Embed Size (px)
Citation preview

IOSR Journal of Nursing and Health Science (IOSR-JNHS)
e- ISSN: 2320–1959.p- ISSN: 2320–1940 Volume 7, Issue 2 Ver. VIII (Mar-Apr .2018), PP 01-18
www.iosrjournals.org
DOI: 10.9790/1959-0702080118 www.iosrjournals.org 1 | Page
Nurses Compliance With Focused Antenatal Care In Siaya
County Kenya
1Rosemary Aoko Chweya, 2 Dr/ Isis E. Gohar, 3Dr/ Niven R. Basyouni,
4Dina J. Chelagat
1Clinical Nurse Educator Of Obstetrics And Gynecologic Nursing, Moi Teaching And Referral Hospital/ Kenya 2Lecturer
Of Obstetric & Gynecologic Nursing. Faculty Of Nursing-Alexandria University-Egypt
3Assistant Professor Of Obstetric & Gynecologic Nursing. Faculty Of Nursing-Alexandria University-Egypt
Senior Lecturer Of Midwifery, 4Faculty Of Nursing, Moi University, Kenya Corresponding Author: Dr/ Niven R. Basyouni
Abstract Background: Antenatal care (ANC) is widely used to improve the health of pregnant women and encourage skilled
attendant at birth. Based on multicenter randomized controlled trial in 2002, WHO recommended implementation of focused
antenatal care (FANC) which is a goal oriented antenatal care approach, consisting of four ANC visits and a well-defined
set of activities proven to be beneficial for maternal and neonatal health. Despite Kenya having adopted Focused Antenatal
Care (FANC) for over a decade ago, little is known about the extent to which the nurses comply with the performance of the
procedures stipulated in its guideline. Especially the maternal morbidity and mortality as well as poor perinatal outcomes
have remained a major problem. The objective of this study was to assess the compliance of nurses with procedures set in the focused antenatal care (FANC)
guidelines in Siaya county of Kenya. Methods: This was a cross sectional observational study whereby quantitative health facility based data was collected by
observing the nurses’ performed actions during antenatal care service delivery. The study was carried out in government of
Kenya antenatal clinics in Siaya County of the former Nyanza province of Kenya. A stratified random sample of 110 nurses
working within the county health facilities was drawn using proportion allocation method. Three tools were used in data
collection. Findings: Nurses in Siaya County did not fully comply with focused antenatal care guideline; health education is given the
least consideration. Compliance was however associated with availability of adequate supplies, amount of time the nurse
spent with the client, the time the clinic services began and the period of time the nurse had worked in the particular clinic. Conclusion and Recommendations: Compliance of nurses can be improved by ensuring availability of supplies and
allowing nurses to have adequate time with clients. There is need to re-examine the core procedures of Focused Antenatal
Care guideline, thus the limited time be used for the procedures found to be most beneficial during the specific visit which
have a great implication in improve nursing care and women health. Key words: Antenatal care guidelines, Focused antenatal care, Nurses’ compliance, Siaya County. ----------------------------------------------------------------------------------------------------------------------------- ---------- Date of Submission: 25-03-2018 Date of acceptance: 16-04-2018
----------------------------------------------------------------------------------------------------------------------------- ---------- What this paper adds: Despite the effort made by the Kenyan Ministry of Health in this context, maternal morbidity and mortality remain a
major reproductive health problem.
Nurses in Siaya County did not fully comply with Focused Antenatal Care guideline; health education is given the least
consideration.
Compliance of nurses can be improved by ensuring availability of supplies and allowing adequate time with clients.
There is need to re-examine the core procedures of Focused Antenatal Care guideline, thus the limited time be used for
the procedures found to be most beneficial during the specific visit which have a great implication in improve nursing
care and women health.
I. Introduction The basic value of health is guaranteed through continuing enhancements in the well-being of women, newborns and
their families, to ensure that they can not only survive, but thrive and transform. Inspired by the Global Strategy for
Women’s, Newborn’s and Adolescents’ Health 2016–30 (1)
Even though there has been a decline in maternal mortality worldwide, sub-Saharan Africa still has the highest
maternal mortality ratio among developing regions(2). In the year 2015, it was estimated that 303,000 women died due to
causes related to pregnancy and child birth globally which translated to 830 maternal deaths daily out of which 530 were
from sub-Saharan Africa(3). Kenya, the African high density country in which maternal morbidity and mortality and perinatal
mortality remain major public health problems (4). Maternal mortality rate stands at 362 deaths in every 100,000 births
country wide with disparity between counties. Siaya county is one of the Kenyan counties with a relatively high maternal
mortality rate compared to the national rate and currently it stands at 691 per 100,000 live births(5).Furthermore it has been

Nurses Compliance With Focused Antenatal Care In Siaya..
DOI: 10.9790/1959-0702080118 www.iosrjournals.org 2 | Page
estimated that 25% of maternal deaths that occur in Kenya occur within the former Nyanza province where Siaya is
located(6).
Appropriate antenatal care is one of the pillars of safe motherhood initiative, a universal effort launched by world
health organization (WHO) and other collaborating agencies in 1987 with an aim of reducing the number of deaths
associated with pregnancy and child birth(7). Previous observational studies however tend to show that women who receive
antenatal care have lower maternal and perinatal mortality and better pregnancy outcomes(8). Antenatal care is a key element
aimed at improving women's health through detection and treatment of pregnancy related illnesses or identification of
women at risk of complications and ensuring that adequate measures are put in place to manage the complications(9).
A randomized controlled trial carried out in 2001 to compare the traditional or standard antenatal care model with a
new WHO model with limited number of visits (four visits) showed that there were no significant differences between the
two models in terms of outcome. The new basic model later named Focused Antenatal Care (FANC) is meant for women
with no evidence of pregnancy related problem and the guideline requires that women are evaluated during the first visit to
rule out any need for specialized care(10).
Kenya adopted FANC in 2003 and added some components to the guideline in response to the national needs.
Basic steps in the FANC requires the health care provider to gather information through history taking, examine the mother
and foetus by carrying out a physical examination and antenatal profile tests namely haemoglobin estimation, blood group
and rhesus type, venereal diseases research laboratory (VDRL), urinalysis and microscopy, HIV test and any other test
stipulated in the facility. The nurse then interprets the gathered information to make a diagnosis and evaluate any risk factors
.An individualized care plan is made for every client, if no abnormalities are identified, the care plan will focus on
counselling, birth preparedness and complication readiness. If the mother needs specialized care, the plan will be to refer her
to a higher health facility. Follow up care in subsequent visits will depend on initial findings of the first visit plus the
findings in the subsequent visits(6).
Clinical guidelines are set to ensure uniformity as well as quality in the provision of care and compliance with these
guidelines translates into the extent to which care giving practice conforms to evidence based practice(11). It is further
thought to be the minimum requirement in relation to quality assurance.
The intriguing question here, while the international community is quite optimistic about the potential of antenatal
care to ensure better maternal and neonatal outcomes, antenatal care programs routinely recommended in developing
countries are often poorly implemented and clinic visits can be irregular with long waiting times and poor feedback to the
clients. Consistent with this despite the effort made by the Kenyan Ministry of Health and other development partners to
train nurses and other health care workers on focused antenatal care, maternal morbidity and mortality as well as poor
perinatal outcomes remain a major problem in some parts of the country.
An antenatal care service like other health care services is provided by a team of health care providers, at the core of
this team is the nurse or midwife who in most cases run the antenatal clinics. The success of care given depends so much on
the nurses’ compliance with the antenatal care guidelines which comprise a number of procedures that are supposed to be
performed by the nurse at every antenatal clinic visit(12).
Previous research papers have outlined some factors that could inhibit effective implementation of FANC such as
inadequate staff training, shortage of equipment/supplies and inappropriate infrastructure(13), however not much has been
looked into in Kenya as far as the compliance of nurses with Focused Antenatal Care guidelines is concerned. The objective
of this study was therefore to establish if the nurses in Siaya County perform all the procedures outlined in the focused
antenatal care guideline and to determine their level of compliance with focus on the barriers encountered in this context.
II. Materials And Method Design:
A cross sectional observational research design was utilized.
Setting:
The study was carried out at the antenatal clinics in ministry of health facilities in Siaya County, Kenya. Health care at the
county is offered at four levels namely: Dispensaries, Health Centers, Sub County and County hospitals.
Dispensaries being the first level are 82; each has one nurse offering antenatal care services.
The second level is the health centers which are 77; each has one nurse offering antenatal care services.
Sub-county hospitals are the third level and are 9 in total and each has 3 nurses offering antenatal care services.
County hospital is the highest level and referral facility for the county, it has three nurses working in the antenatal
clinic.
Subjects:
Subjects of the study consisted of a stratified random sample of 110 nurses working in the previously mentioned antenatal
clinics throughout the county using proportion allocation method according to the number of nurses in the facilities which
total to 189 nurses offering antenatal care services in the county. Epi info program v 7.0 was used to estimate the sample size
by applying the following information:
Dispensaries have 82 nurses, required sample is 44 nurses.
Health centers have 77 nurses, required sample is 43 nurses.
Sub county hospitals have 27 nurses and the required sample is 20 nurses.
County hospital has three nurses working in antenatal clinic and all were included in the sample.
This makes the total sample size to be 110 nurses. All the above sample sizes were based on; Expected frequency =50%,
Acceptable error =10% and Confidence coefficient =95%
Nurses Compliance With Focused Antenatal Care In Siaya..
DOI: 10.9790/1959-0702080118 www.iosrjournals.org 3 | Page
Tools:
Three tools were used to collect data for the study.
Tool I: Nurses’ Socio-demographic data and working experience interview schedule.
Included: Gender, age, level of education, duration of experience in years, duration in current unit, previous training on
focused antenatal care, and level of health care facility.
Tool II: FANC Compliance Observation Checklist This tool was adopted from ministry of health Kenya FANC and mother and child booklet 2013 (14) to assess nurses'
compliance with FANC. It consists of thirty eight items divided into three main sections as follows:
Patient assessment (N=23), Prophylaxis (N=6) and Health Teaching (N=9)
Section A: Patient Assessment includes three parts:
Part 1: History taking (6 items) which include: demographic data, medical and surgical history, family history, past
obstetric and gynecological history, history of current pregnancy (parity, gravida, LMP, EDD), presenting complains if any.
Part 2: Physical examination (10 items) which include: weight and height, blood pressure, head to toe examination, signs of
anemia, breast examination, abdominal palpation, abdominal auscultation for fetal heart, lower limbs for edema and vaginal
exam if necessary.
Part 3: Laboratory investigations (antenatal profile) (7 items) which include: Blood for hemoglobin level, grouping and
Rhesus typing, VDRL for syphilis, HIV, blood slide for malaria parasites, urinalysis for sugar and albumin, any other lab test
done .
Section B: Prophylaxis:
Drugs administered (6 items) which include; Iron and folic acid, SP for malaria prophylaxis, tetanus toxoid injection,
antihelminth (deworming tabs), Insecticide treated mosquito net given and ARVs for HIV positive clients.
Section C: Health Teaching:
This include (9 items) related to information about: danger signs in pregnancy, nutrition in pregnancy, infant feeding,
sexually transmitted infection (STI), prevention of mother to child transmission of HIV (PMTCT), birth
preparedness/individual birth plan, immunization for the baby, post-partum family planning and whether the nurse has
elicited feedback and given client return date.
Scoring system Each practice item was given a score and a total was obtained for each nurse as follows; completely and correctly done
scored (3), incompletely or incorrectly done scored (2) and not done scored (1).
