Embed Size (px)
DESCRIPTION
Nutrition Support of the Surgical Patient. Randa Jaroudi, Pharm.D Clinical Coordinator TPN Coordinator KKUH. Nutrition. - PowerPoint PPT Presentation
Citation preview

Nutrition Support of the Surgical Patient
Randa Jaroudi, Pharm.DClinical Coordinator
TPN Coordinator KKUH

Nutrition
Nutrition allows the body to be provided with all basic nutrients substrates and energy required for maintaining or restoring all vital body functions from carbohydrate and fat and for building up body mass from amino acid.
Malnutrition
Malnutrition—come from extended inadequate intake of nutrient or severe illness burden on the body composition and function—affect all systems of the body

Type of Malnutrition
MarasmusProtein – calorie malnutritionThe patient's oral diet may include an acceptableprotein:calorie ratio but is inadequate in quantity and
calories.
(depleted somatic proteins, normal visceral proteins) Normal Albumin and transferrin Patients look thin and malnourished.
e.g. Patients with mild to moderate starvation, common severe burns, injuries, systemic infections, cancer etc or conditions where patient does not eat like anorexia nervosa

Clinical Manifestations
Weight loss Reduced basal metabolism Depletion skeletal muscle and adipose
(fat) stores Decrease tissue turgor Bradycardia Hypothermia


Kwashiorkor (Kwa-shior-kor)Protein malnutrition the diet contains various amounts of nonprotein calories (inadequate, adequate, or excessive) from carbohydrates
and fats, but is deficient in total protein and essential amino acids.
(normal somatic proteins depleted visceral proteins) ↓ Serum Albumin and transferrin Patients appear normal or overweight e.g. Hypercatabolic critical care patients, chronic diarrhea,
chronic kidney disease, trauma , burns, hemorrhage, and liver cirrhosis
Type of Malnutrition

Clinical Manifestations
Marked hypoalbuminemia Anemia Edema and ascites Muscle atrophy Delayed wound healing Impaired immune function

Diagnosis
MixedMarasmus-Kwashiorkor: (depleted somatic and visceral proteins)All above data are reduced Patients appear cachexic and severely malnourished.e.g. *Chronic hypercatabolic patients (250 to 500g loss of
weight) *Prolonged starvation
Marasmic-kwashiorkor is a mixed form of any PCM symptoms. It frequently occurs when the marasmic patient experiences the catabolic stress of illness or trauma.

