Embed Size (px)
Citation preview

[page 82] [Rare Tumors 2010; 2:e30]
Observation and extirpation of a giant-size type-B2 thymoma IIb with its histological, macroscopic, and computer tomogram correlate, and literature reviewMaximilian de Bucourt, Marc Swierzy,Anja Dankof, Ulf Teichgräber, Jens-Carsten RückertCharité-University Medicine Berlin,Germany
Abstract
This report describes the interdisciplinaryapproach and solving algorithm of a DIN9001:2000 certified tumor board in managing agiant-size type-B2 thymoma IIb in an elderlypatient. The process of managing the thymomawith specialists of surgery, internal medicine,radiology, and pathology until finally extirpa-tion and continuous follow-up is described.Respective computerized tomography scans,histology, macro-pathology, and operative pic-tures of the case are provided as well as an up-to-date literature review.
Introduction
We report an extirpation of a giant-size type-B2-thymoma IIb, according to the modifiedclinical Masaoka1,2 and histological WHO3,4
stages. Previously a period of controlled obser-vation by an interdisciplinary and DIN9001:2000 certified tumor conference teamwas pursued. Our case report is supported byhistological, macroscopic, and computerizedtomography (CT) pictures.
Case Report
An 82-year-old woman presented with acough enduring for weeks and a feeling ofthor acic pressure. Anamnestically the patienthad no history of severe thoracic illness. Onclinical admission, routinely collected labora-tory values – including leukocytes – were nor-mal. A chest CT scan with intravenous contrastwas performed and depicted a solid tumor ofabout 10¥5¥6 cm in the superior anteriormediastinum. The tumor was located in theimmediate vicinity of the pericardium abovethe aortic arch and superior vena cava, with nosigns of infiltrative growth. CT-acquired histol-
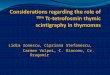
ogy via Biopince (Amgiotech, Medical DeviceTechnologies Inc., Florida, USA; 10 cm, 18ga)revealed a thymoma as the diagnosis. Thepost-diagnosis algorithm for adequate treat-ment of the patient included an interdisciplin -ary and DIN 9001:2000 certified tumor confer-ence with specialists of surgery, internal med-icine, radiology, and pathology. Because thepatient’s symptoms were ameliorated, andespecially given her age, it was decided first topursue a wait-and-see strategy. Half a yearlater the patient presented again. A new CTscan revealed an increase in the size of thethymoma to 10¥6¥10 cm. The continuousgrowth increasingly affected cardiovascularstructures in the mediastinum (Figure 1). Thetrachea was not deviated and the underlyingdiaphragm did not appear paralytic. It wasdecided to extirpate the tumor surgically, tak-ing into account the increased risk of surgicalinterventions, especially in elderly patients.The surgical procedure lasted for about 150
min. It included a complete sternotomy andmobilization of the tumor per continuitatemfrom caudal to cranial, and finally extirpation(Figure 2). Grossly, the tumor was adherent tothe mediastinal pleura and pericardium withoutinvading these structures. It was fed partly byone branch of the right internal thoracic artery– visible in the CT scan – that had to be occlud-ed surgically. One Redon drain (10 Ch.) wasplaced dorsal to the sternum and one pleuraldrain (24 Ch.) was placed on each side as well.Macroscopically, the biggest part of the deli-
cately encapsulated, knotty, and mainly solidtumor measured 75¥70¥55 mm. For histo- andmacro-pathological post-processing, the thym -
oma was cut into slices (Figure 3). In general,the cutting area depicted was of a homo -genous, brown appearance, with some focalcystic and some hemorrhagic lesions of a max-imum of 15 mm. Adjacent extirpated soft tissuemeasured 120¥75¥20 mm. Microscopically, thetumor presented a lobular architecture.Multiple polygonal cells with large nuclei andprominent nucleoli could be identified (Figure4A). Immunohistochemically, a Pan-CK andCK19 expression could be identified (Figure4B) as well as a concomitant infiltrate of part-ly CD3-positive lymphocytes (Figure 4C). The
Rare Tumors 2010; volume 2:e30
Correspondence: Maximilian de Bucourt,Charité-University Medicine Berlin, Departmentof Radiology, Charité Platz 1, 10117 Berlin,Germany. E-mail: [email protected]
Key words: thymoma.
Contributions: all authors have read andapproved the manuscript.
Conflict of interest: the authors report no con-flicts of interest.
Received for publication: 19 March 2010.Revision received: 20 April 2010.Accepted for publication: 23 April 2010.
