Embed Size (px)
Citation preview

Cardiovascular Risk Assessment
UBC Pharmacy Update 2016 Copyright Arden Barry PharmD 1
5 March 2016
Cardiovascular Risk Assessment:Determining Ticking Time Bomb Tickers
Arden Barry, BSc, BSc(Pharm), PharmD, ACPRClinical Pharmacy and Research Specialist, Chilliwack General Hospital
Assistant Professor (Partner), Faculty of Pharmaceutical SciencesAssociate Member, Department of Family Medicine, Faculty of Medicine
University of British ColumbiaEmail [email protected]
Twitter @ArdenBarry
Disclosure
• No real or potential conflicts of interest to declare
• Primary panel member of the 2015 update of the Canadian Cardiovascular Society guidelines for the diagnosis and treatment of dyslipidemia for the prevention of cardiovascular disease in the adult
Objectives
• To identify which patients should undergo a CV risk assessment;
• To gain familiarity with the available CV risk assessment calculators, and identity at least one advantage and disadvantage of each;
• To be able to calculate a patient’s CV risk using the Framingham Risk Score;
• To briefly review the current Canadian treatment recommendations based on a patient’s CV risk score.
Guidelines
Can J Cardiol 2013;29:151-67
Guidelines
Can Pharm J (Ott) 2015;148:21-8
Guidelines
Can Fam Physician 2015;61:857-67

Cardiovascular Risk Assessment
UBC Pharmacy Update 2016 Copyright Arden Barry PharmD 2
5 March 2016
Guidelines
Circulation 2014;129[suppl 2]:S1-S45
CV Risk Assessment
Why?
• Most patients are asymptomatic
• Objective measure of risk
• Reassure low-risk patients
• Identify modifiable CV risk factors
• Encourage healthy lifestyle behaviours
• Motivate patients
Screening
Can J Cardiol 2013;29:151-67
• Secondary prevention (established CVD such as CAD, ACS, CABG surgery, cerebrovascular disease, stroke/TIA, PAD, abdominal aortic aneurysm)
• DM (age ≥40 or age ≥30 with DM duration ≥15 yr or microvascular disease)
• CKD (eGFR ≤45 or ACR ≥30 or eGFR ≤60 and ACR ≥3)
• HTN with ≥3 CV risk factors (age >55, smoker, TC/HDL-C ratio >6, LVH, family history of premature CVD, ECG abnormalities, microalbuminuria)
Is the Patient Already High Risk?
Can J Cardiol 2013;29:151-67

Cardiovascular Risk Assessment
UBC Pharmacy Update 2016 Copyright Arden Barry PharmD 3
5 March 2016
Risk Calculators
Fasting Lipid Profile
• Fasting x ≥10 hr
• Components:– Total cholesterol (TC) (mmol/L)
– High-density lipoprotein cholesterol (HDL-C) (mmol/L)
– Low-density lipoprotein cholesterol (LDL-C) (mmol/L)
– Triglycerides (TG) (mmol/L)
– Non-HDL-C (mmol/L)
– TC/HDL-C ratio
• Alternate: apolipoprotein B (apoB) (g/L)
Calculating CV Risk
• ++ CV risk tools exist
• ++ variance between tools
• No tool is 100% accurate
• Arbitrary thresholds for risk
• Not intended for patients on treatment
• Not intended to estimate effect of treatment
CV Risk Calculators
• Framingham Risk Score
• QRISK2
• ACC/AHA ASCVD Calculator
• Reynolds Risk Score
• CardioRisk Calculator
Framingham Risk Score
• Estimates 10-year risk of total cardiovascular disease (CVD) = CAD, stroke, PAD and HF
• Reported as %
Circulation 2008;117:743-53
Framingham Risk Score
• Components:
– Sex (M or F)
–Age (yr)
– TC (mmol/L)
–HDL-C (mmol/L)
– SBP (mmHg)
–DM (Y or N)
– Smoker (Y or N)
Circulation 2008;117:743-53

