Embed Size (px)
DESCRIPTION
NURSING THEORY ADVANCE CONCEPT
Citation preview

Liaquat University of Medical and Health SciencesJamshoro Sindh
Advance Concept of Nursing
Khairunisa(BScN Year I)
College of Nursing, JPMC
Mrs. Ruth K. Alam

Liaquat University of Medical and Health SciencesJamshoro Sindh
Advance Concept of Nursing
Mussarat Begum(BScN Year I)
College of Nursing, JPMC
Mrs. Ruth K. Alam

LIAQUAT UNIVERSITY OF MEDICAL
AND HEALTH SCIENCEJAMSHORO SINDH
Valvular Heart DiseaseMs. Capt. Dur-e-Yakhta
ACN IIMs. Yasmin

OBJECTIVES
By the end of this session the learners will be
able to:
1. Define Valvular Heart Disease.
2. Discuss etiology and pahtophysiology of Valvular Heart Disease.
3. Identify signs and symptoms of Valvular Heart Disease.
4. Describe the management of Valvular Diseases.
5. Explain Nursing management in Valvular Heart Disease.
6. Enlist Nursing intervention in Valvular Heart Disease.
7. Know about preventing of Valvular Heart Disease.

1
VALVULAR HEART DISEASEThe heart valves when healthy keep blood flowing through the heart an lungs in the proper unilateral direction.
Diseased valve may impede the flow of blood from one chamber to the next (valvular stenosis) or they may allow blood to leak (regurgitate) back into the chamber from which blood is being pumped (valvular insufficiency or regurgitation).
Valvular Disease1. Mitral valve stenosis/Regurgitation.
2. Aortic valve stenosis/Regurgitation.
3. Tricuspid valve/Regurgitation.
4. Mitral valve prolapse syndrome.
Mitral Valvular Disease
The mitral (bicuspid) valve lies between the left atrium and ventricle. The mitral valve allows free blood flow forward, from the left atrium to the left ventricle. Equally important, it prevents backward flow from the ventricle to the atrium. Lesions of the mitral valve either obstruct the flow of blood from atrium to ventricle (stenosis) or allow blood to leak back from ventricle to atrium (regurgitation). In either case, mitral valve lesions overwork the left atrium.
Mitral Stenosis
Mitral stenosis is the commonest valvular lesion in people with rheumatic heart disease.
Etiology
Mitral stenosis results in obstruction to left ventricular filling. It must be differentiated from other (rare) conditions that impede left heart filling such as LA tumors, thrombus and cor triatriatum, and pulmonary vein stenosis.
Reheumatic fever – the most common cause of mitral stenosis, which ultimately leads to retraction, scarring, thickening, calcification, and immobility of the valve leaflets and subvalvular

apparatus. Two-thirds of cases of rheumatic mitral stenosis occur in women.

2
Other conditions – rare causes of mitral include:
Mitral annulus calcification (elderly).
Malignatn carcinoid syndrome.
Systemic lupus erythematosus.
Rheumatoid arthritis.
Congenital causes – in infants and children, mitral stenosis occur as a result of congenital deformity of the mitral valve, obstructing membranes, or abnormalities of the MV apparatus.
Pathophysiology
Valvulitis, from acute rheumatic infective endocarditis.
Leads to fibrosis and retraction of the valve leaflets.
The chordae tendinease contract and shorten and the mitral commissures fuse.
As the valves become calcified and immobile, the valvular orifice narrows, preventing normal passage of blood from left atrium to left ventricle.
The left atrium hypertrophies to compensate for the narrowed orifice.
Blood trapped in the atrium causes congestion and pulmonary hypertension.
These conditions overwork the right ventricle, sometimes leading to right ventricular failure. Inadequate filling of the left ventricle (preload) sometimes results in reduced cardiac output.
Diagnosis
Only 50% to 60% of patients may remember having had an attack of acute rheumatic fever (ARF).

3
Signs and Symptoms
1. Pulmonary Signs and Symptoms
a) Dyspnea
Dyspnea is the most common symptom.
With moderate mitral stenosis, dyspnea occurs in settings that require increased cardiac output (CO) (fever, anemia, pregnancy, exercise).
As mitral stenosis progresses, dyspnea occurs with minimal exertion and eventually at rest.
b) Hemoptysis
Hemoptysis is caused by rupture of thin-walled bronchial veins due to an acute rise in pulmonary venous pressure. Hemoptysis may be massive and life-threatening. Other causes of hemoptysis include pulmonary edema and chronic bronchitis.
c) Hoarseness
Hoarseness due to compression of the left recurrent laryngeal nerve by a dilated left atrium (LA) or pulmonary artery (PA) (Ortner’s syndrome) is a rare symptom.
2. Cardiac Symptoms
Fatigue – is secondary to diminished CO.
Palpitation – is commonly the result of atrial arrhythmias.
Chest pain – occur in 10% to 15% of patients.
Systemic embolism – phenomena occur as a result of LA body or appendage thrombus formation due to AF, stagnant LA blood now, decreased CO, and LA dilatation. Patients with suffering a systemic embolic event than do patients with a normal MV in sinus rhythm.

4
3. Physical Examination
Patients with a low CO have pink patches on the cheeks (mitral facies).
Signs of systemic venous hypertension occur when RV failure is present. These signs include:
Jugular venous distention (a prominent V wave suggests associated TR).
Peripheral edema.
Hepatomegaly.
Ascites
An RV lift is palpable along the left sternal border when significant pulmonary hypertension is present.
Sinus tachycardia or AF (more common) is present in advanced cases.
Diagnostic Findings
Diagnostic Procedure Findings
Chest X-ray Left atrial enlargement; Pulmonary venous congestion; Right ventricular enlargement.
Electrocardiogram Left atrial hypertrophy; P-mitrale (prolonged, notched P wave); Right ventricular hypertrophy; Atrial fibrillation.
Echocardiogram Thickened mitral valve with diminished movement of leaflets; Left atrial enlargement; Right ventricular enlargement.
Cardiac Catheterization Increased pressure gradient across mitral valve; Increased left atrial pressure; Increased pulmonary

vascular resistance; Increased left ventricular end-diastolic pressure (LVEDP) preload); Increased pulmonary artery wedge pressure (PAWP); Decreased cardiac output.