Medical causes (Risk factors for malnutrition)
Recent surgery or trauma Sepsis Chronic illness Gastrointestinal disorders Anorexia, other eating disorders Dysphagia Recurrent nausea, vomiting, or diarrhea Pancreatitis Inflammatory bowel disease Gastrointestinal fistulas Cancer
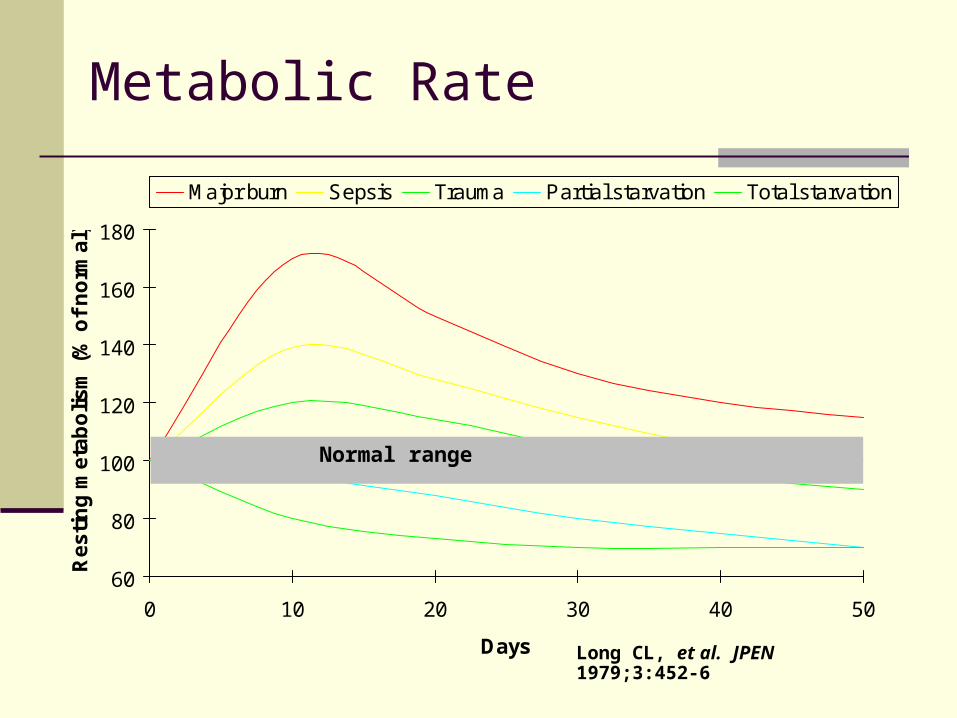
Metabolic Rate
60
80
100
120
140
160
180
0 10 20 30 40 50
Days
Re
sti
ng
me
tab
oli
sm
(%
of
no
rma
l)
Major burn Sepsis Trauma Partial starvation Total starvation
Long CL, et al. JPEN 1979;3:452-6
Normal range

Protein Catabolism
0
5
10
15
20
25
30
0 10 20 30 40
Days
Nit
rog
en
ex
cre
tio
n (
g/d
ay
)
Major burn Trauma Sepsis Partial starvation Total starvation
Long CL. Contemp Surg 1980;16:29-42
Normal range
The Goals of Preoperative Nutrition Support
↓ surgical mortality ↓surgical complications and infection Reduce the catabolic state and restore
anabolism ↓the hospital length of stay Speed the healing/recovery process
Indications
Aggressive nutritional support (enteral or parenteral) should be considered in minimum 3 of: Looks clinically malnourished. Has a low serum albumin <3.5g/dL. Has a recent loss of 10% or greater within Has a history of recent poor intake. Who as a consequence of his illness is going
to be or has been NPO for 5-7 days.
The term “If gut works, use it” remains the golden rule. However, recently this was changed to: If gut works use it; and if gut works partially, use it partially.

Preoperative Nutrition Assessment-1
1. Medical & Nutritional History Medical history includes acute or chronic disease,
medication,surgeries, & other therapies (i.e., chemotherapeutics,
immunosuppressive)
Nutrition History includes recent changes in appetite or
weight, activity level, use of diet.
Subject Global Assessment (SGA)
Preoperative Nutrition Assessment-2
2. Physical examinationLogical assessment from head to toe
3. Anthropometric parameters % of IBW = Actual weight x 100/Ideal body weight
Triceps Skinfold Thickness (TSF) for assessing fat reserve. It is decreased when fat stores are depleted.
Midarm muscle circumference (MAC) to assess the degree of somatic protein depletion. TSF and Mid Arm Circumference are no more recommended as an accurate measurement.
Creatinine Height Index (CHI) to assess somatic protein stores. Serum Protein Determination to assess the degree of visceral protein
depletion, e.g. Albumin, Transferring, Prealbumin. Measure Total Lymphocyte Count (TLC) to assess Immune function
becomes impaired
4. Lab assessment

Fat, Anthropometric parameters
Assessment of body fat Triceps Skinfold Thickness (TSF) for assessing fat reserve. It is decreased
when fat stores are depleted.

