Embed Size (px)
Citation preview

*AdvAPD¼Advanced Accredited Prac-tising Dietitian (Australia).‡Certified inCanada.§Certified in Sweden.¶Certifiedin Israel.
2212-2672/Copyright ª 2017 by theAcademy of Nutrition and Dietetics.http://dx.doi.org/10.1016/j.jand.2017.07.015
ª 2017 by the Academy of Nutrition and Dietetics.
FROM THE ACADEMY
Nutrition Care Process and Model Update:Toward Realizing People-Centered Care andOutcomes Management
William I. Swan, FAND; Angela Vivanti, DHSc, AdvAPD*; Nancy A Hakel-Smith, PhD, RD; Brenda Hotson, MSc, RD‡;Ylva Orrevall, PhD, RD§; Naomi Trostler, PhD, RD¶, FADN; Kay Beck Howarter, MS, RDN; Constantina Papoutsakis, PhD, RDTHE NUTRITION CARE PROCESS(NCP) is a systematic methodthat nutrition and dieteticspractitioners use to provide
nutrition care.1 In this article, nutritionand dietetics practitioners or profes-sionals; dietitians; dietitians-nutritionists; and dietetic technicians,registered, are collectively referred toas professionals. The Nutrition CareProcess Model (NCPM) describes theNCP by presenting the workflow ofprofessionals in diverse individual andpopulation care delivery settings.Implementation of the NCPM hasbeen associated with several advan-tages, including use of a commonframework for nutrition care andresearch, promotion of criticalthinking, more-focused nutrition caredocumentation, increased acknowl-edgement of the value of nutritioncare by other health care professionals,and improved application of evidence-based guidelines.2-5 Potential targetaudiences for the NCPM include practi-tioners, educators and students, profes-sional credentialing agencies, healthsystem accrediting agencies, healthcare funding organizations, payers,and clients.The Academy of Nutrition and Di-
etetics (Academy) adopted the NCP andNCPM for use in the United States in2003.1 Since then, international di-etetics associations have supportedadoption of the NCPM.6 The develop-ment history of the NCPM is describedin detail by Hammond and colleagues.7
The NCPM is updated approximatelyevery 5 years, which aligns with otherAcademy resources such as Evidence-Based Nutrition Practice Guidelines.8
This ensures that the NCPM reflectscurrent practice.This article presents an expert
consensus update review of the NCPMcompleted during the year 2013-2014by the Nutrition Care Process and Ter-minology (NCPT) Committee (whichbecame the Nutrition Care ProcessResearch Outcomes Committee in2015) and its international workgroup.Twenty-four experts from around theworld participated in a consensus-building process for each componentof the NCPM. They considered com-ments submitted to the NCP website,feedback from translators and users, aswell as international information onhealth quality goals. The current NCPMupdate highlights three themes thatemerged as a result of the consensusprocess: use of concise language in theNCPM, promotion of professionals’ re-sponsibility for outcomes manage-ment, and support for people-centeredcare (PCC).9 Finally, experts recom-mend associated actions to advance theNCPM as the Academy embarks into itssecond century initiatives toward aworld where all people thrive throughthe transformative power of food andnutrition. International input was animportant influence for improvementof the current revision. The informationin this article replaces previous infor-mation describing the NCPM.
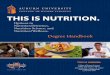
BACKGROUNDThe NCP is a roadmap and consists offour separate yet interconnected steps:Nutrition Assessment and Reassess-ment, Nutrition Diagnosis, NutritionIntervention, and Nutrition Monitoring
JOURNAL OF THE ACA
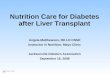
and Evaluation (Figure 1). The foursteps are divided into two compo-nents: problem identification andproblem solving. This distinction isimportant for application purposes.Problem identification includes Nutri-tion Assessment and Reassessment(Step 1), and Nutrition Diagnosis (Step2). Problem solving includes NutritionIntervention (Step 3), and NutritionMonitoring and Evaluation (Step 4). Ithas been helpful for new adopters toimplement the NCP in two consecutivephases where Phase 1 involves imple-mentation of problem identification,and Phase 2 involves the addition ofproblem solving. Each step is impor-tant to complete before advancing tothe next step. In practice, as new in-formation becomes available, pro-fessionals revisit previous steps of theNCP to reassess, update nutrition di-agnoses, adapt interventions, and/ormodify goals and monitor outcomes.The NCPM (Figure 2) is depicted uni-directionally where one progressesfrom Nutrition Assessment and Reas-sessment to Nutrition Diagnosis, and soon; yet, in practice, the model is dy-namic and multidirectional to supportcritical thinking and timely care. This isimportant in follow-up care of clients.As new information is collected, aprofessional may revisit previous stepsof the process to remove, add, orchange nutrition diagnoses, adjust in-terventions, or modify goals andmonitoring data. Monitoring and eval-uation data from the prior clientinteraction (or visit) is data that beginsthe reassessment of the subsequentinteraction. Hence, the model carriesover care from one interaction to thenext.
