Embed Size (px)
Citation preview

Nutri&on approaches to ARDS
(Acute Respiratory Distress Syndrome)
Luisito O. Llido MD, FPCS, DPBCN, FPSGS Clinical Nutri:on Service St. Luke’s Medical Center, Quezon City Philippines

ARDS defini:on
Fanelli V, Vlachou A, Ghannadian S, SimoneI U, Slutsky AS, Zhang H. Acute respiratory distress syndrome: new defini:on, current and future therapeu:c op:ons. J Thorac Dis 2013;5(3):326-‐334

ARDS management
• Protec:ve mechanical ven:la:on
• Non conven:onal therapies in severe ARDS – prone posi:oning, – high frequency oscillatory ven:la:on
– extracorporeal membrane oxygena:on
• Therapies other than mechanical ven:la:on – conserva:ve fluid strategy
– neuromuscular blocking agents
• Future non-‐ven:latory therapeu:c op:ons – gene therapy for ALI/ARDS
Fanelli V, Vlachou A, Ghannadian S, SimoneI U, Slutsky AS, Zhang H. Acute respiratory distress syndrome: new defini:on, current and future therapeu:c op:ons. J Thorac Dis 2013;5(3):326-‐334

Immunopathophysiology
Google Images hdp://www.studyblue.com/notes/note/n/w-‐ards-‐-‐sepsis/deck/1264727
• Alveolar macrophages – APC, cytokines
• Granulocytes – proteases, cytokines, chemotaxis
• Complement – MACs • MALT ac:va:on -‐ cloning • Lymphocyte ac&va&on –
circula:on, cellular and humoral defense ac:va:on, cytokines
• Endothelial changes – chemokines, • Edema, hyaline membrane • Coagula&on changes • Fibroblasts – procollagen, fibrosis • Alveolar collapse

Inflamma:on phases of injury
Moore FA. Presiden&al address: imagina&on trumps knowledge. Am J Surg 2010: 200: 671-‐7.
24 hours
↑inflamma&on→organ dysfunc&on
↑immunosuppression→infec&on→organ dysfunc&on

Immunopathology approach

Nutri:on management approaches • Management phases
– Acute seIng (cri:cal care) • Malnutri:on assessment: Lean body mass management e.g. respiratory muscles, gas exchange
• Macronutrient and micronutrient manipula:ons • Adequacy of intake • Pharmaconutrients e.g. inflamma:on modula:on, protein synthesis • Pulmonary rehabilita:on
– Chronic seIng (long term follow up) • Lean body mass management e.g. respiratory muscle improvement • Adequacy of intake • Pharmaconutrients e.g. inflamma:on modula:on, protein synthesis • Pulmonary rehabilita:on • Exercise

ACUTE SETTING

Nutri:on management approach
Nutri:on Assessment
High Risk of developing complica:ons
Assess Lean Body Mass Loss (% weight loss)
Gas exchange Acid base balance Respiratory muscles
Plan Lean Body Mass maintenance /build up
Diet plan Pharmaconutri:on Adequate intake Pulmonary rehab

Nutri:on assessment Nutri&on screening Nutri&onal assessment
Lacuesta-‐Corro L et al. The results of the valida:on process of a Modified SGA (Subjec:ve Global Assessment) Nutri:on Assessment and Risk Level Tool designed by the Clinical Nutri:on Service of St. Luke’s Medical Center, a ter:ary care hospital in the Philippines. PhilSPEN Online Journal; March 16, 2014. hdp://www.dpsys120991.com/POJ_0002.html.

Part 1: Table of Contents: NST set-‐up, policies, protocols, procedures; Nutri:on Care Plan: 21-‐3. hdp://dpsys120991.com/Part1b_NST_SetUp.pdf

Nutri:on care plan
Part 1: Table of Contents: NST set-‐up, policies, protocols, procedures; Nutri:on Care Plan: 21-‐3. hdp://dpsys120991.com/Part1b_NST_SetUp.pdf

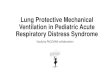
Lean body mass loss and mortality
>60% Mortality*

Lean body mass loss and mortality Loss of Total LBM
Complica&ons Associated Mortality
10% Decreased immunity Increased infec:ons
10%
20% Decrease in healing, increase In weakness, infec:on
30%
30% Too weak to sit, pressure ulcers, Pneumonia, lack of healing
50%
40% Death, usually from pneumonia 100%
Demling RH. Nutri:on, anabolism, and the wound healing process: an overview. Eplasty 2009;9:e9.
LBM=Lean Body Mass

