Embed Size (px)
Citation preview

.
1
NUTRITIONAL PROBLEMS IN PUBLIC
HEALTH
Dr.Indu Mohan
Assistant professor
Dept of Community Medicine
Outline of the talk
• Low Birth Weight
• Protein Energy malnutrition
• Anemia
• Vitamin A deficiency
• Iodine Deficiency Disorders
• Fluorosis
• Lathyrism
Low birth weight Low birth weight
• Birth weight less than 2500 g is a major public
health problem in many developing countries.
• India- 28 % of babies born are LBW
• Western world- 4 %
Low Birth Weight
• Two main groups - Low birth weight babies
1. Born prematurely (short gestation)
2. Foetal growth retardation
• In countries where - population of LBW infants is less, short gestation period is major cause
• In india- major cause of LBW- foetal growth retardation.
Preterm, Term and Post term
• Preterm - Babies born before the end of 37 weeks
gestation (less than 259 days)
• Term - Babies born from 37 completed weeks to less
than 42 completed weeks (259 to 293 days)
• Post term- Babies born at 42 completed weeks or any
time thereafter (294 days and over)
• LBW infant- birth weight of less than 2.5 kg regardless of
gestational age
.
2
Causes of LBW
1. Maternal malnutrition
2. Anaemia
3. Hard physical labour
4. Infections
5. Short maternal stature
6. Very young age
7. High parity
8. Smoking
9. Close birth intervals
LBW- Direct Interventions
• Increasing food intake
• Correction of Anemia
• Supplementary feeding- iron & folic acid tablets, fortification
and enrichment of foods
• Controlling infections (Malaria, UTI, TORCH)
• Early detection & treatment of medical disorders
(hypertension, toxemias, and diabetes)
LBW- Indirect Interventions
• Family planning
• Avoidance of excessive smoking
• Improved sanitation
• Improving health & nutrition of young girls
• Improvements in socio-economic & environmental conditions
especially in the under-served areas
• Govt support - maternity leave with full wages and child benefits
Treatment of LBW
A. Lees than 2 kg - requires first class modern
neonatal care
B. Between 2-2.5 kg- may need ICU for short
duration
Kangaroo Mother Care
• Introduced in Colombia (1979 by Drs. Hector
Martinez and Edzar Rey)
• High infections & mortality rates due to
overcrowding in hospitals
• Essential element in the neonatal care
• Components of kangaroo mother – for LBW
1. Skin-to-skin positioning of baby & mother's chest
2. Adequate nutrition (breast-feeding)
3. Ambulatory care after discharge from hospital
4. Support for the mother and her family0

.
3
Intensive care
• Incubatory care- adjustment of
temperature, humidity & O2 supply
• Hypoxia - cerebral palsy
• Continuous monitoring of the O2
level
• Excessive oxygen- retrolental
fibroplasia
Feeding
• Breast-feeding is difficult if baby cannot suck
• Breast milk should be used if available
• Feeding is often by rylestube
• Prevention of infection-death may occur within a few hours due to RTI
• Prevention of infection -most important functions of an intensive care unit.
Causes of death in LBW
1. Atelectasis
2. Malformation
3. Pulmonary hemorrhage
4. Intracranial bleeding
5. Pneumonia and other infections
• Facility based newborn care services
• Newborn care corner
• Newborn stabilization unit
• Special newborn care unit
• Some of these units are linked to obstetric units capable of monitoring the fetus
• The development of perinatal intensive care units leads to decline in neonatal mortality.
Protein energy malnutrition
• ‘Good nutrition allows children to survive, grow,
develop, learn, play, participate and contribute—
while malnutrition robs children of their futures and
leaves young lives hanging in the balance’.
• Major health and nutrition problem
• Incidence - pre-school age children is 1-2%
• Majority of cases (80%)- mild & moderate cases
which frequently go unrecognized

.
4
PEM in INDIA Trends in various nutritional indicator values and
U5 mortality rate from 2000 to 2018 (India).
Factors for malnutrition - under-5 children
Causes of PEM
1. Inadequate intake of food (food gap) both in
quantity and quality
2. Infections (diarrhea, RTI)
• Measles & intestinal worms- increases
requirements for calories, protein & other
nutrients, while decreases their absorption
and utilization.
.
