Embed Size (px)
Citation preview

November 10th, 2015
Webinar sponsored by:The Center for Excellence in Primary Care and the Center for Care Innovations
Barry L. Carter Pharm.D., FCCP, FAHA, FASH, FAPHA
The Patrick E. Keefe Professor in PharmacyUniversity of Iowa
Moderated By:J. Nwando Olayiwola, MD, MPH, FAAFP
Tem Woldeyesus, BSKira Levy, MS
Center for Excellence in Primary Care

22

Care Integration Resource Center

Team-based Care for Hypertension Team-based Care for Hypertension in the Age of Healthcare Reformin the Age of Healthcare Reform
Team-based Care for Hypertension Team-based Care for Hypertension in the Age of Healthcare Reformin the Age of Healthcare Reform
Barry L. Carter, Pharm.D., FCCP, FAHA, FASH, FAPHAThe Patrick E. Keefe Professor in Pharmacy
Department of Pharmacy Practice and ScienceCollege of Pharmacy and
ProfessorDepartment of Family Medicine
Roy J. and Lucille A. Carver College of MedicineUniversity of Iowa

Disclosure of Relationships
• Grant Support: NIH, AHRQ, VA Grant Support: NIH, AHRQ, VA HSR&D.HSR&D.
• Member of the JNC 5, 6, 7 and 8 Member of the JNC 5, 6, 7 and 8 committeescommittees
• I have had NONE of the following I have had NONE of the following in the past 18 years: in the past 18 years: Consultant, Consultant, Speakers Bureau, Major Stock Speakers Bureau, Major Stock Shareholder, or Other Support from Shareholder, or Other Support from Industry.Industry.

1.To discuss evidence-based strategies for implementing team-based care for the management of hypertension.
2.To describe components and results of the CAPTION Trial.
ObjectivesObjectives

Limitations with many studies evaluating team-based care
Small sample sizes (low power or limited generalizability)
Single site and single intervention pharmacist or nurse
Bias in BP measurementLack of control groups (pre- post- design only)No evaluation of key covariatesFew were intention-to-treat analyses
Carter BL, Bosworth HB, Green BB. State of the Art Review: Carter BL, Bosworth HB, Green BB. State of the Art Review: The Hypertension Team: The role of the pharmacist, nurse The Hypertension Team: The role of the pharmacist, nurse and teamwork in hypertension therapy. J Clin Hypertens and teamwork in hypertension therapy. J Clin Hypertens 2012;14:51-652012;14:51-65

O r i g i n a l P a p e r
A Cluster Randomized Trial to Evaluate Physician/Pharmacist Collaboration toImprove Blood Pressure Control
Barry L. Carter, PharmD; George R. Bergus, MD; Jeffrey D. Dawson, ScD; Karen B. Farris, PhD; William R. Doucette, PhD;
Elizabeth A. Chrischilles, PhD; Arthur J. Hartz, MD, PhD
Funded by NHLBI: RO1 HL69801Funded by NHLBI: RO1 HL69801
Journal of Clinical Hypertension 2008;10:260-Journal of Clinical Hypertension 2008;10:260-271271
Cluster, Randomized Efficacy Trial

Physician/PharmacistPhysician/PharmacistCollaborative ManagementCollaborative Management

Collaborative Management of Collaborative Management of Hypertension StudyHypertension Study: Efficacy : Efficacy
TrialTrial• Only faculty / private physicians involved in the study.• Patients 21-85 years with diagnosis of hypertension.• Baseline BP: 145-179 SBP or 95-109 DBP for
uncomplicated.• 135-179 SBP or 85-109 DBP for diabetes.
• Research BP at 0, 2, 4, 6, 8, 9 months• 24-hour BP at baseline and 9 months
Journal of Clinical Hypertension Journal of Clinical Hypertension 2008;10:260-2712008;10:260-271

InterventionIntervention
• Pharmacist conducted interview and assessed patient for strategies to improve BP control.
• Pharmacist made recommendations to MD and patient to improve BP control.
• Pharmacists and physicians worked to overcome/prevent sub-optimal treatment, clinical inertia, poor adherence, adverse reactions, drug interactions
• Pharmacists saw patients at least every 2 months x 9 months.
NHLBI: RO1 HL69801

Data AnalysisData Analysis
• Continuous variables – likelihood-based mixed models with random patient effects fit to SAS Proc Mixed in an intention-to-treat analysis.
• Models adjusted for baseline BP, age, gender, race, education, insurance status, household income, marital status, smoking status, alcohol intake, BMI, number of co-existing conditions, baseline medication adherence and total number of visits during the study.

