Embed Size (px)
Citation preview

Alfp
0©d
Reviews www.AJOG.org
PATIENT SAFETY SERIES
Managing disruptive behaviors in the healthcare setting: focus on obstetrics services
Alan H. Rosenstein, MD, MBAth
cavc
D isruptive behaviors in the healthcare setting can have a significant
negative impact on staff relationships,team collaboration, and communicationflow, all of which can impact patient out-comes of care adversely. It is not thatanyone starts out the day planning to bedisruptive, it is just that the stress andpressures of the day may trigger an inap-propriate or disruptive response, whichmay result in behaviors that affect co-workers’ thoughts and actions that caninterfere with process flow and task re-sponsibilities. In most cases, individualsare unaware of the clinical consequencesof their behaviors and the downstreameffect on patient care. With a primarygoal of providing the best quality of carein a safe medical environment, we mustaddress the issue head on. Raising levelsof awareness about the seriousness of theissue, holding individuals accountablefor their behaviors, and providing strat-egies not only to reduce the incidenceand consequences of disruptive eventsbut also to improve efficiency of com-munication and team collaboration arethe crucial steps that are needed to sup-port these organizational objectives.
From Medical Consultant and MedicalDirector Physician Wellness Services, SanFrancisco, CA.
Received June 22, 2010; revised July 9, 2010;accepted Oct. 12, 2010.
Reprints: Alan H. Rosenstein, MD, MBA,Medical Consultant in Care Management andMedical Director Physician Wellness Services,San Francisco, 139 15th Ave., San Francisco,CA 94118. [email protected].
uthorship and contribution to the article isimited to the author. There was no outsideunding or technical assistance with theroduction of this article.
002-9378/$36.002011 Mosby, Inc. All rights reserved.
Coi: 10.1016/j.ajog.2010.10.899
BackgroundDisruptive behaviors in health care havebeen around for years but, until recently,were never really addressed in a consis-tent effective manner. Reasons for the re-luctance to address the issue included ahistory of organizational tolerance thatwas related to the fear of antagonizing aphysician who might threaten to take hisor her patients elsewhere, the hierarchalmedical structure that propagated physi-cian autonomy and authority, the un-written code of silence, concerns aboutconflicts of interest, and the lack of will-ingness, initiative, skill set, and organiza-tional structure needed to address one’speers on behavioral rather than clinicalmatters. With the perception of no harmdone, organizations were content to lookthe other way.
However, things have changed. Firstwas the concern about the growing nurs-ing shortage and the relationship of dis-ruptive behaviors to nurse satisfaction,retention, recruitment, and turnover.1
Second was the growing research thatdocumented the impact of disruptivebehaviors on medical errors, adverseevents, and patient safety.2,3 Third washe requirement to have a disruptive be-avior policy in place as part of the Joint
Disruptive behaviors can have a significantmunication flow, task responsibility, and teimpact patient outcomes of care. Addressinemphasizing the benefits of mutual undersherence to accepted standards of care willprocess and outcomes of care. This is particcare is delivered over a continuum of time,care team playing a vital role as the patiestrategies for success include having stronsupport, raising provider insight and awareprocedures, providing appropriate educataction-oriented interventional support.
Key words: disruptive behavior, obstetrics
ommission Accreditation standard.4
MARCH 2011 Am
Fourth was the relationship of disruptivebehaviors to patient satisfaction, patientcomplaints, and malpractice proceed-ings.5,6 The culmination of these factorsan affect the organization’s reputations a workplace of choice and quality pro-ider, which has both staffing and finan-ial implications.