5
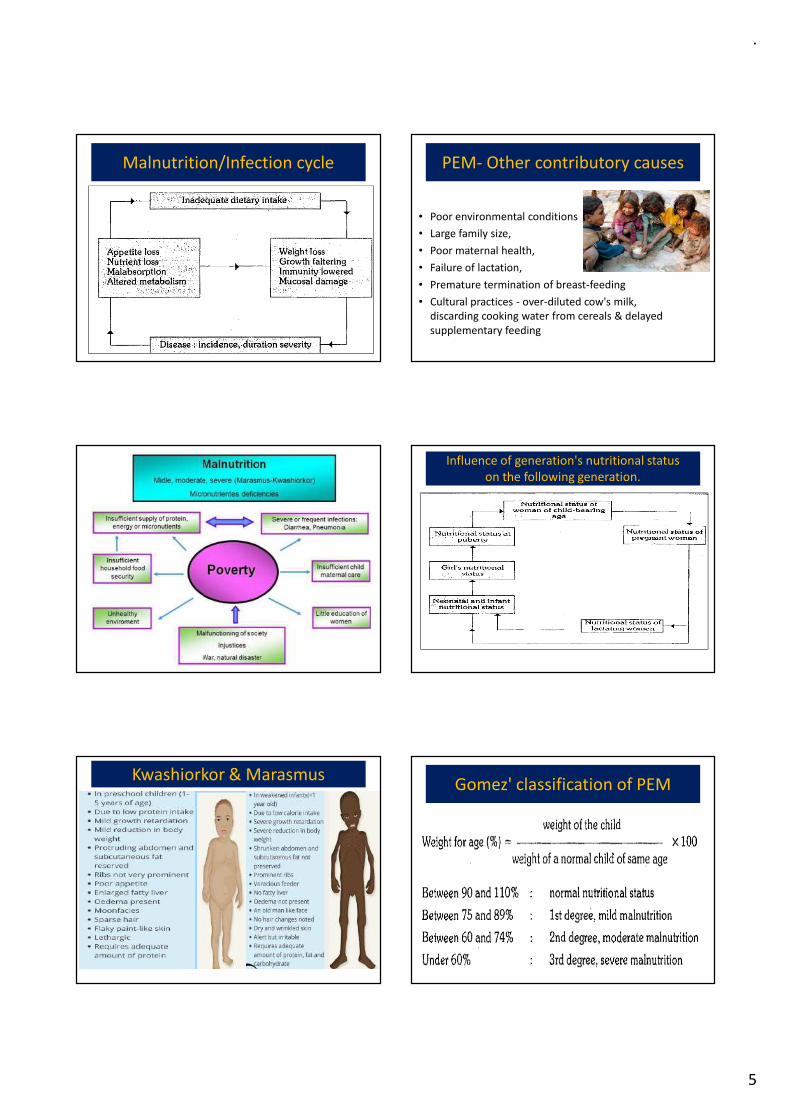
Malnutrition/Infection cycle PEM- Other contributory causes
• Poor environmental conditions
• Large family size,
• Poor maternal health,
• Failure of lactation,
• Premature termination of breast-feeding
• Cultural practices - over-diluted cow's milk,
discarding cooking water from cereals & delayed
supplementary feeding
Influence of generation's nutritional status
on the following generation.
Kwashiorkor & Marasmus Gomez' classification of PEM
.
6
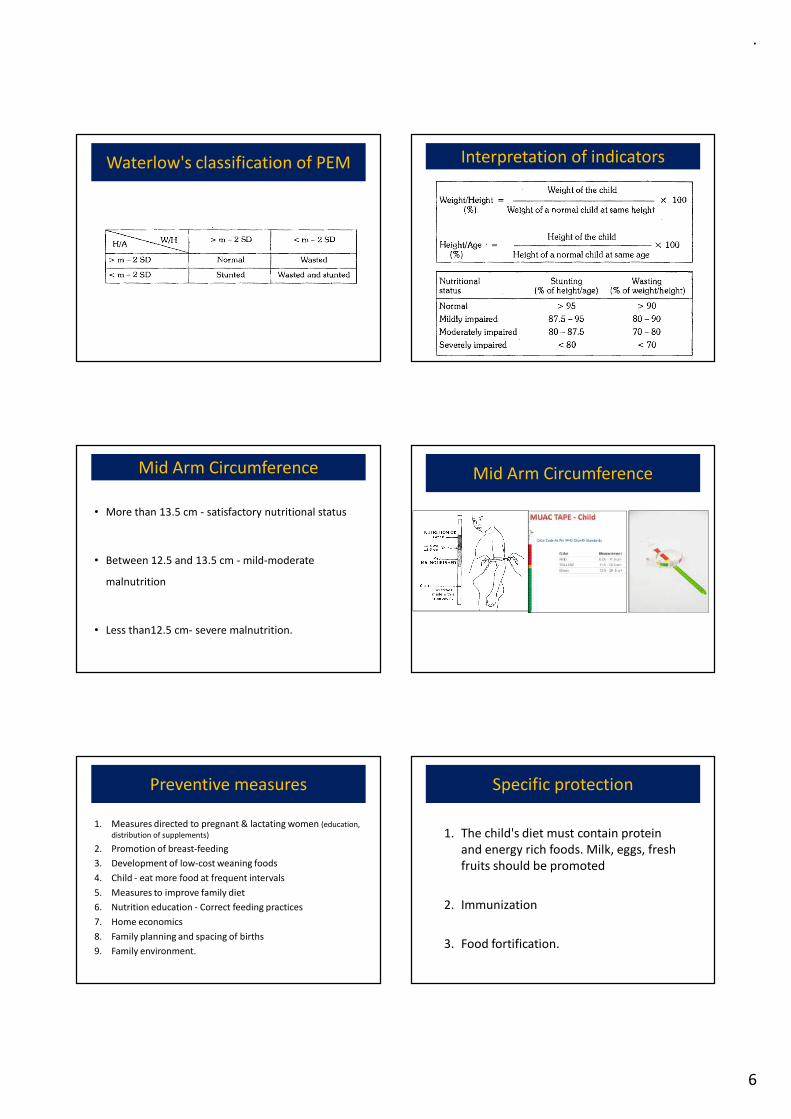
Waterlow's classification of PEM Interpretation of indicators
Mid Arm Circumference
• More than 13.5 cm - satisfactory nutritional status
• Between 12.5 and 13.5 cm - mild-moderate
malnutrition
• Less than12.5 cm- severe malnutrition.
