Embed Size (px)
Citation preview

1
number 6
Done by أبو عوضحسام
Corrected by
Doctor Ashraf

2
Antiviral Drugs
When dealing with drugs, it is always important to keep an eye on what you
want to target (viruses here), so here is a reminder of some of the main
features of viruses:
- Viruses have no cell wall.
- All viruses contain nucleic acids (RNA or DNA).
- Viruses may be enveloped or naked.
- The antigens of the viruses are their spikes or glycoproteins.
- Viruses are obligate intracellular parasites.
- Most of the viruses rely mainly on the host’s mechanisms for their
replication.
- Some viruses replicate in the cytoplasm while others do so in the nucleus.
- Usually, at the time of diagnosis, most of the viral replication would have
already occurred.
By relying on the above noted points (and some others), many antiviral
drugs were developed and the following was noted:
- Many antiviral drugs are purines (A & G) or pyrimidines (C & T)
analogues (anti-metabolites) (Molecularly, the drug looks very similar to
one of the normal nucleosides (A, T, G, C or U), but slight variations on
the structure were made resulting in our drug being able to join the
DNA/RNA synthesis process, but not allowing it to continue. After
activation (changing to nucleotide), the drug joins the DNA/RNA strand
being synthesised (by binding to one other nucleotide) it stops further
synthesis as it can only bind unilaterally (from one-sid) stopping further
synthesis of that DNA or RNA strand).
- Many antiviral drugs are “prodrugs”, i.e. their structures get changed
when they enter the body (by viral or cellular enzymes) resulting in their
activation.
- Ant-viral drugs inhibit the viral replication, so once they are removed the
replication resumes.
- As you can tell from the first point, most antiviral drugs work on the
replicative step of the viral life-cycle, therefore, they can ONLY work
against replicating viruses not latent viruses (see pathogenesis sheet for
different ways in which the viruses infect the body).
- Antiviral drugs only help the immune system in dealing with the virus,
this means that the immune system remains the main factor in dealing
with the infection [that’s why antiviral drugs are rarely prescribed in

3
acute infections, in fact they are only supposed to be prescribed (in acute
infections) to immunocompromised patients] (in viral infections, the
cellular immunity (T-cells) is of greater importance than the humoral
immunity(B-cells); B-cells produce antibodies specific to certain
antigens, these antigens may simply change later on by a mutation, so it
is often that a new immune reaction has to occur to the invading virus
(i.e. no memory cells present) and in such immune reactions T-cells are
of a greater importance, especially the CD8+ T-cells which “kill” the
virus after identifying the infected cell, see the end of the sheet for a
small note about immunity).
- For the drug to be effective clinically it is important for the minimum
inhibitory concentration of the drug to reach the infected cells.
Stages of Viral Replication
I- Cell entry
➢ Attachment (Adhesion)
➢ Penetration
II- Uncoating
III- Transcription of viral genome
IV- Translation
V- Assembly of virion components
VI- Release
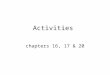
There are antiviral drugs that target each one of the steps mentioned above, but
this is not for all viruses (for example, some viruses may have drugs that are
only active on their
uncoating stage, other
viruses may have no active
drugs against them at all
and others, like HIV, have
active drugs for each stage
of their replication cycles).
The following diagram
shows some antiviral drugs
and the stages that they
work on. [Note: the HIV
drug (enfuvirtide) blocks
the CD-4 receptor on the
T-cell, another drug
(Maraviroc) blocks the CCR5 co-receptor on the T-cell, both give the same

4
result, work on the same virus and at the same stage of the replication cycle].
[Early protein synthesis for the CMV is targeted by the drug (fomivirsen)].
From now on, we will be discussing the antiviral drugs by mentioning a virus
(or a family of viruses) and the drugs against it.
Anti-Herpes Virus Agents
There are 8 genera of the family herpesviridae and they are called human herpes
1 to 8 (human herpes 1 is herpes simplex virus 1 (HSV-1), human herpes 2 is
herpes simplex virus 2 (HSV-2), human herpes 3 is varicella zoster virus (VZV)
and human herpes 5 (5 not 4) is cytomegalovirus (CMV).
The drugs used against the herpesviridae are:
A- Acyclovir / Valacyclovir
B- Famciclovir / Penciclovir
C- Ganciclovir / Cidofovir
D- Foscarnet
E- Trifluridine / Idoxuridine / Vidarabine
The first three groups (A, B and C) are categorised as a single group
pharmacologically as they all have similar mechanisms of action. Vidarabine
makes a second group, trifluridine a third group and foscarnet a fourth group.
Acyclovir and Related Compounds
Valacyclovir is the same as acyclovir except that a “valine” group is added in
valacyclovir. This valine group allows for a better bioavailability than when
using acyclovir. Valacyclovir is a prodrug of acyclovir (apparently, the drug
metabolism results in deactivation of lots of the acyclovir, with valacyclovir,
however, it seems that the metabolism simply removes the valine group leaving
us with acyclovir as is which means that more acyclovir molecules remain
active after the first pass metabolism).
The same concept applies to famciclovir and penciclovir (famciclovir gets
hydrolysed to penciclovir resulting in a higher bioavailability than if
penciclovir was directly used). [In the slides it is written that penciclovir is
given topically while famciclovir is given orally… To me, this makes no
sense, how do you administer a drug with a lower bioavailability in a way
that will decrease its bioavailability even more! (even Wikipedia says that
topical penciclovir has a “negligible” bioavailability!! But I guess we better
follow what is in the slides for exam purposes].

