Embed Size (px)
Citation preview
E-Cigarettes: Smoking Cessation Tool, or Public Health
Nightmare?Andy Peterson, MD, MPH
PGY-3Department of Family and Community Medicine
University of Missouri
Objectives
• 1. Discuss the history and current status of FDA regulations on e-cigarettes in the United States• 2. Understand the health effects of e-cigarettes• 3. Increase knowledge on current patterns and use of electronic
cigarettes in the United States• 4. Learn more about e-cigarettes possible role as a method of nicotine
replacement and as a smoking cessation tool• 5. Improve interactions with patients about e-cigarette use
Public Health Consequences of E-Cigarettes(10)
• Published by the National Academies of Science, Engineering, and Medicine (NASEM) in January 2018• Contracted by the FDA to gather current information on and provide a
consensus report on multiple topics surrounding E-cigarettes, their use, their public and individual health effects, and their role as a smoking cessation tool• You will see their summary statements throughout this presentation
E-Cigarettes – What are they(11)?
• Electronic Nicotine Delivery System (ENDS)• Battery operated, designed to
vaporize a liquid solution of propylene glycol and/or vegetable glycerin in which nicotine/aromas are dissolved (e-juice)• E-Juice can have varying amounts
of nicotine• Inhaling activates battery operated
heating element to vaporize liquid solution to then be inhaled
Ingredients(8)
• Nicotine – varies depending on concentration in e-liquid, puffing intensity, device• E-Juice vapors• Fewer ingredients than combustible cigarettes• Amounts and number of ingredients can vary from product to product• Propylene glycol
• FDA allows its use in food products, medication solvent• Vegetable glycerin• Food grade flavorings• Other carcinogenic compounds found in cigarettes, but at much lower levels
than found in conventional cigarettes• Exposure can depend on puffing intensity
NASEM Conclusion(10)
• After summarizing findings from multiple studies that evaluated and compared air quality, they reported “conclusive evidence that completely substituting e-cigarettes for combustible tobacco cigarettes reduces users’ exposure to numerous toxicants and carcinogens present in combustible tobacco cigarettes.”• There is substantial evidence that completely switching from regular
use of combustible tobacco cigarettes to e-cigarettes results in reduced short-term adverse health outcomes in several organs
However…
• Substantial evidence that some chemicals present in e-cigarette aerosols…supports the biological plausibility that long term exposure…could increase risk of cancer and adverse reproductive outcomes. Whether or not the levels of exposure are high enough to contribute to human carcinogenesis remains to be determined
Other Dangers (3)
• Skin exposure and ingesting
• E-cigarette/e-juice exposure calls across the US to Poison Control Centers
increased from 1 per month in September 2010 to 215 per month in February
2014
• E-cigarette exposure calls were mostly among persons aged 0-5 (51.1% and
>20 years (42.0%).
• Ingestions (68.9%), inhalations (16.8%), eye exposures (8.5%), and skin
exposures (5.9%)
• Deaths reported as result of ingestion, injection
• Machine malfunction
NASEM Conclusion(10)
• There is conclusive evidence that e-cigarette devices can explode and cause burns and projectile injuries• There is conclusive evidence that intentional or accidental exposure