Mid Arm Circumference
Preventive measures
1. Measures directed to pregnant & lactating women (education,
distribution of supplements)
2. Promotion of breast-feeding
3. Development of low-cost weaning foods
4. Child - eat more food at frequent intervals
5. Measures to improve family diet
6. Nutrition education - Correct feeding practices
7. Home economics
8. Family planning and spacing of births
9. Family environment.
Specific protection
1. The child's diet must contain protein
and energy rich foods. Milk, eggs, fresh
fruits should be promoted
2. Immunization
3. Food fortification.

.
7
Early diagnosis and treatment
1. Periodic surveillance
2. Early diagnosis of any lag in growth
3. Early diagnosis, treatment of infections and
diarrhoea
4. Development of programs for early rehydration of children with diarrhoea
5. Development of supplementary feeding programs during epidemics
6. Deworming
Nutritional Rehabilitation
1. Nutritional
rehabilitation services
2. Hospital treatment
3. Follow-up care
Vitamin A deficiencyVitamin A deficiency
Ocular Manifestations
• Night blindness, conjunctival
xerosis, Bitot's spots, corneal
xerosis and keratomalacia
• "xerophthalmia" (dry eye)
comprises all the ocular
manifestations of vitamin A
deficiency ranging from night
blindness to keratomalacia,
Stages of Ocular manifestations of Vit A def Stages of Ocular manifestations of Vit A def
.
8
Stages of Ocular manifestations of Vit A def Stages of Ocular manifestations of Vit A def
Assessment of vitamin A deficiency
• Effective intervention program-
characterization of the problem
• Population surveys - done on preschool
children (6 months to 6 years) - clinical and
biochemical criteria
• The criteria recommended by WHO
Vit A- Prevention and control
• Short-term action- A short-term
preventive approach - administration
of large doses of vitamin A orally, in
recommended doses to vulnerable
groups, on a periodic basis
Prevention of Vit A deficiency
• Fortification of certain foods with vitamin A
• Long-term action - aimed at reduction or elimination of
factors contributing to ocular disease (Educate particularly
mothers to consume DGLV or other vitamin A rich foods)
• Promotion of breast-feeding
• Improvements in environmental health (safe & adequate
water supply, construction & maintenance of sanitary latrines
• Immunization against infectious diseases (measles, prompt
treatment of diarrhea and other associated infections)
• Improved feeding of infants & young children
• Improved health services for mothers and children
• Social & health education
.
