Embed Size (px)
Citation preview

1
Evidence-Based Care Planning
The Route to Effective and Efficient Care
2
Objectives
� To review the care processes underlying assessment and care planning
� To identify the context of the MDS/RAI in the care planning process
� To identify an efficient and effective approach to evidence-based care planning
� To show how evidence-based care planning can help attain individualized ("person-centered") care
Overview
3
The RAI Process
The development of an individualized care plan is predicated upon the RAI Process being used to its fullest and then some.

4
Contemporary Nursing Homes
� Multiple challenges
� High expectations
� Complex patients
� High consequences for failed performance
� Complex payment system and rules
� New MDS
� Regulatory compliance pressure
� Assessment/documentation requirements
5
Steps to Evidence-Based Care
� Collect and analyze informationin order to perform- Accurate problem definition & cause identification
resulting in - Effective clinical problem solving and
decision makingleading to - Appropriately individualized
interventions
Adapted from: Levenson SA. The basis for improving and reforming long-term care, Part 2: Clinical problem solving and evidence-based care. J Am Med Dir Assoc 2009; 10: 520–529.
6
Critical Intermediate Steps to Evidence-Based Care
� Critical intermediate steps in between collecting information and choosing interventions� Accurate problem definition and cause identification
� Effective clinical problem solving and decision making

7
Care Planning
� An enduring tradition in nursing care
� Activities related to identifying basis of care and developing strategies to provide it
� Basically, it is part of the clinical problem solving and decision making process� Relevant to all disciplines
� Different disciplines emphasize various aspects
� Must be in proper context� CMS RAI Manual for MDS 3
� Chapter 4 / Table 2
8
Clinical Problem Solving and Decision Making Process
� Recognition / Assessment
� Diagnosis / cause-effect analysis
� Identify goals and objectives of care
� Select interventions / provide care
� Monitor progress
9
Recognition / Assessment
� Gather essential information about the individual
� To help define conditions, strengths, needs, risks, problems, and prognosis
� Activities
� Obtain a personal and medical history
� Perform a physical assessment

10
Problem Definition
� Define the individual's problems, risks, and issues
� Activities� Identify consequences and complications of the individual's situation, underlying condition and illnesses, etc.
� Clearly state individual’s issues and physical, functional, and psychosocial strengths, problems, needs, deficits, and concerns
� Define significant risk factors
11
Diagnosis / Cause-and-Effect Analysis
� Identify physical, functional, and psychosocial causes of risks, problems, and other issues, and relate to one another and to their consequences
� Activities� Identify causes and contributing factors related to dysfunctions, disabilities, impairments, and risks
� Identify pertinent evaluations and diagnostic tests � Identify relationships among symptoms, signs, diagnoses, test results, impairments, disabilities
� Identify potential impact of addressing causes
12
Identify Goals and Objectives of Care
� Clarify
� Purpose of providing care
� Relevance of specific interventions
� Criteria for determining whether objectives are being met
� Activities
� Clarify prognosis
� Define overall goals for the individual
� Identify criteria for meeting goals

13
Selecting Interventions / Provide Care
� Identify and implement interventions and treatments to address the individual's physical, functional, and psychosocial needs, concerns, problems, and risks
� Activities� Identify specific symptomatic and cause-specific interventions (physical, functional, and psychosocial)
� Clarify anticipated benefits and risks of various interventions
14
Monitor Progress
� Review individual’s progress towards goals and modify approaches as needed
� Activities
� Identify individual’s response to interventions and treatments
� Identify factors affecting progress towards achieving goals
� Define or refine prognosis
15
Monitor Progress
� Activities (continued)� Define or refine when to stop or modify interventions
� Review effectiveness and adverse consequences related to treatments
� Adjust interventions as needed
� Identify when care objectives have been achieved sufficiently to allow for discharge, transfer, or change in level of care

