Embed Size (px)
Citation preview

1
Morbid Obesity: Drugs, Diet or Surgery
John P. Cello, MDProfessor of Medicine and Surgery, UCSF
Stanley J. Rogers, MDAssociate Professor of Surgery, UCSF
Ruth M. Dunn Distinguished Professorship
Rama IX Distinguished Chair in Minimally-Invasive Surgery
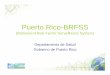
Obesity Trends* Among U.S. AdultsBRFSS, 1990
(*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person)
No Data <10% 10%–14%
1990 – Thirty states with 10-14% obesity prevalence
U.S. Adults: 2000Twenty-two states with > 20 % prevalence of obesity, 27 states with 15-19% obesity, one state with 10-14% obesity
Mokdad A H, et al. J Am Med Assoc 2001; 286:10
(*BMI > 30, or ~ 30 lbs overweight for 5’4” woman)
Obesity Trends* Among U.S. AdultsBRFSS, 2010
(*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
All 50 states with at least 20% of the population obese

2
Women in the USA
The Economist, December 13-19, 2003.
Not Just a Problem for American Women!! Relationship of BMI to Excess Mortality
300Age at Issue
Bray GA. Overweight is risking fate. Definition, classification, prevalence and risks. Ann NY Acad Sci 1987;499:14-28.
20-29250
Body Mass Index (kg/[m2])
200
150
100
50
150
30-39
20 25 30 4035

3
But doctor why am I so fat? I just eat like a bird.
The Answer:First Law of Thermodynamics
� Matter and energy are interchangeable.
� They are neither created nor destroyed
� Calories Ingested minus Calories Expended = Excess Caloric Intake.
� Energy (caloric) excess is stored principally as fat.
Basal Energy Requirements – Man @ 70 kg. (est. total 1940 kcal)
Tissue Weight % B Weight Kcal/day
Liver 1550 2.2 445
Brain 1400 2.0 420
Kidneys 300 0.4 360
Heart 300 0.4 235
Skeletal muscle 28000 40 400
Adipose 15000 21 80
Endogenous Fuel Stores in a 70 Kg. Man
Tissue Fuel Source Grams Kcal.
Adipose Triglyceride 13000 120000 (60 d)
Liver Glycogen 100 400
Protein 300 1200
Triglyceride 50 450
Muscle Protein 6000 24000 (12 d)
Glycogen 400 1600
Triglyceride 50 450
Blood Glucose 15 60
Triglyceride 4 35
Free fatty acids 0.5 5
Non-adipose/muscle energy stores – equivalent to 2 days!!

4
Historical Background – Metabolic Syndrome
� Vague (France) 1947 – first noted that upper body obesity predisposed to diabetes, atherosclerosis, gout
� Avogaro & Crepaldi (Italy) 1967 – describes 6 obese patients with DM, elevated chol. & TG – all responding to dieting with low carbohydrates
� Haller (Germany) 1977- coined term “Metabolic Syndrome” in patients with obesity, DM, atherosclerosis, elevated TG & chol. Associated with hepatic steatosis
� Reaven (England) 1988 – proposed insulin resistance as the underlying factor for “Syndrome X”
Components of the Metabolic Syndrome
� Abdominal Obesity – increased visceral fat (premier feature)
� Insulin Resistance – with glucose intolerance and diabetes mellitus
� Dyslipidemia (consequential)� Hypertension (consequential)
Morbid Obesity and the Metabolic Syndrome
� Markedly increased visceral fat is the core feature of the pathogenesis of the metabolic syndrome
� The key consequence of the increased visceral fat is insulin resistance
Prevalence of Metabolic Syndrome Over 50 years old
� United States – 40% of population
� Europe – 30 % of population
� Developing world – not immune from the entity – India – now 27% of population
� Racial predisposition – Hispanics>African-Americans>Caucasians>Asians
� Sex predisposition – none: males = females

