Embed Size (px)
Citation preview

INDEX
INTRODUCTION TO RESPIRATORY DISEASES
INTRODUCTION TO OBSTRUCTIVE DISEASES
ANATOMY OF RESIRATORY SYSTEM
PHYSIOLOGY OF RESPIRATION
TYPES & DEFINITIONS
EPIDEMIOLOGY
RISK FACTORS
PATHOLOGY
PATHOGENESIS
SIGNS AND SYMPTOMS
STAGES OF COPD
COMPLICATIONS OF COPD
OTHER TYPES OF OBSTRUCTIVE DISEASE
DIAGNOSIS OF OBSRUCTIVE DISEASES
DIFFERENTIAL DIAGNOSIS
CLINICAL MANAGEMENT
PHYSIOTHERAPY ASSESSMENT
PHYSIOTHERAPY MANAGEMENT
CONCLUSION
BIBILOGRAPHY

INTRODUCTION TO RESPIRATORY DISEASE
Respiratory Diseases can be broadly divided into
OBSTRUCTIVE TYPE
&
RESTRICTIVE TYPE
OBSTRUCTIVE DISEASE
It include conditions in which there is a
resistance to air flow either through reversible factors such
as bronchospasm or inflammation or through irreversible
factors such as airway fibrosis or loss of elastic recoil owing
to damage to the airway and the alveoli.
RESTRICTIVE DISORDERS
These are characterised by reduced
lung compliance leading to the loss of lung volume, which
may be caused by disease affecting the lungs, pleura, chest
wall or neuromuscular mechanisms.

INTRODUCTION TO COPD
Chronic obstructive lung disease
(COLD), also known as chronic obstructive pulmonary disease
(COPD), is characterized by a limitation of the airflow in the
lung, which develops over time and is not totally reversible.
The major diseases in this category are:
EMPHYSEMA
CHRONIC BRONCHITIS
ASTHAMATIC BRONCHITIS
BRONCHIECTASIS
CYSTIC FIBROSIS
NOTE :-
EMPHYSEMA & CHRONIC BRONCHITIS comes under
chronic obstructive pulmonary disease hence they are shown under
a common heading COPD.
PLEASE CONSIDER

DEFINITION
CHRONIC BRONCHITIS :-
It is defined as chronic cough and expectoration
for at least 3 months a year for at least 2 successive years.
EMPHYSEMA :-
It is defined as chronic respiratory disease where there is
over-inflation of the air sacs (alveoli) in the lungs, causing a decrease in
lung function, and often, breathlessness.
ASTHMATIC BRONCHITIS :-
It is defined as acute episode of airway obstruction is
characterized by airway hyperactivity to various stimuli that results in
recurrent wheezing brought about by edema and bronchospasm.
BRONCHIECTASIS:-
It is defined as a condition that is characterised by the
permanent dilatation of the bronchi associated with destruction of elastic
and muscular components of their walls, usually due to acute or chronic
infection.
CYSTIC FIBROSIS :-
It is defined as a hereditary disorder of exocrine glands,
with high sodium chloride content in sweat and pancreatic insufficiency,
resulting in mal-absorption. There is hypertrophy and hyperplasia of
mucus-secreting glands, resulting in excessive mucus production in the

lining of bronchi, which predisposes the patient to chronic
bronchopulmonary infection.
Anatomy & Physiology of the
Respiratory System
Human Respiratory System
The respiratory system consists of
all the organs involved in breathing. These include the nose, pharynx,
larynx, trachea, bronchi and lungs.
The respiratory system does two very important things: it brings oxygen
into our bodies, which we need for our cells to live and function properly;
and it helps us get rid of carbon dioxide, which is a waste product of
cellular function.
The nose, pharynx, larynx, trachea and bronchi all work like a system of
pipes through which the air is funnelled down into our lungs. There, in
very small air sacs called alveoli, oxygen is brought into the bloodstream
and carbon dioxide is pushed from the blood out into the air.

The Upper Airway and Trachea
During breathing, air enters into body through nose or
mouth. From there, it travels down your throat through the larynx
(or voice box) and into the trachea (or windpipe) before entering
into the lungs. All these structures act to funnel fresh air down from
the outside into the body.
The upper airway is important because it must always stay
open to be able to breathe. It also helps to moisten and warm the
air before it reaches the lungs.

The Lungs
Structure
The lungs are paired, cone-shaped organs which take up most of
the space in our thorax, along with the heart.
Their role is to take oxygen into the body, which we need for our
cells to live and function properly, and to help us get rid of carbon
dioxide, which is a waste product.
We have two lungs, a left lung and a right lung. These are divided
up into 'lobes', or big sections of tissue separated by 'fissures' or
dividers. The right lung has three lobes but the left lung has only
two, because the heart takes up some of the space in the left side
of our chest.
The lungs can also be divided up into even smaller portions, called
'bronchopulmonary segments'. These are pyramidal-shaped areas
which are also separated from each other by membranes. There
are about 10 of them in each lung. Each segment receives its own
blood supply and air supply.

Physiology of Breathing
When a person inhales, air travels through the following pathways
into the lungs:
Air is carried from the trachea (the windpipe) into the lung through
flexible airways called bronchi.
Like the branches of a tree, bronchi divide successively into over a
million smaller airways called bronchioles.
The bronchioles lead to grape-like clusters of microscopic sacs
called alveoli.
In each adult lung there are millions of these tiny alveoli. The thin
membrane of the alveoli allows oxygen and carbon dioxide to pass
to and from capillaries.
During deep inhalation, the elastic alveoli unfold and unwind
to allow this passage to occur
Capillaries, the smallest of our blood vessels, carry blood
throughout the body. Red blood cells carry oxygen throughout the
body, and return carbon dioxide to the lungs; white blood cells are
the critical infection fighters in our body.

Mechanics of Breathing
To take a breath in, the external intercostal muscles
contract, moving the ribcage up and out.
The diaphragm moves down at the same time, creating
negative pressure within the thorax.
The lungs are held to the thoracic wall by the pleural
membranes, and so expand outwards as well.
This creates negative pressure within the lungs, and so air
rushes in through the upper and lower airways.

Expiration is mainly due to the natural elasticity of the
lungs, which tend to collapse if they are not held against
the thoracic wall.
This is the mechanism behind lung collapse if there is air
in the pleural space (pneumothorax).
The Respiratory System Through the Ages
Breathing for the Premature Baby
When a baby is born, it must convert from getting all of its oxygen
through the placenta to absorbing oxygen through its lungs. This is
a complicated process, involving many changes in both air and
blood pressures in the baby's lungs. For a baby born preterm
(before 37 weeks gestation), the change is even harder. This is
because the baby's lungs may not yet be mature enough to cope

with the transition. The major problem with a preterm baby's lungs
is a lack of something called 'surfactant'. This is a substance
produced by cells in the lungs which helps keep the air sacs, or
alveoli, open. Without surfactant, the pressures in the lungs
change and the smaller alveoli collapse.
This reduces the area across which oxygen and carbon dioxide
can be exchanged, and not enough oxygen will be taken in.
Normally, a foetus will begin producing surfactant from around 28-
32 weeks gestation.
When a baby is born before or around this age, it may not have
enough surfactant to keep its lungs open. The baby may develop
something called 'Neonatal Respiratory Distress Syndrome', or
NRDS.
Signs of NRDS include tachypnoea (very fast breathing), grunting,
and cyanosis (blueness of the lips and tongue). Sometimes NRDS
can be treated by giving the baby artifically made surfactant by a
tube down into the baby's lungs.
The Respiratory System and Ageing
The normal process of ageing is associated with a number of
changes in both the structure and function of the respiratory
system. These include:
Enlargement of the alveoli. The air spaces get bigger and lose
their elasticity, meaning that there is less area for gases to be
exchanged across. This change is sometimes referred to as 'senile
emphysema'.