The NCPM incorporates scientificevidence and aims to move pro-fessionals from experience-based to
DEMY OF NUTRITION AND DIETETICS 1

Step 1: Nutrition Assessment and Reassessment
Definition and purpose Nutrition Assessment is a systematic approach to collect, classify, and synthesize important andrelevant data from clients (where “client” refers to individual and population). This step alsoincludes Reassessment, which additionally includes collection of new data, and comparing and re-evaluating data from the previous interaction to the next. Nutrition Assessment is an ongoing,dynamic process that involves initial data collection as well as continual reassessment and analysisof the client’s status compared with accepted standards, recommendations, and/or goals
Data sources/tools forassessment
� Screening or referral form� Client interview� Medical or health records� Consultation with other caregivers, including family members� Community-based surveys and focus groups� Statistical reports, administrative data, and epidemiologic studies
Types of data collected � Food- and nutrition-related history� Anthropometric measurements� Biochemical data, medical tests, and procedures� Nutrition-focused physical examination findings� Client history
Nutrition assessmentcomponents
� Review data collected for factors that affect nutrition and health status� Cluster individual data to identify at least 1 nutrition diagnosis as described in diagnosis
reference sheets� Identify accepted standards, recommendations, and/or goals by which data will be compared
Reassessmentcomponents
� Collect new data� Compare data with previous interaction/s:� Compare the monitoring and evaluation outcomes/indicators documented in the previous
interaction to new data� Evaluate if the client’s nutritional status has changed to demonstrate effectiveness of
intervention� Evaluate the status of the Nutrition Diagnosis� Evaluate whether the nutrition assessment data from the previous interaction need to be
reassessed or changed depending on the client’s status or situation� Identify new nutrition assessment data to monitor and evaluate during the next interaction
Critical thinking � Determining important and relevant data to collect� Determining the need for additional information� Selecting assessment tools and procedures that match the situation� Applying assessment tools in valid and reliable ways� Validating the data
Determination forcontinuation of care
If upon completion of an initial Nutrition Assessment or Reassessment, it is determined that theproblem cannot be modified by further nutrition care, discharge, or discontinuation from thisepisode of nutrition care may be appropriate
Step 2. Nutrition Diagnosis
Definition and purpose Nutrition Diagnosis is a nutrition and dietetics professional’s identification and labeling of an existingnutrition problem that the nutrition and dietetics professional is responsible for treating
Data sources/tools fordiagnosis
Organized assessment data that is clustered for comparison with defining characteristics ofsuspected diagnoses as listed in diagnosis reference sheets
(continued on next page)
Figure 1. The 4 Steps of the Nutrition Care Process Model with distinguishing characteristics.
FROM THE ACADEMY
2 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS -- 2017 Volume - Number -

Nutrition Diagnosiscomponents
The Nutrition Diagnosis is expressed using nutrition diagnostic terms and the etiologies, signs, andsymptoms that have been identified in the reference sheets describing each diagnosis. There arethree distinct parts to a nutrition diagnostic statement:1. The Nutrition Diagnosis describes alterations in a client’s status2. Etiology is a factor gathered during the Nutrition Assessment that contributes to the exis-
tence or the maintenance of pathophysiological, psychosocial, situational, developmental,cultural, and/or environmental problems� The etiology is preceded by the words “related to”� Identifying the etiology will lead to the selection of a nutrition intervention aimed at
resolving the underlying cause of the nutrition problem whenever possible3. Signs/symptoms (defining characteristics)The defining characteristics are a cluster of signs and symptoms that provide evidence that a
Nutrition Diagnosis exists� The signs and symptoms are preceded by the words “as evidenced by”� Signs are the observations of a trained professional� Symptoms are changes reported by the client
Nutrition diagnosticstatement
A well-written nutrition diagnostic statement should be:� Clear and concise;� Specific to a client;� Limited to a single client problem;� Accurately related to 1 etiology; and� Based on signs and symptoms from the assessment data
Critical thinking � Finding patterns and relationships among the data and possible causes� Making inferences� Stating the problem clearly and singularly� Ruling in/ruling out specific diagnoses� Identifying an etiology that may be resolved, lessened, or managed by the Intervention/s� Identifying signs and symptoms that are measurable or their change may be tracked� Prioritizing identified problems
Determination forcontinuation of care
Because the Nutrition Diagnosis names and describes the problem, the determination for problemsolving follows the Nutrition Diagnosis step. If a professional does not identify a NutritionDiagnosis or the potential exists for a Nutrition Diagnosis to develop, a professional maydetermine an appropriate method and interval for continuation of care
Step 3. Nutrition Intervention
Definition and purpose A Nutrition Intervention is a purposefully planned action(s) designed with the intent of changing anutrition-related behavior, risk factor, environmental condition, or aspect of health status.Nutrition Intervention consists of two interrelated components: planning and intervention. TheNutrition Intervention is typically directed toward resolving the nutrition diagnosis or the nutritionetiology Less often, it is directed at relieving signs and symptoms
Data sources/tools forInterventions
� The Academy of Nutrition and Dietetics’ Evidence-Based Nutrition Practice guidelines or otherevidence-based guidelines from professional organizations
� The Academy of Nutrition and Dietetics’ Evidence Analysis Library and other evidence such asthe Cochrane Library
� Current research literature� Results of outcome management studies or quality improvement projects
(continued on next page)
Figure 1. (continued) The 4 Steps of the Nutrition Care Process Model with distinguishing characteristics.
FROM THE ACADEMY
-- 2017 Volume - Number - JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 3

Nutrition Interventioncomponents
1. Planning� Prioritize interventions based on urgency, influence, and available resources� Write a nutrition prescription based on a client’s individualized recommended dietary
intake of energy and/or selected foods or nutrients based on current reference standardsand dietary guidelines and a client’s health condition and nutrition diagnosis
� Collaborate with the client to identify goals of the intervention for each diagnosis� Select specific intervention strategies that are focused on the etiology of the problem
and that are known to be effective based on best current knowledge and evidence� Define time and frequency or care, including intensity, duration, and follow-up
2. Implementation� Collaborate with the client to carry out the plan of care� Communicate the plan of nutrition care� Modify the plan of care as needed� Follow-up and verify that the plan is being implemented� Revise strategies based on changes in condition or response to intervention
Critical thinking � Setting goals and prioritizing� Defining the nutrition prescription or basic plan� Making interdisciplinary connections� Matching intervention strategies with client needs, nutrition diagnoses, and values� Choosing from among alternatives to determine a course of action� Specifying the time and frequency of care
Determination forcontinuation of care
If a client has met intervention goals or is not at this time able/ready to make needed changes, theprofessional may discharge the client from this episode of care as part of the planned intervention
Step 4. Nutrition Monitoring and Evaluation
Definition and purpose During the first interaction, appropriate outcomes/indicators are selected to be monitored andevaluated at the next interaction. During subsequent interactions, these outcomes/indicators areused to demonstrate the amount of progress made and whether goals or expected outcomes arebeing met. Nutrition monitoring and evaluation identifies outcomes/indicators relevant to thenutrition diagnosis and intervention plans and goals
Data sources/tools forNutrition Monitoringand Evaluation
Self-monitoring data or data from other records including forms, spreadsheets, and computerprogramsAnthropometric measurements, biochemical data, medical tests, and proceduresClient surveys, pretests, posttests, and/or questionnairesMail, telephone, and electronic media follow-up, such as e-mail
Types of outcomesmeasured
� Nutrition-related history� Anthropometric measurements� Biochemical data, medical tests, and procedures� Nutrition-focused physical findings� Knowledge gained� Behavior change
Nutrition Monitoringand Evaluationcomponents
� In the first interaction: Select appropriate outcomes/indicators� In subsequent interactions
This step includes three distinct and interrelated processes1. Monitor progress
� Check client understanding and adherence with plan;� Determine whether the intervention is being implemented as prescribed;
(continued on next page)
Figure 1. (continued) The 4 Steps of the Nutrition Care Process Model with distinguishing characteristics.
