Embed Size (px)
Citation preview

FEBRUARY 2001 • PODIATRY MANAGEMENTwww.podiatrymgt.com 97
the sole of the foot. It has nowbeen well established that pres-sure reduction (off- loading) iscritical for the healing of plantarulcers in the neuropathic diabeticfoot. Off-loading is also crucialfor the patient with acute Charcotfoot for healing and maintenance.
The reason that off-loading is
so important is that 85 percent oflower extremity amputations inpeople with diabetes mellitus arepreceded by a foot ulcer.(2) There-fore, by healing the diabetic footulcer, lower extremity amputa-tions can be prevented. A largestudy of male veterans showed
Continued on page 98
Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Continu-ing Medical Education by the Council on Podiatric Medical Education.
You may enroll: 1) on a per issue basis (at $15 per topic) or 2) per year, for the special introductory rate of $99 (you save $51).You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. In the near future, you maybe able to submit via the Internet.
If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earned credits. You willalso receive a record of any incorrectly answered questions. If you score less than 70%, you can retake the test at no additional cost. Alist of states currently honoring CPME approved credits is listed on pg. 114. Other than those entities currently accepting CPME-approvedcredit, Podiatry Management cannot guarantee that these CME credits will be acceptable by any state licensing agency, hospital, man-aged care organization or other entity. PM will, however, use its best efforts to ensure the widest acceptance of this program possible.
This instructional CME program is designed to supplement, NOT replace, existing CME seminars. Thegoal of this program is to advance the knowledge of practicing podiatrists. We will endeavor to publish high quality manuscripts bynoted authors and researchers. If you have any questions or comments about this program, you can write or call us at: PodiatryManagement, P.O. Box 490, East Islip, NY 11730, (631) 563-1604 or e-mail us at [email protected].
Following this article, an answer sheet and full set of instructions are provided (p. 114).—Editor
Over 40 years ago, Bauman(1)
concluded that heal ingtrophic ulcerat ion in
anaesthetic feet in leprosy pa-tients largely depended on theeven distribution of pressure over
By Ellen Sobel, D.P.M., Ph.D. andSteven J. Levitz, D.P.M.
Objectives1) To know the risk factors for
diabetic foot ulceration and why itis important to unload the diabet-ic foot.
2) To be familiar with the differ-ent off-loading modalities for heal-ing diabetic foot ulcers, including:footwear, insoles, foot orthoses,prefabricated walking braces, totalcontact cast, Charcot Restraint Or-thotic Walker (CROW) Orthosis,and PTB orthosis.
3) To know the indications foreach of the different off-loadingstrategies above.
4) To know the advantages anddisadvantages of each of the dif-ferent off-loading strategiesabove.
5) To have some familiarity withthe latest research in off-loadingthe diabetic foot.
Continuing
Medical Education
C L I N I C A L P O D I A T R YC L I N I C A L P O D I A T R Y
PressureReduction
and Off-Loadingthe Diabetic
FootSteps to take to reduce pressure stress.
PressureReduction
and Off-Loadingthe Diabetic
FootSteps to take to reduce pressure stress.

deformities such as hammer toes,hallux valgus, or Charcot foot aretwice as likely to develop foot ul-cers as those with neuropathyalone.(9) Diabetic neuropathic pa-tients with high plantar pressuresare more likely to develop a foot
ulcer than diabetics with periph-era l neuropathy, and normalplantar pressure.(17)
High plantar pressures occurin people with rheumatoid arthri-tis which are equal to those inpeople with diabetes mellitus, butfoot ulcers do not occur in indi-
viduals with rheumatoid arthritis,suggest ing that high plantarweight-bearing pressures may be anecessary but not sufficient con-dition for a foot ulcer to form.(20)
There are other threats toulcer healing in the diabetic footbeside high plantar pressures. Forexample, peripheral vascular dis-ease is the most important factorrelated to outcome of foot ulcerhealing.(21) A transcutaneous oxy-gen tension of greater than 30mm Hg (normal 55 mm Hg) isnecessary for a diabetic foot ulcerto heal.(22) Control of blood glu-cose is known to delay the onsetof peripheral neuropathy(23-25) andpoor glucose control has been as-sociated with recurrence of dia-betic ulcers . (26-27) F inal ly, thor-oughly debrided ulcers have beenshown to heal faster than non-de-brided ulcers.(28)
There have recently been alarge variety of off-loading modal-ities designed to reduce weightbearing pressure on the diabeticfoot. This article will discuss all ofthe off-loading devices that arecurrently used to reduce pressureand heal diabetic ulcers and ac-
that the most common causalpathway to lower extremity am-putation began with repetitivemicro-trauma, leading to an ulcerthat failed to heal.(2)
People with diabetes mellitushave been found to have highplantar foot pressures on weightbearing most commonly underthe metatarsal heads. High peakplantar pressures are a great riskfactor in the development of afoot ulcer and correlate with thesites of ulceration.(3,4) A number offactors are associated with highplantar pressure and risks for ul-ceration in people with diabetes.These include: peripheral neu-ropathy,(5-7) foot deformities suchas hammer toes and bunions,(8,9)
hyperkeratosis(10,11) limited jointmobility (Figure 1A/1B)(12-15) andhistory of foot ulceration.(16-18)
Although peripheral neuropa-thy is the single greatest risk fac-tor for foot ulceration,(19) two ormore of the risk factors abovegenerally produce a synergistic ef-fect in the production of a footulcer. For example, diabetic indi-viduals with neuropathy and foot
Pressure Reduction...Con
tinuin
g
Medica
l Edu
catio
n
Continued on page 99
98 www.podiatrymgt.comPODIATRY MANAGEMENT • FEBRUARY 2001
A large study of maleveterans showed that the
most common causalpathway to lower
extremity amputationbegan with repetitive
micro-trauma, leading to an ulcer that
failed to heal.
Figure 1B: Same patient. Neuropathiculcer under the base of the hallux,one of the most common sites of ul-ceration in the neuropathic foot. Limi-tation of passive extension of thegreat toe contributes to the risk of ul-ceration in this patient.Figure 1A: 64 year old male with neuropathic foot and hallux limitus.

commodate and off-load the dia-betic foot. However, emphasis isplaced on footwear, insoles/footorthoses and the prefabricatedwalking brace, since they are usedthe most in primary care centers.
The goal of off-loading thera-py is to keep the patient ambula-tory while reducing weight-bear-ing pressure on the foot.(29) Guz-man and associates (20) reviewedthe various pressure removingtreatment modalities and report-ed that a good pressure reductionmodality must be: effective in re-moving pressure from the ulcersite at all times, be able to be ap-pl ied to a l l types of pat ients ,cause no secondary les ions orcomplications, easy to don anddoff , encourage good pat ientcompliance, allow optimal pursuitof other treatment goals and becost effective. The above criteriashould be kept in mind as the off-loading devices are reviewed in
Pressure Reduction... eventual l imb amputa-tion.(31) Shoes reduce plantarweight bearing pressure by in-creasing the weight-bearing sur-face area (Figure 2),(32) reduce cal-lus formation and are criticallyimportant in prevention, healing,and avoiding recurrence of ulcersin the diabet ic foot . (33) Peak
detai l . Most of f - loading tech-niques require between four andtwelve weeks for the ulcer toheal.(28,29)
Foot WearAbout half of diabetic patients
with preexisting peripheral neu-ropathy have a footwear-relatedpivotal event leading to their
Continuing
Medical Education
Circle #2
FEBRUARY 2001 • PODIATRY MANAGEMENTwww.podiatrymgt.com 99
Figure 2: Four different shoe soles demonstrate variability in surface area of thesole of the shoe.
Continued on page 100

were c losed in less than twomonths using therapeutic foot-wear and custom foot orthoses.(37)
Patients with a healed diabeticulcer are frequently placed in spe-cial footwear to prevent the ulcerfrom recurring. The use of thera-peutic shoes has been shown tobe effective in preventing recur-rence in diabetic patients withprevious ulceration. In three stud-ies which measured the relapserate in patients placed in thera-peutic shoes after an ulcer healed,the recurrence rate ranged from
zote/PPT and viscoelastic insolesprovided significant reduction inmean peak pressure with all shoetypes tested including added-depth shoes, running shoes andSAS comfort shoes. (35) The inci-dence of foot ulcers was reducedfrom 72 percent to only 15 per-cent in patients with diabetic footsyndrome wearing molded shoes
with rocker solesand 10mm thickinsoles for 25months.(36) In onestudy eight out of17 open les ions
weight-bearing foot pressureswere found to be lower whenwalking in a shoe than whenwalking barefoot.(34) Adding a softcushioned insert to the shoe de-creases weight-bearing pressurestill further. In one study the ad-dition of a dual density plasta-
Pressure Reduction...Con
tinuin
g
Medica
l Edu
catio
n
100 www.podiatrymgt.comPODIATRY MANAGEMENT • FEBRUARY 2001
Continued on page 101
Figure 5A: Patient with acute Lisfrancfracture dislocation as a first sign ofcharcot neuropathic arthropathy.
Figure 5B: Fscan analysis taken about six months later. Left: Patient walking withEqualizer Below Knee Walking Brace. Center: Patient walking with molded shoe.Right: Patient walking with Apex Ambulator shoe, shows greatest pressure re-duction at Lisfrac joint area.
Figure 3: Extradepth shoe (P.W. Minor & Son, Batavia,NY) with enough room for insert. Shoe has blucher clo-sure, wedge heel, stiff counter, and high wide toe box.
Figure 4: APEX Ambulator (APEX Industries, South Hacken-sack, N.J.).