Nurses' compliance was computed using the following formula: Lowest score is 38, highest score is 114; 114 - 38 = 76, 76÷
3 categories =25.333 which we round up to 25. Thus
Poor compliance ranges from 38 to < 38+25 which is 38< 63.
Fair compliance from 63 < 63+25 which is 63 to < 88
Good compliance is above 88. The same formula was used to categorize level of compliance in specific sections. Nurses with good compliance score are regarded as compliant while poor and fair compliance scores are regarded as
noncompliance.
Tool III: Nurses’ compliance barriers to FANC.
This tool was developed by the researcher to asses barriers associated with compliance and included data about availability
of equipment and supplies required in provision of focused antenatal care namely weighing scale, height measuring scale,
blood pressure machine, and pinard stethoscopes.
Laboratory test reagents and equipment namely, urine testing strips, microscopes, HIV testing kits, blood group testing
reagents, hemoglobin machine, malaria slides or rapid diagnostic test kits for antenatal profile.
Availability of necessary drugs specifically ferrous sulphate tablets, folic acid tablets, antimalarial tablets, tetanus toxoid
vaccine and antiretroviral drugs
Staffing issues precisely time of starting to give services to clients, number of nurses, number of patients seen, time spent
with every client, challenges faced by the nurses while offering antenatal care as well as other activities performed by the
nurse alongside antenatal care that may affect compliance.
III. METHOD The study was carried out according to the following steps:
Approvals: Official approval from the directors of data collections settings was secured through an official letter from the faculty of
nursing Alexandria University after explanation of the purpose of the study
Tools:
Tools I and III were developed by the researcher after extensive review of recent and relevant literature.
Tool II was adopted from ministry of Health Kenya Focused Antenatal Care poster and mother and child health booklet 2013
with some modifications.
Tools content validity was tested by a jury of 5 experts in the field of obstetrics and gynecologic nursing, recommended
modifications were made and final tool produced after proving valid.
The tools reliability was done by Cronbach’s alpha test and was found to be highly reliable at 0.808.

Nurses Compliance With Focused Antenatal Care In Siaya..
DOI: 10.9790/1959-0702080118 www.iosrjournals.org 4 | Page
Pilot study:
A pilot study was carried out on 10 not included among the study participants. The main purpose of the pilot was to evaluate
the clarity and applicability of tools and no modifications was done.
Collection of data:
Data was collected over a period of three months which started on 3rd April and ended on 30th June 2017. All nurses were
individually interviewed to gather data for part I of tool I and tool II and the responses were filled by the researcher in the
relevant tools.
Information on the pregnancy and antenatal care services given during the visit was collected through direct observation of
each nurses’ performed activities during her provision of antenatal care on at least three clients till the researcher observed
all items on the check list and recorded in too II. Information on previous visits if required was confirmed from the client’s
clinic booklet.
Statistical analysis:
Data collected was categorized, coded, computerized, tabulated and analyzed using statistical package for social sciences
(SPSS) version19 program. The necessary tables were then prepared and statistical formula were used as percentage, chi
square test (X2) and fishers exact test at 5% level to find out the statistical significant difference of the results
Ethical considerations: After getting ethical clearance from Faculty of Nursing, Alexandria University Ethics committee, Kenyan ethical clearance
was sought from Maseno University Research and Ethics Committee (MUERC) for the research to be carried out in Kenya
and this was granted.
Witness written consent was then obtained from the County Director of Nursing Services in Siaya County after explaining
the purpose of the study. Confidentiality and privacy were maintained.
IV. Results
The results of this study is presented under the following headings; Nurses’ socio-demographic characteristics (Tables
I), Nurses’ working experience (Table II), Nurses’ performance of procedures in focused antenatal care (Tables III A,B,C -
V), Nurses’ total scores of compliance (Figure I and II), Barriers to nurses’ compliance (Tables VI- VII and figure III-VII),
and Statistical significance with compliance (Tables VIII -XI and Figures VIII -IX).
Table (I) represents the number and percent distribution of the study participants according to their socio-demographic
characteristics. More than two thirds (68.2%), were female. Almost 80% of the nurses observed were below 40 years in age
where 41.8% were aged between 22 and 30 years. The mean age of the study participants was 35.05 + 9.295 years old.
Considering marital status, more than three quarters of the study participants were married (77.3%). As regards level of
education, 80% of the study participants were diploma holders.
Table (I): Number and percent distribution of study participants according to their socio-demographic
characteristics.
Socio-demographic characteristics Number (110) Percentage (%)
Gender:
- Female
- Male
75
35
68.20
31.80
Age (years):
- 22-30 - 31-40
- 41-50
- Above 50
46 41
12
11
41.80 37.30
10.90
10.00
Minimum – Maximum 22 – 58
Mean + SD 35.05 + 9.295
Marital status:
- Married
- Single
85
25
77.30
22.70
Level of Education:
- Certificate
- Diploma - Degree (BSN)
16
88 6
14.50
80.00 5.50
Table (II) illustrates the number and percent distribution of the study participants according to their work
experience. About two thirds of the study participants (66.4%) had worked for ten years and below and only 3.6% had
worked for more than 30 years. The vast majority of the study participants (97.3 %) had stayed in their current clinics for
between 1-10 years. Almost three quarters (74.5%) of the study participants had attended some courses on antenatal care
while 5.5% had done other courses like management of malaria in pregnancy, antiretroviral therapy in pregnancy and
nutritional care in pregnancy. Concerning health facilities, the nurses worked in, two fifths of the study participants (40%)
worked in dispensaries and a minority of them (2.7%) was working in the county referral hospital.
Nurses Compliance With Focused Antenatal Care In Siaya..
DOI: 10.9790/1959-0702080118 www.iosrjournals.org 5 | Page
Table (II): Number and percent distribution of the study participants according to their working experience.
Working experience Number (110) Percentage (%)
Duration of experience in years:
- 1-10 - 11-20
- 21-30
- More than 30
73 22
11
4
66.40 20.00
10.00
3.60
Minimum- Maximum 1 – 36
Mean + Standard deviation 10.39 + 8.830
Duration in the current unit in years: - 1-10
- 11-20 - 21-30
107
2 1
97.30
1.80 0.90
Minimum- Maximum 1-30
Mean + Standard deviation 3.06 + 3.465
Previous training in ANC:
- Yes
- No
82
28
74.50
25.50
Training title:
- FANC - PMTCT
- EMONC
- Others - Not applicable
48 40
12
6 28
43.60 36.40
10.90
5.50 25.50
Health facilities the nurses work in:
- County Referral Hospital - Sub-County Hospital
- Health centre
- Dispensary
3 20
43
44
2.70 18.20
39.10
40.00
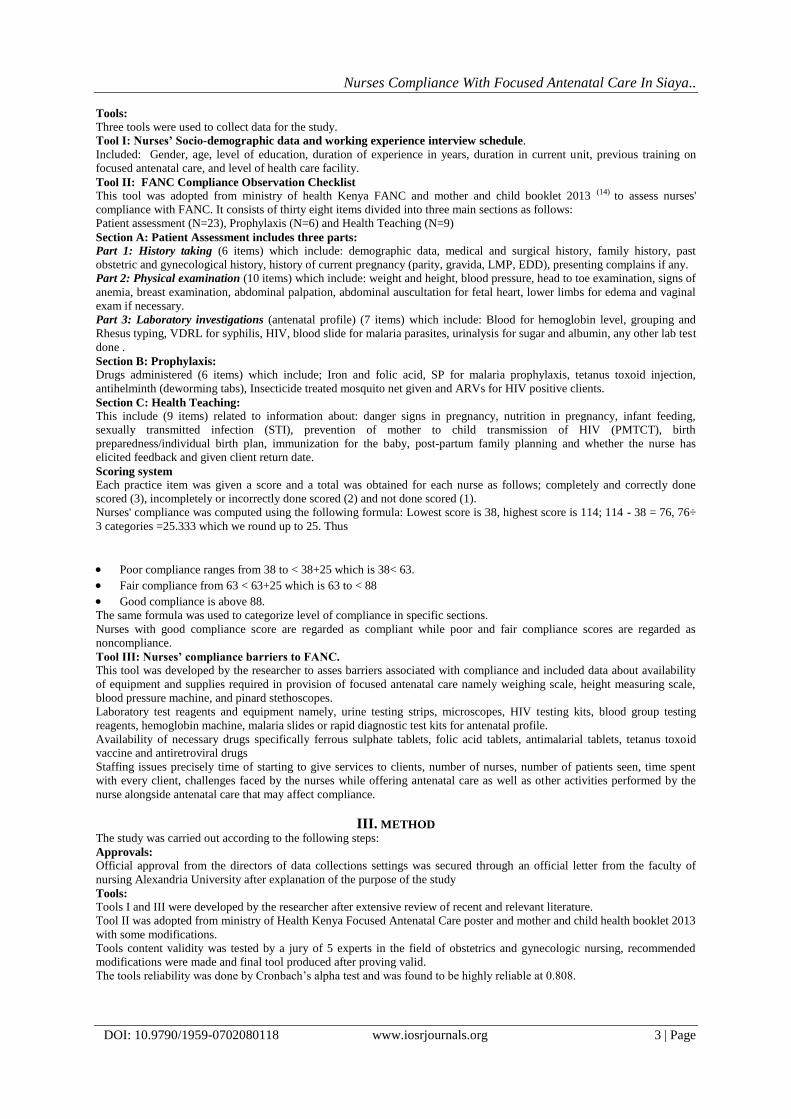
Table (III) represents the number and percent distribution of the study participants according to their performance
in patient assessment (history taking, physical examination and laboratory investigations). More than two thirds of the study
participants (67.3%) took the demographic data completely and correctly while 32.7% of them took incomplete demographic
data. The findings of the study also demonstrate that more than two fifths of the study participants (42.7%) took complete
medical and surgical history while 22.8% did not take any medical/surgical history at all. In addition, family history was
taken completely and correctly by 66.4% of the study participants whereas 23.6% of the participants did not take any family
history. Concerning past obstetrics and gynecological history, the study revealed that 28.2% of the study participants took it
completely and correctly while more than half of the study participants (52.7%) did not take past obstetrics and
gynecological history at all. Finally, current pregnancy history was taken by vast majority of the study participants (98.2%)
with only 1.8% taking it partially. (Table III A)
Table (III A): Number and percent distribution of study participants according to their performance in patient
assessment. (History taking)
A – History taking
Nurses’ performance in
history taking
Complete and
correctly
performed
Partially or incorrectly
performed
Not performed Total
No. % No. % No. % No. %
-Demographic data 74 67.30 36 32.70 0 0.00 110 100
-Medical/surgical history 47 42.70 38 34.50 25 22.80 110 100
-Family history 73 66.40 11 10.00 26 23.60 110 100
-Past obstetric and gynaecological history
31 28.20 21 19.10 58 52.70 110 100
-Current pregnancy history 108 98.20 2 1.80 0 0.00 110 100
-Presenting complains 94 85.50 N/A N/A 16 14.50 110 100
According to nurses' performance in physical examination, almost all (98.2%) of the study participants took the
weight of the clients and only 1.8% did not, however height measurement was done by two fifths (40%) only while 60% did
not measure clients’ height. The table also illustrates that blood pressure of the clients was taken by majority (94.5%) of the
study participants while 5.5% did not take the blood pressure. Additionally, head to toe examination was performed
completely by only 10.9% of the study participants. As far as assessment for anemia is concerned 48.2% of the study
participants performed it completely and correctly. Breast examination was performed completely by 26.4% of the study
participants and 67.3% did not perform breast examination on their clients. It was observed that abdominal palpation and
auscultation for the fetal heart was performed completely by all study participants at 100%. However, assessment for edema
Nurses Compliance With Focused Antenatal Care In Siaya..