FROM THE ACADEMY
4 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS -- 2017 Volume - Number -

� Provide evidence that the plan/intervention strategy is or is not changing client behavioror status;
� Identify other positive or negative outcomes;� Gather information indicating reasons for lack of progress; and� Support conclusions with evidence
2. Measure outcomes/indicators� Gather data for outcomes/indicators that are relevant to the nutrition diagnosis or signs
or symptoms, nutrition goals, medical diagnosis, outcomes, and quality managementgoals
3. Evaluate outcomes/indicators� Compare current findings with previous status, intervention goals, and reference
standards
Critical thinking Selecting appropriate outcomes/indicators� Using appropriate reference standard for comparison� Defining where client is in terms of expected outcomes� Explaining variance from expected outcomes� Determining factors that help or hinder progress� Deciding between discharge or continued care
Determination forcontinuation of care
Based on the findings, the professional may actively continue care; or if nutrition care is complete orno further change is expected, discharge the client. If nutrition care continues, reassessment mayresult in refinements to the diagnosis and intervention. If care does not continue, a client may stillbe monitored for a change in status and re-enter nutrition care at a later date
Figure 1. (continued) The 4 Steps of the Nutrition Care Process Model with distinguishing characteristics.
FROM THE ACADEMY
evidence-based practice. The NCPMstrives to provide quality, consistentpractice and to achieve expected out-comes at all levels of career develop-ment. If the NCPM is appliedconsistently, quality of care andimproved health outcomes shouldenhance recognition for professionalson multidisciplinary teams. Currentresearch demonstrates that it ispossible to measure application of theNCPM and demonstrate efficacy of theNCPM in practice.5
NCPM
CoreThe focus of the NCPM is a central Corethat embraces the many and variedareas in which nutrition and dieteticcare is practiced. Consequently, pro-fessional interactions that influenceindividuals and populations are recog-nized and incorporated into the model.Populations refers to demographicallydefined groups or otherwise identifi-able groups. Individuals and pop-ulations are referred to as clientsthroughout this article and client alsoincludes supportive individuals (eg,
-- 2017 Volume - Number -
family and caregivers) and structures(eg, social service agencies and faith-based organizations). In the Core, theword interacts describes the dynamicrelationship between a professionaland a client in which PCC and clientengagement contribute to treatmentdecisions, intervention strategies,10 orenvironment changes. Interacts is abroader and more inclusive word thanrelationship, which was used in theprevious NCPM.11 Interacting encom-passes the care of populations andgroups as well as individuals. Forexample, a population survey is aninteraction not a relationship. Aninterview is an interaction between aclient and a professional throughwhich a relationship can develop. Also,an in-person or remote visit with cli-ent(s) is an interaction.
Nutrition Assessment andReassessment: Step 1Nutrition Assessment and Reassess-ment is a systematic approach for col-lecting, classifying, and synthesizingdata to describe nutritional status,related nutrition problems, and their
JOURNAL OF THE ACA
causes. Nutrition Assessment is initi-ated from nutrition screening or clientreferral. Nutrition Assessment is acontinuous process requiring initialdata collection with continued reas-sessment and analysis of a client’s datacompared with accepted standards,recommendations, and/or goals likegrowth charts, dietary guidelines, and/or individual needs. Although pro-fessionals are familiar with performinga Nutrition Assessment, the systematicapproach of Nutrition Assessment andReassessment coupled with standard-ized terminology facilitates organizeddocumentation, encourages criticalthinking, and supports communication,collaboration, and quality care for cli-ents with nutrition-related problems.4
In this update, Nutrition Assessmentand Reassessment is clarified further todescribe specifically what a profes-sional is expected to do (Figure 3). Acritically thoughtful professional ac-quires, analyzes, and interprets theimportant and relevant data contrib-uting to the potential nutrition-relatedproblem or problems. Critical thinkingtasks may vary with level of practice(Figure 4).12
DEMY OF NUTRITION AND DIETETICS 5

Figure 2. The Nutrition Care Process (NCP) Model.
FROM THE ACADEMY
The data collected and analyzedduring this step direct professionals inthe selection of a Nutrition Diagnosis.New information that is collected dur-ing follow-up interactions (ie, in-teractions that occur after the initialone), and comparison of data betweeninteractions provide the basis forReassessment, and the possibility forchanged or resolved Nutrition Di-agnoses. As the nutrition interventionunfolds during follow-up interactions,the relevant Monitoring and Evaluation
6 JOURNAL OF THE ACADEMY OF NUTRITIO
data of the previous interaction(s)inform Reassessment and the possibil-ity for changed nutrition diagnoses.Thus, in a follow-up interaction, theReassessment begins where Moni-toring and Evaluation ended during theprevious interaction. It should behighlighted that Reassessment is notonly comparing results from oneinteraction to the next to establishchange/progress between interactions.Reassessment is also an opportunity tocollect new important and relevant
N AND DIETETICS
information to develop or modify aNutrition Diagnosis that best fits thepresent situation of a client.
