Embed Size (px)
Citation preview
cutting edge research world class training and education partnering for patient-centred health services
FACULTY OF HEALTH SCIENCES
UNIVERSITY OF CAPE TOWN
Occupational health in the chemical industry: Respiratory Disorders at Work
Prof Mohamed F JeebhayOccupational Medicine Division and
Centre for Environmental & Occupational Health ResearchSchool of Public Health and Family Medicine, University of Cape Town
South African National Occupational Health & Safety Conference, Gauteng, July 2019
University of Cape Town Faculty of Health Sciences
Outline
• The chemical industry
• The chemical sector in South Africa
• Health effects of chemicals
• Occupational lung diseases in the chemical industry
• Work-related asthma
• Case study of prevention – towards “Vision Zero”
• Strategies for prevention of occupational lung diseases in South Africa
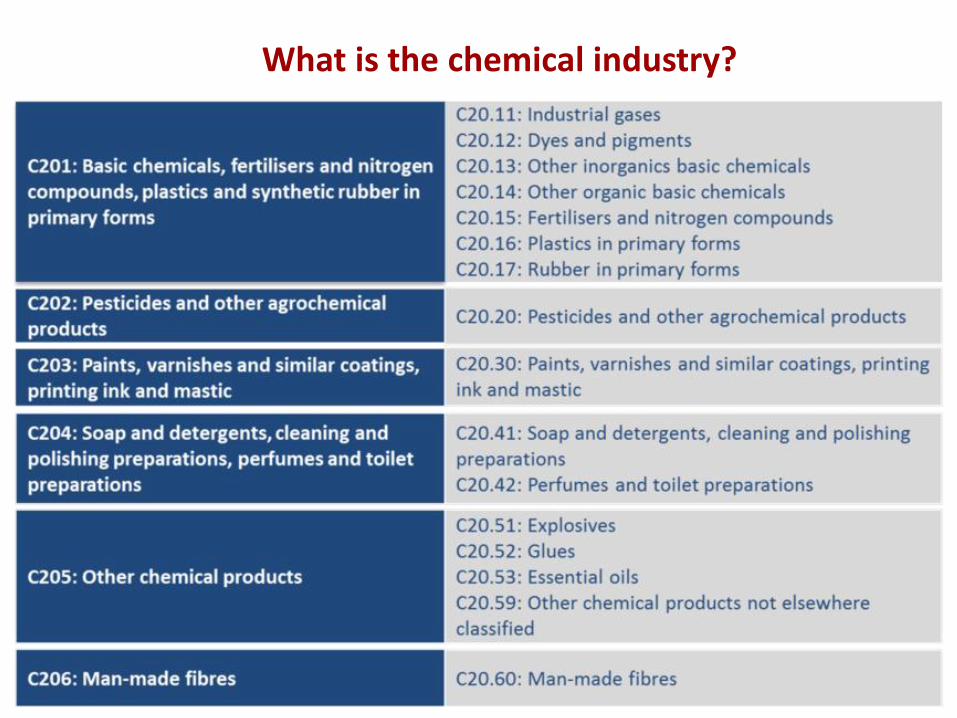
What is the chemical industry?
University of Cape Town Faculty of Health Sciences
Chemical sector in South Africa
• The chemical industry in South Africa:
- Upstream: technology and capital intensive in the manufacture of basic chemicals as raw materials/feedstock. Not well structured to accommodate either high numbers of employment or the development of Small or Micro Enterprises (SMEs)