ResearchWe originally began our research intothe impact of physician disruptive be-haviors on nurse satisfaction and reten-tion during the height of the nursingshortage crisis in early 2000. When wewent to the literature to review the topic,other than finding a few anecdotal re-ports of physicians who yelled at nursesand nurses feeling bad as a result of theinteraction, there were no documentedstudies that related disruptive behaviorto nurse satisfaction. We then decided todevelop our own survey tool. For thepurposes of this survey, disruptive behav-ior was defined as any inappropriate be-havior, confrontation, or conflict, whichranged from verbal abuse (including in-timidation, condescension, or berating,disrespectful, or abusive behaviors) tophysical or sexual harassment. Surveyswere distributed to nurses, physicians,
gative impact on staff relationships, com-collaboration, all of which can adversely
isruptive behaviors in a positive manner byding, shared goals and priorities, and ad-ance communication flow and improve therly relevant in the obstetrics setting, whereh multiple different members of the healthprogresses from labor to delivery. Criticalrganizational commitment and leadershipss, implementing appropriate policies andl and training programs, and facilitating
vice, patient safety, team collaboration
neamg dtanenhulawitntg one
iona
ser
and administrators at �100 acute care
erican Journal of Obstetrics & Gynecology 187

hfdtrdsFoiitbtosm(Csfsgo
Reviews Patient Safety Series www.AJOG.org
hospitals that agreed to participate inthe project. What we found was striking.More than 90% of the respondents re-ported having witnessed disruptive be-havior in physicians, and more than one-third of the respondents reported thatthey were aware of a nurse who left thehospital because of negative interactionswith disruptive physicians.1
Based on comments that were receivedfrom the first phase of the survey, we en-hanced the survey tool to look at not only
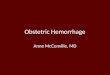
FIGURE 1Linkage between disruptive behavifactors that occur “sometimes,” “f
RN/MD, nurse/doctor.
Rosenstein. Managing disruptive behaviors in obstetrics servi
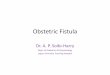
FIGURE 2Linkage of disruptive behavior to uthat occur “sometimes,” “frequent
6671
0
20
40
60
80
100
Ad
vers
e
Even
ts
Err
ors
Perc
en
t
Rosenstein. Managing disruptive behaviors in obstetrics servi
188 American Journal of Obstetrics & Gynecology
physician disruptive behaviors but alsoto assess the incidence of disruptive be-haviors in nurses and other health caredisciplines. We also added a series ofquestions to assess the impact of disrup-tive behaviors on psychologic factorsthat affect emotions and performanceand the linkage of these behaviors tomedical errors, adverse events, and com-promises in patient safety and quality ofcare. What we found is that the incidenceof nurse disruptive behaviors was almost
and undesirable behavioraluently,” and “constantly”
m J Obstet Gynecol 2011.
esirable clinical outcomes” and “constantly”
72
25
75
Safe
ty
Qu
ali
ty o
f
Care
Pati
en
t
Mo
rtali
ty
Pati
en
t
Sati
sfa
cti
on
m J Obstet Gynecol 2011.
MARCH 2011
equal to that of physicians, but it mani-fested in different ways. Physician dis-ruptive behaviors were usually direct andovert and usually subsided after theevent occurred. Nurse disruptive behav-iors, on the other hand, were usuallymore passive-aggressive in nature, had amore continuous undermining currentof activity, and usually occurred morefrequently in a nurse-to-nurse ratherthan a nurse-to-physician encounter.7,8
The most striking findings were in therespondents’ perceptions of the psycho-logic impact of these incidents and theeffect on process and outcomes of care.With the use of a response scale of“never,” “rarely,” “sometimes,” “fre-quently,” and “constantly,” Figure 1
ighlights the high percentage of stress,rustration, loss of concentration, re-uced collaboration, reduced information
ransfer, and reduced communicationesponses that were based on respon-ents rating these factors as occurringometimes, frequently, or constantly.igure 2 highlights the high percentagef adverse events, errors, compromises
n patient safety, compromises in qual-ty, linkage to mortality rate, and nega-ive impact on satisfaction responsesased on respondents rating these fac-ors as occurring sometimes, frequently,r constantly.2,9 Our research and othershowed that these events tended to occur
ore frequently in high-stress areasPerioperative Department, Intensiveare Unit, Emergency Department, Ob-
tetrics Department) and occurred morerequently in certain specialties (generalurgery, anesthesia, cardiovascular sur-ery, cardiology, neurosurgery, neurol-gy, orthopedics, obstetrics).10-14
Cause and effectIn an effort to reduce the incidence ofdisruptive events, it would be helpful tohave a better understanding of the rea-sons these events occur. This is a compli-cated process that involves the interplayof a number of different deeply rootedand situational factors (Table 1).
