Embed Size (px)
Citation preview
November/December 2007726 The Journal for Nurse Practitioners - JNP
JNP
Malnutrition, a deficiency syndrome characterizedby an inadequate intake or absorption of nutri-ents, occurs frequently in older adults, affectingup to16% of community-dwelling elders, 17% to65% of those in acute care facilities, and 5% to59% of seniors living in long-term care.1 It isassociated with adverse health outcomes such aslonger hospital stays, reduced quality of life, poorwound healing, infection, and disability. Numerousstudies show a clear association between malnu-trition and increased rates of mortality in the eld-erly population, with unintentional weight lossalone being independently associated with mor-tality. Nurse practitioners (NPs) should conduct aroutine nutritional assessment as part of the his-tory and examination when working with frail orsick elders.
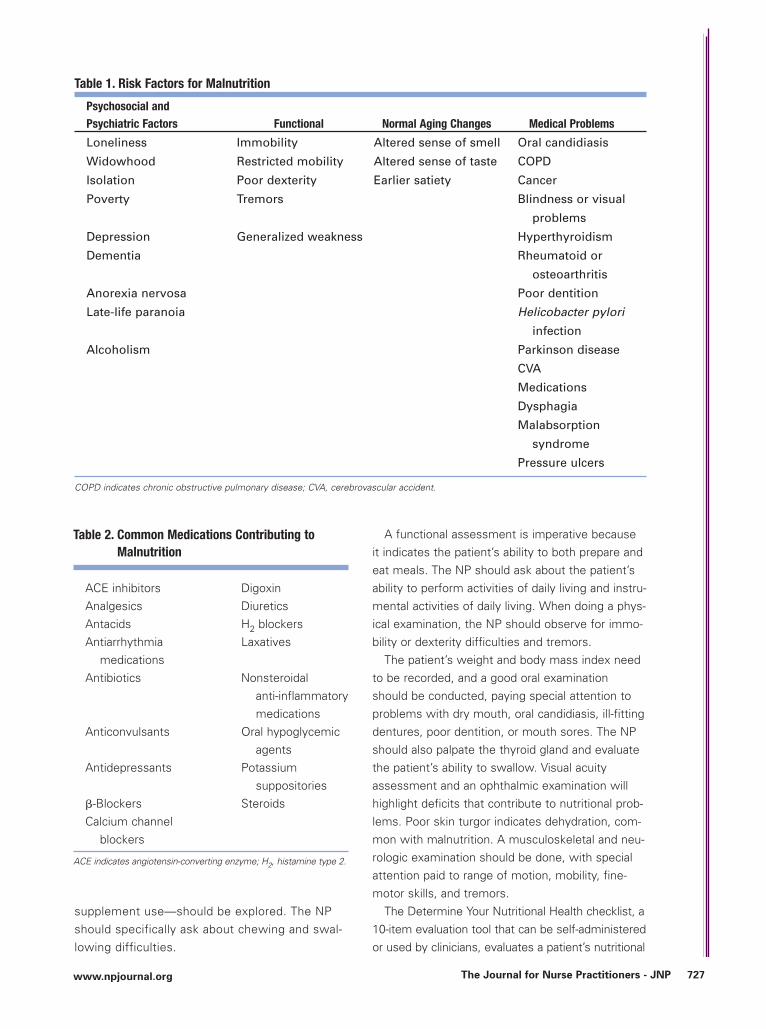
The causes of malnutrition are often complex,with many seniors having more than one risk fac-tor (Table 1). Seniors who are isolated and lonelymay lose the desire to cook or eat and might lacktransportation to purchase food. Poverty may pre-vent adequate food intake, affecting both qualityand quantity of foods consumed. Restrictive ortherapeutic diets may prevent certain food prefer-ences. The normal chemosensory changes ofdiminished sense of smell and taste, as well as dif-ficulty in recognizing taste mixtures, lead todecreased appetite and subsequent low intake.Elders also experience earlier satiety, which furthercontributes to a lower intake and successiveweight loss. Functional impairments can makefood preparation and eating a difficult task.
Numerous medical conditions negativelyaffect an elder’s nutritional status. Elders whohave had a cerebrovascular accident often havedifficulties with dysphagia and mobility, both ofwhich affect intake. Elders with visual problemssuch as macular degeneration may be unable todrive to the market, prepare food, or use con-ventional eating utensils properly. Poor oralhealth and oral candidiasis may result in apainful mouth, thereby reducing the desire andability to eat. Tremors make food preparationand eating much more difficult tasks. Patientswith dementia often forget to eat, can burnmany calories from wandering throughout theday, and experience difficulty in self-feeding inthe later stages.
