Embed Size (px)
Citation preview
Open Access Full Text Article
Integrative Trauma and Emergency Medicine
www.scientonline.org Integr Trauma Emerg MedVolume 1 • Issue 1 • 002
Case Report
Recurrent Dislocation of the Elbow: Report Of Two Cases
Otman Benabdallah*Centres Hospitaliers De Tanger, Morocco
IntroductionRecurrent dislocation of the elbow is infrequent. In 1971, Jacobs [1] found only
forty cases in the literature. More recently, the literature has been enriched with several studies [2-9]. Several theories of the pathogenesis suggest that bone lesions or failure of the lateral ligaments and capsule play a role in the recurrence of this condition. Many surgical procedures have been described for repairing the anatomical lesions: tendon transfers, bone blocks, ligament reconstruction [1,10]. The treatment should target the lesions responsible, principally the capsuloligament [9,11-14]. The purpose of this paper is to present two cases of recurrent dislocation of the elbow and to re-emphasize the importance of repair of the postelateral ligament and capsular structures in the treatment of this unusual disorder.
Case ReportsCase I: A sportsman aged twenty two had sustained a postero-lateral elbow
dislocation in a fall during a tennis match approximately fifteen months prior to admission. This had been reduced by a physician and immobilized by a cast, which was removed by the patient after a week. In the months following the initial injury, he sustained repeated episodes of dislocation after moderate injuries, and these were reduced by friends. Gradually, the patient began to complain of apprehension and pain and important instability when actively using the involved extremity in tennis matches.
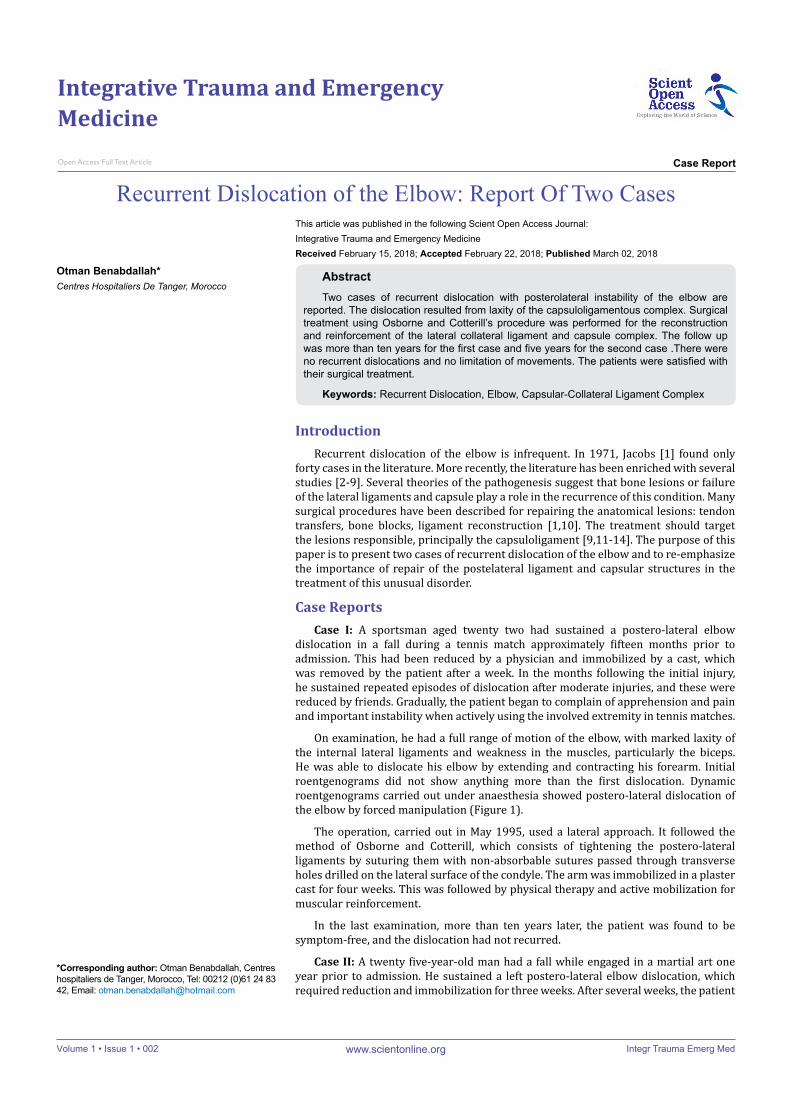
On examination, he had a full range of motion of the elbow, with marked laxity of the internal lateral ligaments and weakness in the muscles, particularly the biceps. He was able to dislocate his elbow by extending and contracting his forearm. Initial roentgenograms did not show anything more than the first dislocation. Dynamic roentgenograms carried out under anaesthesia showed postero-lateral dislocation of the elbow by forced manipulation (Figure 1).