5
Management
1. Medical Therapy
a) Antibiotics
i) Rheumatic fever
Rheumatic fever antibiotic prophylaxis should follow recommended guidelines.
ii) Infective endocarditis
Antibiotic prophylaxis for infective endocarditis is necessary for all patients.
b) Diuretics and Sodium Restriction
Diuretic therapy and dietary sodium restriction are indicated when pulmonary vascular congestion is present.
c) Treatment of Atrial Fibrillation
i) Digitalis
Digitalis is used to decrease the ventricular response to AF.
ii) Beta Blockers and Calcium Channel Blockers
Beta blockers and Calcium channel blockers (verapamil, diltiazem) are alternative agents that can be administered in oral or intravenous form to slow the ventricular response to AF.
iii) Warfarin
Long-term therapy sufficient to prolong the INR to 2.0 to 3.0 is recommended for patients with mitral stenosis and chronic or paroxysmal AF to decrease the risk of thromboembolic events.
2. Surgical Therapya) Valvular Surgery
Valvular surgery is another common operation. Indications for this surgery include:

Progressive impairment of cardiac function due to scarring and thickening of the valve with either (a) impaired narrowing of the valvular opening (stenosis) or (b) incomplete closure (insufficiency, regurgitation).

6
Gradual enlargement of the heart with symptoms of decreased activity, shortness of breath, and congestive heart failure.
Today, surgeons can implant several different types of valves. Valve prostheses are divided into two broad groups:i) mechanical prostheses and (ii) porcine bioprosthetic valves. Commonly implanted mechanical prostheses include:
Caged-ball valve (Starr-Edwards): the most extensively used valve.
Eccentric monocusp or tilting disc valve.
Caged-disc valve (Cooley-Cutter).
3. Intervention Therapy
Intervention therapy is indicated for the patient with moderate to severe symptomatic mitral stenosis despite medical therapy (NYHA class III and IV with mitral valve area <1.0cm2/m2).
a) Open Mitral Commissurotomy
Open mitral commissurotomy, performed with direct vision on cardiopulmonary bypass, is indicated in the symptomatic patient with moderate to severe mitral stenosis whose valve is flexible and free of significant calcification or regurgitation.
At surgery, the fused commissures are separated, atrial thrombus is removed, and separation of fused chordae or papillary muscles is performed.
This procedure is preferable to prosthetic mitral valve replacement (MVR) because of lower periopreative mortality, lower long-term morbidity, and lack of requirement for long-term anticoagulation if sinus rhythm is maintained.
Approximately 50% of patients require repeat surgery (commissurotomy or MVR) within 10 years. After 10 years,

the incidence of restenosis dramatically, requiring repeat operation.
b) Percutaneous Balloon Mitral Valvuloplasty (PBMV)
Percutaneous balloon mitral valvuloplasty is an alternative to surgical commissurotomy.

7
c) Prosthetic Valve Replacement
Mitral valve replacement (MVR) is indicated in symptomatic, severe mitral stenosis when he valve is not amenable to open commissurotomy or percutaneous balloon mitral valvuloplasty.
Mitral valve replacement is associated with greater preioperative mortality and long-term morbidity compared to other mitral procedures.
In most cases, mitral valve replacement requires life-long anticoagulation.
Other Valvular Disorders
Valve
Disorder
Assessment Data Diagnostic Findings Nursing and
Medical
Intervention
Mitral regurgitation (Insufficiency)
Pansystolic, blowing, high-pitched murmur – at apex, radiating to axilla; Weak-ness, fatigue; Left ventricular failure: Dyspnea, orthopnea, PND, pulmonary crackles, S3 and S4; Palpitations; Right ventricular failure: Neck vein distention, peripheral edema, hepatomegaly.
Chest X-ray:
Left atrial and ventricular enlargement; Pulmonary vascular congestion.
Electrocardiogram:
Left atrial hypertrophy;P-mitrale; Atrial fibrillation; Left ventricular hypertrophy.
Echocardiogram:
Bizarre motion of mitral leaflets; Hyperdynamic left ventricle; Enlarged left atrium and ventricle.
Cardiac catheterization:
Increased left atrial pressure; Increased amount of regurgitant flow; Rule out prolapse and congenital disorders; Increased left ventricular end-diastolic pressure (preload); Increased pulmonary artery wedge pressure; Decreased
Antibiotic prophylaxis; Activity limitations; Sodium restriction; Diuretics; Digitalis; Vasodilators; Anticoagulation

cardiac output.
Continued

8
Valve Disorder
Assessment Data Diagnostic Findings Nursing and Medical
Intervention
Aortic stenosis
Systolic, harsh, crescendodecrescendo murmur – right sternal border radiating to neck; Dyspnea, orthopnea, PND S3 and S4; Fatigue; Vertigo and syncope; Chest pain; Ventricular tachycardia; Bradycardia; Low pulse pressure; Palpable thrill at second right intercostals space
Chest X-ray:Calcification of aortic valve; Left ventricular enlargement; Prominent ascending aorta.Electrocardiogram:Left ventricular hypertrophy; Sinus tachycardia, atrial fibrillation; AV conduction delay; Left and right bundle branch block (BBB).Echocardiogram:Limited aortic valve movement; Thickened left ventricular wall.Cardiac catheterization:Increased pressure gradient in systole across aortic valve; Decreased size of aortic orifice; Increased left ventricular end-diastolic pressure.
Antibiotic prophylaxis; Digitalis; Diuretics; Sodium restriction; Activity restrictions; Vasodilators; Oxygen (p.r.n.).
Aortic regurgitation (insufficiency)
Diastolic, blowing, decrescendo murmur – left sternal border, increases with inspiration; Loud S2; Dyspnea, orthopnea, PND; Fatigue, weakness; Syncope; Palpitations (water-hammer pulse); Pulmonary congestion, S3 and S4; Sinus tachycardia, PVCs; Wide pulse pressure; Large and diffuse diastolic thrill, left sternal border; Neck vein distention, ankle edema; hepatomegaly, ascites.
Chest X-ray:Calcification of aortic valve; Left ventricular enlargement; Dilation of ascending aorta.Electrocardiogram:Left ventricular hypertrophy; Sinus tachycardia, PVCs.Echocardiogram:Dilated and hyperdynamic left ventricle; Enlargement of aortic root and left atrium; Early closure of mitral valve; Diastolic fluttering of aortic valve.Cardiac catheterization:Decreased aortic diastolic pressure; Increased left ventricular end-diastolic pressure; Decreased regurgitant flow; Reflux through aortic valve.
Antibiotic prophylaxis; Digitalis; Diuretics; Vasodilators; Sodium restriction; Oxygen (p.r.n.); Activity restrictions..

Continued
9
Valve Disorder
Assessment Data Diagnostic Findings Nursing and Medical
Intervention
Tricuspid stenosis
Diastolic, rumbling murmur – left sternal border, increases with inspiration; Signs of right ventricular failure: neck vein distention, peripheral edema, hepatomegaly, RUQ pain.
Chest X-ray:Right atrial enlargement.Electrocardiogram:Tall, peaked P wave – right atrial hypertrophy; Atrial arrhythmias.Echocardiogram:Thickening and abnormal motion of tricuspid valve.Cardiac catheterization:Increased pressure across tricuspid valvegradient in systole across aortic valve; Decreased size of aortic orifice; Increased left ventricular end-diastolic pressure.
Antibiotic prophylaxis; Digitalis; Diuretics; Sodium restriction.
Tricuspid regurgitation (insufficiency)
Same as for tricuspid stenosis
Chest X-ray:Right atrial and ventricular enlargement.Electrocardiogram:Tall, peaked P wave; Right ventricular hypertrophy.Echocardiogram:Right ventricular dilation; Paradoxical septal motion; Tricuspid valvular thickening and abnormal motion.
Same as for tricuspid stenosis.
Nursing Management in Valvular Heart Disease
1. Nursing Assessment
Nursing assessment involves gathering subjective and objective data concerning (a) the type, severity and progress of the valvular disorder; (b) the degree of heart failure; (c) the person’s tolerance to activity; (d) the person’s support systems; and (e)

the degree of knowledge that the person and significant others have concerning the nature of and intervention for the disorder.

