Embed Size (px)
Citation preview

Obsessive Compulsive Symptoms in Gilles de laTourette Syndrome and Obsessive CompulsiveDisorder: Differences by Diagnosis and Family History
Valsamma Eapen,1 Mary M. Robertson,1 John P. Alsobrook II,2 and David L. Pauls2*1Department of Psychiatry, University of London, London, United Kingdom2Child Study Center, Yale University School of Medicine, New Haven, Connecticut
The distribution of obsessive compulsivesymptoms was compared in 16 individualswith primary obsessive compulsive disorder(OCD) and 16 individuals with Gilles de laTourette syndrome (GTS) and associatedobsessive compulsive behaviors (OCB). Thetwo groups showed significant differencesin the distribution of OC symptomatology.Furthermore, those OCD probands whoshared a similar symptom profile with GTSindividuals all had a positive family historyof OCD. All of the other OCD probands wereisolated cases. Implications of this findingon the etiology and pathogenesis of the twodisorders are discussed. Am. J. Med. Genet.74:432–438, 1997. © 1997 Wiley-Liss, Inc.
KEY WORDS: Gilles de la Tourette syn-drome; obsessive compulsivedisorder; cluster analyses; fa-milial transmission
INTRODUCTIONGilles de la Tourette syndrome (GTS) is a movement
disorder characterized by multiple motor and one ormore vocal tics. Obsessive compulsive disorder (OCD)is characterized by recurrent obsessions or compul-sions that (1) cause marked distress, (2) are time-consuming (take more than an hour a day), or (3) sig-nificantly interfere with the person’s normal routinefunctioning, social activities, or relationships [Ameri-can Psychiatric Association, 1987]. The occurrence ofobsessive compulsive behaviors (OCB) in GTS has beenthe subject of considerable interest and research in therecent past. OCB occurs in approximately 40% of GTScases [Pauls et al., 1995], a rate significantly higher
than in the general population. Family studies haveprovided further evidence that OCB may be etiologi-cally and genetically related to GTS [Pauls et al., 1986,1991, 1995; Eapen et al., 1993].
Furthermore, Nee et al. [1980] and Cummings andFrankel [1985] also observed that GTS and OCD shareclinical features such as waxing and waning of symp-toms, early age of onset, lifelong course, egodystonicbehavior, and worsening with anxiety. Despite consid-erable overlap in the characteristics of these symp-toms, available evidence suggests that the two condi-tions are not phenomenologically identical and thatOCD may well be a heterogeneous entity, a subtype ofwhich is related to GTS.
Earlier, several investigators attempted to identifyOC symptom subtypes with the goal of finding homog-enous subgroups within OCD patients. Hodgson andRachman [1977], using the Maudsley Obsessive Com-pulsive Inventory (MOCI), described four factors:checking, cleaning, slowness, and doubting. However,the MOCI has an inherent problem of item selectionbias. For example, while checking (9 items) and clean-ing (10 items) symptoms are well-represented, others,such as aggressive obsessions (2 items) and symmetry,ordering, and hoarding compulsions (no items), are un-derrepresented [Goodman et al., 1989a; Rasmussenand Eisen, 1988]. Khanna et al. [1990], in a clusteranalysis of 410 OCD patients assessed using a check-list (developed by the authors but with similar symp-tom selection bias), reported five symptom subgroups:checking, washing, and themes relating to past, death,and sex.
The Yale-Brown Obsessive Compulsive Scale(YBOCS) symptom checklist overcomes the symptomselection bias of the MOCI and provides a comprehen-sive list of more than 50 obsessions and compulsionscomprising 15 general symptom categories [Goodmanet al., 1989a]. Using this checklist, Rasmussen and Ei-sen [1988] found that, in a series of 250 OCD patients,60% had multiple obsessions and 48% had multiplecompulsions. Rettew et al. [1992], using the same in-strument, assessed 79 children and adolescents withOCD and found that 47% had both washing and check-ing compulsions at some time and that none main-tained the same symptom constellation at follow-up
Contract grant sponsor: NINDS; Contract grant number: NS-16648.
*Correspondence to: David L. Pauls, Ph.D., Child Study Cen-ter, Yale University School of Medicine, 230 S. Frontage Road,New Haven, CT 06520. E-mail: [email protected]
Received 13 August 1996; Revised 2 April 1997
American Journal of Medical Genetics (Neuropsychiatric Genetics) 74:432–438 (1997)
© 1997 Wiley-Liss, Inc.

2–7 years later. This suggests that it may not be ap-propriate to categorize patients into mutually exclusivesubgroups such as cleaners or checkers based on symp-toms at a given point. Finally, Baer [1994] completed afactor analysis on YBOCS data collected from 107 in-dividuals with OCD. He found that three factors, ‘‘sym-metry/hoarding,’’ ‘‘contamination/cleaning,’’ and ‘‘pureobsessions,’’ best explained the symptoms of theYBOCS symptom checklist. Of interest is that only thefirst factor was significantly related to obsessive com-pulsive personality disorder or a lifetime history ofGTS.