5
ReducedPhysicalActivity
Excessive food intake
Geneticfactors
adiponectin �� leptin
� IL-6� TNF-α
insulinreceptorSubstrate
(IRS-1 & IRS-2)
� blood FFA
� variouscytokines
How Does Abdominal Obesity Cause Insulin Resistance
Inflammation
Parameter (any 3/5 diagnostic) Categorical cutpoints
Elevated waist circumference ≥ 40 inches in men≥ 35 inches in women
Elevated triglycerides ≥150 mg/dl at baseline
Reduced HDL-cholesterol <40 mg/dl in men
<50 mg/dl in womenOr on drug treatment for reduced HDL-C
Elevated blood pressure ≥130 mmHg systolic blood pressure or
≥85 mmHg diastolic blood pressureor on antihypertensive drug treatment in a patient with a history of hypertension
Elevated fasting glucose ≥100 mg/dl at baseline
2005 Revised ATP III Clinical Screening Criteria
to Identify Metabolic Syndrome (AHA and NHLBI)
Metabolic Syndrome - Treatment
� Expectant treatment – treat complications of diseases
� Dietary weight loss� Exercise programs� Pharmacotherapy� Bariatric surgery
Dietary Changes
� Caloric restriction: – Total fat: 25-35% of total calories– Reduced consumption of simple sugars– Increased intakes of fruits, vegetables, and whole grains
� The relative amounts of carbohydrate and unsaturated fats is more controversial

6
� Regular and sustained physical activity will improve all risk factors of the metabolic syndrome
� Current guidelines recommend 30-60 min moderate-intensity exercise daily (e.g., brisk walking)
� Best with a trainer under supervision
Physical Activity Prescription Pharmacotherapy
� Unlicensed for bariatric use: thyroid derivatives, amphetamines
� Approved medications: orlistat (Xenical)
� Withdrawn medications: Phen-Fen, Sibutramine, Rimonabant
Orlistat - XenicalTM
� Pancreatic lipase inhibitor
� Dosage: 120 mg TID ($200/month)
� Side effects: steatorrhea, diarrhea, cramping, flatulence
� Overall efficacy: pts can loose 3-4 kg/year over that achieved by 1500 cal/day alone.
� Over-the-counter in Great Britain
Sibutramine (Meridia TM )� Mechanism of action: monoamine (serotonin and
norepinephrine) reuptake inhibitor
� Side effects: tachycardia, hypertension, seizures, cholelithiasis, depression, suicidality (increased cardiovascular events)
� Efficacy: 4-5 kg extra weight loss over 1 year (with 1500 cal/day diet)
� WITHDRAWN FROM MARKET

7
Rimonabant
� Mechanism of action: selective cannabinoid receptor-1 antagonist
� Dosage: 20 mg QD
� Side effects: mood disorders
� Efficacy: about 4-5 kg added weight loss over one year (over that with 1500 cal/day diet)
� WITHDRAWN FROM MARKET
Morbid obesity: diet, drugs or surgery
Stanley James Rogers, MDAssociate Professor of SurgeryRuth M. Dunn Endowed Chair
Chief, Minimally Invasive SurgeryUniversity of California, San Francisco
UCSF General Surgery Post Graduate CourseSaturday, May 18, 2013
San Francisco

8
Original Article
Long-Term Mortality after Gastric Bypass SurgeryTed D. Adams, Ph.D., M.P.H., et al
University of Utah School of MedicineSalt Lake City, UT
N Engl J MedVolume 357(8):753-761
August 23, 2007
Original Article
Effects of Bariatric Surgery on Mortality in Swedish Obese Subjects
Lars Sjöström, M.D., Ph.D., et al.Swedish Obese Subjects (SOS) Study
Sahlgrenska University Hospital, Gothenburg, Sweden,
N Engl J MedVolume 357(8):741-752
August 23, 2007
� Prospective, controlled Swedish Obese Subjects study involved 4047 obese subjects
� 2010 pts underwent bariatric surgery
� 2037 pts received conventional medical therapy (matched control group)
� Reported overall mortality during an average of 10.9 year follow-up
� 99% of pts followed!� Decreased mortality in surgery
group from MI & CANCER
Bariatric surgery for severe obesity is associated with long-term weight loss & decreased overall mortality
� Compared with usual care, bariatric surgery was associated with reduced number of cardiovascular deaths and lower incidence of cardiovascular events in obese adults.
� Bariatric surgery is more then weight loss; its about treating metabolic diseaseassociated with obesity, reversing morbidity & reducing mortaility