Nutrition Diagnosis: Step 2From Nutrition Assessment data, aprofessional is able to determinewhether there is a nutrition problemand label it as a Nutrition Diagnosis.Nutrition Diagnosis identifies and de-scribes a specific problem or problemsthat can be resolved or improved
-- 2017 Volume - Number -

Function The NCP Model The NCP Model
Review year 2008 2015
Standardized language � International Dietetics and NutritionTerminology
� Print format (book)� Second edition (purple cover)� Third edition (green cover)� Fourth edition (yellow cover)
� Electronic� NCP Terminology� Electronic format (web-based)
Nutrition Assessment andReassessment step(inner ring)
� Obtain/collect timely and appropriate data� Analyze/interpret with evidence-based
standards� Document
� Obtain/collect important andrelevant data
� Analyze/interpret collected data
Nutrition Diagnosis step(inner ring)
� Identify and label problem� Determine cause/contributing risk factors� Cluster signs and symptoms/defining
characteristics� Document
� Identify problem� Determine etiology/cause� State signs and symptoms
Nutrition Interventionstep (inner ring)
� Plan nutrition intervention (set goals anddetermine a plan of action)
� Implement nutrition intervention (care isdelivered and actions are carried out)
� Document
� Determine intervention andprescription
� Formulate goals and determineaction
� Implement action
Nutrition Monitoringand Evaluation step(inner ring)
� Monitor progress� Measure outcome indicators� Evaluate outcomes� Document
� Select or identify quality indicators� Monitor and evaluate resolution of
diagnosis
Outcomes managementsystem
� Monitor the success of the NCPimplementation
� Evaluate influence with aggregate data� Identify and evaluate causes of less-than-
optimal performance and outcomes� Refine use of NCP
� Research NCP� Use aggregated data to conduct
research� Conduct continuous quality
improvement� Calculate and report quality
indicators
Center circle (core) � Relationship between patient/client/groupand nutrition and dietetics practitioner
� Individual/population interacts withnutrition and dietetics practitioner
Middle ring � Dietetics knowledge� Skills and competencies� Critical thinking� Collaboration� Communication� Evidence-based practice� Code of ethics
� Dietetics knowledge� Skills and competencies� Critical thinking� Collaboration� Communication� Evidence-based practice� Code of ethics� Documentation
Outer ring � Practice settings� Health care systems� Social systems� Economics
� Practice settings� Health care systems� Social systems� Economics
(continued on next page)
Figure 3. Comparison of functions in the Nutrition Care Process (NCP) Model.
FROM THE ACADEMY
-- 2017 Volume - Number - JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 7

Function The NCP Model The NCP Model
Screening and referralsystem
� Identify risk factors� Use appropriate tools and methods� Improve interdisciplinary collaboration
� Identify risk factors� Use appropriate tools and methods� Improve interdisciplinary
collaboration
Figure 3. (continued) Comparison of functions in the Nutrition Care Process (NCP) Model.
FROM THE ACADEMY
through Nutrition Intervention. ANutrition Diagnosis (eg, inconsistentcarbohydrate intake)13 is different froma medical diagnosis (eg, diabetes mel-litus). As the client responds to Nutri-tion Intervention, the NutritionDiagnosis can improve or resolve.Critical thinking is needed to prioritizenutrition diagnoses for NutritionIntervention. As shown in Figure 4, avariety of critical thinking tasks areimportant to develop the NutritionDiagnosis. For example, stating theproblem clearly and singularly is ex-pected to be carried out efficiently by anovice professional. Other skills, suchas finding patterns, may be conqueredwith greater experience. It is possibleand desirable that professionals of allcareer stages are able to carry outnecessary critical thinking tasks.14
N Novicea
Rule and tool dependentLacks context and discretionary judgement
B Beginnera
Starts to appreciate contextControlled learningTreats aspects of work equally
C Competenta
Encounters novel careBegins to ID important vs unimportant dataSelects rules and tools appropriate to task
P Proficienta
Organized thought patternsInnovation, PrioritizationSituational discriminationProblem solving based on experience
A Advanced Practice/Experta
Monitors performanceDoes not rely on rules and principlesIntuitive; Sees whole situation
Figure 4. Acquisition of Nutrition Care ProcCritical thinking skills in nutrition assessmenpapers/practice-papers/practice-paper-criticaFebruary 16, 2017.12. bFor each NCP step, thone should feel confident performing the ta
8 JOURNAL OF THE ACADEMY OF NUTRITIO
The Nutrition Diagnosis is commu-nicated as an identify problem, deter-mine etiology/cause, and state signsand symptoms (PES) statement. ThisPES statement is written with linkingwords (ie, problem “related to” etiology“as evidenced by” signs and symp-toms). The NCPT, which is discussedmore later in this article, provides astandardized nutrition diagnostic ter-minology that defines nutrition prob-lems.13 It is important to review thespecific Nutrition Diagnosis definitionto confirm that this is the mostappropriate Nutrition Diagnosis for thesituation. It is as important to reviewthe reference sheet of the NutritionDiagnosis from the NCPT to verify thatat least one indicator described in therespective reference sheet is present inthe client’s assessment data. Next, a
Assessment&Determining imDetermining thSelecting assesituation – Ca
Diagnosisb
Finding patternpossible causeStating the proIdentifying an Emanaged by thIdentifying signchange may bePrioritizing iden
Interventionb
Setting goals aDefining the nuMaking interdisMatching intervdiagnoses, andChoosing fromaction - Ca
Monitoring & Selecting apprUsing appropriExplaining variDeciding betwe
Nutrition
Care
Process
ess (NCP) critical thinking. aAdapted with pt and diagnosis. http://www.eatrightpro.orgl-thinking-skills-in-nutrition-assessment. Pue stated critical thinking task is labeled withsk. ID¼identification.
N AND DIETETICS
professional determines the etiology orroot cause of the nutrition problem.The selection of interventions thataddress the etiology are more likely toprovide desired nutrition care out-comes. To finalize the PES statement, aprofessional selects signs and symp-toms that can demonstrate resolutionor improvement in the nutritionaldiagnosis as a result of NutritionInterventions.