9
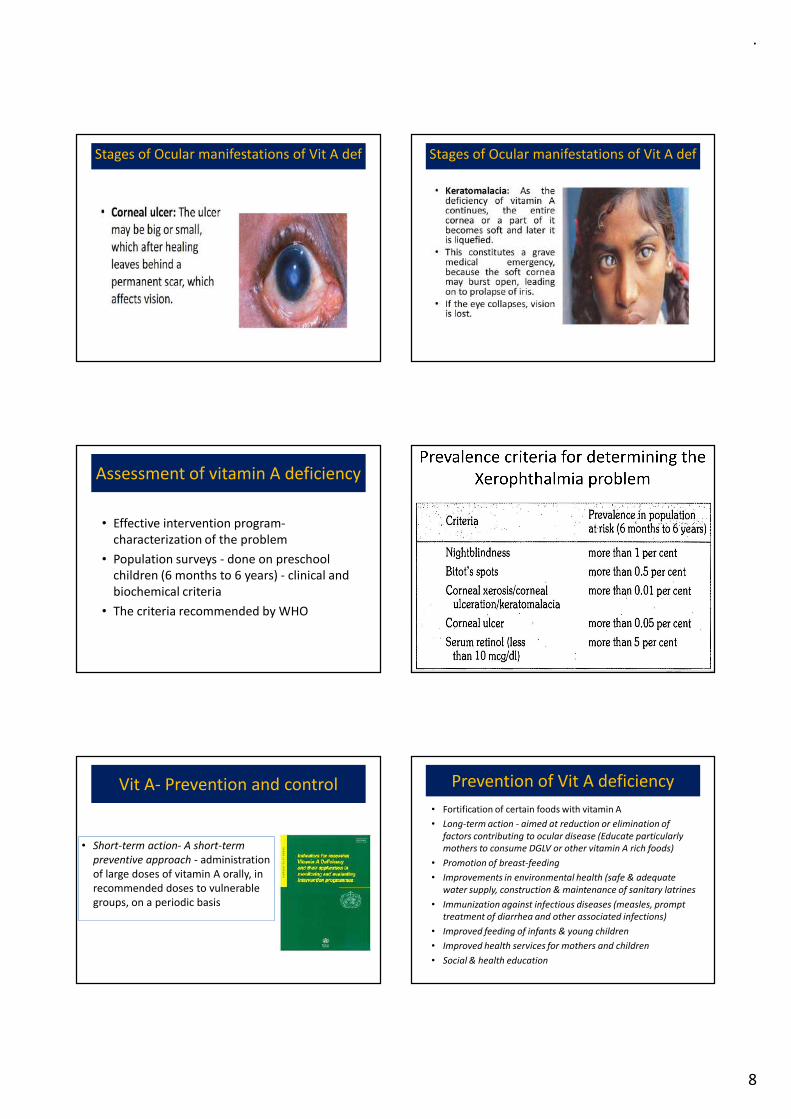
Vitamin A deficiency in India (VAD)
The program focusses on
1. Promoting consumption of vitamin, A rich foods by pregnant and lactating women and by children < 5 years and appropriate breast-feeding
2. Administration of massive dose of vitamin A up to five years. First dose of 100,000 IU with measles vaccination at nine months and subsequent doses of 200,000 IU each, every six months up to the age 5 years
3. All children suffering from measles to be given one dose of vitamin A if they have not received it in the previous one month
4. All cases of severe malnutrition to be given one additional dose of vitamin A
Prevention of vitamin A deficiency
� The National vitamin A prophylaxisprogramme
� 1-6 yrs , every 6 mths
� 2,00,000 IU
� half that dose (100,000 IU) to children between 6
months and one year of age
� Fortification of food (vanaspati ghee, oil)
Anemia WHO- Definition of Anemia
• “A condition in which the haemoglobin content of
blood is lower than normal as a result of a deficiency
of one or more essential nutrients, regardless of the
cause of such deficiency. By far the most frequent
cause of nutritional anaemia is iron deficiency, and
less frequently folate or vitamin B12.
.
10
Magnitude of Problem
• Anemia is global menace affecting both developing
and developed countries
