Embed Size (px)
Citation preview
1
Establishing Emergency Department
Pharmacy Services and Pharmacist
Impact
Glenn R. Oettinger, PharmD, BCPS
and
Robert S. Pugliese, PharmD, BCPS
1
The Pennsylvania Society of Health System Pharmacists
October 29th, 2015
Objectives
1) Explain justification for an Emergency Medicine
Pharmacist (EMP)
2) Describe the core roles of the EMP
3) Describe strategies for implementing an EMP position
4) Identify how to encourage growth in the specialty of
Emergency Medicine (EM) Pharmacy
5) Describe some ways in which EMPs can systematically
improve the care of patients in ED
6) Discuss other key administrative roles of EMPs
2
The Emergency Medicine
Pharmacist A Safety Measure for Hospitals
Glenn Oettinger, PharmD, BCPS
@GlennOettinger
3
Part 1
The Emergency Medicine Pharmacist: A Safety
Measure for Hospitals1
• Justification
• Role
• Implementation
4
JUSTIFICATION Overcoming skepticism
5
The Ideal ED
6
2
The Ideal ED
• No patient is overlooked
• Adequate support for all clinical staff
• Appropriate supervision of all residents and
students
• All patients rest assured medications ordered
are reviewed by a pharmacist
7
Reality
8
Reality
• ED is Vulnerable
• High volume and overcrowding
• Wide spectrum of diseases
• Frequent interruptions and distractions
• Fast paced
• Verbal orders
9
ED is Inherently a Patient Safety Risk2,3,4
• Established safety mechanisms missing from most EDs
• Pharmacy review of medications
• Pharmacy preparation of medications
• Pharmacist involvement in clinical decision making
• Medication-related adverse events in the ED
• 3.6% of ED patients receive inappropriate medication
• 5.6% of ED patients receive inappropriate discharge Rx
10
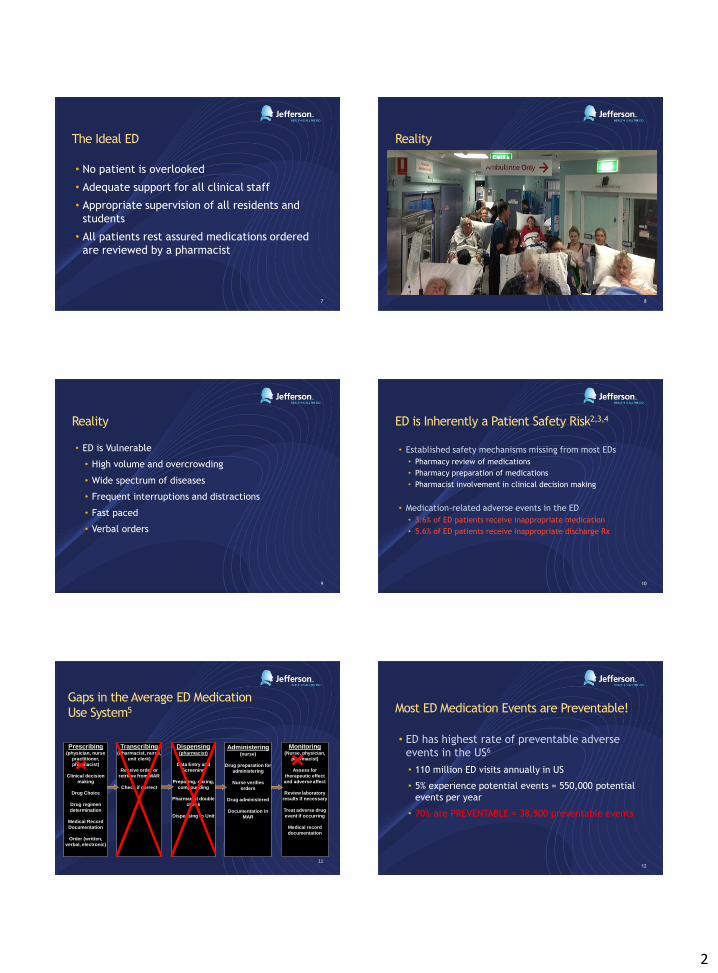
Gaps in the Average ED Medication
Use System5
11
Dispensing (pharmacist)
Data Entry and
Screening
Preparing, mixing,
compounding
Pharmacist double
check
Dispensing to Unit
Transcribing (Pharmacist, nurse,
unit clerk)
Receive order or
retrieve from MAR
Check if correct
Prescribing (physician, nurse
practitioner, pharmacist)
Clinical decision
making
Drug Choice
Drug regimen
determination
Medical Record
Documentation
Order (written,
verbal, electronic)
Monitoring (Nurse, physician,
pharmacist)
Assess for
therapeutic effect
and adverse affect
Review laboratory
results if necessary
Treat adverse drug
event if occurring
Medical record
documentation
Administering (nurse)
Drug preparation for
administering
Nurse verifies
orders
Drug administered
Documentation in
MAR
Most ED Medication Events are Preventable!
