Embed Size (px)
Citation preview
NSAIDs in the ED:NSAIDs in the ED:Focus on Ibuprofen & KetorolacFocus on Ibuprofen & Ketorolac
Andrea WilsonAndrea Wilson
May 6, 2004May 6, 2004

OutlineOutline
NSAID usageNSAID usage ComplicationsComplications The COX stuffThe COX stuff Ibuprofen Ibuprofen KetorolacKetorolac UGIB – what’s importantUGIB – what’s important Prevention of UGIB?Prevention of UGIB? ConclusionsConclusions

NSAID UsageNSAID Usage Among the most widely prescribed Among the most widely prescribed
medicationsmedications 17 million Americans use NSAIDs daily17 million Americans use NSAIDs daily 25% of outpatient & ED prescriptions25% of outpatient & ED prescriptions
(Emergency Medicine Reports January 31, 2000)(Emergency Medicine Reports January 31, 2000)
(Pollison R, ed. Rheumatology, 1997; Elashoff JD, Gastro (Pollison R, ed. Rheumatology, 1997; Elashoff JD, Gastro 1980)1980)


>50% of NSAID prescriptions >50% of NSAID prescriptions are written for OA pts > age 60.are written for OA pts > age 60.
In ED: In ED: NSAIDs often first line for NSAIDs often first line for pain in trauma, ureteral and pain in trauma, ureteral and
biliary colic, dysmenorrhea…biliary colic, dysmenorrhea…
Wang RY, Girard DD, Aleguas A. EMR reports Over-the-Counter (OTC) Medications: A Quick Consult Guide to the Evaluation and Management of Toxic Effects and Adverse Reactions Part II: Systemic, Oral, and Miscellaneous Preparations Feb 2001

Epidemiology of complicationsEpidemiology of complications NSAIDs in N.A. arthritis pts: NSAIDs in N.A. arthritis pts:
~ 100,000 hospitalizations/yr (cost $4 billion) ~ 100,000 hospitalizations/yr (cost $4 billion) >16 000 deaths (Ruffalo, Singh-ARAMIS)>16 000 deaths (Ruffalo, Singh-ARAMIS) Worldwide ?Worldwide ?
For UGIB & perfs in RA/OA pts on Rx NSAIDs:For UGIB & perfs in RA/OA pts on Rx NSAIDs: 1414thth leading cause of death (after homicides and leading cause of death (after homicides and
before atherosclerosis) – ARAMISbefore atherosclerosis) – ARAMIS
Incidence of ulcers +/or ulcer complications - Incidence of ulcers +/or ulcer complications - range 2% - 4% range 2% - 4%
Wang RY, Girard DD, Aleguas A. EMR reports Over-the-Counter (OTC) Medications: A Quick Consult Guide to the Evaluation and Management of Toxic Effects and Adverse Reactions Part II: Systemic, Oral, and Miscellaneous Preparations Feb 2001

The list…The list… UGIB and ulcer perforation UGIB and ulcer perforation
N/V, abd pain, diarrhea, N/V, abd pain, diarrhea, constipation, gastritis, constipation, gastritis, exacerbation of IBD. exacerbation of IBD.
Renal failureRenal failure Elevated liver enzymes (drug-Elevated liver enzymes (drug-
induced hepatitis). induced hepatitis). Electrolyte abnormalities: Electrolyte abnormalities:
hyponatremia / hyperkalemia hyponatremia / hyperkalemia Hypertension Hypertension CHFCHF Inhibit plt aggregation.Inhibit plt aggregation.
(agranulocytosis, leukopenia, (agranulocytosis, leukopenia, thrombocytopemia)thrombocytopemia)
Derm: TEN, Stevens Johnson Derm: TEN, Stevens Johnson Syndrome, rashSyndrome, rash
Cross-reactivity with true ASA Cross-reactivity with true ASA allergyallergy
Aspirin-induced asthmaAspirin-induced asthma Drug interactions: increased Drug interactions: increased
phenytoin, VPA, sulfonylureas,phenytoin, VPA, sulfonylureas, digoxindigoxin
Retinal or optic nerve toxicity Retinal or optic nerve toxicity Aseptic meningitisAseptic meningitis Prolongation of labourProlongation of labour ?Fracture healing?Fracture healing
Emerman CL, Spenetta J. EMR reports: Pain Management in the Emergency Department Feb 2002Kantor TG. Ibuprofen. Annals of Internal Medicine. 1979;91:877-882.Kantor TG. Ibuprofen. Annals of Internal Medicine. 1979;91:877-882.

For NSAIDs, if the associations found in For NSAIDs, if the associations found in epidemiological studies were causal… epidemiological studies were causal…
For every 100,000 person years:For every 100,000 person years: ~ 300 UGIB/perfs, ~ 300 UGIB/perfs, 5 acute liver injuries, 5 acute liver injuries, 4 hospitalizations for ARF4 hospitalizations for ARF undefined # of hospitalizations for CHFundefined # of hospitalizations for CHF
Hernandez-Diaz S, Rogriguez LAG. Epidemiologic Assessment of the Safety Hernandez-Diaz S, Rogriguez LAG. Epidemiologic Assessment of the Safety of Conventional Nonsteroidal Anti-Inflammatory Drugs. Amer J of Med. Feb of Conventional Nonsteroidal Anti-Inflammatory Drugs. Amer J of Med. Feb 2001;110 (3A) 20S-27S.2001;110 (3A) 20S-27S.

Death rate /100,000 and number of deaths associated with NSAID-Death rate /100,000 and number of deaths associated with NSAID-induced GI damage compared with other causes: United States induced GI damage compared with other causes: United States population, 1994. - population, 1994. - Singh G. Recent Considerations in Nonsteroidal Anti-Inflammatory Drug Gastropathy. Singh G. Recent Considerations in Nonsteroidal Anti-Inflammatory Drug Gastropathy. Amer J Med. July 1998; 105 (1B): 31S-38S Amer J Med. July 1998; 105 (1B): 31S-38S