- Downstream: turns raw materials into intermediate and final products. Operations typically labour intensive but greater potential to contribute significantly to large numbers of employment and the development of SMEs
• In the main it is an upstream sector to the mining, manufacturing and agricultural industries, but its success depends on the downstream sectors performing well and growing
• An integrated approach is necessary to support growth in the chemicals sector which provides ~25% employment and input to the total gross value
(http://www.thedti.gov.za/industrial_development/sec_chemicals.jsp; Bhorat and Rooney, DPRU, 2017)
University of Cape Town Faculty of Health Sciences
Health effects of chemicals
• Chemicals are the commonest occupational hazard that can result in OD
• Chemical agents account for 41 of the ODs that are caused by exposure to agents from work activities (ILO List of Occupational Diseases)
• Chemical agents are also the main contributors to ODs classified by target organ systems (especially respiratory and skin diseases), as well as occupational cancers
(Lim and Koh, 2014)
University of Cape Town Faculty of Health Sciences
How do chemicals enter and affect the body?
• Inhalation of airborne chemical agents such as gases, vapors and particulates result in rapid absorption
• Skin absorption usually slower - many chemical compounds, especially fat soluble absorbed through the intact skin
• Oral route: eating/smoking due to contamination of hands
• Absorption causes acute (some reversible e.g. asthma)/chroniceffects (irreversible e.g. COPD)
• Latency period for chronic effects e.g. silicosis, asbestosis
• Mechanism of action: irritants, sensitisers, carcinogens (mutagens, teratogens, genotoxic, reproductive toxins, systemic toxins)
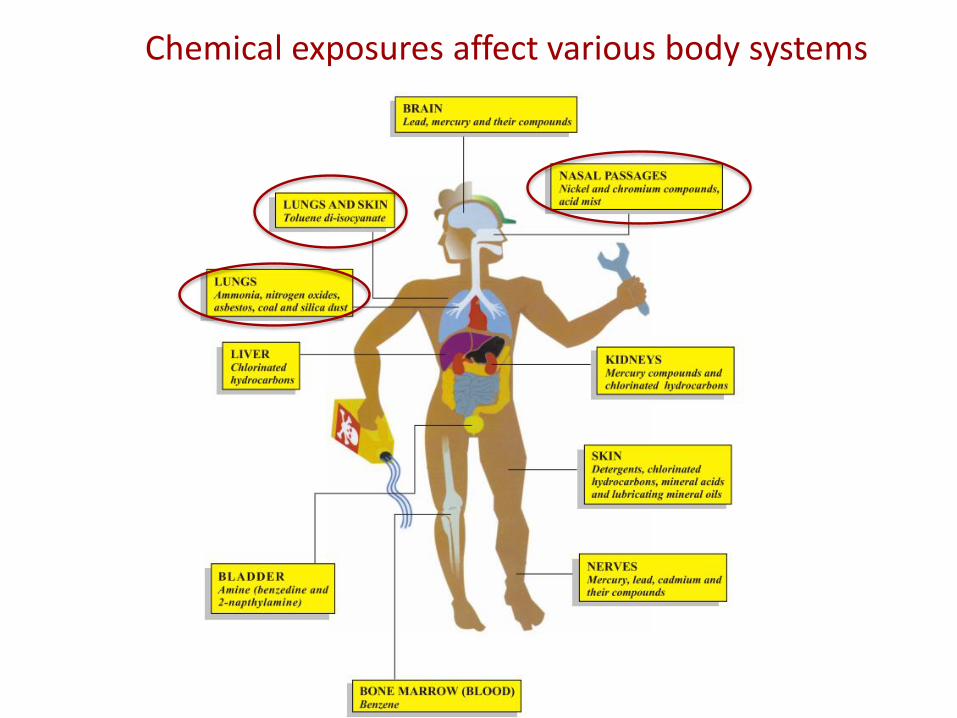
Chemical exposures affect various body systems
University of Cape Town Faculty of Health Sciences
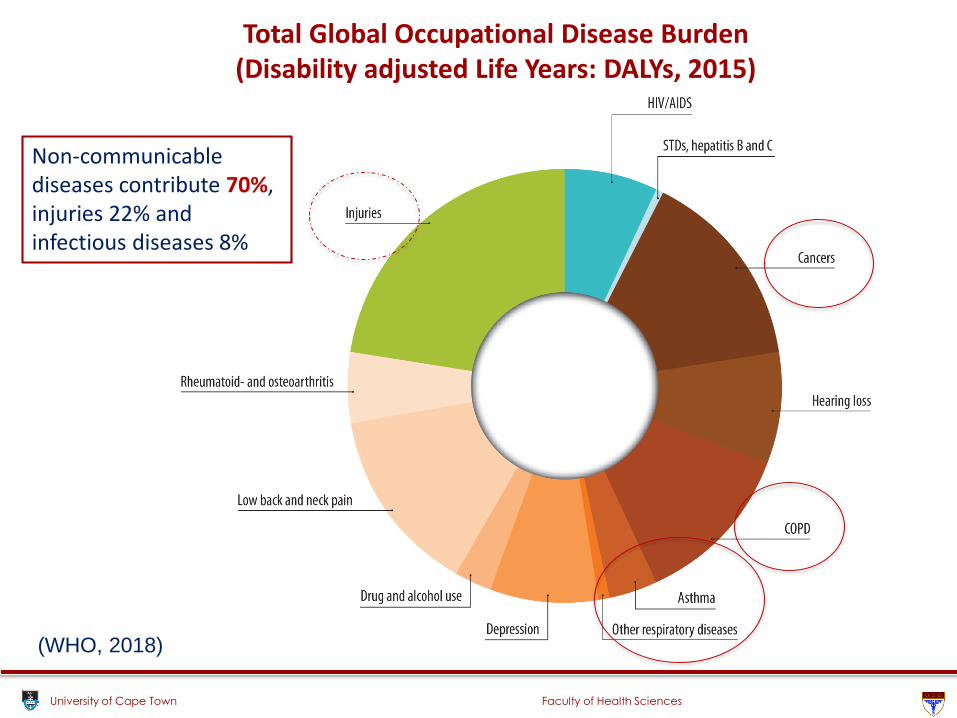
Non-communicable diseases contribute 70%, injuries 22% and infectious diseases 8%
Total Global Occupational Disease Burden (Disability adjusted Life Years: DALYs, 2015)
(WHO, 2018)
University of Cape Town Faculty of Health Sciences
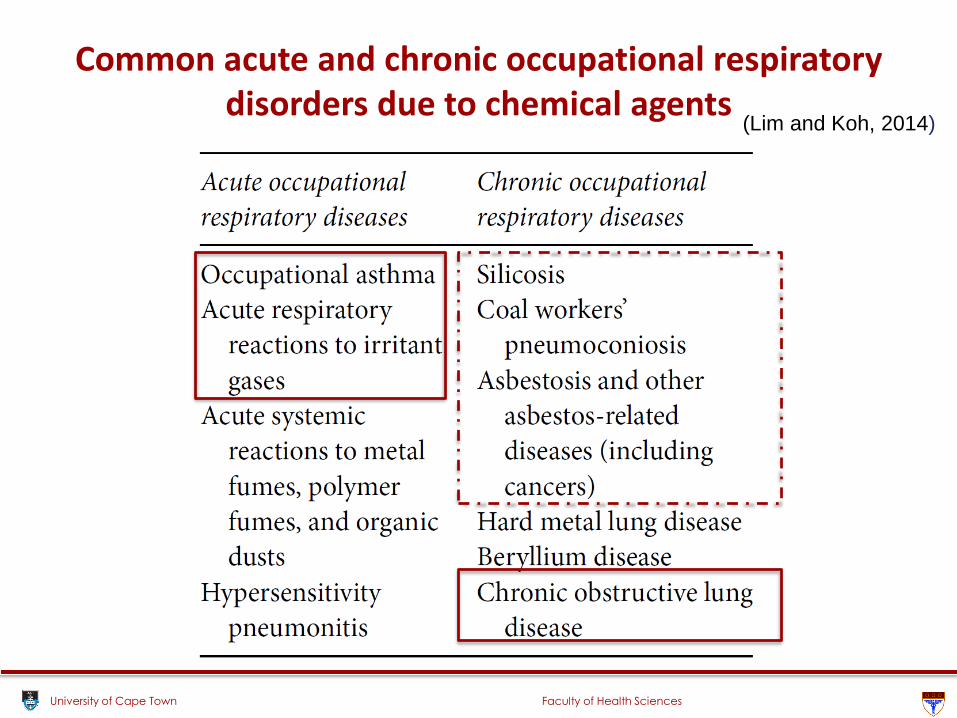
Common acute and chronic occupational respiratory disorders due to chemical agents
(Lim and Koh, 2014)
University of Cape Town Faculty of Health Sciences
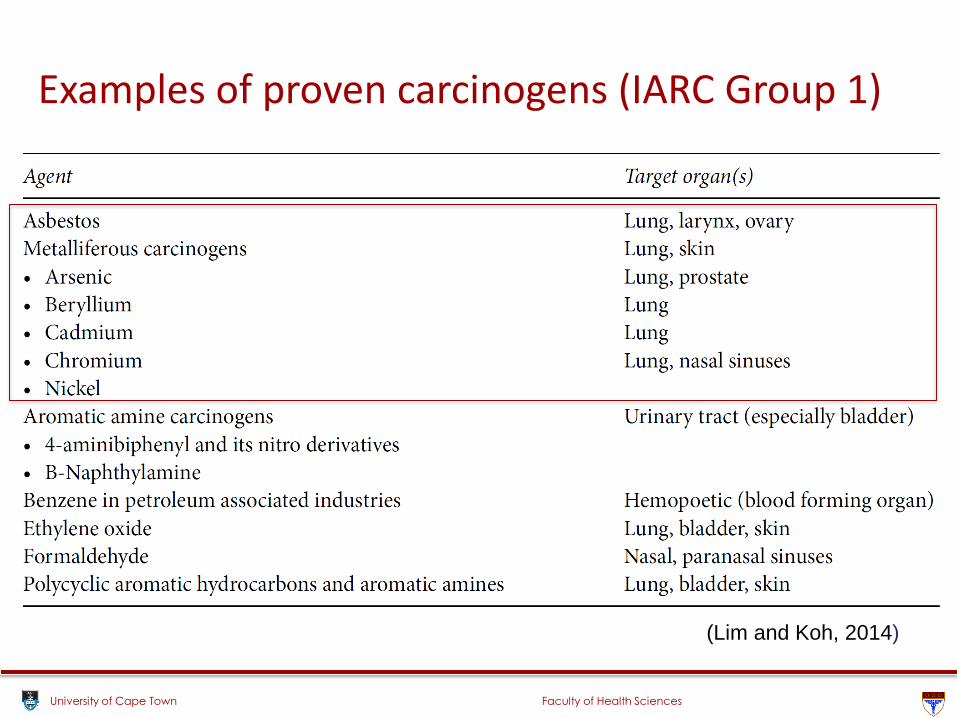
Examples of proven carcinogens (IARC Group 1)
(Lim and Koh, 2014)
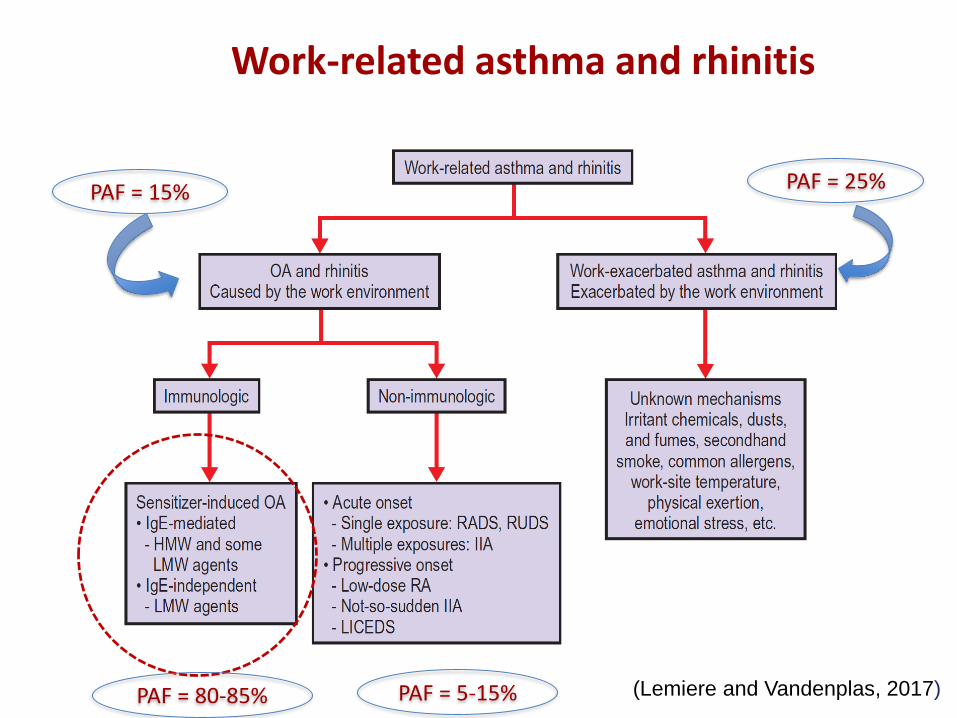
