Embed Size (px)
Citation preview

Cancer Therapy: Preclinical
NovelActionsofNext-GenerationTaxanesBenefitAdvanced Stages of Prostate CancerRen�ee de Leeuw1, Lisa D. Berman-Booty1, Matthew J. Schiewer1, Stephen J. Ciment1,Robert B. Den2,3, Adam P. Dicker2,3,William K. Kelly3,4, Edouard J. Trabulsi3,5,Costas D. Lallas3,5, Leonard G. Gomella3,5, and Karen E. Knudsen1,2,3,4,5
Abstract
Purpose: To improve the outcomes of patients with castra-tion-resistant prostate cancer (CRPC), there is an urgent needfor more effective therapies and approaches that individualizespecific treatments for patients with CRPC. These studies com-pared the novel taxane cabazitaxel with the previous generationdocetaxel, and aimed to determine which tumors are mostlikely to respond.
Experimental design: Cabazitaxel and docetaxel were com-pared via in vitro modeling to determine the molecular mecha-nism, biochemical and cell biologic impact, and cell proliferation,which was further assessed ex vivo in human tumor explants.Isogenic pairs of RB knockdown and control cells were interro-gated in vitro and in xenograft tumors for cabazitaxel response.
Results: The data herein show that (i) cabazitaxel exerts stron-ger cytostatic and cytotoxic response compared with docetaxel,
especially in CRPC; (ii) cabazitaxel induces aberrant mitosis,leading to pyknotic and multinucleated cells; (iii) taxanes do notact through the androgen receptor (AR); (iv) gene-expressionprofiling reveals distinct molecular actions for cabazitaxel; and(v) tumors that have progressed to castration resistance via loss ofRB show enhanced sensitivity to cabazitaxel.
Conclusions: Cabazitaxel not only induces improved cytostat-ic and cytotoxic effects, but also affects distinct molecular path-ways, compared with docetaxel, which could underlie its efficacyafter docetaxel treatment has failed in patientswithCRPC. Finally,RB is identified as the first potential biomarker that could definethe therapeutic response to taxanes in metastatic CRPC. Thiswould suggest that loss of RB function induces sensitization totaxanes, which could benefit up to 50% of CRPC cases. Clin CancerRes; 21(4); 795–807. �2015 AACR.
IntroductionProstatic adenocarcinoma is the most frequently diagnosed
noncutaneous malignancy among men in Western civilizationand a leading cause of death by cancer (1, 2). The first line oftherapeutic intervention for disseminated disease targets theandrogen receptor (AR) through androgen ablative strategies(androgen deprivation therapy, ADT), frequently complementedwith AR antagonists (3). Although initially effective, castration-resistant prostate cancer (CRPC) develops within amedian of 2 to3 years after initiating primary androgen ablation therapy (4).
Prostatic adenocarcinoma generally responds poorly to stan-dard cytotoxic regimens, and modest clinical benefit has beenachieved with the chemotherapeutic docetaxel in metastaticCRPC (mCRPC; ref. 5). Since 2010, several novel therapeutic
agents, with distinct mechanisms of action, have been approvedfor treatment of CRPC. These include: (i) the antiandrogenenzalutamide (6, 7), (ii) the CYP17A1 inhibitor abirateroneacetate (8), (iii) the alpha-emitting radiopharmaceutical radi-um-233 (9), (iv) the immunotherapeutic sipuleucel-T (10), and(v) the new-generation taxane cabazitaxel (11, 12). Althoughradium-233, sipuleucel-T, abiraterone, and enzalutamide can beused pre- or post-docetaxel, cabazitaxel is currently approved forpatients with mCRPC who have progressed on docetaxel therapy(13). Despite the recent increase in treatment options, and poten-tial combination or sequential regimens, patients ultimatelysuccumb to the disease, with a median survival of patients withmCRPC of 48 months in a SWOG III trial (14), and 15 to 18months post-docetaxel (15). The limited therapeutic successemphasizes the need for more efficacious drugs and a patient-tailored approach toward cancer therapy to improve diseaseoutcome.
Cabazitaxel is a second-generation taxane, belonging to a classof compounds that stabilize themicrotubules by binding b-tubu-lin, and promote their polymerized state. Taxanes attenuate themicrotubule dynamicity, impairing the dynamics of the mitoticspindle, and inducingmitotic arrest, microtubule nucleation, andapoptosis (16, 17). Although cabazitaxel and docetaxel bothtarget b-tubulin, the TROPIC clinical trial (NCT00417079) inpatients with mCRPC presenting with progressive diseaseafter docetaxel treatment demonstrated that cabazitaxel stillhas therapeutic efficacy after docetaxel failure (11). Critical gapsin our knowledge of cabazitaxel include understanding of: (i) themolecular mechanisms underlying the differential response tocabazitaxel versus docetaxel; (ii) the optimal clinical state for
1Department of Cancer Biology, Thomas Jefferson University, Phila-delphia, Pennsylvania. 2Department of Radiation Oncology, ThomasJeffersonUniversity, Philadelphia, Pennsylvania. 3KimmelCancerCen-ter,Thomas Jefferson University, Philadelphia, Pennsylvania. 4Depart-ment of Medical Oncology,Thomas Jefferson University, Philadelphia,Pennsylvania. 5Department of Urology, Thomas Jefferson University,Philadelphia, Pennsylvania.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Corresponding Author: Karen E. Knudsen, Thomas Jefferson University, 233South 10th Street, Room 908, Philadelphia, PA 19107. Phone: 215-503-8574; Fax:215-503-0622; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-14-1358
�2015 American Association for Cancer Research.
ClinicalCancerResearch
www.aacrjournals.org 795

administrating cabazitaxel, that is, the novel taxane may outper-form docetaxel when administered to patients earlier in diseaseprogression; and (iii) a clinical biomarker to identify patients thatwill most likely benefit from cabazitaxel treatment.
These studies assessed the molecular and cellular response tocabazitaxel. In vitro analyses showed that cabazitaxel is superior todocetaxel in its antitumor activity. These effects were most pro-nounced in CRPC model systems, wherein taxanes are preferen-tially used. Although it has been suggested that taxanes mayimpinge on AR subcellular localization (18–20), this does notappear to be a major facet of taxane activity, because at the lownanomolar concentrations, which show cytostatic and cytotoxiceffects, no effect on AR was observed. These studies furtheridentified a key biomarker of cabazitaxel responsiveness. In vitroand in vivo analyses of isogenic-paired models with and withoutRB demonstrated that prostatic adenocarcinoma cells that haveprogressed to castration resistance through loss of RB are hyper-sensitive to cabazitaxel. Finally, the molecular activities of caba-zitaxel were discerned using gene-expression analyses thatshowed that the genomic response of cabazitaxel was distinctfrom docetaxel, and was strongly influenced by the hormonalmilieu.
Materials and MethodsCell culture
Androgen-dependent (LNCaP, LNCaP shCon1) and CRPC(C4-2, LNCaP shRB1) cells were maintained as previouslydescribed (21). Unless otherwise indicated, cells were platedovernight in IMEM (Corning Cellgro) using standard serum(5% FBS) and treated with 1 nmol/L cabazitaxel or docetaxel.
Trypan blue exclusion assayCells were treated in duplicate with a dose range of 0.1 to 2
nmol/L of taxane for 48 hours, followed by 48 hours (LNCaP,C4-2) or 96 hours (LNCaP shCon1/shRB1) in fresh media.Cell samples were trypsinized, counted twice on a hemacy-tometer using the trypan-blue exclusion method, and normal-
ized to a drug-free control. Experiments were performed atleast twice.
Flow cytometryProstatic adenocarcinoma cells were treated in triplicate with a
taxane for 16 or 48 hours, or vehicle, adherent and nonadherentcells were combined, gently resuspended in 100% ethanol, andfixed overnight at�20�C. Proliferationwasmeasured by bivariateflow cytometry using a 2-hour pulse-label of bromodeoxyuridine(BrdUrd; Amersham, RPN201) before harvest and cell-cycle posi-tion by propidium-iodide (PI) staining (22). A BD BiosciencesFACSCaliber was used to capture 10,000 BrdUrd/PI events.FlowJo software (TreeStar) was used to gate for the percentageof BrdUrd incorporation or cell cycle.
ImmunoblottingControl and taxane-treated cells were harvested to evaluate
cleaved PARP-1 (Cell Signaling Technology) levels. Total proteinwas extracted by sonication in RIPA buffer, separated bySDSPAGE, transferred to polyvinylidene difluoride, and immu-noblotted overnight at 4�C. Immunoblots were quantified using aBio-Rad Chemidoc MP Imaging System.