Nutrition Intervention: Step 3When possible, Nutrition Interventionis collaborative between a professionaland a client. The professional plans theNutrition Intervention after prioritizingNutrition Diagnoses by criticallyconsidering the severity of the nutri-tion problem and the client’s values
Re-assessmentb
portant and relevant data to collect – Ca
e need for additional information – Ca
ssment tools and procedures that match the
s and relationships among the data and s - Pa
blem clearly and singularly - Na
tiology that may be resolved, lessened or e Intervention/s - Ca
s and symptoms that are measurable or their tracked - Ba
tified problems - Pa
nd prioritizing - Pa
trition prescription or basic plan - Na
ciplinary connections - Pa
ention strategies with client needs, nutrition values - Ca
among alternatives to determine a course of
Evaluationb
opriate outcomes/indicators - Aa
ate reference standard for comparison - Na
ance from expected outcomes – Aa
en discharge or continued care - Ca
ermission from: Charney P, Peterson SJ./resource/practice/position-and-practice-blished November 2013. Accessedthe career development stage by which
-- 2017 Volume - Number -

FROM THE ACADEMY
and safety (Figure 4). Nutrition inter-vention has two related planning pha-ses. In the first phase, the professionaland client jointly determine achievableand measurable goals. These goals areimportant to define the time frameduring which the nutrition problem isto be resolved, provide direction to theplan, select and implement in-terventions intended to achieve thegoals, provide criteria to measure re-sults of intervention during NutritionMonitoring and Evaluation, and eval-uate effectiveness of intervention andrevise when indicated. The next phaseis to determine the nutrition prescrip-tion and interventions that will meetthe agreed upon goals. The specifiedactivity to determine a nutrition pre-scription, a client’s recommended di-etary intake based on current referencestandards and dietary guidelines,13 isnew to the current revision of NCPM(Figure 3).Interventions are a planned set of
specific behaviors or actions per-formed, delegated, coordinated, orrecommended by a professional thatmove a client toward a desiredoutcome. The chosen interventionsintend to alter or eliminate the etiologyto resolve the Nutrition Diagnosis.With goals agreed upon, prescriptionand interventions selected, action isundertaken to implement NutritionIntervention before proceeding toMonitoring and Evaluation.
Nutrition Monitoring andEvaluation: Step 4During Nutrition Monitoring and Eval-uation, a professional examines thetimely results following implementa-tion of Nutrition Interventions. For thisupdate, wording was clarified toincorporate key Nutrition Monitoringand Evaluation practice actions(Figures 2 and 3). These actions includeselecting quality indicators derivedfrom best practices and evidence-basedguidelines. Indicators use readilyavailable data to provide a quantitativemeasure for health professionals, or-ganizations, and planners aiming toachieve improvement in the care andthe processes by which client care isdelivered.15
A professional monitors and evalu-ates the progress or resolution of theNutrition Diagnosis and determineswhether Reassessment is necessary.
-- 2017 Volume - Number -
Standardized terms to assess the extentof Nutrition Diagnosis resolution havenot been developed. But, as anexample, the Academy of Nutrition andDietetics Health Informatics Infra-structure (ANDHII) currently uses thefollowing descriptors for resolution:resolved, continued, and removed (formore information on ANDHII, see thededicated section in this article). ANutrition Diagnosis can be monitoredand evaluated at the end of a singlevisit. For example, learning assessmentmay be evaluated at the conclusion of anutrition education session.
Framing RingsTwo framing rings (outer and middle)contextualize the four steps of the NCP(inner ring), and the Core (Figure 2).The outer ring represents the socialcontext of nutrition care. There are nochanges in the terms used to define theouter ring. However, the scope of theseterms is broader. As defined in 2008,the outer ring represented the in-fluences on how people receivednutrition information.11 In the updatedNCPM, this ring also represents howprofessionals engage their clients. Ex-amples of client engagement in theouter ring include advocating publicpolicy within social systems or using aclient portal within a health care sys-tem’s electronic health record forchronic care management.The middle ring represents the
required qualities and attributes thatdifferentiate the nutrition and dieteticsprofessionals from other professions.11
This is to emphasize that the nutritionand dietetics professionals contributethe critical thinking, code of ethics, andevidence-based practice that areunique to nutrition and dietetics sci-ence and practice. A significant changewithin the middle ring was placing theword documentation in this ring afterremoving the word document fromeach step of the NCP. The expectationto document the NCP remains.Although one may argue that commu-nication, also included in this ring, im-plies the act of documentation, in somecountries communication might belimited to verbal means and docu-mentation may not be required ormight not be an allowed privilege fornutrition and dietetics professionals.The explicit inclusion of the concept ofdocumentation in a framing ring was
JOURNAL OF THE ACA
deemed appropriate and necessary tounderline that documentation is arequirement for professionals adoptingthe NCPT internationally. This wasimportant given the range of practicesor requirements internationally thatvary from documentation in the healthrecord which is a legal requirement insome countries to no written docu-mentation by dietitians because ofdifferent levels of privileges. Docu-mentation is a desirable source of datafor monitoring and evaluating care andsupporting the Outcomes ManagementSystem.
The role and placement of nutritioninformatics in the framing rings wasconsidered. The consensus was thatinformatics provides useful tools for allparts of the NCPM and its supportingstructures and did not need designa-tionwithin the NCPM. Informatics toolsmay not be available to all pro-fessionals and professionals dependupon the outer ring for theiravailability.
SUPPORTING STRUCTURES
Screening and Referral SystemThe Screening and Referral System isexternal to the rings of the NCPbecause it may be carried out by col-laborators outside the nutrition anddietetics profession. This supportingsystem is often developed andmanaged by professionals. The purposeof this system is to identify and referthose individuals and populations whoalready have or are at risk for nutrition-related problems, who are appropriatefor nutrition care services, and whowould benefit from participation in theNCP. The nutrition screening processapplies appropriate, valid, and reliablescreening tools and resources to iden-tify and recognize nutritional riskfactors.
