Embed Size (px)
Citation preview

An increasing number of pediatric practitioners suggestthat pediatric well-baby care must change from routinephysical examinations and immunizations to include anassessment of the infant’s overall development and theparent–child relationship (Paes, 1991). Yet studies indi-cate that practitioners still spend much of an infant’s ini-tial postnatal visits identifying and exploring the parents’concerns about bodily functions, leaving only a few min-utes for psychosocial inquiries (Paes, 1991). While the lit-erature suggests that physicians have become better atsoliciting mental health concerns with parents of school-age children, little change has been documented in theirresponse to psychosocial difficulties of younger children.
For example, Sharp and colleagues (1992) reported that88% of parents expressed psychosocial concerns duringtheir visit to a pediatrician in training when they weregiven the opportunity to do so. However, 60% of physi-cians did not respond effectively to these concerns, i.e.,ignored them (17%) or explored issues but provided noinformation, guidance, or reassurance (43%). Costelloand colleagues (1988) compared pediatricians’ mentalhealth assessments of 300 primary school–age childrenwith their own, using the Child Behavior Checklist (CBCL)by Achenbach (1991) and the Diagnostic InterviewSchedule for Children (DISC-1). They found that pedia-tricians correctly identified 84% of the healthy childrenbut only 17% of the youngsters with behavioral or emo-tional problems. However, no empirical studies haveexamined how physicians and nurses learn about basicfamily problems of their new infant patients. This isdespite recent data by Lavigne and colleagues (1996), whofound that 8.3% of infants aged 2 years scored above the90th percentile on the CBCL within a large communitysample. Likewise, there is no research examining nurses’assessments and management of psychosocial problems inpediatric settings, although one empirical study of nursecommunication with a general patient population dem-
Nurses’ and Physicians’ Assessment of Mother–InfantMental Health at the First Postnatal Visits
KLAUS MINDE, M.D., LEE TIDMARSH, M.D., AND SUSAN HUGHES, PH.D.
ABSTRACTObjective: To examine the degree to which physicians and nurses use their first postnatal contact with mothers and babies
to learn about their psychosocial strengths and problems. Method: Forty-two consecutively born infants and their mothers
were observed during their initial postnatal visit with a public health nurse and their physician in Montreal. Both visits were
audiotaped.Tapes were analyzed for the number of physical and psychosocial topics discussed during the visits. Observers
also rated the professionals’ communication skills. During a later home visit, mothers were given the Edinburgh Postnatal
Depression Scale, the Symptom Checklist-90-Revised, and the Working Model of the Child Interview (WMCI). Results:Nurses spent more time with families, discussed more psychosocial issues, and were rated to be more sensitive inter-
viewers than physicians. They were also concerned about the psychological well-being and psychological difficulties of
more mothers than were the physicians. In contrast, physicians were more sensitive to pregnancy complications in younger
mothers. Mothers’ satisfaction correlated with the number of psychosocial issues discussed by both professional groups.
WMCI data suggest that recent non-Western immigrants are overrepresented among insecurely attached mothers.
Conclusions: Nurses and physicians obtain different data from the same patients and should increase their collaboration.
J. Am. Acad. Child Adolesc. Psychiatry, 2001, 40(7):803–810. Key Words: infancy, family, assessment, nurses, physicians.
J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 40 :7 , JULY 2001 803
Accepted February 7, 2001.Dr. Minde is Professor of Psychiatry and Pediatrics and Dr. Tidmarsh is
Assistant Professor, Division of Child and Adolescent Psychiatry, Psychiatry Depart-ment, McGill University, Montreal, Quebec. Dr. Hughes is Staff Psychologist atPathways for Children and Youth in Kingston, Ontario.
This study was partially funded by a postdoctoral fellowship from theMontreal Children’s Hospital Research Foundation to Dr. Hughes.
Correspondence to Dr. Minde, Division of Child and Adolescent Psychiatry,Montreal Children’s Hospital, 4018 Ste. Catherine Street West, Montreal, Quebec,Canada H3Z 1P2; e-mail: [email protected].
0890-8567/01/4007–0803�2001 by the American Academy of Childand Adolescent Psychiatry.

onstrated that nurse–patient interactions were generallysupportive, but that nurses did not explore the patients’perceptions of their problems adequately (Gallop et al.,1990). One reason given for the lack of more systematicinquiry into family and infant problems identified earlyon is the assumption that behavior in infancy is not stableand does not reflect future behavioral functioning. Thishas been challenged recently. For example, Mrazek et al.(1999) documented that ratings of problems in parentingstyles in families at risk for asthma observed by trained laypersonnel 3 weeks after the birth of a child, together withinfections and elevated immunoglobulin E level, predictedthe onset of asthma before age 3 with a 70% probability.Laucht and colleagues (1994), in a large epidemiologicalstudy (N = 353), also documented that disturbed mother–infant interaction at 12 weeks was the most importantpredictor of infant behavior problems at age 2 years. Fur-thermore, Mrazek, in a later study of a second cohort of140 “at-risk” newborns, provided family interventions tohalf the sample at age 3 weeks and significantly decreasedthe incidence of asthma in treated children at age 3 years(Mrazek, 2000). This finding suggests that the parentingsystem may be less fixed early in an infant’s life and canpossibly be modified more readily at that time (VanIJzendoorn et al., 1997).