PharmacodynamicsPharmacodynamics
Analgesic, anti-inflammatory, antipyretic, platelet Analgesic, anti-inflammatory, antipyretic, platelet inhibitory properties. inhibitory properties.
When prescribed at equipotent doses NSAIDs show When prescribed at equipotent doses NSAIDs show similar clinical efficacysimilar clinical efficacy
Rapidly absorbed PO & highly protein-bound. Rapidly absorbed PO & highly protein-bound.
Acetaminophen and Ketorolac minimally anti-Acetaminophen and Ketorolac minimally anti-inflammatory - proper term? – COX inhibitorsinflammatory - proper term? – COX inhibitors
Wang RY, Girard DD, Aleguas A. EMR reports Over-the-Counter (OTC) Medications: A Quick Consult Guide to the Evaluation and Management of Toxic Effects and Adverse Reactions Part II: Systemic, Oral, and Miscellaneous Preparations Feb 2001
Emerman CL, Spenetta J. EMR reports: Pain Management in the Emergency Department Feb 2002

Phospholipids
Phospholipase A2
Arachidonic Acid
Prostaglandins
Thromboxanes
Prostacyclin
COX
Leukotrienes
Lipoxygenase

Ashburn MA, Rubingh CR. The Role of Non-opioid Analgesics for the Management of Postoperative Painwww.moffitt.usf.edu/.../ images/ashburnfig2.jpg

Cox-3Cox-3 In 2002, COX-3 and two smaller COX-1 proteins In 2002, COX-3 and two smaller COX-1 proteins
derived (PCOX-1)derived (PCOX-1) Expressed in the brain and heartExpressed in the brain and heart Selectively inhibited by acetaminophen.Selectively inhibited by acetaminophen. Potently inhibited by diclofenac, aspirin, and ibuprofen.Potently inhibited by diclofenac, aspirin, and ibuprofen. May explain why acetaminophen is antipyretic and May explain why acetaminophen is antipyretic and
analgesic without affecting COX-1 or COX-2.analgesic without affecting COX-1 or COX-2.
New drug development that selectively inhibits COX-3.New drug development that selectively inhibits COX-3.
Senior K. Homing in on Cox-3 – the elusive target of paracetamol. Lancet 2002 vol 1 399.Senior K. Homing in on Cox-3 – the elusive target of paracetamol. Lancet 2002 vol 1 399.Schwab JM, Schluesener HJ, Laufer S. Lancet 2003; 361: 981-982. Schwab JM, Schluesener HJ, Laufer S. Lancet 2003; 361: 981-982.

PropertyProperty EffectEffect InhibitionInhibition
COX-1COX-1
aspirinaspirin
Most tissues Most tissues – not RBCs– not RBCs
ConstantConstant
PGs: gut protection, PGs: gut protection, renal blood flow, vasc renal blood flow, vasc tone, fetal developmenttone, fetal development
TXA2: plt aggregationTXA2: plt aggregation
GI bleedGI bleed
Dec renal Dec renal blood flow blood flow Dec coronary Dec coronary thrombosisthrombosis
COX-2COX-2
CelecoxibCelecoxib
CNS, CNS, Kidney, Kidney, InducibleInducible
Parturition, renal Parturition, renal development, salt and development, salt and BP regulation, Inflam & BP regulation, Inflam & temp temp
Dec pain and Dec pain and temptemp
Unopposed Unopposed thrombosisthrombosis
COX-3COX-3
acetaminacetamin
Brain, sp. Brain, sp. cord, heartcord, heart
Non-Non-inducibleinducible
Regulates pain Regulates pain response & feverresponse & fever
Decreased Decreased painpain
& ?& ?

NSAIDs (unlike narcotics) have a NSAIDs (unlike narcotics) have a ceiling effect.ceiling effect. Sigmoidal curveSigmoidal curve
Ibuprofen and KetorolacIbuprofen and Ketorolac
Emerman CL, Spenetta J. EMR reports: Pain Management in the Emergency Department Feb 2002

Why study ibuprofen?Why study ibuprofen?
So widely used.So widely used. Works well.Works well. Usually disorders treated not life-Usually disorders treated not life-
threatening and other analgesic options.threatening and other analgesic options. Potential to harmPotential to harm
Moore N, van Ganse E, Le Parc J-M et al (1999) . The PAIN study: paracetamol, aspirin Moore N, van Ganse E, Le Parc J-M et al (1999) . The PAIN study: paracetamol, aspirin and ibuprofen new tolerability study. A large-scale, randomized clinical trial comparing and ibuprofen new tolerability study. A large-scale, randomized clinical trial comparing the tolerability of aspirin, ibuprofen and paracetamol for short-term analgesia. Clin the tolerability of aspirin, ibuprofen and paracetamol for short-term analgesia. Clin Drug Invest 18:89-98Drug Invest 18:89-98
Ibuprofen 101Ibuprofen 101 Introduced in England in 1967. Introduced in England in 1967. 1/3-1/2 less GI adverse effect than aspirin 1/3-1/2 less GI adverse effect than aspirin Lowest risk of NSAIDs for UGIB or perf (Rodriguez)Lowest risk of NSAIDs for UGIB or perf (Rodriguez) Propionic acid derivative: Propionic acid derivative: 2 (4-isobutylphenyl) propionic acid.2 (4-isobutylphenyl) propionic acid. Rapidly absorbed. Peaks between 1.5 and 2 hrs. Rapidly absorbed. Peaks between 1.5 and 2 hrs.
Highly bound to plasma protein. T1/2 ~ 2 hrs. Highly bound to plasma protein. T1/2 ~ 2 hrs.
Kantor TG. Ibuprofen. Annals of Internal Medicine. 1979;91:877-882 Kantor TG. Ibuprofen. Annals of Internal Medicine. 1979;91:877-882 Laska EM, Sunshine A, Marrero I, Olson N, Siegel C, McCormick N. The correlation Laska EM, Sunshine A, Marrero I, Olson N, Siegel C, McCormick N. The correlation between blood levels of ibuprofen and clinical analgesic response. Clin Pharmacol Ther between blood levels of ibuprofen and clinical analgesic response. Clin Pharmacol Ther 1986;40:1-7.1986;40:1-7.