Several other studies have also attempted to definethe precise phenomenology of OC symptoms in GTS.However, few have attempted to compare them to thesymptomatology that occurs in OCD patients without atic disorder. Pitman et al. [1987] reported that certainkinds of compulsions such as touching and symmetrybehaviors occurred more often in GTS patients than inOCD patients. It has also been suggested that OCsymptoms change in character with age, with youngerpatients exhibiting compulsive behavior related to im-pulse control and older patients being more concernedwith checking and arranging [Frankel et al., 1986]. Neeet al. [1982] suggested that the frequency of OC symp-toms increases with the duration of GTS.
As noted, family studies have demonstrated a famil-ial relationship between OCB and GTS [Pauls et al.,1986, 1991, 1995; Eapen et al., 1993]. However, not allcases of OCD are etiologically related to GTS [Pauls etal., 1995]. An implication of this observation is thatthere may be several subtypes of OCD: one that is ge-netically related to GTS, and others that are not.George et al. [1993] compared 10 OCD patients to 15GTS patients with comorbid OCD. These investigatorsfound that violent, sexual, and symmetrical obsessions,as well as forced touching, counting, and self-damagingcompulsions, were more common in comorbid OCD/GTS subjects, while contamination obsessions andcleaning compulsions were more commonly encoun-tered in OCD subjects without GTS. Similarly, Holzeret al. [1994] reported that patients with a history of ticdisorder had significantly more touching, repeating,self-damaging, counting, and ordering compulsions. Fi-nally, in a study of epidemiologically identified indi-viduals with OCD, Zohar et al. [1997] also found sig-nificantly more touching, repeating, ordering, count-ing, violent, and aggressive behaviors among thoseindividuals with a history of comorbid tics.
A problem inherent in the approach of comparingOCD patients with or without tic disorder is that thereis disagreement as to whether certain symptomsshould be classified as compulsions or as complex mo-tor tics [Shapiro and Shapiro, 1992]. In addition, Leck-man et al. [1993] found considerable overlap betweenGTS and OCD symptoms, in that 93% of their 135 sub-jects with tic disorder reported experiencing premoni-tory urges before performing tics. Thus, it seems thatthe common distinction based on the involuntary andpurposeless nature of tics, as compared to OC symp-toms, is not entirely valid. In addition, phenomenasuch as egodystonicity and resistance are generally dif-ficult to ascertain in a reliable fashion.
An alternate approach to distinguish GTS + OCDsubjects from pure OCD individuals would be to searchfor a symptom profile rather than individual symp-toms. By identifying such phenomenological similari-ties and differences, it might be possible to have a bet-ter understanding of the underlying etiology andpathogenesis of both GTS and OCD.
SUBJECTS AND METHODSThe OCD subjects for this study were recruited from
individuals who were consecutively admitted to OCDspecialty clinics in teaching hospitals in the greaterLondon area. A total of 26 individuals and families wasinvited to participate in a family study of OCD. Sixteenof these individuals did not have a personal or familyhistory of GTS or tics, and were used in the currentstudy. Of these 16, 8 were females and 8 were males;the mean age was 22, with a range from 6–47 years.The GTS subjects for this study were recruited fromindividuals who were consecutively admitted to theGilles de la Tourette Clinic at the National Hospital forNeurology and Neurosurgery, Queen Square, London.Altogether, 40 subjects were recruited to participate ina family study [Eapen et al., 1993]. A total of 18 of theseindividuals with GTS also had OCB. The term OCB isused in this context because, although they had obses-sions and compulsions as detailed in criterion A of theDSM III-R diagnosis, these symptoms did not neces-sarily interfere with social or occupational functioningin these individuals. Of these 18, 16 individuals werematched by age and sex to the sample of OCD patientswithout personal or family histories of tics describedabove, and were included in the present study. Of these16 GTS probands, 7 were females and 9 were males.The mean age was 20, with a range from 6–35 years.
All patients and their relatives were evaluated usingthe National Hospital Interview Schedule (NHIS)[Robertson and Eapen, 1997] for the assessment ofGTS, OCB, and related behaviors, the Yale-Brown Ob-sessive Compulsive Scale adult (YBOCS) and child(CYBOCS) versions, and the Leyton Obsessional In-ventory adult and child versions. All of these instru-ments had been used in previous family/genetic studiesof GTS [Robertson and Gourdie, 1990; Eapen et al.,1993]. In addition, each proband and family memberwas asked to provide family history information abouteach of their first-degree relatives using a semistruc-tured instrument developed for other family studies ofGTS [Pauls et al., 1991] and OCD [Pauls et al., 1995].Thus, for each proband and family member, direct in-terview data as well as family history data were avail-able.
