-
8/9/2019 Nucleus Arthroplasty Volume II
1/55
NucleusArthroplasty
Volume II: Biomechanics &Development
Technology
in Spinal Care
-
8/9/2019 Nucleus Arthroplasty Volume II
2/55
Table of Contents
This monograph series is a groundbreaking project in therapidly
emerging field of non-fusion spinal surgery. Thefull range of
nucleus replacement technologies is examined
with discussion on biomechanical and physiological proper-ties
of the disc, detailed information on each cutting-edge
device technology, indications, and patient selection
criteria.
Nucleus Arthroplasty Technology in Spinal Careis
published for the medical profession by Raymedica, LLC,
Minneapolis, MN 55431.
The views expressed in this series are those of the authors
and do not necessarily represent those of Raymedica, LLC.
ACKNOWLEDGEMENT
We, Raymedica, LLC, and the authors of this volume, wish
to acknowledge our debt of gratitude for the important
contribution of Steven J. Seme, Developmental Editor. His
guidance has added a great deal to the teaching value of
this volume.
Copyright 2006 and 2007 Raymedica, LLC. All rights
reserved. Printed in the U.S.A.
2 Introduction
4 Deputy Editorial Board
C H A P T E R 7 6 Biomechanics of the Degenerated Disc
C H A P T E R 8 11 Principles and Mechanical Requirements of
Nucleus Implants
C H A P T E R 9 17 Kinematic Demands of Nucleus Arthroplasty
Technology
C H A P T E R 1 0 24 Device Stiffness vs. Load-Sharing with
Nucleus Arthroplasty Devices
C H A P T E R 1 1 34 Endplate Mechanics
C H A P T E R 1 2 41 Repair of the Anulus Fibrosus of the Lumbar
DiscC H A P T E R 1 3 49 Integration of Nucleus Arthroplasty
Technology into the Continuum of Care
IBC Conclusion
www.nucleusarthroplasty.com
-
8/9/2019 Nucleus Arthroplasty Volume II
3/55
2
The first documented works describing the diagnosis and
treatment of the spine, spinal disorders, and spinal
instabilitydate back to 1900-2500 B.C. Interestingly, the documents
recom-
mended against the treatment of spinal cord injury. The
develop-
ment of therapeutic treatments has a long history starting
with
the cane, the first load-sharing device. Today, our efforts
to
improve therapies to treat spine disease persist. We continue
to
recognize problems, identify issues, and define variables in
an
effort to better understand spinal degeneration and to
develop
innovative solutions that utilize a wide array of materials
and
technologies. Our field has had a rich history of
advancements,
accomplishments, and inventiveness. We owe a great debt to
the
pioneers who, armed with little more than a detailed
knowledge
of anatomy, heralded in the era of spinal surgery. Their
trials,
errors, innovations, and teachings have guided our efforts
to
ultimately improve clinical outcomes.
Early on, it was recognized that the disc played a vital role in
overall
spine health. With great effort and ingenuity, the unique
anatomical,
biomechanical, and physiological properties of the disc were
eluci-
dated and incorporated into elegant treatment algorithms. We
now
have access to an almost overwhelming flow of information
about
lumbar disc arthroplasty from countless sources. Central to the
evo-
lution of therapies is a better appreciation of the complexities
of thelumbar disc. By combining knowledge gleaned from
anatomical
dissection, biochemical processes, and resultant physiology with
a
disciplined foundation in biomechanics, we have created a
fabric
of understanding never before enjoyed. Spine arthroplasty is
now
an important and evolving area within the treatment of
spinal
Reginald J. Davis, MD, FACSCHIEF OF NEUROSURGERY
Baltimore Neurosurgical Associates, PA
Baltimore, MD 21204
Federico P. Girardi, MDASSISTANT PROFESSOR
OF ORTHOPEDIC SURGERY
Hospital for Special Surgery
New York, NY 10021
Frank P. Cammisa, Jr., MD, FACSASSOCIATE PROFESSOR OF CLINICAL
SURGERY
Hospital for Special Surgery
New York, NY 10021
William C. Hutton, DScPROFESSOR AND DIRECTOR OF
ORTHOPEDIC RESEARCH
Emory University
Atlanta, GA 30322
Introduction
-
8/9/2019 Nucleus Arthroplasty Volume II
4/55
disorders. This sub-discipline represents the coalescence of
manyareas of study focused on the development of new and
exciting
solutions to address clinical problems.
These significant advances in our understanding of the spine
rep-
resent a culmination of efforts occurring across many fronts.
Our
increased understanding of the biological factors at work in
disc
disease has been a driving force in the development and
emer-
gence of new materials and delivery methods. The critical
role
that advanced biocompatible alloys, polymers, and
viscoelastic
hydrogels play in the innovation of disc arthroplasty
technologies
cannot be over emphasized.
Technological advancements have played a vital role in
supporting
and expanding our knowledge of motion preserving disc
technolo-
gies. The latest imaging technologies allow a much more
detailed
appreciation of pathological processes, such as disc
degeneration,
and provide the ability to monitor the results of an
intervention.
Computerized finite element analysis offers a risk-free
environment
in which to test hypotheses and predict clinical impact.
Biochemical
advancements yield an intimate understanding of the chemical
envi-
ronment including chemical mediators and potential
intervention
portals. This wealth of knowledge can be used to great
advantage
when developing disc arthroplasty technologies.
Not to be overlooked, the socioeconomic challenges involved in
the
development of new technologies, such as the Nucleus
Arthroplasty
motion preservation system, have also become more apparent.
The all important variable of proper patient selection continues
to
require constant reassessment and vigilance. Increasingly,
third-party
payers control access to care and treatment choice to an
alarming
degree. Such considerations can no longer be ignored in the
quest
for ideal patient management methods.
This publication has been constructed to provide an overview
of
the current biomechanical developments in Nucleus
Arthroplastytechnology. Key elements include the Principles and
Mechanical
requirements of Nucleus Devices, Kinematic Demands, Endplate
Mechanics, Device Stiffness vs. Load Sharing, and Anular
Closure
Techniques. In addition, Volume II of this series will
provide
insight into the potential market and the current players
working
in the forefront of Nucleus Arthroplasty technology
developmentactivities. This is an incredibly exciting field as
technologies
focused on the repair and replacement of the diseased disc
nucleus will catapult us far beyond the treatment options we
have available today.
In conclusion, we can say that the spine arthroplasty
specialist
of today is well prepared to deliver the most advanced
solutions
to the clinical puzzle of disc disease with technologies based
on
a rich tradition of innovation and compassion coupled with a
tremendous wealth of physiological knowledge and assessment
tools. As spine surgery evolves from mechanical solutions to
therapeutic solutions both surgeons and patients will
benefit.
We hope you will find this series on Nucleus Arthroplasty
technology to be a valuable asset.
Reginald J. Davis, MD, FACS
Federico P. Girardi, MD
Frank P. Cammisa, Jr., MD, FACS
William C. Hutton, DSc
3
-
8/9/2019 Nucleus Arthroplasty Volume II
5/55
Reginald J. Davis, MD, FACS
Dr. Davis is founder of Baltimore Neurosurgical Associates,
chief
of Neurosurgery at the Greater Baltimore Medical Center, and
a
faculty member at the Johns Hopkins School of Medicine and
the University of Maryland. He is a Fellow of the American
College of Surgeons and a Diplomate of the American Board of
Surgery. Dr. Davis received his medical degree from Johns
Hopkins University School of Medicine, Baltimore, Maryland.
He has broad experience in advanced procedures such as
spinal
stabilization, intradiscal electrothermal therapy, and
microendo-
scopic discectomy and has conducted physician training pro-
grams on these procedures. His professional affiliations
include
the AANS-CNS Section on Disorders of the Spine, the American
Association of Neurological Surgeons, the Congress of
Neurological Surgeons, and the North American Spine Society.
Federico P. Girardi, MD
Dr. Girardi is assistant professor of orthopedic surgery,
Weill
Medical College of Cornell University and is attending
orthopedic
surgeon at the Hospital for Special Surgery, New York, New
York.
He specializes in the treatment of spinal disorders including
degen-
erative disc disease (DDD), spinal deformities, metabolic
fractures,
and spinal tumors. Dr. Girardi received his medical degree
from
the Universidad Nacional de Rosario, Rosario, Argentina.
He has performed extensive clinical research in the areas of
mini-
mally invasive surgery, clinical outcomes, and spinal imaging.
He
is also interested in basic research on bone, disc, and nerve
tissue
regeneration and in the investigation of alternatives to
spinal
fusion for the treatment of DDD. His professional
affiliations
include the North American Spine Society, Scoliosis Research
Society, the European Spine Society, the International Society
for
the Study of the Lumbar Spine, and the Spine Arthroplasty
Society
Raymedica has selected Drs. Reginald J. Davis, MD, FACS,
Federico P. Girardi, MD, Frank P. Cammisa, Jr., MD, FACS,and
William C. Hutton, DSc to edit this series of monographs on Nucleus
Arthroplasty technology, because of theispecial interest in this
dynamic area of medicine. They are well respected for their
clinical work and travel widely to speakand educate physicians.
Drs. Davis, Girardi, and Cammisa are noted for their expertise in
spine surgery and advanced
training in minimally invasive surgical techniques.
Deputy Editorial Board
4
-
8/9/2019 Nucleus Arthroplasty Volume II
6/55
5
Frank P. Cammisa, Jr., MD, FACS
Dr. Cammisa is associate professor of clinical surgery,
Weill
Medical College of Cornell University and is the Chief of
Spinal
Surgical Service at The Hospital for Special Surgery in New
York,
New York, where he also serves as an associate scientist in
the
research division. Dr. Cammisa received his medical degree
from
the College of Physicians and Surgeons at Columbia
University,
New York, New York.
His clinical interests include non-fusion and motion
preservation
technologies, minimally invasive, laparoscopic, and computer
assisted spinal surgery; microsurgery and athletic spinal
injuries.