Outcomes Management SystemThe Outcomes Management System isa supporting structure outside the NCPbecause it can be operated by membersof various professions. As with Nutri-tion Screening and Referral, the Out-comes Management System intends tobe collaborative with leadership fromprofessionals. In 2008, the OutcomesManagement System emphasizedimproving and strengthening theNCPM within the profession through
DEMY OF NUTRITION AND DIETETICS 9

FROM THE ACADEMY
the following four actions: monitor thesuccess of the NCP implementation,evaluate the influence [of the NCP]with aggregate data, identify andanalyze causes of less than optimal[NCP] performance and outcomes, andrefine the use of the NCP. These out-comes management actions continueand are combined in the updatedmodel as Research NCP (Figure 2 andFigure 3).The updated NCPM challenges pro-
fessionals to demonstrate theimproved nutritional health of clientsthrough participation in research andquality improvement activities. Aggre-gated data continue to be the founda-tion of NCP research. Infrastructure toaggregate and manage data from theNCP did not exist in 2008. An exampleof this new infrastructure is the AND-HII.16 ANDHII makes possible the newactivity, “Use aggregated data toconduct research.” This wording placesOutcomes Management in the center ofresearch priorities, which is necessaryto drive improvements at the organi-zation and health systems levels.17 Theimplication is that all professionalswhen using the NCP become researchparticipants as data contributors. Out-comes Management is no longer afunction reserved for those knowl-edgeable in research design, data pro-cessing, and statistical analysis; rather,it becomes an integral, collaborativeactivity for all professionals.Outcomes research not only includes
NCP research to benefit professionaldevelopment and practice, but alsoaims to show the beneficial effect ofthe NCP on the health of clients.5 Tothis end, two new activities are incor-porated into the Outcomes Manage-ment System of this updated NCPM.First, “Conduct continuous qualityimprovement” applies to improvingthe model and care delivery as pro-fessionals participate in a learning or-ganization. The second activity,“Calculate and report quality in-dicators,” supports the Academy’sengagement to promote the reportingof malnutrition quality measureswithin the US health care system,(http://www.eatrightpro.org/resource/practice/quality-management/quality-improvement/malnutrition-quality-improvement-initiative), and thereporting of quality indicators pursuedby other national health systems. These
10 JOURNAL OF THE ACADEMY OF NUTRITIO
activities support professionals’ abilityto report quality measures and otherresults from the Outcomes Manage-ment System to the framing rings. TheOutcomes Management System islinked to the selection of quality in-dicators during Nutrition Monitoringand Evaluation. Through the fullydeployed Outcomes Management Sys-tem, professionals influence the NCPenvironment defined by the framingrings.
NCPTA terminology that describes the NCP isnecessary to document the deliveryand study of nutrition care. Creation ofthe NCPT is a contemporaneousendeavor with the development of theNCP. Terminology work began in2003,18 and a terminology to supportthe NCP was published as a printedmanual in 2009: International Dieteticsand Nutrition Terminology ReferenceManual: Standard Language for theNutrition Care Process.19 In 2014, Inter-national Dietetics and Nutrition Ter-minology was converted to anelectronic database, called the eNCPT,as the management of an expandingterminology (Figure 3) exceeded thecapabilities of a printed manual. eNCPTis currently translated from US Englishinto Swedish, German (Swiss), French(Canadian), Norwegian, and Danish. Atthe time of this writing, Chinese(Simplified), Chinese (Mandarin), Por-tuguese (Brazilian), and Spanish(Mexican) translations are in progress.NCPT can be used to document
nutrition care in any medium, but it isfundamental when documenting in anelectronic health record. In 2011, workbegan to map and model the NCPT intointernational medical terminologystandards. Mapping and modeling areessential for NCPT to be included in thedocument architecture for certified USelectronic health records. These termi-nologies have also been adopted inother countries. Mapping andmodeling are continuous processesbecause new terms are regularly beingadded to the NCPT. Recent additionsinclude terms describing findings ofthe Nutrition Focused Physical Exami-nation, terms resulting from movingMalnutrition Disorders into the clinicaldomain of Nutrition Diagnosis, acollection of terms focused on public
N AND DIETETICS
health, and alternative synonymsfor some behavior-related termsconsidered harsh by the internationalcommunity. Documentation of the NCPusing the NCPT creates data. The needto systematically collect these data andresearch the NCP led to the design ofANDHII, a web-based data registry.
ANDHIIANDHII is a data aggregation platformdesigned to collect data generated bythe application of the NCP. The plat-form has three functions: Smart Visitsthat enable data entry; Dietetics Out-comes Registry that generates reportsusing the aggregated data and supportcomparative effectiveness studies; andNutrition Research Informatics, whichfacilitates data collection and manage-ment for quality improvement andresearch projects. The structure ofANDHII is the NCP with data beingderived from NCPT.
Data aggregation schemes abound inhealth care. Data are routinely sub-mitted to health information ex-changes, accreditation agencies, payers,and government departments andministries. Examples include metricsrequired by The Joint Commissionconcerning patient safety or informa-tion about 30-day readmissionsrequested by the Centers for Medicareand Medicaid Services.
As with any electronic platform, theAcademy continuously works toimprove ANDHII’s usability and func-tionality to meet technologic, legisla-tive, and international needs. There ispotential for international use of AND-HII, although associated costs, trans-lation, and varying research ethicsregulations will need to be addressed.ANDHII has been used to explore thefeasibility of validating malnutritiondiagnostic criteria by aggregating datafrom the United States and Australia.20
ANDHII has also been used to investi-gate the influence of evidence-basednutrition practice guidelines for theprevention of diabetes on both practicepatterns and patient outcomes.5,21,22
These studies have demonstrated thepotential of incorporating tools such asANDHII into practice. With the avail-ability of ANDHII, the Outcomes Man-agement System can be integrated intopractice much like the process oflearning to write a Nutrition Diagnosis.