Many common medications can contribute tomalnutrition (Table 2). Prescription medicationsoften diminish appetite, change the sense oftaste, and cause xerostomia, drowsiness, andgastrointestinal disturbances.2
When interviewing the elderly patient, the NPshould inquire about usual weight, recent changesin weight, and any current health problems. Agood psychiatric history should be completed,including a Mini-Mental Status Examination and aGeriatric Depression Scale. A detailed history ofchronic medical conditions should be recorded,focusing on conditions that may affect nutritionalstatus now or in the future. A medication listshould be obtained and reviewed by the practi-tioner, being mindful of drugs that contribute tomalnutrition.
Current living situations and the patient’s satis-faction with them should be discussed and theavailability and use of social resources. Assessmentof the patient’s ability to pay for basic necessitiesand food preferences is crucial.
A thorough dietary history—food preferencesand habits, prescribed diets, cultural food habits,meal frequency, alcohol and fluid intake, and
Nutritional Assessment in Elderly Clients
DIAGNOSTIC TIPS
Jennifer Kim
726-728_TJNP520_Kim_CPR 10/31/07 4:15 PM Page 726
www.npjournal.org The Journal for Nurse Practitioners - JNP 727
supplement use—should be explored. The NPshould specifically ask about chewing and swal-lowing difficulties.
A functional assessment is imperative becauseit indicates the patient’s ability to both prepare andeat meals. The NP should ask about the patient’sability to perform activities of daily living and instru-mental activities of daily living. When doing a phys-ical examination, the NP should observe for immo-bility or dexterity difficulties and tremors.
The patient’s weight and body mass index needto be recorded, and a good oral examinationshould be conducted, paying special attention toproblems with dry mouth, oral candidiasis, ill-fittingdentures, poor dentition, or mouth sores. The NPshould also palpate the thyroid gland and evaluatethe patient’s ability to swallow. Visual acuityassessment and an ophthalmic examination willhighlight deficits that contribute to nutritional prob-lems. Poor skin turgor indicates dehydration, com-mon with malnutrition. A musculoskeletal and neu-rologic examination should be done, with specialattention paid to range of motion, mobility, fine-motor skills, and tremors.
The Determine Your Nutritional Health checklist, a10-item evaluation tool that can be self-administeredor used by clinicians, evaluates a patient’s nutritional
Table 2. Common Medications Contributing toMalnutrition
ACE inhibitors DigoxinAnalgesics DiureticsAntacids H2 blockersAntiarrhythmia Laxatives
medicationsAntibiotics Nonsteroidal
anti-inflammatorymedications
Anticonvulsants Oral hypoglycemicagents
Antidepressants Potassiumsuppositories
�-Blockers SteroidsCalcium channel
blockers
ACE indicates angiotensin-converting enzyme; H2, histamine type 2.
Table 1. Risk Factors for Malnutrition
Psychosocial and Psychiatric Factors Functional Normal Aging Changes Medical Problems
Loneliness Immobility Altered sense of smell Oral candidiasis
Widowhood Restricted mobility Altered sense of taste COPD
Isolation Poor dexterity Earlier satiety Cancer
Poverty Tremors Blindness or visual
problems
Depression Generalized weakness Hyperthyroidism
Dementia Rheumatoid or
osteoarthritis
Anorexia nervosa Poor dentition
Late-life paranoia Helicobacter pylori
infection
Alcoholism Parkinson disease
CVA
Medications
Dysphagia
Malabsorption
syndrome
Pressure ulcers
COPD indicates chronic obstructive pulmonary disease; CVA, cerebrovascular accident.
726-728_TJNP520_Kim_CPR 10/31/07 4:15 PM Page 727
JNP
risk.3 The Mini Nutritional Assessment (MNA) is an18-item tool to evaluate nutritional risk and need forfurther assessment. It evaluates subjective andobjective assessment findings, including anthropo-metric measurements. The MNA has been shownto be sensitive, specific, and accurate in identifyingnutritional risks in the elderly.4 This tool is availableat www.mna-elderly.com/index.htm.
Ordering a serum albumin test is an inexpensiveway to evaluate nutritional status because it is anexcellent indicator of protein status. Albumin levelsless than 3.2 g/dL in hospitalized seniors are highlypredictive of subsequent death. Shorter-lived pro-teins, such as pre-albumin and retinol binding pro-tein, help evaluate patient response to nutritionaltherapy in acute care situations.1
Nutrition screening is an important step in identi-fying nutritional risks. Findings can prompt earlyinterventions or preventive measures to ensure thatan elder’s nutritional health is well managed.
References
1. Beers M, Berkow R. Protein-energy undernutrition. In: MerckManual of Geriatrics. 3rd ed. Whitehouse Station, NJ: Merck; 2000.
2. Omran ML, Salem P. Diagnosing undernutrition. Clin Geriatr Med.2002;18(4):719-736.
3. Determine your nutritional health. Available at: www.eatright.org/ada/files/Checklist.pdf. Accessed August 23, 2007.
4. Guigoz Y. The Mini Nutritional Assessment review of the literature:what does it tell us? J Nutr Health Aging. 2006;10(6):466-485.