OCD symptom categories that consisted of 10 obses-sion items and 10 compulsion items were constructed,based on the groupings in the YBOCS and the NHIS(see Table I). The YBOCS has 8 categories of obsessionsand 7 categories of compulsions. For the current study,the YBOCS categories of contamination obsessions,sexual obsessions, and somatic obsessions were usedunchanged. Additional categories of obsessions wereconstructed as follows. The miscellaneous category wasdivided into one group of obsessions concerned withreligious obsessions and the need to tell/ask/know and
OC Symptoms in GTS and OCD 433

remember, and another group in which the content ofthe obsessions was primarily focused on the fear of do-ing/saying something embarrassing. In addition, theYBOCS category of aggressive obsessions was dividedinto three groups: 1) violent or horrific images; 2) fearof harming oneself or others; and 3) fear that some-thing bad would happen that was not the direct resultof active aggression on the part of the individual. Thecompulsive categories consisted of the YBOCS catego-ries of repeating rituals, counting, ordering/arranging,hoarding, and checking. The YBOCS category of wash-ing/cleaning was divided into two separate categoriesof washing and cleaning for the current analyses. Themiscellaneous compulsions category was also dividedinto two groups: the first group was characterized bythe need to say or do things ‘‘just right,’’ and the secondwas characterized by forced touching. An additionalcategory of symmetry and exactness compulsions wasincluded to correspond to the obsessional category ofsymmetry and exactness.
Statistical Analysis
Fisher’s exact tests were computed to compare thefrequencies of specific symptoms in the two probandsamples. In addition, t-tests were used to examine themean differences on continuous measures of anxietyand obsessionality. Finally, cluster analyses were per-formed using the SPSS procedure ‘‘Quick Cluster.’’This method groups cases into a predefined number ofclusters using an algorithm based on the nearest cen-troid sorting [Anderberg, 1973]. In this method, theinitial cluster centers (centroids) are estimated fromthe data by defining them as those cases whose dis-tance is farthest apart, thus ensuring that the clusterswill separate the cases well. The distance betweencases is defined as the squared euclidean distance, i.e.,the sum of the squared differences of the values foreach variable. Each subsequent case is assigned to thenearest cluster, i.e., the distance between the case anda centroid is minimized. After all cases are assigned,the centroids are recalculated as the means of all casesin each cluster, and another iteration of case assign-ment is performed until the limiting criterion of mini-mum change or maximum iteration number is reached.Three sets of analyses which specified four, three, andtwo clusters, respectively, were completed.
RESULTS
The distribution of obsessions was quite different be-tween the samples of GTS and OCD patients (see TableII). Sexual (Fisher’s exact test, P 4 0.029) and violent(Fisher’s exact test, P 4 0.004) obsessions were morecommon in the GTS group, and concern for contamina-tion (Fisher’s exact test, P 4 0.009) and fear of some-thing going wrong/becoming ill/or something bad hap-pening (Fisher’s exact test, P 4 0.001) were moreprevalent in the OCD group.
Likewise, the distribution of compulsions differed be-tween the two proband samples (Table III). Symmetry/evening up behaviors (Fisher’s exact test, P 40.0000009), saying or doing things ‘‘just right’’ (Fisher’sexact test, P 4 0.002), and forced touching (Fisher’sexact test, P 4 0.002) were more prevalent in the GTSgroup, and washing (Fisher’s exact test, P 4 0.001) andcleaning (Fisher’s exact test, P 4 0.001) were morecommon in the OCD group.
Since GTS is more common in males, and given thepossibility that sexual and violent obsessions are morelikely to be present in males, we repeated the analysiscontrolling for gender. Sex of the proband did not ac-count for any of these differences. There was a trendwithin the GTS group for females to endorse more oftenthat they had a fear of saying certain things or doingsomething embarrassing. Likewise, males were more
TABLE I. Categories of Obsessions and Compulsions Derived From the YBOCS and National Hospital Interview Schedule
Categories of obsessions Categories of compulsions
Category 1 Obsessions with a sexual theme Category 1 Compulsions involving symmetryCategory 2 Obsessions focused on contamination Category 2 Compulsions involving doing or saying things
‘‘just right’’Category 3 Obsessions focused on the need to know Category 3 Checking compulsionsCategory 4 Obsessions focused on the fear that something
bad would happenCategory 4 Washing compulsions
Category 5 Obsessions with being neat and clean Category 5 Cleaning compulsionsCategory 6 Obsessions with the fear of harming someone Category 6 Compulsions involving forced touchingCategory 7 Obsessions about the fear of saying or doing
something embarrassingCategory 7 Hoarding
Category 8 Obsessions with a violent or sexual theme Category 8 ArrangingCategory 9 Miscellaneous obsessions Category 9 CountingCategory 10 Somatic obsessions Category 10 Repeating rituals
TABLE II. Number of GTS and OCD Probands WithSpecific Obsessions
GTSprobands(n 4 16)
OCDprobands(n 4 16)
Fisher’sexacttest P
Sexual theme 10 3 0.029Dirt/germs/contamination 2 10 0.009Need to tell/ask/know/
remember4 7 0.458
Fear of something goingwrong/something badhappening/becoming ill
2 12 0.001
Neat and clean 3 6 0.433Fear of harming self/others 11 8 0.473Fear of saying or doing
something embarrassing9 6 0.479
Violent/aggressive theme 12 3 0.004Miscellaneous/superstitious 3 6 0.433Somatic obsessions 0 2 0.484
434 Eapen et al.

likely to endorse having ordering and arranging com-pulsions, but neither of the items reached statisticalsignificance.
Next, anxiety and overall obsessional scores werecompared between the two groups. The GTS group hadsignificantly lower scores on the Speilberger StateAnxiety Scale (t 4 −2.97, df 4 22, P 4 0.007) and onthe Leyton Obsessional Trait Scale (t 4 −2.74, df 412.2, P 4 0.018), when compared to the OCD sample(Table IV). There were no statistically significant dif-ferences on the Speilberger Trait or the Leyton Statescales.