The compliance (or springiness) of the chest wall decreases, so
that it takes more effort to breathe in and out.
The strength of the respiratory muscles (the diaphragm and
intercostal muscles) decreases. This change is closely connected
to the general health of the person.
All of these changes mean that an older person might have
more difficulty coping with increased stress on their respiratory
system, such as with an infection like pneumonia, than a younger
person would.
EPIDEMIOLOGY

Chronic Obstructive Pulmonary Disease (COPD) is one of the
leading causes of morbidity and mortality in the industrialized and the
developing countries.
COPD has been estimated to be the number FOUR to
cerebrovascular diseases in the World to cause death. In 2020
COPD will probably become the third leading cause of death all
over the world, following the trend of increasing prevalence of lung
cancer.
The impact of this respiratory disease worldwide is expected to
increase with a heavy economic burden on individuals and society.
In most of the world, COPD prevalence and mortality are still
increasing and likely will continue to rise in response to increases
in smoking, particularly by women and adolescents.
Morbidity :- The limited data that are available indicate
that morbidity due to COPD increases with age and is greater in
men than women
Mortality :- COPD is currently the fourth leading cause of
death in the world , and further increases in the prevalence and
mortality of the disease can be predicted in the coming decades
RISK FACTORS of COPD :-

Exposure to tobacco smoke :-
The most significant risk factor for COPD is long-term
cigarette smoking. The more years you smoke and the more packs you
smoke, the greater your risk. Symptoms of COPD usually appear about
10 years after you start smoking. Pipe smokers, cigar smokers and
people exposed to large amounts of second hand smoke also are at risk.
Occupational exposure to dusts and chemicals :-
Long-term exposure to chemical fumes, vapours and dusts can irritate and inflame your lungs.
Gastro oesophageal reflux disease (GERD ) :-
This condition is a severe form of acid reflux the backflow of acid and other stomach contents into your oesophagus. GERD can make COPD worse and may even cause it in some people.
Age:-
COPD develops slowly over years, so most people are at least 40 years old when symptoms begin.

Genetics:-
A rare genetic disorder known as alpha-1-antitrypsin deficiency is the source of a few cases of COPD. Researchers suspect that other genetic factors may also make certain smokers more susceptible to the disease.
Cigarette smoking:-
The primary cause of COPD is exposure to tobacco
smoke Clinically significant COPD develops in 15% of
cigarette smokers.
Age of initiation of smoking, total pack-years, and current
smoking status predict COPD mortality. People who smoke
have a greater annual decline in FEV1. Overall, tobacco
smoking accounts for as much as 90% of the risk.
Second hand smoke, or environmental tobacco smoke,
increases the risk of respiratory infections, augments asthma
symptoms, and causes a measurable reduction in pulmonary
function.
Air pollution:-
Although the role of air pollution in the etiology of COPD is
unclear, the effect is small when compared to cigarette
smoking.
The use of solid fuels for cooking and heating may result in
high levels of indoor air pollution and the development of
COPD.
Airway hyper responsiveness:-

Airway hyper responsiveness (i.e., Dutch hypothesis)
stipulates that patients who have nonspecific airway hyper
reactivity and who smoke are at increased risk of developing
COPD with an accelerated decline in lung function.
Nonspecific airway hyper reactivity is inversely related to
FEV1 and may predict a decline in lung function.
The possible role of airway hyper responsiveness as a risk
factor for the development of COPD in people who smoke is
unclear. Moreover, bronchial hyper reactivity may result from
airway inflammation observed with the development of
smoking-related chronic bronchitis.
Alpha1-antitrypsin deficiency : -
AAT deficiency is the only known genetic risk factor for
developing COPD and accounts for less than 1% of all cases
in the United States. AAT is a protease inhibitor produced by
the liver that acts predominantly by inhibiting neutrophil
elastase in the lungs.
CLASSIFICATION
Emphysema can be classified into primary and secondary.
However, it is more commonly classified by location.
Emphysema can be subdivided into panacinary and centroacinary
(or panacinar and centriacinar, or centrilobular and panlobular).
Panacinary (or panlobular) emphysema is related to the destruction
of alveoli, because of an inflammation or deficiency of alpha 1-

antitrypsin. It is found more in young adults who do not have
chronic bronchitis.
Centroacinary (or centrilobular) emphysema is due to destruction of
terminal bronchiole mucosis, due to chronic bronchitis. This is found
mostly in elderly people with a long history of smoking or extreme
cases of passive smoking.
Other types include distal acinar and irregular.
A special type is congenital lobar emphysema (CLE).
Congenital lobar emphysema
CLE is results in overexpansion of a pulmonary lobe and resultant
compression of the remaining lobes of the ipsilateral lung, and
possibly also the contra lateral lung. There is bronchial narrowing
because of weakened or absent bronchial cartilage.
CLE is potentially reversible, yet possibly life-threatening, causing
respiratory distress in the neonate.
PATHOLOGY
Airway Pathology in COPD Pathway
The pathological hallmarks of COPD are destruction of the lung
parenchyma, which characterizes emphysema, inflammation of the
peripheral airways, which characterizes bronchiolitis, and inflammation
of the central airways which characterizes chronic bronchitis.

Functional consequence of these abnormalities is expiratory airflow
limitation.
As flow is the result of a driving pressure (elastic recoil of the lung) and
of an opposing resistance (airway obstruction), it is best to refer to the
changes in flow seen in smokers as airflow limitation, rather than airflow
obstruction, since both loss of elastic recoil and increase in airway
resistance play an important role in the observed decrease in flow .
Emphysema will contribute to the airflow limitation by reducing the
elastic recoil of the lung through parenchyma destruction, as well as by
reducing the elastic load applied to the airways through destruction of
alveolar attachments.
On the other hand, bronchiolitis will contribute to the airflow limitation by
narrowing and obliterating the lumen and by actively constricting the
airways. The role of symptoms of chronic bronchitis in the development
of chronic airflow limitation is still controversial. In fact, chronic sputum
production has traditionally been considered to be irrelevant to the
development of chronic airflow limitation.
However, a recent study has shown that chronic sputum production was
significantly associated with both an increased decline in FEV1 and an
increased risk of subsequent hospitalization because of COPD,
suggesting a causal role of mucus hyper secretion in the development of
chronic airflow limitation in smokers.

PATHOGENESIS
Chronic obstructive pulmonary disease
(COPD) is characterized and defined by limitation of expiratory
airflow.

