Embed Size (px)
Citation preview

J. Neurol. Neurosurg. Psychiat., 1965, 28, 362
Observations on the pathology ofthe Moebius syndrome
SAMUEL E. PITNER, JAMES E. EDWARDS,' AND WILLIAM F. MCCORMICK2
From the Section of Neurology, Department ofPediatrics, and the Section of Neuropathology, Department ofPathology, of the University of Tennessee and the City of Memphis Hospitals, Memphis, Tennessee, U.S.A.
The first report of the congenital facial diplegiasyndrome, or Moebius syndrome, was that ofGraefe (1880). Moebius reported cases in 1888 and1892 and reviewed the prior case reports, thus gain-ing eponymic distinction. Since that time, someauthors have broadened the definition of theMoebius syndrome, as for example, Henderson(1939), who considered some cases of congenitalunilateral facial palsy to belong to the syndrome.We would agree with the definition of Van Allen andBlodi (1960) that the syndrome consists of varyingdegrees of facial paresis, usually a facial diplegia,associated with an apparent paralysis of lateral gaze.This is frequently associated with paresis of othermuscles supplied by the motor cranial nerves, andwith other deformities such as micrognathia, talipes,and the congenital absence of various muscles,particularly the pectoral group. The condition iscongenital and not progressive; the clinical featureshave been reviewed in detail by Henderson (1939).Cases of congenital unilateral facial paralysis withoutother facial muscular weakness or musculo-skeletalanomalies (Richter, 1958 and 1960) and a case ofcongenital bilateral sixth nerve palsy (Phillips,Dirion, and Graves, 1932) possibly represent a formefruste of the syndrome. The syndrome of congenitalflaccid bulbar palsy (Graham, 1964) probablyrepresents essentially the same disorder with pro-minent bulbar symptoms. Some cases of congenitallaryngeal abductor paralysis could represent avariant of the Moebius syndrome, as pointed out byPlott (1964).Only three histological examinations of undis-
puted cases of the complete syndrome could befound (Heubner, 1900; Spatz and Ullrich, 1931;Wallis, 1960); the last author did not report thepathological findings in detail. Two other patho-logical reports (Fenyes, 1937; Riggs, 1958) have beenchallenged by some (Henderson, 1939; Richter,1958) as representing intrapartum brain-stem'Present address: Department of Psychiatry, Washington University,St. Louis, Missouri.'Present address: Section ofNeuropathology, Department of Pathology,State University of Iowa, Iowa City, Iowa.
haemorrhage rather than a true congenital anomaly.Henderson (1939) and Richter (1960) also believe thata case reported by Rainy and Fowler (1903) wasprobably due to trauma to both facial nerves byobstetrical forceps. Pathological examination in theabove cases, except those of Heubner (1900) and ofRainy and Fowler (1903), was limited to the brain;the peripheral portion of the seventh nerve and itsmuscles were not examined. Of the 'partial' forms ofthe syndrome, the central nervous system pathologyin a case of congenital bilateral abducens palsyhas been reported (Phillips et al., 1932) and theneuropathological findings in a case of congenitalunilateral facial paralysis not associated with otherdefects has also been described (Richter, 1958 and1960). In none of these reports have the involvedcranial nerves (when present) been examined in theirextracranial courses, nor are any authors besidesHeubner (1900) and Rainy and Fowler (1903),whose case probably does not represent a truecongenital defect, known to have examined any of theparalytic musculature. Isolated examinations ofinvolved facial or extra-ocular muscles by biopsieshave been reported by several authors (Richards,1953; Yasuna and Schlezinger, 1955; Reed andGrant, 1957; Van Allen and Blodi, 1960; andGraham, 1964). These authors had no opportunityto examine the brain.The purpose of this report is to present the patho-
logical findings in the brain, facial nerves, and in-volved facial muscles of an infant with the Moebiussyndrome, and to comment on the speculations thathave been put forward concerning its aetiology. Toour knowledge, this is the only case of the Moebiussyndrome in which all of the above structures havebeen examined.
CASE REPORT
This white male infant was first seen at 30 hours of agebecause of facial diplegia and poor feeding. He was thethird child of a 22-year-old mother. Pregnancy had beencomplicated by mild vomiting throughout, and by mildpedal oedema in the third trimester. Labour and delivery
362
Protected by copyright.
on March 3, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.28.4.362 on 1 August 1965. D
ownloaded from

Observations on the pathology of the Moebius syndrome
were uneventful. The child had a birth weight of 6 lb.101 oz., and was described as having a prompt, althoughnot vigorous, cry. A right facial paralysis had been notedby the obstetrician at the time of delivery. Initial feedingshad been offered at 12 hours of age and were taken poorly.There was no family history of any similar condition.
General physical examination revealed mild micro-gnathia and an increased antero-posterior diameter of thechest without definite evidence of emphysema or chestwall deformity. There was no evidence of trauma. Nomusculo-skeletal anomalies were found; all somaticmuscle groups were thought to be normal. On the initialand subsequent neurological examinations the followingfindings were present: facial diplegia, most marked on theright side; inability to abduct either eye beyond the mid-line, with the other ocular movements intact; normalpupillary responses and fundi; equivocally decreasedsensation to pin prick over the right face and a con-sistently absent right corneal reflex; bilateral decreaseof palatal elevation on gagging; bilateral decrease in thestrength of the masseter muscles; and atrophy of the rightside of the tongue, without fasciculati3on, and with devia-tion to the right on protrusion. Function of the othercranial nerves was intact and the remainder of theneurological examination was normal.