10
2. Nursing Diagnoses
Nursing diagnoses that may apply to people with valvular disease include the following:
Alteration in cardiac output: decreased, due to valvular abnormalities and/or arrhythmias.
Knowledge deficit regarding the nature of the valvular disorder and its intervention.
Knowledge deficit regarding ongoing home self-care.
Decreased activity tolerance due to valvular dysfunction and heart failure.
Anxiety due to the uncertain nature of the disease and its intervention.
Coping deficit due to the chronic nature of the valvular disease and activity limitations.
3. Nursing Goals
With appropriate and individualized interventions, the nurse can facilitate accomplishment of the following goals and intervention outcomes:
i) The person will maintain or restore hemodynamic stability, as evidenced by clear lungs on auscultation, maintenance of stable dry weight, urine output averaging greater than 30 ml per hour, no reported (or observed) dyspnea of orthopnea, normal vital signs, regular heart rhythm, absence of S3 and 4 heart sounds, and decreased or absent peripheral edema.
ii) The person and/or significant others will demonstrate understanding of the underlying valvular disorder and prescribed treatment as evidenced by ability to describe (a) the disease process, (b) factors contributing to symptoms and (c) rationale for intervention. They will

actively participate in the prescribed health behaviors that enhance success of intervention.

11
iii) The person will demonstrate progression toward an optimal level of physical activity tolerance, based on underlying cardiovascular status and psychosocial readiness. The person will demonstrate the ability to pace activity, verbalize improvement in fatigue, and express acceptance of any imposed activity restrictions.
iv) The person will show few behavioral and physical symptoms of anxiety and will use anxiety relief techniques.
v) The person will use adaptive coping strategies, as evidenced by the ability to recognize personal coping patterns and identify appropriate support systems and personal strengths.
Nursing Intervention
1. Nursing Diagnosis: Alteration in Cardiac Output: Decreased, Due to Valvular Abnormalities and/or Arrhythmias
The main goal of nursing intervention for valvular heart disease is to help the person maintain a normal cardiac output, thereby preventing manifestations of heart failure, venous congestion, and inadequate tissue perfusion.
To evaluate the effectiveness of therapeutic interventions, perform ongoing hemodynamic assessment.
Monitor vital signs closely.
A decrease in cardiac output manifests in a compensatory rise in heart rate, a drop in blood pressure, or a decrease in urinary output.
Carefully auscultate the chest to identify the presence of adventitious breath sounds (crackles, rhonchi) or heart gallops (S3, S4).
2. Nursing Diagnosis: Knowledge Deficit Regarding Ongoing Home Self-care

Before discharge, prepare detailed learning/teaching guidelines for the person and significant others concerning the therapeutic regimen.
Give information concerning prescribed medications.

12
Medications frequently prescribed include digoxin, diuretics, potassium supplements, anticoagulants, and prophylactic antibiotics.
Clearly explain their rationale, dosages, side effects and special considerations in their use.
You must also review exercise prescriptions with the person.
Aortic stenosis often requires activity restrictions, whereas other valve problems usually are self-limiting.
In addition, address dietary restrictions, and plan interdisciplinary follow-up.
Make sure the person knows whom to call when questions arise.
Preventing Valvular Heart Disease
Rheumatic heart disease, the most common cause of valvular heart disease, is preventable. Community nurses working in health care centers or schools can often detect individuals with beta-hemolytic streptococcal infections (the precursor to rheumatic heart disease). The nurse needs to refer these individuals for appropriate diagnosis and intervention.
References
1. Nursing people experiencing cardiovascular structural disorders; pp 991-1001.
2. Chung, EK and Tighe DA (1999). Valvular Heart Disease In: Pocket Guide to Cardiovascular Diseases. Blackwell Science Inc; pp 229-238.

LIAQUAT UNIVERSITY OFMEDICAL & HEALTH SCIENCES
JAMSHORO SINDH
Bladder Cancer
Farzana Kouser(BScN Part I Student)
ACN-II
Mrs. Munira A. Ali

Contents
Bladder Cancer
Definitions
Types
Pathophysiology
Etiology and Incidence
Clinical manifestation.
Investigation.
Management.
Nursing Diagnosis.
Nursing Intervention
References.

1
BLADDER CANCER
Cancer
It is a general term to describe malignant growth in the
tissue of which carcinoma is of epithelial and sarcoma of
connective tissue, origin as in bone and muscle.
Types of Cancer
Cancer are classified by their microscopic appearance and
the body site from which they arise. The name of cancer is
derived from the type of tissue in which develops, most
common are:
1. Carcinomas (Cancer Tumor)
Malignant tumors arise from epithelial cells.
2. Melanomas (Melano-Black)
Cancerous growth of melanocytes, skin cell produces
pigment melanin.
3. Sarcoma
Any cancer arises from muscle cell or connective
tissues.
i) Osteogenic Sarcoma (Bone origin)
Destroy the bone tissues.
4. Leukemia
Cancer of blood.
5. Lymphoma
Malignant disease of lymphatic tissue.

2
Pathophysiology
Cancer is disease process that began
Abnormal cell arise from normal body cell
Result from poorly understood mechanism of change
As disease progresses locally
Abnormal cell proliferate
Ignoring growth – regulating signals in the microenvironment surrounding cell
Cell acquire invasive characteristics
Change occur surrounding the tissue
Cell infiltrates these tissue and access to lymph and blood vessels
By which blood transported metastasis
To other part of body
Cancer is not a single disease with a single cause rather it
is a group of distinct disease with different causes,
manifestations, treatments and prognoses.

3
Bladder
Urinary bladder is a hallow muscular organ, which acts as a
reservoir.
Etiology
1. Cigarette smoking.
2. Carcinogens work environment such as dyes, rubber,
leather, ink or paint.
3. Coffee drinking.
4. Chronic parasitic infection.
Incidence
Age: More common after 50 years.
In man than woman (3:1).
Clinical Manifestions
Hematuria.
UTI.
Producing frequency.
Urgency.
Dysuria.
Alteration in voiding.
Pelvic or back pain.
Investigation
Urography.
Tomography.
Ultrasonography.
Biopsies.