to e-liquids (from drinking, eye contact, or dermal contact) can result in adverse health effects• There is conclusive evidence that intentionally or unintentionally
drinking or injecting e-liquids can be fatal
Public Health Impact(8)
• Second hand smoke exposure• Passive exposure does produce small increases in serum cotinine• Considered to be less toxic to bystanders than traditional cigarettes
• Renormalization of smoking• Concerns that the public health gains by controlling cigarette smoking in past
years will be lost if e-cigarettes continue to gain popularity• Smoking becoming “cool” again
NASEM Conclusion(10)
• There is conclusive evidence that e-cigarette use increases airborne concentrations of particulate matter and nicotine in indoor environments compared with background levels• There is moderate evidence that secondhand exposure to nicotine
and particulates is lower from e-cigarettes compared with combustible tobacco cigarettes
U.S. Timeline
• 2007 – hit the market in the U.S – “cigalikes”• Convenience stores• Independent companies• GreenSmoke was another popular
independent company
U.S Timeline Continued
• 2008 – Vape Shops• Usually locally owned• Sell refillable/rechargeable e-
cigarettes• Sell e-Juice in different flavors and
concentrations of nicotine• Independent companies, labs• No special licensing necessary, no
regulation - unsure of where they get product or what is in it• Estimated 35,000 in U.S. in 2014(4)
U.S Timeline Continued
• 2012 – Big tobacco wants in• Lorillard purchases Blu eCigs in
2012 for 135 million• 2014 – NuMark (part of Altria
Group, parent group of Phillip Morris) purchased GreenSmoke
Non-Tobacco Product - Marketing Marketing
Look Familiar??? Big Tobacco Involved, How Do Independent Companies Compete?• Flavors
Big Tobacco Involved, How Do Independent Companies Compete?• Modifications
And they seemed to be winning…
• 2014 – big tobacco sales of e-cigarettes is declining while population report of e-cigarette use increasing• Independent company/vape shop sales not tracked formally
• Report in 2015 stated that “tobacco giants such as RJ Reynolds and Altria have petitioned to treat small vape shops as manufacturers(4).”• This would lead to inspections/regulations for small independent companies
Upward trend of Use in Recent Years (8)
• Between 2010 and 2013, ever use of e-cigarettes increased from 3.3% to 8.5% of all adults• Current use (use in last 30 days) increased from 1.3% to 1.9%
Prevalence and Use – Adults (12)
• 2014 National Health Interview Survey• 12.6 % of adults had ever used e-cigarette
• 3.7% current users (once in last 30 days)• 1.1% were daily users
• Highest prevalence of e-cigarette use was in current cigarette smokers (16%) and former smokers who had quit in the past year (22%)
• Users tend to be:• Younger• More educated• Have higher incomes
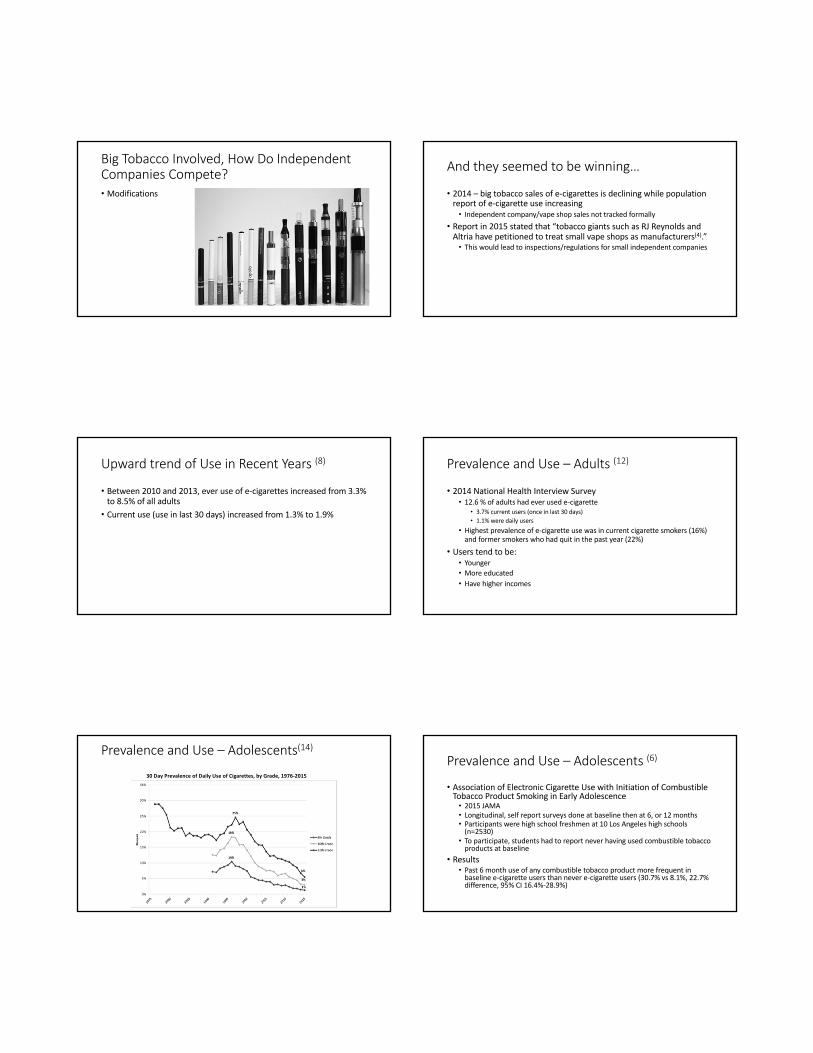
Prevalence and Use – Adolescents(14)
30 Day Prevalence of Daily Use of Cigarettes, by Grade, 1976-2015
Prevalence and Use – Adolescents (6)
• Association of Electronic Cigarette Use with Initiation of Combustible Tobacco Product Smoking in Early Adolescence• 2015 JAMA
• Longitudinal, self report surveys done at baseline then at 6, or 12 months• Participants were high school freshmen at 10 Los Angeles high schools
(n=2530)
• To participate, students had to report never having used combustible tobacco products at baseline
• Results• Past 6 month use of any combustible tobacco product more frequent in