16
Minimum Data Set (MDS)
� Standardized collection of basic data about residents in three key dimensions
� Physical (e.g., medical conditions, weight, skin condition, and vision)
� Functional (e.g., activities of daily living, behavior)
� Psychosocial (e.g., preferences, beliefs, goals, interests, and family interactions)
17
MDS as Foundation
� MDS 3.0 has
� More detail about personal preferences and choices
� Several improved screening tools
� CAM, BIMS, PHQ-9
� Screening tools are not diagnostic
� Foundation for identifying possible issues / concerns needing additional review
18
MDS / RAI & Clinical Problem Solving / Decision Making
� Meaningful and helpful when used correctly for intended purposes
� RAI use can be a problem; especially if� Used without adequate understanding
� Used in a manner that exceeds the user’s knowledge and understanding
� Used for purposes for which not designed
� Critical place in the process� But it is NOT the whole process

19
Recognition / Assessment: MDS Relevance
� Gather essential information about individual
� Function
� Behavior / mood / cognition
� Preferences
� A few select symptoms and conditions
� Pain, skin condition
� Supplemental Activities
� Detailed history, basic physical assessment
20
Essential Basis For Care Planning
� Evidence-based care enhanced when staff focus on � Carefully gathering, documenting, and reporting chronological history (“tell a story”)
� Obtaining as much detail as possible from the resident
� Or, alternatively, constructing and reporting a good, detailed “story” as surrogate historian
� Reporting and documenting objective details of observations and examinations
21
Problem Definition: MDS Relevance
� MDS gives information useful to a problem list� Only fragments of information, but not enough for full problem definition
� Supplemental Activities� Define problems (consequences, risks, and complications) in detail
� Make clear, detailed problem and issue statements
22
Problem Definition
� Evidence-based care requires a clear and detailed statement of the issue
� Difference between a “chief complaint”and a problem statement
� An issue or problem is different from a finding � e.g., a single piece of information from the MDS or a test result
23
Defining the Issue
� Other examples of a “chief complaint”� Resident has a headache
� Resident is vomiting
� Resident cannot be aroused
� Resident is “agitated”
� Resident coughs when she eats
� Resident is not participating as usual
� All of these need much more detail to be meaningful
24
MDS as a Screening Tool
� IF certain responses on the MDS
� THEN Care Area Assessment triggered
� BECAUSE item may be associated with possible presence of a condition, concern, risk, or problem
� Further assessment needed to determine significance
� BECAUSE MDS findings alone cannot guide� Effective clinical problem solving
� Effective decision making, including interventions