On the deeply rooted side are the val-ues and preferences that are influencedby age and generation, sex, culture andethnicity, family upbringing, and early
orreq
ces. A
ndly,
53
Pati
en
t
ces. A
life experiences that shape one’s person-

www.AJOG.org Patient Safety Series Reviews
ality and behavioral style. Although it isdifficult to change the resulting attitudesand perceptions that are crafted by theseexposures and experiences, behavioralreactions may be modified by gaining in-sight through the introduction of spe-cialized training programs that focus onsensitivity training, diversity training,and personality management and by theprovision of workshops that are de-signed to improve communication effi-ciency and team collaboration.15
Situational factors that are related tomedical training and work experiences,later life experiences, and current envi-ronmental, home, and work life pres-sures also contribute to one’s demeanorand emotional state that impact behav-ioral responses. Many of these forcesnegatively impact personal satisfaction,which is influenced by growing levels ofstress, frustration, and anger that maylead to burnout, depression, substanceabuse, or severe personality disordersthat affect home and work relation-ships.16-18 Courses in stress manage-ment, anger management, and conflictmanagement may be beneficial in the
TABLE 1Influencing factors
Deep-seated factors..................................................................................................
Age/generation..................................................................................................
Sex..................................................................................................
Culture/ethnicity..................................................................................................
Upbringing/life experiences..................................................................................................
Personality...........................................................................................................
Situational..................................................................................................
Medical training..................................................................................................
Recent life experiences..................................................................................................
Environmental pressures.........................................................................................
Stress/frustration.........................................................................................
Fatigue/burnout.........................................................................................
Depression.........................................................................................
Substance abuse.........................................................................................
Medical/psychiatric illness..................................................................................................
Provoked response: confrontationalconversation
...........................................................................................................
Rosenstein. Managing disruptive behaviors inobstetrics services. Am J Obstet Gynecol 2011.
management of more acute external
pressures. Customized approaches, whichrange from individual coaching and coun-seling to more comprehensive therapy ses-sions, may be indicated, depending on thecircumstances.
Solution strategiesFixing disruptive behavior is no easytask. The ultimate goal is to either pre-vent disruptive events from occurring orto minimize their impact if they do. Theoverall scope of services includes foster-ing a strong organizational commitmentto patient safety, developing appropriatepolicies and procedures, providing edu-cation and training, having a consistentreporting system, and following up ondisruptive events as warranted. Table 2provides a 10-step process that resultedfrom experiences gained from differenthospitals that have taken steps to addressthe problem of disruptive behaviors; thisprocess can be used as a template for or-ganizations that are beginning theirquest.
The first step is organizational com-mitment. The commitment must comefrom top-level governing and leadershipbodies, which include the Board and se-nior-level administrative and clinicalleadership, and must extend to middlemanagement and front-line staff. Theorganization must endorse a no-toler-ance approach toward disruptive behav-iors and be willing to take action whenindividuals refuse to comply with ex-pected behavioral standards. An internalassessment will help to identify potentialopportunities for improvement. Provi-sion of the necessary resources and sup-port to make it happen are crucial to suc-cess. The endorsement of the process bya clinical or project champion will helpto drive the program forward. Thechampion should be a well-respectedpeer, who firmly believes in the projectand has the leadership and communica-tion skills to make it happen.
Raising levels of awareness and ac-countability are important componentsto provide insight, affirm roles and re-sponsibilities, and promote individualengagement. Providing educational pro-grams that highlight the downstreamnegative effect of disruptive behaviors
touches the core nature of medical prac-MARCH 2011 Am
tice. These sessions can be presented at avariety of different levels, includinggrand rounds, department meetings, orunit-based discussions. Target audiencesshould include physicians, nurses, phar-macists, technicians, and other clinicalpersonnel, administration, human re-sources, risk management, patient safety,and quality management. Sessions shouldbe made available to the medical staff, res-ident staff, medical and nursing students,and all hospital staff members who are in-volved in the health delivery process.
The provision of more in-depth struc-tured educational programs is often ben-eficial, depending on the demographicsof the organization. As mentioned ear-lier, there are many deep-seated valuesand attitudes that affect one’s percep-tion that either consciously or subcon-sciously affect one’s behavior. Courseson diversity training, sensitivity training,and differences in generational and cul-
TABLE 2Strategic approach
1. Organizational culture..................................................................................................
Leadership commitment..................................................................................................
Internal assessment..................................................................................................
Infrastructure/resources...........................................................................................................
2. Clinical champions...........................................................................................................
3. Awareness/insight/accountability:general education
...........................................................................................................
4. Structured education/training..................................................................................................
Diversity/sensitivity/conflictmanagement..................................................................................................
