveyear period, 1 April 1985 to 31 March 1990,and whose stay in hospital was given any ICD577 code (diseases of the pancreas).
In the second step, the hospital notes ofthese patients were inspected for evidencethat the standard diagnostic criteria forchronic pancreatitis had been fulfilled.7 Theseare: either typical histological changes, pan-creatic calculi, advanced change pancreatitisby endoscopic pancreatography, or unequivo-cally reduced exocrine secretary capacity (<mean-3SD); otherwise at least two of thefollowing-moderate change pancreatitis byendoscopic pancreatology, moderatelyimpaired exocrine secretary capacity (betweenmean-3SD and mean-2SD), and intrapan-creatic retention cysts shown by computedtomography. Those who first satisfied thediagnostic criteria between 1 April 1983 and31 March 1990 were considered further ifthey were aged 18 + and had an addresswithin the study area at diagnosis, and if theirillness was not considered to be secondary topancreatic cancer, cystic fibrosis, or abdomi-nal trauma, and there was no record of deathin their notes.
Finally, efforts were made to contact thesepatients, after permission had been obtainedfrom their hospital physicians and generalmedical practitioners. Only those patients
631
on June 25, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.51.9.631 on 1 Septem
ber 1994. Dow
nloaded from

McNamee, Braganaza, Hogg, Leck, Rose, Cherry
general practitioner, or if the subject had diedor could not be contacted, they were replacedby another, chosen in the same way as theoriginal, from the Family Health ServicesAuthority list.
Hospital ICD code577-1
I296
Insufficient Other CPinformation pancreaticto make diseasediagnosis
119 62 115
Othercriteriasatisfied?
YES NO
72
Removal ofduplicate notes
I62 patients
43
l l -1(a) (b) (c) (d)
I 131 6 5 1
Hospital ICD code:577.0, 577.2, 577.8 or 577.9
I1186
Insufficient Other CPinformation pancreaticto make diseasediagnosisII
601 492 93
Othercriteriasatisfied?
YES NO
66
Removal ofduplicate notes
27
(a) (b) (c)
I 616 5 6
47 patients
Selection of cases:ICD codes (9th revision):
557-0 Acute pancreatitis (n = 1082);577-1 Chronic pancreatitis (n = 296);577-2 Cysts and pseudocyst ofpancreas (n = 25);577 8 Other disease ofpancreas (n = 38);577*9 Disease ofpancreas-unspecified (n = 41).
(a) Time of diagnosis outside timeframe; (b) residence at diagnosis outside study area;(c) chronic pancreatitis secondary to pancreatic cancer, trauma, or cystic fibrosis;(d) deceased.
found to be still alive were considered eligiblefor inclusion. None of the 19 subjects fromthe original occupational investigation' isincluded in this case series.
IDENTIFICATION OF REFERENTSComputerised records of the five FamilyHealth Services Authorities that provide pri-mary health care to residents of the sevenhealth districts, were used as a source for ref-erents. When an eligible patient with chronicpancreatitis had agreed to participate in thestudy, two potential referents of the same sexand the same birthdate were chosen at ran-dom from the Family Health ServiceAuthority list which included the case.
General practitioners of these referentswere approached by us for permission to con-
tact their patients, except in one district wherethe Family Health Services Authority pre-ferred to make the initial approach. If permis-sion was refused by the subject or their
INTERVIEWSStructured interviews to ascertain occupa-tional exposure and potential confoundingvariables were carried out in the homes ofcases and referents during the period April1989 to March 1992. As the interviewer wasalso involved in identifying study subjects, itwas not possible for interviews to be con-ducted blind to disease state.
ASSESSMENT OF EXPOSUREA list of jobs thought to involve potentialexposure to hydrocarbons was drawn up atthe beginning of the study. At interview alljobs held since leaving school were recordedand, where one of those on the list wasreported, there followed a further question-naire on workplace ventilation, respiratoryprotection, and work practices.