DOI: 10.9790/1959-0702080118 www.iosrjournals.org 6 | Page
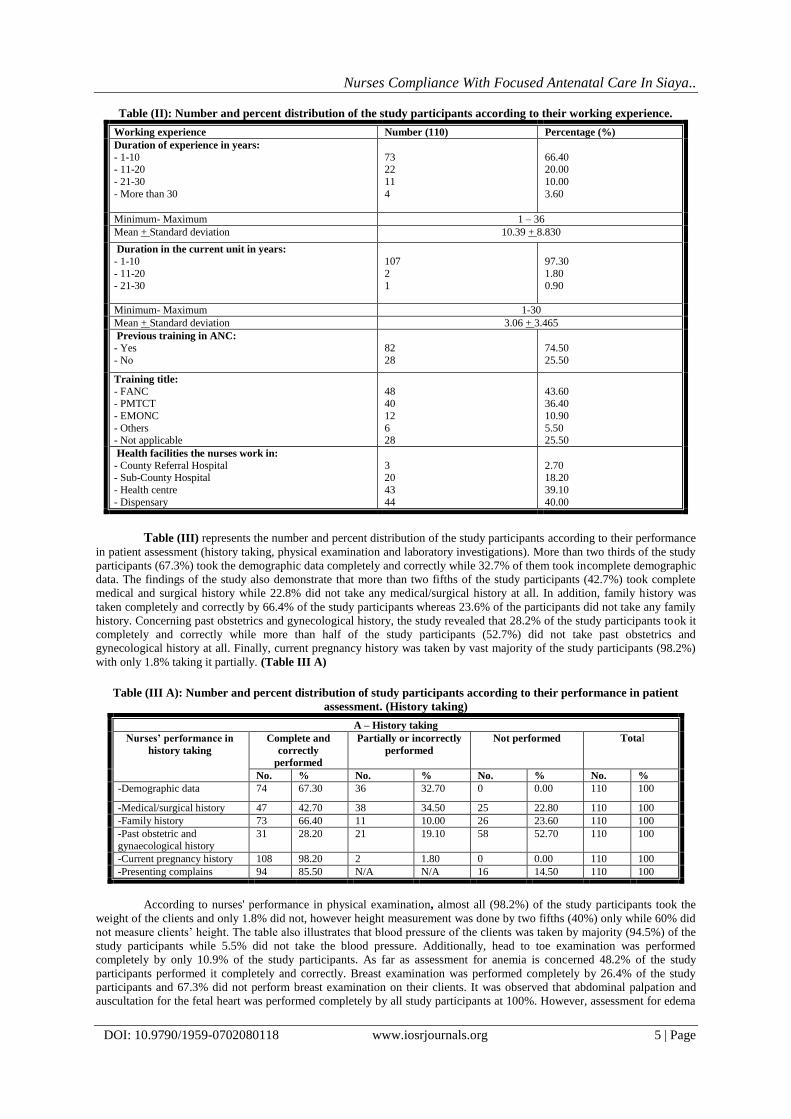
was performed completely by about one third of the study participants (31.8%). Lastly, vaginal examination was performed
by a minority of the study participants (5.5%). (Table III B)
Tables (III B): Number and percent distribution of study participants according to their performance in patient
assessment. (Physical examination)
B – Physical examination
Nurses performance
of physical
examination
Complete and correctly
performed
Partially or incorrectly
performed
Not performed Total
No. % No. % No. % No. %
-Weight measurement 108 98.20 N/A N/A 2 1.80 110 100
-Height measurement 44 40.00 N/A N/A 66 60.00 110 100
-Blood pressure
measurement
104 94.50 N/A N/A 6 5.50 110 100
-Head to toe
examination
12 10.90 24 21.80 74 67.30 110 100
-Anaemia assessment 53 48.20 3 2.70 54 49.10 110 100
-Breast examination 29 26.40 7 6.40 74 67.30 110 100
-Abdominal palpation 110 100 0 0 0 0.00 110 100
-Abdominal
auscultation
110 100 0 0 0 0.00 110 100
-Oedema assessment 35 31.80 0 0 75 68.20 110 100
-Vaginal Examination 6 5.50 N/A N/A 104 94.50 110 100
In relation to performance of the study participants in laboratory investigations or antenatal profile, it depicts that
62.7% of the study participants ensured that hemoglobin estimation was done for their clients. It was noticed that an equal
percentage of the study participants (66.4%) ensured that their clients had blood for grouping and rhesus typing done as well
as being screened for syphilis. HIV screening was performed by all study participants at 100% while screening for malaria
parasites was performed by 88.2% of the participants. Finally, 63.6% of the study participants ensured that their clients had
urine analysis and microscopy done. (Table III C)
Table (III C): Number and percent distribution of study participants according to their performance in patient
assessment. (Laboratory investigations)
C- Laboratory investigations (Antenatal profile)
Nurses performance of
lab investigations
Complete and correctly
performed
Partially or incorrectly
performed
Not performed Total
No. % No. % No. % No. %
-Haemoglobin level
estimation
69 62.70 N/A N/A 41 37.30 110 100
- Blood grouping and
Rh typing
73 66.40 N/A N/A 37 33.60 110 100
- VDRL (test for
syphilis)
73 66.40 N/A N/A 37 33.60 110 100
- HIV screening 110 100 N/A N/A 0 0.00 110 100
- Malaria testing 97 88.20 N/A N/A 13 11.80 110 100
- Urinalysis and
microscopy
70 63.60 N/A N/A 40 36.40 110 100
-Other laboratory tests N/A N/A N/A N/A 110 100 110 100
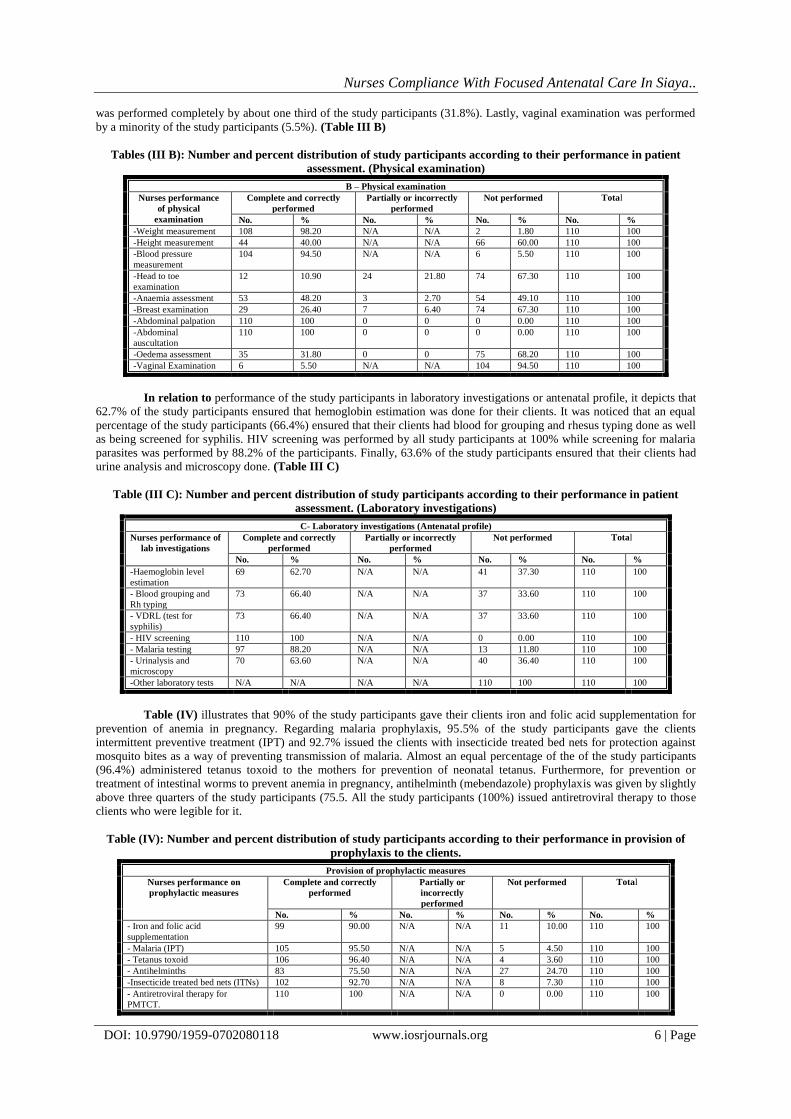
Table (IV) illustrates that 90% of the study participants gave their clients iron and folic acid supplementation for
prevention of anemia in pregnancy. Regarding malaria prophylaxis, 95.5% of the study participants gave the clients
intermittent preventive treatment (IPT) and 92.7% issued the clients with insecticide treated bed nets for protection against
mosquito bites as a way of preventing transmission of malaria. Almost an equal percentage of the of the study participants
(96.4%) administered tetanus toxoid to the mothers for prevention of neonatal tetanus. Furthermore, for prevention or
treatment of intestinal worms to prevent anemia in pregnancy, antihelminth (mebendazole) prophylaxis was given by slightly
above three quarters of the study participants (75.5. All the study participants (100%) issued antiretroviral therapy to those
clients who were legible for it.
Table (IV): Number and percent distribution of study participants according to their performance in provision of
prophylaxis to the clients.
Provision of prophylactic measures
Nurses performance on
prophylactic measures
Complete and correctly
performed
Partially or
incorrectly
performed
Not performed Total
No. % No. % No. % No. %
- Iron and folic acid
supplementation
99 90.00 N/A N/A 11 10.00 110 100
- Malaria (IPT) 105 95.50 N/A N/A 5 4.50 110 100
- Tetanus toxoid 106 96.40 N/A N/A 4 3.60 110 100
- Antihelminths 83 75.50 N/A N/A 27 24.70 110 100
-Insecticide treated bed nets (ITNs) 102 92.70 N/A N/A 8 7.30 110 100
- Antiretroviral therapy for
PMTCT.
110 100 N/A N/A 0 0.00 110 100
Nurses Compliance With Focused Antenatal Care In Siaya..
DOI: 10.9790/1959-0702080118 www.iosrjournals.org 7 | Page
Table (V) Outlines the performance of the study participants on health teaching to the clients. According to the
findings more than half of the study participants (50.9%) did not tell the clients about danger signs in pregnancy. Health
teaching on nutrition was given completely and correctly by 25.5% of the study participant while71.8% did not give the
clients any education about nutrition in pregnancy. Regarding infant feeding, more than four fifths (85.5%) did not give the
clients any health teaching on infant feeding. Additionally, health education about sexually transmitted infections in
pregnancy was not given by almost three quarters of the study participants (74.5%). Concerning prevention of mother to
child transmission of HIV (PMTCT), 34.5% of the study participants gave a complete and correct health talk to the clients,
4.5% gave it partially and 60.9% did not talk to the clients about prevention of mother to child transmission of HIV.
Furthermore, client education on birth preparedness was given completely and correctly by 44.5% of the study participants.
The majority of the study participants (96.4%) did not talk to the clients about immunizations. Regarding family planning
only 15.5% of the study participants gave the clients complete and correct health education about family planning. At the
end of the session around one fifth of the study participants (21.8%) asked for feedback from the clients to confirm if they
understood the messages shared and they gave them a return date for the next clinic visit.
Table (V): Number and percent distribution of study participants according to their performance in health teaching
to clients.