Immunofluorescent microscopyCells were seeded overnight in 6-wells plates on poly-L-
lysine–coated coverslips, treated, fixed with 4% paraformalde-hyde (Acros Organics, 416780250), and permeabilized withTriton-X100 (Amresco, 0694-1L), blocked in 2% goat serum,and stained with rabbit-a-AR (Santa Cruz Biotechnology N-20)and a-rabbit Alexa fluor-546 (red). To stain F-actin, cells wereincubated with Alexa Fluor-488 Phalloidin (Life Technologies).Coverslips were mounted with Prolong Gold Antifade reagentwith DAPI (Invitrogen; P36931). Images were taken with aconfocal laser microscope (Zeiss 510 Meta; �40 objective, �2digital zoom). Quantification of phenotypes was done on afluorescent microscope (Leica DMI3000B, �20 objective) on atleast four coverslips per condition, counting 200 cells perreplicate, calculating the percentage of cells displaying specificmorphologies.
Human prostate tumor explantsFresh primary tumor tissue was obtained from patients with
prostatic adenocarcinoma who underwent radical prostatecto-my at Thomas Jefferson University Hospital in accordance withInstitutional Review Board standards and in compliance withfederal regulations governing research on deidentified speci-mens and/or clinical data (45 CFR 46.102(f)). Tumors weredissected by a clinical pathologist and collected in culturemedia: IMEM [5% FBS, 0.01 mg/mL insulin (Invitrogen;12585-014), 30 mmol/L hydrocortisone (Sigma; H-0888), andpenicillin/streptomycin]. Tissue was subdivided into approxi-mately 1-mm3 pieces and placed (2–3 pieces/well) in a 24-wellplate on presoaked 1-cm3 dental sponges (Novartis; Vetspon)submerged in 0.5 mL culture media in presence or absence ofdrugs (control, 50 nmol/L cabazitaxel or docetaxel). Treatmentswere refreshed every 48 hours, and explants were harvestedafter 6 days, formalin-fixed, paraffin-embedded, and analyzedby standardized IHC methods. Control- and taxane-treatedexplants (n ¼ 3 patients) with glandular epithelial tissue, asdetermined by a certified clinical pathologist, were stained forKi67 (Invitrogen; 180191Z) or AR (Santa Cruz Biotechnology;
Translational Relevance
There is an urgent need for more efficacious therapeutics totreat advanced, castration-resistant prostate cancer (CRPC),which to date remains a uniformly fatal disease. Few chemo-therapeutic options exist that affect overall survival in thisstage of disease, and although the underlying mechanisms areunknown, the most effective chemotherapeutics are taxanes.Furthermore, the next-generation taxane cabazitaxel is effec-tive in patients in whom docetaxel has failed, but the molec-ular basis for this has not been discerned. Viamodeling in vitro,in vivo, and in human tumor explants, studies herein identifydistinct molecular signatures of the taxanes, revealing novelmolecular functions of cabazitaxel associated with enhancedefficacy inCRPC. Furthermore, loss of theRB tumor suppressorwas identified as a biomarker of enhanced response to caba-zitaxel in vivo. These findings reveal unique functions forcabazitaxel in CRPC, and identify the first potential biomarkerfor selecting patients who might most benefit from earlychemotherapy.
de Leeuw et al.
Clin Cancer Res; 21(4) February 15, 2015 Clinical Cancer Research796

N-20) using clinically approved protocols by the ThomasJefferson University Hospital. Cleaved caspase-3 (catalog#9661L; Cell Signaling Technology) staining was outsourcedto the Comparative Pathology and Mouse Phenotyping SharedResource at the Ohio State University (Columbus, OH).
Mouse xenograftsXenograft studies were performed in accordance with NIH
Guidelines and animal protocols were approved by ThomasJefferson University. LNCaP shCon1 or shRB1 cells (3 � 106)were combined 1:1 with Matrigel (BD Biosciences, 354234) andinjected s.c. into the flanks of 6-weeks-old, intact-male athymicnude mice (NCI-Frederick, Frederick, MD). Mice were castratedwhen tumors reached 100 to 150mm3. After a 1-week recovery,themicewere treated 2�perweekwith 8mg/kg cabazitaxel by i.p.injections, and tumor volumes were monitored with calipers 3�per week. Tumors were harvested and processed after 3 weeks oftreatment, or when the tumor exceeded 800mm3. Hematoxylinand eosin (H&E) stained sections of shCon1 and shRB1 LNCaPtumors (n¼6 tumors/group)were evaluatedusing aMotic BA400microscope (Motic). For each tumor section, the number ofmitotic figures in 10 randomly selected �400 (i.e., high power)fields was determined by a board certified veterinary anatomicpathologist (L.D. Berman-Booty). Additional tumor sectionswerestained for Ki67 (1:250; Invitrogen) and AR (Santa Cruz Biotech-nology; N20).
Immunohistochemistry quantificationSections of shCon1 and shRB1 LNCaP xenograft tumors (n¼ 6
tumors/group) and prostate tumor explants (n ¼ 3 tumorexplants/treatment) were immunostained for Ki67 (Invitrogen;180191Z). The prostate tumor explants (n ¼ 3 explants/group)were also immunostained for cleaved caspase-3 (catalog #9661L;Cell Signaling Technology). Three random images from each slidewere obtained at �400 (i.e., high power) magnification. The cellcounter feature of the ImageJ64 (NIH, Bethesda, MD) analysissoftware was used to determine the percentage of immunoposi-tive over all neoplastic cells.
Gene-expression arrayA genome-wide expression array (GSE63479) was per-
formed on a GeneChip Human Gene 2.0ST Array (Affymetrix;902112) with LNCaP cells infected with a control plasmid(MSCV-LMP) and C4-2 cells (23), treated in duplicate for 16hours with 1 nmol/L cabazitaxel, docetaxel, or vehicle (EtOH).The expression data were RMA normalized, and filtered toremove low-expressing genes. Differential gene expression withcorresponding P values (Student t test) was determined of drugtreated over control. Gene lists with P < 0.05 were comparedon the basis of the corresponding AffymetrixIDs, and plottedin a Venn diagram (http://bioinfogp.cnb.csic.es/tools/venny/).Gene ontology (GO) analyses were performed on selectedclusters by separating up- and downregulated genes (http://david.abcc.ncifcrf.gov/), and the resulting GO terms were cut-off at P < 0.05.
Statistical analysesTo determine statistical significance, P values were calcu-
lated by a standard unpaired Student t test, unless other-wise noted. Significant effects: �, P < 0.05; ��, P < 0.01; and���, P < 0.001.
ResultsCabazitaxel shows enhanced antiproliferative and procytotoxiceffects in CRPC
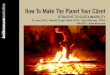
To assess the relative impact of cabazitaxel and docetaxel onprostatic adenocarcinoma cell growth and survival, analyseswere performed in both hormone therapy–sensitive and CRPCmodel systems. Cells were treated with an increasing dose ofeach agent (0.1–1 nmol/L) for 48 hours, followed by a washoutof 48 hours in the absence of drug, and subsequent quantifi-cation of cell viability through cell counting. As shown (Fig.1A), cabazitaxel and docetaxel showed relatively equivalenteffects in hormone therapy–sensitive cells (left), with IC50
values of 0.220 nmol/L for cabazitaxel, and 0.319 nmol/L fordocetaxel. However, cabazitaxel (IC50 ¼ 0.142 nmol/L)resulted in markedly enhanced antitumor effects comparedwith docetaxel (IC50 ¼ 0.269 nmol/L) in CRPC cells (right).Concordantly, flow cytometric analyses monitoring both cell-cycle position (via propidium iodide, PI) and progressionthrough S-phase (via uptake of BrdUrd) revealed reduced S-phase entry after 16 and 48 hours of cabazitaxel treatment inboth cell types, although less pronounced in CRPC cells (Fig.1B, top, quantified in Fig. 1C). Docetaxel (Supplementary Fig.S1 and Fig. 1C) had a similar effect on proliferation of hormonetherapy–sensitive cells, but did not affect S-phase entry of cellsfrom the same lineage that have achieved castration resistance.Thus, cabazitaxel demonstrates an enhanced antiproliferativeeffect in CRPC cells compared with docetaxel. This enhancedeffect was reiterated in ADT-sensitive (LAPC4, VCaP) and CRPC(LCaP-abl) cell models (Supplementary Fig. S2A). In vivo,cabazitaxel successfully induced C4-2 xenograft tumor remis-sion, thereby demonstrating effectiveness of cabazitaxel in aCRPC model (Supplementary Fig. S2B).
In addition to the observed effects on cell cycle, the sub-2Ncontent was enhanced in CRPC cells treated with cabazitaxelcompared with hormone therapy–sensitive models, elicitingalmost double the effect of docetaxel after 48 hours in C4-2 cells(Fig. 1B, bottom; and Fig. 1D). Moreover, cabazitaxel effectivelyinduced apoptosis in C4-2 cells, as measured by PARP cleavage(Supplementary Fig. S3). Together, these data suggest that caba-zitaxel shows enhanced antiproliferative and procytotoxic effectsas compared with docetaxel.