25
The Concept of Screening
� Screening is part of the care process step of recognition� The process of identifying the RISK for, or POSSIBLE or LIKELY presence of, a condition or situation
� Examples of screening� TB screening
� Depression screening
� Fall risk screening
26
Diagnosis / Cause-and-Effect Analysis: MDS Relevance
� Diagnoses are listed
� MDS data are not diagnostic
� Supplemental Activities� Use history and physical assessment results to forumlate diagnostic hypotheses
� Use pertinent evaluations and diagnostic tests to confirm or refute diagnoses
� Use clinician support to identify relationships among diagnoses and between causes and consequences
27
Avoiding Cause-Identification “Fallacies”
� Collecting data without pertinent hypotheses� Collecting data but ignoring, misunderstanding, or misinterpreting findings
� Not collecting enough data� Not knowing significance of data� Failing to have a diagnostic strategy� Oversimplifying a diagnostic problem� Overemphasizing positive findings� Discounting negative findings
28
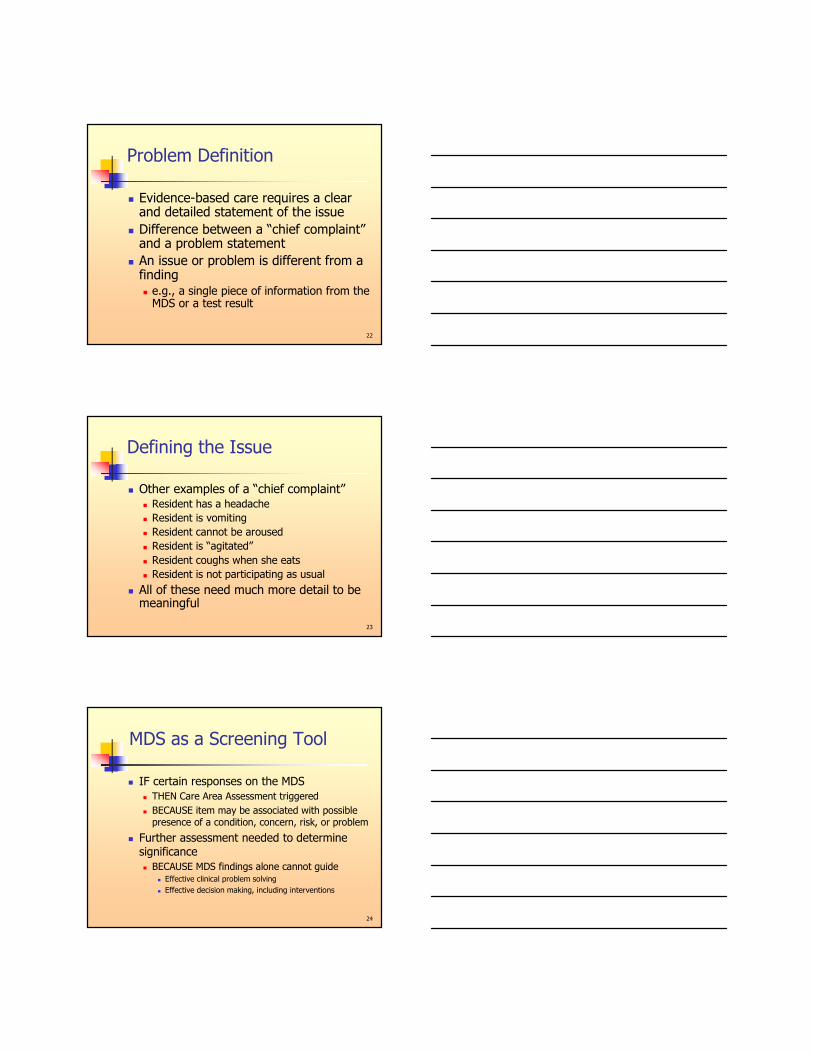
Linking Causes and Consequences
� Four essential steps1) Characterize the disabilities
2) Identify causal impairments
3) Determine specific diseases underlying identified causal impairments
4) Discover any contributing factors� Hoenig H, Nusbaum N, Brummel-Smith K. Geriatric rehabilitation: State of the Art. J Am Geriatr Soc 45:1371-1381, 1997
29
Causes and Consequences
30
31
The Three Human Dimensions
PSYCHOSOCIAL
FUNCTIONAL
PHYSICAL
32
Effective Care and the RAI
� Identify a condition that � Is common� Is under-diagnosed, undertreated � Can trigger 15 or more of the 20 Care Area Triggers (CATs) in the RAI
� Is potentially readily identifiable and treatable
� If treated, can have profound effects on function, psychosocial well being, quality of life, and even return to the community
� Is a prominent example of one cause �many consequences
33
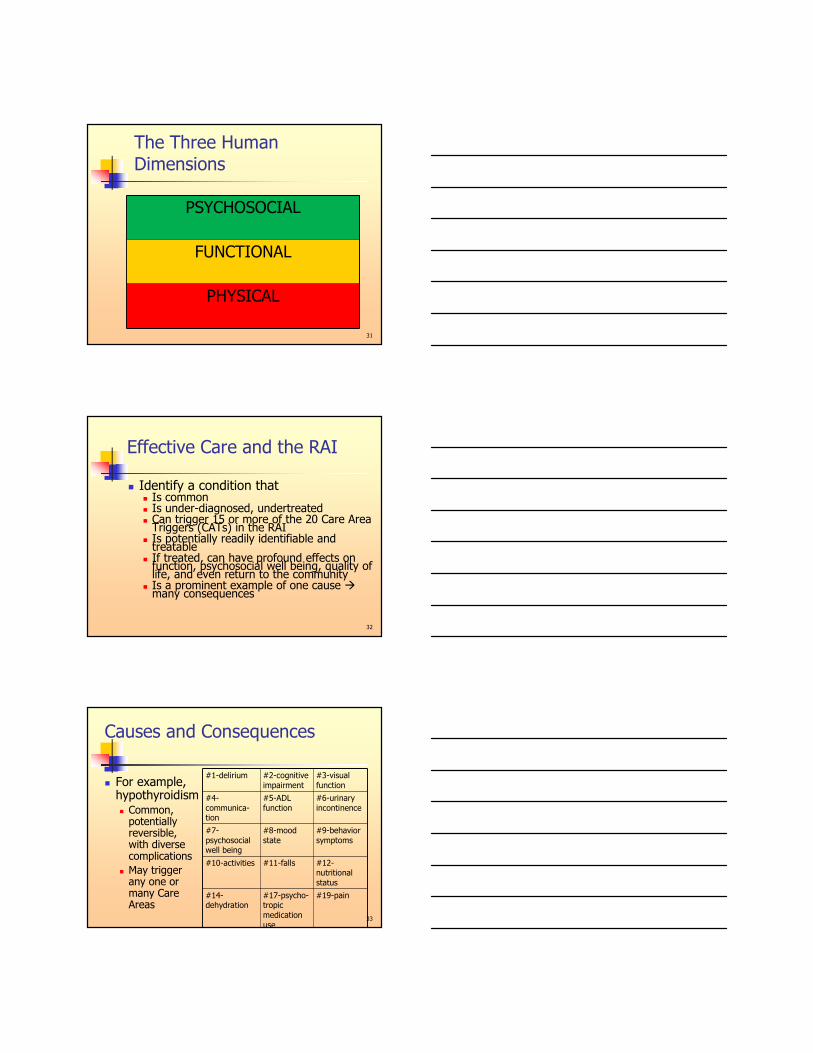
Causes and Consequences
� For example, hypothyroidism � Common, potentially reversible, with diverse complications
� May trigger any one or many Care Areas
#1-delirium #2-cognitive
impairment
#3-visual
function
#4-
communica-tion
#5-ADL
function
#6-urinary
incontinence
#7-
psychosocial well being
#8-mood
state
#9-behavior
symptoms
#10-activities #11-falls #12-nutritional
status
#14-dehydration
#17-psycho-tropic
medication
use
#19-pain

