-
8/7/2019 notes on CHO metab
1/6
-
8/7/2019 notes on CHO metab
2/6
From the notes of Co-Neil Relato and Kathrina Virtusio Page 2 of
6 Brought to you by the Super Cool Non-Nerdy, Ortigas Study Club
(SCNNOSC) of the UERMMMCI College of Medicine and friends.
DISORDERS OF CARBOHYDRATE (CHO) METABOLISM1.
Hyperglycemia raised plasma glucose
2.
Hypoglycemia decreased plasma glucose3.
Normal or lowered plasma glucose but still with problemsof
glucose metabolism
DIABETES MELLITUS
Chronic metabolic disorder associated with increase bloodsugar
level secondary to reduced insulin or impairedinsulin
utilization
Part of metabolic syndrome (patients with
hyperuricemia,hyperlipidemia, etc.)
Associated with cerebrovascular accidents,
angiopathy,microvascular/cardiovascular (ischemic heart
disease)disease, retinopathies, neuropathy (sensorimotor), andthe
more dreaded renal complication (diabetic nepropathy
chronic renal insufficiency/renal failure);
acceleratedatherosclerosis and hypertension
Etiologic Classification of Diabetes MellitusType 1 (juvenile
type)
Beta cell destruction usually leading to absolute
insulindeficiency
Immune-mediated, idiopathic
Diabetic ketoacidosis (DKA) common
Type 2
May range from predominantly insulin resistance (peripheral
resistance particularly the muscle) with relativeinsulin deficiency
to a predominantly secretory defect withinsulin resistance
DKA NOT common
Gestational DM (GDM)Other Specific Types
Genetic defects of beta cell function
Genetic defects in insulin action
Diseases of the exocrine pancreas
Endocrinopathies*
Drug or chemical-induced*
Infections
Uncommon forms of immune-mediated diabetes
*usual causes
DIAGNOSTIC CRITERIA1. History (history alone or on lab results
alone do NOT suffice; itshould be symptoms plus lab result [* see
next table ])
Symptoms : hunger, thirst, weight loss
Triad: polydipsia, polyuria, polyphagia
LABORATORY CRITERIA FOR DIAGNOSIS OF DM
** random plasma glucose (aka random blood sugar [RBS]); fasting
plasmaglucose (fasting blood sugar [FBS]); post-load glucose
(post-prandial glucose[PPG]); OGTT (oral glucose challenge test
[OGCT])**OGTT: glucose is dissolved in 1 glass of water (to be
consumed in5 minutes) determine glucose level after 2 hours (blood
glucoseshould normally go down after 2 hours) if >200,
possible
diabetes.**The above criteria should be confirmed by repeat
testing on adifferent day. The 3-hour OGTT is NOT recommended for
routineclinical use.
** impaired fasting glucose (IFG); impaired glucose tolerance
(IGT)** Patients with IFG and IGT are NOT immediately labeled
asdiabetic; this only signifies that they are at risk for
developingdiabetes in the future.**OGTT/OGCT: 75 g glucose for
non-pregnant and 100 g glucose forpregnant check glucose level
after 30 minutes, 1 hour, 2 hours,and 3 hours
Laboratory Dx of DM
RBS, FBS
Post prandial blood sugar/ OGTT
Glycosylated Hb monitors efficacy of treatment
Ketone to detect DKA
Urine glucose home monitoring tool (self-test)
Other tests to monitor DM complication
Renal function test: creatinine, Creatinineclearance, BUNUrine
albumin, microalbuminemia: to check forimpending diabetic
nepropathyLipid profileRenal infection screen (urinalysis): DM
patientsprone to renal infection
Random blood sugar
Blood sugar level taken at any time of the day
Values = 45- 130mg/dL or 2.5 to 7.2 mmol/L
Upper limit of 180 mg/dL or 10.0 mmol/L for > 65 year-old
healthy patient is acceptable
Fasting Blood Sugar
Blood sugar level taken after overnight fast (at least 8 hrsor
12-14 hrs recommended; you can actually have FBS inthe afternoon as
long as you have a minimum of 8 hoursfast)
Plasma specimen collected after 12 14 hour fast
-
8/7/2019 notes on CHO metab
3/6
From the notes of Co-Neil Relato and Kathrina Virtusio Page 3 of
6 Brought to you by the Super Cool Non-Nerdy, Ortigas Study Club
(SCNNOSC) of the UERMMMCI College of Medicine and friends.
