Embed Size (px)
Citation preview

Obstructive Sleep Apnea
Cory M. Furse, MD, MPH

Disclosure Multiple photographs used
in this presentation have been obtained from GOOGLE.
I have no financial relationships to disclose.
I will be referring to most researchers by first name and/or nickname as if I actually know them.

Objectives
• Review the pathophysiology of obstructive sleep apnea
• Review current recommendations concerning the patient with obstructive sleep apnea for outpatient surgery

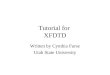
Alae nasi
Tensor palatini
Genioglossis
Geniohyoid
Thyrohyoid
Sternohyoid
Adv Physiol Educ 32: 196–202, 2008Levitsky – LSU
Normal State

Polysomnography• Electroencephalogram• Electrooculogram• Electromyogram of respiratory muscles• Airflow at the nose or mouth via thermistor• End-tidal CO2
• Impedance plethysmography for chest/abdomen movement
• EKG, NIBP, and SpO2
Adv Physiol Educ 32: 196–202, 2008Levitsky – LSU

Polysomnography
Adv Physiol Educ 32: 196–202, 2008Levitsky – LSU

Adv Physiol Educ 32: 196–202, 2008Levitsky – LSU
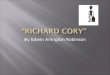
Sleep Apnea Event

Symptoms of OSA Loud snoring
Adv Physiol Educ 32: 196–202, 2008Levitsky – LSU

Adv Physiol Educ 32: 196–202, 2008Levitsky – LSU
Sleep Apnea Event Altered body position
Decreased pharyngeal muscle tone
Respiratory drive depression- MV 16%- SPO2 2%- PaCO2 4-6mmHg
Depression of protective respiratory reflexes during normal Non-REM sleep

DefinitionsOSA: 15 or more apneas/hypopneas per hour during
sleep, caused by collapse of the upper airwayApnea: 10s or more without airflowHypopnea: 50% reduction in thoracoabdominal movement
lasting for 10s
Levitsky – LSU Adv Physiol Educ 32: 196–202, 2008

Curr Opin Anaesthesiol 22:405–411
Epidemiology ~24% of middle-aged men ~9% of middle-aged women ~5% of 3-5yr old children Prevalence of OSA increases with age and
body weight An estimated 85% of people with OSA are
undiagnosed!
Chung – Toronto Western Hospital

Lanphier EH – SUNY at Buffalo J Appl Physiol 18: 471-477, 1963

Lanphier EH – SUNY at Buffalo J Appl Physiol 18: 471-477, 1963

Lanphier EH – SUNY at Buffalo J Appl Physiol 18: 471-477, 1963

Lanphier EH – SUNY at Buffalo J Appl Physiol 18: 471-477, 1963

Symptoms of OSA Loud snoring Hypersomnolence Depressed mentation
Adv Physiol Educ 32: 196–202, 2008Levitsky – LSU

Adv Physiol Educ 32: 196–202, 2008Levitsky – LSU

Levitsky – LSU Adv Physiol Educ 32: 196–202, 2008

Levitsky – LSU Adv Physiol Educ 32: 196–202, 2008

Symptoms of OSA Loud snoring Hypersomnolence and Depressed mentation
– Interference with normal sleep architecture, esp. REM sleep
– Increases risk of motor vehicle accidents Morning Headaches
– Repeated dialation of cerebral blood vessels
Adv Physiol Educ 32: 196–202, 2008Levitsky – LSU

Somers – Iowa J. Clin. Invest. 1995. 96:1897-1904.