34
Evidence-Based Care
� IF a resident has triggered multiple Care Areas
� THEN it is important to consider common cause of multiple triggered areas
� AND multiple causes of a single consequence (e.g., symptom, impairment)
� BECAUSE
� Treating individual findings may not suffice
� Irrelevant interventions may be problematic
35
Causes and Consequences
Complications �
Causes
One Multiple
One + / + + / ++++
Multiple ++++ / + ++++ / ++++
36
Causes and Consequences (1:1)
� One cause � One consequence (1:1)
� No other factors involved
� Usually occurs in otherwise healthy people or those with minor chronic conditions
� Examples
� Fracture � impaired mobility until fracture heals
� Fatigue � headache for a few hours

37
Causes and Consequences (1:Multiple)
� One cause � multiple consequences� Example
� Major stroke in previously well individual �impaired mobility, self-care deficit, pain, altered nutritional status, altered mood
� Altered family processes �mood disturbance � social withdrawal and behavioral symptoms
� COPD (advanced) � activity intolerance, altered breathing patterns, impaired gas exchange, self-care deficit
� New and old impairments may interact to increase risk for additional impairments
38
Causes and Consequences (Multiple:1)
� Multiple causes � one impairment
� Example� Hydration or depression risk due to
� CVA and dementia (neurological), chronic renal failure (urinary), colitis related to antibiotic use (gastrointestinal)
� Pain due to� Parkinson’s Disease (neurological), osteoarthritis (musculoskeletal), side effects of medications used to treat hypertension or lower blood lipids
39
Causes and Consequences (Multiple:Multiple)
� Multiple causes � Multiple impairments � Very common in short-stay and long-stay nursing home population
� Example� [New stroke + diabetes + ischemic cardiovascular disease + chronic renal failure + medication side effects + mood disorder] �[impaired mobility + pain + social withdrawal + altered nutritional status + impaired fluid balance + pain + risk of altered skin integrity]