Protein (Somatic Protein)
Assessment of the fat-free muscle mass (Somatic Protein) depletion
Mid-upper-arm circumference (MAC)TSF and MAC are no morerecommended as an accurate measurement

Creatinine-height index (CHI )
[measured urinary creatinine (24hr)/ Ideal urinary creatinine for a given height]
Ideal Cr = IBW x 23 mg/kg male = IBW x 18 mg/kg female
CHI > 80 mild depletion CHI 60 – 80 moderate CHI < 60 severe
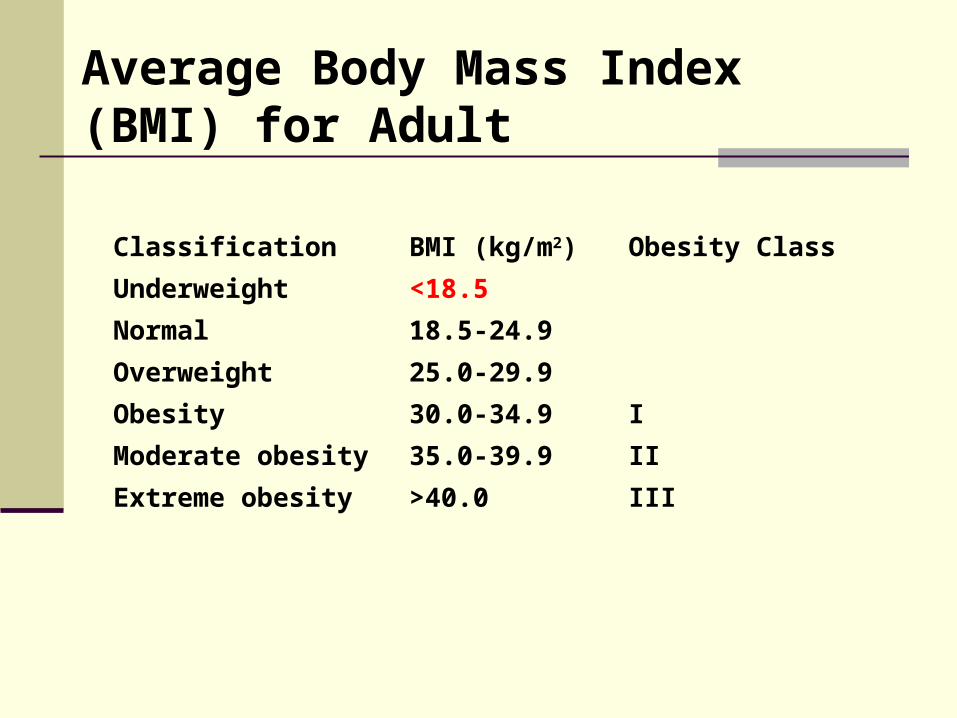
Classification BMI (kg/m2) Obesity Class
Underweight <18.5
Normal 18.5-24.9
Overweight 25.0-29.9
Obesity 30.0-34.9 I
Moderate obesity 35.0-39.9 II
Extreme obesity >40.0 III
Average Body Mass Index (BMI) for Adult
Nutrition Provides
Energy Amino Acid Fluid & Electrolyte Trace minerals (elements) Vitamin Certain drugs

Fluid Requirement
Fluid Requirement
Amount of fluid requirement needed depend on age Pediatric: 1st 10kg = 100ml/kg 2nd 10kg = 50ml/kg 3rd 10kg & up 20ml/kg
Adult: 30-35ml/kg
Additional fluid for vomiting, nasogastric tubeoutput, diarrhea, large open wound, fever, hyperventilation, fistula drainage.
Fluid Requirements
Special situation for fluid restriction: Fluid overload, Cardiac, Renal, or Liver failure Elderly MedicationNRC* recommends 1 to 2 ml of water for
each kcalof energy expenditure*NRC= National research council
Energy Requirements
Total Energy Expenditure
TEE (kcal/day) = BEE x stress/activity factor
BEE: The Harris-Benedict equation is a
mathematical formula used to calculate BEE
Harris-Benedict Equation
Women = 655 + (9.6 x wt) + (1.7 x ht) - (4.7 x
age)
Men =66 + (13.7 x wt) + (5 x ht) - (6.8 x
age)
Calories Multiply by stress factor