4
Management
Treatment of Bladder cancer depends on the grade of
tumor.
1. Transurethral resection or fulguration (superficial
bladder cancer).
2. Chemotherapy.
3. Cystectomy.
Nursing Diagnosis
1. Alteration in urinary elimination pattern.
2. High risk for infection.
3. High risk for injury.
4. Alteration in nutrition.
5. Alteration in comfort (pain).
Nuring Intervention
1. Prevention of infection.
2. Prevention of injury related to bleeding disorder.
3. Maintenance of tissue integrity.
4. Relief of pain.
5. Decreasing fatigue.
6. Rehabilitation.

5
References
Smeltzer SC and Bare BG. Oncology: Nursing the
Patient with Cancer In: Brunner and Suddaraths
Text Book of Medical and Surgical Nursing.
7th Edition. JB Lippincott Co 1992.
Tertora-Grabowski. Principles of Anatomy and
Physiology. 7th Edition.

Estimated Cancer Deaths by Site and Sex


Liaquat University of Medical & Health SciencesJamshoro Sindh
Diabetes Mellitus
ACN-II
Maqbool AhmedM. Farooq SaeedKamla Kumari
(BScN Part-I Students)
Mrs. Munira A. Ali

OBJECTIVES
At the end of this session the learners will be able to:
8. Define Diabetes mellitus.
9. Enlist types of Diabetes mellitus.
10. Describe pathophysiology.
11. Enlist causes of Diabetes mellitus.
12. Explain clinical manifestation of Diabetes mellitus.
13. Enlist investigation for diagnosis of Diabetes mellitus.
14. Manage Diabetes mellitus.
15. Explain complications of Diabetes mellitus.
16. Demonstrate sites of insulin administration.
17. Enlist nursing diagnosis of Diabetes mellitus.
18. Explain necessary nursing intervention regarding Diabetes mellitus.

1
DIABETES MELLITUS
Definition
Diabetes mellitus is a clinical syndrome characterized by hyperglycemia
due to absolute or relative deficiency of insulin.
Diabetes mellitus is a group of chronic endocrine (pancreatic) metabolic
disorder caused by deficiency, absence or resistance to the action of insulin
characterized by hyperglycemia.
Types of Diabetes mellitus
The types of diabetes mellitus is describe by National Data Group in 1979 as
follow:
1. Type 1 or Insulin Dependent Diabetes Mellitus
In this type of diabetes, the beta cell of islet of Langerhans in pancreas could not
produce insulin. It occurs in any age, mostly before 30 years. It is also called
“Juvenile Diabetes Mellitus”.
2. Type 2 or Non-Insulin Dependent Diabetes Mellitus
It was formally called “Adult-Onset” or “Maturity-Onset” diabetes. In this type
insulin are present but there is a resistance to the biologic activity of insulin in liver
and peripheral tissues. This is mostly occurred after 35 years of age.
3. Diabetes Mellitus Associated With Other Condition or Syndrome
Secondary diabetes condition known or suspected to cause the disease like
pancreatic disease, hormonal abnormalities.
4. Gestational Diabetes
Gestational diabetes onset during pregnancy usually in the second or third trimester
due to hormones secreted by the placenta, which inhibit the action of insulin.

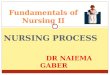
Pancreas
The pancreas is a pale grey gland weighing about 60 grams. It is about 12 to 15 cm
long and is situated in the epigastric and left hypochondriac regions of the
abdominal cavity. It consists of a broad head, a body and a narrow tail. The head
lies in the curve of the duodenum, the body behind the stomach and the tail lies in
front of the left kidney and just reaches the spleen. The abdominal aorta and the
inferior vena cava lie behind the gland.
Structure
The pancreas is both an exocrine an endocrine gland. The exocrine part consists of
a large number of lobules made up of small alveoli, the walls of which consist of
secretory cells. Each lobule is drained by a tiny duct and these unite eventually to
form the pancreatic duct that extends the whole length of the gland and opens into
the duodenum at its midpoint. Just before entering the duodenum the pancreatic
duct joins the common bile duct to form the ampulla of the bile duct. The duodenal
opening of the ampulla is controlled by the sphincter of Oddi.
The islets of Langerhans are the endocrine part, consisting of groups of specialized
cells distributed throughout the gland. They secrete the hormones glucagon and
insulin. The islets have no ducts sot he hormones pass directly into the blood.

The pancreas in relation to the duodenum and biliary tractPart of the anterior wall of the duodenum removed

5
Physiology
1. Endocrine Pancreas Hormones
The endocrine pancreas produces hormones necessary for the metabolism and
cellular utilization of carbohydrates, proteins and fats. The cells that produce these
hormones are clustered in groups of cells called the “Islets of Langerhans”. There
are three different types of cells in these islets.
i) Alpha Cells
These cells produce the hormone “Glucagon”. Glucagon stimulates the
breakdown of glycogen in the liver, the formation of carbohydrates in the
liver and the breakdown of lipids in the liver and in the adipose tissue. The
primary function of glucagon is to decrease glucose oxidation and to
increase blood glucose levels.
ii) Beta Cells
Beta cells secrete the hormone insulin. Insulin facilitates the movements of
glucose across the cell membranes into cells, decreasing blood glucose
levels. Insulin prevents the excessive breakdown of glycogen in the liver
and in muscle, facilitates lipids formation, inhibiting the breakdown of
stored fats and helps move amino acids into cells for proteins synthesis.
iii) Delta Cells
These cells produce a substance called “Somatostatin”. Somatostatin is a
neurotransmitter, and inhibits the production of both glucogan and insulin.

Pathophysiology
Type 1 (IDDM)
Insulin dependent diabetes mellitus/Type 1 or Juvenile diabetes can occurs at any
age but most commonly before the age of 30 years. It is the result of the
destruction of the beta cells of the islets of the Langerhans. When beta cells are
destroyed, then insulin is no longer produced. The destruction of the beta cells is
result from a combination of three factors:
1. Genetic predisposition.
2. Viral or toxic chemical.
3. Autoimmune attack.
The disease develops in five stages.
i) Genetic predisposition.
ii) Environmental trigger.
iii) Active autoimmunity.
iv) Progressive beta cells dysfunction.
v) Overt diabetes mellitus.
1. Genetic Predisposition
There is a relationship between the occurrence of IDDM and genetic
predisposition. The general risk of IDDM ranges from 1 in 400 to 1 in 1000. The
children of a person with diabetes have 1 in 20 to 1 in 50 risks. The genetic
markers that determine immune response have been found in 95% of people
diagnosed with IDDM are DR3 and DR4 histocompalibality. Further, if the father
have DM, then the risk is 2.5%, if mother then 2%, if both then 15% and if sibling,
then 3%.