40
Causes and Consequences
� For any of the 4 key circumstances � 1:1
� 1:Multiple
� Multiple:1
� Multiple:Multiple
� Decisions to intervene are best made in the context of the whole situation� Not just in context of a single symptom or risk factor
41
Sound Care: History and Context
� What are the likely differences in cause, approach, and context if someone� Gets delirium and then gets anorexia � Gets anorexia and then gets delirium� Has a significant condition change with change in mental function and anorexia at the same time
� MDS 3 / RAI focus on “interview”� But only for several areas
� Key element of history taking applies across the board
42
Examples
� If both weight loss and delirium, then � Possible common cause (e.g., medication side effects)
� Delirium may have resulted in impaired nutritional status
� Impaired nutritional status may have led to delirium
� For example, due to fluid and electrolyte imbalance

43
Identify Goals and Objectives of Care: MDS Relevance
� Identifies preferences, interests, wishes
� Includes data to help confirm prognosis and framework for establishing goals
� Supplemental Activities
� Use clinician support to clarify prognosis
� Consider overall goals for the individual
� Identify criteria for meeting goals
44
Selecting Interventions / Provide Care: MDS Relevance
� Lists current interventions including medications and treatments
� Alone, inadequate basis for selecting interventions
� Supplemental activities� Use clinical support and results of problem definition, cause identification to identify specific symptomatic and cause-specific interventions
45
Monitor Progress: MDS Relevance
� Useful to compare findings over time, help identify discharge potential
� Supplemental activities� Identify individual’s response to interventions and treatments
� Use clinical support to identify whether interventions are still relevant, need adjustment, or are causing problems or impeding progress

46
Delirium Care Area Assessment
Linking Assessment and Care Planning
47
Care Plan Separately or Together?
� Separate care plan often not required for each finding
� BECAUSE a single trigger can have multiple causes and contributing factors AND multiple items can have a common cause or related risk factors
� THEREFORE, often appropriate to combine care plans or cross-reference related interventions
48
Combining Approach to Triggers
� Makes sense to consider together, before going off in diverse directions� 1-Delirium� 2-Cognitive loss� 4-Communication� 7-Psychosocial well being� 8-Mood state� 9-Behavioral symptoms � 17-Psychotropic medications

4949
Some Key Concepts
� Altered mental function or problematic cognition, behavior, and mood� Symptoms or syndromes (collections of signs and symptoms) needing careful evaluation and thoughtful management
� Disruptive or problematic behavior itself is not an illness or disease
� Management and care planning symptoms requires good detective work
5050
Managing Behavior and Mood Symptoms
� Many situations can be readily addressed with a careful assessment and systematic approach� Almost always time to think it through� Helps avoid (re)hospitalization
� Common (not always effective) responses� Send the patient to the ER� Call the police� Get a psychiatric consultation� Get a urine culture
51
Clinical Decision Making Process
� Follow the steps� Assessment / recognition, cause identification, management, monitoring
� Incorporate information from the MDS and other sources at each step
� Use results at each step as basis for subsequent steps
� Obtain additional information as indicated� Resist temptation to intervene blindly or prematurely� Educated hypothesis based on effective clinical problem solving and decision making, not just guess

5252
Key Step: Identify Situation
� Review recent and previous history
� MDS does not provide detailed “story”
� Observe individual in various situations
� Identify and document pertinent details
� How the individual looks, thinks, and acts
� Affect, appearance, insight, judgment, sensorium, thought content & process
5353
Identify Current Situation
� Sources of information � Current diagnoses, e.g.
� Dementia, schizophrenia, or bipolar disorder
� History of symptoms � History of behavioral symptoms / episodes
� Medications� Patient receiving psychopharmacologic medications or other medications that can affect behavior and mental function
� Especially, any “anti-” medications
54
Details Count
� Why is it important to identify behavior, mood, and mental function in detail?� That is, more specifically than “agitated,”“combative,” “confused,” “having a psych problem,” “off the wall,” etc.
� “Agitated” can mean anxious, irritable, angry, restless, aggressive, screaming, rummaging, resistant to care, disinhibited, or more
� Common practice of documenting or treating “agitation” lacks clinical validity