For further reading
Ham RJ, Sloane PD. Primary Care Geriatrics: A Case-BasedApproach. 5th ed. Philadelphia, PA: Mosby; 2007.
1555-4155/07/$ see front matter© 2007 American College of Nurse Practitionersdoi:10.101 /j.nurpra.2007.09.007
November/December 2007728 The Journal for Nurse Practitioners - JNP
Guest Writers Wanted
If you are interested in contributing anarticle to Diagnostic Tips, please [email protected].
Jennifer Kim, MSN, APRN, BC, is an assistant professor ofnursing at the Vanderbilt University School of Nursing inNashville, Tennessee. She can be reached at [email protected].
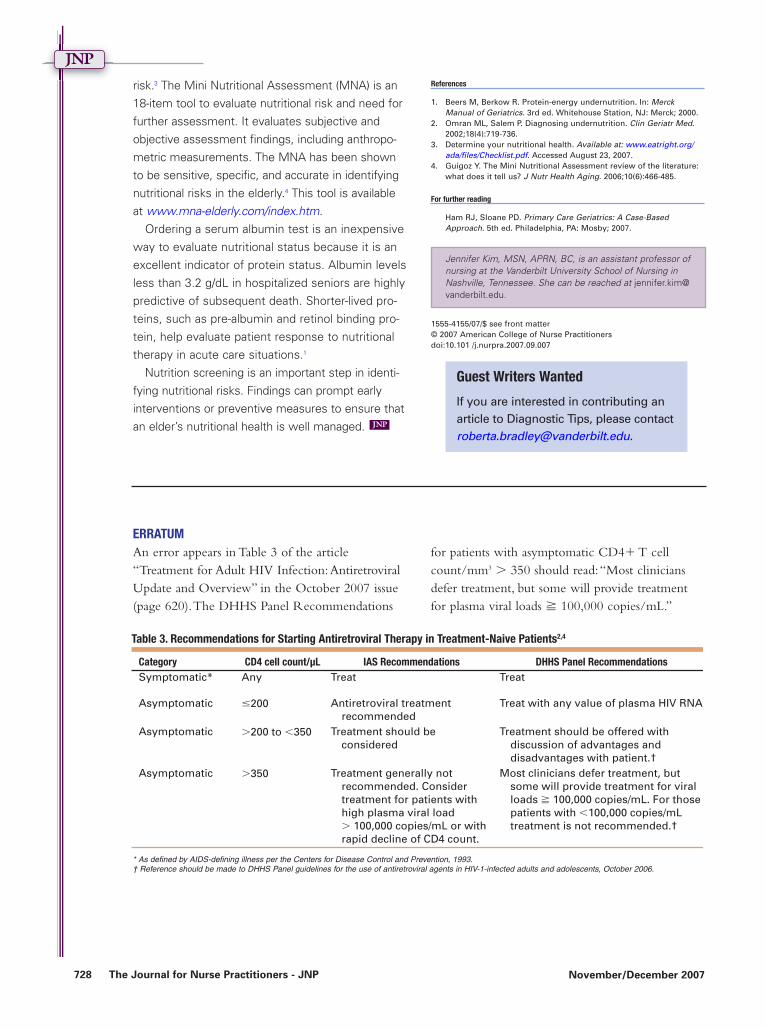
Table 3. Recommendations for Starting Antiretroviral Therapy in Treatment-Naive Patients2,4
Category CD4 cell count/µL IAS Recommendations DHHS Panel RecommendationsSymptomatic* Any Treat Treat
Asymptomatic �200 Antiretroviral treatmentrecommended
Treat with any value of plasma HIV RNA
Asymptomatic �200 to �350 Treatment should be considered
Treatment should be offered with discussion of advantages anddisadvantages with patient.†
Asymptomatic �350 Treatment generally notrecommended. Considertreatment for patients with high plasma viral load � 100,000 copies/mL or with rapid decline of CD4 count.
Most clinicians defer treatment, but some will provide treatment for viral loads � 100,000 copies/mL. For those patients with �100,000 copies/mL treatment is not recommended.†
* As defi ned by AIDS-defi ning illness per the Centers for Disease Control and Prevention, 1993.
† Reference should be made to DHHS Panel guidelines.
ERRATUMAn error appears in Table 3 of the article“Treatment for Adult HIV Infection:AntiretroviralUpdate and Overview” in the October 2007 issue(page 620).The DHHS Panel Recommendations
for patients with asymptomatic CD4� T cellcount/mm3 � 350 should read:“Most cliniciansdefer treatment, but some will provide treatmentfor plasma viral loads � 100,000 copies/mL.”
* As defined by AIDS-defining illness per the Centers for Disease Control and Prevention, 1993.† Reference should be made to DHHS Panel guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents, October 2006.
726-728_TJNP520_Kim_CPR 10/31/07 4:15 PM Page 728