• ED has highest rate of preventable adverse
events in the US6
• 110 million ED visits annually in US
• 5% experience potential events = 550,000 potential
events per year
• 70% are PREVENTABLE = 38,500 preventable events
12

3
ED Systems are Stretched7,8 ED overcrowding = Reduced capacity to deliver safe care
• Over last decade
• ED visits 26%
• 9% of EDs closing nationwide
• 198,000 hospital beds closed
• Reduced capacity to deliver safe care
• Boarding inpatients
• Contributes to overcrowding and elevated risk
13
Safety Benefits of an ED Pharmacist Program
Providing an extra layer of protection
• Available for immediate high risk med review
• Respond to all traumas, resuscitations, and critical patients
• Pharmacotherapy consults with physicians for medication selection
• Staff education
14
Joint Commission Compliance9,10
ED Pharmacist improves JC compliance
• Increased oversight of high yield medications
• Increased monitoring of drug effect
• Enhanced degree of communication with nurses and
physicians
• Development of processes for managing high risk
medications (i.e. TPA, sepsis antibiotics, pediatric
meds)
15
Adding Value
It has been shown that staff value the ED Pharmacist
• 26 item survey to random ED staff with 82%
response11
• 99% felt ED pharmacist improves quality of care
• 96% felt ED pharmacist was an integral part of ED team
• 95% indicated they had consulted with ED pharmacist at
least a few times during last 5 shifts
16
The ED Pharmacist – A Safety Measure in
Emergency Medicine
• ED pharmacist improves process measures such as:
• Time to cath lab, abx in pna, pain management, etc12
• Adds critical layer of safety to vulnerable patients13
• Adds cost-saving benefit to the ED14
17
Cost-savings in the Emergency Room:
A Four Month Study of ED Pharmacist
Interventions14 Type of
Intervention
No.Interventio
ns
Average Cost
Avoidance per Intervention ($)
Cost Avoidance ($)
Drug-drug or drug disease
interactions
or drug
incompatibilities identified
334 1,647 297,053
Therapeutic recommendation
523 1,188 273,383
Adverse drug event
prevented
48 1,098 23,190
Medication error prevented
488 1,375 436,150
Total 1393 5,308 $1,029,776 18

4
Role of the ED Pharmacist
19
Role of the ED Pharmacist
• Clinical Consultation Duties
• Responds to pharmacotherapy consultations
• Provides drug selection and dose recommendations
• Therapeutic substitutions
• Recognizes disease state specific pharmacotherapy
• Implements patient-specific pharmacokinetics
20
Other Clinical Duties
• Order screening
• Focus on allergies, drug interactions, and
appropriate dosing
• Selection and preparation of medications
• High Risk Medications, RSI, codes
• Resuscitations and trauma response
• ED pharmacist at bedside actively overseeing
medication use process
21
Pediatric ADE’s in the ED15
• For every 1000 pediatric patients
• 100 prescribing errors
• 39 administration errors
• 22% of acetaminophen doses incorrect
22
Pediatric patients at risk
• Most ED’s generally not well-prepared to
manage pediatrics16
• 6% “well” prepared nationwide
• Pediatrics account for 27% of ED visits
• All children need weight-based dosing, increasing the
likelihood for errors
23
ED Pharmacist – An Educator
• New medications
• Drug warnings
• Drug-drug interactions
• Provides current, evidenced-based information on
pharmacological therapy
• Simulation exercises
• Becomes an established authority through education
24
5
Benefits of Having an ED Pharmacist17,18,19
• Research and educational advancements
• Vulnerable populations
• i.e. Severe sepsis, severe trauma, patients
requiring sedation, pediatrics
• Patient safety
• Reduced rate of adverse events
• Medication selection, order screening, stat
bedside preparation
25
IMPLEMENTATION
26
National Implementation20
• 3-5% of EDs in U.S. have a dedicated clinical pharmacist
• 18.3% have attempted to gain funding for a pharmacist
position
• Primarily through pharmacy budget
• 30.1% plan to request funding
• demand
27
Bottom Line
• ED’s across America are in need of dedicated
pharmacy specialists
• Arrive with a plan and they will embrace you
28
Step I: Assess Individual ED Environment
• Size of hospital
• Academic center vs. non-academic
• Urban vs. rural
• Patient demographics
• Annual patient volume
• Trauma center
Have potential ED pharmacist candidate shadow medical staff
• Determine needs
29
Step 2: Recruitment
Finding a full time dedicated ED Pharmacist
• Education
• PharmD
• Residency – PGY1 preferred
• PGY2 accredited emergency pharmacist
programs emerging
• ACLS, PALS certification
30
6
Step 2: Recruitment
Experience
• Critical/acute Care
• Emergency Medicine
• Pediatrics
31
What to Look for
Characteristics
• Proactive – continually offers assistance
• Build relationships with all medical staff
• Actively seeks out patients that can benefit from
ED pharmacist intervention
• Ability to appear helpful and not confrontational
• Ability to work well under pressure and time
constraints
32
Step 3: Overcoming Challenges
Funding
• Grants
• EM department co-funding
• Couple implementation with a residency project
Staff Resistance
• Temporary response to change
33
Financial Challenges
Important to demonstrate return on investment
• ED pharmacist save money
• Recommend lower cost meds with equal or better efficacy
• Reduce adverse drug events
• Waste reduction
34
ROI
4 month study – 2150 interventions21
• 1393 directly related to ADE’s
• Cost avoidance of estimated $1,029,776
35
Availability, Accessibility, and Visibility
• Dedicated to the ED
• Physically located in ED (not isolated to a satellite)
• Easily accessible and visible to all staff with frequent
“walk-through”
36
7
Resources
Provide ED Pharmacist with necessary equipment (laptop,
cell phone, pager, computer space centrally located in ED)
37 38
Go Team ED!