Overnight fasting glucose concentration between 50 and110 mg/dl
( 2.8 6.2 mmol/l ) accepted normal value
Diabetes mellitus can be dx by:
glucose level >140 mg/dl (7.8mmol/L ) orconsistently elevated
glucose on 2 separateoccasions (e.g. after a month)
2-hour Postprandial Plasma glucose or Post-oral glucose test
Simplest loading test
Measurement of plasma glucose concentration 2 hrs after
the px consumes a load containing 100g of carbohydrate(either in
a sachet or the px is given a meal [i.e. 1 full cupof rice, 2 eggs,
banana, fish or meat, or 2-4 slices of bread])
Screening test in diagnosing GDM
Abnormal: Venous plasma level > 200mg/dl (11.1 mmol/L); 150
gm CHO for 3 daysNO alcohol, unrestricted activity for 3 daysNOT
done after acute illness, surgery, emotionalstress, trauma,
pregnancy, inactivity due tochronic illness, hospitalization10 12
hrs fastingAVOID oral diuretics, contraceptives phenytoinbecause
they have hyperglycemic effect
Loading dose :
Must be consumed within 5 min
Adults = 75 gms
Children = 1.75 gms / kg BW
Pregnant = 100 gms
After drinking, instruct patient to sit down andrest or NOT walk
around too much.
Draw blood
after an 8-hour fast; after extracting the FBS (1 st blood
extraction), give the glucose load.Extract another blood specimen
at 30 (2 nd bloodextraction), 60 (3 rd), and 120 minutes (4 th)
postglucose challengeIntrusive to the patient due to 4
bloodextractions
OGTT CriteriaPlasma Glucose( mmol/L )
Plasma Glucose( mmol/L )
0 min 120 minNon-diabetic 7 >11.1
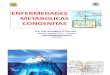
** I think the abscissa should be hours and NOT days.
** normal (blue line): This is a typical behavior of an OGTT of
a non-pregnant patient (75 g). When you give the glucose challenge,
itmaximally increases after 30 minutes to 170-180 and normalizes
tofasting levels at the 2 nd hour and 3 rd hour.** IGT (pink line):
slightly elevated glucose at the fasting level,higher than normal
level at 30 minutes (about 200), and does NOTreturn to normal
limits at the 2 nd and 3 rd hour (still at 160-180).** Diabetic
(yellow): elevated glucose at fasting (140), 250 or >300after 30
minutes, and also does NOT normalize in the 2 nd /3 rd hour.
* Maam did not discuss the details of this table.
**In many laboratories, urine sample is collected at the same
timeas the plasma samples (OGTT).
Advantage correlation between any glycosuria and
thecorresponding plasma glucose levels
Disadvantage cost; another stress for the patient (4
urinesamples are also required together with 4 extractions of
blood)
Impaired Glucose Tolerance
Higher than normal plasma glucose but lower than thediagnostic
values for DM
Precursor for Type II DM (may have preclinical DM)
Only about 25% develop into type II and rest go back tonormal
depending on the persons lifestyle
Patients are more susceptible to macrovascular diseases(i.e.
atherosclerosis)
Similar risk factors as DM II
OGTT Clinical use
Reflex testing for px with borderline FBS (110-140 gm/dl):means
that if the FBS is within this range, the next step inthe algorithm
is OGTT.
