Embed Size (px)
Citation preview

http://ncp.sagepub.com/Nutrition in Clinical Practice
http://ncp.sagepub.com/content/28/6/639The online version of this article can be found at:
DOI: 10.1177/0884533613508435
2013 28: 639 originally published online 31 October 2013Nutr Clin PractAinsley Malone and Cynthia Hamilton
Consensus Malnutrition Characteristics: Application in PracticeThe Academy of Nutrition and Dietetics/The American Society for Parenteral and Enteral Nutrition
Published by:
http://www.sagepublications.com
On behalf of:
The American Society for Parenteral & Enteral Nutrition
can be found at:Nutrition in Clinical PracticeAdditional services and information for
http://ncp.sagepub.com/cgi/alertsEmail Alerts:
http://ncp.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Oct 31, 2013OnlineFirst Version of Record
- Nov 21, 2013Version of Record >>
at A.S.P.E.N on July 9, 2014ncp.sagepub.comDownloaded from at A.S.P.E.N on July 9, 2014ncp.sagepub.comDownloaded from

Nutrition in Clinical PracticeVolume 28 Number 6 December 2013 639 –650© 2013 American Societyfor Parenteral and Enteral NutritionDOI: 10.1177/0884533613508435ncp.sagepub.comhosted at online.sagepub.com
Invited Review
The recognition of malnutrition in adult hospitalized patients has existed for almost 40 years. Beginning with the classic 1974 article “The Skeleton in the Hospital Closet” by Dr Charles Butterworth and subsequent work by Drs George Blackburn and Bruce Bistrian, nutrition clinicians have contin-ued to recognize the importance of assessing hospitalized patients for malnutrition risk and document the presence of malnutrition.1,2 The 1977 publication by Blackburn and Bistrian offered a well-defined methodology for malnutrition assessment based on the prevailing understanding of disease pathophysiology and nutrient metabolism.2
In 2007, the Centers for Medicare and Medicaid Services (CMS) altered its reimbursement processes to incorporate a disease severity component of which malnutrition was included.3 Based on an individual patient’s diagnosis(s), the addition of malnutrition as a comorbid condition provides an opportunity for increased reimbursement reflecting a higher cost for delivery of care. As a result of this process change, multiple queries from members of both the Academy of Nutrition and Dietetics (the Academy) and the American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.) as well as from CMS regarding specific malnutrition criteria prompted the creation of an Academy/A.S.P.E.N. Malnutrition Workgroup. This workgroup was charged with developing a standardized approach to diagnosing malnutrition in the adult hospitalized patient
In 2012, the Academy/A.S.P.E.N. Malnutrition Workgroup culminated their work with the publication of the Consensus
Statement: Academy of Nutrition and Dietetics and the American Society for Parenteral and Enteral Nutrition: Characteristics Recommended for the Identification and Docu-mentation of Adult Malnutrition (Undernutrition).4 This paper provided a framework for diagnosing malnutrition using the construct developed by the International Guidelines Group.5 The use of an etiology basis for malnutrition diagnosis is cou-pled with the delineation of specific criteria or characteristics to define malnutrition (Table 1 outlines these general charac-teristics). The authors of this consensus statement outlined a short term “call to action” for clinicians to consider how to begin implementing the recommended characteristics within their practice setting. The purpose of this article is to provide practical strategies for criteria implementation and to describe one institution’s experience in implementing a broad based “malnutrition program” within their healthcare system.
508435 NCPXXX10.1177/0884533613508435Nutrition in Clinical PracticeMalone and Hamiltonresearch-article2013
From 1Mt. Carmel West, Columbus, Ohio; and 2Center for Human Nutrition, Cleveland Clinic, Cleveland, Ohio.
Financial disclosure: None declared.
This article originally appeared online on October 31, 2013.
Corresponding Author:Ainsley Malone, MS, RD, LD, CNSC, Pharmacy Department, Mt. Carmel West, 793 West State St, Columbus, OH 43222, USA. Email: [email protected].
The Academy of Nutrition and Dietetics/The American Society for Parenteral and Enteral Nutrition Consensus Malnutrition Characteristics: Application in Practice
Ainsley Malone, MS, RD, LD, CNSC1; and Cynthia Hamilton, MS, RD, LD2
AbstractMalnutrition in adult hospitalized patients has been a significant issue for almost 40 years. Changes in 2007 to the diagnosis related groups reimbursement methodology, as outlined by the Center for Medicare and Medicaid Services, provided an impetus to improve the diagnosis and documentation of malnutrition in adult patients. Being able to accurately assess, diagnose, and document malnutrition has been challenged by the lack of a standard malnutrition definition. In 2012 a workgroup of the Academy of Nutrition and Dietetics and the American Society for Parenteral and Enteral Nutrition published a consensus paper outlining characteristics for the diagnosis of adult hospital malnutrition. Using the etiology approach for defining malnutrition as outlined by Jensen and colleagues, 6 general characteristics are outlined with specific thresholds to delineate severe and nonsevere malnutrition. The purpose of this article is to provide practical strategies for criteria implementation and to describe one institution’s experience in implementing a broad-based “malnutrition program” within its healthcare system. (Nutr Clin Pract. 2013;28:639-650)
Keywordsnutrition assessment; malnutrition; nutritional status
at A.S.P.E.N on July 9, 2014ncp.sagepub.comDownloaded from

640 Nutrition in Clinical Practice 28(6)
Malnutrition Assessment
Nutrition Risk
As outlined by the consensus document, the first step in assess-ing patients for malnutrition is to identify those patients con-sidered at “risk.” For patients newly admitted to the hospital, this is best accomplished through nutrition screening, a process adopted by the Joint Commission in 1996 as a required prac-tice.6 How hospitals implement this requirement is quite vari-able with some developing their own “screening tool” and others using validated screening tools such as the Malnutrition Screening Tool or the Nutrition Risk Screening 2002.7 Several organizations including A.S.P.E.N. recommend the use of a valid nutrition screening tool to identify those high risk patients who are likely to be malnourished.8 For a more thorough review of applicable nutrition screening tools, please see Skipper et al.9 Other “screening” processes to identify patients “at malnutrition risk” during the course of their hospitalization are of importance since it is well documented that malnutrition can develop while in the hospital despite being normally nour-ished upon admission.10 Such processes are often institution specific and are developed based on hospital demographics, service entities, and/or average length of stay. Processes used
for ongoing risk assessment have not been studied or well described. Examples of specific components to monitor for malnutrition risk may include diet order, length of time with suboptimal nutrient intake, oral diet intake, and participation in multidisciplinary rounds.