This can result from several types of anatomical lesions, including
loss of lung elastic recoil and fibrosis and narrowing of small
airways.
Inflammation, oedema, and secretions also contribute variably to
airflow limitation. Smoking can cause COPD through several
mechanisms.
First, smoke is a powerful inducer of an inflammatory response.
Inflammatory mediators, including oxidants and proteases, are
believed to play a major role in causing lung damage.
Smoke can also alter lung repair responses in several ways.
Inhibition of repair may lead to tissue destruction that
characterizes emphysema, whereas abnormal repair can lead to
the peribronchiolar fibrosis that causes airflow limitation in small
airways.
Genetic factors likely play a major role and probably account for
much of the heterogeneity susceptibility to smoke and other
factors. Many factors may play a role, but to date, only alpha-1
protease inhibitor deficiency has been unambiguously identified.
Exposures other than cigarette smoke can contribute to the
development of COPD. Inflammation of the lower respiratory tract
that results from asthma or other chronic disorders may also
contribute to the development of fixed airway obstruction.
COPD is not only a disease of the lungs but is also a systemic
inflammatory disorder. Muscular weakness, increased risk for
atherosclerotic vascular disease, depression, osteoporosis, and

abnormalities in fluids and electrolyte balance may all be
consequences of COPD.
Advances in understanding the pathogenesis of COPD have the
potential for identifying new therapeutic targets that could alter the
natural history of this devastating disorder.
SIGNS and SYMPTOMS
Many of the signs of COPD are caused by the body's attempt to
compensate for a damaged respiratory system.
Symptoms develop as a direct result of disease processes

SIGNS
Signs of COPD are consequences of the anatomical changes
caused by the disease processes
Barrel chest
Pursed-lip breathing
Productive cough and
Cyanosis
Barrel-chest :-
One telling sign is the change in the shape of the chest, known as
barrel chest.
When the lungs become enlarged, the diaphragm is displaced
downward and able to contract efficiently.
Then the chest wall is enlarged, making the accessory muscles
(muscles in the neck, upper chest, and between the ribs) less
efficient as well.
These changes contribute to shortness of breath. This becomes
apparent when a person with COPD tries do something with the
arms raised above the head, such as changing a light bulb in a
ceiling fixture, and becomes short of breath.
To compensate, a person with COPD often sits leaning forward
with their arms supported on a surface in front of them or on their
knees. This stabilizes the upper chest and shoulders and allows
them to use accessory respiratory muscles more efficiently.

Pursed-lip breathing :-
Because airflow out of the lungs becomes limited,
exhalation takes longer. Because the alveoli lose their elasticity,
one tries to shorten the time needed for exhalation by forcefully
exhaling.
Unfortunately, forced exhalation increases pressure on the lungs
and causes structurally weakened airways to collapse. To prevent
airways from closing during forced exhalation, pursed-lip breathing
is used.
In this the lips are narrowed together, which slows exhalation at
the mouth. This keeps positive pressure in the airways, thus
preventing their collapse and allowing some forced exhalation.
Productive cough :-
A productive cough is caused by inflammation and
excessive amounts of mucus in the airways. Coughing becomes
less effective because of
obstructed airflow.
Cyanosis :-
People who have a poor supply of oxygen usually have a
bluish tinge to their skin, lips, nail beds. Called cyanosis.
Symptoms

Shortness of Breath (Dyspnea)
Dyspnea, the most common symptom of COPD.
It comes on gradually and is first noticed during physical exertion
or during acute exacerbations. So it usually begins at60s and. 70s
and slowly becomes more prominent .
It is closely associated with lung function decline and it is not
always associated with low oxygen in the blood.
Patients often wonder why Dyspnea occurs so long after beginning
to smoke, say 50 to 60 years later.
Some patients have even quit smoking several years before
symptoms appear.
The main reason is that lung function declines slowly with age,
even in a nonsmoker.
At approximately age 30, people begin to lose lung function at
expiratory volume in 1 second FEV1.
People who smoke lose lung function at a more rapid rate,
approximately 125 mL/year.
Because the lungs have a considerable amount of reserve, a
large portion must become nonfunctional before symptoms occur.
If can take more than 30 years to lose enough Lung function to
experience symptoms.
Chronic Cough:-

Chronic cough typically begins as morning cough
and slowly progresses to an all-day cough.
The cough usually produces small amounts of
sputum (less than 60ml/day) and is clear or whitish but may be
discolored.
Sputum production decreases when one quits smoking.
Wheezing :-
It is a high pitched sound of air passing through narrowed
airways. A person with copd may wheeze during on acute
exacerbation or chronically.
Sometimes the wheezing is heard only at night or with exertion.
Hemoptysis :-
COPD is one of the more common causes of hemoptysis
(coughing up blood).
It usually occurs during an acute exacerbation, when there is a lot
of coughing with purlent sputum (sputum containing pus).
Usually, there are only very small amounts of blood streaking the
sputum. Hemoptysis may be a sign of lung cancer in a patient with
COPD, so any blood appearing in the sputum should be brought to
a doctor's attention.
Weight Loss :-
Patient with COPD work hard and burn a lot of calories just
breathing.
Lower Extremity Edema :-

In severe cases of COPD. Pulmonary artery pressures increase
and the right ventricle of the heart contracts less efficiently.
When the heart is unable to pump enough blood to meet the needs
of the kidneys and liver, edema (swelling) in the feet, ankles, and
lower legs results.
SOME IMPORTANT CLINICAL AND HISTORICAL DIFFERENCES CAN EXIST BETWEEN THE TYPES OF COPD.
In the chronic bronchitis group, classic symptoms include the
following:
o Productive cough, with progression over time to intermittent
dyspnoea
o Frequent and recurrent pulmonary infections
o Progressive cardiac/respiratory failure over time, with
oedema and weight gain
In the emphysema group, the history is somewhat different and
may include the following set of classic symptoms:
o A long history of progressive dyspnoea with late onset of
non-productive cough
o Occasional mucopurulent relapses
o Eventual cachexia and respiratory failure
Physical
Depending on the type of COPD, physical examination may vary.
Chronic bronchitis (blue bloaters)

Patients may be obese.
Frequent cough and expectoration are typical.
Use of accessory muscles of respiration is common.
Coarse rhonchi and wheezing may be heard on auscultation.
Patients may have signs of right heart failure (i.e., Cor
Pulmonale), such as oedema and cyanosis.
Because they share many of the same physical signs, COPD
may be difficult to distinguish from congestive heart failure
(CHF). One crude bedside test for distinguishing COPD from
CHF is peak expiratory flow. If patients blow 150-200 ml or
less, they are probably having a COPD exacerbation; higher
flows indicate a probable CHF exacerbation.
Emphysema (pink puffers)
o Patients may be very thin with a barrel chest.
o They typically have little or no cough or expectoration.
o Breathing may be assisted by pursed lips and use of
accessory respiratory muscles; they may adopt the tripod
sitting position.
o The chest may be hyper resonant, and wheezing may be
heard; heart sounds are very distant.
o Overall appearance is more like classic COPD exacerbation.
Stages of COPD
Stage I: mild COPD: Characterized by mild airflow limitation
(FEV1/FVC < 0.70, FEV1 80% predicted). Symptoms of chronic
cough and sputum production may be present, but not always.

At this stage, the individual is usually unaware that his or her lung
function is abnormal.
Stage II: moderate COPD: Characterized by worsening airflow
limitation (FEV1/FVC < 0.70, 50% FEV1 < 80% predicted), with
shortness of breath typically developing on exertion and cough and
sputum production sometimes also present.
This is the stage at which patients typically seek medical attention
because of chronic respiratory symptoms or an exacerbation of
their disease.
Stage III: severe COPD: Characterized by further worsening of
airflow limitation (FEV1/FVC < 0.70, 30% FEV1 < 50% predicted),
greater shortness of breath, reduced exercise capacity, fatigue,
and repeated exacerbations that almost always have an impact on
patients' quality of life.
Stage IV: very severe COPD: Characterized by severe airflow
limitation (FEV1/FVC < 0.70, FEV1 < 30% predicted or FEV1 < 50%
predicted plus the presence of chronic respiratory failure).
Respiratory failure is defined as an arterial partial pressure of O2
(PaO2) less than 8.0 kPa (60 mm Hg), with or without an arterial
partial pressure of CO2 (PaCO2) greater than 6.7 kPa (50 mm Hg)
while breathing air at sea level.
Respiratory failure may also lead to effects on the heart such as
Cor Pulmonale (right heart failure).
Clinical signs of Cor Pulmonale include elevation of the jugular
venous pressure and pitting ankle oedema. Patients may have stage IV COPD even if their FEV1 is greater
than 30% predicted whenever these complications are present. At this stage, quality of life is very appreciably impaired and
exacerbations may be life threatening.

