Embed Size (px)
Citation preview

Biology of Human Tumors
Obesity and Fatty Pancreatic Infiltration Are RiskFactors for Pancreatic Precancerous Lesions(PanIN)Vinciane Rebours1,2, S�ebastien Gaujoux2,3, Gaspard d'Assignies4, Alain Sauvanet3,Philippe Ruszniewski1,2, Philippe L�evy1, Val�erie Paradis2,5, Pierre Bedossa2,5, andAnne Couvelard2,6
Abstract
Purpose: The roles of intravisceral and subcutaneous fat areunknown, and the prevalence of precancerous lesions in obesepatients was never evaluated. This study aims to assess thefrequency and severity of pancreatic intraepithelial neoplasia(PanIN) and to correlate pathologic findings with metabolicabnormalities, type of fat, and fatty pancreatic infiltration.
Experimental Design: Normal pancreatic tissue from surgicalspecimens was analyzed. Fatty infiltration and fibrosis in intra-and extralobular locations and PanIN lesions were assessed.General characteristics were collected: body mass index (BMI),diabetes, and tobacco intake. Liver steatosis and subcutaneousand intravisceral fat were assessed by CT scan (ImageJ software).
Results: Of note, 110 patients were included [median age, 53.8(17–85) years]. Arterial hypertension, diabetes, and tobacco intakewere found in19%,9%,and23%, respectively.MedianBMIwas24(16–37; BMI < 25: 45%, 25� 30: 24%,�30: 11%).Overall, PanIN
lesions were found in 65% (type I, II, and III PanIN in 62%, 38%,and 1%, respectively). Fibrosis and fatty pancreas (intra- andextralobular locations) were found in 1% and 24% and in 30%and 51%, respectively. A correlation was observed between PanINlesions and fatty pancreas [extralobular (0.01) and intralobular(<0.0001)], intralobularfibrosis (0.003), high BMI (P¼ 0.02), andsubcutaneous (P ¼ 0.02) and intravisceral fat (P ¼ 0.02). Thenumber of PanIN lesions was correlated with intravisceral fat (r ¼0.22, P¼ 0.04), but notwith subcutaneous fat (r¼ 0.14, P¼ 0.22).In multivariate analysis, PanIN lesions were associated with intra-lobular fibrosis [OR, 5.61; 95% confidence interval (CI), 1.18–42.99] and intralobular fat (OR, 17.86; 95% CI, 4.935–88.12).
Conclusions: Obesity (especially android obesity) and pan-creatic fatty infiltration are risk factors for pancreatic precancerouslesions. Clin Cancer Res; 21(15); 3522–8. �2015 AACR.
See related commentary by Wang et al., p. 3369
IntroductionThe role of overweight and obesity as a risk factor of pancreatic
cancer was previously debated. It is now well established that upto 20% of all cancers can be attributed to obesity (1). In epide-miologic data, a large American cohort, compassing 19-pooledprospective studies, encompassing 1.46 million white adults,confirmed that the relative risk ofmortality due to cancer increasesin obese patients who never smoked [body mass index (BMI)>30kg/m2] and was assessed to 1.34 (1.27–1.42; ref. 2). In a meta-analysis, the relation between BMI and pancreatic cancer was
confirmed, especially in women. In women, a 5 kg/m2 increase inBMI was determined as an independent risk factor of pancreaticcancer [relative risk (RR), 1.12; 95% confidence interval (CI),1.02–1.2; P ¼ 0.01; ref. 3] . Recently, in the NIH cohort, obesity,and overweight at any age were associated with increased inci-dence of pancreatic cancer, with HR ranging from 1.15 to 1.53.Moreover, a longer duration of BMI > 25 kg/m2 was significantlyassociated with pancreatic cancer (HR/10 year increment ofduration: 1.06; 95% CI, 1.05–1.32; ref. 4). This study demon-strated that adiposity at younger ages and across a lifetime isprobably a surrogate risk factor of pancreatic cancer.
However, the interpretation of these findings could be debatedregarding the lackof knowledge in thephysiopathologic role of fatand the interaction between obesity and other comorbidities. It isnow well demonstrated that obesity is associated with diabetesmellitus type II, an independent risk factor of pancreatic cancer. Astudy of 29,133 Finnish male smokers revealed that the presenceof diabetes mellitus and, independently, elevated insulin con-centrations, both showed a significant 2-fold increased risk for thesubsequent development of pancreatic cancer more than 10 yearsafter baseline. These results support the hypothesis that exposureto higher insulin concentrations and insulin resistance affects therisk for exocrine pancreatic cancer (5). Obesity as a risk factor ofpancreatic cancer could be an indirect association with a long-term evolution of diabetes. Moreover, the physiopathologic roleof fat (according to the intravisceral or subcutaneous fat location)in the pancreatic oncogenesis process is still poorly understood.