Copies of the occupational questionnairewere sent to each of two occupational hygien-ists and two occupational physicians whowere not informed about the state of the sub-ject. These assessors independently rated eachjob both for likelihood (definitely no, probablyno, probably yes, definitely yes) and intensity(low, medium, high) of exposure to each of 12groups of chemicals. In guidelines for ratingexposure, it was suggested that the labels low,medium, and high be thought of as <30%,30%-80% and >80% of occupational expo-sure limits where these existed.A method for calculating a cumulative
hydrocarbon exposure (CHE) score was
devised independently of the data and isshown in the appendix. Only ratings of proba-ble or definite exposure of a medium or highintensity were considered further, with allsuch medium and high intensity ratings givenscores of 1 and 2 respectively. These scoreswere combined together in three consecutivesteps: across chemical groups, across asses-sors, and across jobs. In step one, a singlescore for each combination of job and assessor
(the assessor job scores) was calculated byadding together the chemical specific scores.At step two, a single score for each job was
found by taking the median of the four indi-vidual assessor scores (the median job score).Finally, a CHE score up to the date of diagno-sis in cases (or the same date for their agematched referents) was found as a weightedsum of the scores for each job, the weightsreflecting time spent in the jobs.
Three categories of lifetime exposure weredefined from the CHE score: 0 (zero), 0<CHE <10 (low), and CHE >-10 (high), andwere used to examine the relation betweenexposure and risk.
Cumulative exposure scores (CEs) werealso compiled for each of the 12 chemicalgroups separately by combining ratings acrossassessors and jobs only (see appendix).
Information on exposures outside the work
Hospital notesinspected
1482
632
on June 25, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.51.9.631 on 1 Septem
ber 1994. Dow
nloaded from

Occupational exposure to hydrocarbons and chronic pancreatitis: a case-referent study
environment-for example, domestic expo-sure, hobbies-was also collected, but as theintensity was never more than the equivalentof low occupational exposures, it was not con-sidered further.
ASSESSMENT OF POTENTIAL CONFOUNDERSAt interview, subjects were questioned aboutalcohol, cigarettes, and dietary intake, both atthe time of interview and two years before theestimated time of first symptoms. Questionsabout current consumption of alcohol andcigarettes were based on those used in theUnited Kingdom Government GeneralHousehold Survey.11 A weekly food frequencyquestionnaire derived from previous work wasalso completed.910 To measure presymptomintakes of all variables, subjects were firstquestioned about present consumption andthen asked how their consumption x years agodiffered (where x for each case and the twomatching referents was two years earlier thanthe dates of onset of symptoms in the case).Only presymptom intakes are used in thisstudy.
For the main analysis, weekly alcohol con-sumption was expressed as a multiple of therecommended safe upper limits for men (21standard units) and women (14 standardunits).'2 Cigarette consumption before symp-toms was classified as "ever" or "never". Thedietician, who was unaware of subjects' dis-ease state, derived dietary intakes of antioxi-dants from questionnaire responses. Thesedata were then expressed as percentages ofrecommended daily intakes.To assess social class, all job titles were
coded to the Office of Population Censusesand Surveys 1990 standard occupational clas-sification'3 from which the United Kingdomstandard social class groups (I: professional toV: unskilled) were derived. Where a subjectheld jobs with different social classifications,he or she was allocated to the class in whichthey spent most time. Three groups wereformed for the main analysis: social classes I+ II, III, and IV + V. A second measure ofclass was based on age at which full time edu-cation ended: at the minimum school leavingage, up to two years after the minimum, andlater.
STATISTICAL ANALYSIS AND POWERConditional logistic regression techniqueswere used to estimate odds ratios (ORs) andto control for confounding. Where appropri-ate, 90% confidence intervals (90% CIs) werecalculated, which may also be interpreted asone tailed tests (a = 0-05) of the hypothesisunder study. To test for trend with level ofexposure, a regression coefficient was esti-mated from the data on those with exposurescores >0; this coefficient divided by its stan-dard error was used to provide an (approxi-mate) one tailed test.Under the assumption that 15% of the ref-
erents would be exposed to hydrocarbons, itwas estimated that the study would have 70%power to detect an increased risk correspond-ing to an OR of 2 and 90% power for an OR of
2-5, with a one-tailed test with a significancelevel of 5%. Analyses of the relations betweenindividual chemical groups and risk would beexpected to have low power.