References – Part One
1. Emergency Pharmacist Research Team, University of Rochester Department of Emergency Medicine. Rollin J. (Terry) Fairbanks, Principal Investigator; Karen E. Kolstee, Project Coordinator; Daniel P. Hays, Lead Pharmacist. www.EmergencyPharmacist.org Supported by The Agency for Healthcare Research and Quality, Partnerships in Patient Safety, Grant no. 1 U18 HS015818
2. Hafner JW, et al. Annals of Emergency Medicine, 2002; 39(3).
3. Leape LL, et al. JAMA, 1995; 27(1).
4. Sanders MS, et al. Human Factors Engineering and Design. 7th ed. McGraw Hill, Inc.,1993.
5. Aspden P et al, Preventing Medication errors: Quality Chasm Series. Nat’l Academy Press: 1st ed, 2007
6. USP Patient Safety CAPS
7. Institute of Medicine, The Future of Emergency Care. Nat’l Academies Press; 2007
8. Derlet RW. Overcrowding in emergency departments: increased demand and decreased capacity. Ann Emerg Med. 2002;39(4):430-2.
9. Fairbanks, Patel, and Shannon. EPh Time-Motion Study (2007). Results presented at AHSP Mid-Year Clinical Meeting, December 5, 2007. (available at www.emergencypharmacist.org/toolkit.html)
10. Conners GP, Hays D. Emergency Department Drug Orders: Does Drug Storage Location Make a Difference? Annals of Emergency Medicine. 2007;50:414-418
11. Fairbanks RJ, Hildebrand JM, Kolstee KE, Schneider SM, Shah MN. Medical and nursing staff value and utilize clinical pharmacists in the Emergency Department. Emergency Medicine Journal Oct 2007; 24:716-719.
12. Fairbanks RJ, Results of the AHRQ Emergency Pharmacist Outcomes Study. American Society of Health-System Pharmacists 42nd Mid-Year Clinical Meeting, Las Vegas: 12/5/07. (available at www.EmergencyPharmacist.org).
13. Fairbanks RJ et al, The Optimized Emergency Pharmacist Role, Presented at AHRQ Patient Safety & Health IT Conference, June 2006 (available at www.EmergencyPharmacist.org).
14. Lada P, Delgardo G. Documentation of Pharmacists' Interventions in an Emergency Department and Associated Cost Avoidance. Am J Health-Syst Pharm-Vol 64 Jan 1, 2007
15. Aspden P et al, Preventing Medication errors: Quality Chasm Series. Nat’l Academy Press: 1st ed, 2007
16. Institute of Medicine, The Future of Emergency Care. Nat’l Academies Press; 2007
17. Bond CA, et al, Pharmacotherapy, 1999; 19(6).
18. Leape LL, et al JAMA, Mar 2000; 283(10).
19. Gattis WH, et al, Arch Internal Med, 1999; 159(16).
20. Thomasset and Faris, Am J Health-Syst Pharm, Aug 2003; 60
21. Lada, P. et al, Am J Health-Syst Pharm, Jan 2007; 61(4)
39
The Emergency Medicine
Pharmacist Systematically improving patient care hospital wide
Robert S. Pugliese, PharmD, BCPS
@theEDpharmacist 40
Part 2
Emergency Medicine Pharmacists recognized by
American College of Emergency Physicians (ACEP)
“RESOLVED, That ACEP create a policy statement that
supports clinical pharmacy services in emergency
departments and collaboration among emergency medicine
providers to promote safe, effective, and evidence-based
medication practices, to conduct emergency-medicine-
related clinical research, and to foster an environment
supporting pharmacy residency training in emergency
medicine”2
41
Resolution 44
Emergency Medicine Pharmacists recognized by
American College of Emergency Physicians (ACEP)
“Any of us who’s ever had access to
clinical pharmacy services in the
[emergency room] know it’s really
important”
–Louise A Prince, President, ACEP New York1
42
8
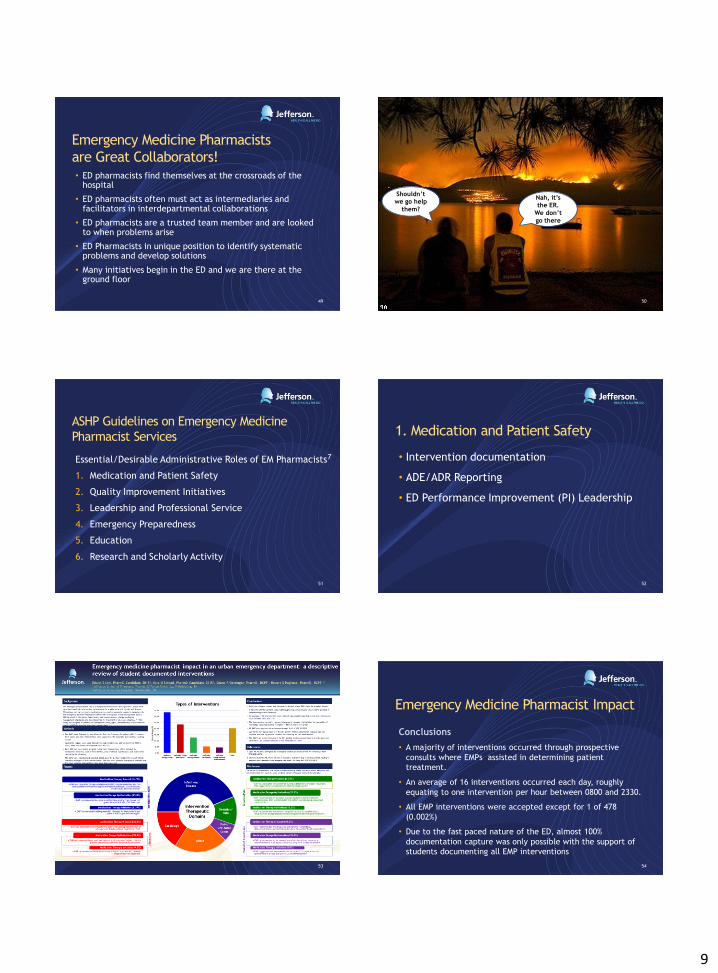
Surprise!?