Work-related asthma and rhinitis
(Lemiere and Vandenplas, 2017)
PAF = 15% PAF = 25%
PAF = 80-85% PAF = 5-15%
University of Cape Town Faculty of Health Sciences
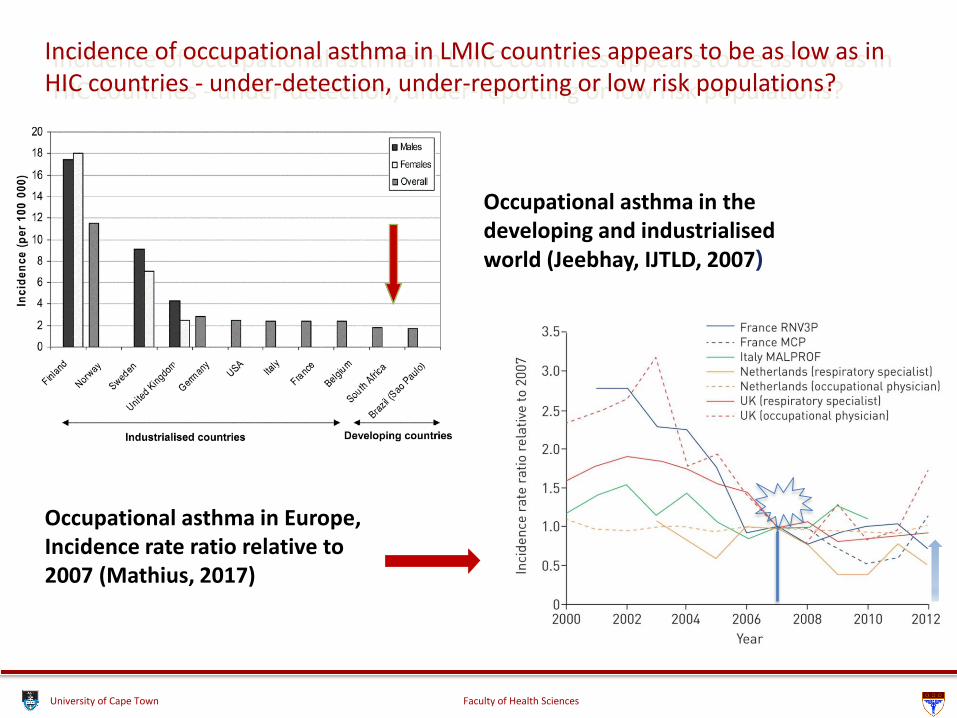
Incidence of occupational asthma in LMIC countries appears to be as low as in HIC countries - under-detection, under-reporting or low risk populations?
Occupational asthma in Europe, Incidence rate ratio relative to 2007 (Mathius, 2017)
Occupational asthma in the developing and industrialisedworld (Jeebhay, IJTLD, 2007)
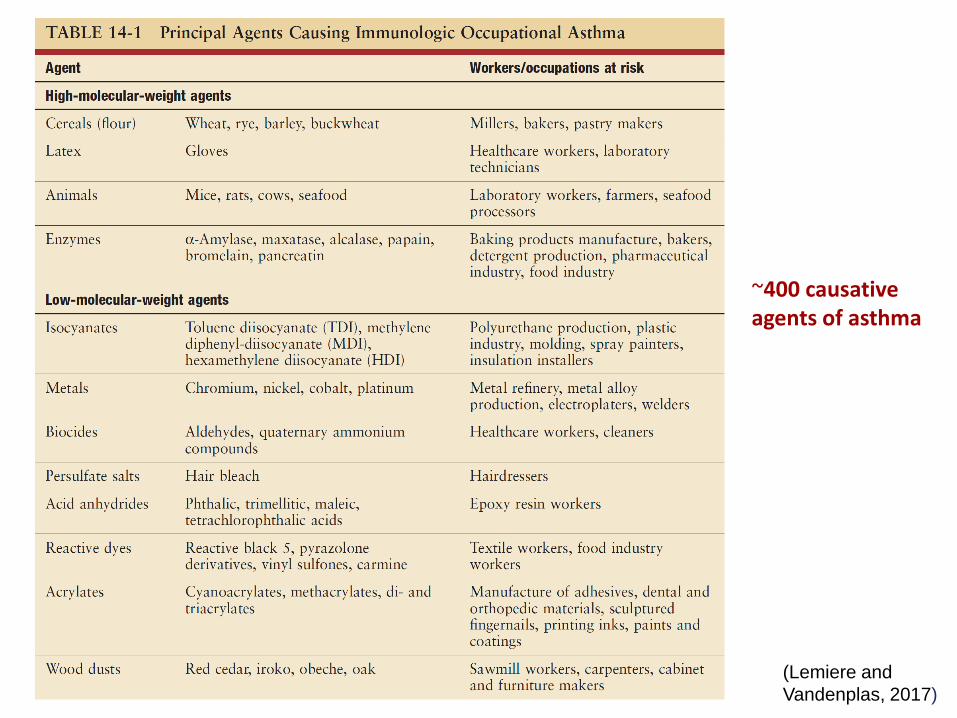
(Lemiere and
Vandenplas, 2017)
~400 causative agents of asthma
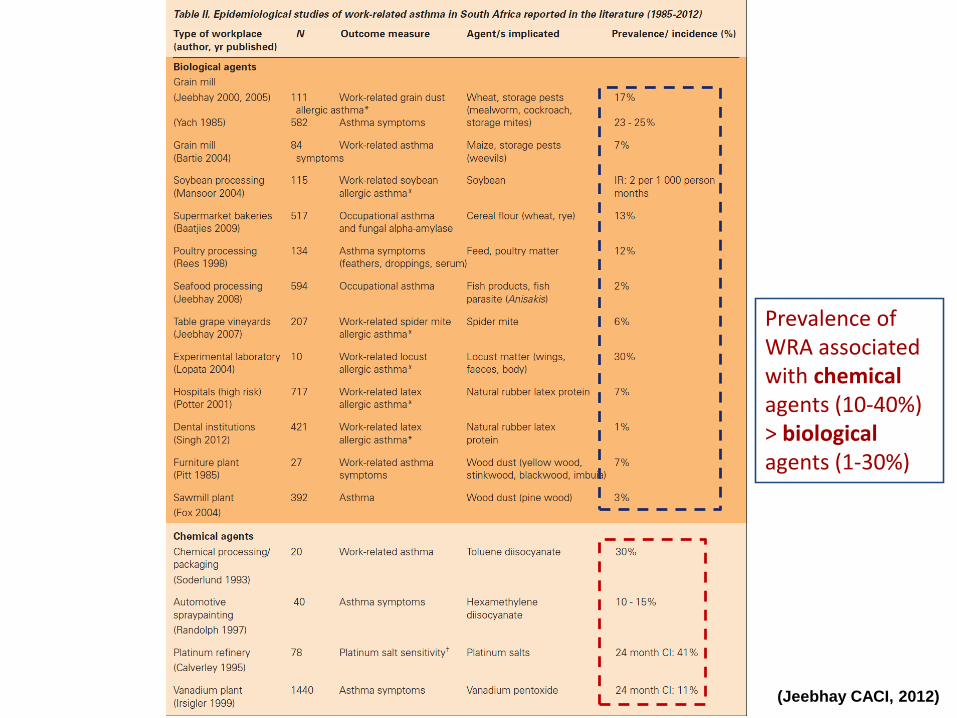
(Jeebhay & Quirce, IJTLD, 2007)(Jeebhay CACI, 2012)
Prevalence of WRA associated with chemicalagents (10-40%)> biologicalagents (1-30%)
University of Cape Town Faculty of Health Sciences
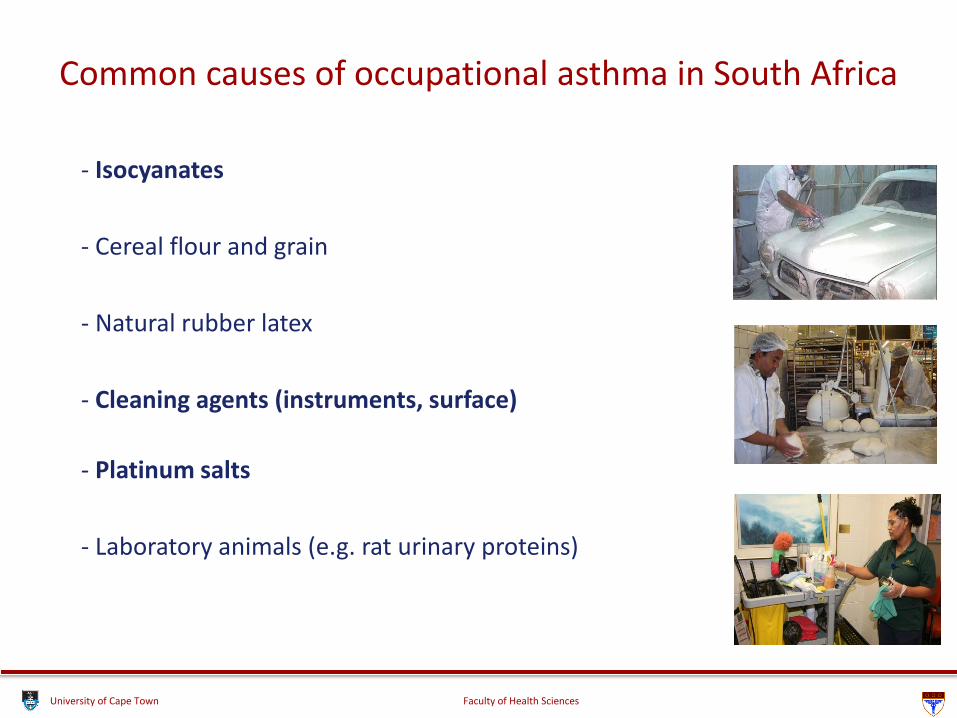
- Isocyanates
- Cereal flour and grain
- Natural rubber latex
- Cleaning agents (instruments, surface)
- Platinum salts
- Laboratory animals (e.g. rat urinary proteins)
Common causes of occupational asthma in South Africa
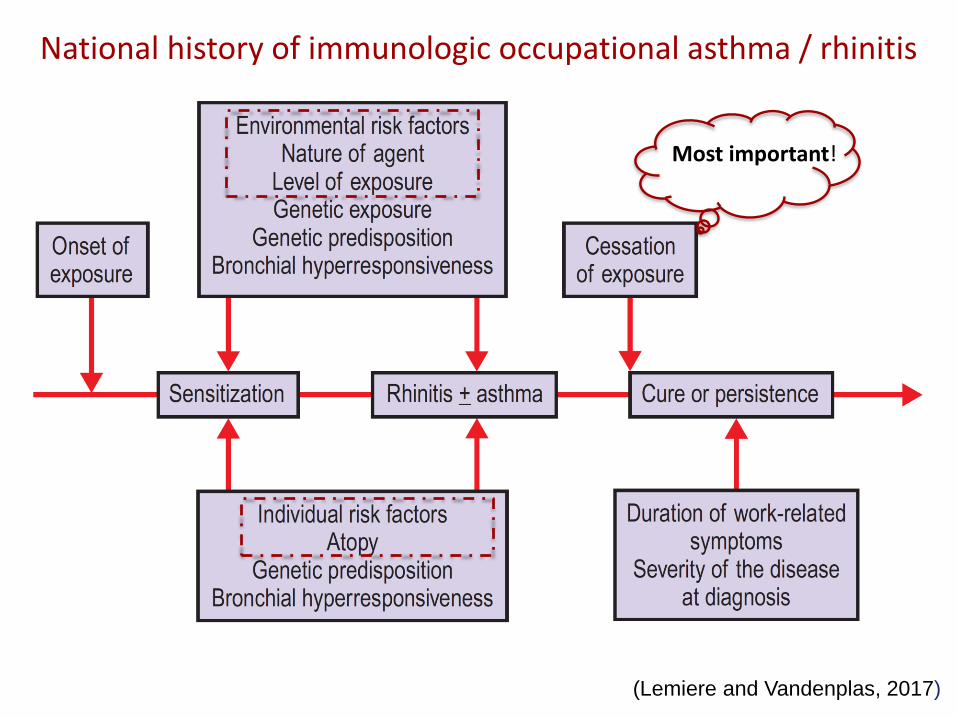
National history of immunologic occupational asthma / rhinitis
(Lemiere and Vandenplas, 2017)
Most important!