9
0
10
20
30
40
50
60
70
80
90
100
Diabetes Hyperlipidemia HTN Sleep apnea
BandVBGGBPD Switch
% R
esol
utio
n C
omor
bidi
ty
Resolution of Comorbidities – 22,094 patientsBariatric Surgery – A Systematic Review and Meta-analysis
Buchwald H. et al.JAMA. 2004; 292(14):1724-37
• For patients who have:� BMI of 40 or more, (i.e., 100 lb or more overweight),
� BMI of 35 or more & significant health complications,
� or have failed to lose weight with more conservative approaches,
• gastric surgery may be an option.
NIH Consensus Panel – March 25-27, 1991
Clinically Severe Obesity: Surgical Indications
Patients who are candidates for surgical
procedures should be selected carefully after
evaluation by a multidisciplinary team with
medical, surgical, psychiatric and nutritional
expertise.
NIH Consensus Panel – March 25-27, 1991
Clinically Severe Obesity: Surgical Indications

10
UCSF - Multidisciplinary approach
� Primary Care
� Gastroenterology
� Anesthesia
� Cardiology & Pulmonology
� Clinical Nutrition� 10% BW Loss
� Psychiatry / Psychology
� Endocrinology
� Physical Therapy
Surgery
Surgery for Morbid Obesity
Year SurgeriesChange fromprior year
1992 16,2001993 16,800 4%1994 16,200 -4%1995 18,100 12%1996 20,500 13%1997 23,100 13%1998 25,800 12%1999 28,800 12%2000 36,700 27%2001 47,200 29%2002 63,100 34%2003 103,200 64%2004 140,640 36%2005 171,000 22%2006 177,600 4%2007 205,000 15%2008 220,000 7%2009 220,000 0%
Bariatric Surgery: US Case Volume

11
Surgical options• Malabsorptive procedure
• Types:• Jejunoileal Bypass
• Duodenal Switch
• Biliopancreatic Diversion
• Restrictive procedure• Types:
• Vertical Banded Gastroplasty (VBG)
• Adjustable Lap-Band
• Sleeve Gastrectomy
• Combined procedure • Types:
• Roux-en-Y Gastric Bypass

12
Lap Band:Patient preference for lowest risk
& reversibility– Advantages:� Least invasive � No gastric stapling / division or
intestinal rerouting� Adjustable� Reversible� Lowest operative complications� Lowest mortality� Low malnutrition risk
– Disadvantages:� Slower, less significant weight loss
than gastric bypass� Regular follow-up critical for
optimal results� Dependence on band adjustments

13
� Arch Surg. 2011;146(7):802-807. Published online March 21, 2011. doi:10.1001/archsurg.2011.45
� 151 patients underwent gastric banding from 1994 – 1997, contacted for follow-up
� 84 pts completed follow-up� 39% experienced major complications
(28% erosions)� 49% of bands had been removed� 17% converted to gastric bypass
Gastric banding being replaced by sleeve gastrectomy
� Arch Surg. 2011;146(7):802-807. Published online March 21, 2011. doi:10.1001/archsurg.2011.45
� Nearly half of patients who have laparoscopic gastric banding for obesity eventually need to have the devices removed because of erosion or other malfunction
� "The high failure rate of laparoscopic adjustable gastric banding….. detrimental to its future continued widespread use as a restrictive weight-loss operation“
There is currently a request for a congressional investigation by members of the U.S. Congress into lapband safety, prompted by recent patient deaths after lapbandsurgeries at clinics affiliated with the 1-800-GET-THIN advertising campaign in Southern California.

14
• Many opportunities for investigation – should be conducted in an academic fashion thru PRCT
• Questions regarding expectations (patients, providers, suppliers, hospitals, insurance providers) should not stifle innovation when it comes to treating the worldwide obesity epidemic
• Provision: investigational therapy is safely conducted with full transparency and appropriate oversight
Innovation in Bariatric Surgery�Endoscopic restriction devices
• Endoluminal suturing and stapling�Endoscopic injection of polymers at GE
junction• Enteryx
�Prosthesis• Intragastric balloon (similar to Garren balloon
used previously)• Endo-barrier
�Novel devices -> novel procedures• NOTES / SILS• Ablation / electrical / energy technologies
(gastric pacing)• Endoscopic stapling devices: TOGAFew licensed in US by FDA
Innovation: DEVICES
• BioEnterics Intragastric balloon BIB System
• Not yet available in US• Widely available overseas• Licensed for 6 month use• Placed and removed using
endoscopic control
Innovation in Bariatric Surgery : BIBInamed Bioenteric Intragastric Balloon
EndoBarrier: Duodenojejunal bypass liner
Gersin et al. Gastrointest Endosc 2010;71:976-82