1Pancreatology Department, Beaujon Hospital, DHU Unity, AP-HP,Clichy, Paris-Diderot University, Paris, France. 2Inserm U773-CRB3,DHUUnity, Paris-DiderotUniversity, Paris, France. 3PancreaticSurgeryDepartment, Beaujon Hospital, DHU Unity, AP-HP, Clichy, Paris-Diderot University, Paris, France. 4Radiology Department, BeaujonHospital, DHU Unity, AP-HP, Clichy, Paris-Diderot University, Paris,France. 5Pathology Department, Beaujon Hospital, DHUUnity, AP-HP,Clichy, Paris-Diderot University, Paris, France. 6Pathology Depart-ment, Bichat Hospital, DHU Unity, AP-HP, Paris-Diderot University,Paris, France.
Corresponding Author: Vinciane Rebours, Pole des Maladies de l'AppareilDigestif, Service de Pancr�eatologie, INSERM U773, Hopital Beaujon, 100, bou-levard du G�en�eral Leclerc, Clichy 92110, France. Phone: 331-4087-5225; Fax: 331-4270-3784; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-14-2385
�2015 American Association for Cancer Research.
ClinicalCancerResearch
Clin Cancer Res; 21(15) August 1, 20153522
on May 11, 2019. © 2015 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 19, 2015; DOI: 10.1158/1078-0432.CCR-14-2385

The aim of this study was to characterize the frequency and theseverity of pancreatic intraepithelial neoplasia (PanIN) in patientswith fatty pancreas, to correlate pathologic findings with meta-bolic abnormalities, hepatic steatosis, tobacco intake, and distri-bution of fat infiltration (intravisceral or subcutaneous fat).
Materials and MethodsPatients
Before select normal pancreatic tissue, all consecutive patientsoperated on for benign and small neuroendocrine tumors from2008 to 2011 were selected. All patients with ductal tumors(pancreatic adenocarcinoma and intraductal pancreatic mucin-ous neoplasia) were excluded. All specimens presented well-differentiated neuroendocrine tumors, grade 1 or 2, according tothe 2010 WHO classification. An Institutional Review Board(CEERB, comit�e d'�ethique en recherche biom�edicale du Groupehospitalier universitaire Nord) approval for the study design andthe ethical measures were obtained. The ethical committeereviewed all the written consents.
Pathologic examinationThe normal pancreatic parenchyma was analyzed at least 2 cm
apart from the tumor and downstream of the tumor to minimizethe risk of chronic obstructive pancreatitis lesions. All hematox-ylin–eosin–safran-stained slides of pancreatic tissue were retro-spectively analyzed by light microscopy by two investigators(A. Couvelard and V. Rebours) for each case, both blinded tothe patient's clinical data. The total surface area of nontumoralpancreas analyzedwas calculated for each case in cm2.We selectedall blocks of tissue at least 2 cmapart from the tumor andone slideper block was taken into account. The number of blocks availableper specimen depended on the size of specimens. The thickness ofeach block varied from 2 to 3 mm.
PanIN lesions were graded according to criteria established bythe National Cancer Institute–sponsored Pancreas Cancer Think
Tank (6) into PanIN-1 (flat, papillary or micropapillary epitheliallesions with mild dysplasia), PanIN-2 (epithelial lesions withmoderate dysplasia), and PanIN-3 (epithelial lesions with highgrade dysplasia; ref. 7). The extent and distribution of fibrosis wereevaluated using the score established byKl€oppel and colleagues (8)in intra- and extralobular locations. This score (0–3)was defined asthe presence of connective tissue (0, no connective tissue; 1, milddeposits of fibrosis; 2, moderate; or 3, severe amounts of fibrosis)within the interlobular space and into the lobules. Samples with ascore >3 were considered at high degree of fibrosis. The same scorewas adapted to quantify the fat infiltration (ranging from 0 to 2).Perilobular fatty infiltration was defined as the presence of adipo-cytes within the interlobular space and was scored as follows: 0, nofatty infiltration; 1, some adipocytes; and 2, numerous adipocytesseparating the lobules. Intralobular fatty infiltrationwas scoredas0,no or rare adipocytes in some lobules; 1, scattered adipocytesamong most of the lobules; and 2, numerous adipocytes amongmost of the lobules forming clusters of more than 10 cells.
CT scan analysisWithin 4 weeks before surgery, all patients had a preoperative
multiphasic (nonenhanced, arterial, pancreatic parenchymal, andportal venous phases) multidetector CT scan performed for allpatients with a General Electric CT Light Speed VCT 64 4.3 (GEHealthcare). It included an initial nonenhanced acquisitionwith asection thickness of 5 mm, at the level of the umbilicus with thepatient in the supine position. Images were saved as DICOMimages for analysis. By way of this imaging, radiologic data wereassessed by two investigators (V. Rebours and G. d'Assignies),both blinded to clinical and pathologic data, using ImageJ free-ware (http://rsb.info.nih.gov/ij/).