Baseline Demographics
Control (n=78) Intervention (n=101)
Age 61.0 + 11.3 59.6 + 13.7*
BP meds 1.4 + 1.0 1.5 + 1.0
Baseline med adherence
88.6% 71.1%*
# co-existing DX 0.46 + 0.78 0.47 + 0.81
Diabetes 24.4% 24.8%
BMI (kg/m2) 31.8 (+14.7) 32.3 (+7.7)
* p < 0.001* p < 0.001

Results: BP Control RatesResults: BP Control Rates
Control Interven-tion
Adjusted OR
CI; p value
All patients
52.9% 89.1% 8.9 3.8-20.7P<0.00
1
Diabetes
23.5% 81.8% 40.1 4.1-394.7
P=0.002
- Carter BL, Bergus GR, Dawson et al. Journal of - Carter BL, Bergus GR, Dawson et al. Journal of Clinical Hypertension 2008;10:260-271.Clinical Hypertension 2008;10:260-271.
- Von Muenster SJ, et al. Pharmacy World & - Von Muenster SJ, et al. Pharmacy World & Science 2008:30:128-135.Science 2008:30:128-135.
Main Finding: The major reason for the high control was due to intensification of medications.

Physicians accepted 95.8% of 267 pharmacist recommendations
Recommendation Frequency by Visit
0
MoOpt
2 Mo
4 Mo
6 Mo
8 Mo
9 Mo
Added Thiazide n=45 40 2 3 0 0 0 NA
Added Other Drug n=79
30 13 18 9 6 3 NA
Increased Dose n=89 28 21 14 9 9 8 NA
Changed Dose Frequency n=7
2 0 1 3 1 0 NA
Switch Within Class n=15 6 3 1 3 2 0 NA
Decreased Dose n=14 3 3 3 2 3 0 NA
Drug Discontinued n=18 2 4 8 3 1 0 NA
Total n=267
111 46 48 29 22 11 NA
BP Control Rate n=101 0 - 52% 67% 73% 84% 89%• Von Muenster SJ, Carter BL, Weber CA et al. Description of Description of
pharmacist interventions during physician-pharmacist co-pharmacist interventions during physician-pharmacist co-management of hypertension. Pharmacy World & Science management of hypertension. Pharmacy World & Science 2008:30:128-135.2008:30:128-135.

ORIGINAL INVESTIGATIONORIGINAL INVESTIGATION
Physician and Pharmacist Collaboration to Improve Blood Pressure Control
Barry L. Carter, PharmD; Gail Ardery, PhD; Jeffrey D. Dawson, ScD; Paul A. James, MD; George R. Bergus, MD; William R. Doucette, PhD; Elizabeth A. Chrischilles, PhD; Carrie L. Franciscus, MA; Yinghui Xu, MS
HEALTH CARE REFORMHEALTH CARE REFORM
Trial Registration: clinicaltrials.gov Identifier:Trial Registration: clinicaltrials.gov Identifier:NCT00201019NCT00201019
Arch Intern Med. 2009;169(21):1996-2002Arch Intern Med. 2009;169(21):1996-2002
““MixedMixed”” Efficacy-Effectiveness Efficacy-Effectiveness trialtrial

Guideline Adherence Study: Guideline Adherence Study: Combination of Efficacy and Combination of Efficacy and
EffectivenessEffectiveness
Guideline Adherence Study: Guideline Adherence Study: Combination of Efficacy and Combination of Efficacy and
EffectivenessEffectiveness• Prospective, cluster-randomized controlled trial in 6
community-based family medicine residency clinics all with clinical pharmacist faculty in the medical office.
• Research nurse in each clinic measured BP at baseline, 3 and 6 months and 24-hour BP at baseline and 6 months.