Cabazitaxel promotes defective mitosisTo address the means by which cabazitaxel exhibits
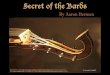
enhanced antitumor effects, the impact on nuclear integritywas assessed. Cells were fixed after 16 hours of exposure, andnuclear features assessed after DAPI staining (Fig. 2A). Visual-ization on a confocal microscope demonstrated a modestenrichment of mitotic figures after 16 hours (quantifiedin Fig. 2C, left), but evidence of defective mitoses was apparentin the asymmetric appearance of segregating nuclei. Pyknoticnuclei were also observed (Fig. 2A), as quantified in Fig. 2C(right), demonstrating a significant increase after 48 hourscabazitaxel exposure, further supporting the contention thatcabazitaxel exerts cytotoxic effects.
Given the known function of taxanes in serving as microtubulestabilizers and perturbing cytoskeletal integrity, treated cells werealso stained with fluorescently labeled phalloidin to visualize thecellular architecture. This revealed a reduction in cytoplasmicvolume in all cells (Fig. 2B), and allowed for clear definition of
Impact of Cabazitaxel on CRPC
www.aacrjournals.org Clin Cancer Res; 21(4) February 15, 2015 797

cell borders, revealing enhanced presence ofmultinucleate cells inCRPC cells treated with cabazitaxel, likely resulting from aberrantmitosis.Multinucleate LNCaP andC4-2 cells were quantified in atleast four duplicates for cabazitaxel versus control-treated sam-ples, which demonstrated a highly significant increase in poly-nuclear cells after 16 and 48 hours (Fig. 2C right). Together, thesedata support the hypothesis that cabazitaxel fosters an enhanced
antitumor capacity via disruption of the cell architecture anddefective mitoses.
Taxane action is independent of effects on AR localizationTaxanes have been reported to affect AR localization, and could
thereby potentially block prostate cancer proliferation (18–20).In these previous studies, supraclinical doses (mmol/L) levels of
CBTX
DCTX
0
2.5
5
0
2.5
5
0
5
10
15
20
25
0
5
10
15
20
25
CBTX
DCTX
A
B
0.0
0.5
1.0
1.5
0 0.1 0.2 0.3 0.4 0.5 0.75 1
Rel
ativ
e ce
ll vi
abili
ty
C4-2CBTX
DCTX***
**
D
LNCaP
0.0
0.5
1.0
1.5
0 0.1 0.2 0.3 0.4 0.5 0.75 1
Rel
ativ
e ce
ll vi
abili
ty
Concentration (nmol/L) Concentration (nmol/L)
LNCaPCBTX
DCTX
**
C4-2
−− − −
− −+ +
+ +
LNCaP
CBTX
DCTX
−− − −
− −+ +
+ +
C4-2
Brd
Urd
PI
CTRL 48 h CBTX16 h CBTXCTRL 48 h CBTX16 h CBTX
Cel
l nu
mb
er
PI
Rel
ativ
e ce
ll d
eath
Rel
ativ
e ce
ll d
eath
%B
rdU
rd+
cells
%B
rdU
rd+
cells
LNCaP C4-2
CBTX
DCTX
−−
−+
−+
+ +
− −−−
−+
−+
+ +
− −
C
*
16 h
48 h
16 h48 h
**
600
400
200
050k 100k 150k 200k 250k
105
104
103
–103
50k 100k 150k 200k 250k
14.7 0.35 105
104
103
–103
50k 100k 150k 200k 250k
12.3 0.68
50k 100k 150k 200k 250k
105
104
103
–103
10.2 0.37 105
104
103
–103
50k 100k 150k 200k 250k
18.0 2.37 105
104
103
–103
50k 100k 150k 200k 250k
16.5 2.32 105
104
103
–103
50k 100k 150k 200k 250k
17.0 0.44
600
400
200
050k 100k 150k 200k 250k
0.09 0.76
300
200
100
0
400
500
50k 100k 150k 200k 250k
3.25
600
400
200
0
800
50k 100k 150k 200k 250k
0.11
600
400
200
050k 100k 150k 200k 250k
0.79
600
400
200
050k 100k 150k 200k 250k
3.14
Figure 1.Cabazitaxel shows enhanced antitumor effects in CRPC. A, dose-dependent response to 48 hours cabazitaxel (CBTX) and docetaxel (DCTX) treatment and 48 hoursfresh media without drugs was assessed in hormone therapy–sensitive (LNCaP) and –resistant prostate cancer cells (C4-2) by trypan blue exclusion, andcell numbers were normalized to EtOH treatment. B, bivariate flow-cytometry analyses of LNCaP and C4-2 cells treatedwith 1 nmol/L cabazitaxel or control for 16 or48 hours. In the top graphs, the x-axis represents relative DNA content as indicated by PI staining; the y-axis shows cells undergoing active S-phase as indicatedby 2 hours BrdUrd labeling. Inset values, the percentage of BrdUrd incorporation in viable cells (mean � SD, from an experiment performed in biologic triplicate).The bottom graphs represent the corresponding PI traces only, showing a G2–M arrest, followed by cell death after cabazitaxel exposure. C, quantification of thepercentage of BrdUrdþ cells in B and Supplementary Fig. S1; significant reduction is observed in taxane over control (LNCaP, P < 0.05; C4-2, P < 0.0005for all conditions). Cabazitaxel appears to have a mild effect on proliferation of C4-2, although not significant, whereas docetaxel does not. D, taxanes inducesignificant cell death after 48 hours of cabazitaxel or docetaxel over CTRL in both LNCaP and C4-2 cells (P < 0.01, detected as an increase in sub-G1 content by flowcytometry (PI in B), with enhanced effects in the CRPC cells. Asterisks indicate significant differences between cabazitaxel and docetaxel at the same treatmentduration, showing no significance in LNCaP, but improved efficacy for cabazitaxel in C4-2 cells (16 hours, P ¼ 0.0042; 48 hours, P ¼ 0.0092).
de Leeuw et al.
Clin Cancer Res; 21(4) February 15, 2015 Clinical Cancer Research798

taxanes were used, whereas in vitro IC50 values for these drugs arein the nanomolar range (24, 25). Thus, it is imperative to deter-mine whether the reported effects occur at doses that are robustlycytostatic and cytotoxic, and are clinically attainable. As shown,using doses and time points sufficient to both suppress pro-liferation and induce cell death, endogenous AR remains nucle-ar in the presence of androgen-replete media (Fig. 3A). Todetermine whether these effects hold true under conditionsthat mimic castration, parallel studies were conducted in thepresence of charcoal–dextran-treated serum. As expected,androgen deprivation alone resulted in loss of nuclear ARenrichment in hormone therapy–sensitive cells; however, inCRPC cells, AR is retained in the nucleus even under castrate
conditions (Fig. 3B). Cabazitaxel or docetaxel had no impacton AR localization at a nanomolar level (1 nmol/L) in eithercell line. Taken together, the enhanced cytotoxic and cytostaticeffects of cabazitaxel appear to be independent of AR subcel-lular regulation.
Cabazitaxel exerts enhanced antitumor effects in humantumors
Given desirable cytostatic and cytotoxic effects of cabazitaxel inmodel systems, the antitumor effects were further assessed usingnext generation, ex vivo tumor explants that allow for determina-tion of effects on the complex 3D tumor microenvironment.Fresh tumor material was obtained from radical prostatectomy
CTRL
16h
CBTX
48h
CBTX0
2
4
6C4-2
%P
ykn
oti
c ce
lls
CTRL 16 h CBTX
DAPI
LNCaP
16 h DCTX
C4-2
B
DAPIF-Actin
A
CTRL
16h
CBTX
48h
CBTX0
20
40
%M
ult
inu
clea
te c
ells C4-2
*****
**
CTRL
16h
CBTX
48h
CBTX0
2
4
6
8C4-2
%M
ito
tic
fig
ure
sCTRL
16h
CBTX
48h
CBTX0
20
40
%M
ult
inu
clea
te c
ells LNCaP
CTRL
16h
CBTX
48h
CBTX0
2
4
6
8
%M
ito
tic
fig
ure
s LNCaP
*****
CTRL
16h
CBTX
48h
CBTX0
2
4
6
%P
ykn
oti
c ce
lls
LNCaP
**
CTRL 16 h CBTX 16 h DCTX
LNCaP
C4-2
C
Figure 2.Cabazitaxel treatment results in increased multinucleated cells and aberrant nuclei. A, the nuclei of fixed LNCaP and C4-2 cells that were treated for 16 hours withtaxaneswere visualizedwithDAPI staining (cyan) on a confocalmicroscope (�40), demonstrating defectivemitosis andpyknotic nuclei (yellowandorange arrows).B, F-Actin stained with Alexa Fluor 488–labeled phalloidin shows changes in cytoplasmic volume and cell morphology, as induced by taxanes after 16 hourscompared with control. The pink arrows, multinucleate cells, which are quantified in the whisker plots in C. C, quantification of mitotic figures, pyknotic cells,and multinucleate cells after cabazitaxel (CBTX) treatment in at least quadruplicate shows significant elevation of multinucleate LNCaP and C4-2 cells after16 hours (P¼0.0055 andP¼0.0042, respectively) and 48 hours (P <0.0001 in both cell lines), and pyknotic cells after 48 hours (P¼0.0107;P¼0.0096). C4-2 cellsshow a modest, however, nonsignificant increase in mitotic figures after 16 hours. � , P < 0.05; �� , P < 0.01; ��� , P < 0.001.