The total fat area (TFA) and the visceral fat area (VFA) wereevaluated by measuring pixels with densities in the �190 to �30Hounsfield units range after delineating the total and visceralcompartments and computing the cross-sectional area of each incm2, as previously reported (9). The subcutaneous fat area (SFA)was obtained by subtracting VFA from TFA. The �190 to �30Hounsfield units range density allows tomeasure only fat, exclud-ing bone, muscle, and other intraabdominal organs such as liver,spleen, or small bowel, each having a density far higher or lower(tutorials available at http://rsbweb.nih.gov/ij/docs/examples/index.html); Fig. 1.
The liver steatosis was assessed by CT scan. The liver densitymeasurement was performed on nonenhanced slices by usingregion of interest (ROI) as large and homogeneous as possible,placed on the liver for three measurements (one in the left lobeand two in the right lobe), avoiding liver vessels and artifact zones.Liver steatosis was assessed by averaging the three ROI measure-ments and considered when the mean was >48 Hounsfield units,as reported previously (10).
Data collectionClinical, radiologic, and pathologic data were obtained from a
prospective database with additional retrospective medical recordsreviewed when necessary. Data recorded included: (i) preoperativeclinical characteristics (age at surgery, BMI, diabetes mellitus,smoking status, and arterial hypertension); (ii) radiologic data(liver steatosis assessment, the subcutaneous, and intravisceral fatarea (percentage of the total area); and (iii) the pathologic features(number and grade of PanIN lesions,fibrosis, and fat infiltration inintra- and extra-pancreatic lobular locations).
Translational Relevance
Obesity is now well known as a risk factor of pancreaticcancer. Adipose tissue, particularly visceral fat, is known toplay a key role in themetabolic dysfunctions as a consequenceof obesity. In addition, obesity causes fat infiltration of organs.Pancreatic precancerous lesions (PanIN) are rare in normalpancreatic tissue and are of a low grade of dysplasia. In thisstudy, we assessed for the first time the presence and theseverity of PanIN lesions according to obesity and fatty pan-creatic infiltration in a large series of patients. Data wereassessed by morphological and pathological analyses. Theselesions were frequent and severe, and probably account for theincreasing incidence of pancreatic cancer in obese patients. Theclinical consequences of these findings should be consideredwithin the framework of the current debate over obesity andpancreatic cancer. The association between android obesityand fatty pancreatic infiltration should be considered as amajor risk factor of pancreatic cancer. Among individuals athigh risk for pancreatic cancer, a more cautious screeningprobably should be performed in obese patients with fattypancreas.
Fatty Pancreatic Infiltration and PanIN Lesions
www.aacrjournals.org Clin Cancer Res; 21(15) August 1, 2015 3523
on May 11, 2019. © 2015 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 19, 2015; DOI: 10.1158/1078-0432.CCR-14-2385

Clinical definitionsSmoking status was categorized as smokers if patients had
smoked for at least 2 years (current and ex-daily smokers) andnonsmokers. The number of cigarettes smoked per day andduration of smoking were recorded and expressed as pack-years(pack-years of smoking were calculated at the baseline examina-tion as number of cigarettes per daymultiplied bynumber of yearsof smoking divided by 20).
The BMI was defined as weight (kg) divided by height squared(m2). Overweight and obesity were defined as BMI � 25 to 29.9kg/m2 and BMI � 30 kg/m2, respectively.
Diabetes mellitus according to WHO criteria was defined as awhole venous blood fasting glucose concentration recorded�126mg/dL (6.99mmol/L) at least two determinations or >11mmol/L,post-prandially, at one determination. Insulin requirement wasdefined by the inefficacy of adequate diet and oral drugs inpreventing hyperglycemias.
Statistical analysisGeneral characteristics were expressed as median and range or
percentages. Comparisons of general characteristics, clinical fea-tures, morphologic characteristics, and pathologic data were
performed using the Kruskall–Wallis test for continuous data andthe c2 test or the Fisher exact test for categorical data. A Spearmancorrelation coefficient was used to search for correlation betweencontinuous variables. A multidimensional analysis was per-formed using a logistic regression analysis to search for risk factorsof PanIN lesions. The stepwise selection optionwas used. P valuesbelow 0.20 were considered as significant as level of entry in themodel. Datawere analyzedwith the SAS 9.1 statistical software forWindows (SAS Institute Inc.). All statistical tests were two-sided.The critical level of statistical significance was set at a P valueof <0.05.