The operation, carried out in May 1995, used a lateral approach. It followed the method of Osborne and Cotterill, which consists of tightening the postero-lateral ligaments by suturing them with non-absorbable sutures passed through transverse holes drilled on the lateral surface of the condyle. The arm was immobilized in a plaster cast for four weeks. This was followed by physical therapy and active mobilization for muscular reinforcement.
In the last examination, more than ten years later, the patient was found to be symptom-free, and the dislocation had not recurred.
Case II: A twenty five-year-old man had a fall while engaged in a martial art one year prior to admission. He sustained a left postero-lateral elbow dislocation, which required reduction and immobilization for three weeks. After several weeks, the patient
*Corresponding author: Otman Benabdallah, Centres hospitaliers de Tanger, Morocco, Tel: 00212 (0)61 24 83 42, Email: [email protected]
AbstractTwo cases of recurrent dislocation with posterolateral instability of the elbow are
reported. The dislocation resulted from laxity of the capsuloligamentous complex. Surgical treatment using Osborne and Cotterill’s procedure was performed for the reconstruction and reinforcement of the lateral collateral ligament and capsule complex. The follow up was more than ten years for the first case and five years for the second case .There were no recurrent dislocations and no limitation of movements. The patients were satisfied with their surgical treatment.
Keywords: Recurrent Dislocation, Elbow, Capsular-Collateral Ligament Complex
This article was published in the following Scient Open Access Journal:Integrative Trauma and Emergency MedicineReceived February 15, 2018; Accepted February 22, 2018; Published March 02, 2018
Citation: Otman Benabdallah (2018). Recurrent Dislocation of the Elbow: Report of Two Cases
Page 2 of 3
www.scientonline.org Integr Trauma Emerg MedVolume 1 • Issue 1 • 002
sustained a new fall on the same elbow with another dislocation, which was reduced by a colleague. Then over the next few months he had multiple recurrent dislocations while practising sport.
On examination, the elbow had an almost full range of motion, but with apprehension for some movements liable to cause instability of the elbow (extending the elbow and contracting the muscle). Laterality movements showed a certain complaisance even without anaesthesia. Roentgenograms confirmed this complaisance (abnormal internal laterality, Figure 2A) and dislocation expressed by vacuity of the coronoid fossa in the dynamic x-ray (Figure 2B) with no other anomaly in the humero-radial and humero-ulnar joint.
Exploration was carried out via a postero-lateral incision. Considerable laxity of the postero-lateral ligament structure
was evident (avulsion of the postero-lateral capsuloligamentous complex and the presence of a lateral pocket palpable with the finger). With the lateral ligament tightened by pulling it upwards with the finger, dislocation of the elbow was difficult. A capsuloligamentous repair was carried out by making drill holes and suturing the ligament in the lateral epicondyle (Osborne and Cotterill’s method). The elbow was immobilized for four weeks in a plaster cast.
Follow up more than five years later revealed a stable, pain-free elbow, and dislocation had not recurred.
Discussion Hassman, et al. [9] reported that in thirty one surgically
treated recurrent dislocations of the elbow, the instability was attributed to:
- a bone lesion in ten cases
- a capsuloligamental lesion in seventeen cases
- bone and ligament lesions in two cases
Surgery included- bone block in ten cases
- dynamic tendon transfer in four cases
- ligament and capsular repair in fifteen cases
However, in some cases, the follow-up periods were too short to permit assessment of the results. In one case, treatment by a bone block failed, but there were no failures after capsule ligament repair.