He is an active member of many spine societies, academic
com-
mittees and editorial review boards. He has lectured widely
and
published in numerous peer-reviewed journals and books.
William C. Hutton, DSc
Dr. Hutton is professor and director of orthopedic research,
Emory University in Atlanta, Georgia. He also attended
Universities in Glasgow, Birmingham, and London. Before
coming
to Atlanta, he worked at educational institutes in London
and
Adelaide, Australia. In Adelaide, he was professor of
biomechanics
and chairman of the Department of Mechanical Engineering.
His major area of interest is biomechanics with a particular
focus on the spine. Dr. Hutton has published over 180 papers
in peer review journals. He has won many prizes for his
work,
most recently (2004) the Russell S. Hibbs Award from the
Scoliosis Research Society. At present, he has a Research
Career
Science Award from the Department of Veterans Affairs. He is
a member of the International Society for the Study of the
Lumbar Spine.
-
8/9/2019 Nucleus Arthroplasty Volume II
7/55
6
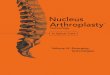
Chapter 7 Biomechanics ofthe Degenerated Disc
Andrew A. Sama, MD
ASSISTANT PROFESSOR OF ORTHOPEDIC SURGERYWeill Medical College
of Cornell University
Hospital for Special Surgery
New York, NY 10021
Federico P. Girardi, MDASSISTANT PROFESSOR
OF ORTHOPEDIC SURGERY
Hospital for Special Surgery
New York, NY 10021
INTRODUCTION
A s people age, the lumbar discs undergo a progressivealteration
of chemical composition and biomechanicalproperties. This
combination of chemical and biomechanical
changes can lead to back pain. Nucleus Arthroplasty inter-
ventions are emerging that intend to replace the nucleus of
the
diseased lumbar disc for treatment of patients with
discogenic
pain. Understanding the natural progression of disc
degenera-
tion is paramount to under-
standing the function of such
devices. This chapter summa-
rizes what is generally under-
stood about the degenerative
cascade and the resulting
biomechanical changes.
NUCLEUS ARTHROPLASTY INTERVENTIONS ARE
EMERGING THAT INTEND TO REPLACE THE NUCLEUS
OF THE DISEASED LUMBAR DISC FOR TREATMENT OF
PATIENTS WITH DISCOGENIC PAIN.
-
8/9/2019 Nucleus Arthroplasty Volume II
8/55
AGING AND LUMBAR DISC DEGENERATION
There is a complex arrangement of bones and cartilage that
make
up each spinal motion segment. The intervertebral disc along
with
the apophyseal joints allow for flexibility while also helping
to
maintain the stability of the spine (Figure 1).1 The disc is
some-
times seen as a cushion between vertebral bodies to help
absorb
and distribute applied forces. Each disc is made up of an
anulus,
a nucleus pulposus, and the cartilage endplates. The
intricate
lamellar arrangement between the fibers of the anulus
fibrosus
exteriorly, and the nucleus pulposus within, serve to absorb
the
forces applied to the spine. In healthy discs, there is a
harmonious
relationship between the components, such that compressive
axial
forces produce an increase in hydrostatic pressure in the
nucleus
pulposus, and this pressure is transmitted to the anulus where
it
is absorbed as tensile stress.2 Thus, the anulus sees tensile
stress as
well as compressive stress. The need to support this complex
stress
explains, to some extent, the orientation of the fibers of
the
anulus. The hydrophilic proteoglycans in the nucleus control
the
diurnal influx and efflux of water and nutrients that keep the
discs
healthy and give them their normal function. The osmotic and
hydrostatic properties of the disc are not static.3, 4 As people
age,
the discs can begin to desiccate and become depleted of
nutrients.Disc waste products accumulate, decreasing the
concentration of
viable cells, resulting in changes in the biomechanical
properties
of the disc.5
THE DEGENERATIVE CASCADE
As explained in Book IFundamentals, Chapter 1 of this
series,
the result of the disc aging and degenerating is a net decrease
in
the amount of aggregated proteoglycan and an increase in the
non-aggregated proteoglycans, which leads to lower osmotic
water binding capacity and loss of compressive resistance in
the
lumbar disc. As forces are applied to these biologically
altered
discs, there is a greater likelihood that damage will occur to
the
anulus fibrosus creating a vicious cycle of degeneration.6,
7
Kirkaldy-Willis et al8 described lumbar disc degeneration as
a
cascade that impacts the three joint complex. The first stage
of
the cascade is known as the Dysfunctional Stage and
corresponds
to the early onset of disc degeneration. The net result of
the
Dysfunctional Stage is a tearing of the outer anulus fibrosus
sec-
ondary to repetitive micro trauma. This is clinically
manifested
7
Nucleus Anulus
IntervertebralDisc
Figure 1Major components of spinal complex.
THE RESULT OF THE DISC AGING AND DEGENERATING IS A NET DECREASE
IN THE
AMOUNT OF AGGREGATED PROTEOGLYCAN AND AN INCREASE IN THE
NON-AGGREGATED
PROTEOGLYCANS, WHICH LEADS TO LOWER OSMOTIC WATER BINDING
CAPACITY AND
LOSS OF COMPRESSIVE RESISTANCE IN THE LUMBAR DISC.
THERE IS A COMPLEX ARRANGEMENT OF BONES AND
CARTILAGE THAT MAKE UP EACH SPINAL MOTION SEG-
MENT. THE INTERVERTEBRAL DISC ALONG WITH THE
APOPHYSEAL JOINTS ALLOW FOR FLEXIBILITY WHILE AL
HELPING TO MAINTAIN THE STABILITY OF THE SPINE.
ApophysealJoint
-
8/9/2019 Nucleus Arthroplasty Volume II
9/55
8
as a mechanical low back pain that is episodic. During this
stage
there is also a dehydration of the nucleus pulposus.8
The second stage is called the Instability Stage. This is
represen-
tative of more significant damage to the disc secondary to a
delamination of the layers of the anulus fibrosus. Vertebral
seg-
mental instability can occur resulting in further damage and
loss
of proteoglycan composition in the nucleus pulposus.8
The third stage is the Stabilization Stage. This occurs when
there
is resorption of the nucleus pulposus and worsening of
interver-
tebral disc space collapse. This is the stage where
osteophytes
form secondary to anular traction on vertebral endplates and
spinal stenosis may result.8
MRI CHARACTERISTICS OF
LUMBAR DISC DEGENERATION
The Kirkaldy-Willis stages described above can be
radiographi-
cally characterized by multiple imaging techniques, but
magnetic
resonance imaging (MRI) evaluation is the gold standard. Stage
I
(Dysfunctional) is usually manifested on MRI imaging
techniques
by the presence of a High Intensity Zone lesion of the
posterior
anulus fibrosus, and an overall decrease signal intensity of the
disc
on T2-weighted sequences in the sagittal plane (Figure 2a).9
Stage II (Instability) is manifested on MRI with further
loss
of disc space height and progressive desiccation resulting in
a
darker disc (Figure 2b). Disc herniations can present in Stage
II
because a loss of anular integrity may result in herniation of
the
nucleus pulposus.9
Stage III (Stabilization) is manifested on MRI by worsening
of
disc space collapse and by the presence of osteophyte
formation
coupled with soft tissue redundancy or hypertrophy,
resulting
in central canal, subarticular lateral recess, or foraminal
stenosis
(Figure 2c).9
Figure 2MRI images of degenerative cascade. (a) Dysfunction
StageHigh Intensity Zone lesion of the posterior anulus fibrosus
with decrease
signal intensity of the disc on T2-weighted image. (b)
Instability StageDisc collapse with continued decrease in signal
intensity.
(c) Stabilization StageContinued disc collapse, osteophyte
formation, stenosis of neural structures.
a Dysfunction bInstability cStabilization
THE KIRKALDY-WILLIS STAGES DESCRIBED
CAN BE RADIOGRAPHICALLY CHARACTERIZED
BY MULTIPLE IMAGING TECHNIQUES BUT MRI
EVALUATION IS THE GOLD STANDARD.
-
8/9/2019 Nucleus Arthroplasty Volume II
10/55
9
THE PAIN GENERATOR
The radiographic findings and histomorphology of disc
degener-
ation are objective signs of the presence of a disease state
that can
be measured, but these findings may not always correlate with
the
patients symptoms.10 The pain generators in degenerative
disc
disease (DDD) are multifactorial and can be chemically
mediated
or mechanically induced. The loss of disc structure and
biome-
chanical integrity results in alterations of the load-sharing
prop-
erties of the lumbar disc and the vertebral bodies.3 The
nerve
endings in the facet joints, spinal ligaments, and
para-spinous
musculature are then stimulated and result in pain. The
chemical
mediation of back pain occurs from the release of cytokines
and
free radicals along with cellular debris from matrix
degeneration.
This results in nocioceptive stimulation of nerve endings
and
resultant back pain. These conclusions are based on
Buckwalters
articles.5 As discs become progressively more degenerated,
they
demonstrate an ingrowth of blood vessels and nerve fibers
beyond the outer anulus which may also contribute to the
onset
of back pain. Normal lumbar discs do not typically have
blood
vessels or nerve fibers inside of the outer anulus.
BIOMECHANICAL CHANGES
According to Horst et al, non-degenerated discs exhibit
fluid-like
properties, whereas degenerated discs have properties that
are
more like those of a solid. The normal nucleus pulposus
behavessimilar to a viscous fluid: with degeneration, it shows an
increase
in shear modulus and becomes stiffer and more elastic.11 As
the
tissue transitions from fluid-like to more solid-like
properties, there
is an associated decrease in hydrostatic pressurization.
Hydrostatic
pressurization of the nucleus pulposus allows the intervertbral
disc
to support large loads which may be several times total body
weight.16 The majority of these loads are typically carried
through
the anterior column of the spine. However, as the nucleus
pulposus
degenerates, a large proportion of load transmission is shifted
to
the posterior elements and facet joints.13,17 This results in
increased
facet loading and degeneration as well as an increase in back
pain.
