Embed Size (px)
Citation preview

Obstetrical
Emergencies
Avera McKennan Hospital &
University Health Center

•“there's no harm in hoping for the best as long as you're prepared for the worst.” ― Stephen King, Different Seasons

OB Emergencies…
• Do not happen often, but when they do…. Seconds do matter
• Important for everyone to act together as quickly as possible
• Anticipate possible problems, think 1-2 hours ahead
• Be assertive – make sure others know the importance of the emergency

• Patient care emergencies may occur at any time in any setting, particularly the inpatient setting..

• It is important that obstetrician–
gynecologists prepare themselves by
assessing potential emergencies,
establishing early warning systems,
designating specialized first
responders, conducting emergency
drills, and debriefing staff after actual
events to identify strengths and
opportunities for improvement.
Having such systems in place may
reduce or prevent the severity of
medical emergencies

Excellent communication and
teamwork will further increase
the efficiency and effectiveness
of the emergency response.
ACOG Committee Opinion, Preparing
for Clinical Emergencies in Obstetrics and
Gynecology, March, 2014

Abruption • Premature separation of the placenta
• Incidence: about 1% of pregnancies
• Leading cause of vaginal bleeding in the latter half of pregnancy
• Maternal effect depends primarily on severity
• Fetal effects depend on severity and gestational age
• Often associated with fetal death when involving more than 50% of the placenta


Risk Factors for Abruption
• Prior abruption
• Smoking
• Trauma
• Cocaine use
• Multifetal
gestation
• Hypertension
• Preeclampsia
• thrombophilias
• Advanced
maternal age
• PPROM
• Intrauterine
infection
• hydramnios

Signs/Symptoms of abruption
• Uterine pain-may be mild-severe
• Back pain
• Vaginal bleeding
• Uterine irritability,UC’s,hard/tender
abdomen
• Fetal distress
• Signs of hypovolemia and/or shock,
may be without visible blood loss
• May be asymptomatic

Tachysystole

Diagnosis
• Physical exam, assessing
patient’s S/S
• Ultrasound to R/O placenta
previa/identify retroplacental
hematoma
• Lab values
• Examination of placenta at
delivery

Placental Abruption

Maternal Effects
• Excessive blood loss
• DIC
• Hypovolemic shock
• Renal failure
• Adult Respiratory Distress Syndrome
• Multiorgan failure
• PP hysterectomy
• Death (rarely)

Fetal Effects
•Hypoxemia
•Asphyxia
•Low birth weight/IUGR (chronic
abruption)
•Preterm delivery
•Death

Management of acute
abruption •Prompt evaluation
•Continuous fetal monitoring
•Establish IV access/draw labs
•Notify blood bank so replacement products are
readily available
•Monitor VS closely
•Keep maternal oxygen saturation >95%
•Notify anesthesia of potential emergency
cesarean
•Delivery

Placenta Previa
• Presence of placental tissue
that extends over or lies
proximate to the internal
cervical os
• Incidence: 3.5-4.6 per 1000
births
• Pathogenesis is unknown

Descriptions
• Low-lying –The placenta is in the
lower portion of uterus, but not truly a
previa
• Marginal – The placental is adjacent
to or at the margin of the internal os
• Partial – The placental edge appears
to cover part, but not all, of the internal
os
• Total – The placenta completely
covers the internal os


Risk Factors for Previa • Previous placenta previa
• Previous c-section/uterine surgery
• Multiple gestation
• Multiparity
• Infertility treatment
• Previous abortion
• Smoking
• Cocaine
• Male fetus
• Non-white race

Manifestations & Diagnosis
• Clinical
Manifestations
–Painless vaginal
bleeding in 2nd
half of pregnancy
–Bleeding and
contractions
• Diagnosis
–Transabdominal/tr
ansvaginal
ultrasound
–Spec exam to R/O
other causes of
bleeding

Maternal & Fetal Effects • Maternal
– Hemorrhage
– hypovolemic shock
– Rh sensitization
– Anemia
– Abnormal
implantation of
placenta
• Fetal
– Prematurity
– IUGR
– Congenital
abnormalities
– Anemia
– Malpresentation

Asymptomatic
Goals/Management • Determine whether the previa resolves
with increasing gestational age – Serial ultrasounds
• Reduce the risk of bleeding – Avoid intercourse and exercise after 20 weeks
– Decrease overall physical activity in 3rd trimester
• Reduce the risk of preterm birth

• Achieve and/or maintain maternal
hemodynamic stability
–Monitor VS & urine output
–Estimate blood loss
–Evaluate labs
– IV fluids/transfusion

•Determine if emergent cesarean delivery is
indicated -Consider tocolysis to decrease contractions
which may promote placental separation and
bleeding
-Indications for delivery include: A
nonreassuring fetal heart rate tracing, life-
threatening refractory maternal hemorrhage,
or significant bleeding after 34 weeks gestation
Acute/Emergent
Goals/Management

Abnormal Implantation
• Accreta - placenta attaches directly
to myometrium
• Increta - invades the myometrium
• Percreta - penetrates through the
myometrium


Risk Factors • Previous cesarean delivery
• Placenta previa
• Advanced maternal age
• multiparity
• Endometrial defects (Asherman syndrome)
• Submucous leimomyomata
• Myometrial damage (myomectomy)
• Thermal ablation
• Uterine artery embolization

Diagnosis
•The diagnosis is usually
established by ultrasonography
and occasionally supplemented
by magnetic resonance imaging
(MRI).