Since there was considerable overlap between thetwo samples for some symptoms, cluster analyses wereundertaken to determine if there were different con-stellations of symptoms that would differentiate be-tween individuals. As described earlier, cluster analy-ses were performed using the SPSS procedure ‘‘QuickCluster.’’ This method groups cases into a predefinednumber of clusters using an algorithm based on near-est centroid sorting [Anderberg, 1973].
As noted in Subjects and Methods, analyses wereperformed examining four, three, and two clusters, re-spectively. There was no compelling evidence that thefour- and three-cluster solutions gave different results;analysis of variance suggested that there was not goodseparation of the symptoms into distinct groups. Incomparing the three-cluster solution with the two-cluster solution, it was apparent that two of the threeclusters were simply combined to form cluster 1 of the
two-cluster solution. Furthermore, the distance be-tween the centroids of those two clusters was minimal,whereas both were quite far away from the centroid ofthe third cluster. Finally, in comparing the distributionof symptoms in the three- and two-cluster solutions, itwas apparent that the two-cluster solution resulted ina better separation of individuals into distinct groups.Thus, a solution with two clusters gave the most par-simonious fit to the data.
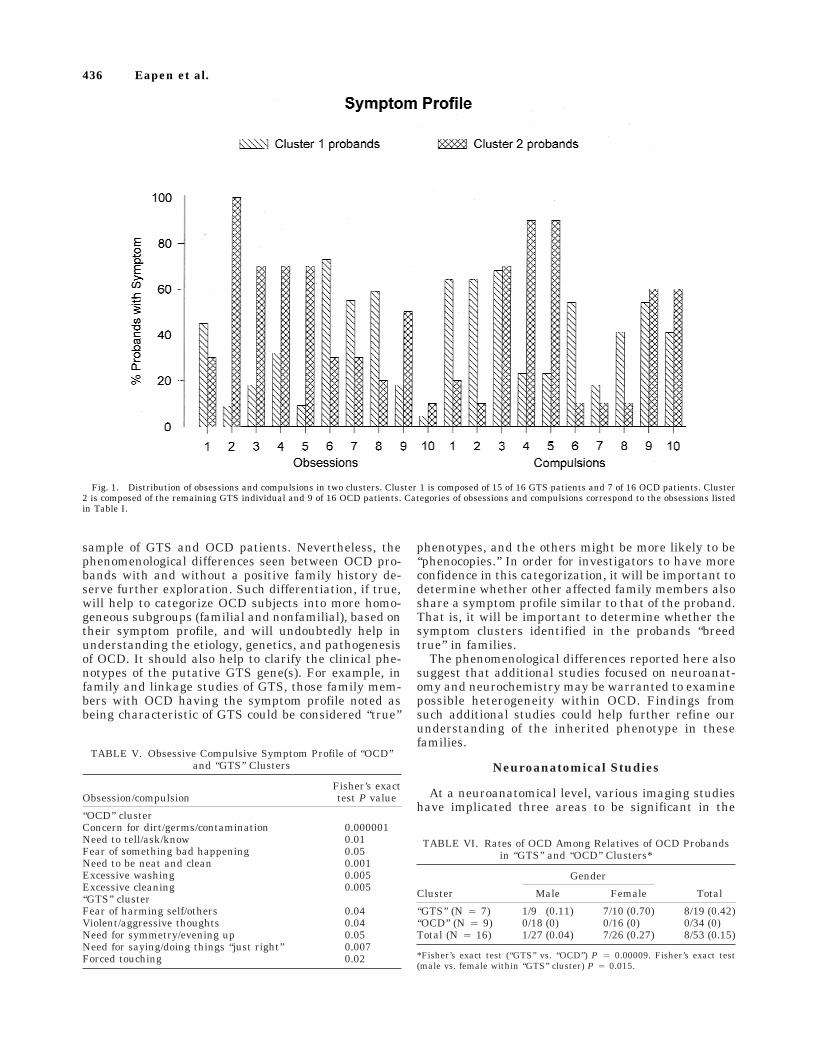
In the two-cluster solution, cluster 1 contained 15 ofthe 16 GTS probands and 7 of the 16 OCD probands.The GTS proband who was not in cluster 1 was a 17-year-old male with other psychopathology, includingpsychosis. In addition to this GTS proband, 9 of the 16OCD probands formed the second cluster. The distri-bution of symptoms in these two clusters is presentedin Figure 1. Note that aggressive obsessions (either toself or others) were more prevalent in cluster 1, andobsessions dealing with contamination and the need toknow characterized the second cluster. Compulsionsthat were more prevalent in the first cluster includedsymmetry, doing things ‘‘just right,’’ and forced touch-ing, while the second cluster was characterized bywashing and cleaning compulsions.
Additional analyses were completed to compare thedistribution of symptoms between the two clusters. The‘‘GTS’’ cluster was characterized by: fear of harmingself/others, obsessions with violent/aggressive themes,symmetry/evening up, saying/doing things ‘‘just right,’’forced touching, and arranging. The items found to becontributing to the ‘‘OCD’’ cluster were: concerns aboutdirt, germs, and contamination, the need to tell, ask, orknow, the fear that something bad was going to hap-pen, the need to be neat and clean, and excessive wash-ing and cleaning (see Table V).