Health teaching
Performance of Nurses on
health teaching
Complete and correctly
performed
Partially or incorrectly
performed
Not performed
Total
No. % No. % No. % No. %
- Danger signs in
pregnancy
13 11.80 41 37.30 56 50.90 110 100
-Nutrition Education 28 25.50 3 2.70 79 71.80 110 100
- Infant feeding 14 12.70 2 1.80 94 85.50 110 100
-Sexually transmitted
infections
24 21.80 4 3.60 82 74.50 110 100
- Prevention of mother to
child transmission of HIV
(PMTCT)
38 34.50 5 4.50 67 60.90 110 100
-Birth preparedness 49 44.50 21 19.10 40 36.40 110 100
- Immunizations 4 3.60 0 0.00 106 96.40 110 100
-Post-partum family
planning
17 15.50 1 0.90 92 83.60 110 100
- Feedback from client and
return date
24 21.80 86 78.20 0 0.00 110 100
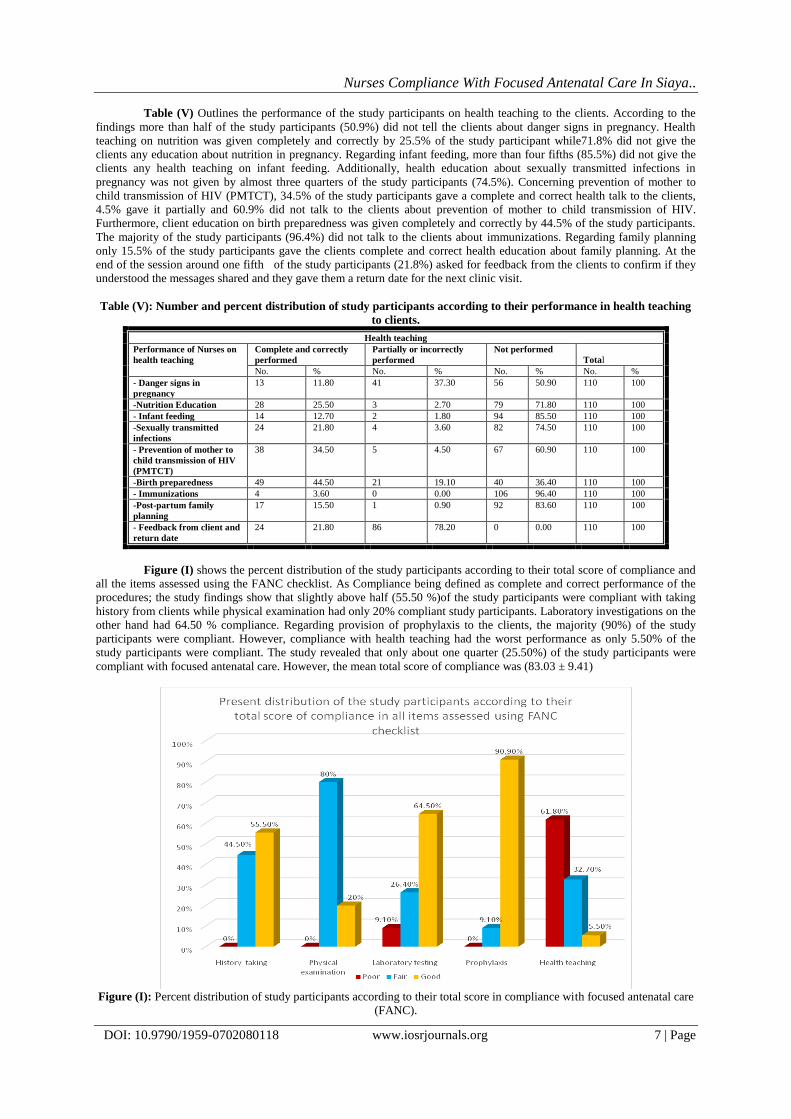
Figure (I) shows the percent distribution of the study participants according to their total score of compliance and
all the items assessed using the FANC checklist. As Compliance being defined as complete and correct performance of the
procedures; the study findings show that slightly above half (55.50 %)of the study participants were compliant with taking
history from clients while physical examination had only 20% compliant study participants. Laboratory investigations on the
other hand had 64.50 % compliance. Regarding provision of prophylaxis to the clients, the majority (90%) of the study
participants were compliant. However, compliance with health teaching had the worst performance as only 5.50% of the
study participants were compliant. The study revealed that only about one quarter (25.50%) of the study participants were
compliant with focused antenatal care. However, the mean total score of compliance was (83.03 ± 9.41)
Figure (I): Percent distribution of study participants according to their total score in compliance with focused antenatal care
(FANC).

Nurses Compliance With Focused Antenatal Care In Siaya..
DOI: 10.9790/1959-0702080118 www.iosrjournals.org 8 | Page
Figure (II) represents the percentage distribution of the study participants according to their level total score of compliance
with FANC. It was obvious that almost three quarters (74.50 %) of the study participants were fairly compliant with FANC
compared to 25.50 % of them who had good compliance whereas no study participant had poor compliance.
Figure (II): Percent distribution of study participants according to their total score of compliance with FANC
Barriers to compliance with FANC Table (VI) demonstrates the findings on infrastructure assessment about availability of equipment, laboratory reagents and
drugs required. Regarding equipment, the vast majority (98.20%) of the study participants had weighing scales and blood
pressure machines respectively in their facilities. Also height measuring scale was available to 74.50% of the study
participants. However stethoscopes were available to 69.10% of the study participants. Fetoscopes were available to all the
110 study participants at 100%. Looking at the laboratory equipment and reagents, almost an equal percentage of study
participants (60.90% and 60%) had urine testing strips and microscopes in their facilities. All the study participants (100%)
had HIV testing kits in their facilities; however blood grouping and rhesus typing reagents were available to 64.50% of the
study participants. Furthermore hemoglobin estimation machine (haemocue) was available to 59.10% of the study
participants. Malaria testing kits (rapid diagnostic test) was available in more than four fifths of the facilities (88.20%) where
the study participants worked at. Concerning the prophylactic measures majority of the study participants had most of the
drugs. Ferrous sulphate and Folic acid tablets were available to 92.70% and 91.80% of the study participants respectively,
most facilities had the combination tablet of folic and ferrous popularly known as Ifas. All the study participants (100%) had
antiretroviral drugs and sulfadoxine-pyrimethamine (SP or fansidar) tablets for malaria prophylaxis and tetanus toxoid was
available to 99.10% of the study participants.
Table (VI): Number and percent distribution of the study participants according to availability of supplies and
equipment required for compliance with FANC
Equipment and supplies
Study participants
(n = 110)
Available Not available
No. % No. %
A. Equipment
Weighing scale 108 98.20 2 1.80
Height measure 82 74.50 28 25.50
Blood pressure machine 108 98.20 2 1.80
Stethoscope 76 69.10 34 30.90
Fetoscope 110 100 0 0.00
B. Laboratory testing reagents and equipment
Dipsticks for urinalysis 67 60.90 43 39.10
Microscope for microscopic examinations 66 60.00 44 40.00
HIV test kits 110 100 0 0.00
Blood grouping reagents 71 64.50 39 35.50
Haemoglobin estimation machine 65 59.10 45 40.90
Malaria testing kits (slides or RDT) 97 88.20 13 11.80
C. Drugs
Ferrous sulphate tabs 102 92.70 8 7.30
Folic acid tabs 101 91.80 9 8.20
Antiretroviral drugs 110 100 0 0.00
Antimalarial tabs (SP) 110 100 0 0.00
Tetanus toxoid 109 99.10 1 0.90

Nurses Compliance With Focused Antenatal Care In Siaya..
DOI: 10.9790/1959-0702080118 www.iosrjournals.org 9 | Page
Fig (III) illustrates that almost three quarters (74.50%) of the study participants had adequate supplies and equipment
required for compliance in their health facilities
Figure (III): Percent distribution of the study participants according to supplies and equipment adequacy in their
facilities of work.
Figure (IV) demonstrates that slightly above three quarters (75.40%) of the study participants started attending to the clients
between 8.30am and 9.30am while 16.40% started between 7.30am and 8.30am. However, 8.20% of them started giving
services at the clinic after 9.30am.
Figure (IV): Percent distribution of the study participants according to their time of starting clinic services
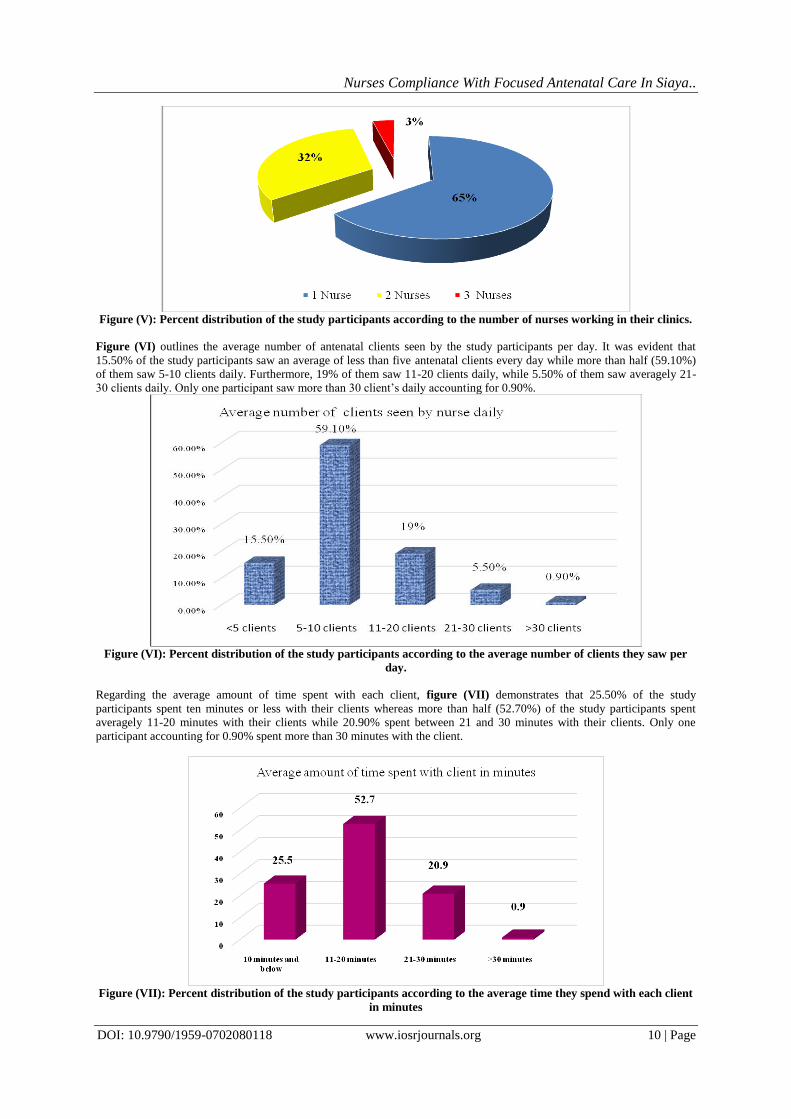
Figure (V) reveals that almost two thirds of the study participants worked alone in the clinic accounting for 65%, whereas
32% worked in clinics where they were two nurses and lastly 3% worked in clinics where they were three nurses.
Nurses Compliance With Focused Antenatal Care In Siaya..
DOI: 10.9790/1959-0702080118 www.iosrjournals.org 10 | Page
Figure (V): Percent distribution of the study participants according to the number of nurses working in their clinics.
Figure (VI) outlines the average number of antenatal clients seen by the study participants per day. It was evident that
15.50% of the study participants saw an average of less than five antenatal clients every day while more than half (59.10%)
of them saw 5-10 clients daily. Furthermore, 19% of them saw 11-20 clients daily, while 5.50% of them saw averagely 21-
30 clients daily. Only one participant saw more than 30 client’s daily accounting for 0.90%.