Lean body mass changes in elderly
COMPLICATIONS SARCOPENIA

Lean body mass enhancers
• Acute phase – High protein intake
• Branched chain AA – Pharmaconutrients
• Fish oil (EPA/DHA) • Glutamine • HMB, glutamine, arginine combina:ons
– Adequate intake • Pulse feeding
– Insulin
• Long term – High protein intake – Pharmaconutrients – Adequate intake – Insulin – Exercise
• Impact of free radicals • Not too much an:-‐oxidants

Nutri:on management in ARDS Approach Acute Se]ng Long Term Se]ng
Lean body mass management e.g. respiratory muscle improvement
✔
Adequacy of intake (macro and micronutrients)
✔
Pharmaconutrients e.g. inflamma:on modula:on, protein synthesis
✔
Pulmonary support/fluid management/ rehabilita:on
✔
Exercise

Protein synthesis
Leucine (branched chain AA)
Hydroxy-‐methyl-‐butyric acid (HMB)
éPROTEIN SYNTHESIS
PROTEIN BUILD UP (LBM enhanced)
mTOR pathway
BCAA
Slows down protein degrada:on
Fish Oil (EPA/DHA)
(enteral and/or parenteral)
(enteral and/or parenteral)
(enteral)

Feeding approaches
Enteral nutri:on
Adequate intake Inadequate intake
Supplemental PN Enteral nutri:on • EPA/DHA • GLA • Glutamine • HMB • An:oxidants
Assess outcome
Assess outcome
• EPA/DHA • Glutamine • An:oxidants • Pulse feed
Assess outcome
GLA HMB
• ASPEN 2009 (cri&cal care) Guideline E2, E3, E4, H1 • ESPEN 2006 (cri&cal care) Guideline 1, 2
• ESPEN 2009 (cri&cal care) Guideline 1, 2, 6-‐17

Vitamin D3: immune-‐competence
Respiratory LN -‐ MALT
M-‐cells: An&gen Presen&ng Cells (APC)
Peyer’s Patches -‐ GALT
Lymphocyte ac:va:on
T-‐Cells upregulate gut homing receptors
Lamina propria – • Assist IgA forming B-‐Cells • Secretory IgA • T-‐Cell/B-‐Cell clones
VITAMIN D3
Alveolar macrophage (APC)
GIT PULMONARY
The role of the gut in immune competence
Van der Stede Y et al. 1alpha,25-‐dihydroxyvitamin D3 increases IgA serum an:body responses and IgA an:body-‐secre:ng cell numbers in the Peyer's patches of pigs aoer intramuscular immuniza:on. Clin Exp Immunol 2004;135(3):380-‐90.

Pharmaconutri:on • HMB, glutamine, arginine combina:on
– HMB (β-‐hydroxy-‐β-‐methyl-‐butyric acid) • reduces inflamma:on • Improves protein synthesis • Improves ven:latory capacity
– Glutamine • Improves WBC func:on • An:-‐oxidant precursor
– Arginine • Improves microcircula:on • Enhances T-‐cell func:on
– Fish Oil (EPA/DHA) • Immunomodula:on • Protein synthesis
– An:oxidants • Metabolism enhancement
• Ven:lator improvement
• Pressure ulcer healing
• Organ func:on improvement
• Immune modula:on

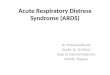
IMD (Inflamma:on modula:ng diet)
Gadek et al. Effect of enteral feeding with EPA, GLA, and an:oxidants in pa:ents with ARDS. Crit Care Med 1999; 27:1409-‐1420
N=146

(y2009)
N=38
Days

Elamin EM*, Miller AC, Ziad S. Immune Enteral Nutri:on Can Improve Outcomes in Medical-‐ Surgical Pa:ents with ARDS: A Prospec:ve Randomized Controlled Trial. J Nutr Disord Ther 2012; 2: 109.
17.5% 12%
N=22
P=0.01

Eicosanoids

Glutamine Saline group
Glutamine group
Animal study, sepsis model (cecal liga:on)
Singleton KD and Wischmeyer P. Glutamine Adenuates Inflamma:on and NF-‐kB Ac:va:on Via Cullin-‐1 Deneddyla:on. Biochem Biophys Res Commun. 2008 August 29; 373(3): 445–449.
* P < 0.05

Glutamine
Lai CC, Liu WL, Chen CM. Glutamine Adenuates Acute Lung Injury Caused by Acid Aspira:on. Nutrients 2014, 6, 3101-‐3116;
* animal study Legend: HV = acid aspira:on, high volume HVG = acid aspira:on, high volume + GLN LV = acid aspira:on, low volume LVG = acid aspira:on, low volume + GLN
* P < 0.05