Impact of Cabazitaxel on CRPC
www.aacrjournals.org Clin Cancer Res; 21(4) February 15, 2015 799

of high-volume disease, and tissue slices randomized into controlor taxane-treated arms. As has been previously reported, thesetumor slices retain the salient features of the tumor at the time ofresection (including AR expression and proliferative capacity; Fig.4A; refs. 22, 26). These studies allow for intrinsically controlledanalyses of taxane effects within the same tumor. Tumors wereharvested after 6 days of treatment, formalin-fixed and paraffin-embedded. Standard H&E staining confirmed retention of thetumor microenvironment (Fig. 4B left). IHC to assess the prolif-erative indices (using an antibody to Ki67) was performed inparallel, of which representative examples are shown in Fig. 4B(middle), and quantified (Fig. 4C, top). Strikingly, this directcomparison in fresh tumor explants confirmed that cabazitaxelexerts a markedly enhanced cytostatic response compared withdocetaxel. Caspase-3 staining revealed an increasing trend, how-ever nonsignificant, likely due to the limited sample number (n¼3; Fig. 4C right). Finally, assessment of AR localization in responseto 50 nmol/L drug treatment revealed retention of nuclear AR inthe tumor cells (Fig. 4D). Thus, similar to what was observed invitro, the antitumor effects of nanomolar level cabazitaxel appearto occur independently of altered AR localization. Collectively,these data identify an enhanced capacity of cabazitaxel to elicitantiproliferative and proapoptotic events in primary humantumors.
Tumors that progress to CRPC by RB loss show hypersensitivityto cabazitaxel
Although the above studies suggest that cabazitaxel harborsproperties that are highly desirable in the clinical setting, a majorhurdle is to identify tumor subtypes that wouldmost benefit fromtreatment with the agent. It has been previously demonstratedthat loss of RB tumor-suppressor protein or function occurs withhigh frequency in CRPC, and that this event alone can promotebypass of hormone therapy (21). Conversely, we and others haveshown that RB loss compromises selected DNA damage check-points, and can result in sensitization to a subset of chemother-apeutics, including docetaxel (23, 27). These findings put forwardthe provocative hypothesis that prostate cancers that achievecastration resistance via loss of RB may be exquisitely responsiveto taxanes. To assess this, isogenic pairs of LNCaP cells withcontrol shRNA or shRNA directed against RB (shCon1 and shRB1cells; ref. 21), were initially assessed in vitro for differentialresponse to cabazitaxel. In these studies, shRB1 cells demonstrat-ed amodest sensitization to cabazitaxel as comparedwith shCon1(Fig. 5A). To challenge this in vivo, cells were s.c. injected intomaleathymic nude mice; when the xenograft tumors (n ¼ 5/group)reached a size of 100 to 150mm3, the mice were surgicallycastrated, allowing a week of recovery before starting 8 mg/kgcabazitaxel treatment by i.p. injections twice a week (Fig. 5B
A
B
AR MergeDAPI
CTRL
16 h CBTX
16 h DCTX
LNCaP C4-2AR MergeDAPI
STEROID REPLETE
STEROID DEPLETEDLNCaP C4-2
AR MergeDAPIAR MergeDAPI
CTRL
16 h CBTX
16 h DCTX
Figure 3.The effects of taxanes areindependent of altered ARlocalization. A, immunofluorescenceafter 16 hours of 1 nmol/L cabazitaxel(CBTX), docetaxel, or CTRLtreatment demonstrates nuclearlocalization of AR (red) is unaffectedin presence of steroids. DAPI staining(cyan) denotes cell nuclei. B, inandrogen deprivation, AR resides inthe cytoplasm of LNCaP cells, butremains nuclear in C4-2 CRPC cells(steroid depleted), even after16 hours cabazitaxel exposure.
de Leeuw et al.
Clin Cancer Res; 21(4) February 15, 2015 Clinical Cancer Research800

schematic). Tumor volumes were monitored three times a weekwith calipermeasurements, and as shown, a remarkably enhancedtumor-suppressive effect was observed in the shRB1 tumors (Fig.5B left). Normalization of individual tumor volumes at 14 daysafter start of treatment compared with their respective volumes att ¼ 0 shows a significant difference in cabazitaxel responsebetween the shCon1 tumors (n ¼ 4) and the shRB1 tumors(n¼ 5; Fig. 5B right). Notably, the fifthmouse growing an LNCaPshCon1 tumor had to be sacrificed before this time point, because
the tumor volume had already exceeded 800 mm3, despitecabazitaxel administration. These in vivofindings robustly supportthe concept that RB-deficient tumors are hypersensitive to treat-ment with cabazitaxel.
To further probe the underlying basis of the observed enhancedeffect in RB-deficient tumors, histopathologic analyses were per-formed. Through H&E and Ki67 IHC analyses, shCon1 tumorcells showed expected accumulation of mitotic figures, indicatingan appropriate cell-cycle arrest in metaphase as a result of
B
A HistologyEx vivo cultureRadical prostatectomy
Subdivide Harvest
t=0 1 2 3 4 5 6 days
Fresh media + 50 nmol/Lcabazitaxel or docetaxel
CTRL
CBTX
DCTX
C
AR(×40)
D
% K
i67+
cel
ls
CTRL
CBTXDCTX
CTRL
CBTXDCTX
0
20
40
60
0
5
10
15
20
25
% C
l. C
3+ c
ells
*
CTRL CBTX DCTX
H&E (×20) H&E (×40) Ki67 (×40) Cl. caspase-3 (×40)
Figure 4.Cabazitaxel (CBTX) exerts enhanced antitumor effects in human tumors. A, schematic overview of the ex vivo explant assay. Fresh tissue obtained from radicalprostatectomy is subdivided and cultured for 6 days on dental sponges submerged in cell culture media with different treatments (CTRL, 50 nmol/L cabazitaxel ordocetaxel, DCTX), after which tissue is formalin-fixed, paraffin-embedded, and analyzed by standardized IHC methods. B, H&E and IHC on explant tissuesdemonstrate that taxane treatment reduces tumor cell proliferation (Ki67) and induces cell death (caspase-3). C, quantification of Ki67 (top) in three independentexplant assays, performed on tissue from 3 patients, shows reduced proliferation in cabazitaxel-treated samples compared with control (P < 0.05 by Kruskal–Wallis nonparametricmultiple comparison analysis). Cabazitaxel demonstrates improved drug efficacy comparedwith docetaxel ex vivo. Quantification of caspase-3 in the three explant assays (bottom) indicates a moderate yet nonsignificant increase in cell death, as induced by taxane treatment. D, AR (IHC) remainsnuclear in tumor specimens after 6 days of taxane treatment. � , P < 0.05.
Impact of Cabazitaxel on CRPC
www.aacrjournals.org Clin Cancer Res; 21(4) February 15, 2015 801

shCon1
shRB1
020406080
100
shCon1
shRB1
0
50
100
150
200M
ito
tic
fig
ure
s/10
HP
F
0.5
1
1.5
2
2.5
Tu
mo
r vo
lum
e re
lati
ve t
o s
tart
Tx
t=14
0.0
0.5
1.0
0 0.1 0.3 0.5 1 2
Rel
ativ
e ce
ll vi
abili
ty
CBTX nmol/L
***
**
P = 0.014
Tu
mo
r vo
lum
e (m
m3 )
Days CBTX Tx
LNCaP
shCon1shRB1
1,500
1,000
500
–7 0 7 14 21
A
B
α-RB
α-Lamin B
Cx
t=–7100–150 mm3
t=0
Start Tx
t=7 t=14 t=21
Sacrificeand harvest
CBTX 8 mg/kg 2x a week
shCon1shRB1
C
shCon1
shRB1
Ki67 (×40) DAR (×40)
LNCaP
shRB1or
shCon1
H&E (×40)
*
***
0
shCon1shRB1
% K
i67+
cel
ls
100
RB1oron1
Figure 5.Tumors that progress to CRPC by RB loss show hypersensitivity to cabazitaxel (CBTX). A, RB knockdown LNCaP cells (shRB1) show a modest sensitization invitro to 48 hours cabazitaxel and 96 hours in fresh media (no cabazitaxel) in culture conditions mimicking ADT, but not in presence of hormones (in serum), asmeasured by cell viability in a trypan blue exclusion assay. B, treatment schematic for nude athymic mice s.c. injected with LNCaP shRB1 or LNCaP shCon1 cellsto obtain xenograft tumors in vivo (n ¼ 5/group). Growth analysis of xenograft tumors was monitored over time of cabazitaxel treatment (start t ¼ 0). Thegraph on the right denotes the sizes for each tumor at t ¼ 14 relative to the size at start of treatment (t ¼ 0), showing that only LNCaP shRB1 tumorsrespond to cabazitaxel (P ¼ 0.014). C, RB-proficient LNCaP xenograft tumors display decreased Ki67 staining (unpaired t test, P < 0.0001), and elevatednumbers of mitotic figures after cabazitaxel treatment. AR remains nuclear after cabazitaxel exposure, irrespective of RB status. D, quantification ofmitotic figures (top) and Ki67-positive cells (bottom) in 10 high power fields (HPF,�400) per tumor show the elevated percentage of mitotic figures in shCon1tumors, and a reduction in proliferating cells in shRB1 tumors. � , P < 0.05; �� , P < 0.01; ���, P < 0.001.
de Leeuw et al.