InterventionIntervention
• Pharmacist conducted interview and assessed patient for strategies to improve BP control.
• Pharmacist made recommendations to MD and patient to improve BP control.
• Pharmacists and physicians worked to overcome/prevent sub-optimal treatment, clinical inertia, poor adherence
• Pharmacists only encouraged to see patients at baseline and 1 month with a telephone call at 3 months with a goal to achieve BP control by 6 months (but they could see patients more often).

Research BP MeasurementResearch BP Measurement
• Automated Omron Device
• Measure 1 BP, record but do not use for research value
• Measure 2 BP values and average them if less than 4 mm Hg apart.
• If more than 4 mm different, measure a 4th BP and average the 2 closest BP values (from the 2nd to 4th BP measurements).

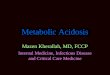
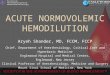
Systolic Blood Pressure
•- p<0.001; **- p=0.0015; *** - p=0.0023- p<0.001; **- p=0.0015; *** - p=0.0023Arch Intern Med. 2009;169(21):1996-2002Arch Intern Med. 2009;169(21):1996-2002Journal of Clinical Hypertension 2011;13:431-437.Journal of Clinical Hypertension 2011;13:431-437.
Retrospective evaluation of sustainability…

21
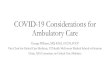
Meta-Analysis: Potency of individual components of team-based care (n=37 controlled trials)
Median reduction in SBP(mm Hg)
Pharmacist recommended medication to physician -9.3*
Education on BP medications -8.75*
Pharmacist did the intervention -8.44
Assessed medication compliance -7.9
Counseling on lifestyle modification -7.59
Nurse did the intervention -4.8*
Carter BL, Rogers M, Daly J, Zheng S, James JA. Quality Improvement Strategies Carter BL, Rogers M, Daly J, Zheng S, James JA. Quality Improvement Strategies for Hypertension: The Potency of Team-based Care Interventions. Archives of for Hypertension: The Potency of Team-based Care Interventions. Archives of Internal Medicine 2009; 169:1748-1755.Internal Medicine 2009; 169:1748-1755. Adapted from the methods of:Adapted from the methods of:Walsh J et al. Hypertension Care. Closing the Quality Gap: A critical analysis of quality Walsh J et al. Hypertension Care. Closing the Quality Gap: A critical analysis of quality improvement strategies. (Prepared by Stanford -UCSF Evidence-based Practice Center, improvement strategies. (Prepared by Stanford -UCSF Evidence-based Practice Center, Contract No. 290-02-0017). AHRQ publication No. 04-0051-3, Rockville, MD. January 2005.Contract No. 290-02-0017). AHRQ publication No. 04-0051-3, Rockville, MD. January 2005.
*- statistically *- statistically significantsignificant

22
Meta-analysis of Potency of individual components of team-based care
Odds that BP was controlled (95% confidence Interval)
Studies involving nurses 1.69 (1.48-1.93)
[69% increased chance]
Studies involving pharmacists within physician offices or clinics
2.48 (2.05-2.99)
[148% increased chance]
Studies done in community pharmacies
2.89 (1.83-4.55)
[189% increased chance]
Carter BL, et al. Archives of Internal Medicine 2009; 169:1748-Carter BL, et al. Archives of Internal Medicine 2009; 169:1748-1755.1755.
Conclusion: All were effective but Conclusion: All were effective but interventions by pharmacists appear to be interventions by pharmacists appear to be more potent than by nurses.more potent than by nurses.

Collaboration Among Pharmacists
and Physicians To Improve
Outcomes Now
(CAPTION)
Collaboration Among Pharmacists
and Physicians To Improve
Outcomes Now
(CAPTION) Barry L. Carter, Pharm.D.Barry L. Carter, Pharm.D.Principal Investigator, CCCPrincipal Investigator, CCCDepartment of Pharmacy Practice and Department of Pharmacy Practice and Science, College of Pharmacy andScience, College of Pharmacy andProfessor Professor Department of Family MedicineDepartment of Family Medicine Roy J. and Lucille A. Carver College of Roy J. and Lucille A. Carver College of MedicineMedicine
Christopher Coffey, Ph.D.Christopher Coffey, Ph.D.Principal Investigator, DCCPrincipal Investigator, DCCProfessor and Director, Clinical Trials DataProfessor and Director, Clinical Trials Data Management CenterManagement Center
College of Public HealthCollege of Public Health
• Funded by NHLBI/NIH, R01 HL091841Carter et al. A Cluster-randomized Trial of a Physician/Pharmacist Collaborative Model to Improve Blood Pressure Control. Circulation: Cardiovascular Quality and Outcomes. 2015; 8:235-43..