baseline e-cigarette users than never e-cigarette users (30.7% vs 8.1%, 22.7% difference, 95% CI 16.4%-28.9%)
Prevalence and Use – Adolescents (14)
• Percent of high school seniors who had used an e-cigarette in the past 30 days increased from 1.5 percent in 2010 to 13 percent in 2017• Biggest jump from 2013-2014 where the use of e-cigarettes tripled• Teens are now more likely to use e-cigarettes than conventional
cigarettes
NASEM Conclusion(10)
• There is substantial evidence that e-cigarette use increases risk of ever using combustible tobacco cigarettes among youth and young adults• Among youth and young adult e-cigarette users who ever use
combustible tobacco cigarettes, there is moderate evidence that e-cigarette use increases the frequency and intensity of subsequent combustible tobacco cigarette smoking
U.S Timeline Continued
• May 2016 – “Deeming Rule” - FDA used Family Smoking Prevention and Tobacco Control Act of 2009 to deem e-cigarette devices/e-liquids to be tobacco products and therefore under FDA authority• Prohibit sales to those <18, vending machine sales in adult-only venues, no
free samples
• Nicotine warning on packaging, health risks on packaging
• Manufacturers/retailers required to register with FDA and be compliant with regulations set forth by the FDA within two years, August 2018 and meet the FDA standards• Expensive, exhaustive process• Only big tobacco likely to be able to afford
E-cigarette Use and Associated Changes in Population Smoking Cessation: Evidence from US Current Population Surveys (13)
• BMJ July 2017**• Objective: to examine whether increase in use of e-cigarettes in US,
which became noticeable in 2010 and increased dramatically by 2014, was associated with a change in overall smoking cessation rate at the population level• Compared 2014-15 US Current Population Survey-Tobacco Use
Supplement (surveys smokers and quitters) to multiple other years’ CPS-TUS
What Did They Find?
• E-cigarette users were more likely than non-users to attempt to quit smoking combustible cigarettes (65.1% v 40.1%, 25% change, 95% CI 23.2-26.9%, P<.001), and more likely to succeed in quitting combustible cigarettes (8.2% vs 4.8%, 3.5% difference, 95%CI 2.5-4.5% P<.001)
• The overall cessation rate for 2014-15 was significantly higher than that for 2010-11 (5.6% v 4.5% - 1.1% difference, 95% CI 0.6-1.5%, P<.001)
• Would equate to approximately 350,000 fewer US adult smokers
• The increase in e-cigarette use was associated with a statistically significant increase in the smoking cessation rate at the population level when compared to all previous years cessation rates
Updated FDA Regulations
• July 2017 – FDA extended deadline to submit application and substantial equivalence report for manufacturers/retailers to August 2022• Allow more time for “public comment and industry guidance(4).”• Aims to “develop an appropriate balance between regulation and
encouraging development of innovative tobacco products that may be less dangerous than cigarettes(4).”• A “key piece of the FDA’s approach is demonstrating a greater awareness that
nicotine, while highly addictive, is delivered through products that represent a continuum of risk and is most harmful when delivered through smoke particles in combustible cigarettes(4).”
Are e-Cigarettes a Smoking Cessation Tool?
Have there been studies to look at the effectiveness of e-cigarettes to help individuals quit smoking traditional, combustible cigarettes?