University of Cape Town Faculty of Health Sciences
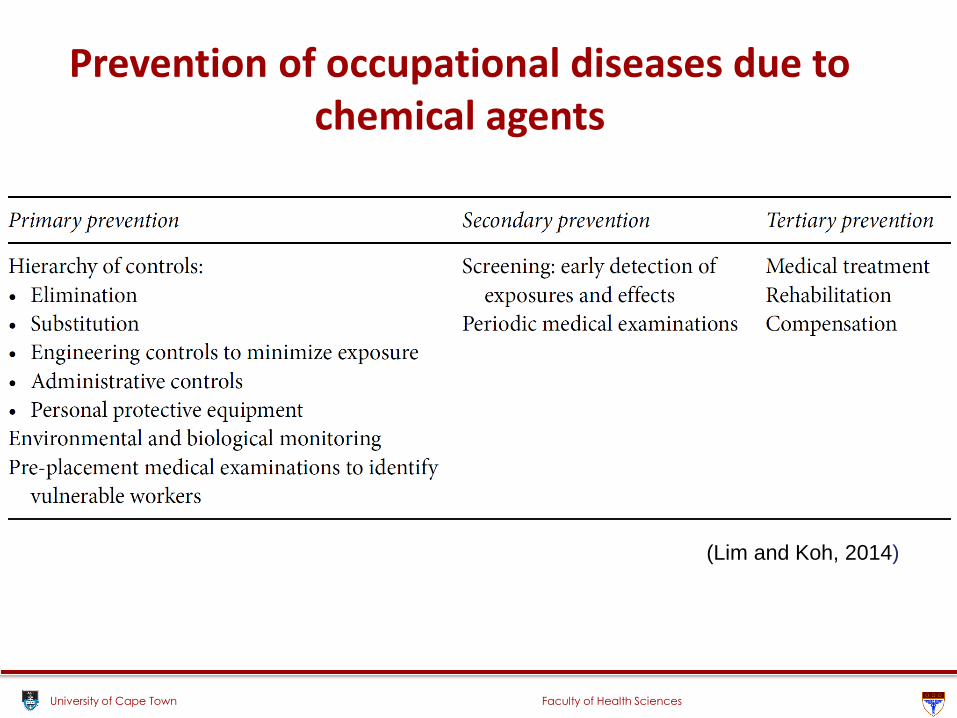
Prevention of occupational diseases due to chemical agents
(Lim and Koh, 2014)
University of Cape Town Faculty of Health Sciences
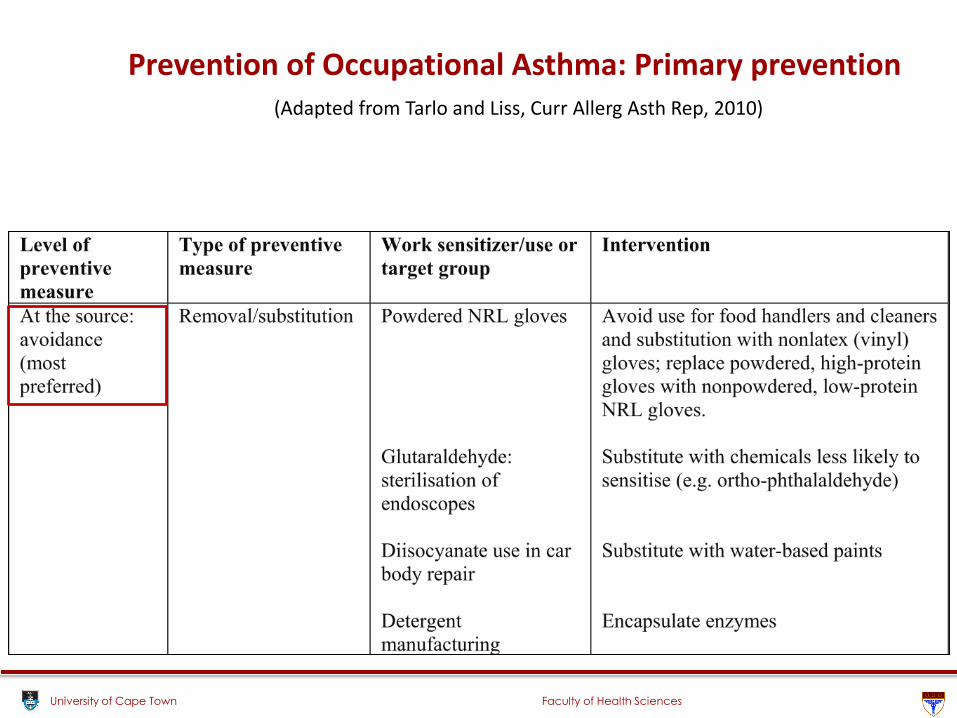
Prevention of Occupational Asthma: Primary prevention(Adapted from Tarlo and Liss, Curr Allerg Asth Rep, 2010)
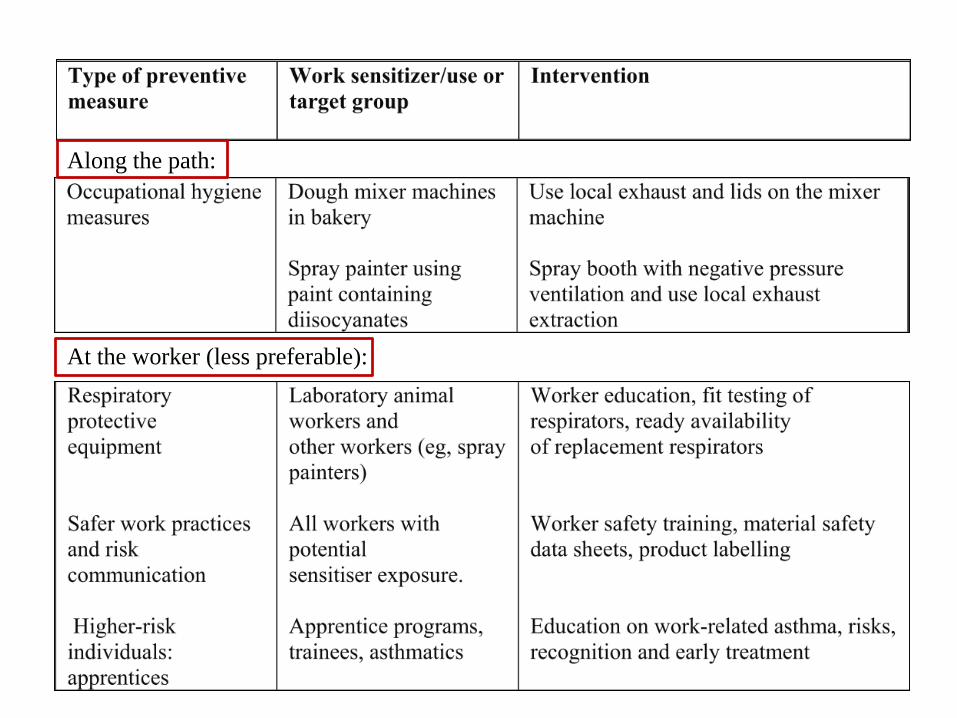
Along the path:
At the worker (less preferable):
University of Cape Town Faculty of Health Sciences
Case Study to illustrate Prevention
University of Cape Town Faculty of Health Sciences
Average current wheat exposure g/m3
0 10 20 30 40 50
Pre
va
len
ce
0.0
0.1
0.2
0.3
0.4
0.5
0.6
Sensitisation to wheat
Allergic chest symptoms
Probable occupational asthma
Allergic ocular-nasal symptoms
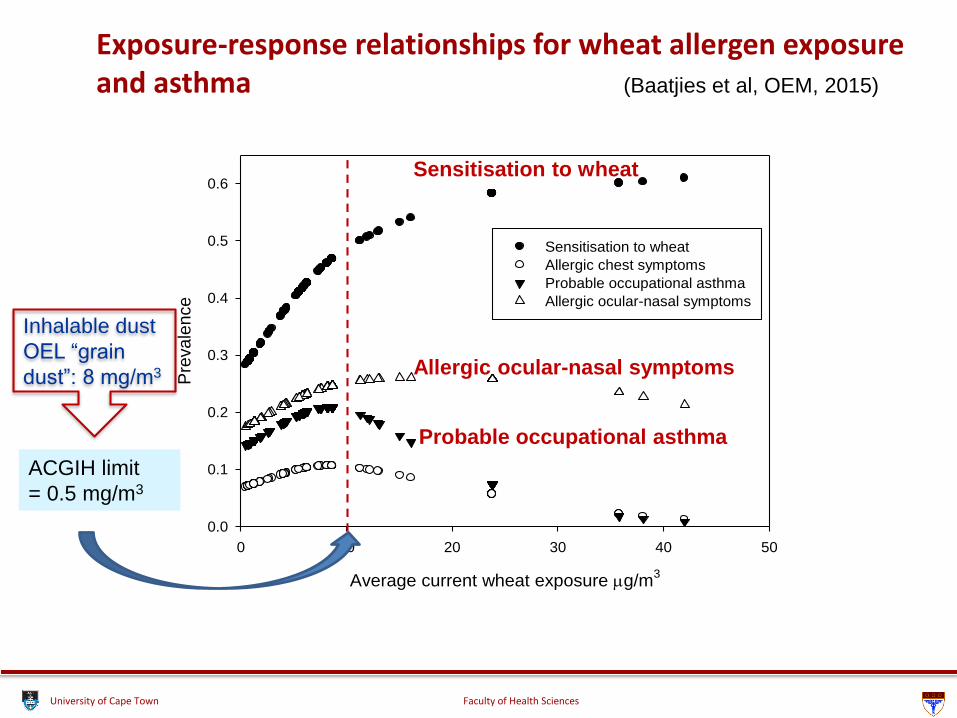
Exposure-response relationships for wheat allergen exposure and asthma (Baatjies et al, OEM, 2015)
Sensitisation to wheat
Allergic ocular-nasal symptoms
Probable occupational asthma
ACGIH limit
= 0.5 mg/m3
Inhalable dust
OEL “grain
dust”: 8 mg/m3
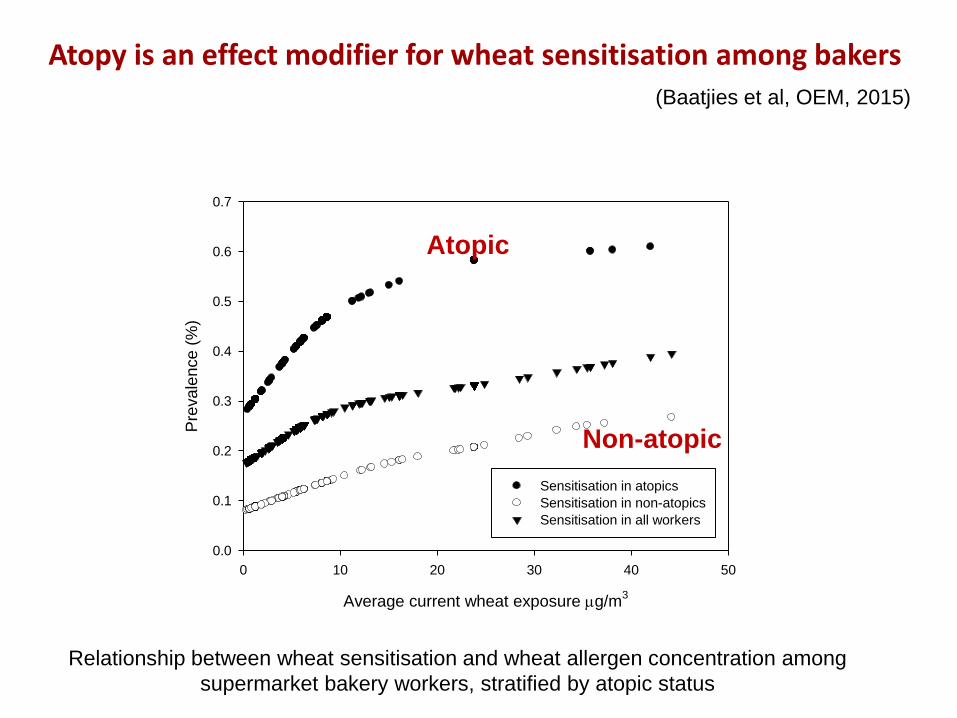
Atopy is an effect modifier for wheat sensitisation among bakers (Baatjies et al, OEM, 2015)
ATOPIC
NON-ATOPIC
Average current wheat exposure g/m3
0 10 20 30 40 50
Pre
vale
nce (
%)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