Management
• Delivery planning
–cesarean with hysterectomy
–Uterine conservation may be
attempted if fundal or posterior
placenta accreta
• Maintain hemodynamic status,
prevent shock
–2 large bore IVs
–Cross-matched blood available

Velamentous cord insertion/
Vasa Previa
• Velamentous insertion -
umbilical vessels diverge as they
traverse between the amnion and
chorion before reaching the
placenta
• Vasa previa- fetal blood vessels
are present in the membranes
covering the internal os

Velamentous cord insertion/
Vasa Previa


Velementous Insertion-
pathogenesis • Pathogenesis is unknown
• Most popular hypothesis is that the cord
is initially inserted centrally, but its
location progressively becomes
peripheral as one half of the placenta
actively proliferates toward the well-
vascularized uterine fundus while the
other pole involutes

Amniotic Fluid Embolism
• Rare and frequently fatal obstetrical emergency
• Occurs in 1 in 30,000 births
• Maternal mortality 60-80%
• Diagnosis:
– Presence of fetal squamous cells, lanugo, vernix, mucin and/or meconium in the maternal pulmonary vascular space

Clinical Presentation
• 5 signs that occur in this sequence:
– Respiratory distress
– Cyanosis
– Cardiovascular collapse
– Hemorrhage
– Coma

Phase 1
• Pulmonary artery vasospasm with
pulmonary hypertension and
elevated right ventricular pressure,
causes hypoxia
• Hypoxia causes myocardial capillary
damage & pulmonary capillary
damage, left heart failure, and acute
respiratory distress syndrome

Phase II
• Hemorrhagic phase characterized
by massive hemorrhage with
uterine atony & DIC
–Fatal consumptive coagulopathy
may be the initial presentation.

Treatment
• Maintain airway via ET
tube/ventilations
• Restore cardiovascular equilibrium
• Central line – pulmonary artery
catheter
• Treat shock

Uterine Rupture
• Separation of the myometrium or
previous scar, with expulsion of
membranes and fetus into
peritoneal cavity
• Types: rupture & dehiscence
• Incidence: 1:1200 deliveries

Causes Uterine Rupture • Previous uterine surgery
• Hyperstimulation/hypertonus
• Grand multiparity
• Invasive or blunt trauma
• Obstructed labor
• Maneuvers within the uterus
• Midforceps rotation of the fetus
• Abnormal fetal lie
• Previous termination(s)

Signs/Symptoms
• Dehiscense
– May be
asymptomatic
– S/S may develop
over several hrs
– Minimal bleeding
– “Normal” UC’s
– FHR may be
reassuring
• Rupture
– Sharp, tearing pain
– Bleeding
– UC’s may be absent
– Fetal bradycardia
– May be unable to
reach presenting part
– May see fetus
through abd. wall
– Shock, CV collapse

Management Uterine Rupture
• Anticipate “at risk” pts and be ready
• Evaluate c/o unusual pain
• Physiologic 2nd stage management
• Assess uterine activity/tone
• Assess fetal status
• Stat C/S
• Maternal VS, pulse ox
• Maternal hemodynamic stabilization
• Accurate I&O

Uterine Inversion
• The turning “inside out” of the uterus
• 1:2,500 - 3,600 births
• Types of inversion
–1° fundus inverts, but not
through cervix
–2° fundus inverts through cervix
–3° fundus inverts & protrudes
beyond vulva

Contributing Factors and S/S
• Traction to cord
• Fundal pressure
• Fundal
implantation
• Uterine atony
• Leimyomas
• Adherent placenta
• Fetal macrosomia
• Use of oxytocin
• Hemorrhage
• Hypotension
• May visualize the uterus
• Unable to palpate uterus or can palpate a depression in the uterine fundus

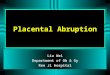
Management of Inversions
• Prevention best -
don’t pull on cord!
• Immediate attempts
to replace uterus
• Tocolysis to relax
uterus
• Closely monitor VS
• Withhold pitocin
until uterus replaced
• O2 @ 15 LPM
• IV fluid, large bore
• Blood replacement,
labs to assess coag
• Notify Anes. & OR
• Strict I&O
• Monitor maternal ECG
• Antibiotics
• Possible NG
• Monitor bleeding,
correct fundal
massage

