Embed Size (px)
Citation preview
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8
ª 2 0 1 8 T H E A U T H O R S . P U B L I S H E D B Y E L S E V I E R O N B E H A L F O F T H E AM E R I C A N
C O L L E G E O F C A R D I O L O G Y F O U N DA T I O N . T H I S I S A N O P E N A C C E S S A R T I C L E U N D E R
T H E C C B Y - N C - N D L I C E N S E ( h t t p : / / c r e a t i v e c o mm o n s . o r g / l i c e n s e s / b y - n c - n d / 4 . 0 / ) .
Novel Electrocardiographic Criteriafor Real-Time Assessment ofAnterior Mitral Line Block“V1 Jump” and “V1 Delay”
Heiko Lehrmann, MD,a Amir S. Jadidi, MD,a Jan Minners, MD, PHD,a Juan Chen, MD,a Björn Müller-Edenborn, MD,a
Reinhold Weber, MD,a Olaf Dössel, PHD,b Thomas Arentz, MD,a Axel Loewe, PHDb
ABSTRACT
ISS
Fro
an
fin
ha
All
ins
vis
Ma
OBJECTIVES This study hypothesized that P-wave morphology and timing under left atrial appendage (LAA) pacing
change characteristically immediately upon anterior mitral line (AML) block.
BACKGROUND Perimitral flutter commonly occurs following ablation of atrial fibrillation and can be cured by an AML.
However, confirmation of bidirectional block can be challenging, especially in severely fibrotic atria.
METHODS The study analyzed 129 consecutive patients (66 � 8 years, 64% men) who developed perimitral flutter
after atrial fibrillation ablation. We designed electrocardiography criteria in a retrospective cohort (n ¼ 76) and analyzed
them in a validation cohort (n ¼ 53).
RESULTS Bidirectional AML block was achieved in 110 (85%) patients. For ablation performed during LAA pacing
without flutter (n ¼ 52), we found a characteristic immediate V1 jump (increase in LAA stimulus to P-wave peak interval in
lead V1) as a real-time marker of AML block (V1 jump $30 ms: sensitivity 95%, specificity 100%, positive predictive value
100%, negative predictive value 88%). As V1 jump is not applicable when block coincides with termination of flutter,
absolute V1 delay was used as a criterion applicable in all cases (n ¼ 129) with a delay of 203 ms indicating successful
block (sensitivity 92%, specificity 84%, positive predictive value 90%, negative predictive value 87%). Furthermore, an
initial negative P-wave portion in the inferior leads was observed, which was attenuated in case of additional cavotri-
cuspid isthmus ablation. Computational P-wave simulations provide mechanistic confirmation of these findings for
diverse ablation scenarios (pulmonary vein isolation � AML � roof line � cavotricuspid isthmus ablation).
CONCLUSIONS V1 jump and V1 delay are novel real-time electrocardiography criteria allowing fast and straightforward
assessment of AML block during ablation for perimitral flutter. (J Am Coll Cardiol EP 2018;4:920–32) © 2018 The
Authors. Published by Elsevier on behalf of the American College of Cardiology Foundation. This is an open access article
under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
P erimitral flutter is a common macro–re-entrantarrhythmia during and after ablation proced-ures in patients with persistent atrial fibrilla-
tion (AF) (1–3). In addition, some centers that follow alow-voltage/substrate-guided ablation approach inpatients with persistent AF, apply “strategic” linear le-sions independent of a macro–re-entrant tachycardia
N 2405-500X
m the aDepartment of Cardiology and Angiology II, University Heart Cente
d the bInstitute of Biomedical Engineering, Karlsruhe Institute of Techno
ancial support from the “Deutsche Forschungsgemeinschaft (DFG)” thro
ve no relationships relevant to the contents of this paper to disclose.
authors attest they are in compliance with human studies committe
titutions and Food and Drug Administration guidelines, including patien
it the JACC: Clinical Electrophysiology author instructions page.
nuscript received November 13, 2017; revised manuscript received March
history (4). Three potential ablation strategies existfor a mitral line: an anterior mitral line (AML), a lateralmitral line or ethanol injection into the vein ofMarshall � additional radiofrequency ablation in theadjacent lateral wall (5,6). Compared with the AML,ablation of the lateral mitral isthmus is associatedwith an increased procedure time and the necessity
https://doi.org/10.1016/j.jacep.2018.03.007
r Freiburg/Bad Krozingen, Bad Krozingen, Germany;
logy (KIT), Karlsruhe, Germany. This study received
ugh CRC 1173. The authors have reported that they
es and animal welfare regulations of the authors’
t consent where appropriate. For more information,
1, 2018, accepted March 6, 2018.
AB BR E V I A T I O N S
AND ACRONYM S
AF = atrial fibrillation
AML = anterior mitral line
CTI = cavotricuspid isthmus
ECG = electrocardiography
IQR = interquartile range
LA = left atrium/atrial
LAA = left atrial appendage
NPV = negative predictive
value
PPV = positive predictive value
PV = pulmonary vein
ROC = receiver-operator
characteristic
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8 Lehrmann et al.J U L Y 2 0 1 8 : 9 2 0 – 3 2 ECG Criteria to Assess Anterior Mitral Line Block
921
for coronary sinus ablation with risk of coronary injury(5,7). The major disadvantage of the AML lies in the“transection” of the anterior left atrium (LA), with aseverely delayed activation of the LA appendage(LAA) and reduced atrial transport function. Becauseof a high prevalence of preexistent low-voltage areasespecially in the anterior and septal parts of the LA incomparison with the lateral LA (8), the AML is never-theless usually the preferred linear ablation target inour hospital in these patients. However, assessmentof bidirectional block with the classical criteria (9,10)can be complex and time consuming in these casesbecause of low amplitude signals in fibrotic tissue.We therefore searched for additional AML blockcriteria utilizing the surface electrocardiography(ECG) to overcome this limitation.
SEE PAGE 933
sinus rhythm
METHODS
PATIENT SELECTION AND PROCEDURAL
DETAILS. From January 2014 to July 2017, data fromconsecutive patients scheduled for LA ablation pro-cedures (paroxysmal and persistent AF), in whom theAML was targeted for ablation (because of perimitralflutter or after a low-voltage or substrate-guidedablation approach), were analyzed. Our ECG criteriawere retrospectively developed (January 2014 toDecember 2016) and checked in a validation cohort(January to July 2017) (Figure 1). The study wasapproved by the Institutional Research Board. Adetailed description of the AF ablation procedure waspublished previously (11). Ablation was performedusing irrigated-tip ablation catheters (ThermoCool/ThermoCool Smarttouch, Biosense Webster, Irvine,California; CoolFlex/Tacticath, St. Jude Medical, St.Paul, Minnesota). Guided by preexistent low-voltageareas (<1.0 mV in sinus rhythm [SR]; <0.5 mV duringAF) (12), the AML was applied between the ante-roseptal mitral annulus and the left superior pulmo-nary vein, a roof line, or the right superior PV (OnlineFigure 1). The endpoint was electrical isolation ofthe PVs and bidirectional block of all applied linearlesions. Block was confirmed using previouslypublished criteria (9,10): 1) widely spaced doublepotentials along the entire line under LAA pacing;2) differential pacing on both sides of the line; and3) mapping of the activation detour during pacingfrom either side of the line.
V1 JUMP AND V1 DELAY CRITERIA. In case of SR atthe time of AML completion, continuous pacingfrom the LAA was performed. The time interval be-tween the pacing stimulus and the maximal positive
deflection of the P-wave in ECG lead V1 wasmonitored (V1 delay). A sudden increase inthis interval was termed “V1 jump” and cor-relation with synchronous bidirectional blockof the AML was assessed. For patients inwhom complete block was achieved, V1 jumpwas defined as the difference between V1
delay directly after block and the shortest V1
delay in the 5 preceding beats. If block couldnot be achieved, we defined V1 jump as thedifference between V1 delay after and beforethe unsuccessful AML ablation in this group.Furthermore, concomitant changes in theP-wave morphology of the inferior ECG leadswere analyzed.
