Embed Size (px)
Citation preview

09.12.2011 NYSORA - The New York School of Regional Anesthesia - Ankle Block
1/7nysora.com/peripheral_nerve_blocks/…/3035-ankle_block.html?print
Ankle Block
01/03/2009 04:33:00
Copyright NYSORA © 1996, 2008 NYSORA.com
Loading Image...
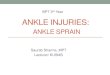
Ankle BlockAn ankleblock isessentially ablock of fourbranches ofthe sciaticnerve (deepandsuperficialperoneal,tibial andsural nerves)and onecutaneousbranch of thefemoral nerve(saphenousnerve).
TABLE OF CONTENTS (click here to expand)
OverviewGeneral ConsiderationsRegional Anesthesia AnatomyDistribution of AnesthesiaPatient PositioningEquipmentLandmarksTechniqueChoice of Local AnestheticBlock Dynamics and Perioperative ManagementComplications and How to Avoid Them
Overview
Indications: Surgery on foot and toesNerves:Two deep nerves: Posterior tibial, deep peronealThree superficial nerves: superficial peroneal, sural, saphenousNever use an epinephrine-containing local anesthetic
Local anesthetic: 6 mL per nerve

09.12.2011 NYSORA - The New York School of Regional Anesthesia - Ankle Block
2/7nysora.com/peripheral_nerve_blocks/…/3035-ankle_block.html?print
Local anesthetic: 6 mL per nerveComplexity level: Basic
General considerations
An ankle block is essentially a block of four branches of thesciatic nerve (deep and superficial peroneal, tibial and suralnerves) and one cutaneous branch of the femoral nerve (saphe-nous nerve). An ankle block is a basic, peripheral nerve blocktechnique. It is simple to perform, essentially devoid of systemiccomplications, and highly effective for a wide variety ofprocedures on the foot and toes. As such, this technique shouldbe in the armamentarium of every anesthesiologist. In ourinstitution, an ankle block is most commonly used in podiatrysurgery and foot and toe debridement or amputation.
Regional anesthesia anatomyWith exception of the saphenous nerve (sensory branch of the femoralnerve), an ankle block is essentially a block of the terminal branches ofthe sciatic nerve. It is useful to think of the ankle block as the block oftwo deep nerves (posterior tibial and deep peroneal nerves) and threesuperficial nerves (saphenous, sural and superficial peroneal). Thisconcept is crucial for the success of the block, because the two deepnerves are anesthetized by injecting local anesthetic underneath thesuperficial fascia, whereas the three superficial nerves are anesthetizedby a simple subcutaneous injection of local anesthetic.Common peroneal nerveThe common peroneal (lateral popliteal) nerve separates from the tibialnerve (L4-5 and S1-2) and descends along the tendon of the bicepsfemoris muscle and around the neck of the fibula. Just below the head ofthe fibula, the common peroneal nerve divides into its terminalbranches: the deep peroneal and superficial peroneal nerves. Theperoneus longus muscle covers both nerves.Deep peroneal nerveThe deep peroneal nerve runs downward below the layers of the peroneus longus, extensordigitorum longus, and extensor hallucis longus muscles to the front of the leg. (Figure 2) At theankle level, the nerve lies anterior to the tibia and the interoseeous membrane and close to theanterior tibial artery. It is usually "sandwiched" between the tendons of the anterior tibial andextensor digitorum longus muscles. At this point, the nerve divides into two terminal branches forthe foot: the medial and the lateral branches. The medial branch passes over the dorsum of thefoot, along the medial side of the dorsalis pedis artery, to the first interosseous space, where itdivides into two dorsal digital branches for the nerve supply to the first web space between the bigtoe and the second toe. The lateral branch of the deep peroneal nerve is directed anterolaterally,penetrates and innervates the extensor digitorum brevis muscle, and terminates as the second,third, and fourth dorsal interosseous nerves. These branches provide the nerve supply to thetarsometatarsal, metatarsophalangeal, and interphalageal joints of the lesser toes.Superficial peroneal nerve
The superficial peroneal nerve (also called the musculocutanous nerve ofthe leg) is a branch of the common peroneal nerve. The superficialperoneal nerve gives muscular branches to the peroneus longus andbrevis muscles. After piercing the deep fascia covering the muscles, the