• Many Emergency Departments:
• Overcrowded (primary care)
• Understaffed (5-to-1 nursing ratio!)
• Provide ICU level care (and fix tummy aches)
• Mixed population (inpatient/outpatient)
• Lack common medication safety protections
• Prospective medication order review not
mandated by Joint Commission
43
Do you
ED Pharmacist?
44
First mention of EM Pharmacy service was in 1977
published in American Journal of Hospital Pharmacy3
Yes 14%
No 86%
ER Pharmacist Survey 2000 (n=119)4
Yes 30%
No 70%
ER Pharmacist Survey 2007 (n=99)5
Pharmacy residency
programs surveyed Emergency Medicine
residency programs surveyed
45
Yes 62%
No 38%
?
Yes 14%
No 86%
ER Pharmacist Survey 2000 (n=119) 4
Yes 30%
No 70%
ER Pharmacist Survey 2007 (n=99) 5
Yes 62%
No 38%
Critical Care Pharmacist Survey 2006 (n=382) 6
Hospitals with ICUs surveyed 46
We need more Emergency Medicine
Pharmacists
216
27 0
50
100
150
200
250
Critical Care Emergency Medicine
ASHP Accredited PGY2 Residency Programs*
*Source: ASHP Online Residency Directory. Available at:
http://accred.ashp.org/aps/pages/directory/residencyProgramSearch.aspx. Accessed 1-8-2015
47
Emergency Medicine Pharmacy
A long road ahead 48
9
Emergency Medicine Pharmacists
are Great Collaborators! • ED pharmacists find themselves at the crossroads of the
hospital
• ED pharmacists often must act as intermediaries and facilitators in interdepartmental collaborations
• ED pharmacists are a trusted team member and are looked to when problems arise
• ED Pharmacists in unique position to identify systematic problems and develop solutions
• Many initiatives begin in the ED and we are there at the ground floor
49 50
Shouldn’t we go help
them?
Nah, it’s
the ER.
We don’t
go there
ASHP Guidelines on Emergency Medicine
Pharmacist Services
Essential/Desirable Administrative Roles of EM Pharmacists7
1. Medication and Patient Safety
2. Quality Improvement Initiatives
3. Leadership and Professional Service
4. Emergency Preparedness
5. Education
6. Research and Scholarly Activity
51
1. Medication and Patient Safety
• Intervention documentation
• ADE/ADR Reporting
• ED Performance Improvement (PI) Leadership
52
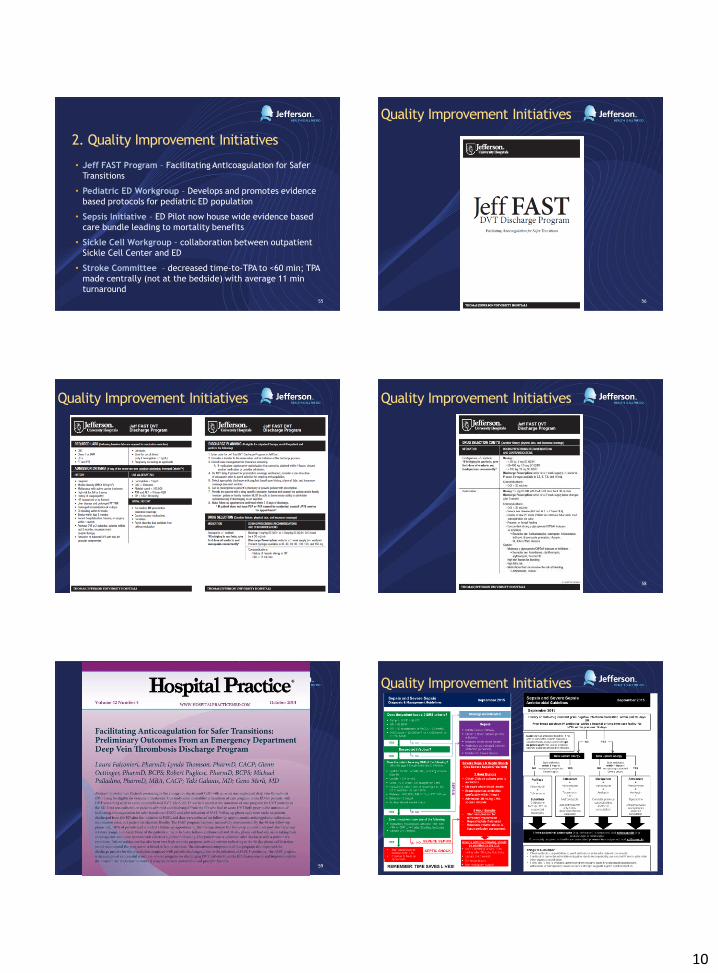
53
Emergency Medicine Pharmacist Impact
Conclusions
• A majority of interventions occurred through prospective
consults where EMPs assisted in determining patient
treatment.
• An average of 16 interventions occurred each day, roughly
equating to one intervention per hour between 0800 and 2330.