CAPTION Study OutcomesPrimary outcome = BP control @ 9 months
BP control defined as:• < 140/90 for patients with uncomplicated
hypertension
• < 130/80 for patients with diabetes or chronic kidney disease**
Secondary endpoints:
• Mean BP @ 12, 18, 24 months

CAPTIONCAPTIONCAPTIONCAPTION
Offices Stratified on: 1. Pharmacy Structure Score (high vs. low) 2. Percent minorities (<44% vs. >44%)
32 offices randomized to:1. Usual care group2. 9-month pharmacist intervention3. 24-month pharmacist intervention.
Subjects followed for 24 months to determine:1. What happens when the intervention is
stopped?2. Does the intervention benefit patients from
minority groups?

Participating Locations

DemographicsDemographicsDemographicsDemographicsVariable 9 Month
(N=194)N (%)
24 Month (N=207)
N (%)
Control (N=224)N (%)
Total (N=625)N (%)
p-value
Female 119 (61.3) 125 (60.4) 133 (59.4) 377 (60.3) 0.938
Age (SD) 60.6 (12.4) 56.7 (11.8) 60.5 (13.8) 59.3 (12.8) 0.055BMI (SD) 33.8 (8.5) 35.2 (9.0) 32.9 (7.7) 33.9 (8.5) 0.090DM or CKD *
102 (52.6%)
109 (52.7%)
103 (46.0%)
314(50.2%)
0.599
5SBP (SD)
147.6 (13.7)
149.8 (15.6)
149.6 (15.3)
149.1 (15.0)
0.458
* lower treatment goal (<130/80) making it more * lower treatment goal (<130/80) making it more difficult to achieve controldifficult to achieve control
Carter et al. Carter et al. Circulation: Circulation: Cardiovascular Quality and Cardiovascular Quality and Outcomes. 2015; 8:235-43.Outcomes. 2015; 8:235-43.

Primary Outcome 9-Month BP Primary Outcome 9-Month BP ControlControl
Primary Outcome 9-Month BP Primary Outcome 9-Month BP ControlControl
Variable
Intervention Groups
(N = 401)(N=226
minorities)
Control Group
(N = 224) (N=111
minorities)
Model-Adjusted Difference –
Intervention vs. Control(95% CI)
p-value
BP Control All subjects
43% 34% 1.57 ( 0.99 , 2.50 )
0.059
BP Control Minorities
37% 28% 1.54 ( 0.83 , 2.86 ) 0.17
* Defined as <140/90 for uncomplicated BP, <130/80 for diabetes or * Defined as <140/90 for uncomplicated BP, <130/80 for diabetes or CKDCKD Carter et al. Carter et al. Circulation: Circulation:
Cardiovascular Quality and Cardiovascular Quality and Outcomes. 2015; 8:235-43.Outcomes. 2015; 8:235-43.

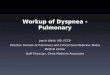
9 – month BP- All subjects9 – month BP- All subjects9 – month BP- All subjects9 – month BP- All subjects
VariableIntervention
Groups(N = 401)
Control Group
(N = 224)
Model-Adjusted
Difference – Intervention vs. Control
(95% CI)
p-value
SBP Mean (SD)
131.6 (15.8)
138.2 (19.7)
-6.1( -9.75, -2.39 )
0.002
DBP Mean (SD)
76.3 (11.1)
78.0 (14.5)
-2.9( -4.85, -0.93 )
0.005
Carter et al. Carter et al. Circulation: Circulation: Cardiovascular Quality and Cardiovascular Quality and Outcomes. 2015; 8:235-43.Outcomes. 2015; 8:235-43.