Is Ibuprofen safe?Is Ibuprofen safe? Blinded RCT comparing adverse events for Blinded RCT comparing adverse events for
ASA tabs (up to 3 g/day) ASA tabs (up to 3 g/day) Acetaminophen (up to 3 g/d) and Acetaminophen (up to 3 g/d) and Ibuprofen (up to 1.2 g/day) Ibuprofen (up to 1.2 g/day)
8233 completed study. 8233 completed study. Adverse events: Adverse events:
Ibuprofen Ibuprofen 13.7%,13.7%, acetaminophen acetaminophen 14.5%14.5% aspirin 18.7%. aspirin 18.7%. No stat difference btw ibuprofen and acetaminophen No stat difference btw ibuprofen and acetaminophen GI events:GI events:
• ibuprofen (4%) acetaminophen (5.3%) aspirin (7.1%) ibuprofen (4%) acetaminophen (5.3%) aspirin (7.1%) 6 GI bleeds: 4 with acetaminophen and 2 with aspirin. 6 GI bleeds: 4 with acetaminophen and 2 with aspirin.
Moore N, van Ganse E, Le Parc J-M et al (1999) . The PAIN study: paracetamol, aspirin and ibuprofen new Moore N, van Ganse E, Le Parc J-M et al (1999) . The PAIN study: paracetamol, aspirin and ibuprofen new tolerability study. A large-scale, randomized clinical trial comparing the tolerability of aspirin, ibuprofen and tolerability study. A large-scale, randomized clinical trial comparing the tolerability of aspirin, ibuprofen and paracetamol for short-term analgesia. Clin Drug Invest 18:89-98paracetamol for short-term analgesia. Clin Drug Invest 18:89-98

Is Ibuprofen safe in peds?Is Ibuprofen safe in peds? Abstract Abstract RCT of 27065 children RCT of 27065 children
acetaminophen (12 mg/kg), acetaminophen (12 mg/kg), ibuprofen (5 mg/kg) ibuprofen (5 mg/kg) or ibuprofen (10 mg/kg). or ibuprofen (10 mg/kg).
No statistically significant difference between No statistically significant difference between groups for risk of hospitalization including GI groups for risk of hospitalization including GI bleeds. bleeds.
Abstract: Lesko SM, Mitchell AA (1999). The safety of Abstract: Lesko SM, Mitchell AA (1999). The safety of acetaminophen and ibuprofen among children younger than two acetaminophen and ibuprofen among children younger than two years old. Pediatrics 104(4):e39years old. Pediatrics 104(4):e39

Safe in max OTC doses?Safe in max OTC doses? Low dose = low risk Low dose = low risk So what about max OTC dose?So what about max OTC dose?
Limit of 1200 mg/day for 10 days of continuous use. Limit of 1200 mg/day for 10 days of continuous use. Double-blind RCT 1206 ptsDouble-blind RCT 1206 pts GI adverse events of max OTC dose ibuprofen vs placebo GI adverse events of max OTC dose ibuprofen vs placebo Adverse events: Adverse events:
16% with placebo and 19% with ibuprofen. (Not statistically different.) 16% with placebo and 19% with ibuprofen. (Not statistically different.) Occult bloods not different between groups. Occult bloods not different between groups.
ConclusionConclusion: Non-prescription ibuprofen max 1200 mg/day for 10 days is : Non-prescription ibuprofen max 1200 mg/day for 10 days is well-tolerated.well-tolerated.
Doyle G, Furey S, Berlin R et al (1999). Gastrointestinal safety and tolerance of Doyle G, Furey S, Berlin R et al (1999). Gastrointestinal safety and tolerance of ibuprofen at maximum over-the-counter dose. Aliment Pharmacol Ther 13:897-906.ibuprofen at maximum over-the-counter dose. Aliment Pharmacol Ther 13:897-906.

Safe… but does it work?Safe… but does it work?Cooper SA, Schachtel BP, Goldman E, et al. Ibuprofen and acetaminophen in the relief of Cooper SA, Schachtel BP, Goldman E, et al. Ibuprofen and acetaminophen in the relief of acute pain: a randomized, double-blind, placebo-controlled study. J Clin Pharm, 1989;29:1026-acute pain: a randomized, double-blind, placebo-controlled study. J Clin Pharm, 1989;29:1026-1030.1030.
Double-blind, placebo-controlled, RCT. Double-blind, placebo-controlled, RCT. 184 after dental impaction surgery. 184 after dental impaction surgery. Ibuprofen 400 mg, acetaminophen 1000 mg and placebo. Ibuprofen 400 mg, acetaminophen 1000 mg and placebo.
Ibuprofen better than acetaminophen Ibuprofen better than acetaminophen (Sum Pain Intensity Difference, Total Pain Relief, sum pain half-gone, and overall (Sum Pain Intensity Difference, Total Pain Relief, sum pain half-gone, and overall
evaluation. evaluation. Side effects Side effects
8% ibuprofen pts, 17% acetaminophen pts and 11% placebo. 8% ibuprofen pts, 17% acetaminophen pts and 11% placebo. Conclusions: Conclusions:
Both drugs safe. Both drugs safe. Ibuprofen - longer duration of analgesia and higher peak pain relief than Ibuprofen - longer duration of analgesia and higher peak pain relief than
acetaminophen. acetaminophen.
74.2 % of pts on ibuprofen rated tx good, (higher rating than for paracetamol 74.2 % of pts on ibuprofen rated tx good, (higher rating than for paracetamol (69.2%) or ASA (68.6%) (p<0.001) Moore’s PAIN study(69.2%) or ASA (68.6%) (p<0.001) Moore’s PAIN study

What is the ceiling analgesic dose What is the ceiling analgesic dose of Ibuprofen?of Ibuprofen?
Increasing doses = more antiinflammatory Increasing doses = more antiinflammatory effects and added side effects effects and added side effects
Anti-inflammatory doses needed for Anti-inflammatory doses needed for inflammatory conditions – inflammatory conditions – not usually for acute pain.not usually for acute pain.
Goal: use the lowest effective dose (remember Goal: use the lowest effective dose (remember some inter-individual variation)some inter-individual variation)

Dose ceiling – 400 vs 800Dose ceiling – 400 vs 800 Double-blind RCT – 510 pts post oral surgeryDouble-blind RCT – 510 pts post oral surgery
400mg and 800 mg ibuprofen vs 650mg aspirin, 65mg of 400mg and 800 mg ibuprofen vs 650mg aspirin, 65mg of propoxyphene HCl (Darvon max dose), and placebo propoxyphene HCl (Darvon max dose), and placebo
2 doctors with separate pts populations. Patients pooled. 2 doctors with separate pts populations. Patients pooled. 5 groups evaluated pain over 3 hr period. 5 groups evaluated pain over 3 hr period.
Efficacy: Efficacy: Motrin (either dose) > aspirin >Darvon >placebo. Motrin (either dose) > aspirin >Darvon >placebo. (For peak analgesia and duration)(For peak analgesia and duration)
For one group, 400 mg Motrin appeared most effective and for For one group, 400 mg Motrin appeared most effective and for the other 800 mg most effective. the other 800 mg most effective.
??? ???
Winter L, Bass E, Recant B, Cahaly JF. Analgesic activity of ibuprofen (Motrin) in postoperative Winter L, Bass E, Recant B, Cahaly JF. Analgesic activity of ibuprofen (Motrin) in postoperative oral surgery pain. Oral Surg Oral Med Oral Path 1978;45:159-166.oral surgery pain. Oral Surg Oral Med Oral Path 1978;45:159-166.