Inflammation
Once nutrition risk has been identified, using an etiology approach to describing malnutrition will involve assessing the patient for the presence of inflammation. It is now well under-stood that inflammation is a potent contributor to disease related malnutrition and is a not a valid marker of nutrition status.11 Initially the inflammatory response is a desired response to a host “insult” and is generally self limiting.12 It is when the response becomes exaggerated and prolonged that its effects on nutrition status can be profound.11 While there is no one “parameter” to verify the presence of inflammation, a con-stellation of measures including those from the laboratory as well those demonstrated clinically by the patient may be useful in delineating the presence of inflammation. Table 2 outlines these potential parameters.
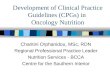
The influence of inflammation on visceral protein levels is now well established and as such these “negative acute phase proteins” may be considered to reflect the presence of inflam-mation.11 While the specific level of a particular visceral pro-tein cannot in of itself specify the severity of the inflammatory response, it can be evaluated in the context of the patient’s overall clinical picture. Congruent to this understanding is the potential for “positive acute phase proteins” such as C-reactive protein (CRP),11 to assist in identifying inflammation. In response to infection or tissue inflammation, CRP production is stimulated by several cytokines, particularly, interleukin-6, interleukin-1, and tumor necrosis factor-alpha. Like many acute phase proteins, CRP increases rapidly and dramatically in response to a variety of infectious or inflammatory condi-tions.12,13 Significantly elevated CRP levels have been demon-strated in the presence of infection and sepsis,13 while lower levels are more common in low-lying inflammatory states such as obesity, malignancies, and chronic organ failure.14-17 Table 3 outlines various acute and chronic disease entities where inflammation is likely to be present. Once inflammation along with its severity has been identified, the patient will be further assessed. If malnutrition is identified based on the specific cri-teria, the etiology of that patients malnutrition will be deter-mined using the algorithm outlined in Figure 1.
Malnutrition Characteristics
The Academy/A.S.P.E.N. Malnutrition workgroup identified 6 characteristics to assess for the presence of malnutrition. If a patient demonstrates 2 or more characteristics, malnutrition can be diagnosed with its severity further defined via specific thresholds and/or descriptives. Tables 4 and 5 outline the 6
Table 1. General Characteristics for the Diagnosis of Malnutrition.4
•• Weight loss•• Inadequate energy intake•• Loss of muscle mass•• Loss of subcutaneous fat•• Fluid accumulation•• Hand grip strength
Table 2. Parameters Useful to Assess for Inflammation.4
Laboratory Clinical
● Decreased serum albumin ● Fever● Decreased serum transferrin ● Hypothermia● Decreased serum prealbumin ● Presence of infection● Elevated C-reactive protein ● Urinary tract infection● Elevated blood glucose ● Pneumonia● Decreased or increased white
blood cell count● Blood stream infection● Wound or incisional
infection● Abscess
● Increased percentage of neutrophils in the cell differential
● Decreased platelet count● Marked negative nitrogen
balance
at A.S.P.E.N on July 9, 2014ncp.sagepub.comDownloaded from

Malone and Hamilton 641
Table 3. Association of Acute and Chronic Conditions Associated With the Inflammatory Response.20
Acute Disease—Severe Inflammatory Response Chronic Disease—Mild to Moderate Inflammatory Response
Adult respiratory distress syndrome Cardiovascular diseaseClosed head injury Celiac diseaseCritical illness Chronic pancreatitisMajor abdominal surgery Chronic obstructive pulmonary diseaseMajor infection/sepsis Congestive heart failureMultitrauma Cystic fibrosisSystemic inflammatory response syndrome DementiaSevere burns Diabetes mellitusSevere acute pancreatitis Inflammatory bowel disease Hematologic malignancies Metabolic syndrome Neuromuscular disease Obesity Organ failure/transplant (kidney, liver, heart, lung, or gut) Pressure wounds Rheumatoid arthritis Solid tumors
Adapted from A.S.P.E.N. Adult Nutrition Support Core Curriculum, 2nd ed.
Figure 1. Etiology approach to the diagnosis of malnutrition.Based on Jensen et al.11
at A.S.P.E.N on July 9, 2014ncp.sagepub.comDownloaded from

642 Nutrition in Clinical Practice 28(6)
characteristics and their respective thresholds for both severe and nonsevere (moderate) malnutrition. Gathering the respec-tive data to determine if malnutrition is present requires a sys-tematic approach beginning with review of the patient’s medical record, verbal discussion with the patient and/or care-giver coupled with physical assessment. The following infor-mation will highlight each of the 6 malnutrition characteristics and offer further detail specific to their use.
Weight Loss
Assessing weight loss in a specific patient requires the ability to obtain the patient’s usual or previous body weight along with his or her current weight. Admission weight is frequently obtained by the admitting clinician as either an actual or reported measurement. Caution must be exercised in evaluat-ing admission weights in those patients who have been fluid resuscitated or who are demonstrating signs of dehydration. In these settings, it will require further assessment by the clinician to ascertain the patient’s “dry” weight for evaluation. When interviewing the patient and/or caregiver, the clinician must identify the patient’s “usual” body weight and at what point in time the patient demonstrated that weight. This can be difficult for the patient and/or caregiver to remember. Often times it
may coincide with a recent surgical procedure or before the patient was diagnosed with his or her current disease entity.