In case of AML ablation during AF or atrialflutter, bidirectional block can precede
termination to SR or occur simultaneously. Underthese circumstances, the V1 jump criterion cannot beassessed. To overcome this limitation, we sought foran absolute V1 delay reflecting bidirectional block.The composition of the analyzed group is outlined inFigure 1.COMPUTER SIMULATIONS. Because of the heteroge-neity regarding ablation targets covered by the studypopulation, we leveraged an in silico approach tomechanistically dissect the differential effects of thelesions. The simulation setup for excitation propa-gation and computation of body surface ECGs hasbeen described and validated previously (13,14). Inbrief, an anatomical model of the torso including theheart, lungs, liver, and kidney was created based onmagnetic resonance imaging data of a healthy subject(47 years of age). The biatrial model was augmentedwith rule-based fiber orientation, interatrial connec-tions (via Bachmann’s bundle, the coronary sinus andposteriorly), and tissue labels to represent anisotropicand heterogeneous excitation propagation (14,15).Compared with Loewe et al. (14), monodomain tissueconductivity was homogeneously reduced to matchV1 delay before AML ablation to that observed in theclinical study population. In silico ablation wasmodeled by rendering the tissue nonconductive.Starting from a reference setup without ablations, PVisolation was performed followed by AMLs that wereconnected with the left superior PV, the right superiorPV, or an additional roof line. Besides successful le-sions, scenarios with a gap in the inferior third of themitral line were investigated. In a second set of sim-ulations, additional cavotricuspid isthmus (CTI)ablation was considered (Online Figures 2 and 3).
STATISTICAL ANALYSIS. Normal distribution ofdata was evaluated by visual assessment of
SR =
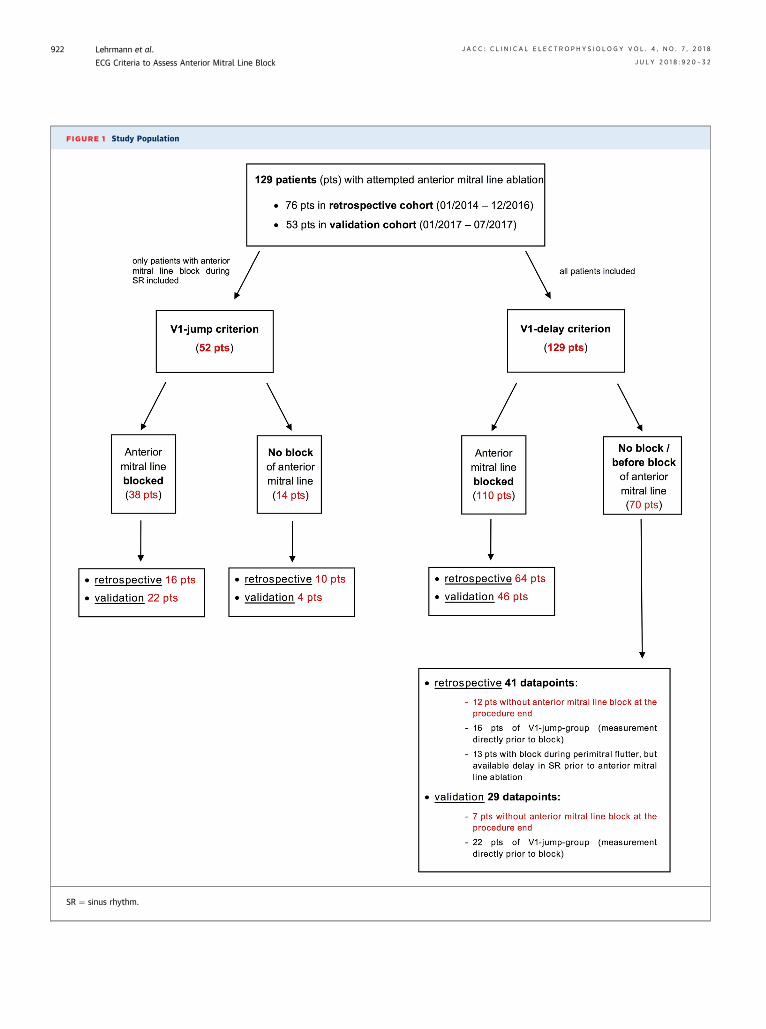
FIGURE 1 Study Population
SR ¼ sinus rhythm.
Lehrmann et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8
ECG Criteria to Assess Anterior Mitral Line Block J U L Y 2 0 1 8 : 9 2 0 – 3 2
922
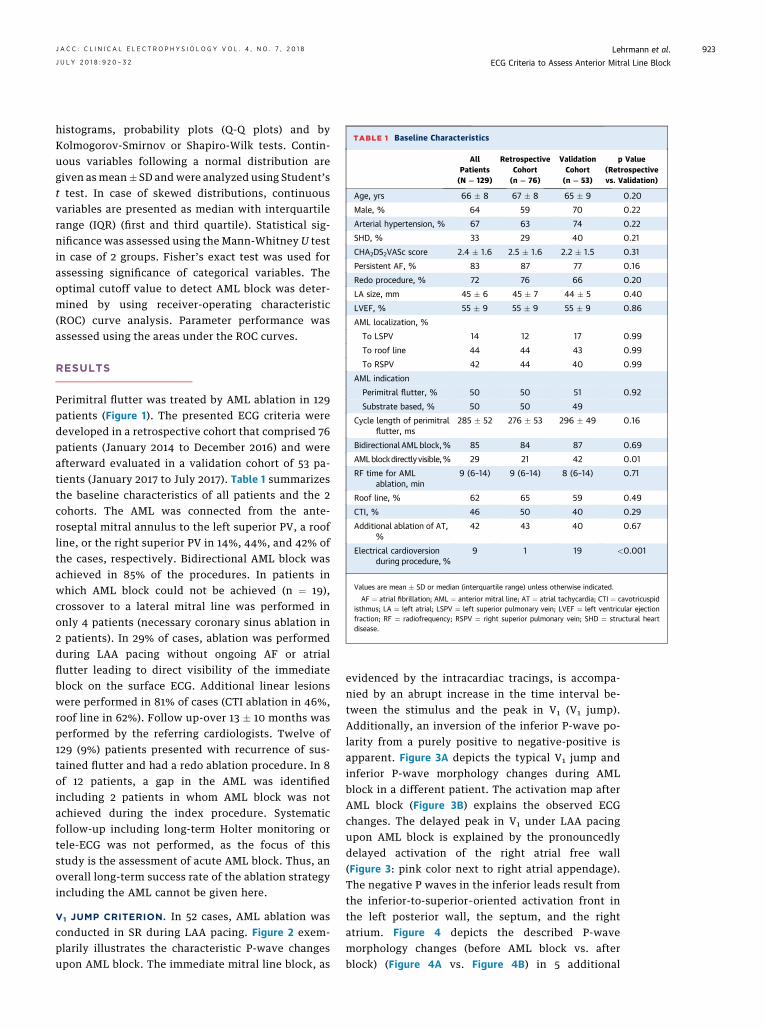
TABLE 1 Baseline Characteristics
AllPatients(N ¼ 129)
RetrospectiveCohort(n ¼ 76)
ValidationCohort(n ¼ 53)
p Value(Retrospectivevs. Validation)
Age, yrs 66 � 8 67 � 8 65 � 9 0.20
Male, % 64 59 70 0.22
Arterial hypertension, % 67 63 74 0.22
SHD, % 33 29 40 0.21
CHA2DS2VASc score 2.4 � 1.6 2.5 � 1.6 2.2 � 1.5 0.31
Persistent AF, % 83 87 77 0.16
Redo procedure, % 72 76 66 0.20
LA size, mm 45 � 6 45 � 7 44 � 5 0.40
LVEF, % 55 � 9 55 � 9 55 � 9 0.86
AML localization, %
To LSPV 14 12 17 0.99
To roof line 44 44 43 0.99
To RSPV 42 44 40 0.99
AML indication
Perimitral flutter, % 50 50 51 0.92
Substrate based, % 50 50 49
Cycle length of perimitralflutter, ms
285 � 52 276 � 53 296 � 49 0.16
Bidirectional AMLblock,% 85 84 87 0.69
AMLblockdirectlyvisible,% 29 21 42 0.01
RF time for AMLablation, min
9 (6–14) 9 (6–14) 8 (6–14) 0.71
Roof line, % 62 65 59 0.49
CTI, % 46 50 40 0.29
Additional ablation of AT,%
42 43 40 0.67
Electrical cardioversionduring procedure, %
9 1 19 <0.001
Values are mean � SD or median (interquartile range) unless otherwise indicated.