A correlation factor that estimates the extent
of hyper-metabolism
1.15 for bedridden patients 1.10 for patients on ventilator support 1.25 for normal patients The stress factors are: 1.3 for low stress 1.5 for moderate stress 2.0 for severe stress 1.9-2.1 for burn
Calories Requirements
Obesity: 18-20kcal/kg/day of IBW
Normal need: 25-30kcal/kg/day
Elective surgery: 28-30kcal/kg/day
Severe injury: 30-40kcal/kg/day
Extensive trauma/burn: 40-45kcal/kg/day
Carbohydrate
Primary energy substrate The amount of carbohydrate is
determined by patient’s calorie requirement glucose oxidation rate optimal balance of carbohydrate and fat
Maximum oxidized rate 4 - 7mg/kg/min (adult).
Carbohydrate
Provide from a non nitrogen source
Energy requirement depends on number of factors!
Stress factors, increase calories requirements
60% - 80% of caloric requirement as glucose
CHO Oxidation Rate
1gm = 3.4kcal Kcl ÷ 3.4 x 1000 ÷ 1440 ÷ wt kg = not more than 5mg/kg/min e.g. 1700 ÷ 3.4 x 1000 ÷ 1440 ÷ 70 = 4.9mg/kg/min or 5 mg x 3.4 ÷ 1000 x wt x 1440 5 x 3.4 ÷ 1000 x 70 x 1440 = ~ 1700
kcal

Carbohydrate Source
Starting with: 200 - 250 gm or 15% dextrose solution
started or 2.5 mg/kg/min 100 - 150 gm or 10% - 15% dextrose
solution in stress & DM
Increase gradually up to 5 mg/kg/min, Max 7 mg/kg/min

How to Calculate Percentage
Total volume of fluid x 3.4 x %
e.g. 2000ml x 3.4 x 0.20 = 1360 kcal.
Or
1400 ÷ 3.4 ÷ 2000ml = 20% as started then 1700 ÷ 3.4 ÷ 2000ml = 25% full requirement

Protein (Amino Acid)
AAs are the vital components of body protein. The
primary aim of providing AAs to the body is to prevent: Disease related catabolic state. The development of manifest protein deficiency
with subsequent impaired wound healing. Disturbances of blood clotting. The impairment of hepatic and renal function. A reduced immuno-competence.
Protein (Amino Acid)
1g of protein = 4 Kcal 1g of nitrogen is equivalent to 6.3g of protein Non-protein k.cal: nitrogen 150-200: 1 (normal patient) Note: In renal and hepatic failure the ratio is 1:300-400.
Adult dose: Normal patients requirement 0.8-1.0 g/kg
max. 2.5g/kg depend on patient status Renal failure patient 0.6 g/kg
Protein (Amino Acid)
12% - 16% of calories as protein
Note: Products containing only essential Aas
have been formulated for renal failure.
BCAA (Branched Chain Amino Acids) are used for Hepatic Encephalopathy or in severely stressed patients.

Fat Emulsion
Essential linoleic acid stabilized by egg yolk phospholipids
Delivered in the form of an emulsion fat emulsion has no isotonicity by itself,
glycerol is added to render emulsion isotonic (300 mosm/l).
Concentrated source of calories Source of essential fatty acids (EFAs) Substitute for carbohydrate in diabetic &
fluid restricted patients