It may be that the clinician can obtain a patient’s previous weight from a recent hospitalization or from information avail-able at the physician’s office. If the nutrition assessment is being conducted during the patient’s hospitalization, the admission weight can be compared to the patient’s current weight for evaluation.2,18,19
Certain factors may contribute to inaccuracies with obtain-ing weight loss information. In addition to the underlying fluid status, which can mask weight loss, other factors include the inability of the patient to recall his or her weight correctly as well as equipment error and measurement/documentation error.20
Insufficient Energy Intake
Identifying how well a newly admitted patient has been able to consume nutrients is best achieved through verbal questioning of the patient and/or caregiver. In those who have been hospi-talized, reviewing meal intake data, assessing “calorie counts,” and/or reviewing enteral/parenteral intake via intake and out-put records will provide data for assessment. It should be noted that “calorie counts” can be problematic in providing adequate
Table 4. Characteristics to Diagnose Severe Malnutrition.4
CharacteristicAcute Illness or Injury Related
MalnutritionChronic Disease Related
MalnutritionSocial or Environmental Related
Malnutrition
Weight loss >2%/1 week >5%/1 month >5%/1 month >5%/1 month >7.5%/3 months >7.5%/3 months >7.5%/3 months >10%/6 months >10%/6 months > 20%/1 year > 20%/1 yearEnergy intake ≤50% for ≥5 days ≤75% for ≥1 month ≤50% for ≥1 monthBody fat Moderate depletion Severe depletion Severe depletionMuscle mass Moderate depletion Severe depletion Severe depletionFluid accumulation Moderate → severe Severe SevereGrip strength Not recommended in intensive
care unitReduced for age/gender Reduced for age/gender
Table 5. Characteristics to Diagnose Nonsevere (Moderate) Malnutrition.4
CharacteristicAcute Illness or Injury Related
MalnutritionChronic Disease Related
MalnutritionSocial or Environmental Related
Malnutrition
Weight loss 1%-2%/1 week 5%/1 month 5%/1 month 5%/1 month 7.5%/3 months 7.5%/3 months 7.5%/3 months 10%/6 months 10%/6 months 20%/1 year 20%/1 yearEnergy intake <75% for >7 days <75% for ≥1 month <75% for ≥3 monthsBody fat Mild depletion Mild depletion Mild depletionMuscle mass Mild depletion Mild depletion Mild depletionFluid accumulation Mild Mild MildGrip strength Not applicable Not applicable Not applicable
at A.S.P.E.N on July 9, 2014ncp.sagepub.comDownloaded from

Malone and Hamilton 643
data for evaluation. For those newly admitted patients who have been able to consume oral foods, information should be obtained from the patient and/or caregiver as to the patient’s general meal intake over a specific period.20-21 In those who have been previously or are currently hospitalized, identifying periods of inadequate intake will assist in delineating the over-all percentage of a patient’s energy intake he or she has been able to achieve.
The objective data obtained from medical record review and/or patient/caregiver interview will be compared to the patient’s estimated energy requirements. This will then deter-mine the specific percentage of requirements the patient has achieved and therefore which severity level is demonstrated for this characteristic. Requirements can be measured via indi-rect calorimetry, for example in the critically ill patient, or can be estimated with prediction equations such as Mifflin St-Jeor or Penn State.22-23
Physical Assessment Components
Three of the 6 malnutrition criteria are those that must be deter-mined through performance of a nutrition focused physical exam. This aspect of physical assessment is an important con-tribution by the registered dietitian (RD) as when coupled with the patient interview it can provide sufficient data to diagnose the presence of malnutrition. Nutrition-focused physical assessment will assist in identifying the presence of muscle and/or subcutaneous fat loss, the presence of fluid accumula-tion, along with the severity of these characteristics. Tables 6 and 7 outline specific areas of the body to assess for fat and muscle loss along with details for delineating severity of the loss, if applicable.
Nutrition-focused physical exam is a component of the nutri-tion care process and is an important competency for all RDs. This component of dietetic practice is included in the Academy of Nutrition and Dietetics: Revised 2012 Standards of Practice
in Nutrition Care and Standards of Professional Performance for Registered Dietitians.24 In the Nutrition Assessment Standard 1.3, “each RD shall assess nutrition focused physical findings including those, among others, muscle and subcutaneous fat wasting and signs of edema.”24 In addition, the Accreditation Council for Education in Nutrition and Dietetics has included nutrition-focused physical assessment as a competency for supervised practice program participants. Performing nutrition focused physical assessment is increasing among RDs. Compared to the 1995 and 2000 Dietetics Practice Audits, Mackle and colleagues in 2003 demonstrated greater use of physical assessment parameters by RDs.25
The presence of fluid accumulation is accessed via physical exam evaluating both the presence of local and/or generalized accumulation.4 It is important to first evaluate overall fluid sta-tus to help determine other etiologies for any fluid accumula-tion. Areas useful to assess include the lower and upper extremities, face and eyes, the scrotal area and ascites. In those patients with underlying disease states such as congestive heart failure or chronic kidney disease, discerning fluid accumula-tion due to malnutrition will be difficult. Table 8 outlines 1 method for assessment of edema.
Hand Grip Strength
Hand grip strength has been validated as a proxy for lean body mass and as such was chosen by the workgroup as an important functional parameter in assessing for malnutri-tion.4,26 Assessment of grip strength is performed via a dyna-mometer by those experienced/trained in its use. Abnormal grip strength measurements will be based on the specified dynamometer utilized. Diseases and/or conditions that limit the patient’s ability to perform a valid hand grip strength mea-surement must be considered including, among others, rheuma-toid arthritis, cerebrovascular accident, neuromuscular disease, and dementia. In addition, patients who are heavily sedated and/
Table 6. Specific Areas to Assess for Subcutaneous Fat Loss.