Clin Cancer Res; 21(4) February 15, 2015 Clinical Cancer Research802

cabazitaxel treatment. By contrast, shRB1 tumors elicited fewermitotic figures (Fig. 5C, quantified in Fig. 5D, top), consistentwith previously reported "mitotic slippage" in cells lacking cell-cycle checkpoints (28). Quantification of Ki67-positive cells inthree images per tumor slide confirmed a strong reduction inproliferative cells in the shRB1 tumors versus shCon1 (Fig. 5D,bottom). Taken together, the in vivo data suggest that RB-deficienttumors are hypersensitive to cabazitaxel, and support the postu-late that RB should be developed as a biomarker to identifytumors that may be most responsive to taxanes.
Cabazitaxel displays novel actions in prostate cancer cells byexpression profiling
Although the above studies identify novel antitumor effectsof cabazitaxel and putative biomarkers to identify tumors thatwould be most responsive to this taxane, additional studieswere performed to further uncover the molecular basis ofdivergent cabazitaxel function. Hormone therapy–sensitiveLNCaP, and castration-resistant C4-2 cells were treated for16 hours with cabazitaxel or docetaxel, in presence or absenceof steroid hormones, and subjected to a genome-wide mRNAanalysis. The resulting expression data were filtered to removelow-expressing genes, to reduce background and false-positivehits. Triplicate expression values were averaged, after whichsamples from the individual taxanes (cabazitaxel or docetaxel)were normalized to the corresponding values for control-trea-ted samples either with or without steroids. Differentiallyexpressed genes were selected by a Student t test (P < 0.05),and compared between treatments, as visualized by the twoVenn diagrams representing the two cell models (Fig. 6A).Complete gene lists and fold alterations for each gene clusterare provided in Supplementary Table S1 (LNCaP) and Supple-mentary Table S2 (C4-2). Notably, distinct gene-expressionoutcomes were readily apparent between the two taxanes.Furthermore, these analyses revealed divergent effects of theagents in cells that are cycling (steroid replete) versus those thatwere arrested via steroid depletion (androgen deprived). Thesefindings suggest, as expected on the basis of the data above, thatcabazitaxel exerts differential effects compared with docetaxel,and that the proliferative status of the tumor cell can alterdownstream biologic effects.
To gain deeper understanding of the cellular response tocabazitaxel and docetaxel, GO analyses were performed on bothcastrate (in blue and red, respectively, corresponding to the Vennclusters in Fig. 6A) and steroid replete (yellowandgreen) gene lists(Supplementary Fig. S4, LNCaP and Supplementary Fig. S5, C4-2). For complete gene lists per GO term, see in SupplementaryTable S3. These studies revealed enrichment of genes involved incell cycle and chromosomal organization and regulation aftercabazitaxel treatment exclusively inC4-2 cells (Fig. 6B), consistentwith the enhanced antiproliferative effect of this agent in CRPCcells (Supplementary Fig. S3). In the ADT-sensitive LNCaP cellsunder androgen-deprived conditions, cabazitaxel and docetaxelshare enrichment in gene transcription–related pathways. How-ever, these appear to be negatively regulated by cabazitaxel,versus a positive impact by docetaxel, which supports thehypothesis that these drugs have distinct downstream effects.In C4-2 cells, transcription was affected regardless of steroidconditions; however, chromosomal regulation appears to suffera greater impact during steroid repletion, which supports thehypothesis that hormone conditions matter for chemothera-
peutic response even in castration-resistant tumor cells. Doc-etaxel and cabazitaxel may affect similar pathways, nonethe-less, cabazitaxel has a stronger effect on cell-cycle and chroma-tin regulation, whereas docetaxel appears to have a moresignificant impact on transcription and repair. These differencescould be caused by differences in microtubule stabilization.Although a general mechanism has been described for taxaneaction, these drugs may act with differing kinetics, or be less ormore efficient at stabilizing the tubulin dimers, resulting invarious degrees of aberrant mitotic events. Notably, CRPC cellshave a more substantial taxane response in terms of chromatinorganization and regulation, which downstream would ulti-mately lead to aberrant mitosis and cell death. As shown, genesmost altered (up- or downregulated) by cabazitaxel in absenceor presence of steroids are displayed in tables (Fig. 6C). Genesthat are common between the two cell models are marked withan asterisk. Classical AR targets (KLK3, TMPRSS2, FKBP5, andKLK2) are not affected by cabazitaxel or docetaxel, and are onlyaltered by steroid deprivation (data not shown). Strikingly, thehormone conditions affect the molecular response of taxanes,demonstrated by enrichment of distinct pathways in hormonereplete versus androgen-deprived media, even in castration-resistant tumor cells. This differential response to cabazitaxel(or docetaxel) will likely be of relevance for designing combi-nation therapies with AR pathway–targeting drugs, such asenzalutamide and abiraterone acetate. These unbiased analysesfurther illustrate the divergent effects of cabazitaxel and doc-etaxel, and provide a gene "signature" of response to cabazi-taxel in the presence and absence of androgen.
DiscussionCurrently, no durable cure exists for advanced CRPC, and only
limited therapeutic success has been achieved in terms ofimproved overall survival (OS). One of the few options availablefor advanced disease is taxane-based chemotherapy, and the new-generation drug cabazitaxel has been shown to exert antitumoreffects even after docetaxel has failed (11). This study presentsfirst-in-field distinctions between these two agents, using clini-cally relevant conditions. Key findings are: (i) cabazitaxel inducesimproved cytostatic and cytotoxic response, especially in CRPC;(ii) cabazitaxel induces aberrant mitosis, leading to pyknoticand multinucleated cells; (iii) taxanes do not act through AR toinduce cytostatic and cytotoxic effects at nanomolar concentra-tions; (iv) novelmolecular actions for cabazitaxel are identifiedbygene-expression profiling; and (v) tumors that have progressed tocastration resistance via loss of RB show enhanced sensitivity tocabazitaxel.