Routine blood counts and urine analyses were normal.Radiographs of the skull were normal, but those of thechest showed bilateral pneumonitis, which did not clearcompletely throughout the infant's hospital course.Lumbar punctures and subdural taps were normal.Electromyography and muscle biopsy were planned, butcould not be carried out due to the moribund conditionof the patient.The hospital course was one of progressive deteriora-
tion, marked by recurrent aspiration pneumonia. Thisoccurred in spite of a gastrostomy for feeding (done at20 days of age), postural drainage, continuous naso-pharyngeal suction, and appropriate antibiotic therapy.Continuous oxygen therapy was required throughout the
FIG. 1. Photograph of the patient (asleep) at 1 monthof age.
patient's life to prevent cyanosis. The infant succumbedto aspiration pneumonia at 48 days of age. His appearanceat one month of age is shown in Figure 1.
NECROPSY The general necropsy was performed 16hours after death. Dissection of the facial musculature andthe removal of the petrous portion of the temporal boneswere done after embalming, and approximately 30 hoursafter death.The only significant finding, either grossly or micro-
scopically, outside of the brain, middle and inner ears,and facial musculature was in the respiratory system
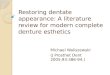
FIG. 2. Gross section of the brain-stem, showing theasymmetry of the two sides, the indistinct olive on the left,and the smaller olivary prominence on that side ( x 4).
363
Y.
.4
.:F: .:i:;,-
Protected by copyright.
on March 3, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.28.4.362 on 1 August 1965. D
ownloaded from

64Samuel E. Pitner, James E. Edwards, and William F. McCormick
where bilateral aspiration bronchopneumonia waspresent. Multiple samples of somatic muscles andperipheral nerves were normal. No description of theremainder of the organs is deemed necessary, exceptto note that no malformations were found.The petrous portions of the temporal bones were re-
moved en bloc and decalcified in 5% formic acid. Thedecalcified blocks were cut at 3 mm. intervals and sub-serially sectioned following double embedding in celloidinand paraffin wax. The middle ears and mastoid air cellswere free of exudate; the internal acoustic meati werenormal bilaterally.
Dissection of the face after embalming revealed arelative increase in subcutaneous fat and an almost totalabsence of muscle; tissue recognizable as muscle wasfound only in the orbicularis oris, the buccinator, andthe zygomaticus. The great majority of the facial musclescould not be identified. The dissection of the face waslargely limited to the right side, but the incompletedissection of the left side also revealed little recognizablemuscle. Both eyes were removed and appeared normalgrossly, as did their attached muscles. Hemi-atrophyof the tongue was confirmed.The brain was of normal size for an infant 7 weeks of
age. The cerebral hemispheres were symmetrical and thegyri and sulci were ofnormal size, shape, and distribution.The leptomeninges were thin and transparent throughout;no haemorrhage or exudate was present in the sub-arachnoid space. The vessels of the circle of Willis werefree of abnormalities. There were no cerebral hernias.The only abnormalities on gross examination were in thecerebellum and brain-stem, where it was noted that theleft olivary prominence was missing (Fig. 2); there wasalso moderate hypoplasia of the right cerebellar hemi-sphere, maximal in the ansiform lobule and biventer(Fig. 3). All of the cranial nerves could be identified onthe gross specimen and appeared to be normal.
Serial sections of the cerebral hemispheres at 05 cm.intervals revealed moderate congestion of the vessels inthe centrum semiovale, a small cavum septi pellucidi,and no abnormalities of the ventricles or basal ganglia.Sections of the brain-stem at 3 mm. intervals showed al-most complete absence of the left inferior olivary nucleus.No abnormalities could be seen grossly in the mesence-phalon or pons. The aqueduct of Sylvius and the fourthventricle were normal. Sections of the cerebellum at 4 mm.intervals revealed microgyria of the right hemisphericfolia with no apparent involvement of the vermis. The
FIG. 3. A low-power view of the cerebellum showing the presence ofpolymicrogyria on the right, and the absence of theipsilateral dentate nucleus (haematoxylin and eosin x 2).
364
Protected by copyright.
on March 3, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.28.4.362 on 1 August 1965. D
ownloaded from

Observations on the pathology of the Moebius syndrome
right dentate nucleus was very small and indistinct, andthere was less conspicuous reduction in size of the rightemboliform nucleus (Fig. 3).The gross neuropathological diagnosis was congenital
hypoplasia of the cerebellum and facial musculature.
MICROSCOPIC Multiple sections from the cerebralhemispheres (right and left superior frontal gyri, rightand left basal ganglia, left calcarine cortex, and threecoronal sections of the cerebri), stained with haematoxylinand eosin, thionine (Nissl), luxol fast blue-P.A.S.H.,phosphotungstic acid-haematoxylin, Weil's and Bodian'sstains, were prepared for examination. Numerous neu-rones in multiple areas were undergoing eosinophilic(anoxic) necrosis, and were most numerous in the superiorfrontal gyri and in the hippocampal gyri. True sectornecrosis was not present. Myelination was normal for aninfant of 7 weeks. Marked vascular congestion was presentin all sections. Multiple discrete foci of neuroblasts werepresent about veins in the subependymal plate; these weremaximal adjacent to the bodies of the caudate nuclei.
Multiple sections of the cerebellum were taken so as toinclude both hemispheres, the mid-line nuclei and thevermis (Fig. 3). The same battery of special stains wasdone on the cerebellum as on the cerebrum. Immaturity,as evidenced by a thick outer granular layer and incom-pletely myelinated white matter, was noted. Vasculardilatation and congestion was present, as was anoxic
necrosis of moderate numbers of Purkinje cells. Theneurones of the right dentate nucleus were greatlyreduced in number. Moderate astrogliosis was presentin the dentate nucleus. Mild to moderate neuronal losswith mild gliosis was present in the adjacent emboliformnucleus. The mid-line nuclei on the left were present innormal numbers. Polymicrogyria was conspicuous in theright hemispheric folia (Fig. 3), while the folia of thevermis and left hemisphere wcre normal. All layers of thefolia in the right hemisphere were abnormal, but paucityof neurons was most marked in the inner granular layer.Gliosis was relatively mild. Myelination of the convo-lutional and central white matter was more completeon the left than on the right. There was no evidence of aninflammatory process, remote haemorrhage, or activecellular degeneration, other than anoxic, in the cere-bellum.