Fat Emulsion
Fat should provide 20-40% of total calories.
Fat provides a concentrated caloric source. 1g provide 10 Kcal.
Also fat is an alternative source to dextrose to the patients with compromised respiration since it does produce little CO2 in its metabolism. While dextrose, when oxidized, it produces CO2 which must be eliminated via lungs.
Start with 0.5g/kg/d gradually up to1.5g/kg/d.
Administer over 12hr or max rate 15ml/hr
The caloric density 10% FE is 1.1 kcal/ml 20% FE is 2 kcal/ml 30% FE is 3 kcal/ml
There is LCT, and MCT/LCT products 1gm = 9kcal of fat Each 1ml = 2kcal
Lipid emulsions contain glycerol, so lipid emulsion does not have 9 kcal per gram as it would if it were pure fat. Some use 10 kcal/gm for lipid emulsions.
Propofol: Soybean oil in water emulsion, 1ml - 1.112kcal
Fat Emulsion

Fat Emulsion Contraindications
Hyperlipdemia Acute pancreatitis Previous history of fat embolism Severe liver disease Allergies to egg, soybean oil or safflower
oil

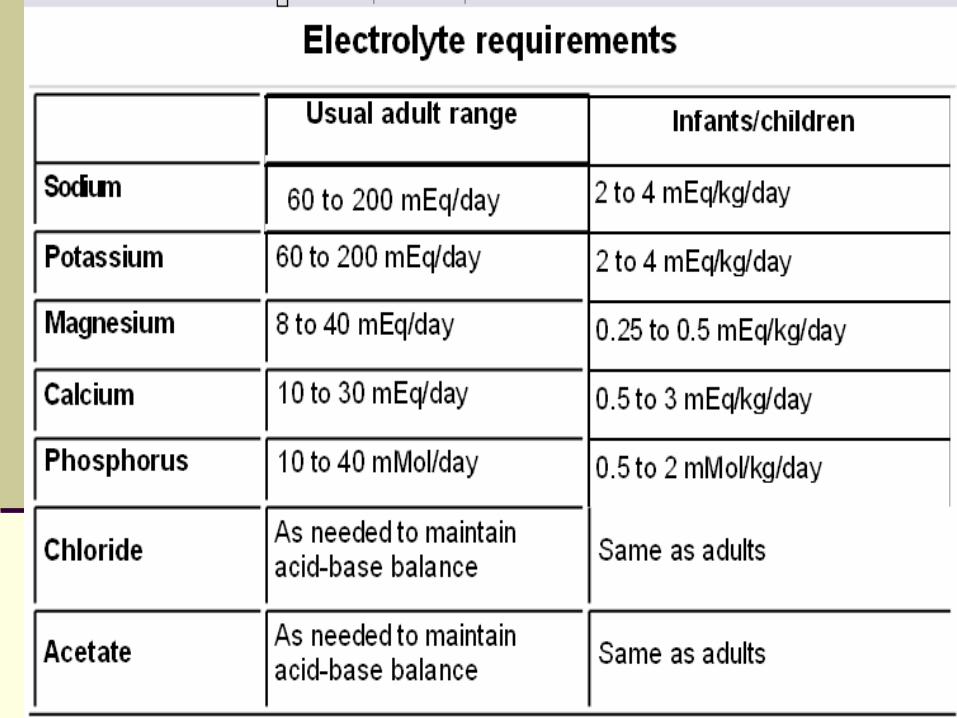
Electrolytes
Na, K, CL, Ca, Mg, PO4, & acetate.
Electrolytes given to maintain normal serum concentration or to correct deficit.
Requirements for specific electrolytes will vary according to the patients disease state
Restrict electrolytes
Severe renal dysfunction. Edema & congestive heart failure. Patients on corticosteroids. Metabolic acidosis, acute pancreatitis
fistulas, or diarrhea. Metabolic alkalosis, vomiting.
Multivitamins
B – Complex: Co-enzyme in absorptive and metabolic processes,
transfer of energy from protein, fat and carbohydrate to the cells and their
storage as ATP.
Ascorbic Acid: Required for collagen synthesis, wound healing. An
additional amount may be required in major burns, traumas, and extensive
surgeries.
Vitamin A: Essential for vision, the production of mucus-secreting
epithelial cells and bone growth.
Vitamin D: For calcium and phosphate hemeostasis and boncalcification.
Vitamin K: For prothrombin generation (Fibrin Fibrinogen).
Vitamin K
TPN solution does not contain vitamin K and it can predispose patient to deficiency
Vitamin K 10 mg should be given weekly IV or IM if patient is on long-term TPN