Sensitisation in atopics
Sensitisation in non-atopics
Sensitisation in all workers
Relationship between wheat sensitisation and wheat allergen concentration among
supermarket bakery workers, stratified by atopic status
Atopic
Non-atopic
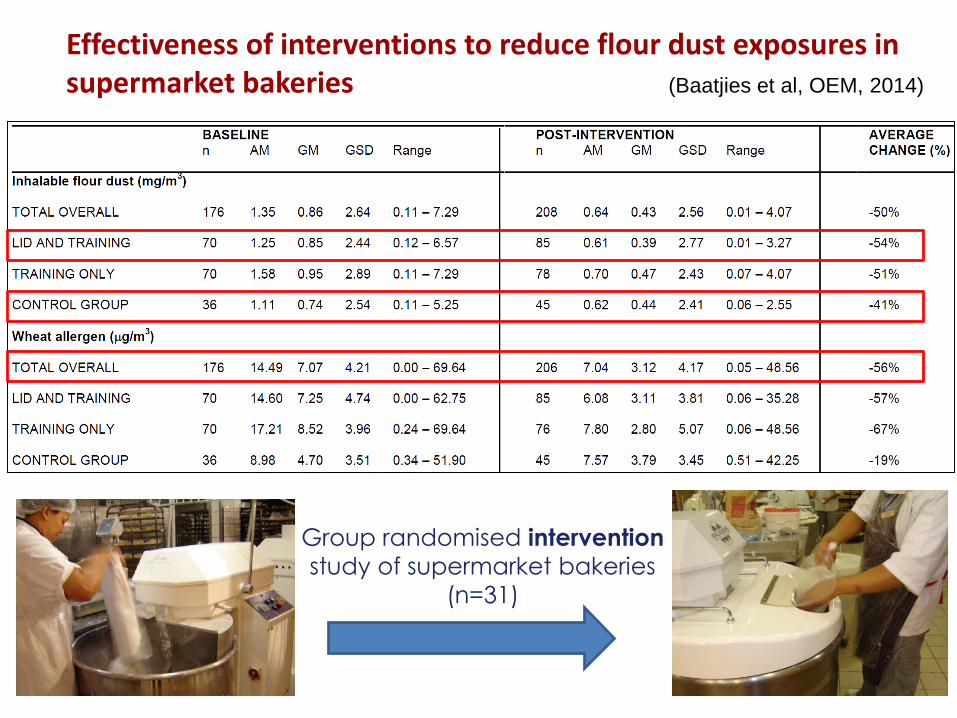
Group randomised intervention
study of supermarket bakeries
(n=31)
Effectiveness of interventions to reduce flour dust exposures in supermarket bakeries (Baatjies et al, OEM, 2014)
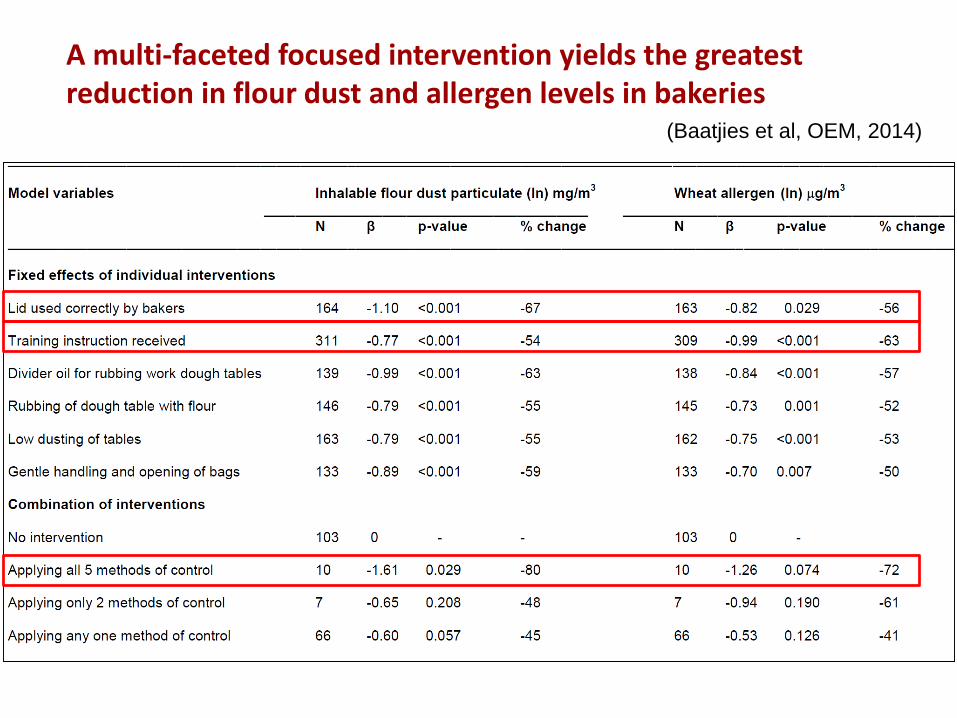
A multi-faceted focused intervention yields the greatest reduction in flour dust and allergen levels in bakeries
(Baatjies et al, OEM, 2014)
University of Cape Town Faculty of Health Sciences
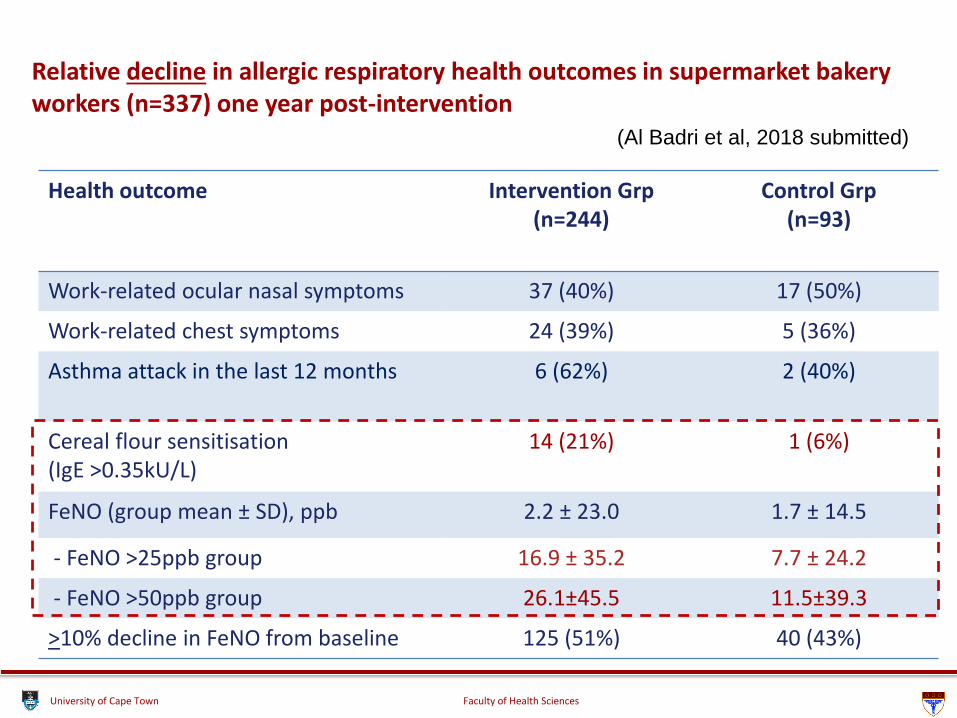
Relative decline in allergic respiratory health outcomes in supermarket bakery workers (n=337) one year post-intervention
(Al Badri et al, 2018 submitted)
Health outcome Intervention Grp (n=244)
Control Grp (n=93)
Work-related ocular nasal symptoms 37 (40%) 17 (50%)
Work-related chest symptoms 24 (39%) 5 (36%)
Asthma attack in the last 12 months 6 (62%) 2 (40%)
Cereal flour sensitisation(IgE >0.35kU/L)
14 (21%) 1 (6%)
FeNO (group mean ± SD), ppb 2.2 ± 23.0 1.7 ± 14.5
- FeNO >25ppb group 16.9 ± 35.2 7.7 ± 24.2
- FeNO >50ppb group 26.1±45.5 11.5±39.3