Cardiovascular Risk Assessment
UBC Pharmacy Update 2016 Copyright Arden Barry PharmD 4
5 March 2016
Framingham Risk Score
• Limitations:
–Middle-aged white American population
–Not validated in patients >75 years of age
–Calculates total CVD
– Limited to 10-year risk
– Family history (“modified FRS”)
QRISK2
• Calculates 10-yr % risk of CVD
– MI, angina, stroke, TIA
• Components:
– Sex (M or F) and age (yr)
– Ethnicity
– DM, AF, CKD or RA (Y or N)
– Family history of CVD (first-degree relative <60)
– TC/HDL-C ratio, SBP (mmHg) and BMI (kg/m2)
– Smoker (Y or N)
qrisk.orgBMJ 2010;340:c2442
QRISK2
qrisk.orgBMJ 2010;340:c2442
QRISK2
• Limitations:
–Middle-aged United Kingdom population
– Limited to age 35-73 yr
–Calculates total CVD
• Angina or TIA vs MI or stroke
– Limited to 10-year risk
–Does not account for family history
– Less patient-friendly to complete
ACC/AHA ASCVD Risk Estimator
• Based on American community-based cohort of African-American and non-Hispanic white men/women aged 40-79
• Calculates 10-year % risk of fatal/nonfatal MI and fatal/nonfatal stroke
• Also calculates lifetime % risk for those aged 20-59 years
tools.acc.org/ASCVD-Risk-EstimatorCirculation 2014;129:S49-S73
ACC/AHA ASCVD Risk Estimator
• Components:– Age (20-79 yr)
– Sex (M or F)
– Race (AA, WH or other)
– TC (mg/dL)
– HDL-C (mg/dL)
– SBP (mmHg)
– DM (Y or N)
– Smoker (Y or N)
tools.acc.org/ASCVD-Risk-EstimatorCirculation 2014;129:S49-S73

Cardiovascular Risk Assessment
UBC Pharmacy Update 2016 Copyright Arden Barry PharmD 5
5 March 2016
ACC/AHA ASCVD Risk Estimator
tools.acc.org/ASCVD-Risk-Estimator
ACC/AHA ASCVD Risk Estimator
• Limitations:
–Middle-aged American population
–Patients >79 yr of age not included
–Only calculates MI and stroke
–10-year risk may exceed lifetime risk
–Does not account for family history
– Less clinical experience
–American units and guidelines
http://bestsciencemedicine.com/chd/calc2.html http://cvrisk.mvm.ed.ac.uk/calculator/calc.asp
Reynolds Risk Score
• Calculates 10-year % risk of CV death, MI, stroke or coronary revascularization
• Components:– Sex (M or F) and age (yr)
– Smoker (Y or N)
– SBP (mmHg)
– TC and HDL (mg/dL or mmol/L)
– hsCRP (mg/L)
– Family history (parent with MI <60 years of age)reynoldsriskscore.org
JAMA 2007;297:611-9Circulation 2008;118:2243-51
Reynolds Risk Score
reynoldsriskscore.org

Cardiovascular Risk Assessment
UBC Pharmacy Update 2016 Copyright Arden Barry PharmD 6
5 March 2016
Reynolds Risk Score
• Limitations:
–Middle-aged white American population
–Utilizes hsCRP (not CRP)
–Coronary revascularization vs CV death/MI/stroke
– Excludes DM
–Maximum age 80 yr
CardioRisk Calculator
www.circl.ubc.ca/webcardiorisk.html
Metabolic Syndrome
• No uniform classification system
• Higher risk than individual risk factors alone?
• Do not use metabolic syndrome for CV risk assessment
Diabetes Care 2005;28:2289-304
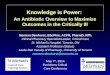
Framingham Risk Score
Framingham Risk Score

Cardiovascular Risk Assessment
UBC Pharmacy Update 2016 Copyright Arden Barry PharmD 7
5 March 2016
• Step 1: calculate total points
• Step 2: use points to determine risk %
• Step 3: modify for family history of premature CVD
• Step 4: use points to determine “heart age”
• Step 5: use risk % to determine risk level
Framingham Risk Score
Low risk Intermediate risk High risk
<10% 10-19% ≥20%
Case Example
Case: B.S.
• 66 yo M with a hungry heart
• PMHx: Ø
• SocHx: non-smoker, Ø EtOH, vegetarian
• Rx: Ø
• Would you screen this patient?
• Why or why not?
Case: B.S.
• Based on your recommendation, he has a fasting lipid profile drawn:
• BP 135/80 mmHg
• Non-diabetic
TC LDL-C HDL-C TG
5.6 mmol/L 3.9 mmol/L 1.25 mmol/L 1.0 mmol/L
Case: B.S.
• Is he primary or secondary prevention?
• What additional information do you require?
• What is his FRS?
–Points =
–10-year CVD risk =
• Heart age =
• Risk level =
• What if he was 56-years-old?
• What if he was 64-years-old?
• What if he was a 66-year-old female?
• What if he was a 76-year-old female?
Case: B.S.