Finally, we examined whether membership in a clus-ter was related to familiality of OCD in families of OCDprobands. Results are presented in Table VI. All of theOCD probands in the ‘‘GTS’’ cluster had at least onefirst-degree relative with OCD, while none of the pro-bands in the ‘‘OCD’’ cluster had a positive family his-tory of OCD. The rate of OCD among relatives of OCDprobands in the ‘‘GTS’’ cluster was 0.42 compared to 0among the relatives of the OCD probands in the ‘‘OCD’’cluster (Fisher’s exact test, P 4 0.00009). Of interest isthat there appears to be a gender difference, with fe-male relatives being more likely to be affected thanmale relatives (Fisher’s exact test, P 4 0.015).
DISCUSSION
These preliminary findings indicate significant dif-ferences in the distribution of OC symptoms betweenOCD and GTS probands. Furthermore, those OCD in-dividuals who share a similar OCD symptom profilewith GTS + OCB individuals are those with a positivefamily history of OCD. This latter finding suggests acommon etiology and pathogenesis for GTS and famil-ial OCD, while implying that alternative mechanismsmay be in operation for nonfamilial OCD.
It is important to raise the caveat that the samplesize in the current study is quite small. It is imperativethat the current findings be replicated in a larger
TABLE III. Number of GTS and OCD Probands WithSpecific Compulsions
GTSprobands(n 4 16)
OCDprobands(n 4 16)
Fisher’sexacttest P
Symmetry/evening up 15 1 0.0000009Saying/doing things
‘‘just right’’13 2 0.0002
Checking 10 12 0.704Washing 2 12 0.001Cleaning 2 12 0.001Forced touching 12 1 0.0002Hoarding 1 4 0.333Arranging 7 3 0.252Counting 8 10 0.722Repeating rituals 5 10 0.156
TABLE IV. Anxiety and Obsessional Scores in GTS andOCD Probands
Mean SD t df P
Speilberger State scoresGTS 41.90 8.56 −2.970 22.0 0.007OCD 53.00 9.54Speilberger Trait scoresGTS 51.54 10.34 −0.429 22.0 0.672OCD 53.30 9.76Leyton State scoresGTS 20.00 8.52 −0.782 22.0 0.442OCD 22.76 8.74Leyton Trait scoresGTS 9.54 4.41 −2.736 12.2 0.018OCD 13.38 1.60
OC Symptoms in GTS and OCD 435
sample of GTS and OCD patients. Nevertheless, thephenomenological differences seen between OCD pro-bands with and without a positive family history de-serve further exploration. Such differentiation, if true,will help to categorize OCD subjects into more homo-geneous subgroups (familial and nonfamilial), based ontheir symptom profile, and will undoubtedly help inunderstanding the etiology, genetics, and pathogenesisof OCD. It should also help to clarify the clinical phe-notypes of the putative GTS gene(s). For example, infamily and linkage studies of GTS, those family mem-bers with OCD having the symptom profile noted asbeing characteristic of GTS could be considered ‘‘true’’
phenotypes, and the others might be more likely to be‘‘phenocopies.’’ In order for investigators to have moreconfidence in this categorization, it will be important todetermine whether other affected family members alsoshare a symptom profile similar to that of the proband.That is, it will be important to determine whether thesymptom clusters identified in the probands ‘‘breedtrue’’ in families.
The phenomenological differences reported here alsosuggest that additional studies focused on neuroanat-omy and neurochemistry may be warranted to examinepossible heterogeneity within OCD. Findings fromsuch additional studies could help further refine ourunderstanding of the inherited phenotype in thesefamilies.
Neuroanatomical Studies
At a neuroanatomical level, various imaging studieshave implicated three areas to be significant in the
TABLE V. Obsessive Compulsive Symptom Profile of ‘‘OCD’’and ‘‘GTS’’ Clusters
Obsession/compulsionFisher’s exacttest P value
‘‘OCD’’ clusterConcern for dirt/germs/contamination 0.000001Need to tell/ask/know 0.01Fear of something bad happening 0.05Need to be neat and clean 0.001Excessive washing 0.005Excessive cleaning 0.005‘‘GTS’’ clusterFear of harming self/others 0.04Violent/aggressive thoughts 0.04Need for symmetry/evening up 0.05Need for saying/doing things ‘‘just right’’ 0.007Forced touching 0.02
TABLE VI. Rates of OCD Among Relatives of OCD Probandsin ‘‘GTS’’ and ‘‘OCD’’ Clusters*
Cluster
Gender
TotalMale Female
‘‘GTS’’ (N 4 7) 1/9 (0.11) 7/10 (0.70) 8/19 (0.42)‘‘OCD’’ (N 4 9) 0/18 (0) 0/16 (0) 0/34 (0)Total (N 4 16) 1/27 (0.04) 7/26 (0.27) 8/53 (0.15)
*Fisher’s exact test (‘‘GTS’’ vs. ‘‘OCD’’) P 4 0.00009. Fisher’s exact test(male vs. female within ‘‘GTS’’ cluster) P 4 0.015.