Results – Minority subjectsResults – Minority subjectsResults – Minority subjectsResults – Minority subjects
VariableIntervention
Groups(N = 226)
Control Group
(N = 111)
Model Adjusted
Difference – Intervention vs. Control
(95% CI)
p-value
SBP Mean (SD)
133.0 (16.3)
140.3 (21.4)
-6.4( -11.16, -1.68 ) 0.009
DBP Mean (SD)
77.9 (10.7)
78.8 (15.9)
-2.9( -5.88, -0.08 ) 0.044

Pharmacist Visits/ContactsPharmacist Visits/ContactsPharmacist Visits/ContactsPharmacist Visits/Contacts
GroupFirst 9 Months (rate/month)
9-24 Months(rate/month)
9 –Month Group 0.58 0.07
24 – Month Group 0.50 0.26

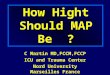
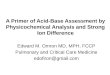
Dose Increase or Dose Increase or Medication Addition at 9 Medication Addition at 9
monthsmonths
Dose Increase or Dose Increase or Medication Addition at 9 Medication Addition at 9
monthsmonths
Time Period
Usual Care9-month
intervention24-month
intervention
0 to 9Months
0.7 + 1.0* 3.1 + 3.2 2.7 + 3.1
* p<0.001* p<0.001

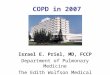
Systolic BP ResultsSystolic BP Results

2014 Evidence-Based 2014 Evidence-Based Guideline for the Management Guideline for the Management
of High Blood Pressure in of High Blood Pressure in AdultsAdults
ReReport from the Panel Members port from the Panel Members Appointed to the Eighth Joint National Appointed to the Eighth Joint National
Committee (JNC 8)Committee (JNC 8)James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, Lackland DT, Lefevre ML, Mackenzie TD, Ogedegbe O,
Smith SC Jr, Svetkey LP, Taler SJ, Townsend RR, Wright JT Jr, Narva AS, Ortiz E
James PA, Oparil S, Carter BL et al. JAMA. 2014; 311 (February James PA, Oparil S, Carter BL et al. JAMA. 2014; 311 (February 5):507-520. 5):507-520.

Sensitivity Analysis Using JNC-8Sensitivity Analysis Using JNC-8
• If we exclude 138 subjects who would If we exclude 138 subjects who would not have qualified because their BP not have qualified because their BP would have been considered controlled would have been considered controlled by JNC-8, 9-month BP Control:by JNC-8, 9-month BP Control:
Intervention BP Control
Usual Care BP Control
OR(95% CI)
p-value
61% 45% 2.03 (1.29, 3.22)
0.003
Carter et al. Carter et al. Circulation: Circulation: Cardiovascular Quality and Cardiovascular Quality and Outcomes. 2015; 8:235-43.Outcomes. 2015; 8:235-43.

Economics of Team Care: Economics of Team Care: Community Preventive Community Preventive
Services Task Force: 2012Services Task Force: 2012• 31 studies total31 studies total• Intervention for BP cost $198 per Intervention for BP cost $198 per person per year.person per year.• $87 per mm reduction in SBP.$87 per mm reduction in SBP.• 20 year cost per QALY:20 year cost per QALY:
– $24,042 for Nurse$24,042 for Nurse– $10,244 for Pharmacist and other$10,244 for Pharmacist and other
Jacob V et al. Am J Prev Med 2015;49:772-83.Jacob V et al. Am J Prev Med 2015;49:772-83.

37
Community Preventive Services Task Force
(30% of studies non-U.S.)Median %
improved BP control
Median reduction SBP
mm HG
Nurses
(n=16 studies)
8.5 5.4
Pharmacists
(n=11 studies)
22.0 5.0
Nurse + Pharmacist
(4=studies)
16.2 5.6
Proia KK, et al. Am J Prev Med 2014;47:86-99Proia KK, et al. Am J Prev Med 2014;47:86-99

CAPTION Cost and RVU CAPTION Cost and RVU AnalysesAnalyses
CAPTION Cost and RVU CAPTION Cost and RVU AnalysesAnalyses
Included Brian Isetts, Ph.D. and Dan Included Brian Isetts, Ph.D. and Dan Buffington, Pharm.D. as consultants to Buffington, Pharm.D. as consultants to perform RVU analysis.perform RVU analysis.
Linnea Polgreen, Ph.D. conducting cost-Linnea Polgreen, Ph.D. conducting cost-effectiveness analysis. effectiveness analysis.
Manuscript in reviewManuscript in review