AF ¼ atrial fibrillation; AML ¼ anterior mitral line; AT ¼ atrial tachycardia; CTI ¼ cavotricuspidisthmus; LA ¼ left atrial; LSPV ¼ left superior pulmonary vein; LVEF ¼ left ventricular ejectionfraction; RF ¼ radiofrequency; RSPV ¼ right superior pulmonary vein; SHD ¼ structural heartdisease.
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8 Lehrmann et al.J U L Y 2 0 1 8 : 9 2 0 – 3 2 ECG Criteria to Assess Anterior Mitral Line Block
923
histograms, probability plots (Q-Q plots) and byKolmogorov-Smirnov or Shapiro-Wilk tests. Contin-uous variables following a normal distribution aregiven as mean� SD and were analyzed using Student’st test. In case of skewed distributions, continuousvariables are presented as median with interquartilerange (IQR) (first and third quartile). Statistical sig-nificance was assessed using the Mann-Whitney U testin case of 2 groups. Fisher’s exact test was used forassessing significance of categorical variables. Theoptimal cutoff value to detect AML block was deter-mined by using receiver-operating characteristic(ROC) curve analysis. Parameter performance wasassessed using the areas under the ROC curves.
RESULTS
Perimitral flutter was treated by AML ablation in 129patients (Figure 1). The presented ECG criteria weredeveloped in a retrospective cohort that comprised 76patients (January 2014 to December 2016) and wereafterward evaluated in a validation cohort of 53 pa-tients (January 2017 to July 2017). Table 1 summarizesthe baseline characteristics of all patients and the 2cohorts. The AML was connected from the ante-roseptal mitral annulus to the left superior PV, a roofline, or the right superior PV in 14%, 44%, and 42% ofthe cases, respectively. Bidirectional AML block wasachieved in 85% of the procedures. In patients inwhich AML block could not be achieved (n ¼ 19),crossover to a lateral mitral line was performed inonly 4 patients (necessary coronary sinus ablation in2 patients). In 29% of cases, ablation was performedduring LAA pacing without ongoing AF or atrialflutter leading to direct visibility of the immediateblock on the surface ECG. Additional linear lesionswere performed in 81% of cases (CTI ablation in 46%,roof line in 62%). Follow up-over 13 � 10 months wasperformed by the referring cardiologists. Twelve of129 (9%) patients presented with recurrence of sus-tained flutter and had a redo ablation procedure. In 8of 12 patients, a gap in the AML was identifiedincluding 2 patients in whom AML block was notachieved during the index procedure. Systematicfollow-up including long-term Holter monitoring ortele-ECG was not performed, as the focus of thisstudy is the assessment of acute AML block. Thus, anoverall long-term success rate of the ablation strategyincluding the AML cannot be given here.
V1 JUMP CRITERION. In 52 cases, AML ablation wasconducted in SR during LAA pacing. Figure 2 exem-plarily illustrates the characteristic P-wave changesupon AML block. The immediate mitral line block, as
evidenced by the intracardiac tracings, is accompa-nied by an abrupt increase in the time interval be-tween the stimulus and the peak in V1 (V1 jump).Additionally, an inversion of the inferior P-wave po-larity from a purely positive to negative-positive isapparent. Figure 3A depicts the typical V1 jump andinferior P-wave morphology changes during AMLblock in a different patient. The activation map afterAML block (Figure 3B) explains the observed ECGchanges. The delayed peak in V1 under LAA pacingupon AML block is explained by the pronouncedlydelayed activation of the right atrial free wall(Figure 3: pink color next to right atrial appendage).The negative P waves in the inferior leads result fromthe inferior-to-superior–oriented activation front inthe left posterior wall, the septum, and the rightatrium. Figure 4 depicts the described P-wavemorphology changes (before AML block vs. afterblock) (Figure 4A vs. Figure 4B) in 5 additional
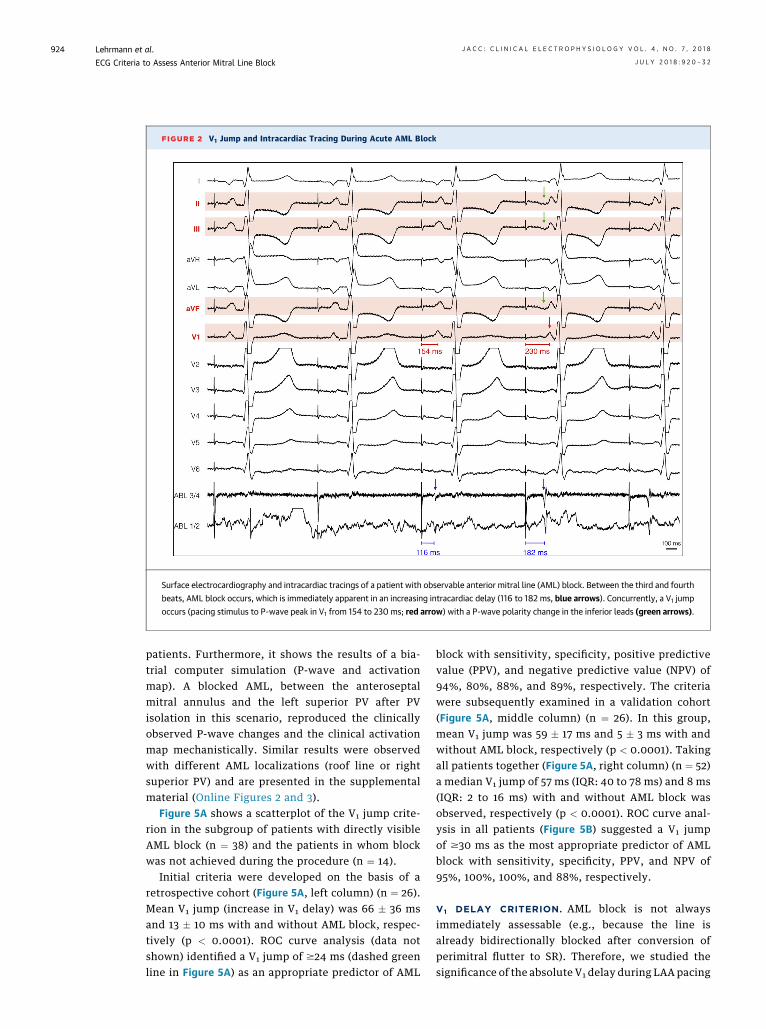
FIGURE 2 V1 Jump and Intracardiac Tracing During Acute AML Block
Surface electrocardiography and intracardiac tracings of a patient with observable anterior mitral line (AML) block. Between the third and fourth
beats, AML block occurs, which is immediately apparent in an increasing intracardiac delay (116 to 182 ms, blue arrows). Concurrently, a V1 jump
occurs (pacing stimulus to P-wave peak in V1 from 154 to 230 ms; red arrow) with a P-wave polarity change in the inferior leads (green arrows).