Adjunct to diagnose IGT and IFG (as a confirmatory test)
Gold standard for dx of gestational DM
OGTT is NOT indicated in:
Persistent fasting hyperglycemia (> 140 mg/dl )
Persistent fasting normoglycemia(< 110 mg/dl )
Px with s/sx of DM with FBS > 200 mg/dl (this is already
adiagnosis of DM so you do NOT need to confirm it withOGTT)
Secondary DM
Evaluation of reactive hypoglycemia
dx of DM in children (because the reference values arethat of
the adults)
Ancillary TestsUrine Tests (Dipstick Method)
Principle: There is a renal threshold for glucose in the
renaltubules (blood glucose 180 mg/dl). If this value isexceeded,
glucose spills off into the urine.
Diagnostic reagent: glucose oxidase (enzymatic
reagent)impregnated in a strip checks for enzyme reduction of the
glucose
URINE "GLUCOSE"
lacks sensitivity = positivity in diseasepoor specificity =
negativity in health
GLUCOSE LEVEL
0
100
200
300
0 0.5 1 2 3
DAYS
GLUCOSE
NORMAL
IMPAIRED
TOLERANCE
DIABETIC
-
8/7/2019 notes on CHO metab
4/6
From the notes of Co-Neil Relato and Kathrina Virtusio Page 4 of
6 Brought to you by the Super Cool Non-Nerdy, Ortigas Study Club
(SCNNOSC) of the UERMMMCI College of Medicine and friends.
Problems
renal threshold variable 6 to 15 mg/dL thereforelacks
sensitivity and has poor specificityinterferences : Clinitest /
Glucose oxidase stripsif urine test is positive, a confirmatory
blood testis NEEDED; do NOT presume that if the result inthe
dipstick is 1+, then the blood sugar is 180.This is due to the
variability in renal threshold
Glycosylated proteins
Glycosylated haemoglobin (HbA1c)
to monitor blood sugar levels for an extendedperiod of timeto
monitor patient compliance to treatmentregimento monitor adequacy
of blood glucose controlstable; most importanta form of fetal
hemoglobinHbA1c LGI reference range 4.6-6.5%; 6%indicates good
control and level >8% indicatesaction is neededglucose canNOT be
dissociated from hemoglobinso HbA1c indicates cumulative glucose
exposure
for the preceeding 2-3 months (3 months beingthe life expectancy
of a normal RBC)Glucose binds continuously and IRreversibly withHb
during life span of RBC (120 days)Disadvantage: affected by altered
red cellsurvival (canNOT be used inhemoglobinopathies, thalassemia,
haemolyticdse because of shortened RBC survival)If with good
diabetic control, test HbA1c q6months; if poor control, test
quarterly.
Fructosamine
mirrors glycosylation of all serum proteinsindicates previous
2-3 weeks glycaemic exposureused pregnancy/children in some
sites
Glycosylated albuminindicates previous several days
glycaemicexposurenot commonly used
Glycosylated HB (HbA1c)
Indicates average plasma glucose level for 6 to 12 weeks
Clinical use :
monitor diabetic px compliance
a lot of patients cheat blood glucose bydieting for a week
before they aretested; a px canNOT cheat HbA1clevels
index of diabetic control (direct relationship of poor control
and increased complication)predicts development and progression of
microvascular complication
Dietary preparation not required
N: 4 8 % (*Maam said 4-6%)
Can estimate the mean daily glucose level
mean daily carbohydrate (CHO) level in mg/dl =10 x (HbA1c value
+ 4)
Interpretation :
Increased levels implies poor diabetic controlwhen FBS is <
110 mg/dl, HbA1c is normal in 96%of caseswhen FBS is 110-125 mg/dl,
HbA1c is normal in80% of caseswhen FBS is > 126 mg/dl, HbA1c is
normal in>60% of cases
HbA1c in known diabetics
< 7 % indicates good diabetic control
10 % indicates fair diabetic control
13 20 % indicates poor diabetic control
Increased HbA1c levels in:
Presence of HbF (fetal hemoglobin)
Chronic renal failure
Post splenectomy
Iron deficiency anemia