Fig. 1. Distribution of obsessions and compulsions in two clusters. Cluster 1 is composed of 15 of 16 GTS patients and 7 of 16 OCD patients. Cluster2 is composed of the remaining GTS individual and 9 of 16 OCD patients. Categories of obsessions and compulsions correspond to the obsessions listedin Table I.
436 Eapen et al.

pathophysiology of OCD symptoms: the orbitofrontalcortex, cingulate cortex, and head of the caudatenucleus. It has been postulated that these regions forma circuit that is ‘‘hyperactive’’ in OCD and that theincreased orbitofrontal metabolic activity in patientswith OCD might be a neural substrate for the resis-tance or effort expended to control intrusive thoughts[Insel, 1992]. Consistent with this hypothesis are thefindings of La Plane et al. [1989], who described casesof necrosis of the globus pallidus associated with obses-sional symptoms but with low levels of anxiety andresistance. In the present study, GTS subjects who hadmany of the symptoms of OCD showed lower levels ofanxiety on the Speilberger State Anxiety score andlower scores on the Leyton Obsessional Trait Scale. Itis important to note that functional neuroimagingstudies of GTS individuals have shown ‘‘hypoperfu-sion’’ of the basal ganglia and frontal lobe areas. Thus,it may be that OC symptoms associated with low levelsof anxiety and resistance are linked to ‘‘hypoperfusion.’’On the other hand, it could be postulated that otherspecific types of obsessions associated with consider-able levels of underlying anxiety (e.g., fear of germ/dirt/contamination and fear of something going wrong) andthe compulsions to counter these fears (e.g., washingand cleaning) could be more commonly associated withhyperperfusion, as seen in OCD. It would be interest-ing to compare these measures on OCD individualswho are more similar to GTS + OCB individuals withother OCD and GTS individuals. If the OCD individu-als in cluster 1 were more similar to GTS individualswith OCB, it would provide more evidence for a com-mon pathogenesis for some forms of OCD and GTS.
In a recent GTS family study using single photonemission computed tomography (SPECT) imaging [Mo-riarty et al., 1997], it was noted that the affected familymembers of GTS probands, irrespective of whetherthey had GTS, OCD, or tics, showed hypoperfusion indifferent brain areas. None of the affected subjects, in-cluding those with only obsessive compulsive symp-toms, showed hyperperfusion. These findings are incontrast to the available perfusion findings indicatinghyperperfusion in primary OCD subjects [Baxter et al.,1987; Swedo et al., 1992; Rubin et al., 1992]. It was alsonoted that the State Anxiety scores at the time of in-jection of the dye were lower in ‘‘affected’’ family mem-bers when compared to those in unaffected familymembers. Swedo et al. [1992] found a trend towards apositive correlation between improvement in globalanxiety in response to treatment with a specific sero-tonin reuptake inhibitor (SSRI) and a reduction inright orbitofrontal metabolism in OCD subjects. Thus,it is possible that the difference in perfusion findingsbetween OCD subjects and GTS subjects with OCsymptoms is related to the difference in the anxietylevels of these individuals, which in turn could be re-lated to the specific OC symptom profile of the twogroups.
Neurochemical Studies
At a biochemical level, dopamine is the neurotrans-mitter primarily implicated in GTS, while serotoninhas been implicated in OCD. However, given the com-
plex interactions between dopaminergic and serotoner-gic systems in the brain, it is not surprising that thereis significant overlap in the OC symptoms in GTS andOCD. Considerable preclinical data suggest the exis-tence of anatomic and functional interactions between5-hydroxytryptamine (5HT) and the dopaminergic sys-tems [Graybiel, 1990]. 5HT neurons are believed tomaintain a tonic inhibitory influence on dopaminergicfunction in some regions of the brain, especially themidbrain and brain stem projections to the forebrain[Graybiel, 1990]. The neuroanatomic hypothesis thatthe basal ganglia and their orbitofrontal connectionsmay form the neuronal circuit which subserves OCB iscompatible with the neurochemical hypothesis that the5HT and dopaminergic systems may play a role in thepathophysiology of at least GTS-spectrum OCD. And ifthe current findings are true, they may also play a rolein some forms of familial OCD.
McDougle et al. [1994], in a study of treatment-resistant OCD patients, found that comorbid tic spec-trum disorders were associated with a positive re-sponse to the addition of neuroleptic to a specific sero-tonin reuptake inhibitor (SSRI) drug. George et al.[1993] also reported a synergistic effect with a combi-nation of a neuroleptic and an SSRI in the treatment ofGTS patients with OC symptoms, while the SSRI byitself caused worsening of GTS symptoms, and the neu-roleptic alone was not effective in controlling the OCsymptoms. Thus phenomenological and neuroimagingdata, as well as the pharmacological treatment profile,suggest that there may be etiologically distinct sub-groups within the OCD population.