density accommodative in-serts.(43) Shoe modifications in-clude: rocker soles, metatarsalbars, wedges, flared heels, velcroclosures, and toe fillers.(43) How-ever, the Medicare Shoe Bill isgrossly underutilized because ofthe difficult access and only .6percent of beneficiaries meetingthe Medicare inclusion criteria
Continuing
Medical Education
Foot deformity such as rigid ham-mer digits, requires the roominessof an added-depth shoe with ahigh toe box. Generally a multi-laminated insole will only fit intoan added-depth shoe.
Medicare reimburses patientswith diabetes mellitus with pe-ripheral neuropathy for one pairof therapeutic shoes, shoe modifi-cations, and three pairs of dual
Pressure Reduction...
26 percent to 42 percent in pa-t ients who continued to weartheir therapeutic footwear versus58 percent to 87 percent whenpat ients wore thei r ownshoes.(36,38,39)
In those who did have anulcer recurrence, i t tended tooccur earlier in those who did notwear therapeutic shoes (3 monthsin those not wearing special shoesversus 9 months in those wearingtherapeutic shoes).(39) The type oftherapeutic shoe worn (custommolded versus added-depth) didnot affect the recurrence rate ofulcers.(36,38) It is important that pa-tients wear the shoes all of thetime. In one study patients wear-ing their prescribed shoes morethan 60 percent of the time re-
duced the ulcer relapse rate bygreater than 50 percent comparedto patients who wore their pre-scribed shoes for less time.(40)
Converse ly , the shoe maycause an ulcer mostly on the toesand the dorsum of the foot whenthe shoe is too tight. The mostcommon cause of minor traumato the diabetic foot is from poorlyfitting shoes.(1,41,42) Shoe selectionfor the diabetic foot depends onthe presence of peripheral neu-ropathy, foot deformity, and his-tory of ulceration.(32) Patients withinsensate feet are more likely tobe unaware of foreign bodies inthe sole of the shoe or adjustproperly to poor walking surfacesand may require accommodativeadditional insoles in the shoe.
Circle #45
Continued on page 102
FEBRUARY 2001 • PODIATRY MANAGEMENTwww.podiatrymgt.com 101
Foot ulcers do not occurin individuals with
rheumatoid arthritis,suggesting that high
plantar weight-bearingpressures may be anecessary but not
sufficient condition for afoot ulcer to form.

heel and toe. The heel should beno higher than one inch. Thereshould be 3/8 to 5/8 inch inlength beyond the longest toeand the end of the shoe.(46,47) Shoesolder than two years tend to losetheir shock absorption.(34)
Medicare regulations stipulatethat the depth inlay shoe musthave a minimum of 3/16 inch ad-ditional depth through the shoewhen removable insoles are takenout of the shoe.(43) Standard dualdensi ty insoles for the extra -depth shoe consist of mediumpink plastazote 2 and firm whiteplastazote 3 . The Extra-depthshoe (P.W. Minor & Son, Batavia,
NY) is one of the most commonlyprescr ibed shoes for the footpathology associated with the dia-betic foot (Figure 3). Extra-depthshoes combined with paddedstockings were found to reducein-shoe foot pressures in diabeticpatients at risk for foot ulcerationwhen compared to thei r ownfootwear. (48) SAS comfort shoes(SAS Shoemakers, San AntonioTX) have recently been found tobe as effective in pressure reduc-tion as the extra depth shoe orrunning shoes.(35)
The APEX Ambulator (SouthHackensack, NJ) shoe includes aninsole made of blue ethyvinylac-etate (EVA), antishock-Apex pinkplastazote top and thermoformedurethane (Figure 4). The APEXAmbulator shoe was the most ef-fect ive of f - loading device asdemonstrated by F-scan analysisfor a pat ient with Charcotarthropathy with LisFranc frac-ture dislocation at the authors’institution (Figure 5A/B).
Molded shoes have a place inthe treatment of the diabetic footespecially when the deformity issevere, such as in Charcot foot oreven in severe hammer toe andhallux valgus. The MABAL mold-ed therapeutic shoe and custominsole served as the primary un-loading device healing 21 of 23two-centimeters -square ulcersunder the metatarsals and halluxwith a mean healing time of thir-ty-four days.(49)
Running shoes also have beenfound to be effective in reducingthe size of plantar calluses in dia-betics(50) as well as a reduction of30 percent in forefoot pressure.(51)
IPOS Postoperative HalfShoe/Healing Sandal
The IPOS postoperative shoewas originally designed to take allpressure off the forefoot for useafter surgery.(52,43) The shoe has a10 dorsiflexory wedge and theheel is elevated four centimetersto avoid any forefoot contactwith the ground when walking(Figure 6). The shoe cannot beworn by individuals with ankleequinus or used for bilateral ul-cers. Half shoes were shown to
had a therapeut ic footwearclaim in 1995.(44)
The shoe for the diabetic footwith peripheral neuropathy, mod-erate forefoot deformities, and ahealing or healed ulcer should belaced with blucher closure to pro-vide maximum adjustability.(45) Anadded-depth shoe with wide hightoe box, soft leather upper, cush-ioned rubber crepe sole and re-movable insoles is preferred (Fig-ure 3). A low wedged sole offersgreater support and stability andhas a greater sole surface area forpressure reduction than a separate
Pressure Reduction...Con
tinuin
g
Medica
l Edu
catio
n
102 www.podiatrymgt.comPODIATRY MANAGEMENT • FEBRUARY 2001
Continued on page 103
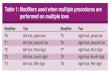
TABLE 1MATERIALS USED
FOR SHOE INSERTS IN DIABETIC INDIVIDUALS
PLASTAZOTE (Apex Foot Products, South Hackensack, N.J.)
Closed cell cross linked irradiated polyethylene foam with nitrogen gas. Durometer Medium=20; firm=35; Rigid=69 (Skin=20). Thermomolding and pressure holding. Will deform to contours of foot.
PPT (Langer Biomechanics Group, Inc., Deer Park, NY),
Open cell urethane foam. About 20 durometers. Smooth on one side. Abraded on other side. Covered with nylon or synthetic suede. Thermosetting.
SPENCO (Spenco Medical Corp., Waco, Tx)
Neoprene rubber foam with enclosed nitrogen gas with nylon covering. Has three way stretch. Decreases shock and shear. Thermosetting.
PELITE (Durr-Fillauer Medical Inc., Chattanooga, TN),
Cross-linked copolymer of polyethylene and EVA. Comes in 4 durometers. Thermomolding.
SORBOTHANE (Sorbothane, Inc., Kent, OH)
Non cellular polyurethane visco-elastic polymer. Thermosetting

The main pressure dispersing materialused for shoe inserts in individuals with diabeticfoot problems is plastazote (Apex Foot Products,South Hackensack, N.J), a closed-cell polyethylene
foam available in three color-codedgrades of density. It can be heatedto 280º F and molded directly tothe patient’s foot. The main shockabsorbing materials are PPT (LangerBiomechanics Group, Inc., DeerPark, NY), an open-cell urethanefoam and Spenco (Spenco MedicalCorp., Waco, TX), a neoprene rub-ber foam with nylon cover ing(Table 1).
Medium plastazote (plastazote1; pink plastazote) fatigues veryrapidly in both compression andshear corresponding clinically tothe phenomenon of “bottomingout.” For the insensitive foot usingplastazote, the force of walking willdissipate through compression ofthe inser t rather than through
breakdown of the plantar skin. This is a function ofthe easy compression of the material.(56) However,due to its extreme loss of thickness upon loading,
Continuing
Medical Educationheal ulcers faster and be associated with fewer seri-ous infections than patients treated with standardwound care therapy.(52)
In a retrospective review of pa-tients with Wagner grade 1 and 2neuropathic forefoot ulceration, 77percent of patients healed their ul-cers with an IPOS postoperativehalf shoe and wore prescription in-serts and extra-depth shoes at amean of 8 weeks follow-up. How-ever , compl icat ions consis t ingmostly of imbalance, falls, boneand joint pain and new ulcerationsoccurred in 38 percent of pa-tients. (52) In another study a cus-tomized healing sandal with a 25degree rigid forefoot rocker signifi-cantly reduced forefoot pressure ascompared to prescription addeddepth shoes.(54)
InsolesInsoles are an important effective treatment for
neuropathic ulcers and markedly help the shoe inpressure reduction. In one large study 88 percent ofulcers were fully healed by soft inserts and correc-tive foot wear within the eighteen-month study pe-riod.(55) The type of materials, thickness, and shapeare all important. Shoe inserts for the diabetic pa-tient are most commonly soft and accommodativewith good cushioning. The insert must be of an ap-propriate thickness and the greater the thicknessthe better the pressure reduction.(36)
Pressure Reduction...
Circle #52
Continued on page 104
FEBRUARY 2001 • PODIATRY MANAGEMENTwww.podiatrymgt.com 103
In one study the additionof a dual density
plastazote/PPT andviscoelastic insoles
provided significantreduction in mean peakpressure with all shoetypes tested including
extra-depth shoes,running shoes and SAS
comfort shoes.
Figure 6: IPOS Postoperative Half Shoe.