Lehrmann et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8
ECG Criteria to Assess Anterior Mitral Line Block J U L Y 2 0 1 8 : 9 2 0 – 3 2
924
patients. Furthermore, it shows the results of a bia-trial computer simulation (P-wave and activationmap). A blocked AML, between the anteroseptalmitral annulus and the left superior PV after PVisolation in this scenario, reproduced the clinicallyobserved P-wave changes and the clinical activationmap mechanistically. Similar results were observedwith different AML localizations (roof line or rightsuperior PV) and are presented in the supplementalmaterial (Online Figures 2 and 3).
Figure 5A shows a scatterplot of the V1 jump crite-rion in the subgroup of patients with directly visibleAML block (n ¼ 38) and the patients in whom blockwas not achieved during the procedure (n ¼ 14).
Initial criteria were developed on the basis of aretrospective cohort (Figure 5A, left column) (n ¼ 26).Mean V1 jump (increase in V1 delay) was 66 � 36 msand 13 � 10 ms with and without AML block, respec-tively (p < 0.0001). ROC curve analysis (data notshown) identified a V1 jump of $24 ms (dashed greenline in Figure 5A) as an appropriate predictor of AML
block with sensitivity, specificity, positive predictivevalue (PPV), and negative predictive value (NPV) of94%, 80%, 88%, and 89%, respectively. The criteriawere subsequently examined in a validation cohort(Figure 5A, middle column) (n ¼ 26). In this group,mean V1 jump was 59 � 17 ms and 5 � 3 ms with andwithout AML block, respectively (p < 0.0001). Takingall patients together (Figure 5A, right column) (n ¼ 52)a median V1 jump of 57 ms (IQR: 40 to 78 ms) and 8 ms(IQR: 2 to 16 ms) with and without AML block wasobserved, respectively (p < 0.0001). ROC curve anal-ysis in all patients (Figure 5B) suggested a V1 jumpof $30 ms as the most appropriate predictor of AMLblock with sensitivity, specificity, PPV, and NPV of95%, 100%, 100%, and 88%, respectively.
V1 DELAY CRITERION. AML block is not alwaysimmediately assessable (e.g., because the line isalready bidirectionally blocked after conversion ofperimitral flutter to SR). Therefore, we studied thesignificance of the absolute V1 delay during LAA pacing
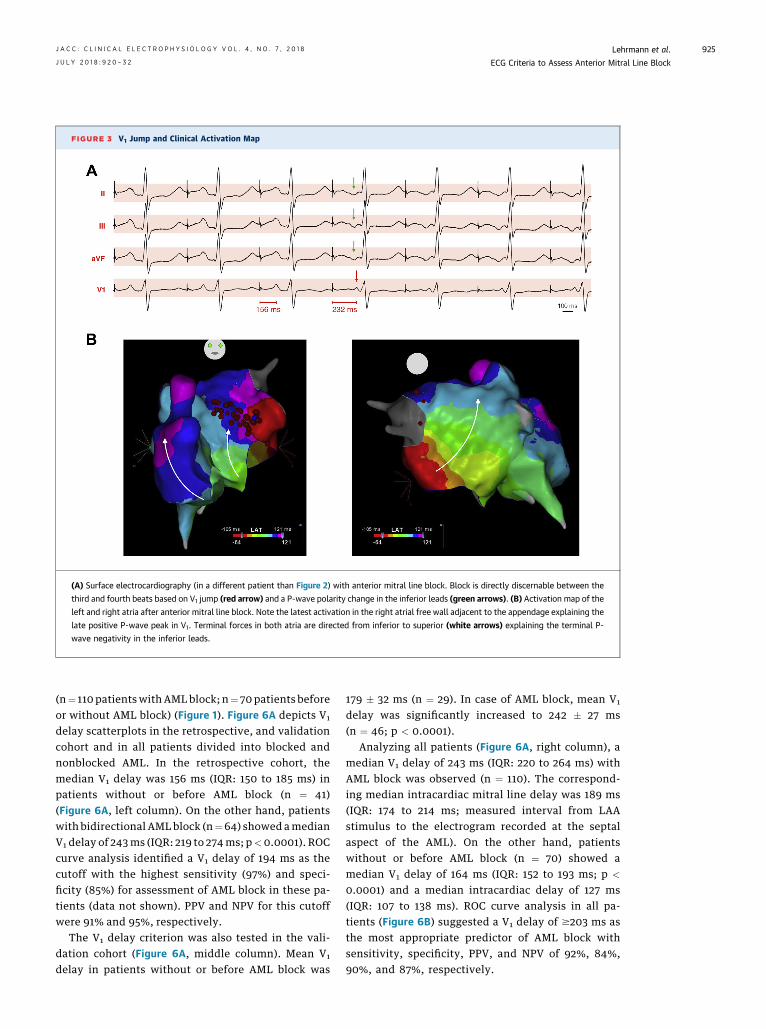
FIGURE 3 V1 Jump and Clinical Activation Map
(A) Surface electrocardiography (in a different patient than Figure 2) with anterior mitral line block. Block is directly discernable between the
third and fourth beats based on V1 jump (red arrow) and a P-wave polarity change in the inferior leads (green arrows). (B) Activation map of the
left and right atria after anterior mitral line block. Note the latest activation in the right atrial free wall adjacent to the appendage explaining the
late positive P-wave peak in V1. Terminal forces in both atria are directed from inferior to superior (white arrows) explaining the terminal P-
wave negativity in the inferior leads.
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8 Lehrmann et al.J U L Y 2 0 1 8 : 9 2 0 – 3 2 ECG Criteria to Assess Anterior Mitral Line Block
925
(n¼ 110 patientswith AML block; n¼ 70 patients beforeor without AML block) (Figure 1). Figure 6A depicts V1
delay scatterplots in the retrospective, and validationcohort and in all patients divided into blocked andnonblocked AML. In the retrospective cohort, themedian V1 delay was 156 ms (IQR: 150 to 185 ms) inpatients without or before AML block (n ¼ 41)(Figure 6A, left column). On the other hand, patientswith bidirectional AML block (n¼64) showed amedianV1 delay of 243ms (IQR: 219 to 274ms; p<0.0001). ROCcurve analysis identified a V1 delay of 194 ms as thecutoff with the highest sensitivity (97%) and speci-ficity (85%) for assessment of AML block in these pa-tients (data not shown). PPV and NPV for this cutoffwere 91% and 95%, respectively.
The V1 delay criterion was also tested in the vali-dation cohort (Figure 6A, middle column). Mean V1
delay in patients without or before AML block was
179 � 32 ms (n ¼ 29). In case of AML block, mean V1
delay was significantly increased to 242 � 27 ms(n ¼ 46; p < 0.0001).
Analyzing all patients (Figure 6A, right column), amedian V1 delay of 243 ms (IQR: 220 to 264 ms) withAML block was observed (n ¼ 110). The correspond-ing median intracardiac mitral line delay was 189 ms(IQR: 174 to 214 ms; measured interval from LAAstimulus to the electrogram recorded at the septalaspect of the AML). On the other hand, patientswithout or before AML block (n ¼ 70) showed amedian V1 delay of 164 ms (IQR: 152 to 193 ms; p <
0.0001) and a median intracardiac delay of 127 ms(IQR: 107 to 138 ms). ROC curve analysis in all pa-tients (Figure 6B) suggested a V1 delay of $203 ms asthe most appropriate predictor of AML block withsensitivity, specificity, PPV, and NPV of 92%, 84%,90%, and 87%, respectively.