• All EMP interventions were accepted except for 1 of 478
(0.002%)
• Due to the fast paced nature of the ED, almost 100%
documentation capture was only possible with the support of
students documenting all EMP interventions
54
10
2. Quality Improvement Initiatives
• Jeff FAST Program – Facilitating Anticoagulation for Safer
Transitions
• Pediatric ED Workgroup – Develops and promotes evidence
based protocols for pediatric ED population
• Sepsis Initiative – ED Pilot now house wide evidence based
care bundle leading to mortality benefits
• Sickle Cell Workgroup – collaboration between outpatient
Sickle Cell Center and ED
• Stroke Committee – decreased time-to-TPA to <60 min; TPA
made centrally (not at the bedside) with average 11 min
turnaround
55
Quality Improvement Initiatives
56
Quality Improvement Initiatives
57
Quality Improvement Initiatives
58
59
Quality Improvement Initiatives
60
11
Quality Improvement Initiatives
61
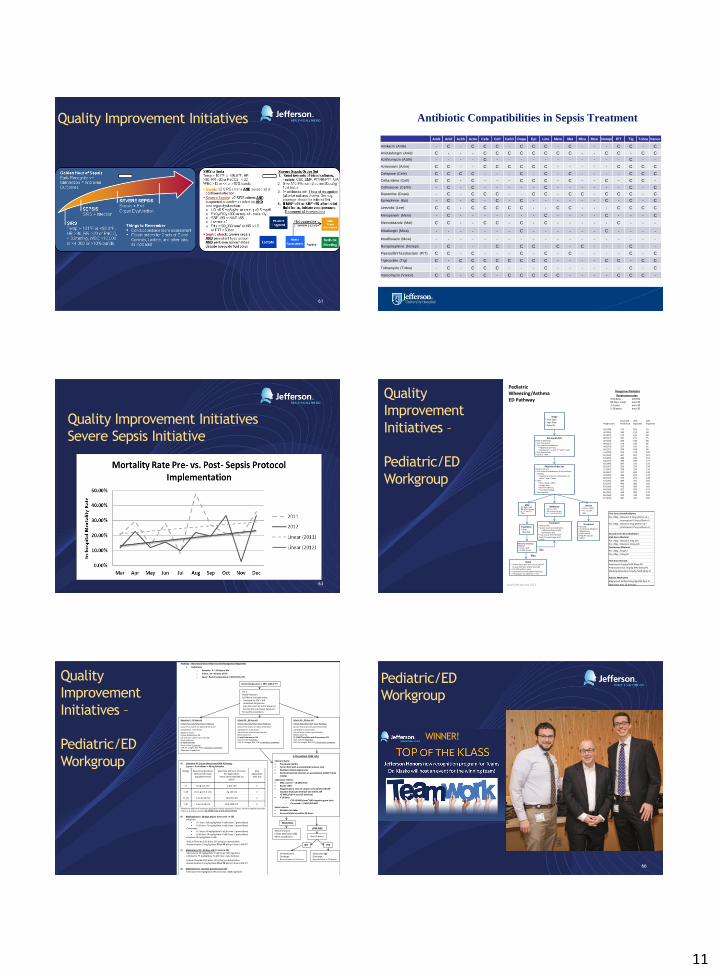
Antibiotic Compatibilities in Sepsis Treatment
Amik Anid Azith Aztre Cefe Ceft Ceftri Dopa Epi Line Mero Met Mica Moxi Norepi P/T Tig Tobra Vanco
Amikacin (Amik) - C - C C C - C C C - C - - - C C - C
Anidulafungin (Anid) C - - - C C C C C C C C - - C C - C C
Azithromycin (Azith) - - - - C - - - - - - - - - - - C - -
Aztreonam (Aztre) C C - - C C C C C C - - - - - C C C C
Cefepime (Cefe) C C C C - - - C - C - C - - - - C C C
Ceftazidime (Ceft) C C - C - - - C C C - C - - C - C C -
Ceftriaxone (Ceftri) - C - C - - - - - C - - - - - - C - C
Dopamine (Dopa) - C - C C C - - C C - C C - C C C - C
Epinephrine (Epi) - C - C - C - C - - - - - - C - C - C
Linezolid (Line) C C - C C C C C - - C C - - - C C C C
Meropenem (Mero) - C - - - - - - - C - - - - C - - - C
Metronidazole (Met) C C - - C C - C - C - - - - - C - - -
Micafungin (Mica) - - - - - - - C - - - - - - C - - - -
Moxifloxacin (Moxi) - - - - - - - - - - - - - - - - - - -
Norepinephrine (Norepi) - C - - - C - C C - C - C - - - C - -
Piperacillin/Tazobactam (P/T) C C - C - - - C - C - C - - - - C - C
Tigecycline (Tig) C - C C C C C C C C - - - - C C - C C
Tobramycin (Tobra) - C - C C C - - - C - - - - - - C - C
Vancomycin (Vanco) C C - C C - C C C C C - - - - C C C -
Quality Improvement Initiatives
Severe Sepsis Initiative
63
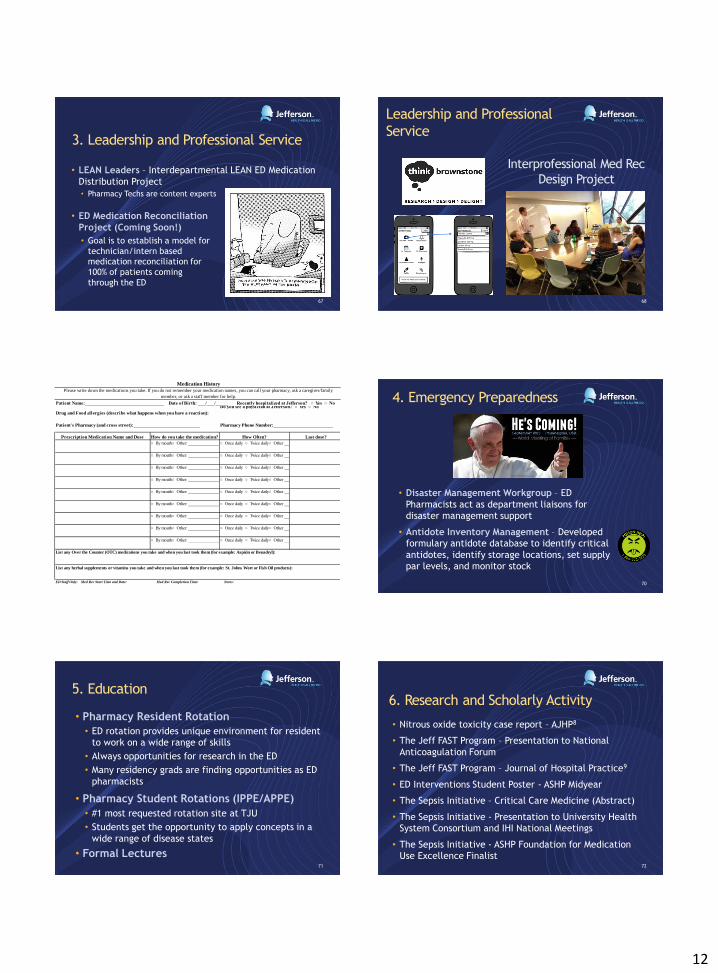
Quality
Improvement
Initiatives –
Pediatric/ED
Workgroup
Triage• Vital Signs• Peak Flow• Pulse Ox
Physician Order SetPediatric Asthma• First series Bronchodilators (if not previously
ordered):• Albuterol q 20 min x3 +Ipratropium x 2
with 2nd and 3rd nebs• CXR if:
• Fever (Temp ≥ 100.4• Foreign Born• First-time Wheeze• Focal Lung Findings
• Assess Severity
Treatment• Oral
Steroids
Nursing ED FLOPediatric Wheezing• Peak Flow pre-Rx• First series Bronchodilators:
• Albuterol q 20 min x3• +Ipratropium x2 with 2nd and 3rd nebs
• Peak Flow post-Rx• O2 NC if < 93%
Mild• O2 Sat > 93%• RR WNL for age• If > 7 yrs PF >
70%
Meets ALL Discharge Criteria?• O2 Sat > 93%• RR WNL for age
Treatment• Oral Steroids• Second series bronchodilators:
• High dose albuterol q2h• Ipratropium q4h
• Peds consult 877-656-5559• Peds RT consult pager 2141• Admit