Subserial sections of the mid-brain, pons, and medullawerc examined with the use of the special stains. Theabnormalities consisted of an almost complete absence ofthe inferior olivary nucleus on the left and a moderatedecrease in the prominence of the restiform body on theright (Fig. 4); marked hypomyelination and hypoplasiaof the right brachium conjunctivum and central tegmentaltract in the pontine sections (Fig. 5); and hypomyelina-tion of the right superior colliculus in the mesencephalicsections. All cranial nerve nuclei and fibres appearedwell preserved. The facial nuclei were of equal size and
_ _ - ;-
FIG. 4. Weil stain of the rostral medulla, showing the virtual absence of the left olive and the course of the facial nerves(x 10).
365
Protected by copyright.
on March 3, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.28.4.362 on 1 August 1965. D
ownloaded from

Samuel E. Pitner, James E. Edwards, and William F. McCormick
FIG. 5. Section of the pons showing the small and hypo-myelinated left brachium conjunctivum (Luxol-Fast Blue)P.A.S.-H., x 8).
FIG. 6. Nissl stain of the caudalpons showing one of thefacial nuclei (x 60). These were identical and were notthought to show any abnormality.
.:
.: ^ :. .:0s; b.
... r .:... .. _
.... .... .....Sl.
iL-... d: .:.0 .e,., #* 0/ s a_ ... U , :o .
.. j.;.'.. ' .......... .... : ........ ...
| ::.,, . . .. +:. E..
t ^ ;fS
o .............. ... . ........ ... .s
$_ _..X.. ts
II | .............. C .0g F .... t . ;. * .,>:Y X,itE,$s ... ':o '.° > . .. ' . 8
.:. :. :: .: h
*t :-: ^:::
1?!i,* .. ^ : ' +..: :::.. -̂* :. .. :g
... ....* .. . ' .aS..... _.
FIG. 5.
jr.
FIG6 *t 'S#+ s *LSt %i ;;, ssy ; ;
FIG. 6.
366
...
l,-.
Protected by copyright.
on March 3, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.28.4.362 on 1 August 1965. D
ownloaded from

Observations on the pathology of the Moebius syndrome 36o
FIG. 7. Section of the<9=- +>% S4¢vst<|^c.t$%wxinner ear showing compo-'I'='4' 2' / ~~~nents of cranial nervesVII, VIII, and IX
1A ~~~~~~~~~~~~~~~(haematoxylin and eosin,x 8). These are thought
4 ggautolytic changes.
FLoS;'C;P
V,~~N6.~.#~~~~~~~~~~~~ 9' .9 9t.
FIG. 8. Inner ear at thelevel of the oval window,showing portions ofcranial nerves VII andVIII (haem-atoxylin andeosin, x 20); incidentalotosclerosis is present.
Is -117
AL.
Protected by copyright.
on March 3, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.28.4.362 on 1 August 1965. D
ownloaded from

'4
FIG. 9. Section of the right Gasserian ganglion, which is thought to be normal (Bodian, x 60).
FIGS. 10 AND 11. Muscle from the right buccinator, showing (left) adipose and fibrous 'replacement' of the muscle(haematoxylin and eosin, x 100), and (right) a more involved area at a higher power (x 200).
,.,
Protected by copyright.
on March 3, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.28.4.362 on 1 August 1965. D
ownloaded from

Observations on the pathology of the Moebius syndrome
cellularity, and were considered to contain normal num-bers of neurons (Fig. 6). The individual neurons appearednormal. The facial nerves could be identified in theirintraparenchymal course, as well as in the subarach-noid space, and also appeared normal.
Examination of the subseriel sections of the petrousportions of the temporal bones revealed no significantabnormalities and demonstrated the presence of the intra-osseous portions of cranial nerves VII, VIII, and IX(Fig. 7). Autolytic and embalming artefacts prevented adetailed evaluation of the fine structure of the facialnerves in the temporal bone, but they appeared normal(Fig. 8). Otosclerosis was an incidental finding on the right
E side. Sections of the Gasserian ganglia revealed normalstructures (Fig. 9). Autolytic changes were moderate inits neurones, but no significant decrease in the number ofneurones could be seen. The axons of the trigeminal nervewere intact.Normal nerve trunks thought to represent the more
peripheral branches of the facial nerves were seen passingthrough the parotid glands in sections of those organs.
Multiple sections of the facial and extraocular muscleswere prepared with haematoxylin and eosin, trichrome,phosphotungstic acid-haematoxylin, Bielschowsky's,and Bodian's stains. The extraocular muscles were normal.A decrease in the bulk of the right side of the tongue wasapparent, but no definite microscopic changes were foundin the muscle fibres. Severe alterations of the facialmuscles were present. The primary finding was a decreasein the number of myofibres present, ranging from verysevere (Fig. 10) to moderate (Fig. 11). Those myofibrespresent were generally small, ranging from 4 ,t to 30 ,t indiameter. Variation in myofibre size was conspicuous,but not to the degree usually seen in an active and pro-gressive dystrophic process. Fine structural analysis ofthe muscle was not completely satisfactory due to auto-lytic and embalming artefacts. It appeared from thearrangement of fibrous elements in the sections that somemuscle fascicles had formed. Although fibrosis was mildto moderate, adipose 'replacement' of muscle was severe.There was nothing to indicate active degeneration orregeneration of muscle, nor was there any phagocytosisof muscle apparent. Migration of sarcolemmal nuclei wasnot prominent. The changes did not have the distributionof a typical neurogenic atrophy, and nerve fibres werepresent among the identifiable muscles and in the adiposetissue. While in the absence of satisfactory motor endplate stains they could not be proven to be motor fibres,it was felt probable that many were. The changes werethought to represent a primary failure of formation,differentiation, or maintenance of the involved muscle,rather than changes secondary to a neuronal dysplasia ordegeneration.The microscopic neuropathological diagnosis was
congenital cerebellar hypoplasia with associated changesin the midline cerebellar nuclei, pons, and olives; uni-lateral otosclerosis; and probable primary dysplasia ofthe facial muscles.