>10% decline in FeNO from baseline 125 (51%) 40 (43%)
University of Cape Town Faculty of Health Sciences
Strategies for prevention of occupational respiratory disorders due to chemicals in South Africa
University of Cape Town Faculty of Health Sciences
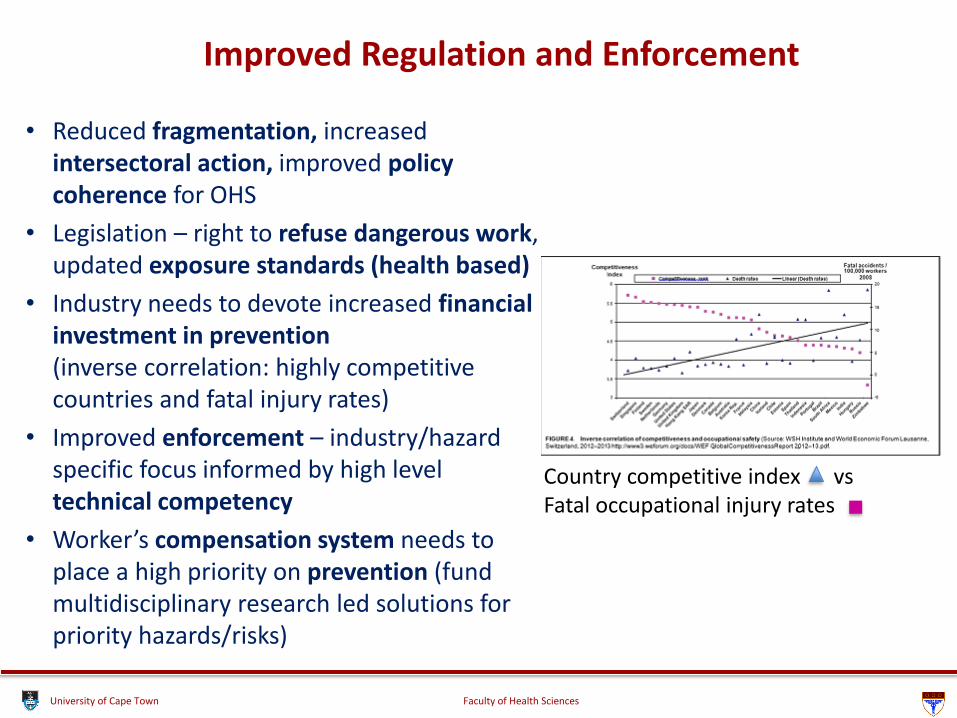
Improved Regulation and Enforcement
• Reduced fragmentation, increased intersectoral action, improved policy coherence for OHS
• Legislation – right to refuse dangerous work, updated exposure standards (health based)
• Industry needs to devote increased financial investment in prevention (inverse correlation: highly competitive countries and fatal injury rates)
• Improved enforcement – industry/hazard specific focus informed by high level technical competency
• Worker’s compensation system needs to place a high priority on prevention (fund multidisciplinary research led solutions for priority hazards/risks)
Country competitive index vs Fatal occupational injury rates
University of Cape Town Faculty of Health Sciences
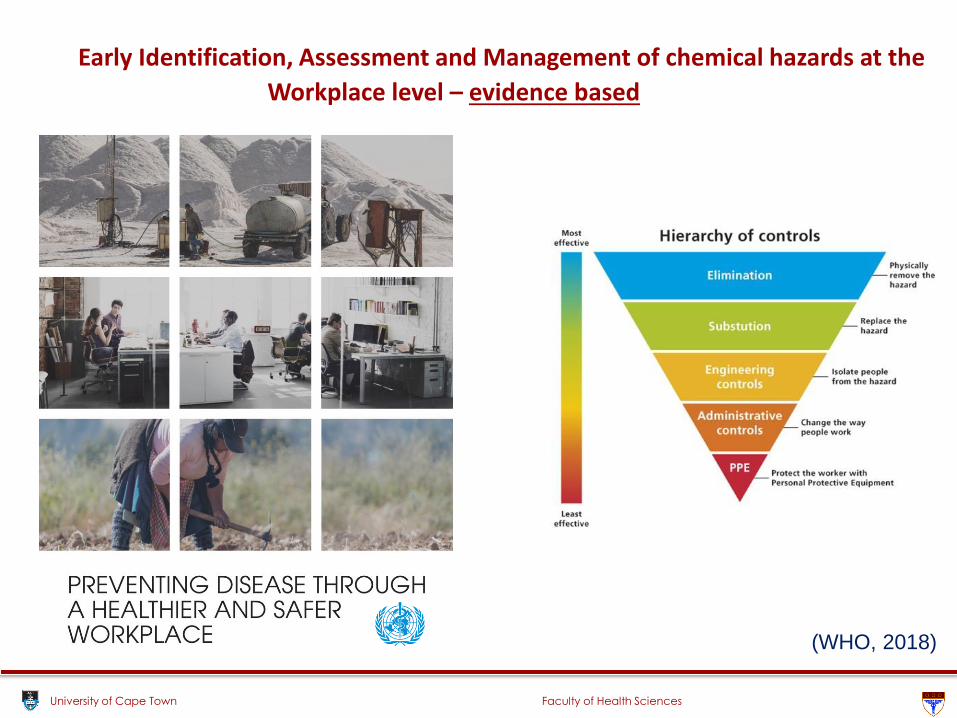
Early Identification, Assessment and Management of chemical hazards at the
Workplace level – evidence based
(WHO, 2018)
University of Cape Town Faculty of Health Sciences
Medical surveillance of high-risk working populations
• Improved medical surveillance protocols – evidence based