5
Pharmacology of this group: Acyclovir, valacyclovir, ganciclovir,
famciclovir and penciclovir are all guanine analogues (the nucleoside they
look similar to is guanine). Cidofovir is a cysteine analogue.
Mechanism of Action: All the drugs in this group (except cidofovir which
needs no phosphorylation and inhibits viral DNA synthesis) get
phosphorylated by the viral thymidine-kinase (ganciclovir is activated by
UL-97 enzyme by CMV) changing them from nucleosides to nucleotides,
monophosphate though (it must be a triphosphate to be used in nucleic acids
synthesis). Further phosphorylations are done by the kinases of the host cell
producing the required nucleotides. When the drug molecule adds to the
DNA strand being synthesised viral DNA-polymerase cannot add more
nucleotides (so it inhibits DNA-polymerase). As you can see (also
mentioned in page 2), the drug can only work on replicating viruses (not
latent).
These drugs are selective to the virus (as their activation has to be done by
the viral thymidine-kinase), therefore, only infected cells are affected by the
drug (the drug affects both, the infected cells and the viruses, but not in an
equal proportion (i.e. not 1:1 ratio) since the viral replication is faster and
the virus has a higher affinity to the drug (a drug with a 1:1 ratio of affecting
the viruses and the infected cells does more damage to the tissue and so
makes the situation worse) [some drugs are not selective (not mentioned
here) and damage uninfected cells and often cause bone marrow
suppression].
Spectrum: Following is the spectrum for all the drugs mentioned in this
group:
i- Valacyclovir / Acyclovir: HSV-1, HSV-2, VZV [VZV causes
Shingles in adults (chickenpox in kids) by travelling in a dermatome
(a superficial nerve that circles around the body (e.g. T1 dermatome))
and blisters appear in the area that the dermatome innervates].
ii- Ganciclovir / Cidofovir: CMV (Cidofovir is approved for treating
CMV retinitis in immunocompromised patients and adenovirus
infections, it is not specific to these, but a fine effect is seen here).
iii- Famciclovir: Herpes genitalis and shingles (diseases).
iv- Penciclovir: Herpes labialis (a disease).
Pharmacokinetics of Acyclovir (I don’t know if the list is for the entire
group or only acyclovir)
Oral bioavailability: 20-30%

6
Distribution: All the tissues including the CNS.
Renal excretion: >80%
Half-lives: 2-5 hours
Administration: Topical, oral or IV (cidofovir is available topically,
intravenously and as an intravitreal injection (vitreus is a structure in the
eye, so intravitreal injection = an injection in the eye).
Adverse Effects:
Acyclovir and Ganciclovir: - Nausea, vomiting and diarrhea.
- Nephrotoxicity (crystalluria, haematuria,
renal insufficiency)
- Myelosuppression (bone-marrow
suppression) (neutropenia and
thrombocytopenia) (only ganciclovir).
Cidofovir: - Nephrotoxicity (a major disadvantage for the
drug).
Therapeutic Uses
Acyclovir is the Drug of Choice for: HSV genital infections (oral, also in not-
so-serious shingles you can give oral acyclovir, if too serious you must give the
acyclovir IV), HSV encephalitis [needs to be given IV as this is a very
dangerous situation; a pregnant mother with encephalitis can only give a
caesarean delivery (والدة قيصرية), it’s too dangerous otherwise] and HSV
infections in immunocompromised patients.
Ganciclovir is the Drug of Choice for: CMV retinitis in immunocompromised
patients and in prevention of CMV in transplant patients.
Vidarabine
It is also a nucleoside analogue, but this time of adenosine (so its mechanism of
action is similar to acyclovir).
Pharmacokinetics
Bioavailability: ~2% (oral)
Administration: Ophthalmic (eye) ointment.