ResultsCharacteristics of the patients and indications for pancreaticsurgery
One hundred and ten consecutive patients were includedbetween 2008 and 2011. Women represented 57% (n ¼ 63) ofthe patients. All patients were operated on for well-differentiatedneuroendocrine tumors, grade 1 (n¼ 69, 63%) or grade 2 (n¼ 41,37%). Surgical procedure was a Whipple procedure (n ¼ 61,55%), left pancreatectomy (n ¼ 30, 28%), or median
A1
B1
C1 C2
B2
A2
Figure 1.Assessment of the total, visceral, andsubcutaneous fat using the ImageJ software (A,thin patient; B and C, fatty patient). A1–C1,nonenhanced CT scanwith a section thickness of5 mm, at the level of the umbilicus with thepatient in the supine position. A2–C2, Measuringpixels with densities in the range of�190 to�30Hounsfield units (in red on the figure) todelineate the subcutaneous and visceralcompartments. B2, delineation of the TFA. C2,delineation of the VFA. SFA is obtained bysubtracting VFA from TFA.
Rebours et al.
Clin Cancer Res; 21(15) August 1, 2015 Clinical Cancer Research3524
on May 11, 2019. © 2015 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 19, 2015; DOI: 10.1158/1078-0432.CCR-14-2385
pancreatectomy (n ¼ 19, 17%). The median age at surgery was53.8 (17–85) years. Arterial hypertension, diabetes, and tobaccointake were found in 19% (n ¼ 19), 9% (n ¼ 10), and 27% (n ¼25), respectively. The median tobacco consumption was 20 (1–60) pack-years. The median BMI was 24 [16–37; BMI < 25: 56%(n ¼ 50), 25 � 30: 30% (n ¼ 27), �30: 13% (n ¼ 12)].
Pathologic dataThe median surface of pancreatic tissue, evaluated per speci-
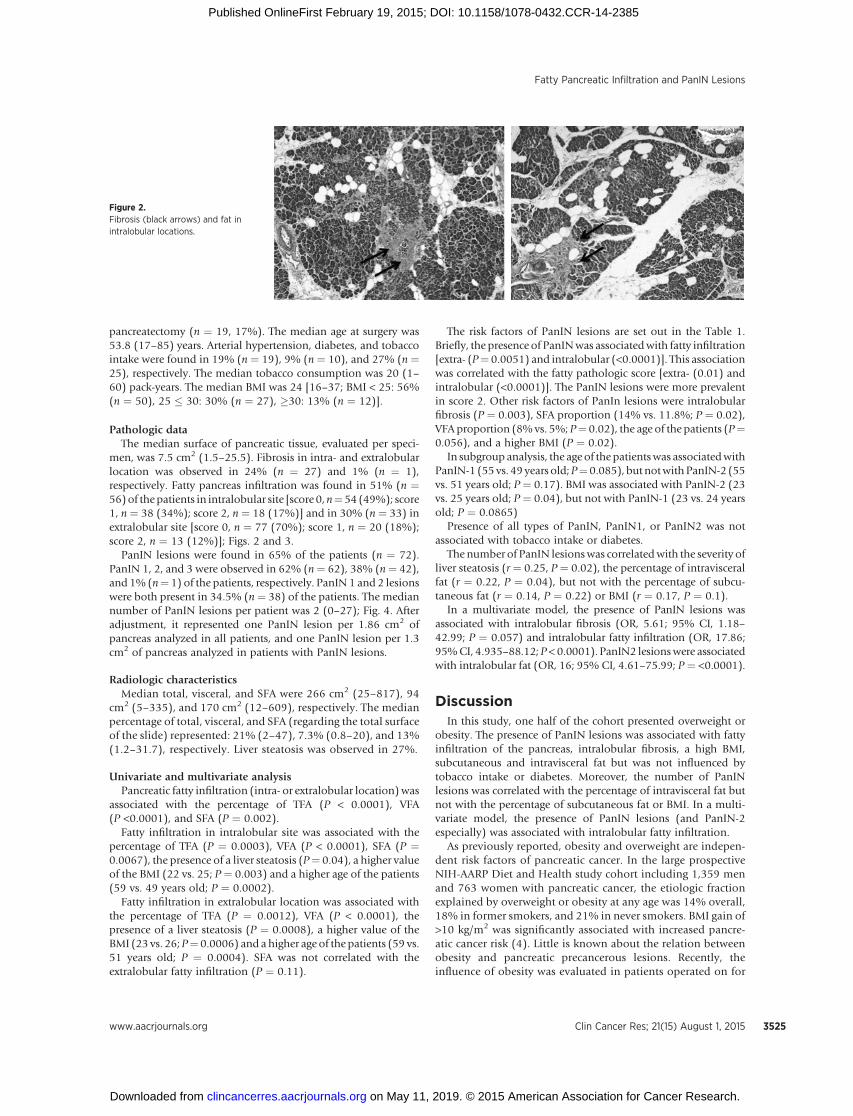
men, was 7.5 cm2 (1.5–25.5). Fibrosis in intra- and extralobularlocation was observed in 24% (n ¼ 27) and 1% (n ¼ 1),respectively. Fatty pancreas infiltration was found in 51% (n ¼56)of thepatients in intralobular site [score 0,n¼54 (49%); score1, n ¼ 38 (34%); score 2, n ¼ 18 (17%)] and in 30% (n ¼ 33) inextralobular site [score 0, n ¼ 77 (70%); score 1, n ¼ 20 (18%);score 2, n ¼ 13 (12%)]; Figs. 2 and 3.