Ceiling dose – 400?Ceiling dose – 400? Double blind, parallel group study Double blind, parallel group study
200 pts post oral surgery200 pts post oral surgery Correlation between serum levels & clinical analgesia Correlation between serum levels & clinical analgesia 400, 600, 800 mg ibuprofen & placebo. 400, 600, 800 mg ibuprofen & placebo. √ √ Correlation between log dose & serum concentration. Correlation between log dose & serum concentration. √ √ Decrease in pain with inc serum concentration. Decrease in pain with inc serum concentration. But… No statistical difference in pain relief btw 400, 600 and But… No statistical difference in pain relief btw 400, 600 and
800 mg of regular ibuprofen. 800 mg of regular ibuprofen. For ibuprofen, For ibuprofen, no evidence of a dose-response relationship no evidence of a dose-response relationship
past 400 mgpast 400 mg in terms of clinical efficacy. in terms of clinical efficacy.
Laska EM, Sunshine A, Marrero I, Olson N, Siegel C, McCormick N. The correlation Laska EM, Sunshine A, Marrero I, Olson N, Siegel C, McCormick N. The correlation between blood levels of ibuprofen and clinical analgesic response. Clin Pharmacol between blood levels of ibuprofen and clinical analgesic response. Clin Pharmacol Ther 1986;40:1-7.Ther 1986;40:1-7.

Ibuprofen + Acetaminophen?Ibuprofen + Acetaminophen? Rodriguez & Hernandez-Diaz Rodriguez & Hernandez-Diaz Case-control study: Case-control study:
2105 cases, 11,500 controls2105 cases, 11,500 controls Post-hoc analysisPost-hoc analysis
No increased risk if using daily doses of acetamin <2gNo increased risk if using daily doses of acetamin <2g Dose >2g/day = RR 3.6 (2.6-5.1)Dose >2g/day = RR 3.6 (2.6-5.1) If doses >2g/day + NSAIDs = If doses >2g/day + NSAIDs = NASTYNASTY
Increased Increased RR 13.2 RR 13.2 for UGIB (9.2-18.9)for UGIB (9.2-18.9)
In contrast: Lewis no UGIB with acetaminophen In contrast: Lewis no UGIB with acetaminophen alonealone at any at any dosedose
Rodriguez LAG, Hernandez-Diaz S. Relative Risk of Upper Gastrointestinal Complications Rodriguez LAG, Hernandez-Diaz S. Relative Risk of Upper Gastrointestinal Complications among Users of Acetaminophen and Nonsteroidal Anti-Inflammatory Drugs. Epidemiology. among Users of Acetaminophen and Nonsteroidal Anti-Inflammatory Drugs. Epidemiology. 2001; 12(5):570-576. 2001; 12(5):570-576.

Ketorolac – Why care?Ketorolac – Why care?
Effective analgesicEffective analgesic No resp depression, minimal sedation, no No resp depression, minimal sedation, no
abuse potential.abuse potential. No evidence to suggest ketorolac more No evidence to suggest ketorolac more
effective than other NSAIDseffective than other NSAIDs
Major advantage = parenteral.Major advantage = parenteral.
Turturro MA, Paris PM, Seaberg DC. Intramuscular Ketorolac Versus Oral Turturro MA, Paris PM, Seaberg DC. Intramuscular Ketorolac Versus Oral Ibuprofen in Acute Musculoskeletal Pain. Annals of Emergency Medicine. Ibuprofen in Acute Musculoskeletal Pain. Annals of Emergency Medicine. 1995; 26(2): 117-122.1995; 26(2): 117-122.
Ketorolac basicsKetorolac basics At 30 mg IV/IM dose – single most likely At 30 mg IV/IM dose – single most likely
NSAID to cause GI bleedNSAID to cause GI bleed Oral dose is 10 mg!! Why give 30 mg IM?Oral dose is 10 mg!! Why give 30 mg IM? T1/2 = 6 hrs if normal renal functionT1/2 = 6 hrs if normal renal function 10mg (30mg?) IM Ketorolac = 12 10mg (30mg?) IM Ketorolac = 12
morphine sulphatemorphine sulphate
Yee JP, Koshiver JE, Allbon C. Comparison of intramuscular Ketorolac Yee JP, Koshiver JE, Allbon C. Comparison of intramuscular Ketorolac Tromethamine and Morphine Sulfate for Analgesia of Pain After major Tromethamine and Morphine Sulfate for Analgesia of Pain After major Surgery. Pharmacotheraphy. 1986; 6(5): 253-261.Surgery. Pharmacotheraphy. 1986; 6(5): 253-261.
Is Ketorolac safe?Is Ketorolac safe?
Rodriguez : case control study 1505 Rodriguez : case control study 1505 UGIB/perfsUGIB/perfs
Ketorolac daily dose Ketorolac daily dose (outpatient mainly chronic pain and OA)(outpatient mainly chronic pain and OA)
≤≤20 mg 20 mg RR 20.0 (4.3-93.6)RR 20.0 (4.3-93.6) >20 mg>20 mg RR RR 28.128.1 (8.7-90.9) (8.7-90.9) PO PO RR 19.9 (4.2-93.0)RR 19.9 (4.2-93.0) IMIM RR 28.3 (8.7-92.0)RR 28.3 (8.7-92.0)

What dose of Ketorolac should we What dose of Ketorolac should we use for analgesia?use for analgesia?
Staquet 1989 – double blind RCT for cancer Staquet 1989 – double blind RCT for cancer pain. 10, 30, 60, 90 mg IMpain. 10, 30, 60, 90 mg IM No difference in pain reliefNo difference in pain relief
Menotti similar study for cancer pain - 10 and Menotti similar study for cancer pain - 10 and 30 mg IM ketorolac vs 75 mg diclofenac: 30 mg IM ketorolac vs 75 mg diclofenac: No differenceNo difference
Reuben post op pts on PCA morphine with Reuben post op pts on PCA morphine with Ketorolac as adjunct: Ketorolac as adjunct: Morphine sparing effect from Morphine sparing effect from 7.5 mg7.5 mg vs 5mg or vs 5mg or
placebo. placebo. No additional benefit from higher doses.No additional benefit from higher doses.