DISCUSSION
Throughout the literature of the Moebius syndrome,
most authors, with or without pathological evidence,have speculated concerning the responsible defect.Moebius (1892) thought that the disorder wasdegenerative in nature (infantiler Kernschwund). Inthe absence of morphological evidence of degenera-tion, most later authors have felt that this view wasincorrect. The various possible aetiologies outlinedby Lennon (1910) have all had their proponents inthe subsequent literature. Lennon thought that thedefect could be either degenerative or dysplastic,and that it could involve either the brain-stem, thefacial nerve in the temporal bone, or the facialmusculature. Since that time, as pointed out byRichter (1960), discussion of the syndrome hascentred around the question as to whether the dis-order is primarily degenerative or dysplastic, andas to the location of the primary defect. The postu-lated primary defects in the Moebius syndrome,together with their proponents, are summarized inTable I. Most of the evidence favours the dysplasticrather than the degenerative theory of pathogenesis.
TABLE IPOSTULATED DEFECTS IN THE MOEBIUS SYNDROME
Type of Defect
I DegeneratitreA Primarily in the brain-
stem
B Primarily involving thecranial nerves outsidethe brain-stem
C Primarily involving theaffected muscles
II Dysplastic or AplasticA Primarily in the brain-
stem
B Primarily involving thecranial nerves outsidethe brain-stem
C Primarily involving theaffected muscles
Author and Year
Mobius (1892)Rainy and Fowler (1903)Fenyes (1937)Marfan and Armand-Delille (1901)
Heubner (1900)Spatz and Ullrich (1931)Richter (1960)Van Allen and Blodi (1960)
Neurath (1907)Lennon (1910)Richards (1953)Evans (1955)Wallis (1960)
The static clinical course of the disorder is initself indirect evidence against a degenerative process,as a degeneration would be expected to continueinto post-natal life. No convincing evidence favour-ing a degenerative process has been produced.Moebius (1892), who first postulated that the dis-order was degenerative, had no pathologicalmaterial. None of the authors supporting this viewhave had unequivocal histological evidence. Marfanand Armand-Delille (1901) found degenerativechanges in the brain-stem in their case of congenitalunilateral facial palsy, but these were probablysecondary either to entrapment of the facial nerve
369
Protected by copyright.
on March 3, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.28.4.362 on 1 August 1965. D
ownloaded from

Samuel E. Pitner, James E. Edwards, and William F. McCormick
in a malformed temporpressure on the develo;mechanism in all probabof congenital unilateral
Neurath (1907). We wou
1960) that the findings reRiggs (1958) are possibhaemorrhage into the b
representative of the Mc
of Rainy and Fowler (were found in the facial
nerves, and the nerves
and temporal bone; the
could be found was desc
out by both Henderson
the absence of any im
diplegia plus the historywith obvious trauma vei
degenerative changes irto trauma to the facial n
have not been reportedined an unequivocal cas
(Table II). Human ai
experimental embryololsuggest by analogy that
marily degenerative. T
strongly suggests that tdrome is dysplastic ranature.
It is more difficult t(
primary defect. Two opformation have evolved
holds that the Moebius
dysplasia involving mu
TA.REPORTED NECROPSIES IN C.
RELATED ISOLATED CC
Author and Yei
INNERVATED B
Par
Classical cases
Heubner (1900)
Spatz and Ullrich (1931)Wallis (1960)
Current case (1965)
II Disputed cases
Rainy and Fowler (1903)
Fenyes (1937)
Riggs (1958)
III Congenital unilateral facial pMarfan and Armand-
Delille (1901)
Neurath (1907)Richter (1960)
IV Congenital bilateral abducensPhillips, Dirion, and
Graves (1932)
-al bone, or to intra-uterine branchial arches (and frequently musculature de-ping facial nerve. The same rived from somites) and that any changes found iniility was involved in the case the brain-stem are secondary. Lennon (1910),l facial palsy examined by Richards (1953), Evans (1955), and Wallis (1960>ild agree with Richter (1958; seem to be proponents of this view (Table I). Theported by Fenyes (1937) and other theory is that the syndrome is the result of anly the result of intrapartum ectodermal dysplasia involving primarily the centralrain-stem, and are not truly nervous system, and that any associated musculo-)ebius syndrome. In the case skeletal anomalies are either secondary or fortuitous.11903) degenerative changes Heubner (1900), Spatz and Ullrich (1931), Richternerve nuclei, the genu of the (1958; 1960), and Van Allen and Blodi (1960),in the subarachnoid space among others, appear to accept this view (Table I).small amount of muscle that As there is no evidence to suggest that there is dys-sribed as normal. As pointed plasia of the facial nerve in its course beyond the(1939) and Richter (1960), brain-stem, or in its termination at the motor endpairment other than facial plates, most authors have supported one or the otherof an instrumental delivery of these divergent views.
