Embed Size (px)
Citation preview

Obstructive Sleep Apnea
and Obesity
Luisito O. Llido, MD, FPCS
Head
Center for Obesity and Weight Management
St. Luke’s Medical Center

Objectives of the presentation
To present prevalence of sleep apnea in the
general population and obese patients
To show the prevalence of obesity in the local
setting
To present the approaches in the management
of obesity
To present outcome data on the outcome of
obesity management in the Philippines
(specifically St. Luke’s Medical Center)
Some practical suggestions

Prevalence of obstructive sleep
apnea in the population
2% of women and 4% of men in the general population Strollo PJ Jr, Rogers RM. Obstructive sleep apnea. N Engl J Med
1996; 334: 99-104.
70% in morbidly obeseFritscher LG, Mottin CC, Canani S, Chatkin JM Obes Surg. 2007
Jan;17(1):95 .
In the Philippines? in St. Luke’s ?– IDK, please ask the other speakers

Prevalence of obesity
Worldwide: BMI > 30: 1.7 billion
number of overweight is equal to the underweights
(Worldwatch Institute)
United States:
2/3 are overweight
Obese = 50 million
Philippines:
21% (PASOO)

Obesity prevalence snap shots
Hospital BMI < 18.5 BMI > 30
Marikina, Rizal 1 38% 15%
Lipa City, Batangas 2 48%
Quezon City 3 22% 20%
1. Amang Rodriguez Medical Center (n = 61)
2. Mary Mediatrix Medical Center (n = 2,345)
3. St. Luke’s Medical Center (n = 41,676)

Overweight and obesity
in St. Luke’s Medical Center

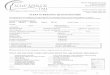
Obesity in pediatric patients of
St. Luke’s Medical Center
• Y2000, n = 4678
• Y2003, n = 3770
Obesity pattern per age group: y2000, 2003, 2005,2006 (slmc)
0%
5%
10%
15%
20%
25%
30%
35%
40%
1yr 2yr 3yr 4yr 5yr 6yr 7yr 8yr 9yr 10yr 11yr 12yr 13yr 14yr 15yr 16yr 17yr 18yr
age group
pe
rce
nt
of
tota
l
y2000_%
y2003_%
y2005_%
y2006_%
Log. (y2000_%)
Log. (y2003_%)
Log. (y2005_%)
Log. (y2006_%)
• 1 to 2 y/o = 33%
• 18 y/o = 12% to 15%
• Y2005, n = 4006
• Y2006, n = 2151

Stroke 1.6
Low mood poor self esteem
Hypertension 2.9
Coronary heart disease 2.5
Thromboembolism 1.5
Heart failure 1.5
Infertility
Pregnancy problems 2.0
Cancer of uterus 4.6
Menorrhagia 1.8
Diabetes mellitus 10
Dyslipidemias 1.5
Hyperinsulinemia
Gallstones 2.7
Cancer of colon 1.5
Cancer of pancreas 1.6
Kidney disease
Breast cancer 1.3
Hypoventilation
Sleep apnea
Breathlessness 3.5
Hirsutism 2
Sweating
Obesity complications, relative risk

Multidisciplinary:
nutrition support
endocrinologist
cardiac rehab
pulmonologist
psychiatrist
physiatrist
pediatrician
surgeon
physical therapist
nurse
dietitian

Management of obesity
SCREENING
NON-SURGICAL
• diet
• exercise
• drugs
• behavioral mx
SURGICAL
BMI > 30
Adult and pediatric: Failed
non-surgical programs
BMI 30 – 34.9 with
co-morbidity
Balloon?

Non-surgical program

Pediatric obese: outcomePatient Profile and baseline values
Total patients 46
Age Range 5 to 17 years; Median: 14 yrs
(95% LCL: 11 yrs, 95% UCL: 15 yrs)
Pre-adolescent (5-9 years) 9 (20%)
Early Adolescent (10-13 years) 14 (30%)
Mid Adolescent (14-16 years) 19 (41%)
Late Adolescent (17-18 years) 4 (9%)
Male to female ratio (29M : 17F) or 1.7 to 1
Tan-Ting A, Llido LO, Gepte AT. Outcome of Ambulatory Weight Management Program in Obese Children

Pediatric obese: outcome
Figure 1: Number of sessions versus outcome; * P < 0.05, One Way ANOVA;
** P < 0.05, Wilcoxon Rank Sum Test.
Tan-Ting A, Llido LO, Gepte AT. Outcome of Ambulatory Weight Management Program in Obese Children

Weight loss: bariatric surgery
Obesity Surgery in the Philippines: Experience in a Private Tertiary Care Hospital for Years
2002 to 2004. Dineros H, MD; Sinamban R, Siozon M, Llido L, Yumang E, Gregorio IV AE,
Cacas Jr R.. Obesity Surgery, 17, 82-87.

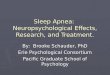
Weight Loss: comparison between non-surgical
and surgical programs
0
5
10
15
20
25
30
35
30d 60d 90d 120d 150d 180d 270d 360d >360d
Time interval
Wt
Lo
ss
(k
g)
Non_Surg
Surg
Experience of multidisciplinary approach to weight management,
St. Luke’s Medical Center; report for years 2003 to 2006
Non-surgical vs. surgical

Body composition changes: non surgical
weight loss program
*

Effect of weight loss on sleep apnea
Prospective, randomized, one year follow up study
(n=72)
Method of weight loss: (grp1) counselling alone vs.
(grp2) counselling + very low calorie diet
Result:
Weight loss: grp1 = -6.5 kg; grp2 = -10.7 kg
BMI change: grp1 = -2.1 units; grp2 = 3.5 units
Improvement in Apnea-Hypopnea Index (AHI): OR 0.24 (95%
CI 0.08-0.72, P=0.011) in group 2
Tuomilehto HP, Seppa JM, Partinen MM et al. Lifestyle Intervention with
Weight Reduction-First Line Treatment in Mild Obstructive Sleep Apnea.
Am J Respir Crit Care Med. 2008.

How to control your weight
Count your calories – if you don’t know
how, consult/ask our clinical dietitians or
clinical nutrition fellows
Exercise – don’t take the elevator, leave
this to the old and weak people
Check your family history – if there is a
diabetic or obese, the statistical chance of
you becoming one is highly significant

Physical activity and risks to obesity and
diabetes
24
14
5 7
-9-12
-24
-34-40
-30
-20
-10
0
10
20
30
Obesity Risk Diabetes Risk
pe
rce
nt
2 hrs w atching TV
Sitting at w ork
2 hrs standing/
w alking (home)
1 hr brisk w alking
JAMA 2003; 289, 1785-1791

Conclusion
Obesity is on the rise from the pediatric to the
adult population
We can deal with it – for those who are far gone
into the problem, there are several ways of
dealing with it
Obesity management is best managed with a
multidisciplinary approach
Managing complications related to obesity is
expensive and difficult; prevention always gives
the best outcome for you