Embed Size (px)
Citation preview

OBESITY DRUGS: CURRENT STATUS AND FUTURE POTENTIAL
Richard L. Atkinson, M.D.
Director, Obetech Obesity
Research Center
Virginia Biotechnology Research Park
Richmond, Virginia
obesityvirus.com

DEFINITION OF OBESITY
Obesity is a chronic disease of multiple etiologies characterized by
the presence of excess adipose tissue
RL Atkinson, 1980

RATIONALE FOR DRUG TREATMENT OF OBESITY
1. Obesity is a chronic disease
2. Most chronic diseases are treated with drugs
3. The biochemistry of obese individuals is different from that of lean people
4. When obese people lose weight, their biochemistry does not become the same as in lean people
5. Biochemistry is changed with drugs

BARRIERS TO USE OFOBESITY DRUGS
1. Discrimination against obesity
2. Physician/clinician ignorance
3. Economic factors
4. Policy/political barriers
5. Lack of advocacy by obese people
6. Modest effectiveness of obesity drugs

OBESITY IS THE LAST BASTION OF SOCIALLY ACCEPTABLE BIOGTRY

AREAS OF DISCRIMINATION:DEFINITION
“Labeling obesity a disease may be expedient but it is not a necessary step in a campaign to combat obesity and it may be interpreted as self-serving advocacy without a sound scientific basis.”
Heshka and Allison, IJO, 2001

AREAS OF DISCRIMINATION:LACK OF MEDICALIZATION
Comparison with other chronic diseases:
1. Newly diagnosed Type 2 diabetes and hypertension respond very well to diet and exercise - but the primary treatments are drugs
2. The primary treatment for obesity is diet and exercise, drugs are an “adjunct”. Many patients must demonstrate that they have failed D&E before getting drugs or surgery

BARRIERS TO OBESITY DRUGS:PHYSICIAN/CLINICIAN IGNORANCE
1. Obesity thought not to be a real disease
2. Uncomfortable about counseling overweight or obese patients
3. Physicians/clinicians not knowledgeable about nutrition, physical activity, obesity drugs
4. Unaware of referral information
5. Bias that drug treatments are dangerous, ineffective, and somehow not worthy

BARRIERS TO OBESITY DRUGS:ECONOMIC FACTORS
1. Third party payers, government don’t cover
2. Treatment expensive, break the bank
a. Large number of overweight/obese people
b. A high % of patients would use obesity drugs
3. Savings in future costs too remote compared to current expenses

BARRIERS TO OBESITY DRUGS: GOVERNMENT: FDA
1. Past bias of FDA personnel against obesity/ obesity drugs (quote: “Gaining weight doesn’t hurt you and losing weight doesn’t help you”)
2. Obesity drugs have been held to a different standard than drugs for other diseases (eg phen-fen debacle vs troglitazone)
3. Experience of recent obesity drugs: dexfenfluramine, sibutramine, orlistat
4. Intense political pressure on FDA

BARRIERS TO OBESITY DRUGS: GOVERNMENT: CMS
1. Recent language in Medicare/Medicaid regulations:
“Obesity is not a disease”
2. Efficacy standards for treatment apparently will be applied, in contrast to most other chronic diseases

BARRIERS TO OBESITY DRUGS
The expectations and behavior of obese people themselves:
1. Do not believe they are worthy of respect
2. Discriminate against the obese as much or more than do thin people
3. Do not bind together for action
4. Do not act as advocates for obesity

BARRIERS TO OBESITY DRUGS:LIMITED CHOICES, POOR EFFICACY
1. Only two drugs still on patent
2. Only three categories of drugs
3. Poor understanding of etiology of obesity, mechanisms of action of drugs
4. Typical weight loss with single agents only about 10% of initial body weight
5. Very limited use of combinations of drugs



26
104104
8888
9090
9292
9494
9696
9898
100100
102102
00 22 44 66 88 1010 1414 1616 1818 2020 2222
Bod
y W
eigh
t (kg
)B
ody
Wei
ght (
kg)
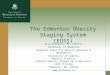
SibutramineSibutramine: 2: 2--Year EfficacyYear EfficacyWeight Loss and Weight MaintenanceWeight Loss and Weight Maintenance
Placebo + Diet & Exercise M 6Placebo + Diet & Exercise M 6--2424
SibutramineSibutramine + Diet & Exercise M 6+ Diet & Exercise M 6--2424
MonthMonth
Adapted from: James WPT, et al. Lancet. 2000;356:2119-2125.
1212 2424
SibutramineSibutramine + Diet + Diet & Exercise M 1& Exercise M 1--66