What aspect of an infant’s environment should beassessed at the first postnatal visit with a health profes-sional? Three influences on early behavior and develop-ment emerge as important: (1) parental and childcharacteristics, (2) parenting style, and (3) the larger familyand social context in which parenting occurs. Maternaldepression and anxiety are particularly important parentalcharacteristics to assess, given their frequency and the find-ing that periods of depression may have enduring effectson the socioemotional and cognitive development of thechild (Sameroff, 1993). Eliciting a mother’s perception ofher pregnancy, delivery, and competence in the maternalrole may also yield valuable information for treatment,given the associations of these factors with maternal behav-ioral competence, sensitivity, and type of attachment(Zeanah and Benoit, 1995). Inasmuch as infants areextremely dependent on their immediate environment fortheir growth and development, an assessment shouldinclude the family context. Of specific importance here areineffective parental management and socialization,expressed in harsh, erratic, or abusive disciplining (Minde,1996) and the signs of insecure parental attachment(Greenberg et al., 1993). Finally, it is important to evaluate
social support as well as marital and family distress, whichare strong predictors of postnatal depression, poor mother–child interactions, and later child behavioral and physicalproblems (Minde, 1996).
This study examines how nurses and physicians inter-view a community sample of parents and their newborninfants and to what degree their findings of parent andchild characteristics, parenting style, and the social con-tacts of the family are validated by objective criteria. Wehypothesized that nurses would spend more time withfamilies, evaluate more psychosocial topics, and thereforeidentify more patients at risk for mental health problems.
METHOD
Subjects
The participants of this study were 45 mothers and their newborninfants who came from six community health clinics in Montreal.Each of these clinics serves a specific territory and is staffed by 8 to 10nurses and physicians as well as varying numbers of nonmedicalhealth professionals and provides a wide range of health and social ser-vices to a population of approximately 65,000 people. For example,nurses visit the home of all first-born infants at 1 or 2 weeks unlessmothers specifically refuse. More than 90% of the mothers welcomethe nurse. The 6 clinics were selected from 29 in Montreal to cover awide range of socioeconomic groups.
Nurses at these clinics routinely receive a list from hospitals of new-borns living in their territory. In our case they then phoned the firstmother who had given birth in a given week and asked whether shewould like to be visited by a nurse and participate in a study describ-ing the initial response of a family to a new baby’s entrance into thefamily. To be included, infants had to be full-term (i.e., a minimum of37 weeks’ gestation) and have an Apgar score of at least 6 and 8 at 1and 5 minutes, respectively; a birth weight greater than 2,500 g; andno congenital abnormalities. Parents had to speak either English orFrench and had no prior contact with the physician they had chosento care for their infant.
Of 45 mothers approached, 42 (93.3%) agreed to participate inthe study and comprised our final sample. Of 21 nurses involved inpostnatal visits in the 6 clinics, 18 participated, as well as the 25 pri-vate physicians of the families.
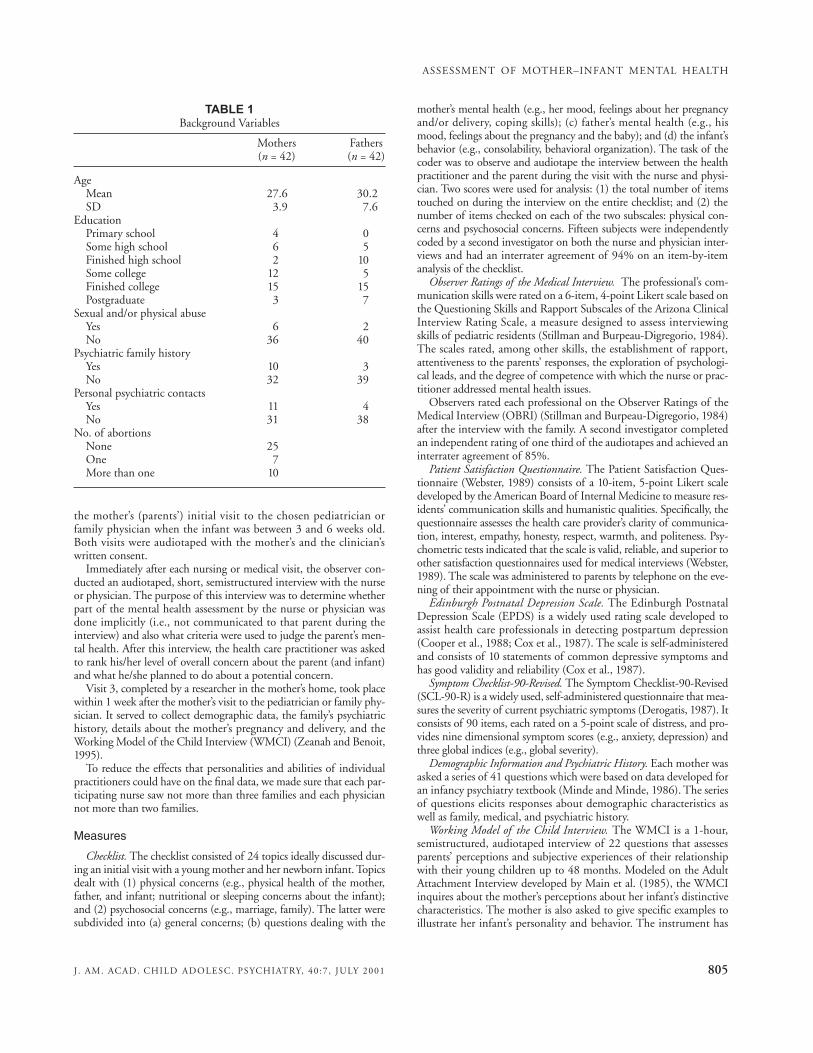
Table 1 provides some of the background data of our sample. Themajority of parents in the study were between 27 and 30 years old andwere married or lived together. They also had a wide range of edu-cational experiences. Furthermore, 40% of the mothers had one ormore previous abortions, 14% had experienced physical and/or sexualabuse, and approximately 25% had a family history of personal psy-chiatric contacts. Fathers reported approximately one third of this rateof personal psychiatric contacts.