2. Viral or toxic chemical (Environmental)
The environmental factors precipitate rather than initiate the diabetes mellitus and
also trigger the development of DM. The triggers are infections as mumps, rubella
or coxsachie virus BA, or chemical toxin such as those found in smoked and cured
meats. An exposure to the virus or chemical, an abnormal autoimmune response
occurs in which antibodies respond to normal islet beta cells as though they were
foreign substances, destroying them. The symptoms of IDDM appear when about
90% of the beta cells are destroyed or in the acute stage of the process. When an
illness or stress increase the demand of insulin beyond the reserves of the damaged
cells.
3. Autoimmune Attack
(HLA-DR-3 and B-15 known to be associated with immune endocrinopathy are
found with increased frequency in IDD patient). There is a co-existence of IDDM
and other forms of autoimmune endocrinopathy such as adrenal insufficiency,
hoshimotois thyriditis, hyperthyroidism, pernicious anemia and collagen vascular
disease.
Type 2 (NIDDM)
There are two main problems related to insulin:
Insulin resistance.
Impaired insulin secretion.
Insulin Resistance
Insulin resistance to a decreased sensitivity of the tissue to insulin normality.
Insulin binds to special receptors on cell surfaces due to this binding a series of
reaction involved in glucose metabolism occurs with the cell.

Causes of Diabetes Mellitus
Type 1 is characterized by destruction of the pancreatic beta cell. Currently, it is
thought that a combination of genetic, immunologic and possibly environmental
factors contribute to beta cell destruction.
1. Immunological Factors
In diabetes, there is evidence of an autoimmune response. This is an abnormal
response in which antibodies are directed against normal tissue of a body.
2. Environmental Factors
It has been proposed that certain viruses or toxins may precipitate the autoimmune
process that leads to beta cell destruction.
3. Genetic Factors
Genetic factors are thought to play a role in the development of insulin resistance.
In addition, these certain risk factors that are known to be associated with the
development of type 2 diabetes is included.
Signs and Symptoms
Type 1 (IDDM)
Hyperglycemia/Glucose urea.
Polyuria.
Polydipsia.
Polyphagia.
Weight loss.
Malaise.
Fatigue.
Abrupt and rapid onset of hyperglycemia.
Postural hypotension.Type 2 (NIDDM)

Slow onset of manifestation.
Polyuria.
Polydipsia.
Polyphagia.
Weight is mostly gained/obese.
Blurred vision.
Fatigue.
Paresthesias.
Skin infection (pruritis, vaginitis).
Lack of energy.
Delay wound healing.
Diagnostic Tests
Blood test is a major test, which is employed to diagnose the presence and severity
of diabetes and includes:
Fasting blood sugar.
Random blood sugar.
Glucose tolerance test.
Urine ketoacetosis (Urine test for glucose).

Management
There are three methods of management of diabetes.
1. Diet alone.
2. Diet and oral hypoglycemic drug.
3. Diet and insulin.
1. Diet
The patient of diabetes mellitus needs balance and special diet as mention below:
Foods to be avoided altogether include sucrose, glucose and foods high in
sucrose/glucose.
Carbohydrate foods to be eaten in moderation such as breads of all kinds,
rolls, scones, biscuits, crisp breads; breakfast cereals and porridge,
potatoes, peas, baked beans; all fresh and dried fruit; pasta, custard, thick
soups; ‘diabetic foods’, milk; meat, fish, eggs, cheeses.
Foods, which can be eaten, as desired include green vegetables, clear soups,
meat extracts, tomato or lemon juice, tea and coffee.
Beside this, routine should be made for regular exercise and daily walk to
induce weight loss and to reverse the insulin resistance.
2. Oral Hypoglycemic Drugs
These drugs are valuable in the treatment of patient with NIDDM who fail to
respond to simple dietary restriction. There are two groups of oral hypoglycemic
drugs.
a) Sulphonylureas - Non-obese.
b) Biguanides - Obese.

3. Insulin
Types of Insulin
a) Regular (R) (Humiten R)
i) Clear solution.
ii) Rapid onset.
iii) Short duration.
Indication
New cases of diabetes with dehydration and or ketoacidosis.
In emergencies e.g., ketoacidosis or surgical procedure.
In all IDDM in combination with depot insulin.
b) Modified or Intermediate and long acting Insulin
(Mixtard – 70% N + 30% R)
i) Cloudy solution.
ii) Delayed onset.
iii) Prolong duration because insulin is pre-mixed with retarding agents e.g.,
protamine or zinc.
Indication
In IDDM along with unmodified insulin.
c) NPH (N) Intermediate Acting (Isophane)

Sites of Injection
Any areas of the body with subcutaneous tissue may be used for injection of
insulin. The sites that allow the most rapid absorption are:
1. Abdomen (around umbilicus – 2 inch diameter).
2. Deltoid muscles.
3. Thigh.
4. Hip.
Sites of Insulin Injection

Preparation of Insulin
Administration of Insulin
1. Select site.
2. Clean with spirit swab.
3. While administrating insulin gently pinch a fold of skin and inject the
needle at 90 degree angle.
4. Do not massage after injected insulin.
5. Rotation of injection sites is recommended, distance about one inch.

Complications of Diabetes Mellitus
Hypoglycemia.
Hyperglycemia.
Macrovascular disease.
Microvascular disease.
Retinopathy.
Nephropathy.
Coronary artery disease (Myocardial Infarction).
Cardiovascular disease (Stroke).
Peripheral vascular disease.
Neuropathy (Nerve damage).
Sensorimotor.
Autonomic neuropathy.
Foot ulcers.
Nursing Diagnosis
Risk for injury.
Anxiety.
Fatigue.
Ineffective management of therapeutic regimen.
Risk for fluid volume deficit.
Sexual dysfunction related to vaginitis.
Altered nutrition.

Nursing Intervention
Maintenance of fluid and electrolyte balance. Intake and output are
measured.
Vital signs are monitored to detect signs of dehydration, tacychardia,
orthostatic, hypertension, etc.
Correction of metabolic abnormalities, glucose monitoring is performed
before meal and at bedtime. Insulin is administered as ordered.
In patient educational patient is taught survival skills including simple
pathophysiology, treatment modalities (insulin administration), monitoring
of blood glucose, urine ketones and prevention from complications.
Regular visit to the physician.
Teaching about appropriate preventive behavior (e.g., foot care and eye
care).
Normal range of blood glucose, the patient should know it.
Low literacy information is used as needed.
Family should be instructed to assist in diabetic management.

References
Smeltzen SC and Bare BG (1992). Text Book of Medical and Surgical
Nursing. Brunner and Suddarath (ed.). 7th Edition. JB Lippincott Co.
Kumar PJ. Clinical Medicine. 2nd Edition.
Edward CRW. Davidson’s Principles and Practice of Medicine. 16th
Edition.
Andeoli, Plum and Smith. Cecil Essentials of Medicine. 2nd Edition.
Schroeder SA. Current Medical Diagnosis and Treatment. 32nd Edition.
Baunwald and Wilson. Harison’s Principles of Internal Medicine. 12th
Edition.