Exam Areas Tips Severe MalnutritionMild-Moderate
Malnutrition Well Nourished
Orbital Region –Surrounding the Eye
View patient when standing directly in front of them, touch above the cheekbone
Hollow look, depressions, dark circles, loose skin
Slightly dark circles, somewhat hollow look
Slightly bulged fat pads. Fluid retention may mask loss
Upper Arm Region: Triceps/biceps
Arm bent, roll skin between fingers, do not include muscle in pinch
Very little space between folds, fingers touch
Some depth pinch, but not ample
Ample fat tissue obvious between folds of skin
Thoracic and Lumbar Regions: Ribs, Lower back, Midaxillary line
Have patient press hands hard against a solid object
Depression between ribs very apparent. Iliac Crest very prominent
Ribs apparent, depressions between them less pronounced. Iliac Crest somewhat prominent
Chest is full; ribs do not show. Slight to no protrusion of the Iliac Crest
Reprinted with permission from White JA. Nutrition Care Manual. Academy of Nutrition and Dietetics; 2013.
at A.S.P.E.N on July 9, 2014ncp.sagepub.comDownloaded from

644 Nutrition in Clinical Practice 28(6)
or unresponsive such as those in the intensive care unit (ICU) will be unable to complete hand grip measurements.
Some practitioners have chosen not to utilize hand grip strength7 in assessing for malnutrition. Other parameters that
could be considered for functional assessment include general performance status, ability to perform activities of daily living, ability to tolerate physical therapy, and ability to wean from mechanical ventilation. Validity and usability testing of addi-tional functional parameters will shed light on alternate param-eters that may be useful in addition to grip strength.
General Considerations in Applying the Malnutrition Characteristics
When evaluating a patient’s specific malnutrition criteria the possible etiologies for malnutrition may not always be clear. It may be that the patient’s characteristics fit within >1 etiology, for example, in both acute illness and chronic disease related malnutrition. The malnutrition etiology can change as clinical course evolves which is why characteristics should be rou-tinely assessed at frequent intervals. Some degree of 1 or more
Table 7. Specific Areas to Assess for Muscle Loss.
Exam Area Tips Severe MalnutritionMild-Moderate
Malnutrition Well Nourished
Temple Region: Temporalis Muscle
View patient when standing directly in front of them, ask patient to turn head side to side
Hollowing, scooping, depression
Slight depression Can see/feel well defined muscle
Clavicle Bone Region: Pectoralis Major, Deltoid, Trapezius Muscles
Look for prominent bone. Make sure patient is not hunched forward
Protuding, prominent bone Visible in male, some protrusion in female
Not visible in male, visible but not prominent in female
Clavicle and Acromion Bone Region: Deltoid Muscle
Patient arms at side: observe shape
Shoulder to arm joint looks square, bones prominent; acromion protrusion very prominent
Acromion process may slightly protrude
Rounded, curves at arm/shoulder/neck
Scapular Bone Region: Tapezius, Supraspinus, Infraspinus Muscles
Ask patient to extend hands straight out, push against solid object.
Prominent, visible bones, depressions between ribs/scapula or shoulders/spine
Mild depression or bone may show slightly
Bones not prominent, no significant depressions
Dorsal Hand: Interosseous muscle
Look at thumb side of hand; look at pads of thumb when tip of forefinger touching tip of thumb
Depressed area between thumb–forefinger
Slightly depressed Muscle bulges, could be flat in some well nourished people
Lower body less sensitive to change Patellar Region:
Quadricep MuscleAsk patient to sit with leg
propped up bent at kneeBones prominent, little sign
of muscle around kneeKnee cap less
prominent, more rounded
Muscles protrude, bones not prominent
Anterior Thigh Region: Quadricep Muscles
Ask patient to sit prop leg up on low furniture; grasp quads to differentiate amount of muscle tissue from fat tissue.
Depression/line on thigh, obviously thin
Mild depression on inner thigh
Well rounded, well developed
Posterior Calf Region: Gastrocnemius Muscle
Grasp the calf muscle to determine amount of tissue
Thin, minimal to no muscle definition
Not well developed Well-developed bulb of muscle
Reprinted with permission from White JA. Nutrition Care Manual. Academy of Nutrition and Dietetics; 2013.
Table 8. Assessment of Edema.
1+ 2 mm depression, barely detectableImmediate rebound
2+ 4mm deep pitA few seconds to rebound
3+ 6 mm deep pit10-12 seconds to rebound
4+ 8 mm: very deep pit>20 seconds to rebound
Based on Hogan M. Medical-Surgical Nursing. 2nd ed. Salt Lake City, UT: Prentice Hall; 2007.
at A.S.P.E.N on July 9, 2014ncp.sagepub.comDownloaded from

Malone and Hamilton 645
characteristics may be present in patients without malnutrition. Conversely, characteristics may not be present in patients at high risk for malnutrition. These patients are likely those who are well nourished prior to admission and due to the nature of their illness are considered “high risk,” that is, the burn or mul-tiple trauma patient. Close and frequent monitoring of these patients will be essential as nutrition status may certainly change as clinical condition changes.4,19
In addition, it is important to point out that the use of an etiology approach in the diagnosis and documentation of malnutrition in a specific patient should lead to collaborative efforts between the RD and the physician. Confirmation of the RD’s findings and malnutrition nutrition diagnosis can result in accurate documentation in the medical record and most impor-tantly timely and appropriate nutrition intervention
The following 2 patient cases highlight the application of the malnutrition characteristics in assessing for malnutrition. These were patients presented to this author’s facility, a 450-bed teaching institution.