ResultsASCERTAINMENT OF CASES AND REFERENTSThe Korner episode system search yielded1482 hospital case notes of which 296 hadbeen coded as ICD 577 1 (chronic pancreati-tis). On inspection, only 72 of these satisfiedall the criteria, which gave 62 patients afterelimination of duplications (fig). A review ofnotes with other ICD 577 codes yielded a fur-ther 66 eligible notes, corresponding to 47patients. Of the total of 109 patients thusidentified, four had died before the studystarted, one declined to take part, and twocould not be contacted, leaving 102 cases.Two hundred and four people were initially
chosen from Family Health ServicesAuthority files to serve as referents, but only129 (63%) of these were included in thestudy. The main reasons for non-participationwere: general practitioner refused permission(7 4%), subject refused (16-7%), and noresponse from subject (11-8%). Where non-response could be investigated-that is, in alldistricts except that where the Family HealthServices Authority made the initial contact-the overwhelming reason was that the subjectno longer lived at the address held by theFamily Health Services Authority or generalpractitioner. To replace the 75 refusals andnon-responders, a further 110 names had tobe found from Family Health ServicesAuthority lists, giving a total of 314 names.The median age of cases at the time of
diagnosis was 44 years (range 19-81) and 77(75%) of them were men. Seventy per centhad a presymptom weekly alcohol intakeabove the safe level compared with 45%among referents (table 1). Cases left school atan earlier age than referents and were morelikely to belong to social class IV or V; a largerproportion of them had a diet that was defi-cient in ascorbic acid or selenium and theywere more likely to have smoked.
OCCUPATIONAL EXPOSURESTable 2 summarises the occupational expo-sure profiles of cases and referents where asubject is classified as having had a particularexposure if they have a CE score >0 (individ-ual chemical groups) or a CHE score >0 (anychemical group). The most common exposurewas to paint solvents which includes paint,paint thinners, varnishes, etc (59 subjects),followed by diesel exhaust fumes (33 sub-jects), paraffin, kerosine, petrol, or diesel (28subjects), and chlorinated solvents (21 sub-jects). Fifty five percent (n = 56) of cases and40% (n = 81) of referents had a CHE score>0, which is considerably more exposure inboth groups than anticipated.The crude (unadjusted) OR, which con-
trasts those with a positive CHE score andthose with a zero score was 2-21 (90% CI:1-38-3-53) (table 3); the OR for the low
633
on June 25, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.51.9.631 on 1 Septem
ber 1994. Dow
nloaded from

McNamee, Braganaza, Hogg, Leck, Rose, Cherry
Table 1 Alcohol, cigarette, and dietary antioxidantintake, and social class of cases and referents
Cases Referent:(n CIO) ) (n (0),0
Presymptom alcohol consumption (standard units/week,Men Women'-21 -,14 31 (30) 112 (55.22-4A 15-34 23 (23) 48 (24'
'5(0 35 48 (47) 44 (22,
Age left school2+ v after min<2 y after mur,At min ag-
Standard social ciassificatiorI + IIIIINHIMID + VUnclassified'
Presymptom smoking (cigarette;Never smokedSmoked
Presymptom antioxidant intake: asci(o0 recommended daily intake)>100
50-99<5(Unknown*
Presymptom antioxidant intake: sele(% recommended daily intake)
>10050-99<50
Unknown*"
*Never worked outside the home.*Dietary information incomplete.