COMPLICATIONS OF COPD
COPD complications can be serious and even life-
threatening. Proper recognition of signs and symptoms as well as
adherence to a medical plan of care is paramount to successful

treatment. The following provides a detailed list of the complications of
COPD:
1. Cor Pulmonale
Cor Pulmonale is caused by an increase in blood pressure in the
pulmonary artery, the vessel that carries blood from the heart to the
lungs. This leads to enlargement and subsequent failure of the right side
of the heart.
2. Acute Exacerbation of COPD

In its simplest terms, an exacerbation can be
defined as a worsening of COPD symptoms. Many people with COPD
suffer several episodes of acute exacerbation a year, often leading to
increased hospitalizations, respiratory failure and even death.
3. Pulmonary Hypertension

Pulmonary hypertension occurs when there is abnormally high pressure
within the blood vessels of the lungs.
Normally, the blood flows from the heart to pass through the lungs,
where blood cells pick up oxygen and deliver it to the body.
In pulmonary hypertension, the pulmonary artery is thickened. This
means less blood is able to flow through the blood vessels
4. Pneumothorax

Pneumothorax is defined as the accumulation of air or gas in the space
between the lung and the chest wall.
Pneumothorax occurs because of a hole that develops in the lung, which
allows air to escape in the space around the lung, causing the lung to
partially or completely collapse.
People who have COPD are at greater risk for pneumothorax because
the structure of their lungs is weak and vulnerable to the spontaneous
development of these types of holes
5. Secondary Polycythemia

Secondary polycythemia is acquired from a rare
disorder that is characterized by an overproduction of red blood cells in
the blood.
When too many red blood cells are produced, the blood becomes thick,
hindering its passage through the smaller blood vessels.
In patients with COPD, secondary polycythemia can occur as the body
tries to compensate for decreased amounts of oxygen in the blood.
6. Respiratory Failure
Respiratory failure occurs when the lungs are
unable to successfully extract sufficient oxygen and/or remove the
carbon dioxide from the body.
DIAGNOSIS

Pulmonary Function Tests (PFTs)
Pulmonary function tests are the primary diagnostic tools for COPD.
Lung biopsy is rarely used to diagnose emphysema.
There are four components to pulmonary function testing:
Spirometry,
Post bronchodilator spirometry
Lung volumes and
Diffusion capacity.
Spirometry: -
The most reliable way to determine reversible airway
obstruction is with spirometry.
It is a simple test procedure that measures the amount of air
entering and leaving the lungs.
With the patient sitting comfortably in front of the spirometry
machine. The machine measures airflow that passes through the
inhalation port attached to the machine. The inhalation device is
usually a disposable cardboard tube or a reusable tube that can be
sterilized after use.
Those most commonly used for interpretation are
(1) forced expiratory volume after 1 second [FEV1]

(2) forced vital capacity [FVC]and
(3) forced expiratory flow at 25%-75% of maximal lung
volume [FEF25-75].
For COPD the results may be:-
The amount of air exhaled (forced vital capacity, or FVC) is
reduced, compared to a person with normal lung function.
The amount of air exhaled during the initial 1 second (FEV1) is
reduced and is reduced to a greater degree than the entire FVC.
Therefore, the ratio of air exhaled after 1 second is low compared
to the total amount of air exhaled. In healthy lungs, 70%-75% of all
the air exhaled after maximum inhalation (FVC) is exhaled within
the first second (FEV1), known as the FEV1/FVC ratio. In lungs
with COPD, the FEV1/FVC ratio falls below 70%-75
PREVENTION
Lifestyle modifications that can help prevent COPD, or improve function

in COPD patients, include:
Quitting smoking
Avoiding respiratory irritants and infections
Avoiding allergens
Maintaining good nutrition
Drinking lots of fluids
Avoiding excessively low or high temperatures
Very high altitudes
Maintaining proper weight,
Exercising to increase muscle tone.
Avoid smoking tobacco or exposure to second hand tobacco smoke.
Smoking is the leading cause of COPD. Although you cannot undo the
damage that smoking has already caused, you can prevent further lung
damage by quitting. Avoiding conditions that may irritate the lungs can
reduce breathing problems in people with COPD. These conditions
include indoor and outdoor air pollution; smog; cold, dry air; hot, humid
air; or high altitudes. Avoiding respiratory illnesses, such as the flu
(influenza) and pneumonia, can decrease the risk of your COPD
worsening. Talk with your doctor about getting vaccinations
against them. Use appropriate protective gear (e.g. face mask) in the
workplace to avoid inhaling hazardous substance. Get plenty of physical
activity for good lung health. If you already have COPD, avoid colds and
flu’s, which can worsen the disease. Get annual flu and pneumococcal
vaccinations to avoid such infections. Quitting smoking is the most
important thing you can do to prevent or slow damage to your lungs.

CLINICAL MANAGEMENT
Non-drug treatment
Advice on how to respond promptly to symptoms of an
exacerbation, including starting oral corticosteroid therapy,
starting antibiotic therapy if their sputum is purulent and adjusting
their bronchodilator therapy to control their symptoms.
Advice on when and how to contact a health care professional if
symptoms do not improve.
Smoking cessation: an up to date smoking history, including pack
years smoked (number of cigarettes smoked per day, divided by
20, multiplied by the number of years smoked), should be
documented for everyone with COPD. An assessment of their
"readiness to change" should also be made.2
Nutrition: BMI should be calculated. If the BMI is abnormal (high or
low), or changing over time, the patient should be referred for
dietetic advice. If the BMI is low, patients should also be given
nutritional supplements to increase their total calorific intake, and
be encouraged to take exercise to augment the effects of
nutritional supplementation.
Drug therapy
Bronchodilator therapy:

Long-acting bronchodilators are not suitable for the relief
of acute bronchospasm but may have additional benefits
over combinations of short-acting drugs. However they
may also have additional side effects:
Long acting beta2 agonists:
o The use of long term beta2 agonists in the absence of
inhaled steroids appears to carry an increased
incidence of death or near death complications in
some groups.3
o Recent research has also suggested that patients
taking long acting beta2 agents also appear to have
more difficulties during an exacerbation due to down
regulation of the receptors.
o Therefore the role of long acting beta2 agonists in the
management of COPD is currently being re-
evaluated.
Tiotropium (a long-acting anticholinergic bronchodilator):4
o Is effective in controlling symptoms and improve
exercise capacity in patients who continue to
experience problems despite the use of short-acting
drugs.
o Tiotropium reduces COPD exacerbations and hospital
admissions and improves health-related quality-of-life
in patients with moderate and severe disease.
o Tiotropium possibly slows the decline in FEV1.
o Additional long-term studies are required to evaluate
its effect on mortality and change in FEV1, to confirm
its role compared to, or in combination with, long-

acting beta2-agonists, and to assess its effectiveness
in mild and very severe COPD.
Mucolytic drug therapy: should be considered in patients
with a chronic cough productive of sputum and continued
if there is symptomatic improvement (e.g. reduction in
frequency of cough and sputum production).
Theophylline: should only be used after a trial of short-
acting bronchodilators and long-acting bronchodilators, or
in patients who are unable to use inhaled therapy.
Phosphodiesterase type 4 inhibitors: there is insufficient
long-term data on which to base any evidence statements
or recommendations.
Inhaled corticosteroids:
o None of the inhaled corticosteroids currently
available are licensed for use alone in the treatment
of COPD.
o Oral corticosteroid reversibility tests do not predict
response to inhaled corticosteroid therapy.
o Inhaled corticosteroids should be prescribed for
patients with an FEV1 50% or less of predicted, who
are having 2 or more exacerbations requiring
treatment with antibiotics or oral corticosteroids in a
12 month period.
o The aim of treatment is to reduce exacerbation rates
and slow the decline in health status and not
necessarily to improve lung function.