Etiquette/assertiveness training...........................................................................................................
5. Communication/team collaborationtools
...........................................................................................................
6. Relationship building...........................................................................................................
7. Policies and procedures...........................................................................................................
8. Reporting/follow-up procedures...........................................................................................................
9. Interventions..................................................................................................
Pre-event..................................................................................................
Concurrent..................................................................................................
Retrospective...........................................................................................................
10. Reinforcement of patient safetyinitiatives
...........................................................................................................
Rosenstein. Managing disruptive behaviors inobstetrics services. Am J Obstet Gynecol 2011.
tural values will help to enhance under-
erican Journal of Obstetrics & Gynecology 189

ardsetat
a
aatccenalibaadtrc
cwcnsttdioetc
lTocabnhfphirhpitapataW
Reviews Patient Safety Series www.AJOG.org
standing of which inherent values andpriorities individuals have that influencethe way they react to others. Other typesof programs that might be offered in-clude courses on stress management, an-ger management, or conflict manage-ment to help staff adjust to the pressuresof the surrounding environment.
Implementation of processes that im-prove communication and team collab-oration skills is a pivotal part of thesolution set. Scripting techniques, suchas the situation/background/assessment/recommendation tool, have been ex-tremely helpful in the improvement ofthe overall efficiency of 1-on-1 commu-nication by providing a template thathelps to organize the delivery of impor-tant information into a format that effec-tively outlines the issues at hand and therequest for response. Some organiza-tions have introduced a linguistic train-ing program to help individuals forwhom English is not the primary lan-guage to learn how to converse more ef-fectively with their colleagues.
Team collaboration tools have beendemonstrated to be of benefit in certainteam settings. Many of these programshave been based on the crew resourcemanagement principles that have beenset forth in the aviation, auto racing, andnuclear power plant industries that out-line the importance of team valuesrelated to trust and respect, role un-derstanding, anticipation, assertiveness,and group discussion. In the obstetricsarea, the results of these programs are alittle more controversial. Some studieshave shown only incremental value;other studies have shown more positiveresults.19-21 Obviously, more studies inthis area are needed.
Communication and team trainingtools provide an operational structure toimprove efficiency of interactions, butthey do not deal with the behind-the-scene differences in assumptions, per-ceptions, biases, conflicting opinions,priorities, and motivations that influ-ence behaviors and the way they impactstaff relationships.22,23 Sitting on top ofthe deep-seated influences posed by gen-eration gaps, sex, cultural, and trainingdifferences is the importance of trust, re-
spect, and mutual understanding. One l190 American Journal of Obstetrics & Gynecology
part of trust and respect is role recogni-tion and competency assurance. Partic-ularly in obstetrics, where the care is de-livered more over a continuum ratherthan as a scheduled timed event or treat-ment for an emergency situation andwhere there may be differences of opin-ion on how best to get there, sharing amutual goal of processes and protocolsthat lead to a safe delivery are key to suc-cess. Physicians must understand thenurses’ role and believe that they arecompetent in carrying out their respon-sibilities. Competency is a combinationof technical competency, knowledgecompetency, and communication com-petency in being able to get the messageacross. Physicians also must understandthe bedside nurse’s priorities for patientcare, discuss the reason that their prior-ities might be diverging from acceptedprocedural guidelines, and make them-selves available to advise and assist in aprofessional manner. Nurses must un-derstand the importance of physicianpriorities to juggle a busy schedule andmaintain work/life balance. Educationand discussion that are based on a truth-ful and open sharing of concerns andpriorities is the best way to achieve ahappy medium. Changing the practicemodel through the use of scheduled in-house coverage (laborists) and changingthe reimbursement model will also helpresolve some of the underlying concernsand priorities.24
As part of its basic structure, the orga-nization must have the right policiesand procedures in place that define ap-propriate behavioral standards and set aprocess for addressing those who arenoncompliant. In 2007, the AmericanCollege of Obstetricians and Gynecolo-gists issued a report that addressed theissues of disruptive behavior.25 In Janu-ry 2009, the Joint Commission issued aequirement that a hospital must have aisruptive policy in place and provideupporting education as one of its lead-rship standards for hospital accredita-ion.26 The policy must be consistentlynd equitably applied across all levels ofhe organization.