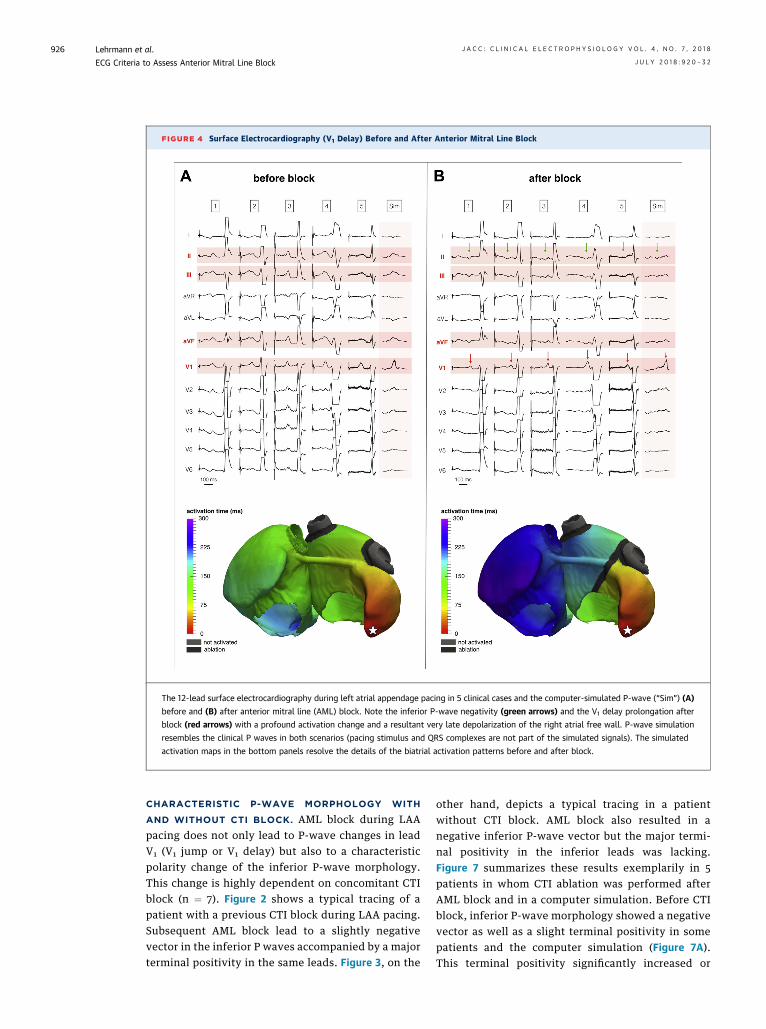
FIGURE 4 Surface Electrocardiography (V1 Delay) Before and After Anterior Mitral Line Block
The 12-lead surface electrocardiography during left atrial appendage pacing in 5 clinical cases and the computer-simulated P-wave (“Sim”) (A)
before and (B) after anterior mitral line (AML) block. Note the inferior P-wave negativity (green arrows) and the V1 delay prolongation after
block (red arrows) with a profound activation change and a resultant very late depolarization of the right atrial free wall. P-wave simulation
resembles the clinical P waves in both scenarios (pacing stimulus and QRS complexes are not part of the simulated signals). The simulated
activation maps in the bottom panels resolve the details of the biatrial activation patterns before and after block.
Lehrmann et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8
ECG Criteria to Assess Anterior Mitral Line Block J U L Y 2 0 1 8 : 9 2 0 – 3 2
926
CHARACTERISTIC P-WAVE MORPHOLOGY WITH
AND WITHOUT CTI BLOCK. AML block during LAApacing does not only lead to P-wave changes in leadV1 (V1 jump or V1 delay) but also to a characteristicpolarity change of the inferior P-wave morphology.This change is highly dependent on concomitant CTIblock (n ¼ 7). Figure 2 shows a typical tracing of apatient with a previous CTI block during LAA pacing.Subsequent AML block lead to a slightly negativevector in the inferior P waves accompanied by a majorterminal positivity in the same leads. Figure 3, on the
other hand, depicts a typical tracing in a patientwithout CTI block. AML block also resulted in anegative inferior P-wave vector but the major termi-nal positivity in the inferior leads was lacking.Figure 7 summarizes these results exemplarily in 5patients in whom CTI ablation was performed afterAML block and in a computer simulation. Before CTIblock, inferior P-wave morphology showed a negativevector as well as a slight terminal positivity in somepatients and the computer simulation (Figure 7A).This terminal positivity significantly increased or
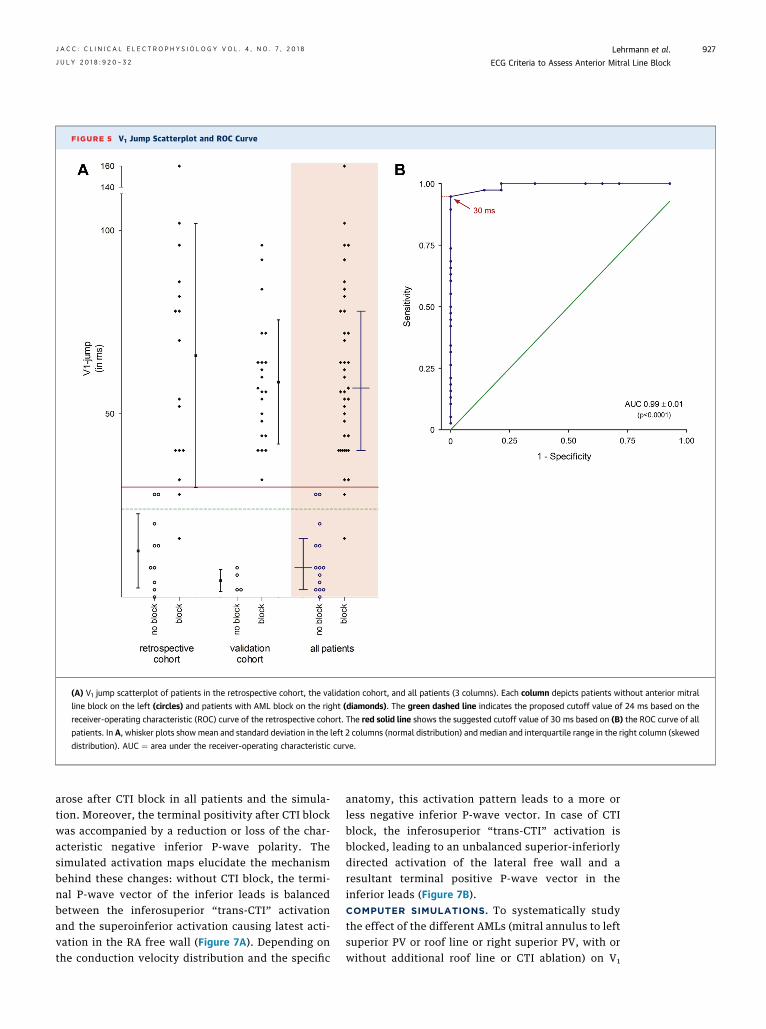
FIGURE 5 V1 Jump Scatterplot and ROC Curve
(A) V1 jump scatterplot of patients in the retrospective cohort, the validation cohort, and all patients (3 columns). Each column depicts patients without anterior mitral
line block on the left (circles) and patients with AML block on the right (diamonds). The green dashed line indicates the proposed cutoff value of 24 ms based on the
receiver-operating characteristic (ROC) curve of the retrospective cohort. The red solid line shows the suggested cutoff value of 30 ms based on (B) the ROC curve of all
patients. In A, whisker plots show mean and standard deviation in the left 2 columns (normal distribution) and median and interquartile range in the right column (skewed
distribution). AUC ¼ area under the receiver-operating characteristic curve.