3 (3)18 (18)81 (79'
4 (4320 (20)44 (43)
Table 3 Crude and adjusted* ORs for hvdrocarbor,exposure as measured by CHE score
CHE Cases Rejerents Crude OR Adjusted ORscore (n (0)) (n (O)y (90%0 CI) (9000 (71
0 46 (45' 124 (60) 1 00 1 00Low 32 (31) 60 (29) 1 61 (0 93 2-77? 1 20 (0 61- 2 35,High 24 (24) 21 (10) 3-61 (1 91-6 823 2 67 (1-22-5 87>0 56 (55) 56 (55) 2 21 (138-3 53) 1-64 (0-92-2 93
*Adjusted for social class (two measures), alcohol; cigaretteconsumption, and dietary intakes of selenium and ascorbic
24 (12) acide before symptoms, Four subjects were excluded Iront53 (26) adjusted analyses--three because one case did not complete127 (62) the dietary assessment and so she and her matching referents
could not be used, and one (referent) because she could notbe classified bv social class.
36 (1841(20)90 (44
34 (33? 36 (18) Table 3 also shows the adjusted ORs for0 1 low and high CHE categories given by this
analysis. Both the ORs have been reduced but
84(82) 130 (4. the adjusted OR of 2-67 for those with a highscore is still significantly increased (90% Cl:
orbic acid 1 22 5 87). The test for trend among those
80 (78) 190 (93' with scores >0 now gave p = 0O09.19 (19 14 (7' The relations between CHE and risk of
(1l (} chronic pancreatitis were examined separatelynium for those who drank less than harmful levels of
alcohol (as defined above) and those who20 (20 43 (21) drank than this. To reduce confounding
50 (49) 125 (61)
31 (30, 36 (18) of the associations between risk and CHE by(1 level of consumption within each of these two
exposure score category was 1-61 (90% CI:0(93-2-77) and for the high 3-61 (90% CI:1-9]-6 82). Among those with scores >0, atrend showing increasing ORs with increasingscore was significant at the 5% level (p =0-05).The risk of chronic pancreatitis showed a
strong (roughly exponential) relation withpresymptom alcohol consumption. Alcoholconsumption was also positively correlatedwith hydrocarbon exposure in the referentgroup. Together these two associations indi-cate confounding by alcohol consumption.14To control confounding, alcohol consump-tion was included in a conditional logisticregression model, as were the two measures ofsocial class and smoking state. Those antioxi-dant measures that showed independentassociations with risk of chronic pancreatitis-ascorbic acid and selenium were aiseincluded. Four subjects are excluded fromthis analysis because of missing information.
Table 2 Cases and rejerents with occupational exposurescores >0)
Cases Referents Total7:ype ofexposure n (0) (n ( ii)i(X1 ('o)
Dyes 5 (5) 4 (2) 9 (3)Petrol exhaust fumes 8 (8, 10 (5) 18 (6)Diesel exhaust fumes I 5 ( 15o 18 (9 33 ( 1iGlues, adhesive: 5 (5, 6 (3 11 (4Weedkillers, pesticides 2 (2 1 (0 5 3 (1)Oil mist" 4 )4 10 (5. 14 (5Paint solvents 23 (23! 36 (18 59)( 19)Paraffin, kerosinc.
petrol, diesel 15 (15; 13 (6 28 (9Disinfectants 2 (2 2 (2:a 4 (1:Chlorinated solvents 10 (10 1 (5 21 (7,Printing inks 3 (3 6 (3) 9 (3.Rubber fumc 2 (2 2 (1) 4 (1,Any of these 56 (55) 81 (40) 137 (45)
categories of alcohol, the continuous variablemeasuring alcohol intake was included as acovariate in these analyses. In the low alcoholgroup, the ORs for none, low, and highhydrocarbon scores were 100. 1 75 (900:: CI.0 77-3 98), and 4 20 (90% CI: 1-41-12-57:.In the high alcohol group, the correspondingORs calculated relative to the no exposure,low alcohol group were 3-80 (90% CL:0 97-14 86), 2-29 (90%/o CI: 0A49-10(74), and5 51 (90% CI: 1 11-27 36). The associationwith hydrocarbon exposure seems weaker foralcoholic compared with non-alcoholicchronic pancreatitis, but the numbers are toosmall to allow firm conclusions for the alco-holic group.