Patient Case 1
Admission History
A 24-year-old female was admitted directly from her physi-cian’s office for “malnutrition” secondary to gastroparesis. She had been referred to this surgeon for evaluation of gastric pacer placement. Her chief complaints involved early satiety, nausea, and vomiting over 6 months. The severity of her symptoms had worsened over the past month.
Past Medical History
This was unremarkable other than for admitting diagnosis.
Nutrition Risk Assessment
Admission nutrition screen: Malnutrition Screening Tool Score of 5—referral to RD. RD completed nutrition assessment in next 24 hours.
Clinical Presentation
Anthropometrics. Height: 62 inchesCurrent weight: 68 poundsWeight 1 year ago: 110 poundsWeight 3 months ago: 90 poundsWeight 1 month ago: 80 pounds
Diet history. Complained of early satiety after taking minimal amounts of liquids and foods. Was drinking 4 ounces of a high-calorie oral nutrition supplement and taking small amounts of soft foods twice per day over past 3 months. Intake over recent month averaged only 8 ounces of a high-calorie oral nutrition supplement per day.
Physical assessment. Head/face: severe temporal wastingShoulders/torso: Prominent scapula and clavicle; severe rib
prominenceArms: severe loss of subcutaneous fat in triceps areaLower extremities: prominent knee bone with noted loss of
quadriceps muscleNo evidence of fluid accumulation in upper or lower
extremities
Clinical data. White blood cells: normalTemperature: 98.4°FSerum albumin level: 4.3 g/dLPrealbumin: 15.6 mg/dL
Functional status. Patient was unable to perform her activities of daily living (ADLs) and was living with her parents who were assisting in her care.
What Is This Patient’s Nutrition Status?
Severe malnutrition related to social/environmental circum- stances.
No evidence of inflammationShe meets several criteria for this diagnosis:
Weight loss•• 1 year– 38%•• 3 months: 24%•• 1 month: 15%
Energy intake•• Over last month: 360 kcal/day•• Estimated over last 3 months: 600 kcal/day•• <50% of estimated energy requirements (1225 kcal/day)
Physical assessment•• Severe loss of both muscle and subcutaneous fat in mul-
tiple areas
Functional assessment•• Unable to perform ADLs—severe impairment
This patient achieved 4 of the 6 defined criteria along with functional impairment. The RD collaborated with the patient’s physician and determined that enteral feeding initiation would be the most appropriate nutrition intervention to begin nutri-tion repletion.
Patient Case 2
Admission History
A 59-year-old male was admitted from the Emergency Department with acute rectal bleeding. Colonoscopy on hospi-tal day (HD) 3 revealed a partially obstructing midrectal mass
at A.S.P.E.N on July 9, 2014ncp.sagepub.comDownloaded from

646 Nutrition in Clinical Practice 28(6)
suspicious for malignancy. On HD 6, the patient underwent a lower anterior resection (colon) with anastomosis.
Past Medical History
Cholecysectomy due to cholelithiasis; status post endo scopic ret-rograde cholangiopancreatography 9 months prior to admission.
Diabetes mellitus–type 2
Nutrition Risk Assessment
Admission nutrition screen: Malnutrition Screening Tool Score: 0
RD monitored patient during admission and completed fur-ther assessment on HD 7 due to NPO status.
Clinical Presentation
Anthropometrics. Height: 66 inchesCurrent weight: 263 poundsAdmission weight: 268 poundsWeight 3 months ago: 290 pounds (per patient interview by
RD)
Diet history. NPO since admissionAnorexia and reduced oral intake over last 3 months—
patient reported eating about half of his normal meal intake during same time period.
Physical assessment. No evidence of subcutaneous fat or mus-cle loss
Bilateral lower extremities: pitting edema: 2+
Clinical data. White blood cells: 16 KTemperature: 99.9°FSerum albumin level: 1.8 g/dLPrealbumin: 7.8 mg/dL
Functional status. Physical therapy evaluation: generalized weakness on admission
What Is This Patient’s Nutrition Status?
Severe malnutrition related to acute illness/injuryHe meets several criteria and demonstrates significant
inflammation:
Weight loss•• 3 months: 9%
Energy intake•• No nutrient intake since hospital admission (7 days)
Physical assessment•• Moderate edema
Functional assessment•• Generalized weakness—not part of current criteria
This patient achieved 3 of the 6 defined criteria along with mild functional impairment. Upon discussion with the patient’s physician, the need to initiate nutrition intervention was recog-nized. Due to the patient’s ongoing prolonged ileus, it was determined parenteral nutrition (PN) support would be the most appropriate nutrition intervention.
It is important to note that the nutrition assessment process for both patients required approximately 45-60 minutes by the RD to complete. This included time for the electronic medical record (EMR) review, patient visit, performance of physical assessment, EMR documentation and for physician collaboration.
Implementation of a Malnutrition Program
Implementation of the consensus criteria4 is a process that is best accomplished through a collaborative approach within the healthcare institution. To be successful in achieving the full spectrum of evaluating, diagnosing, documenting, and receiv-ing reimbursement for malnourished patients requires collabo-ration between several healthcare professionals. While the dietitian, physician, and nurse function at the patient bedside, other “behind-the-scenes” healthcare personnel also contribute to the full implementation of these activities. This generally includes those from the health information management department (HIM) (clinical documentation, coding, reimburse-ment, medical records), finance department, information technology, and hospital administration. We describe the implementation of a malnutrition program incorporating the consensus criteria in collaboration with all healthcare person-nel as described above at the Cleveland Clinic, a large health-care system comprising a main campus hospital and 8 regional hospitals.