Nutrient modifica:on
• CO2 load can be reduced through lipids – Non-‐protein calorie ra:o of 60%-‐70% lipid and 40%-‐30% carbohydrate
– Modified through modular feeding: enteral or parenteral • ESPEN 2009 guideline 2.6 (Grade B)
– Usually done when pa:ent is already in stable status in the acute and long term seIng
• Increased protein through pulse feeding

Pulse feeding

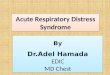
Adequate intake and survival in the ICU
Manuales G et al. Cri:cal Care Nutri:on -‐ the effect of adequate calorie and protein intake on mortality, ven:lator days, ICU and hospital stay: report from a private ter:ary care hospital in the
Philippines. PhilSPEN Online Journal 2014. hdp://www.dpsys120991.com/POJ_0001.html
71%
29% 74%
26%
N=80 Ven:lator: 55/80 (69%)

Nutri:on team and adequate intake
(n=80)
hdp://www.dpsys120991.com/POJ_0001.html

EN/PN GUIDELINES

ASPEN 2009 guideline
• E. Selec(on of Appropriate Enteral Formula – E2. Pa(ents with ARDS and severe acute lung injury (ALI) should be placed on an enteral formula(on characterized by an an(-‐inflammatory lipid profile (ie, ω-‐3 fish oils, borage oil) and an(oxidants. (Grade: A)
– E3. To receive op(mal therapeu(c benefit from the immune-‐modula(ng formula(ons, at least 50%-‐65% of goal energy requirements should be delivered. (Grade: C)
JPEN J Parenter Enteral Nutr 2009 33: 277

ASPEN 2009 guideline
• H. Pulmonary Failure – H1. Specialty high-‐lipid low-‐carbohydrate formula(ons designed to manipulate the respiratory quo(ent and reduce CO2 produc(on are not recommended for rou(ne use in ICU pa(ents with acute respiratory failure. (Grade: E) (This is not to be confused with guideline E2 for ARDS/ALI).
JPEN J Parenter Enteral Nutr 2009 33: 277

ESPEN 2009 Guidelines/ Recommenda:on/Grade
Macronutrient / Micronutrient
Type Dose Grade
Carbohydrate Minimum amount = 2 g/kg/day
Hyperglycemia = increased mortality
Grade B
Tight glucose control = increased hypoglycemia
Grade A
Protein balanced amino acid mixture
1.3–1.5 g/kg ideal body weight per day
Grade B
Glutamine 0.2–0.4 g/kg/day Grade A
Lipid To be provided daily Grade B
LCT/MCT | Fish Oils Grade C | B
Mul:vitamins Water soluble daily Grade C
Fat soluble daily Grade C
Trace elements daily Grade C

LONG TERM SETTING (POST ARDS)

Long term outcome • Survival sta:s:cs – Schmidt et al (1): Six months post-‐ICU discharge, 84 (60%) pa:ents were s:ll alive
– Herridge et al: (2) • Most deaths occurred within 6 months aoer discharge • Mostly due to exis:ng medical condi:on • Acute seIng sta:s:cs:
– Median 25 days in ICU; 48 days in the hospital – Lost 18% of baseline body weight
1. Schmidt M et al. The PRESERVE mortality risk score and analysis of long-‐term outcomes aoer extracorporeal membrane oxygena:on for severe acute respiratory distress syndrome. Intensive Care Med. 2013 Oct;39(10):1704-‐13.
2. Herridge MS et al. One-‐Year Outcomes in Survivors of the Acute Respiratory Distress Syndrome. NEJM 2003; 348 (8): 683-‐93.

Philippine experience

Long term outcome
Francisco EM. Report of home care clinical nutri:on program in a ter:ary care hospital in Metro-‐Manila. Abbod Nutri:on Symposium. PENSA 2011 Congress, Taipei, Taiwan.

Francisco EM. Report of home care clinical nutri:on program in a ter:ary care hospital in Metro-‐Manila. Abbod Nutri:on Symposium. PENSA 2011 Congress, Taipei, Taiwan.