Table 4 shows the associations between riskof chronic pancreatitis and the four chemical
Table 4 Crude and adjusted ORs Jor exposure to seletreachemicals
CalfScore
Paint solve0
Low*High*>0
Cases Referents(}l ('%m) ( I1 (°o,) )
nts,.79 1i6814 2
9i 1 'I
2)3 36
Diesel exhaust fumes:0 8- 186Low* 10 I1High* -s (i>0 1-@ 18
C(nde AdjusteJOR OR (900 ('1
1001 221 7'1-41
l Of)
1 Q962 1)82-04
Paraffin, kerosme, petrol, or diesel:0 87 191 1l0CLow* I 8 3 09High* 4 5 1 86>0a 1's I 2 by
Chlorinated solvents0 9 19Low0* 7 9
High0 3 2
>0 10 II
I 0"
I .-23 1I1 88
I o(11 02 (0 43-0-87 (0-31-10-96 (0-48-
-2-44.2-52,s1 93'
)0(1-96 (063 6-6)9'4 18 (1-09-16061)2 66 (1 05 6 73.
1 0(02 70 (0-99 7 310-92 (0 26--3 301 82 (0 80-4 II
1 000 96 (0 30 -3 04j441 (069--28 19,1-49 (0 58--381"
*Low: 0 < score <5. High: score a;Adjustments and exclusions as explained in table ..
634
on June 25, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.51.9.631 on 1 Septem
ber 1994. Dow
nloaded from

Occupational exposure to hydrocarbons and chronic pancreatitis: a case-referent study
groups for each of which there were at least 20exposed subjects. The ORs are adjusted foralcohol, smoking, dietary and social class vari-ables as before, but not other occupationalexposures. Because of the small number ofpeople with scores >10, a cut off point of 5was used to define high exposure for thesevariables. Although there is a suggestion of arelation between paint solvents and risk in thecrude data, this disappears after adjustmentfor confounding. The adjusted OR for dieselexhaust exposure is significant at the 5% level,OR = 2-66, (90% CI: 1-05-6&73), and there issome suggestion of a dose-response relation.The ORs for paraffin, kerosine, petrol, ordiesel (1-82), and for chlorinated solvents(1 -49) are not significantly increased.
DiscussionA positive association has been found betweena high (> 10) CHE score and risk of chronicpancreatitis. Aspects of the study methodol-ogy that might be judged logically to havecontributed to a false positive association, andthe implications of the results, are consideredseparately.
METHODOLOGYUndoubtedly some cases of chronic pancreati-tis in the study area have been omittedbecause the required diagnostic procedureswere not carried out, but as these exclusionswere not related to exposure, this is not asource of bias. Similarly, the restriction tocases still alive at the time of the study isunimportant unless exposure is related to sur-vival.
Ideally, the referents should have been cho-sen from those people resident in the studyarea at the time of diagnosis of the cases (1April 1983 to 31 March 1990). It was notpossible to sample this population retrospec-tively; instead referents were chosen from res-idents at the time of the study. This couldlead to bias if the exposure profile of the popu-lation has changed over time. Information onthe previous residence of all study subjectswas available and showed that six referentshad lived outside the study area at the time ofdiagnosis of their matching case. A reanalysisomitting these six gave very similar results(OR for high CHE score = 2 59).The response rate (63%) among the 204
people originally chosen as referents wassomewhat low, and non-participants werereplaced. This could lead to a false positiveresult if participating referents had less expo-sure than non-participants. This could occurif, for example, participation was related tosocial class. As almost the entire population isregistered with a Family Health ServicesAuthorities in England and Wales, the socialclass of referents should be broadly similar tothat of the entire population of the study area.To check this, a comparison of the socialclasses of the referents with those of age, sex,and area specific figures from the 1981 censusof Great Britain'5 was carried out; this showedthat the referents in the study were slightlymore likely to belong to the manual classes
(62% v 57%). Thus it seems unlikely thatpopulation exposure has been underestimatedin this referent group.