First, let’s review what is traditionally used…
Comparative Effectiveness of 5 Smoking Cessation Pharmacotherapies in Primary Care Clinics(9)
• 2009, Archives of Internal Medicine• Inclusion criteria – 18+, average 10 cigarettes per day for at least 6 months,
motivated to quit• Six month abstinence rates
• Bupropion SR 16.8%• Lozenge 19.9%• Patch 17.7%• Patch + lozenge 26.9%• Bupropion + lozenge 29.9%
• Counseling available – initial session, and up to 4 extra; could call anytime as well• <90 minutes of counseling quit rate of 19.6%, >90 minutes of counseling quit rate of 35.8%
• Self reported numbers (no confirmatory exhaled CO)
Smoking Cessation with Varenicline, a Selective alpha4-beta2 nicotinic receptor partial agonist: results from a 7-week, randomized, placebo-and bupropion- controlled trial with 1-year follow-up (7)
• 2006, Archives of Internal Medicine; Randomized, double blinded, active control (bupropion)
• Subjects 18-65, required to have smoked an average of 10 cigarettes/day during the previous year, motivated to quit
• Quit rates at 1 year• 14.4% for varenicline• 6.3% for bupropion• 4.9% for placebo• All confirmed by exhaled CO
• Counseling sessions part of intervention (7-10 sessions)
More info on Varenicline
https://www.aafp.org/afp/2017/0901/od1.html
EffiCiency and safety of an eLectronic cigAreTte(ECLAT): A Prospective 12-Month Randomized Control Design Study (2)• Italy, published in 2013, double blind, randomized• 300 smokers – inclusion criteria >10 cigs/day for at least 5 years, 18-70, good general
health, and not currently attempting to quit or wishing to do so in the next 30 days (and no emphasis on or encouragement/motivation/reward for quitting)
• They were informed that the product used was a “healthier alternative to tobacco smoke, and that it could be freely used as a tobacco cigarette substitute, as much as they liked”
• Three groups: • Group A: 7.2 mg nicotine cartridges for 12 weeks (n=100)• Group B: 7.2 mg nicotine cartridges for 6 weeks, then 5.4 mg nicotine cartridges for 6 weeks
(n=100)• Group C: 0.0 mg nicotine cartridges for 12 weeks (n=100)
• Told to use as they like – Primary outcome of cigarette reduction, abstinence, and safety of e-cigs
Results of ECLAT (confirmed by exhaled CO)
• 1 Year – Abstinence in Group A+B was 22/200 (11%), Group C was 4/100 (4%)• Of quitters, 7/26 (27%) were still using e-cigs at 52 weeks • Somewhere between 7.5% and 9.5% is the percentage of intervention group
subjects who were not smoking any nicotine product at 1 year• Those who abstained completely from tobacco from the beginning of
study were more likely to stay quit than dual users• No counseling available
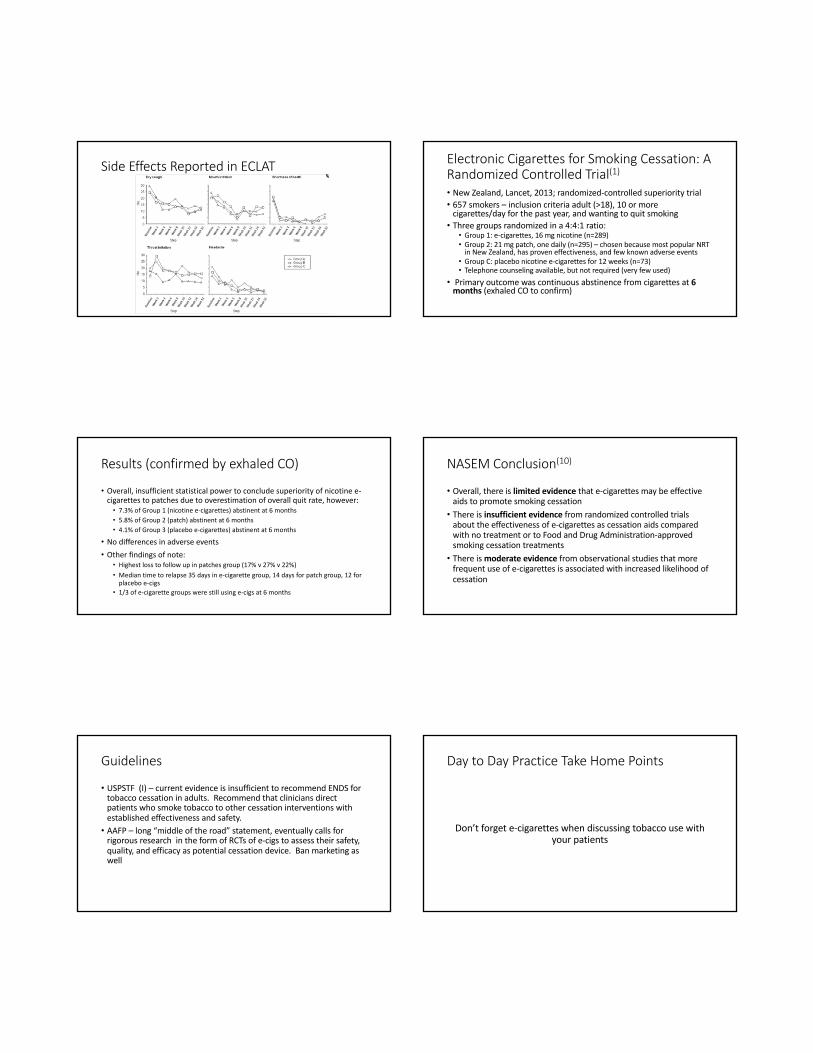
Side Effects Reported in ECLAT Electronic Cigarettes for Smoking Cessation: A Randomized Controlled Trial(1)
• New Zealand, Lancet, 2013; randomized-controlled superiority trial• 657 smokers – inclusion criteria adult (>18), 10 or more