Moderate• O2 Sat > 93%• RR elevated for age• If > 7 yrs PF 40-70%
Home• Asthma action plan (can consult peds RT
to assist with plan and/or teaching)• F/U PMD within 1 week• Equipment at home (Spacer/nebulizer)• Prescriptions for Albuterol +/- ICS
Treatment• Steroids• Continuous albuterol• Magnesium• Peds consult• Peds RT consult• Admit
Severe• O2 Sat ≤ 93%• If > 7 yrs PF <
40%
Yes
No
Dangerous Pediatric
Respiratory rates 0-60 days over 60 60 days- 1year over 401-5 years over 305-18 years over 20
Expected 70% 40%Height (cm) Peak Flow Expected Expected
43 (108) 147 103 5944 (112) 160 112 6445 (114) 173 121 6946 (117) 187 131 7547 (119) 200 140 8048 (122) 214 150 8649 (124) 227 159 9150 (127) 240 168 9651 (130) 254 178 10252 (132) 267 187 10753 (135) 280 196 11254 (137) 293 205 11755 (140) 307 215 12356 (142) 320 224 12857 (145) 334 234 13458 (147) 347 243 13959 (150) 360 252 14460 (152) 373 261 14961 (155) 387 271 15562 (157) 400 280 16063 (160) 413 289 16564 (163) 427 299 17165 (165) 440 308 17666 (168) 454 318 18267 (170) 487 341 195
Pediatric Wheezing/Asthma ED Pathway
Pts <20kg Albuterol 2.5mg q20min x3 +
Ipratropium 0.5mg q20min x2
Pts >20kg Albuterol 5mg q20min x3 +
Ipratropium 0.5mg q20min x2
Pts <20kg Albuterol 5mg q2h
Pts >20kg Albuterol 10mg q2h
Pts <20kg 5mg/hr
Pts >20kg 10mg/hr
Prednisone 2mg/kg MAX 60mg PO
Prednisolone Sol 2mg/kg MAX 60mg PO
Methylprednisolone 2mg/kg MAX 60mg IV
Magnesium Sulfate 50mg/kg MAX 2gm IV
administer over 20 minutes
First Series Bronchodilators
Second Series Bronchodilators
First Dose Steroids
Adjunct Medication
High Dose Albuterol
Continuous Albuterol
Issue Date January 2013 64
Quality
Improvement
Initiatives –
Pediatric/ED
Workgroup
65
Pathway – Neonate/Infant 0-90d Fever ED Management Algorithm
Definitions
o Neonate: 0 – 28 days of life
o Infant: 29 – 90 days of life
o Fever: Rectal temperature ≥ 38ºC (100.4 ºF)
Obtain IV access Initiate Medications (C) Admit to pediatrics
Rectal temperature ≥ 38ºC (100.4 ºF)
Neonates 0 – 28 days old
Initiate Neonate/Infant Fever Pathway
(Assure FLO orders are placed if not done)
Call pediatric consult (CC)
Obtain IV access Initiate Medications (B) UA and urine culture (use Cath Kit) Blood culture x1 LP with HSV PCR Stool culture if diarrhea CXR, Flu antigen, RSV PCR if respiratory symptoms Admission to pediatrics
ESI 2 Notify Physician FLO/Nurse initiated orders -Heelstick for CBC + diff -Accucheck for glucose -Lido 4% cream x1 prn IV place (A) -Sucrose Sol oral (Sweet-Ease) prn for painful procedures
Infants 29 – 60 days old
Initiate Neonate/Infant Fever Pathway
(Assure FLO orders are place if not done)
Call pediatric consult (CC) UA and urine culture (use Cath Kit) Blood culture x1 LP with Enterovirus PCR Stool culture if diarrhea CXR, Flu antigen, RSV PCR if respiratory symptoms
Infants 61 – 90 days old
Initiate Neonate/Infant Fever Pathway
(Assure FLO orders are place if not done)
Call pediatric consult (CC) UA and urine culture (use Cath Kit) Blood culture x1 LP (if NOT Low Risk) with Enterovirus PCR Stool culture if diarrhea CXR, Flu antigen, RSV PCR if respiratory symptoms
Is the patient LOW risk?