PanIN lesions were found in 65% of the patients (n ¼ 72).PanIN 1, 2, and 3 were observed in 62% (n¼ 62), 38% (n¼ 42),and 1% (n¼ 1) of the patients, respectively. PanIN 1 and 2 lesionswere both present in 34.5% (n ¼ 38) of the patients. The mediannumber of PanIN lesions per patient was 2 (0–27); Fig. 4. Afteradjustment, it represented one PanIN lesion per 1.86 cm2 ofpancreas analyzed in all patients, and one PanIN lesion per 1.3cm2 of pancreas analyzed in patients with PanIN lesions.
Radiologic characteristicsMedian total, visceral, and SFA were 266 cm2 (25–817), 94
cm2 (5–335), and 170 cm2 (12–609), respectively. The medianpercentage of total, visceral, and SFA (regarding the total surfaceof the slide) represented: 21% (2–47), 7.3% (0.8–20), and 13%(1.2–31.7), respectively. Liver steatosis was observed in 27%.
Univariate and multivariate analysisPancreatic fatty infiltration (intra- or extralobular location)was
associated with the percentage of TFA (P < 0.0001), VFA(P <0.0001), and SFA (P ¼ 0.002).
Fatty infiltration in intralobular site was associated with thepercentage of TFA (P ¼ 0.0003), VFA (P < 0.0001), SFA (P ¼0.0067), the presence of a liver steatosis (P¼ 0.04), a higher valueof the BMI (22 vs. 25; P ¼ 0.003) and a higher age of the patients(59 vs. 49 years old; P ¼ 0.0002).
Fatty infiltration in extralobular location was associated withthe percentage of TFA (P ¼ 0.0012), VFA (P < 0.0001), thepresence of a liver steatosis (P ¼ 0.0008), a higher value of theBMI (23 vs. 26; P¼ 0.0006) and a higher age of the patients (59 vs.51 years old; P ¼ 0.0004). SFA was not correlated with theextralobular fatty infiltration (P ¼ 0.11).
The risk factors of PanIN lesions are set out in the Table 1.Briefly, the presence of PanINwas associatedwith fatty infiltration[extra- (P¼ 0.0051) and intralobular (<0.0001)]. This associationwas correlated with the fatty pathologic score [extra- (0.01) andintralobular (<0.0001)]. The PanIN lesions were more prevalentin score 2. Other risk factors of PanIn lesions were intralobularfibrosis (P ¼ 0.003), SFA proportion (14% vs. 11.8%; P ¼ 0.02),VFA proportion (8%vs. 5%; P¼ 0.02), the age of the patients (P¼0.056), and a higher BMI (P ¼ 0.02).
In subgroup analysis, the age of the patientswas associatedwithPanIN-1 (55 vs. 49 years old;P¼0.085), but notwithPanIN-2 (55vs. 51 years old; P ¼ 0.17). BMI was associated with PanIN-2 (23vs. 25 years old; P ¼ 0.04), but not with PanIN-1 (23 vs. 24 yearsold; P ¼ 0.0865)
Presence of all types of PanIN, PanIN1, or PanIN2 was notassociated with tobacco intake or diabetes.
The number of PanIN lesionswas correlatedwith the severity ofliver steatosis (r ¼ 0.25, P ¼ 0.02), the percentage of intravisceralfat (r ¼ 0.22, P ¼ 0.04), but not with the percentage of subcu-taneous fat (r ¼ 0.14, P ¼ 0.22) or BMI (r ¼ 0.17, P ¼ 0.1).
In a multivariate model, the presence of PanIN lesions wasassociated with intralobular fibrosis (OR, 5.61; 95% CI, 1.18–42.99; P ¼ 0.057) and intralobular fatty infiltration (OR, 17.86;95%CI, 4.935–88.12; P < 0.0001). PanIN2 lesionswere associatedwith intralobular fat (OR, 16; 95% CI, 4.61–75.99; P ¼ <0.0001).
DiscussionIn this study, one half of the cohort presented overweight or
obesity. The presence of PanIN lesions was associated with fattyinfiltration of the pancreas, intralobular fibrosis, a high BMI,subcutaneous and intravisceral fat but was not influenced bytobacco intake or diabetes. Moreover, the number of PanINlesions was correlated with the percentage of intravisceral fat butnot with the percentage of subcutaneous fat or BMI. In a multi-variate model, the presence of PanIN lesions (and PanIN-2especially) was associated with intralobular fatty infiltration.