Signs of OSA Systemic hypertension
- Chronic recurrent sympathetic stimulation- Increase in endothelin, a potent, long lasting
vasoconstrictor Heart failure
- Right heart 2° to pulmonary HTN- Left heart 2° to systemic HTN
Arrhythmias- Atrial fibrillation
Ann Intern Med. 2005;142:187-197.Caples – Mayo Clinic

Signs of OSA Polycythemia
- Chronic hypoxic episodes stimulate renal release of renin
- Increase in blood viscosity further exacerbating heart failure if present
Metabolic alkalosis- Respiratory acidosis while asleep with renal
retention of bicarbonate ions and excretion of H+
Ann Intern Med. 2005;142:187-197.Caples – Mayo Clinic

Obstructive Sleep Apnea
Signs Systemic HTN Heart Failure Arrhythmias Polycythemia Metabolic Alkalosis
Symptoms Loud Snoring Hypersomnolence Depressed Mentation Morning Headaches Nocturia

Why do we care?• Difficult Intubation
– If GA is employed
• Difficult Sedation– If MAC/Regional is employed
• Postoperative Pain Control– May increase the severity of
their OSA
• Liability?– If a patient with OSA has an
adverse event at home

Gross – Farmington, CT Anesthesiology 2006; 104:1081–93


Endorsed- American Academy of Sleep Medicine- American Academy of Otorhinolaryngology – Head and Neck Surgery
“Affirmation of Value” - American Academy of Pediatrics
Gross – Farmington, CT Anesthesiology 2006; 104:1081–93

Chung – Toronto Western Hospital Curr Opin Anaesthesiol 22:405–411
Identification of Patients with OSA

Identification of Perioperative Risk
Gross – Farmington, CT Anesthesiology 2006; 104:1081–93

Preoperative Preparation
Gross – Farmington, CT Anesthesiology 2006; 104:1081–93
Recommendations- Initiation of CPAP- Use of mandibular advancement devices- Preoperative weight loss
Prior corrective surgery for OSA- Assume these patients are still at risk, unless they
have a normal sleep study Beware of the difficult airway

Liang – MGH Anesthesiology 2008; 108:998–1003

Liang – MGH Anesthesiology 2008; 108:998–1003

Intraoperative Management
Gross – Farmington, CT Anesthesiology 2006; 104:1081–93
Recommendations- Intraoperative medications should be selected
with consideration of the potential for postoperative respiratory compromise
- If moderate sedation is used, consider using the patients CPAP or oral appliance
- Awake extubation- Extubation and recovery in the lateral,
semiupright, or other nonsupine position

Postoperative Management
Gross – Farmington, CT Anesthesiology 2006; 104:1081–93
Recommendations- Regional > Neuraxial > Oral Opioids > Parental
Opioids - Supplemental O2 until at baseline SPO2 on RA- CPAP when feasible- Nonsupine positions- Continuous monitoring of SPO2 when hospitalized

Outpatient Surgery?
Gross – Farmington, CT Anesthesiology 2006; 104:1081–93

Discharge Criteria
Gross – Farmington, CT Anesthesiology 2006; 104:1081–93
Recommendations- SPO2 should return to baseline on RA- Patients should be monitored a median of 3hr
longer then their non-OSA counterparts- Monitoring should continue for a median of 7hr
after last episode of obstruction or hypoxemia while breathing RA in an unstimulating environment

Appendix:
Gross – Farmington, CT Anesthesiology 2006; 104:1081–93
A median of 10% of outpatients would need to be inpatients if these guidelines were followed
73% indicate that sensitivity of the criteria for detecting patients previously undiagnosed with OSA is “about right”
82% indicate that the scoring system for assessing perioperative risk is “about right”

Chung – University of Toronto Anesthesiology 2008; 108:812–21

STOP BANG
S – Snoring, loudly, heard through a closed doorT – Tiredness, during daytimeO – Observed, witnessed apneic episodesP – Pressure, hypertension
B – BMI, > 35A – Age, > 50 yrN – Neck Circumference, > 40 cmG – Gender, Male
Chung – University of Toronto Anesthesiology 2008; 108:812–21

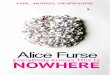
STOP BANG vs. ASA guidelines
Sensitivity AHI >5 AHI >15 AHI >30
STOP-BANG 83.6 92.9 100
ASA Guidelines 72.1 78.6 87.2
Advantage of STOP-BANG is the markedly decreased amount of time required to administer the questionnaire as compared to ASA guideline checklist
Chung – University of Toronto Anesthesiology 2008; 108:822–830

QUESTIONS?