Clinical criteria:
Previously healthy
Term infant with uncomplicated nursery stay
Nontoxic clinical appearance
No focal bacterial infection on examination (EXCEPT otitis media)
Laboratory criteria:
WBC count 5 – 15,000/mm3
Bands <20%
Negative gram stain of unspun urine (preferred) OR negative leukocyte esterase and nitrite, OR <5 WBCs/hpf in stool (if diarrhea)
If LP done o CSF <8 WBCs/mm3 AND negative gram stain o Corrected: <1 WBC/500 RBC
Social criteria:
Reliable care taker
Assured follow up within 24 hours
A) Lidocaine 4% Cream (Anecream/LMX-4) Dosing: 1 gram = 5 cm ribbon = 40 mg lidocaine
Wt(kg) Recommended Dose (Amount of Cream Applied) Per Site
Max Dose (Amount of Cream Per Application)
TOTAL AMT USED ON ALL SITES*
Max Application Time (hr)
< 5 0.5 g (2.5 cm) 1 g (5 cm) 1
5-10 0.5-1 g (2.5-5 cm) 2 g (10 cm) 2
11-20 1-2 g (5-10 cm) 10 g (50 cm) 2
> 20 1-2 g (5-10 cm) 20 g (100 cm) 2
*Maximum amount of cream per application may be repeated in 2 hours; not to be applied more than 3 times in a 24 hour period / NO MORE THAN 2 SITE APPLICATIONS
B) Medications 0 – 28 days old (x1 doses only in ED)
-Ampicillin
0-7 days: 100 mg/kg/dose IV q8h (max: 2 grams/dose)
8-28 days: 75 mg/kg/dose IV q6h (max: 2 grams/dose) -Cefotaxime
0-7 days: 50 mg/kg/dose IV q12h (max: 2 grams/dose)
8-28 days: 50 mg/kg/dose IV q8h (max: 2 grams/dose) -Acyclovir 20 mg/kg/dose IV q8h
-Sodium Chloride 0.9% Bolus (20 ml/kg) prn dehydration -Acetaminophen 15mg/kg/dose PO or PR q6h prn fever ≥100.4°F
C) Medications 29 – 90 days old (x1 dose in ED) -Vancomycin 15 mg/kg/dose IV q6h (max: 500 mg/dose) -Cefotaxime 75 mg/kg/dose IV q6h (max: 2 grams/dose)
-Sodium Chloride 0.9% Bolus (20 ml/kg) prn dehydration -Acetaminophen 15mg/kg/dose PO or PR q6h prn fever ≥100.4°F
D) Medication for Low Risk patients (post-LP)
-Ceftriaxone 50 mg/kg/dose IM once (max: 1000 mg/dose)
Was LP done?
NO YES
Medication (D) Discharge Reevaluation in 24 hours Reevaluation in 24 hours
HIGH RISK
LOW RISK
No Medication
Discharge Reevaluation in 24 hours Reevaluation in 24 hours
66
WINNER!
Pediatric/ED
Workgroup
12
3. Leadership and Professional Service
• ED Medication Reconciliation
Project (Coming Soon!)
• Goal is to establish a model for
technician/intern based
medication reconciliation for
100% of patients coming
through the ED
• LEAN Leaders – Interdepartmental LEAN ED Medication
Distribution Project
• Pharmacy Techs are content experts
67
Interprofessional Med Rec
Design Project
68
Leadership and Professional
Service
69
Patient's Pharmacy (and cross street):___________________________
Please write down the medications you take. If you do not remember your medication names, you can call your pharmacy, ask a caregiver/family
member, or ask a staff member for help.