greatest reduction in pressure inone study(58) although others havefound no difference in pressurereduction prop-erties of plasta-zote , Spenco,and PPT, but didfind significantplantar pressurereduct ion ofthese mater ia l sas compared tono insole.(59)
A l t h o u g hplastazote in-soles are consis-tently found tolower plantarpressure, modify-ing the insoleswith metatarsalpads and media l longitudinalarch pads did not improve onpressure reduction in diabetic pa-tients with and without hallux
amputations.(60)
In a study testing the effec-tiveness of insoles to heal ulcers,
37 out of 38 dia-bet ic pat ientswith foot ulcersh e a l e d a f t e rusing a specially-constructed in-sole for an aver-a g e o f 3 . 6months . (61) Inthis study a tem-porary insolewas dispensedfor the pat ientto walk with forthe f i r s t twoweeks and subse-quently a modi-f ied insole was
manufactured from imprints in aplastazote model.(61) The pressureunder the ulcer was redistributedby redirecting it more proximallyby excavating the insole underthe ulcerated area.(61)
Recent ly a rocker insole(Langer Biomechanics, Deer Park,New York) has been found to beef fect ive for the t reatment ofmetatarsal head ulceration.(62) Therocker insole works to alleviateforefoot pressure like the rocker-bottom, with the advantage that
plastazote works best whencombined with other materials(Figure 7). Plastazote is generallylaminated as the top layer againstthe skin with PPT or Spenco onthe bottom for shock absorption.A 1/4 inch medium plastazote in-sert used in a sedentary diabeticindividual is estimated to lasteight weeks.(56)
PPT and Spenco inserts werenot found to be reduced in pres-sure relief after being worn forone month. (57) When plastazoteand Poron are used together theyprovide excel lent cushioning,self accommodation and shockattenuation.
Plastazote, latex foam, PPT,Spenco, ortho felt, and molo haveall been demonstrated to decreaseplantar pressure; however, plasta-zote and Spenco resulted in the
Pressure Reduction...Con
tinuin
g
Medica
l Edu
catio
n
104 www.podiatrymgt.comPODIATRY MANAGEMENT • FEBRUARY 2001
Figure 7: Prefabricated molded insole shows laminations of medium pink plasta-zote with blue PPT sole.
Figure 8: Custom foot orthosis for people with diabetes mellitus. (LBG, Biome-chanics, Deer Park, New York).
Figure 9A: DH-Pressure Relief Walker(Royce Medical Co., Camarillo, CA).
Continued on page 105
Extra-depth shoescombined with paddedstockings were found to
reduce in-shoe footpressures in diabetic
patients at risk for footulceration when
compared to their ownfootwear.

with foot deformities must redirect pressureaway from the high pressure callused metatarsalheads and support the arch in the hyperpronatedfoot. The prescription generally consists of a medi-um plastazote top cover, a PPT dispersion pad and athin polyethylene thermoplastic, or rigid plastazote
shell for arch support.
Total Contact CastingThe total contact cast is a well-
molded, thinly padded below-kneecast that covers the entire foot. Itcan be fabricated of plastic or fiber-glass with or without a walkingheel and can be used to unweightulcers on the plantar forefoot, mid-foot or heel. The total contact castunweights the foot by transferringpressure to the walls of the cast.(68)
It is indicated for superficial plantarulcers (i.e., Wagner grades I and II)
in the presence of decreased or absent sensation.(69)
The patient does not have to have diabetes mellitus.Neuropathic ulcers of virtually any etiology can betreated with a total contact cast. However, the pa-tient must have adequate circulation and theremust be no sign of infection. The total contact cast
Continuing
Medical Educationthe patient is not exposed to the likelihood of trip-ping in a rocker bottom sole.
Custom Foot OrthosesCustom foot orthoses seem to
work better than insoles in pressurereduction and ulcer healing and themechanism at least in some casesseems to be by increasing surfacearea (Figure 8). In one study sevendiabetic patients with foot ulcers orpast histories of foot ulcers, plantarpressures were reduced 56 percentin patients wearing custom foot or-thoses and there was a correspond-ing 63 percent increase in contactarea suggesting a more even pres-sure distribution in the custom footorthoses.(63) Custom foot orthoseswere found to reduce plantar pressure in diabeticpatients with a pronated foot type.(64)
Custom foot orthoses have been shown to re-duce forefoot peak plantar pressure more effectivelythan flat inserts.(65) The custom foot orthoses in thisstudy were fabricated with a rigid plastazote shell, aPPT middle layer and a soft plastazote top coverwith a thickness of 19 mm in the forefoot area. Theflat PPT insoles were 6 mm thick. The reduction offorefoot pressure with the custom foot orthoses wasthought to have been achieved partly by redistribu-tion of the load into the midfoot area as well as theincreased cushioning from the thickness of the cus-tom foot orthoses. Although foot orthoses for dia-betics tend to be soft and accommodative, rigid or-thoses have also been found to reduce plantar pres-sures in the insensitive foot.(66) After 12 months oftreatment with rigid foot orthoses, diabetic patientsshowed a significant reduction in callosities.(67)
The custom foot orthosis for diabetic patients
Pressure Reduction...
Circle #74
Continued on page 106
FEBRUARY 2001 • PODIATRY MANAGEMENTwww.podiatrymgt.com 105
The reduction of forefootpressure with the custom
foot orthoses wasthought to have been
achieved partly byredistribution of the load
into the midfoot area.
Figure 9B: Hexagonal Plugs of the DH-Pressure ReliefWalker should be left in place.

lapse and rockerbottom deformi-ty.(75) The complication rate fortotal contact casting ranges from6 percent to 54percent. The re-currence ratewithin the firstfour weeks afterhealing with totalcontact casting isbetween 35 per-cent and 57 per-cent.(76)
The l ike l i -hood of re-ulcer-ation within thefirst six monthsafter initial heal-ing of a footulcer is so highthat some con-s ider heal ingsuccess ful onlyafter six monthsof continuous skin closure. (77,78)
The total contact castmay soon be replaced bythe prefabricated walk-ing brace as the most ef-fective unweighting de-vice for the diabetic foot(see below).
Prefabricated Below-Knee Walking BraceAlthough the custom
ankle-foot orthosis hasbeen recommended forclosing ulcers in the dia-
betic foot and preventing their re-currence , (79) the prefabr icatedbelow-knee walking braces, in-
cluding the DH-Pressure Rel ie fWalker (RoyceMedical Co., Ca-marillo, CA) (Fig-ure 9A/B). (80,81)
Equalizer Premi-um Walker (RoyceMedical Co., Ca-marillo, CA), (82)
and Aircast Pneu-matic Walker(Summit, NJ) (Fig-ure 10),(83,84) for-mer ly used forlower extremitytrauma, have re-cent ly beenfound to be ef-fective in reduc-ing plantar pres-
sure in the diabetic foot and havebecome very popular unweightingdevices. Average peak forefootpressures were reduced greaterthan 51 percent using the Equal-izer Premium Walker and AircastWalker.(82)
In contrast to the total contactcast these prefabricated walkingbraces are relatively easy to use,inexpensive, and allow easy ac-cess to the wound for dressingchanges. The prefabricated walk-ing brace provides the necessary
has been used on pedal ulcers indiabetic immunosuppressed pa-t ients after transplantation. (70)
Hard-to-heal interphalangeal ul-cers under the great toe have beentreated with Keller arthroplasty inconjunction with total contactcasting.(71)
Healing ulcers with the totalcontact cast is reported to occuron average 91 percent of the time(range 73 percent to 100 percent)and takes one to two monthsfrom the initial start of casting.(72)
Al though the total contactcast remains the gold standard foroff-loading the diabetic foot,(73) nosignificant differences were foundin plantar pressure measurementsbetween conventional short legcasts and total contact casts inhealthy volunteers(74) nor in pa-tients with Charcot midfoot col-
Pressure Reduction...Con
tinuin
g
Medica
l Edu
catio
n
106 www.podiatrymgt.comPODIATRY MANAGEMENT • FEBRUARY 2001
Continued on page 107
Prefabricated walkingbraces have been foundto reduce plantar weight
bearing pressure inhealthy and diabetic
subjects, but theireffectiveness in actuallyhealing diabetic ulcers
in random clinical trials has not yet been
demonstrated.
Figure 11: Charcot Restraint Orthotic Walker (CROW) Orthosis.
Figure 10: Aircast Pneumatic Walker (Summit,New Jersey). This brace is most commonly com-pared to the Total Contact Cast because it hugsthe foot and leg, maintaining total contact for re-duction of edema and pressure.