ry strongly suggests that the A theory of the pathogenesis of the Moebiusi this case were secondary syndrome that invokes both ectodermal and meso-ierves. Degenerative changes dermal involvement has been put forward by Ullrich -A
by any authors who exam- (1949). He described an entity which he called 'the-e of the complete syndrome asymmetric form of status Bonnevie-Ullrich', manynd animal teratology and cases of which fulfil our criteria for the diagnosis ofgy present no findings to the Moebius syndrome in that they show multiplethe condition could be pri- pareses of muscles innervated by cranial nerveshe available evidence thus together with limb deformities. He based his theorythe basic defect in the syn- on the experiments of Bonnevie (1934), who studiedither than degenerative in the evolution of genetically determined limb and eye
deformities in an inbred strain of experimental mice,D determine the site of the and concluded that these deformities were caused byinions as to the site of mal- overproduction of spinal fluid resulting in the forma-in the literature. One theory tion of subcutaneous cysts over the myelencephalon;syndrome is a mesodermal these cysts subsequently migrated to the eye andsculature derived from the limb anlage and produced various deformities by
pressure. While the limb deformities were similar toBLE II those described in the Moebius syndrome, the eye.,anomalies at maturity consisted of absent or atrophicASES OF THE MOEBIUS SYNDROME eyelids, corneal opacity, cataracts, or microphthal-)NGENITAL PALSIES OF MUSCLES mia; the facial or extraocular musculature was notIY CRANIAL NERVES specifically involved. Not only was the conditionTissue Examined dissimilar to the Moebius syndrome, but manyCentral Peripheral Involved embryologists thought the mode of formation of theNervous Nerve VII Muscles blebs and their subsequent migration to be in-System
sufficiently proven (Gruneberg, 1952). However,Bonnevie's work, with the addition of the suggestion
YYes YesToongueonly that pressure on the floor of the fourth ventricleYes Unknown Unknown from the overproduction of spinal fluid could com-Yes Yes Yes press the developing facial and abducens nucleiYes Yes Yes and thus cause facial diplegia and paresis of lateralYes No No gaze, was used by Ullrich (1949) to explain the occur-Yes Absent Unknown gaeby (Paralysis rence of cranial nerve palsies and limb deformities. XYes Yes No Although it has been suggested that some portions ofYes No No this hypothesis could be applicable to the MoebiusYes Absent No syndrome (Evans, 1955), we consider it to be un-s paralysis proven in mice much less in man, and would concurYes - No with Van Allen and Blodi (1960) and Adams,
370
Protected by copyright.
on March 3, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.28.4.362 on 1 August 1965. D
ownloaded from

Observations on the pathology of the Moebius syndrome
Denny-Brown, and Pearson (1962) that it lackscredibility.However, the possibility that the syndrome is the
result of involvement of both mesoderm and ecto-derm by an unknown factor or factors operatingearly in embryogenesis cannot be ruled out. Finally,it must be acknowledged that the complex relation-ship of the developing neurone to its peripheral fieldis incompletely understood, even in the normalorganism (Hamburger and Levi-Montalcini, 1950),and that any conclusion as to pathogenesis that isbased on morphological changes in the matureorganism, in view of the present knowledge ofneuroembryology, must remain tentative. With theselimitations in mind, it seems worthwhile to reviewthe evidence on which the mesodermal (peripheral)and ectodermal (central) theories of pathogenesisare based.
THE CASE FOR THE MESODERMAL (PERIPHERAL)THEORY The case for a primary mesodermal defectwas first stated by Lennon (1910). The frequentassociation of musculo-skeletal defects, such asabsent muscles, club feet, syndactly, and otherpresumably mesodermal abnormalities, is the main-stay of this argument (Evans, 1955). Congenitalfacial diplegia not associated with apparent extra-ocular palsies does occur in dystrophia myotonica(Parker, 1963), thus demonstrating that at least thisportion of the syndrome can have a myopathic basisin certain other disorders. Other clinical argumentsthat have been advanced for a primary mesodermaldefect such as absence of sensory change, the distri-bution of the facial weakness, and the absence offacial sagging (Richards, 1953) do not appear to bevalid, as pointed out by Sprofkin and Hillman (1956).Laboratory evidence supporting this view is limitedto altered creatine and creatinine metabolismsuggestive of a muscular defect, as reported byWallis (1960). However, some authors, notablyYasuna and Schlezinger (1955), reported normalcreatine and creatinine levels. We are unable to findany reports of electromyographic examinations thatconvincingly point to a myopathic origin. Patho-logical studies that would tend to support this pointof view are those of Wallis (1960) in which noabnormality was found in the brain, and the currentcase, in which the abnormality in the brain was anapparently unrelated hemi-dysplasia of the cerebel-lum, with the cranial nerve nuclei intact. It is notknown whether muscles were examined in the formercase; in the present case the appearance of thosemuscles that could be identified was somewhat moresuggestive of a myogenic origin than a neurogenicorigin. Most of the cases in which muscle examina-tions have been done were limited to biopsy speci-
mens, which have been quite inconclusive. Richards(1953) obtained biopsies in three cases, but thereported 'absence ofmuscles' in the biopsy specimensdoes not really support either view. Fragments ofextraocular muscle were examined microscopicallyby Yasuna and Schlezinger (1955) and by Reed andGrant (1957). In the former case a resected lateralrectus muscle was reported as showing equivocalneurogenic atrophy. In the latter case, a resectedlateral rectus was reported as consisting only ofdense fibrous tissue resembling tendon or fascia,without any muscle fibres present. In contrast,VanAllen and Blodi (1960) reported muscle fragmentsfrom the levator palpebrae and the lateral rectus asbeing histologically normal. A biopsy of an involvedmuscle (site not specified) suggested to Graham(1964) that a primary developmental defect ofmuscle was present in his case. Thus, some of theconfficting clinical and pathological evidence doeslend support to the theory of a mesodermal originof the defect.Evidence from human teratology is also conflict-
ing. In the majority of cases of congenital absenceof muscles there has been no associated dysplasia ofneurones in the spinal cord (Bing, 1902). There arereports of cases with absent muscles and intact spinalcords, and reports of cases with intact muscles andabsent spinal cords; as Zelena' (1962) states, theevidence from human teratology regarding the inter-relationship of the developing motor neurone and itsmuscle is inconclusive.Some support for the mesodermal theory of
pathogenesis derives from experimental neuro-embryology. It has been shown in amphibian andchick embryos that excision of a limb bud before itreceives its innervation results in a lessened numberof motor cells in the appropriate cord segment atmaturity (Hamburger and Levi-Montalcini, 1950).This same phenomenon has been demonstrated inthe brain-stem of the chick embryo by Dunnebacke(1953). She excised the primordium of the superioroblique muscle before its innervation, and found thatthe number of motor neurones in the trochlearmucleus at termwas markedly reduced, and that manyof those that were present were unusually small.This experimental work would tend to support thetheory of a primary mesodermal defect, in that itwould offer an explanation for those cases of theMoebius syndrome in which a decreased number ofcells has been found in the appropriate motor nucleiof the brain-stem, thus showing that these changescould be secondary to a muscle defect.
