Embed Size (px)
Citation preview

Nutrition Support for Burn Injury
Andreina Martin, Stephanie Ontiveros, Claudia Rodriguez,
Stephanie Villalobos, Nelson Zeledon
Patient IntroductionJA is a 65 y/o male, admitted as a level 2 trauma with 40% TBSA to the Surgical ICU for a burn injury.
● Chief Complaint: ○ Two different stories. ○ Patient says body caught on fire and he put it out by jumping on the floor
or into a ravine.

Social History ○ JA is a smoker, 1 pack per day for more than 30 years○ Alcohol- 2-3 beers daily and a case on Saturdays and
Sundays○ Years of education: 11.○ Unemployed and lives alone
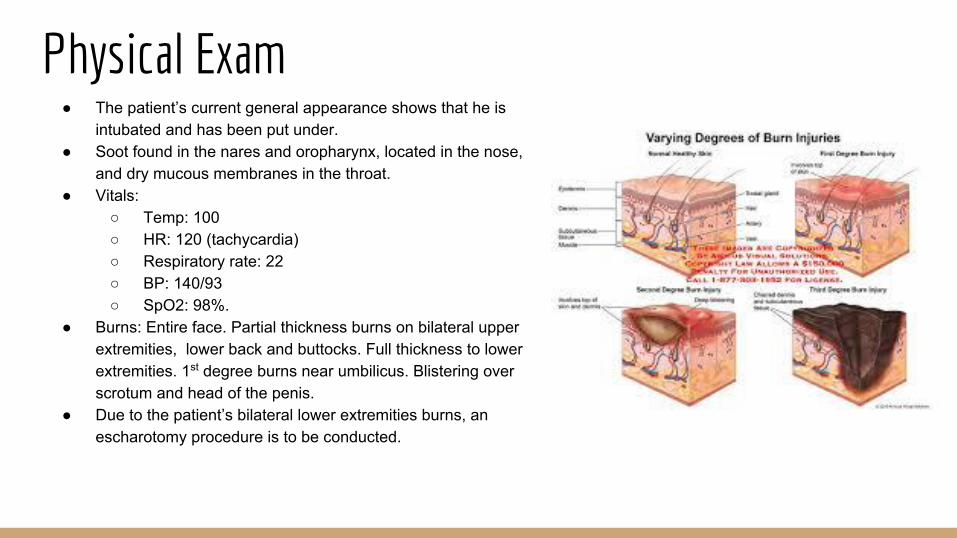
Physical Exam● The patient’s current general appearance shows that he is
intubated and has been put under. ● Soot found in the nares and oropharynx, located in the nose,
and dry mucous membranes in the throat.● Vitals:
○ Temp: 100○ HR: 120 (tachycardia)○ Respiratory rate: 22○ BP: 140/93○ SpO2: 98%.
● Burns: Entire face. Partial thickness burns on bilateral upper extremities, lower back and buttocks. Full thickness to lower extremities. 1st degree burns near umbilicus. Blistering over scrotum and head of the penis.
● Due to the patient’s bilateral lower extremities burns, an escharotomy procedure is to be conducted.


Class of Burns

Zone Of NecrosisZone of Coagulative Necrosis
Zone of Stasis
Zone of Hyperaemia

Burn Patient Considerations Shock
Sepsis
Respiratory Insufficiency
Shift of Body fluids into interstitial compartments
Loss of Protein in Plasma causing edema
Excess loss of heat > Hypermetabolic State > Increased Kcal Needs
At risk for Opportunistic infection/growth of microorganism > Pseudomonas Aeruginosa, MRSA, Candida infections > Sepsis

Common InvestigationsHemoglobin
Blood gases
Chest xray
Haematocrit
Electrolyte balance
Blood glucose
ECG
Creatine Kinase
Urinary myoglobinBun