According to Buckwalter it appears that the degenerative
process
affects the nucleus pulposus and cartilage endplate more
sig-
nificantly than the anulus fibrosus with respect to changes
in
material properties.5, 17
Studies have shown that there also are changes in the
kinematics
of the discs as a result of varying degrees of degeneration.
The
relationships between the soft tissue laxity and changes in
kine-
matics of the lumbar spine were studied extensively by
Mimura,
Fujiwara, Krismer, and Frei.12-15
Despite the fact that there weremixed results from the studies,
an assessment of the general
trends suggests that segmental motion is increased and the
motion segment becomes more unstable in the earlier phases
of
degeneration when the anulus becomes slack. As degeneration
continues to more advanced stages, a re-stabilization seems
to
occur as disc space height is lost, the nucleus becomes more
fibrotic, and there is a net decrease in the flexibility.
Nucleus Arthroplasty technologies are emerging as an
alternative
early surgical treatment for patients with degenerative disc
dis-
ease. Removing the diseased disc nucleus and replacing it with
a
nuclear replacement device could improve and possibly
restore
the load bearing and kinematic properties of the degenerated
segment to a more physiologic level.19 Providing resistance
to
compressive loads while reducing segment instability may
help
ensure transmission of loads applied to the spine will be
pre-
dominantly maintained in the anterior column, thereby
unload-
ing the facet joints and decreasing pain.2 Also, by
maintaining
segment height and anular stability, the stimulation of the
free
nerve endings in the outer anulus may be minimized and
there-
fore decrease discogenic back pain. Biomechanical studies
evalu-
ating the kinematic restoration, axial load sharing,
endplate
mechanics and anular repair with Nucleus Arthroplasty repair
are discussed in more detail in the following chapters.
PROVIDING RESISTANCE TO COMPRESSIVE LOADS
WHILE REDUCING SEGMENT INSTABILITY MAY HELP
ENSURE TRANSMISSION OF LOADS APPLIED TO THE
SPINE WILL BE PREDOMINANTLY MAINTAINED IN THE
ANTERIOR COLUMN, THEREBY UNLOADING THE
FACET JOINTS AND DECREASING PAIN.
-
8/9/2019 Nucleus Arthroplasty Volume II
11/55
10
CONCLUSION
Taking into consideration the varying degrees of disc
degeneration
and the biomechanical changes that occur, one of the challenges
of
treatment becomes defining a point for surgical
intervention.
Considering the important biomechanical role of the nucleus
pul-posus, an attempt to restore or recreate the function of a
healthy
nucleus appears to be a target point for intervention.18
Patients who
are found to have early or mid-stage degenerative disc disease,
and
who show signs of progression of degeneration, are potential
can-
didates for nucleus replacement. Removing the damaged
nucleus
pulposus and replacing it with a Nucleus Arthroplasty device
to
restore the biomechanical properties of the given motion
segment
may be beneficial in breaking the degenerative cascade.
REFERENCES
1. White AA, Panjabi MM. Clinical Biomechanics of the Spine.
Philadelphia:
Lippincott Williams & Wilkins; 1990.
2. Goins ML, Wimberley DW, Yuan PS, Fitzhenry LN, Vaccaro AR.
Nucleus
pulposus replacement: an emerging technology. Spine J 2005
Nov-Dec;
5(6 Suppl):317S-24S.
3. Setton LA, Chen J. Mechanobiology of the intervertebral disc
and relevance to
disc degeneration. J Bone Joint Surg Am 2006 Apr;88 Suppl
2:52-7.
4. Buckwalter JA, Mow VC, Bowden SD, Eyre DR, Weidenbaum M.
Intervertebral
Disk Structure, Compostion, and Mechanical Function. In:
Buckwalter JA,
Ainhorn TA, Simon SR, editors. Orthopaedic Basic Science Biology
and
Biomechanics for the Musculoskeletal System. 2nd ed. Rosemont,
IL:
American Academy of Orthopaedic Surgeons; 2000. p.548.
5. Buckwalter JA, Boden SD, Eyre DR, Mow VC, Weidenbaum M.
IntervertebralDisk Aging, Degeneration, and Herniation. In:
Buckwalter JA, Ainhorn TA,
Simon SR, editors. Orthopaedic Basic Science Biology and
Biomechanics for
the Musculoskeletal System. 2nd ed. Rosemont, IL: American
Academy of
Orthopaedic Surgeons; 2000. p.558.
6. Kurowski P, Kubo A. The relationship of degeneration of the
intervertebral
disc to mechanical loading conditions on lumbar vertebrae. Spine
1986
Sep;11(7):726-31.
7. Rohlmann A, Zander T, Schmidt H, Wilke HJ, Bergmann G.
Analysis of the
influence of disc degeneration on the mechanical behaviour of a
lumbar
motion segment using the finite element method. J Biomech
2006;39(13):2484-90.
8. Kirkaldy-Willis WH, Wedge JH, Yong-Hing K, Reilly J.
Pathology and patho-
genesis of lumbar spondylosis and stenosis. Spine 1978
Dec;3(4):319-28.
9. Benneker LM, Heini PF, Anderson SE, Alini M, Ito K.
Correlation of radi-
ographic and MRI parameters to morphological and biochemical
assessment
of intervertebral disc degeneration. Eur Spine J 2005
Feb;14(1):27-35.
10. Kjaer P, Albert H, Jensen TS, Leboeuf-Yde C, Bendix T,
Wedderkopp N, et al.
Back pain, radiology and end plate changes by means of Modic.
Ugeskr
Laeger 2006 Apr 24;168(17):1668,9; author reply 1669.
11. Horst M, Brinckmann P. 1980 Volvo award in biomechanics.
Measurement of
the distribution of axial stress on the end plate of the
vertebral body. Spine
1981 May-Jun;6(3):217-32.
12. Mimura M, Panjabi MM, Oxland TR, Crisco JJ, Yamamoto I,
Vasavada A.
Disc degeneration affects the multidirectional flexibility of
the lumbar spine.
Spine 1994 Jun 15;19(12):1371-80.
13. Fujiwara A, Lim TH, An HS, Tanaka N, Jeon CH, Andersson GB,
et al. The
effect of disc degeneration and facet joint osteoarthritis on
the segmental
flexibility of the lumbar spine. Spine 2000 Dec
1;25(23):3036-44.
14. Krismer M, Haid C, Behensky H, Kapfinger P, Landauer F,
Rachbauer F.
Motion in lumbar functional spine units during side bending and
axial
rotation moments depending on the degree of degeneration. Spine
2000
Aug 15;25(16):2020-7.
15. Frei H, Oxland TR, Rathonyi GC, Nolte LP. The effect of
nucleotomy on
lumbar spine mechanics in compression and shear loading. Spine
2001
Oct 1;26(19):2080-9.
16. Johannessen W, Elliott DM. Effects of degeneration on the
biphasic material
properties of human nucleus pulposus in confined compression.
Spine 2005
Dec 15;30(24):E724-9.
17. Niosi CA, Oxland TR. Degenerative mechanics of the lumbar
spine. Spine J
2004 Nov-Dec;4(6 Suppl):202S-8S.
18. Di Martino A, Vaccaro AR, Lee JY, Denaro V, Lim MR. Nucleus
pulposus
replacement: basic science and indications for clinical use.
Spine 2005 Aug
15;30(16 Suppl):S16-22.
19. Le Huec JC, Aunoble S, Basso Y, Tournier C, Yamada K.
Biomechanical
Considerations for Total Lumbar Disk Replacement. In: Kim DH,
Cammisa
FP, Fessler RG, editors. Dynamic Reconstruction of the Spine.
Thieme
Medical Publishers; 2006. p.149.
CONSIDERING THE IMPORTANT BIOMECHANICAL ROLE OF THE NUCLEUS
PULPOSUS, AN ATTEMPT TO RESTORE OR RECREATE THE FUNCTION OF
A
HEALTHY NUCLEUS APPEARS TO BE A TARGET POINT FOR
INTERVENTION.
-
8/9/2019 Nucleus Arthroplasty Volume II
12/55
11
Chapter 8 Principles and MechanicalRequirements of Nucleus
Implant
Prof. Dr. Hans-Joachim Wilke
PROFESSSORInstitute of Orthopaedic Research and Biomechanics
University of Ulm
Ulm, Germany 89081
BASIC BIOMECHANICAL CONSIDERATIONS
N
on-fusion technologies in spinal surgery gain more and
more popularity. Constantly, new ideas are created and
turned into new products. Each idea has its own philosophy
with
the principle goal to maintain the motion in the treated
segment.
In contrast to total disc implants, nucleus implants are
designed
to preserve as many spinal structures as possible. These
implants
restore and maintain disc height and/or original mobility.
In many cases, disc degeneration or disc prolapse is treated
just by
nucleotomy and decompression; this can produce a good out-
come due to decom-
pression of the nerve
roots. However, in some
patients this treatment isinsufficient and back
pain recurs after a while.
This may be explained
by the nucleotomy,
which causes a reduc-
tion in disc height proportional to 0.8 mm/g removed
material.
Thus the average amount of removed nucleus material of 3 g
leads
to a height loss of 2.4 mm, which can be associated with an
THE AVERAGE AMOUNT OF REMOVED NUCLEUS MATERIAL
OF 3 G LEADS TO A HEIGHT LOSS OF 2.4 MM, WHICH CANBE ASSOCIATED
WITH AN INCREASE IN THE SEGMENTAL
RANGE OF MOTION OF ABOUT 20-30%, AND AN INCREASE
IN THE NEUTRAL ZONE OF UP TO 100%.