• It leads to major consequences for human health as
well as social and economic development.
• It occurs at all stages of the life cycle
• It is more prevalent in the woman especially
pregnant women and young adolescent
Magnitude of Problem of Anaemia
Globally anaemia is a problem of public health
significance when the prevalence exceeds certain levels
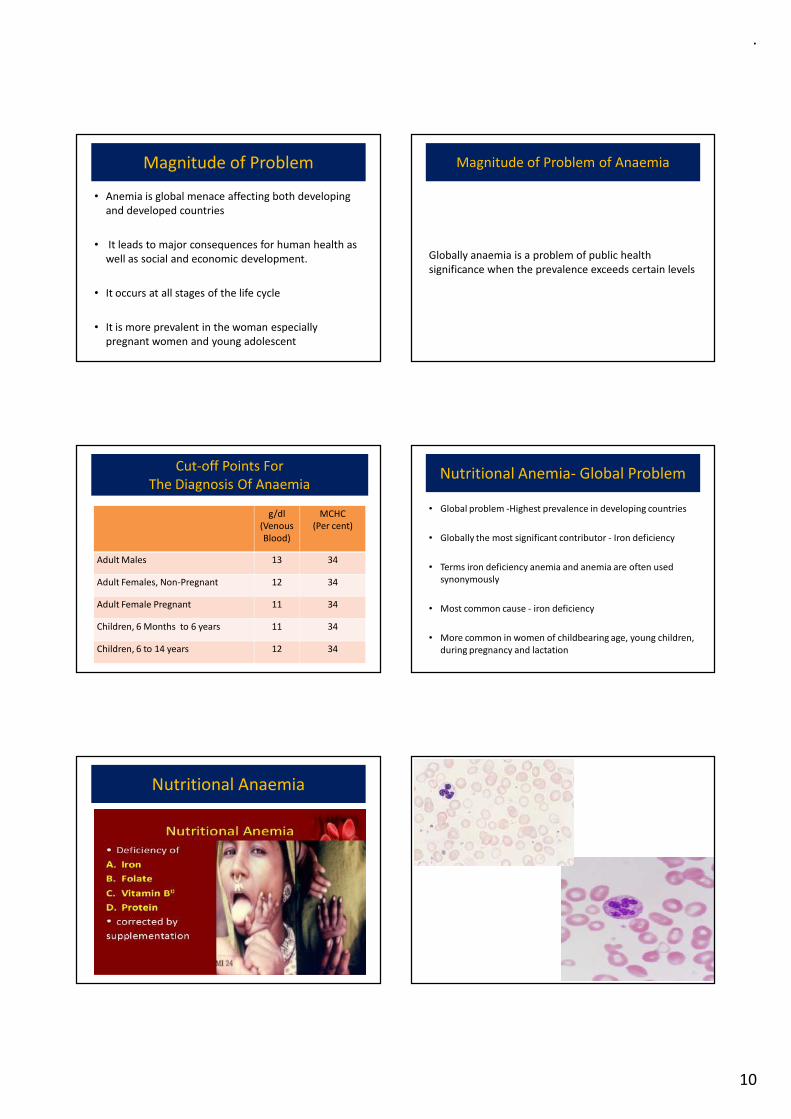
Cut-off Points For
The Diagnosis Of Anaemia
g/dl
(Venous
Blood)
MCHC
(Per cent)
Adult Males 13 34
Adult Females, Non-Pregnant 12 34
Adult Female Pregnant 11 34
Children, 6 Months to 6 years 11 34
Children, 6 to 14 years 12 34
Nutritional Anemia- Global Problem
• Global problem -Highest prevalence in developing countries
• Globally the most significant contributor - Iron deficiency
• Terms iron deficiency anemia and anemia are often used
synonymously
• Most common cause - iron deficiency
• More common in women of childbearing age, young children,
during pregnancy and lactation
Nutritional Anaemia
.
11
61
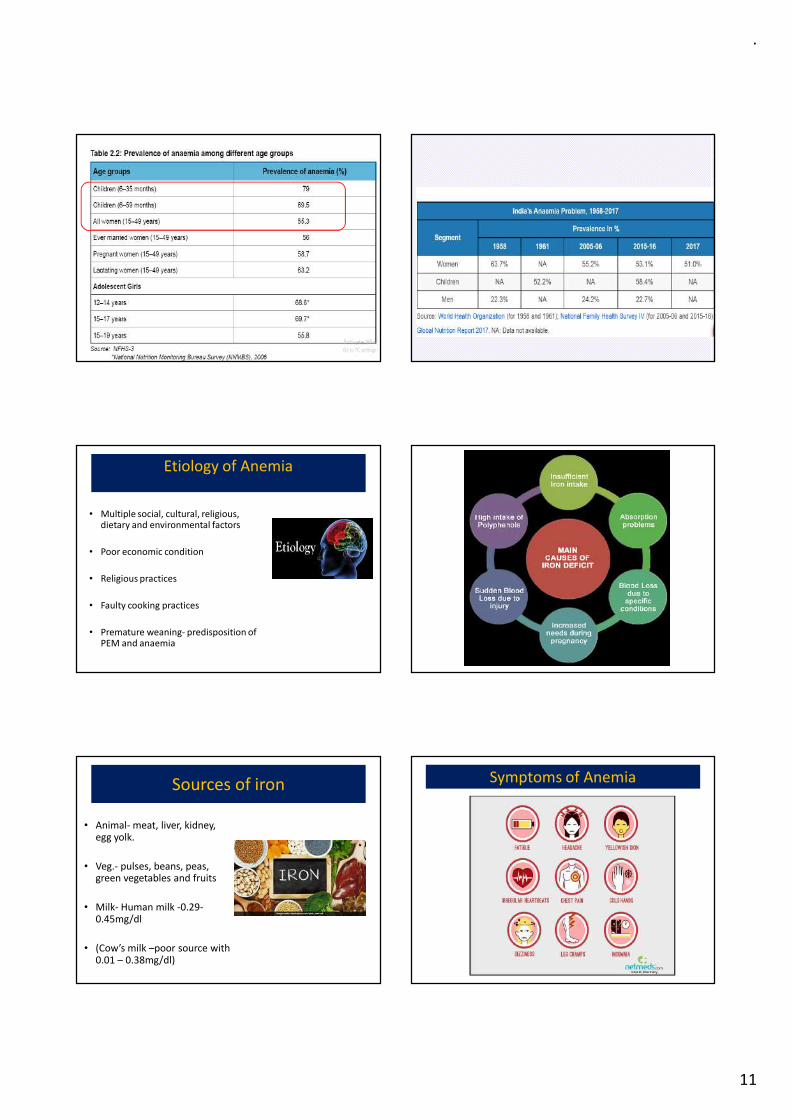
Etiology of Anemia
• Multiple social, cultural, religious, dietary and environmental factors
• Poor economic condition
• Religious practices
• Faulty cooking practices
• Premature weaning- predisposition of PEM and anaemia
Sources of iron
• Animal- meat, liver, kidney, egg yolk.