In addition, 24 mothers were born in Canada and 18 had immi-grated during the past 10 years. Thirty-five of the children were first-born and seven were second-born infants.
ProcedureData collection involved the audiotaping of three visits per sub-
ject. Visit 1 was the postnatal home visit by the nurse, whichoccurred when the infant was 1 or 2 weeks old. Visit 2 consisted of
MINDE ET AL.
804 J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 40 :7 , JULY 2001
the mother’s (parents’) initial visit to the chosen pediatrician orfamily physician when the infant was between 3 and 6 weeks old.Both visits were audiotaped with the mother’s and the clinician’swritten consent.
Immediately after each nursing or medical visit, the observer con-ducted an audiotaped, short, semistructured interview with the nurseor physician. The purpose of this interview was to determine whetherpart of the mental health assessment by the nurse or physician wasdone implicitly (i.e., not communicated to that parent during theinterview) and also what criteria were used to judge the parent’s men-tal health. After this interview, the health care practitioner was askedto rank his/her level of overall concern about the parent (and infant)and what he/she planned to do about a potential concern.
Visit 3, completed by a researcher in the mother’s home, took placewithin 1 week after the mother’s visit to the pediatrician or family phy-sician. It served to collect demographic data, the family’s psychiatrichistory, details about the mother’s pregnancy and delivery, and theWorking Model of the Child Interview (WMCI) (Zeanah and Benoit,1995).
To reduce the effects that personalities and abilities of individualpractitioners could have on the final data, we made sure that each par-ticipating nurse saw not more than three families and each physiciannot more than two families.
Measures
Checklist. The checklist consisted of 24 topics ideally discussed dur-ing an initial visit with a young mother and her newborn infant. Topicsdealt with (1) physical concerns (e.g., physical health of the mother,father, and infant; nutritional or sleeping concerns about the infant);and (2) psychosocial concerns (e.g., marriage, family). The latter weresubdivided into (a) general concerns; (b) questions dealing with the
mother’s mental health (e.g., her mood, feelings about her pregnancyand/or delivery, coping skills); (c) father’s mental health (e.g., hismood, feelings about the pregnancy and the baby); and (d) the infant’sbehavior (e.g., consolability, behavioral organization). The task of thecoder was to observe and audiotape the interview between the healthpractitioner and the parent during the visit with the nurse and physi-cian. Two scores were used for analysis: (1) the total number of itemstouched on during the interview on the entire checklist; and (2) thenumber of items checked on each of the two subscales: physical con-cerns and psychosocial concerns. Fifteen subjects were independentlycoded by a second investigator on both the nurse and physician inter-views and had an interrater agreement of 94% on an item-by-itemanalysis of the checklist.
Observer Ratings of the Medical Interview. The professional’s com-munication skills were rated on a 6-item, 4-point Likert scale based onthe Questioning Skills and Rapport Subscales of the Arizona ClinicalInterview Rating Scale, a measure designed to assess interviewingskills of pediatric residents (Stillman and Burpeau-Digregorio, 1984).The scales rated, among other skills, the establishment of rapport,attentiveness to the parents’ responses, the exploration of psychologi-cal leads, and the degree of competence with which the nurse or prac-titioner addressed mental health issues.
Observers rated each professional on the Observer Ratings of theMedical Interview (OBRI) (Stillman and Burpeau-Digregorio, 1984)after the interview with the family. A second investigator completedan independent rating of one third of the audiotapes and achieved aninterrater agreement of 85%.
Patient Satisfaction Questionnaire. The Patient Satisfaction Ques-tionnaire (Webster, 1989) consists of a 10-item, 5-point Likert scaledeveloped by the American Board of Internal Medicine to measure res-idents’ communication skills and humanistic qualities. Specifically, thequestionnaire assesses the health care provider’s clarity of communica-tion, interest, empathy, honesty, respect, warmth, and politeness. Psy-chometric tests indicated that the scale is valid, reliable, and superior toother satisfaction questionnaires used for medical interviews (Webster,1989). The scale was administered to parents by telephone on the eve-ning of their appointment with the nurse or physician.
Edinburgh Postnatal Depression Scale. The Edinburgh PostnatalDepression Scale (EPDS) is a widely used rating scale developed toassist health care professionals in detecting postpartum depression(Cooper et al., 1988; Cox et al., 1987). The scale is self-administeredand consists of 10 statements of common depressive symptoms andhas good validity and reliability (Cox et al., 1987).
Symptom Checklist-90-Revised. The Symptom Checklist-90-Revised(SCL-90-R) is a widely used, self-administered questionnaire that mea-sures the severity of current psychiatric symptoms (Derogatis, 1987). Itconsists of 90 items, each rated on a 5-point scale of distress, and pro-vides nine dimensional symptom scores (e.g., anxiety, depression) andthree global indices (e.g., global severity).
Demographic Information and Psychiatric History. Each mother wasasked a series of 41 questions which were based on data developed foran infancy psychiatry textbook (Minde and Minde, 1986). The seriesof questions elicits responses about demographic characteristics aswell as family, medical, and psychiatric history.