5555
Define Behavioral Issues: Details
� Nature and relevant factors� Onset, preceding factors or triggers
� Course� Duration and frequency, continuous or intermittent, compared to usual
� Severity� Consequences of the behavior or change in mental function, reason why individual is problematic, danger to self / others
5656
Delirium: Tools to Help Identify
� Confusion Assessment Method (CAM)� Based on consideration of 11 different issues
� Lead to answering 4 questions� Is change in mental status acute and does it fluctuate throughout the day?
� Difficulty in focusing attention? � Disorganized or incoherent speech? � Altered level of consciousness?
� Possible delirium if [1 and 2] AND [3 or 4]
5757
Delirium: Several Varieties
� Varieties� Hyperactive (approximately one-fourth)� Hypoactive (approximately one-fourth)� Fluctuating activity levels (approximately one-third)
� No change in activity levels (approximately 15 percent)
� Source: Liptzin B, Levkoff SE. An empirical study of delirium subtypes. Br J Psychiatry 1992 Dec; 161: 843-845
� May have different etiologies

5858
Cause Identification: Examples
� Medication adverse consequences
� Fluid and electrolyte imbalance
� Infections� Hypoglycemia or
marked hyperglycemia � Acute renal failure /
Acid-base imbalance� Hepatic failure� Hypo-/ hyperthyroidism
� Respiratory failure, hypoxia, CO2 retention
� Cardiac arrhythmia, MI, CHF
� Head trauma� Stroke or seizure� Pain, acute or chronic� Alcohol or drug abuse
or withdrawal� Sensory deficits� B12, folate deficiency
5959
Medication-Related Causes
� Medications are common and important causes of many psychiatric symptoms
� Drugs that may cause psychiatric symptoms. Medical Letter 2002; 44(1134):59-62
� Staff and practitioner, with consultant pharmacist’s input as needed, review current medication regimen
� Practitioner acts as needed to modify regimen
6060
Medications Affecting Mood, Behavior, Cognition
� Antiarrhythmic agents
� Anticholinergic agents + medications with anticholinergic side effects
� Antidepressants
� Anticonvulsants
� Antiemetics
� Antihistamines / decongestants
� Antihypertensive agents
� Antineoplastic agents
� Anti-Parkinsons agents
� Corticosteroids
� Muscle relaxants
� Antipsychotic medications
� Opioids
� Sedatives/sleep medications

6161
Bacteriuria and Problematic Behavior
� When does bacteriuria cause problematic behavior or altered mental function?
� Common practices� Order urine cultures for any problematic behavior, altered mental function
� Attribute problematic behavior and altered mental states to “UTI”
� Give antibiotics for positive urine culture� Regardless of whether criteria for infection met
6262
Bacteriuria and Problematic Behavior / Delirium
� UTIs not prominently associated with physical or verbal aggression in individuals with dementia
� Arch Intern Med 2006;166:1295-1300
� Interpret urinalyses and urine cultures cautiously
� Don’t confuse asymptomatic bacteriuriawith infection
6363
Bacteriuria and Problematic Behavior / Delirium
� Positive urine culture, with or without abnormal urinalysis, does not prove UTI
� Even if UTI is a possibility� Consider other causes of symptoms instead of, or in addition to urinary source
� Review current medication regimen � Consider possible fluid and electrolyte imbalance (dehydration, high or low sodium)
� Skilled clinician should interpret test results and assess the situation, as needed

64
Evidence-Based Care Planning
65
Care Plan Together or Separately?
� Evidence-based approach� Define problem / issue / concern clearly
� Figure out what is linked to what
� Develop sound hypotheses� Based on careful problem definition and cause identification
� Identify relevant interventions
� To extent possible, care plan related issues together
66
Evidence-Based Care
� Evidence-based care refers to evidence about the illness, symptom, condition, or risk AND evidence about the resident � Requires detailed and clear findings and problem statement
� Requires a “story”� Chronology of symptoms and events, not just random data / diagnoses
� Thus, a history is key to identifying causes and choosing appropriate interventions