These studies demonstrate that the cellular consequences ofcabazitaxel are distinct from that of docetaxel in CRPC. In general,it is thought that taxanes inhibit mitosis by binding b-tubulin andstabilizing the microtubules. In CRPC, taxanes induced bothcytostatic and cytotoxic effects, but these properties wereenhanced with cabazitaxel. Cabazitaxel induced an increase inmitotic figures in vitro and in vivo, often asymmetrical in shape,suggestive of a prolonged, aberrant mitotic arrest, resultant inmultinucleated cells likely due to mitotic checkpoint slippage.Previous studies in which lung carcinoma cells were treated withlow molecular levels support this concept, as such that cellsescaped from a prolonged mitotic arrest without a proper celldivision, resulting in tetraploid cells (29). Clinically, cabazitaxel is
Impact of Cabazitaxel on CRPC
www.aacrjournals.org Clin Cancer Res; 21(4) February 15, 2015 803

– steroids
P < 0.05
CBTX DCTX+ steroids + steroids
P < 0.05
CBTX DCTX+ steroids
A LNCaP C4-2
– steroids
CB GO analysis comparison
+ steroids
– steroids– steroids
DownUp
CBTXsteroid replete
DownUp
CBTXandrogen deprived
Gene FoldHIST2H4 –1.36NECAB3 –1.30TSSK2 –1.29NYX –1.26PDIA3 –1.25OGN –1.25DDRGK1 –1.24EBP –1.23MCM10 –1.23TRAF3IP1 –1.21FANCB –1.20TSPAN11 –1.20ANG –1.19BLM –1.19ARAP1 –1.18TCEAL3 –1.18ZNF98 –1.18IGLJ5 –1.18ANO10 –1.17ZNF485 –1.17ATP1B3 –1.17PPAP2C –1.17TGOLN2 –1.17CYP51A1 –1.16ASF1B –1.15
Gene FoldSKA2 1.30RGL1 1.27BTG2 1.26TP53INP1 1.25TARP 1.24GOLGA8S 1.23SH3D19 1.22WNT7A 1.22IGLV4-60 1.22CRYZ 1.22NUCB1 1.21TRIP11 1.21CHCHD10 1.21INO80C 1.21KBTBD4 1.21TUBB2A 1.21ADCY1 1.20DBN1 1.19NUP93 1.18LGALS1 1.18OXR1 1.18PSMB9 1.17RABGGTA 1.17DENND1A 1.17NWD1 1.17
Gene FoldBRCA2 –1.37ORC6 –1.37EME1 –1.31ATAD2 –1.3GNA13 –1.28BRD4 –1.27CCNE2 –1.26KIF24 –1.25EXO1 –1.24TMED8 –1.24EIF5A2 –1.23AGPAT3 –1.23SLC16A10 –1.23MCM6 –1.23OGFOD3 –1.22OGFR –1.22POLA2 –1.21ZNF143 –1.21RPS18 –1.21CNOT10 –1.2IKBKAP –1.2SRSF10 –1.2CCDC111 –1.2EPHA3 –1.19ATP6V1E2 –1.19
Gene FoldPRAMEF3 1.47PFKFB4 1.31POTEF 1.26ARSG 1.25RNF135 1.24RSPH3 1.23RIPPLY1 1.23TMEM9 1.22ZNF582 1.22CEL 1.2TUBA3E 1.2PCBP4 1.2CCNJL 1.19CCDC23 1.19PRAC 1.18FLCN 1.18IGKC 1.18GAR1 1.18MROH5 1.18DUSP18 1.17LRCH1 1.17KCNG2 1.16FABP5P3 1.16XK 1.16RAE1 1.15
LNCaP
*****
*
*
*
DownUp
CBTXsteroid replete
DownUp
CBTXandrogen deprived
Gene FoldBTG2 1.55MYNN 1.46GK 1.45NDST1 1.45ADAMTS1 1.37JARID2 1.36HINT3 1.31MDM2 1.3AMZ2P1 1.29SYCN 1.26TNFRSF10D 1.26RGPD3 1.26KLF9 1.25ABHD15 1.25SKIL 1.24PAX1 1.23ZNF35 1.23DDX43 1.23DUSP10 1.23PDCL3 1.23HCG14 1.23RASA4B 1.22ZNF582 1.22TENM3 1.21SH2D5 1.21
Gene FoldCLSPN –1.72HIST1H2AM –1.66MCM5 –1.52POLE2 –1.51EXO1 –1.5WDR76 –1.49HIST2H2AB –1.48RAD51 –1.48HIST1H1C –1.47CDC6 –1.47SLC25A40 –1.45BRIP1 –1.44PRIM1 –1.43MCM6 –1.43POLA1 –1.42GMNN –1.42MMS22L –1.42GSG2 –1.41RFC4 –1.41HIST2H2BE –1.41CHAF1B –1.38ZNF726 –1.38PSMC3IP –1.38DNA2 –1.37DTL –1.37
Gene FoldTP53INP1 1.52PTPN20A 1.43TCP10 1.38KRTAP5-1 1.37PLK2 1.33PLCH2 1.27ACSM2A 1.27TEKT4 1.24CD300LD 1.23TSPAN11 1.22MUC22 1.22ACMSD 1.22MTVR2 1.21RSPO4 1.21CCDC60 1.21IGFALS 1.21RHBDD1 1.21B3GNT8 1.21CDRT15L2 1.21CLCNKB 1.2CTRB2 1.2DHH 1.2AKAP6 1.2RASA4 1.2DNAH1 1.2
Gene FoldHIST1H2BM –2.03HIST2H2AB –1.91HIST1H2A –1.82MCM10 –1.48HIST1H4 –1.44E2F8 –1.4CLSPN –1.36FBXO5 –1.36HIST1H1C –1.34POLA2 –1.33MNS1 –1.31TICRR –1.3SPC24 –1.3MEIS3 –1.3MCM3 –1.28FANCD2 –1.27CCNE2 –1.25AP1M1 –1.25FEN1 –1.25COTL1 –1.24PLEKHM3 –1.23KIF24 –1.23HJURP –1.23HELLS –1.22IRX5 –1.21
C4-2
*
*
*
*
*
*
*
*common genes
Specific GOterm LNCaP* Specific GOterm C4-2*GO pathway C4-2*GO pathway LNCaP*
*P < 0.05
GO pathways LNCaP C4-2
CBTX steroid: Deprived Replete Deprived Replete
Transcrip�on
Transcrip�on 0.043 0.037
DNA binding 0.015 0.016
Posi�ve regula�on of transcrip�on factor ac�vity 0.031
Transcrip�on regulator ac�vity 0.019
Transcrip�on factor ac�vity 0.011
Regula�on of transcrip�on 0.024
Posi�ve regula�on of DNA binding 0.046
Protein–DNA complex assembly 0.016
DNA replica�on
DNA replica�on 0.025 0.001
DNA-dependent DNA replica�on 0.014 0.013
DNA repair
DNA repair 0.000
Response to DNA damage s�mulus 0.001
Cytoskeleton components
Cytoskeletal protein binding 0.050
Tubulin binding 0.031
Microtubule organizing center part 0.027
Cytoskeletal part 0.025
Microtubule cytoskeleton 0.001
Microtubule organizing center 0.000
Chromosomal organiza�on/regula�on
Covalent chroma�n modifica�on 0.047
Histone modifica�on 0.042
Chromosomal part 0.034
Chroma�n modifica�on 0.028
Nucleosome organiza�on 0.018
Chroma�n assembly 0.014
Histone binding 0.013
Nucleosome assembly 0.013
Chroma�n assembly or disassembly 0.012
DNA packaging 0.008
Chroma�n organiza�on 0.008
Centriole 0.005
Chromosome 0.001
Chromosome organiza�on 0.000
Centrosome 0.000
Histone acetyltransferase ac�vity 0.047
Cell cycle
Cell-cycle phase 0.034
M phase 0.025
Cell cycle 0.001
Posi�ve regula�onof cell cycle 0.015
Prolifera�on
Nega�ve regula�on of cell prolifera�on 0.045
Death
Induc�on of apoptosis by extracellular signals 0.007
de Leeuw et al.
Clin Cancer Res; 21(4) February 15, 2015 Clinical Cancer Research804

effective in patientswhohave failed docetaxel, which suggests thatcabazitaxel could prolong OS when used as a first-line chemo-therapeutic (13). In this study, cabazitaxel elicits strongerresponses in CRPC models, as opposed to ADT-sensitive cells,and distinctly shows an improved response window versus doc-etaxel.Moreover,metastatic diseasemay respondbetter to taxanesupon first diagnosis than after exposure to other treatment regi-mens, which allows cells to evolve into even more aggressivedisease.
Contrary to expectation, the effects of taxanes at clinicallyrelevant (nanomolar) doses appear to be independent of ARregulation. In prostatic adenocarcinoma models, it has beenpreviously suggested that taxanes may inhibit AR translocationto the nucleus and activity, and thus contribute to antitumorefficacy (18–20). However, these studies were performed insuprapharmacologic concentrations of taxane (50 nmol/L–1mmol/L), whereas the IC50 values described for this class ofchemotherapeutics are in the single nanomolar range (24, 25).AR and downstream targets are not affected by cabazitaxel atthe nanomolar level, as demonstrated by the gene-expressionanalysis. Taken together, the studies herein provide evidencethat taxanes do not affect AR localization and activity at the lownanomolar levels in vitro, or clinically relevant concentrations invivo and ex vivo, whereas cytostatic and cytotoxic effects areobserved. Although it is probable that at higher (mmol/L) levelsAR transport is impaired, and thus its activity, this is likely abystander effect of the disruption of the cellular highwayaffecting general cellular trafficking that depends on themicrotubules.