-- 2017 Volume - Number -

FROM THE ACADEMY
LOOKING AHEADThis article describes the current NCPMupdate and compares and contrasts itwith the 2008 version of the model.11
Themes that emerged were conciselanguage to promote translation,dissemination and adoption of NCP,promotion of professional-driven out-comes management with the emer-gence of smartphone applications andweb-based data aggregation tools, andembracing PCC.9 Further, the articledescribes how the NCPM is supportedby its standardized terminology, NCPT,and outlines ongoing integration ofNCPM/NCPT into an innovative out-comes management platform.16
The NCP and NCPM will continue toundergo evaluation and updating. Thesupporting NCPT will require refine-ment to sustain the reporting of qualitymeasures and outcomes. Over the 14years of the NCPM’s adoption, the NCPcommunity has been growing andactively contributes to the global up-take, improvement, and research of theNCP.4-6,23-30 The NCPM has evolvedwith practice from a professional-defined care delivery system to a PCCinteraction. The NCPM progresses fromlearning to write nutrition diagnoses toroutinely entering outcomes of careusing a data aggregation tool. The NCPis evolving to become the internationalstandard for nutrition and dieteticscare delivery. To foster this maturation,three areas of focus are recommended:
Creation of New Knowledge
� Support NCP-related research;� use aggregated data to study all
steps of the NCP in a variety ofpopulations, practice cultures,and stages of professionals’career development;
� validate expected plans of carethat link nutrition diagnoseswith specific interventions todemonstrate effectiveness;
� investigate whether the NCPimproves outcomes comparedwith not using the NCP;
� define appropriate nutrition anddietetics outcomes; and
� enhance and develop electronic,digital standards, and structuresthat accept NCP data.
Globalization of the NCP
� Promote adoption of the NCPand translations of the NCPT;
-- 2017 Volume - Number -
� support the NCP in diversepractice cultures;
� determine economic value ofdietitian/nutritionist inter-ventions with clients; and
� continue internationalcollaborations.
Continuous Training Focused onPractice Area and Professional’sCareer Development Stage
� Adopt NCPM to all stages ofcareer development, novicethrough expert;
� use NCPM as a framework for allpractice areas, including publichealth, health promotion, anddisease prevention;
� study NCPM as an effective toolfor educating professionals inscience-based practice; and
� train professionals to effectivelyand efficiently use PCC resourcesand techniques.
What Professionals Can Do
� Participate in the future andshare your plans at [email protected].
� Contribute data to ANDHII tosupport outcomes research.
� Collaborate in a translation ofNCP and NCPT.
� Pursue continuing educationfocused on quality indicators.
� Advocate for the value that theNCP brings to the health ofclients.
� Apply the NCP to create oppor-tunities that integrate research,professional development, andpractice for innovation anddiscovery.
References1. Lacey K, Pritchett E. Nutrition Care Pro-
cess and Model: ADA adopts road map toquality care and outcomes management.J Am Diet Assoc. 2003;103(8):1061-1072.
2. Hakel-Smith N, Lewis NM. A standardizednutrition care process and language areessential components of a conceptualmodel to guide and document nutritioncare and patient outcomes. J Am DietAssoc. 2004;104(12):1878-1884.
3. Memmer D. Implementation and practicalapplication of the Nutrition Care Processin the dialysis unit. J Ren Nutr. 2013;23(1):65-73.
4. Vivanti A, Ferguson M, Porter J,O’Sullivan T, Hulcombe J. Increased fa-miliarity, knowledge and confidence withNutrition Care Process Terminology
JOURNAL OF THE ACAD
following implementation across a state-wide health-care system. Nutr Diet.2015;72(3):222-231.
5. Thompson KL, Davidson P, Swan WI, et al.Nutrition care process chains: The“missing link” between research andevidence-based practice. J Acad Nutr Diet.2015;115(9):1491-1498.
6. International Confederation of DieteticAssociations. “Dietetics around theWorld: The Newsletter of the ICDA.”2011;18(2):2.
7. Hammond MI, Myers EF, Trostler N.Nutrition Care Process and Model: Anacademic and practice odyssey. J AcadNutr Diet. 2014;114(12):1879-1894.
8. Papoutsakis C, Moloney L, Sinley RC,Acosta A, Handu D, Steiber AL. Academyof Nutrition and Dietetics methodologyfor developing evidence-based nutritionpractice guidelines. J Acad Nutr Diet.2016;117(5):794-804.
9. World Health Organization. People Cen-tred Care in Low- and Middle-IncomeCountries—Meeting Report. Geneva,Switzerland: World Health Organization;2010.
10. Sladdin I, Ball L, Bull C, Chaboyer W. Pa-tient-centred care to improve dieteticpractice: An integrative review. J HumNutr Diet. 2017;30(4):453-470.
11. Nutrition Care Process and Model part I:The 2008 update. J Am Diet Assoc.2008;108(7):1113-1117.
12. Charney P, Peterson SJ. Practice Paper ofthe Academy of Nutrition and Dietetics:Critical thinking skills in nutritionassessment and diagnosis. J Acad NutrDiet. 2013;113(11):1545.
13. Academy of Nutrition and Dietetics.Nutrition Terminology Reference Manual(eNCPT): Dietetics Language for NutritionCare. Chicago, IL: Academy of Nutritionand Dietetics; 2016.
14. Shiner R, Tanner E, Collins C. RDN practicelevel and application of the Nutrition CareProcess. J Acad Nutr Diet. 2015;115(9):A25.
15. Mainz J. Defining and classifying clinicalindicators for quality improvement. Int JQual Health Care. 2003;15(6):523-530.
16. Murphy WJ, Steiber AL. A new breed ofevidence and the tools to generate it:Introducing ANDHII. J Acad Nutr Diet.2015;115(1):19-22.
17. Porter ME, Larsson S, Lee TH. Standard-izing patient outcomes measurement.N Engl J Med. 2016;374(6):504-506.
18. Nutrition Care Process part II: Using theInternational Dietetics and Nutrition Ter-minology to document the Nutrition CareProcess. J Am Diet Assoc. 2008;108(8):1291-1293.
19. International Dietetics and Nutrition Ter-minology (IDNT) Manual. Chicago, IL:American Dietetic Association; 2012.
20. Hand RK, Murphy WJ, Field LB, et al.Validation of the Academy/A.S.P.E.N.malnutrition clinical characteristics.J Acad Nutr Diet. 2016;116(5):856-864.
21. Hand RK, Abram JK. Sense of competenceimpedes uptake of new AcademyEvidence-Based Practice Guidelines: Re-sults of a survey. J Acad Nutr Diet.2016;116(4):695-705.
EMY OF NUTRITION AND DIETETICS 11

FROM THE ACADEMY
22. Murphy WJ, Yadrick MM, Hand RK. Vali-dation of an Automated Process for theComparison of Nutrition Care withEvidence-Based Nutrition Practice Guide-lines. Chicago, IL: American MedicalInformatics Association; 2016.