Hypertriglycerenemia
Alcohol, lead and opiate toxicity
Salicylate treatment
Decreased HbA1c levels in:
Shortened RBC life span particularly in hemolytic anemias
Following transfusion
Pregnancy
Ingestion of large amounts of Vit C/E
Hemoglobinopathies
Recommendations of the International Expert CommitteeFor the
diagnosis of diabetes:
The HbA1c is an accurate, precise measure of chronicglycaemic
levels and correlates well with the risk of diabetes
complications
It has several advantages over laboratory measures of
glucose
DM is diagnosed when HbA1c is 6.5 %. Diagnosis should be
confirmed with a repeat HbA1c test. Confirmation isnot required in
symptomatic subjects with plasma glucoselevels >200 mg/dl
(>11.1 mmol/l)
If HbA1c testing is not possible, previously
recommendeddiagnostic methods (e.g., FBG or 2hPPG,
withconfirmation) are acceptable
HbA1c testing is indicated in children in whom diabetes
issuspected but the classic symptoms and a casual plasmaglucose
>200 mg/dl (>11.1 mmol/l) are not found
Clinical implications
HbA1c for diabetes diagnosis offers greater convenienceand
accuracy than glucose measurements and correlateswell withlong-term
complications
HbA1c may be too expensive for routine use in some partsof
world
HbA1c may be influenced by haemoglobin traits andprecluded for
people with conditions that affect red cellturnover (haemolytic
anaemia, chronic malaria)
HbA1c not gold standard for diabetes diagnosis, as nosingle
assay can define the relationship between glucoseand vascular
complications
**Micral Test: to test for microalbuminuria; to detect for
thepresence of early renal nephropathy
-
8/7/2019 notes on CHO metab
5/6
From the notes of Co-Neil Relato and Kathrina Virtusio Page 5 of
6 Brought to you by the Super Cool Non-Nerdy, Ortigas Study Club
(SCNNOSC) of the UERMMMCI College of Medicine and friends.
POC (Point of Care) testing for glucose
Portable, can be used for home testing, physician s officesor
bedside
Uses a refractometer (about the size of a Blackberry)
Uses capillary whole blood
Skin is pricked and blood is put in strip impregnated
withglucose oxidase. The strip is then put into therefractometer
for reading
Principle: glucose oxidase enzymatic method
approximately 10-15% lower glucose readings than
venous sample
Used for immediately monitoring blood glucose levels
should NEVER be used to diagnose DM or hypoglycemicdisorders; it
is only used to monitor blood glucoseparticularly in patients with
DKA and hypoglycemicdisorders
Home glucose monitoring
Require a drop of whole blood obtained by fingerstick tobe
applied to a reagent test strip
After incubation of color development, test is read
byreflectance photometer
Strips usually use a a glucose oxidase enzymatic methodembedded
in the strip
GESTATIONAL DIABETES
**Screening test is 2-hour postprandial glucose test (1 st
step). Whenthe result is abnormal, do reflex confirmatory testing
(OGTT).
**I dont know what values are to be followed. Hindi nya rin
na-mentionwhich one. Pick one nalang. Halos pareho lang naman
hehehe
Other lab tests for CHO disorders: ketone testingKETONE
TESTING
The ketone bodies
beta-hydroxybutyric acidacetoacetic acidacetone which are
products of fatty degradation
(diagnostic substance of choice)
Used in dx of DKA in type I DM
DKA
a serious and potentially fatal hyperglycemiccondition
conversion of excess glucose intoketone bodiesS/Sx: nausea,
vomiting, abdominal pain,electrolyte disturbances, mental
obtundation,ocular disturbances, seizures, and severedehydrationCan
go into coma
* Maam did not discuss the details of this table.
Renal testing in DM
* Maam did not discuss the details of this table.