7
Spectrum: HSV-1, HSV-2 and VZV.
Therapeutic Uses: Only for HSV keratitis (inflammation of the cornea) and for
HSV keratoconjunctivitis in immunocompromised patients (inflammation of
both, the cornea and the conjunctiva).
Adverse Effects: Anemia and SIADH (Syndrome of Inappropriate Antidiuretic
Hormone secretion).
Trifluridine
This drug is a pyrimidine nucleoside analogue which inhibits viral DNA
synthesis (similar mechanism to acyclovir).
Spectrum: HSV-1, HSV-2 and VZV.
Therapeutic Uses: Only for topical-ocular HSV keratitis and herpetic
keratoconjunctivitis.
Foscarnet
Mechanism of Action: It is an analogue for the inorganic pyrophosphate and so
it directly inhibits viral DNA and RNA polymerases and viral reverse
transcriptase (it does not need phosphorylation to produce its antiviral activity).
Spectrum: HSV-1, HSV-2, VZV, CMV and HIV
Pharmacokinetics
Bioavailability: 10-20% (oral).
Distribution: All the tissues including the CNS.
Administration: IV
Therapeutic Uses: It is an alternative drug for acyclovir in HSV infections (if
the patient is resistant to acyclovir or is immunocompromised) and for
ganciclovir in CMV retinitis (if the patient is resistant to ganciclovir or is
immunocompromised).
Respiratory Viral Infections
There are two viruses to deal with in this group; Influenza and RSV
(Respiratory Syncytial Virus) (often causes bronchiolitis).
Influenza

8
There are two groups of drugs for the influenza virus: Amantadine and
rimantadine and oseltamivir and zanamivir (neuraminidase inhibitors).
Amantadine and Rimantadine
These work against influenza A only because they inhibit the viral membrane
protein M2 which is only present in influenza A.
Mechanism of Action: by blocking the M2 protein channel, these drugs disrupt
hydrogen transport and, therefore, disrupt viral uncoating in the host cell
(remember that uncoating often occurs by hydrogen ions transport leading to a
change in the pH resulting in dissolving the vesicle that is carrying the virus,
thus letting the virus release its genome and proteins) (so viral RNA
transcription is prevented) (90-95% of influenza A are now resistant to these
drugs) [when the patient visits the doctor, the infection would have already
happened and most of the viral replication would have been done, so the
treatment is more of a symptomatic treatment (Panadol and things similar to it)
rather than a curative one].
Pharmacokinetics
Bioavailability: ~50-90%.
Distribution: Amantadine extensively crosses the blood brain barrier whereas
rimantadine does not cross it extensively.
Administration: Oral.
Oseltamivir and Zanamivir
These drugs are neuraminidase inhibitors and they affect influenza A and B.
Mechanism of Action: Neuraminidase is an enzyme present within the
influenza virus which is essential for its replication (during the release process a
bit of the virion remains attached with the cellular membrane, neuraminidase
enzyme “cuts” this final attachment setting the virion free). Therefore, these
neuraminidase inhibitors keep the virions “stuck” and unable to leave the cell’s
surface preventing their release and not allowing them to spread from cell to
cell. These two drugs do not interfere with the immune response to the influenza
A vaccine and they can be used prophylactically and for treating an acute
infection.
Pharmacokinetics: Oseltamivir is an oral drug while zanamivir is an intranasal
drug.
Adverse effects: There is a risk of bronchospasm with zanamivir.

9
RSV
This virus often causes bronchiolitis (an upper respiratory tract infection that
often catches new-borns and children less than 2 years old) and it is treated with
“Ribavirin”.
Mechanism of Action: Ribavirin is a guanosine analogue and it requires
phosphorylation to its mono- di- and tri- phosphate forms. Its triphosphate
inhibits RNA polymerase, depletes the cellular storages of guanine (inhibits
IMDH) and decreases the synthesis of the mRNA 5’ cap (by interfering with the
guanylation and the methylation of the nucleic acid bases).
Spectrum: RNA viruses including influenza, parainfluenza, RSV and Lassa
virus.
Pharmacokinetics
Distribution: All body tissues except the CNS.
Administration: Oral, IV and inhalation in RSV.
Adverse Effects: Anaemia and jaundice (contraindicated in pregnant women).
Therapeutic Uses: RSV bronchiolitis and pneumonia in hospitalized children
(given by aerosol) and Lassa fever. Ribavirin serves as an alternative drug for
infections caused by influenza, parainfluenza and measles virus infection in
immunocompromised patients.
Hepatic Viral Drugs
These are viral infections caused to the liver and we’ll only mention a bit about
them.
Drugs
Interferons
Lamivudine (a cytosine analogue used against the hepatitis B virus)
Entecavir (a guanosine analogue used against the lamivudine resistant strains
of the hepatitis B virus)
Ribavirin (used with interferons against the hepatitis C virus)
SOFOSBUVIR (a nucleotide analogue used in combination with ribavirin and
interferons for the treatment of the hepatitis C viral infection. It’s a 12-week
course that costs a total of 84,000$ (1000$ for each pill).