CAPTION Cost and RVU CAPTION Cost and RVU Analyses (N=390) first 9 Analyses (N=390) first 9
monthsmonths
CAPTION Cost and RVU CAPTION Cost and RVU Analyses (N=390) first 9 Analyses (N=390) first 9
monthsmonths Pharmacists made 1,169 Pharmacists made 1,169 recommendations to:recommendations to:
start a new drug (443)start a new drug (443) discontinue a drug (283)discontinue a drug (283) increase dose (329)increase dose (329) decrease dose (94)decrease dose (94) change regimen-same dose (20)change regimen-same dose (20)
Physicians accepted 1,153 (Physicians accepted 1,153 (98.6%98.6%))

CAPTION Pharmacist TimeActivity Minutes to complete activity (circle one)
Medical record review prior to patient visit.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 >30
Consultation with other provider or family
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 >30
Patient assessment/medication history
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 >30
Medical record review during patient visit
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 >30
Order laboratory 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 >30
Order medications/write prescriptions
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 >30
Medical education 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 >30
Lifestyle modification education
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 >30
Education on BP measurement
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 >30
Recommendations to MD 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 >30
Documentation in medical record
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 >30

CAPTION Cost and RVU CAPTION Cost and RVU AnalysesAnalyses
CAPTION Cost and RVU CAPTION Cost and RVU AnalysesAnalyses
Drs. Isetts and Buffington consult Drs. Isetts and Buffington consult directly with CMS and AMA on CPT directly with CMS and AMA on CPT coding.coding.
These data will be used to better These data will be used to better establish relative value units establish relative value units (RVUs) for pharmacist intervention (RVUs) for pharmacist intervention and re-imbursement mechanisms.and re-imbursement mechanisms.

Cost-Effectiveness AnalysisCost-Effectiveness AnalysisCost-Effectiveness AnalysisCost-Effectiveness Analysis The additional cost of the The additional cost of the
intervention was $203 or $33 for intervention was $203 or $33 for each mm Hg reduction in SBP or each mm Hg reduction in SBP or $23 for each percentage point $23 for each percentage point increase in BP control over 9 increase in BP control over 9 months.months.
Polgreen LA, Han J, Carter BL et al. Polgreen LA, Han J, Carter BL et al. Hypertension 2015 (in press)Hypertension 2015 (in press)

Cost-Effectiveness AnalysisCost-Effectiveness AnalysisCost-Effectiveness AnalysisCost-Effectiveness AnalysisVariable Intervention*
(N=539)Control *(N = 194)
P value
Changed BP Medications
251 (493) 160 (392) 0.028
Total cost BP Medications
857 (829) 838 (982) 0.808
Pharmacists Costs
144 (102) 0 <0.001
Physician Costs
88 (105) 105 (88) 0.055
Total Costs
1340 (1064)
1103 (1118)
0.017* - Mean (SD) U.S. * - Mean (SD) U.S. dollarsdollars

CAPTION Conclusions• Clinic-based pharmacists in primary care
enhance effectiveness for BP control.• 53% were minorities (2/3 AA, 1/3 Hispanic).• Many of the subjects in CAPTION had not had
controlled BP for years.• > 25% - Medicaid/ self-pay, about 50% had
incomes <$25,000/yr, 50% had DM or CKD.• Cost compared to usual care - $203 ($33/mm
Hg reduction in SBP), $23 for each percentage point increase in BP control.

Recommendations of the Recommendations of the Community Preventive Community Preventive
Services Task ForceServices Task Force• Include team-based care to improve Include team-based care to improve BP.BP.• More research needed on the type of More research needed on the type of provider-patient interaction needed.provider-patient interaction needed.• More research needed in More research needed in disadvantaged populations.disadvantaged populations.• Need more information on strategies Need more information on strategies to develop teams, resources to develop teams, resources infrastructure and costs.infrastructure and costs.
Am J Prev Med 2014;47:100-102Am J Prev Med 2014;47:100-102

Recommendations• Team-based care should be a critical component
of primary care to improve BP control in African Americans (SBP reductions of 5-14 mm Hg).
• A pharmacist and nurse should be integrated into practices to improve BP control.
• Several studies have found that the most potent strategy appears to be medication intensification.
• The team member (pharmacist or nurse) should independently implement the intervention as this is the most effective strategy for rapid implementation.

Comments and QuestionsComments and QuestionsComments and QuestionsComments and Questions