Medications Nutrient/Drug Interactions ● Docusate- Monitor fluid status, electrolyte balance and fiber intake ● Silver sulfadiazine - topical antibiotic. ● Acetaminophen -Limit alcohol, caffeine and Vitamin C● Midazolam - Caution with grapefruit, herbal sedatives and stimulants
● Hydromorphone- Fluid status must be
monitored
● Propofol-Need to consider kcal intake ● 1.1 Kcal per mL ● Famotidine

Anthropometric Data
○ Patient J.A., male, 65 y/o. ○ Height: 6 feet (72”). ○ Weight (actual) 71.2kg (156.64#). ○ Weight (usual): 71.2 kg (156.64#). ○ Weight (ideal): 80.9kg (178#). ○ 88% IBW. 100%UBW. ○ BMI: 21.24 (normal - stable weight for past 6 mo.)
Diet History
○ Diabetic ○ No Specific diet ○ Has not monitored blood glucose for ~1 year.○ NPO with EN upon admission.
■ (ASPEN: begin EN 4-6 hours upon onset of injury).

Final Nutrition Care Plan
ESTIMATED CALORIE NEEDS
Zawacki Equation
1440 Kcal/d × BSA
Patient BSA: 1.82m²
1440 kcal/d x 1.82m² =
4,752 kcal/day
ESTIMATED PROTEIN NEEDS
1.5-2.0g/kg for burn patients
Patient IBW: 178#, 81kg
2.0g x 81kg =
162 g/day

Final Nutrition Care PlanNutrition diagnosis:
● Recommend NPO with EN Pivot 1.5 @60 ml/hr with final goal rate of 120 ml/hr to provide: 4300 kcal, 497g CHO, 146g Fat, 270g Protein, 2.2L free water.
● Total kcals adjusted due to propofol providing about 280 kcals from Fat

Final Nutrition Care PlanPES
1. Inadequate energy intake R/T patient in hypermetabolic state AEB Predicted energy
of 4750 kcal
2. Inadequate enteral nutrition infusion R/T current diet order AEB Current infusion rate
only meets 40% of estimated needs
3. Altered nutrition related lab values R/T altered kidney function and catabolic
response to burn injury AEB hyperkalemia, low total protein, hypercalcemia,
hyperglycemia and hypomagnesemia

Final Nutrition Care Plan● Nutrition Intervention
○ Assure pt is meeting daily energy requirements (Total: 4700 kcal)
○ Assure pt is meeting daily protein requirements (Total: 280g)
○ Reach proper infusion rate of 120 ml/hr within 36 hrs to prevent sepsis.
○ Prevent progression of kidney damage by discussing possible drug-nutrient interactions with MD.
● Monitoring and Evaluation
○ Monitor Pts. daily EN intake to assure he’s receiving 4,300 Kcal, 497 g CHO, 146g fat, 270g protein,
and 2.2 L water, and make adjustments as his condition progresses.
i. Monitor gastric residuals to determine tolerance
○ With adjustment of EN the following labs will stabilize as follows
i. Pt. blood K+ levels will lower to a normal range of 3.5-5.0 mEq/L,
ii. Pt. blood Ca+ levels will lower to a normal range of 8.8-10.4 g/dL
iii. Pt. Total protein will increase to normal range of 6.0-8.3 g/dL

Multiple Choice Questions1. Which of the following is NOT a type of burn
a. Electricalb. Chemicalc. Thermald. Sepsis
Multiple Choice Questions1. Which of the following is NOT a type of burn
a. Electricalb. Chemicalc. Thermald. Sepsis

Multiple Choice Questions2. According to ASPEN guidelines, Enteral nutrition should be administered to burn patients within:
a. 4-6 hours of injury onset. b. 24 hours of injury onsetc. 48 hours of injury onsetd. 72 hours of injury onset

Multiple Choice Questions2. According to ASPEN guidelines, Enteral nutrition should be administered to burn patients within:
a. 4-6 hours of injury onset. b. 24 hours of injury onsetc. 48 hours of injury onsetd. 72 hours of injury onset





