10
Retroviruses
We treat the retroviruses (the family of the HIV) using the “HAART” (Highly
Active Anti-Retroviral Therapy) which is simply a “cocktail” of at least three
medications that work via different mechanisms to reduce the viral load.
(As we mentioned in the second page, every single step of the viral life-cycle
for the HIV has a drug that was made to inhibit it).
Cell Entry Inhibitors
The drugs that inhibit this stage are called “Fusion inhibitors” (or “Entry
Inhibitors”) (i.e. they do not allow the virus to “fuse” with the cell membrane).
This is the newest class of antiretroviral drugs. Enfuvirtide (Fuzeon) is a good
example (we talked a bit about it in the second page).
These drugs are used in combination with other drugs active against HIV.
Adverse Effects: Peripheral neuropathy (damage to peripheral nerves),
insomnia (sleeplessness), depression, cough, dyspnea (shortness of breath),
anorexia (فقدان الشهية) and arthralgia (joint pain).
Another drug, maraviroc (Selzentry, outside the US: Celsentri), inhibits the co-
receptor (CCR5) instead of the receptor on the T-cells (as mentioned in page 3).
This drug was approved by the FDA in 2007. This drug is used in combination
with other drugs active against HIV. (HIV can use other co-receptors like
CXCR4 so an HIV tropism test (e.g. trofile assay test) is needed to prove the
drug’s efficacy for this patient).
There are some safety issues in blocking the CCR5 co-receptor as its function
(in a normal situation) is yet to be known.
Important Note: in the slides, maraviroc is placed in a separate group called
“Entry inhibitors” and the first group is called “Fusion inhibitors”, but a quick
search on google showed that “Entry Inhibitors” and “Fusion Inhibitors” are just
two names for the same group of drugs, still, if a question like (Under which
group does maraviroc fall?) was asked and you had both “Fusion Inhibitors”
and “Entry Inhibitors” present in the choices, I guess you must go with “Entry
Inhibitors” (if the question was about enfuvirtide then go with “Fusion
inhibitors”).
Reverse Transcriptase Inhibitors (RTI)

11
These drugs block the activity of the reverse transcriptase enzyme preventing
the production of new viral DNA (from RNA). Below are the sub-groups of
reverse transcriptase inhibitors and the associated examples [the doctor said that
he won’t ask about the sub-groups’ examples (I don’t know if he will ask about
the following explanations about each subgroup), but he might bring a drug
name from one of the examples below and ask to which group (not sub-group) it
belongs (the answer would be reverse transcriptase inhibitors].
a- Nucleoside RTIs (NRTIs): Azidothymidine (AZT), Didanosine (ddI),
Stavudine (D4T), Lamivudine (3TC).
b- Nonnucleoside RTIs (NNRTIs): Nevirapine, delavirdine, efavirenz.
c- Nucleotide RTIs (NTRTIs): Tenofovir, Adefovir
NRTIs: These drugs require phosphorylation by the host cellular kinases to
become in their active (triphosphate) forms. Still, selectivity is noted with AZT
as HIV’s reverse transcriptase has a higher affinity to AZT than the DNA
polymerase of the host cell. (A table showing all the information about each of
the drugs in this group is found at page 14, the doctor said that he won’t ask
about the side effects of these drugs).
NNRTIs:
➢ They are active against HIV-1 and do not require cellular enzymes to be
phosphorylated.
➢ They do not inhibit the human DNA polymerase.
➢ They are relatively safe (noncytotoxic).
➢ They are highly prone to drug resistance.
➢ They are used with other drugs that are active against HIV.
Integrase Inhibitors
The drugs of this group block the action of the enzyme integrase (an enzyme
that allows the virus to insert its genome into the DNA of the host cell). The
drugs are: Raltegravir, Elvitegravir, Dolutegravir and MK-2048.
Protease Inhibitors
These drugs inhibit the action of the protease retroviral enzyme (remember that
HIV produces a “poly-protein” after the translation of its mRNA; the protease
enzyme cuts this “poly-protein” to individual proteins) preventing viral
replication. So, inhibition of the protease enzyme prevents the re-assembly and
the release steps from occurring.