09.12.2011 NYSORA - The New York School of Regional Anesthesia - Ankle Block
3/7nysora.com/peripheral_nerve_blocks/…/3035-ankle_block.html?print
brevis muscles. After piercing the deep fascia covering the muscles, thenerve eventually emerges from the anterolateral compartment of thelower part of the leg and surfaces from beneath the fascia 5-10 cmabove the lateral malleolus. At this point, the nerve divides into terminalcutaneous branches: the medial and lateral dorsal cutaneous nerves.These branches carry sensory innervation to the dorsum of the foot andcommunicate with the saphenous nerve medially, with deep peronealnerve in the first web space and sural nerve on the lateral aspect of thefoot.Tibial nerve
The tibial nerve (medial popliteal orposterior tibial nerve) separates fromthe common popliteal nerve atvarious distances from the poplitealfossa crease and joins the tibial arterybehind the knee joint. The nerve runsdistally in the thick neurovascular fascia and emerges at theinferior third of the leg, from beneath the soleus andgastrocnemius muscles on the medial border of the Achillestendon. At the level of the medial malleolus, the tibial nerve iscovered by the superficial and deep fasciae of the leg. It ispositioned laterally and posteriorly to the posterior tibial artery,
and midway between the posterior aspect of the medial malleolus and posterior aspect of theAchilles tendon. Just beneath the malleolus, the nerve divides into lateral and medial plantarnerves. The posterior tibial nerve provides cutaneous, articular, and vascular branches to the anklejoint, medial malleolus, inner aspect of the heel, and Achilles tendon. It also carries the branchesto the skin, subcutanous tissue, muscles, and bones of the sole.Sural nerve
The sural nerve is a sensory nerve formed by the union of themedial sural nerve - a branch of the tibial nerve - and lateralsural nerve, a branch of the common peroneal nerve. The suralnerve courses between the heads of the gastrocnemius muscleand after piercing the fascia covering the muscles, emerges onthe lateral aspect of the Achilles tendon, 10 to 15 cm above thelateral mallelus. After giving lateral calcaneal branches to theheel, the sural nerve descends 1-1.5 cm behind the lateralmalleolus, anterolateral to the short saphenous vein and on thesurface of the fascia covering the muscles and tendons. At thislevel, the nerve supplies the lateral malleolus, Achilles tendon,and the ankle joint. The sural nerve continues on the lateral
aspect of the foot supplying innervation to the skin, subcutaneous tissue, fourth interosseousspace, and sensory innervation of the fifth toe.Saphenous nerveThe saphenous nerve is a terminal cutaneous branch (branches) of the femoral nerve. Its course isin the subcutaneous tissue of the skin on medial aspect of the ankle and foot.TIP: All superficial (cutaneous) nerves of the foot should be thought of as a neuronal network,rather than single strings of nerves with a well-defined and consistent anatomic position.
Distribution of anesthesia
An ankle block results in anesthesia of the foot. The proximal extension of the blockade is to thelevel at which the blocks are performed. However, it should be noted that an ankle block does notresult in anesthesia of the ankle itself. The more proximal branches of the tibial and peronealnerves provide innervation to the deep structures of the ankle joint (see "Anatomy"). Cutaneousinnervation of the foot is provided by three superficial nerves (saphenous, sural, superficialperoneal). The two deep nerves (tibial, deep peroneal) confer anesthesia to the deep structures,bones, and cutaneous coverage of the sole and web between the first and second toes.

09.12.2011 NYSORA - The New York School of Regional Anesthesia - Ankle Block
4/7nysora.com/peripheral_nerve_blocks/…/3035-ankle_block.html?print
Patient positioning
The patient is in the supine position with the foot resting on a foot stand.TIPSPosition the foot on a footrest so that an access to all nerves to beblocked is maintained.Walk from one side of the foot to the other while performing the blockprocedure instead of bending and leaning to reach the opposite side.
Equipment
A standard regional anesthesia tray is prepared with thefollowing equipment:Sterile towels and 4"x4" gauze packsThree 10-mL syringes with local anestheticSterile gloves, marking pen, and surface electrodeOne 1½" 25-gauge needle
LandmarksThe deep peroneal nerve is located immediately lateral to the tendon ofthe extensor hallucis longus muscle (between extensor hallucis longusand extensor digitorum longus). The pulse of the anterior tibial artery(dorsalis pedis) can be felt at this location; the nerve is immediatelylateral to the artery.TIP: This landmark is easily palpated and can be accentuated by askingthe patient to dorsiflex the foot or toes.The posterior tibial nerve is located just behind and distal to the medialmalleolus. The pulse of the posterior tibial artery can be felt at thislocation; the nerve is just posterior to the artery.The superficial peroneal, sural, and saphenous nerves are located in thesubcutaneous tissue alongside a circular line that stretches from thelateral aspect of the Achilles tendon across the lateral malleolus, anterioraspect of the foot, and medial malleolus to the medial aspect of theAchilles tendon.TIP: These nerves branch out and anastomose extensively and do not
have a single, consistently positioned nerve trunk that can be anesthetized by a single, preciseinjection, as is often depicted in various regional anesthesiology books.
Technique
The anesthesiologist needs to change his or her position from lateral to