Establishing Support
The consensus statement is an evidence-based document that provides a purpose and rationale for hospital clinicians to develop a consistent approach to the identification and docu-mentation of malnutrition in healthcare institutions. The consen-sus statement was developed collaboratively by 2 of the country’s most credible professional nutrition societies, the Academy and A.S.P.E.N., and therefore was used to establish our malnutrition program.4 Support for the program was first gained from our physician nutrition director. Patient care treatment plans and decisions are directed by physicians (or authorized providers) so establishing a physician-champion was important. Additional support was also gained from an executive healthcare adminis-trator. Apprising him of the anticipated effect of increased hospi-tal reimbursement by identifying malnourished patients was positively received. To promote institutional success of our
at A.S.P.E.N on July 9, 2014ncp.sagepub.comDownloaded from

Malone and Hamilton 647
malnutrition program the physician-champion actively engaged in communicating and collaborating with other physicians and administrators.
Upon establishing institution support, a Malnutrition Task Force was formed comprising dietitians and dietetic technicians from the main campus and regional hospitals. The committee met on a regular basis to design and implement the various com-ponents of our program as described below. The completion of the initial program aspects took approximately 18 months.
Benchmarking Malnutrition Data
Baseline data were gathered on our health system’s current usage of the International Classification of Diseases (ICD) codes for malnutrition (Table 9) prior to implementing the pro-gram. The current version of ICD codes is the 9th version.27 The finance department provided this data for in-patient hospital stays for each hospital. The consensus statement recommends ICD-9 code 262 for the diagnosis of severe protein-calorie mal-nutrition and ICD-9 code 263.0 for moderate (nonsevere) mal-nutrition. These ICD-9 codes have definitions that best match the malnutrition criteria for severe and moderate (nonsevere) malnutrition as established in the consensus statement.4 The ICD-9 codes 262 and 263.0 are included in the CMS Medical Severity-Diagnosis-Related Group classification with 262 as a major comorbid condition/complication and 263.0 as a less severe comorbid condition/complication. The application of one of these malnutrition codes to the DRG may increase reim-bursement. In addition, the overall rate of patients diagnosed with malnutrition at each hospital was determined based on the number of hospital discharges. Research studies indicate the rate of malnutrition of hospitalized patients ranges from 15% to 60%,8 depending on the patient population and clinical criteria used. However, U.S. statistical reports indicate that only 3% of patients admitted to acute care settings are diagnosed with mal-nutrition.4 Our intention is to gather data annually on code usage for malnutrition with the expectation that severe and non-severe malnutrition will be identified with the ICD-9 codes
262 and 263.0, respectively. We also will investigate actual received reimbursement for malnutrition. A recent report indi-cated significant reimbursement was received by a small hospi-tal (100+/daily census) when malnutrition was identified by the dietitian and subsequently documented by the physician in the EMR.28
Health Information Management and Reimbursement Specialists
The HIM department and reimbursement specialists were con-tacted early during our program development. These profes-sionals are responsible for reviewing the patient medical record and assuring the correct ICD-9 code assignment. Patient health information must be fully documented, be accurate, and meet the definition of the ICD-9 code, otherwise reimbursement for services may not be obtained. We presented the consensus cri-teria4 and goals of our malnutrition program to the department. This was exceptionally well received, and they appreciated the evidence-based criteria and documentation that would appear in the EMR to substantiate the malnutrition diagnosis. They noted it as being particularly helpful when collaborating with physicians/providers during review of the patient medical record since most health information, including malnutrition documentation, can be gathered only from the authorized pro-vider’s documentation for reimbursement
Dietitian Training for Diagnosing Malnutrition
One of the most important aspects of the malnutrition program was to educate and train the dietitians from our health system hospitals (approximately 95 dietitians). The Cleveland Clinic promotes standardization of clinical policies across our health system; standardizing our malnutrition diagnosis and docu-mentation process provided an opportunity to continue our standardization efforts.
We designed a 2-part education program for dietitian train-ing. Dietitians and dietetic interns were first required to attend a half-day didactic program (2 dates were available) which included the following lectures:
• etiology based definition of malnutrition• clinical characteristics (consensus paper)• nutrition assessment• inflammation• physical exam• coding and documentation• case studies (interactive)
All references and lecture materials were made available to the dietitians and dietetic interns via a share-point website. The lectures were videotaped and also made available on the share-point website and subsequently are viewed by new hires.
Table 9. ICD-9 Codes for Nutrition Deficiencies (Applicable to Adult Malnutrition).27
Term Code
Kwashiorkor 260Marasmus 261Other, severe protein-calorie malnutrition 262a
Other and unspecified protein-calorie malnutrition 263Moderate malnutrition 263.0b
Mild malnutrition 263.1Other protein-calorie malnutrition 263.8Unspecified protein-calorie malnutrition 263.9
aRecommended for diagnosis of severe malnutrition.bRecommended for diagnosis of nonsevere (moderate) malnutrition.
at A.S.P.E.N on July 9, 2014ncp.sagepub.comDownloaded from

648 Nutrition in Clinical Practice 28(6)
The second part of our education program was to train the dietitians and dietetic interns on performing a nutrition-focused physical examination (NFPE). Several half-day training ses-sions were scheduled at the Cleveland Clinic main campus Simulation Center. The Simulation Center provided equip-ment, including mannequins, examination rooms, classrooms, and videotaping capabilities. It took approximately 8 months to train all dietitians and interns due to the limited training space. Dietitians and dietetic interns rotated each through 3 hands-on workshops for muscle and fat examination, edema examination and micronutrient examination. While micronu-trient deficiencies are not currently one of the consensus char-acteristics, our Malnutrition Task Force felt they provided supportive evidence for signs of malnutrition. The micronutri-ent workshop included examination of hair, skin, eyes, oral cavity, and nails for deficiencies.