Long term outcome (one year) N=109

Long term outcome (five years)
Herridge MS et al. Func&onal Disability 5 Years aher Acute Respiratory Distress Syndrome. NEJM 2011; 364 (14): 1293-‐1304
(N=83) (N=69) (N=71) (N=63) (N=64)
Post-‐discharge program • Self-‐instruc:on
exercise manual • Regular trainer visits • Nurse-‐led follow up
program • ICU diary interven:on • Nutri:on?
Change in weight

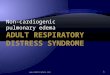
Long term outcome (five years)
66 68 67 71
76
40 45
50 46
49
0
10
20
30
40
50
60
70
80
1yr 2yr 3yr 4yr 5yr
Distance walked Return to work
Percen
t of p
redicted
Herridge MS et al. Func&onal Disability 5 Years aher Acute Respiratory Distress Syndrome. NEJM 2011; 364 (14): 1293-‐1304
Post-‐discharge program • Self-‐instruc:on
exercise manual • Regular trainer visits • Nurse-‐led follow up
program • ICU diary interven:on • Nutri:on?

Nutri:on management approaches Approach Acute Se]ng Long Term Se]ng
Lean body mass management e.g. respiratory muscle improvement
✔ ✔
Adequacy of intake (macro and micronutrients) ✔ ✔ Pharmaconutrients e.g. inflamma:on modula:on, protein synthesis
✔ ✔
Pulmonary support/fluid management/ rehabilita:on
✔ ✔
Exercise ✔

Manner of feeding
Needham DM et al. One year outcomes in pa:ents with acute lung injury randomised to ini:al trophic or full enteral feeding: prospec:ve follow-‐up of EDEN randomised trial. BMJ 2013;346:
Days aoer randomiza:on
P=0.54 N=525

Inflamma:on modula:ng diets
Rice TW et al. Enteral Omega-‐3 Fady Acid, γ-‐Linolenic Acid, and An:oxidant Supplementa:on in Acute Lung Injury. JAMA. 2011; 306(14): 1574–1581. (OMEGA trial)
N=143 (study) 129 (control)
* Trial stopped due to fu:lity

Inflamma:on modula:ng diets
Rice TW et al. Enteral Omega-‐3 Fady Acid, γ-‐Linolenic Acid, and An:oxidant Supplementa:on in Acute Lung Injury. JAMA. 2011; 306(14): 1574–1581. (OMEGA trial)
N=143 (study) 129 (control)
* Trial stopped due to fu:lity
Study group: • More sick (pneumonia, sepsis) • Poorer lung func:on • Very low protein/day (3.8g vs. 20g):
lost lean body mass daily • Very low carbo/day (4.2g vs. 31.8g):
lost protein due to gluconeogenesis • Higher fat (44.6g vs. 22g) and fish oil
levels (EPA/DHA=10g; GLA=10g) • Very high Vitamin C and E: leads to
inefficient protein synthesis • Bolus feeding (=diarrhea), reduced
intake • Became more malnourished at the
end of the study

Fish oils and protein synthesis
1.86g EPA 1.50g DHA
Clamp = insulin + glucose + amino acid infusion

HMB: β-‐hydroxy-‐β-‐methyl-‐butyrate

HMB: Hydroxy-‐methyl-‐butyrate
Deutz N, Hays N, Pereira S, et al.. Clin Nutr. 2011;6:219.


Summary: long term seIng Approach Long Term Details
Lean body mass management e.g. respiratory muscle improvement
✔ • 1.5 g/kg/day, BCAA, Pulse feeding, Fish oils, Insulin, HMB, Exercise
Adequacy of intake (macro and micronutrients) ✔ • Records
• Nutri:on team
Pharmaconutrients e.g. inflamma:on modula:on, protein synthesis
✔ • EPA/DHA/GLA, Glutamine, Arginine, An:oxidants
Pulmonary support/rehabilita:on ✔ • Lean body mass
enhancers (HMB, Fish oils, pulse feeding, exercise)
• Non-‐nutri:on mgt
Exercise ✔

Summary: acute and long term mgt Approach Acute Long Term Details
Lean body mass management e.g. respiratory muscle improvement
✔ ✔ • 1.5 g/kg/day, BCAA, Pulse feeding, Fish oils, Insulin, HMB, Exercise
Adequacy of intake (macro and micronutrients) ✔ ✔ • Records
• Nutri:on team
Pharmaconutrients e.g. inflamma:on modula:on, protein synthesis ✔ ✔ • EPA/DHA/GLA,
Glutamine, Arginine, An:oxidants
Pulmonary support/fluid management/ rehabilita:on
✔ ✔ • Lean body mass enhancers (HMB, Fish oils, pulse feeding, exercise)
• Non-‐nutri:on mgt Exercise ✔

THANK YOU