Oral corticosteroids:
o Maintenance use of oral corticosteroid therapy in
COPD is not normally recommended. If oral
corticosteroids cannot be withdrawn following an
exacerbation, the dose of oral corticosteroids should
be kept as low as possible.
o Patients treated with long term oral corticosteroid
therapy should be monitored for the development of
osteoporosis.
Combination therapy:
o If patients remain symptomatic on monotherapy,
effective combinations include:
Beta 2-agonist and anticholinergic
Beta 2-agonist and theophylline
Anticholinergic and theophylline
Long-acting beta 2-agonist and inhaled
corticosteroid
Combination treatment should be discontinued if there is
no benefit after 4 weeks.
Delivery systems:
o In most cases bronchodilator therapy is best
administered using a hand held inhaler device
(including a spacer device if appropriate).

o There is no evidence to suggest superiority of
nebulised therapy over the use of an MDI with a
spacer device.
Non-invasive ventilation:
o Adequately treated patients with chronic hypercapnia
ventilator failure who have required assisted
ventilation (whether invasive or non-invasive) during
an exacerbation or who are hypercapnia or acidosis
on oxygen therapy should be referred to a specialist
centre for consideration of long-term NIV.
Treatments not recommended include anti-oxidant
therapy with alpha-tocopherol and beta-carotene
supplements, anti-tussive therapy and prophylactic
antibiotic therapy.
Vaccination and anti-viral therapy
Pneumococcal vaccination and an annual influenza vaccination
should be offered to all patients with COPD.
Antiviral for influenza: zanamivir and oseltamivir are recommended
for the treatment of at-risk adults who present with influenza-like
illness and who can start therapy within 48 hours of the onset of
symptoms.
Zanamivir should be used with caution in people with COPD
because of a risk of bronchospasm and patients prescribed
zanamivir should have a fast-acting bronchodilator available.
Lung surgery

Patients who are breathless, and have a single large bulla on a CT
scan and an FEV1 less than 50% predicted should be referred for
consideration of bullectomy.
Patients with severe COPD who remain breathless with marked
restrictions of their activities of daily living despite maximal medical
therapy should be referred for consideration of lung volume
reduction surgery if they meet all of the following criteria:
1. FEV1 more than 20% predicted 2. PaCO2 less than 7.3kPa 3. Upper lobe predominant emphysema 4. TLCO more than 20% predicted
Patients with severe COPD who remain breathless with marked
restrictions of their activities of daily living despite maximal medical
therapy should be considered for referral for assessment for lung
transplantation bearing in mind comorbidities and local surgical
protocols.
Considerations include: age, FEV1, PaCO2, homogeneously
distributed emphysema on CT scan, elevated pulmonary artery
pressures with progressive deterioration.
Palliative care
Opioids should be used when appropriate to palliate
breathlessness in patients with end-stage COPD which is
unresponsive to other medical therapy.
Benzodiazepines, tricycle antidepressants, major tranquillisers and
oxygen should also be used when appropriate for breathlessness
in patients with end stage COPD unresponsive to other medical
therapy.

Patients with end stage COPD and their family and carers should
have access to the full range of services offered by
multidisciplinary palliative care teams, including admission to
hospices.
ASTHMA
Asthma is an obstructive lung disease where the bronchial tubes
(airways) are extra sensitive (hyper responsive).
The airways become inflamed and produce excess mucus and the
muscles around the airways tighten making the airways narrower.
It is characterised functionally by the presence of airflow
obstruction which is variable over short periods of time, or is
reversible with treatment.
Asthma is usually triggered by breathing in things in the air such as
dust or pollen that produce an allergic reaction.
It may be triggered by other things such as an upper respiratory
tract infection, cold air, exercise or smoke.
Asthma is a common condition and affects over 300 million people
around the world.

Asthma causes recurring episodes of wheezing, breathlessness,
chest tightness, and coughing, particularly at night or in the early
morning.
AETIOLOGY
The aetiology of asthma is complex, and multiple environmental
and genetic determinants are implicated.
Living in farms, large families, childhood infections, including
parasites, exposure to pets in early life.
Obesity may also increase the risk of asthma.
Smokers may be at high risk.

PATHOPHYSIOLOGY
The inhalation of an allergens rapidly interacts with mucosal mast
cells via an IgE dependent mechanism,
Resulting in release of mediators such as histamine and the
cysteinyl leukotrienes with resulting in bronchi constriction.
Airway hyper reactivity is integral to diagnosis of asthma.

Others factors are the behaviour of airway smooth muscles,
degree of airway narrowing and influence of neurogenic
mechanism.
TYPES OF ASTHMA
It is divided into two types:
Extrinsic asthma
Intrinsic asthma
Extrinsic asthma
Extrinsic asthma is also called atopic asthma.
It occurs in younger age group. Patients are sensitive to different
factors like pollen, dust, mites, and have family history.
These subjects show immediate skin reaction.
Intrinsic asthma
It is called non-atopic asthma which tends to occur in older
patients.
It is precipitated by chronic bronchitis, strenuous exercise, stress
or anxiety.
Respiratory infections are also common cause.
CLINICAL FEATURES

Recurrent episodes of wheezing, chest tightness, breathlessness
and cough.
The patient will prefer to sit upright with shoulder girdle fixed to
assist accessory muscles of respiration
Nocturnal asthma is common with cough and wheeze during
sleep.
Mild intermittent asthma are usually asymptomatic
Breath sounds are vesicular.
Crackles may also be heard if sputum is present.
On percussion hyper-resonant.
In persistent asthma the pattern is one chronic wheeze and
breathlessness.
Cough variant asthma may be present with cough as dominant
symptom.
INSVESTIGATIONS
Asthma is diagnosed by the characteristic pattern of symptoms.

A peak flow meter can record variations in the severity of asthma
over time.
Spirometry, a measurement of lung function, can provide an
assessment of the severity, reversibility, and variability of airflow
limitation, and help confirm the diagnosis of asthma.
An elevated sputum or peripheral blood eosinopil count may be
observed.
In radiological examination of acute asthma hyperinflation and
lobar collapse may be seen.
Induced sputum and exhaled breath allow the non invasive
assessment of airway inflammation.
In emergency department doctors use capnography which
measures the amount of exhaled carbon dioxide along with pulse
oxymetry.
More recently, exhaled nitric oxide has been studied as breath test
indicative of airway inflammation in asthma.
MEDICAL TREATMENT
The most effective treatment for asthma is identifying triggers,
such as pets or aspirin and limiting or eliminating exposure to
them.
Desensitization is currently the only known cure to the disease.
Other form of treatment includes relief medication, prevention
medication, long-acting beta agonists and emergency treatment.
Bronchodilators are recommended for short term relief in all
patients

For those with persistent disease low dose inhaled glucocorticoids
or leukotriene modifier’s mast cell stabilizer or theophylline may be
administered
For sever patients a higher dose of glucocortcoids with long acting
inhaled beta2 agonist
Beta2 agonist like salbutamol, levabuterol, terbutaline and
bitolterol are used.
Nebulised salbutamol or terbutaline often combined with
ipratropium is given.
System steroids, oral or intravenous like prednisolne,methyl
prednisone, dexamethasone or hydrocortisone are used
Methylxanthines like theophylline, aminophylline may be used
Intubation and mechanical ventilation for patients with respiratory
arrest
Heliox is used in hospital setting as it has more laminar flow than
ambient air and moves easily through constricted airways.