Pressure Reduction... of wear of a removablewalking brace.
Although these prefabricatedwalking braces have been foundto reduce plantar weight bearingpressure in healthy and diabeticsubjects, their effectiveness in ac-tually healing diabetic ulcers inrandom clinical trials has not yetbeen demonstrated.
Crow OrthosisFor patients with Charcot foot
too deformed to fit into an added-depth shoe, the Charcot RestraintOrthotic Walker (CROW) may beindicated (Figure 11). The CROWorthosis is a rigid, custom full-foot enclosure ankle-foot ortho-sis(87) which provides immobiliza-tion and protection during the
prolonged heal ing of diabet icneuroarthropathy. The orthosis isconstructed with a total posteriorand anterior shell which includesthe foot so that a patient does notneed to wear a shoe with thebrace as would be necessary witha regular plastic AFO or PTBO.Eighteen pat ients rated thei rCROW orthosis as good to excel-lent and none reported signifi-cant activity restrictions whilewearing the orthosis and all pa-tients believed that their life stylewas markedly improved. (87) Thetotal contact bi-valved, rocker-bottom-sole ankle-foot orthosiswas shown to be effective in con-trolling the complications in 14
stability while allowing easy don-ning and doff ing for physical
therapy sessions, washingand sleeping. A rocker soleor ankle jo ints may beadded to facilitate ambula-tion. (84) The prefabricatedwalking brace can be usedfor immobilization of theCharcot foot in diabetic pa-tients.(85)
In one study the DH Pres-sure-Relief walker (RoyceMedical Orthopaedics, Car-marillo, CA) (Figure 9) re-duced plantar pressures underall the metatarsals and thegreat toe significantly betterthan several other off-loadingdevices tested and reducedforefoot pressure equally aswell as the total contactcast.(80) In another study com-paring the DH Pressure ReliefWalker with the Total Con-tact Cast in the reduction ofplantar pressure reduction,the DH Pressure Relief Walkerreduced plantar forefoot pres-sure 85 percent from baselineas compared to 76 percent re-duction in plantar pressurewith a Total Contact Cast.(81)
The Aircast PneumaticWalker, because of its airbladders in the rigid shell,has the advantage overother prefabricated below-knee walkers of a total con-tact fit to reduce edema andshear forces (Figure 10).(86)
In a study comparing theAircast Pneumatic Walkerwith the total contact cast,the Aircast Pneumatic Walk-er decreased peak plantarfoot pressures to an equal orgreater degree than thetotal contact cast in all test-ed locations of the forefoot,midfoot and hindfoot in 10healthy male volunteers.(83)
Recently introduced isthe new prefabricated walk-ing brace, the Bledsoe Con-former Diabetic Boot (Bled-soe Brace Systems, GrandPrairie, TX) which has beenreported to combine thepressure reduction featuresof the total contact castwith the comfort and ease
Continuing
Medical Education
Continued on page 108
FEBRUARY 2001 • PODIATRY MANAGEMENTwww.podiatrymgt.com 107
The felted-foam paddingwith an aperture for the ulcer is directlyapplied to the full
length of the plantaraspect of the foot.
The felted foam paddingworks well as
additional padding inthe prefabricated walking brace.
Figure 12B: PTB Orthosis, metal double uprighttype.
Figure 12A: Patellar Tendon Bearing (PTB) Or-thosis, plastic type, was designed to simulatethe weight bearing of a PTB Prosthesis (shownon left).

original orthoses for unweightingthe rearfoot and the leg.(90,91) It hasa pretibial component in whichthe patient rests his upper leg andknee when ambulating (Figure12A/B). Patients are trained towalk by sinking their weight intothe pretibial shell and the weightis transferred down the uprightsto the floor, bypassing the leg andthe rearfoot. When patients walkproperly with the PTB and a cane,i t has been found to reduceweight bearing on the leg and
rearfoot up to sixty percent.(92)
The PTB was originally indi-cated for patients with fracturesof the leg and rearfoot, and to un-weight a painful diabetic Charcotrearfoot.(90) It has been used to un-weight pat ients with painfulchopart joint amputations.(93)
More recently, a study of 10healthy subjects showed the PTBorthosis was significantly more ef-fective in reducing plantar pres-sure than walking with a castshoe.(94) The PTBO has also recent-ly been found to be successful asan adjunctive treatment in pa-tients with significant lower-limbischaemia and tissue loss compli-cated by neuropathy.(95) Eight pa-tients with lower-limb ischaemiaand neuropathy had ulcer healingwearing the PTBO within f ivemonths.(96)
Patients are able to walk withthe PTBO while the ulcer is heal-ing and once the u lce r hashealed the brace can be used pro-phylactically. The PTBO has theadvantage over to ta l contac tcasting of being removable and iseasier to maintain.(96) It comes inmetal and plastic varieties andmust have a solid ankle and rigidanterior shel l c losure to workproperly.(97-99)
I t i s a lso helpful to have aheel-shoe clearance of 3/8 inch toone inch and a rocker sole.(100) Theadvantage of the metal doubleupright variety is that patientswith diabetes with neuropathy,who are most likely to use this or-thosis, may not be able to toleratea plastic orthosis directly againstthe skin even if the orthosis isl ined with pelite or plastazotefoam.(96)
Felt and Foam Total ContactPadding
Foam and felt padding is atechnique used to off-load ulcerson the plantar and marginal as-pect of the foot.(30) One-quarterinch foam with single-sided adhe-sive positioned on the plantar as-pect of the foot is combined withone-quarter inch felt. The felted-foam padding with an aperturefor the ulcer is directly applied tothe full length of the plantar as-
individuals with Charcot foot.(88)
In a more recent report, all pa-tients wearing the CROW orthosisnoted varying measures of im-provement in symptoms andfunction at an average 12-monthfollow-up.(89)
Patellar Tendon BearingOrthosis
The Patellar Tendon BearingOrthosis (PTBO) is one of the
Pressure Reduction...Con
tinuin
g
Medica
l Edu
catio
n
Continued on page 109
108 www.podiatrymgt.comPODIATRY MANAGEMENT • FEBRUARY 2001
TABLE 2SUMMARY OF METHODS OF
OFF-LOADING THE DIABETIC FOOT
Off-Loading Modality Comments/Advantages/Disadvantages
Complete Bed Rest Compliance is difficult
Assistive Device Canes/Crutches
Total Contact Cast Gold Standard of Off-loading Modalities Can be constructed of plaster or fiberglass.Indications: Neuropathic ulcers from anycause/Wagner Grade 1 & 2 ulcers which are not infected; Circulation must be good. Ulcer may occur anywhere on the plantar aspect including: forefoot, midfoot, orrearfoot, however most effective in healingforefoot ulcers. Cast should be changedusually weekly. Effective in healing 80% of neuropathic ulcers Wagner Grade 1 & 2 within twomonths.Advantages—Efficient off-loading; Totalpatient compliance; Controls edema.Disadvantages—Expensive, hard to use,cannot be tolerated by many patients.
Walking Brace Prefabricated. DH Pressure Relief (Royce MedicalCo.,Camarillo, CA) Aircast Pneumatic Walker (Aircast, Summit,New Jersey) Has been shown in pressure reduction Studies with in-shoe pressure reductionMeasurements to be as effective in reducingplantar pressure as the Total Contact Cast.Advantages—Inexpensive, easy to use, offerseasy access to the wound, can be used withinfected wounds, has been shown to reducepressure effectively with in-shoe pressuremeasurement systems; Good for patients whocannot tolerate a cast. Disadvantages—Patients may have a tendencyto not be compliant and not wear the walkingbrace.
Continued on page 110