Medication History
Drug and Food allergies (describe what happens when you have a reaction):
Pharmacy Phone Number:________________________
Patient Name:________________________________ Date of Birth: ___/___/_____ Recently hospitalized at Jefferson? ○ Yes ○ No Do you see a physician at Jefferson? ○ Yes ○ No
ED Staff Only: Med Rec Start Time and Date: Med Rec Completion Time: Notes:
○ Once daily ○ Twice daily ○ Other ________________
○ By mouth ○ Other: ________________
○ By mouth ○ Other: ________________
○ By mouth ○ Other: ________________
List any Over the Counter (OTC) medications you take and when you last took them (for example: Aspirin or Benadryl):
Prescription Medication Name and Dose
List any herbal supplements or vitamins you take and when you last took them (for example: St. Johns Wort or Fish Oil products):
○ By mouth ○ Other: ________________
○ By mouth ○ Other: ________________
○ Once daily ○ Twice daily ○ Other ________________
○ Once daily ○ Twice daily ○ Other ________________
○ Once daily ○ Twice daily ○ Other ________________
○ Once daily ○ Twice daily ○ Other ________________
Last dose?
○ By mouth ○ Other: ________________
○ By mouth ○ Other: ________________
○ Once daily ○ Twice daily ○ Other ________________
○ Once daily ○ Twice daily ○ Other ________________
How do you take the medication? How Often?
○ Once daily ○ Twice daily ○ Other ________________
○ By mouth ○ Other: ________________
○ By mouth ○ Other: ________________
○ Once daily ○ Twice daily ○ Other ________________
4. Emergency Preparedness
• Disaster Management Workgroup – ED
Pharmacists act as department liaisons for
disaster management support
• Antidote Inventory Management – Developed
formulary antidote database to identify critical
antidotes, identify storage locations, set supply
par levels, and monitor stock
70
5. Education
• Pharmacy Resident Rotation
• ED rotation provides unique environment for resident
to work on a wide range of skills
• Always opportunities for research in the ED
• Many residency grads are finding opportunities as ED
pharmacists
• Pharmacy Student Rotations (IPPE/APPE)
• #1 most requested rotation site at TJU
• Students get the opportunity to apply concepts in a
wide range of disease states
• Formal Lectures
71
6. Research and Scholarly Activity
• Nitrous oxide toxicity case report – AJHP8
• The Jeff FAST Program – Presentation to National
Anticoagulation Forum
• The Jeff FAST Program – Journal of Hospital Practice9
• ED Interventions Student Poster - ASHP Midyear
• The Sepsis Initiative – Critical Care Medicine (Abstract)
• The Sepsis Initiative - Presentation to University Health
System Consortium and IHI National Meetings
• The Sepsis Initiative - ASHP Foundation for Medication
Use Excellence Finalist 72
13
6. Research and Scholarly Activity
Pharmacy Resident Research Manuscripts
• Post Intubation Sedation ED Protocol
• Establishing the Jeff FAST Program
• ED Pharmacist Effect on Sepsis Protocol
Adherence
• Pharmacy Led Med Rec in ED
• Improving the Pharmacologic Management of
Severe Sepsis
73 74
6. Research and Scholarly
Activity
6. Research and Scholarly Activity
• Social Media and FOAMed?
• Blogs/Podcasts – ALiEM, EMPharmD, LITFL
• Twitter - @PharmERToxGuy, @ASHP_EMPharm, @theEDpharmacist
• YouTube
• WikiEM
75 76
ASHP Emergency Care
Section Advisory Group
Questions?
77
References – Part Deux
1. American College of Emergency Physicians. 2014 Council Resolutions, Chicago. Resolution 44: Support for Clinical Pharmacists as Part of the Emergency Medicine Team. Available at: https://www.acep.org/uploadedFiles/ACEP/About_Us/Leadership/Council/2014%20Resolutions%20Compendium.pdf. Accessed January 8, 2015.
2. Cheryl A. Thompson. Pharmacy News: Emergency Physicians Group Supports ED Clinical Pharmacy Services. AJHP News. December 15, 2014. Available at: http://www.ashp.org/menu/News/PharmacyNews/NewsArticle.aspx?id=4140. Accessed January 8, 2015.
3. Elenbaas RM, Waeckerle JF, Mcnabney WK. The clinical pharmacist in emergency medicine. Am J Hosp Pharm. 1977;34(8):843-6.
4. Thomasset KB, Faris R. Survey of pharmacy services provision in the emergency department. Am J Health Syst Pharm. 2003;60(15):1561-4.
5. Szczesiul JM, Fairbanks RJ, Hildebrand JM, Hays DP, Shah MN. Survey of physicians regarding clinical pharmacy services in academic emergency departments. Am J Health Syst Pharm. 2009;66(6):576-9.
6. Maclaren R, Devlin JW, Martin SJ, Dasta JF, Rudis MI, Bond CA. Critical care pharmacy services in United States hospitals. Ann Pharmacother. 2006;40(4):612-8.
7. Eppert HD, Reznek AJ. ASHP guidelines on emergency medicine pharmacist services. Am J Health Syst Pharm. 2011;68(23):e81-95.
8. Pugliese RS, Slagle EJ, Oettinger GR, Neuburger KJ, Ambrose TM. Subacute combined degeneration of the spinal cord in a patient abusing nitrous oxide and self-medicating with cyanocobalamin. Am J Health Syst Pharm. 2015;72(11):952-7.
9. Falconieri L, Thomson L, Oettinger G, et al. Facilitating anticoagulation for safer transitions: preliminary outcomes from an emergency department deep vein thrombosis discharge program. Hosp Pract (1995). 2014;42(4):16-45.
78









![LTRUCC 2150 Slides[1]](https://img.pdfslide.us/doc/110x75/5447d0c6b1af9ff9778b45bb/ltrucc-2150-slides1.jpg)



