This work is licensed under a Creative CommonsAttribution 3.0 License (by-nc 3.0).
©Copyright M. de Bucourt et al., 2010Licensee PAGEPress, ItalyRare Tumors 2010; 2:e30doi:10.4081/rt.2010.e30
Figure 1. Intravenous chest CT scan.(A) Axial view. Note the vicinity of thetumor (*) to the internal thoracicartery (arrow). (B) Sagittal view. Notethe delicate location of the tumor (*)above the right atrium (#). (C)Coronal view. Note the vicinity of thetumor (*) to the mediastinal cardiovas-cular structures such as the ascendingaorta and aortic arch (+), right atrium(#), and left brachiocephalic vein (~).

[Rare Tumors 2010; 2:e30] [page 83]
lymphocytological proliferation rate MIB1 aver-aged 80% (Figure 4D).In the final pathological classification, the
tumor was staged type-B2 thymoma IIb accord-ing to the modified clinical Masaoka1,2 and his-tological WHO3,4 stages. As expected, CRP rosepost-intervention to a maximum of 11.54mg/dL (<0.5) on day 4 and decreased there-after, to 6.67 mg/dL on day 5. The postoperativecourse was ceteris paribus uneventful. Thepatient was discharged on postoperative day 6.Follow-up studies up to this date have notrevealed any recurrence of the tumor and willbe continued.
Discussion
Thymomas have a prevalence of 0.1-0.4/100,000.5 They account for about 0.2-1.5%of all malignant tumors and for about 50% of alltumors in the upper ventral mediastinum; dis-
tribution between sexes is about equal, andthe majority of patients are aged between 40and 60 years.6 Thymomas are epithelial tumorsgenerally considered to have an indolent andslow growth pattern, but should be regarded asmalignant nonetheless because of the poten-tial for local invasion and, less often, systemicmetastases. One third of thymomas is detected casually
in body imaging, one third of patients presentswith local symptoms, and one third is diag-nosed within myasthenia gravis evaluation.6
The latter seems especially noteworthy asother paraneoplastic autoimmune diseasesoccur only occasionally; for example, withsmall cell lung cancers or gynecologicaltumors, whereas myasthenia gravis is associ-ated with thymomas in at least 30% ofpatients.7 Ectopic cervical thymomas are a rareand diagnostically challenging entity that fre-quently is misdiagnosed on fine needle aspir -ation cytology and frozen sections.8
The most commonly used classification ofthymomas was initially introduced by Masaokaet al.1 in 1981, and describes four stages ofthym oma with special reference to the clinicalstage. The most recent modifications werepublished in 20033 and included more histolog-ical data. Generally, recurrences after completesurgical resection are rare but have beendescribed in the literature.9-11 Spontaneoustumor regression of invasive thymoma12 as well
as of thymoma-associated immunodeficiencyhave been described as well.13
The effect of radiation therapy is discussedcontroversially. It is generally agreed thatpatients with a Masaoka III stage and higherbenefit from radiation therapy. Chen et al.state that adjuvant radiotherapy after completetumor resection for patients with stage IIthym oma neither reduced recurrence ratessignificantly, nor improved survival rates.14
Several prognostic factors for thymic tumors,including the Masaoka stage, WHO histology,complete resection, great vessel invasion, andsize of thymoma have been identified.15 In arecent publication, Wright et al. demonstratedthat thymoma size is an independent risk fac-tor and tumors measuring >8 cm were foundto be recurrent in 29%,16 further justifying con-tinuous follow-up studies of the patient pre-sented. Tumor size of >11 cm as well as thehistological type-B3 thymoma14 have also beendescribed as significant independent prognos-tic variables.17 Concerning prognostic indica-tors after surgery for thymoma, Okereke et al.recently stated that long-term disease-specificsurvival can be expected not only after surgeryfor early-stage thymoma but also after surgeryfor advanced disease, including patients withpleural metastases but limited, however, bypatients who undergo surgery for stage IV-Adisease, who do have reduced disease-free sur-vival.18 If the tumor is indeed malignant, the
Case Report
Figure 2. Intraoperative photograph of therecently extirpated thymoma.
Figure 3. Cross-section preparation photo-graph of the macro-pathological, post-processed, delicately capsulated, knotty,and mainly solid thymoma.