Figure (VI): Percent distribution of the study participants according to the average number of clients they saw per
day.
Regarding the average amount of time spent with each client, figure (VII) demonstrates that 25.50% of the study
participants spent ten minutes or less with their clients whereas more than half (52.70%) of the study participants spent
averagely 11-20 minutes with their clients while 20.90% spent between 21 and 30 minutes with their clients. Only one
participant accounting for 0.90% spent more than 30 minutes with the client.
Figure (VII): Percent distribution of the study participants according to the average time they spend with each client
in minutes
Nurses Compliance With Focused Antenatal Care In Siaya..
DOI: 10.9790/1959-0702080118 www.iosrjournals.org 11 | Page
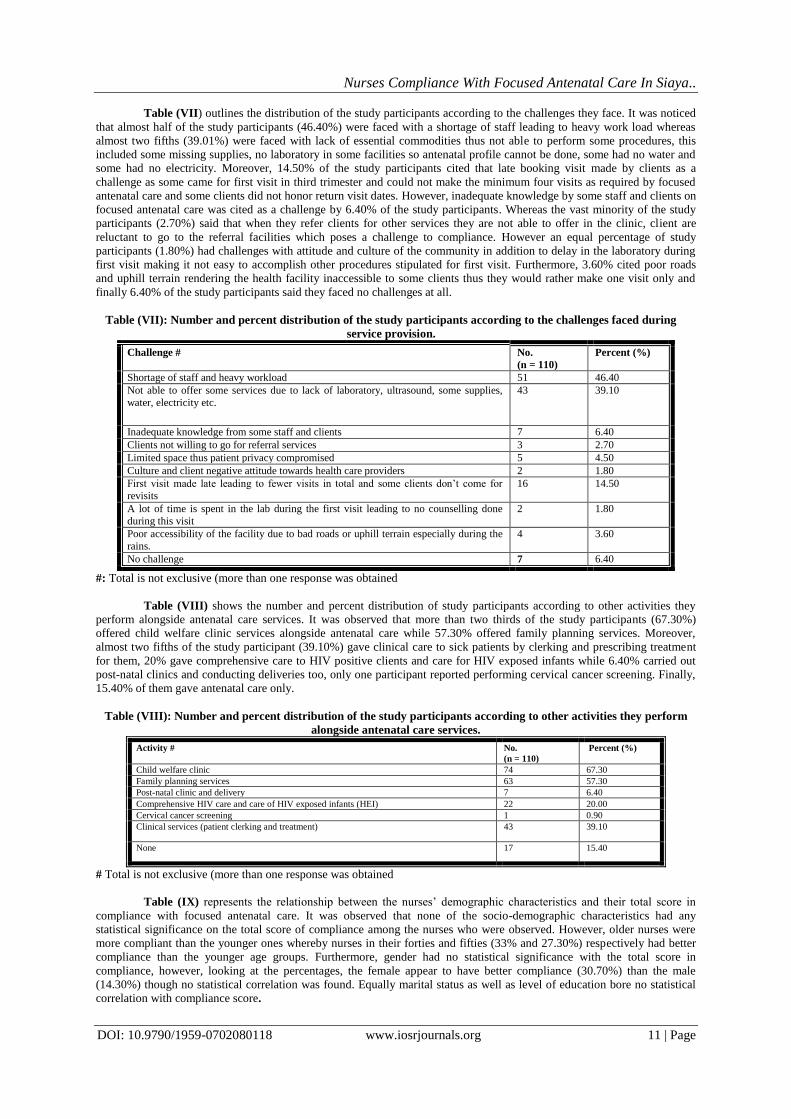
Table (VII) outlines the distribution of the study participants according to the challenges they face. It was noticed
that almost half of the study participants (46.40%) were faced with a shortage of staff leading to heavy work load whereas
almost two fifths (39.01%) were faced with lack of essential commodities thus not able to perform some procedures, this
included some missing supplies, no laboratory in some facilities so antenatal profile cannot be done, some had no water and
some had no electricity. Moreover, 14.50% of the study participants cited that late booking visit made by clients as a
challenge as some came for first visit in third trimester and could not make the minimum four visits as required by focused
antenatal care and some clients did not honor return visit dates. However, inadequate knowledge by some staff and clients on
focused antenatal care was cited as a challenge by 6.40% of the study participants. Whereas the vast minority of the study
participants (2.70%) said that when they refer clients for other services they are not able to offer in the clinic, client are
reluctant to go to the referral facilities which poses a challenge to compliance. However an equal percentage of study
participants (1.80%) had challenges with attitude and culture of the community in addition to delay in the laboratory during
first visit making it not easy to accomplish other procedures stipulated for first visit. Furthermore, 3.60% cited poor roads
and uphill terrain rendering the health facility inaccessible to some clients thus they would rather make one visit only and
finally 6.40% of the study participants said they faced no challenges at all.
Table (VII): Number and percent distribution of the study participants according to the challenges faced during
service provision.
Challenge # No.
(n = 110)
Percent (%)
Shortage of staff and heavy workload 51 46.40
Not able to offer some services due to lack of laboratory, ultrasound, some supplies,
water, electricity etc.
43 39.10
Inadequate knowledge from some staff and clients 7 6.40
Clients not willing to go for referral services 3 2.70
Limited space thus patient privacy compromised 5 4.50
Culture and client negative attitude towards health care providers 2 1.80
First visit made late leading to fewer visits in total and some clients don’t come for
revisits
16 14.50
A lot of time is spent in the lab during the first visit leading to no counselling done
during this visit
2 1.80
Poor accessibility of the facility due to bad roads or uphill terrain especially during the
rains.
4 3.60
No challenge 7 6.40
#: Total is not exclusive (more than one response was obtained
Table (VIII) shows the number and percent distribution of study participants according to other activities they
perform alongside antenatal care services. It was observed that more than two thirds of the study participants (67.30%)
offered child welfare clinic services alongside antenatal care while 57.30% offered family planning services. Moreover,
almost two fifths of the study participant (39.10%) gave clinical care to sick patients by clerking and prescribing treatment
for them, 20% gave comprehensive care to HIV positive clients and care for HIV exposed infants while 6.40% carried out
post-natal clinics and conducting deliveries too, only one participant reported performing cervical cancer screening. Finally,
15.40% of them gave antenatal care only.
Table (VIII): Number and percent distribution of the study participants according to other activities they perform
alongside antenatal care services.
Activity # No.
(n = 110)
Percent (%)
Child welfare clinic 74 67.30
Family planning services 63 57.30
Post-natal clinic and delivery 7 6.40
Comprehensive HIV care and care of HIV exposed infants (HEI) 22 20.00
Cervical cancer screening 1 0.90
Clinical services (patient clerking and treatment) 43 39.10
None 17 15.40
# Total is not exclusive (more than one response was obtained
Table (IX) represents the relationship between the nurses’ demographic characteristics and their total score in
compliance with focused antenatal care. It was observed that none of the socio-demographic characteristics had any
statistical significance on the total score of compliance among the nurses who were observed. However, older nurses were
more compliant than the younger ones whereby nurses in their forties and fifties (33% and 27.30%) respectively had better
compliance than the younger age groups. Furthermore, gender had no statistical significance with the total score in
compliance, however, looking at the percentages, the female appear to have better compliance (30.70%) than the male
(14.30%) though no statistical correlation was found. Equally marital status as well as level of education bore no statistical
correlation with compliance score.

Nurses Compliance With Focused Antenatal Care In Siaya..
DOI: 10.9790/1959-0702080118 www.iosrjournals.org 12 | Page
Table (IX): Relationship between the nurses’ socio-demographic characteristics and their total score of compliance
with focused antenatal care.
Socio-demographic
characteristics
Study participants
(n=110)
Total
Significance
Total score of compliance
Fair Good
No % No % No %
Age (years):
20 -30 >31-40
>40 -50
> 50
35 31
8
8
76.10 75.60
66.70
72.70
11 10
4
3
23.90 24.40
33.30
27.30
46 41
12
11
41.82 37.27
10.91
10.00
X2 =0.741 P =0.902
Gender:
Female
Male
52
30
69.30
85.70
23
5
30.70
14.30
75
35
68.18
31.82
X2 = 3.375
P = 0.066
Marital status:
- Married
- Single
60
22
70.60
88.00
25
3
29.40
12.00
85
25
77.27
22.73
X2 = 3.086
P = 0.079
Level of Education:
- Certificate
- Diploma
- Degree (BSN)
12
64
6
75.00
72.70
100.00
4
24
0
25.00
27.30
0.00
16
88
6
14.55
80.00
5.45
X2 = 1.789 FEP = 0.485
X2: Chi-square testFEP: Fisher’s Exact test No Significance at P > 0.05
According to table (X), nurses’ total score of compliance had statistical association with their working experience
in years and duration in the current unit where P = 0.048 and 0.015 respectively. That is to say, nurses with more years of
experience had good compliance (50 %) compared to those who had less years of experience (23.30%). Moreover, those
who had stayed in the clinic for more years also had better scores of compliance (100%) compared to those who had been in
their clinics for shorter duration in years (24.30%).
Regarding previous training in antenatal care and level of facility the nurse worked in, no statistical correlation of total score
of compliance was observed as P= (0.571 and 0.067) respectively.
Table (X): Relationship between the nurses’ working experience and their total score of compliance with FANC.