Working Model of the Child Interview. The WMCI is a 1-hour,semistructured, audiotaped interview of 22 questions that assessesparents’ perceptions and subjective experiences of their relationshipwith their young children up to 48 months. Modeled on the AdultAttachment Interview developed by Main et al. (1985), the WMCIinquires about the mother’s perceptions about her infant’s distinctivecharacteristics. The mother is also asked to give specific examples toillustrate her infant’s personality and behavior. The instrument has
ASSESSMENT OF MOTHER–INFANT MENTAL HEALTH
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 40 :7 , JULY 2001 805
TABLE 1Background Variables
Mothers Fathers(n = 42) (n = 42)
AgeMean 27.6 30.2SD 3.9 7.6
EducationPrimary school 4 0Some high school 6 5Finished high school 2 10Some college 12 5Finished college 15 15Postgraduate 3 7
Sexual and/or physical abuseYes 6 2No 36 40
Psychiatric family historyYes 10 3No 32 39
Personal psychiatric contactsYes 11 4No 31 38
No. of abortionsNone 25One 7More than one 10
good psychometric properties, and attachment classifications corre-late highly with those obtained with the Ainsworth Strange Situation(Benoit et al., 1997).
RESULTS
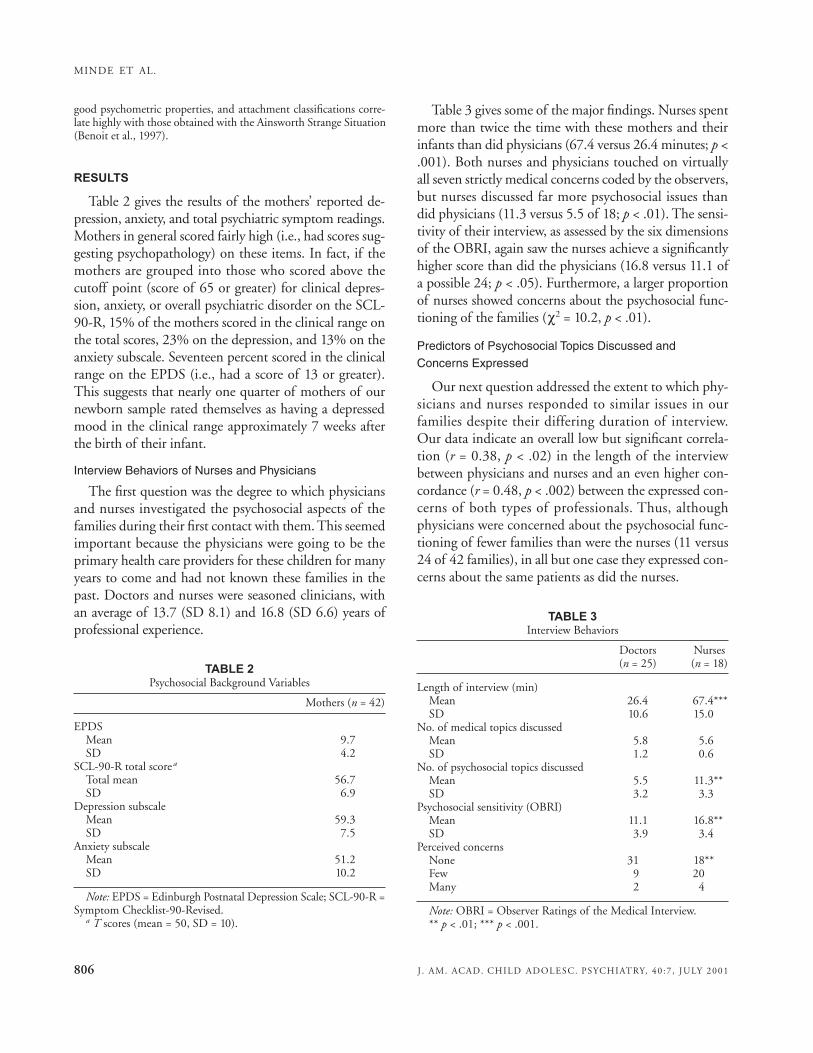
Table 2 gives the results of the mothers’ reported de-pression, anxiety, and total psychiatric symptom readings.Mothers in general scored fairly high (i.e., had scores sug-gesting psychopathology) on these items. In fact, if themothers are grouped into those who scored above thecutoff point (score of 65 or greater) for clinical depres-sion, anxiety, or overall psychiatric disorder on the SCL-90-R, 15% of the mothers scored in the clinical range onthe total scores, 23% on the depression, and 13% on theanxiety subscale. Seventeen percent scored in the clinicalrange on the EPDS (i.e., had a score of 13 or greater).This suggests that nearly one quarter of mothers of ournewborn sample rated themselves as having a depressedmood in the clinical range approximately 7 weeks afterthe birth of their infant.
Interview Behaviors of Nurses and Physicians
The first question was the degree to which physiciansand nurses investigated the psychosocial aspects of thefamilies during their first contact with them. This seemedimportant because the physicians were going to be theprimary health care providers for these children for manyyears to come and had not known these families in thepast. Doctors and nurses were seasoned clinicians, withan average of 13.7 (SD 8.1) and 16.8 (SD 6.6) years ofprofessional experience.
Table 3 gives some of the major findings. Nurses spentmore than twice the time with these mothers and theirinfants than did physicians (67.4 versus 26.4 minutes; p <.001). Both nurses and physicians touched on virtuallyall seven strictly medical concerns coded by the observers,but nurses discussed far more psychosocial issues thandid physicians (11.3 versus 5.5 of 18; p < .01). The sensi-tivity of their interview, as assessed by the six dimensionsof the OBRI, again saw the nurses achieve a significantlyhigher score than did the physicians (16.8 versus 11.1 ofa possible 24; p < .05). Furthermore, a larger proportionof nurses showed concerns about the psychosocial func-tioning of the families (χ2 = 10.2, p < .01).