Figure 4. (A) Neoplastic epithelial cells of the thymoma in a lymphocytic background(Giemsa stain; 200X magnification). (B) Immunohistochemical expression of cytoker-atin 19 highlights the neoplastic epithelial component (CK19; 100X magnification). (C)Perivascular accumulation of mature CD3-positive T-lymphocytes (CD3; 100x magnifi-cation). (D) High proliferative activity, sparing areas of accumulated mature T-lympho-cytes (MIB1; 50X magnification).

[page 84] [Rare Tumors 2010; 2:e30]
risk of lymph node metastasis generally is esti-mated to be 1.8% and does not seem to impacton overall survival rate.19
Twenty-year survival rates of type II thym -omas, according to the Masaoka staging sys-tem, are reported to be 91%.20 Thymomas of thepresented giant size are extremely rare. It isnoteworthy that the delicate size and locationof the tumor and the age of our patient neces-sitated deliberate surgical intervention.
References
1. Masaoka A, Mondem Y, Nakahara K, et al.Follow-up study of thymomas with specialreference to their clinical stage. Cancer1981;48:2485-92.
2. Weydert JA, De Young BR, Leslie KO.Recommendations for the reporting of sur-gically resected thymic epithelial tumors.Hum Pathol 2009;40:918-23.
3. Rosai J. Histological typing of tumors ofthe thymus. World Health OrganizationInternational Histological Classification ofTumors. 2nd ed. New York, Berlin:Springer, 1999.
4. Nakagawa K, Asamura H, Matsuno Y, et al.Thymoma: a clinicopathologic study basedon the new World Health Organizationclassification. J Thor Cardiovasc Surg2003;126:1134-40.
5. Kahraman A, Miller M, Maldonado-LopezE, et al. A 55-year-old woman with thym -oma and hypogammaglobulinemia (Goodsyndrome), ulcerative colitis, and cyto -megalovirus infection. Med Klin (Munich)2009;104:150-4.
6. Giaccone G. Treatment of malignant thym -oma. Curr Opin Oncol 2005;17:140-6.
7. Marx A, Willcox N, Leite MI, et al.Thymoma and paraneoplastic myastheniagravis. Autoimmunity 2010, Apr 12. [Epubahead of print]
8. Yan B, Lim D, Petersson F. Ectopic CervicalThymoma: A Report of Two Cases of a RareEntity Frequently Misdiagnosed on FineNeedle Aspiration Cytology and FrozenSection. Head Neck Pathol 2010, Mar 24.[Epub ahead of print]
9. Fechner RE. Recurrence of noninvasivethymomas. Cancer 1969;23:1423-7.
10. Kirschner PA. Reoperation for thymoma:report of 23 cases. Ann Thorac Surg 1990;49:550-5.
11. Regnard JF, Magdeleinat P, Dromer C, et al.Prognostic factors and long-term resultsafter thymoma resection: a series of 307patients. J Thorac Cardiovasc Surg 1996;112:376-84.
12. Yutaka Y, Omasa M, Shikuma K, et al.Spontaneous regression of an invasivethymoma. Gen Thorac Cardiovasc Surg2010;58:212-3.
13. Vitiello L, Masci AM, Montella L, et al.Thymoma-associated immunodeficiency:
a syndrome characterized by severe alter-ations in NK, T- and B-cells and progres-sive increase in naïve CD8+ T-cells. Int JImmunopathol Pharmacol 2010;23:307-16.
14. Chen YD, Feng QF, Lu HZ, et al. Role ofadjuvant radiotherapy for stage II thym -oma after complete tumor resection. Int JRadiat Oncol Biol Phys 2010, Apr 6. [Epubahead of print]
15. Wright CD, Kessler KA. Surgical treatmentof thymic tumors. Semin Thorac Cardio -vasc Surg 2005;17:20-6.
16. Wright CD, Wain J, Wong DR, et al.Predictors of recurrence in thymic tumors:importance of invasion, WHO histology,and size. J Thorac Cardiovasc Surg 2005;130:1413-21.
17. Blumberg D, Port JL, Weksler B, et al.Thymoma: a multivariate analysis of fac-tors predicting survival. Ann Thorac Surg1995;60:908-14.
18. Okereke IC, Kesler KA, Morad MH, et al.Prognostic indicators after surgery forthym oma. Ann Thorac Surg 2010;89:1071-9.
19. Kondo K, Monden Y. Lymphogenous andhematogenous metastasis of thymicepithelial tumors. Ann Thorac Surg 2003;76:1859-5.
20. Okumura M, Ohta M, Tateyama H, et al.The World Health Organization histologicclassification system reflects the oncologicbehaviour of thymoma: a clinical study of273 patients. Cancer 2002;94:624-32.
Case Report