Working experience
Study participants
(n=110)
Total
Significance
Level of compliance
Fair
(n = 110)
Good
(n = 110)
No % No % No %
Duration of experience in years:
1-10 >10 -20
>20-30
> 30
56 15
7
2
76.70 68.20
63.60
50.00
17 7
4
2
23.30 31.80
36.40
50.00
73 22
11
4
66.36 20.00
10.00
3.64
X2= 2.411 P = 0.048*
Duration in the current unit in
years
1-10 >10 -20
>20 -30
81 1
0
75.70 50.00
0.00
26 1
1
24.30 50.00
100.00
107 2
1
97.30 1.80
0.90
X2 = 3.675 P = 0 .015*
Previous training in ANC
Yes
No
60
22
73.20
78.60
22
6
26.80
21.40
82
28
74.50
25.50
X2 = 0.321
P = 0.571
Level of Health facility of work
County Referral Hospital
Sub-County Hospital
Health centre Dispensary
2
15
27 38
66.70
75.00
62.80 86.40
1
5
16 6
33.30
25.00
37.20 13.60
3
20
43 44
2.70
18.20
39.10 40.00
X2 = 6.809
P = 0.067
X2: Chi-square test*: Significant at P ≤ 0.05
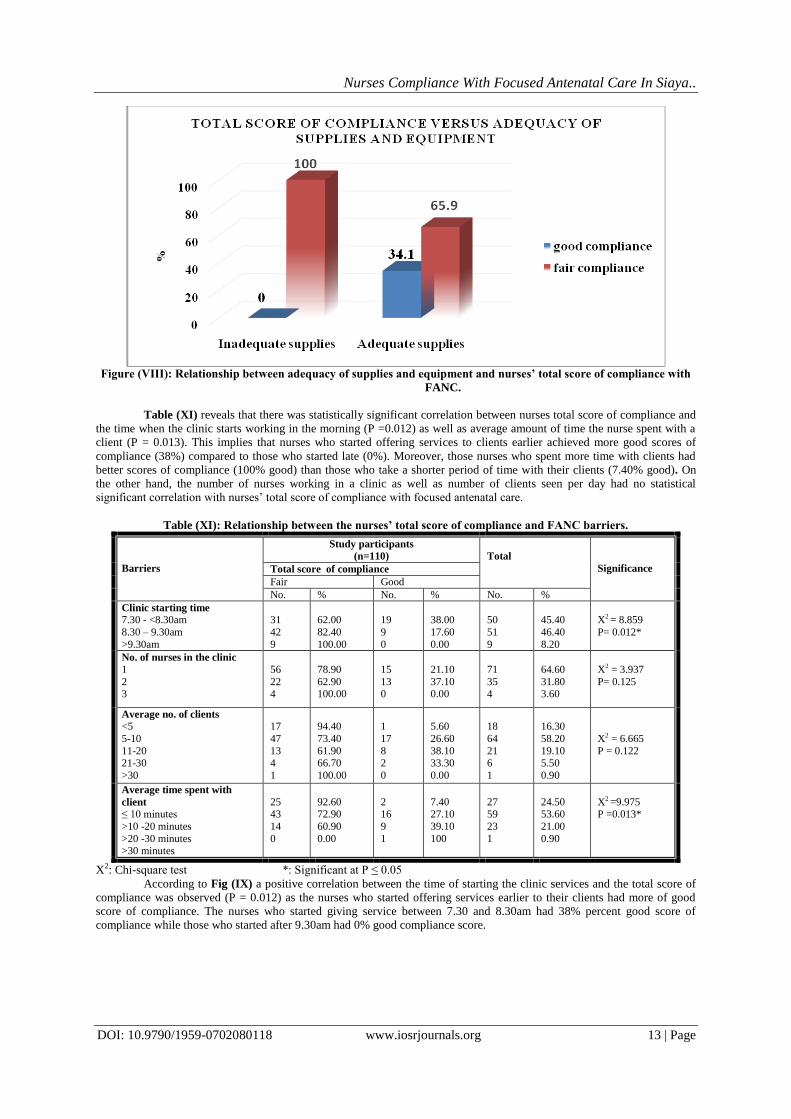
Figure (VIII) shows that there was a statistically significant correlation between adequacy of supplies and nurses total score
of compliance. The nurses who had adequate supplies achieved 34.10% good compliance while those who had inadequate
supplies achieved 0% good compliance with focused antenatal care, whereby P = 0.000
Nurses Compliance With Focused Antenatal Care In Siaya..
DOI: 10.9790/1959-0702080118 www.iosrjournals.org 13 | Page
Figure (VIII): Relationship between adequacy of supplies and equipment and nurses’ total score of compliance with
FANC.
Table (XI) reveals that there was statistically significant correlation between nurses total score of compliance and
the time when the clinic starts working in the morning (P =0.012) as well as average amount of time the nurse spent with a
client (P = 0.013). This implies that nurses who started offering services to clients earlier achieved more good scores of
compliance (38%) compared to those who started late (0%). Moreover, those nurses who spent more time with clients had
better scores of compliance (100% good) than those who take a shorter period of time with their clients (7.40% good). On
the other hand, the number of nurses working in a clinic as well as number of clients seen per day had no statistical
significant correlation with nurses’ total score of compliance with focused antenatal care.
Table (XI): Relationship between the nurses’ total score of compliance and FANC barriers.
Barriers
Study participants
(n=110)
Total
Significance Total score of compliance
Fair Good
No. % No. % No. %
Clinic starting time
7.30 - <8.30am
8.30 – 9.30am
>9.30am
31
42
9
62.00
82.40
100.00
19
9
0
38.00
17.60
0.00
50
51
9
45.40
46.40
8.20
X2 = 8.859
P= 0.012*
No. of nurses in the clinic
1
2 3
56
22 4
78.90
62.90 100.00
15
13 0
21.10
37.10 0.00
71
35 4
64.60
31.80 3.60
X2 = 3.937
P= 0.125
Average no. of clients
<5
5-10
11-20 21-30
>30
17
47
13 4
1
94.40
73.40
61.90 66.70
100.00
1
17
8 2
0
5.60
26.60
38.10 33.30
0.00
18
64
21 6
1
16.30
58.20
19.10 5.50
0.90
X2 = 6.665
P = 0.122
Average time spent with
client
≤ 10 minutes
>10 -20 minutes
>20 -30 minutes >30 minutes
25 43
14
0
92.60 72.90
60.90
0.00
2 16
9
1
7.40 27.10
39.10
100
27 59
23
1
24.50 53.60
21.00
0.90
X2 =9.975 P =0.013*
X2: Chi-square test *: Significant at P ≤ 0.05
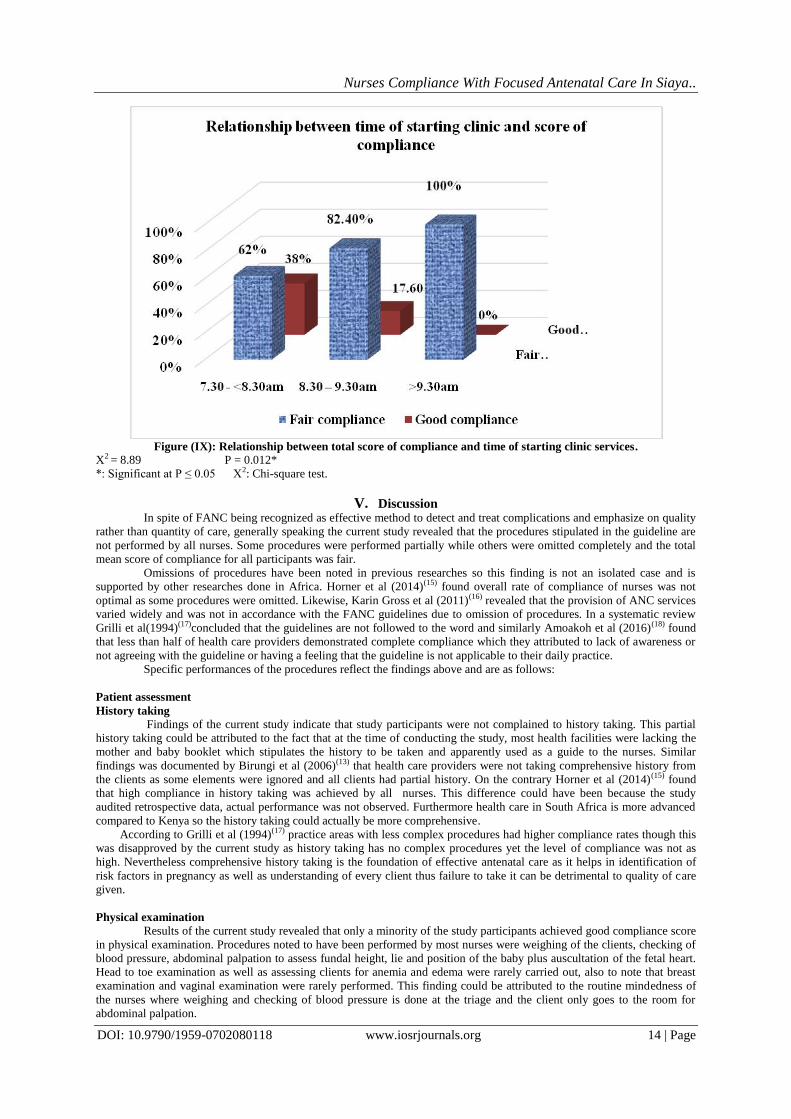
According to Fig (IX) a positive correlation between the time of starting the clinic services and the total score of
compliance was observed (P = 0.012) as the nurses who started offering services earlier to their clients had more of good
score of compliance. The nurses who started giving service between 7.30 and 8.30am had 38% percent good score of
compliance while those who started after 9.30am had 0% good compliance score.
Nurses Compliance With Focused Antenatal Care In Siaya..
DOI: 10.9790/1959-0702080118 www.iosrjournals.org 14 | Page
Figure (IX): Relationship between total score of compliance and time of starting clinic services.
X2 = 8.89 P = 0.012*
*: Significant at P ≤ 0.05 X2: Chi-square test.
V. Discussion In spite of FANC being recognized as effective method to detect and treat complications and emphasize on quality
rather than quantity of care, generally speaking the current study revealed that the procedures stipulated in the guideline are
not performed by all nurses. Some procedures were performed partially while others were omitted completely and the total
mean score of compliance for all participants was fair.
Omissions of procedures have been noted in previous researches so this finding is not an isolated case and is
supported by other researches done in Africa. Horner et al (2014)(15) found overall rate of compliance of nurses was not
optimal as some procedures were omitted. Likewise, Karin Gross et al (2011)(16) revealed that the provision of ANC services
varied widely and was not in accordance with the FANC guidelines due to omission of procedures. In a systematic review
Grilli et al(1994)(17)concluded that the guidelines are not followed to the word and similarly Amoakoh et al (2016)(18) found
that less than half of health care providers demonstrated complete compliance which they attributed to lack of awareness or
not agreeing with the guideline or having a feeling that the guideline is not applicable to their daily practice.
Specific performances of the procedures reflect the findings above and are as follows:
Patient assessment
History taking
Findings of the current study indicate that study participants were not complained to history taking. This partial
history taking could be attributed to the fact that at the time of conducting the study, most health facilities were lacking the
mother and baby booklet which stipulates the history to be taken and apparently used as a guide to the nurses. Similar
findings was documented by Birungi et al (2006)(13) that health care providers were not taking comprehensive history from
the clients as some elements were ignored and all clients had partial history. On the contrary Horner et al (2014)(15) found
that high compliance in history taking was achieved by all nurses. This difference could have been because the study
audited retrospective data, actual performance was not observed. Furthermore health care in South Africa is more advanced
compared to Kenya so the history taking could actually be more comprehensive.
According to Grilli et al (1994)(17) practice areas with less complex procedures had higher compliance rates though this
was disapproved by the current study as history taking has no complex procedures yet the level of compliance was not as
high. Nevertheless comprehensive history taking is the foundation of effective antenatal care as it helps in identification of
risk factors in pregnancy as well as understanding of every client thus failure to take it can be detrimental to quality of care
given.
Physical examination
Results of the current study revealed that only a minority of the study participants achieved good compliance score
in physical examination. Procedures noted to have been performed by most nurses were weighing of the clients, checking of
blood pressure, abdominal palpation to assess fundal height, lie and position of the baby plus auscultation of the fetal heart.
Head to toe examination as well as assessing clients for anemia and edema were rarely carried out, also to note that breast
examination and vaginal examination were rarely performed. This finding could be attributed to the routine mindedness of
the nurses where weighing and checking of blood pressure is done at the triage and the client only goes to the room for
abdominal palpation.

Nurses Compliance With Focused Antenatal Care In Siaya..
DOI: 10.9790/1959-0702080118 www.iosrjournals.org 15 | Page
These findings are in agreement with other previous researches done which include Ouma et al (2010)(19)where the
data before and after the training nurses on FANC agreed that majority of the health care providers palpated the clients
abdomen and listened to the fetal heart. Moreover Mekonnenet al (2017)(20)found that weighing, blood pressure
measurement, abdominal palpation and auscultation for fetal heart was done regularly and the same findings were echoed by
Horner et al (2014)(15). Conrad et al (2012)(21) also reported that the only procedures performed by all health care workers
were abdominal palpation and fetal heart auscultation.
On the contrary Coleman et al (2016)(18) had abdominal palpation and auscultation as the least performed
procedure by the nurses in Ghana. The difference can be attributed to the fact that the above study looked at performance
during first antenatal clinic visit only and if this is done in first trimester as required by the guideline then the abdomen may
have no palpable mass and fetal heart sounds cannot be heard on auscultation. Similarly Sarker et al (2010)(22)reported that
blood pressure was not taken for most clients because there was no working blood pressure machine. This finding as
explained just points out to lack of compliance due to unavailability of equipment. A rise in blood pressure is a sign that can
precede cases of pre-eclampsia thus if noted early can be treated to improve on the pregnancy outcome thus blood pressure
measurement is considered as one of the best practices in antenatal care.