Predictors of Psychosocial Topics Discussed andConcerns Expressed
Our next question addressed the extent to which phy-sicians and nurses responded to similar issues in ourfamilies despite their differing duration of interview.Our data indicate an overall low but significant correla-tion (r = 0.38, p < .02) in the length of the interviewbetween physicians and nurses and an even higher con-cordance (r = 0.48, p < .002) between the expressed con-cerns of both types of professionals. Thus, althoughphysicians were concerned about the psychosocial func-tioning of fewer families than were the nurses (11 versus24 of 42 families), in all but one case they expressed con-cerns about the same patients as did the nurses.
MINDE ET AL.
806 J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 40 :7 , JULY 2001
TABLE 2Psychosocial Background Variables
Mothers (n = 42)
EPDSMean 9.7SD 4.2
SCL-90-R total scorea
Total mean 56.7SD 6.9
Depression subscaleMean 59.3SD 7.5
Anxiety subscaleMean 51.2SD 10.2
Note: EPDS = Edinburgh Postnatal Depression Scale; SCL-90-R =Symptom Checklist-90-Revised.
a T scores (mean = 50, SD = 10).
TABLE 3Interview Behaviors
Doctors Nurses(n = 25) (n = 18)
Length of interview (min)Mean 26.4 67.4***SD 10.6 15.0
No. of medical topics discussedMean 5.8 5.6SD 1.2 0.6
No. of psychosocial topics discussedMean 5.5 11.3**SD 3.2 3.3
Psychosocial sensitivity (OBRI)Mean 11.1 16.8**SD 3.9 3.4
Perceived concernsNone 31 18**Few 9 20Many 2 4
Note: OBRI = Observer Ratings of the Medical Interview.** p < .01; *** p < .001.
Because these findings do not tell us which aspect of apatient’s behavior or background detail caused each pro-fessional group to express their concern, specific psycho-logical (e.g., depression), psychosocial (e.g., mother’s ageor socioeconomic status [SES]), and medical events weresubjected to a forward stepwise linear regression analysisin which the most highly correlated items were used asfactors.
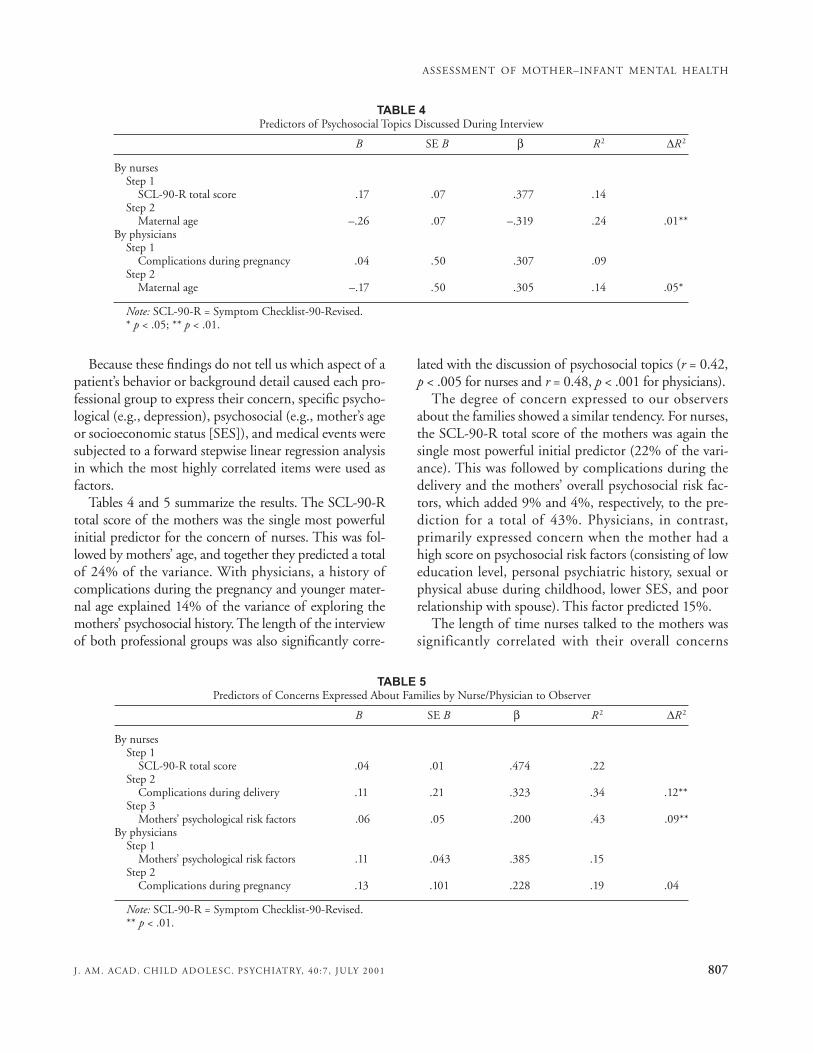
Tables 4 and 5 summarize the results. The SCL-90-Rtotal score of the mothers was the single most powerfulinitial predictor for the concern of nurses. This was fol-lowed by mothers’ age, and together they predicted a totalof 24% of the variance. With physicians, a history ofcomplications during the pregnancy and younger mater-nal age explained 14% of the variance of exploring themothers’ psychosocial history. The length of the interviewof both professional groups was also significantly corre-
lated with the discussion of psychosocial topics (r = 0.42,p < .005 for nurses and r = 0.48, p < .001 for physicians).