-
8/9/2019 Nucleus Arthroplasty Volume II
13/55
12
increase in the segmental range of motion of about 20-30%,
and
an increase in the neutral zone of up to 100%. This
instability
can lead to more stress in the remaining anulus and facet
joints
resulting in further degeneration. This height loss may also
be
associated with bulging of the anular ring leading to an
unphysi-
ological strain pattern in the anulus; this may affect the cells
in
these structures. Bulging of the disc is about 1mm per 1 kN
up
to 2.5 kN axial preload.1 It seems that this disc bulging is
slightly
higher anteriorly than posteriorly.2 The data suggests that
this
bulging may even increase further when the spine is bent.
This
effect sometimes is compared with a rather flat car tire
(this
problem is sometimes called flat-tire syndrome). Removing
the
disc from one side creates a slight asymmetry due to the
hole.
Finite element analysis suggests that the regions of the disc
that
show the largest bulging also show the highest strain. This
seems
to be the posterolateral region of the disc, where the strain
is
exaggerated after removal of the nucleus.
VARIOUS TYPES OF NUCLEUS DEVICES
The advantage of a nucleus prosthesis as compared to a total
disc prosthesis is that the nucleus device generally allows
the
preservation of the existing anatomical structures including
the anulus, vertebral endplates, and ligaments.
In theory, an optimum nucleus replacement should restore the
mobility and re-establish the intact disc height, thereby
restoring
the nominal stresses and strains of the collagen fibres in the
anu-
lus. This seems to be a superior situation as compared to
leaving
the disc alone after a discectomy.
The origin of the idea to replace the nucleus goes back to
the
1950s. The first idea was to fill the nuclear cavity with
polymethyl
methacrylate (PMMA) or silicone.3,4 Since that time a variety
of
solutions to replace the nucleus have been developed.5 This
pres-
ent article tries to classify the different ideas into the three
cate-
gories: mechanical nucleus devices, polymer implants, and
tissue
engineered nucleus implants.
Nucleus Implants
Polymer Tissue EngineeredMechanical
Steelball, Fernstrm
Regain, Biomet Inc.
IPD, Dynamic Spine
knitted titanium, Buck
Natural
ScaffoldsSyntheticScaffolds
Pre-FormedIn situ
Formed
Hydrogel Polyurethane
with jacket w/o jacket
Silicone Hydrogel Other
Material
ThermoResponsive
PolymerDual Disc cylinders,
Ray and Corbin
PDN, Raymedica, LLC
SaluDisc, Spine Medica
Aquarelle, Stryker
NeuDisc,Replication Medical, Inc.
Newcleus, Zimmer Spine
DASCOR, DiscDynamics Inc.
SINUX ANR, DePuy
NuCore, Spine Wave
BioDisc, CryoLife
PNR, TranS1
DiscCell, Gentis
PMMA, Hamby andGlaser
Collagen Gels Hyaluronic Acid
Fleece of PLA Textiles
PDN-SOLO, Raymedica, LLC
PDR, TranS1
NUBAC, Pioneer Surgical
CL-Disc, Interpore Cross
Gelifex SP/ IP,SYNTHES Inc.
with balloon w/o balloon
HydroFlex, Raymedica, LLC Figure 1Classification chart of the
different nucleus replacement devices.
-
8/9/2019 Nucleus Arthroplasty Volume II
14/55
13
MECHANICAL IMPLANTS
Fernstrm implanted the first mechanical nucleus replacement
device in 1966. This implant consisted of a stainless steel
ball
that was placed in the disc space.6 Clinically, it proved
unsuc-
cessful because the ball subsided into the endplates and
served
as a fusion device. Later, other mechanical devices were
devel-
oped that were made of less stiff materials and incorporated
a
larger contact area with the endplates. As an example,
Regain
(Biomet, Inc.) is made of one piece of highly-polished,
pyrolytic
carbon with a Youngs modulus similar to cortical bone.
NUBAC (Pioneer Surgical Technology) is a ball and socket
nucleus replacement device made of PEEK with tantalum mark-
ers. Other mechanical devices include the CL-Disc (Biomet,
Inc.) which is composed of solid, zirconia ceramic,
incorporat-
ing a porous titantium keel; and the IPD (Dynamic Spine)
that
consists of metallic springs and is fixed to the vertebrae.
The TranS1 PDR (Percutaneous Disc Reconstruction) can also
be considered as a mechanical device; this device allows a
sup-
ported nucleus or mechanical nucleus replacement. It has all
the
benefits of the PNR with an in situformed silicone absorber
(as
described later), and a metal-on-metal central pivot that
helps
share the load. The device is implanted using a TranS1
pre-sacral
axial approach to the lumbar spine. With the pre-sacral
approach,
the integrity of the anulus and ligaments is maintained, as are
any
future surgical options.
A new idea describes an implant made of knitted titanium
fila-
ments Buck (Germany), which provides the physiological
stiffness
and motion of a spinal segment and seems to have no
dislocation
tendency. All these mechanical implants require suturing the
anu-
lus after implantation.
POLYMER IMPLANTS
As the mechanical devices are often too stiff, many researchers
have
experimented with various polymers to create softer nucleus
implants. These softer nucleus implants are used as either
preformed
shapes or alternatively the shape is allowed to developin
situ.
Preformed
Hydrogel
Hydrogel is the most preferred material for preformed
nucleus
devices made of polymers. It has been demonstrated that
PVA(non-ionic hydrogel) has a similar swelling pressure
characteris-
tic of the natural nucleus. Due to their hydrophilic
characteristic
the hydrogels can swell. This means that they can be
implanted
in the dehydrated state through smaller channels in the
anulus.
After implantation the hydrogel increases in size; this can
reduce
the risk of expulsion.
In 1988, Charles Dean Ray, MD, FACS had the idea for a
nucleus
implant that consisted of a doppel woven spiral of flexible,
high-
tensile-strength polymeric fibers and tissue
ingrowth-promoting,
polyglycolic acid filaments. The cylinder contained a
viscous
hygroscopic semifluid. This resulted in the development of
the
prosthetic disc nucleus (PDN) device marketed by Raymedica,
LLC. In the first stages of development, the PDN device
consisted
of two parts, an anterior and posterior hydrogel pellet
comprised
of hydrolyzed poly-acrylonitrile polymer (Hypan), each
enclosed
in a woven polyethylene jacket. These were both oriented in
a
transverse position within the disc cavity. Once implanted,
the
hydrophilic hydrogel pellet absorbed fluid and increased in
volume
until restricted by the confines of the now tight,
polyethylene
jacket. The original intact disc height was restored after
implanta-
tion of the device. However, an effect from the hydration
could
not be measured.7 Because of a high expulsion rate, this
two-part
device was modified into a single, but bigger, implant
called
PDN-SOLO. The current version, the HydraFlex device, is a
softer, faster hydrating, more contoured device compared to
the
PDN-SOLO, and its preformed shape fits the endplate surface
geometry better with the goal to minimize the risk of
subsidence.
A hydrogel without a jacket was also used. The Aquarelle
(1998,
Stryker Spine) is made of a semihydrated poly-vinyl-alcohol
(PVA) hydrogel allowing 80% water content. This provides
vis-
coelastic properties similar to the nucleus. Unfortunately,
clinical
trails have demonstrated a high expulsion rate.
In 2000, Replication Medical presented the NeuDisc; a modi-
fied hydrolyzed poly-acrylonitrile polymer (Aquacryl) rein-
forced by a Dacron mesh. This anisotropic implant is able to
absorb up to 90% of its weight. It takes 18 hours to reach
full
size in laboratory testing.
Another hydrogel implant called SaluDisc (Spine Medica)
is made of Salubria. This material contains water in similar
proportions to human tissue.
THE FIRST MECHANICAL NUCLEUS IMPLANT
WAS SUGGESTED IN 1966 BY FERNSTRM WHO
IMPLANTED A STAINLESS STEEL BALL AS A
SPACER INTO THE DISC.
-
8/9/2019 Nucleus Arthroplasty Volume II
15/55
14
Polyurethane
Polycarbonate urethane (PCU) was used for the Newcleus
(Zimmer Spine) in 2003. This consisted of a preformed spiral
which allowed implantation using a minimally invasive tech-
nique. The implant material was able to absorb water up to
35% of its own weight. Functionally, it acted as a spacer
with
some shock-absorbing capabilities.
In situ formed
Manyin situformed nucleus prostheses have been tried out
since
the first attempt by Nachemson in the early 1960s. The concept
is
to inject a curable polymer into the nuclear space. The
advantage
of anin situformed nucleus replacement is that it can be
injected
non-invasively using a small needle. It is hoped that this type
of
implant will be at a low risk for expulsion. In contrast to the
pre-
formed implants, which are implanted into the cavity and can
increase disc height, the injectable polymers cannot be
injected
with enough pressure to increase disc height.
It has yet to be proved that in situcured polymer can provide
enough
mechanical strength to support the applied load plus have
the
required mechanicalin vivofatigue life. One potential
disadvantage
ofin situformed devices is toxicity due to unreacted
monomers.
Therefore, forin situformed devices, the polymerization
process
is critical to ensure long-term biocompatability.
Thermo responsive polymer
One product that is injected as anin situformed material is
DASCOR (Disc Dynamics). The material, a cool polyurethane
polymer (18 C), is injected under pressure into a
polyurethaneballoon through an attached catheter. It takes a
minimum of 12
to 15 minutes to solidifyin situ.
Another thermo-responsive polymer is poly
(N-isopropylacrylamide)
or PNIPAAm, although specific details are not yet available.
A polymer-based hydrogel which is liquid at room temperature
is used for the Gelifex (SYNTHES). This implant looks like a
porous rubber ball after solidification at body temperature.
Silicone
A silicone-based artificial nucleus replacement SINUX ANR
(SiniTech AG, Depuy Spine) is made of a liquid
polymethylsilox-
ane (PMSO) polymer. This is also injected into the void of
the
disc and curesin situin approximately 15 minutes.