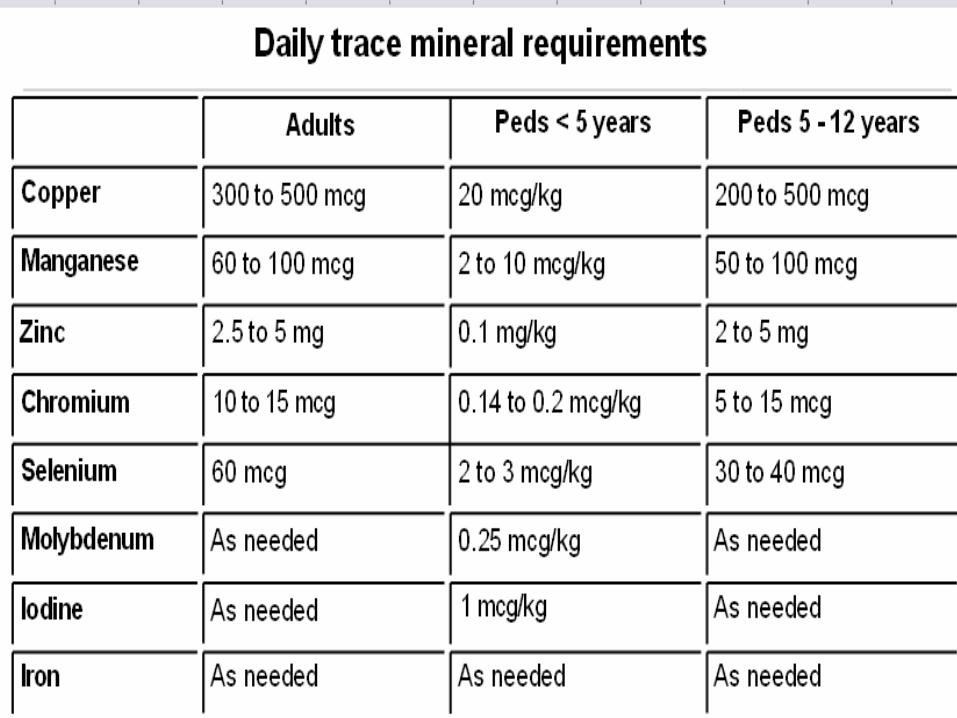
Multivitamin and Trace Minerals
Standard form of multivitamin & trace mineral use.
Zinc, copper, manganese & chromium. Additional of trace mineral required
depend on GI losses. Renal failure patients reduce dose Biliary stasis disease, avoid copper &
manganese

Additives
INSULIN: For hyperglycemia when glucose is spilling in urine.
HEPARIN: To promote blood circulation (especially with
peripheral TPN) and to prevent thrombophlebitis.
HYDROCORTISONE: To prevent thrombophlebitis in patients receiving peripheral TPN.
ACETATE: For acidosis.
ZINC: Extra amount is needed for patient with severe stress,
diarrhea, and ileostomy.
Status of Organic failure
Hypermetabolism Tachycardia, Tachypnea, Fever,
Leucocytosis
Hypercatabolism Hyperglycemia, Uremia,
Hypertriglyceridemia, -NB

Renal Failure Considerations
Present with problems of volume limitation and poor tolerance of nitrogen wastes.
Treated with 0.5-0.6g/kg amino acid, higher glucose and lipid concentration.
Limit amounts of sodium, potassium, magnesium, and phosphate.
Liver Failure Considerations
Inability to tolerate large fluid volume and difficulty with nitrogen loads
Maintain glucose
Supply moderate protein(1.0-1.3g/kg) and fat intake up to 30% of T.k.calorie
Restrict fluid and salt intake
BCAA
Fluid Restricted Considerations
As pulmonary, cardiac failure, head injuries, and elderly.
Special concentrated TPN solution.
High fat emulsion, low glucose.
Normal protein requirement.
Normal electrolyte.