• Veg.- pulses, beans, peas, green vegetables and fruits
• Milk- Human milk -0.29-0.45mg/dl
• (Cow’s milk –poor source with 0.01 – 0.38mg/dl)
Symptoms of Anemia
.
12
Excessive losses
• Occult bleeding (erosive gastritis, drug indusedgastritis)
• Recurrent diarrhea
• Hookworm
• Polyposis
• Prolapse rectum
• Portal hypertension
• Dysentry
• Meckel’s diverticulum
• Hiatus hernia
• Cephalhematoma
Public Health Consequences Of Anaemia
General
• Weakness, easy fatigability, lethargy
• Inhibition of lymphocyte proliferation
• Lowered cell mediated immunity
• Reduced neutrophil bactericidal activity
• Vulnerability to infections
• Diminished physical and earning capacity
• Reduced work capacity reduced endurance.
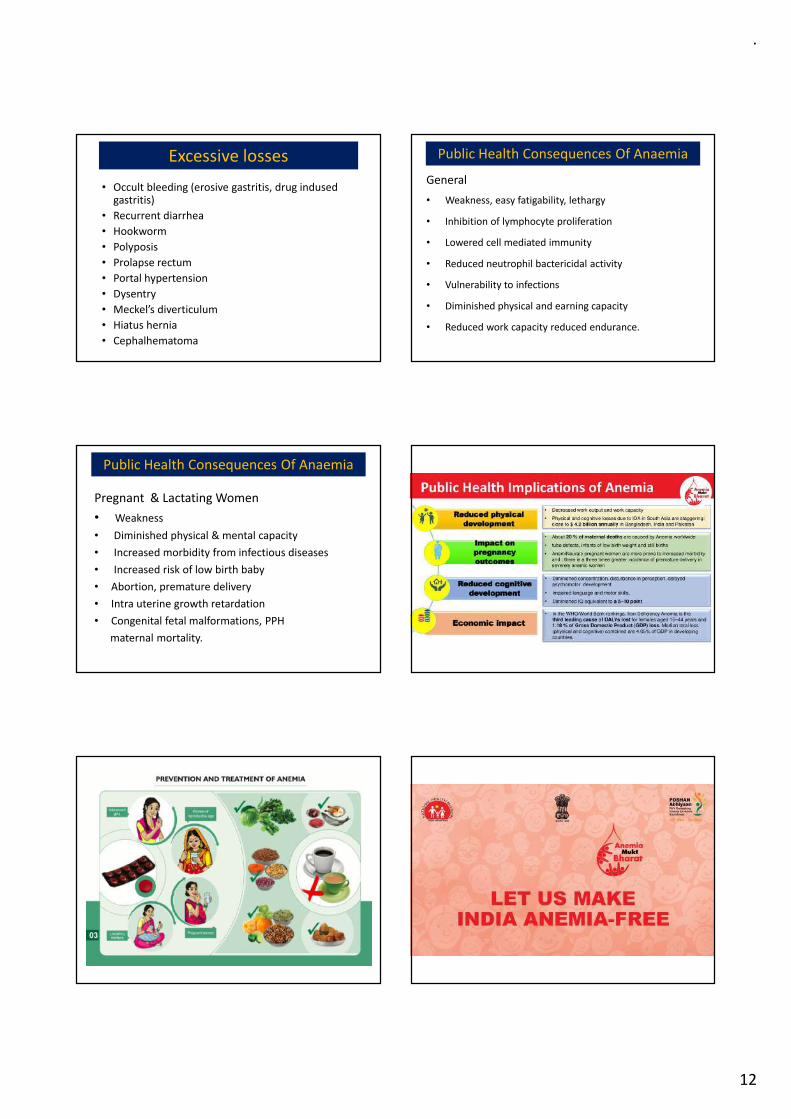
Pregnant & Lactating Women
• Weakness
• Diminished physical & mental capacity
• Increased morbidity from infectious diseases
• Increased risk of low birth baby
• Abortion, premature delivery
• Intra uterine growth retardation
• Congenital fetal malformations, PPH
maternal mortality.
Public Health Consequences Of Anaemia
.