WEIGHT LOSS WITH PHENTERMINE
36 week trials:
Wt loss % Wt loss
Munro, et al -12.3 kg -13.0%
BMJ, ‘68
Steel, et al -12.0 kg -12.8%
(Practitioner, ‘73)

DRUGS FOR OBESITY:THE FUTURE

POTENTIAL FUTURE AGENTS
1. Gut peptides
2. Opioid antagonists
3. Neurotransmitter agonists & antagonists
4. Thermogenic agents
5. Growth hormone, growth factors
6. Lipid oxidizing agents
7. Nutrient partitioning agents

POTENTIAL OBESITY AGENTS
Bupropion Axokine
Topiramate Melanocortin
Zonisamide Serotonin agonists
Rimonabant Exendin-4
Glucagon-like peptide Leptin analogues
PYY 3-36 GH analogues
CCK agonists NPY antagonists
Enterostatin Beta-3 agonists
Lipid oxidizing agents Oleoyl-estrone


Topiramate: Body Weight Loss in Adults vs Treatment Duration (Months)*
3 6 12 18 24 30 36 42 48 54 600
2
4
6A
vera
ge W
eigh
t Los
s (k
g)
*N=126-833
TPM Treatment Duration (mos)

ZONISAMIDE FOR WEIGHT LOSS
16 wk, randomized trial in 60 subjects
400-600 mg/d for 16 wk, 16 wk extension
Placebo Zonisamide
16 wk wt loss (kg) 0.9 + 0.4 5.9 + 0.8
32 wk wt loss (kg) 1.5 + 0.7 9.2 + 1.7
32 wk loss of %IBW 1.8% 9.4%
% losing 5% of IBW 10% 57% (16 wk) Gadde, et al JAMA 289:1820, ‘03

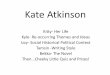
RATIONALE FOR OBESITYDRUG COMBINATIONS
1. Obesity is a chronic disease
2. Most chronic diseases are treated with drugs
3. Most chronic diseases require more than one drug
4. Combinations of drugs may have additive or synergistic effects
5. Side effects may be offset



30
32
34
36
38
40
42
44
46
Baseline Month 3 Month 6
BM
I
Body Mass Index of subjects who completed 6 months of treatment. Closed circle = Phen-fen; Open circle = Phen-flu.

THOUGHTS ON FDA GUIDANCES FOR OBESITY DRUGS
1. Obesity is a major public health problem - should obesity drugs be fast-tracked?
a. Efficacy shown by virtually all at 6 mo
b. Virtually all safety issues seen by then
2. Extended run in periods serve little use
3. If safe, modest weight loss holds promise, particularly in combination with other drugs
4. Varied indications for use are justified

RATIONAL EXPECTATIONS FOR OBESITY DRUGS
1. Current drugs are modestly effective
2. Drugs in pipeline appear to be similar in
terms of efficacy - maximum wt loss about 17%
3. Overhype by companies detrimental
4. Overcaution by FDA, others, detrimental
5. Media hasn’t always been responsible
6. General public desperate, need perspective and understanding of obesity as a disease
7. For now, long term lifestyle changes needed

OBESITY DRUGS:PROMISE FOR THE FUTURE
1. Drugs are the future of obesity treatment
2. Obesity is due to biochemical differences
3. Drugs change biochemistry
4. Surgery produces wt losses of 25%-40% of initial body weight
5. Surgery changes biochemistry
6. At least 350 drugs are in the pipeline
7. Combination treatment will be necessary
8. The future is extremely bright

AMERICAN OBESITY ASSOCIATION
A lay advocacy association dedicated to obesity
Mission:
To improve the quality of life of obese people
Contact information:
Website: obesity.org
Phone: 202-776-7711

FOR COPIES OF SLIDES OR FURTHER INFORMATION
Richard L. Atkinson, M.D.
Obetech Obesity Research Center
Virginia Biotechnology Research Park
Richmond, Virginia
804-344-5360
obesityvirus.com