LIAQUAT UNIVERSITY OFMEDICAL & HEALTH SCIENCE
JAMSHORO SINDH
Health Perceptions / Management Pattern
Aster GhulamMahmood AhmedMaqbool Ahmed
Rukhsana Perveen
ACN-I
Miss. Yasmin Parpio

OBJECTIVES
By the end of this session the learners will
be able to:
19. Define the terms health, wellness and illness.
20. Explain the Health Belief Model (HBM).
21. Identify the risk factors affecting health.
22. Describe implementation of nursing measures for promotion of health behavior, lifestyle and elderly care.
23. Explain nursing care process related to altered health maintenance.

1
Definitions
1. Health
Health is a state of complete physical, mental
and social well being and not merely the absence of
disease or infirmity (WHO 1947).
2.. Wellness
Wellness is a level of well being in which a
person perceives of being healthy.
3. Illness
Illness is a highly personal state in which the
person feels unhealthy or ill. Disease alters body
function and results in a reduction of capacities or a
shortened life span.
Models of Health and Wellness
Health is such a complex concept for which
various researchers have developed models or
paradigms to explain health and its relationship to
illness or injury. Models help health professionals to
meet health and wellness needs.

2
Smith’s Model of Health
Judith Smith (1981) describes four models of
health.
1. Clinical Model
Health is identified by the absence of
sign/symptoms of disease and injury. When
sign/symptoms disappear, a person is considered
healthy.
2. Role Performance Model
In this model a person is considered healthy if
he can perform work, although he may possess any
potential problem (e.g., lung tumor).
3. Adaptive Model
In this model health is a creative process,
disease is a failure in adaptation. The aim of
treatment is to restore the ability to adapt and to
cope.
4. Eu-daemonistic Model
When people fulfill their requirements and
complete development that is actualization.
Actualization is fully developed personality. In this
model health is seen as a condition of actualization
or realization of a person’s potential.

3
Leavell and Clark’s (1965) Agent Host
Environment
This is also called ecologic model. It is used to
identify the risk factors that result from interaction
of environment, host and agent.
1. Agent – any environmental factor or
stressor, biochemical, physical,
mechanical or psychological.
2. Host – a person who is caused family.
3. Environment – all factors external to the
host, climate, sound, economic.
Health Illness Continuum
a) Dunn’s High Level Wellness Grid
Dunn describes a health grid. The gird
demonstrates the interaction of environment with
wellness-illness continuum.
i) High level wellness in a favorable
environment – a person implements to
support his lifestyle by using all resources.
ii) Emergent high level wellness in an
unfavorable environment – a person has
knowledge but does not implement
adequate self-care.

4
iii) Protected poor health in a favorable
environment – an ill person (multiple
fracture) or hypertensive who meets
health care system.
iv) Poor health in unfavorable environment
e.g., a young child starving in a drought
stricken country.
b) Travis Illness-Wellness Continuum
According to this continuum health is not a
state but an ability to function with different levels.
Health is dynamic process with one end to death
and other to highest level of wellness and the
individuals can place themselves at different
locations at one point a time. Just like different
culture had their own norms and standards, health
has its levels.
Illness-wellness Continuum
Wellness model
Treatment model
DeathDisability Symptoms Signs Awareness Education Growth
Wellness
Neutral point

5
Elder Client Problems and Care
Physiologic changes such as decreased vision,
loss of hearing, diminished sense of smell and taste,
tooth loss, poor reflex reactions, memory
impairment, skin lost effectiveness as barrier,
general hair loss, range of motion of joints
decreases may be incontinence of urine, food
absorption disturbance and constipation may occur.
Nursing Care
Focus especially on known problems, check
nutritional status, disability and establish
supportive relationship. Teach activities of daily
living, any associated disease such as arthritis,
COPD and CHF should be monitored carefully. Be
careful when take a sample of specimen of elder
client.
Smoking
Smoking is a dangerous and risky habit for
health. It drains economically and affects the
respiratory system, which may cause respiratory
problems and lung cancer in a client. Many deaths
occur in world due to smoking every year.

Teach a client the effects of smoking and its
results in future. Counsel, if a client is interested
himself to stop smoking.

6
Obesity
Obesity is a common problem of our society,
which is a main cause of disease of cardiovascular
system. Increased level of cholesterol suffers a
client for it.
Provide food pyramid guide to an obese client
and teach him to walk, jogging, and exercise and to
participate social activities to control his weight.
Infection
Establishment of a disease process that
involves invasion of the body tissue by
microorganisms and the reaction of the tissues to
their presence and to the toxins generated by them.
Infectious Agent
Bacteria, virus and fungi.
Mode of Transmission
Direct, indirect and airborne.
a)Direct Transmission – by coughing,
sneezing, kissing, sexual intercourse.
b)Indirect Transmission – using patient’s
utensils, clothes, needles, soiled dressing,
contaminated food, water, by vectors.

c)Airborne – by droplet infection like
tuberculosis, whooping cough, etc.
7
Barrier to Infection
Body is protected against infection by
immunities. Body’s natural immunity, antitoxins,
vaccines and phagocytosis.
Conditions Predisposing to Infection
1. Surgical wound – microorganisms can enter
during post-surgical procedures.
2. Anti-bacterial Immune Mechanisms –
abnormalities limited, prohibited, synthesis of
antibodies against foreign bodies
(microorganisms).
Entrance of microorganisms in these route can
cause infection through procedures.
3. Respiratory Tract.
4. Genito-urinary Tract
5. Invasive Drugs – contaminated drugs I/V
solutions can be infective cause.
24. Vein Puncture Site – I/V canula, syringe can
enter bacteria to vein.
25. Implanted Prosthetic Devices – PPM shunts,
etc.

8
Standard Precaution to Control Infection
1. Hand washing before and after every
procedure.
2. Gloves (sterilize).
3. Mask eye protection face shield.
4. Gown.
5. Linen (clean, dry linen) (remove soiled and
contaminated linen).
6. Discard syringe needles in a container and
place contaminated articles in a leak proof
bags/containers.
7. Place client in isolation room if have
communicable disease.
8. Prepare a sterile field e.g., an operation theatre
by fumigation by carbolizing, etc. and by
supplying pre-packed supplies.

Scenario
Zahid Ali age 54 years old admitted with a
complaint of dyspnea and cough. He is a known
asthmatic patient. His recent investigation report of
CBC shows decreased Hb 4.0 g/dl, WBC 3.7 and Plt
is 49.
Nursing Diagnosis
Altered breathing pattern.
Altered health maintenance i.e., high risk for
infection.
Altered health maintenance i.e., high risk for
injury.