THE CASE FOR THE ECTODERMAL (CENTRAL) THEORYThe evidence for the theory that holds the syndrometo be due to a primary developmental defect of the
371
Protected by copyright.
on March 3, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.28.4.362 on 1 August 1965. D
ownloaded from

Samuel E. Pitner, James E. Edwards, and William F. McCormick
central nervous system (usually held to be an aplasiaof the motor nuclei) has been described by someauthors (Van Allen and Blodi, 1960) as 'virtuallyunassailable'. With the single exception of thenecropsy in the case of Wallis (1960), which theyprobably did not have access to, they are quitecorrect in stating that no histological examinationin an unequivocal case of the Moebius syndromehas revealed a normal brain-stem. There are alsosome clinical observations that have been cited tosupport this view, such as the not infrequent asso-ciation of mental retardation and abnormal electro-encephalograms and pneumoencephalograms (VanAllen and Blodi, 1960). While we are aware of noconvincing reports of electromyography demon-strating denervation of the facial or extraocularmuscles, the same authors used this technique todemonstrate a failure of reciprocal innervation of theextraocular muscles in their case, and postulatedthat a defect of supranuclear innervation was present.Such a defect cannot be excluded in the current case,as the extraocular muscles and their nuclei werenormal on histological examination, and the (normal)hypomyelination of the supranuclear pathways inan infant of 7 weeks would make it impossible tostate categorically that these were normal. Althoughsome of the conflicting clinical evidence points to acentral nervous system defect, the mainstays of thistheory are the reported necropsies in undisputedcases of the Moebius syndrome.Heubner (1900) reported the pathological findings
in a child who undoubtedly had the Moebiussyndrome and expired at 20 months of age. Histo-logical examination showed asymmetry of themedulla with hypoplasia of the olive and pyramid onthe left side, absence of neurones in the left hypo-glossal nucleus, and marked reduction in thenumber of neurones present in the left spinal acces-sory nucleus and facial nucleRs and both abducensnuclei. The involved cranial nerves were said to besomewhat small. Although no note is made of othermuscles, the tongue was examined and was thoughtto show neurogenic atrophy on the left side. Heinterpreted these findings as representing primarydysplasia of the brain-stem. Spatz and Ullrich (1931)reported a similar case in which they described eitheran absence of neurones or a reduction in theirnumber bilaterally in the oculomotor, trochlear,abducens, and facial nuclei, together with dysplasiaof the intraparenchymal portions of the associatednerves. Only in the case of Wallis (1960) was thecentral nervous system reported to be normal.Although no conclusions can be drawn from thedisputed cases (Table II), the partial forms are ofsome interest. The case of congenital unilateral facialpalsy reported by Richter (1958; 1960) showed a
reduction in the number of neurones in the affectednucleus, together with the presence of some abnorm-ally small neurones, and the absence of a recog-nizable facial nerve. In the case of congenital bi-lateral abducens paralysis reported by Phillips et al.(1932), no neurones of these nuclei could be identi-fied, and an aberrant fibre tract was present. Un-fortunately, examinations of involved muscles in allof these cases have been infrequent and inconclusive,and some proponents of the mesodermal theory(Evans, 1955) point out that the changes in themotor nuclei could be secondary to a disorder inthe peripheral field of the involved neurones earlyin embryogenesis.
Experimental neuroembryology also gives somesupport to the theory of a primary central dysplasia.In both amphibian and chick embryos, limb budsand their associated muscles develop normally to apoint in spite of failure of innervation to reach thelimb; this has been demonstrated in the chickembryo by grafting the developing limb bud to ananeural area such as the coelomic cavity before itreceives its normal innervation, and in the frogembryo by removal of the lower spinal cord (Ham-burger, 1939). While the formation, initial differen-tiation, and growth of muscle occurs without in-nervation, it is necessary for the final differentiationand the maintenance of the embryonic muscle;without innervation differentiation arrests at themyotubal stage and fascicle formation is thought notto occur (Zelena, 1962). Not only does an arrestof final differentiation occur, but after a period oftime the developing muscle disintegrates and under-goes phagocytosis and fatty replacement (Eastlickand Wortham, 1947). Thus absence of facial musclealone cannot be used as evidence in support of themesodermal theory, as has been suggested beRichards (1953).