67
Comprehensive Assessment: Key Elements
� DeGowin: Bedside Assessment (original title)
� Since 1965, a classic reference on the key elements of history taking and examination
� Content is universal, enduring, and relevant to anyone of any discipline who assesses a human being
� Source: LeBlond RF, Brown DD, DeGowin RL. DeGowin’s Diagnostic Examination. (9th ed.). New York:McGraw-Hill, 2008
68
History Taking: Key Objectives
� Taking a . . . history has four objectives:
� 1) Discovering symptoms (issues, concerns, wishes, goals, preferences)
� 2) Obtaining accurate quantitative descriptions
� 3) Securing a precise chronology of events
� 4) Determining how the illness (impairment, psychosocial concern) has changed the resident/patient’s life
69
DeGowin: History is Essential
� History: � “an account of the events in the [individual’s] life that have relevance to the patient’s physical and mental health”
� Chief purpose: to help form hypotheses regarding the process unfolding
� Take care to establish sequence of events� Task at this time
� Try to understand resident/patient’s experience and their interpretation of situation (e.g., illness, fear, concerns)

70
DeGowin: All-Important History
� Evaluation of a symptom can be straightforward� However, nonspecific symptoms require more information
� History for an apparent, uncomplicated acute problem may be brief, e.g.� Nasal congestion from a cold� Resident/patient upset, anxious, concerned about
something that just happened
� History for a more complex situation must be more detailed� Chronic disease or enduring symptoms may require long,
careful history� Updated as results open new diagnostic possibilities
7171
History is Most Important (1992)
0
1
2
3
4
5
6
7
8
9
10
After Labs
After Physical
After History
7272
History is Most Important (1975)
0
2
4
6
8
10
12
After Labs
After Physical
After History

73
Implications
� Detailed chronological history and basic physical assessment are essential� Especially, in those with complex acute or chronic disease or multiple causes and consequences
� Otherwise, little more than guesswork
� History and exam help with thinking about situation and its causes� Testing and consultation often less helpful
74
History: The Chief Complaint
� DeGowin: Chief complaint is only general statement of primary issue or concern from the patient’s perspective� Start history with the chief complaint (CC)
� Starting point for cause identification
� Details of symptoms critical� For more complex story and broad diagnostic possibilities, more details essential
� “You cannot be certain what is pertinent and what superfluous.”
� Additional details often essential before care planning interventions
75
Implications
� MDS data often at level of a chief complaint or isolated finding� Missing important detail / lacks a chronological story
� Common practice: treat/care plan chief complaint � May result in inadequate or problematic care
� Important to avoid premature interpretation� Such as failing to record seemingly irrelevant symptoms or events
� May be problematic to assume the conclusion and thereby fail to seek additional information
� e.g., behavior due to UTI, depression, or comfort needs

76
DeGowin: Signs and Symptoms
� “Insist that the patients [residents] describe their symptoms.”
� “Do not accept diagnoses or medical jargon as a substitute.”
� “When the symptoms suggest several conditions, note the absence of concomitant symptoms, ascertained by direct questioning, whose presence would favor one or another of the possibilities (pertinent negatives).”
77
Seeing, Hearing, and Believing
� Common widespread advice � “Believe whatever the resident tells you.”
� “Accept whatever the resident tells you about pain”
� However, that can easily be misunderstood or misrepresented � It does not mean
� Don’t question; don’t challenge
� Just take whatever you are told and act on it
� Don’t try to confirm by examining the individual
78
Beyond Forms and Checklists
� In order to use the information from the RAI effectively, we need to go beyond the forms and checklists
� What?
� So What?
� Now What?
Rolfe et al (2001)
Framework for reflective practice
79
Beyond Forms and Checklists
� What?
� The essential message
� Based on observation about a situation that needs to be addressed
Rolfe et al (2001)
Framework for reflective practice
80
Beyond Forms and Checklists
� So What?
� What makes this important?
� What is at stake if we don’t address it?
� Resident needs, desires, goals, and wishes
81
Beyond Forms and Checklists
� Now What?
� Going forward statements
� Intevention choices – effective choices that we (inclusive of residents, family, interdiciplinary team, etc.) feel will result in the best outcome

82
Beyond Forms and Checklists
� Requirements
� Current, evidence-based, expert endorsed
� Facility must be able to identify resources upon request
� F492 – Services must meet professional standards of quality
� Checklists are provided as a resource they are NOT mandated
83
Part 5: Nutrition Care Area Assessment
Using MDS Information Effectively
84
Weight Change and Anorexia
� Weight change and anorexia are symptoms, not diseases
� Diverse causes
� Common emphasis: percent / time frame
� 5% in 1 month
� 7.5% in 3 months
� 10% in 6 months