The degree of concern expressed to our observersabout the families showed a similar tendency. For nurses,the SCL-90-R total score of the mothers was again thesingle most powerful initial predictor (22% of the vari-ance). This was followed by complications during thedelivery and the mothers’ overall psychosocial risk fac-tors, which added 9% and 4%, respectively, to the pre-diction for a total of 43%. Physicians, in contrast,primarily expressed concern when the mother had ahigh score on psychosocial risk factors (consisting of loweducation level, personal psychiatric history, sexual orphysical abuse during childhood, lower SES, and poorrelationship with spouse). This factor predicted 15%.
The length of time nurses talked to the mothers wassignificantly correlated with their overall concerns
ASSESSMENT OF MOTHER–INFANT MENTAL HEALTH
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 40 :7 , JULY 2001 807
TABLE 4Predictors of Psychosocial Topics Discussed During Interview
B SE B β R 2 ΔR 2
By nursesStep 1
SCL-90-R total score .17 .07 .377 .14Step 2
Maternal age –.26 .07 –.319 .24 .01**By physicians
Step 1Complications during pregnancy .04 .50 .307 .09
Step 2Maternal age –.17 .50 .305 .14 .05*
Note: SCL-90-R = Symptom Checklist-90-Revised.* p < .05; ** p < .01.
TABLE 5Predictors of Concerns Expressed About Families by Nurse/Physician to Observer
B SE B β R 2 ΔR 2
By nursesStep 1
SCL-90-R total score .04 .01 .474 .22Step 2
Complications during delivery .11 .21 .323 .34 .12**Step 3
Mothers’ psychological risk factors .06 .05 .200 .43 .09**By physicians
Step 1Mothers’ psychological risk factors .11 .043 .385 .15
Step 2Complications during pregnancy .13 .101 .228 .19 .04
Note: SCL-90-R = Symptom Checklist-90-Revised.** p < .01.

expressed to us (r = 0.40, p < .001), as was the mothers’SES (r = –0.31, p < .025). Physicians, likewise, spent sig-nificantly more time with mothers about whom theyexpressed concerns (r = 0.27, p < .05). This means thatnurses responded with concern both to the presence ofpsychiatric and psychosocial maternal risk factors as wellas to possible health problems of the baby. In contrast,physicians responded more directly to psychosocial riskfactors in the mothers.
Nevertheless, in no case did a nurse or physician com-municate concerns for a particular family to the otherprofessional, although both groups at times offeredpatients they worried about a subsequent appointment.
Mother Satisfaction With Interviews
Our next question was whether any specific activity orclinical approach by the nurses and physicians was asso-ciated with more or less patient satisfaction. The resultsshow that the mother’s satisfaction with the nurse inter-view was related to the number of psychosocial topicsdiscussed (r 2 = 11%). A lower number of complicationsduring the pregnancy added 8% to the explained vari-ance (p < .05), and the rating on the SCL-90-R depres-sion scale added a further 8%, for a total of r 2 = 25%.
Mothers also judged their interview with their physi-cian as more satisfactory if the doctor touched on morepsychosocial issues. This was more relevant for mothersfrom SES classes IV and V and those who had fewergeneral psychosocial problems.
Moreover, there was a moderate correlation betweenthe way our observers rated the overall quality of thenurses’ or physicians’ interviews and the mothers’ satis-faction (r = 0.27, p < .05 for nurses and r = 0.49, p <.001 for physicians). This suggests that these mothersappreciated being asked about their feelings and con-cerns about themselves and their infants and also tendsto validate the results of our observation procedure.
Attachment Ratings
Finally, we were interested in analyzing our data froman attachment perspective as provided by the WMCI. Wewondered whether the mothers’ score on this interviewwas associated with their relationship with their spouse orparent(s) or with specific psychological abnormalities andthe way they were handled by the nurses and physicians.
The overall results indicate that of 40 mothers whocompleted the WMCI, 24 (60%) showed a balanced(secure) attachment, 4 (10%) were classified as disengaged,
and 12 (30%) were classified as having a distorted attach-ment pattern. There was no relationship between theattachment category of the mothers and their stated rela-tionships with their own mothers and spouses. However,of the 16 insecurely attached mothers, only 3 (19%) versus15 (62%) of secure mothers (χ2 = 7.4; p < .01) reported agood relationship with their father. Insecure mothers alsoscored higher on the depression scale of the SCL-90-R(mean 64.1 versus 57.9; p < .02) and on the EPDS (mean11.5 versus 8.3; p < .02).There were also differences in theconcerns shown by the nurses toward both groups. Nursesshowed no concerns for 15 and mild concerns for 9“secure” mothers. In contrast, they considered only 2 inse-cure mothers to do well and had mild and serious concernsabout 3 and 11 insecurely attached mothers, respectively(χ2 = 14.6; p < .006). Physicians did not show differentialconcerns toward the two groups.
On closer inspection of the “nonbalanced” subgroupof 16 mothers, we found that 8 of them belonged to the9 mothers who had immigrated from Sri Lanka and theCaribbean during the past 5 years, making up 88% ofthis subgroup. This ratio was significantly different fromthe rest of the sample (χ2 = 4.1; p < .05). The same sub-group of mothers also reported a higher rate of compli-cations of their pregnancy (χ2 = 16.2; p < .005) and anonsignificantly lower score on the SCL-90-R anxiety(mean 52.8 versus 58.6), depression (mean 62.5 versus65.9), and total score (mean 59.1 versus 62.8).