Additional studies with conflicting results Additional studies with conflicting results and high patient drop-out due to and high patient drop-out due to inadequate pain relief.inadequate pain relief.
Dose ceiling probably 10 mgDose ceiling probably 10 mg

Ketorolac vs IbuprofenKetorolac vs Ibuprofen
Turturro et al Turturro et al Double-blind RCT Double-blind RCT
comparing 60 mg IM comparing 60 mg IM ketorolac vs 800 mg PO ketorolac vs 800 mg PO ibuprofen for MSK painibuprofen for MSK pain
No difference in efficacyNo difference in efficacy Big difference in price. Big difference in price.
(170x)(170x)
Turturro MA, Paris PM, Seaberg DC. Intramuscular Ketorolac Versus Oral Turturro MA, Paris PM, Seaberg DC. Intramuscular Ketorolac Versus Oral Ibuprofen in Acute Musculoskeletal Pain. Annals of Emergency Medicine. Ibuprofen in Acute Musculoskeletal Pain. Annals of Emergency Medicine. 1995; 26(2): 117-122.1995; 26(2): 117-122.

Let’s talk about GI bleedsLet’s talk about GI bleeds
Million dollar question:Million dollar question:
Who is going to get the bleed?Who is going to get the bleed?
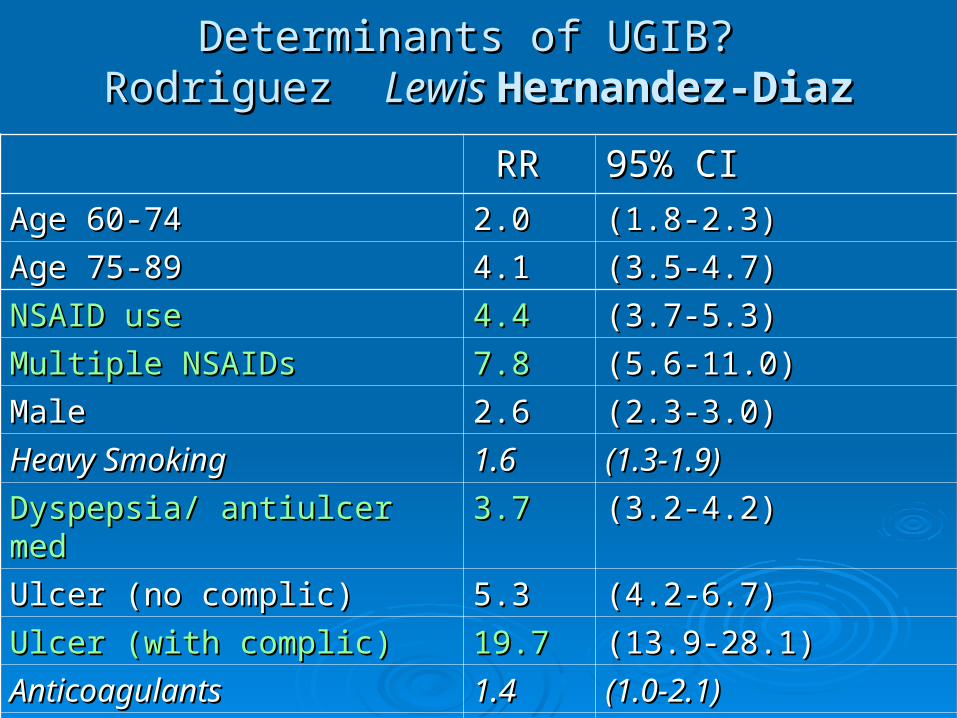
Determinants of UGIB? Determinants of UGIB? Rodriguez Rodriguez Lewis Lewis Hernandez-DiazHernandez-Diaz
RRRR 95% CI95% CIAge 60-74Age 60-74 2.02.0 (1.8-2.3)(1.8-2.3)
Age 75-89Age 75-89 4.14.1 (3.5-4.7)(3.5-4.7)
NSAID useNSAID use 4.44.4 (3.7-5.3)(3.7-5.3)
Multiple NSAIDsMultiple NSAIDs 7.87.8 (5.6-11.0)(5.6-11.0)
MaleMale 2.62.6 (2.3-3.0)(2.3-3.0)
Heavy SmokingHeavy Smoking 1.61.6 (1.3-1.9)(1.3-1.9)
Dyspepsia/ antiulcer medDyspepsia/ antiulcer med 3.73.7 (3.2-4.2)(3.2-4.2)
Ulcer (no complic)Ulcer (no complic) 5.35.3 (4.2-6.7)(4.2-6.7)
Ulcer (with complic)Ulcer (with complic) 19.719.7 (13.9-28.1)(13.9-28.1)
AnticoagulantsAnticoagulants 1.41.4 (1.0-2.1)(1.0-2.1)
CorticosteroidsCorticosteroids 1.61.6 (1.2-2.2)(1.2-2.2)

Duration controversyDuration controversy Highest risk during first week (conflicting btw studies) – Highest risk during first week (conflicting btw studies) –
LewisLewisShort term NANSAID useShort term NANSAID use 11.711.7 (6.5-(6.5-
21.0)21.0)Continuing NANSAID useContinuing NANSAID use 5.65.6 (4.6-7.0)(4.6-7.0)Recent NANSAID useRecent NANSAID use 3.23.2 (2.1-5.1)(2.1-5.1)
ARAMIS (Singh): INCREASING RISKARAMIS (Singh): INCREASING RISK After 5 yrs – 5x the risk as 1 yrAfter 5 yrs – 5x the risk as 1 yr After 1 yr - 4x the risk of 3 mosAfter 1 yr - 4x the risk of 3 mos Therefore no mucosal adaptationTherefore no mucosal adaptation
Age – steady increase in risk (ARAMIS) ~4% /yr increaseAge – steady increase in risk (ARAMIS) ~4% /yr increase

SSRI association?SSRI association? Case-control study of 1651 UGIB and 248 perfs Case-control study of 1651 UGIB and 248 perfs
Found UGIB RR of 3.0 (2.1-4.4) for current use of SSRIs Found UGIB RR of 3.0 (2.1-4.4) for current use of SSRIs
SSRI + NSAID increased risk of UGIB beyond sum of SSRI + NSAID increased risk of UGIB beyond sum of independent effects independent effects 15.615.6 ( 6.6 to 36.6) ( 6.6 to 36.6)
No effect on ulcer perforation.No effect on ulcer perforation.
De Abajo FJ, Rodriguez LA, Montero D. Association between selective serotonin reuptake De Abajo FJ, Rodriguez LA, Montero D. Association between selective serotonin reuptake inhibitors and upper gastrointestinal bleeding: population based case-control study. BMJ inhibitors and upper gastrointestinal bleeding: population based case-control study. BMJ 1999; 319: 106-1109. 1999; 319: 106-1109.