Respiratory Failure
Non-protein calories to nitrogen ration is not a major consideration.
Major problem total calories, either from CHO or fat or both
Protein increases oxygen consumption demands and that is not indicated to reducing protein

Going to surgery
In postoperative surgical patients; TPN is indicated if the patient is indicatedto stay NPO for 5 – 7 days in malnourished patients, and 7 – 10 days in well-nourished patients.
In preoperative patients;TPN should be considered in patients who cannot or should not eat for more than 3 –
5 days.
Practice Guidelines Preoperative
NS should be administered for 7-14 days to moderately or severely malnourished patients undergoing major GI surgery
PN should NOT be routinely given in the
immediate postoperative period to patients undergoing major GI procedures

OR Patient
Hold TPN during OR if it more than 1 1/2 hrs
2hrs pre-operation: ↓ TPN rate 50% for 1hr Hold TPN Start D10% infusion at same TPN rate
6hrs post – operation Start new TPN bottle at 50% of TPN rate for 1hr ↑ TPN rate as in order
MONITORING BLOOD SUGAR
Routes of Nutrition Support


Enteral Nutrition
Enteral Nutrition Indication
Inability to consume or absorb adequate nutrition
e.g. who do not eat or receive nutrition support for ≥10-14 days after hospital admission
Functional or partially functional gute.g. who are unable or not allowed to eat, or partial
functional gut
Potential benefits of EN over PN Nutrients are metabolized and utilized
more effectively via the enteral than parenteral route
Gut and liver process EN before their release into systemic circulation
Gut and liver help maintain the homeostasis of the AA pool and skeletal muscle tissue
EN (Immunologic)
Gut integrity is maintained by enteral feeding and prevent the bacterial translocation from the gut and minimize risk of gut related sepsis

Enteral nutrition (EN)
Long-term nutrition: Gastrostomy Jejunostomy
Short-term nutrition: Nasogastric feeding Nasoduodenal feeding Nasojejunal feeding

Benefits of EN
Physiological/metabolic benefits The gut can be used for administration of complex
nutrients that cannot be given intravenously e.g. intact protein, peptides, fiber
Safety benefitsSafer than PN and less side effects
Cost benefits

Contraindication to EN
Terminal illness Short bowel Obstruction GI bleeding Vomiting and diarrhea Fistulas GI ischemia Illues GI inflammation A. pancreatitis

Enteral Nutrition Complications
Mechanical complication During placement of feeding tube
Airway injury, infection, ↑ICP Presence of a feeding tube Tube clogging Declogging methods Aspiration
GI complication Gastroesophageal reflux duodenal gastric reflux Diarrhea Metabolic complication
Enteral Nutrition Complications
Metabolic complication Hyperglycemia Electrolyte and mineral deficiences Refeeding syndrome
Total Parentral Nutrition