BRONCHIECTASIS
Bronchiectasis is a disease that causes localized, irreversible
dilation of part of the bronchial tree.
It is classified as an obstructive lung disease, along with bronchitis
and cystic fibrosis.
Involved bronchi are dilated, inflamed, and easily collapsible,
resulting in airflow obstruction and impaired clearance of
secretions.
Bronchiectasis is associated with a wide range of disorders, but it
usually results from necrotizing bacterial infections, such as
infections caused by the Staphylococcus or Klebsiella species or
Bordetella pertussis.

PATHOGENSIS
Dilation of the bronchial walls results in airflow obstruction and
impaired clearance of secretions because the dilated areas disrupt
normal air pressure in the bronchial tubes, causing sputum to pool
inside the dilated areas instead of being pushed upward.
The pooled sputum provides an environment conducive to the
growth of infectious pathogens, and these areas of the lungs are
thus very vulnerable to infection.
The more infections that the lungs experience, the more damaged
the lung tissue and alveoli become.
When this happens, the bronchial tubes become more inelastic
and compressed, creating a self-perpetuating cycle of further
damage to the lungs.
TYPES OF BROCHIECTASIS
There are three types of bronchiectasis, varying by level of severity.
Fusiform (cylindrical) bronchiectasis (the most common type)
refers to mildly inflamed bronchi that fail to taper distally.
In varicose bronchiectasis, the bronchial walls appear beaded,
because areas of dilation are mixed with areas of constriction.
Saccular (cystic) bronchiectasis is characterized by severe and
irreversible ballooning of the bronchi peripherally, with or
without air-fluid levels.

Chronic productive cough is prominent, occurring in up to 90% of
patients with bronchiectasis.
Generally, persons suffering from bronchiectasis tend to be
infected by Haemophilus influenza early on in the disease course.
Secondary infection is usually due to Staphylococcus aureus;
followed by Moraxella catarrhalis and finally Pseudomonas
aeruginosa.
CAUSES
There are both congenital and acquired causes of bronchiectasis.
Kartagener syndrome, which affects the mobility of cilia in the
lungs, aids in the development of the disease.
Young's syndrome, which is clinically similar to cystic fibrosis, is
thought to significantly contribute to the development of
bronchiectasis. This is due to the occurrence of chronic, sin
pulmonary infections.
Patients with alpha 1-antitrypsin deficiency have been found to be
particularly susceptible to bronchiectasis. Acquired bronchiectasis
occurs more frequently, with one of the biggest causes being
tuberculosis.
Endobronchial tuberculosis commonly leads to bronchiectasis,
either from bronchial stenosis or secondary traction from fibrosis.
An especially common cause of the disease in children is acquired
immune deficiency syndrome, stemming from the human insulin
immunodeficiency virus.
Other acquired causes of bronchiectasis involving environmental
exposures include respiratory infections, obstructions, inhalation

and aspiration of ammonia and other toxic gases.
SIGNS AND SYMPTOMS
Persistent Cough and purulent sputum is present
The sputum is green, foul smelling and in large volume
Pyrexia, night sweats, anorexia, malaise, weight loss, lassitude
and joint pains are present
Shortness of breath is seen in severe conditions
Haemoptysis is common usually associated with acute infection
Recurrent pneumonia is present
Chronic sinusitis is present in most of patients
In 50% patients clubbing is present
Thoracic mobility decreases
DIAGNOSIS
The diagnosis of bronchiectasis is based on the review of clinical
history and characteristic patterns in high-resolution CT scan
findings.

Such patterns include "tree-in-bud" abnormalities and cysts with
definable borders. In one small study, CT findings of
bronchiectasis and multiple small nodules were reported to have a
sensitivity of 80%, specificity of 87%, and accuracy of 80% for the
detection of bronchiectasis.
Bronchiectasis may also be diagnosed without CT scan
confirmation if clinical history clearly demonstrates frequent,
respiratory infections, as well confirmation of an underlying
problem via blood work and sputum culture samples.
COMPLICATIONS
Recurrent haemoptysis
Pneumonia
Pleurisy and empyema
Respiratory failure
Right ventricular failure
Emphysema and systemic amyloidosis are rare
TREATMENT
Treatment of bronchiectasis is aimed at controlling infections and
bronchial secretions, relieving airway obstruction, and preventing
complications.

This includes the prolonged usage of antibiotics to prevent
detrimental infections, as well as eliminating accumulated fluid with
postural drainage and chest physiotherapy.
Surgery may also be used to treat localized bronchiectasis,
removing obstructions that could cause progression of the disease.
Inhaled steroid therapy that is consistently adhered to can reduce
sputum production and decrease airway constriction over a period
of time, and help prevent progression of bronchiectasis.
One commonly used therapy is beclometasone dipropionate,
which is also used in asthma treatment.
Use of inhalers such as albuterol (salbutamol), fluticasone
(Flovent/Flixotide) and ipratropium (Atrovent) may help reduce
likelihood of infection by clearing the airways and decreasing
inflammation.
PREVENTION
In order to prevent future development of bronchiectasis, an x-ray
of the chest should be taken after any severe attack of measles,
whooping cough or other acute respiratory infection in childhood.
CYSTIC FIBROSIS
Cystic fibrosis (also known as CF, mucovoidosis, or
mucoviscidosis) is a genetic disorder known to be an inherited

disease of the secretory glands, including the glands that make
mucus and sweat.
The hallmarks of cystic fibrosis are salty tasting skin, normal
appetite but poor growth and poor weight gain, excess mucus
production, and coughing/shortness of breath. Males can be
infertile due to the condition Congenital absence of the vas
deferens. Often, symptoms of CF appear in infancy and childhood.
Meconium ileus is a typical finding in newborn babies with CF.
Although technically a rare disease, cystic fibrosis is ranked as one
of the most widespread life-shortening genetic diseases.
CAUSES

Cystic Fibrosis has an autosomal recessive pattern of inheritance.
CF is caused by a mutation in the gene cystic fibrosis
transmembrane conductance regulator (CFTR). The product of this
gene is a chloride ion channel important in creating sweat,
digestive juices and mucus.
Although most people without CF have two working copies
(alleles) of the CFTR gene, only one is needed to prevent cystic
fibrosis. CF develops when neither allele can produce a functional
CFTR protein.
Therefore, CF is considered an autosomal recessive disease.

PATHOPHYSIOLOGY
The protein created by this gene is anchored to the outer
membrane of cells in the sweat glands, lungs, pancreas, and other
affected organs.
The protein spans this membrane and acts as a channel
connecting the inner part of the cell (cytoplasm) to the surrounding
fluid.
This channel is primarily responsible for controlling the movement
of chloride from inside to outside of the cell; however, in the sweat
ducts it facilitates the movement of chloride from the sweat into the
cytoplasm.
When the CFTR protein does not work, chloride is trapped inside
the cells in the airway and outside in the skin.
Because chloride is negatively charged, positively charged ions
cross into the cell because they are affected by the electrical
attraction of the chloride ions.
Sodium is the most common ion in the extracellular space and the
combination of sodium and chloride creates the salt, which is lost
in high amounts in the sweat of individuals with CF. This lost salt
forms the basis for the sweat test.
One theory suggests that the lack of chloride exodus through the
CFTR protein leads to the accumulation of more viscous, nutrient-
rich mucus in the lungs that allows bacteria to hide from the body's
immune system.