Fundal Massage

Prolapsed Cord
• Occult vs. overt
• Risk factors:
– ROM without engaged presenting part
– Malpresentation
– Preterm or IUGR fetus
– Multiple gestation
– Hydramnios
– Maneuvers

Clinical Manifestations
• FHR changes
• Cord palpated on vaginal
exam
• Cord visualized in vagina
or protruding from vagina

Management of Cord Prolapse
• Call for help
• DC pitocin
• Relieve cord
compression
against cervix
• Minimize cord
manipulation
• Knee-chest or
trendelenberg
• Do not remove hand!
• Cover cord with sterile
saline-soaked gauze
• O2
• Prepare for emergent
C/S & neo resuscitation
• Consider tocolytics
• Assess FHR
• Bladder inflation
– Prolapse Kit

Prolapse Kit
• Sterile no. 16 foley catheter, drainage tubing & bag
• Hemostat
• 1000 ml bottle sterile water, sterile bladder irrigation fluid, or 1000 ml NS with IV tubing
• Large syringe with pointed tip, preferably 60 ml

Bladder Inflation
• Insert foley cath & inflate balloon
• Clamp catheter with hemostat; remove drainage tubing
• Assemble IV of dextrose-free sol’n (i.e., NS), flush tubing
• Insert IV tubing into end of foley cath, remove hemostat.
• Infuse 400-750 ml into end of catheter & reclamp foley w/hemostat.
• Reattach foley drainage tube/bag – keep hemostat in place.
• Remove hemostat just prior to peritoneum incision

Labor Epidurals
• Regional block
– Local anesthetics
– Epinephrine
– Lipid-soluble opioid
• Test dose, bolus or
continuous, PCEA
option

Benefits to Epidurals
• Good to excellent analgesia
• Infrequent nausea
• Minimal sedation
• ↓ anxiety
• Retention of cough reflex
• ↓pulmonary dysfunction
• Can be used continuously for several hours
• Doesn’t cause significant slowing of labor
• Presence of catheter allows flexibility in type & amount of medication given
• Can be used for anesthesia if C/S necessary

Risks of Epidural
• Systemic toxicity
• High spinal/epidural
• Hypotension
• Inadequate or failed block
• Pruritis
• Nausea/Vomiting
• Respiratory Depression
• Intrapartum Fever

Risks of Epidural
• Severe Headache
• Epidural Hematoma
• Fetal bradycardia

BP & FHR Assessment
• Although insufficient evidence to
support definitive recommendations
about BP & FHR assessment, literature
review reveals that hypotension can
occur within the first 5 to 15 minutes
following initiation or re-bolus.
– Suggested: BP & FHR q. 5 minutes during
the 1st 15 minutes of initiation or re-bolus

Effects on Labor & Delivery
• A meta-analysis of randomized trials of epidural versus no epidural or no analgesia in labor found that epidural analgesia was associated with a longer second stage
• No significant effect on the duration of the first stage of labor

Effects on Labor & Delivery
• A meta-analysis of 38 randomized trials comparing all modalities of epidural with any form of pain relief not involving regional blockade or no pain relief in labor, concluded epidural analgesia did not significantly increase the risk of cesarean delivery

Effects on Labor & delivery
• The same meta-analysis found that neuraxial labor analgesia was associated with an increased risk of instrumental vaginal birth

Effects on Labor & Delivery
• An American College of
Obstetricians and Gynecologists
Committee Opinion concluded
that "maternal request is
sufficient medical indication for
pain relief during labor" and that
neuraxial anesthesia does not
increase the frequency of
cesarean delivery

Inadvertent Spinal
• S/S
– Inability to get
air, dyspnea
– Loss of
consciousness
– Bradycardia
– Hypotension
– Respiratory
arrest
• Rx/Interventions
– Immediate
respiratory support
(PPV)
– Atropine & ephedrine
for C.O
– IV fluids
– Elevate legs
– Maintain calm
– Deliver w/in 4-5’ if
cardiac arrest

Systemic Local Toxicity
• S/S
– Ringing in ears,
tingling around
mouth,
restlessness,
nervousness,
blurred vision,
incoherent speech
• Muscle twitching
• Convulsions
• Rx/Interventions
– Establish airway, O2
per PPV
– Intubate
– Valium for seizures
– Lateral positioning
– IV fluids, ephedrine
– Atropine (brady)
– Bretylium

Post-Epidural
• Catheter removal by RN if approved
per policy (documented competency)
– Withdraw slowly, do not force
– Assess for integrity of cath tip
– Band-Aid to site, monitor q. shift for
bruising, leaking fluid
• Carefully document amount wasted
(if narcotic added)