abetic American Indians with hallux limitus. J AmPodiatr Med Assoc 79: 447-50, 1989.
19 Boulton AJM: The pathogenesis of diabetic footproblems: An overview. Diabet Med 13: 12, 1996.
20 Masson EA, Hay EM, Stockley I, Veves A, Betts RP,Bouton AJM: Abnormal foot pressures alone may not causeulceration. Diabetic Med 6: 426-8, 1989.
21 Apelqvist J: Wound healing in diabetes Outcomeand costs. Clin Podiatr Med Surg 15(1): 21-39, 1998, Jan-uary.
22 Steed DL: Foundations of good ulcer care. Am J Surg176(Suppl 2A): 20S-25S, 1998.
23 Consensus Development Conference on DiabeticFoot Wound Care. Diabetes Care 22(3): 1354-60, 1999, Au-gust.
24 Prospective Diabetes study Group (See comments)Tight blood pressure control and risk of macrovascularand microvascular complications in type 2 diabetes:UKPDS 38. UK Prospective Diabetes Study Group (see com-ments) (published erratum appears in BM 1999 Jan 2;318(7175): 29) BMJ, 1998. 317(7160): 703-13.
25 The Diabetes Control and Complications (DCCT)Research Group. Effect of intensive therapy on the devel-opment and progression of diabetic nephropathy in theDiabetes Control and Complications Trial. The DiabetesControl and Complications (DCCT) Research Group. Kid-ney Int 47(6): 1703-20, 1995.
26 Boyko EJ, Ahroni JH, Stensel V, Forsberg RC, Davi-gnon DR, Smith DG: A prospective study of risk factors fordiabetic foot ulcer. The Seattle Diabetic Foot Study. Dia-
Continuing
Medical Educationpect of the foot. The felted foam padding workswell as additional padding in the prefabricatedwalking brace. Contraindications include interdigi-tal or dorsal ulcers, severely atrophic plantar skin,acute tinea pedis, and adhesive sensitivity. SeeTable 2 for a summary of the off-loading devices. �
References1 Bauman JH, Girling JP, Brand PW: Plantar pressures
and trophic ulceration An evaluation of footwear. J BoneJoint Surg 45B(4): 652-673, 1963.
2 Pecoraro RE, Reiber GE, Burgess EM: Pathways to dia-betic limb amputation: basis for prevention. Diabetes Care13: 513-521, 1990.
3 Ahroni JH, Boyko EJ, Forsberg RC: Clinical correlatesof plantar pressure among diabetic veterans. Diabetes Care22(6): 965-72, 1999.
4 Stokes IAF, Faris IB, Hutton WC: The neuropathiculcer and loads on the foot in diabetic patients. Acta Or-thop Scan 46: 839-47, 1975.
5 Armstrong DG, Lavery LA: Elevated peak plantarpressures in patients who have charcot arthropathy. JBone Joint Surg 80A(3): 365-9, 1998, March.
6 Ctercteko Gc, Dhanendran M, Hutton WC et al: Ver-tical forces acting on the feet of diabetic patients withneuropatic ulceration. Br J Surg 68: 608-14, 1981.
7 Sims DS, Cavanagh PR, Ulbrecht JS: Risk factors inthe diabetic foot. Recognition and management. PhysTher 68: 1887-902, 1988.
8 B i rke JA, Novick A, Graham S , Coleman WC,Brasseaux DM: Methods of treating plantar ulcers. PhysTher 71: 116-22, 1991.
9 Rith-Najarian SJ, Stolusky T, Gohdes DM: Identifyingdiabetic patients at high risk for lower-extremity amputa-tion in a primary health care setting. A prospective evalua-tion of simple screening criteria. Diabetes care 15(10):1386-9, 1992.
10 Boulton AJ, Betts RP, Franks CI, et al.: The naturalhistory of foot pressure abnormalities in neuropathic dia-betic subjects. Diabetes Res. 5: 73-7, 1987.
11 Young MJ, Cavanagh PR, Thomas G, et al.: The ef-fect of callus removal on dynamic plantar foot pressures indiabetic patients. Diabetic med 9: 55-7, 1992.
12 Boulton AJ, Hardisty CA, Betts RP: Dynamic footpressure and other studies as diagnostic and managementaids in diabetic neuropathy. Diabetes Care. 6: 26-33, 1983.
13 Campbell RR, Hawkins SJ, Maddison PJ et al.,: limit-ed joint mobility in diabetes mellitus. Annals Rheum Dis44: 93-7, 1985.
14 Dijs HM, Roofthooft JMA, Driessens MF et al: Effectof physical therapy on limited joint mobility in the dia-betic foot A Pilot study. J Amer Podiatr Med Assoc 90: 126-32, 2000.
15 Fernando DJS, Masson EA, Veves A, et al: Relation-ship of limited joint mobility to abnormal foot pressuresand diabetic foot ulceration. Diabetes care 14: 8, 1991.
16 Boulton AJM, Franks CI, Betts RP, et al.: Reductionof abnormal foot pressures in diabetic neuropathy using anew polymer insole material. Diabetes Care 7(1): 42-51,1984, Jan/Feb.
17 Veves A, Murray HJ, Young MJ, Boulton AJ: The riskof foot ulceration in diabetic patients with high foot pres-sure: A prospective study. Diabetologia 35(7): 660-3, 1992.
18 Dannels E: Neuropathic foot ulcer prevention in di-
Pressure Reduction...
Circle #84
Continued on page 110
FEBRUARY 2001 • PODIATRY MANAGEMENTwww.podiatrymgt.com 109

29 Armstrong DG, Lavery LA: Evi-dence-based options for off-loadingdiabetic wounds. Clin Podiatr MedSurg 15(1): 95-104, 1998
30 Guzman B, Fisher G, PalladinoSJ, Stavosky JW: Pressure-removingstrategies in neuropathic ulcer thera-py An alternative to total contact cast-ing. Clin Podiatr Med Surg 11(2): 339-353, 1994, April.
31 Reiber GE: Who is at risk oflimb loss and what to do about it? J
Rehabil Res Dev 31: 357-62, 1994.32 Mueller MJ: Therapeutic foot-
wear helps protect the diabetic foot. JAm Podiatr Med Assoc 87(8): 360-4,1997, August.
33 Mayfield JA, Reiber GE, SanderLJ, Janisse D, Pogach LM: Preventivefoot care in people with diabetes. Dia-betes Care 21(12): 2161-77, 1998.
34 Sarnow MR, Veves A, GiuriniJM, et al: In-shoe foot pressure mea-surements in diabetic patients with at-risk feet and in healthy subjects. Dia-betes Care 17: 1002-1006, 1994.
35 Lavery LA, Vela SA, Fleischli JG,Armstrong DG, et al.: Reducing plan-tar pressure in the neuropathic foot Acomparison of footwear. DiabetesCare 20(11): 1706-10, 1997, Nov.
36 Chantelau E, Kushner T, SpraulM: How effective is cushioned thera-peutic footwear in protecting diabeticfeet? Diabet ic Medic ine 7 : 355-9,1990.
37 Slavens ER, Slaven ML: Thera-peutic footwear for neuropathic ul-cers. Foot Ankle Inter 16(10): 663-6,1995.
38 Edmonds ME, Blundel l MP,Morris ME, et al: Improved survival ofthe diabetic foot: the role of a special-ized foot c lnic . QJ Med 232: 763,1986.
39 Uccioli L, Faglia E, Monticone Get al.: Manufactured shoes in the pre-vention of diabetic foot ulcers. Dia-betes Care 18: 1376-1378, 1995.
40 Chantelau E, Haage P: An auditof cushioned diabetic footwear: rela-tion to patient compliance. DiabetMed 11: 114-6, 1994.
41 Isakov E, Susak Z, Budoragin N,Mendelevich I: Self-injury resulting inamputation among vascular patients:a retrospective epidemiological study.Disability and Rehabilitation 14: 78-80, 1992.
42 Rausher H, Rausher SR, Fried-man EA: Preserving feet in the uremicdiabetic: the physician’s role. J Dia-betic Complications 2: 145-9, 1988.
43 Janisse DJ: Accessing the thera-peutic shoe bill. Commentary. J AmerPodiatr Med Assoc 89(9): 460-1, 1996,Sept.
44 Sugarman JR, Reiber GE, Baum-gardner G, Prela CM, Lower J: Use ofthe therapeut ic footwear benef i tamong diabetic medcare beneficiariesin three states, 1995. Diabetes care21(5): 777-81, 1998, May.
45 Janisse DJ: Pedorthic care of thediabetic foot. In The Diabetic Foot,5th ed. Levin ME, O’Neal LW, BowkerJH, Eds. St. Louis, Mosby Year Book,1993, p. 549-575.
46 Coleman WC: Footwear in a
betes Care 22(7): 1036-442, 1999.27 Mantey I, Foster AV, Spencer S
& Edmonds ME: Why do foot ulcersrecur in diabetic patients? Diabet Med16(3): 245-9, 1999.
28 Catanzariti AR, Haverstock BD,Grossman JP et al.: Off-loading tech-niques in the treatment of diabeticplantar neuropathic foot ulceration.Adv Wound Care 12(9): 452-8, 1999.
Pressure Reduction...Con
tinuin
g
Medica
l Edu
catio
n
Continued on page 111
110 www.podiatrymgt.comPODIATRY MANAGEMENT • FEBRUARY 2001
TABLE 2 (CONTINUED)
SUMMARY OF METHODS OF OFF-LOADING THE DIABETIC FOOT
Off-Loading Modality Kinds/Advantages/Disadvantages
Half-Shoe OrthoWedge Healing Shoe (DarcoInternational, Inc. Huntington, WV) Has a 10˚ dorsiflexory wedge. Patient musthave good ankle dorsiflexion range of motion.Good for ulcers under the hallux and lesserdigits. Cannot be used bilaterally.Complications include balance problems andfalling.Advantages—Easy to use, inexpensive,provides total unloading of the forefoot, easyaccess to the wound. Disadvantages—Cannot be used for patientswith ankle equinus. Tendency to createinstability and patients may fall, this mayespecially be a problem in the elderly.
Insoles Should be multidensity, soft, full footPlastazote/PPT Combination with plastazoteagainst the skin for dispersion of pressure and PPT closest to ground for cushioning andshock absorption.
Shoe Wear Extradepth shoes with plastazote insoles form the standard of care for the basicpressure reduction for the diabetic foot. A rocker bottom sole may be helpful inreducing pressure from the metatarsal heads.Molded shoes may be necessary for diabeticpatients with severe charcot foot deformity.
Custom Foot Orthosis Should be accommodative and soft.
Patellar Tendon Bearing Unweights the rearfoot (PTB) Orthosis Can effectively reduce rearfoot pressure up to
60% when used with a cane. Must be constructed with a solid ankle and astable pretibial shell. Can be made of plastic or metal.Disadvantages—Not a comfortable brace.Patients must use a cane and be taught towalk in a new way sinking their upper leg into the brace in order for maximalunweighting of the rearfoot to occur.
Continued on page 112