TranS1 PNR (Percutaneous Nucleus Replacement) is an in situ
formed nucleus replacement technology. The nucleotomy and
device implantation is completed using the trans-sacral
axial
approach to the lumbar spine, preserving the anulus and
liga-
ments. A hollow screw is threaded axially providing
distraction
of the disc space. Silicone is injected through the screw to
fill
the created cavity and help maintain motion.
Hydrogel
Severalin situcurable hydrogel implants are currently under
development. The Biodisc (CryoLife) is a protein hydrogel
device (PHD), which cures in 2 minutes after injection into
the
disc space. The properties are supposedly similar to the
human
nucleus and there is no exothermic reaction during the
harden-
ing process. The material is similar to epoxy glue and bonds
to
the anulus, which hopefully reduces the expulsion risk.
The NuCore Nucleus Device (Spine Wave) is based on a
hydrogel composed of synthetic silk-elastin copolymer. This
material has no measurable exothermic reaction.
Other Polymers
In 1959, Hamy and Glaser suggested injecting PMMA into the
disc. PMMA, which is commonly used as bone cement, cures
with
a high exothermic reaction. This is a cheap procedure and
was
often used clinically, particularly by neurosurgeons in
Germany.
Anotherin situcured nucleus implant is the DiscCell
(Gentis).
This is anin situpolymerising material that is injected into
the
disc space. Little information is available at the present
time.
Tissue Engineered Implants
Recently, it has been shown that seeding or reinserting cells
inside
the intervertebral disc may preserve disc structures by
slowing
down the degeneration processes.8,9 It was also hypothesized
that the
inserted cells might restore the anulus and nucleus tissue.
These cell
injection methods could not produce a restoration of disc
height.
MANY IN SITUFORMED NUCLEUS PROSTHESES HAVE
BEEN TRIED OUT SINCE THE FIRST ATTEMPT BY
NACHEMSON IN THE EARLY 1960S. THE CONCEPT IS TO
INJECT A CURABLE POLYMER INTO THE NUCLEAR SPACE.
-
8/9/2019 Nucleus Arthroplasty Volume II
16/55
15
The idea of a tissue-engineered nucleus implant is to seed
cells
in a three-dimensional matrix. This matrix would serve as a
scaf-
fold to produce a structure of mechanical stiffness and
adequate
mechanical properties. The seeded cells could be
intervertebral
disc cells or mesenchymal progentitor cells (MPCs).
Natural Scaffolds
Nucleus scaffolds can be produced from natural materials
such
as collagen or hyaluronic acid. A recent study presented a
three-
dimensional collagen-I matrix made of rat-tail collagen (ARS
Arthro, AG, Esslingen, Germany) that might be suitable to
serve
as scaffold for cell seeding and eventual nucleus
replacement.10
The problems of restoring disc height and implant expulsion
using a tissue-engineered nucleus have yet to be solved.11
Scaffolds
made of hyaluronic acid could be utilized, although the
implant
might degrade after regeneration of the disc.
Natural material composites are currently being developed
for
use as nucleus scaffolds. In any case, it is questionable
whether
a natural scaffold would be sufficiently load-bearing.
Synthetic Scaffolds
Better load-bearing characteristics may be obtained with
synthetic
materials, which may be fabricated of fleece or other
combina-
tions of textiles. Because of a higher density and stiffness,
they
might be introduced into the disc space and further
compressed
to increase the stiffness, allowing more volume to be
inserted.
Such approaches are currently under study at universities in
Dresden, Heidelberg and Ulm.
PRECLINICAL MECHANICAL AND BIOMECHANICAL
TESTING OF NUCLEUS DEVICES
Before being put into clinical practice, nucleus implants and
the
surgical approaches for implantation should be tested. Some
of the new biological solutions may not be testable in all
test
configurations. Nevertheless, the following principles are
suggested in order to compare the different nucleus devices.
Mechanical tests
Static tests
Prior to any implantation, mechanical tests on the implant
mustbe carried out to ensure that the implant can sustain certain
loads
and has sufficient fatigue life. For example, static loads are
used to
determine the stiffness and the yield point of the implant.
Dynamic tests
Dynamic loads at a rate of 4 Hz or less are necessary to
prove
that the implants are able to withstand at least 10,000,000
cycles
without collapsing, disconnecting, or deforming permanently.
They also may be used as wear tests to determine how much
and
what kind of debris are produced under expectedin vivoloads
and motions.
These mechanical tests should be performed between two
polyac-
etal or equivalent test blocks. The test blocks will eliminate
the
effects of the variability of bone properties and morphology for
the
fatigue tests. These tests should be performed in a defined
testing
environment (e.g. in a 0.9% saline environmental bath at
37C).
Other tests such as hydrating tests may also be important
with
implants made of hydrogel.
Biomechanical tests
Functional in vitro flexibility tests
In contrast to the pure mechanical tests, another category of
tests
with the goal to determine thein situperformance is
flexibility
tests. These are ideally performed using human cadaveric
spine
specimens. These tests require mechanical testing machines
that
allow loads that simulate the physiological motion of the
specimens
with the implants in place.
TH E ID EA OF A T IS S U E- ENGINEERED NU C L EU S IM PL A NT IS
TO S EED C EL L S
IN A TH REE- D IM ENS IONA L M A TRIX. TH IS M A TRIX W OU L D S
ERVE A S A
S C A FFOL D TO PROD U C E A S TRU C TU RE OF M EC H A NIC A L S
TIFFNES S A ND
A D EQU ATE M EC H A NIC A L PROPERTIES .
-
8/9/2019 Nucleus Arthroplasty Volume II
17/55
16
They should be carried out in flexion/extension, lateral
bending,
and axial rotation. It is recommended for standardization
that
they are tested under pure moments without preload.12
Eventually,
tests under shear loading, compression, muscle forces, and
other
representativein vivoloads should also be carried out. To
decidethe best approach in a given clinical situation, in
vitroevaluation
involving intact, nucletomized, or degenerated specimens with
the
device implanted provide the most realistic option.
The parameters which should be determined are the range of
motion and the neutral zone in the different motion planes,
shear
translations, and height changes. These parameters, however,
do
not represent the full information about the kinematics.
Therefore,
the center of rotation or helical axis could also be important
infor-
mation about the load sharing between the different structures
of
the spinal segment.
Additional biomechanical tests
A hard implant leads to a high stress concentration on the
end-
plate (seen as Modic changes) which may lead to remodeling,
subsidence, or even to failure of the endplate, particularly
with
poor bone quality. For this reason, other specific set-ups may
be
required to determine the endplate deformations.
One of the goals of nucleus replacement is to re-establish
the
physiological strain on the anulus, which is assumed to be one
of
the prerequisites in order to maintain healthy tissue. This may
beindirectly determined by comparing the bulging of the intact,
nucleotomized, treated disc.
In vitro test with cyclic loading
Depending on the type of device, expulsion or subsidence of
the
implant may be a problem. In order to evaluate these types
of
biomechanical failures the specimens should be subjected to
cyclic loading as well. Because of degradation of the
cadaveric
tissue the testing time may be limited. Thus 100,000 cycles
with
possibly exaggerated loads should at least be attempted.
Following this cyclic test or several times during the test
secondary
stability tests should be performed as described above.12
Animal experiments
In addition to the tests described above, animal experiments
may
be useful to evaluate the efficacy and reliability of
nucleus
implants. However, the ability to design a scaled version for
ani-
mal implantation, coupled with the validity of the available
ani-
mal species, has potential limitations for extrapolating
expected
human performance.
CONCLUSION
Nucleus replacement is an exciting technology and may be a
promising alternative to other non-fusion technologies. Many
different ideas are available or in the development stages.
Besides
the mechanical challenges presented to the implant, the
implant
has to re-establish the physiological biomechanics of a
spinal
segment, plus remain in the disc space and not expulse or
sub-
side through the endplate. However, the ultimate judge of
the
implant is not the biomechanical data, but the clinical
outcome.
REFERENCES
1. Stokes, I. A. (1988). Bulging of lumbar intervertebral discs:
non-contacting
measurements of anatomical specimens. J Spinal Disord 1(3):
189-93.
2. Brinckmann, P. (1986). Injury of the anulus fibrosus and disc
protrusions. An
in vitroinvestigation on human lumbar discs. Spine 11(2):
149-53.
3. Hamby, W. B. and H. T. Glaser (1959). Replacement of spinal
intervertebral disc
with locally polymerizing methyl methacrylate: experimental
study of effectsupon tissues and report of a small clinical series.
J Neurosurg 16(3): 311-3.
4. Nachemson, A. (1962). Some mechanical properties of the
lumbar interverte-
bral discs. Bull Hosp Joint Dis 23: 130-43.
5. Carl, A., E. Ledet, et al. (2004).New developments in nucleus
pulposus
replacement technology. Spine J 4(6 Suppl): 325S-329S.
6. Fernstrm, U. (1966). Arthroplasty with intercorporal
endoprothesis in
herniated disc and in painful disc. Acta Chir Scand Suppl 357:
154-9.
7. Wilke, H. J., S. Kavanagh, et al. (2001). Effect of a
prosthetic disc nucleus on
the mobility and disc height of the L4-5 intervertebral disc
postnucleotomy.
J Neurosurg 95(2 Suppl): 208-14.
8. Nishimura, K. and J. Mochida (1998). Percutaneous reinsertion
of the nucleu
pulposus. An experimental study. Spine 23(14): 1531-8;
discussion 1539.9. Okuma, M., J. Mochida, et al. (2000).
Reinsertion of stimulated nucleus pul-
posus cells retards intervertebral disc degeneration: an in
vitroand in vivo
experimental study. J Orthop Res 18(6): 988-97.
10. Neidlinger-Wilke, C., K. Wurtz, et al. (2005).A
three-dimensional collagen
matrix as a suitable culture system for the comparison of cyclic
strain and hydro-
static pressure effects on intervertebral disc cells.J Neurosurg
Spine 2(4): 457-65
11. Wilke, H. J., F. Heuer, et al. (2006). Is a collagen
scaffold for a tissue engi-
neered nucleus replacement capable of restoring disc height and
stability in
an animal model? Eur Spine J 15 Suppl 3: S433-8.