CONCLUSIONS
Although the neurochemical mechanisms and ana-tomical substrates involved in GTS have not beenclearly identified, there is a considerable body of evi-dence to suggest that basal ganglia and related corticaland thalamic structures are involved in GTS and OCD[Chappell et al., 1990]. The evidence comes from im-munohistological studies in animals [Lavoie et al.,1992], postmortem studies of GTS patients [Singer,1992; Anderson et al., 1992], and neuroimaging studies[Riddle et al., 1992; Brooks et al., 1992].
The combination of somatosensory urges and frag-mentary motor behaviors is consistent with the in-volvement of the cortico-striato-thalamo-cortical cir-cuits that channel and subchannel information in-volved in the anticipation and performance of motorbehaviors. The existence of contiguous projection areaswithin the striatum from both the motor and sensori-motor cortical areas suggests that these projectionsmay be involved in GTS and, if the current data arecorrect, in some forms of OCD.
Other aspects of the circuitry of the basal gangliamay provide important clues concerning anatomic dis-tribution of tics in GTS as well as the themes and con-tent of obsessions and compulsions in OCD. An abnor-mality in the function of dopamine in the substantianigra or receptors in the striatum, even if limited to asmall region, could affect wide areas of the cortico-striatal loops, modulating and integrating both limbic
OC Symptoms in GTS and OCD 437

and frontal motor circuits. Thus, the site and extent ofinvolvement of these structures and their connections,as well as other modifying factors such as age, sex, anddevelopmental stage of the individual concerned, could,in turn, determine the clinical presentation and thesymptom profile.
The findings in the current study give additionalsupport to the hypothesis that there is an etiologicalrelationship between the obsessive compulsive behav-iors seen in GTS patients and those seen in some OCDindividuals. Of interest is that individuals with OCDwho share the OCD symptom profile seen in individu-als who have both GTS and OCB appear to be muchmore likely to have a familial form of OCD. These re-sults, if true, suggest a series of additional researchendeavors that could help to elucidate more homoge-neous groups of OCD individuals, which in turn couldhelp to clarify the underlying genetic mechanisms ofthis complex disorder.
ACKNOWLEDGMENTSThis work was supported in part by a National In-
stitute of Mental Health Research Scientist Award toD. Pauls (MH-00508) and by National Institute of Neu-rologic Disease and Stroke grant NS-16648.
REFERENCESAmerican Psychiatric Association (1987): ‘‘Diagnostic and Statistical
Manual of Mental Disorders, 3rd Edition, Revised.’’ American Psychi-atric Association, Washington, DC. pp. 234–235.
Anderberg M (1973): ‘‘Cluster Analysis for Applications.’’ New York. Ple-num Press. pp. 43–57.
Anderson GM, Pollak ES, Chatterjee D, Leckman JF, Riddle MA, CohenDJ (1992): Postmortem analysis of subcortical monoamines and aminoacids in Tourette syndrome. Adv Neurol 58:123–133.
Baer L (1994): Factor analysis of symptom subtypes of obsessive compul-sive disorder and their relation to personality and tic disorders. J ClinPsychiatry 55 Suppl:18–23.
Baxter LR, Phelps ME, Mazziotta JC, et al. (1987): Local cerebral glucosemetabolic rates in obsessive compulsive disorder: A comparison withrates in unipolar depression and in normal controls. Arch Gen Psychia-try 44:211–218.
Brooks DJ, Turjanski N, Sawle GV, Playford ED (1992): PET studies on theintegrity of the pre and postsynaptic dopaminergic system in Tourettesyndrome. Adv Neurol 58:227–231.
Chappell PB, Leckman JF, Pauls DL, Cohen DJ (1990): Biochemical andgenetic studies of Tourette’s syndrome: Implications for treatment andfuture research. In Deutch SI, Weizman A, Weizman R (eds): ‘‘Appli-cation of Basic Neuroscience to Child Psychiatry.’’ New York: PlenumMedical Book Company.
Cummings JL, Frankel M (1985): Gilles de la Tourette syndrome and theneurological basis of obsessions and compulsions. Biol Psychiatry 20:1117–1126.
Eapen V, Pauls DL, Robertson MM (1993): Evidence for autosomal domi-nant transmission in Tourette’s syndrome—United Kingdom CohortStudy. Br J Psychiatry 162:593–596.
Frankel M, Cummings JL, Robertson MM, Trimble MR, Hill MA, BensonDF (1986): Obsessions and compulsions in Gilles de la Tourette’s syn-drome. Neurology 36:378–382.
George MS, Trimble MR, Ring HA, et al. (1993): Obsessions in obsessivecompulsive disorder with and without Gilles de la Tourette’s syndrome.Am J Psychiatry 150:93–96.
Goodman WK, Price LH, Rasmussen SA, Mazure C, Fleischmann RL, HillCL, Heninger GR, Charney DS (1989a): The Yale-Brown ObsessiveCompulsive Scale. I. Development, use and reliability. Arch Gen Psy-chiatry 46:1006–1011.
Goodman WK, Price LH, Rasmussen SA, Mazure C, Delgado P, HeningerGR, Charney DS (1989b): The Yale-Brown Obsessive CompulsiveScale. II. Validity. Arch Gen Psychiatry 46:1012–1016.
Graybiel AM (1990): Neurotransmitters and neuromodulators in the basalganglia. Trends Neurosci 13:244–254.