JB, Hoard AS, Hawkins ES: Reduction of plantarpressure with rigid relief orthosis. J Am Podiatr MedAssoc 83(3): 115-122, 1993.
67 Colagiuri S, Marsden LL, Naidu V, Taylor L: The useof orthotic devices to correct plantar callus in people withdiabetes. Dabetes Res Clin Practice 28: 29-34, 1995.
68 Shaw JE, His WL, Ulbrecht JS, Norkitis A: The mech-anism of plantar unloading in total contact casts: Implica-tions for design and clinical use. Foot Ankle Inter 18: 809-17, 1997.
69 Sinacore Dr, Mueller MJ: total contact casting in thetreatment of neuropathic ulcers. In: Levin ME, O’Neal,LW, Bowker JH, eds. The Diabetic Foot. 5th ed. St Louis,Mo: Mosby-Year Book Inc; 1993: 285-304.
70 Sinacore DR: Healing times of pedal ulcers in diabet-ic immunosuppressed patients after transplantation. ArchPhys Med Rehabil 80: 935-40, 1999, Aug.
71 Lin SS, Bono CM, Lee TH: Total contact casting andKeller Arthroplasty for diabetic great toe ulceration underthe interphalangeal joint. Foo Ankle 21(7): 588-93, 2000.
72 Sinacore D: Total contact casting for diabetic neuro-pathic ulcers. Phys Ther 76(3): 296-301, 1996, March.
73 Fleishli JG, Laughlin TJ: TCC remains gold standardfor off-loading plantar ulcers. Biomechanics. 5: 43-53,1998.
74 Conti SF, Martin RL, chaytor ER, Hughes C, Lutter L:Plantar pressure measurements during ambulation inweight bearing conventional short leg casts and total con-tact casts. Foot Ankle Inter 17: 464, 1996.
75 Martin RL, Conti SF: Plantar pressure analysis of dia-
Continuing
Medical Educationmanagement program for injury prevention. In The Dia-betic Foot. 5th ed. Levin ME, O’Neal LW, Bowker JH, Eds.St. Louis, Mosby Year Book, 1993, p. 531-547.
47 Schwartz RS, Schwartz RB: Fitting footwear for dia-betic foot disorders. Physical Therapy Products 48-50,1995.
48 Donaghue VM, Sarnow MR, Giurini JM, Chrzan JS,Habershaw GM, Veves A: Longitudinal in-shoe foot pres-sure relief achieved by specially designed footwear in highrisk diabetic patients. Diabetes Research & Clinical Prac-tice 31(1-3): 109-14, 1996, Mar.
49 Hissink RJ, Manning HA, van Baal JG: The MABALshoe, an alternative method in contact casting for thetreatment of neuroapathic diabetic foot ulcers. Foot AnkleIntern 21(4): 320-3, 2000.
50 Soulier SM: The use of running shoes in the preven-tion of plantar diabetic ulcers. J Am Podiatr Med Assoc76(7): 395-400, 1986.
51 Perry J, Ulbrecht J, Derr J, et al: The use of runningshoes to reduce plantar pressures in patients who have di-abetes. J bone Joint Surg 77A: 1819, 1995.
52 Chantelau E, Breuer U, Leisch AC, et al: Outpatienttreatment of unilateral diabetic foot ulcers with ‘halfshoes’. Diabetic Med 10: 267-70, 1993.
53 Needleman RL: Successes and pitfalls in the healingof neuropathic forefoot ulcerations with the IPOS postop-erative shoe. Foot Ankle Inter 18(7): 412-17, 1997.
54 Giacalone VF, Armstrong DG, Ashry HR, Lavery DC,Harkless LB, Lavery LA: A quantitative assessment of heal-ing sandals and postoperative shoes in offloading the neu-ropathic diabetic foot. J Foot Ankle Surg 36: 28-30, 1997.
55 Larsen K, Holstein P, Decker T: Limb salvage in dia-betics with foot ulcers. Prosthet Orth Intern 13: 100-103,1989.
56 Brodsky JW, Kourosh S, Still M, Mooney V: Objec-tive evaluation of insert material for diabetic and athleticfootwear. Foot Ankle 9(3): 111-6, 1988.
57 Barrow J, Hughes J, Clark P, Klenerman L: A study ofthe effect of wear on the pressure-relieving properties offoot orthosis. The Foot 1: 195-9, 1992.
58 Leber C, Evanski PM: A comparison of shoe insolematerials in plantar pressure relief. Prosthet Orthot Int 10:135-8, 1986.
59 Sanfilippo PB, Stess RM, Moss KM: Dynamic plantarpressure analysis Comparing common insole materials. JAmer Podiatr Med Assoc 82(10): 507-513, 1992, Oct.
60 Ashry HR, Lavery LA, Murdoch DP, Frolich M, Lav-ery DC: Effectiveness of diabetic insoles to reduce footpressures. J Foot Ankle Surg36(4): 268-71, 1997.
61 Holstein P, Larsen K, Sager P: Decompression withthe aid of insoles in the treatment of diabetic neuropathiculcers. Acta Orthop Scand 47: 463-8, 1976.
62 Frykberg RG: Offloading properties of a new rockerinsole. Diabetes, A Journal of the American Diabetes Asso-ciation, 47(Suppl 1): A168.
63 Kato H, Takada T, Kawamura T, Hotta N, Torii S:The reduction and redistribution of plantar pressuresusing foot orthoses in diabetic patients. Diabetes Research& Clinical Practice. 31(1-3): 115-8, 1996, March.
64 Albert S, Rinoie C: Effect of custom orthotics onplantar pressure distribution in the pronated diabetic foot.J Foot ankle Surg 33: 598-604, 1994.
65 Lord M, Hosein R: Pressure redistribution by moldedinserts in diabetic footwear: a pilot study. J Rehabil ResDev 31: 213, 1994.
66 Novick A, Stone J, Birke Ja, Brasseaux dM, broussard
Pressure Reduction...
Circle #5
Continued on page 112
FEBRUARY 2001 • PODIATRY MANAGEMENTwww.podiatrymgt.com 111