CONCLUSIONS
We regard neither theory as proven on the basis ofthe available evidence, and must admit that thepresent case fails to clear completely the murkywaters of aetiology. However, we feel that there isindirect evidence that peripheral factors were themajor ones in this case, in spite of the pathologicalfindings in the brain. The changes in the brain-stemare believed to be secondary to the hemihypoplasiaof the cerebellum, and are characteristic of thosefound in such conditions (Dow and Moruzzi,1958). Although a case has been recorded in whichdysplasia of the auditory, vestibular, and spinalfifth cranial nerve nuclei was associated with such acerebellar defect (Rubenstein and Freeman, 1940),we cannot find an instance in which the motor
372
Protected by copyright.
on March 3, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.28.4.362 on 1 August 1965. D
ownloaded from

Observations on the pathology of the Moebius syndrome
cranial nerves or their muscles have been involved.We feel that the central nervous system pathology inour case is fortuitous and unrelated to the musculardefect. The facial nuclei appeared normal in everyway. The facial nerves were normal in the brain-stem,subarachnoid space, and within the temporal bone.Moreover, apparently normal neural elements wereseen passing through the parotid gland and were inclose opposition to both the preserved facial muscleand to the areas of presumed adipose replacement.Finally, there was suggestive evidence of the forma-tion of muscle fascicles even in the latter areas,which would imply that innervation was present,as final differentiation of muscle is not believed tooccur in its absence (Zelena, 1962).On the other hand, it can be objected that the
muscle findings are not characteristic of a myo-pathy. Certainly extreme variation in fibre size,sarcolemmal proliferation, and central migration of
-.nuclei is not prominent. Degenerating or regenerat-ing muscle fibres and those undergoing phagocytosisare also absent. All of these changes have beendescribed in the probably related condition ofarthrogryposis multiplex congenita when it is due tocongenital muscular dystrophy (Banker, Victor, andAdams, 1957). However, it is not established that
a these changes, usually associated with a progressivemyopathy, would of necessity be present if the pri-mary defect were a failure of proper formation ofmuscle. Although we think that our findings arecompatible with a primary failure of muscle forma-tion, histological standards by which to diagnosesuch a failure are obscure. As it has been shownexperimentally in the chick embryo that musclebreakdown and its adipose replacement is presentat term if innervation fails to reach the developingmuscle (Eastlick and Wortham, 1947), it seems likelythat the end result of such a failure of innervationwould be histologically similar, particularly if finaldifferentiation of muscle had failed to occur. Thus,we doubt if histological examination of only the'end stage muscle' found in the face of the matureneonate or older child could in itself conclusivelyprove either theory of pathogenesis.
However, the presence of morphologically normalelements of the facial nerve, from the facial nucleusat least to the parotid gland and probably into thefacial muscles, suggests to us that a primary failureof formation of the facial musculature produced theMoebius syndrome in this case. Although we believethat the Moebius syndrome in our case probablywas due to a primary dysplasia of the facial muscles,we think it likely that in other instances (Heubner,1900; Spatz and Ullrich, 1931) it was due to a pri-mary neuronal dysplasia. Thus we regard theMoebius syndrome as 'bulbar arthrogryposis', if
such a tortured phrase is permissible, in that it canhave more than one aetiology and can involve thebrain-stem and/or musculature derived from thebranchial arches in much the same way as arthro-gryposis can involve the spinal cord and/or muscula-ture derived from the somites. This conclusion mustbe regarded as tentative. While some might agreewith Richter (1960) that pathological changes of adevelopmental nature must be interpreted as primaryto the structure in which they are found, we wouldagree with Hamburger and Levi-Montalcini (1950)that the incompletely understood and extremelycomplex relationships between nervous structuresand their peripheral fields in the developing embryoare reciprocal, and that much caution must be exer-cised in assigning primacy to one or the other site.
SUMMARY
A patient with the Moebius syndrome is describedand the necropsy findings are presented. We believethis to be the only reported case in which the brain,facial nerves, and involved muscles have all beenexamined. The literature of the subject is reviewed,with particular attention to the few reported necrop-sies and the pertinent findings of experimentalembryology. It has been postulated that the syndromeis due to a dysplasia of either the involved musclesor the motor nuclei of the brain-stem. We think thatthe present case is due to a dysplasia of the facialmuscles, but, by analogy with arthrogryposis, it isconsidered probable that both myopathic and neuro-genic forms of the syndrome exist.
This study was supported in part by U.S.P.H.S. grantnumber NB-05274-04 of the National Institute of Neuro-logical Diseases and Blindness (Dr. Pitner) and by agrant from the Hoffmann-LaRoche Company (Dr.Edwards). The authors are indebted to Dr. WarrenJohnson, Pathologist to the Clinic for Muscle Diseases,St. Jude's Children's Hospital, Memphis, for reviewingthe temporal bone and facial muscle slides. Dr. HansZellweger, State University of Iowa, kindly translatedthe German articles. Dr. Robert A. Utterback, Professorof Neurology, University of Tennessee, Dr. MauriceVan Allen, Associate Professor of Neurology, StateUniversity of Iowa, and Dr. Viktor Hamburger, Professorof Zoology, Washington University, reviewed the manu-script and made helpful suggestions, thus being largelyresponsible for any of the merit, but none of the defects,of this study.
REFERENCES
Adams, R. D., Denny-Brown, D., and Pearson, C. M. (1962). Diseasesof Muscle, 2nd ed., pp. 301-304. Hoeber, New York.
Banker, B. Q., Victor, M., and Adams, R. D. (1957). Arthrogryposismultiplex due to congenital muscular dystrophy. Brain, 80319-334.
373
Protected by copyright.
on March 3, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.28.4.362 on 1 August 1965. D
ownloaded from

Samuel E. Pitner, James E. Edwards, and William F. McCormick
Bing, R. (1902). t1eber angeborne Muskeldefecte. Virchows Arch.path. Anat., 170, 175-228.
Bonnevie, K. (1934). Embryological analysis of gene manifestation inLittle and Bagg's abnormal mouse tribe. J. exp. Zool., 67,443-520.