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8 Lehrmann et al.J U L Y 2 0 1 8 : 9 2 0 – 3 2 ECG Criteria to Assess Anterior Mitral Line Block
927
arose after CTI block in all patients and the simula-tion. Moreover, the terminal positivity after CTI blockwas accompanied by a reduction or loss of the char-acteristic negative inferior P-wave polarity. Thesimulated activation maps elucidate the mechanismbehind these changes: without CTI block, the termi-nal P-wave vector of the inferior leads is balancedbetween the inferosuperior “trans-CTI” activationand the superoinferior activation causing latest acti-vation in the RA free wall (Figure 7A). Depending onthe conduction velocity distribution and the specific
anatomy, this activation pattern leads to a more orless negative inferior P-wave vector. In case of CTIblock, the inferosuperior “trans-CTI” activation isblocked, leading to an unbalanced superior-inferiorlydirected activation of the lateral free wall and aresultant terminal positive P-wave vector in theinferior leads (Figure 7B).COMPUTER SIMULATIONS. To systematically studythe effect of the different AMLs (mitral annulus to leftsuperior PV or roof line or right superior PV, with orwithout additional roof line or CTI ablation) on V1
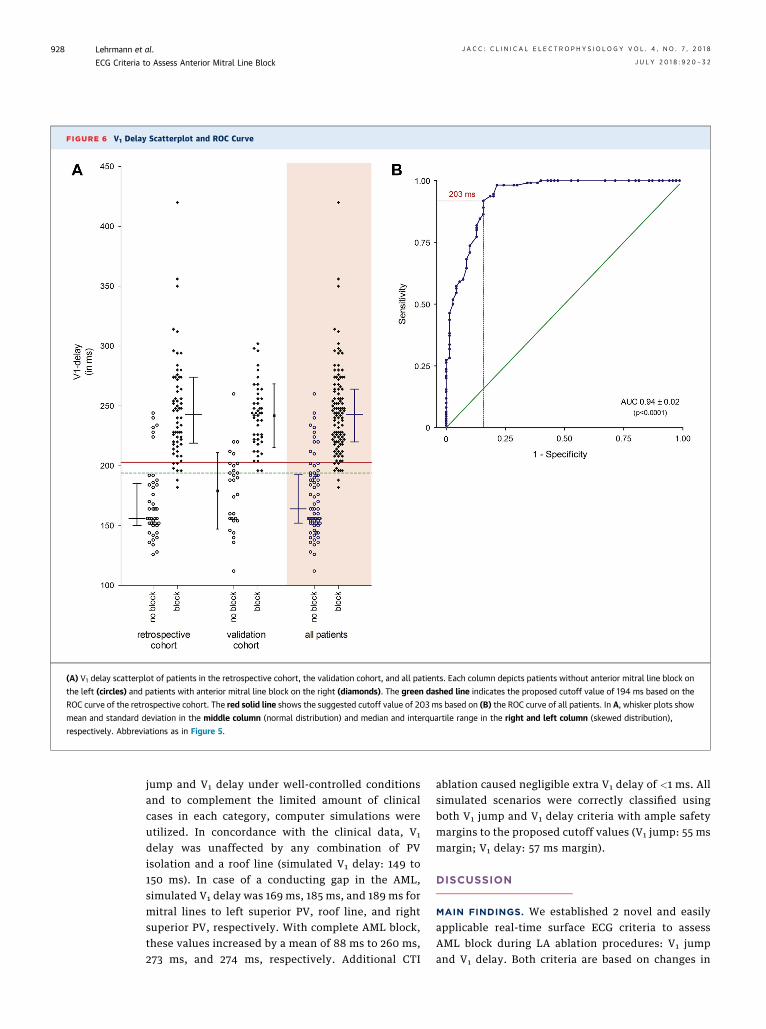
FIGURE 6 V1 Delay Scatterplot and ROC Curve
(A) V1 delay scatterplot of patients in the retrospective cohort, the validation cohort, and all patients. Each column depicts patients without anterior mitral line block on
the left (circles) and patients with anterior mitral line block on the right (diamonds). The green dashed line indicates the proposed cutoff value of 194 ms based on the
ROC curve of the retrospective cohort. The red solid line shows the suggested cutoff value of 203 ms based on (B) the ROC curve of all patients. In A, whisker plots show
mean and standard deviation in the middle column (normal distribution) and median and interquartile range in the right and left column (skewed distribution),
respectively. Abbreviations as in Figure 5.
Lehrmann et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8
ECG Criteria to Assess Anterior Mitral Line Block J U L Y 2 0 1 8 : 9 2 0 – 3 2
928
jump and V1 delay under well-controlled conditionsand to complement the limited amount of clinicalcases in each category, computer simulations wereutilized. In concordance with the clinical data, V1
delay was unaffected by any combination of PVisolation and a roof line (simulated V1 delay: 149 to150 ms). In case of a conducting gap in the AML,simulated V1 delay was 169 ms, 185 ms, and 189 ms formitral lines to left superior PV, roof line, and rightsuperior PV, respectively. With complete AML block,these values increased by a mean of 88 ms to 260 ms,273 ms, and 274 ms, respectively. Additional CTI
ablation caused negligible extra V1 delay of <1 ms. Allsimulated scenarios were correctly classified usingboth V1 jump and V1 delay criteria with ample safetymargins to the proposed cutoff values (V1 jump: 55 msmargin; V1 delay: 57 ms margin).
DISCUSSION
MAIN FINDINGS. We established 2 novel and easilyapplicable real-time surface ECG criteria to assessAML block during LA ablation procedures: V1 jumpand V1 delay. Both criteria are based on changes in
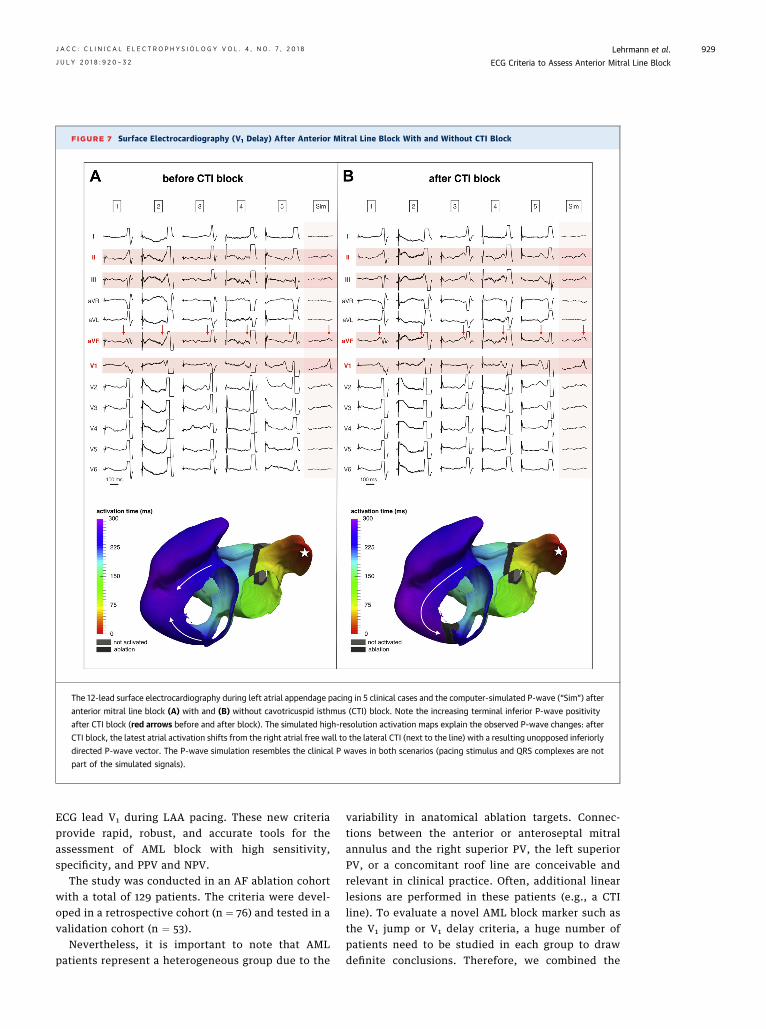
FIGURE 7 Surface Electrocardiography (V1 Delay) After Anterior Mitral Line Block With and Without CTI Block
The 12-lead surface electrocardiography during left atrial appendage pacing in 5 clinical cases and the computer-simulated P-wave (“Sim”) after
anterior mitral line block (A) with and (B) without cavotricuspid isthmus (CTI) block. Note the increasing terminal inferior P-wave positivity
after CTI block (red arrows before and after block). The simulated high-resolution activation maps explain the observed P-wave changes: after
CTI block, the latest atrial activation shifts from the right atrial free wall to the lateral CTI (next to the line) with a resulting unopposed inferiorly
directed P-wave vector. The P-wave simulation resembles the clinical P waves in both scenarios (pacing stimulus and QRS complexes are not
part of the simulated signals).