Total Parenteral Nutrition Indication
When normal oral feeding is not possible.e.g.: Chron’s disease, gastric & esophageal
carcinoma, paralytic ileus, generalized peronitis, GI. obstruction, intractable vomiting.
When food is incompletely absorbed.e.g.: Major burns, multiple injuries, radiation
therapy, ulcerative colitis, chemotherapy treatment, short bowel syndrome.
When food intake is undesirable, in case it is prudent to rest the bowel.
e.g.: Post GIT surgery, chronic inflammatory diseases, intractable diarrhea.
Total Parenteral Nutrition Indication
In patients who are able to ingest food, but refuse to do so.
e.g.: Geriatric post-operative patients, adolescents with anorexia nervosa, some psychiatric patients with prolonged depression.
In patients who, as a consequence of their illness are going to be, or have been NPO for 5 – 7 days.
Administration
Parenteral Nutrition
Central Nutrition Subclavian line Long period Hyperosmolar
solution Full requirement Minimum volume Expensive More side effect
Peripheral nutrition Peripheral line Short period <
14days Low osmolality < 900 mOsm/L Min. requirement Large volume Thrombophlebitis
Routes of TPN
Central TPN(usual osmolarity = 2000 mosmol/L)Advantages: Can provide full nutritional support (No limits in concentration of dextrose and amino
acids) No risk of thrombophlebitis, No pain.Disadvantages: Requires surgery More risk of sepsis than peripheral TPN High risk of mechanical complications
Routes of TPN
Peripheral TPN
maximum osmolarity;neonates = 1100/L, Pediatrics = 1000/L, Adults = 900/L
Advantages: Does not require surgery Less risk of sepsis than central TPN No risk of mechanical complications
Disadvantages: High risk of thrombophlebitis Painful Does not provide full nutrition support. Needs more fluids to provide more nutrition. (maximum dextrose = 7.5% and AA = 2.5%).

Note
PPN can infuse through central line but
central TPN can NOT infuse through
the peripheral line

Calculating the Osmolarity of a Parenteral Nutrition Solution
Multiply the grams of dextrose per liter by 5. Example: 100 g of dextrose x 5 = 500 mOsm/L
Multiply the grams of protein per liter by 10. Example: 30 g of protein x 10 = 300 mOsm/L
Multiply the (mEq per L sodium + potassium + calcium + magnesium) X 2
Example: 80 X 2 = 160
Total osmolarity = 500 + 300 + 160 = 960 mOsm/L

Monitoring
Monitoring
Avoid overfeeding Avoid respiratory problem Promote nitrogen retention Triglyceride clearance Fluid and electrolyte Weight Liver function
Monitoring for Complications
Malnourished patients at risk for refeeding syndrome should have serum phosphorus, magnesium, potassium, and glucose levels monitored closely
In patients with diabetes or risk factors for glucose
intolerance, insulin infusion should be initiated with a low dextrose infusion rate and blood and urine glucose monitored closely.
Blood glucose should be monitored frequently upon initiation, any change in insulin dose, and until measurements are stable.
Monitoring for Complications
Serum electrolytes (sodium, potassium, chloride, and bicarbonate) should be monitored frequently until measurements are stable.
Patients receiving intravenous fat emulsions
should have serum triglyceride levels monitored until stable and when changes are made in the amount of fat administered.
Liver function tests should be monitored periodically in patients receiving PN.

Complications of TPN

Complication
Mechanical: occlusion, catheter removal, improper rate, thromboses, pneumothorax.
Infection: catheter related
Metabolic: re-feeding syndrome, hyperglycemia, fluid & electrolyte disturbance
(cont..)

Complication
Organic system: hepatobiliary complication respiratory cardiovascular renal
Transitional Feeding
Maintain full PN support until pt is tolerating 1/3 of needs via enteral route
Decrease TPN by 50% and continue to taper as the enteral feeding is advanced to total
TPN can reduce appetite if >25% of calorie needs are met via PN
TPN can be tapered when pt is consuming greater than 500 calories/d and d-c’d when meeting 60% of goal
TPN can be rapidly d-c’d if pt is receiving enteral feeding in amount great enough to maintain blood glucose levels

Defense Against NS Complications
Select appropriate patients to appropriate nutrition
Aseptic technique Do not overfeed
Maintain glycemic control <150-170 mg/dl Limit lipids to 1 gm/kg and monitor TG levels Adjust protein based on metabolic demand
and organ function Monitor fluid/electrolyte/mineral status Provide standard vitamin and trace
element preps daily

Thank you