cigarettes/day for the past year, and wanting to quit smoking• Three groups randomized in a 4:4:1 ratio: • Group 1: e-cigarettes, 16 mg nicotine (n=289)• Group 2: 21 mg patch, one daily (n=295) – chosen because most popular NRT
in New Zealand, has proven effectiveness, and few known adverse events• Group C: placebo nicotine e-cigarettes for 12 weeks (n=73)• Telephone counseling available, but not required (very few used)
• Primary outcome was continuous abstinence from cigarettes at 6 months (exhaled CO to confirm)
Results (confirmed by exhaled CO)
• Overall, insufficient statistical power to conclude superiority of nicotine e-cigarettes to patches due to overestimation of overall quit rate, however:• 7.3% of Group 1 (nicotine e-cigarettes) abstinent at 6 months• 5.8% of Group 2 (patch) abstinent at 6 months• 4.1% of Group 3 (placebo e-cigarettes) abstinent at 6 months
• No differences in adverse events• Other findings of note:
• Highest loss to follow up in patches group (17% v 27% v 22%) • Median time to relapse 35 days in e-cigarette group, 14 days for patch group, 12 for
placebo e-cigs• 1/3 of e-cigarette groups were still using e-cigs at 6 months
NASEM Conclusion(10)
• Overall, there is limited evidence that e-cigarettes may be effective aids to promote smoking cessation• There is insufficient evidence from randomized controlled trials
about the effectiveness of e-cigarettes as cessation aids compared with no treatment or to Food and Drug Administration-approved smoking cessation treatments• There is moderate evidence from observational studies that more
frequent use of e-cigarettes is associated with increased likelihood of cessation
Guidelines
• USPSTF (I) – current evidence is insufficient to recommend ENDS for tobacco cessation in adults. Recommend that clinicians direct patients who smoke tobacco to other cessation interventions with established effectiveness and safety.• AAFP – long “middle of the road” statement, eventually calls for
rigorous research in the form of RCTs of e-cigs to assess their safety, quality, and efficacy as potential cessation device. Ban marketing as well
Day to Day Practice Take Home Points
Don’t forget e-cigarettes when discussing tobacco use with your patients
Day to Day Practice Take Home Points
Discuss e-cigarettes with your adolescents, as they are an at risk age group
Day to Day Practice Take Home Points
• If patients are using e-cigarettes, other topics that could be discussed:• Keep out of reach of children – risk of ingestion, skin
exposure• Care for equipment as directed – risk of burns, explosions• Recommend complete cessation of combustible smoking
products• Discuss that long term health effects of e-cigarettes are
unknown, and cessation from e-cigarettes should be encouraged as well
More information to come in the upcoming years
Questions?