Estimation of past exposure to hydrocar-bons was carried out in three stages: inter-view, assessment of interview material by apanel, and construction of an exposure scorefrom these assessments. Some misclassifica-tion with respect to exposure is inevitablewhen it is assessed retrospectively, but pro-vided this operates equally in both case andreferent groups, it should not produce falsepositive associations.'4 Study subjects werenot told of the study hypothesis, but as theinterviewer was aware of the group to whichsubjects belonged, the possibility of informa-tion bias must be acknowledged. The transla-tion of job descriptions into exposures,however, was done by a team who wereunaware whether the subject was a case or areferent. Also reassuring was the interviewer'sopinion, on completion of all interviews, thatthe job profiles of cases and referents seemedto be similar.The CHE measure of exposure used here
was just one of several possible approaches tosummarising the exposure data but, impor-tantly, it was the one chosen in advance. Inretrospect, this method of classifying jobs as"exposed" might be said to have erred on theside of sensitivity at the expense of specificity:to receive a score > 0, only two of the fourassessors needed to rate the job as exposed. Infact, had a stricter criterion-that three of thefour were needed-been used, the strength ofthe association with risk would haveincreased. (Adjusted ORs for low CHE scoreswould then be 1-32 (90% CI: 0-62-2 80) andfor high scores 3 17 (90% CI: 1-41-7 13)).
Furthermore, the CHE measure followed a"broad-brush" approach in terms of (a) thetiming of exposure ("ever" before diagnosis);(b) assumptions about the respective effects ofintensity and duration of exposure, and (c)type of hydrocarbons (any of the groups intable 2). This approach seems warranted inthe absence of a more specific hypothesis.Retrospective analyses to clarify the roles ofintensity, duration, and timing in relation todisease presentation -were carried out and,although inconclusive,- were consistent withthe view that exposure had a cumulativeeffect.To allow for confounding, the interview
schedule included questions on all known orpostulated risk factors for chronic pancreati-tis, and these were included as covariates in aregression model. In general, adjustment forconfounding effects by statistical analysis doesnot remove the problem in its entirety, aserror in the measurement of confoundersresults in residual confounding after adjust-ment. 16 In fact, after adjustment for othervariables the relations between social classand chronic pancreatitis, and smoking andchronic pancreatitis were not significant.Inclusion of these variables together with thedietary measures made little difference to theestimates of ORs for hydrocarbon exposure.
Alcohol consumption is a particularly
635
on June 25, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.51.9.631 on 1 Septem
ber 1994. Dow
nloaded from

McNamee, Braganaza, Hogg, Leck, Rose, Cherry
strong risk factor for chronic pancreatitis andtherefore the methods for measurement andanalytical control of this variable are criticallyimportant. It was the interviewer's impressionthat subjects were quite willing to admit toheavy drinking in the past. This, and theheavy consumption of alcohol reported byboth cases and referents, suggests that previ-ous consumption may be less prone to theunder reporting that is said to occur for cur-rent habits. In the statistical analysis effortswere made to model the relation betweenalcohol and risk of chronic pancreatitis asaccurately as possible. The inclusion of alco-hol as a continuous variable (with the atten-dant assumption of an exponential relation)was considered to be the most accurateapproach. It also reduced the associationbetween the CHE score and risk of chronicpancreatitis more than other methods-forexample, with categories of alcohol. It seemsunlikely therefore that the association can
simply be explained by the confoundingeffects of alcohol.