Individual NSAIDsIndividual NSAIDs
Big differences in toxicityBig differences in toxicity Acetaminophen and Ibuprofen lower risk Acetaminophen and Ibuprofen lower risk
for UGIB.for UGIB. Ketorolac more toxicKetorolac more toxic

Relative Risk for UGIB by individual Relative Risk for UGIB by individual NSAID (prescription dosing)NSAID (prescription dosing)
LewisLewis RodriguezRodriguez
AcetaminAcetamin 1.2 1.2
(1.1-1.5)(1.1-1.5)
IbuprofenIbuprofen 1.7 1.7
(1.1-2.5)(1.1-2.5)
2.1 2.1
(0.6-7.1)(0.6-7.1)
DiclofenacDiclofenac 4.9 4.9
(3.3-7.1)(3.3-7.1)
2.7 2.7
(1.5-4.8)(1.5-4.8)
NaproxenNaproxen 9.1 9.1
(6.0-13.7)(6.0-13.7)
4.3 4.3
(1.6-11.2)(1.6-11.2)
IndomethacinIndomethacin 6.0 6.0
(3.6-10.0)(3.6-10.0)
5.5 5.5
(1.6-18.9)(1.6-18.9)
KetorolacKetorolac 24.724.7
(9.6-63.5)(9.6-63.5)
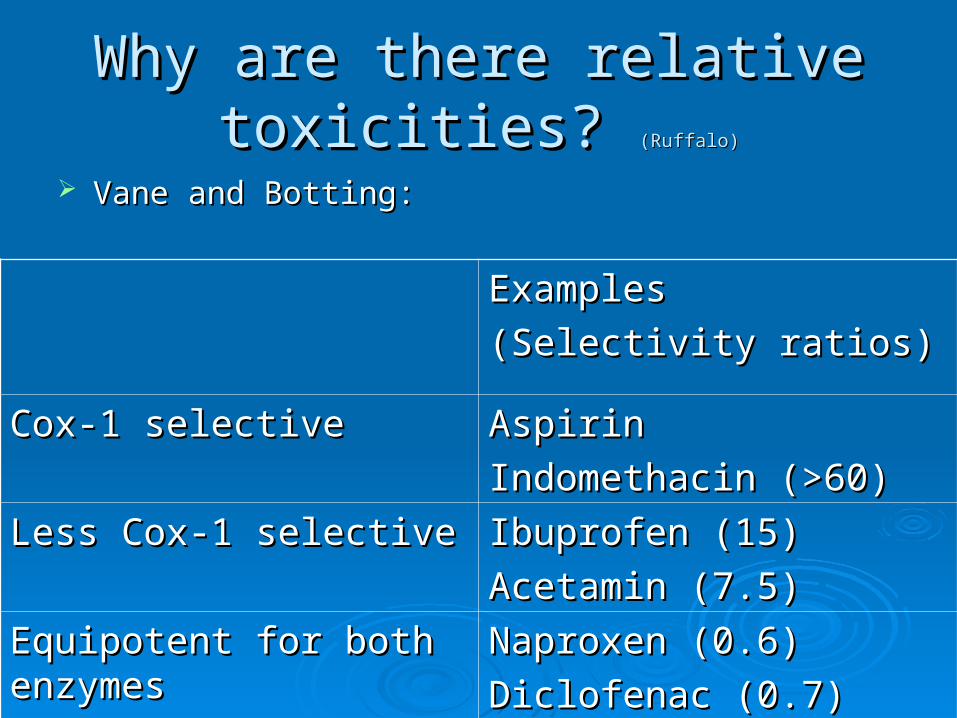
Why are there relative Why are there relative toxicities? toxicities? (Ruffalo)(Ruffalo)
Vane and Botting:Vane and Botting:
Examples Examples
(Selectivity ratios)(Selectivity ratios)
Cox-1 selectiveCox-1 selective AspirinAspirin
Indomethacin (>60)Indomethacin (>60)
Less Cox-1 selectiveLess Cox-1 selective Ibuprofen (15)Ibuprofen (15)
Acetamin (7.5)Acetamin (7.5)
Equipotent for both Equipotent for both enzymesenzymes
Naproxen (0.6) Naproxen (0.6)
Diclofenac (0.7)Diclofenac (0.7)
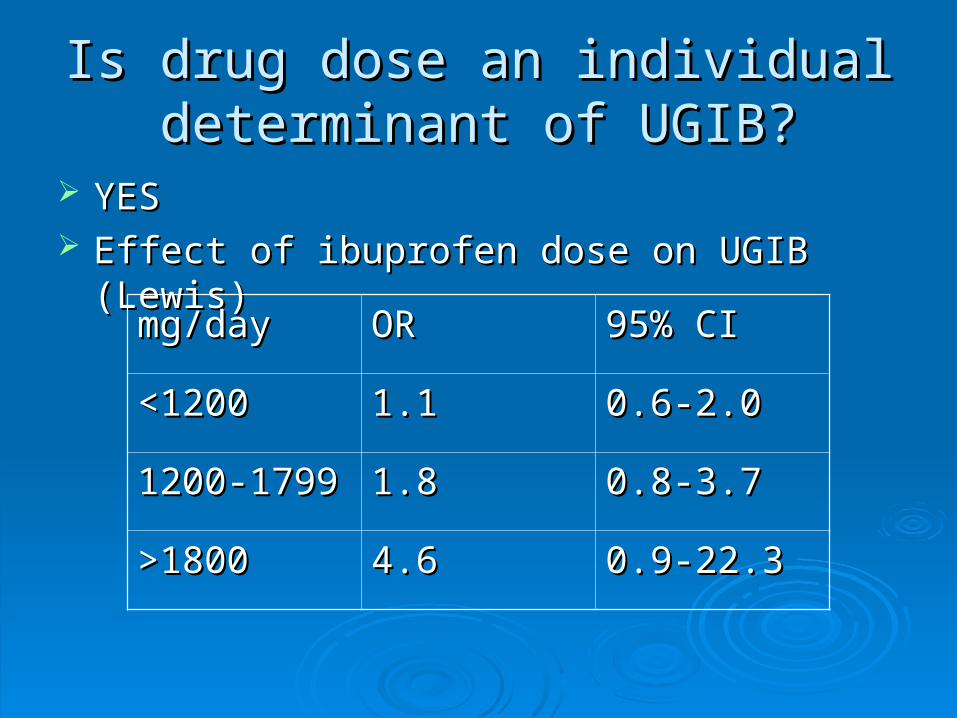
Is drug dose an individual Is drug dose an individual determinant of UGIB?determinant of UGIB?
YESYES Effect of ibuprofen dose on UGIB (Lewis)Effect of ibuprofen dose on UGIB (Lewis)
mg/daymg/day OROR 95% CI95% CI
<1200<1200 1.11.1 0.6-2.00.6-2.0
1200-17991200-1799 1.81.8 0.8-3.70.8-3.7
>1800>1800 4.64.6 0.9-22.30.9-22.3
Are there reliable warning Are there reliable warning signals before UGIB?signals before UGIB?
Singh: noSingh: no Dyspepsia is a common side effect but is Dyspepsia is a common side effect but is
poorly correlated with endoscopic lesions poorly correlated with endoscopic lesions or GI bleeding.or GI bleeding.
81% of pts81% of pts in ARAMIS study with serious in ARAMIS study with serious GI complications had no prior GI GI complications had no prior GI symptoms.symptoms.