12. Wilke, H.-J., K. Wenger, et al. (1998). Testing Criteria for
Spinal Implants:
Recommendations for the Standardization ofIn VitroStability
Testing of
Spinal Implants. European Spine Journal 7: 148-154.
-
8/9/2019 Nucleus Arthroplasty Volume II
18/55
Chapter 9 Kinematic Demands ofNucleus ArthroplastyTechnolog
Denis J. DiAngelo, PhD
ASSOCIATE PROFESSORDepartment of Biomedical Engineering and
Imaging
The University of Tennessee Health Science Center
Memphis, TN 38138
Brian P. Kelly, PhDASSISTANT PROFESSOR
Department of Biomedical Engineering and Imaging
The University of Tennessee Health Science Center
Memphis, TN 38138
17
KEY POINTS
The instantaneous axis of rotation (IAR) is an important
factor
of spinal segment kinematics; however, there is no consensus
on
where the IAR of the lumbar disc is during
flexion/extension.
Alignment of device IAR and spinal segment IAR is important
for
optimal performance of interbody motion preservation
devices.
Previous testing of non-compliant interbody motion technolo-
gies demonstrated non-concentric IARs may lead to an over
constrained condition, resulting in failure of the device to
provide adequate motion restoration. Compliant nucleus
replacement technologies do not have a pre-
scribed axis of rotation. A new test methodology is proposed
for
evaluating the kinematic restorative effect for such
devices.
-
8/9/2019 Nucleus Arthroplasty Volume II
19/55
DEFINITIONS AND TERMINOLOGY
Kinematics:describes the movement between two rigid bodieswith
no consideration to the forces involved. Movement of a
body can be described in Cartesian coordinates as having
three
orthogonal translations and three rotations about each
transla-
tional axis. The motion can be described in two-dimensions
(2D) or three dimensions (3D). For 2D motion, two
translations
and one rotation are required. Additional kinematic
parameters
can be calculated that describe motion and include the center
of
rotation (CR) in 2D, the helical axis of motion (HAM) in 3D,
or
their instantaneous components (ICR or IHAM).
Stiffness (inverse of flexibility):the ability of a structure
todeform per unit displacement. The typical load-displacement
curve for spinal MSU displays a non-linear relationship
having
two different regions: a low load region and a high load
region
(Figure 1). As tissue is exposed to increasing
displacements,
stiffness is greatly increased and small changes in
displacement
induce large load responses.
Coordinate System:a reference system used to define the
posi-tion and orientation of a body in space or relative to another
body.
Motion Segment Unit (MSU):two adjacent vertebrae
andinterconnecting disc and surrounding ligamentous tissues.
Intervertebral Disc:an inner nucleus pulposus core surroundedby
an anulus fibrosus tissue.
NUCLEUS ARTHROPLASTY DESIGNS
Various types of nucleus arthroplasty (NA) devices exist
which
can be categorized into three groups: Void fillers (NuCore,
Spine
Wave; BioDisc, CryoLife), kinematically-constrained
mechanical
devices (NUBAC, Pioneer; Regain, Biomet), and load sharing
devices (HydraFlex, Raymedica, LLC; NeuDisc, Replication
Medical; DASCOR, Disc Dynamics).1, 2, 3 Further, each device
has
an associated surgical procedure for preparing the nucleus
site
and placing the NA device that alters the physical properties
of
the treated spinal level. Hence, in addition to studying the
biome-
chanical properties and function of NA devices, one should
also
understand the impact that the various surgical techniques
have
on the stability and function of the treated disc. The influence
of
these techniques include facet disruption, bony removal, the
sur-
gical approach (anterior versus posterior), affect of an
annular
incision (which depressurizes the nucleus), and the amount
of
nucleus material removal: micro (associated with
discectomies)
or complete. All of these incremental surgical alterations
intro-
duce different degrees of instability to the spinal joint that
must
be compensated for by the NA device itself.
HOW TO STUDY THE KINEMATICS
OF NUCLEUS ARTHROPLASTY
The nucleus pulposus is a pressurized gelatinous region
consist-
ing of proteoglycans (glycosaminoglycans), loose Type II
colla-gen fibrils, mineral salts, and water that is surrounded by
an
anulus fibrosus structure. Together, the nucleus and anulus
dis-
play nonlinear material properties that influence the
biomechanics
of a spinal MSU. The goal of nucleus arthroplasty is to restore
the
compliant function of the disc and spinal MSU and prevent
over-
loading of the adjacent bony and soft tissue structures.
The design rationale for nucleus arthroplasty differs from that
of
total disc arthroplasty. Total disc arthroplasty devices are
non-
compliant devices designed to restore motion to the
degenerative
disc. However, there is no consensus on where the IAR of the
lum
bar disc is during flexion/extension activities, with various
loca-
tions reported in the literature. Since most total disc
replacement
devices (TDR) are mechanical joints, if the IAR of the device
does
not coincide with that of the native spine an over constrained
con-
dition within the MSU may occur, leading to overloading of
adja-
cent structures or failure to provide adequate motion
restoration.4
The goal of nucleus arthroplasty is to restore the compliancy of
the
native intervertebral disc and recreate a flexible load bearing
MSU
STIFFNESS
Displacement
Load
Low Load High Load
18
Figure 1Typical stiffness curve. The curve is generally
nonlinear and has
two regions: a low load region and a high load region.
AS TISSUE IS EXPOSED TO INCREASING DISPLACEMENTS,STIFFNESS IS
GREATLY INCREASED AND SMALL CHANGES
IN DISPLACEMENT INDUCE LARGE LOAD RESPONSES.
-
8/9/2019 Nucleus Arthroplasty Volume II
20/55
19
system. A more flexible system serves to reduce the occurrence
of
an over constrained, non-mobile condition. Moreover, if the
IAR
of the MSU varies, the NA device may dynamically deform to
accommodate the positional changes. An improved method for
evaluating nucleus arthroplasty devices and their ability to
restoresegment compliancy and motion is to impose a series of
different
kinematic motion profiles and measure their reaction loads.
The
different motion profiles force the implanted MSU to adjust to
the
prescribed kinematic pattern since the axes of rotation would
be
selected such that they are not co-centric with the disc
center.
Thus, the reactive forces needed to follow the prescribed
motion
represent how well the NA device performs. This chapter
discusses
a new approach for studyingin vitro, the capacity of nucleus
arthroplasty to restore the kinematic of a spinal MSU in a
human
cadaveric model. This new testing methodology is a paradigm
shift
from the conventional displacement or load control methods.5
CURRENT BIOMECHANICAL TESTING METHODS
Limited biomechanical studies exist that evaluate NA
devices.
Although the conventional testing method of applying a pure
or
constant bending moment across the spinal construct and
meas-
uring the motion response to that loading condition can be
done, there are significant limitations with this testing
method-
ology. Physiologically, the spine is not loaded with a
constant
bending moment, but rather experiences a moment distribution
that varies across all spinal levels as you go down the
spine.
Although pure moment methods provide a standard approach
for comparing different lumbar spinal devices and may be
acceptable for testing fusion instrumentation,5 it is not well
suited
for studying any type of spinal device that permits motion
and/or
has a variable stiffness or modulus (i.e., is not a rigid metal
struc-
ture). Alternatively, eccentric compressive load test methods
havebeen used to study both fusion and non-fusion spinal
instrumen-
tation.6 A compressive load is typically applied eccentric to
the
long axis of the spine causing the spine to flex or extend
under
a combined compressive load and bending moment. Using this
testing method, a more physiologic response in the
rotational
involvement of each MSU occurs throughout the lumbar spine
(Figure 2).7, 8, 9, 10 However, even though the eccentric
loading
method induces a physiologic rotational response across the
intact lumbar spine, this method may not have the sensitivity
to
study the compliant properties and kinematic requirements of
NA devices or different disc conditions. With either load
controlor displacement control methods limited information is
available
about the loads acting on the disc and/or NA device, or the
amount of load sharing that occurs between the NA and
adjacent
supporting structures as the MSU moves through a functional
range of motion.
NEW KINEMATIC TESTING PROTOCOL FOR
STUDYING COMPLIANT STRUCTURES
Human joints move under a state of minimum energy; they fol-
low the path of least resistance. A new testing protocol is
pro-
posed that involves prescribing a known kinematic input to a
spinal MSU and measuring the capacity of the intact MSU to
accommodate the motion. The effects of changing the MSU
properties via surgery (nucleotomy) or placement of a
nucleus
arthroplasty device, changes the effort or work required to
move
the altered spine condition through a prescribed motion path
relative to the intact spine condition. The closer the
loading
mechanics of the altered spine are to the intact spine
condition,
the better the likelihood the device will restore the native
prop-
erties. Further, the kinematic path can be a simple rotation
about
a fixed point in space, or a coupled movement (displacement
and
rotation) along a path.
Combined MSU Flexion/ExtensionRotation of the Lumbar Spine
0 5 10 15 20
L1-L2
L2-L3
L3-L4
L4-L5
L5-S1
MotionS
egmentUnitLevel
Range of Rotation (Degrees)
In Vitro
In Vivo (4 sources*)
Figure 2In VitroversusIn VivoMSU rotations of the lumbar spine.
6, 7, 8, 9
-
8/9/2019 Nucleus Arthroplasty Volume II
21/55
A custom-designed spine robot (Figure 3) was used that
consisted
of four programmable degrees of freedom that can each be
inde-
pendently operated under displacement control, force
feedback
control, and combinations thereof.11 Using the spine robot,
the
kinematic profile of an intact MSU can be programmed to
follow
a specified path or to rotate about a fixed point in space
(Figure
4). More advanced kinematic analyses are possible that map
out
the motion response to a given multi-directional force
profile.