Cardiovascular Risk Assessment
UBC Pharmacy Update 2016 Copyright Arden Barry PharmD 8
5 March 2016
Practical Tips
• What is the biggest contributor to risk?
• Access to labs via my ehealth
• Ex-smokers
• Positive family history of premature CVD
• Communicating risk
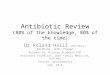
Case: B.S.
FRS 25.3%
CardioRisk 22%
QRISK2 16.3%
ASCVD 16.1%
RRS 13%
The Absolute CVD Risk/Benefit Calculator
FRS 23.5%QRISK 15.4%ASCVD 14.6%
Treatment
• Recommend for all patients at risk of CVD
• Health behaviours:
– Smoking cessation
– Exercise (150 min per week)
– Limit EtOH intake (1-2 drinks per day)
– Dietary modifications
– Psychological stress management
Lifestyle Modifications
0-5-30
Can J Cardiol 2013;29:151-67
Dyslipidemia
Can J Cardiol 2013;29:151-67
Dyslipidemia
Can J Cardiol 2013;29:151-67

Cardiovascular Risk Assessment
UBC Pharmacy Update 2016 Copyright Arden Barry PharmD 9
5 March 2016
Statin Myth-Busting
www.albertahealthservices.ca/scns/page10585.aspx
Hypertension
Can J Cardiol 2015;31:549-68
Hypertension
Can J Cardiol 2015;31:549-68
ASA
Can J Cardiol 2011;27:208-21
Case Examples
Case 1
ID 45-year-old F
PMHx Ø
MedHx Salmon oil 1000 mg PO daily, ECASA 81 mg PO daily
SocHx Ex-smoker, Ø EtOH
FamHx Father had MI at age 45
BP 122/66 mmHg
Labs TC 8.0 mmol/LLDL-C 5.7 mmol/LHDL-C 1.9 mmol/LTG 1.0 mmol/LFBG 5.6 mmol/L

Cardiovascular Risk Assessment
UBC Pharmacy Update 2016 Copyright Arden Barry PharmD 10
5 March 2016
Case 2ID 50-year-old F
PMHx DM type 2, dyslipidemia, hypothyroidism
MedHx Metformin 500 mg PO bid, ramipril 5 mg PO daily, levothyroxine 112 mcg PO daily
SocHx Non-smoker, Ø EtOH
FamHx Non-contributory
BP 128/73 mmHg
Labs TC 5.7 mmol/LLDL-C 3.7 mmol/LHDL-C 1.0 mmol/LTG 2.3 mmol/LA1c 8.6%
Case 3
ID 29-year-old M of Indian descent
PMHx Ø
MedHx Ø
SocHx Smoker (1 ppd x 15 yr)
FamHx Father has DM type 2 (Ø CVD)
BP 134/82 mmHg
Labs TC 6.2 mmol/LLDL-C 4.3 mmol/LHDL-C 1.2 mmol/LTG 1.5 mmol/LFBG 6.2 mmol/L
Case 4ID 56-year-old M
PMHx HTN, dyslipidemia, chronic back pain
MedHx Ramipril 10 mg PO bid, amlodipine 10 mg PO daily, atorvastatin 10 mg PO daily, naproxen 500 mg PO bid
SocHx Smoker (40 pack-yr hx)
FamHx Unknown
BP 118/65 mmHg
Labs TC 3.2 mmol/LLDL-C 1.9 mmol/LHDL-C 0.8 mmol/LTG 1.0 mmol/LA1c 6.5%
Case 5ID 71-year-old F
PMHx DM type 2
MedHx Metformin 500 mg PO bid
SocHx Non-smoker
FamHx Non-contributory
BP 124/83 mmHg
Labs TC 4.5 mmol/LLDL-C 1.7 mmol/LHDL-C 2.1 mmol/LTG 1.4 mmol/LA1c 6.8%
Case 6
ID 35-year-old M from Fort McMurray
PMHx Obesity (BMI 33 kg/m2)
MedHx Ø
SocHx Smoker (½ ppd x 25 yr), occasional cocaine use
FamHx Non-contributory
BP 148/90 mmHg
Labs TC 6.8 mmol/LLDL-C unable to measureHDL-C 0.8 mmol/LTG 5.5 mmol/LA1c 9.6%
Case 7ID 92-year-old F
PMHx AF, OA, HTN, osteoporosis
MedHx Alendronate 70 mg PO q weekly, warfarin 5 mg PO daily, bisoprolol 5 mg PO daily, acetaminophen 1000 mg PO tid, calcium 500 mg PO bid, vitamin D 1000 units PO daily
SocHx Ex-smoker (quit in 1956)
FamHx Non-contributory
BP 110/70 mmHg
Labs TC 4.3 mmol/LLDL-C 2.1 mmol/LHDL-C 1.8 mmol/LTG 0.8 mmol/L

Cardiovascular Risk Assessment
UBC Pharmacy Update 2016 Copyright Arden Barry PharmD 11
5 March 2016
Case 8ID 65-year-old M
PMHx CAD (STEMI 6 months ago), HTN, dyslipidemia
MedHx ECASA 81 mg PO daily, ticagrelor 90 mg PO bid, rosuvastatin 40 mg PO daily, bisoprolol 5 mg PO daily, perindopril 4 mg PO daily
SocHx Ex-smoker (quit 6 months ago)
FamHx Non-contributory
BP 112/72 mmHg
Labs TC 3.4 mmol/LLDL-C 2.3 mmol/LHDL-C 0.7 mmol/LTG 0.8 mmol/L
Questions?