In addition to demonstrating the commonalities betweencabazitaxel and docetaxel actions, gene-expression analyses revealamolecular basis for the divergent effects that cabazitaxel exerts ascompared with docetaxel, even in hormone therapy–sensitivecells. Cabazitaxel elicits a stronger response than docetaxel acrossdifferent model systems, which could be attributed to differentdownstreammolecular pathways affected by the drug. A commonpathway described for docetaxel in a previous genomewide studyis cell cycle (30), nonetheless, cabazitaxel appears to have anelevated effect on cell cycle andmitosis as evident from relatedGOterms in the cabazitaxel-distinct gene clusters in the study pre-sented here. Moreover, chromatin organization is exquisitelyaffected by cabazitaxel in CRPC cells, likely underlying the stron-ger response to the novel therapeutic, as well as its effectivity inpatients who have progressed on docetaxel. Docetaxel seemsmore enriched for transcription pathways, as previously reported(Li and colleagues; ref. 30). It has been speculated that docetaxelresistance can occur via bIII-tubulin overexpression or mutation,or by increased P-glycoprotein (13, 31, 32). Improved response tocabazitaxel was proposed to be due to a lower binding affinity forthis drug pump, but this has not been demonstrated. Conversely,it has been shown that P-glycoprotein regulates cabazitaxel levelsin the brain in vivo (33, 34). In sum, cabazitaxel has an elevated
impact on cell-cycle pathways and chromatin organization com-paredwith docetaxel, resulting in stronger cytostatic and cytotoxiceffects, and does not act via AR. Of note, the molecular impact ofcabazitaxel depends on the hormone conditions, which empha-sizes the need to further explore the optimal treatment conditions;for example, it should be determined whether this novel drugshould be administered as a single therapeutic, or in combinationwith ADT.
In addition to definition of the optimal treatment regimen,there is an urgent need for biomarkers in prostate cancer, todetermine which patients are most likely to benefit. Currently,cabazitaxel utilization is approved only in patients with pro-gressive disease after docetaxel has failed, without knowledgeof tumor markers to indicate who might most benefit fromtaxane therapy. Striking data herein show that tumors thatprogressed to CRPC via loss of RB are hypersensitized tocabazitaxel in vitro and in vivo, supporting the hypothesis thatRB could be applied as a biomarker for treatment outcomepredictions in patients. Given the fact that prostatic adenocar-cinoma is a leading cause of death in the United States andEurope, and currently few therapeutic options are available forCRPC, it is imperative to improve treatment. Loss of RB func-tionality is associated with up to 60% of all CRPC cases(21, 23). This study provides preclinical evidence that RB losssensitizes tumor cells to taxanes, supporting the hypothesis thatRB status could be applied as a metric to determine treatmentstrategies for patients with CRPC, as such that RB-deficienttumors would be treated with taxane-based chemotherapy.This approach would not only improve chances at longerrecurrence-free survival, but also limit unnecessary treatmentwith drugs that are less likely to be successful for an individualpatient, thereby avoiding potential adverse side effects. Despiteprevious reports that in other tumor types a high level ofchromosomal instability (CIN) is associated with taxane resis-tance (35), and dysregulation of the RB pathway has beendescribed to cause genomic instability and aneuploidy (36,37), suggesting that RB loss would induce cabazitaxel resis-tance, the opposite was observed here. This could mean thattaxanes have an additive effect to the already existing high levelsof CIN in RB-deficient cells, leading to catastrophic segregationerrors and reduced cancer cell viability (38). Other potentialbiomarkers for taxane sensitivity reported across differenttumor types are BRCA1, negative Bcl2, negative SIRT2 protein(39–42). However, the data herein present the first in vivoevidence of a single gene, RB, as a potential biomarker fortreatment response in prostate cancer, which is a crucial steptoward patient-tailored treatment decisions and improved careof CRPC.
Overall, the data presented here support that cabazitaxel wouldimprove therapeutic response compared with docetaxel, likely asapplied to the docetaxel space of CRPC. This hypothesis iscurrently being tested in a phase III clinical trials [FIRSTANA
Figure 6.Expression profiling reveals novel action(s) of cabazitaxel in ADT-sensitive and CRPC prostate cancer cells. A, Venn diagrams of twomicroarray analyses of P < 0.05after background filtering reveal differential response of castrate-sensitive LNCaP cells and castrate-resistant C4-2 cells to 16 hours 1 nmol/L cabazitaxel (CBTX)compared with docetaxel (DCTX), dependent on culture conditions: steroid-rich (þ) versus -depleted (�) media, in triplicate. B, David Bioinformatics GOanalyses with P < 0.05 (P values in table) reveal common and distinct pathways for the two taxanes, dependent on cell context and steroid conditions. C, top25 significant hits of cabazitaxel unique in androgen-deprived (blue) or steroid replete (yellow) conditions are displayed for each cell line, with the correspondingmean fold change over control-treated samples. Asterisks, common genes between LNCaP and C4-2 cells.
Impact of Cabazitaxel on CRPC
www.aacrjournals.org Clin Cancer Res; 21(4) February 15, 2015 805

NCT01308567]. Moreover, a recent report of an interim analysison another trial in ADT-sensitive metastatic disease (CHAARTEDNCT00309985) shows a striking benefit from addition of doc-etaxel to standard ADT, underlining the importance of testingchemotherapeutics in earlier disease states. The gene-expressiondata in these studies suggest that the hormone conditions affecttaxane action, not only in ADT-sensitive, but also in CRPC cells.The preclinical data strongly support the rationale behind a newphase II clinical trial that is currently recruiting chemotherapy-na€�ve patients presenting with mCRPC to retrospectively assessthe potential impact of RB as a biomarker for cabazitaxel sensi-tivity (ABICABAZI NCT02218606), which will compare theeffects of abiraterone alone versus abiraterone in combinationwith cabazitaxel. In summary, this article and recent clinicaldevelopments underpin that redefining the optimal clinical spaceand approach for chemotherapeutics would likely improve OS ofpatients with advanced prostate cancer.
In conclusion, these studies demonstrate the first molecularand cellular distinctions between cabazitaxel versus docetaxelin prostate cancer. The data provided not only demonstratethat these agents elicit differential molecular effects that aredistinct from AR regulation, but show that the enhancedeffects of cabazitaxel in CRPC can be preclinically modeled.Moreover, the studies described put forth the first putativebiomarker to select for patients that might most benefit fromcabazitaxel therapy. Combined, these studies provide the basisfor improving efficacy of taxane-based therapy in prostatecancer.
Disclosure of Potential Conflicts of InterestA.P. Dicker reports receiving speakers bureau honoraria from Bayer and is a
consultant/advisory board member for Merck, Merck EMD, and Vertex. W.K.Kelly is a consultant/advisory boardmember for Sanofi-Aventis. K.E. Knudsen isa consultant/advisory board member for and reports receiving commercialresearch support fromSanofi. Nopotential conflicts of interest were disclosed bythe other authors.
Authors' ContributionsConception and design: R. de Leeuw, W.K. Kelly, L.G. Gomella, K.E. KnudsenDevelopment of methodology: R. de Leeuw, M.J. Schiewer, S.J. Ciment,R.B. DenAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): R. de Leeuw, M.J. Schiewer, S.J. Ciment, E.J. Trabulsi,L.G. GomellaAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): R. de Leeuw, L.D. Berman-Booty, M.J. Schiewer,R.B. Den, A.P. Dicker, E.J. Trabulsi, K.E. KnudsenWriting, review, and/or revision of themanuscript: R. de Leeuw, L.D. Berman-Booty, M.J. Schiewer, R.B. Den, A.P. Dicker, W.K. Kelly, E.J. Trabulsi, C.D. Lallas,L.G. Gomella, K.E. KnudsenAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): R. de Leeuw, A.P. Dicker, L.G. Gomella,K.E. KnudsenStudy supervision: W.K. Kelly, C.D. Lallas, K.E. Knudsen
AcknowledgmentsThe authors thank members of the K. Knudsen laboratory for input
and commentary. The authors specifically acknowledge Dr. Michael A.Augello, Dr. Clay Comstock, and Daniela Pollutri. The microarray studieswere performed with support of the Kimmel Cancer Center Cancer Geno-mics Core.
Grant SupportThis work was supported, in whole or in part, by a Department of Defense
PCRP postdoctoral award (FY2012 PC121719; to R. de Leeuw), NIH grantK01 OD010463 (to L.D. Berman-Booty), a Prostate Cancer Foundation YoungInvestigator Award (toM.J. Schiewer), a Sanofi-Aventis grant (to K.E. Knudsen),NIH grants (R01 CA099996-11, CA159945-03, and CA176401-01A1; toK.E. Knudsen), and a Commonwealth of Pennsylvania Cure grant (SAP#41000548782; to K.E. Knudsen).
The costs of publication of this articlewere defrayed inpart by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received May 27, 2014; revised November 19, 2014; accepted November 27,2014; published online February 17, 2015.
References1. Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007.
CA Cancer J Clin 2007;57:43–66.2. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of
worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer2010;127:2893–917.
3. KnudsenKE, Penning TM.Partners in crime: deregulation ofARactivity andandrogen synthesis in prostate cancer. Trends Endocrinol Metab 2010;21:315–24.
4. Knudsen KE, Scher HI. Starving the addiction: new opportunities fordurable suppression of AR signaling in prostate cancer. Clin Cancer Res2009;15:4792–8.
5. Berthold DR, Pond GR, Roessner M, de Wit R, Eisenberger M, Tannock AI,et al. Treatment of hormone-refractory prostate cancer with docetaxel ormitoxantrone: relationships between prostate-specific antigen, pain, andquality of life response and survival in the TAX-327 study. Clin Cancer Res2008;14:2763–7.