13
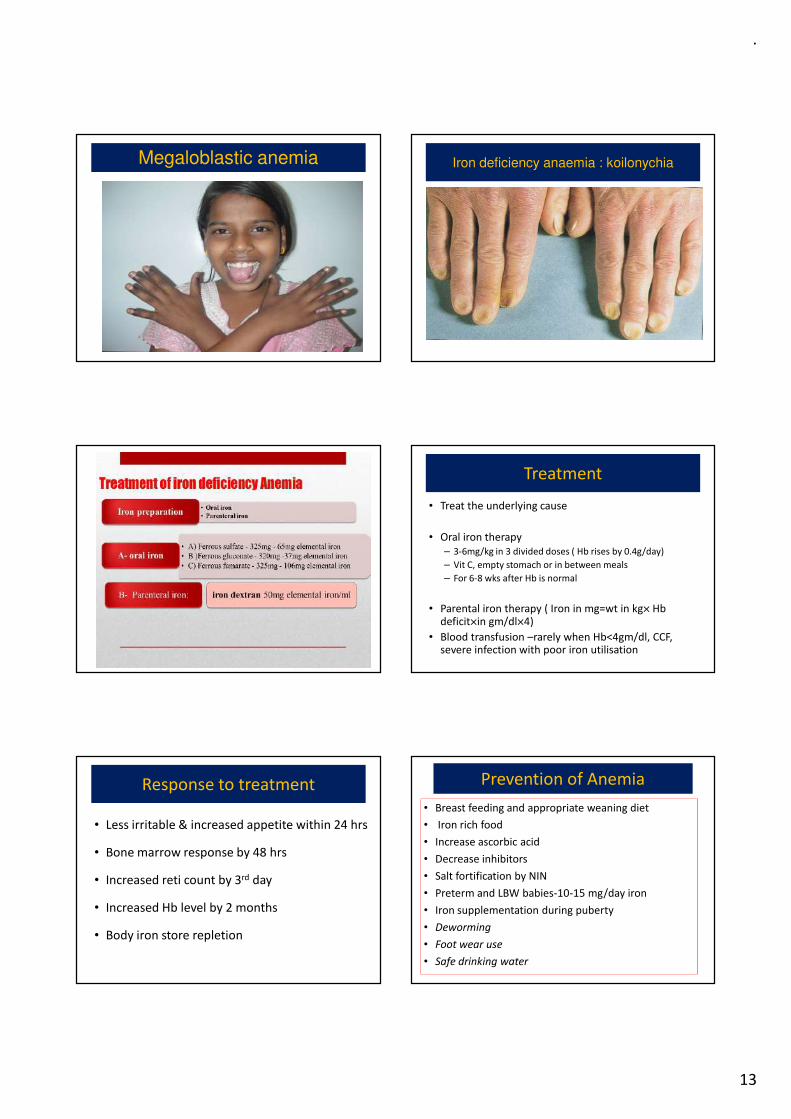
Megaloblastic anemia Iron deficiency anaemia : koilonychia
Treatment
• Treat the underlying cause
• Oral iron therapy
– 3-6mg/kg in 3 divided doses ( Hb rises by 0.4g/day)
– Vit C, empty stomach or in between meals
– For 6-8 wks after Hb is normal
• Parental iron therapy ( Iron in mg=wt in kg× Hb deficit×in gm/dl×4)
• Blood transfusion –rarely when Hb<4gm/dl, CCF, severe infection with poor iron utilisation
Response to treatment
• Less irritable & increased appetite within 24 hrs
• Bone marrow response by 48 hrs
• Increased reti count by 3rd day
• Increased Hb level by 2 months
• Body iron store repletion
Prevention of Anemia
• Breast feeding and appropriate weaning diet
• Iron rich food
• Increase ascorbic acid
• Decrease inhibitors
• Salt fortification by NIN
• Preterm and LBW babies-10-15 mg/day iron
• Iron supplementation during puberty
• Deworming
• Foot wear use
• Safe drinking water
.
14
Iodine deficiency disorders (IDD)
Iodine deficiency disorders (IDD)
• Goitre control
• Control program- iodized salt or oil,
monitoring and surveillance, manpower
training and mass communication.
IDD- (1) Iodized salt
• Most widely used prophylactic public health measure
• Level of iodization - not < 30 ppm at the production point, and not < 15 ppm of iodine at the consumer level
• Iodized salts most economical, convenient, effective means of mass prophylaxis
• Under the national !DD control activities-
• Proposed to completely replace common salt with iodized salt
• New product- "two-in-one" salt, common salt fortified with iron and iodine
• Iodized oil – IM injection (mostly poppy-seed oil)- 1 ml= 4 yrsprotection
IDD- Iodine monitoring
• Network of laboratories for iodine monitoring and surveillance
• To determine iodine excretion determination
• To determine iodine in water, soil and food as part of
epidemiological studies
• To determine iodine in salt for quality control
• Neonatal hypothyroidism is a sensitive pointer to environmental
iodine deficiency and can thus be an effective indicator for
monitoring the impact of a program
.