A preliminary series of kinematic tests were performed on
the
spine robot to study the flexion and extension mechanics of
three
lumbar MSUs. Each specimen was tested in three different
spine
conditions: the intact harvested condition, post-nucleotomy
con-
dition, and post-implanted nucleus arthroplasty condition.
The
hydrated HydraFlex device (Raymedica, LLC) was used for the
implanted condition. The orientation of each MSU in a
neutral
alignment was measured on a radiograph (Figure 5A) and used
to establish the orientation of the MSU (Figure 5B) when
mounted
in the spine robot (Figure 5C). The MSUs were tested under
three
fixed points of rotation along the center line of the disc in
the ante-
rior-posterior (A-P) direction: 1) the mid point of the disc
(C), 2)
half way between the mid-point and anterior aspect of the
disc
(A), and 3) half way between the mid-point and posterior aspect
o
the disc (P) (Figure 5B). The MSUs were rotated about the
desig-
nated fixed points of rotation until a target bending moment
of
8Nm of flexionextension was reached or the shear or compres-
sive forces exceeded 400N. For all test conditions, MSU axial
force
(+Fz net MSU tissue tension, -Fz net MSU tissue compres-sion),
A-P shear force (+Fx net MSU posterior shear, -Fx net
MSU anterior shear), sagittal rotation (+y flexion, -y
extension)
and sagittal bending moment were measured and compared using
a one-way ANOVA (P=0.05).
20
Figure 3Programmable
multi-axis
Spine Robot.
Figure 4Schematic of the
Spine Robot used
to move a verte-
bral body about a
fixed center of
rotation relative
to an adjacent
vertebral body.
Figure 5A) Radiograph showing neutral
alignment of lumbar spine MSU.
B) Maintenance of neutral align-
ment of MSU in mounting potsand location of fixed points of
rotation. C) Potted MSU specimen
mounted in Spine Robot.
A B C
-
8/9/2019 Nucleus Arthroplasty Volume II
22/55
21
PRELIMINARY FINDINGS USING KINEMATIC
TESTING PROTOCOL
The mean values of the axial load, shear force, and MSU
rotation
for the three different fixed axes of rotation conditions were
cal-
culated and graphed (Figure 6). Using data for the
harvestedspine condition, significant differences in the MSU
rotation, axial
force, and shear force values occurred between the three
different
points of rotation (P, C, A). MSU rotations were significantly
dif-
ferent between all points of rotation in flexion and
extension,
except between points C and P in flexion. The axial forces
were
significantly different between P versus A and P versus C in
flex-
ion. A similar trend occurred with the axial force values
during
extension but the differences were not significant (likely due
to
the small sample size). Shear forces were significantly
different
between points P versus A and P versus C during flexion. In
extension the shear forces were significantly different between
all
points of rotation (P versus A, P versus C, and A versus C).
In
general, for the harvested intact MSU, when rotated in
flexion
about the mid-point of the disc (location C), MSU posterior
soft
tissue tension and resistance to posterior directed shear
provided
the stabilization effect. When the point of rotation was
shifted
posterior (location P), MSU anterior tissue compression and
resistance to anterior directed shear provided the
stabilization
effect. Shifting the rotation point anterior (location A) had
mini-
mal effect on tissue stabilization response, but decreased
seg-
mental rotation compared to point C. The data demonstrates
that the point about which a single MSU is rotated has a
signifi-
cant effect on the rotational range of motion as well as the
soft
tissue stabilization response.
Compressive Force (Fz): Flexion
-350
-250
-150
-50
50
150
250
Harvested Nucleotomy Implant
Spine Conditions
For
ce A
CP
Compressive Force (Fz): Extension
-350
-250
-150
-50
50
150
250
Harvested Nucleotomy Implant
Spine Conditions
For
ce
A
CP
Shear Force (Fx): Flexion
-250
-200-150
-100
-50
0
50
100
Harvested Nucleotomy Implant
Spine Conditions
Force
A
C
P
Shear Force (Fx): Extension
-250
-200-150
-100
-50
0
50
100
Harvested Nucleotomy Implant
Spine Conditions
A
C
P
-8
-3
2
7
12
Harvested Nucleotomy Implant
Spine Conditions
Degrees
DegreesA
C
P
-8
-3
2
7
12
Harvested Nucleotomy Implant
Spine Conditions
A
C
P
Rotation (0y) Flexion Rotation (0y) Extension
Figure 6Comparison of the three fixed points of rotations. Mean
values of the axial compressive load, A-P shear force, and MSU
rotation
during flexion and extension.
-
8/9/2019 Nucleus Arthroplasty Volume II
23/55
Compressive Force (Fz): Flexion
-350
-250
-150
-50
50
150
250
A C P
Point of Rotation
Harvested
NucleotomyImplant
Compressive Force (Fz): Extension
-350
-250
-150
-50
50
150
250
A C P
Point of Rotation
Harvested
NucleotomyImplant
Shear Force (Fx): Flexion
-250
-200
-150
-100
-50
0
50
100
A C P
Point of Rotation
Harvested
Nucleotomy
Implant
Shear Force (Fx): Extension
-250
-200
-150
-100
-50
0
50
100
A C P
Point of Rotation
Harvested
Nucleotomy
Implant
-8
-6-4-202468
101214
A C P
Point of Rotation
Harvested
Nucleotomy
Implant
-8
-6-4-202468
101214
A C P
Point of Rotation
Harvested
Nucleotomy
ImplantDegrees
Degrees
Force
Force
For
ce
Force
Rotation (0y) Flexion Rotation (0y) Extension
22
When comparing between the different spine conditions (har-
vested, nucleotomy, and implanted) there was a trend in the
data
that demonstrated the nucleotomy increased the MSU rotation,
altered the load response and appears to have more variation
in
response (e.g. less stable). Following implantation of the
HydraFlex device, the MSU rotation returned to the harvested
condition and had less variation compared to the denucleated
condition (Figure 7). Alterations to the harvested MSU via
the
nucleotomy or NA implant tended to reduce/lessen the A-P
shear forces, with the denucleated condition having a large
varia-
tion. At posterior point P, the denucleated and implanted
states
demonstrated less tissue compression. In extension, the
implant
condition tended to reduce the compressive response of the
posterior elements at Point C and P.
In general, for all test conditions, the rotational range of
motion
and the tissue loading response differed depending on the
selected
kinematic axis of rotation (point C, P or A). Denucleating
the
MSU led to more rotation and increased variation in the test
data,
indicative of a less stable/predictable response. After
implantation
of a hydrated HydraFlex device, variation was reduced and
the
response profile trended more towards the intact state for all
test
points. However, the small sample size and large variation
noted
in the denucleated specimens may have limited significance
from
occurring. Increasing the sample size should further confirm
sig-
nificant differences between the spine conditions or points
of
rotation, but the test method utilized demonstrates the
impor-
tance of understanding the constraints of a test setup and
how
results may vary as the constraints are changed.
Figure 7Comparison of the three different spine conditions at
specific points of rotations. Mean values of the axial compressive
load, A-P shear
force, and MSU rotation during flexion and extension.
-
8/9/2019 Nucleus Arthroplasty Volume II
24/55
23
CONCLUSION
As new technologies evolve, the methods utilized to analyze
their biomechanical performance must evolve. The preliminary
data from this study demonstrated that utilizing a robot to
change the location of the MSU axis of rotation had an
effect
on the kinematic response of the harvested, denucleated and
implanted MSU. Since thein vivoMSU axis of rotation is not
believed to be a single point of rotation and since
compliant
nucleus replacement technologies do not have a prescribed
axis
of rotation, evaluating the kinematic response at multiple
loca-
tions of rotation may more effectively characterize the
restora-
tive effect of these technologies compared to more
traditional
test methods. Additional testing is being performed to
furtherevaluate the utility of this method as well as evaluating
the
restorative effect of the implant on a path that matches the
nat-
ural motion of the MSU. Overall, this method looks very
prom-
ising for thoroughly understanding the kinematic response of
Nucleus Arthroplasty technologies.
ACKNOWLEDGMENT
Elizabeth Sander and Nephi Zufelt for assistance with the
bio-
mechanical tests and data processing.
REFERENCES
1. Davis R. J., and Girardi F. (eds.) 2006. Nucleus Arthroplasty
in Spinal Care:
Book 1 Fundamentals. Minneapolis (MN): Raymedica, LLC.
2. Di Martino A., Vaccaro A., Lee J., et al. Nucleus pulposus
replacement: basic
science and indications for clinical use. Spine. 2005;30 (suppl
16):16-22.
3. Klara P., Ray C. Artificial nucleus replacement: clinical
experience. Spine.
2002;27:1374-77.
4. DiAngelo DJ, Foley KT, Morrow B, Kiehm KJ, Gilmour L, The
Effects of Over-
Sizing of a Disc Prosthesis on Spine Biomechanics, Proceedings
of the Sixth
Annual Spine Arthroplasty Society Meeting, 2006.
5. Goel VK, Wilder DG, Pope MH, and Edwards WT. Biomechanical
testing of
the spine. Load controlled versus displacement-controlled
analysis. Spine
1995;20:2354-7.
6. DiAngelo DJ, Scifert JL, Kitchel S, Cornwall GB, McVay BJ,
Bioabsorbable
Anterior Lumbar Plate Fixation in Conjunction with Cage Assisted
AnteriorInterbody Fusion, J Neurosurg. Nov;97(4 Suppl):447-55,
2002.
7. Dvorak J., Panjabi M.M., Chang D.G., et al. Functional
radiographic diag-
nosis of the lumbar spine: flexion/extension and lateral
bending. Spine 16
(5):562-71, 1989.
8. Pearcy M.J., Portek I., and Shepherd J.. Three-dimensional
x-ray analysis of
normal movement in the lumbar spine. Spine 9 (3):294, 1984.
9. Froning E.C. and Frohman B. Motion of the lumbosacral spine
after laminec-
tomy and spine fusion: Correlation of motion with the result.