Shoulder Dystocia
• Impaction of the fetal shoulders within the maternal bony pelvis – Shoulders don’t deliver with maternal
expulsive efforts & gentle traction
• Incidence: 0.25% to 2.0% of all vaginal births
• Risk is greater in macrosomic infants – 11 x relative risk in > 4,000 gms
– 22 x relative risk in > 4,500 gms

Dystocia Risk Factors
• Maternal diabetes
• Maternal obesity
• Excessive wt gain
• Abnormal labor
progress
• Disproportionate
fetal growth
• Multiparity
• Male infant
• Prior large baby
• Prior dystocia
• Midforceps/vacuum
• Labor induction
• Macrosomia
• Abnormal pelvis
• > maternal age
• Short stature
• Post term

ADOPE
• A = Age
• D = Diabetes
• O = Obesity
• P = Prior large infant and/or
post dates
• E = Excessive weight gain

Dystocia Complications
• Fetal/newborn
– Anoxia,
asphyxia
– Erb’s palsy
– Fx clavicle
– Brain damage
– Death
• Maternal
– Extensive vaginal
& perineal
lacerations
– Emotional trauma

Management of Dystocia
• Labor Mechanisms
–Engagement
–Descent
–Flexion
– Internal rotation
–Extension
–External rotation
–Expulsion


Management of Dystocia
• Early recognition: double chin, “Turtle Sign”
• Note time head delivers
• Note time dystocia recognized
• Signal 1 min. intervals
• May cut larger epis
• Notify peds/anes.
• Place patient in
lithotomy at edge
of delivery
bed/table

Turtle Sign

McRobert’s Maneuver
• Sharp hyperflexion of legs against abdomen
• Straightens the sacrum, angle of inclination
• Two assistants

Manual Pressure
• Gentle pressure on fetal head inferiorly & posteriorly
• Pushes shoulder into hollow of sacrum
• room for anterior shoulder

Suprapubic Pressure
• Direct pressure posteriorly & laterally above symphysis to dislodge anterior shoulder
• Empty bladder to avoid trauma & allow more room

Rubin Maneuver

Wood’s Screw Maneuver

Posterior Arm Delivery

Fracture of the Clavicle
• Diminishes the rigidity and size of
shoulder girdle
• Anterior clavicle broken first to
collapse the anterior shoulder and
dislodge it from behind the
symphysis
• Exert pressure away from lung to
avoid puncture

Gaskin Maneuver
• Hands & knee
(not knee chest)
• Mechanism of
action unknown
• Consider trying
first if no
epidural

Zavanelli Maneuver
(Cephalic Replacement)
• Manually return head to OA
• Flex the head & replace in vagina
• Hold fetal head in place until
C/birth

HELPERR
• H - call for help
• E - Episiotomy
• L - Legs back (McRobert’s)
• P - Suprapubic pressure (not fundal)
• E - Enter vagina for shoulder rotation
• R - Reach for posterior arm & deliver posterior shoulder
• R – Roll the patient (Gaskin) – Replace head
– Rotate head to A-P, flex, replace in vagina
– Proceed with emergent C/S

PERSPIRE
• P = Prepare (be prepared, every delivery)
• E = Episiotomy (cut generous epis)
• R = (Mc)Roberts (flex thighs to diameter)
• S = Suprapubic pressure (at MD’s request)
• P = Position (Gaskin maneuver, all 4’s)
• I = Internal (rotation, Wood screw maneuver)
• R = Rotation (presenting part clockwise)
• E = Emergency (fracture of clavicle and/or
Zavanelli maneuver)

Additional Nsg Responsibilities
• Note time head delivers on all deliveries,
call out 1 minute intervals
• Obtain additional help
• Detailed documentation of steps taken
and time for each
• Prepare warmer for resuscitation
• Observe for & be ready for complications
• Assess for fetal fx’s and injury
–Document full movement of arms, etc.

ACOG Committee Opinion, April, 2011
Oyelese Y, Ananth CV, Placental abruption, Obstet Gynecol, 2006
Oct;108(4)
Ananth CV, Kinzler WL, Placental abruption: Clinical Features
and diagnosis, UpToDate, 2014
Oyelese Y, Ananth CV, Placental abruption: Management,
UpToDate 2014
Lockwood CJ, Russo-Stieglitz K, Clinical features, diagnosis, and
course of placenta previa, UpToDate, 2014
Lockwood CJ, Russo-Stieglitz K, Management of placenta previa,
UpToDate, 2014
ACOG Committee Opinion, July, 2012
Resnik R, Management of placenta accreta, increta, and percreta,
UpToDate 2014
Grant, G. Adverse Effects of Neuraxial Analgesia and Anesthesia
for Obstetrics, UpToDate 2014