DISCUSSION
This study provides us with an interesting cluster offindings. One cluster suggests that nurses and physiciansbehave differently during their initial encounter with thefamily. Nurses talk more about psychosocial issues andseem to show a higher degree of psychosocial sensitivityand skill in their interviewing techniques than do physi-cians, confirming our hypothesis. This difference was notdue to gender differences between the two professionalgroups, inasmuch as 11 (44%) of the 25 physicians werefemale and separate analyses comparing male and femalephysicians showed no differences in their behaviors; it ismore likely a reflection of the different amounts of timenurses and physicians spent with the mothers and theirbabies (26 minutes for physicians, 67 minutes for nurses).This explanation is validated by the more positive obser-ver rating of the nurses on the OBRI. Nevertheless, thisfinding should not obscure some essential differences. All
MINDE ET AL.
808 J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 40 :7 , JULY 2001

nurses spent at least 30 minutes with the patients andhence all had sufficient time to obtain meaningful psycho-social information. Physicians, in contrast, often sched-uled only 15- to 20-minute interviews, which did notallow them to inquire about the family’s psychologicalfunctioning. In fact, a scattergram showed that only thosephysicians who spent more than 20 minutes with theirpatients (approximately 50% of the group) learned aboutany psychological aspects of their families and contrib-uted to the statistical correlation. Another explanation forthe observed difference in the psychosocial sensitivity ofnurses and physicians may be the different settings ofthese interviews: nurses visited the families at their homeswhereas doctors talked to them in their offices.
The question to what extent the study itself may havechanged the professionals’ behavior is relevant here.Both nurses and physicians were told that we were inter-ested in learning what parents with a newborn infantand physicians/nurses talked about during their first pro-fessional meeting. However, we did not specify that wewould compare the mother–nurse and mother–physicianinterviews. Yet all professionals knew that we were mentalhealth specialists and in our private discussions expresseda high level of satisfaction with their sensitivity towardpsychosocial issues in their patients.
The second group of findings deals with the relation-ship between psychosocial concerns discussed and con-cerns expressed to our observers by nurses and physicians.It seems that nurses based their expressed concerns onpsychosocial and historical data that have good face valid-ity. Thus they picked up not only on some of the psycho-logical problems and psychosocial risks (e.g., low SES andyoung age) of the mothers but also recognized that prob-lems experienced during the pregnancy and delivery areimportant for a mother’s well-being and her future rela-tionship with her infant. In contrast, physicians expressedconcerns when they learned about a mother’s potentialglobal psychosocial risks but did not seem especially sensi-tive to psychological and health risk factors.
This finding goes together with our data on the num-ber of psychosocial topics discussed. Both groups exploredmore psychosocial items with mothers who were younger.In addition, nurses also asked more questions of motherswith psychological difficulties whereas physiciansresponded only when there were difficulties during thepregnancy. Thus nurses again were more geared toexplore both psychological and social factors, whereasphysicians responded more to the mother’s pregnancy.
The next group of findings deals with the satisfactionthese mothers expressed with the treatment they receivedfrom the nurses and doctors. A significant amount of thevariance here is related to the psychosocial interest dis-played during the interview by the respective professionals.This relationship suggests that the mothers appreciatedthe psychosocial sensitivity of the physicians and nurses,and this finding in turn was validated by our observer rat-ings. In addition, the interview with the physician wasrated highly by the more educated mothers and thosewho had few psychosocial risk factors. In contrast, theinterview with the nurses was appreciated more bymothers who showed some depressed symptomatologybut had fewer actual difficulties during their pregnancy.This difference may reflect the fact that better-educatedwomen are more at ease with physicians, regardless oftheir gender, while the greater psychosocial sensitivity ofthe nurses is appreciated by mothers with higher depres-sion scores. However, it is important to stress that mothersgave both professional groups comparatively high satis-faction scores (44.8 for nurses versus 42.0 of a possible50 for physicians; t = 2.21, p < .04). Two possible inter-pretations of this phenomenon may be an overall reluc-tance of parents to judge the sensitivity of their chosenmedical practitioner after a single interview or a lowexpectation for any psychosocial treatment from theirmedical practitioner.
The final interesting result is the suggestion that thecultural orientation of a mother may have an impact onher responses and subsequent ratings on the WMCI.Thus 88% of the recent immigrants from developingcountries (N = 9) were designated to have an insecureattachment, in contrast to 26% of the rest of the sample.As the WMCI ratings were done by three independentraters who did not know the immigration status of themothers and whose agreement for the three main categorieswas good (κ = 0.75), rater bias is unlikely. Furthermore,the overall distribution of attachment categories andtheir correlation with specific background data confirmthose in previous studies (Benoit et al., 1997). However,the WMCI is an interview whose scoring is based on arespondent’s verbally transmitted form and content tospecific questions. This raises the possibility that cul-turally determined taboos may prevent mothers fromnon-Western cultures to share their inner thoughtsabout their infants (Westermeyer and Janca, 1997),causing them to be placed in an insecure attachment cat-egory of the WMCI.
ASSESSMENT OF MOTHER–INFANT MENTAL HEALTH
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 40 :7 , JULY 2001 809

Clinical Implications
Because nurses explore psychosocial issues more thanphysicians and have concerns about both moderate andsevere problems, they are in a good position to inform aphysician, who can confirm these findings and furthersupport the family. In this sample, there was no communi-cation between the nurses and physicians, leaving espe-cially physicians ignorant of their patients’ often significantpsychosocial vulnerabilities and concerns. While the dataobtained by the nurses and physicians in an initial postna-tal interview usually are not identical, one can argue thatthere should be obligatory communication between thetwo professional groups in “high-risk” cases. High-riskcases would include recent immigrants, single and youngmothers, and those with histories of psychiatric or psycho-social difficulties or with children who suffer from chronicmedical conditions. Physicians, in turn, should encouragenurses to follow up identified problem cases, and togethernurses and physicians should devise possible interventionstrategies.