Another theory proposes that the CFTR protein failure leads to a
paradoxical increase in sodium and chloride uptake, which, by
leading to increased water reabsorption, creates dehydrated and
thick mucus.
Yet another theory focuses on abnormal chloride movement out of
the cell, which also leads to dehydration of mucus, pancreatic
secretions, biliary secretions, etc.
These theories all support the observation that the majority of the
damage in CF is due to blockage of the narrow passages of
affected organs with thickened secretions.
These blockages lead to remodelling and infection in the lung,
damage by accumulated digestive enzymes in the pancreas,
blockage of the intestines by thick faeces, etc
SYMPTOMS
Thick, viscous mucus secretions in the lungs
Repeated infections: The accumulation of sticky, thick mucus in
the lungs creates a favourable environment for infectious
microorganisms to inhabit and flourish.
Stools, pale or clay colour, foul smelling, or stools that float
Recurrent pneumonia
Chronic cough, possibly with blood streaking
Wheezing

Bronchitis
Chronic sinusitis
Asthma
Weight loss, failure to thrive in infants, abdominal swelling
Excessive salt in sweat, dehydration
Failure of newborn to pass stool
Abdominal pain, flatulence
Fatigue
Enlarged fingertips (clubbing)

Changes in colour and amount of sputum (material coughed
up from the lungs)
DIAGNOSIS
CF can be diagnosed at birth, but most often is diagnosed during
the early childhood years in young children (by the age of 3 years)
who have had a history of respiratory infections, excessive fat in
their stools, and who have poor weight gain.
Nearly 8 percent of people with CF are diagnosed at 18 years of
age or older because they have experienced only mild symptoms
of CF.
CF's major symptoms is respiratory infection, a CF diagnosis
sometimes may be confused with other respiratory conditions such
as asthma, pneumonia, or chronic bronchitis.
Genetic Testing
Couples planning a family may decide to have themselves
tested if one or both have a family history of CF
Sweat Test
The sweat test is an accurate, safe, and painless way to
diagnose CF. In the sweat test, a small electric current is used to
carry the chemical pilocarpine into the skin of the forearm. This
stimulates sweat glands in the area to produce sweat. Over a
period of 30 to 60 minutes, sweat is collected on filter paper (or
gauze) and tested for chloride. A chloride reading of more than 60
mEq/L points to CF.

Pulmonary Function Tests :-
PFTs; Spirometry; Spirogram; Lung function tests
Pulmonary function tests (PFTs) are breathing tests that help
measure lung reserve and degree of airflow obstruction. Infant
PFTs are currently being studied.
COMPLICATIONS
Haemoptysis
Spontaneous pneumothorax
Osteoporosis
Liver diseases
Diabetes mellitus
Deformities like kyphosis and lordosis
Cor Pulmonale
MANAGEMENT
The cornerstones of management are proactive treatment of
airway infection, and encouragement of good nutrition and an
active lifestyle.
Targets for therapy are the lungs, gastrointestinal tract (including
insulin treatment and pancreatic enzyme supplements), the
reproductive organs (including Assisted Reproductive Technology
(ART)) and psychological support.

In addition, therapies such as transplantation and gene therapy
aim to cure some of the effects of cystic fibrosis.
Gene therapy aims to introduce normal CFTR to airway.
Theoretically this process should be simple as the airway is easily
accessible and there is only a single gene defect to correct.
However there are some problems associated with these methods
involving efficiency (liposome’s insufficient protein) and delivery
(virus provokes an immune response).
The most consistent aspect of therapy in cystic fibrosis is limiting
and treating the lung damage caused by thick mucus and infection
with the goal of maintaining quality of life.
Intravenous, inhaled, and oral antibiotics are used to treat chronic
and acute infections.
Mechanical devices and inhalation medications are used to alter
and clear the thickened mucus
Antibiotics to treat lung disease
Many CF patients are on one or more antibiotics at all times,
even when they are considered healthy, to suppress the
infection as much as possible.
Many bacteria common in cystic fibrosis are resistant to
multiple antibiotics and require weeks of treatment with
intravenous antibiotics such as vancomycin, tobramycin,
meropenem, ciprofloxacin, and piperacillin.

Inhaled therapy with antibiotics such as tobramycin and
colistin is often given for months at a time in order to improve
lung function by impeding the growth of colonized bacteria.
Inhaled therapy with the antibiotic aztreonam is also being
developed and clinical trials have shown great promise.
Oral antibiotics such as ciprofloxacin or azithromycin are
given to help prevent infection or to control ongoing infection.
Some individuals spend years between hospitalizations for
antibiotics, whereas others require several antibiotic
treatments each year.
Transplantation and gene therapy
Lung transplantation often becomes necessary for individuals
with cystic fibrosis as lung function and exercise tolerance
declines.
Although single lung transplantation is possible in other
diseases, individuals with CF must have both lungs replaced
because the remaining lung would contain bacteria that could
infect the transplanted lung.
A pancreatic or liver transplant may be performed at the same
time in order to alleviate liver disease and/or diabetes.
Gene therapy holds promise as a potential avenue to cure
cystic fibrosis.

Gene therapy attempts to place a normal copy of the CFTR
gene into affected cells. Studies have shown that to prevent the
lung manifestations of cystic fibrosis, only 5–10% the normal
amount of CFTR gene expression is needed.
Ideally, transferring the normal CFTR gene into the affected
epithelium cells would result in the production of functional
CFTR in all target cells, without adverse reactions or an
inflammation response.
PT ASSESSMENT
PATIENT PROFILE:
NAME:
AGE/SEX:
ADDRESS:
SUBJECTIVE ASSESSMENT:
OCCUPATION:
CHIEF COMPLIANT:
PRESENT HISTORY:
PAST HISTORY:
PAST MEDICAL HISTORY:
PRESENT MEDICAL HISTORY:
FAMILYHISTORY:

PRESONAL HISTORY:
OCCUPATIONAL HISTORY:
SOCIO-ECONOMICAL HISTORY:
OBJECTIVE ASSESSMENT:
ON OBSERVATION:
BUILT
POSITION OF PATIENT
POSTURE
BREATHING PATTERN
CLUBBING
CYANOSIS
CHEST WALL DEFORMITIES
OEDEMA
TROPICAL CHANGES
RESPIRATORY MUSCLES
DYSPNOEA
SPUTUM
HAEMOPTYSIS
CHEST PAIN
SKELETAL MOBILITY

ON EXAMINATION
VITAL SIGNS
TEMPERATURE
RESPIRATORY RATE
PULSE RATE BLOOD PRESSURE
ON PALPATION
PRESENCE OF NODULES
TENDERNESS
WARMTH
SWELLING
CHECK THE INSPIRATORY EFFORT
COUGH REFLEX
FREMITUS
ON AUSCULTATION
COARSE CREPITATIONS
WHEEZES
CHEST MEASUREMENTS
LEVEL OF FOURTH COSTAL CARTILAGE

XIPHISTERNUM
NINTH COSTAL CARTILAGE
PHYSIOTHERAPY MANAGEMENT :-
Chronic obstructive pulmonary disease (COPD) is characterised by
intractable dyspnoea, reduced functional capacity and episodes of acute
exacerbation.
Physiotherapy plays a key role in multidisciplinary interventions. The
evidence in relation to airway clearance, pulmonary rehabilitation,
Inspiratory muscle training and non-invasive ventilation is now robust
whilst further evidence is required for other interventions in order to
clarify where application, skills and training should be focused.
The challenge is to translate sound clinical evidence-based practice into
novel models of service with resultant improvements in care for patients
with COPD.

POSITIONING :-
THE PURPOSE OF POSITIONING
1. To improve oxygen transport in acute pulmonary
dysfunction of COPD
2. To improve oxygen transport in the post acute
and chronic stages of COPD
3. To prevent the negative effects of restricted
mobility, particularly those that adversely
affect oxygen transport.