15
• Open-label, sham-controlled trial of an endoscopic duodenojejunal bypass liner (DJBL) for preoperative weight loss in bariatric surgery candidates• Liner creates a duodenojejunal bypass resulting in
weight loss and improvement in type 2 diabetes mellitus.
• Prospective, randomized, sham-controlled trial, multicenter, tertiary care, teaching hospitals.
• 21 obese subjects in the DJBL arm and 26 obese subjects in the sham arm using an intent-to-treat approach.
EndoBarrier: Duodenojejunal bypass liner
Gersin et al. Gastrointest Endosc 2010;71:976-82
EndoBarrier: Duodenojejunal bypass liner
• SILS for standard bariatric procedures• Band• Sleeve
• Gastric Plication (and sleeve gastrectomy)• Transoral Gastroplasty (TOGA)
Innovation in Bariatric Surgery: PROCEDURES
Innovation: SILS BAND
de la Torre, et al. Obesity 2009, 19:1707-1710

16
NOVEL APPROACHES: SILS BAND
de la Torre, et al. Obesity 2009, 19:1707-1710
Laparoscopic Gastric Plication→ decreased gastric capacity
Ramos et al. Obes Surg, 2010
• Transoral gastroplasty procedure• Satiety, Inc.• Endoscopic stapling of stomach• Incisionless creation of gastric partition and pouch• Creation of restrictive passage from pouch to stomach• Similar outcomes as some current treatments
NOVEL APPROACHES: TOGA
• TOGA® Sleeve Stapler• 54F (18mm) diameter• Designed to pass an 8.6 mm endoscope• Direct visualization during key procedure steps• Creates stapled sleeve along lesser curve
The TOGA® System

17
• TOGA® Restrictor • 45F (15mm) diameter, delivered alongside endoscope• Creates stapled “pleats” at distal end of sleeve,
restricting outflow
The TOGA® System Sleeve Stapler inserted, positioned along lesser curve
Sail / wire deployed to separate / spread tissueVacuum applied to anchor anterior & posterior gastric walls

18
Stapler jaws closed and fired Result is an endoscopic stapled sleeveRepeat to create longer sleeve (2 shown)
Restrictor inserted to reduce size of outflow tract TOGA Pilot Study Excess Weight Loss (Phase 1 n=21, Phase II n=41)
0%
10%
20%
30%
40%
50%
0 1 2 3 4 5 6 7 8 9 10 11 12
Months
%EWL (MetLife)
TOGA Ph I
TOGA Ph II
Realize Band(adjusted)
n=21n=21
n=20n=39
n=26
n=18
TOGA Ph I: Moreno C IFSO 2008 presentationTOGA Ph II: Moreno C IFSO 2008 presentation

19
TOGA Trial: multicenter, prospective, randomized, sham controlled trial (all + SEM)
Entire National Cohort
Results: TOGA v. LRYGBP
TOGA Roux Y GB P value
Age (yrs) 41.5 +2.3 48.0 +2.1 0.027
Sex (f/m) 22 / 0 29 / 1 NS
Starting BMI 44.9 +1.0 44.0 +0.8 NS
OR time (min) 72.6 +3.0 115.0 +5.8 <0.0001
Recovery time (min) 127.7 +13.5 197.8 +16.7 0.0030
Hospital stay (hrs) 30.8 +0.7 63.5 +3.3 <0.0001
Follow-up BMI (@ 12 mo) 39.6 +1.3 31.8 +1.3 <0.0001
Change in BMI (@ 12 mo) 5.3 (11.8%) 12.2 (27.7%) <0.0001
TOGA (randomized) vs. Gastric Bypass (non-randomized) -single-site (UCSF), cotemporally treated (all + SEM)
� In selected patients, TOGa®, was associated with good results after two years in terms of weight loss, even in comparison with LRYGBP and BPD.
� Minimal trauma, absence of complications, and short hospital stay justify this procedure for patients with low BMI.
• GOALS�Less invasive�Fewer complications�Improved results
Innovation in Bariatric Surgery

20
Thank you
























![Daftar Pustaka [1724 KB]](https://img.pdfslide.us/doc/110x75/586771db1a28ab17578b5daa/daftar-pustaka-1724-kb.jpg)