15
IDD
• Manpower training of HCW in all aspects of
goiter control including legal enforcement and
public education
• Mass communication- powerful tool for
nutrition education, public awareness
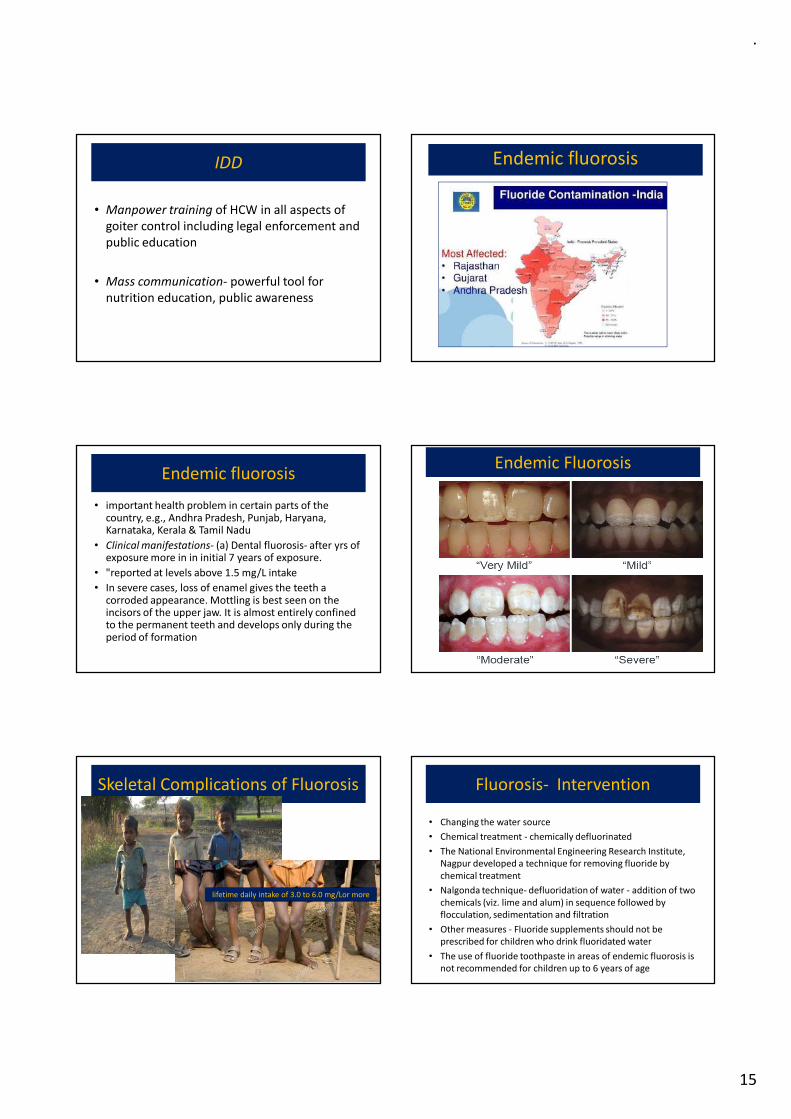
Endemic fluorosis
Endemic fluorosis
• important health problem in certain parts of the country, e.g., Andhra Pradesh, Punjab, Haryana, Karnataka, Kerala & Tamil Nadu
• Clinical manifestations- (a) Dental fluorosis- after yrs of exposure more in in initial 7 years of exposure.
• "reported at levels above 1.5 mg/L intake
• In severe cases, loss of enamel gives the teeth a corroded appearance. Mottling is best seen on the incisors of the upper jaw. It is almost entirely confined to the permanent teeth and develops only during the period of formation
Endemic Fluorosis
Skeletal Complications of Fluorosis
lifetime daily intake of 3.0 to 6.0 mg/Lor more
Fluorosis- Intervention
• Changing the water source
• Chemical treatment - chemically defluorinated
• The National Environmental Engineering Research Institute,
Nagpur developed a technique for removing fluoride by
chemical treatment
• Nalgonda technique- defluoridation of water - addition of two
chemicals (viz. lime and alum) in sequence followed by
flocculation, sedimentation and filtration
• Other measures - Fluoride supplements should not be
prescribed for children who drink fluoridated water
• The use of fluoride toothpaste in areas of endemic fluorosis is
not recommended for children up to 6 years of age
.
16
Lathyrism
• Paralyzing disease - affects the
nervous system
• Neurolathyrism is a crippling
disease - developing spastic
paralysis of lower limbs,
occurring mostly in adults
consuming the pulse, Lathyrus
sativus in large quantities
• Toxin- Beta oxalyl amino alanine
Conclusions
1. Nutritional problems are common
2. Leads to many serious complications
3. LBW, Anemia, Vit A deficiency, Iodine deficiency, Fluorosis, lathyrisim are major problems in india
4. High morbidity and mortality
5. Largely preventable
6. National Programs
7. Responsibility of all of us
Thanks