vices. J Foot & Ankle Surg 35(2): 149-54, 1996.
83 Baumhauer JF , Wervey R,McWilliams J, Harris GF, Shereff MJ: Acomparison study of plantar foot pres-sure in a standardized shoe, total con-tact cast, and prefabricated pneumaticwalking brace. Foot & Ankle Inter 18:26-33, 1997.
84 Ritz G, Rowland WD, RowlandJW: Use of the Cam Walker in treatingdiabetic ulcers . J Am Podiatr MedAssoc 86(6): 253-6, 1996, June.
85 Brodsky JW: Outpatient diagno-sis and care of the diabetic foot. in In-structional Course Lectures 42: 121,1993.
86 Myerly SM, Stavosky JW: An al-ternative method for reducing plantarpressure in neuropathic ulcers AdvWound Care 10(1): 26-29, 1997.
87 Morgan JM, Biehl WC, WagnerfW: Management of neuropathicarthropathy with the Charcot Re-straint Orthotic Walker. Clin OrthopRel Res 296: 58-63, 1993.
88 Boninger ML, Leonard JA: Useof bivalved ankle-foot orthosis in neu-ropathic foot and ankle lesions. JRehab Res Dev 33: 16, 1996.
89 Mehta JA, Brown C, Sargeant N:Charcot Restraint Orthotic Walker.Foot Ankle Int 19: 619, 1998.
90 Rubin G: The patellar-tendon-bearing (PTB) orthosis. Bull Hosp J Dis33: 155, 1972.
91 Cohen-Sobel E: “Advances inFoot Prosthetics,” in Advances in Pod-
iatric Medicine and Surgery, volume1, ed by SJ Kominsky, Mosby-YearBook, Inc., St. Louis, Missouri, 1995.pp. 213-294.
92 Lehmann JF, Warren CG: Is-chial and patellar-tendon weight-bear-ing braces: Function, design, adjust-ment, and training. Bull Prosthet Res10: 6, 1973.
93 Cohen-Sobel E, Caselli MA, Riz-zuto J: Prosthetic management of achopart amputation variant. J. AmerPodiat Med Assoc 84: 505, 1994.
94 Birke JA, Sims DS, Buford WL:Walking casts: effect on plantar footpressures. J Rehab Res 22: 18-22, 1985.
95 Khaira HS, Coddington T, DrewA, Roberts PN, Imray CHE: Patellartendon bearing orthosis—Applicationas adjunctive treatment in healing oflower-limb tissue loss. Eur J Vasc En-dovasc Surg 16: 485-88, 1998.
96 Guse ST, Alvine FG: Treatmentof diabetic foot ulcers and charcotneuroarthropathy using the patellartendon-bearing brace. Foot Ankle In-tern 18: 675-7, 1997.
97 Rubin G, Staros A, Cohen-SobelE: Letter to the editor. Foot Ankle 15:46, 1994.
98 Saltzman CL, John KA, Gold-stein RH, Donnelly RE: The patellar-tendon bearing brace as treatment forneurotrophic arthropathy. A dynamicforce monitoring study. Foot AnkleInt 13: 14-22, 1992.
99 Sobel E, Levitz SJ, Jones LS: Or-thotic Variants. Journal of the Ameri-can Podiatric Medical Association vol-ume 87 23-31, 1997.
100 Lehmann JF, Warren CG, Pem-berton DF, Simons BC DeLateur BJ:Load-bearing function of patellar ten-don bearing braces of various designs.Arch Phy Med Rehabi l 52 : 36-70,1971.
betic rockerbottom deformity intotal contact casts. Foot Ankle Inter17: 470, 1996.
76 Helm PA, Walker SC, PulliumGF: Recurrence of neuropathic ulcera-tion following healing in a total con-tact cast. Arch Phy Med Rehabil 72:967-70, 1991.
77 Apelqvist J, Castenfors J, Lars-son J, et al. Wound classification ismore important than site of ulcera-tion in the outcome of diabetic footulcers. Diabet Med. 6: 526-30, 1989.
78 Apelqvist J, Larsson J, AgardhCD: Long-term prognosis for diabeticpatients with foot ulcers. J Intern Med233: 485-01, 1993.
79 Landsman AS, Sage R: Off-load-ing neuropathic wounds associatedwith diabetes using an ankle-foot or-thosis. J Amer Podiatr Med Assoc 87:349, 1997.
80 Lavery LA, Vela SA, Lavery DC,Quebedeaux TL: Reducing dynamicfoot pressures in high-risk diabeticsubjects with foot ulcerations: a com-parison of treatments. Diabetes Care19: 818-821, 1996.
81 Fleishli JG, Lavery LA, Vela SA,Ashry H, Lavery DC: Comparison ofstrategies for reducing pressure at thesites of neuropathic ulcers. J Am Podi-atr Med Assoc 87: 46-72, 1997.
82 Glod DJ, Fettinger P, GibbonsRW: A comparison of weightbearingpressures in various postoperative de-
Pressure Reduction...Con
tinuin
g
Medica
l Edu
catio
n
112 www.podiatrymgt.comPODIATRY MANAGEMENT • FEBRUARY 2001
TABLE 2 (CONTINUED)
SUMMARY OF METHODS OF OFF-LOADING THE DIABETIC FOOT
Off-Loading Modality Kinds/Advantages/Disadvantages
Felted Foam Dressing Consists of foam-felt dispersive padding overthe ulcer. Has been shown to be effective inhelping to heal ulcers and is used at a varietyof centers. Advantages—Effective, easy to use,InexpensiveDisadvantages—Cannot be used withsensitive skin which is common in patientswith diabetes mellitus
CROW Orthosis Charcot Restraint Orthotic Walker Consists of a bivalved (total contact) AFOwhich can be worn directly without a shoe.For the very deformed foot. Advantages:Good stability and provides mobility for a verydeformed foot which would not be able to fitinto a store bought shoe.
Ellen Sobel, D.P.M., Ph.D., is Asso-ciate Professor of Podiatric Ortho-pedics at NYCPM. Dr. Sobel was agrant reviewer this past summerfor the Nat ional Inst i tute ofHealth (NIH) in the area of Diabet-ic Foot Research. Steven J. Levitz,D.P.M., is a Professor of PodiatricOrthopedics at NYCPM.

with plastazote/PPT/Spencocombinations with plastazoteclosest to the skin and worn withtherapeutic shoes.B) The insole should be as thinand light weight as possible.C) If the insole is made particular-ly well, therapeutic footwear willnot improve upon the effects ofwearing the insoles alone.D) Custom molded shoes do notrequire an insole.
7) In studies comparing the effective-ness of prefabricated insoles withcustom foot orthoses for the diabeticfoot:
A) Prefabricated insoles reduceplantar foot pressure more thancustom foot orthoses.B) Custom foot orthoses reduceplantar foot pressure more thanprefabricated insoles.C) Prefabricated insoles and cus-tom foot orthoses reduce plantarweight bearing pressure equallywell.D) It is not known whether cus-tom foot orthoses or prefabricat-ed foot orthoses work equallywell in reducing plantar foot pres-sure in the diabetic foot.
8) What has been shown regardingthe prefabricated walking bracessuch as the DH Pressure-Relief Walkerand the Pneumatic AirCast Walker?
A) The prefabricated walkingbraces are ineffective in off-load-ing diabetic foot ulcers.B) The prefabricated walkingbraces are effective in reducingpressure and off-loading the di-abetic foot, but have not beenshown to actually heal ulcers indiabetic patients in clinicalstudies.C) The prefabricated walkingbraces are effective in reducingpressure and off-loading the dia-betic foot, and have recentlybeen shown to actually heal ul-cers in diabetic patients in clinicalstudies.D) The prefabricated walkingbraces are not effective off-load-ing devices, but they have beeneffective in healing ulcers anyway.
1) What percentage of lower extremi-ty amputations is preceded by a footulcer in diabetic people?
A) 85 percentB) About 50 percentC) 15 percentD) Impossible to tell
2) The most common pathway lead-ing to lower extremity amputation inpeople with diabetes was found tobe:
A) Neuropathy—Infection—Ulcer-ationB) Neuropathy—Peripheral Vascu-lar Disease—GangreneC) Repetitive Microtrauma—Neu-ropathy—InfectionD) Repetitive Microtrauma—Ul-ceration—Failure to Heal
3) Where is the most common site ofulceration in the diabetic foot?
A) MidfootB) HeelC) Metatarsal headsD) All of these
4) Approximately how long should ittake for an ulcer to heal using an un-loading device?
A) 2 weeks-4 weeksB) 4 weeks to 12 weeksC) Up to 6 months is normalD) Can not tell
5) What can be concluded about therole of shoewear in off-loading the di-abetic foot?
A) Shoewear is important afterthe primary unloading device isused, but can never be used as aprimary unloading device.B) Molded shoes have been foundto be more effective in reducingplantar weight-bearing pressurethan added-depth shoes.C) Therapeutic shoes have beenfound to be highly effective inpreventing ulcer recurrence.D) Therapeutic shoes in peoplewith diabetes work mostly by pro-viding good arch support.
6) In order to get the maximum ben-efit from the insole for the diabeticfoot:
A) The insole should be laminated
9) A contraindication for total contactcasting is:
A) Severe neuropathyB) Wagner grade 1 and 2 ulcersC) ImmunosuppressionD) Minor infection
10) How does the pressure reductioncapacity of the prefabricated walkingbrace compare with the total contactcast?
A) Prefabricated walking brace re-duces pressure as well or betterthan the total contact cast.B) Total contact cast reduces pres-sure greater than the prefabricat-ed walking braces.C) It is unknown whether prefab-ricated walking braces reducepressure greater than the totalcontact cast.D) Neither the prefabricatedwalking brace or the total contactcast reduce pressure very well.
11) The PTB orthosis can be said to:A) Totally unweight the forefoot.B) Totally unweight the rearfoot.C) Unweight the rearfoot 60 per-cent and also the leg.D) Unweight the rearfoot 60 per-cent, and also the leg, and shouldbe worn with a cane.
12) For patients with a deformedCharcot foot who cannot fit into anadded-depth shoe, a good unweight-ing choice would be:
A) Running shoe with customfoot orthosisB) Crow OrthosisC) Custom molded shoesD) Crow Orthosis or Custommolded shoes
13) The prefabricated walking bracewas originally used for:
A) Post-operative surgical braceB) Diabetic foot ulcersC) Lower extremity traumaD) Infection
14) How is insole thickness related topressure reduction for unloading thediabetic foot?
A) The thicker the insole thegreater the pressure reduction.
Continuing
Medical EducationE X A M I N A T I O N
See answer sheet on page 115.
FEBRUARY 2001 • PODIATRY MANAGEMENTwww.podiatrymgt.com 113
Continued on page 114