23. Hakel-Smith NA, Lewis NM, Eskridge KM.A methodology for evaluating documen-tation of the Nutrition Care Process. J AmDiet Assoc. 2007;107(8):A79.
24. AtkinsM, Basualdo-HammondC,HotsonB.Canadian perspectives on the nutritioncare process and international dieteticsand nutrition terminology. Can J Diet PractRes. 2010;71(2):e18-e20.
12 JOURNAL OF THE ACADEMY OF NUTRITIO
25. Porter JM, Devine A, O’Sullivan TA.Evaluation of a Nutrition Care Processimplementation package in hospital di-etetic departments. Nutrition & Dietetics.2015;72(3):213-221.
26. Lovestam E, Orrevall Y, Koochek A,Karlstrom B, Andersson A. Evaluation of aNutrition Care Process-based audit instru-ment, the Diet-NCP-Audit, for documen-tation of dietetic care in medical records.Scand J Caring Sci. 2014;28(2):390-397.
27. Rossi M, Campbell KL, Ferguson M.Implementation of the Nutrition CareProcess and International Dietetics andNutrition Terminology in a single-center
N AND DIETETICS
hemodialysis unit: Comparing paper vselectronic records. J Acad Nutr Diet.2014;114(1):124-130.
28. Porter JM, Devine A, Vivanti A, FergusonM,O’Sullivan TA. Development of a NutritionCare Process implementation package forhospital dietetic departments. Nutr Diet.2015;72(3):205-212.
29. Murphy WJ, Hand RK, Steiber AL. Practi-calities of using the Nutrition Care Processin research. J RenNutr. 2015;25(4):393-394.
30. Steiber AL, Leon JB, Hand RK, et al. Using aweb-based nutrition algorithm in hemo-dialysis patients. J Ren Nutr. 2015;25(1):6-16.
AUTHOR INFORMATIONW. I. Swan is chair, Nutrition Care Process Outcomes Committee of the Academy of Nutrition and Dietetics, Taos, NM. A. Vivanti is chair, NutritionCare Process Outcomes International Workgroup of the Academy of Nutrition and Dietetics; a research and development dietitian, Departmentof Nutrition and Dietetics, Princess Alexandra Hospital, Brisbane, Australia; and a senior lecturer, School of Human Movement and NutritionStudies, University of Queensland, Queensland, Australia. N. A. Hakel-Smith is a member of the Nutrition Care Process Outcomes AdvisoryWorkgroup of the Academy of Nutrition and Dietetics, and a manager, Clinical Nutrition Services, Bryan Medical Center, Lincoln, NE. B. Hotson is amember of the Nutrition Care Process Outcomes Committee of the Academy of Nutrition and Dietetics; a member of the Nutrition Care ProcessOutcomes International Workgroup of the Academy of Nutrition and Dietetics; and a regional clinical manager-acute care, Nutrition & FoodServices, Winnipeg Regional Health Authority, Winnepeg, Manitoba, Canada. Y. Orrevall is a member of the Nutrition Care Process OutcomesInternational Workgroup of the Academy of Nutrition and Dietetics; head of research and development, Education & Innovation, Function AreaClinical Nutrition, Karolinska University Hospital, Stockholm, Sweden; and is in the Department of Learning, Informatics, Management, and Ethics,Karolinska Instutet, Stockholm, Sweden. N. Trostler is a member of the Nutrition Care Process Outcomes Committee of the Academy of Nutritionand Dietetics; a member of the Nutrition Care Process Outcomes International Workgroup of the Academy of Nutrition and Dietetics; and aretired professor, Faculty of Agriculture, Food, and Environmental Sciences, Hebrew University of Jerusalem, Rehovot, Israel. K. Beck Howarter isprincipal, Ms. Nutrient Food and Nutrition Consulting Services, Evanston, IL; at the time of the study, she was director, Nutrition Care Process,Research International Scientific Affairs, Academy of Nutrition and Dietetics, Chicago, IL. C. Papoutsakis is director, Nutrition Care Process,Research International Scientific Affairs, Academy of Nutrition and Dietetics, Chicago, IL; at the time of the study, she was member of theNutrition Care Process Outcomes International Workgroup of the Academy of Nutrition and Dietetics, Chicago, IL.
Address correspondence to: Constantina Papoutsakis, PhD, RD, Academy of Nutrition and Dietetics, 120 S Riverside Plaza, Suite 2190, Chicago,IL 60606. E-mail: [email protected]
STATEMENT OF POTENTIAL CONFLICT OF INTERESTNo potential conflict of interest was reported by the authors.
FUNDING/SUPPORTThe Academy is the source of funding for the present Nutrition Care Process Model update. The authors and experts who conducted theNutrition Care Process Model update had complete autonomy during all stages of the update and writing of the present manuscript.
ACKNOWLEDGEMENTSThe authors thank those additional members of the Nutrition Care Process and Terminology Committee Research (NCP/T) Committee and theNCP/T International Workgroup who served during 2013-2014 (Terry Brown, MBA, MPH, RD, LD, CNSC; Joyce Buhler, RDN, CDE, CD; ElizabethCopes, RDN, LD, CNSC; Ingrid Darnley, Maree Ferguson, PhD, MBA, AdvAPD, RD; Margaret Garner, MS, RD, LD; Debra Geary Hook, MPH, RD, CNSD,CHES; Sue Kellie, MSc, FBDA; Yen Peng Lim, MHSc (Aust), PhD, ADS (Accredited Dietitian Singapore); Elisabet Rothenberg, PhD, RD; Carolyn Silzle,MBA, MS, RD, LD; Christina Sollenberg, MSc, RD; Lyn Lloyd, RD; Maggie Gilligan, RD, CSG; Paula-Ritter-Gooder, PhD, RD, CSG, LMNT; Camela Rising,MS, RDN, LDN; Lorraine Witherspoon, PhD, RD; and Jennifer A. Wooley, MS, RD, CNSC); and Academy of Nutrition and Dietetics staff membersAlison Steiber, PhD, RDN (chief science officer), Katie Gustafson (research assistant), and Robert Voss (NCP manager).
-- 2017 Volume - Number -