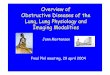
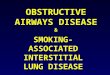
cystic fibrosisA) Relaxed sitting posture (posterior view). Note: Forward head position,tight sub occipital and mid-cervical extensors, tight upper and middle fibres of trapezius, asymmetry and abducted and protracted position of the scapulae, increased thoracic kyphosis, reduced upper lumbar lordosis, posterior rotation of pelvis.
B) Relaxed sitting posture (side view). Note: Forward head position, increasedsternocleidomastoid activity, increased low cervical lordosis and thoracic kyphosis, abducted and protracted scapulae, anterior position of humerus in glenoid fossa, internal rotation of humerus, lax abdominal muscles.

POSTURAL DRINAGE:-

BREATHING EXERCISES
These exercises are fundamental interventions for prevention
or comprehensive management of COPD. These exercises are
diaphragmatic.
Breathing exercises are designed to restrain the muscles of
respiration and improve or redistribute ventilation, lessen the work of
breathing, and improve the gas exchange and oxygenation.
Active range of motion exercises, to the shoulders and trunk also
help expand the chest, facilitate deep breathing, and often stimulate the
cough reflex.
Goals of Breathing Exercises
Improve ventilation.
Increase the effectiveness of the cough mechanism.
Prevent pulmonary impairments.
Improve the strength, endurance, and coordination of
respiratory muscles.
Maintain or improve chest and thoracic spine mobility.
Correct inefficient or abnormal breathing patterns.
Promote relaxation.
Teach the patient how to deal with shortness of breath
attacks.
Improve a patient’s overall functional capacity.

TYPE OF BREATHING EXERCISE
Three basic breath-training methods are
diaphragmatic breathing, pursed-lip breathing, and breathing while
bending forward. They can be used to help you get through periods
when you feel more short of breath.
Diaphragmatic Breathing
Pursed-lip Breathing
Breathing while bending forward
Diaphragmatic breathing helps your lungs expand so that they take in
more air. (Your diaphragm is a muscle that helps draw air into your
lungs as you breathe.) Many, but not all, people with COPD find this
breathing method helpful.
Lie on your back, or prop yourself up on several pillows.
With one hand on your belly and the other on your chest, breathe in,
pushing your belly out as far as you can. You should be able to feel
the hand on your belly moving out, while the hand on your chest
should not move.
When you breathe out, you should be able to feel the hand on your
belly moving in.
After you can do this kind of breathing well lying down, you can learn
to do it sitting or standing.
Practice this breathing for 20 minutes, 2 or 3 times a day.

Pursed-lip breathing may help you breathe more air out so that your
next breath can be deeper. Pursed-lip breathing reduces shortness of
breath and improves your ability to exercise.
Breathe in through your nose and out through your mouth while
almost closing your lips.
Breathe in for about 4 seconds, and breathe out for 6 to 8 seconds.
Breathing while bending forward at the waist may make it easier for
you to breathe. Bending forward while breathing may reduce shortness
of breath in those with severe COPD, both at rest and during exercise.
This may be because bending forward allows the diaphragm to move
more easily.

Precautions
Never allow a patient to force expiration. Expiration should be
relaxed and passive. Forced expiration only increases turbulence
in the airways, which can lead to bronchospasm and increased
airway restriction.
Do not allow a patient to take a very prolonged expiration. This
causes the patient to gasp with the next inspiration. The patient’s
breathing pattern then becomes irregular and inefficient.
Do not allow the patient to initiate inspiration with the accessory
muscles and the upper chest. Advise the patient that the upper
chest should be relatively quiet during breathing.
Allow the patient to practice deep breathing for only three or four
inspirations and expirations at a time to avoid hyperventilation.
OTHERS TECHNIQUES USED:
HUMIDIFICATIONS :-
Respiratory gas humidification is a method
of artificial warming and humidifying of respiratory gas for the patient
during mechanical ventilation.
THE ACTIVE CYCLES OF BRETHING TECHNIQUE
It involves three phases repeated in cycles

Breathing Control
The patient is instructed to breath in a relaxed manner using
normal tidal volume.
The upper chest and shoulder remain relax, lower chest and
abdomen should be active.
Preparation for next phase in 5-10 seconds
Thoracic Expansion
The emphasis during this phase is on inspiration.
The patient is instructed to take in a breath to Inspiratory reserve
expiration is passive and relaxed.
Chest percussion shaking or vibration may be performed in
combination within thoracic expansion as the patient exhales.
Forced Expiratory Techniques
It consists of huffing interpersed within breathing control. A huff is
a rapid, forced exhalation but not within maximal effort.
INCREASING/MAINTAINING EXERCISE TOLERANCE
Before Exercise training, the Exercise tolerance and dyspnoea is
done by BORG’S scale for Exertion(R.P.E –RATING PERCEIVED
EXERTION)
15 Point Scale
6 - 20% effort

7 - 30% effort - Very, very light (Rest)
8 - 40% effort
9 - 50% effort - Very light - gentle walking
10 - 55% effort
11 - 60% effort - Fairly light
12 - 65% effort
13 - 70% effort - Somewhat hard - steady pace
14 - 75% effort
15 - 80% effort – Hard
16 - 85% effort
17 - 90% effort - Very hard
18 - 95% effort
19 - 100% effort - Very, very hard
20 - Exhaustion
Training Intensity
Aerobic training is usually target at 60-90% of predicted maximal
heart rate or 50-80% of maximal oxygen intake or 60-90%mhr of
pulse oxymetry.
This level is sustained for 20-45% and repeated 3-4 times a week
Training at this intensity, within is well above the anaerobic
threshold, increase maximal exercise performance, causes
physiologic adaptations in peripheral muscle and improves cardiac
function in healthy subjects.
Most exercise tolerance programs emphasis endurance training,
utilizing periods of sustained exercise for about 20-30 minutes, 2-5
times a week.

Training specificity
Refers to the observation that benefit is gained only in those
activities involving the muscle groups that are specifically trained.
INSPIRATORY MUSCLE TRAINING
Inspiratory muscles may be compromised in majority of lung
diseases and contribute to dyspnoea – exercise limitation and
hypercapnia.
Generally initiated at low intensity then gradually increased to
achieve 60-70% of maximum.
NON-INVASIVE POSITIVE PRESSURE VENTILATION
In selected patients with hypercapnia respiratory failure due to
an acute exacerbation of chronic obstructive pulmonary disease
(COPD), non-invasive positive pressure ventilation (NIPPV) is an
effective adjunct to usual medical therapy.
In controlled trials, it reduced the need for endotra-
cheal intubation, the length of hospital stay, and the
risk of death.
Patients with decompensate respiratory
failure lack sufficient alveolar ventilation, owing to
abnormal respiratory mechanics and Inspiratory
muscle fatigue. For these patients, breathing faster does not fully
compensate.

Non-invasive positive pressure ventilation partially counteracts these
factors by providing a larger tidal volume with the same Inspiratory effort.
Additionally, this treatment can decrease the work of breathing by
partially overcoming auto-PEEP (positive end-expiratory pressure) in
certain situations. Auto-PEEP is pressure greater than the atmospheric
pressure remaining in the alveoli at the end of exhalation. This condition
is related to limited expiratory flow and is common in those with severe
COPD. Non-invasive positive pressure ventilation decreases the
pressure difference between the atmosphere and the alveoli, thereby
reducing the Inspiratory force needed for initiation of Inspiratory effort,
which may reduce the work of breathing.
BIBILOGRAPHY

DAVIDSON-GENERAL MEDICINE
HARRISON’S-INTERNAL MEDICINE
HARSHA MOHAN-PATHOLOGY
JULLIAN-
JENNIFER PRIOR-
TIDY’S PHYSIOTHERAPY
CASH TEXTBOOK OF CARDIOVASCULAR
DISEASE FOR PHYSIOTHERAPY
INTERNET