Having a consistent action-orientedpproach to event reporting and fol-
ow-up procedures helps to ensure that tMARCH 2011
ll issues are addressed appropriately inn efficient manner. One recommenda-ion is to have a standard process for in-ident reviews performed by a multidis-iplinary committee that is trained tovaluate each event in a professionalonbiased manner and to make theppropriate recommendation for fol-ow-up procedures. Individuals who reg-ster complaints should be given feed-ack to thank them for the report and tossure them that the event will be evalu-ted. Although the specific recommen-ations should not be discussed to main-ain confidentiality, they are requested toeport back if they do not see any notablehanges over a selected period of time.
The intervention cycle is the most cru-ial part of the solution. On the surface,e recommend that the intervention fo-
us on the opportunity to raise aware-ess and facilitate improvement thoughelf-correction, rather than approachinghe incident in a confrontational puni-ive manner. Interventions are best con-ucted by staff members who are trained
n conflict management and dispute-res-lution skills. There should be no appar-nt conflicts of interest or other biaseshat may impede the process and out-ome of these interventions.
Interventions can occur at 3 differentevels. The first level is the preevent stage.he changing health care environmentf increasing complexity, growing ac-ountability, sense of loss of autonomynd control, coupled with reduced reim-ursements, the escalating costs of run-ing a practice, and fears of malpractice,ave led to increasing levels of dissatis-
action, stress, frustration, burnout, de-ression, and more, all of which certainlyave taken their toll on physicians.16 The
dentification of physicians who are atisk early on and a proactive approach inelping them adjust to the surroundingressures of the environment will help to
mprove overall satisfaction and produc-ivity that affect relationships at homend the workplace and have a better op-ortunity for success than waiting for andverse incident to occur.27 Many ofhese services may be available throughn organization’s existing Physician
ellness Committee, Employee Assis-
ance Program, Human Resources De-
tomhtacfatipnocgeapt
tsitmttirt
www.AJOG.org Patient Safety Series Reviews
partment, or Medical Staff Office or canbe made available through a variety ofoutside services that use experts in phy-sician coaching or counseling.
Real-time intervention is necessary toprevent a disruptive event from escalat-ing to a point at which it potentially com-promises staff or patient safety. Theproblem with this is that the hierarchalnature of the medical system perpetuatesa code of silence in which individuals arereluctant to speak up about a negativeincident that involves one of their peers.Courses in assertiveness training andteam training help to emphasize the im-portance of speaking up; however, fearspersist, particularly if it involves a physi-cian who has a history of disruptive be-havior. The rallying point must bearound patient safety. A recent survey ofobstetrics services suggested that the de-cision to speak up is predicated on pro-fessional role, years of experience, andthe perception of potential for harm,with differing perspectives of harm be-tween physicians and nurses. Individualsmust understand that it is their duty tospeak up when they see something iswrong, to be taught how to speak up in aprofessional manner, to feel secure in thefact that the organization is behind them,and to be protected from retaliation.
Interaction after the event falls intoseveral categories. First and easiest to ad-dress is the first-time offender. In manycases the individual was not aware of theconsequences of the behaviors; after aninformal conversation to make the per-son aware of the incident, he/she willtake the necessary steps to correct it.When the level of frequency or intensityescalates, then the intervention shouldinvolve a conversation that is conductedby an individual who is trained in con-flict-resolution skills. Recommenda-tions at this level might include courseson stress management, anger manage-ment, or diversity management or rec-ommendations for therapeutic counsel-ing. Substance abuse must always be keptin mind as a possibility, with appropriatereferrals as indicated. The most difficultsituation occurs with the physician whois resistant to change. In these cases, theorganization must be prepared to sanc-
tion the individual and, if necessary, to cterminate privileges. In all cases, the at-tempt is physician salvage. As are allhealth care professionals, physicians area precious resource, and we must do ourbest to work with them in an effort tohelp them maintain a satisfying produc-tive practice.
In the end, it is all about supportingpatient safety. Programs that are aimedat reducing the incidence of disruptivebehavior must be intertwined with all theother programs and initiatives that en-hance patient safety, quality improve-ment, and risk-management initiatives.