*Non-diabetic renal disease is suspected when there is absence
of diabetic retinopathy in a person with renal disease, there are
urinaryabnormalities such as haematuria or casts, or when there is
renaldisease without microalbuminuria or proteinuria.
Tests for Diabetic renal disease:
Urinary albumin:creatinine ratio (ACR)
Serum creatinine
Estimated Glomerular Filtration Rate (eGFR) reducedGFR means
there is significant nephron mass loss
Urinalysis , micral test
Note : These tests are performed on px suspected withrenal
complication or if there is proteinuria ormicroalbuminuria
These tests are repeated annually in px with DM
Albumin : creatinine ratio
provides an estimate of daily urinary albumin excretion.
Microalbuminuria cannot be detected on a conventionalurinary
protein dip stick.
-
8/7/2019 notes on CHO metab
6/6
From the notes of Co-Neil Relato and Kathrina Virtusio Page 6 of
6 Brought to you by the Super Cool Non-Nerdy, Ortigas Study Club
(SCNNOSC) of the UERMMMCI College of Medicine and friends.
Microalbuminuria is urinary albumin excretion between 30and 300
mg/day; above 300mg/day representsproteinuria.
ACR is best measured in the laboratory using a firstmorning
urine sample where possible when the patient iswell.
An abnormal initial test requires confirmation by testingon two
further occasions. If at least one of these tests ispositive
microalbuminuria has been confirmed.
Complications of DM:
CVS, renal, micro-angiopathy, retinopathy, neural
Other tests:
Lipid profile: at least annually if stable; if unstable,
q3-4months until levels become stable and 6-12
monthsthereafter.
**It is important that management should be individualised
Parameter Optimal ValueTotal cholesterol < 4 mmol/LLDL
cholesterol < 2.5 mmol/LHDL cholesterol > 1 mmol/LTC:HDL
ratio < 4.5
Triglycerides < 1.7 mmol/LHbA1C < 7 mmol/L
Self-Monitoring blood glucose (SMBG)
People who take insulin should regularly self-monitorblood
glucose
Makes use of a point of care device (i.e. a refractometer)
For people with non-insulin treated type 2 diabetes testingis
most useful if patients use the results to learn and
alterbehaviour, or medication.
...SMBG is most useful if patients use the results to learn,as
part of an overall diabetes education package.
Other tests
Testing of LFTs (liver function test?) is recommended for px
with DM
at diagnosis
at the start of antidiabetic drug therapy
at any other time indicated by clinical judgement
**In patients with type 1 diabetes, intermittent checks for
otherautoimmune conditions may be useful. This could include
testing forthyroid dysfunction or celiac disease.
**usually you give D 10W
HYPOGLYCEMIAClinical classification:
Critical illnesses (can have reactive hypoglycemia)
Hepatic/renal/cardiac failure
Sepsis
Malnutrition
Hormonal deficiencies of
Glucagon, epinephrine, cortisol, growthhormone
Endogenous hyperinsulinism
Pancreatic beta cell disorders
Tumor (insulinoma)
Non-tumor (nesidioblastosis or diffusehyperplasia of the
pancreatic islet cells)
Autoimmune hypoglycemia
Insulin antibodies
Insulin receptor antibodies
Non-beta cell tumors (can present with
non-resolvinghypoglycemia)
Mesenchymal: Fibrosarcoma, mesothelioma,rhabdomyosarcoma,
leiomyosarcoma,liposarcoma, lymphosarcoma,hemangiopericytoma
Carcinomas: Hepatomas, adrenocortical tumors,hypernephroma,
Wilms' tumor
Neurological and neuroendocrine tumors:Pheochromocytoma,
carcinoid tumor,
neurofibroma
Hematologic: Leukemias, lymphoma, myeloma
INSULINOMA
Beta islet cell tumor
Caused by excess and inappropriate secretion of insulin byB cell
tumors
Triad
Hypoglycemic attacks precipitated by fastingPlasma glucose