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8 Lehrmann et al.J U L Y 2 0 1 8 : 9 2 0 – 3 2 ECG Criteria to Assess Anterior Mitral Line Block
929
ECG lead V1 during LAA pacing. These new criteriaprovide rapid, robust, and accurate tools for theassessment of AML block with high sensitivity,specificity, and PPV and NPV.
The study was conducted in an AF ablation cohortwith a total of 129 patients. The criteria were devel-oped in a retrospective cohort (n ¼ 76) and tested in avalidation cohort (n ¼ 53).
Nevertheless, it is important to note that AMLpatients represent a heterogeneous group due to the
variability in anatomical ablation targets. Connec-tions between the anterior or anteroseptal mitralannulus and the right superior PV, the left superiorPV, or a concomitant roof line are conceivable andrelevant in clinical practice. Often, additional linearlesions are performed in these patients (e.g., a CTIline). To evaluate a novel AML block marker such asthe V1 jump or V1 delay criteria, a huge number ofpatients need to be studied in each group to drawdefinite conclusions. Therefore, we combined the
Lehrmann et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8
ECG Criteria to Assess Anterior Mitral Line Block J U L Y 2 0 1 8 : 9 2 0 – 3 2
930
clinical data with biatrial computer simulations toinvestigate each scenario mechanistically and toresolve the underlying mechanisms. In summary, wefound that both criteria are independent of AMLlocalization and additional ablation lines (e.g.,concomitant roof or CTI lines).V1 de lay . Considering both criteria separately, themain strength of the V1 delay criterion lies in its abilityto rapidly evaluate AML block during an ablationprocedure after termination to SR. Thus, it is muchfaster than time-consuming multipoint activationmapping, differential pacing, and a search for doublepotentials, which can be cumbersome due to very low-voltage signals as a result of extensive atrial fibrosis(9,10). In contrast, our new approach, which consistsof simple LAA pacing and surface ECG monitoring, isindependent of intracardiac signal amplitude and cantherefore be rapidly applied even under these cir-cumstances. A limitation of the V1 delay criterion is theremaining overlap between the groups with andwithout AML block. However, the proposed cutoffvalue of 203 ms serves as a good discriminator in themajority of patients according to our data.V1 jump. The V1 jump criterion provides an easilyapplicable real-time tool to assess instantaneous AMLblock during ablation in SR with excellent test char-acteristics. The V1 jump definition in the “no block”cohort was set as the difference in V1 delay directlybefore and after the attempted AML because no real“jump,” but rather a continuously increasing delaywas observed in these patients. Due to this strictdefinition, sensitivity and NPV are presumably evenhigher in practice.COMPARISON WITH PREVIOUS PUBLICATIONS. In2015, Huemer et al. (16) reported their experiencewith AML ablation in SR. They observed an LAAconduction jump of at least 50 ms at the time ofsuccessful AML block (mean 81 ms). Only 1 patientwith a previous AML ablation and subsequent con-duction recovery showed an LAA jump of only 30 ms.These data are in accordance with our results with amedian V1 jump of 57 ms. Furthermore, an additionalroof line did not alter the LAA conduction jump asobserved in our study. Nevertheless, a couple oflimitations apply to the previous study (16): 1) Thereported LAA conduction jump is only applicable ifAML block occurs during ablation in SR. In contrast,we provide a V1 delay cutoff serving as an indicator ofblock even in cases when the AML is already blockedafter termination to SR. 2) The previous work islimited to an AML connecting to the left superior PVwhereas our clinical data and computer simulationscover all AML locations and combinations with otherrelevant lines (roof line, CTI ablation).
STUDY LIMITATIONS. Several limitations need to beacknowledged. First, the reported V1 jump and V1
delay criteria can only assess unidirectional AMLblock (from the lateral to the septal side), althoughall patients in the presented cohort had bidirec-tional block confirmed by the “classical criteria.”Second, the classical criteria were used as the goldstandard for AML block assessment. Although theiruse is fairly straightforward, despite all care, amisclassification can never be completely ruled out.Third, 2 potential limitations of the V1 jump and V1
delay criteria were identified through simulations:1) A completely isolated block of Bachmann’sbundle without AML block led to an activation mapand V1 delay (229 ms) similar to the AML blockscenario; and 2) An AML connecting the mitralannulus to the right superior PV but not affectingBachmann’s bundle did not increase V1 delay uponAML block (149 ms) (Online Figures 2 and 3).Although generally possible, it does not seem to bea desired procedural endpoint because of the riskfor biatrial tachycardia in these cases (17). Of note,both these scenarios were not observed in theclinical cases. Fourth, the diagnostic thresholdstogether with the related values for sensitivity andspecificity as well as NPV and PPV need to beconsidered as specific for our study population. Inthis population, the desired outcome (AML block)was achieved in 85% of patients. The previouslymentioned measures might differ in a populationwith a lower AML block prevalence.
CLINICAL IMPLICATIONS. We currently adhere tothe following protocol in our laboratory: If an AML isattempted during ongoing perimitral flutter, V1 delayis measured immediately after conversion to SR torapidly check for AML block. Hereby, a V1 delayof <203 ms makes AML block unlikely and weimmediately look for gap signals on the whole linewithout performing differential pacing or activationmapping. In case of a remaining AML gap, the V1 jumpcriterion ($30 ms) can then be used as a real-timeindicator of AML block. Moreover, V1 jump can beapplied in patients with a history of perimitral flutteror after a substrate-guided ablation approach withapplication of a “strategic” AML (4), who are ablatedduring SR. Its main advantage lies in its real-timecapability of AML block assessment and is thereforecomparable to the coronary sinus activation reversalduring LAA pacing with lateral mitral isthmus block(10). Real-time AML block detection is particularlyvaluable during ablation, which often obscures theintracardiac signals due to radiofrequency noise. Inthese cases, instantaneous AML block can still be
PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: Our novel sur-
face ECG criteria (V1 jump and V1 delay) provide the practicing
electrophysiologist with a powerful and easy-to-use tool for
AML block assessment during LA ablation procedures. These
new criteria are rapidly applicable, whereas proof of AML block
with the classical block criteria can be challenging and time
consuming, especially in severely diseased or fibrotic left atria
due to low-voltage signals. The new criteria are not meant to
be exclusive, but rather increase the electrophysiologist’s
armamentarium for block assessment (clinical competency:
“procedural skills”). Furthermore, V1 jump, a real-time detector
of AML block, is useful even if intracardiac signals are obscured
due to radiofrequency application noise or in case of severe
atrial fibrosis. This allows for additional ablation time on a
crucial atrial tissue area for long-term consolidation of AML
block (clinical competency: “improved patient care”).
TRANSLATIONAL OUTLOOK: Our collaborative work shows
that combining clinical research with computational modeling
allows easier understanding of an observed clinical phenomenon.
Furthermore, hypothesis testing can be facilitated even in a
complex patient cohort (e.g., patients with different anatomical
AML lines or additional ablation targets). Nevertheless, further
research is desirable to confirm our results in an even bigger
patient cohort.