As previously reported, obesity and overweight are indepen-dent risk factors of pancreatic cancer. In the large prospectiveNIH-AARP Diet and Health study cohort including 1,359 menand 763 women with pancreatic cancer, the etiologic fractionexplained by overweight or obesity at any age was 14% overall,18% in former smokers, and 21% in never smokers. BMI gain of>10 kg/m2 was significantly associated with increased pancre-atic cancer risk (4). Little is known about the relation betweenobesity and pancreatic precancerous lesions. Recently, theinfluence of obesity was evaluated in patients operated on for
Figure 2.Fibrosis (black arrows) and fat inintralobular locations.
Fatty Pancreatic Infiltration and PanIN Lesions
www.aacrjournals.org Clin Cancer Res; 21(15) August 1, 2015 3525
on May 11, 2019. © 2015 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 19, 2015; DOI: 10.1158/1078-0432.CCR-14-2385

intraductal papillary mucinous neoplasm (IPMN). High-gradelesions were mainly found in obese patients. Of 254 patientswith a BMI of <35 kg/m2, 30% had malignant IPMN versus50% in patients with BMI > 35 kg/m2 (P ¼ 0.08). In branch-duct IPMN, patients with a BMI < 35 kg/m2 had 12% ofmalignant IPMN compared with 46% in severely obese patients(P¼ 0.01). Alternatively, in main-duct IPMN, no difference wasfound in the malignancy rate (11). However, the way by whichfat influence the risk of cancer is still poorly understood. Isobesity the indirect reflect of an associated diabetes or glucoseintolerance or is there a direct role due chronic inflammation.In an in vivo model of lean and obese mice inoculated with
murine pancreatic cancer cells, obese mice developed largertumors, and significantly more developed metastases. Theserum adiponectin concentration correlated negatively andserum insulin concentration correlated positively with tumorproliferation. The intratumoral adipocyte mass in tumors fromobese mice was significantly greater than that in lean mice.These data could suggest that both insulin resistance andaltered adipokine milieu could lead directly to changes of themicroenvironment (12). In our study, the main risk factor ofPanIN lesions in univariate and multivariate model was thefatty infiltration, especially in intralobular location (OR, 17.86;95% CI, 4.935–88.12). This risk factor was independent of theage of the patients and the presence of diabetes. Several studieswell demonstrated that the prevalence and incidence of PanINlesions were higher in cases of chronic pancreatitis comparedwith normal pancreas. Except in cases of hereditary pancreatitis,in all studies, all the lesions were of low grade of dysplasia;PanIN-2 lesions were exceptionally described and PanIn-3,never (13–16). In this series, PanIN-2 lesions were frequentlyobserved (38% of the patients) and the main and independentrisk factor was intralobular fat (OR, 16; 95% CI, 4.61–75.99).In previous publications, it was demonstrated that PanINlesions could be associated with a lobulocentric atrophy, sur-rounding the lesions, and the tissue could be replaced by fattissue. So the role of PanIN lesions could be debated, if they aredue or the cause of fatty changes. In this study, we found thatfatty infiltration was not specifically localized around PanINlesions. This observation suggested that PanIN lesions were dueto fatty changes and did not promote the fat infiltration. Thissuggests a possible role of this type of fatty infiltration in theoncogenic process and points out the possible local role of fatin close contact with PanIN. Moreover, our study highlights thespecific role of the intravisceral fat correlated with the numberof PanIN lesions.
Obesity is associated with chronic low-grade inflammation(also called meta-inflammation), characterized by abnormalproinflammatory cytokine production, immune activation, dis-ruption in autophagy, promotion of endoplasmic reticulumstress, mitochondrial dysfunction, and increased inflammatorysignaling. This chronic inflammation is more pronounced inthe visceral than in the subcutaneous fat compartment. Obesityincreases the size of adipocytes, leading to their necrosis and asignificant accumulation of activated macrophages. The inflam-matory mediators, including IL6, IL1, and TNFa, have beenimplicated in development of insulin resistance and their levels
Figure 4.Multiple PanIN-1 lesions associated with intralobular fatty infiltration.
A
B
C
Figure 3.Fatty infiltration in an intralobular location (A and B) and an extralobularsite (C).
Rebours et al.
Clin Cancer Res; 21(15) August 1, 2015 Clinical Cancer Research3526
on May 11, 2019. © 2015 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 19, 2015; DOI: 10.1158/1078-0432.CCR-14-2385

increase within adipose tissue. This inflammation is accom-panied by an upregulation of anti-inflammatory factors, suchas IL10, IL4, and TGFb (17–22). The inflammatory mediatorssecreted by macrophages act not only locally, in a paracrinemanner, but also contribute to general inflammation. Obesityincreases levels of the proinflammatory hormone leptin anddecreases its anti-inflammatory counterpart, adiponectin (23).These data probably explain the high prevalence of intralob-ular fibrosis in our study, correlated with obesity and fatinfiltration. Moreover, it highlighted our findings regardingthe association of PanIN lesions and predominant intravisceralobesity.