09.12.2011 NYSORA - The New York School of Regional Anesthesia - Ankle Block
5/7nysora.com/peripheral_nerve_blocks/…/3035-ankle_block.html?print
The anesthesiologist needs to change his or her position from lateral tothe medial side of the foot to accomplish blockade of all five nerves. Acontrolled or regular syringe can be used. It makes sense to begin thisprocedure with blocks of the two deep nerves because subcutaneousinjections for the superficial blocks will inevitably deform the anatomy.Before beginning the procedure, the entire foot should be cleansed witha disinfectant.Deep peroneal blockThe finger of the palpating hand is positioned in the groove just lateral tothe extensor hallucis longus. The needle is inserted under the skin andadvanced until stopped by the bone. At this point, the needle iswithdrawn back 1-2 mm and 2-3 mL of local anesthetic is injected.
TIPSDeep peroneal block is a "blind" injection of local anesthetic. Instead of relying on a singleinjection, a "fan" technique is recommended to increase the success rate. The needle is withdrawn
back to the skin, redirected 30o laterally, and advanced again to contact the bone. After pulingback 1-2 mm off the bone, an additional 2 mL of local anesthetic is injected. A similar procedure isrepeated with a medial redirection of the needle.Mentally visualize the plane of the needle insertion for the deep peroneal and posterior tibialnerves. Do not move the palpating finger during the injection to ensure proper needle reinsertions
(30o lateral/medial).
Posterior Tibial BlockPosterior tibial nerve is anesthetized by injecting local anesthetic just behind the medial malleolus.Similar to the deep peroneal nerve, its position is deep to the superficial fascia. With theanesthesiologist facing the medial aspect of the foot, the needle is introduced in the groove behindthe medial malleolus and advanced until contact with the bone is felt. At this point, the needle iswithdrawn back 1-2 mm and 2-3 mL of local anesthetic is injected.

09.12.2011 NYSORA - The New York School of Regional Anesthesia - Ankle Block
6/7nysora.com/peripheral_nerve_blocks/…/3035-ankle_block.html?print
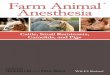
Superficial peroneal nerve isblocked by subcutaneousinfiltration of local anesthetic overthe lateral aspect of the foot.
TIPSimilar to the technique used for deepperoneal nerve, a "fan" techniqueshould be used to increase thesuccess rate. The needle is pulledback to the skin and two additionalboluses of 2 mL of local anesthetic areinjected after lateral and medialneedle reinsertions.
Block of the Superficial Peroneal, Sural and Saphenous NervesThese three nerves are superficial cutaneous extensions of the sciatic and femoral nerve. Sincethey are positioned superficial to the deep fascia, a simple injection of local anesthetic in theterritory in which they descend to the distal foot is adequate to achieve their blockade. Blockade ofall three nerves is accomplished using a simple circumferential injection of local anestheticsubcutaneously.The sural nerve is a sensory nerve formed by the union of themedial sural nerve - a branch of the tibial nerve - and lateralsural nerve a branch of the common peroneal nerve. The suralnerve courses between the heads of the gastrocnemius muscleand after piercing the fascia covering the muscles, emerges onthe lateral aspect of the Achilles tendon, 10 to 15 cm above thelateral mallelus. After giving lateral calcaneal branches to theheel, the sural nerve descends 1-1.5 cm behind the lateralmalleolus, anterolateral to the short saphenous vein and on thesurface of the fascia covering the muscles and tendons. At thislevel the nerve supplies the lateral malleolus, Achilles tendonand the ankle joint. The sural nerve continues on the lateralaspect of the foot supplying the skin, subcutanous tissue, fourthinterosseous space and sensory innervation of the fifth toe.To block the saphenous nerve, a 25-gauge 1½" needle isinserted at the level of the medial malleous and a "ring" of localanesthetic is raised from the point of needle entry to the Achille's tendon and anteriorly to the tibialridge. This can be usually accomplished through one or two needle insertions. Five mL of localanesthetic suffices.TIPRemember the subcutaneous position of the superficial nerves and think of their blockade like a"field block". A distinct subcutaneous "wheal" should be with injection into a proper plane to blockthe superficial nerves.
Saphenous nerve isblocked bysubcutaneousinfiltration of localanesthetic over themedial as pect of thefoot.
Choice of local anesthetic