References• 1 - Bullen, Christopher et al. Electronic cigarettes for smoking cessation: a randomised controlled trial. The Lancet , Volume 382 , Issue 9905 , 1629 - 1637
• 2 - Caponnetto, P., Campagna, D., Cibella, F., Morjaria, J. B., Caruso, M., Russo, C., & Polosa, R. EffiCiency and Safety of an eLectronic cigAreTte (ECLAT) as Tobacco Cigarettes Substitute: A Prospective 12-Month Randomized Control Design Study. 2013. PLoS ONE, 8(6), e66317. http://doi.org/10.1371/journal.pone.0066317
• 3 – Centers for Disease Control and Prevention. Notes from the Field: Calls to Poison Centers for Exposures to Electronic Cigarettes – United States, September 2010-February 2014. April 4, 2014. 63 (13); 292-293. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6313a4.htm?wptouch_preview_theme=enabled
• 4 - Ellis, James. Vaping: Big Tobacco’s Big Gamble On The Future. Apr 24 2016. Newsweek. Newsweek LLC. http://www.newsweek.com/vaping-big-tobacco-big-gamble-future-451074. Accessed October 29, 2017
• 5 - Esterl, Mike "Big Tobacco's E-Cigarette Push Gets a Reality Check". (26 August 2014). The Wall Street Journal
• 6 - Leventhal, A. M., Strong, D. R., Kirkpatrick, M. G., Unger, J. B., Sussman, S., Riggs, N. R., Audrain-McGovern, J. Association of electronic cigarette use with initiation of combustible tobacco product smoking in early adolescence. JAMA, 314(7), 700–707. http://doi.org/10.1001/jama.2015.8950
• 7 - Nides M, Oncken C, Gonzales D, Rennard S, Watsky EJ, Anziano R, Reeves KR, Varenicline Study Group. Smoking Cessation With Varenicline, a Selective α4β2 Nicotinic Receptor Partial AgonistResults From a 7-Week, Randomized, Placebo- and Bupropion-Controlled Trial With 1-Year Follow-up. Arch Intern Med. 2006;166(15):1561–1568. doi:10.1001/archinte.166.15.1561
• 8 - Rigotti, Nancy, MD, Kalkhoran, Sara, MD. E-Cigarettes. Post TW, ed. UpToDate. Waltham, MA: UpToDate Inc. Htt.://www.uptodate.com (Accessed on October 14, 2017.)
• 9 - Smith SS, McCarthy DE, Japuntich SJ, Christiansen B, Piper ME, Jorenby DE, Fraser DL, Fiore MC, Baker TB, Jackson TC. Comparative Effectiveness of 5 Smoking Cessation Pharmacotherapies in Primary Care Clinics. Arch Intern Med. 2009;169(22):2148–2155. doi:10.1001/archinternmed.2009.426
• 10 – The National Academies of Sciences, Engineering, and Medicine. Public Health Consequences of E-Cigarettes. Health and Medicine Division. January 23 2018.
• 11 - U.S Food & Drug Administration. Vapes, E-Cigs, Hookah Pens, and other Electronic Nicotine Delivery Systems (ENDS). Last Updated 09/18/2017. Silver Spring, MD. https://www.fda.gov/TobaccoProducts/Labeling/ProductsIngredientsComponents/ucm456610.htm#regulation. Accessed October 16, 2017.
• 12 – Watkins, SL, Glantz, SA, Chaffee, Benjamin. Association of Noncigarette Tobacco Product Use With Future Cigarette Smoking Among Youth in the Population Assessment of Tobacco and Health (PATH) Study, 2013-2015. JAMA Pediatr. 2018; 172(2): 181-187. Published online January 2, 2018
• 13 - Zhu Shu-Hong, Zhuang Yue-Lin, Wong Shiushing, Cummins Sharon E, Tedeschi Gary J. E-cigarette use and associated changes in population smoking cessation: evidence from US current population surveys BMJ2017; 358 :j3262
• 14 – Office of Adolescent Health. (2016). Adolescents and Tobacco: Trends. U.S Department of Health and Human Services. Accessed April 5. https://www.hhs.gov/ash/oah/adolescent-development/substance-use/drugs/tobacco/trends/index.html





