Can we prevent the GI problem Can we prevent the GI problem with H2 antagonists/antacids?with H2 antagonists/antacids?
Singh – H2 antagonists, sucralfate and antacids Singh – H2 antagonists, sucralfate and antacids no protectionno protection ARAMIS cohort: pts with no previous GI SFX - use of ARAMIS cohort: pts with no previous GI SFX - use of
prophylactic GI meds had 2.5 x more hospitalizations for NSAID-prophylactic GI meds had 2.5 x more hospitalizations for NSAID-related GI complications – related GI complications –
OR 2.69 (1.36-5.31)OR 2.69 (1.36-5.31)
RRRR 95% CI95% CI
OmeprazoleOmeprazole 0.60.6 (0.4-0.9)(0.4-0.9)
MisoprostolMisoprostol 0.60.6 (0.4-1.0)(0.4-1.0)
H2-antagonistsH2-antagonists 1.41.4 (1.2-1.8)(1.2-1.8)

What should I remember from this What should I remember from this presentation?presentation?
Ibuprofen safe and effectiveIbuprofen safe and effective Ketorolac = astronomical risk of GI bleed.Ketorolac = astronomical risk of GI bleed. High risk: elderly, hx of PUD, smokers, High risk: elderly, hx of PUD, smokers,
steroids/anticoag, SSRIsteroids/anticoag, SSRI Unless previously established increased Unless previously established increased
NSAID requirements…NSAID requirements… Think Ibuprofen 400 mgThink Ibuprofen 400 mg Think Ketorolac 10 mg Think Ketorolac 10 mg
All NSAIDs have a dose ceiling!All NSAIDs have a dose ceiling!

ReferencesReferences Ashburn MA, Rubingh CR. The Role of Non-opioid Analgesics for the Management of Postoperative Pain Ashburn MA, Rubingh CR. The Role of Non-opioid Analgesics for the Management of Postoperative Pain
www.moffitt.usf.edu/.../ images/ashburnfig2.jpg www.moffitt.usf.edu/.../ images/ashburnfig2.jpg Cooper SA, Schachtel BP, Goldman E, et al. Ibuprofen and acetaminophen in the relief of acute pain: a randomized, double-Cooper SA, Schachtel BP, Goldman E, et al. Ibuprofen and acetaminophen in the relief of acute pain: a randomized, double-
blind, placebo-controlled study. J Clin Pharm, 1989;29:1026-1030.blind, placebo-controlled study. J Clin Pharm, 1989;29:1026-1030. De Abajo FJ, Rodriguez LA, Montero D. Association between selective serotonin reuptake inhibitors and upper gastrointestinal De Abajo FJ, Rodriguez LA, Montero D. Association between selective serotonin reuptake inhibitors and upper gastrointestinal
bleeding: population based case-control study. BMJ 1999; 319: 106-1109. bleeding: population based case-control study. BMJ 1999; 319: 106-1109. Doyle G, Furey S, Berlin R et al (1999). Gastrointestinal safety and tolerance of ibuprofen at maximum over-the-counterDoyle G, Furey S, Berlin R et al (1999). Gastrointestinal safety and tolerance of ibuprofen at maximum over-the-counter dose. dose.
Aliment Pharmacol Ther 13:897-906.Aliment Pharmacol Ther 13:897-906. Emerman CL, Spenetta J. EMR reports: Pain Management in the Emergency Department Feb 2002Emerman CL, Spenetta J. EMR reports: Pain Management in the Emergency Department Feb 2002 Hernandez-Diaz S, Rogriguez LAG. Epidemiologic Assessment of the Safety of Conventional Nonsteroidal Anti-Inflammatory Hernandez-Diaz S, Rogriguez LAG. Epidemiologic Assessment of the Safety of Conventional Nonsteroidal Anti-Inflammatory
Drugs. Amer J of Med. Feb 2001;110 (3A) 20S-27S.Drugs. Amer J of Med. Feb 2001;110 (3A) 20S-27S. Laska EM, Sunshine A, Marrero I, Olson N, Siegel C, McCormick N. The correlation between blood levels of ibuprofen and Laska EM, Sunshine A, Marrero I, Olson N, Siegel C, McCormick N. The correlation between blood levels of ibuprofen and
clinical analgesic response. Clin Pharmacol Ther 1986;40:1-7.clinical analgesic response. Clin Pharmacol Ther 1986;40:1-7. Kantor TG. Ibuprofen. Annals of Internal Medicine. 1979;91:877-882.Kantor TG. Ibuprofen. Annals of Internal Medicine. 1979;91:877-882. Lesko SM, Mitchell AA (1999). The safety of acetaminophen and ibuprofen among children younger than two years old. Lesko SM, Mitchell AA (1999). The safety of acetaminophen and ibuprofen among children younger than two years old.
Pediatrics 104(4):e39Pediatrics 104(4):e39 Lewis SC, Langman MJS< Laporte JR et al. Dose-response relationships between individual nonaspirin nonsteroidal anti-Lewis SC, Langman MJS< Laporte JR et al. Dose-response relationships between individual nonaspirin nonsteroidal anti-
inflammatroy drugs (NANSAIDs) and serious upper gastrointestinal bleeding: a meta-analysis based on indivicual patient data. inflammatroy drugs (NANSAIDs) and serious upper gastrointestinal bleeding: a meta-analysis based on indivicual patient data. Br J Clin Pharmacol . 54:320-26.Br J Clin Pharmacol . 54:320-26.
Moore N, van Ganse E, Le Parc J-M et al (1999) . The PAIN study: paracetamol, aspirin and ibuprofen new tolerability study. Moore N, van Ganse E, Le Parc J-M et al (1999) . The PAIN study: paracetamol, aspirin and ibuprofen new tolerability study. A large-scale, randomized clinical trial comparing the tolerability of aspirin, ibuprofen and paracetamol for short-term analgesia. A large-scale, randomized clinical trial comparing the tolerability of aspirin, ibuprofen and paracetamol for short-term analgesia. Clin Drug Invest 18:89-98Clin Drug Invest 18:89-98