09.12.2011 NYSORA - The New York School of Regional Anesthesia - Ankle Block
7/7nysora.com/peripheral_nerve_blocks/…/3035-ankle_block.html?print
Choice of local anestheticThe choice of the type and concentration of local anesthetic for an ankle block is based on thedesired duration of the blockade. Because it is almost always beneficial that the analgesia after anankle block lasts some time after surgery, a long-acting local anesthetic is most commonly used.The following table provides onset times and duration for some commonly used local anestheticsmixtures.
Onset (min)Anesthesia (hrs)Analgesia (hrs)
1.5% Mepivacaine (+ HCO3) 15-20 2-3 3-5
2% Lidocaine (+ HCO3) 10-20 2-5 3-8
0.5% Ropivacaine 15-30 4-8 5-12
0.75% Ropivacaine 10-15 5-10 6-24
0.5 Bupivacaine (or I-bupivacaine)15-30 5-15 6-30
Block Dynamics and Perioperative ManagementAlthough the ankle block is considered a "superficial block" procedure, it is one of the mostuncomfortable block procedures for the patients. The reason is that an ankle block involves fiveseparate needle insertions; subcutaneous injections to block the cutaneous nerves result inpressure distension of the skin and nerve endings. Additionally, the foot is supplied by anabundance of nerve endings and it is exquisitely sensitive to needle injections. For that reason, thisblock requires significant sedation/analgesia to make it acceptable to patient. We routinely usecombination of midazolam (2-4 mg IV) and a narcotic (500-750 µmg alfentanyl) to ensure thepatient's comfort during the procedure. A typical onset time for this block is 10-25 minutes,depending primarily on the concentration of the local anesthetic used. Sensory anesthesia of theskin with this block develops faster than the motor block. Placement of an Esmarch or a tourniquetat the level of the ankle is well tolerated and typically does not require additional blockade.
Complications and How to Avoid ThemComplications after an ankle block are typically limited to residual paresthesias due to aninadvertent intraneuronal injection. Systemic toxicity is rare because of the distal location of theblockade.
Infection Rare with the use of an aseptic technique
HematomaAvoid multiple needle insertionsMost superficial blocks can be acomplished through one or two needle insertionsUse 25-gauge needle and avoid puncturing superficial veins.
Vascularpuncture
Avoid puncturing the greater saphenous vein at the medial malleolusIntermittent aspiration should be performed to avoid an intravascular injection
Nerve injuryDo not inject when the patient complains of pain or high pressures are met oninjectionDo not re-inject deep tibial and peroneal nerves
Other Instruct the patient on the care of the insensate extremity
BibliographyDelgado-Martinez AD, Marchal-Escalona JM: Supramalleolar ankle block anesthesia and ankletourniquet for foot surgery. Foot Ankle Int 2001; 22:836-8Hadzic A,Vloka JD, Kuroda MM: The use of peripheral nerve blocks in anesthesia practice. Anational survey. Reg Anesth Pain Med 1998; 23:241-6Mineo R, Sharrock NE: Venous levels of lidocaine and bupivacaine after midtarsal ankle block. RegAnesth 1992; 17:47-9Myerson MS, Ruland CM, Allon SM: Regional anesthesia for foot and ankle surgery. Foot Ankle1992; 13:282-8Needoff M, Radford P, Costigan P: Local anesthesia for postoperative pain relief after foot surgery:a prospective clinical trial. Foot Ankle Int 1999; 16:11-3Noorpuri BS, Shahane SA, Getty CJ: Acute compartment syndrome following revisionalarthroplasty of the forefoot: the dangers of ankle-block. Foot Ankle Int 2000; 21:680-2Reilley TE, Gerhardt MA: Anesthesia for foot and ankle surgery: Clin Podiatr Med Surg 2002;19:125-47Schurman DJ: Ankle-block anesthesia for foot surgery. Anesthesiology 1976; 44:348-52Sharrock NE, Waller JF, Fierro LE: Midtarsal block for surgery of the forefoot. Br J Anaesth 1986;58:37-40 Back to Peripheral Nerve Blocks