Following the workshops we utilized the objective struc-tured clinical exam (OSCE) method to assess the skills of RDs utilizing the consensus criteria and performing a NFPE. The OSCE method has been successful in training a variety of skills to healthcare professionals. It was first developed for use with medical students to objectively assess clinical competencies such as history-taking, physical examination, communication skills, and data interpretation.29 Students participate by moving through a series of timed stations, with each station devoted to a particular area of a predetermined competency. Each station uses a standardized patient (trained to portray a medical condi-tion) and an observer. The observer provides feedback to the student at the end of each station. The OSCE has been used to assess multiple dietetic student clinical skills including com-munication skills and interviewing patients, interpretation and food knowledge skills, performing a nutrition assessment, planning a nutrition intervention, and calculating and planning an enteral feeding regimen.30-32 We developed malnutrition scenarios for use with the OSCE exercises and used our own nutrition department members (dietitians, dietetic technicians, managers, clerical support staff) as standardized patients and observers (dietitian only). Training of the standardized patients was provided by the Simulation Center manager. Dietitians rotated through the scenarios in 15-minute intervals including interviewing the patient, performing a NFPE and identifying the presence and degree of malnutrition. The observer pro-vided feedback to the dietitian on his/her performance. Dietitians were provided with laminated pocket cards of the Academy’s clinical characteristics table (Tables 4 and 5) for use during the OSCE and subsequently for clinical practice.33 Evaluations of the workshops and OSCE sessions were col-lected from the participating dietitians. In all, 98% rated the overall experience as good to excellent and 97% rated the OSCE as a good to excellent experience.
Documentation
The Malnutrition Task Force created a standard template for documentation of malnutrition in the EMR and is used by
the dietitians at all the hospitals. The template includes all 6 clinical characteristics of the consensus paper, including spe-cific physical parameters and a final malnutrition diagnosis section to indicate severe protein-calorie malnutrition, moder-ate (nonsevere) malnutrition or no malnutrition identified. A drop-down selection format is used for all characteristics and for ease of moving through the documentation template quickly. The development and implementation of the EMR template required collaboration with a clinical informatic tech-nology specialist.
Provider Education and Communication
We designed a malnutrition presentation (PowerPoint) to be used by the dietitians to educate providers (physicians, nurse practitioners, physicians assistants). Key components of the presentation included dietitian documentation of malnutrition in the EMR and the specific documentation steps required for the provider. In addition, the importance of collaboration between the dietitian and the provider when determining the presence and degree of malnutrition and the subsequent care plan was emphasized. Dietitians use the presentation for pro-vider staff meetings and in-services. This was a first-step com-munication process with providers, but we expect to explore potential future communication methods, especially for new hires.
Next Steps
As we move into our malnutrition program’s second year, we will review malnutrition coding practices and reimbursement data. We are continuing our training process including hands-on workshops for NFPE and the OSCE method at our Simulation Center for new dietitians and dietetic interns. To ensure quality of dietitian practices, we are developing a con-tinuous process improvement monitor for malnutrition docu-mentation and a competency for the NFPE.
Summary
The consensus-based malnutrition criteria offers a standard-ized approach to the assessment, diagnosis, and documentation of malnutrition in the adult hospitalized patient. Assessing nutrition risk followed by identifying the presence of inflam-mation will delineate the patient’s malnutrition etiology. Identifying a patient’s specific malnutrition characteristics requires in-depth data gathering and patient assessment. As usability and validity data is generated and reported, including identification of specific patient population criteria such as for the critically ill or obese, the malnutrition criteria will be reevaluated, updated, and revised accordingly.
Developing an institution based malnutrition program will most likely be directed by the Clinical Nutrition Department. Identifying, treating, and documenting malnutrition is a col-laborative effort between the bedside clinicians including the
at A.S.P.E.N on July 9, 2014ncp.sagepub.comDownloaded from

Malone and Hamilton 649
dietitian, physician (or provider) and nurse, and nonclinicians such as health information management, reimbursement spe-cialist, and finance and informatics technologists (Table 10). For allocation of appropriate reimbursement, all healthcare personnel must share the same vision to accurately identify patient malnutrition utilizing the same clinical criteria.
References
1. Butterworth CE. The skeleton in the hospital closet. Nutr Today. 1974;9(2):4-8.
2. Blackburn GL, Bistrian BR, Maini BS, et al. Nutritional and meta-bolic assessment of the hospitalized patient. JPEN J Parent Ent Nutr. 1977;1:11-22.
3. U.S. Department of Health and Human Services, Center for Medicare and Medicaid Services. MS-DRG summary table: summary of the changes to the MS-DRG’s for FY 2008. Available at: www.cms.gov/Medicare/AcuteInpatientPPS.
4. White JV, Guenter P, Jensen GL, et al. Consensus statement: Academy of Nutrition and Dietetics and the American Society for Parenteral and Enteral Nutrition: Characteristics Recommended for the Identification and Documentation of Adult Malnutrition (Undernutrition). JPEN J Parent Ent Nutr. 2012;36:275-283.
5. Jensen GL, Mirtallo JA, Compher C, et al. Adult starvation and disease-related malnutrition: A proposal for etiology-based diagnosis in
the clinical practice setting from the International Consensus Guideline Committee. JPEN J Parent Ent Nutr. 2010:34;156-159.
6. Joint Commission on Accreditation of Healthcare Organizations. Comprehensive Accreditation Manual for Hospitals. Chicago, IL: Joint Commission on Accreditation of Healthcare Organizations; 2007.
7. A.S.P.E.N. Nutrition Screening and Assessment Survey 2012. 8. Mueller C, Compher C, Druyan ME. A.S.P.E.N. clinical guidelines nutri-
tion screening, assessment, and intervention in adults. JPEN J Parent Ent Nutr. 2011;35:16-24.