11
References
1. Erb and Kozier. Fundamental of Nursing. 5th
Edition. Blaise Wilkinsin California.
2. White L. Fundamental of Nursing. 1995
3. Smith and Duell. Clinical Nursing Skills. 4th
Edition. Appleton and Lange 1996.

Role Relationship PatternSTANDARD NURSING CARE PLAN
TITILE: HIGH RISK FOR INFECTIONPATENT’S NAME: Zahid Ali
D.O.A. 10/10/2005AGE:
54 YearsDIAGNOSIS: Anemia
C.R. NO.65296
CO-MORBITIES: AsthmaWARD NO.
12SIGN/DATE/TIME: M. Ahmed/10-10-05
BED NO.15
Date
Assessment(Data Statement)
Nursing Diagnosis Goal/Planning Nursing Intervention
10-1
0-20
05
Subjective Data:
Objective Data:A male patient 54 years old looks pale, weak and with respiratory distess.
Vital Sign:
Altered health mainten-ance i.e., high risk for infection related to decreased WBC i.e.,3.7 x 103 secondary to disease process and neutropnea
Short-term Goals:
Patient will be able to identify the measures to prevent infection within a day.
Long-term Goals:
Till hospitalization patient will remain free from symptoms of infection.Patient will not develop complications
Check vital signs 4 hourly.
Wash hands before and after any procedure and wear gloves.
Encourage iron supple-mentary diet to the patient.
Patient should be isolated.
Send and collect Lab reports.
Give medications on proper time and dose as prescribed by the doctor.
Check transfusion orders and transfuse to the patient on advised blood components.
Blood Pressure Temperature Heart rate Respiratory rate
Lab. Investigations
Hb WBC Platelet
90/70 mmHg 98 F 96 per min 30 per min
4 mg/dl 3.7 x 103
49
64

Role Relationship Pattern
LIAQUAT UNIVERSITY OF MEDICAL & HEALTH SCIENCES
JAMSHORO SINDH
Role Relation Pattern
Muhammad Farooq Saeed
ACN I
Miss. Yasmin Parpio
65

Role Relationship Pattern
Role is a comprehensive pattern of behaviors that is socially recognized
provides a means of identification and placing an individual in a society. Role is an
interaction point between the individual and society. Roles are responsibilities
including roles in family, work and social relationship. There are three types of
role i.e., acquired roles, achieved roles and interdependent roles.
Family is a structured system of a relationship in which individuals are
bound to one another by complex, interlocking relationship. Such type of
relationship is also known as kinship system. There are several forms of family.
Nuclear family consists of husband, wife and children. Nuclear Dyad family
consists of Husband and wife alone. Single Parent family consists of one head of
household (mother or father). Single Adult Alone family emerged either by chance
or choice, divorce or death of a spouse. Three Generation family consists of three
or more generations living in a single house. In Kin Networking family, nuclear
household or unmarried members live in close geographical proximity. Institution
family depends on children in orphanages or residential schools (hostel), and
Homosexual family depends upon homosexual couple with or without children.
The primary relationship in family members are husband and wife, mother and
daughter, father and son, father and daughter, mother and son, elder and younger
brother, elder and younger sister or brother and sister.
A Genogram resembles a family tree, however, it includes additional
relationships among individuals. The advantages of Genogram uses are to permit
the therapist and the patient to quickly identify and understand patterns in family
history. To map out relationships and traits that may otherwise be missed on family
background chart. To include basic information about number of families, number
of children of each family, birth order and deaths. Some gonograms also include
information on disorders running in the family such as alcoholism, depression,
diseases, alliances and living situations.
The factors affecting role relationship in family include socioeconomic
condition, family dynamics, changing roles (of institution), and gender role
expectation, type of personality and communication skills.
The development considerations according to age in neonate and infant are
attachment behavior such as crying, smiling, clinging, following and cuddling.
Depends on parents for basic needs, reciprocal interaction between infant and
parents, feeling of fear in case of loneliness and behavior in despair. In specific
66

Role Relationship Pattern
consideration, it includes fulfilling of basic needs, assess infants emotionally
especially when they are alone or in despair, understand crying process and
respond symbolic interaction. In toddler, it includes sense of right or wrong,
confirmation of social demands, depend of mother (parents) and starting of social
interaction. In preschooler, make friends of same sex, capable of internalizing the
social norms and tolerate brief separation of their parents. In terms of school age
child, learn social roles as male and female, enjoy school and peer interaction,
make friends of same sex, capability of expressing feelings, acknowledge
limitations, get allowance for increasing interest outside from the home. In
adolescent, dependence and interdependence, intensive relationship with opposite
sex, spend more time alone, peer and social interaction according to family needs.
Young adults, peak level of biophysical and cognitive skills, meaningful intimate
relationship, primary focus on establishment of family, marriage and parenting,
thinking involves reasoning, consider past experiences, education and possible
outcomes of a situation and learn how to deal with personal and desired needs of
others. In middle age adult, productive years for an individual, parenting role,
mostly secure in a profession/career, initiation of biological and physical changes,
accept the changes of age, prone to chronic diseases/illnesses and finally for older
adult, volunteer role (choice, demand), elder role modeling and depending upon
others.
Manifestation of altered family functions depends on stress, life
disturbance, impaired concentration, effectiveness of performance even at job,
decreased thinking capability and affected decision-making process. Mediators of
roles include role playing skills (symbolic interaction) and self-conception
(values/attitudes, body image, self-esteem and self-awareness about abilities). Role
relationship should be assessed by altered family process,, anticipatory grieving,
dysfunctional grieving, social isolation, impaired social interaction, impaired
verbal communication and altered role performance.
Nursing diagnoses can be made in terms of altered family process by the
state in which a family that normally function effectively experiences a
dysfunction.. A state in which an individual or family experiences a natural
response involving psychosocial, physiological reactions to an actual or perceived
loss (person, object, function, status, relationship) is known as grieving. It further
divided into anticipatory grieving and dysfunctional grieving. Anticipatory
67

Role Relationship Pattern
grieving is the state in which an individual/group experiences reactions in response
to an expected significant loss or extended, unsuccessful use of intellectual and
emotional responses by which individual attempts to work through the process of
modifying self-concept based up the perception of potential loss. Dysfunction
grieving is the state in which and individual/group experiences prolong unresolved
grief and engage in detrimental (harmful) activities or extended, unsuccessful use
of intellectual and emotional responses by which individual attempts to work
through the process of modifying self-concept based up the perception of actual
loss.
Social isolation or aloneness experienced by the individual and perceived
as imposed by others and as a negative or threatened state. Impaired social
interaction is the state in which an individual participates insufficiently, excessive
quantity, or ineffective quality of social exchange. Impaired verbal communication
is the state in which an individual experiences a desired or absent ability to use or
understand language in human interaction, and altered role performance is
disruption in the way one perceives one’s role performance.
68