Journal of Bone
and Joint Surgery 50-A (5):897-918, 1968.
10. White A.A. and Panjabi M.M. Clinical biomechanics of the
spine,
Philadelphia:J.B. Lippincott Co., 1990.
11. Kelly BP, DiAngelo DJ, Foley KT, Design Of A Multi-Axis
Programmable
Spine Robot For The Study Of Multi-Body Spinal Biomechanics,
Proceedingsof the 32th Annual Meeting of the Cervical Spine
Research Society, Dec. 2004.
AS NEW TECHNOLOGIES EVOLVE, THE METHODS UTILIZED TO ANALYZE
THEIR
BIOMECHANICAL PERFORMANCE MUST EVOLVE. THE PRELIMINARY DATA FROM
THIS
STUDY DEMONSTRATED THAT UTILIZING A ROBOT TO CHANGE THE LOCATION
OF
THE MSU AXIS OF ROTATION HAD AN EFFECT ON THE KINEMATIC RESPONSE
OF
THE HARVESTED, DENUCLEATED AND IMPLANTED MSU.
-
8/9/2019 Nucleus Arthroplasty Volume II
25/55
24
Chapter 10 Device Stiffness vs.Load-Sharing with
NucleusArthroplastyDevices
Brian P. Beaubien, BME, MS
LEAD ENGINEERMidwest Orthopaedic Research Foundation
and the Gustilo Medical Education Center
Minneapolis, MN 55415
Andrew L. Freeman, BME, MSLEAD ENGINEER
Midwest Orthopaedic Research Foundation
and the Gustilo Medical Education Center
Minneapolis, MN 55415
KEY POINTS
The engineering term elastic modulus is used to characterize
the uni-axial stress-strain response of linear-elastic
materials.
Biologic tissues and advanced polymeric biomaterials are
typically
not linear-elastic and the stress-strain relationship is
complex.
Physiologic interactions significantly impact the response
char-
acteristics of devices made from advanced biomaterials.
Cadaver evaluation of polymeric devices demonstrated differ-
ences in the compressive load transfer through a device based
on
bulk device properties (i.e. device modulus) as well as changes
in
the level of constraint provided by physiologic tissue.
It is proposed that device design differences, as well as
physiologic
interactions, require characterization of a Nucleus
Arthroplasty
devices load-sharing properties in simulated use conditions,
which provides a more thorough characterization of
performance
with increased clinical understanding.
-
8/9/2019 Nucleus Arthroplasty Volume II
26/55
25
INTRODUCTION
The engineering term modulus is perhaps the most widelyused
descriptor of the mechanical properties of a material.For the most
basic conditions and materials, the modulus simply
relates the amount of stress and strain seen in a material and
is
useful in predicting and describing the load-deformation
behav-
ior. However, with biological tissues and advanced
biomaterials
the stress-strain response is more complex and is dependent
on
the surrounding environment. This chapter aims to highlight
important considerations in describing the stress-strain
relation-
ship of tissues and biomaterials and to discuss the effects of
these
properties, implant design and spine mechanics on thein
vitro
performance of the native nucleus pulposus, anulus fibrosus
and
Nucleus Arthroplasty (NA) devices.
MATERIAL PROPERTIES:
DEFINITIONS AND EXAMPLES
The modulus of elasticity (E)
The modulus of elasticity is used in Hookes Law (Robert
Hooke, 1635-1703) to describe a linear relationship between
stress and strain:
In this equation, stress (, force per unit area) and strain (,
elon-
gation per unit length) are linearly related by the modulus
of
elasticity (E), which is often called the elastic modulus or
Youngs
Modulus (Thomas Young, 1773-1829). The elastic modulus is
measured in the linear region of the stress-strain curve and
represents the slope of the curve. Each material generally has a
unique
elastic modulus (Figure 1). In general, a low modulus equates
to
a softer, more easily deformable material.
The elastic modulus provides a simple but powerful
relationship
between the stress and recoverable strain in materials as
diverse
as bone, rock and steel. However, this limited version of
Hookes
Law accurately describes only tension and compression
behavior
of linearly elastic materials in a uni-axial direction. It
should be
noted that modulus may be direction-dependent or
anisotropic.
This is important to consider for composite materials (e.g.
car-
bon fiber implants, reinforced concrete) as well as biologic
tissues
with internal structured arrangement (e.g. tendon,
ligament).
Tangent modulus
For other materials, such as many used in NA devices, the
rela-
tionship between stress and strain is nonlinear. In other words,
at
small strains many polymers and biological tissues exhibit a
rela-
tively low elastic modulus, whereas the same materials exhibit
a
higher elastic modulus at higher strains (Figure 2). Two or
more
Figure 1Diagram of a simple tension test (left) and typical
stress-strain curves and elastic modulus values for materials
commonly encountered in orthopaedics.
-
8/9/2019 Nucleus Arthroplasty Volume II
27/55
26
distinct regions may be observed, but the transition is
generally
gradual, and the stress-strain relationship can thus be
described
as nonlinear. For non-linear materials, the modulus is
deter-
mined by the slope of a line tangent to the stress-strain curve
at a
given point; this is called the tangent modulus. The tangent
mod-ulus provides an intuitive measure of a materials
non-linear
stress-strain response, analogous to the elastic modulus.
Viscoelasticity: Modulus dependence with time
For biological tissues and advanced polymeric biomaterials,
the
stress-strain relationship is usually dependent upon the
duration
of loading. When these materials are exposed to a given
stress,
the resulting strain increases with time at a rate dependent
upon
the material; this phenomenon is known as creep. Similarly,
an
applied strain results in a steadily decreasing amount of
stress
over time (Figure 3), and this stress relaxation may or may
not
proceed at a rate proportional to creep.1 Materials
exhibiting
time-dependent material properties are considered
viscoelastic.
An important consideration in defining the elastic modulus
for a viscoelastic material is the rate and duration of loading.
The
stress-strain-time relationship can be simplified from static
tests
by describing the apparent modulus upon immediate loading or
deformation (instantaneous modulus) and after a long
duration
of loading or deformation (equilibrium modulus). It is
important
to recognize the various methods for calculating modulus and
the potential variation in outcomes with viscoelastic
materials.
Fluid flow
For biologic tissue and some biomaterials (e.g. hydrogels),
fluid
flow in and out of the material is important in determining
the
time-dependent properties of the material. For example, the
load
bearing capacity of the nucleus is attributed to its
hydration
level.2 However, as hydration levels change as a result of
mechan-
ical pressure, the permeability of the anulus and endplates
allows
an outflow of water, altering the mechanical response of the
disc.3,4 Thus, the disc response to load is viscoelastic in
nature.
Figure 2Stress-strain curve for a typical soft tissue or
nonlinearly-elastic biomaterial.
Tangent lines for points A and B are indicated and the tangent
modulus
calculation is shown for Point B (EB).
Figure 3Results for the stress-relaxation response of a porcine
spinal ligament. An imme-
diate strain step was applied and held (top) and the resulting
stress response was
observed (bottom). Stress-relaxation experiments are performed
to explore the
stress-strain-time relationship.
FOR BIOLOGICAL TISSUES AND ADVANCED POLYMERIC
BIOMATERIALS, THE STRESS-STRAIN RELATIONSHIP IS
USUALLY DEPENDENT UPON THE DURATION OF LOADIN
-
8/9/2019 Nucleus Arthroplasty Volume II
28/55
27
Over a 24 hour period the balance of mechanical and osmotic
pressure causes the disc volume and height to decrease such
that
a ~20mm decrease in height is seen over the entire length of
the
spine.5 In the healthy disc this change is balanced by
swelling
during the discs nightly intake of water while the spine
isunloaded.6 Factors governing the rate of fluid flow include
osmotic and physical pressure gradients, porosity, and the
avail-
ability and viscosity of the surrounding fluid. While
inherent
viscoelastic properties of a hydrogel or soft tissue and
fluid-flow
appear similar in the discs response to loading, the
respective
contributions of these variables to material properties are at
least
partially independent.7
Radial deformations and the effect of constraint
The three-dimensional behavior of a material is only
partiallydescribed by the uni-axial stress-strain and time
dependency.
Equally important is the behavior of a material in a plane
per-
pendicular to the applied force, or stated otherwise, the
radial
direction. For the simple bar shown in Figure 1, the radial
defor-
mation can be described as a proportion of the axial strain
as
shown in the following relationship:
where is a constant known as Poissons ratio. Poissons ratio
is
important not only in describing radial deformation, but
also
the amount of volume change exhibited by a material for a
given
load. The unit change in volume (V) of a cube of solid
material
can be described using the following equation:
Note that for a Poissons ratio of 0.5, this change in volume is
zero.
Such a material is considered incompressible. Water is the
most
common example of a nearly incompressible material. Water
can
easily undergo a shape change, but imposing a volume change
is
nearly impossible if the water is constrained radially.
Biological tis-
sues, rubber and other polymeric materials are examples of
materi-
als that are often considered nearly incompressible with
sufficient
radial constraint.
The apparent modulus of a water-containing material is
depend-
ent upon the rigidity and permeability of its physical
constraints.
If constrained radially in an undeformable and impermeable
con-
tainer, such a material would behave in a relatively
incompressible
manner and could thus withstand high loads with negligible
deformation. If the constraining container were made
permeable,
then volume change of the same material would occur over
time
as water seeped from the material. In a permeable container,
the
material would appear to have a high modulus under rapid
dynamic loading, but would have a relatively low apparent
modu-
lus after many hours of loading as the water content
decreased
with time. Stress or time-dependent deformation of the con-
straining container would similarly result in decreased
rigidity.
This phenomenon is illustrated by the varying tangent
modulus
of a hydrogel material subjected to various constraints (Figure
4).
Thus, material modulus is dependent on both the constraint
rigidity and the constraint permeability for
water-containing
materials such as cartilage, the nucleus pulposus, the anulus
fibro-