IMPLICATIONSIf the OR of 2-67 associated with a high expo-sure score is correct, then with calculationsbased on the attributable risk, one can esti-mate that exposure at this level played a partin 15 cases (15% of the total) in this urbanstudy population. The industries or jobs ofthose placed in the high exposure group were
varied, but with metal production or working,transport, and motor repair being the mainsectors. The SOC code 540, motor mechanicsand auto engineers, (who can be exposed topaints as well as petrochemicals) was a partic-ularly common code in this group, but itshould be noted that there is not a one to one
correspondence between job types and expo-sure.
In the subsidiary analyses, which had lim-ited statistical power, the greatest risk seemedto be associated with diesel exhaust fumes. It isnot evident why this product should be a par-ticular hazard as its hydrocarbon content isfairly low, but it may contain other toxic sub-stances. If hydrocarbons alone play a part inchronic pancreatitis, then those chemicalgroups that are almost purely hydrocarbon(groups 7 and 8) might be expected to showthe strongest associations. Surprisingly, no
relation was found with paint solvents.It has been hypothesised that chronic pan-
creatitis is a product of heightened but unmit-igated oxidative detoxification reactionsmediated by cytochromes P450.317 Underthis model, aetiologically relevant chemicalswould be inducers of P450 and undergometabolic activation. Damage would onlyoccur if the supply of antioxidants were insuf-ficient to meet the increased demand fromreactive oxygen or xenobiotic metabolites.10 17
In this study, a relation between chronic pan-
creatitis and antioxidant intake was found.Consideration of this and the interactionsbetween antioxidant intake and occupationalexposures in determining risk of chronic pan-creatitis will be examined elsewhere.
Chronic pancreatitis is a rare disease but adisabling one; if occupational exposure toorganic chemicals is indeed a risk factor, assuggested by our study, then identification ofthe most heavily implicated chemicals, andreduction of these exposures, must be a prior-ity. If further studies are set up to confirm (orrefute) the main results here, then it would bedesirable to put particular emphasis on thevalid differentiation between different types ofchemicals containing hydrocarbons.
We thank the North Western Regional Health Authority whofunded this study, and G Fletcher, W R Lee, M Molyneux,and D Turner who carried out the occupational assessments.We also thank the Medical and Ethics Committees and FamilyHealth Services Authorities of the seven Health Districts inGreater Manchester (North, Central, and South Manchester,Salford, Stockport, Tameside, and Trafford) and the subjectsthemselves who gave their consent to the study.
Appendix: illustration of derivation ofexposure scores
(A) CUMULATIVE HYDROCARBON EXPOSURE(CHE) SCORE TO DIAGNOSISHypothetical job with scores >0 for chemicalgroups 3, 8, and 9 only
Chemical groupAssessor's
Assessor 3 8 9 job score
1 0 M M 22 0 0 M 13 0 M 0 14 M H M 4Median 1 5
Cumulative hydrocarbon exposure score to diagnosis =Ej (median intensity for group 3 x years in job x hours per
weekl40).j = all jobs to diagnosis.
(B) CUMULATIVE EXPOSURE (CE) SCORE UPTO DIAGNOSIS FOR EACH CHEMICAL GROUPSEPARATELY
Chemical group
Assessor 3 8 9
0 M M2 0 0 M3 0 M 04 M H MMedian 0 1 1
Cumulative exposure to diagnosis for chemical group 3, sayEs (median intensity for group 3 x years in job x hours per
week/40).j = all jobs to diagnosis.
1 James 0, Agnew JE, Bouchier IAD. Chronic pancreatitisin England: a changing picture? BMJ 1974;2:34-8.
2 Braganza JM. Hypothesis. Pancreatic disease: a casualty ofhepatic "detoxification"? Lancet 1983;ii: 1000-3.
3 Braganza JM. Chronic pancreatitis. In: International teachingsessions of the golden jubilee. Meeting of the British Society ofGastroenterology. London: John Wiley, 1987.
4 Acheson DWK, Rose P, Houston JB, Braganza JM.Induction of cytomchromes P-450 in pancreatic disease:consequence, coincidence or cause? Clin Chim Acta1985;153:7384.