9. Skipper AL, et al. Nutrition screening tools: an analysis of the evidence. JPEN J Parent Ent Nutr. 2012;36:292-298.
10. McWhirter JP, Pennington CR. Incidence and recognition of malnutrition in hospital. BMJ. 1994;308:945.
11. Jensen GL, Bistrian B, Roubenoff R, Heimburger DC. Malnutrition syn-dromes: a conundrum vs continuum. JPEN J Parent Ent Nutr. 2009; 33:710-716.
12. Medzhitov R. Origin and physiological roles of inflammation. Nature. 2008;454:428-435.
13. Kolb-Bachofen V. A review on the biological properties of C-reactive pro-tein. Immunobiology. 1991;183:133-145.
14. Gian P, Castelli, Claudio Pognani, et al. Procalcitonin and C-reactive pro-tein during systemic inflammatory response syndrome, sepsis and organ dysfunction. Critical Care. 2004,8:R234-R242.
15. Visser M, Lex M, Bouter G, et al. Elevated C-reactive protein levels in overweight and obese adults. JAMA. 1999;282(22):2131-2135.
16. Solem CA, Loftus EV, Tremaine WJ, et al. Correlation of C-reactive protein with clinical, endoscopic, histologic, and radiographic activity in inflammatory bowel disease. Inflammatory Bowel Dis. 2005;11:707-712.
17. Pepys MB, Hirschfield GM. C-reactive protein: a critical update. J Clin Invest. 2003;111(12):1805-1812.
18. Rosenbaum K, Wang J, Pierson RN Jr, Kotler DP. Time-dependent varia-tion in weight and body composition in healthy adults. JPEN J Parent Ent Nutr. 2000;24:52-55.
19. Keys A, Brozek J, Henschel A, Mickelsen O, Taylor HL. The Biology of Human Starvation. Minneapolis: University of Minnesota Press; 1950.
20. Jensen GL, Hsaio PY, Wheeler D. Nutrition screening and assessment. In: A.S.P.E.N. Adult Nutrition Support Core Curriculum. 2nd ed. Silver Spring, MD: A.S.P.E.N.; 2012.
21. Kondrup J, Johansen N, Plum LM, et al. Incidence of nutritional risk and causes of inadequate nutritional care in hospitals. Clin Nutr. 2002;21(6):461-468.
22. Frankenfield DC, Coleman A, Alam S, Cooney R. Analysis of estima-tion methods for resting metabolic rate in critically ill adults. J Parenter Enteral Nutr. 2009;33:27.
23. Mifflin MD, St Jeor ST, Hill LA, Scott BJ, Daugherty SA, Koh YO. A new predictive equation for resting energy expenditure in healthy indi-viduals. Am J Clin Nutr.1990;51(2):241-247.
24. The Academy Quality Management Committee and Scope of Practice Subcommittee of the Quality Management Committee. Academy of Nutrition and Dietetics: Revised 2012 standards of practice in nutrition care and standards of professional performance for registered dietitians. J Acad Nutr Diet. 2013;113:S29-S45.
25. Mackle TJ, Touger-Decker R, O’Sullivan-Maillet J, Holland BK. Registered dietitians’ use of physical assessment parameters in profes-sional practice. J Am Diet Assoc. 2003;103:1632-1638.
26. Norman K, Stobäus N, Gonzalez MC, et al. Hand grip strength: outcome predictor and marker of nutritional status. Clin Nutr. 2011;30:135.
27. Buck CJ. International Classification of Disease, 9th Revision; Clinical Modification (ICD-9-CM), for Physicians. Vols 1-2. Burlington, MA: Elsevier; 2011.
28. Cobb B, Hardin E, Click A, Watson L. Customizing malnutrition docu-mentation accelerates hospital revenue and RD value. J Am Diet Assoc. 2011;111(9 suppl):A77.
Table 10. Areas to Include When Developing a Malnutrition-Identification Program.
•• Establish a physician-champion-Collaborates with other physicians-Addresses hospital medical executive council
•• Solicit hospital administration support-Allocation of resources
•• Benchmark institutional data-Collaborate with finance department-Assess current use of ICD-9 codes for malnutrition-Determine rate of overall malnutrition
•• Collaborate with health information management department (reimbursement, medical records, coding)-Review consensus criteria- Determine documentation methods of malnutrition as it applies to ICD-9 codes
•• Train dietitian staff-6 consensus criteria and etiology- Physical assessment skills for muscle, fat, fluid accumulation, and functional status
•• Develop documentation template-Include etiology and consensus criteria- Collaborate with informatic technology (clinical support) department for implementation into electronic medical record
•• Ensure nursing screening process- Utilize nutrition screening tool for assessment of risk and to consult the dietitian
•• Develop sustainable provider education- Utilize methods such as presentations at department staff meetings, electronic communication, online education modules, bedside rounds
at A.S.P.E.N on July 9, 2014ncp.sagepub.comDownloaded from

650 Nutrition in Clinical Practice 28(6)
29. Harden RM, Gleeson FA. Assessment of clinical competence using an objec-tive structured clinical examination (OSCE). Med Educ. 1979;13:41-54.
30. Pender FT, de Looy AE. The testing of clinical skills in dietetic students prior to entering clinical placement. J Hum Nutr Dietet. 2004;17:17-24.
31. Hawker JA, Walker KZ, Barrington V, Andrianopoulos N. Measuring the success of an objective structured clinical examination for dietetic stu-dents. J Hun Nutr Dietet. 2010;23:212-216.
32. Lambert L, Pattison DJ, de Looy AE. Dietetic students’ performance of activities in an objective structured clinical examination. J Hum Nutr Dietet. 2010;23:224-229.
33. Academy/A.S.P.E.N. Clinical Characteristics that the RD can obtain and document to support a diagnosis of malnutrition. Available at: http://nutritioncaremanual.org/category.cfm?ncm_category_id=11. Accessed June 20, 2013.
at A.S.P.E.N on July 9, 2014ncp.sagepub.comDownloaded from