Dow, R. S., and Moruzzi, G. (1958). The Physiology and Pathologyof the Cerebellum, pp. 416-444. University of MinnesotaPress, Minneapolis.
Dunnebacke, T. H. (1953). The effects of the extirpation of thesuperior oblique muscle on the trochlear nucleus in the chickembryo. J. comp. Neurol., 98, 155-175.
Eastlick, H. L., and Wortham, R. A. (1947). Studies on transplantedembryonic limbs of the chick. III. The replacement of muscleby 'adipose tissue'. J. Morph, 80, 369-389.
Evans, P. R. (1955). Nuclear agenesis. Mobius' syndrome: the con-
genital facial diplegia syndrome. Arch. Dis. Childh., 30,237-243.
F6nyes, 1. (1937). Zur Frage der Entstehung von angeborenenBeweglichkeitsstorungen im Gehirnnervenbereich. Ein klinisch-anatomischer Beitrag. Arch. Psychiat. Nervenkr., 106, 296-311.
Graefe, A. (1880). Handbuch der gesammten Augenheilkunde, ed.A. Graefe and T. Saemisch, vol. 6, p. 60. Engelmann, Leipzig.
Graham, P. J. (1964). Congenital flaccid bulbar palsy. Brit. med. J.,2, 26-28.
Gruneberg, H. (1952). The Genetics ofthe Mouse, 2nd ed., pp. 147-162.Nijhoff, The Hague.
Hamburger, V. (1939). The development and innervation of trans-planted limb primordia of chick embryos. J. exp. Zool., 80,347-389.and Levi-Montalcini, R. (1950). Some aspects of Neuro-embryology. In Genetic Neurology, edited by P. Weiss, pp.128-160. University of Chicago Press, Chicago.
Henderson, J. L. (1939). The congenital facial diplegia syndrome:clinical features, pathology, and aetiology. A review of sixty-one cases. Brain, 62, 381-403.
Heubner, 0. (1900). tJeber angeborenen Kernmangel (infantilerKernschwund, Moebius). Charite-Ann., 25, 211-243.
Lennon, M. B. (1910). Congenital defects of the muscles of the faceand eyes. Infantiler Kernschwund of Moebius. Report ofthree cases. Calif. State J. Med., 8, 115-117.
Marfan, A.-B., and Armand-Delille (1901). Paralysie faciale congeni-tale du cot6 droit. Agenesie de la portion p6ripherique du nerffacial avec agen6sie des diverses parties constituantes del'oreille du meme c6te. Atrophie probablement secondairede la racine et du noyau du facial. Bull. Soc. Med. H6p.Paris, 3rd ser., 18, 1007-1014.
Mobius, P. J. (1888). Ueber angeborenen doppelseitige Abducens-Facialis-Lahmung. Munch. med. Wschr., 35, 91-94.
(1892). Ueber infantilen Kernschwund. Ibid., 39, 17-21, 41-43,55-58.
Neurath, R. (1907). Zur Frage der angeborenen Funktionsdefecte imGebiete der motorischen Hirnnerven. Ibid., 54, 1224-1228.
Parker, N. (1963). Dystrophia myotonica presenting as congenitalfacial diplegia. Med. J. Aust., 2, 939-944.
Phillips, W. H., Dirion, J. K., and Graves, G. 0. (1932). Congenitalbilateral palsy of the abducens. Arch. Ophthal. (Chic.), 8,355-364.
Plott, D. (1964). Congenital laryngeal-abductor paralysis due tonucleus ambiguus dysgenesis in three brothers. New Engl.J. Med., 271, 593-597.
Rainy, H., and Fowler, J. S. (1903). Congenital facial diplegia due tonuclear lesion. Rev. Neurol. Psychiat., 1, 149-155.
Reed, H., and Grant, W. (1957). Mobius's syndrome. Brit. J. Ophthal.,41, 731-740.
Richards, R. N. (1953). The Mobius syndrome. J. Bone Jt. Surg.(Amer.), 35, 437-444.
Richter, R. B. (1958). Congenital hypoplasia of the facial nucleus.J. Neuropath. exp. Neurol., 17, 520.
(1960). Unilateral congenital hypoplasia of the facial nucleus.Ibid., 19, 33-41.
Riggs, E. H. (1958). Congenital hypoplasia of the facial nucleus.(Discussion). Ibid., 17, 520.
Rubinstein, H. S., and Freeman, W. (1940). Cerebellar agenesis. J.nerv. ment. Dis., 92, 489-502.
Spatz, H., and Ullrich, 0. (1931). Klinischer und anatomischerBeitrag zu den angeborenen Beweglichkeitsdefeckten imHirnnervenbereich. Z. Kinderheilk, 51, 579-597.
Sprofkin, B. E., and Hillman, J. W. (1956), Moebius's syndrome-congenital oculofacial paralysis. Neurology (Minneap.), 6,50-54.
Ullrich, 0. (1949). Turner's syndrome and Status Bonnevie-Ullrich.Amer. J. hum. Genet., 1, 179-202.
Van Allen, M. W., and Blodi, F. C. (1960). Neurologic aspects of theMobius syndrome. Neurology (Minneap.), 10, 249-259.
Wallis, P. G. (1960). Creatinuria in Mobius' syndrome. Arch. Dis.Childh., 35, 393-395.
Yasuna, J. M., and Schlezinger, N. S. (1955). Congenital bilateralabducens: facial paralysis (Mobius syndrome). Arch. Ophthal.(Chic.), 54, 137-139.
Zelena, J. (1962). The effect of denervation on muscle development.In The Denervated Muscle, edited by E. Gutmann, pp. 103-126.Czechoslovak Academy of Sciences, Prague.
374
Protected by copyright.
on March 3, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.28.4.362 on 1 August 1965. D
ownloaded from