Participants who attempted to perform head to toe examination on their clients did not examine the client
completely and a very small minority performed a complete head to toe exam, this however did not include listening to heart
and lung sounds, this is because most nurses observed were diploma holders and at their level they are not trained to
auscultate the chest. Assessment for anemia and edema was done by almost half of the participants, however breast
examination was attempted by a very small fraction of nurses and some male nurses expressed that some women would not
allow them to examine their breasts. Lodge N et al (1997)(23)had made the same observation where majority of gynecology
patients expressed feelings of embarrassment while being given intimate care involving exposure of the private parts by a
male nurse. Moreover, vaginal examination was not performed by almost all of the study participants but this could be
attributed to the fact that most clients seen were in second trimester.
Laboratory investigations (antenatal profile)
Concerning laboratory investigations, results of the current study revealed that there was good compliance in
ensuring that clients had the investigations done especially those carried out by the nurses which are HIV screening and
malaria screening in some clinics. This is attributed to the fact that HIV/Aids services in the county is largely supported by
donor partners who ensure that the testing kits and antiretroviral drugs are available to promote adherence and they also go
an extra mile to employ nurses in some facilities to ensure that the care is not compromised. In addition, screening and
prevention of malaria is also donor funded and these partners have made sure that rapid diagnostic tests are available in most
health facilities making it easy for the nurses to test the patient for malaria parasites where laboratory services are not
available for a blood slide for malaria parasites to be done.
The other tests that required clients to be sent to the lab had lower percentages in performance as some clinics lacked labs or
lab technologist or even the reagents. Hemoglobin estimation, blood grouping and Rhesus typing, VDRL and urine analysis
and microscopy were done in facilities of more than two thirds of the study participants.
The current study findings are contrary to an earlier research done in Kenya by Van Eijk et al (2006)(24)which
indicated performance of laboratory tests was very low and the only tests offered were hemoglobin testing, syphilis and
urine analysis. The difference could be attributed to lack of laboratory supplies during that study which apparently had
improved and all antenatal mothers were being tested for HIV while the other tests were also performed when supplies are
available. Secondly Gross Schelenberg et al (2011)(16)reported that most health facilities did not check clients hemoglobin
levels since they did not have an HB machine, clients were told to come at a later date for screening for syphilis while HIV
screening was not done at all. Additionally, Villar et al (2007)(25)points out that routine hemoglobin checking is best done
after 30 weeks gestation though Iron and folic acid should be supplemented throughout pregnancy to ensure no woman goes
into labor with a low hemoglobin level.
Prophylaxis
The findings of the current study demonstrate that this was the best performed activity since averagely all nurses
had good compliance. This was a great improvement compared to a previous finding by Pell, Menacaet al (2013)(26) in
Kenya, Ghana and Malawi where inconsistency in provision of prophylaxis was reported due to unavailability of the
necessary drugs or inability of the women to pay for the services. The improvement can be attributed to free antenatal and
delivery services as well as donor support in some facilities.
Malaria prophylaxis in the current study was actually being given under direct observation treatment (DOTS)
whereby the client swallows the drug in the health facility under the observation of the nurse to ensure it is actually taken in
almost all the facilities. Compliance in malaria prophylaxis is in line with Abuja declaration 2000 which had set a target of
above 60% coverage of pregnant women with IPT and ITNs by 2005 and beyond(27). Insecticide treated bed nets were given
by a vast majority of the study participants and equally, iron and folic acid supplementation as well as deworming tablets
were issued by majority of the study participants. Moreover antiretroviral drugs were available in all the clinics and all study
participants were able to give those who were HIV positive. HIV care was observed to be well complied with courtesy of
development partners.
Health teaching
An alarming finding of the current study is that health education was not given or partially given to clients by a
vast majority of the study participants. Furthermore in some clinics student nurses gave group teaching to the clients without
supervision before start of clinic while in others the nurses reported that health education is given to the clients by
community health volunteers when they visit them in their homes.

Nurses Compliance With Focused Antenatal Care In Siaya..
DOI: 10.9790/1959-0702080118 www.iosrjournals.org 16 | Page
Provision of information on danger signs should be mandatory at every antenatal clinic visit because complications
like hemorrhage and puerperal sepsis cannot be predicted through antenatal screening. Women should be made aware of the
symptoms and advised on what to do in case of such occurrences(28). However, the current study reveals that just above one
tenth of the study participants had good compliance on education about danger signs in pregnancy.
Several previous studies have come up with similar findings that indicate that health teaching during antenatal
clinics is not adequate. These include Kearns Annie et al (2014)(29). On the same line Conrad et al (2012)(21) observed that
very few health workers talked to the clients about danger signs in pregnancy and likewise Sarker et al (2010)(22) concluded
that linking danger signs to clinical examination and laboratory results with effective client follow-up is crucial for success
of antenatal care services.
Birth preparedness was not covered by more than half of the study participants. The same findings have been
documented in other researches where health education was noted as a major gap existing between actual performance and
ideal performance in FANC by Von Both(2006)(30), Omari(2016)(31) and Mutiso (2008)(32).
Given that development of an individual birth plan and birth preparedness are major components of focused
antenatal care, this gap is likely to be the explanation behind suboptimal achievement of aims of antenatal care as has been
indicated in other researches in the past that health education is ignored in most antenatal care clinics. This observation was
made in the same regard of inadequate health teaching given to clients by Nikiema et al 2009(35) to emphasize on unmet
needs in provision of information in pregnancy in Sub Saharan Africa and she reported that pregnant women are not
routinely given information especially on danger signs of pregnancy, likewise Harriet Birungi et al (2006)(13)shared the
same sentiments.
Regarding health teaching on nutrition and infant feeding, the current study revealed that majority of the study
participants did not give nutritional advice to the clients nor tell them about infant feeding, a finding supported by
Mekonnenet al (2017)(20)who stated that nutritional advice was rarely given to women. Likewise, prevention of mother to
child transmission of HIV was talked about by minority of the study participants despite the high prevalence of HIV in the
county. Moreover, information on sexually transmitted infections as well as health teaching on family planning was given by
a very small percentage of the study participants.
Current study findings reveal that nurses are not utilizing information, education and counseling (IEC) which is an
important component of focused antenatal care(33). This coupled with the fact that feedback from the client at the end of the
session to confirm understanding of the content was rarely elicited, raises the question as to whether health teaching during
the antenatal clinics has been given the importance it deserves by the nurses.
Most of the health information required during antenatal clinic visits is outlined in the mother and baby booklet so
some study participants were observed telling the clients that the book had so much information and they should read it at
their own time. The finding is consistent with Schellenberg et al (2011)(16) who noted that the nurses relied much on what
was indicated in the antenatal cards or books for service provision other than FANC guidelines. On the other hand Magoma
et al (2010)(34) attributed low skilled birth attendance despite high antenatal clinic attendance to lack of health education
especially on birth preparedness during antenatal clinic which includes information on hospital delivery. To stress on this as
unmet educational need, Nikiema et al (2009)(35) reiterated that receiving information on birth preparedness and danger signs
in pregnancy increases the chances of having skilled attendant at birth as well as chances of making the minimum four visits
required by focused antenatal care. Moreover this represents a missed opportunity and is basically a result of little time spent
with the clients during a session as the health care provider rush to clear the queue.
Determinants of nurses’ compliance with focused antenatal care
The current study revealed that compliance of nurses with focused antenatal care had statistically significant
relationship with their working experience in years, how long they had worked in their current unit, availability of supplies,
time of starting to offer services at the clinic and the amount of time the nurse spent with their client. However, there was no
statistical significance with their age, marital status, gender, level of education, previous training in antenatal care or the
level of facility they worked in whether it is a dispensary, health centre, sub county or county hospital. Moreover no
statistical significance was shown in compliance with number of nurses working in the clinic, number of clients seen per
day, challenges met during service provision and other activities or services the nurse gave alongside antenatal care.
The current study revealed that nurses with more years of experience demonstrated better compliance than the ones
who had worked for fewer years as evidenced by more of them having good compliance scores. This finding contradict
Choudhry et al (2005)(36) where health care providers who had been in practice for more years were less likely to give good
quality of care as they had less factual knowledge and less likely to comply with standards. On the same line of argument
was Cabana et al (1999)(11)who stated that familiarity and inability to overcome inertia of previous practice made it difficult
for staff who had worked in an area for long to comply with new guidelines. This deference could be attributed to the fact
that procedures in the focused antenatal care guideline do not involve application of new knowledge so old knowledge was
still valuable.
Infrastructure assessment revealed that some nurses had adequate supplies and equipment while others had
inadequate supplies and equipment necessary for implementation of focused antenatal care. A highly positive statistical
significance was found between availability of supplies and level of compliance with FANC whereby nurses who worked in
better equipped facilities or those that had adequate supplies and equipment had better compliance than those whose
facilities had inadequate supplies. This finding is supported by Wang W. et al (2017)(37)who indicated that available supplies
used in service provision improved performance while lack of supplies compromised quality of care. Secondly, Sarker et al
(2010)(22) attributed selective performance of procedures and lack of compliance to lack of supplies seen in infrastructure
assessment. Similarly this view is supported by a systematic review by Simkhanda et al (2008)(38) where availability of
supplies had a positive correlation with quality of care. Still on the same line Scribano et al (2011)(39) stated that better
compliance was achieved when the equipment to be used was available and in good working order.
Nurses Compliance With Focused Antenatal Care In Siaya..
DOI: 10.9790/1959-0702080118 www.iosrjournals.org 17 | Page
The current study further revealed that time of starting clinic services had significance in compliance. This
confirms lack of punctuality as a possible barrier to compliance with focused antenatal care. The average amount of time
spent with the client also had a positive correlation with compliance as nurses who spent more time with clients had better
compliance than those who spent a very short time with clients. This finding echoes the outcome of a simulation study
carried out in Tanzania which estimated time for each client to be 40 minutes for first visit and about twenty minutes for
revisits in order to give quality care in focused antenatal care(30). Similarly Anya et al (2008)(33) had corresponding findings
where they found that time spent with the client was a barrier to effective health teaching as most health workers spent about
three minutes with their clients and poor performance was the outcome.
Level of education and previous training however had no significance in nurses’ compliance with focused antenatal
care guideline in the current study which is contrary to the findings of Shih et al (2011)(40)where nurses with higher
education and specialization conformed to guidelines more than those with lower qualifications. This difference could be
attributed to the fact that at higher levels of nursing education in Kenya the nurses are not exposed to so much practical skills
that is different from what the junior level nurses are exposed to unless they are specializing, thus their performance despite
higher papers is not different from the ones with lower qualification. A different scenario is seen in the developed countries
where the educational level could be equal to the skill acquired. Similarly further training in a particular field had also been
observed by Burua et al (2014)(41)to improve compliance but the current study disapproves this by giving no relationship
between previous training in antenatal care and compliance to the guideline. This difference could be attributed to the
duration of these causes which is more of a five day seminar in a hotel which the nurses may take as a break from the routine
and relax without learning much.
Burua et al (2014)(41)further observed that nurses who worked in lower health facilities were more likely to follow
guidelines, a finding which contradicts the current study findings as the compliance scores did not have any difference at
different levels of health facilities. This could be attributed to the uniformity in the characteristics of nurses working in these
facilities.