Given the fact that there are multiplefactors that contribute to disruptive be-haviors, it is hard to pinpoint a cause-and-effect relationship as to the benefitof each of these steps in the reduction ofthe occurrence and negative impact ofdisruptive behaviors on patient care.None of the steps are mutually exclusive;in fact, they all enhance the value of eachother. The real question is, are you will-ing to pay the price of not addressingthe problem with only a piecemealapproach?28
ConclusionDisruptive behavior is a difficult issue toaddress. Recent surveys have confirmedthe continued occurrence of disruptivebehavior and its adverse impact on staffrelationships, communication flow, andpatient care.29 Factors that contribute tohis ongoing problem include a historyf tolerance, a complex hierarchic-basededical care system, different stake-
older motivations, priorities and incen-ives to act, and an overall difficulty inddressing behavioral rather than clini-al issues. The problem is compoundedurther in obstetrics services. Issues thatre related to timing, convenience, mo-ivation, priorities, roles and responsibil-ties, and clinical interpretation oftenut a wedge between the physician,urse, and patient. With a primary focusn providing best patient care, physi-ians and nurses must work together toain a better understanding of each oth-rs’ roles, responsibilities, and prioritiesnd come up with a mutually agreed onrocess of care to ensure a positive pa-ient outcome. Organizations must be
ommitted to the process and provideMARCH 2011 Am
he necessary educational and resourceupport to make it happen. Taking a pos-tive supportive approach to identify po-ential problem areas early on and imple-
enting appropriate programs, not onlyo address disruptive behaviors but alsoo enhance opportunities to improve sat-sfaction, communication, and collabo-ation, will provide the best opportuni-ies for success.
CASE EXAMPLE
� Table 2 gives a list of strategies that aredesigned to help organizations to ad-dress disruptive behaviors. Althoughthe model provides a sound concep-tual framework for going forward, inreality, things do not always go ac-cording to plan. It is not that peopledo not know what they must do, it isthe barriers that get in the way of do-ing it. One way to flush out potentialstrategies for action is to use a case ex-ample for group discussion. An illus-trative example selected from actualcaregiver comments is presented.
� Dr Sour is a 55-year-old obstetricianwho brings lots of patients to the hos-pital. He has always had a very strongdemanding personality but recentlyappears to be acting more agitated. Arecent incident occurred in what wasscheduled to be a routine delivery. Inthe course of induction, the nurse be-came concerned about the protocolthat was being used for the pitocindrip and called Dr Sour for clarifica-tion. Dr Sour yelled at the nurse forquestioning him on what he was do-ing and told the nurse that he neededto have the baby delivered by 4:00 PM.He then went on to make a sly remarkabout her training and experience:“Let me know when you finish medi-cal school.” Frustrated and intimi-dated, the nurse continued the dripand then began to notice signs of fetaldistress. Given Dr Sour’s history, shebegrudgingly called Dr Sour again. Heresponded by raising the level of in-tensity by screaming at her and ques-tioning her as to how she had the au-dacity to call him again and said thathe did not want to be bothered unless
there was an emergency. When askederican Journal of Obstetrics & Gynecology 191

Qc
h2p22rtR22h
Reviews Patient Safety Series www.AJOG.org
to come in to evaluate the patient, heagain questioned the nurse about hercompetency and authority and toldher to continue to push the pitocindrip as he had ordered and that hewould come in when the patient wasready to deliver. Stressed and aggra-vated, the nurse called the unitsupervisor.
uestions to consider for discussion in-lude:1. What is the concern?2. What are the underlying issues
(goals/perceptions/motivations/priorities)?
3. What should the nurse do in realtime?
4. How do you think it will go?5. What should the organization do?6. Who will do it?7. How will it be done?8. What else would you like to know
about the situation?9. What can be done to prevent further
incidents like this?10. Describe potential organizational/
personal barriers and how theymight be addressed.