PM’sCPME Program
Welcome to the innovative Continuing EducationProgram brought to you by Podiatry ManagementMagazine. Our journal has been approved as asponsor of Continuing Medical Education by theCouncil on Podiatric Medical Education.
Now it’s even easier and more convenientto enroll in PM’s CE program!
You can now enroll at any time during the yearand submit eligible exams at any time during yourenrollment period.
PM enrollees are entitled to submit ten examspublished during their consecutive, twelve–monthenrollment period. Your enrollment period beginswith the month payment is received. For example,if your payment is received on September 1, 1999,your enrollment is valid through August 31, 2000.
If you’re not enrolled, you may also submit anyexam(s) published in PM magazine within the pasttwelve months. CME articles and examinationquestions from past issues of Podiatry Man-agement can be found on the Internet athttp://www.podiatrymgt.com/cme. All lessonsare approved for 1.5 hours of CE credit. Please readthe testing, grading and payment instructions to de-cide which method of participation is best for you.
Please call (631) 563-1604 if you have any ques-tions. A personal operator will be happy to assist you.
Each of the 10 lessons will count as 1.5 credits;thus a maximum of 15 CME credits may beearned during any 12-month period.
The Podiatry Management MagazineCPME program is approved by the Council onPodiatric Education in all states where creditsin instructional media are accepted. This arti-cle is approved for 1.5 Continuing EducationHours (or 0.15 CEU’s) for each examinationsuccessfully completed.
PM’s CME program is valid in all statesexcept Kentucky, Pennsylvania, and Texas.
www.podiatrymgt.com
B) The thinner the insole the greater the pressure re-duction.C) There is no relationship between thickness of theinsole and pressure reduction.D) The insole material is more important than thethickness of the insole.
15) How is the IPOS dorsiflexory half shoe used in theoff-loading of diabetic foot ulcers?
A) It should not be used because it is ineffective.B) Used for ulcers under the forefoot.C) Used for ulcers under the heel.D) Used for ulcers anywhere under the plantar aspectof the foot as long as it is unilateral and the patienthas adequate dorsiflexion.
16) In general how should the pegged hexagons be usedwith the DH Pressure Relief Walker?
A) They should be removed exactly where the ulcer isfor dispersion.B) They should be removed a little wider than the di-ameter of the ulcer to avoid the edge effect.C) They should be removed a little narrower than thediameter of the ulcer.D) They should not be removed.
17) All of the following are risk factors for foot ulcers EX-CEPT:
A) NeuropathyB) Reduced passive joint range of motionC) Foot deformity such as hammer toes and bunionsD) Abnormally reduced plantar foot pressures
18) The felted foam dressing should NOT be used:A) On plantar foot ulcers in patients with severe neu-ropathyB) In elderly patientsC) On sensitive skinD) With prefabricated walking braces
19) The gold standard for unweighting the diabetic foot is:A) In-depth inlay shoes and dual density insolesB) Dorsiflexory wedge half shoeC) Prefabricated walking braceD) Total Contact Cast
20) What is the relationship between high plantar pressuresand plantar foot ulcers in people with diabetes mellitus?
A) High plantar pressure is a necessary but not suffi-cient condition for a foot ulcer to develop.B) High plantar pressure is a necessary and sufficientcondition for a foot ulcer to develop.C) There is no relationship between high plantarpressures and the development of plantar foot ulcers.D) There is an inverse relationship between highplantar pressures and the development of plantarfoot ulcers.
E X A M I N A T I O N
(cont’d)
Contin
uing
Medica
l Edu
catio
n
See answer sheet on page 115.
114 PODIATRY MANAGEMENT

Over, please
Continuing
Medical Education
Please print clearly...Certificate will be issued from information below.
Name _______________________________________________________________________Soc. Sec. #______________________________Please Print: FIRST MI LAST
Address_____________________________________________________________________________________________________________
City__________________________________________________State_______________________Zip________________________________
Charge to: _____Visa _____ MasterCard _____ American Express
Card #________________________________________________Exp. Date____________________
Note: Credit card payment may be used for fax or phone-in grading only.
Signature__________________________________Soc. Sec.#______________________Daytime Phone_____________________________
State License(s)___________________________Is this a new address? Yes________ No________
Check one: ______ I am currently enrolled. (If faxing or phoning in your answer form please note that $2.50 will be charged to your credit card.)
______ I am not enrolled. Enclosed is a $15.00 check payable to Podiatry Management Magazine for each exam submitted. (plus $2.50 for each exam if submitting by fax or phone).
______ I am not enrolled and I wish to enroll for 10 courses at $99.00 (thus saving me $51 over the cost of 10 individual exam fees). I understand there will be an additional fee of $2.50 for any exam I wish to submit via fax or phone.
Note: If you are mailing your answer sheet, you must completeall info. on the front and back of this page and mail with yourcheck to: Podiatry Management, P.O. Box 490, East Islip,NY 11730. Credit cards may be used only if you are faxing orphoning in your test answers.
TESTING, GRADING AND PAYMENT INSTRUCTIONS(1) Each participant achieving a passing grade of 70% or high-
er on any examination will receive an official computer form statingthe number of CE credits earned. This form should be safeguardedand may be used as documentation of credits earned.
(2) Participants receiving a failing grade on any exam will benotified and permitted to take one re-examination at no extra cost.
(3) All answers should be recorded on the answer formbelow. For each question, decide which choice is the best an-swer, and circle the letter representing your choice.
(4) Complete all other information on the front and back ofthis page.
(5) Choose one out of the 3 options for testgrading: mail-in,fax, or phone. To select the type of service that best suits yourneeds, please read the following section, “Test Grading Options”.
TEST GRADING OPTIONSMail-In GradingTo receive your CME certificate, complete all information and
mail with your check to:Podiatry Management
P.O. Box 490, East Islip, NY 11730There is no charge for the mail-in service if you have already
enrolled in the annual exam CPME program, and we receive this
Enrollment/Testing Informationand Answer Sheet
exam during your current enrollment period. If you are not en-rolled, please send $15.00 per exam, or $99 to cover all 10exams (thus saving $51 over the cost of 10 individual exam fees).
Facsimile GradingTo receive your CPME certificate, complete all information and
fax 24 hours a day to 1-631-563-1907. Your CPME certificate willbe dated and mailed within 48 hours. This service is available for$2.50 per exam if you are currently enrolled in the annual 10-examCPME program (and this exam falls within your enrollment period),and can be charged to your Visa, MasterCard, or American Express.
If you are not enrolled in the annual 10-exam CPME pro-gram, the fee is $17.50 per exam.
Phone-In GradingYou may also complete your exam by using the toll-free
service. Call 1-800-232-4422 from 10 a.m. to 5 p.m. EST, Mon-day through Friday. Your CPME certificate will be dated thesame day you call and mailed within 48 hours. There is a $2.50charge for this service if you are currently enrolled in the annual10-exam CPME program (and this exam falls within your enroll-ment period), and this fee can be charged to your Visa, Master-card, or American Express. If you are not currently enrolled, thefee is $17.50 per exam. When you call, please have ready:
1. Program number (Month and Year)2. The answers to the test3. Your social security number4. Credit card information
In the event you require additional CPME information,please contact PMS, Inc., at 1-631-563-1604.
E N R O L L M E N T F O R M & A N S W E R S H E E T
✄
115

Contin
uing
Medica
l Edu
catio
n
E N R O L L M E N T F O R M & A N S W E R S H E E T (cont’d)
✄
LESSON EVALUATION
Please indicate the date you completed this exam
_____________________________
How much time did it take you to complete the lesson?
______ hours ______minutes
How well did this lesson achieve its educational objectives?
_______Very well _________Well
________Somewhat __________Not at all
What overall grade would you assign this lesson?
A B C D
Degree____________________________
Additional comments and suggestions for future exams:
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
EXAM #2/2001Pressure Reduction and Off-Loading
the Diabetic Foot(Sobel & Levitz)
1. A B C D
2. A B C D
3. A B C D
4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
11. A B C D
12. A B C D
13. A B C D
14. A B C D
15. A B C D
16. A B C D
17. A B C D
18. A B C D
19. A B C D
20. A B C D
Circle:
116 www.podiatrymgt.comPODIATRY MANAGEMENT • FEBRUARY 2001