This study supports epidemiologic evidence that obesity is anindependent risk factor of pancreatic cancer and suggests thatfatty infiltration per se plays a role in pancreatic oncogenesis.Obesity, and especially android obesity with increased intra-visceral fat, is a risk factor for precancerous lesions of thepancreas.
Disclosure of Potential Conflicts of InterestP. L�evy is a consultant/advisory board member for Abbvie and Mayoly
Splinder. No potential conflicts of interest were disclosed by the other authors.
Authors' ContributionsConception and design: V. Rebours, S. Gaujoux, P. Ruszniewski, P. L�evy,P. Bedossa, A. CouvelardDevelopment of methodology: V. Rebours, S. Gaujoux, G. d'Assignies,P. Ruszniewski, A. CouvelardAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): V. Rebours, S. Gaujoux, G. d'Assignies, A. Sauvanet,P. Ruszniewski, A. CouvelardAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): V. Rebours, S. Gaujoux, G. d'Assignies, A. Sauvanet,P. Ruszniewski, A. CouvelardWriting, review, and/or revision of the manuscript: V. Rebours, S. Gaujoux,A. Sauvanet, P. Ruszniewski, P. L�evy, A. CouvelardAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): V. Rebours, A. CouvelardStudy supervision: V. Rebours, P. L�evy, V. Paradis, A. Couvelard
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received September 14, 2014; revised January 19, 2015; accepted January 21,2015; published OnlineFirst February 19, 2015.
References1. Wolin KY, Carson K, Colditz GA. Obesity and cancer. Oncologist 2013;
15:556–65.2. Berrington de Gonzalez A, Hartge P, Cerhan JR, Flint AJ, Hannan L, Mac
Innis RJ, et al. Body-mass index and mortality among 1.46 million whiteadults. N Engl J Med 2010;363:2211–9.
3. Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M. Body-mass indexand incidence of cancer: a systematic review and meta-analysis of prospec-tive observational studies. Lancet 2008;371:569–78.
4. Stolzenberg-Solomon RZ, Schairer C, Moore S, Hollenbeck A, Silver-man DT. Lifetime adiposity and risk of pancreatic cancer in the NIH-AARP Diet and Health Study cohort. Am J Clin Nutr 2013;98:1057–65.
5. Stolzenberg-Solomon RZ, Graubard BI, Chari S, Limburg P, Taylor PR,Virtamo J, et al. Insulin, glucose, insulin resistance, and pancreatic cancer inmale smokers. JAMA 2005;294:2872–8.
6. Kern S, Hruban R, Hollingsworth MA, Brand R, Adrian TE, Jaffee E, et al. Awhite paper: the product of a pancreas cancer think tank. Cancer Res2001;61:4923–32.
7. Hruban RH, Takaori K, KlimstraDS, AdsayNV, Albores-Saavedra J, BiankinAV, et al. An illustrated consensus on the classification of pancreaticintraepithelial neoplasia and intraductal papillary mucinous neoplasms.Am J Surg Pathol 2004;28:977–87.
8. Kl€oppel G, Maillet B. Pseudocysts in chronic pancreatitis: a morphologicalanalysis of 57 resection specimens and 9 autopsy pancreata. Pancreas1991;6:266–74.
9. Guiu B, Petit JM, Bonnetain F, Ladoire S, Guiu S, Cercueil JP, et al. Visceralfat area is an independent predictive biomarker of outcome after first-linebevacizumab-based treatment in metastatic colorectal cancer. Gut 2010;59:341–7.
10. Pickhardt PJ, Park SH, Hahn L, Lee SG, Bae KT, Yu ES. Specificity ofunenhanced CT for non-invasive diagnosis of hepatic steatosis: implica-tions for the investigation of the natural history of incidental steatosis. EurRadiol 2012;22:1075–82.
11. Sturm EC, Roch AM, Shaffer KM, Schmidt CM II, Lee SJ, Zyromski NJ, et al.Obesity increases malignant risk in patients with branch-duct intraductalpapillary mucinous neoplasm. Surgery 2013;154:803–8.
12. Zyromski NJ, Mathur A, Pitt HA, Wade TE, Wang S, Nakshatri P, et al.Obesity potentiates the growth and dissemination of pancreatic cancer.Surgery 2009;146:258–63.
13. Volkholz H, Stolte M, Becker V. Epithelial dysplasias in chronic pancrea-titis. Virchows Arch A Pathol Anat Histol 1982;396:331–49.