85
Weight Loss Patterns:Vital to Know
135140145150155
Dec
Jan
Feb
Mar
Weight130
140
150
160
Dec
Jan
Feb
Mar
Weight
130
140
150
160
Dec
Jan
Feb
Mar
Weight
130
140
150
160
Dec
Jan
Feb
Mar
Weight
86
History: Details Matter
� What is the story (chronology)?� What was the rate, and over what period?
� What was the pattern of weight loss?� Gradual, progressive� Abrupt, then continuing� Gradual or abrupt, then stabilized
� Was there anything that the individual ate most or all of, most of the time?
� Questions essential to identifying causes � Using weight loss percentages only => guesswork
87
Things Happen in a Sequence
� Symptoms (including those related to medications) often part of a cascade of problems
� Pneumonia � confusion � decreased intake � lethargy
� Medication � lethargy � decreased oral intake �fluid/electrolyte imbalance �further lethargy � weight loss �skin breakdown

88
Nutrition Approaches: Options
� Weigh properly and consistently; verify accuracy
� Define the weight or nutrition-related problem appropriately
� Characterize nutritional issue correctly before acting
� Identify presence of anorexia� Recognize predisposing factors� Identify medical causes of anorexia and weight loss (via differential diagnosis)
89
Nutrition Approaches: Options
� Establish realistic goals� Reconcile simultaneous or conflicting goals � Use lab testing judiciously� Limit therapeutic / modified consistency diets� Assess food preferences and eating patterns� Make the food palatable� Improve dining environment� Use tube feeding sparingly
� After seeking modifiable causes, resident preferences
90
Appetite “Stimulation”
� Not indicated to substitute for detailed investigation and cause identification
� Rarely helpful� Not a first line symptomatic treatment� Antidepressants are not reliable or consistent “appetite stimulants”
� Example: Remeron has < 15% prevalence of weight gain, and significant side effects
� Medications often introduce risks / hazardous� Often don’t address underlying causes

91
Remainder of RAI
� CAAs and Utilization Guidelines start to direct thinking about � Areas for possible additional concern and investigation
� Whether findings represent a problem or risk requiring further intervention
� Causes and risk factors related to triggered care area
� Formulating a care plan� Partial—not total—foundation
92
Care Area Assessments
� Identified by responses to items on the MDS
� Care Area Assessments replace RAPs
� e.g., delirium, urinary incontinence, pain, falls
� CAAs reflect conditions, symptoms, and other areas of possible concern, pending review
� Need further assessment before proceeding to care planning
� Supplement MDS data with additional information
93
Care Area Assessments and Beyond
� RAI manual not intended to address
� How to analyze triggers in depth
� How to select pertinent interventions as a basis for care plan development
� No specific tool mandated to subsequently assess triggered areas
� No specific guidance on how to understand or interpret triggered areas

94
Summary
� MDS 3.0 is a great opportunity to rethink:
� Meaning and implications of “assessment”
� Use and limitations of the tools
� How RAI fits in context of the entire clinical problem solving and decision making process
� Critical steps to use RAI components to develop individualized care planning and subsequent care
95
Summary: Decision Making / Documentation
� Formulate clear picture of the resident/patient
� Resident/patient-centered care plan � Based on conclusions from the full clinical problem solving and decision making process AND
� Resident preferences, personal goals
� Document basis for conclusions� Not just conclusions
96
Summary: IDT Responsibility
� Facility’s IDT, including physicians, must identify causes and connect causes and consequences� BECAUSE it is essential to resident-centered care and the MDS and CAAs not designed to do so
� Qualified, interested, and capable practitioners are needed to� Identify multiple causes of a single problem or multiple problems or complications related to one or more underlying causes
� Identify appropriate generic and cause-specific interventions











![WELCOME [eo2.commpartners.com]eo2.commpartners.com/users/bu/downloads/150527_Handout.pdf · 5/26/2015 3 MORAL INJURY The lasting psychological, biological, spiritual, behavioral,](https://img.pdfslide.us/doc/110x75/5aebc38e7f8b9a45568d8363/welcome-eo2-eo2-3-moral-injury-the-lasting-psychological-biological-spiritual.jpg)

