The current study also revealed that the number of nurses working in a clinic, number of clients seen per day,
challenges met during service provision and other activities performed by the nurse had no significant correlation with their
compliance. As much as these are critical areas that in normal circumstances would be expected to affect the nurses’ work, it
could not come out clearly due to the nature of observation that was carried out. Individual nurse patient interaction for every
antenatal client regardless of other activities going on was carried out. How much the nurse was able to perform on a
particular client as far as FANC guideline is concerned was noted. This could be seen as a limitation to the findings of the
current study since the same nurse involved in offering other services including curative services and child welfare clinic
cannot have sufficient time for the antenatal client.
From the findings of the current study, it is evident that among all procedures stipulated in FANC guideline, health
education is given the least consideration and this has a serious implication on the quality of antenatal care offered to
mothers. Provision of information on danger signs should be made mandatory at every antenatal visit as this empowers the
women to be able to make good decision in case of any problem. Furthermore a woman with knowledge is an asset to any
community as far as decision making is concerned. So there is need for antenatal care nurses to prioritize the need for health
teaching during clinic visits.
VI. Conclusion Based on the findings of the present study it can be concluded that most of the study participants were not
compliant FANC. The nurses failed to perform many crucial procedures which could have serious implication on women’s’
health and may directly influence maternal and neonatal mortality. This situation can be improved by ensuring availability of
adequate supplies and equipment plus ensuring that the nurses have adequate time for every client.
VII. Recommendations Based on the findings of the current study, the following recommendations are suggested:
There is need to revisit the core procedures outlined in the FANC guideline and determine the necessity thus the limited
time available be used for the procedures found to be beneficial during the specific visit especially health teaching.
Periodic audits should be organized in the facilities to monitor the provision of antenatal care if it is in line with FANC
especially following trainings as this study was done just after AMREF had concluded a training in the county on
FANC yet the results are not impressive.
Include FANC guideline in the continuous professional development (CPD) programs so that the nurses get regular
updates.
Conduct a similar study in other counties on a larger scale in order to be able to generalize the findings.
Qualitative studies should be conducted to identify the real reasons behind low levels of compliance.
References [1]. Every Woman Every Child. Saving lives, protecting futures: progress report on the global strategy for women's and children's health. New
York: United Nations, 2015.
[2]. Hogan,M C., Foreman, K J., Naghavi, M. Ahn S et al. Maternal mortality for 181 countries,1980-2008. A systematic analysis of progress
towards Millenium Development goal 5. Lancet. 375(9726):1609–23.
[3]. WHO. Maternal mortality fact sheet [Internet]. World Health Organization; 2016. Available from:
www.who.int/mediacentre/factsheet/fs348/en/
[4]. UNICEF. UNICEF Annual Report 2015. 2015;(February):1–71. Available from: http://unicef.us2.list-
manage.com/track/click?u=868bc193d9fcfe837d3fb7bc3&id=2253469023&e=1d4dc2ba38 [5]. UNFPA. UNFPA Kenya | Counties with the Highest Burden of Maternal Mortality [Internet]. UNFPA Kenya News: Dispatch. 2014.
Available from: http://kenya.unfpa.org/news/counties-highest-burden-maternal-mortality
Nurses Compliance With Focused Antenatal Care In Siaya..
DOI: 10.9790/1959-0702080118 www.iosrjournals.org 18 | Page
[6]. Owino J, Legault PF, Mumbo HM, Odera O, Ayugi ME. a Grounded Theory Study for Antenatal Care in Kenya. Eur Sci J. 2013;9(23):229–
38.
[7]. Starrs A [editor]. The safe motherhood action agenda : priorities for the next decade. 1997;1–107. Available from:
http://documents.worldbank.org/curated/en/1997/10/442078/safe-motherhood-action-agenda-priorities-next-decade
[8]. Villar J, Carroli G, Khan‐Neelofur D, Piaggio GGP, Gülmezoglu AM. Patterns of routine antenatal care for low‐risk pregnancy. Cochrane Libr [Internet]. 2001; Available from: http:https://doi.org/10.1002/14651858.CD000934
[9]. Lalonde A. Global Strategy for Women’s and Children’s Health. Vol. 32, Journal of obstetrics and gynaecology Canada : JOGC = Journal
d’obstétrique et gynécologie du Canada : JOGC. 2010. 1130-1131 p.
[10]. Chama-Chiliba CM, Koch SF. Utilization of FANCin Zambia: Examining individual- and community-level factors using a multilevel
analysis. Health Policy Plan. 2015; [11]. Cabana, MD., Rand, CS., Powe, NR., Wu A. Why dont physicians follow clinical practice guidelines? A framework for improvement.
JAMA. 1999;282(5):1458–65.
[12]. Lincetto O, Mothebesoane-anoh S, Gomez P, Munjanja S. Antenatal Care: Opprotunities for Africa’s Newborns. Int J Sci Technol Res.
2013;2(2):51–62.
[13]. Harriet Birungi & W. Onyango. Acceptability and Sustainability of the WHO FANCpackage in Kenya. Popul Counc Front Reprod Heal.
2006;(June):17.
[14]. Republic of kenya mimistry of health. Mother and child health booklet. Revised ed. MOH216; 2013.
[15]. HornerVV, Mashamba TJ, Mbananga N, Olorunju S, Ramahlo T, H K, et al. Audit of antenatal care at a community health centre in Tshwane North subdistrict, Gauteng province. South African Family Practice J 2014;56(2):153–8.
[16]. Gross Schellenberg, Joanna Armstrong., Kessy, Flora., Pfeiffer, Constanze., Obrist, Brigit. K, Gross K, Schellenberg JA, Kessy F, Pfeiffer
C, Obrist B. Antenatal care in practice: an exploratory study in antenatal care clinics in the Kilombero Valley, south-eastern Tanzania. BMC
Pregnancy Childbirth 2011 May;11(1):36.
[17]. Grilli, R., Lomas J. Evaluating the message: The relationship between compliance rate and the subject of a practice guideline. Medical Care
1994;32(3):202–13.
[18]. Amoakoh-Coleman M, Agyepong IA, Zuithoff NPA, Kayode GA, Grobbee DE, Klipstein-Grobusch K, et al. Client factors affect provider
adherence to clinical guidelines during first antenatal care. PLoS One. 2016;11(6):1–13. [19]. Ouma PO, Van Eijk a M, Hamel MJ, Sikuku ES, Odhiambo FO, Munguti KM, et al. Antenatal and delivery care in rural western Kenya:
The effect of training health care workers to provide “focused antenatal care.” Reprod Health. 2010;7(1):1–9.
[20]. Mekonnen, N., Berheto, TM,. Ololo, S., Tafese F. Quality of antenatal care services in Demba Gofa Woreda, Gamo Gofa zone, Rural
Ethiopia. Heal Sci J. 2017;11(3).
[21]. Conrad P, Schmid G, Tientrebeogo J, Moses A, Kirenga S, Neuhann F, et al. Compliance with focused antenatal care services: Do health
workers in rural Burkina Faso, Uganda and Tanzania perform all ANC procedures? Trop Med Int Heal. 2012;17(3):300–7.
[22]. Sarker M, Schmid G, Larsson E, Kirenga S, De Allegri M, Neuhann F, et al. Quality of antenatal care in rural southern Tanzania: a reality check. BMC Research Notes 2010;3.
[23]. Lodge N, Mallett J, Blake P, MSc IF. A study to ascertain gynaecological patients’ perceived levels of embarrassment with physical and
psychological care given by female and male nurses. Journal of Advanced Nursing 1997;25(5):893–907.
[24]. Van Eijk AM, Bles HM, Odhiambo F, Ayisi JG, Blokland IE, Rosen DH, et al. Use of antenatal services and delivery care among women in
rural western Kenya: a community based survey. Biomed Cent 2006;3:2.
[25]. Villar J, Bergsjo P. Scientific basis for the content of routine antenatal care. I. Philosophy, recent studies, and power to eliminate or alleviate
adverse maternal outcomes. Acta Obstet Gynecol Scand 1997;76.
[26]. Pell C, Meñaca A, Were F, Afrah NA, Chatio S, Manda-Taylor L, et al. Factors Affecting Antenatal Care Attendance: Results from Qualitative Studies in Ghana, Kenya and Malawi. Vol. 8, PLoS ONE. 2013.
[27]. Mubyazi GM, Bygbjerg IC, Magnussen P, Olsen O, Byskov J, Hansen KS, et al. Prospects, achievements, challenges and opportunities for
scaling-up malaria chemoprevention in pregnancy in Tanzania: the perspective of national level officers. Malaria J. 2008;7.
[28]. Pembe AB, Urassa DP, Carlstedt A, Lindmark G, Nystrom L, Darj E. Rural Tanzanian women’s awareness of danger signs of obstetric
complications. BMC Pregnancy Childbirth 2009;9.
[29]. Kearns Annie, Hurst Taylor, Caglia Jacquelyn LA. Focused antenatal care in Tanzania. 2014;(July):1–13.
[30]. Von-Both C, Steffen F, Ahmad M, Mpembeni R, Jahn A, von Both C, et al. How MuchTime do Health Services spend on Antenatal Care?
Implications for the Introduction of the Focused Antenatal Care Model in Tanzania. BMC Pregnancy Childbirth 2006;6(1):22. [31]. Omari PK, Afrane YA, Ouma P. Birth Preparedness and Complication Readiness among Women Attending Antenatal Care Clinic in Health
Facilities within Bureti Sub County of Kericho County ,. 2016;6(4):123–8.
[32]. Mutiso SM, Qureshi Z, Kinuthia J. Birth preparedness among antenatal clients. East Afr Med J. 2008;
[33]. Anya SE, Hydara A, Jaiteh LE. Antenatal care in The Gambia: missed opportunity for information, education and communication. BMC
Pregnancy and Childbirth . 2008;8.
[34]. Magoma M, Requejo J, Campbell OM, Cousens S, Filippi V. High ANC coverage and low skilled attendance in a rural Tanzanian district: a
case for implementing a birth plan intervention. BMC Pregnancy Childbirth. 2010;10. [35]. Nikiema, B. , Beninguisse, g. ,Haggerty J L, Beninguisse G, Haggerty JL. Providing information on pregnancy complications during
antenatal visits: unmet educational needs in sub-saharan Africa. Health Policy Plan journal 2009;24(5):367-75.
[36]. Choudhry NK, Fletcher RH, Soumerai SB. Improving Patient Care Systematic Review : The Relationship between Clinical Experience and
Quality of Health Care. American College of Physicians. 2005.
[37]. Do, M., Wang,W., Hembling,J., Ametepi P. Quality of antenatal care in Kenya and Namibia. Int J Qual Heal care. 2017;29(2):183–93.
[38]. Simkhada B, Van Teijlingen ER, Porter M, Simkhada P. Factors affecting the utilization of antenatal care in developing countries:
Systematic review of the literature. Journal of Advanced Nursing. 2008;61(3):244–60.
[39]. Scribano, PV., Lerer, T., Kennedy, D., Clautia M. Provider adherence to clinical practice guideline for acute asthma in pediatric emergency department. Academy of Emergency Medicine. 2011;8(12):1147–52.
[40]. Shih, TY., Gaydes, CA., Rothman, RE., Hsieh Y. Poor provider adherence to the center for control and prevention treatment guidelines in
US emergency department visits with diagnosis of pelvic inflammatory disease. Sexually Transmitted Diseases J. 2011;38(4):299–305.
[41]. Burua, A., Nuwaha, F., Waiswa P. Adherence to standards of quality HIV/AIDS care and anteretroviral therapy in the West Nile region of
Uganda. BMC Health Service Research. 2014;18(14):521.