12
Examples: Amprenavir (Agenerase), Indinavir (Crixivan), Nelfinavir
(Viracept), Ritonavir (Norvir), Saquinavir (Invirase). [Hepatotoxicity is noted].
These drugs are used in combination with other drugs active against HIV.
(Combining multiple antiretroviral drugs is common).
Adverse Effects: vary from drug to drug and may be severe (the patient must be
monitored to avoid dose-limiting toxicities and for signs of opportunistic
diseases).
Interferons (IFNs)
This is the final group of drugs for today (!أخيرا).
Interferons are natural proteins produced by the cells of the immune system in
response to any foreign agents they face (viruses, bacteria, fungi, tumour, etc.).
These interferons result in some antiviral, immune modulating and anti-
proliferative actions.
There are three classes of interferons (α, β and γ).
Interferons α and β are produced by all the cells in response to viral infections
while interferon γ is only produced by the T-lymphocytes and by the NK-cells
in response to cytokines (interferon γ is more into immune regulation, while
interferons α and β are more into producing antiviral effects).
Mechanism of Action: The interferons induce some enzymes including a
protein kinase (inhibits protein synthesis), an oligo-adenylate synthase (leads
to degradation of viral mRNA) and a phosphodiesterase (inhibits tRNA),
together, these three enzymes lead to the inhibition of translation.
Spectrum: Hepatitis B Virus (HBV), Hepatitis C Virus (HCV) [pegylated
interferons (pegylation: addition of polyethylene glycol to the interferons) are
used to prolong the duration (increase half-life) for which the interferons remain
inside the body] and Human Papilloma Virus (HPV).
Anti-proliferative actions (of the interferons) may inhibit the growth of some
cancers (E.g. Kaposi sarcoma and hairy cell leukemia).
Pharmacokinetics
Bioavailability: <1% (Oral).
Administration: Intralesional, Sub-cutaneous and IV.
Distribution: All the tissues except the CNS.

13
Half-lives: 1-4 hours.
Adverse Effects
➢ Acute Flu-like syndrome (fever, headache).
➢ Bone-marrow suppression (granulocytopenia, thrombocytopenia).
➢ Neurotoxicity (confusion, seizures).
➢ Cardiotoxicity (arrhythmia).
➢ Impairment of fertility.
Therapeutic Uses
➢ Chronic hepatitis B and C (complete disappearance in 30% of the patients).
➢ Herpes Zoster viral (HSV) infection in cancer patients (prevent
dissemination of the infection).
➢ CMV infections in renal transplant patients.
➢ Condylomata acuminate (genital wart caused by some subtypes of HPV)
(intralesional injection, complete clearance is seen in 50%).
➢ Hairy cell leukemia (in combination with zidovudine).
➢ AIDS related Kaposi’s sarcoma.
The following table summarizes some of what was said in this sheet:

14
The following table is the one that shows the drugs of the NRTIs group:
The note about immunity: All cells have a protein called “MHC-I” (Major
histocompatibility complex -1) and antigen presenting cells (macrophages, B-
cells and dendritic cells) have MHC-II. When a pathogen invades a cell, the cell
uses its proteasomes to “cut” the pathogen into pieces and take its “antigen”.
The MHC (I or II) binds to that antigen and takes it to the surface of the cell
presenting it. A T-cell, which has receptors to MHC-I and II, binds to that
antigen and begins the immune response [CD4+ T-cells are the ones that do this
job (also known as T-helper cells)]. This process initiates the production of T-
killer cells (or CD8 + T-cells) which release substances that kill the invading
pathogen.
Drug Toxicity Special
Considerat
ions
Dosing Adverse
Effects
3TC
(Lamivudine
/ Epivir)
Few
Hepatitis B
exacerbation
Hepatitis B 150mg bid
or 300mg
qd.
Renal
dosing
available
Few; class
effect
Combination
with AZT
D4T
(Stavudine /
Zerit)
Lipoatrophy
Peripheral
neuropathy
Pancreatitis
Lactic acidosis
- 40mg bid (if
>60kg)
30mg bid (if
<60kg)
Gen well-
tolerated
H/N/V
Combination
only
AZT
(Zidovudine /
Retrovir)
Anemia
Neutropenia
Thrombocytopenia
Myopathy
- 300mg bid Nausea /
vomiting
Headache
Dizziness
Combination
Only
DDI
(Didanosine /
Videx)
Lactic acidosis
Peripheral
neuropathy
Pancreatitis
Lipodystrophy
- If EC,
400mg QD
(<60kg:
250mg qd)
If reg tabs,
200mg bid
(<60kg:125
bid/250qd)
Empty
stomach
GI Combination
Only