Limitations
The most obvious limitation of the study is the speci-ficity of our patient sample, i.e., mothers of primarilyfirst-born children who have access to a private albeitgovernment-reimbursed physician. This makes generali-zations to other populations questionable. In addition,our sample was small because only a limited number ofnurses and physicians made neonatal visits or acceptednew patients in their practice.
Another potential difficulty is the heterogeneity of oursample. Of the 42 mothers, 18 (43%) were immigrantsand 9 had been in Canada for less than 5 years. Thesewomen often had been highly educated in their countriesof origin but usually had not found employment inCanada that matched their level of education. This factormay also explain the comparatively high rate of depres-sive symptoms the mothers showed on the SCL-90-R(23%) and the EPDS (17%), surpassing rates seen inother samples of women in the postpartum period(Wendell et al., 1987). On the other hand, the compara-tively high incidence of obvious psychosocial stress fac-tors in this sample can be seen as a potential signal for theprofessionals to investigate the mental health of mothersand infants in more detail. That few physicians did soemphasizes the great need to create health care systems inwhich public health nurses and physicians readily com-municate with each other. This will help mothers start
life with a new baby under an umbrella of support andcare that embraces both the physical and emotionalaspects of their future life together.
REFERENCESAchenbach TM (1991), Manual for the Child Behavior CheckList 14–18 and
1991 Profile. Burlington: University of Vermont Department of PsychiatryBenoit D, Parker CH, Zeanah CH (1997), Mothers’ representations of their
infants assessed prenatally: stability and association with infants’ attach-ment classifications. J Child Psychol Psychiatry 38:307–313
Cooper PJ, Campbell E, Day A, Kennerley H, Bond A (1988), Non-psychotic psychiatric disorder after child-birth. Br J Psychiatry 152:799–806
Costello EJ, Costello AJ, Edelbrock C et al. (1988), Psychiatric disorders inpediatric primary care: prevalence and risk factors. Arch Gen Psychiatry45:1107–1116
Cox JL, Holden JJ, Sagovsky R (1987), Detection of postnatal depression:development of the 10-item Edinburgh Postnatal Depression Scale. Br JPsychiatry 150:782–786
Derogatis L (1987), SCL-90-R: Administration, Scoring and Procedures.Baltimore: Clinical Psychometric Research
Gallop R, Lancee W, Garfinkel P (1990), The expressed empathy of psychiat-ric nursing staff. Can J Nurs Res 22:7–18
Greenberg MT, Speltz ML, DeKlyen M (1993), The role of attachment in theearly development of disruptive behavior problems. Dev Psychopathol5:191–213
Laucht M, Esser G, Schmidt MH (1994), Parental mental disorder and earlychild development. Eur Child Adolesc Psychiatry 3:125–137
Lavigne JV, Gibbons RD, Christoffel KK et al. (1996), Prevalence rates andcorrelates of psychiatric disorders among preschool children. J Am AcadChild Adolesc Psychiatry 35:204–214
Main M, Kaplan N, Cassidy J (1985), Security of attachment in infancy, child-hood and adulthood: a move to the level of representation. In: GrowingPoints in Attachment Theory and Research, Bretherton I, Waters E, eds.Society for Research in Child Development Monograph 50, no. 209.Chicago: University of Chicago Press, pp 66–104
Minde K (1996), Effect of disordered parenting on the development of chil-dren. In: Child and Adolescent Psychiatry: A Comprehensive Textbook, 2nded, Lewis M, ed. Baltimore: Williams & Wilkins, pp 398–407
Minde K, Minde R (1986), Infant Psychiatry: An Introductory Textbook. In:Sage Series in Developmental Clinical Psychology and Psychiatry, Kazden E,ed. Beverly Hills: Sage
Mrazek DA (2000), Somatic expression of disease. In: Handbook of InfantMental Health, 2nd ed, Zeanah CH, ed. New York: Guilford, pp 425–436
Mrazek DA, Klinnert M, Mrazek P et al. (1999), Prediction of early onsetasthma in genetically at risk children. J Pediatr Pulmonol 27:89–94
Paes B (1991), The infant check-up: points to ponder. Can J Diagn 8:135–151Sameroff A (1993), Models of development and developmental risk. In:
Handbook of Infant Mental Health, Zeanah CH, ed. New York: Guilford,pp 3–13
Sharp L, Pantell RH, Murphy LO, Lewis CC (1992), Psychosocial problemsduring child health supervision visits: eliciting, then what? Pediatrics89:619–623
Stillman P, Burpeau-Digregorio M (1984), Teaching and evaluating inter-viewing skills. Adv Dev Behav Pediatr 5:109–145
Van IJzendoorn MH, Bakermans-Kranenburg MJ (1997), Intergenerationaltransmission of attachment: a move to the contextual level. In: Attach-ment and Psychopathology, Atkinson L, Zucker KJ, eds. New York:Guilford, pp 135–170
Wendell RE, Chalmers JC, Platz C (1987), Epidemiology of puerperal psy-choses. Br J Psychiatry 150:662–671
Webster G (1989), Final Report on the Patient Satisfaction QuestionnaireProject. Philadelphia: University City Science Center, American Board ofInternal Medicine
Westermeyer J, Janca A (1997), Language, culture and psychopathology: con-ceptual and methodological issues. Transcultural Psychiatry 34:291–311
Zeanah C, Benoit D (1995), Clinical applications of a parent perceptioninterview. In: Child and Adolescent Psychiatric Clinics of North America,Vol 4, Minde K, ed. Philadelphia: Saunders, pp 539–554
MINDE ET AL.
810 J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 40 :7 , JULY 2001