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8 Lehrmann et al.J U L Y 2 0 1 8 : 9 2 0 – 3 2 ECG Criteria to Assess Anterior Mitral Line Block
931
easily assessed by the V1 jump criterion. This allowsfor additional ablation at this crucial point toconsolidate AML block. Furthermore, reversion of V1
jump (decreasing V1 delay), which can easily berecognized on the surface ECG, serves as a real-timeindicator of conduction recovery across the AMLduring the procedure (Online Figure 4). In addition, asimultaneous negativity in the inferior leads canserve as an additional block marker and is easilyvisualized during the procedure. As mentioned pre-viously, this polarity reversal may be attenuated oreven reversed by CTI ablation.
Finally, 3 points should be emphasized. First, thenew criteria are not meant to be exclusive markersfor block, but rather should be used in conjunctionwith the classical block criteria (9,10). Second, thecurrent study is not intended to promote the AMLapproach above the lateral approach. Both ablationstrategies have their advantages and disadvantages.The major disadvantage of the AML is the “transec-tion” of the anterior LA with a substantially delayedelectrical LAA-activation (in our cohort: median in-terval from LAA potential to QRS onset �10 ms (IQR:�44 to þ8 ms; data not shown), which potentiallyresults in an impaired atrial transport function.Moreover, it must be emphasized that additionalablation of the lateral wall (e.g., crossover to lateralmitral line in case of AML failure) should be avoidedto prevent accidental electrical LAA isolation, whichis associated with higher thromboembolic riskdespite therapeutic oral anticoagulation (18). Third,the current study does not suggest a substrate-guided linear ablation approach in patients withoutperimitral flutter. Whether this improves long-termoutcome has to be shown in prospective multi-center trials. On the contrary, we think that purelyempiric linear lesion sets should be avoided in pa-tients treated for AF, as was shown (e.g., in theSTAR AF II [Substrate and Trigger Ablation forReduction of Atrial Fibrillation Trial-Part II] trial)(19). An important aspect is conduction recovery oflinear lesions during follow-up with a resultant“proarrhythmic” effect (20).
CONCLUSIONS
With the novel V1 jump and V1 delay criteria, AMLblock can easily be assessed during LAA pacing by
monitoring the surface ECG. V1 delay primarilyserves as a sensitive (92%), rapid rule-out criterionfor AML block after termination of perimitral flutterto SR. On the other hand, V1 jump can be used as areal-time indicator of AML block in patients with aremaining AML gap with a high specificity and PPVof 100%. In combination, these criteria provide arapid and accurate tool to evaluate AML blockintraprocedurally.
ACKNOWLEDGMENT The authors would like tothank Dr. Gunnar Seemann for initiating the contactleading to the collaborative research presented here.
ADDRESS FOR CORRESPONDENCE: Dr. HeikoLehrmann, Department of Cardiology and AngiologyII, University Heart Center Freiburg/Bad Krozingen,Suedring 15, 79189 Bad Krozingen, Germany. E-mail:[email protected].

Lehrmann et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8
ECG Criteria to Assess Anterior Mitral Line Block J U L Y 2 0 1 8 : 9 2 0 – 3 2
932
RE F E RENCE S
1. Page RL, Joglar JA, Caldwell MA, et al. 2015ACC/AHA/HRS guideline for the management ofadult patients with supraventricular tachycardia: areport of the American College of Cardiology/American Heart Association Task Force on ClinicalPractice Guidelines and the Heart Rhythm Society.J Am Coll Cardiol 2016;67:e27–115.
2. Matsuo S, Wright M, Knecht S, et al. Peri-mitralatrial flutter in patients with atrial fibrillationablation. Heart Rhythm 2010;7:2–8.
3. Ammar S, Luik A, Hessling G, et al. Ablation ofperimitral flutter: acute and long-term success ofthe modified anterior line. Europace 2015;17:447–52.
4. Kircher S, Arya A, Altmann D, et al. Individuallytailored vs. standardized substrate modificationduring radiofrequency catheter ablation for atrialfibrillation: a randomized study. Europace 2017Nov 21 [E-pub ahead of print].
5. Huemer M, Wutzler A, Parwani AS, et al. Com-parison of the anterior and posterior mitralisthmus ablation lines in patients with perimitralannulus flutter or persistent atrial fibrillation.J Interv Card Electrophysiol 2015;44:119–29.
6. Baez-Escudero JL, Morales PF, Dave AS, et al.Ethanol infusion in the vein of Marshall facilitatesmitral isthmus ablation. Heart Rhythm 2012;9:1207–15.
7. Wittkampf FH, van Oosterhout MF, Loh P, et al.Where to draw the mitral isthmus line in catheterablation of atrial fibrillation: histological analysis.Eur Heart J 2005;26:689–95.
8. Yagishita A, De Oliveira S, Cakulev I, et al.Correlation of left atrial voltage distribution be-tween sinus rhythm and atrial fibrillation:
identifying structural remodeling by 3-D electro-anatomic mapping irrespective of the rhythm.J Cardiovasc Electrophysiol 2016;27:905–12.
9. Shah D, Haissaguerre M, Takahashi A, Jais P,Hocini M, Clementy J. Differential pacing for dis-tinguishing block from persistent conductionthrough an ablation line. Circulation 2000;102:1517–22.
10. Jais P, Hocini M, Hsu LF, et al. Technique andresults of linear ablation at the mitral isthmus.Circulation 2004;110:2996–3002.
11. Arentz T, Weber R, Burkle G, et al. Small orlarge isolation areas around the pulmonary veinsfor the treatment of atrial fibrillation? Resultsfrom a prospective randomized study. Circulation2007;115:3057–63.
12. Jadidi AS, Lehrmann H, Keyl C, et al. Ablationof persistent atrial fibrillation targeting low-voltage areas with selective activation character-istics. Circ Arrhythm Electrophysiol 2016;9:e002962.
13. Krueger MW, Seemann G, Rhode K, et al.Personalization of atrial anatomy and electro-physiology as a basis for clinical modeling ofradio-frequency ablation of atrial fibrillation. IEEETrans Med Imaging 2013;32:73–84.
14. Loewe A, Krueger MW, Holmqvist F, Dossel O,Seemann G, Platonov PG. Influence of the earliestright atrial activation site and its proximity tointeratrial connections on P-wave morphology.Europace 2016;18:iv35–43.
15. Wachter A, Loewe A, Krueger M, Dössel O,Seemann G. Mesh structure-independentmodeling of patient-specific atrial fiber orienta-tion. Curr Direct Biomed Eng 2015;1:409–12.
16. Huemer M, Wutzler A, Parwani AS, et al. Leftatrial appendage conduction jump for real-timeevaluation of conduction block over the anteriormitral annulus line. J Cardiovasc Electrophysiol2015;26:730–6.
17. Mikhaylov EN, Mitrofanova LB, Vander MA,et al. Biatrial tachycardia following linearanterior wall ablation for the perimitralreentry: incidence and electrophysiologicalevaluations. J Cardiovasc Electrophysiol 2015;26:28–35.
18. Rillig A, Tilz RR, Lin T, et al. Unexpectedly Highincidence of stroke and left atrial appendagethrombus formation after electrical isolation ofthe left atrial appendage for the treatment ofatrial tachyarrhythmias. Circ Arrhythm Electro-physiol 2016;9:e003461.
19. Verma A, Sanders P, Macle L, et al. Substrateand Trigger Ablation for Reduction of AtrialFibrillation Trial-Part II (STAR AF II): design andrationale. Am Heart J 2012;164:1–6.e6.
20. Sawhney N, Anand K, Robertson CE,Wurdeman T, Anousheh R, Feld GK. Recoveryof mitral isthmus conduction leads to thedevelopment of macro-reentrant tachycardiaafter left atrial linear ablation for atrialfibrillation. Circ Arrhythm Electrophysiol 2011;4:832–7.
KEY WORDS ablation, anterior mitral line,bidirectional block, P-wave, perimitral flutter
APPENDIX For supplemental figures, pleasesee the online version of this article.





