ReferencesReferences Raney LH. Emedhome.com Evidence-bsed Use of NSAIDs in the ED. 2004.Raney LH. Emedhome.com Evidence-bsed Use of NSAIDs in the ED. 2004. Reuben SS, Connelly NR, Lurie S et al. Dose-Response of Ketorolac as an Adjunct to Patient-Controlled Analgesia Morphine in Patients Reuben SS, Connelly NR, Lurie S et al. Dose-Response of Ketorolac as an Adjunct to Patient-Controlled Analgesia Morphine in Patients
After Spinal Fusion Surgery. Anesthesia & Analgesia. 1998; 87(1): 98-102.After Spinal Fusion Surgery. Anesthesia & Analgesia. 1998; 87(1): 98-102. Rodriguez LAG, Cataruzzi C, TRoncon MG, et al. Risk of Hospitalization for Upper Gastrointestinal Tract Bleeding Associated with Rodriguez LAG, Cataruzzi C, TRoncon MG, et al. Risk of Hospitalization for Upper Gastrointestinal Tract Bleeding Associated with
Ketorolac, Other Nonsteroidal Anti-inflammatory Drugs, Calcium Antagonsits, and Other Antihypertensive Drugs. Arch Intern Med. Jan Ketorolac, Other Nonsteroidal Anti-inflammatory Drugs, Calcium Antagonsits, and Other Antihypertensive Drugs. Arch Intern Med. Jan 1998. 158:33-39.1998. 158:33-39.
Rodriguez LAG, Hernandez-Diaz S. Relative Risk of Upper Gastrointestinal Complications among Users of Acetaminophen and Rodriguez LAG, Hernandez-Diaz S. Relative Risk of Upper Gastrointestinal Complications among Users of Acetaminophen and Nonsteroidal Anti-Inflammatory Drugs. Epidemiology. 2001; 12(5):570-576. Nonsteroidal Anti-Inflammatory Drugs. Epidemiology. 2001; 12(5):570-576.
Ruffalo RL, Jackson RL, Ofman JJ. The Impact of NSAID Selection on Gastrointestinal Injury and Risk for Cardiovascular Events: Ruffalo RL, Jackson RL, Ofman JJ. The Impact of NSAID Selection on Gastrointestinal Injury and Risk for Cardiovascular Events: Identifying and Treating Patients at Risk. P&T. Nov 2002 27 (11):570-576.Identifying and Treating Patients at Risk. P&T. Nov 2002 27 (11):570-576.
Senior K. Homing in on Cox-3 – the elusive target of paracetamol. Lancet 2002 vol 1 399.Senior K. Homing in on Cox-3 – the elusive target of paracetamol. Lancet 2002 vol 1 399. Schwab JM, Schluesener HJ, Laufer S. Lancet 2003; 361: 981-982. Schwab JM, Schluesener HJ, Laufer S. Lancet 2003; 361: 981-982. Singh G. Recent Considerations in Nonsteroidal Anti-Inflammatory Drug Gastropathy. Amer J Med. July 1998; 105 (1B): 31S-38SSingh G. Recent Considerations in Nonsteroidal Anti-Inflammatory Drug Gastropathy. Amer J Med. July 1998; 105 (1B): 31S-38S Staquet MJ. A Double-Blind Study with Placebo Control of Intramuscular Ketorolac Tromethamine in the Treatment of Cancer Pain. J Staquet MJ. A Double-Blind Study with Placebo Control of Intramuscular Ketorolac Tromethamine in the Treatment of Cancer Pain. J
Clin Pharmacol 1989;29:1031-1036.Clin Pharmacol 1989;29:1031-1036. Turturro MA, Paris PM, Seaberg DC. Intramuscular Ketorolac Versus Oral Ibuprofen in Acute Musculoskeletal Pain. Annals of Turturro MA, Paris PM, Seaberg DC. Intramuscular Ketorolac Versus Oral Ibuprofen in Acute Musculoskeletal Pain. Annals of
Emergency Medicine. 1995; 26(2): 117-122.Emergency Medicine. 1995; 26(2): 117-122. Wang RY, Girard DD, Aleguas A. EMR reports Over-the-Counter (OTC) Medications: A Quick Consult Guide to the Evaluation and Wang RY, Girard DD, Aleguas A. EMR reports Over-the-Counter (OTC) Medications: A Quick Consult Guide to the Evaluation and
Management of Toxic Effects and Adverse Reactions Part II: Systemic, Oral, and Miscellaneous Preparations Feb 2001Management of Toxic Effects and Adverse Reactions Part II: Systemic, Oral, and Miscellaneous Preparations Feb 2001 Winter L, Bass E, Recant B, Cahaly JF. Analgesic activity of ibuprofen (Motrin) in postoperative oral surgery pain. Oral Surg Oral Med Winter L, Bass E, Recant B, Cahaly JF. Analgesic activity of ibuprofen (Motrin) in postoperative oral surgery pain. Oral Surg Oral Med
Oral Path 1978;45:159-166.Oral Path 1978;45:159-166. Yee JP, Koshiver JE, Allbon C. Comparison of intramuscular Ketorolac Tromethamine and Morphine Sulfate for Analgesia of Pain After Yee JP, Koshiver JE, Allbon C. Comparison of intramuscular Ketorolac Tromethamine and Morphine Sulfate for Analgesia of Pain After
major Surgery. Pharmacotheraphy. 1986; 6(5): 253-261.major Surgery. Pharmacotheraphy. 1986; 6(5): 253-261.

Questions?Questions?





