In the literature, apart from cases of a disorder of connective tissue like Ehlers-Danlos syndrome[15], where the elbow can be dislocated on single occasions (the joints are hypermobile), the pathogenesis of recurrent dislocations of the elbow was attributed to bone lesions (dysplasia of the coronoid fossa, anterior fracture of the apophysis during the initial dislocation, trochlear notch insufficiency, or a defect in the postero-lateral margin of the capitellum, as well as a shovel-like defect in the head of the radius), to bone and ligament lesions, or to ligament and capsular lesions [9,10]. This last condition seems to be the most probable and now a majority of authors [9,11,13,14] insist on the importance of the lateral ligament and capsule for stability of the elbow (seventeen cases cited in Hassman, et al. [9]). We agree with Osborne and Cotterill and others [9,13] that axial loading of the extended humero-ulnar joint forces the coronoid process against the laterally sloping surface of the trochlea, and if the lateral capsulo-ligament system is lax, the radio-ulnar complex simply displaces posteriorly and laterally . Repeated dislocations result in the formation of the lateral pocket. Also according to Osborne and Cotterill [3], the essential lesion of the elbow is a “failure of the postero-lateral ligamentous and capsular structures, torn or stretched at the time of an initial simple traumatic dislocation, to become reattached”.
Some authors [13] consider that bone defects of the joint are just a secondary phenomenon in the pathogenesis.
Could inadequate immobilization be one cause of the failure of the ligament to heal? The literature [1,14] does not define the best treatment for an initial dislocation. In practice, many
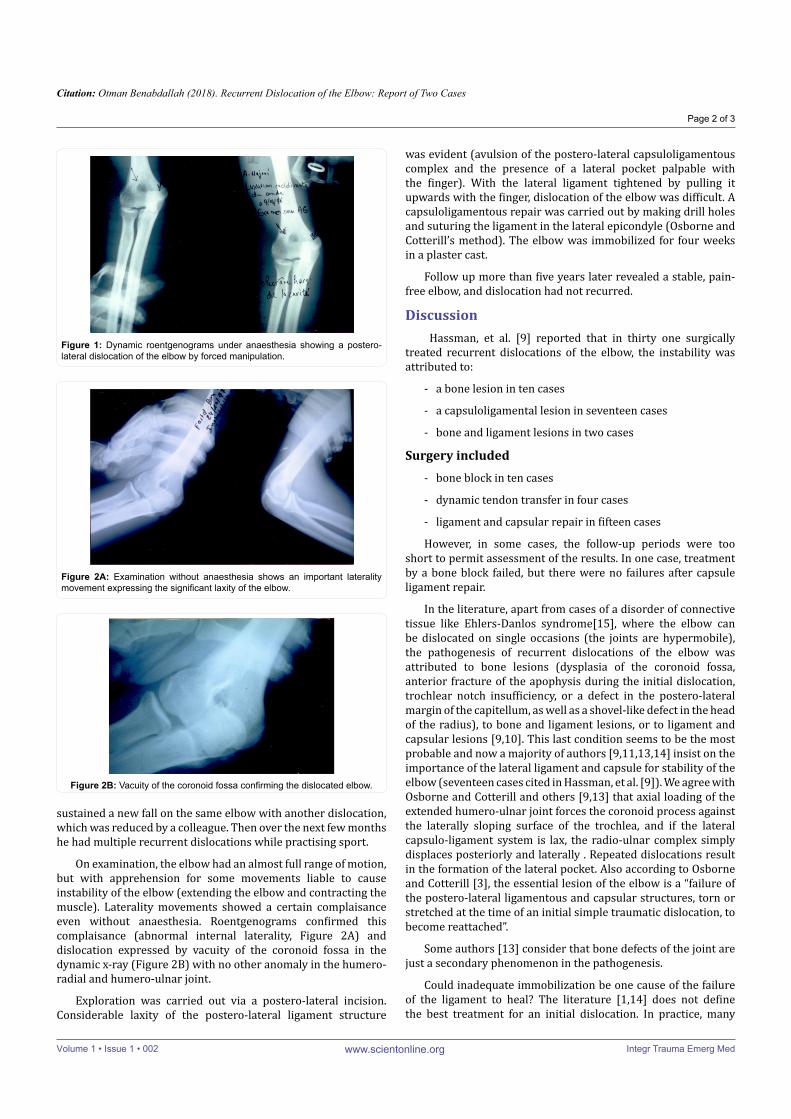
Figure 1: Dynamic roentgenograms under anaesthesia showing a postero-lateral dislocation of the elbow by forced manipulation.
Figure 2A: Examination without anaesthesia shows an important laterality movement expressing the significant laxity of the elbow.
Figure 2B: Vacuity of the coronoid fossa confirming the dislocated elbow.