5 Braganza JM, Jolley JE, Lee WR. Occupational chemicalsand pancreatitis: a link? IntJ Pancreatol 1986;1:9-19.
6 Worning H. Chronic pancreatitis: pathogenesis, naturalhistory and conservative treatment. Clin Gastroenterol,1984;13:871-94.
7 Braganza JM. The pancreas. In: Pounder RE, ed. Recentadvances in gastroenterology. Vol 6. London: ChurchillLivingstone, 1986;251-80.
636
on June 25, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.51.9.631 on 1 Septem
ber 1994. Dow
nloaded from

Occupational exposure to hydrocarbons and chronic pancreatitis: a case-referent study
8 Yen S, Hsieh C, MacMahon B. Consumption of alcoholand tobacco and other risk factors for pancreatitis. Am JEpidemiol 1982;116:407-14.
9 Rose P, Fraine E, Hunt LP, Acheson DWK, Braganza JM.Dietary anti-oxidants and chronic pancreatitis. HumanNutrition: Clinical Nutrition 1986;40c: 151-64.
10 Uden S, Acheson DWK, Reeves J, Worthington HV, HuntLP, Brown S, et al. Antioxidants, enzyme induction andchronic pancreatitis. EurJ Clin Nutr 1988;42:561-9.
11 Office of Population Censuses and Surveys. General house-hold survey 1984. London: HMSO, 1986.
12 Royal College of General Practitioners. Alcohol-a bal-
anced view. Reportfrom general practice 1986:24.13 Office of Population Censuses and Surveys. Standard occu-
pational classification. London: HMSO, 1990.14 Rothman K. Modern epidemiology. Boston: Little, Brown
1986.15 Office of Population Censuses and Surveys. Census 1981
county report, Greater Manchester, part 2. London:HMSO, 1982.
16 Greenland S. The effect of misclassification in the pres-ence of covariates. AmI Epidemiol 1980;112:564-9.
17 Braganza JM, ed. The pathogenesis of pancreatitis.Manchester: Manchester University Press, 1991.
Vancouver styleAll manuscripts submitted to Occup EnvironMed should conform to the uniformrequirements for manuscripts submitted tobiomedical journals (known as theVancouver style.)
Occup Environ Med, together with many
other international biomedical journals, hasagreed to accept articles prepared in accor-
dance with the Vancouver style. The style(described in full in the BM7, 24 February1979, p 532) is intended to standardiserequirements for authors.
References should be numbered consec-
utively in the order in which they are firstmentioned in the text by Arabic numeralsabove the line on each occasion the refer-ence is cited (Manson' confirmed otherreports2-5 . .). In future references topapers submitted to Occup Environ Med
should include: the names of all authors ifthere are seven or less or, if there are more,the first six followed by et al; the title ofjournal articles or book chapters; the titlesof journals abbreviated according to thestyle of Index Medicus; and the first and finalpage numbers of the article or chapter.Titles not in Index Medicus should be givenin full.
Examples of common forms of refer-ences are:
1 International Steering Committee of Medical Editors,Uniform requirements for manuscripts submitted tobiomedical journals. Br MedJ 1979;1:532-5.
2 Soter NA, Wasserman SI, Austen KF. Cold urticaria:release into the circulation of histamine and eosino-phil chemotactic factor of anaphylaxis during coldchallenge. N EnglJtMed 1976;294:687-90.
3 Weinstein L, Swartz MN. Pathogenic properties ofinvading micro-organisms. In: Sodeman WA Jr,Sodeman WA, eds. Pathologic physiology, mechanismsof disease. Philadelphia: W B Saunders, 1974:457-72.
637
on June 25, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.51.9.631 on 1 Septem
ber 1994. Dow
nloaded from























![Lezione-2-Chronic Pancreatitis [modalità compatibilità]](https://img.pdfslide.us/doc/110x75/615bbaf9c02f8f30647023ab/lezione-2-chronic-pancreatitis-modalit-compatibilit.jpg)