For the correct answers, contactDr Alan Rosenstein at [email protected]. f
REFERENCES1. Rosenstein A. The impact of nurse-physicianrelationships on nurse satisfaction and reten-tion. Am J Nurs 2002;102:26-34.2. Rosenstein A, O’Daniel M. A survey of theimpact of disruptive behaviors and communica-tion defects on patient safety. Jt Comm J QualPatient Saf 2008;34:464-71.3. Simpson K, Kortz C, Knox E. A comprehen-
sive perinatal patient safety program to reduce192 American Journal of Obstetrics & Gynecology
preventable adverse outcomes and costs ofliability claims. Jt Comm J Qual Patient Saf2009;35:565-74.4. Rosenstein A. The Joint Commission disrup-tive behavior standard: intent and impact. Jour-nal of the Association of Staff Recruiters2009;16:6-7.5. Hickson G, Entman S. Physician practice be-havior and litigation risk: evidence and opportu-nity. Clin Obstet Gynecol 2008;51:688-99.6. Clark S, Belfort M, Dildy G, Meyers J. Reduc-ing obstetric litigation through alterations inpractice patterns. Obstet Gynecol 2008;112:11279-83.7. Bartholomew K. Ending nurse-to-nurse hos-tility. Marblehead, MA: HealthPro; 2006.8. Rosenstein A. Differences in disruptive be-haviors. Hosp Health Netw 2010;84:8-10.9. Rosenstein A, O’Daniel M. Disruptive behav-ior and clinical outcomes: perceptions of nursesand physicians. Am J Nurs 2005;105:54-64.10. Rosenstein A, O’Daniel M. Impact and im-plications of disruptive behavior in the peri-operative arena. J Am Coll Surg 2006;203:96-105.11. Rosenstein A, O’Daniel M. Impact of disrup-tive behaviors on clinical outcomes of care.J Neurol 2008;70:1564-70.12. Sexton J, Thomas E, Helmreich R. Error,stress, and teamwork in medicine and aviation:cross sectional surveys. BMJ 2000;320:745-9.13. Baggs J, Schmitt M, Mushlin A, et al. Asso-ciation between nurse-physician collaborationand patient outcomes in three intensive careunits, Crit Care Med 1999;27:1991-8.14. Veltman L. Disruptive behavior in obstetrics:a hidden threat to patient safety. Am J ObstetGynecol 2007;196:587.e1-5.15. Rosenstein A. Measuring and managing theeconomic impact of disruptive behaviors in thehealth care setting: process, policy, preventionand intervention. In: Columbus AM, ed. Ad-vances in psychology research, vol 72. NewYork: Nova Publications New York; 2009:1-14.16. Rosenstein A, Mudge-Riley M. The impactof stress and burnout on physician satisfactionand behaviors. Physician Exec 2010;36:16-23.17. Wetzel C, Kneebone R, Woloshynowych M,et al. The effects of stress on surgical perfor-
mance. Am J Surg 2006;191:5-10. EMARCH 2011
18. Shanafelt T, Balch M, Bechamps G, et al.Burnout and career satisfaction among Ameri-can surgeons. Ann Surg 2009;250:463-71.19. Nielson P, Goldman M, Mann S, et al. Ef-fects of teamwork training on adverse out-comes and process of care in labor and deliv-ery: a randomized control trial. Obstet Gynecol2007;109:48-55.20. Pratt S, Mann S, Salisbury M, et al. Impactof CRM based team training on obstetric out-comes and clinicians’ patient safety attitudes. JtComm J Qual Patient Saf 2007;12:720-5.21. Merien A, Van de Ven J, Mol B, et al. Multi-disciplinary team training in a simulation settingfor acute obstetric emergencies: a systematicreview. Obstet Gynecol 2010;115:1021-31.22. Simpson K, James D, Knox E. Nurse-phy-sician communication during labor and birth:implications for patient safety. J Obstet GynecolNeonat Nurs 2006;35:547-56.23. Simpson K, Lyndon A. Clinical disagree-ments during labor and birth: how does real lifecompare to best practice? Am J Matern ChildNurs 2009;34:31-9.24. Simpson K. Reconsideration of the costs ofconvenience: quality, operational, and fiscalstrategies to minimize elective labor induction. JPerinatol Neonat Nurs 2010;24:43-52.25. American College of Obstetricians and Gy-necologists. ACOG committee opinion on dis-ruptive behavior. Obstet Gynecol 2007;109:1261-2.26. Joint Commission Standard LD.03.01.01.Available at: http://www.jointcommission.org/NewsRoom/PressKits/Behaviors�that�Undermine�a�Culture�of�Safety/app_stds.tm. Accessed July 1, 2010.7. Rosenstein A. Early intervention can helprevent disruptive behavior. Physician Exec009;35:14-5.8. Rosenstein A. The economic impact of dis-uptive behaviors: the risks of non-effective in-ervention. American Society for Healthcareisk Management Publication pending October010.9. Johnson C. Bad blood: doctor-nurse be-avior problems impact patient care. Physician
xec 2009;35:6-11.