• Medical surveillance based on health risk assessment and adequacy of existing control measures
• Targeted medical surveillance on specific key health outcomes as opposed to general “annual medical”
• Linked to workplace control measures (to reduce group risk)
• Post-employment surveillance
University of Cape Town Faculty of Health Sciences
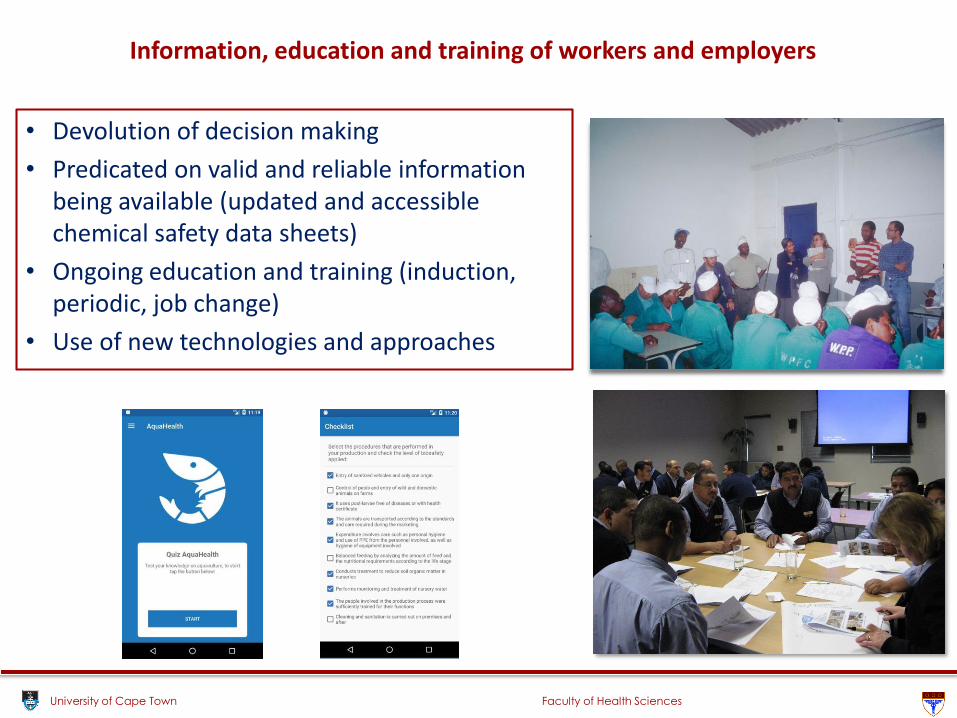
Information, education and training of workers and employers
• Devolution of decision making
• Predicated on valid and reliable information being available (updated and accessible chemical safety data sheets)
• Ongoing education and training (induction, periodic, job change)
• Use of new technologies and approaches
University of Cape Town Faculty of Health Sciences
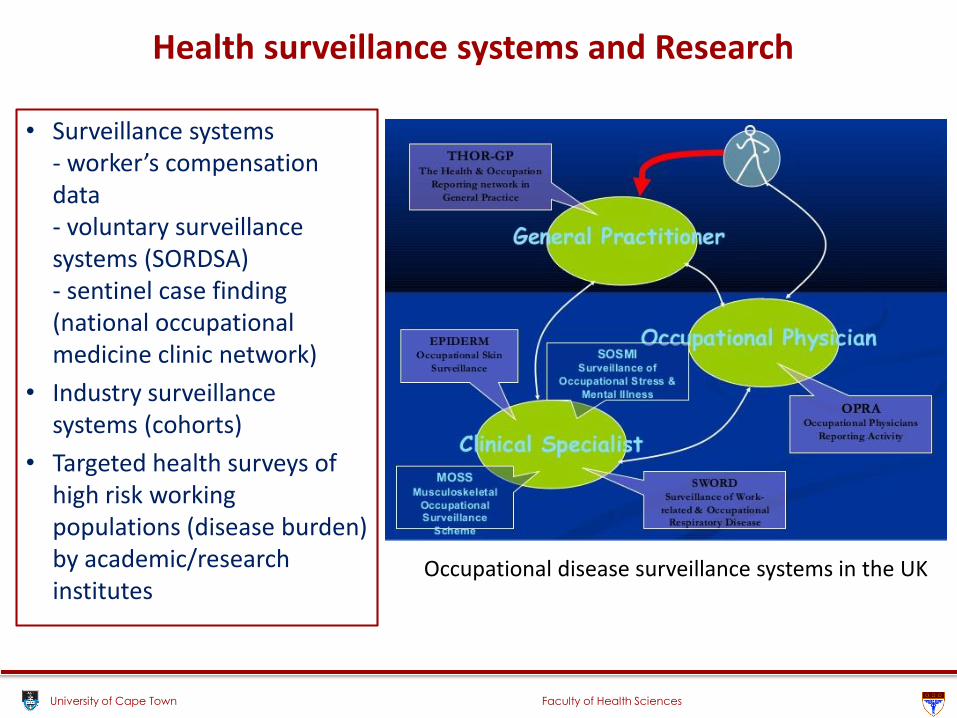
Health surveillance systems and Research
• Surveillance systems- worker’s compensation data- voluntary surveillance systems (SORDSA)- sentinel case finding (national occupational medicine clinic network)
• Industry surveillance systems (cohorts)
• Targeted health surveys of high risk working populations (disease burden) by academic/research institutes
Occupational disease surveillance systems in the UK
cutting edge research world class training and education partnering for patient-centred health services
FACULTY OF HEALTH SCIENCES
UNIVERSITY OF CAPE TOWN
THANK YOU