14. Gerdes B, RamaswamyA,KerstingM, ErnstM, Lang S, SchuermannM , et al.p16(INK4a) alterations in chronic pancreatitis-indicator for high-risklesions for pancreatic cancer. Surgery 2001;129:490–7.
Table 1. Risk factors of all grade PanIN lesions: Univariate analysis
PanIN lesions (N ¼ 72) No PanIN lesions (N ¼ 38) P
Tobacco consumption, n (%)a 17 (24) 8 (21) NSDiabetes mellitus, n (%)a 8 (11) 2 (5) NSBMIb 25 (16–37) 22 (17–32) 0.02Age at surgery, yb 55 (19–77) 49 (16–86) 0.056Extralobular fatty infiltration, n (%)a 28 (39) 5 (13) 0.0051Intralobular fatty infiltration, n (%)a 51 (71) 5 (13) <0.0001Intralobular fibrosis, n (%)a 24 (33) 3 (8) 0.003Extralobular fibrosis, n (%)a 1 (1) 0 NSSFA proportion (%)b 14% (1.3–32) 11.8% (1.2–27) 0.02VFA proportion (%)b 8% (0.8–20) 5% (1.4–15) 0.02TFA proportion (%)b 25% (2–47) 15.7% (3.7–42) 0.007Liver steatosis, n (%)a 23 (32) 7 (18) 0.08
Abbreviation: NS, nonsignificant.aResults are expressed as percentage.bMedian and (range).
www.aacrjournals.org Clin Cancer Res; 21(15) August 1, 2015 3527
Fatty Pancreatic Infiltration and PanIN Lesions
on May 11, 2019. © 2015 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 19, 2015; DOI: 10.1158/1078-0432.CCR-14-2385
15. L€uttges J, Diederichs A, Menke MA, Vogel I, Kremer B, Kl€oppel G. Ductallesions in patients with chronic pancreatitis show K-ras mutations in afrequency similar to that in the normal pancreas and lack nuclear immu-noreactivity for p53. Cancer 2000;88:2495–504.
16. Rebours V, L�evy P, Mosnier JF, Scoazec JY, Soubeyrand MS, Fl�ejou JF, et al.Pathology analysis reveals that dysplastic pancreatic ductal lesions arefrequent in patients with hereditary pancreatitis. Clin Gastroenterol Hepa-tol 2010;8:206–12.
17. Cinti S, Mitchell G, Barbatelli G, Murano I, Ceresi E, Faloia E, et al.Adipocyte death defines macrophage localization and function in adiposetissue of obese mice and humans. J Lipid Res 2005;46:2347–55.
18. Strissel KJ, Stancheva Z, Miyoshi H, Perfield JW II, DeFuria J, Jick Z, et al.Adipocyte death, adipose tissue remodeling, and obesity complications.Diabetes 2007;56:2910–8.
19. Olefsky JM, Glass CK. Macrophages, inflammation, and insulin resistance.Annu Rev Physiol 2010;72:219–46.
20. Alem�an JO, Eusebi LH, Ricciardiello L, Patidar K, Sanyal AJ, Holt PR.Mechanisms of obesity-induced gastrointestinal neoplasia. Gastroenterol-ogy 2014;146:357–73.
21. Weisberg SP, McCann D, Desai M, Rosenbaum M, Leibel RL, Ferrante AWJr. Obesity is associated with macrophage accumulation in adipose tissue.J Clin Invest 2003;112:1796–808.
22. Johnson AR, Milner JJ, Makowski L. The inflammation highway: metab-olism accelerates inflammatory traffic in obesity. Immunol Rev 2012;249:218–38.
23. Gukovsky I, Li N, Todoric J, Gukovskaya A, Karin M. Inflammation,autophagy, and obesity: common features in the pathogenesis of pancre-atitis and pancreatic cancer. Gastroenterology 2013;144:1199–209.
Clin Cancer Res; 21(15) August 1, 2015 Clinical Cancer Research3528
Rebours et al.
on May 11, 2019. © 2015 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 19, 2015; DOI: 10.1158/1078-0432.CCR-14-2385

2015;21:3522-3528. Published OnlineFirst February 19, 2015.Clin Cancer Res Vinciane Rebours, Sébastien Gaujoux, Gaspard d'Assignies, et al. Pancreatic Precancerous Lesions (PanIN)Obesity and Fatty Pancreatic Infiltration Are Risk Factors for
Updated version
10.1158/1078-0432.CCR-14-2385doi:
Access the most recent version of this article at:
Cited articles
http://clincancerres.aacrjournals.org/content/21/15/3522.full#ref-list-1
This article cites 23 articles, 5 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/21/15/3522.full#related-urls
This article has been cited by 5 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/21/15/3522To request permission to re-use all or part of this article, use this link
on May 11, 2019. © 2015 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 19, 2015; DOI: 10.1158/1078-0432.CCR-14-2385





