Role Relationship Pattern
LIAQUAT UNIVERSITY OF MEDICAL & HEALTH SCIENCE
JAMSHORO SINDH
Sexuality and Reproductive Pattern
Mukhtari SardarNabeela TabassumMuhammad Yousaf
ACN
Miss. Yasmin Parpio
69

Role Relationship Pattern 70

Role Relationship Pattern
OBJECTIVES
By the end of this session the learners will
be able to:
26. Explain pattern description of sexual reproductive aspects of individual.
27. Enlist internal and external genital organs of male and female.
28. Define sexuality, sex and gender identity.
29. Describe types of sex.
30. Explain sexual concept and psychodynamic concern.
31. Enlist biological factors influencing sexuality.
32. Explain Nursing diagnosis and intervention.
71

Role Relationship Pattern
1
Pattern Description
This pattern focuses on the sexual reproductive
aspects of individual over the entire life span.
Sexuality pattern involve sex male behavior gender
identification and physiologic and biology function
as well as the cultural and societal expectations of
sexual behavior. An individual’s anatomic structure
identifies sexual status, which determine the social
and cultural responses of other toward the
individual’s responsive behavior toward other.
Reproductive pattern involve the capability to
procreate, actual procreation and the ability to
express sexual feeling the success or failure of
psychologically and physically expressing sexual
feeling and procreating can effect an individual’s
lifestyle, health and self-concepts.
The Nurse may care for client who, because of
illness, violence or lifestyle experience alteration or
disturbance in their sexual health and affect their
sexuality and reproductive pattern.
72

Role Relationship Pattern
2
Internal and External Male and Female Genital Organs
The internal and external genital organs of
male and female are:
Male Genital Organs Female Genital Organs
1. Scrotum 1. Labia majora
2. Penis. 2. Labia menora
3. Perineum 3. Vestibules
4. Testes 4. Glands of biathlon
5. Epididymis 5. Prepuce
6. Vas deference (Ductus)
6. Clitoris
7. Seminal vesicles 7. Vagina
8. Ejaculatory ducts 8. Uterus
9. Prostate glands 9. Fallopian tubes
10 Bulbourethral gland (Cowper’s)
10. Ovaries
11. Male urethra
73

Role Relationship Pattern
3
Sexuality
Sexuality includes all of those aspects of the human being that relate specifically to being boy or girl, man or woman. It is subject to life long dynamic change, as a function of the total personality. It concerned with the biologic, psychologic, sociologic, spiritual, and cultural variable of life.
Sex
It is the term most commonly used to denote biologic male and female status balance. It is also used to describe specific sexual behavior such as sexual intercourse.
Gender Identity
It is the individual’s persisting inner sense o the being male or female. It is development based on biologic sex and socio-cultural reinforcement, which is being at birth with identification of the baby as male or female.
Types of Sex
Biologic Sex
It includes the entire human being genetically determined anatomy and physiology, which is also influenced by intrauterine condition.
Sexual Identity or Sexual Orientation
It is the preference of a person for one sex or the other. Examples are:
1. Heterosexual – one who is sexually attracted to persons of the opposite sex (straight).
74

Role Relationship Pattern
2. Homosexual – one who is sexually attracted to persons of the same sex (gay, both sexes) and lesbian (woman).
75

Role Relationship Pattern
3
3. Rape – the act of forcing of a woman who has sexual intercourse against her will.
4. Gender Role Behavior – is the way a person acts as female or male, including the expression of what is perceived as gender appropriate behavior.
Sexual Concept
The development of sexuality begins with conception and changes throughout the life span. Every society develops expectations about acceptable forms of sexual expression.
Psychodynamic Concern
It is dynamic entity that changes our life span sexuality is a basic human characteristics and cannot be separated from life events.
Biological Factors Influencing Sexuality
Many factors influence a person’s sexuality.
1. Developmental level.
33. Culture.
34. Religion.
35. Values.
36. Personal ethics.
37. Disease processes.
38. Medication.
76

Role Relationship Pattern
4
Nursing Diagnosis
1. Sexual Dysfunction
It is defined as the state in which an individual experiences a change in sexual function that is viewed as unsatisfied unrewarding or inadequate.
2. Sexuality Pattern Altered
It is the state in which individual expresses concern regarding his/her sexuality.
3. Rape Trauma Syndrome
Force violent sexual penetration against the victim’s will and consents the trauma syndrome.
Nursing Intervention
(Dysfunction)
a) Assess and monitor the patient and partner’s level of knowledge and understanding of his/her dysfunction.
b) Provide the patient (couple) with privacy and maintain confidently.
c) Provide the patient with a safe non-judgmental atmosphere.
(Pattern Altered)
d) Provide the patient with accurate information to increase the level of awareness.
e) Involve the couple in decision about the plan of care.
(Rape Trauma Syndrome)
77

Role Relationship Pattern
f) Assess the rape belief pattern and educate as needed.
g) Provide psychotherapy and rape support groups.
78

Role Relationship Pattern
Scenario
Razia Begum age 45 years old have difficulty in
sexual desire and stated that, “I have irritation,
burning and feeling uncomfortable and also
unsatisfied in sex.
I am depressed and felt change in my interest in
others and myself. I am unable to achieved desired
satisfaction.
79

Role Relationship Pattern
STANDARD NURSING CARE PLAN
TITILE: UNCOMFORT SEXUAL PATTERNPATENT’S NAME: Razia Begum
D.O.A. 10/10/2005AGE: 45 Years
DIAGNOSIS: Sexual DysfunctionC.R. NO. 67296
CO-MORBITIES: NilWARD NO.
SIGN/DATE/TIME: M. Yousuf/11-10-05BED NO. 15
Date
Assessment(Data Statement)
Nursing Diagnosis Goal/Planning Nursing Intervention
10-1
0-20
05
Subjective Data:Patient verbalized that, “I have difficulty in sexual desire and have irritation, burning, feeling uncomfortable and also unsatisfied in sex. I am depressed and change my interest ourself and other and I am feeling. I am unable to achieve desired satisfaction.
Objective Data:Female patient 45 years old was admitted with diagnosis sexual dysfunction change complaining of sex and change in sexual desire and feeling uncomfortable the during sex eue to this she is not satisfied from sexual desire and looking depress.
Vital Sign:
Sexual dysfunction related to sexual desire and burning during sex.
Short-term Goals:
Patient will have decrease complaint of sexual dysfunction after 3 days.
Long-term Goals:
Patient will have identify and know how to manage sexual dysfunction.
Build the relationship with patient.
Provide privacy for expressing sexuality.
Provide accurate information on affects of treatment on sexual function.
Use adequate amount of water soluble lubricant.
Use vaginal steroid cream and take sizs bath.
Advised the investigation, e.g., Urine C/S.
Blood Pressure Temperature Heart rate Respiratory rate
Lab. Investigations
Hb ESR
110/75 mmHg 99.8 F 96 per min 20 per min
12 mg/dl 12 mg/dl
80