Hodgson RJ, Rachman S (1977): Obsessional-compulsive complaints. Be-hav Res Ther 15:389–395.
Holzer JC, Goodman WK, McDougle CJ, Baer L, Boyarsky BK, LeckmanJF, Price LH (1994): Obsessive-compulsive disorder with and without achronic tics disorder. A comparison of symptoms in 70 patients. Br JPsychiatry 164:469–473.
Insel TR (1992): Toward a neuroanatomy of obsessive compulsive disorder.Arch Gen Psychiatry 49:739–744.
Khanna S, Kaliaperumal VG, Channabasavanna SM (1990): Clusters ofobsessive-compulsive phenomena in obsessive-compulsive disorder. BrJ Psychiatry 156:51–54.
La Plane D, Levasseur M, Pillon B, et al. (1989): Obsessive compulsive andother behavioural changes with bilateral basal ganglia lesions. Brain112:699–725.
Lavoie B, Cote PY, Parent A (1992): Immunohistochemical study of thebasal ganglia in normal and parkinsonian monkeys. Adv Neurol 58:115–121.
Leckman JF, Walker DE, Cohen DJ (1993): Premonitory urges in To-urette’s syndrome. Am J Psychiatry 150:98–102.
McDougle CJ, Goodman WK, Leckman JF, et al. (1994): Haloperidol addi-tion in fluvoxamine refractory obsessive compulsive disorder. Arch GenPsychiatry 51:302–308.
Moriarty J, Eapen V, Costa DC, et al. (1997): HMPAO SPECT does notdistinguish obsessive compulsive and tic syndromes in families multi-ply affected with Gilles de la Tourette syndrome. Psychological Med (inpress).
Nee LE, Caine ED, Polinsky RJ, Eldridge R, Ebert MH (1980): Gilles de laTourette syndrome: Clinical and family study of 50 cases. Ann Neurol7:41–49.
Nee LE, Polinsky RJ, Ebert MH (1982): Tourette syndrome: Clinical andfamily studies. In Chase TN, Friedhoff AJ (eds): ‘‘Gilles de la TouretteSyndrome.’’ New York: Raven Press, pp 291–295.
Pauls DL, Towbin KE, Leckman JF, Zahner GEP, Cohen DJ (1986): Gillesde la Tourette syndrome and obsessive compulsive disorder: Evidencesupporting an etiological relationship. Arch Gen Psychiatry 43:1180–1182.
Pauls DL, Raymond CL, Leckman JF, Stevenson JM (1991): A family studyof Tourette’s syndrome. Am J Hum Genet 48:154–163.
Pauls DL, Alsobrook JP II, Goodman W, Rasmussen S, Leckman JF (1995):A family study of obsessive compulsive disorder. Am J Psychiatry 152:76–84.
Pitman RK, Green RC, Jenike MA, Mesulam MM (1987): Clinical compari-son of Tourette’s disorder and obsessive-compulsive disorder. Am JPsychiatry 144:1166–1171.
Rasmussen SA, Eisen JL (1988): Clinical and epidemiological findings ofsignificance to neuropharmacologic trials in OCD. PsychopharmacolBull 24:466–470.
Rettew DC, Swedo SE, Leonard HL, Lenane MC, Rapoport JL (1992):Obsessions and compulsions across time in 79 children and adolescentswith obsessive-compulsive disorder. J Am Acad Child Adolesc Psychia-try 31:1050–1056.
Riddle MA, Rasmusson AM, Woods SW, Hoffer PB (1992): SPECT imagingof cerebral blood flow in Tourette syndrome. Adv Neurol 58:207–211.
Robertson MM, Eapen V (1997): The National Hospital Interview Schedulefor the assessment of Gilles de la Tourette syndrome and related be-haviours. Int J Res Methods Psychiatry (in press).
Robertson MM, Gourdie A (1990): Familial Tourette’s syndrome in a largeBritish pedigree. Associated psychopathology, severity, and potentialfor linkage analysis. Br J Psychiatry 156:515–521.
Rubin RT, Villanueva-Meyer J, Ananth J, et al. (1992): Regional xenon 133cerebral blood flow and cerebral technetium 99m HMPAO uptake inunmedicated patients with obsessive compulsive disorder and matchednormal control subjects. Arch Gen Psychiatry 49:695–702.
Shapiro AK, Shapiro E (1992): Evaluation of the reported association ofobsessive compulsive symptoms or disorder with Tourette’s disorder.Compr Psychiatry 33:152–165.
Singer HS (1992): Neurochemical analysis of postmortem cortical andstriatal brain tissue in patients with Tourette syndrome. Adv Neurol58:135–144.
Swedo SE, Pietrini P, Leonard HL, et al. (1992): Cerebral glucose metabo-lism in childhood onset obsessive compulsive disorder: Revisualizationduring pharmacotherapy. Arch Gen Psychiatry 49:690–694.
Zohar AH, Pauls DL, Apter A, Dycian A, Kron S, Binder M, King R, Leck-man JF, Cohen DJ (1997): OCD with and without tics in an epidemio-logical sample of Israeli adolescents: Are they distinct subtypes? Am JPsychiatry (in press).
438 Eapen et al.