Citation: Otman Benabdallah (2018). Recurrent Dislocation of the Elbow: Report of Two Cases
Page 3 of 3
www.scientonline.org Integr Trauma Emerg MedVolume 1 • Issue 1 • 002
patients remove the immobilization earlier than recommended and experience no instability or recurrences. This could even be considered a preventive measure, as it allows the soft tissues to heal. The primum movens is the lesion of the ligamentous capsular complex and its healing with sufficient or insufficient immobilization after a primary traumatism.
In our two cases, significant laxity of the postero-lateral ligament was found in both patients clinically and operatively. No bone lesions or intra-articular loose bodies were found in our patients, perhaps because the traumatism was not very old and was not accompanied by initial fractures, as was true of cases cited in some articles [9,12,13]. After ligamentous capsular repair, the results were encouraging after follow-up of ten and five years respectively. The patients had no recurrences, and they were pain free with a good range of motion. Both patients returned to their normal activities.
We felt that Osborne and Cotterill’s procedure was the most suitable for our two cases because the anatomical element responsible was the capsuloligamental complex. The result of the capsuloligamentous repair is encouraging, based on follow-up of 10 years for case 1 and 5 years for case 2. This technique is recommended for its simplicity and for the fact that it attacks the essential lesion. Until now there have been no reported failures after capsuloligament repair. Of course, the number of reported cases remains too small to draw significant conclusions.
ConclusionInadequate immobilization of the elbow following the initial
injury seems not to be the only cause of recurrent dislocation of the elbow; failure of the lateral capsuloligament complex is the primum movens of instability of the elbow. Surgical repair using the procedure of Osborne and Cotterill is the recommended technique for this disorder because it attacks the essential lesion.
Aknowlegement I want to thank very much Professor Eirlys Davis for her
invaluable help.
References1. Jacobs RL. Recurrent dislocation of the elbow joint: Case report and review
of the literature. Clin Orthop Relat Res. 1971;74:151-154.
2. Kolb K, Holz U. The unstable elbow joint. Unfallchirug. 1999;102(7):554-571.
3. Olsen BS, Sojbjerg JO. The treatment of the posterolateral instability of the elbow. J Bone Joint Surg Br. 2003;85(3):342-346.
4. Doria A, Gil E, Delgado E, Alonso-Llames M. Recurrent dislocation of the elbow. Int Orthop. 1990;14(1):41-45.
5. O’Driscoll SW, Morrey BF, Korinek S, An KN. Elbow subluxation and dislocation: A spectrum of instability. Clin Orthop Relat Res. 1992;280:186-197.
6. Hannouche D, Begue T. Functionnal anatomy of the lateral collareral complex of the elbow. Surg Radiol Anat. 1999;21(3):187-191.
7. Fontaine C, Sensey JJ, Razemon JP, Mestdagh H, Duquennoy A. Treatment of recurrent dislocations of the elbow using the Osborne-Cotterill technique for capsulloraphy: à propos of 7 cases. Rev Chir Orthop. 1985;71(2):86-88.
8. Hackl M, Leschinger T, Muller LP, Wegmann K. Chronic ligamentous instability of the elbow. Orthopade. 2016;45(10):809-821.
9. Hassman BC, Brunn F, Neer CS. Recurrent dislocation of the elbow. J Bone Joint Surg Am. 1975;57(8):1080-1084.
10. Roy CR, Laurin CA, Riley LH. Atlas de chirurgie orthopédique. Tome 2: Membre supérieur. Masson. 1990;157-161.
11. Osborne G, Cotterill P. Recurrent dislocation of the elbow. J Bone Joint Surg Br. 1966;48:340-346.
12. Spring WE. Report of a case of recurrent dislocation of the elbow. J Bone Joint Surg Br. 1953;35(1):55.
13. Symeonides PP, Paschaloglou C, Stavrou Z, Pangalides T. Recurrent dislocation of the elbow: Report of two cases. J Bone Joint Surg Am. 1975;57(8):1084-1086.
14. Trias A, Comeau Y. Recurrent dislocation of the elbow in the children. Clin Orthop Relat Res. 1974;100:74-77.
15. Beighton P, Horan F. Orthopaedic aspects of the Ehlers-Danlos syndrome. J Bone Joint Surg Br. 1969;51(3):444-453.
Copyright: © 2018 Otman Benabdallah. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.