6. Scher HI, Beer TM, Higano CS, Anand A, Taplin ME, Efstathiou E, et al.Antitumour activity of MDV3100 in castration-resistant prostate cancer: aphase 1–2 study. Lancet 2010;375:1437–46.
7. ScherHI, Fizazi K, Saad F, TaplinME, SternbergCN,Miller K, et al. Increasedsurvival with enzalutamide in prostate cancer after chemotherapy. N Engl JMed 2012;367:1187–97.
8. de Bono JS, Logothetis CJ, Molina A, Fizazi K, North S, Chu L, et al.Abiraterone and increased survival in metastatic prostate cancer. N Engl JMed 2011;364:1995–2005.
9. Parker C, Nilsson S, Heinrich D, Helle SI, O'Sullivan JM, Fossa SD, et al.Alpha emitter radium-223 and survival in metastatic prostate cancer. NEngl J Med 2013;369:213–23.
10. Kantoff PW, Higano CS, Shore ND, Berger ER, Small EJ, Penson DF, et al.Sipuleucel-T immunotherapy for castration-resistant prostate cancer. NEngl J Med 2010;363:411–22.
11. de Bono JS, Oudard S, Ozguroglu M, Hansen S, Machiels JP, Kocak I, et al.Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: a rando-mised open-label trial. Lancet 2010;376:1147–54.
12. Omlin A, Pezaro C, Gillessen Sommer S. Sequential use of novel thera-peutics in advanced prostate cancer following docetaxel chemotherapy.Ther Adv Urol 2014;6:3–14.
13. Abidi A. Cabazitaxel: a novel taxane for metastatic castration-resistantprostate cancer-current implications and future prospects. J PharmacolPharmacother 2013;4:230–7.
14. TangenCM,HussainMH,HiganoCS, EisenbergerMA, Small EJ,WildingG,et al. Improved overall survival trends of men with newly diagnosed M1prostate cancer: a SWOG phase III trial experience (S8494, S8894, andS9346). J Urol 2012;188:1164–9.
15. Lorente D, de Bono JS. Molecular alterations and emerging targets incastration resistant prostate cancer. Eur J Cancer 2014;50:753–64.
16. Stanton RA, Gernert KM, Nettles JH, Aneja R. Drugs that target dynamicmicrotubules: a new molecular perspective. Med Res Rev 2011;31:443–81.
Clin Cancer Res; 21(4) February 15, 2015 Clinical Cancer Research806
de Leeuw et al.

17. Mukhtar E, Adhami VM, Mukhtar H. Targeting microtubules by naturalagents for cancer therapy. Mol Cancer Ther 2014;13:275–84.
18. Darshan MS, Loftus MS, Thadani-Mulero M, Levy BP, Escuin D, Zhou XK,et al. Taxane-induced blockade to nuclear accumulation of the androgenreceptor predicts clinical responses in metastatic prostate cancer. CancerRes 2011;71:6019–29.
19. van Soest RJ, van RoyenME, deMorree ES, Moll JM, Teubel W,Wiemer EA,et al. Cross-resistance between taxanes and new hormonal agents abirater-one and enzalutamide may affect drug sequence choices in metastaticcastration-resistant prostate cancer. Eur J Cancer 2013;49:3821–30.
20. Zhu ML, Horbinski CM, Garzotto M, Qian DZ, Beer TM, Kyprianou N.Tubulin-targeting chemotherapy impairs androgen receptor activity inprostate cancer. Cancer Res 2010;70:7992–8002.
21. Sharma A, Yeow WS, Ertel A, Coleman I, Clegg N, Thangavel C, et al. Theretinoblastoma tumor suppressor controls androgen signaling and humanprostate cancer progression. J Clin Invest 2010;120:4478–92.
22. Comstock CE, Augello MA, Goodwin JF, de Leeuw R, Schiewer MJ,Ostrander WF Jr, et al. Targeting cell cycle and hormone receptor pathwaysin cancer. Oncogene 2013;32:5481–91.
23. Sharma A, Comstock CE, Knudsen ES, Cao KH, Hess-Wilson JK, Morey LM,et al. Retinoblastoma tumor suppressor status is a critical determinant oftherapeutic response inprostate cancer cells. CancerRes2007;67:6192–203.
24. Singh RK, Lokeshwar BL. Depletion of intrinsic expression of Interleukin-8in prostate cancer cells causes cell cycle arrest, spontaneous apoptosis andincreases the efficacy of chemotherapeutic drugs. Mol Cancer 2009;8:57.
25. Yang DR, Ding XF, Luo J, Shan YX, Wang R, Lin SJ, et al. Increasedchemosensitivity via targeting testicular nuclear receptor 4 (TR4)-Oct4-inter-leukin 1 receptor antagonist (IL1Ra) axis in prostate cancer CD133þ stem/progenitor cells to battle prostate cancer. J Biol Chem 2013;288:16476–83.
26. Centenera MM, Raj GV, Knudsen KE, Tilley WD, Butler LM. Ex vivo cultureof human prostate tissue and drug development. Nat Rev Urol 2013;10:483–7.
27. Bosco EE, Mayhew CN, Hennigan RF, Sage J, Jacks T, Knudsen ES. RBsignaling prevents replication-dependent DNA double-strand breaks fol-lowing genotoxic insult. Nucleic Acids Res 2004;32:25–34.
28. Burkhart DL, Sage J. Cellular mechanisms of tumour suppression by theretinoblastoma gene. Nat Rev Cancer 2008;8:671–82.
29. Chen JG,YangCP,CammerM,Horwitz SB.Gene expressionandmitotic exitinduced by microtubule-stabilizing drugs. Cancer Res 2003;63:7891–9.
30. Li Y, Li X,HussainM, Sarkar FH. Regulation ofmicrotubule, apoptosis, andcell cycle-related genes by taxotere in prostate cancer cells analyzed bymicroarray. Neoplasia 2004;6:158–67.
31. Villanueva C, Bazan F, Kim S, Demarchi M, Chaigneau L, Thiery-VuilleminA, et al. Cabazitaxel; A novel microtubule inhibitor. Drugs 2011;71:1251–8.
32. Antonarakis ES, Armstrong AJ. Evolving standards in the treatment ofdocetaxel-refractory castration-resistant prostate cancer. Prostate CancerProstatic Dis 2011;14:192–205.
33. Cisternino S, Bourasset F, Archimbaud Y, Semiond D, Sanderink G,Scherrmann JM. Nonlinear accumulation in the brain of the new taxoidTXD258 following saturation of P-glycoprotein at the blood-brain barrierin mice and rats. Br J Pharmacol 2003;138:1367–75.
34. SemiondD, Sidhu SS, BisseryMC, Vrignaud P. Can taxanes provide benefitin patients with CNS tumors and in pediatric patients with tumors? Anupdate on the preclinical development of cabazitaxel. Cancer ChemotherPharmacol 2013;72:515–28.
35. SwantonC,Nicke B, SchuettM, EklundAC,NgC, LiQ, et al. Chromosomalinstability determines taxane response. Proc Natl Acad Sci U S A 2009;106:8671–6.
36. Manning AL, Dyson NJ. pRB, a tumor suppressor with a stabilizingpresence. Trends Cell Biol 2011;21:433–41.
37. Manning AL, Dyson NJ. RB: mitotic implications of a tumour suppressor.Nat Rev Cancer 2012;12:220–6.
38. Manning AL, Yazinski SA, Nicolay B, Bryll A, Zou L, DysonNJ. Suppressionof genome instability in pRB-deficient cells by enhancement of chromo-some cohesion. Mol Cell 2014;53:993–1004.
39. Sung M, Giannakakou P. BRCA1 regulates microtubule dynamics andtaxane-induced apoptotic cell signaling. Oncogene 2014;33:1418–28.
40. Yang D, Chen MB, Wang LQ, Yang L, Liu CY, Lu PH. Bcl-2 expressionpredicts sensitivity to chemotherapy in breast cancer: a systematic reviewand meta-analysis. J Exp Clin Cancer Res 2013;32:105.
41. Inoue T,HiratsukaM,OsakiM, YamadaH, Kishimoto I, Yamaguchi S, et al.SIRT2, a tubulin deacetylase, acts to block the entry to chromosomecondensation in response to mitotic stress. Oncogene 2007;26:945–57.
42. Bonezzi K, Belotti D, North BJ, Ghilardi C, Borsotti P, Resovi A, et al.Inhibition of SIRT2 potentiates the anti-motility activity of taxanes: impli-cations for antineoplastic combination therapies. Neoplasia 2012;14:846–54.
www.aacrjournals.org Clin Cancer Res; 21(4) February 15, 2015 807
Impact of Cabazitaxel on CRPC